Embed Size (px)
Citation preview

Sleep Apnea: Wake Up to the Problem
Better Sleep for Better Health
Dr. Erin E. Elliott
Awareness Diagnosis
FinancialsTreatment Financialswww.3d-dentists.com
Workflow Success
www.3d-dentists.com
Sleep 101
Understanding the diagnosis
Fatigue reversal and restoration
Memory Psychologic well-being
Biochemical refreshment
Immune function
Functions of SleepHow much sleep do you really need?
Age Sleep Needs
Newborns (0-2 months) 12-18 hours
Infants (3-11 months) 14-15 hours
Toddlers (1-3 years) 12-14 hours
Preschoolers (3-5 years) 11-13 hours
School-age children (5-10 years)10-11 hours (naps end around 6
years old)
Teens (10-17) 8.5-9.25 hours
Adults 7-8 hours
Study of 1.1 million men and women from 30-102 years old
Best survival was 7 hours of sleep
Increased mortality with >8 hours and <6 hours of sleep (15%)
Right Amount of Sleep?
7.7

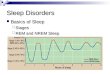
Normal SleepArchitecture
Called a hypnogram
Mainly for BODY restoration
Neuronal rest and repair
Release of essential hormones for growth and recovery
Biologic Functionsof NREM Sleep
Mainly for BRAIN restoration Mood
Biologic Functionsof REM Sleep
Learning 20%Memory
The body is paralyzed
5% of sleep cycle
Transitional stage- 1-7 minutes duration
Easy to awake from
“Drowsy” stage Heart rate begins to slow
Stage 1 (N1)
Deeper stage of sleep with reduction in HR and BP, but still light
45-55% of total sleep time
Most body movements including bruxing
Stage 2 (N2)
Deep sleep or Delta sleep
Hormones and blood sugars regulate 20%
Restorative- growth and rejuvenation
Stage 3 (N3)

REM Sleep
Increase in heart rate, respiration, blood flow, BP
Apnea and hypopnea can increase
Dominates last third of night’s sleep
WHY??
Sympathetic nerves 2x more active as when awake
20%
Insomnia
Repeated difficulty with sleep initiation, duration, consolidation, or quality
10 types
More common in women
Caused by fear, stress, anxiety, medications, poor sleep habits, herbs, caffeine
Finding the cause is usually needed to cure it
Mayo Clinic finding: High correlation between insomnia patients failing pharmaceuticals and undiagnosed OSA
Sleep-RelatedBreathing Disorders
Disordered respiration during sleep
Obstructive Sleep Apnea
Central Sleep Apnea
Primary Snoring
——————->
Upper Airway Resistance Syndrome (UARS)
———————>
Cheyne-Stokes Respiration
Primary Snoring
40% of the population snores
Narrowing of the airway and vibration of the soft tissue
59% of people say their partner snores
With no arousal
25% of married couples are no longer sleeping in the same bedroom
Arousal = Going from a deeper stage of sleep to lighter stage- increased brain waves
Upper Airway ResistanceSyndrome (UARS)
Arousals associated with snoring but no accompanying oxygen desaturation
Arousals lead to sleep fragmentation/disruption and/or sleepiness
RERA’s- Respiratory Effort Related Arousals
Common in young female TMD patients
Central Sleep Apnea

OSA
Complete obstruction of the airway
Hypopnea
Obstructive Sleep Apnea AHIApnea-Hypopnea Index
5-15 mild- must show EDS with ESS15-30 moderate- green light
Apneas + Hypopneas/ # of hours slept
<5 normal- no coverage
>30 severe- CPAP intolerance

