Embed Size (px)
Citation preview

Relationship Between Response to MethylphenidateTreatment in Children With ADHD and Psychopathology
in Their Families
NATALIE GRIZENKO, M.D., BOJAN KOVACINA, LEILA BEN AMOR, M.D., M.SC.,
GEORGE SCHWARTZ, M.SC., MARINA TER-STEPANIAN, B.A., AND RIDHA JOOBER, M.D., PH.D.
ABSTRACT
Objective: To compare the pattern of familial aggregation of psychopathology in children who are good responders (GR) to
methylphenidate (MPH) versus those who are poor responders (PR). Method: A total of 118 clinically referred children
ages 6 to 12 years, diagnosed with ADHD participated in a double-blind, placebo-controlled, randomized 2-week crossover
trial of MPH from 1999 to 2004. A low dose of 0.5mg/kg of body weight of MPH divided in two equal doseswas used. Family
history was obtained by interviewing at least one key historian relative of each subject using Family Interview for Genetic
Studies. Information was collected on 342 first-degree and 1,151 second-degree relatives of children with attention-deficit/hy-
peractivity disorder. Results: Forty-four subjects showed mild or no improvement (PR) and 74 showed moderate or very
much improvement (GR) on MPH over placebo. First-degree relatives of GR subjects were at significantly higher risk of
attention-deficit/hyperactivity disorder than the relatives of PR subjects (p < .05). Second-degree relatives of theGRwere at
significantly higher risk of antisocial personality disorder compared to the relatives of PR subjects (p < .05). Conclusions:
The significantly higher presence of attention-deficit/hyperactivity disorder in the first-degree relatives and of antisocial
personality disorder in the second-degree relatives of GR children suggests that this groupmay, at least partially, be distinct
from the PR group on the basis of genetic determinants. J. Am. Acad. Child Adolesc. Psychiatry, 2006;45(1):47–53.
Key Words: attention-deficit/hyperactivity disorder, methylphenidate, family psychopathology.
Attention-deficit/hyperactivity disorder (ADHD) isone of the most frequently occurring behavioral disor-ders in young children, estimated to affect 3% to 7% ofschool-age children (American Psychiatric Association,2000) and 2% of children from 3 to 5 years old(Lavigne et al., 1996). The syndrome is characterized
by impulsivity, emotional instability, inattention,and hyperactivity.The most common medications used for ADHD
are stimulants, mainly methylphenidate (MPH). Un-fortunately, not all patients respond equally to MPH(Spencer et al., 1996). It is estimated that only 70%of treated patients responded to MPH. Other medica-tions have also been used to treat ADHD such as dex-troamphetamine, desipramine, imipramine, bupropion,clonidine, and atomoxetine, but there may be numerousside effects associated with these medications (Spenceret al., 2002). It is therefore important to try to developindicators of therapeutic response to MPH that mayhelp in decision making with regard to treatmentchoice and adjustment.The pathogenesis of ADHD is still unclear, but it is
believed that both genetic and environmental factorsare implicated. For example, family genetic studies
Accepted August 2, 2005.Dr. Grizenko, Dr. Joober, and Mr. Schwartz are with McGill University and
Douglas Hospital; Mr. Kovacina is with McGill University; Dr. Ben Amor andMs. Ter-Stepanian are with Douglas Hospital, Montreal, Quebec, Canada.
The authors thank the Canadian Institutes for Health Research, le Fonds de laRecherche en Sante du Quebec, and The Roaster’s Foundation for their financialsupport. The authors thank Johanne Bellingham, Anna Polotskaia, and NicolePawliuk for their help in this study.
Correspondence to Dr. Natalie Grizenko, Bond Pavilion, Douglas Hospital,6875 LaSalle Blvd., Verdun, Quebec, Canada H4H 1R3; e-mail: [email protected].
0890-8567/05/4501–0047�2005 by the American Academy of Child
and Adolescent Psychiatry.
DOI: 10.1097/01.chi.0000184932.64294.d9
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:1, JANUARY 2006 47

(Biederman et al., 1990, 1992) show strong evidence ofa genetic contribution to the etiology of the disorder,whereas studies on maternal smoking during pregnancy(Milberger et al., 1996) and on pregnancy, labor/deliv-ery, and neonatal complications (Ben Amor et al., 2005;Lou, 1996; Low et al., 1992) suggest the presence ofenvironmental factors.Several studies proposed a link between ADHD and
parental psychopathology. Biederman et al. (1990, 1992)showed in their family studies that relatives of childrenwith ADHDwere at significantly higher risk of ADHD,antisocial disorders, mood disorders, substance depen-dence, and anxiety disorders compared with non-ADHDpsychiatric and normal controls. Similarly, Roizen et al.(1996) demonstrated higher prevalence of depression inthe parents of hyperactive children than in the parents ofchildren with Down syndrome or a normal population.Moreover, they found a greater incidence of alcoholism,ADHD, and drug abuse in relatives of probands withADHD than in relatives of controls (Down syndrome).More recently, a study done by Spreich et al. (2000)showed that biological parents of children with ADHDwere at higher risk of ADHD, severe major depression,and multiple anxiety disorders. Similarly, Faraone et al.(2000) demonstrated that relatives of the girls withADHD are at an elevated risk of ADHD, mood, anti-social, substance use, and anxiety disorders; however,the researchers did not find a risk for conduct disorderamong relatives of the hyperactive girls. Braaten et al.(2003) showed that ADHD had higher incidence in rel-atives of children with ADHD and of children withADHD/anxiety than in relatives of normal children.Finally, Clark et al. (2004) suggested in their study thatADHD was significantly more common in children offathers with a history of substance abuse and high rateof antisocial personality disorder (APD), major depres-sive disorder, and anxiety disorders.All of these studies suggest an important relationship
between family psychopathology and ADHD. To ourknowledge, no reports questioned the relationship be-tween children’s response to MPH and psychopathologypresent in their family. The present study examineswhether the presence of specific psychopathologies inthe families may provide another element, which wouldhelp predict who may be a good responder to MPH. Infact, genetic loading of psychiatric problems may wellyield a specific subgroup that may respond better toMPH.
