Embed Size (px)
Citation preview

REMARKABLE EFFECT OF ENDOCRINE THERAPY ON
BRAIN METASTASIS FROM PROSTATIC CARCINOMA
HIRUYUKI SENOH, M.D. HARUHIKO IWATSUBO, M.D. YASUJI ICHIKAWA, M.D. YUICHI KUMAHARA, M.D. MINORU MATSUDA, M.D. SHIRO SAGAWA, M.D.
From the Departments of Urology, Medicine, and Geriatrics, Osaka University Hospital, Osaka, Japan
ABSTRACT- The brain metastasis of prostatic carcinoma is rare and is distinguished by its poor prognosis in ca.sc~s which are not surgically resectable. Herein we report on a case of brain metastasis of prostatic carcinoma which showed a dramatic regression through bilateral orchiectomy and doses (?f diethylstilbe~strol diphosphate and estramustine phosphate. Neurologic and psychiatric symptoms diminished within three months, and the patient is alive and well without any subjective symptoms after twdvc months.
Prostatic adenocarcinoma is one of the most common cancers occurring in men over fift? years of age. Even a small focus of the cancer in the prostate can be biologically active, giving rise to metastases without producing any symp- toms. While widespread metastatic deposits are usual characteristics of the disease, one third of the lesions are visceral, most commonly in the lungs and liver, with lymph node and bone metastases constituting the remaining deposits. l Metastases of prostatic adenocarcinoma in cen- tral nervous system are not frequent, with inva- sion of spinal cord secondary to osseous metas- tasis much more common than involvement of brain or meninges. The incidence of the latter is estimated as approximately 2-4 percent in statistical studies.
Herein reported is a case of prostatic adeno- carcinoma; a brain tumor with Gerstmann syn- drome which showed a dramatic regression through surgical and medical endocrine therap?:
Case Report
On January 24, 1984, a seventy-eight-year- old right-handed man was brought to our hos- pital b!r his family. He had a history of acalculia
for three months, motor aphasia for two months. and confusion for the month prior to his arrival. His past history was not contribu- tory. Physical examination revealed motor aphasia, disorientation, diminished recent memory, spatial disorientation, and construc- tional apraxia. No pathologic reflexes were ob- served. A fixed hard tumor (4.5 x 3.0 cm) was palpable at the right inguinal region. Prostatic carcinoma was suspected after rectal examina- tion revealed an almost normal prostate with a rock hard irregular nodule on right lateral lobe. Laboratory results were normal except for ele- vated serum prostatic acid phosphatase (PAP), 16.0 U/L. Roentgenologic examination re- vealed multiple snowball-like bone metastases in vertebrates, ribs, right femoral head, pelvis, and jat\..
A transrectal needle biopsy was done and diagnosed as moderately differentiated adeno- carcinoma of prostate (Figs. 1, 2). Computer- ized tomographic (CT) scan showed a large enhancing lesion in the left temporal region (Fig. 3A), which was thought to be metastasis of the prostatic cancer. Five hundred mg of diethylstilbestrol diphosphate (DES diphos- phate) per day was prescribed beginning Feb- ruary 15. A bilateral orchiectomy was done on
IlROI.OC~ I I\lANCII 1989 VOLUME XXSIII, A’UMBER 3 243
PAP w/o
15-c
I OS
5.c
I .c
4.5X3cm 3X 1.3cm 2X 1.2cm 0.8 X 0.7cm
UM M M train CT
1 1 1 1 3iopsy Op.
