Embed Size (px)
Citation preview

Relaparotomies: Why is Mortality Higher?Ercan Gedik, Kazym Söylemez, Sadullah Girgin, Ersin Uysal, Ybrahim Taçyyldyz1
AbstractBackground: Relaparotomy is sometimes required forcomplications that develop after abdominal surgery,but it is associated with high mortality. We aimed toinvestigate the independent risk factors related tomortality in patients that undergo relaparotomies.Materials and Methods: One hundred and fourteenpatients who had relaparatomies were evaluated. Riskfactors studied were patient characteristics, cause ofthe first operation, condition of the first operation,systemic diseases, presence of peritonitis, relaparoto-my interval, cause of relaparatomy, APACHE II score,transfused blood units, number of relaparatomies,length of hospital stay, and mortality. In order todetermine the independent risk factors, we carried outmultivariate logistic regression analysis.Results: There were 75 male and 39 female patientswith a mean age of 46.06 ± 19.98 (15–84). The mostcommon reasons for relaparotomy were leakage fromintestinal primary repair or anastomosis (29.8%).Mortality developed in 55 (48.2%) patients undergoingrelaparatomy. Intestinal necrosis (p = 0038) and intra-abdominal sepsis (p = 0.027) were found to be riskfactors in mortality. In multivariate logistic regressionanalysis, advanced age (OR 0.966, p = 0. 0.017) andAPACHE II score ‡20 (OR 0.137, p < 0.0001) were foundto be independent risk factors affecting mortality.Conclusion: Advanced age and APACHE II score ‡20were found to be independent risk factors affectingrelaparotomy-related mortality.
Key WordsRelaparotomy Æ Mortality Æ Risk factors
Eur J Trauma Emerg Surg 2009;35:547–52
DOI 10.1007/s00068-009-8221-2
IntroductionRelaparotomy (RL) may be required for complicationsthat develop after abdominal surgery. The term ‘‘rel-
aparotomy’’ signifies a new abdominal operation oroperations performed within 60 days after an initialabdominal surgical operation [1, 2]. The requirementfor relaparotomy varies depending on the disease forwhich the patient was operated on, the surgery per-formed and the emergent complications. The highmortality rate of RL has been reported in many re-views [2–7]. Despite the high mortality rates observedafter relaparotomy performed due to postabdominalcomplications of surgery, we did not detect any studyof this issue in a literature search that investigatedmortality factors. The current review was designed toinvestigate the independent risk factors in RL opera-tions performed due to complications following post-abdominal surgery and to elucidate how the causes ofRL are associated with mortality.
Materials and MethodsAmong 6,125 patients undergoing abdominal surgeryat the Dicle University Medical Faculty HospitalGeneral Surgery Clinic between January 2002 and July2007, the files of 114 patients who had relaparotomywere evaluated. Operations performed within 60 daysof the first operation in relation to the first operationwere considered relaparotomies. Patients undergoinginjury control surgery, planned relaparotomies, mini-mally invasive interventions such as percutaneousdrainage and evisceration/eventration operations ofthe abdominal wall were excluded from the study.Complications in patients with clinical deterioration orlack of clinical improvement with a likely intra-abdominal cause were defined by specific laboratoryand radiological tests, observing for the presence ofblood, pus, bile or intestinal contents in the drainsplaced in the abdominal cavity at the first operation.Criteria for urgent relaparotomy included medicaltreatment-resistant hemorrhage, presence of progres-sive peritonitis, presence of abscesses where percuta-neous drainage was not feasible or effective, continued
Eur J Trauma Emerg Surg 2009 Æ No. 6 � URBAN & VOGEL 547
1 Department of General Surgery, Dicle University, Diyarbakir,Turkey.
Received: November 12, 2008; revision accepted: March 3, 2009;Published Online: May 12, 2009
European Journal of Trauma and Emergency Surgery Original Article

contamination of the abdominal cavity with fecalcontent, presence of necrosis, presence of ileus resis-tant to medical treatment or decompression, anddeterioration in patient’s medical status despite medi-cal treatment [2].
The epidemiological and clinical features wereevaluated as probable risk factors for mortality in the RL.Findings for risk factors included: patient characteristics(age and gender), cause of the first operation, conditionof the first operation (urgent/elective), systemic diseases,presence of peritonitis, the period between the firstoperation and relaparotomy (relaparotomy interval),cause of RL, APACHE II score, transfused blood units,number of RLs, length of hospital stay, and mortality.