Must be >11!!!!!
Epworth Sleepiness Scale
MUST BE >11
CO-MORBIDITIES
EDS HISTORY OF ISCHEMIC HEART DISEASE
HISTORY OF STROKE
DOCUMENTED HYPERTENSION
DOCUMENTED SYMPTOMS OF IMPAIRED COGNITION, MOOD DISORDERS OR INSOMNIA
RDI
Respiratory Disturbance Index
Takes into account RERA’s
Apnea + Hypopnea + RERA’s/ number of hours slept
Oxygen Desaturation
ODI Nadir How much time was spent under 90%?
17-20% of adults have OSA
Up to 80-90% remain undiagnosed
More prevalent than diabetes or asthma
1 in 4 men and 1 in 10 women
50% over the age of 50
Epidemiology
Incidence become = in men and women at menopause age
Sequela: why should we treat this?
Stroke
Optometry
Heart Attacks Hypertension
Obesity
Impotence
Diabetes
Dementia
Periodontal Disease
Auto Accidents
Acid Reflux
Depression
Cancer

Obesity
Obesity is a dominant factor in only 60% of the cases of OSA
Twice as likely to die in men aged 30-70 with severe untreated OSA
Wisconsin Sleep Cohort
Sleep apnea raises risk of dying by 46%
Awareness
Financials
www.3d-dentists.com
Workflow Success Sleep disordered breathingThe dentist’s role in CREATING AWARENESS
Health History
Heart Disease
Glaucoma
Previous Strokes Depression
High Blood Pressure
Diabetes
Headaches
Fibromyalgia? Periodontal Disease
Acid Reflux/GERD

Add Questions
****Change Health History
Do you wear a C-PAP? or have you in the past? Have you been told to?
Do you snore or have you been told you snore?
Have you had a sleep study or been told to get a sleep study?
Have you been diagnosed with sleep apnea?
70% predictive of AHI >5
89% postive predictive of O2 desaturation >4%
ScallopedTongue
Crico-MentalSpace
Overbite
Crico-mental space <1.5mm
Overbite = Positive predictor value of 95% OSA
Pharyngeal grade 2 or greater
Lavigne et al; 2006 n= 13
OAT reduced bruxism by 42%
Bruxing
Kobayashi et al; 2002 n=20
Direct relationship between AHI severity and bruxism severity

MallampatiScore
Class I-IV American Academy of Sleep Medicine 2005
Presence or absence of OSA (Obstructive Sleep Apnea) must be determined before initiating treatment to diagnose and to provide a baseline
Sleep study and/or recommendation from MD
AASM Practice Parameters
STOP MAKING SNOREGUARDS!!!!Awareness Diagnosis
Financials
www.3d-dentists.com
Workflow Success PSG

Saves the insurance company money
Can have the patient “titrated”
An overnight PSG in which the patient is fitted with a C-PAP if they meet criteria
Patient only has to come to the lab once
Split-Night Study
Types II, III, and IV
Must have a Type II or III to be covered by medical insurance
Dependent on how many channels
HST (Home sleep studies)
Can get false negatives
Used often because cheap and accessible
Considered a Type IV device
Only measures pulse and oxygen
Pulse-Oximetry
Accurately predict who and how to treat Awareness Diagnosis
Financials
Financialswww.3d-dentists.com
Workflow Success
Consult- exam 9920X, 3D CBCT 70486/ 76376
Delivery- E0486 (preauth) (physician)
F/U exam 9921X
HST- 95806 (preauth)
Records- N/A
All you need to know
HST- 95806 (preauth)

You will need1) Medical claim form printing- CMS 1500 as a paper claim or electronic claim- Cannot be hand-written
2) ICD diagnosis code made by a physician from the sleep study
3) The sleep study with the diagnosis of OSA from a sleep MD
4) CPT codes (E0486, exam codes, etc)
5) SOAP reports and narratives that the patient was seen by you and is an appropriate candidate for OAT
6) C-PAP Intolerance Form
7) An order (or prescription) for the oral appliance signed by a physician or healthcare provider (MD, DO, ARNP, PA-C)
Awareness Diagnosis
Financials
Treatment Financialswww.3d-dentists.com
Workflow Success Treatment Options
Lifestyle Modifications
Oral Appliance
Positional Therapy Sleep Hygiene
Pharmacological Treatment
Surgery C-PAP
Sleep Hygiene
Avoid big meals No dogs/ pets
Hot shower to cold, dark room
No electronics
7.7 hours of sleep Early to bed, early to rise- same routine every night
Sinus rinses Falls short of being primary treatment
Flonase Nasonex
Pharmacological Treatment
Compliance rate reported as 40-80%*
Continuous Positive Airway Pressure
Different types of masks, tubes, and machines
C-PAP

