Embed Size (px)
Citation preview

ORIGINAL PAPER
Relationship and prognostic value of microvascular obstructionand infarct size in ST-elevation myocardial infarctionas visualized by magnetic resonance imaging
Suzanne de Waha • Steffen Desch • Ingo Eitel • Georg Fuernau •
Philipp Lurz • Anja Leuschner • Matthias Grothoff •
Matthias Gutberlet • Gerhard Schuler • Holger Thiele
Received: 9 August 2011 / Accepted: 23 January 2012 / Published online: 8 February 2012
� Springer-Verlag 2012
Abstract
Background Both infarct size and microvascular obstruc-
tion (MO) assessed by cardiac magnetic resonance imaging
(CMR) are known to be predictors for adverse clinical out-
come after ST-elevation myocardial infarction (STEMI). We
hypothesized that a ratio of MO and infarct size (MO/infarct
size) might be an even stronger predictor for outcome after
STEMI, which has not been investigated yet.
Methods STEMI patients reperfused by primary angio-
plasty (n = 438) within 12 h after symptom onset under-
went contrast-enhanced CMR at a median of 3 days
(interquartile range [IQR] 2;4) after the index event. MO
and infarct size were measured 15 min after intravenous
gadolinium injection. Follow-up was conducted after
19 months (IQR 10;27). The primary end point was defined
as a composite of death, non-fatal myocardial reinfarction
and congestive heart failure (major adverse cardiac events
[MACE]).
Results The extent of MO was only weakly correlated
with infarct size (r = 0.21, p \ 0.001). In a first multivar-
iate analysis including extent of MO, infarct size, ejection
fraction, end-systolic and end-diastolic volume, the extent
of MO was independently associated with MACE (hazard
ratio [HR] 1.03, 95%CI 1.02–1.05, p \ 0.001). In a second
multivariate analysis including MO/infarct size on top of
the extent of MO, infarct size, ejection fraction, end-systolic
and end-diastolic volume, MO/infarct size was identified as
the strongest independent predictor for MACE (HR 2.22
[95%CI 1.60–3.08, p \ 0.001]).
Conclusions In contrast to infarct size, MO is associated
with adverse clinical outcome after STEMI even after
adjustment for other CMR parameters. However, MO/
infarct size is a more powerful predictor for long-term
outcome after STEMI than either parameter alone.
Keywords Microvascular obstruction � Infarct size �ST-elevation myocardial infarction � Cardiac magnetic
resonance imaging
Introduction
In acute ST-elevation myocardial infarction (STEMI),
reperfusion has contributed to improved survival due to
limitation of myocardial necrosis. In daily clinical practice,
assessment of reperfusion success is performed using sur-
rogate markers including clinical, angiographic and elec-
trocardiographic parameters [1–4]. In contrast to indirect
markers of myocardial ischemia such as troponin [5–7], with
the introduction of cardiac magnetic resonance imaging
(CMR), direct visualization and quantification of infarct
expansion and microvascular obstruction (MO) have been
made possible [8–10]. Both infarct size and MO have been
shown to be prognostic markers for adverse clinical out-
come after STEMI [11–14]. We could previously demon-
strate that MO is a strong independent prognostic marker for
hard clinical end points, even after adjustment for traditional
outcome measures [15]. However, we observed that some
patients displayed large zones of infarcted myocardium
S. de Waha (&) � S. Desch � I. Eitel � G. Fuernau � P. Lurz �A. Leuschner � G. Schuler � H. Thiele
Department of Internal Medicine, Cardiology,
University of Leipzig-Heart Center,
Strumpellstr. 39, Leipzig 04289, Germany
e-mail: [email protected]
M. Grothoff � M. Gutberlet
Department of Diagnostic and Interventional Radiology,
University of Leipzig-Heart Center, Leipzig, German
123
Clin Res Cardiol (2012) 101:487–495
DOI 10.1007/s00392-012-0419-3

constituting of only small areas of MO, whereas others
displayed infarcts mainly constituting of MO. MO reflects
zones of impaired microcirculation and its development is
influenced by factors beyond the actual ischemic damage of
the myocyte, such as reperfusion injury, swelling and pro-
trusion of the endothelial cells, leading to compression of
the capillaries, microvascular plugging by neutrophils, red
blood cells and platelets and even rupture of the microves-
sels [16]. In contrast, the infarcted non-obstructed regions
display intact or less impaired microvasculature and it is
therefore likely that this leads to differing pathophysiolog-
ical consequences [17]. Thus, we hypothesized that a ratio of
MO and infarct size (MO/infarct size) might be a better
predictor for clinical outcome than either parameter on its
own, which has not been investigated so far. Furthermore,
previous studies analyzing the relation of infarct size and
MO led to inconsistent results and are limited due to small
study cohorts, analysis of combined end points including
weak components (including unstable angina, re-hospital-
ization and repeat revascularization) and relatively short
follow-up periods [11, 14, 18].
We therefore sought to analyze the comparative impact
and relation of (1) MO, (2) infarct size and (3) MO/infarct
size as predictors for long-term clinical outcome after
STEMI in a large prospective cohort.