METHOD
Children were recruited sequentially from the Disruptive Behav-ior Disorders Program and from the general sector outpatient clinicof the Douglas Hospital in Montreal, a psychiatric university teach-ing hospital. Hence, the full spectrum of the disorder was repre-sented in the study, from mildly to severely ill subjects. Ninety-fivepercent of eligible subjects agreed to participate in the trial. Allof the subjects were enrolled in our study immediately after the as-sessment; thus, no major psychological intervention had been car-ried out before the clinical trial. The sample consisted of 103 boysand 15 girls, all between 6 and 12 years old with a mean age of 9.04(SD = 1.8). Of all of the subjects, 92.3% were white, whereas 3.3%,2.5%, 0.8%, and 0.8% of themwere half-black, black, half-Asian, andhalf-Hispanic, respectively. Every subject had to be diagnosed withADHD, using DSM-IV criteria. The diagnosis was based on clinicalinterviews of both child and parent by two independent childpsychiatrists, school reports including the Conners Global Index-Teacher (CGI-T) version questionnaire, and the Diagnostic Sched-ule for Children (DISC)-version IV (Shaffer et al., 2000), which isa structured parent interview. McGrath et al. (2004) have shownthat adolescent and caretaker DISC reports of ADHD demonstratedsignificant agreement with clinician diagnosis. The exclusion criteriaincluded having an IQ of less than 70, as measured with the Wechs-ler Intelligence Scale for Children-III (WISC-III; Wechsler, 1991),Tourette syndrome, pervasive developmental disorder, and psycho-sis. Moreover, children taking any medication other than MPH orwho had previous intolerance or an allergic reaction to MPH wereexcluded. Of children in the study, 44.5% were from a family withan income of less than $20,000 Canadian/year (low income), 24.8%were from families that earned between $20,000 and $40,000 Ca-nadian/year (lower middle income), and 30.7% came from familieswith an income of more than $40,000 Canadian/year. Fathers of theassessed children had a mean of 11.8 years of education (range 3 to25 years, SD = 3.3). Similarly, mothers received a mean of 12.1 yearsof education (range 6 to 20 years, SD = 2.8). In our sample, 66% ofchildren had the combined subtype of ADHD, 23% were inatten-tive, and 11% were hyperactive. A total of 47 (39.8%) of the chil-dren with ADHD had a diagnosis of oppositional defiant disorder(ODD), 41 (34.7%) had a diagnosis of conduct disorder (CD), 35(29.7%) had a diagnosis of anxiety disorder, and 6 (5.19%) also hada diagnosis of depression. Of the children, 41.5% had been on somemedication in the past; however, all of the medication was stoppedfor a period of 2 weeks before the start of the clinical trial.The children with ADHD participated in a double-blind, placebo-
controlled, 2-week, crossover, randomized MPH trial. The studywas approved by the Research and Ethics Board of the DouglasHospital. Parents signed informed consent and all of the childrenassented to participate in the trial. Baseline evaluations were com-pleted after at least a 2-week washout period before the clinical trial.Children were assessed for comorbidity using the DISC and theirrelatives assessed for psychiatric problems using the Family Interviewfor Genetic Studies (FIGS).After baseline assessments, children randomly received either placebo
or 0.5mg/kg ofMPHadjusted to body weight and divided in two equaldoses (morning and noon) during a 1-week period and were crossedover during the second week. Although MPH takes effect shortly afteradministration, subjects were kept onmedication for 7 consecutive daysto account for individually or environmentally caused day-to-day var-iability in behavior. The pharmacist prepared both drug and placebo incolored gelatin capsules and was not involved in the clinical evaluations.Adherence to medication was evaluated by a weekly pill count.
GRIZENKO ET AL.
