Embed Size (px)
Citation preview
European Journal of Obstetrics & Gynecology and Reproductke Biology, 43 (1992) 137- 142 0 1992 Elsevier Science Publishers B.V. All rights reserved 0028-2243/92/$05.00
137
EUROBS 01255
Reliability of urinary LH testing for planning of endometrial biopsies
Antonio R. Martinez ‘, Feja J. Voorhorst ’ and Joop Schoemaker a * Dioision of Reproductiw Endocrinology and Fertiliry, Department of Obstetrics and Gynecology,
and ’ Department of Theory of Medicine and Biostatistics, Free Unillersity Hospital, Amsterdam, The Netherlands
Accepted for publication 9 July 1991
Summary
A rapid urinary luteinizing hormone (LH) test was used to plan a late luteal phase endometrial biopsy from 20 women undergoing an infertility evaluation. Histologic dating was correlated with the day of urinary LH surge detection, the day of the basal body temperature (BBT) nadir, and the onset of the next menstrual period (NMP). From 17 interpretable specimens, histologic dating correlated well with the day of the biopsy as determined following a positive LH test detection (P = 0.079). No correlation was found following the BBT shift (P = 0.651, and it was significantly correlated with the NMP (P = 0.016). Moreover, the urinary LH test showed to be the best method to predict the onset of the NMP. These findings confirm urinary LH testing as a valuable adjunct in the investigation of luteal phase disorders.
Endometrial biopsy; LH test: Luteal phase defect
Introduction
Evaluation of the luteal phase is an important step in the study of infertile couples [ll. Because the endometrial biopsy directly determines the end organ response to the postovulatory milieu, when dated according to the criteria defined by Noyes et al. [2], it has been considered the stan- dard method of assessment of luteal phase ade- quacy. To achieve satisfactory results, it is gener- ally held that the specimen should be taken as
Correspondence: Antonio R. Martinez, M.D., Ph.D.; Depart- ment of Obstetrics and Gynecology, Free University Hospital, P.O. Box 7057, 1007 MB, Amsterdam, The Netherlands.
close as possible to the next menstrual period (NMP) [31.
To plan the endometrial biopsy, the method traditionally used is based on the shift in basal body temperature (BBT). However, the length of the secretory phase can be variable, and it is well known that timing of ovulation by the tempera- ture shift may be in error by up to 4 days [4]. Moreover, assuming that endometrial changes are linked to ovulation in a programmed sequence, a more precise detection of the time of ovulation might contribute to a better interpretation of the postovulatory changes.
In a previous study [5], the efficacy of a rapid urinary luteinizing hormone (LH) test (LH Color”, Organon, Oss, The Netherlands) to de-
138
tect the LH surge and predict the time of ovula- tion, was demonstrated. In the present trial,the accuracy and reliability of the test for planning the endometrial biopsy was investigated. Histo- logic dating of the specimens, as performed by two independent observers, were correlated with the day of LH surge detection, the day of the BBT nadir, and the onset of the NMP. Addition- ally, daily pregnanediol excretion in the postovu- latory phase was measured.
Materials and Methods
Twenty women, aged 24 to 38 years (mean 30.5; SD f 3.5 years), attending the outpatient department of our division, and being scheduled for an endometrial biopsy as part of their infertil- ity work-up, volunteered to participate in the study. All had regular menstrual cycles, as con- firmed by at least three biphasic BBT records. After the fertility investigation had been com- pleted, including semen analysis, postcoital test, screening for sperm agglutinating antibodies, hys- terosalpingography and diagnostic laparoscopy combined with chromopertubation, the cause of the infertility appeared to be related to the male partner in 10 cases; 2 women presented a tubal factor, and 1 suffered from endometriosis. In 7 cases, one of whom complained of habitual abor- tion, no causal factor could be identified, and these were labelled as idiopathic.