Methods
Patients and study design
From February 2006 to July 2008, 512 consecutive STEMI
patients underwent primary percutaneous coronary inter-
vention (PCI). Inclusion criteria were the presence of
symptoms \12 h and ST-segment elevation in C2 leads
with C0.2 mV in the precordial leads or C0.1 mV in
extremity leads. Data from the current cohort were previ-
ously analyzed to study the impact of early versus late MO
on clinical outcome after STEMI [15]. Patients with prior
fibrinolysis and contraindications to CMR at study entry
were excluded. All patients received 500 mg of aspirin and
unfractionated heparin (60 IU/kg bodyweight) intrave-
nously prior to PCI. Clopidogrel with a 600-mg loading
dose and subsequently 75 mg for 12 months plus aspirin
indefinitely were mandatory. All other medications
including glycoprotein IIb/IIIa-inhibitors were adminis-
tered according to current guidelines [19, 20].
Primary PCI was performed according to standard
clinical practice. Additional thrombectomy was used
depending on thrombus burden in the infarct-related
artery. Coronary angiography of the target lesion, defined
as an angiographically significant stenosis with significant
ST-elevations in the corresponding ECG-leads, was performed
before and after PCI with the same projections to allow
optimal offline evaluation of the thrombolysis in myocar-
dial infarction (TIMI) flow of the infarct-related artery by
two independent observers [2].
The TIMI-risk score was calculated as described previ-
ously [4]. Early ST-segment resolution, expressed as per-
centage from before to after PCI, was evaluated by
measuring the sum of ST-segment elevation 20 ms after the
end of the QRS complex in the ECG before and after PCI [3].
The study was approved by the University of Leipzig
Ethics Committee and all patients gave written informed
consent.
CMR imaging
All patients were examined at rest in the supine position
with a whole-body 1.5-T MR scanner (Gyroscan Intera CV,
Philips Medical Systems, Best, The Netherlands) equipped
with a five-element cardiac phased-array coil for signal
reception. A vectorcardiogram for gating and triggering
was used. To define the orientation of the heart, a real-time
interactive tool was applied. All images were acquired
during breath-hold at end expiration.
Left ventricular (LV) function was assessed by a stan-
dard steady-state free precession technique acquiring short-
axis slices from base to apex and also horizontal and vertical
long-axis views. Delayed enhancement short-axis images
covering the whole ventricle were acquired at mid-diastole
approximately 15 min after bolus injection (0.2 mmol/kg/
bodyweight) of gadolinium-chelate (Gadovist, Schering,
Germany). A three-dimensional inversion-recovery (IR)
turbo gradient echo sequence (typical spatial resolution
2.0 9 2.0 9 5 mm, prepulse delay 175–300 ms) was used
for image acquisition. The individual IR prepulse delay was
defined to obtain the maximal contrast between viable and
necrotic myocardium. Additionally, myocardial edema
imaging was performed to differentiate between acute and
chronic infarction, acquiring three short-axis slices using a
T2-weighted turbo spin-echo sequence before contrast
administration. Only delayed enhancement displaying the
typical pattern of myocardial infarction with corresponding
myocardial edema was interpreted as the CMR equivalent
for the acute event and thus was further analyzed [21].
CMR measurements were performed off-line in a CMR
core laboratory by observers blinded to clinical, angio-
graphic and electrocardiographic parameters. The perfor-
mance of the CMR core laboratory has been demonstrated
previously [22, 23]. LV ejection fraction (EF), end-diastolic
and end-systolic volumes were calculated from the short-
axes functional views. LV function was graded according to
the corresponding EF: \25, 25–35, 35–45, 45–55 and
[55%. LV mass was assessed for the delayed enhancement
images by tracing the endocardial and epicardial contours
488 Clin Res Cardiol (2012) 101:487–495
123

manually; papillary muscles were included. Once the
myocardial contours were identified, the infarct size was
determined by manual delineation of delayed enhancement
in each of the short-axis images. MO was assessed 1 and
15 min after gadolinium injection (early and persistent
MO). The current analysis was limited to persistent MO due
to its superior prognostic value in comparison to early MO
[13, 24, 25]. The obstructed area within the infarction of the
short-axes slices was manually drawn. MO was analyzed
qualitatively (=presence of MO) and quantitatively (=extent
of MO expressed as percentage of LV mass [%LV]). Infarct
size was expressed as %LV. The MO/infarct size ratio was
calculated for all patients.
End points and definitions
Clinical follow-up was conducted via a structured ques-
tionnaire by telephone. Any clinical event was verified by
hospital charts, or direct contact with the treating physician
or contact with the local government registration. The
follow-up interviewer was not aware of the results of the
CMR studies.
The primary end point was defined as major adverse
cardiac events (MACE) comprising a composite of death,
non-fatal myocardial reinfarction and congestive heart
failure. Death was defined as death from any cause; how-
ever, it was further classified as cardiac and non-cardiac
death. Death was regarded as cardiac in origin unless
obvious non-cardiac causes could be identified. In case of
any doubt, death was counted as cardiac. The diagnosis of
reinfarction during the index hospitalization was based on
clinical symptoms, new ST-segment changes and an
increase in the creatine kinase-MB levels above the refer-
ence limits in patients with normalized values or if there
was an increase of C20% from the last non-normalized
measurement [26]. At follow-up, any new ischemic symp-
toms requiring hospital admission accompanied by troponin
elevation were defined as recurrent myocardial infarction
[26]. New heart failure was defined as any congestive heart
failure (rales, dyspnea, New York Heart Association class
III–IV) leading to medical attention [24 h after the index
event. In patients experiencing[1 event, the first event was
chosen for the combined clinical end point. When C1
events occurred simultaneously, the most severe event was
chosen (death [ myocardial reinfarction [ congestive
heart failure). All outcomes were adjudicated by a clinical
events committee unaware of the CMR results.