OAT (Oral appliance therapy)
Practice Parameters
AASM 2006
Sleep study and/or recommendation from an M.D.
Presence or absence of OSA must be determined before initiating treatment to diagnose and to provide a baseline
Practice Parameters
Should be fitted by qualified dental personnel
Trained and experienced in the overall care of oral health, the TMJ, dental occlusion and associated oral structures
Management of patients should be overseen by practitioners who have undertaken serious training in sleep medicine with focused emphasis on the proper protocol for diagnosis, treatment, and follow-up
Practice Parameters-Treatment Objectives
Primary snoring with no OSA
OSA Resolution of clinical signs and symptoms
Normalization of AHI (<5) oxyhemoglobin saturation
Treat snoring to subjectively acceptable level

Practice Parameters
C-PAP is a gold standard
Mild to moderate OSA
Are not appropriate candidates for C-PAP
When patients prefer MADs to C-PAP (new recommendation)
Who do not respond to C-PAP
Fail treatment attempts with C-PAP, weight loss or sleep position change
MAD’s have a more limited use in severe OSA and high BMI
Practice ParametersFollow-upNot indicated in primary snoring
Follow-up PSG with oral appliance in place after final adjustments have been made
Changed to include mild OSA due to data that shows even low AHI is associated with adverse health outcomes
Practice ParametersFollow-upPatients must return for follow-up visits with dentist
Must return to referring physician to assess signs and symptoms of worsening OSA
Compliance, Fit, Occlusion, Patient Alteration
Published in July 2015:
“In the first official joint guideline from the American Academy of Sleep Medicine (AASM) and American Academy of Dental Sleep Medicine (AADSM), oral appliance therapy is recommended for the treatment of adult patients with obstructive sleep apnea (OSA) who are intolerant of continuous positive airway pressure (CPAP) therapy or prefer alternate therapy.”
New Practice Parameters Effectiveness Studies Effective Treatment Oral Appliance C-PAP
Total Population(n=103)
76.5% (39/51)56.9% (29/51)
82.7% (43/52)76.9% (40/52)
Non-severe OSA(n=50)
84% (21/25)84%(21/25)
80% (20/25)80% (20/25)
Severe OSA(n=53)
69.2% (18/26)30.8% (8/26)
85.2% (23/27)74.1% (20/27)
AHI <5 or decrease of 50% and <20 from baseline in a patient with no symptoms
AHI < 5
Good for mild to moderate
Respiration (October 2010)
Conclusion: “There is no clinically relevant difference between MAD and CPAP in the treatment of mild/moderate OSA when both treatment modalities are titrated objectively.”
Effectiveness

Disease Alleviation
FinalOption
Tracheostomy
Oral AppliancesWhat Do I Choose?
Conclusion: A custom-made device turned out to be more effective than a thermoplastic device in the treatment of SBD. Results suggest that the thermoplastic device can’t be recommended as a therapeutic option nor can it be used as a screening tool to find a good candidate for mandibular advancement therapy. [Bold added]
Am J Respir Crit Care Med. 2008 Jul 15

EMA Silent-nite TAP-3 and TAP-3 Elite
Two liners available- Thermacryl and Durasoft
Dream TAP
Herbst
SUAD