48 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:1, JANUARY 2006

A comprehensive series of both ecological and laboratory meas-ures were carried out starting 45 minutes after administration ofMPH or placebo. To evaluate the behavior of the children at schooland at home, we asked teachers to complete the CGI-T, after ob-serving the children for 5 days at school, and parents were asked tocomplete the Conners Global Index-Parent Version (CGI-P) on theSunday after giving the medication to the children during the week-end (Conners et al., 1998a,b). The two scales assess the frequencyof occurrence of 10 types of ecologically relevant behavior. The Clin-ical Global Impression Scale (National Institute for Mental Health,1985) was administered by a research assistant, with extensive expe-rience with children with ADHD, on the third day of each weekwhen the child came in for laboratory testing. It is based on the di-rect observation of the child and evaluates the severity of illness ofchildren and improvement after administration of the treatment.Laboratory measures consisted of the Restricted Academic SituationScale (RASS) (Barkley, 1990), evaluating the following behaviors:being off-task, fidgeting, vocalizing, playing with objects, and beingout of seat. The RASS has been identified as a significant tool todiscriminate children with ADHD from normal children (Milichet al., 1982). We also administered the Conners (1995) ContinuousPerformance Task, a vigilance task measuring inhibition and im-pulse control together with sustained attention.At the end of the trial and before breaking the drug code, the
research team (including at least two experienced child psychiatrists,a psychologist, child care workers, and research assistants) deter-mined the consensus clinical response (CCR) corresponding to over-all degree of improvement during the active week compared with theplacebo week on the following 4-point Likert scale: large = 3, mod-erate = 2, mild = 1, or nonresponder = 0. CCR takes into accountmultiple factors that can vary from objective and acute laboratorymeasures like RASS to personal impressions of clinicians such ason the CGI-P and CGI-T. It is also important to note that theCCR allows for an assessment of improvement in multiple settings:home, school, and laboratory. Our good responder (GR) groupshowed improvement in a minimum of two settings. It is importantto note that the reason we chose to proceed with the CCR to assessoverall degree of improvement was that in a previous study (Grizenkoet al., 2004), we found that children of different ages responded withvarying levels of accuracy to different tests. For example, the RASS andCGI were valid in young children, but the Continuous PerformanceTest (CPT) was not valid in determining improvement in symptom-atology. In older children, the Clinical Global Impressions Scale andCGI-T were the most valid measures. Therefore, it was important totake into account, for each child individually, how to weigh each scalein the overall interpretation of the degree of improvement. Second,situational factors needed to be taken into account; for example, if thechild had a cold, then he or she may have been moving less and there-fore appeared less hyperactive on the RASS.Overall, we believe that byincorporating a clinical filter with which to examine the data allowedus to detect with greater validity the overall improvement in symp-tomatology. For the analysis, we grouped mild responders and non-responders together into a poor responder group (PR), and moderateand very much improved into a GR group.Family history of psychiatric disorders was assessed using the
FIGS (Maxwell, 1992). We interviewed at least one key historianof each subject; 79% of informants were mothers, 19% were fathers,and 2% of informants were maternal grandmothers. For two pa-tients, there were two informants. Family history was completedby medical records whenever possible.Family informants were asked to complete a family genogram be-
fore entering the double-blind, placebo-controlled MPH trial. They
then completed a general screening questionnaire on all familymembers to identify family members with psychopathology. Spe-cific modules based on the DSM-IV criteria were completed by thefamily informant on each family member with specific identifiedproblems. We added to the modules available in the FIGS moduleson CD,ODD, and ADHD. The diagnosis on the added FIGSmod-ules were shown to be concordant with diagnosis made on the DISC.We administered the FIGS modules and the DISC to siblings ofsix subjects.The data regarding each relative of subjects were summarized and
presented to a psychiatrist. Having looked at all of the available dataon the FIGS, the psychiatrist, who had remained blind to the pa-tients’ responsiveness to MPH, made a diagnosis of the presence ofADHD, substance abuse (drug and alcohol), affective disorders(manic and major depressive episodes), APD, CD, ODD, andschizophrenia in all family members based on DSM-IV criteria.The final diagnosis made by the psychiatrist was based on the symp-toms reported by the informant on all family members, based on thegeneral screening questionnaire, together with medical diagnosis,which were reported by the informant or derived from medical files.Statistical comparisons used the psychiatrist’s final diagnosis.
ANALYSIS
Morbid risk (MR) was calculated using theWeinbergercorrection for age according to MR = N/BZ 3 100,where N = number of affected subjects, and BZ (Bezugs-ziffer) = number of individuals at risk of the disease. BZwas calculated by BZ = N + 1/2U1 + U2, where U1 =number of unaffected subjects within the period of riskand U2 = number of unaffected subjects beyond the pe-riod of the risk. For all disorders, the nonaffected subjectswho had not reached the period of risk were not includedin the analysis and weighted 0. The nonaffected subjectswho were within the period of risk were weighted 0.5,and the nonaffected subjects older than the period of riskwere weighted 1. The at-risk period for ADHD, CD, andODDwas taken to be between 5 and 18 years of age. Theat-risk period for affective disorders, substance abuse,and APD was taken to be between 20 and 60 years ofage. Finally, the at-risk period for schizophrenia was es-tablished as being between 15 and 45 years of age. MRswere compared with 2 3 2 tables and x2 statistics withthe continuity correction.