All patients received standard life-supportingresuscitation protocols. The Acute Physiology andChronic Health Evaluation (APACHE) II score [8] wascalculated on the day of relaparotomy. All patients re-ceived prophylactic antibiotics before the operation andfor 24 h postoperatively. Patients with peritonitis re-ceived intravenous combined antibiotic coverage, whichincluded third-generation cephalosporin, and metroni-dazole was added to the treatment in patients with co-lon-associated complications for enteric pathogens. Inpatients with septic complications, antibiotherapy wascontinued based on the culture antibiogram result.Sequential compression devices were placed in all pa-tients for deep venous thrombosis prophylaxis, and theywere started on low molecular weight heparin as soon asactive bleeding had ceased. Mortality was defined asdeath during hospitalization. Systemic diseases werepresent as comorbidity in 34 patients, and these wereconsidered cardiac (e.g., ischemic heart disease), respi-ratory (e.g., chronic obstructive lung disease), renal(e.g., chronic renal failure), hepatic (e.g., chronic liverdisease), or diabetes.
All data were entered into a statistical model foranalyzing mortality factors for relaparotomy, and thiswas performed using SPSS (SPSS 10.0 for Windows,SPSS Inc.). For all univariate analyses, a chi-squaretest was used for binary variables. To assess predictorsof morbidity, multivariable analysis using logisticregression was performed. Candidate variables thatwere of biological importance or those with a p < 0.2were entered using an entry approach. Predictorvariables were retained in the final model if p < 0.05.
ResultsThis study includes 114 (1.8%) patients undergoingrelaparotomy among 6,125 patients who underwentabdominal surgery at our clinic. The first operation
occurred under urgent conditions in 88 (77.2%) andelective conditions in 26 (22.8%) patients. Mortalitydeveloped in 55 (48.2%) patients undergoing relapar-otomy. The relaparotomy mortality rates were 45.4%(40/88) and 57.7% (15/26) in patients undergoing thefirst operation under urgent conditions and electiveconditions, respectively. There were 75 (65.8%) malepatients and 39 (34.2%) female patients involved, andthe average age was 46.06 ± 19.98 (15–84) years. Thecauses of first laparotomy are presented in Table 1.RLs were performed most commonly following lowergastrointestinal system surgeries (50%).
In the preoperative period, 34 (29.8%) patients had48 systemic diseases and 17 (28%) patients had dia-betes mellitus, which was the most common systemicdisease. The mortality rate was 70.6% (24/34) in pa-tients with systemic disease. The mean APACHE IIscore was calculated to be 19.23 ± 8.06 (2–44) in 114patients undergoing relaparotomy. The mean periodbetween the first operation and relaparotomy was7.87 ± 7.70 (0–60) days. Seventy-nine (69.3%) of the144 patients had a peritonitis; the mortality rate amongthese was 53.2% (42/79). Ninety-four of 114 patientsundergoing relaparotomy received 6.2 ± 6.47 (0–31) Ublood transfusions on average. Multiple relaparoto-mies were performed in 15 patients (13.2%) undergo-ing relaparotomy to control the complications.Thirteen patients received relaparotomy twice, twopatients received relaparotomy thrice, and the meanrelaparotomy number was found to be 1.15. The mor-tality rates were 44.4% (44/99) and 73.3% (11/15) inpatients receiving single and multiple relaparotomies,respectively. The mean duration of hospitalization was24.32 ± 18.69 (1–91) days.
Table 1. The causes of relaparotomy according to organ system.
Cause of the first laparotomy n (%)
Lower gastrointestinal system 57 (50.0)Colon and rectum 24 (21.0)Small intestine 18 (15.8)Appendix 15 (13.2)
Upper gastrointestinal system 10 (8.8)Stomach 9 (7.9)Duodenum 1 (0.9)
Hepato-pancreatico-biliary system 16 (14.0)Gall bladder 11 (9.6)Pancreas 5 (4.4)
Multiple organ system 19 (16.7)Vascular system 4 (3.5)Gynecologic system 3 (2.6)Other 5 (4.4)
Gedik E, et al. Relaparotomies: Why is Mortality Higher?
