Embed Size (px)
Citation preview

The Knee 21 (2014) 216–220
Contents lists available at ScienceDirect
The Knee
Relationship between leg extensor muscle strength and knee joint loading during gaitbefore and after total knee arthroplasty
Doris Vahtrik ⁎, Helena Gapeyeva, Jaan Ereline, Mati PääsukeInstitute of Exercise Biology and Physiotherapy, University of Tartu, 5 Jakobi Street, 51014 Tartu, Estonia
⁎ Corresponding author. Tel./fax: +372 7 375379.E-mail address: [email protected] (D. Vahtrik).
0968-0160/$ – see front matter © 2013 Elsevier B.V. Allhttp://dx.doi.org/10.1016/j.knee.2013.05.002
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 29 December 2012Received in revised form 22 April 2013Accepted 1 May 2013Keywords:Isometric muscle contractionKnee joint loadingGaitKnee osteoarthritisTotal knee arthroplasty
Objective: The aim of the present study was to evaluate an isometric maximal voluntary contraction (MVC)force of the leg extensor muscles and its relationship with knee joint loading during gait prior and aftertotal knee arthroplasty (TKA).Methods: Custom-made dynamometer was used to assess an isometric MVC force of the leg extensor musclesand 3-D motion analysis system was used to evaluate the knee joint loading during gait in 13 female patients(aged 49–68 years) with knee osteoarthritis. Patients were evaluated one day before, and three and sixmonths following TKA in the operated and non-operated leg.Results: Six months after TKA, MVC force of the leg extensor muscles for the operated leg did not differ signifi-cantly as compared to the preoperative level, whereas it remained significantly lower for the non-operated legand controls. The knee flexion moment and the knee joint power during mid stance of gait was improved six
months after TKA, remaining significantly lowered compared with controls. Negative moderate correlationbetween leg extensor muscles strength and knee joint loading for the operated leg during mid stance wasnoted three months after TKA.Conclusions: The correlation analysis indicates that due toweak leg extensormuscles, an excessive load is appliedto knee joint during mid stance of gait in patients, whereas in healthy subjects stronger knee-surroundingmuscles provide stronger knee joint loading during gait.Level of Evidence: III (correlational study)© 2013 Elsevier B.V. All rights reserved.
1. Introduction
Osteoarthritis (OA) of the knee affects the major biomechanicalfactors ensuring the optimal load to the joint during walking [1].Biomechanical factors may play a part in the modulation of knee jointpathogenesis [2], in which large knee adduction moment and higherjoint dynamic load during gait is mostly related to the severity oftibiofemoral OA [3,4]. Besides, muscle weakness causes modificationsin the timing of muscle action [5], which help to avoid threateningpostures and induce protective alignment during stance. Despite thatseveral studies refer improvements in the temporospatial parametersof gait following total knee arthroplasty (TKA) [6–8], inter-limb differ-ences in knee kinematics andmoments persists as compared to healthycontrols. It has been found that quadriceps femoris muscle weaknesshas a substantial impact on themovement patterns [9], but no significantrelationship between the overall magnitude of quadriceps femorismuscle strength and rate of loading during heel strike transient hasbeen suggested [1].
Since the maintenance of stance limb stability requires a goodinterplay of lower limbmuscle activations [10], themethods estimating
rights reserved.
knee joint contact loads should also evaluate the surrounding musclesand soft tissues of the knee [11]. In spite of difficulties in measuringknee joint contact loads and muscle forces in vivo [12], 3D analysisallows evaluating the dynamic behavior of a subject during walking.Knee joint loading indicators such as the knee joint flexion momentand knee joint power are the predictors of load distribution across thetibiofemoral joint reflecting a special time point during stance. Only afew studies have provided data on the relative force demands onlower limb muscles and joints during gait [13]. It is therefore informa-tive to investigate the relationship between the entire leg muscles'strength and knee joint loading during gait in OA patients withoutand with knee prosthesis. As the leg muscles are working during legstraightening in the concentric regimen, then it is important to findthe relationship between muscle strength and knee joint loadingduring mid stance phase of gait. For clinicians and knee OA patients, itis important to know whether the knee mechanics in the operated legis normal after TKA, to reduce the risk of further damage and deteriora-tion of lower extremity joints, also in the non-operated knee [7]. To thebest of our knowledge, this is thefirst study to evaluate the impact of legextensor muscle strength to knee joint loading during gait.
