Embed Size (px)
Citation preview

198
THE RELATIONSHIP BETWEEN THESERUM LIPIDS AND THE DEVELOPMENT
OF ISCHAEMIC HEART DISEASEBy B. BRONTE-STEWART, M.D., M.R.C.P.
Clinical Nutrition Research Unit, Department of Medicine, University of Cape Town
TABLE I.-DISTR::BUTION OF CHOLESTEROL BETWEEN THE LIPOPROTEIN ]FRACTIONS(Adapted from Barr (I953), and other data)
Total cholesterol Alpha Betamg. per ioo ml. % %
Dog:Normal . .. .. 210 83 17With atheroma .. .. 2,000 6 94
Rabbit:Normal .. .. .. 51 53 47With atheroma .. .. 2,000 9 91
Human:At birth .. .. 65 43 57American female (18-35 yrs.) 187 34 66
(45-65 yrs.) 252 24 76Bantu male (40-49 yrs.) x68 28 72American male (18-35 yrs.) 197 25 75
(45-65 yrs.) 239 22 78With ischaemic heart disease .. 259 14 86
iMuch of the research on ischaemic heart diseasetoday throughout the world is concerned solelywith changes in the serum lipids. In certaininstances, hypotheses on the pathogenesis ofischaemic heart disease have been founded merelyon such changes. It becomes, then, a matter ofparamount importance to examine how closelythis relationship exists, and on its closeness willdepend the validity of many of the hypothesespropounded.Few will doubt the very close relationship that
exists in the experimental animal between changesin the serum lipids and the development of athero-sclerosis. This has been known for nearly half acentury (Anitschkow, 1933). During the courseof the experiment, the serum. usually would be-come lipaemic with a rapid rise in the serum-cholesterol level and an alteration in the distribu-tion of the serum cholesterol between the twolipoprotein fractions, in that a greater proportionof the cholesterol would be found in the beta frac=tion and less in the alpha fraction. The higherthe cholesterol level, the more rapidly wouldatherosclerosis ensue. In these acute short-termexperiments, if the serum-cholesterol level did notbecome elevated in one of the group no athero-sclerosis would be seen in that par'ticular animal.
The resultant arterial lesion had certain similaritieswith atheroma in man but certain features werelacking and, due largely to the concomitant grosshypercholesterolaemia and organ lipoidosis, appli-cation of such experiments to the problem ofatherosclerosis in man became a controversialissue. The experiments were designed to beshort-term, a situation hardly analagous to that inman, and, furthermore, although occlusion of thesmaller intramuscular branches of the coronaryarteries occurred and occasionally areas of fibrosiswere seen in a patchy distribution throughout themyocardium, no lesion typical of myocardial in-farction could be produced by these means.The position in man is less clear, however. In
certain diseases, such as diabetes mellitus andessential xanthomatosis, a disordered fat meta-bolism exists and there is an increased tendencytowards severe atherosclerosis and a higher incidence of ischaemic heart disease. The lipidmetabolic derangement resembles that seen inpatients affected by ischaemic heart disease. This,added to the great accumulation of data fromclinical, epidemiological and experimental sources,could suggest that ischaemic heart disease resultsfrom a disorder in fat metabolism. Much of this,unfortunately, is based or associations and extra-
by copyright. on F
ebruary 21, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.402.198 on 1 A
pril 1959. Dow
nloaded from

April 1959 BRONTE-STEWART: Relationship Between Serum Lipids and Ischaemic Heart Disease I99
polations, and parallelism of trends need notindicate causal connection. In addition, the termsatherosclerosis and ischaemic heart disease havebeen used synonymously, as it is generally assumedthat the latter arises on the basis of the former.Certain data indicate that this may not be so,which could suggest that mechanisms underlyingthe development of the one may not be commonto the development of the other.Serum Lipid Abnormalities in Patients withIschaemic Heart DiseaseOral Fat Tolerance TestThere are several studies now to show that the
lipaemia following the feeding of a standard fatmeal is more intense and more prolonged inpatients than in age-matched controls (Barritt,I956; Bronte-Stewart and Blackburn, I958). Evenin the fasting state the patients have a greateropalescence of the serum. Usually, considerableoverlap between patient and control groups occurs,and it is not until late in the lipaemic phase thatthe differences become statistically significant.Due to this, it has been claimed that the patientslack a sufficiency of the clearing factor, and thisclaim has been substantiated by certain experi-ments using heparin to activate the clearingmechanism (Oliver and Boyd, 1953). Others,however, have been unable to confirm this viewand have found that the heparin-activated clearingmechanism and the respective plasma lipid sub-strates are similar in both affected and unaffectedindividuals (Mitchell and Bronte-Stewart, 1959).The significance of these findings of oral fattolerance tests has yet to be elucidated as thelipaemic response to the same fat in the same in-dividual is very variable and may be dependent onthe amount and nature of the dietary fat intakeprior to the test (Pomeranze et al., 1954; Bronte-Stewart and Blackburn, 1958).Cholesterol Lipoprotein SystemThe most publicized metabolic difference be-