Statistical analysis
Each categorical variable is expressed as the number and
percentage of patients. Continuous data are reported as
medians with the corresponding interquartile range (IQR).
For comparison of continuous data, the nonparametric
Wilcoxon rank-sum test was used. Survival curves were
estimated using Kaplan–Meier distributions with log-rank
comparison to illustrate the time-dependent occurrence of
the combined clinical end point in relation to the presence
of MO, as well as to infarct size and MO/infarct size for
Cmedian versus \median.
We fitted univariate Cox proportional-hazards models to
estimate the hazard ratios (HR) for the combined clinical
end point. All parameters with a p value \0.05 entered
multivariate analysis, which was performed using a stepwise
algorithm. A first multivariate Cox regression analysis was
performed including extent of MO, infarct size, EF, end-
systolic and end-diastolic volume. A second multivariate
Cox regression analysis was fitted including MO/infarct size
as well as the extent of MO, infarct size, EF, end-systolic
and end-diastolic volume. In the subgroup of patients dis-
playing extensive myocardial damage defined as an infarct
size Cmedian, a third multivariate analysis including the
parameters of the second multivariate model was per-
formed. In univariate and multivariate Cox regression
analysis, parameters were included as continuous variables.
All statistical tests were performed with SPSS software,
version 17.0 (SPSS Inc., Chicago, Il). All probability val-
ues were two tailed with a = 0.05 and all confidence
intervals (CI) were calculated to the 95th percentile.
Results
Of the 512 STEMI patients referred for primary PCI, 438
underwent CMR 2–7 days (in median 3 days [IQR 2;4])
after the index event with a similar time delay between
patients with and without MO (p = 0.65). In addition,
infarct size did not differ significantly according to the time
of CMR image acquisition (p = 0.73). In total, 74 patients
had to be excluded from CMR due to claustrophobia
(n = 19), death before CMR (n = 18), refusal (n = 15),
prior pacemaker implantation (n = 5), obesity (n = 7),
metallic implant (n = 1), dyspnea (n = 2) or technical
reasons (n = 7). Patient follow-up was performed at a
median of 19 months (IQR 11;27) after index infarction
and was completed for 97% of the patients (n = 423).
All patients displayed myocardial edema in the infarct
region indicative of acute myocardial infarction. In addition,
10% of all patients (n = 42) displayed delayed enhance-
ment with a typical post-infarction pattern, but without
corresponding edema in T2-weighted imaging. These
regions were interpreted as chronic or prior myocardial
infarctions and were therefore not further analyzed. The
median infarct size in the overall study cohort was 17.7%LV
(IQR 8.5;28.0) and MO was detected in 68% (n = 296) of
patients involving 1.2%LV (IQR 0.6;3.0). Infarct size and
Clin Res Cardiol (2012) 101:487–495 489
123

MO were only weakly correlated (r = 0.21). The median
value of MO/infarct size was 0.07 (IQR 0.03;0.13) ranging
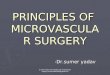
from 0 to 1. A typical patient example showing infarct size
and the corresponding MO is shown in Fig. 1.
Baseline clinical characteristics as well as electrocar-
diographic, angiographic and CMR data are shown in
Table 1. Importantly, 89.7% of all patients (n = 379)
received glycoprotein IIb/IIIa-inhibitors. However, we
could not observe an association between administration of
glycoprotein IIb/IIIa-inhibitors and MO (presence of MO:
p = 0.38/extent of MO: p = 0.22).
Outcome analysis
Overall, 69 events were recorded throughout the follow-up
period consisting of death in 25 patients (cardiac death
n = 20, stroke n = 4, cancer n = 1), non-fatal myocardial
infarctions in 19 and new congestive heart failure in 25.
Both the extent of MO and infarct size were significantly
greater in patients with MACE compared to patients
without MACE (MO: 1.9%LV [IQR 0.8;3.6] vs. 1.1%LV
[IQR 0.5;2.9], p \ 0.001; infarct size: 24.7%LV [IQR
11.2;34.9], vs. 16.2%LV [IQR 7.9;26.2], p \ 0.001). Fur-
thermore, patients in whom the combined clinical end point
occurred demonstrated a significantly greater value of MO/
infarct size compared to patients who displayed an event-
free survival throughout the follow-up period (0.6 [0.3;0.2]
vs. 0.3 [0;0.1], p = 0.002).
Prognostic evaluation
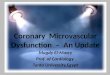
Kaplan–Meier curves revealed a significant association of
MO, infarct size and MO/infarct size with the occurrence
of MACE (Fig. 2a–d).