548 Eur J Trauma Emerg Surg 2009 Æ No. 6
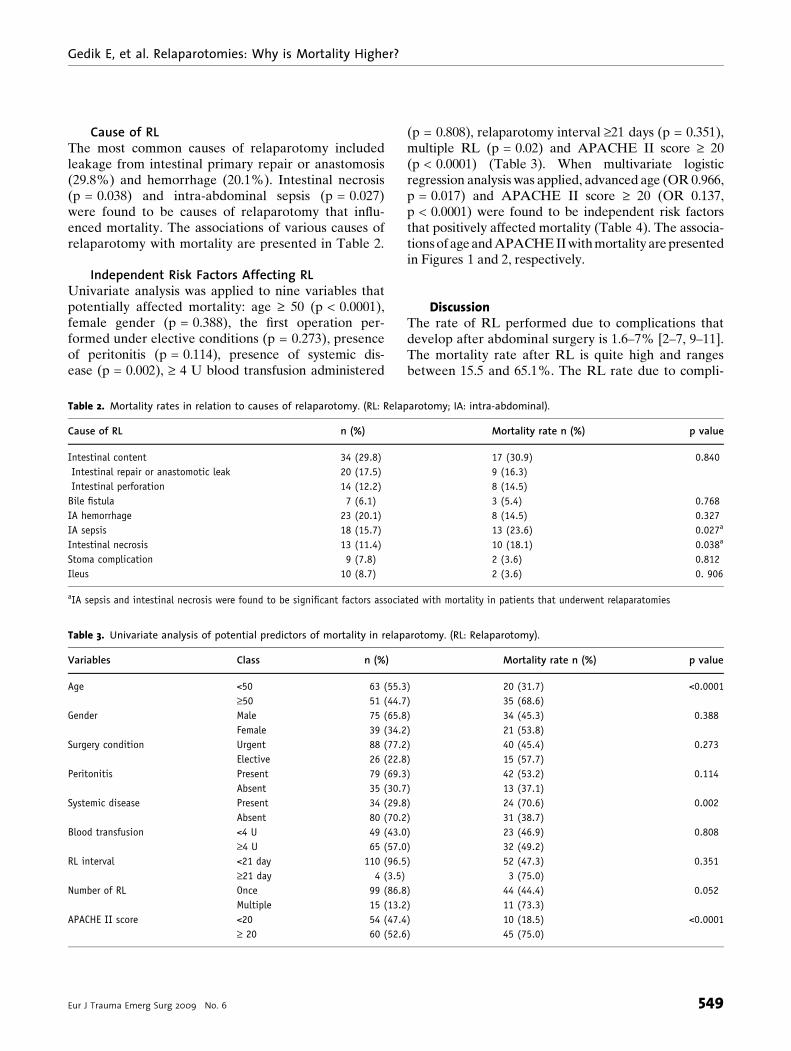
Cause of RLThe most common causes of relaparotomy includedleakage from intestinal primary repair or anastomosis(29.8%) and hemorrhage (20.1%). Intestinal necrosis(p = 0.038) and intra-abdominal sepsis (p = 0.027)were found to be causes of relaparotomy that influ-enced mortality. The associations of various causes ofrelaparotomy with mortality are presented in Table 2.
Independent Risk Factors Affecting RLUnivariate analysis was applied to nine variables thatpotentially affected mortality: age ‡ 50 (p < 0.0001),female gender (p = 0.388), the first operation per-formed under elective conditions (p = 0.273), presenceof peritonitis (p = 0.114), presence of systemic dis-ease (p = 0.002), ‡ 4 U blood transfusion administered
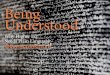
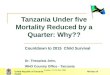
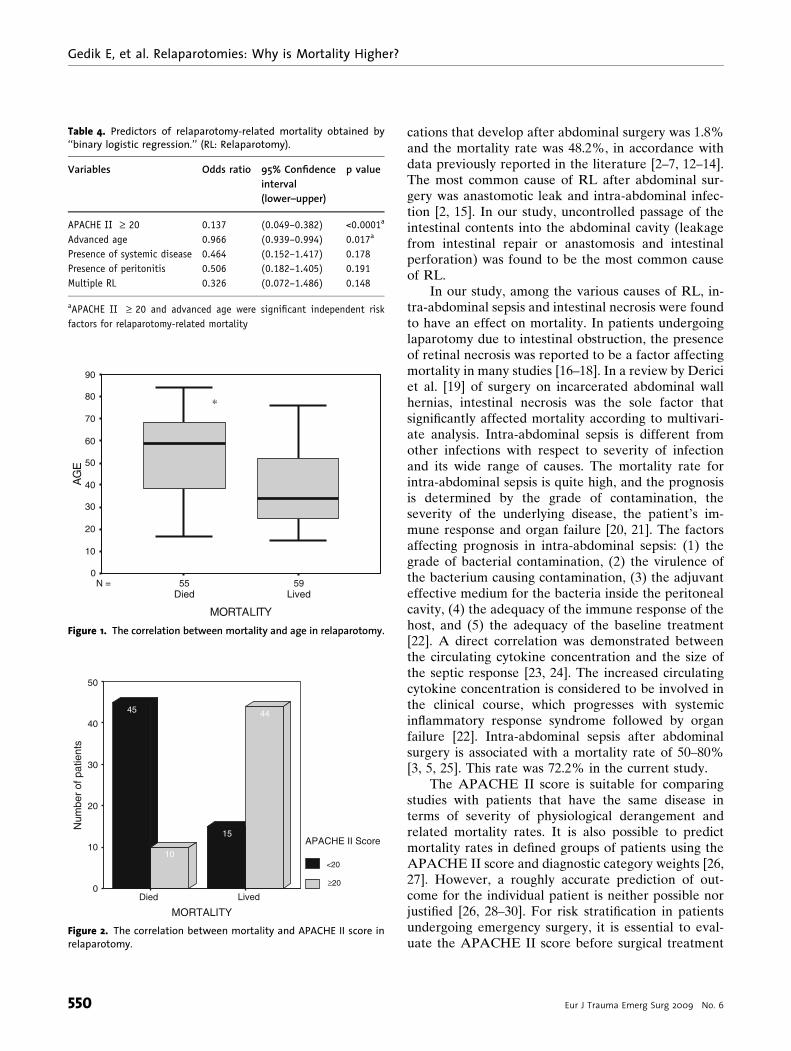
(p = 0.808), relaparotomy interval ‡21 days (p = 0.351),multiple RL (p = 0.02) and APACHE II score ‡ 20(p < 0.0001) (Table 3). When multivariate logisticregression analysis was applied, advanced age (OR 0.966,p = 0.017) and APACHE II score ‡ 20 (OR 0.137,p < 0.0001) were found to be independent risk factorsthat positively affected mortality (Table 4). The associa-tions of age and APACHE II with mortality are presentedin Figures 1 and 2, respectively.
DiscussionThe rate of RL performed due to complications thatdevelop after abdominal surgery is 1.6–7% [2–7, 9–11].The mortality rate after RL is quite high and rangesbetween 15.5 and 65.1%. The RL rate due to compli-