RESULTS
The breakdown of the CCR rating was as follows: 44subjects showed mild or no response (PR) and 74 sub-jects showed significant improvement with MPH (GR).Table 1 shows demographics and baseline characteris-tics of the population according to CCR results. Thetwo groups differed statistically significantly in age.
MPH RESPONSE AND FAMILY PSYCHOPATHOLOGY
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:1, JANUARY 2006 49
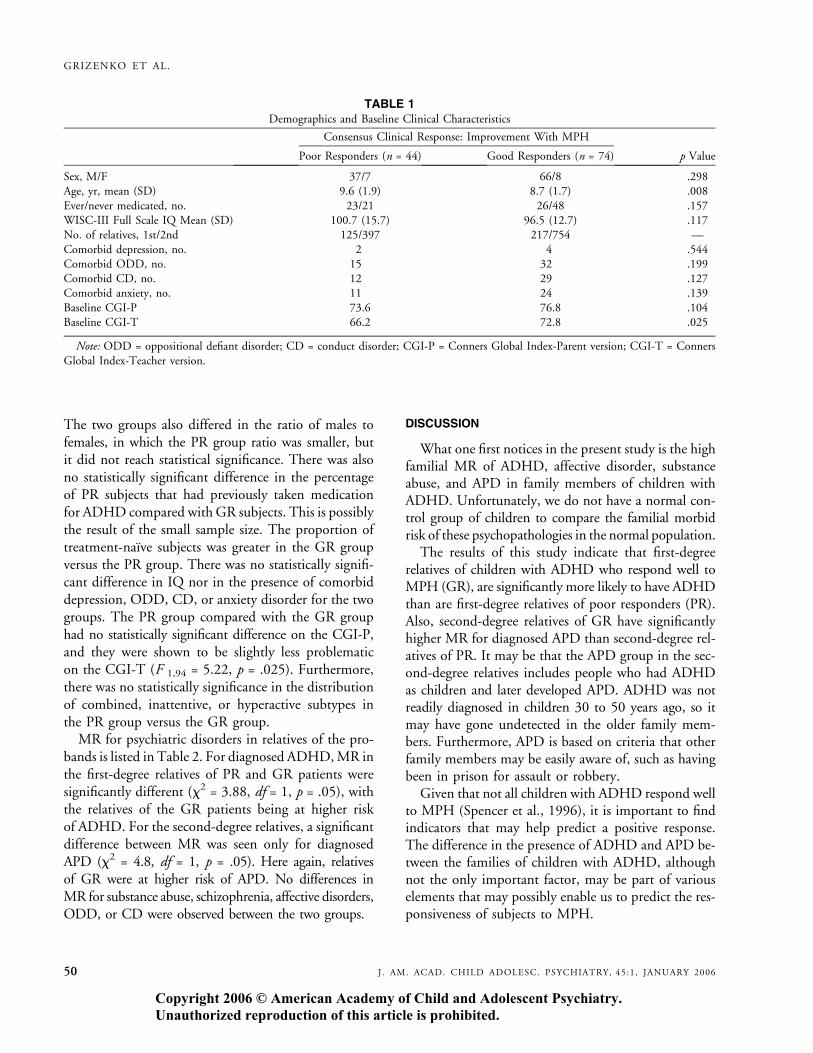
The two groups also differed in the ratio of males tofemales, in which the PR group ratio was smaller, butit did not reach statistical significance. There was alsono statistically significant difference in the percentageof PR subjects that had previously taken medicationfor ADHD compared with GR subjects. This is possiblythe result of the small sample size. The proportion oftreatment-naıve subjects was greater in the GR groupversus the PR group. There was no statistically signifi-cant difference in IQ nor in the presence of comorbiddepression, ODD, CD, or anxiety disorder for the twogroups. The PR group compared with the GR grouphad no statistically significant difference on the CGI-P,and they were shown to be slightly less problematicon the CGI-T (F 1,94 = 5.22, p = .025). Furthermore,there was no statistically significance in the distributionof combined, inattentive, or hyperactive subtypes inthe PR group versus the GR group.MR for psychiatric disorders in relatives of the pro-
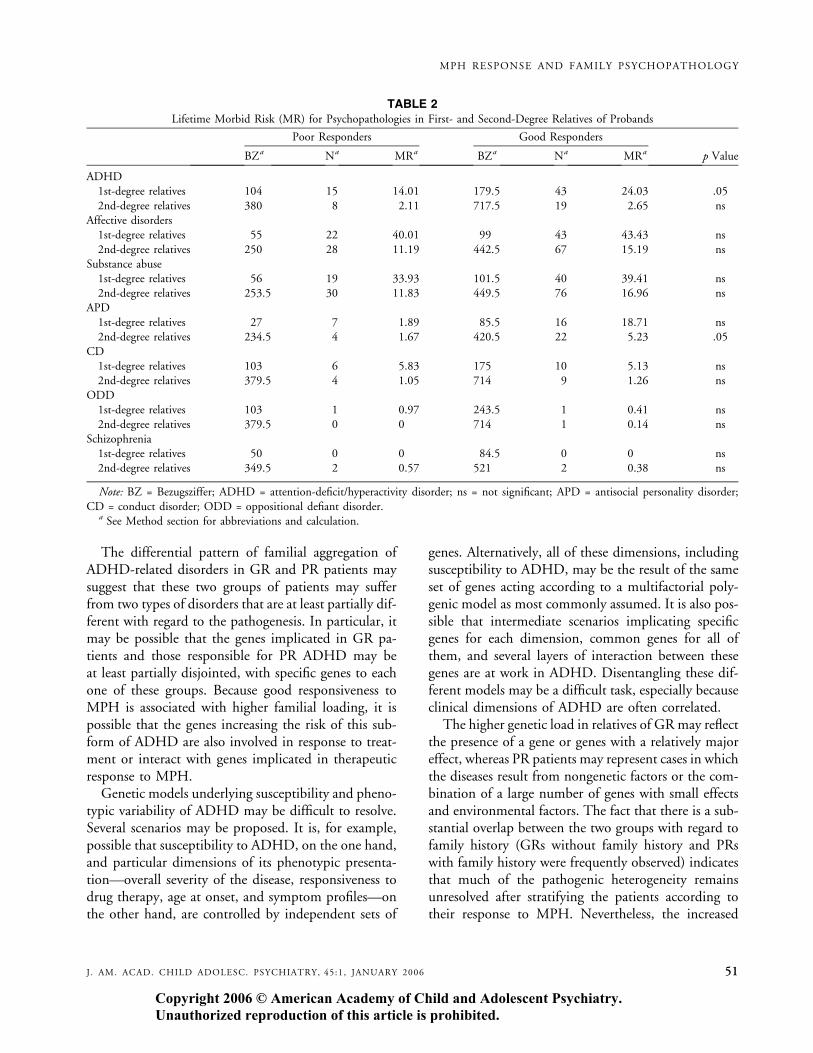
bands is listed in Table 2. For diagnosed ADHD,MR inthe first-degree relatives of PR and GR patients weresignificantly different (x2 = 3.88, df = 1, p = .05), withthe relatives of the GR patients being at higher riskof ADHD. For the second-degree relatives, a significantdifference between MR was seen only for diagnosedAPD (x2 = 4.8, df = 1, p = .05). Here again, relativesof GR were at higher risk of APD. No differences inMR for substance abuse, schizophrenia, affective disorders,ODD, or CD were observed between the two groups.
DISCUSSION