1
yl IO 20 3/l IO 20 4/l IO 20 5/l IO $6 50 (date) *DES: Diethylstilbestrol diphowhate
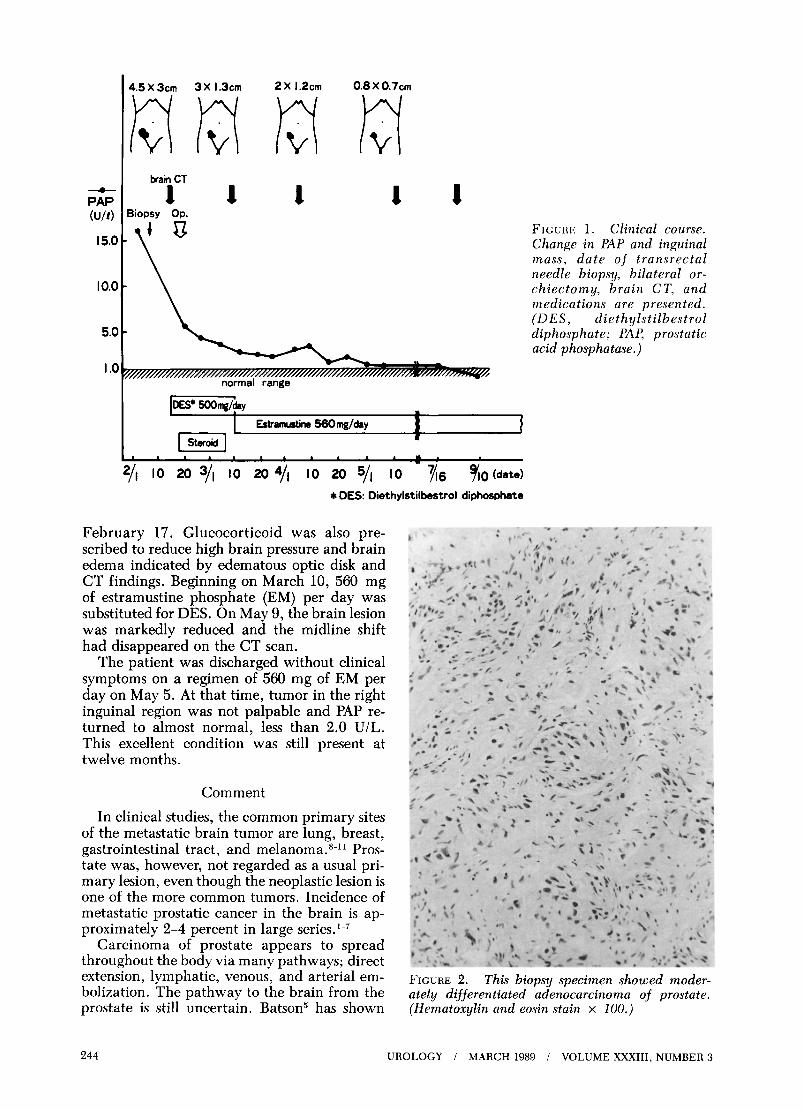
February 17. Glucocorticoid was also pre- scribed to reduce high brain pressure and brain edema indicated by edematous optic disk and CT findings. Beginning on March 10, 560 mg of estramustine phosphate (EM) per day was substituted for DES. On May 9, the brain lesion was markedly reduced and the midline shift had disappeared on the CT scan.
The patient was discharged without clinical symptoms on a regimen of 560 mg of EM per day on May 5. At that time, tumor in the right inguinal region was not palpable and PAP re- turned to almost normal, less than 2.0 U/L. This excellent condition was still present at twelve months.
Comment
In clinical studies, the common primary sites of the metastatic brain tumor are lung, breast, gastrointestinal tract, and melanoma.8-11 Pros- tate was, however, not regarded as a usual pri- mary lesion, even though the neoplastic lesion is one of the more common tumors. Incidence of metastatic prostatic cancer in the brain is ap- proximately 2-4 percent in large series.‘-’
Carcinoma of prostate appears to spread throughout the body via many pathways; direct extension, lymphatic, venous, and arterial em- bolization. The pathway to the brain from the prostate is still uncertain. Batson has shown
FIGURE 1. Clinical course. Change in PAP and inguinal mass, date of transrectal needle biopsy, bilateral or- chiectomy, brain CT, and medications are presented. (DES, diethylstilbestrol diphosphate; PAP, prostatic acid phosphatase.)
FIGURE 2. This biopsy specimen showed moder- ately differentiated adenocarcinoma of prostate. (Hematorylin and eosin stain x 100.)