The aim of the present study was to evaluate isometric strength ofthe leg extensor muscles, knee joint loading during mid stance of gaitand their possible relationship prior and after TKA. According to the

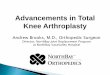
Fig. 1. The experimental setup for the measurement of the isometric maximal voluntarycontraction force of the leg extensor muscles.
217D. Vahtrik et al. / The Knee 21 (2014) 216–220
hypothesis, the deficit in the leg extensor muscle strength describedin knee OA patients is related with the deficit in knee joint loadingduring gait, before and half a year after TKA.
2. Methods
2.1. Subjects
Thirteen women with degenerative knee OA in stage III or IVaccording to the Kellgren–Lawrence Scale, who underwent unilateralTKA were recruited and assessed one day before, three and sixmonths after knee surgery. Six subjects also had a diagnosis of kneeOA in the contralateral leg, but the disease was in the first stageaccording to the Kellgren–Lawrence Scale. The patients' mean age was60 years (SD 7.7 years, range 49–68 years) and the mean body massindex 33 kg m−2 (SD4.4 kg m−2, range 25–41 kg m−2). These thirteensubjects were part of a cohort whose data have been previously pub-lished [14]. The subjects were initially selected from surgical waitinglists. The inclusion criteria of the study were the diagnosis of primaryknee OA, the first TKA, and the ability to walk without aid. The patients'exclusion criteria were cardiovascular, pulmonal or neuromuscular dis-eases and any other joint replacement of lower limb. The average periodof knee OA symptoms before the operation was six years. The assumedcauses of knee OA of the patients in the current study were strenuousphysical work (n = 7) and prior trauma (n = 6). The data of patientswere compared to ten healthy women aged 47–70 years (controls, BMIranged 27–38 kg m−2). Individuals were excluded from the controlgroup if they had had joint replacement of any joint of lower limbs, pain-ful joints, or any other criteria listed for the patients' group. Before partic-ipation in the study, all subjects gave a written informed consent. Thestudy received the approval from the regional ethics committee.
2.2. Clinical intervention
All thirteen patients with knee OA received the condylarendoprosthesis GEMINI (W. Link Gmbh and Co., Germany) with rotat-ing platform because of moderate knee varus deformity (up to 10°)and stable knee ligaments. In all cases endoprosthesis componentswere fixed onto the bone with cementation, the posterior cruciate lig-ament was preserved. During the operation any knee deformitieswere corrected and the ligaments were balanced. During postopera-tive rehabilitation performed in hospital, all patients were motivatedto continue specific exercises in home. Each subject received a de-tailed supporting handout containing instructions and photographsof the exercises including range of motion exercises, strengtheningand stretching exercises for thigh and shank muscles [15], movementcontrol, balance and coordination exercises [16]. In addition, walking,cycling and swimmingwere recommended. All subjects filled in a train-ing diarywith the number of exercises from the handout, the number ofrepetitions and series, and comments in free form (e.g., cycling for25 min). The study's author made phone calls to the patients monthlyto check on the subjects' recovery and make sure they performed theexercises. Additionally, during the third and sixth month examination,the subjects received counselling and encouragement to continue phys-ical activity.Walkingwithout crutches andwith full weight bearingwasallowed about one and a half-month after TKA or when walking wassecure and painless.
2.3. Leg extensor muscle strength
During the measurement of isometric maximal voluntary contrac-tion (MVC) force of the leg extensor muscles the subjects were seatedon a custom-made dynamometric chair in a horizontal frame withknee and hip angles equal to 110° and 120°, respectively (Fig. 1). Thetested foot was placed on a footplate mounted on a steel bar held inball bearings on the frame.
The subjects were instructed to push the footplate as forcefully aspossible for two-three seconds in two cases: unilateral contraction ofthe operated leg and unilateral contraction of the non-operated leg.Three trials were performed for each case and the greatest valuewas taken as the MVC force [17]. Strong verbal encouragement wasused to motivate the participants. A rest period of two minutes wasallowed between the trials.