Patients entering the study were supplied with the commercially available LH Color test package which contains material for 7 days, testing twice daily. It also includes a leaflet with instructions on test performance and a reference color chart for the interpretation of results. The LH Color test is a qualitative agglutination tube test based on the Sol Particle Immunoassay (SPIA) technol- ogy [6] Urinary LH concentrations above the cut- off level of 50 IU/l will cause, after an incubation period of 30 min, a decoloration of the test solu- tion which is interpreted as positive. According to daily ultrasound monitoring, ovulation has been found to occur approximately 16 to 28 h there- after [5].
The test was performed in early morning (first void) and evening urine samples. The first day of testing was calculated according to individual cy- cle length as advised by the manufacturer follow- ing Mclntosh criteria [7]. Patients carried out the test at home and contacted the hospital when a positive test appeared. Endometrial biopsies were planned accordingly, between 9 to 12 days there- after. Basal body temperature charts were recorded from cycle day 1 onwards. Patients were instructed to consult with the investigator if the temperature record did not show a shift 4 days after the LH peak had been detected, or after the temperature had become elevated and had re- mained so for more than 3 days without a positive test decoloration having been recorded. In the first case the patients were asked to continue testing till the appearance of a new positive read- ing or till a thermal shift of 3 days had been recorded. In the second situation the biopsy would be scheduled 9 to 12 days after the day of the BBT nadir.
The urine specimens used for testing were coded and stored at -4°C and later retested by one of the authors (ARM), being unaware of the patient’s results. In order to avoid interobserver variation, only readings performed by the investi- gator were considered in the analysis of results. In addition, the intraobserver variation was evalu- ated by the investigator, blindly retesting his own findings. Daily 24-h urine collection, for determi- nation of pregnanediol excretion, were started after LH surge detection till the day of the biopsy.
All EBs were performed with a Novak curette in an outpatient setting. A single specimen was attempted to be obtained from the upper part of the fundus of the uterus. After fixation in forma- lin, this was sent to the pathologist. Histological evaluation was performed by two experienced observers independently using the criteria of Noyes et al. [21, both not being informed of the timing of the biopsy. The specimens were dated using the traditional 2-days spread evaluation method. To facilitate statistical analysis, in each case the mean was taken. Cycle day numbers were assigned to the day of the biopsy consider- ing either the day of urinary LH surge detection or the day of the BBT nadir as cycle day 14 and

139
counting forwards; or by considering the day the NMP started as cycle day 29 and counting back- wards.
Data were analyzed by means of paired t-tests, linear regression analysis, and Fisher’s exact test, whenever appropriate.
Results
The occurrence of a urinary LH surge was detected by the investigator in all 20 cycles that entered the study. After retesting his own find- ings there was a complete agreement in 19 (95%) cases, whereas in 1 (5%) case a 12 h difference in the same day urine specimens was observed. When patient’s test readings were compared to the investigator’s results a complete agreement was found in 15 (75%) of the cycles. One (5%) case differed by 12 h, and in other the 2 (10%) cases the difference was of k24 h. Two (10%)
patients were not able to identify the occurrence of a test decoloration.
All studied cycles were ovulatory according to the pregnanediol excretion and biphasic BBT charts. The mean cycle length f SD of the 20 women was 28.3 + 3.0 days with a range of 24 to 34 days (Table I>. The interval from LH peak to onset of menses varied from 11 to 16 days, with a mean of 13.4 + 1.5 days. The interval from BBT shift to onset of menses varied from 9 to 17 days with a mean interval of 13.3 f 2.1 days. The mean of the maximum daily urinary pregnanediol ex- cretion of 15.3 + 5.2 (range 6.4 to 29.4) nmol/l, was seen on day 7.9 k 1.4 (range 5 to 10 days) after the LH peak. There was no correlation between the maximal excretion of pregnanediol and the length of the luteal phase.
The endometrial biopsy could not be per- formed in one patient (No. 20) because menstrual bleeding had started on the day it was scheduled.