tween affected and unaffected individuals concernsthe cholesterol lipoprotein complex in the serum.Fats, as such, are insoluble in blood serum or otherwatery media in the body, whereas lipoproteins arereadily soluble. To be absorbed and transportedabout the body, fats must be combined withcholesterol and proteins in the soluble form oflipoproteins. When these lipoproteins are es-timated by means of the ultracentrifuge, affectedindividuals have higher values of the low-densitybeta lipoproteins of flotation rates Sf I2-20 and35-I00, and from the values can be calculated anintricate index, called the atherogenic index, whichhas been claimed to indicate the presence of thedisease (Gofman et al., 1954). Electrophoretically,two major lipoprotein classes occur, the alpha or
faster migrating component, and the beta. Bothfractions contain cholesterol, cholesterol ester,phospholipid, triglyceride and protein, but theyare present in different proportions.The serum lipoprotein pattern is different in
different species, and in man is influenced by bothage and sex (Table I). Individuals affected withischaemic heart disease have a higher beta-lipopro-tein and a lower alpha-lipoprotein level than age-matched controls. As the alpha fraction containsmore phospholipid than the beta fraction, this isthought to be the explanation for the highercholesterol-phospholipid (C/P) ratio found in theserum of affected individuals (Gertler and White,1954). Recently, attention has been focused on afaster-moving component in the beta-lipoproteinfraction, called the pre-beta lipoprotein, and thisfraction has been noted as a transient phenomenonin the early weeks following myocardial infarction(Smith, I957).
Far greater emphasis has been placed on themore easily estimated serum cholesterol. As yetthere is no evidence to contradict its use as areflector of disturbances in lipoprotein metabolism,or that it is inferior to the ultracentrifugal patternin predicting manifest ischaemic heart disease(Lawry et al., I957). Comparisons betweenaffected and unaffected individuals have shownthat the former not only possess on the averagegreater concentrations of serum total cholesterol,but the distribution is altered in that more ispresent in the beta-lipoprotein fraction and less inthe alpha lipoprotein (Barr et al., I95I; Barr, 1953;Oliver and Boyd, 1955). These differences inserum-cholesterol levels are seen to their bestadvantage on comparisons between younger menand when the manifestation of ischaemic heartdisease was myocardial infarction and not anginapectoris. In men over 50 years, mean differencesbetween affected and unaffected individuals havebeen as little as between io and 20 mg. per Ioo ml.(Biorck et al., 1957; Lawry et al., I957). Oliver(I958), emphasizing the importance of age in thisdifference, expresses it in a different way. On in-cluding the cholesterol-phospholipid (C/P) ratioand the alpha-beta lipoprotein ratio in addition tothe serum-cholesterol level, he found that 48 percent. of the group with ischaemic heart diseaseaged 60 to 69 years had ' normal' values, whereasunder the age of 40, less than o per cent. had' normal' values.
It will be seen, then, that in individuals withclinically manifest ischaemic heart disease, thereported biochemical abnormalities are seen onlyon group comparisons. Considerable overlapoccurs with the unaffected groups. A case couldbe made for the view that these differences are theresult and not the cause of the disease, except for
by copyright. on F
ebruary 21, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.402.198 on 1 A
pril 1959. Dow
nloaded from

20) POSTGRADUATE MEDJCAL JOURNAL April 1959
the fact that in the prospective Framingham study(Dawber et al., I957) those with high serum-cholesterol levels were more liable to ischaemicheart disease than those with low values. Never-theless, particularly at the age when the disease ismost common, the serum-cholesterol-lipoproteinabnormalities at present recognized in ischaemicheart disease cannot be used with confidence topredict its' development in the individual.