2.4. Gait analysis
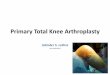
Three-dimensional gait analysis was performed using optic-electronic movement analysis system Elite (BTS, Italy). Reflectivemarker trajectories were recorded with six cameras at a frequency of100 Hz, and the ground reaction forces (GRF) were measured simulta-neouslywith twoKistler force platforms (Kistler 9286A, Sweden) embed-ded in a 10 m walkway. Reflective markers were placed to the subjects'skin bilaterally over the following anatomical landmarks regarding tothe Davis protocol: acromion, processus spinosus C7 and L4, anteriorand posterior superior iliac spines, lateral femoral trochanter, lateralaspect of thigh, lateral femoral epicondyle, lateral tibial epicondyle, lateralaspect of the shank, lateral malleolus, calcaneus, and the top of the foot atthe base of the second metatarsal [18]. Temporospatial data and GRFwere computed by Elite Clinic (BTS S.p.A., Italy) software. Rates ofknee joint loading were calculated from the vertical component of theGRF using a computer-driven algorithm with all values normalized tobody mass. Values of stance time (ms), cadence (step/min), and kneejoint flexionmoment as KM2 (the first maximal knee extensionmomentin early stance) and knee joint power as KP2 (maximal power generationin stance corresponding to concentric knee extensor activity) duringmidstance were used for future analysis. Step length data was normalizedwith subject's height. The trial was selected as successful when eachfoot contacted one platform, and the gait cycle was time-normalized to100%. Three successful gait cycles were averaged to obtain a mean foreach patient and control subject. All subjects were instructed to walk attheir self-selected normal speed on barefoot. Fig. 2 provides an exampleof the typical knee extension/flexion moment curve obtained duringone gait cycle. The approach used to collect temporospatial data of gaitis identical to that described in previous investigations [1,19].
2.5. Experimental protocol
The women with knee OA were examined one day before, three andsixmonths after TKA in the Laboratory of Kinesiology and Biomechanics.After each patient had signed the informed consent, gait analysis wasperformed. Before the leg extensor muscle strength testing, the subjects

0
Mo
men
t (N
m .
kg-1
)
Knee flexion
Knee extension
Preop 3 m postop 6 m postop KM2
-40
-30
-20
-10
10
20
30
40
Fig. 2. A typical curve of knee extension/flexionmoment for one gait cycle preoperatively,three and six months after unilateral total knee arthroplasty. KM2 - knee joint flexionmoment during mid stance.
0
200
400
600
800
1000
1200
1400
1600
1800
2000
Preop 3 monthspostop
6 monthspostop
Controls
MV
C (
N)
op
nonop
***
***
**
**
***
Fig. 3. Isometric maximal voluntary contraction (MVC) force of the leg extensor musclesinwomenwith knee osteoarthritis (n = 13) before, three and sixmonths after unilateraltotal knee arthroplasty and controls. Values are mean (SE). **P b 0.01; ***P b 0.001.
Preop 3 monthspostop
6 monthspostop
Controls
Ste
p le
ng
th (
mm
) :
hei
gh
t
op
nonop
postop postop
Gai
t ve
loci
ty (
m .
s-1)
op
nonop
a
b
**
***
*
***
**
*
***
*
***
***
***
***
***
**
***
0
100
200
300
400
500
600
700
800
0
0,5
1
1,5
2
2,5
3
3,5
4
Preop 3 months 6 months Controls
Fig. 4. Step length (a) and gait velocity (b) in women with knee osteoarthritis (n = 13)before, three and six months after unilateral total knee arthroplasty and controls. Valuesare mean (SE). *P b 0.05; **P b 0.01; ***P b 0.001.
218 D. Vahtrik et al. / The Knee 21 (2014) 216–220
performed a warm-up with exercise bike during five minutes. Todetermine MVC force of the leg extensor muscles, three attemptswere performed with two-minute recovery time. In patients, the non-operated leg was tested initially, thereafter the operated leg. In controlsonly the dominant leg was tested.
2.6. Statistical analysis
All data are presented as means and standard error of mean (SE)with probability values of b0.05 to indicate statistical significance.One-way analysis of variance followed by Bonferroni post hoc com-parisons was used to evaluate differences between the operated andnon-operated leg. A paired t-test was used to evaluate differences be-tween pre- and postoperative characteristics. Relationship betweenthe lower leg extensor muscle strength and knee joint loading duringmid stance was examined using a Spearman's correlation coefficients.