244 UROLOGY / MARCH 1989 / VOLUME XxX111, NUMBER 3
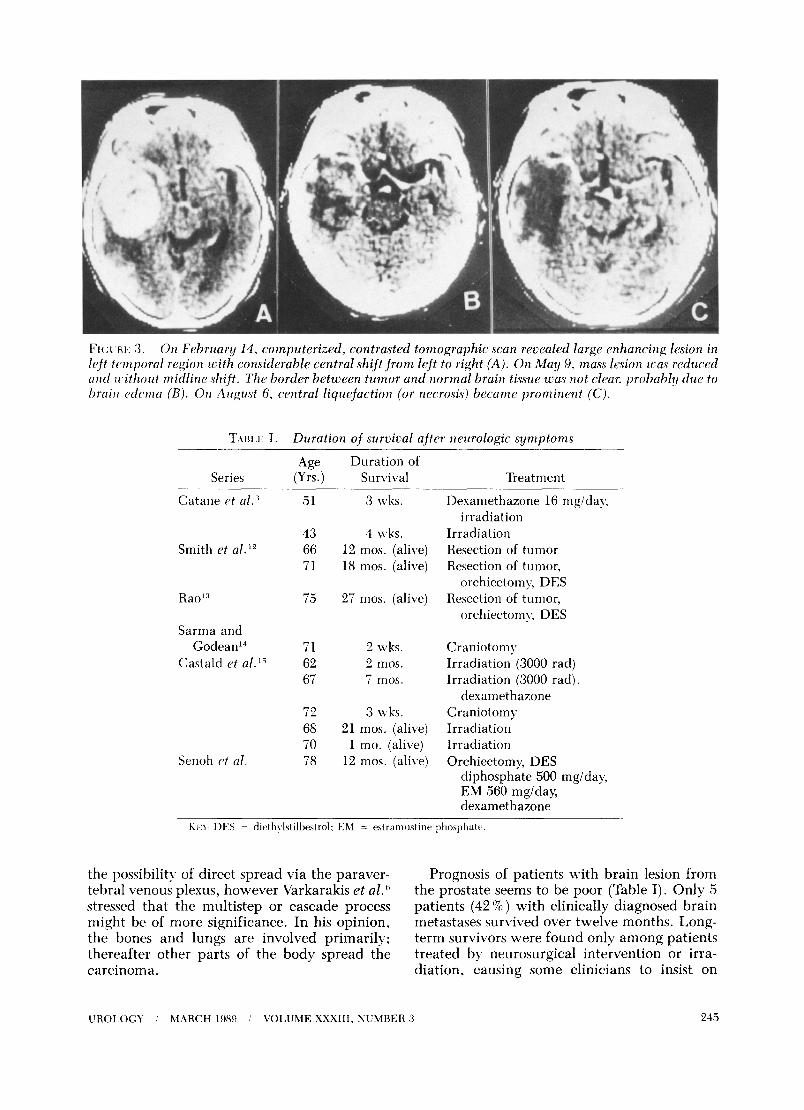
FI(:~.RI~: 3. 0~ Februury 13, computerized, contrasted tomographic Scan revealed large enhancing lesion in left temporal region with considerable central shift from left to right (A). On h4ay 9, mass l&on xas reduced anti without midline shift. The border between tumor and normul brain tissue zL‘a,r not clear. probahl!y due to bruit1 cdcma (B). On Arlgu~t 6. central liquefaction (or necrosis) became prominent (C).
?‘AHI.l~: I. Duration of survival after neurologic symptoms
Series
Catane clt al.”
Smith et a1.12
Rae’:’ 75 27 mos. (alive)
Sarma and Godean14
Castald et al.‘” J
Senoh c? al.
Age (Yrs.)
51
Duration of Survival
3 \vks.
43 4 wks. 66 12 mos. (alive) 71 18 mos. (alive)
71 2 wks. 62 2 mos. 67 7 mos.
72 3 wks. 68 21 mos. (alive) 70 1 mo. (alive) 78 12 mos. (alive)
Treatment
Desamethazone 16 mgiday. irradiation
Irradiation Resection of tumor Resection of tumor,
orchiectomy, DES Resection of tumor,
orchiectomy, DES
Craniotomy Irradiation (3000 rad) Irradiation (3000 rad),
dexamethazone Craniotomy Irradiation Irradiation Orchiectomy, DES
diphosphate 500 mglday, EM 560 mg/day, dexamethazone
- EI~Y DES = dit~th~lstilbestrol: EM = estramustine phosphate.
the possibility of direct spread via the paraver- Prognosis of patients with brain lesion from tebral venous plexus, however Varkarakis et al. 6 the prostate seems to be poor (Table I). Only 5 stressed that the multistep or cascade process patients (42%) with clinically diagnosed brain might be of more significance. In his opinion, metastases survived over twelve months. Long- the bones and lungs are involved primarily; term survivors were found only among patients thereafter other parts of the body spread the treated by neurosurgical intervention or irra- carcinoma. diation, causing some clinicians to insist on
UROI,OCY I MARCII 1989 i VOLUME XxX111, NUMBER 3 245

surgical resection of the tumor when general physical condition of the patient is fair.