Dorsal Fin
Edentulous
Classic (hard acrylic) vs. Flex
DE (Discluding Element) ramp option
Cover distal of mandibular 2nd molars
Elastic hooks- I put on all appliances
Anterior opening option
Acrylic Appliances
Metal reinforcement
Prosomnus (Prosomnus lab only) Optisleep- Sicat Approach:• Can I make a Optisleep? (have the technology, posterior teeth and retention)
• Can I make a Prosomnus?
• Select if small mouth/female, otherwise IA
• Add DE if they are a clencher
• Do I need to make a Herbst (Prosomnus PH)?
• side to side wear pattern
• or insurance mandates
• Somnomed Fusion w Flex liner (dorsal fin) if all else fails
• Great for edentulous areas
• SUAD or SUE- big, strong bruxers that break everything

Prosomnus (IA, CA, PH, Select)- Prosomnus
Sirona- Optisleep
Somnomed- SUAD and Dorsal [email protected]
LabsProtocols
Maybe even someone who struggles with OSA
Trained to do consults, deliveries, adjustments, medical insurance, follow-ups, HST
Financial arrangements
Dental Sleep Medicine Champions
All coordination Someone who has passion and loves to learn
They need help
Works with appeals and denials
Financial arrangements
Track medical insurance payments
Tracks down referrals
Eligibility checks, pre-auths, and submit claims
Scheduling
Consult without sleep study- 4 units
One- Three week check- 3 units- Assistant time
Delivery- 3 units- Assistant time
Consult w/ sleep study & Impressions- 9 units
Impressions- 4 units
Scheduling
One month check- 3 units- Assistant time
Annual check- 3 units- Assistant time
3/6 month check- 3 units- Assistant time

Reviewing Sleep Study
Review AHI or RDI
apneas vs. hypopneas
supine vs. non-supine
Reviewing Sleep Study
Oxygen level
how long <90%?
Nadir
Reviewing Sleep Study
Snoring
Sleep efficiency- “Doc, I didn’t sleep at all”
Sleep stages- any REM?
PLM
Better Candidate
Low BMI
No nasal obstructions
Female CPAP pressure under 10.5
Retrognathic
Positional OSA
Big ROM
Younger More hypopneas vs. apneas
Shallow MP angle
Initial Paperwork
Sample oral appliances
Discussion of their CC and sleep study
Overview of OSA
Treatment options
Consult
Doctor exam- including discussion of previous history
Previous History
Surgeries
Previous oral appliances?
Previous TMJ
Previous sleep studies
C-PAP experience

Patient History
Hours of sleep a night
Exercise Habits
Caffeine Intake
Morning headaches
Dry Mouth
Alcohol Intake
Full Exam
Vital signs- BP and Height and Weight
TMJ- Clinical, palpation, stethoscope
Tooth exam Neck size
Tongue
Periodontal disease Occlusion and Orthodontic Class
Range of Motion
Soft palate and uvula
Jaw relationship
Malampatti score
Nasal exam- Narrow nares? Large turbinates? Septal deviation? Occluded? Mouth breather?
Full Exam
Cottle Maneuver:
If it’s easier, then it is a valve issue. There are no good surgical treatment for this Patient is a good candidate for MUTE
www.breathright.com
www.mutesnoring.com
www.maxairnosecones.com
Nasal Breathing
MUTESNORING.COM/DRELLIOTT
Skeletal and dental classifications
Cone Beam
Location and severity of airway obstructions
Nasal passageways and sinuses
Oral Maxillofacial pathology