Statistical power analysis demonstrated that thirteen patientswere sufficient to detect a significant difference (alpha = 0.05) inthe operated leg's lower limb extensor muscle force before and sixmonths after TKA (power > 0.95). Statistical power of the operatedleg's knee flexion moment before and six months after TKA was0.61. Statistically significant difference was set at alpha level 0.05.
3. Results
Isometric MVC force of the leg extensor muscles for the operated leg did not differsignificantly before TKA when compared to the non-operated leg (Fig. 3). The isometricMVC force for the operated leg did not differ significantly before and six months afterTKA. However, compared to the non-operated leg, MVC force for the operated leg wassignificantly lower three and six months after TKA. Compared to healthy controls, MVCforce for the operated leg was significantly lower before, three and six months afterTKA.
Step length during gait for the operated leg was significantly longer six monthsafter TKA when compared with the same parameter before and three months afterTKA (Fig. 4a). Compared with the controls, step length for the operated leg was signif-icantly shorter before and three months after TKA, whereas six months after TKA it didnot differ significantly compared with controls.
Gait velocity for the operated and non-operated leg increased significantly sixmonths after TKA when compared with the same characteristic before and threemonths after TKA (Fig. 4b). When compared to healthy controls, gait velocity inpatients was prolonged significantly both before, three and six months after TKA.
In patients, knee flexion moment for the operated leg during mid stance did notimprove significantly six months after TKA, compared to the preoperative level(Fig. 5a). Compared to healthy controls, the knee flexion moment for the operatedleg differed significantly before, three and six months after TKA.
Patients produced significantly less knee joint power for the operated leg duringmid stance three months after TKA than pre-TKA (Fig. 5b). Six months after TKA,knee joint power in patients for the operated leg was significantly weaker than forthe non-operated leg and in healthy controls.
In patients, no significant correlation between the isometric MVC force of the legextensor muscles and knee joint loading for operated leg was found preoperatively
and six months after TKA (Table 1). Three months after TKA, a moderate negativecorrelation (r = −0.55; p b 0.01) between the isometric MVC force of the leg extensormuscles and knee joint power for the operated leg emerged. In healthy controls, a

0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
Preop 3 monthspostop
6 monthspostop
ControlsKn
ee f
lexi
on
mo
men
t (N
m .
kg-1
)opnonop
00,050,1
0,150,2
0,250,3
0,350,4
0,450,5
Preop 3 monthspostop
6 monthspostop
Controls
Kn
ee jo
int
po
wer
(W
. K
g-1
)
opnonop
**
*
a
b
***
*
***
*
***
***
***
*
***
***
Fig. 5. Knee flexion moment (a) and knee joint power (b) during mid stance in womenwith knee osteoarthritis (n = 13) before, three and six months after unilateral total kneearthroplasty and controls. Values are mean (SE). *P b 0.05; **P b 0.01; ***P b 0.001.
219D. Vahtrik et al. / The Knee 21 (2014) 216–220
moderate positive correlation between leg extensor muscle strength and knee jointloading was noted (KM2 r = 0.59; p b 0.01; KP2 r = 0.63; p b 0.01).
4. Discussion
The important finding of the present study was that in patientswith knee OA, the increase of leg extensor isometric strength, steplength, gait velocity and the knee joint loading during gait for theoperated leg, was noted six months after TKA. The second finding ofthe study was that due to weak leg extensor muscles, on a third post-operative month patients applied an excessive load to knee joint dur-ing mid stance of gait. In healthy subjects stronger knee surroundingmuscles provided stronger knee joint loading during gait.
Table 1The correlation between leg extensor muscle strength and gait temporospatial param-eters in knee OA patients before and after total knee arthroplasty.
Preoperatively 3 months postop 6 months postop
MVC op MVC non MVC op MVC non MVC op MVC non
MVC non 0.55* x 0.44 x 0.83* xst length op 0.21 0.48 −0.02 0.43 0.51* 0.63 *st length non 0.57* 0.33 0.37 0.50* 0.53* 0.37vel op 0.61* 0.56* 0.24 0.24 −0.55* −0.52*vel non 0.70* 0.65* 0.23 0.27 −0.17 0.07KM2 op −0.08 0.20 0.27 0.30 −0.10 −0.05KM2 non −0.20 −0.03 −0.27 0.20 0.56* 0.19KP2 op −0.30 −0.08 −0.55* 0.10 −0.28 −0.29KP2 non −0.20 0.20 −0.01 0.02 −0.19 0.01
Note. MVC- maximal voluntary contraction; op- operated leg; non- non-operated leg;st- step; vel-velocity; KM2- knee flexion moment in mid stance; KP2- knee jointpower in mid stance. *P b 0.05.