What one first notices in the present study is the highfamilial MR of ADHD, affective disorder, substanceabuse, and APD in family members of children withADHD. Unfortunately, we do not have a normal con-trol group of children to compare the familial morbidrisk of these psychopathologies in the normal population.
The results of this study indicate that first-degreerelatives of children with ADHD who respond well toMPH (GR), are significantly more likely to have ADHDthan are first-degree relatives of poor responders (PR).Also, second-degree relatives of GR have significantlyhigher MR for diagnosed APD than second-degree rel-atives of PR. It may be that the APD group in the sec-ond-degree relatives includes people who had ADHDas children and later developed APD. ADHD was notreadily diagnosed in children 30 to 50 years ago, so itmay have gone undetected in the older family mem-bers. Furthermore, APD is based on criteria that otherfamily members may be easily aware of, such as havingbeen in prison for assault or robbery.
Given that not all children with ADHD respond wellto MPH (Spencer et al., 1996), it is important to findindicators that may help predict a positive response.The difference in the presence of ADHD and APD be-tween the families of children with ADHD, althoughnot the only important factor, may be part of variouselements that may possibly enable us to predict the res-ponsiveness of subjects to MPH.
TABLE 1Demographics and Baseline Clinical Characteristics
Consensus Clinical Response: Improvement With MPH
Poor Responders (n = 44) Good Responders (n = 74) p Value
Sex, M/F 37/7 66/8 .298Age, yr, mean (SD) 9.6 (1.9) 8.7 (1.7) .008
Ever/never medicated, no. 23/21 26/48 .157WISC-III Full Scale IQ Mean (SD) 100.7 (15.7) 96.5 (12.7) .117No. of relatives, 1st/2nd 125/397 217/754 —
Comorbid depression, no. 2 4 .544Comorbid ODD, no. 15 32 .199Comorbid CD, no. 12 29 .127Comorbid anxiety, no. 11 24 .139
Baseline CGI-P 73.6 76.8 .104Baseline CGI-T 66.2 72.8 .025
Note: ODD = oppositional defiant disorder; CD = conduct disorder; CGI-P = Conners Global Index-Parent version; CGI-T = Conners
Global Index-Teacher version.
GRIZENKO ET AL.