Epidemiological Evidence for a Disorder inLipid MetabolismBy its very nature, the disease accounts for the
absence of any reliable measure of its presence inthe living. It has protean manifestations, with anonset that may be insidious, or so abrupt that in asusceptible area an individual in a short space mayhave to leave the unaffected or control group forthe affected group. This could, in part, possiblyaccount for the considerable overlap in studiesdone on very susceptible populations.
Despite wide differences in the mothers, new-born infants, irrespective of their racial origin,have similar serum-cholesterol levels (Bersohn andWayburne, I955). Deviations then begin tooccur, and by age 20 significant differencesin the serum-cholesterol levels can be seen, notonly between races but between income groupswithin the same race (Bronte-Stewart, 1957).TABLE 2.-SERUM CHOLESTEROL MG. PER I00 ML. MEN
AGED 20-29 YEARS
Bantu Coloured EuropeanLow income .. 122.5 146.1 188.3High income .. 178.o I85.1 223.0Serum cholesterol levels (mg. per Ioo ml.) of young
men residing in the same area. Income grading appliesto the particular racial group, for example, high-incomeBantu are on a lower economic plane than low-incomeEuropeans.
In the more prosperous peoples, peoples with ahigh prevalence of ischaemic heart disease, theserum-cholesterol levels steadily rise, thereafter toreach a maximum in the male at about 50 years ofage. In peoples in whom ischaemic heart diseaseis rare, such as the South African Bantu, theChimbu of New Guinea (de Wolfe and Whyte,1958), and the Japanese (Keys et al., 1958), thisrise with age is not seen.* The serum-cholesterol levels of men exceedthose of women throughout the period of life whenthe sex ratio in prevalence of the disease is veryprominent. After the sixth decade the levels forthe female reach and surpass those for the male(Lawry et al., I957).During the war years in Europe, when a sharpfall in the prevalence of ischaermic heart disease was
Bantu Coloured European
194-5200 - 52'8
1605± 54.4
150 122,3122 .3±83%
§.h ,oo - 77%
72%
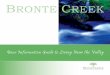
s 5 oc I I.t *: (FIG. i.--nter-racial lipoprotein cholesterol differences.
Mean serum-cholesterol levels (in alpha and betalipoprotein fractions) in 132 Bantu, 117 colouredand 114 European men aged 40-49 years, allresident in Cape Town. (Adapted from Bronte-Stewart, Keys an. Brock, I955.)
noted, lower serum-cholesterol levels were re-corded from many of the countries subjected tothe deprivations of the war (Gsell, 1948). InGermany, an increase in serum-cholesterol leveloccurred in groups studied in 1947 and again inI949 (Schettler, I950). Other intra-racial dif-ferences are seen when one compares Japanesewho have remained in Japan with those who haveemigrated to come under the American way of lifeon Hawaii or in Los Angeles (Fig. 2). In thelatter, ischaemic heart disease is more prevalent,and serum-cholesterol levels are higher than inthose who have remained in Japan (Keys et al.,1958).
Parallel with these changes in the total serum-cholesterol level, run differences in the manner inwhich it is distributed between the two lipoproteinfractions. Masculinity and age tend to influencea distribution characterized by the major portionof the cholesterol being in the beta fraction(Table i). In populations with a low degree ofsusceptibility to the disease, this does not appearto be the case (Fig. i). For example, Bantu andJapanese males have a cholesterol distribution be-tween the lipoprotein fractions resembling that ofthe younger European females.
It would seem, therefore, that in comparisonsbetween populations with wide differences inprevalence of the disease, ischaemic heart diseaseis associated with an abnormality of lipid meta-bolism. Unfortunately, in this epidemiologicalapproach lie several variables difficult to control.Amongst them may be another factor, genetic or
by copyright. on F
ebruary 21, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.402.198 on 1 A
pril 1959. Dow
nloaded from

April 1959 BRONTE-STEWART: Relationship Between Serum Lipids and Ischaemic Heart Disease 201
JAPANESE
IN
JAPAN HAWAII U. SA.