Fig. 1 Patient examples. Assessment of microvascular obstruction
(MO) and infarct size using delayed enhancement imaging in two
different patients with anterior myocardial infarction. Patient 1 upper
row without and with infarct size (green) and MO (red) contours (a,
b). Patient 2 lower row without and with infarct size and MO contours
(c, d). Note that the MO/infarct size differs between patients 1 and 2
490 Clin Res Cardiol (2012) 101:487–495
123

In comparison to the extent of MO, infarct size, EF, and
end-systolic and end-diastolic volume, MO/infarct size
demonstrated the strongest unadjusted association with
MACE (Table 2).
In a first multivariate analysis including extent of MO,
infarct size, EF as well as end-systolic and end-diastolic
volume, the extent of MO remained independently associ-
ated with MACE (HR 1.03, 95%CI 1.02–1.05, p \ 0.001;
Table 3).
In a second multivariate analysis including MO/infarct
size on top of the parameters included in the first model, MO/
infarct size was identified as the strongest independent pre-
dictor for MACE (HR 2.22; 95%CI 1.60–3.08, p \ 0.001;
Table 4).
In the subgroup of patients displaying extensive myo-
cardial damage defined as an infarct size Cmedian, a third
multivariate analysis including the parameters of the second
multivariate model, MO/infarct size was the only indepen-
dent predictor for MACE (HR 2.03; 95%CI 1.38–2.98,
p \ 0.001).
Discussion
The main findings of this large outcome analysis in STEMI
patients using CMR parameters can be summarized as
follows: (1) presence and extent of MO, infarct size and
MO/infarct size were associated with adverse clinical
outcome defined by death, reinfarction and congestive
heart failure in univariate analysis; (2) in contrast to infarct
size, the extent of MO was independently associated with
MACE; (3) the newly introduced MO/infarct size ratio is
an even stronger predictor for long-term prognosis after
STEMI than either parameter alone.
With the introduction of CMR, it has been made pos-
sible to directly visualize and quantify regions of acute
myocardial infarction and identify zones of impaired
microperfusion, also referred to as MO. In animal models,
an almost exact relationship between the extent and shape
of MO and infarct size assessed by CMR and histopa-
thological results could be demonstrated [9, 27]. The
results of previous trials examining MO and infarct size as
outcome measures have been ambiguous: Wu et al. [11]
reported a significant association of infarct size with worse
clinical outcome independent of other CMR parameters,
such as MO. In contrast, in other studies, infarct size did
not remain significant in multivariate analysis adjusting for
traditional CMR parameters [12, 13]. Our results could
confirm these findings, which are supported by previous
studies identifying MO as a stronger predictor for LV
remodeling in the post-infarction period than infarct size
[24, 28]. This might be explained in part by altered local
properties in the presence of MO, as well as pre-existing
patient characteristics influencing both the development of
MO and post-infarction outcome, such as endothelial dys-
function [16, 29].
Since infarct size and MO have both been associated
with adverse clinical outcome after STEMI, we hypothe-
sized that the analysis of a ratio of the two parameters
might add incremental prognostic value, as the extent of
MO can widely differ in infarctions of similar size as
demonstrated in Fig. 1. Indeed, we could demonstrate a
strong prognostic association of MO/infarct size with long-
term clinical outcome after STEMI. The pathophysiologi-
cal consequences and the consecutive impact on functional
recovery after STEMI of an expansion of MO and infarct
size might be slightly different. While MO reflects truly
non-viable regions associated with greater apoptosis and
cellular loss leading to local involution and wall thinning
[30], infarct expansion might also increase wall stress in
adjacent or remote non-infarcted regions [31]. The extent
of infarct size and the development of MO are influenced
by diverging parameters, as MO is known to be associated
with factors beyond the ischemic damage itself, such
as reperfusion injury. Our data emphasize, therefore, the
Table 1 Characteristics of the study cohort
All patients (n = 423)
Age, years 65 (55;73)
Male sex, n (%) 318 (75.4)
Cardiovascular risk factors, n (%)
Hypertension 287 (68.3)
Diabetes mellitus 111 (26.4)
Hyperlipoproteinemia 140 (33.3)
Current smoking 177 (42.1)
BMI, kg/m2 27 (25;30)
Maximal creatine kinase, lmol/l 6.8 (2.8;20.6)
Maximal creatine kinase-MB, lmol/l 1.1 (0.5;2.7)
TIMI-risk score 3.0 (2.0;5.0)
ST-segment resolution, % 73 (50;100)
Angiographic findings, n (%)
TIMI-flow pre-PCI: 0–II 252 (64.8)
TIMI-flow pre-PCI: III 137 (35.2)
TIMI-flow post-PCI: 0–II 20 (5.1)
TIMI-flow post-PCI: III 372 (94.9)
Magnetic resonance imaging
Infarct size, %LV 17.7 (8.5;28.0)
Extent of MO, %LV 1.2 (0.6;3.0)
LV–EF, % 50.1 (40.9;58.4)
LV end-diastolic volume index, mL/m2 143 (121;167)
LV end-systolic volume index, mL/m2 72 (50;93)
Glycoprotein IIb/IIIa-inhibitor use, n (%) 379 (89.7)
Continuous data are presented as median and interquartile range
BMI body mass index (weight in kilograms divided by the square of
the height in meters), TIMI thrombolysis in myocardial infarction,
PCI percutaneous coronary intervention, MO microvascular obstruc-
tion, LV left ventricle, EF ejection fraction
Clin Res Cardiol (2012) 101:487–495 491
123

importance of reperfusion strategies aiming at a reduction
of infarct size while preserving microvascular function,
such as thrombectomy. Therefore, it is conceivable that
MO/infarct size represents a broader reflection of the
degree of injury after STEMI than the separate analysis and
may therefore be considered as an outcome measure for
future reperfusion studies. Focusing solely on infarct size
independent of the microvascular state might not improve
the clinical outcome in patients. As CMR visualizes and
quantifies both infarct size and MO accurately, it may be
judged as a principal imaging technique in studies evalu-
ating reperfusion success in the setting of STEMI.