50 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:1, JANUARY 2006
The differential pattern of familial aggregation ofADHD-related disorders in GR and PR patients maysuggest that these two groups of patients may sufferfrom two types of disorders that are at least partially dif-ferent with regard to the pathogenesis. In particular, itmay be possible that the genes implicated in GR pa-tients and those responsible for PR ADHD may beat least partially disjointed, with specific genes to eachone of these groups. Because good responsiveness toMPH is associated with higher familial loading, it ispossible that the genes increasing the risk of this sub-form of ADHD are also involved in response to treat-ment or interact with genes implicated in therapeuticresponse to MPH.Genetic models underlying susceptibility and pheno-
typic variability of ADHD may be difficult to resolve.Several scenarios may be proposed. It is, for example,possible that susceptibility to ADHD, on the one hand,and particular dimensions of its phenotypic presenta-tion—overall severity of the disease, responsiveness todrug therapy, age at onset, and symptom profiles—onthe other hand, are controlled by independent sets of
genes. Alternatively, all of these dimensions, includingsusceptibility to ADHD, may be the result of the sameset of genes acting according to a multifactorial poly-genic model as most commonly assumed. It is also pos-sible that intermediate scenarios implicating specificgenes for each dimension, common genes for all ofthem, and several layers of interaction between thesegenes are at work in ADHD. Disentangling these dif-ferent models may be a difficult task, especially becauseclinical dimensions of ADHD are often correlated.The higher genetic load in relatives of GR may reflect
the presence of a gene or genes with a relatively majoreffect, whereas PR patients may represent cases in whichthe diseases result from nongenetic factors or the com-bination of a large number of genes with small effectsand environmental factors. The fact that there is a sub-stantial overlap between the two groups with regard tofamily history (GRs without family history and PRswith family history were frequently observed) indicatesthat much of the pathogenic heterogeneity remainsunresolved after stratifying the patients according totheir response to MPH. Nevertheless, the increased
TABLE 2Lifetime Morbid Risk (MR) for Psychopathologies in First- and Second-Degree Relatives of Probands
Poor Responders Good Responders
BZa Na MRa BZa Na MRa p Value
ADHD1st-degree relatives 104 15 14.01 179.5 43 24.03 .05
2nd-degree relatives 380 8 2.11 717.5 19 2.65 nsAffective disorders1st-degree relatives 55 22 40.01 99 43 43.43 ns
2nd-degree relatives 250 28 11.19 442.5 67 15.19 nsSubstance abuse1st-degree relatives 56 19 33.93 101.5 40 39.41 ns2nd-degree relatives 253.5 30 11.83 449.5 76 16.96 ns
APD1st-degree relatives 27 7 1.89 85.5 16 18.71 ns2nd-degree relatives 234.5 4 1.67 420.5 22 5.23 .05
CD1st-degree relatives 103 6 5.83 175 10 5.13 ns2nd-degree relatives 379.5 4 1.05 714 9 1.26 ns
ODD1st-degree relatives 103 1 0.97 243.5 1 0.41 ns2nd-degree relatives 379.5 0 0 714 1 0.14 ns
Schizophrenia1st-degree relatives 50 0 0 84.5 0 0 ns2nd-degree relatives 349.5 2 0.57 521 2 0.38 ns
Note: BZ = Bezugsziffer; ADHD = attention-deficit/hyperactivity disorder; ns = not significant; APD = antisocial personality disorder;
CD = conduct disorder; ODD = oppositional defiant disorder.a See Method section for abbreviations and calculation.
MPH RESPONSE AND FAMILY PSYCHOPATHOLOGY
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:1, JANUARY 2006 51

prevalence of ADHD and related disorders in the rel-atives of GRs, in conjunction with the fact that themechanisms of action of MPH are well known (i.e.,blockade of catecholamine [dopamine and norepineph-rine] transporters), strongly points to genes coding forproteins implicated in the brain catecholamine path-ways as excellent candidates modulating the risk ofADHD and response to MPH. Consistent with thishypothesis, several studies have identified an associationbetween specific genotypes of the dopamine transporter(Kirley et al., 2003; Roman et al., 2004) and theDRD4 (Hamarman et al., 2004) genes and responseto psychostimulant medication. The usefulness of thisapproach has also been demonstrated in other complexdisorders. For example, specific mutations have beenidentified for a subgroup of patients suffering from dys-tonia (a complex and heterogeneous syndrome) onthe basis of their therapeutic response to L-DOPA(Furukawa and Kish, 1999).
Limitations
Our study has several limitations. The first limitationis that the PR group was older than the GR group. Theage difference can be explained in part because parentswho have relatives who have a clear ADHD diagnosisand have responded well to MPH may ask that theirchildren participate at an earlier age in the trial giventhat they may recognize similar symptoms in their chil-dren as in their relatives. Second, the gender distri-bution in the GR and PR sample is not the same.There was a higher proportion of girls in the PR group.Girls tend to be less disruptive. This may have influ-enced the evaluation of responsiveness to MPH becausethere may not have been the same magnitude of changein girls as in boys. From a genetic point of view, how-ever, it is expected that familial aggregation is higher inrelatives of the proband whose gender has the least prev-alence of the disorder in the general population, a phe-nomenon referred to in genetics as the Carter effect(Carter, 1961). Thus, this gender difference is ratherconservative with respect to our findings. The third lim-itation is that only 13% of our sample is female, andhence the overall results of the study may only applyto boys. The fourth limitation is that our sample wasalmost exclusively white. The fifth limitation is thatwe did not have a normal control group to examinethe overall morbid risk of psychopathology in familiesof children with ADHD compared with families of
nonaffected children. Sixth, our results are at p = .05,which is at the limit of significance.We performed com-parisons on multiple psychopathologies in the family.Although these family psychopathologies are not en-tirely independent comparisons, we cannot formally ex-clude a type I error. The sample size must be enlargedto validate these results. The seventh limitation is thatthe family history was gathered using the FIGS ques-tionnaire, which was completed by only one informant,frequently the mother. This may have introduced animportant underestimation of the MR. Indeed, it mustbe noted that a family member is not likely to be able toidentify all problems in their relatives. This, in fact, isa general limitation of the family history method, whichis recognized to be specific (low rate of false positives)but not sensitive (considerable rate of false negatives;Roy et al., 1996). If there is this bias, however, thenit is expected to be equally operant in the two groupsof patients (GR and PR) and therefore should not biasour general conclusion of an increased prevalence ofmorbidity in the relatives of PR patients.