Based on the knowledge that knee mobility and stability are themajor factors in the normal pattern of walking, the purpose of thecurrent study was to assess the isometric strength of knee surround-ing muscles, and the economics and the rate of force development inknee joint during gait. For clinicians it is important to reduce the dif-ferences between leg extensor muscle strength and knee joint loadingfor the operated and non-operated leg during gait, to avoid potentialbilateral knee arthroplasty [6].
In the current study, leg extensor muscle strength achieves half ayear after TKA to the preoperative level (difference being only 3%), re-mains still weaker than the non-operated leg (38%) and the dominantleg of controls (44%). Since there is a strong association between theclosed-chain assessment of leg extensor muscles strength and physicalfunction according toWestern Ontario andMcMaster Universities Oste-oarthritis Index (WOMAC) [20], the activation of all the leg muscles ineveryday activities may be one reason for better recovery of the entireleg muscles' strength after TKA.
It has been found that unilateral total knee replacement producesasymmetrical gait in bilateral severe OA knee patients [6,19]. In the cur-rent study, the step length and gait velocity in knee OA patients wereincreased significantly (respectively 12% and 19%) half a year afterTKA. The step length did not differ significantly six months after TKA(650 mm) from healthy controls (690 mm) but gait velocity wassignificantly prolonged (1.24 m s−1) as compared to control subjects(1.5 m s−1). In comparison, one year after TKA was patients' length ofstep 630 mm and walking speed 1.12 m s−1 [21]. In summary, nosignificant differences between the operated and non-operated legemerged in the temporospatial data of gait. One major contributor togood functional results may be the postsurgical rehabilitation duringwhich patients perform for several months after TKA home-basedexercises [15,16]. Therapeutic exercises, including land-based aerobicand strengthening exercises or physical activity are very important forpatients with knee osteoarthritis [22–24].
Unilateral TKA affects not only knee kinetics and kinematics of theoperated leg but also the motion of the non-operated knee [3,6]. Theunderstanding of the forces reaction impacting the lower limb jointspermits to prevent or to limit the overload. In the current study bothfactors indicating knee joint loading, the knee flexion moment and theknee joint power for the operated leg during mid stance, did not im-prove significantly half a year after TKA. Compared to healthy controls,named characteristics were significantly lower before, three and sixmonths after TKA. This result is consistent with the findings of previousstudies, confirming that the maximum external knee flexion momentduring weight acceptance is lower in arthroplasty groups compared tocontrols [7,25]. Despite the fact that preoperatively and three monthpost-operatively the knee joint loading for the non-operated leg wassignificantly weaker, it did not differ significantly from controls sameparameters six months after TKA. It has been found that the kneeadduction moment can be reduced by supervised exercise in middle-aged patients presenting early signs of knee OA [26]. A recent studyhas been found that 12 months after TKA the inter-limb differences inpeak knee flexion angle and range of motion persist [8], but 28 monthsfollowing recovery from unilateral TKA, peak vertical GRF and jointloading rates are similar in the involved and uninvolved limbs [27].Therefore it is essential to teach patients to shift the body weight tothe operated leg (total body weight is allowed one and a half monthafter surgery) together with appropriate exercises, in order to reducethe differences in leg extensor muscles strength, gait temporospatialand knee joint loading parameters between the operated and non-operated leg.