Some limitations of the current trial need to be addres-
sed. First, we performed CMR in median 3 days (IQR 2;4)
after the index event. Despite previously published data on
animals indicating a stable phase of infarct size and MO
between day 2 and 7 after the acute ischemic event [32],
there is emerging evidence that infarct size assessed by
CMR decreases within the first week after STEMI [33–36].
However, these data are limited due to small study sample
sizes and a selection in patients. In addition, the exact
evolvement of post-infarction CMR parameters within the
first few days after the index event has not been investi-
gated in a large cohort of unselected STEMI patients so far.
Fig. 2 a Major adverse cardiovascular events with and without
microvascular obstruction. Kaplan–Meier curve for the cumulative
incidence of major adverse cardiac events in patients with and without
microvascular obstruction (MO). b Major adverse cardiovascular
events depending on median infarct size. Kaplan–Meier curve for the
cumulative incidence of major adverse cardiac events in patients with
an infarct size \median versus Cmedian. c Major adverse cardio-
vascular events depending on median ratio of microvascular obstruc-
tion/infarct size. Kaplan–Meier curve for the cumulative incidence of
major adverse cardiac events in patients with a ratio of microvascular
obstruction and infarct size (MO/infarct size) \median versus
Cmedian. d Major adverse cardiovascular events depending on the
presence of microvascular obstruction and the median ratio of
microvascular obstruction/infarct size. Kaplan–Meier curve for the
cumulative incidence of major adverse cardiac events in patients
without microvascular obstruction (MO) versus with MO, and a ratio
of MO and infarct size (MO/infarct size) \median versus with MO
and a MO/infarct size Cmedian
492 Clin Res Cardiol (2012) 101:487–495
123

In the current study, CMR image acquisition was per-
formed in a relatively narrow period of time in comparison
to many previously published studies (in median 3 days
after STEMI, IQR 2;4). However, we cannot definitely rule
out potential changes of infarct size and MO within the first
days after myocardial ischemia, although it is unlikely that
these changes would substantially influence the current
results. Indeed, neither infarct size nor MO was signifi-
cantly influenced by the timing of CMR assessment fol-
lowing infarction. Second, CMR image analysis was
performed by manual delineation. Recently, an alternative
method using automatic planimetry for quantification of
infarct size and MO has been suggested to achieve higher
reproducibility. However, the optimal method for automatic
analysis has not been fully established [37–39] and notably
our CMR core laboratory has proven excellent reproduc-
ibility and low interobserver and intraobserver variability
for manual analysis of infarct size [22, 23]. Given these
issues, we prefer to planimeter the infarct manually in our
core laboratory using experienced readers who can care-
fully segment myocardial borders and can account for
artifacts, no-reflow regions and areas with intermediate
image intensity. Third, the study sample size is still limited
to draw definitive conclusions on clinical outcome. Finally,
all patients were treated at a single high-volume tertiary
referral center. As a consequence, the results may not be
generalized to the entire STEMI population.
In conclusion, in contrast to infarct size, the extent of
MO is associated with adverse clinical outcome after
STEMI even after adjustment for other CMR parameters.
However, MO/infarct size is an even more powerful pre-
dictor for long-term outcome after STEMI.
Conflict of interest The authors have nothing to disclose.
References
1. Ndrepepa G, Mehilli J, Schulz S, Iijima R, Keta D, Byrne RA,
Pache J, Seyfarth M, Schomig A, Kastrati A (2008) Prognostic
significance of epicardial blood flow before and after percuta-
neous coronary intervention in patients with acute coronary
syndromes. J Am Coll Cardiol 52(7):512–517
2. TIMI Study Group (1985) The thrombolysis in myocardial
infarction (TIMI) trial: phase 1 findings. N Engl J Med 312:932–
936. doi:10.1056/NEJM198504043121435
3. Schroder R (2004) Prognostic impact of early ST-segment reso-
lution in acute ST-elevation myocardial infarction. Circulation
110:e506–e510. doi:10.1161/01.CIR.0000147778.05979.E6
4. Morrow DA, Antman EM, Charlesworth A, Cairns R, Murphy SA,
de Lemos JA, Giugliano RP, McCabe CH, Braunwald E (2000)
TIMI risk score for ST-elevation myocardial infarction: a con-
venient, bedside, clinical score for risk assessment at presentation.
Circulation 102:2031–2037. doi:10.1161/01.CIR.102.17.2031
5. Klug G, Mayr A, Mair J, Schocke M, Nocker M, Trieb T, Jaschke
W, Pachinger O, Metzler B (2011) Role of biomarkers in
assessment of early infarct size after successful p-PCI for STEMI.