Paperwork If no sleep study?
Refer directly to sleep lab for PSG or HSAT
Third party service
Refer to MD
Get diagnosis from a board certified sleep physician
You will need1) Medical claim form printing- CMS 1500 as a paper claim or electronic claim- Cannot be hand-written
2) ICD diagnosis code made by a physician from the sleep study (G47.33)
3) The sleep study with the diagnosis of OSA
4) CPT codes (E0486, exam codes, etc)
5) SOAP reports and narratives that the patient was seen by you and is an appropriate candidate for OAT
6) C-PAP Intolerance Form
7) An order (or prescription) for the oral appliance signed by a physician or healthcare provider (MD, DO, ARNP, PA-C)
What You Will Need:
• Impressions
• Putty/ Wash
• Digital
• Bite
Soak prior to arrival (ONLY IF ACRYLIC)
Check occlusion
Discuss morning exercises and make “chew toy”
Have patient lay back or sit upright in chair with it in for 5 minutes
Adjust- Occlude or Hydent (white) spray
Appointment 3: Delivery Delivery
Go over informed consent again (meaning discuss there may be TMJ pain and a different bite in the morning)
Show the patient how to advance if you feel they can handle it
Instructions

Prodent Clean
WWW.PRODENTCLEAN.COM
Proof of delivery
MorningExercises
“When you wore it, how did it fit?”
Questionnaire Adjustments/try it in
BP/Pulse Epworth
One/two week check
Show them how to advance/ calibrate
BP/Pulse
Experience? Consider calibration HST
Epworth Questionnaire
One-month check
Try to get rid of them (IN THE NICEST WAY POSSIBLE)
BP/Pulse
Build value into these appointments
Consider possible calibration check with HST
Epworth Questionnaire
Three/six -month check

Release on an annual basis
Letter to Physician and copy of HST report
Request for follow-up PSG
Success?
BP/Pulse
Questionnaire/Epworth
Adjustments? Fit? Comfort? Compliance?
CLEAN THE APPLIANCE/Try in
Annual check
SLEEP STUDY
Initial Contact NP Intake Form Medical Insurance Eligibility / Benefit Check
NO Give Medical Biller a
Medical Billing Slip & Write HST Preauth on it
YES Have Pt sign Records
Release Obtain Copy of Sleep
Study no more than 7 years old!
Records CPAP Intolerance Form Records U/L Bite 3D XRay W/ Bite OSA Treatment Consent Medical Billing Slip write “Pre-Auth for
Appliance Delivery Deliver Appliance - Home Care
Instructions Proof of Delivery - AM Aligner Medical Billing Slip - Letter to Pt MD
1 Month Follow Up Adjustment Form Medical Billing Slip Follow Up HST Letter to PT MD
1 Week Follow Up Adjustment Form Medical Billing Slip Letter to PT MD
Initial Consult / HST HST Demo HST Release Form Collect $100 for HST
Sleep Consult / With Sleep Study
Review Sleep Study Test Results
SLEEP CONSULTS Sleep Questions 3D XRay / Air
Segment Photos Review Appliances Go Over Patient
Financial Resp. Letter to PT MD Physician Order Epworth Sleepiness
Scale
HST Review Review
Results Letter to Pt
MD
4 Month Follow Up Adjustment Form Medical Billing Slip Letter to PT MD
6 Step Action Plan:
• #1- Change Health History
• Do you snore? Or have you been told you snore?
• Do you wear a CPAP? Have you in the past? Or have you been told to get one?
• Have you had a sleep study? Or have you been told to get one?
6 Step Action Plan:
• #2- Put Evaluator in each operatory
• Scalloped tongue
• Small airway
• Bruxing/ Wear
• Acid Reflux
6 Step Action Plan:
• #3- Medical Insurance
• Collect cards on EVERY patient
• AND DRIVER’S LICENSE!
• Learn how to do EC (Eligibility Checks)
• Sign up with 3rd party biller

6 Step Action Plan: • #4- Morning Huddle Identification
• Did they check any of the questions?
• Previous nightguards
• Health history
• Hypertension
• Psych meds
• Acid Reflux
• Diabetes
6 Step Action Plan:
• #5- Photos
• Bruxing Wear
• Airway
• 3D
6 Step Action Plan:
• #6- Start talking to patients and get more in depth training
www.joinsleep101.com
fb: erin elliottddstwitter: @erinelliottddsinsty: @erinelliottddslinkedin: Dr. Erin Elliott