An eighth limitation is the fact that ADHD in childrenwas not really diagnosed many decades ago, and adultADHD is not readily diagnosed at present. Thus, manycases of ADHD may not have been reported by inform-ants. Here again, this is not expected to affect differentiallythe diagnosis of ADHD in relatives of GR and PR pa-tients because the average ages of the relatives of thetwo groups are similar. Also, the Weinberger correctionthat was used to adjust theMR corrected grossly for agesand did not take into account the pedigree structure.
Finally, the ninth limitation is that the response tomedication was assessed using only one specific amountof MPH per day (adjusted to body weight). Childrenreceived a relatively low dose of MPH (0.25 mg/kg)in a twice-daily dose. This low dose was given for threereasons. The first is because many of the patients weredrug naıve and to avoid the possibility of side effects.Second, we wanted to study predictors/covariates of re-sponse to MPH in children, which is better served byusing doses in a lower therapeutic range to allow for alarge variation in response. Third, it was shown byKonrad et al. (2004, p. 196) that ‘‘while alertness andfocus and sustained attention seemed to be improvedfollowing a linear trend, inhibition and set shifting per-formance were enhanced at a lower dose (0.25 mg/kg),but worsened at a moderate dose (0.5 mg/kg).’’ Chil-dren who were assessed as PR may have responded
GRIZENKO ET AL.
52 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:1, JANUARY 2006

better to a larger dose. In the future, a similar trial couldbe repeated with multiple doses.
Clinical Implications
To our knowledge, no studies have so far questionedthe relationship between the psychopathology presentin the families of children with ADHD and the respon-siveness of those children to MPH. Because psychosti-mulants (e.g., MPH) are considered to be the treatmentof choice for ADHD, it is important to discriminatebetween nonresponders and responders to the drug.Our study presents one area for further study to possiblydifferentiate between the responders and nonrespond-ers. Children who are GR to MPH have a significantlyhigher percentage of first-degree relatives with ADHDand second-degree relatives with APD. It is prematureto suggest that, based on this study, clinicians could nowuse family history to make medication selections for thetreatment of ADHD in individual cases, but it does en-tice us to explore through future research the negative orpositive predictive values of family psychopathology inpredicting MPH treatment response.
Disclosure: The authors have no financial relationships to disclose.
REFERENCES
American Psychiatric Association (2000),Diagnostic and Statistical Manual ofMental Disorders, 4th edition (DSM-IV). Washington, DC: AmericanPsychiatric Association
Barkley RA (1990), Attention Deficit Hyperactivity Disorder: A Handbook forDiagnosis and Treatment. New York: The Guilford Press
Ben Amor L, Grizenko N, Schwartz G et al. (2005), Perinatal complicationsin children with attention deficit hyperactivity disorder and their unaf-fected siblings. J Psychiatry Neurosci 30:120–126
Biederman J, Faraone SV, Keenan K, Knee D, Tsuang MT (1990), Family-genetic and psychosocial risk factors in DSM-III attention deficit disor-der. J Am Acad Child Adolesc Psychiatry 29:526–533
Biederman J, Faraone SV, Mick E et al. (1992), Further evidence for familygenetic risk factors in attention deficit hyperactivity disorder: patterns ofcomorbidity in probands and relatives in psychiatrically and pediatricallyreferred samples. Arch Gen Psychiatry 49:728–738
Braaten EB, Biederman J, Monuteaux MC et al. (2003), Revisiting the as-sociation between attention-deficit/hyperactivity disorder and anxietydisorders: a familial risk analysis. Biol Psychiatry 53:93–99
Carter CO (1961), The inheritance of congenital pyloric stenosis. Br MedBull 17:251–254
Clark DB, Cornelius J, Wood DS, Vanyukov M (2004), Psychopathologyrisk transmission in children of parents with substance use disorders.Am J Psychiatry 161:685–691
Conners CK (1995), Conners Continuous Performance Test Computer Program.Toronto: MultiHealth Systems
Conners CK, Sitarenios G, Parker JD, Epsteins JN (1998a), Revision andrestandardization of the Conners Teacher Rating Scale (CTRS-R): factorstructure, reliability, and criterion validity. J Abnorm Child Psychol 26:279–291