TABLE I
Results of the study group when biopsy date was assigned following the day of LH surge detection (LH), day of BBT nadir (BBT),
onset of next menstrual period (NMP) and histologic dating by two observers COBS1 and OBS2)
Pat. No. LH a BBT NMP OBSl 0BS2 Cycle
1 23e 24 25
2 26m 24 26
3 24m 23 24
4 23m 23 26
5 26m 24 25 6 26e 26 28 7 23e 22 25
8 26e 23 25 9 25m 25 25
10 26m 25 24 11 27m 28 27 12 24e 24 24 13 25m 26 25 14 25e 24 26 1.5 27m 29 26 16 25m 22 27 17 23e 23 21 18 25m 25 26 19 24m 25 26 20 25m 25 28
25-26 24-25
26-27 26-27
24-25 24-25 _
23-24
25-26
24-25
26-27
25-26
25-26
25-26
24-25
24-25
25-26
24-25
25-26
25-26
25-26
24-25
23-24
26-27
24-25
23-24
24-25 _
26-27
23-24
26-27
24-25 _
24-25
22-23
26-27
25-26 _
28
33
28
24
29
25
25
27
28
28
32
28
29
26
27
24
33
34
30 27
Mean 24.9 24.5 25.4 25.2 24.9 28.3 SD 1.3 1.8 1.5 1.0 1.1 2.9
’ Evening (e) or morning (m) urine LH test detection.
140
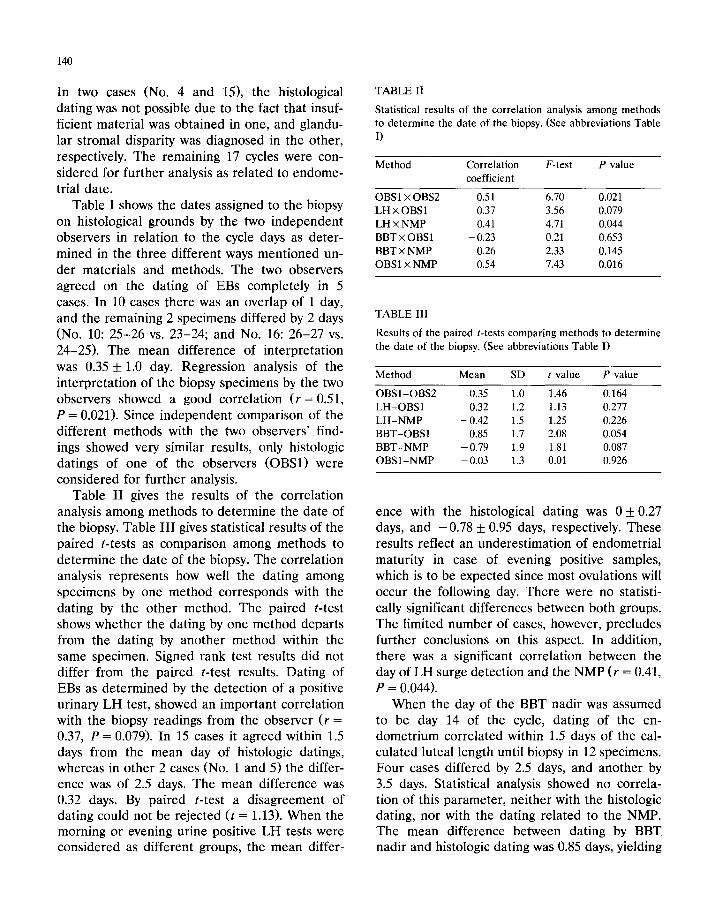
In two cases (No. 4 and 151, the histological dating was not possible due to the fact that insuf- ficient material was obtained in one, and glandu- lar stromal disparity was diagnosed in the other, respectively. The remaining 17 cycles were con- sidered for further analysis as related to endome- trial date.