The clinical course of this case, however, showed marked effectiveness of hormonal therapy in treating the brain lesion. The blood- brain barrier permeability of drugs could be the key to brain tumor chemotherapy. Regional capillary permeability varied with the ana- tomic location and size of the tumor. Intra- parenchymal tumors less than 1 mm in diame- ter showed no increased permeability. As tumors grew to over 1 mm, their permeability increased proportionally. l6
Osaka, Japan 553 (DR. SENOH)
References
1. Arnheim FK: Carcinoma of the prostate: a study of the post- mortem findings in one hundred and seventy-six cases, J Urol60: 599 (1948).
2. Mintz ER, and Smith GG: Autopsy findings in 100 cases of prostatic cancer, N Engl J Med 211: 479 (1934).
3. Catane R, et al: Brain metastasis from prostatic carcinoma, Cancer 38: 2583 (1976).
4. Rodin AE, Larson DL, and Roberts DK: Nature of the peri- neural space invaded by prostatic carcinoma, Cancer 20: 1772 (1967).
5. Batson OV: The function of the vertebral veins and their role in the spread of metastases, Ann Surg 112: 138 (1940).
6. Varkarakis MJ, et al: Lung metastases in prostatic car- cinoma. Clinical significance, Urolog) 3: 447 (1974).
7. Baker GS, Kernohon JW, and Kiefer EJ: Metastastic tumors of the brain. Surg Clin North Am 31: 1143 (1951).
8. Globus JH, and Meltzer T: Metastatic tumors of the brain. Arch Neurol Psychiatry 48: 163 (1942).
9. Hare CC, and Schwarz GA: Intracerebral carcinomatous metastases, Arch Intern Med 64: 542 (1939).
10. Knights EM Jr: Metastatic tumors of the brain and their relation to primary and secondary pulmonary cancer, Cancer 7: 259 (1954).
11. Lesse S, and Netsky MG: Metastasis of neoplasms to the central nervous system and meninges, Arch Neurol Psychiatry 72: 133 (1984).
12. Smith VC, Kasdon DL, and Hardy RC: Metastatic brain tumor from the prostate. Two unusual cases, Surg Neurol 14: 189 (1980).
13. Rao KG: Carcinoma of prostate presenting as intracranial tumor with multiple cranial nerve palsies, Urology 19: 433 (1982).
14. Sarma DP, and Godean L: Brain metastasis from prostatic cancer, J Surg Oncol 23: 173 (1983).
15. Castald JE, et al: Intracranial metastases due to prostatic carcinoma, Cancer 52: 1739 (1983).
16. Hasegawa H, et al: Change of the blood-brain barrier in experimental metastatic brain tumors, J Neurosurg 59: 304 (1983).
246 UROLOGY / MARCH 1989 / VOLUME XXXIII, NUMBER 3







![Metastatic breast cancer: an unusual cause of …their primary site. Indeed, breast cancer accounts for the highest incidence of metastasis to the orbit, [2,3,5-9] followed by prostatic,](https://img.pdfslide.us/doc/110x75/5ecaf31acc431657a15621be/metastatic-breast-cancer-an-unusual-cause-of-their-primary-site-indeed-breast.jpg)


![Metastasis of Renal Cell Carcinoma to the Bladder · stump, bladder, and prostatic fossa [1,2]. Patients with RCC metastatic to the bladder typically present with gross hematuria](https://img.pdfslide.us/doc/110x75/5e4ab3c0bb39856c894f36dc/metastasis-of-renal-cell-carcinoma-to-the-bladder-stump-bladder-and-prostatic.jpg)