Conners CK, Sitarenios G, Parker JD, Epsteins JN (1998b), The revisedConners Parent Rating Scale (CPRS-R): factor structure, reliability,and criterion validity. J Abnorm Child Psychol 26:257–268
Faraone SV, Biederman J, Mick E et al. (2000), Family study of girls withattention deficit hyperactivity disorder. Am J Psychiatry 157:1077–1083
Furukawa Y, Kish SJ (1999), Dopa-responsive dystonia: recent advances andremaining issues to be addressed. Mov Disord 14:709–715
Grizenko N, Lachance M, Collard V et al. (2004), Sensitivity of tests toassess improvement in ADHD symptomatology. Can Child AdolescRev 13:36–40
Hamarman S, Fossella J, Ulger C, Brimacombe M, Dermody J (2004),Dopamine receptor 4 (DRD4) 7-repeat allele predicts methylphenidatedose response in children with attention deficit hyperactivity disorder:a pharmacogenetic study. J Child Adolesc Psychopharmacol 14:564–574
Kirley A, Lowe N, Hawi Z et al. (2003), Association of the 480 bp DAT1allele with methylphenidate response in a sample of Irish children withADHD. Am J Med Genet B Neuropsychiatr Genet 121:50–54
Konrad K, Gunter T, Manisch C, Herpertz-Dahlmann B (2004), Differen-tial effects of methylphenidate on attentional function in children withattention deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychi-atry 43:191–198
Lavigne JV, Gibbons RD, Christoffel KK et al. (1996), Prevalence rates andcorrelates of psychiatric disorders among preschool children. J Am AcadChild Adolesc Psychiatry 35:204–214
Lou HC (1996), Etiology and pathogenesis of attention-deficit hyperactivitydisorder: significance of prematurity and perinatal hypoxic-haemodynamicencephalopathy. Acta Pediatr 85:1266–1271
Low JA, Froese AB, Smith JT, Galbraith RS, Sauerbrei EE, Karchmar EJ(1992), Hypotension and hypoxemia in the preterm newborn duringthe four days following delivery identify infants at risk of echosonograph-ically demonstrable cerebral lesions. Clin Invest Med 15:60–65
McGrath A, Handwerk ML, Armstrong KJ, Lucas CP, Friman PC (2004),The validity of the ADHD section of the Diagnostic Interview Schedulefor Children. Behav Modif 28:349–374
Maxwell ME (1992), Family Interview for Genetic Studies (FIGS): A Manualfor FIGS. Bethesda, MD: Clinical Neurogenetics Branch, IntramuralResearch Program, National Institute of Mental Health
Milberger S, Biederman J, Faraone SV, Chen L, Jones J (1996), Is maternalsmoking during pregnancy a risk factor for attention deficit hyperactivitydisorder in children? Am J Psychiatry 153:1138–1142
Milich R, Loney J, Landau S (1982), Independent dimensions of hyper-activity and aggression: a validation with playroom observation data.J Abnorm Psychol 91:183–198
National Institute for Mental Health (1985), CGI (Clinical Global Impres-sion) Scale. Psychopharmacol Bull 21:839–841
Roizen NJ, Blondis TA, Irwin M, Rubinoff A, Kieffer J, Stein M (1996), Psy-chiatric and developmental disorders in families of children with attention-deficit hyperactivity disorder. Arch Pediatr Adolesc Med 150:203–208
Roman T, Rohde LA, Hutz MH (2004), Polymorphisms of the dopaminetransporter gene: influence on response to methylphenidate in attentiondeficit-hyperactivity disorder. Am J Pharmacogenomics 4:83–92
Roy MA, Walsh D, Kendler KS (1996), Accuracies and inaccuracies of thefamily history method: a multivariate approach. Acta Psychiatr Scand93:224–234
Shaffer D, Fisher P, Lucas CP, Dulcan MK, Schwab-Stone, ME (2000),NIMH diagnostic interview schedule for children version IV (NIMHDISC-IV): description, differences from previous versions, and reliabilityof some common diagnoses. J Am Acad Child Adolesc Psychiatry 39:28–38
Spencer TJ, Biederman J, Wilens TE, Harding M, O’Donnell D, Griffin S(1996), Pharmacotherapy of attention-deficit/hyperactivity disorder acrossthe life cycle. J Am Acad Child Adolesc Psychiatry 34:886–896
Spencer TJ, Biederman J, Wilens TE, Faraone SV (2002), Novel treatments forattention-deficit hyperactivity disorder in children. J Clin Psychiatry 63:16–22
Spreich S, Biederman J, Harding-Crawford M, Mundy E, Faraone SV(2000), Adoptive and biological families of children and adolescents withADHD. J Am Acad Child Adolesc Psychiatry 39:1432–1437
Wechsler D (1991), Wechsler Intelligence Scale for Children-Third Edition:Manual. San Antonio, TX: The Psychological Corporation
MPH RESPONSE AND FAMILY PSYCHOPATHOLOGY
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:1, JANUARY 2006 53