2127
200 I2oo /t183.0
-J
E08
i_ ?ootn '
o oC
·-~I
FIG. 2.-Intra-racial lipoprotein cholesterol differences.Mean serum-cholesterol levels (in alpha and betalipoprotein fractions) in Japanese men aged 40-49years, resident in Japan, Hawaii and U.S.A.(Adapted from. ]Keys et al., 1958.)
environmental, as yet undisclosed, that accountsfor the particular findings recorded.The Chemistry of the Atheromatous PlaqueA strengthening link in this association between
abnormal blood lipids and atherosclerosis arosefrom the early chemical studies on the athero-matous plaque, which revealed that the fat withinthe plaque resembled that within the blood plasma(Weinhouse and Hirsch, 1940). Upon this grewup the filtration theory of the pathogenesis of theatheromatous plaque. This theory (Page, I954)implied that the lipid infiltration into the intimawas the primary process and that the other majorcomponent of the plaque, fibrous tissue, developedsubsequently as a reaction to the presence of thisfat. The centrifugal forces of the circulationdrove the fat in contact with the arterial intima.Over the years, lipid deposition would accumulateand would be accelerated or intensified in thepresence of blood lipid in excess amount or ab-normal form, if the intraluminar or lateral filtrationpressure within the artery was high, or if thevascular endothelium was abnormally permeable.This theory supplied a satisfactory explanation forthe particular localization of the plaque at theorigins of branches, at other sites of pressure orvelocity change within the circulatory system, andfor the increased severity of atherosclerosis in thepresence of hypertension and such disorders oflipid metabolism as diabetes mellitus and essentialxanthomatosis.
Data accumulated to suggest that the lipids didexist in abnormal form. Moreton's (1950)nephelometric studies on the chylomicra followingfat feeding, suggested that it was the bio-physicalstate of suspension that may govern individualsusceptibility to atherosclerosis, in that prolonga-tion of the lipaemic phase would allow prolongedcontact of abnormal lipids with the arterial intimaand subsequent deposition. It is cholesterol, par-ticularly, that is in high concentration in the lipidof the atheromatous plaque. Other theories ondeposition, then, centred around quantitative andqualitative differences in the serum-cholesterollevels. Lewis's (1958) data are very suggestive inthis regard. He analysed the cholesterol esterfatty acids in Bantu and White individuals, thelatter with and without ischaemic heart disease,and the cholesterol ester fatty acids in atheroma-tous coronary arteries. He found that the pro-portion of saturated and oleic acids in the choles-terol ester was far higher in the atheromatousplaque than in the plasma, while in the plasmaitself it was highest in subjects with establishedischaemic heart disease and lowest in the Bantu.Furthermore, Rutstein et al. (I958), in tissue-culture studies on aortic cells, showed that intra-cellular cholesterol was greatest when the moresaturated fatty acids were present in the mediumin which the cells were being grown. The pos-sibility exists, then, that when the cholesterol esterfatty acids are unduly saturated, deposition in thearterial intima follows.These data are certainly not proof that the fat in
the atheromatous plaque originates from abnormalblood lipids. Chernick et al. (I949) have demon-strated that the arterial wall is capable of synthesiz-ing cholesterol. Paterson and Derrick (i957)failed to find a relationship between the totalserum-cholesterol levels and the total lipid sub-sequently extracted from large segments of thecoronary arteries of these subjects. It should beemphasized, however, that the age range of theirsubjects was 60 to 89 years, the period of lifeduring which biochemical differences are notmarked. Blankenhorn et al. (I956) have demon-strated the presence of the fat-soluble carotenoidpigment in atheromatous plaques. As the caro-tenes cannot be synthesized in the human body,and in electrophoretic studies the pigment migrateswith the beta-lipoprotein fraction, this findingprovides very suggestive evidence that at leastsome of the fat present in the atheromatous plaqueis deposited there.