Clin Res Cardiol 100(6):501–510. doi:10.1007/s00392-010-
0273-0
6. Neizel M, Futterer S, Steen H, Giannitsis E, Reinhardt L,
Lossnitzer D, Lehrke S, Jaffe AS, Katus HA (2009) Predicting
Table 3 Multivariate Cox regression models for major adverse car-
diac events and traditional CMR parameters including infarct size and
microvascular obstruction
MACE (n = 69)
HR (95%CI) p value
Extent of MO, %LV 1.03 (1.02–1.05) \0.001
LV-EF, % 1.66 (1.34–2.04) \0.001
Infarct size, %LV – –
LV end-diastolic volume
index, mL/m2– –
LV end-systolic volume
index, mL/m2– –
MACE major adverse cardiac event, MO microvascular obstruction,
LV left ventricle, EF ejection fraction
Table 4 Multivariate Cox regression models for major adverse car-
diac events and traditional CMR parameters, and the ratio of micro-
vascular obstruction and infarct size
MACE (n = 69)
HR (95%CI) p value
MO/infarct size 2.22 (1.60–3.08) \0.001
LV–EF, % 1.74 (1.40–2.15) \0.001
Extent of MO, %LV – –
Infarct size, %LV – –
LV end-diastolic volume
index, mL/m2– –
LV end-systolic volume
index, mL/m2– –
MACE major adverse cardiac event, MO/infarct size ratio of micro-
vascular obstruction and infarct size, EF ejection fraction, MOmicrovascular obstruction, LV left ventricle
Table 2 Unadjusted hazard ratios for major adverse cardiac events
MACE (n = 69)
HR (95%CI) p value
MO/infarct size 1.83 (1.34–2.50) \0.001
Extent of MO, %LV 1.03 (1.01–1.04) \0.001
Infarct size, %LV 1.03 (1.01–1.05) \0.001
LV-EF, % 1.04 (1.02–1.06) \0.001
LV end-diastolic volume
index, mL/m21.00 (0.99–1.01) 0.28
LV end-systolic volume
index, mL/m21.02 (1.01–1.03) 0.001
MACE major adverse cardiac event, MO/infarct size ratio of micro-
vascular obstruction and infarct size, MO microvascular obstruction,
LV left ventricle, EF ejection fraction
Clin Res Cardiol (2012) 101:487–495 493
123

microvascular obstruction with cardiac troponin T after acute
myocardial infarction: a correlative study with contrast-enhanced
magnetic resonance imaging. Clin Res Cardiol 98(9):555–562.
doi:10.1007/s00392-009-0041-1
7. Neizel M, Steen H, Korosoglou G, Lossnitzer D, Lehrke S,
Ivandic BT, Katus HA, Giannitsis E (2009) Minor troponin T
elevation in patients 6 months after acute myocardial infarction:
an observational study. Clin Res Cardiol 98(5):297–304. doi:
10.1007/s00392-009-0002-8
8. Kim RJ, Fieno DS, Parrish TB, Harris K, Chen E-L, Simonetti O,
Bundy J, Finn JP, Klocke FJ, Judd RM (1999) Relationship of
MRI delayed contrast enhancement to irreversible injury, infarct
age, and contractile function. Circulation 100:1992–2002
9. Rochitte CE, Lima JAC, Bluemke DA, Reeder SB, McVeigh ER,
Furuta T, Becker LC, Melin JA (1998) Magnitude and time
course of microvascular obstruction and tissue injury after acute
myocardial infarction. Circulation 98:1006–1014
10. Schujif JD, Kaandorp TA, Lamb HJ, van der Geest RJ, Viergever
EP, van der Wall EE, de Roos A, Bax JJ (2004) Quantification of
myocardial infarct size and transmurality by contrast-enhanced
magnetic resonance imaging. Am J Cardiol 94:284–288
11. Wu KC, Zerhouni EA, Judd RM, Lugo-Olivieri CH, Barouch LA,
Schulman SP, Blumenthal RS, Lima JAC (1998) Prognostic
significance of microvascular obstruction by magnetic resonance
imaging in patients with acute myocardial infarction. Circulation
97:765–772. doi:10.1161/01.CIR.97.8.765
12. Hombach V, Grebe O, Merkle N, Waldenmaier S, Hoher M,
Kochs M, Wohrle J, Kestler HA (2005) Sequelae of acute myo-
cardial infarction regarding cardiac structure and function and
their prognostic significance as assessed by magnetic resonance
imaging. Eur Heart J 26:549–557
13. Cochet AA, Lorgis L, Lalande A, Zeller M, Beer JC, Walker PM,
Touzery C, Wolf JE, Brunotte F, Cottin Y (2009) Major prog-
nostic impact of persistent microvascular obstruction as assessed
by contrast-enhanced cardiac magnetic resonance in reperfused
acute myocardial infarction. Eur Radiol 19(9):2117–2126. doi:
10.1007/s00330-009-1395-5
14. Larose E, Rodes-Cabau J, Pibarot P, Rinfret S, Proulx G, Nguyen
CM, Dery JP, Gleeton O, Roy L, Noel B, Barbeau G, Rouleau J,
Boudreault JR, Amyot M, De Larochelliere R, Bertrand OF
(2010) Predicting late myocardial recovery and outcomes in the