Table I shows the dates assigned to the biopsy on histological grounds by the two independent observers in relation to the cycle days as deter- mined in the three different ways mentioned un- der materials and methods. The two observers agreed on the dating of EBs completely in 5 cases. In 10 cases there was an overlap of 1 day, and the remaining 2 specimens differed by 2 days (No. 10: 25-26 vs. 23-24; and No. 16: 26-27 vs. 24-25). The mean difference of interpretation was 0.35 * 1.0 day. Regression analysis of the interpretation of the biopsy specimens by the two observers showed a good correlation (r = 0.51, P = 0.021). Since independent comparison of the different methods with the two observers’ find- ings showed very similar results, only histologic datings of one of the observers (OBSl) were considered for further analysis.
Table II gives the results of the correlation analysis among methods to determine the date of the biopsy. Table III gives statistical results of the paired r-tests as comparison among methods to determine the date of the biopsy. The correlation analysis represents how well the dating among specimens by one method corresponds with the dating by the other method. The paired t-test shows whether the dating by one method departs from the dating by another method within the same specimen. Signed rank test results did not differ from the paired t-test results. Dating of EBs as determined by the detection of a positive urinary LH test, showed an important correlation with the biopsy readings from the observer (r =
0.37, P = 0.079). In 15 cases it agreed within 1.5 days from the mean day of histologic datings, whereas in other 2 cases (No. 1 and 5) the differ- ence was of 2.5 days. The mean difference was 0.32 days. By paired t-test a disagreement of dating could not be rejected (t = 1.13). When the morning or evening urine positive LH tests were considered as different groups, the mean differ-
TABLE II
Statistical results of the correlation analysis among methods
to determine the date of the biopsy. (See abbreviations Table
I)
Method Correlation
coefficient
F-test P value
OBSl x 0BS2 -0.51 6.70 0.021
LH x OBSl 0.37 3.56 0.079
LH x NMP 0.41 4.71 0.044
BBT x OBSl - 0.23 0.21 0.653
BBT x NMP 0.26 2.33 0.145
OBSl x NMP 0.54 7.43 0.016
TABLE III
Results of the paired t-tests comparing methods to determine
the date of the biopsy. (See abbreviations Table I)
Method
OBSl-OBM
LH-OBSl
LH-NMP
BBT-OBSl
BBT-NMP
OBSl-NMP
Mean SD t value P value
0.35 1.0 1.46 0.164
0.32 1.2 1.13 0.277
- 0.42 1.5 1.25 0.226
0.85 1.7 2.08 0.054
- 0.79 1.9 1.81 0.087
- 0.03 1.3 0.01 0.926
-
ence with the histological dating was 0 k 0.27 days, and -0.78 + 0.95 days, respectively. These results reflect an underestimation of endometrial maturity in case of evening positive samples, which is to be expected since most ovulations will occur the following day. There were no statisti- cally significant differences between both groups. The limited number of cases, however, precludes further conclusions on this aspect. In addition, there was a significant correlation between the day of LH surge detection and the NMP (r = 0.41, P = 0.044).
When the day of the BBT nadir was assumed to be day 14 of the cycle, dating of the en- dometrium correlated within 1.5 days of the cal- culated luteal length until biopsy in 12 specimens. Four cases differed by 2.5 days, and another by 3.5 days. Statistical analysis showed no correla- tion of this parameter, neither with the histologic dating, nor with the dating related to the NMP. The mean difference between dating by BBT. nadir and histologic dating was 0.85 days, yielding

141
an almost significant difference (t = 2.08). The mean difference between the date of biopsy cal- culated by the BBT nadir and dating calculated in relation to the next menstrual period was 0.79 days. A significant difference could not be ex- cluded (t = 1.81).
Assuming that the onset of menses occurred following the 28th day of the cycle, the dating of the endometrial biopsy specimens agreed with dating by the day of onset of menses up to 1.5 day in 16 cases. The remaining difference being 2.5 days. This difference was not significant (t = 0.01); whereas the correlation between both methods was statistically significant (r = 0.54, P = 0.016).