Preoperatively and six months after TKA, no correlation betweenthe isometricMVC force of the leg extensormuscles and knee joint load-ing for the operated leg was found. Three months after TKA a moderatenegative correlation between these characteristics was noted. Althoughthree months after TKA, both MVC force of leg extensor muscles andknee joint power for the operated leg were decreased, the correlation

220 D. Vahtrik et al. / The Knee 21 (2014) 216–220
analysis indicated that because of weak leg extensor muscles, an exces-sive load is applied to knee joint. In healthy controls, a moderate posi-tive correlation between leg extensor muscle strength and knee jointloading was noted. Despite that the relationship between quadricepsfemoris muscle strength and joint impact loading is non-significant[1], there is a study reporting positive relationship between musclestrength and gait performance [28]. Because individuals with motordisabilities use an intra-limb and between-limbs compensations tomaintain gait speed [13], it is essential to avoid potential bilateralarthroplasty or other secondary musculoskeletal disorders. Thereforeit is very important that patients with knee OA get individual rehabilita-tion both pre- and postoperatively.
The hypothesis set out for this study was confirmed—the weakerthe leg muscles, the more excessive load is applied to knee joint,and stronger knee surrounding muscles provide stronger knee jointloading during gait. This knowledge can be emphasized to patientsto train the knee surrounding muscles achieving a stable knee jointfor everyday activities or postpone potential TKA surgery.
In conclusion, the present study demonstrated that half a yearafter TKA leg extensor muscle isometric strength for the operated legachieved the preoperative level, remaining still significantly decreasedcompared with the non-operated leg and the respective characteristicsof controls. Temporospatial parameters of gait were at an equal levelwith the non-operated leg, the knee joint loading during mid stanceand gait velocity for the operated leg was six months after TKA signifi-cantly lower compared to healthy controls. Due to weak leg extensormuscles, on a third postoperative month patients applied an excessiveload to knee joint during mid stance of gait.
5. Conflict of interest
The authors confirm that there are no potential conflicts of interestincluding any personal or other relationships with other people or orga-nizations associatedwith thework submitted that could inappropriatelyinfluence their work.
Acknowledgment
The authors are very grateful to Professor Tiit Haviko, doctor AareMärtson and physiotherapist Galina Schneider for their contributionin subject's operative treatment and postoperative rehabilitation. Weare also indebted to Herje Aibast and Monika Rätsepsoo for their assis-tance with data collection. We acknowledge that this study was partlysupported by the Estonian Ministry of Education and Research projectNo SF0180030s07 and Estonian Science Foundation project No 7939.
References
[1] HuntMA, Hinman RS, Metcalf BR, Lim B-W,Wrigley TV, Bowles KA, et al. Quadricepsstrength is not related to gait impact loading in knee osteoarthritis. Knee 2010;17:296–302.
[2] Amin S, Luepongsak N, McGibbon CA, LaValley MP, Krebs DE, Felson DT. Kneeadduction moment and development of chronic knee pain in elders. Arthritis CareRes 2004;51:371–6.
[3] Alnahdi AH, Zeni JA, Snyder-Mackler L. Gait after unilateral knee arthroplasty:frontal plane analysis. J Orthop Res 2011;29:647–52.
[4] Winby CR, Loyd DG, Besier TF, Kirk TB. Muscle and external load contribution toknee joint contact loads during normal gait. J Biomech 2009;42:2294–300.
[5] Erler K, Neumann U, Brückner J, Venbrocks R, Anders C, Scholle HC. EMG mapping-applications and results in assessment of muscle coordination disorders in patientswith a knee endoprosthesis (knee TEP). Z Orthop Ihre Grenzgeb 2000;138:197–203.
[6] Huang HT, Chen CH, Chang JJ, Guo LY, Lin HT, Wu WL. Quantitative gait anlysisafter unilateral knee arthroplasty for patients with bilateral knee osteoarthritis.J Med Biol Eng 2007;28:11–6.
[7] Milner CE. Is gait normal after total knee arthroplasty? Systrematic review of theliterature. J Orthop Sci 2009;14:114–20.
[8] Yoshida Y, Mizner RL, Ramsey DK, Snyder-Macler L. Examining outcomes fromtotal knee arthroplasty and the relationship between quadriceps strength andknee function over time. Clin Biomech 2008;23:320–8.
[9] Mizner RL, Snyder-Mackler L. Altered loading during walking and sit-to-standis affected by quadriceps weakness after total knee arthroplasty. J Orthop Res2005;23:1083–90.
[10] Jonkers I, Stewart C, Spaepen A. The complementary role of the plantarflexors,hamstrings and gluteus maximus in the control of stance limb stability duringgait. Gait Posture 2003;17:264–72.