early hours of ST-segment elevation myocardial infarction tra-
ditional measures compared with microvascular obstruction,
salvaged myocardium, and necrosis characteristics by cardio-
vascular magnetic resonance. J Am Coll Cardiol 55(22):2459–
2469. doi:10.1016/j.jacc.2010.02.033
15. de Waha S, Desch S, Eitel I, Fuernau G, Zachrau J, Leuschner A,
Zachrau J, Schuler G, Thiele H (2010) Impact of early versus late
microvascular obstruction assessed by magnetic resonance
imaging on long-term outcome after ST-elevation myocardial
infarction—a comparison to traditional prognostic markers. Eur
Heart J 31(21):2660–2668. doi:10.1093/eurheartj/ehq247
16. Niccoli G, Burzotta F, Galiuto L, Crea F (2009) Myocardial no-
reflow in humans. J Am Coll Cardiol 54:281–292
17. Bekkers SC, Yazdani SK, Virmani R, Waltenberger J (2010)
Microvascular obstruction: underlying pathophysiology and
clinical diagnosis. J Am Coll Cardiol 55(16):1649–1660. doi:
10.1016/j.jacc.2009.12.037
18. Hombach V, Grebe O, Merkle N, Waldenmaier S, Hoher M, Kochs
M, Wohrle J, Kestler HA (2005) Sequelae of acute myocardial
infarction regarding cardiac structure and function and their
prognostic significance as assessed by magnetic resonance imag-
ing. Eur Heart J 26(6):549–557. doi:10.1093/eurheartj/ehi147
19. Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA,
Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA,
Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC (2004)
ACC/AHA guidelines for the management of patients with ST-
elevation myocardial infarction—executive summary. Circula-
tion 110:588–636. doi:10.1161/01.CIR.0000134791.68010.FA
20. Van de Werf F, Bax J, Betriu A, Blomstrom-Lundqvist C, Crea F,
Falk V, Filippatos G, Fox K, Huber K, Kastrati A, Rosengren A,
Steg PG, Tubaro M, Verheugt F, Weidinger F, Weis M (2008)
Management of acute myocardial infarction in patients presenting
with persistent ST-segment elevation: The Task Force on the
management of ST-segment elevation acute myocardial infarc-
tion of the European Society of Cardiology. Eur Heart J
29(23):2909–2945. doi:10.1093/eurheartj/ehn416
21. Abdel-Aty H, Zagrosek A, Schulz-Menger J, Taylor AJ, Mess-
roghli D, Kumar A, Gross M, Dietz R, Friedrich MG (2004)
Delayed enhancement and T2-weighted cardiovascular magnetic
resonance imaging differentiate acute from chronic myocardial
infarction. Circulation 109:2411–2416. doi:10.1161/01.CIR.
0000127428.10985.C6
22. Thiele H, Kappl MJ, Conradi S, Niebauer J, Hambrecht R,
Schuler G (2006) Reproducibility of chronic and acute infarct
size measurement by delayed enhancement magnetic resonance
imaging. J Am Coll Cardiol 47(8):1641–1645. doi:10.1016/j.jacc.
2005.11.065
23. Desch S, Engelhardt H, Meissner J, Eitel I, Sareban M, Fuernau
G, de Waha S, Grothoff M, Gutberlet M, Schuler G, Thiele H
(2011) Reliability of myocardial salvage assessment by cardiac
magnetic resonance imaging in acute reperfused myocardial
infarction. Int J Cardiovasc Imaging. doi:10.1007/s10554-011-
9802-9 (Epub ahead of print)
24. Nijveldt R, Beek AM, Hirsch A, Stoel MG, Hofman MBM,
Umans VAWM, Algra PR, Twisk JWR, van Rossum AC (2008)
Functional recovery after acute myocardial infarction: compari-
son between angiography, electrocardiography, and cardiovas-
cular magnetic resonance measures of microvascular injury. J Am
Coll Cardiol 52(3):181–189
25. Nijveldt R, Beek AM, Hofman MB, Umans VA, Algra PR,
Spreeuwenberg MD, Visser CA, van Rossum AC (2007) Late
gadolinium-enhanced cardiovascular magnetic resonance evalu-
ation of infarct size and microvascular obstruction in optimally
treated patients after acute myocardial infarction. J Cardiovasc
Magn Reson 9:765–770
26. Thygesen K, Alpert JS, White HD, Jaffe AS, Apple FS, Galvani
M, Katus HA, Newby LK, Ravkilde J, Chaitman B, Clemmensen
PM, Dellborg M, Hod H, Porela P, Underwood R, Bax JJ, Beller
GA, Bonow R, Van der Wall EE, Bassand JP, Wijns W, Ferguson
TB, Steg PG, Uretsky BF, Williams DO, Armstrong PW, Antman
EM, Fox KA, Hamm CW, Ohman EM, Simoons ML, Poole-
Wilson PA, Gurfinkel EP, Lopez-Sendon JL, Pais P, Mendis S,
Zhu JR, Wallentin LC, Fernandez-Aviles F, Fox KM, Park-
homenko AN, Priori SG, Tendera M, Voipio-Pulkki LM, Vaha-