Discussion
In the present study the clinical usefulness and accuracy of a rapid urinary LH test for planning the endometrial biopsy was evaluated. A positive test, reflecting urine LH concentrations above 50 IU/I, was detected in all cycles when tests were performed by the investigator. The low intraob- server variation after rechecking of his own find- ings suggests a high reproducibility of results when performed by an experienced examiner. The missed LH surges and discrepancies observed in the patients results could be related to less de- fined test decolorations and/or lack of experi- ence of the patient to perceive more subtle color changes.
In 17 cases where the endometrial biopsy could be dated, a high correlation between the results of both observers was found. This confirms the accuracy of the procedure itself. The biopsies were planned either from the day after LH surge detection or from the BBT shift through the day prior to menses. Using the LH surge detection as the reference point proved to result in a more precise prediction of the date of the NMP than the BBT nadir. The wide variation of the BBT nadir around the LH surge has previously been reported [41, and corroborates its inaccuracy in estimating the day of ovulation. Moreover, the low correlation with histologic dating precludes its use as a method for the diagnosis of luteal phase insufficiency.
The urinary LH test showed to be an accurate method to predict the onset of the NMP. The biopsy therefore should be planned according to this parameter. The high correlation between the histologic method of determining the day of ovu- lation with the day of the midcycle LH peak, as measured in plasma or urine, has been already reported [8,91. The small range of the days at which the biopsies were taken in this study, how- ever, does not allow reliable conclusions on this aspect other than for late luteal phase biopsies. A much wider range of postovulatory days at which biopsies are taken would be necesary to reliably correlate the endometrial dates to the day of LH surge detection.
Given the fact that no cases of corpus luteum insuficiency were recorded, dating of the en- dometrium as calculated from the onset of NMP showed the best correlation in this study. Whether dating of endometrial biopsies as related to uri- nary LH test detection will contribute to improve the accuracy in the diagnosis of luteal phase insuffiency need to be further investigated. Nev- ertheless, cases with a ‘short’ luteal phase (< 11 days) [l] can be better confirmed with this method. These findings confirm urinary LH testing as a reliable method to be used for the study and management of luteal phase disorders.
Acknowledgement
This study was supported by Organon Interna- tional, Oss, The Netherlands.
References
1 McNeely MJ, Soules MR. The diagnosis of luteal phase
deficiency: a critical review. Fertil Steril 1988;50:1-15.
2 Noyes RW, Hertig AT, Rock J. Dating the endometrial
biopsy. Fertil Steril 1950;1:3-25.
3 Rosenfeld DL, Chodow S, Bronson RA. Diagnosis of luteal
phase inadequacy. Obstet Gynecol 1980;56:193-196.
4 Quagliarello J, Arny M. Inaccuracy of basal body tempera-
ture charts in predicting urinary luteinizing hormone surges,
Fertil Steril 1986;45:334-337.
5 Martinez AR, Bernardus RE, Kucharska D, Schoemaker J.
Urinary luteinizing hormone testing and prediction of ovu-
lation in spontaneous, clomiphene citrate and human
menopausal gonadotropin stimulated cycles. A clinical eval-
uation. Acta Endocrinol 1991:124:357-363,

142
6 Bosch AMG, Leuvering JHW, Stevens JHM, V Buul CPJJ,
White DD. Sol particle immunoassays for polypeptide hor-
mones. Prog Clin Biol Res 1988;285:201-203.
7 McIntosh JFA, Matthews CD, Cracker JM, Broom TJ, Cox
LW. Predicting the luteinizing hormone surge: relationship
between the duration of the follicular and luteal phases and
the length of the human menstrual cycle. Fertil Steril
1980;34:125-130.
8 Li T, Rogers AW, Lenton EA, Dockery P, Cooke Ian. A
comparisson between two methods of chronological dating
of human endometrial biopsies during the luteal phase, and
their correlation with histologic dating. Fertil Steril
1987;48:928-932.
9 Johannisson E, Landgren BM, Rohr HP, Diczfalusy E.
Endometrial morphology and peripheral hormone levels in
women with regular menstrual cycles. Fertil Steril
1987;48:401-408.