The Relationship ofCoronary Atherosclerosisto Ischaemic Heart DiseaseThe balance of this evidence would imply that
atherosclerosis is the algebraic product of time
by copyright. on F
ebruary 21, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.402.198 on 1 A
pril 1959. Dow
nloaded from

202 POSTGRADUATEI MEDICAL JOURNAL April 1959and a disorder in fat metabolism. Now it isgenerally accepted that atheroma forms the basisof occlusive coronary artery disease, but the rela-tionship to myocardial infarction is not clear.Despite the rapid rise in mortality from ischaemicheart disease over the last few decades, Morris(I95I) has claimed the incidence of severe athero-sclerosis has not risen, or has even declined. Hisuse of calcification and other criteria as the indexof severity may be open to question, in that theymay merely depict chronicity, but other data sup-port the view. In the animal, atherosclerosis iseasily produced, but not the classical picture ofmyocardial infarction. The reported sex dif-ferences in the prevalence of severe atherosclerosisat autopsy (Lober, I953) are far less than the re-markable sex difference in the incidence of myo-cardial infarction (Oliver and Boyd, 1955). It iswell known, too, that severe occlusive disease ofthe coronary arteries may exist without apparentill effects, but the problem of relating severity ofthe occlusive disease to its effects is made evenmore difficult when one notes that, in a largeproportion of cases with. myocardial infarction atautopsy, no subtending occlusion was found des-pite careful dissection (Yater et al., I95I;Branwood and Montgomery, 1956).
It is, therefore, conceivable that in addition toatherosclerosis a process may exist for the fullexplanation of the clinical manifestations ofischaemic heart disease. This becomes a vitalpoint for clarification, because if this is true littleadvantage might accrue from measures aimed atlowering blood-cholesterol levels. This point, too,has revived a great deal of interest in thromboticand other mechanisms that interfere with circula-tory flow, and a relationship of these mechanismsto alterations in the blood lipids has been suggestedand is at present a controversial matter (Merskeyand Lackner, 1959). This merely emphasizes thatischaemic heart disease may be the end result of aseries of processes, not least in importance beingthe state of the collateral circulation and thefunctional status of the heart at the time of initialattack. The association, then, between the bio-chemical abnormalities reported in ischaemic heartdisease and the prevalence of the disease is astatistical one. A considerable overlap betweenaffected and unaffected groups exists, particularlyin the age range where clinical disease is most fre-quently encountered. Unless more precise mea-surements prove the contrary, the biochemicalabnormalities at present recognized in ischaemicheart disease cannot be used with confidence topredict susceptibility in the individual. It is onthis background, a background which shows thatthere is no precise measure of the prevalence of thedisease or of its development in the living, and a
background where there is no unanimity on itspathogenesis or its underlying pathology, that onemust study hypotheses founded merely on altera-tions in the blood lipids.Summary
I. The evidence for a relationship betweeraltered blood lipids and ischaemic heart disease isreviewed. There are two major differences be-tween affected and unaffected individuals. Affectedindividuals as a group exhibit a more extensive andmore prolonged lipaemia following an oral fat mealthan unaffected groups. The other major difference is seen in the serum-cholesterol-lipoproteinsystem.
2. In the experimental animal and in epidemio-logical studies comparing groups with wide dif:ferences in prevalence of ischaemic heart disease,there are wide differences in the total serum-cholesterol level, the manner in which it is dis-tributed between the two lipoprotein fractions andthe ultra-centrifugal lipoprotein pattern.
3. When studies are conducted on more homo-geneous groups in highly susceptible areas, how-ever, these differences are less wide and, in fact,may be insignificant in men over the age of 50, theage at which ischaemic heart disease is mostprevalent.
4. Chemical analyses of the atheromatousplaques could suggest that atheroma results froma disorder in the blood lipids, but the relationshipof atherosclerosis to ischaemic heart disease needsfurther clarification.
5. Although highly suggestive, the evidence asyet is insufficient to state that ischaemic heartdisease is the end product of a disordered fatmetabolism acting over a period of time. Con-siderable overlap between affected and unaffectedgroups exist and the biochemical abnormalities atpresent recognized in ischaemic heart disease can-not be used with confidence to predict susceptibilityin the individual.