nian A, Camm AJ, De Caterina R, Dean V, Dickstein K,
Filippatos G, Funck-Brentano C, Hellemans I, Kristensen SD,
McGregor K, Sechtem U, Silber S, Widimsky P, Zamorano JL,
Morais J, Brener S, Harrington R, Morrow D, Lim M, Martinez-
Rios MA, Steinhubl S, Levine GN, Gibler WB, Goff D, Tubaro
M, Dudek D, Al-Attar N (2007) Universal definition of
myocardial infarction. Circulation 116(22):2634–2653. doi:
10.1161/CIRCULATIONAHA.107.187397
27. Amado LC, Gerber BL, Gupta SN, Rettmann DW, Szarf G,
Schock R, Nasir K, Kraitchman DL, Lima JAC (2004) Accurate
and objective infarct sizing by contrast-enhanced magnetic res-
onance imaging in a canine myocardial infarction model. J Am
Coll Cardiol 44:2383–2389
28. Orn S, Manhenke C, Greve OJ, Larsen AI, Bonarjee VV,
Edvardsen T, Dickstein K (2009) Microvascular obstruction is a
major determinant of infarct healing and subsequent left ven-
tricular remodelling following primary percutaneous coronary
494 Clin Res Cardiol (2012) 101:487–495
123

intervention. Eur Heart J 30(16):1978–1985. doi:10.1093/eurheartj/
ehp219
29. Reffelmann T, Kloner RA (2002) The ‘‘no-reflow’’ phenomenon:
basic science and clinical correlates. Heart 87:162–168
30. Rogers WJ Jr, Kramer CM, Geskin G, Hu YL, Theobald TM,
Vido DA, Petruolo S, Reichek N (1999) Early contrast-enhanced
MRI predicts late functional recovery after reperfused myocardial
infarction. Circulation 99(6):744–750
31. Kramer CM, Lima JA, Reichek N, Ferrari VA, Llaneras MR,
Palmon LC, Yeh IT, Tallant B, Axel L (1993) Regional differ-
ences in function within noninfarcted myocardium during left
ventricular remodeling. Circulation 88(3):1279–1288
32. Wu KC, Kim RJ, Bluemke DA, Rochitte CE, Zerhouni EA,
Becker LC, Lima JAC (1998) Quantification and time course of
microvascular obstruction by contrast-enhanced echocardiogra-
phy and magnetic resonance imaging following acute myocardial
infarction and reperfusion. J Am Coll Cardiol 32:1756–1764. doi:
10.1016/S0735-1097(98)00429-X
33. Dall’Armellina E, Karia N, Lindsay AC, Karamitsos TD, Ferreira
V, Robson MD, Kellman P, Francis JM, Forfar C, Prendergast
BD, Banning AP, Channon KM, Kharbanda RK, Neubauer S,
Choudhury RP (2011) Dynamic changes of edema and late
gadolinium enhancement after acute myocardial infarction and
their relationship to functional recovery and salvage index. Circ
Cardiovasc Imaging 4(3):228–236. doi:10.1161/CIRCIMAGING.
111.963421
34. Engblom H, Hedstrom E, Heiberg E, Wagner GS, Pahlm O,
Arheden H (2009) Rapid initial reduction of hyperenhanced
myocardium after reperfused first myocardial infarction suggests
recovery of the peri-infarction zone: one-year follow-up by MRI.
Circ Cardiovasc Imaging 2(1):47–55. doi:10.1161/CIRCIMAGING.
108.802199
35. Ibrahim T, Hackl T, Nekolla SG, Breuer M, Feldmair M, Schomig
A, Schwaiger M (2011) Acute myocardial infarction: serial car-
diac MR imaging shows a decrease in delayed enhancement of the
myocardium during the 1st week after reperfusion. Radiology
254(1):88–97. doi:10.1148/radiol.09090660
36. Mather AN, Fairbairn TA, Artis NJ, Greenwood JP, Plein S
(2011) Timing of cardiovascular MR imaging after acute myo-
cardial infarction: effect on estimates of infarct characteristics
and prediction of late ventricular remodeling. Radiology. doi:
10.1148/radiol.11110228
37. Beek AM, Bondarenko O, Afsharzada F, van Rossum AC (2009)
Quantification of late gadolinium enhanced CMR in viability
assessment in chronic ischemic heart disease: a comparison to
functional outcome. J Cardiovasc Magn Reson 11:6. doi:10.1186/
1532-429X-11-6
38. Bondarenko O, Beek AM, Hofman MB, Kuhl HP, Twisk JW, van
Dockum WG, Visser CA, van Rossum AC (2005) Standardizing
the definition of hyperenhancement in the quantitative assessment
of infarct size and myocardial viability using delayed contrast-
enhanced CMR. J Cardiovasc Magn Reson 7(2):481–485
39. Flett AS, Hasleton J, Cook C, Hausenloy D, Quarta G, Ariti C,
Muthurangu V, Moon JC (2011) Evaluation of techniques for the
quantification of myocardial scar of differing etiology using
cardiac magnetic resonance. JACC Cardiovasc Imaging 4(2):
150–156. doi:10.1016/j.jcmg.2010.11.015
Clin Res Cardiol (2012) 101:487–495 495
123