[11] Lloyd DG, Buchanan TS. Strategies of muscular support of varus and valgus isometricloads at the human knee. J Biomech 2001;34:1257–67.
[12] Erdemir A, McLean S, Herzog W, van de Bogert AJ. Model-based estimation ofmuscle forces exerted during movements. Clin Biomech 2007;22:131–54.
[13] Reguião LF, Nadeau S, Milot MH, Gravel D, Bourbonnais D, Gagnon D. Quantificationof level of effort at the plantarflexors and hip extensors and flexor muscles inhealthy subjects walking at different cadences. J Electromyogr Kinesiol 2005;15:393–405.
[14] Vahtrik D, Gapeyeva H, Aibast H, Ereline J, Kums T, Haviko T, et al. Quadricepsfemoris muscle function prior and after total knee arthroplasty in women withknee osteoarthritis. Knee Surg Sports Traumatol Arthrosc 2012;20:2013–21.
[15] Deyle GD, Allison SC, Matekel RL, Ryder MG, Stang JM, Gohdes DD, et al. Physicaltherapy treatment effectiveness for osteoarthritis of the knee: a randomizedcomparison of supervised clinical exercise and manual therapy procedures versusa home exercise program. Phys Ther 2005;85:1301–17.
[16] Hurley MV. Muscle dysfunction and effective rehabilitation of knee osteoarthritis:what we know and what we need to find out. Arthritis Care Res 2003;49:444–52.
[17] Müürsepp I, Aibast H, Pääsuke M. Motor performance and haptic perception inpreschool boys with specific imparment of expressive language. Acta Paediatr2011;100:1038–42.
[18] Davis RB, Õunpuu S, Tyburski D. Gage JR.A gait analysis data collection and reductiontechnique. Hum Mov Sci 1991;10:575–87.
[19] Mündermann A, Dyrby CO, Andriacchi TP. Secondary gait changes in patients withmedial compartment knee osteoarthritis. Arthritis Rheum 2005;52:2835–44.
[20] Rossi MD, Hasson S, Kohia M, Pineda E, Bryan W. Relationship of closed and openchain measures of strength with perceived physical function and mobility followingunilateral total knee replacement. J Geriatr Phys Ther 2007;30:23–7.
[21] Börjesson M, Weidenhielm L, Mattsson E, Olsson E. Gait and clinical measurementsin patients with knee osteoarthritis after surgery: a prospective 5-year follow-upstudy. Knee 2005;12:121–7.
[22] Brown K, Swank AM, Quesada PM, Nyland J, Malkani A, Topp R. Prehabilitationversus usual care before total knee arthroplasty: a case report comparing outcomeswithin the same individual. Physiother Theory Pract 2010;26:399–407.
[23] Rooks DS, Huang J, Bierbaum BE, Bolus SA, Rubano J, Connolly CE, et al. Effect of pre-operative exercise on measures of functional status in men and women undergoingtotal hip and knee arthroplasty. Arthritis Care Res 2006;55:700–8.
[24] Valderrabano V, Steiger C. Treatment and prevention of osteoarthritis through exerciseand sports. J Ageing Res 2011;10:1–6.
[25] Smith AJ, Lloyd DG, Wood DJ. Pre-surgery knee joint loading patterns duringwalking predict the presence and severity of anterior knee pain after total kneearthroplasty. J Orthop Res 2004;22:260–6.
[26] Thorstensson CA, Hendriksson M, von Porat A, Sjödahl C, Roos EM. The effect ofexercise on knee adduction moment in early knee osteoarthritis- a pilot study.Osteoarthritis Cartilage 2007;15:1163–70.
[27] Milner CE. Interlimb asymmetry during walking following unilateral total kneearthroplasty. Gait Posture 2008;28:69–73.
[28] Nadeau S, Gravel D, Arsenault AB, Bourbonnais D. A mechanical model to studythe relationship between gait speed and muscular strength. IEEE Trans RehabilEng 1996;4:386–94.
![Current Trends in Knee Arthroplasty · Current Trends in Knee Arthroplasty ... Pain is one of the major problem for patients underwent Total Knee Arthroplasty [TKA]; appropriate pain](https://img.pdfslide.us/doc/110x75/5afbb9d07f8b9abd588ff30e/current-trends-in-knee-trends-in-knee-arthroplasty-pain-is-one-of-the-major.jpg)