BIBLIOGRAPHY
ANITSCHKOW, N. (I933), in ' Cowdry's Arteriosclerosis,' p. 271,Macmillan, New York.BARR, D. P. (1953), Circulation, 8, 641.BARR, D. P., RUSS, E. M., and EDER, H. A. (Ig95), Amer. J.Med., II, 480.BARRITT, D. W. (1956), Brit. med. J., ii, 640.BERSOHN, I., and WAYBURNE, S. (x955), Amer. J. clin. Nutr.,
4, 117.BIORCK, G., BLOMQVIST, G., and SIEVERS, J. (1957),Acta. med. scand., x56, 493.BLANKENHORN, D. H., FREIMAN, D. G., and KNOWLES,H. C. (1956), Circulation, 4, 912.BRANWOOD, A. W., and MONTGOMERY, G. L. (1956),Scottish med. J., I, 367.BRONTE-STEWART, B., KEYS, A., and BROCK, J. F. (1955),Lancet, ii, I103.BRONTE-STEWART, B. (I957), Nutrition (Lond.), Ix, 60.
Bibliography continued on page 232
by copyright. on F
ebruary 21, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.402.198 on 1 A
pril 1959. Dow
nloaded from

232 POSTGRADl)UA'l MW )CAL JOU(RNAL April 1959
MORRIS, J. N., and CRAWFORD, M. D. (1958), Brit. med. J.,ii, 14, 85.
MORRIS, J. N., HEADY, J. A., and RAFFLE, P. A. B. (1956),Lancet, ii, 569.
MORRIS, J. N., HEADY, J. A., RAFFLE, P. A. B., ROBERTS,C. G., and PARKS, J. W. (I953), Ibid., ii, 1053 and IIIi.
ORDMAN, B. (1948), Clin. Proc., 7, I83.PICK, R., STAMLER, J., ROBARD, S., and KATZ, L. N.
(1952), Circulation, 6, 858.POLITZER, W. M., and ANDERSON, I. (1957), S. Afr. J. med.
Sci., 22, 23.REGISTRAR-GENERAL, Decennial Supplement, England and
Wales (1951), 'Occupational Mortality,' part I, p. 13,H.M.S.O., London.
SCHLESINGER, M. J. (1938), Amer. Heart J., I5, 528.SCHRIRE, V., and GANT, J. (1958), in press.SCHRIRE, V., and UYS, C. J. (1958), in press.SELIGMAN, C. G. (1957), 'Races of Africa,' Oxford University
Press, London.SINGER, R. (I953), Amer. Anthrop., 55, 634.SINGER, R. (1958), Amer. J. Anat., in press.SPRAGUE, H. B. (1958), Circulation, 17, I.SQUIRES, B. T. (1941), S. Afr. J. med. Sci., 6, 53.STAMLER, J. (1956), Neb. St. rmed. J., 41, 75.STONE, W. (1936), Trans. roy. Soc. trop. Med. Hyg., 30, I65.
THOMAS, W. A., BLACHE, J. O., and LEE, K. T. (i957),Arch. intern. Med., o00, 423.
TROWELL, H. C., and SINGH, S. A. (r956), E. Afr. med. J.,33, 39I.
van OYE, E., and CHARLES, P. (1952), Ann. Soc. beige Med. trop.,32, 297.
VINT, F. W. (I937), E. Afr. med. J., 13, 332.VOGELPOEL, L., and SCHRIRE, V. (I955), Lancet, ii, IIo8.WALKER, A. R. P., and ARVIDSSON, U. V. (1954), . clin.
Invest., 33, 1358.WALKER, A. R. P., and BERSOHN, I. (1957), S. Afr. med. J.,
suppl. 'Medicine in South Africa,' p. Io6.WALKER, A. R. P., and SIMSON, I. W. (1958), Lancet, i, 1126.WASSERBURGER, R. H. (r955), Amer. J. Med., 18, 428.WHITE, P. D. (I947), 'Heart Disease,' 3rd ed., MacMillan, New
York.WHITE, N. K., EDWARDS, J. E., and DRY, T. J. (1950),
Circulation, I, 645.WILENS, S. L. (1947), Arch. intern. Med., 79, 129.WOOD, P. (1956), ' Diseases of the Heart and Circulation,' 2nd ed.,
Eyre and Spottiswoode, London.WORLD HEALTH ORGANISATION (1957), Techn. Rep. Ser.,
No. II7.WORLD HEALTH ORGANISATION (1958), Techn. Rep. Ser.,
No. I43.
This symposium was contributed on invita-tion of the editor, by the staff of the Depart-ment of Medicine, University of Cape Town,South Africa.The original work on which many of the
views are based was carried out with thefinancial support of many organizations, towhich grateful acknowledgment is made. TheCouncil for Scientific and Industrial Researchsupports the Clinical Nutrition Research Unitin the Department and has supported other
parts of the studies ad hoc. Acknowledgmentis also made to the National Heart Institute,Public Health Service, United States ofAmerica; the Cape Town City Council; theSouth African Mutual Life Assurance Societyof Cape Town; Irwin and Johnson Ltd., ofCape Town; the South African Fish OilProducers' Association (Pty.) Ltd., of CapeTown; the A. R. Richardson Research Fundand the Senate Research Fund of the Univer-sity of Cape Town.
Bibliography continued from page 202-B. Bronte-Stewart, M.D., M.R.C.P.
:BRiONTE-STEW'ART, B., and BLACKBURN, H. (1958),'Essential Fatty Acids' (Proceedings of the Fourth Inter-national Conference held at the University of Oxford in July,I957, on the Biochemical Problems of Lipids, p. I8o, Butter-worths Scientific Publications, London).
CHERNICK, S., SRERE, P. A., and CHAIKOV, I. L. (1949),J. biol. Chem., 179, 113.
DAWBER, T. R., MOORE, F. E., and MANN, G. V. (1957),Amer. J. publ. Hlth., 47, No. 4, part 2, p. 4.
de WOLFE, M. S., and WHYTE, H. M. (1958), Atst. Ann. Med.,7, 47.
GERTLER, M. M., and WHITE, P. D. (I954), ' Coronary HeartDisease in Young Adults: A Multidisciplinary Study,' p. 103,Commonwealth Fund, Cambridge (Mass.), Harvard UniversityPress.
GOFMAN, J. W., GLAZIER, F., TAMPLIN, A., STRISOWER,B., and DE LALLA, 0. (1954), Phys. Rev., 34, 589.
GSELL, 0. (1948), In: Hottinger, A., Gsell, 0., Uuehlinger, E.,Salzmann, C., and Labhart, A., 'Hungerkrankheit, Hun-gerodem und Hungertuberkulose,' p. 161, Schwabe, Basel.
KEYS, A., KIMURA N., KUSUKAWA, A., BRONTE-STEWART, B., LARSEN, N., and KEYS, M. H. (1958),Ann. intern. Med., 48, 83.
LAWRY, E. Y., MANN, G. V., PETERSON, A., WYSOCKI,A. P., O'CONNELL, R., and STARE, F. J. (I957), Amer. J.Med., 22, 605.
LEWIS, B. (1958), Lancet, ii, 71.LOBER, P. H. (i953), Arch. Path., 55, 357.MERSKEY, C., and LACKNER, H. (1959), Postgrad. med. J.,
35, 203.MITCHELL, J. R. A., and BRONTE-STEWART, B. (1959),
Lancet, in press.MORETON, J. R. (1950), J. Lab. clin. MIed., 35, 373.MORRIS, J. N. (195I), Lancet, i, 69.OLIVER, M. F. (1958), Practitioner, 180, 202.OLIVER, M. F., and BOYD, G. S. (1953), Clin. Sci., 12, 293.OLIVER, M. F., and BOYD, G. S. (1955), Brit. Heart3., 17, 299.PAGE, I. H. (1954), Circulation, Io, I.PATERSON, J. C., and DERRICK, J. B. D. (1957), Ibid., x6, 512.POMERANZE, J., BEINFIELD, W. H., and CHESSIN, M.
(1954), Ibid., 10, 742.RUTSTEIN, D. D., INGENITO, E. F., CRAIG, J. M., and
MARTINELLI, M. (I958), Lancet, i, 545.SCHETTLER, G. (1950), Klin. Wschr., 28, 565.SMITH, E. B. (1957), Lancet, ii, 910.WEINHOUSE, S., and HIRSCH, E. F. (1940), Arch. Path., 29, 31.YATER, W. M., WELSH, P. P., STAPLETON, J. F., and
CLARK, M. L. (I951), Ann. intern. Med., 34, 352.
by copyright. on F
ebruary 21, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.402.198 on 1 A
pril 1959. Dow
nloaded from

















![Charlotte Bronte[1][1]](https://img.pdfslide.us/doc/110x75/549897d0b479594c4d8b5476/charlotte-bronte11.jpg)