Table 2. Mortality rates in relation to causes of relaparotomy. (RL: Relaparotomy; IA: intra-abdominal).
Cause of RL n (%) Mortality rate n (%) p value
Intestinal content 34 (29.8) 17 (30.9) 0.840Intestinal repair or anastomotic leak 20 (17.5) 9 (16.3)Intestinal perforation 14 (12.2) 8 (14.5)
Bile fistula 7 (6.1) 3 (5.4) 0.768IA hemorrhage 23 (20.1) 8 (14.5) 0.327IA sepsis 18 (15.7) 13 (23.6) 0.027a
Intestinal necrosis 13 (11.4) 10 (18.1) 0.038a
Stoma complication 9 (7.8) 2 (3.6) 0.812Ileus 10 (8.7) 2 (3.6) 0. 906
aIA sepsis and intestinal necrosis were found to be significant factors associated with mortality in patients that underwent relaparatomies
Table 3. Univariate analysis of potential predictors of mortality in relaparotomy. (RL: Relaparotomy).
Variables Class n (%) Mortality rate n (%) p value
Age <50 63 (55.3) 20 (31.7) <0.0001‡50 51 (44.7) 35 (68.6)
Gender Male 75 (65.8) 34 (45.3) 0.388Female 39 (34.2) 21 (53.8)
Surgery condition Urgent 88 (77.2) 40 (45.4) 0.273Elective 26 (22.8) 15 (57.7)
Peritonitis Present 79 (69.3) 42 (53.2) 0.114Absent 35 (30.7) 13 (37.1)
Systemic disease Present 34 (29.8) 24 (70.6) 0.002Absent 80 (70.2) 31 (38.7)
Blood transfusion <4 U 49 (43.0) 23 (46.9) 0.808‡4 U 65 (57.0) 32 (49.2)
RL interval <21 day 110 (96.5) 52 (47.3) 0.351‡21 day 4 (3.5) 3 (75.0)
Number of RL Once 99 (86.8) 44 (44.4) 0.052Multiple 15 (13.2) 11 (73.3)
APACHE II score <20 54 (47.4) 10 (18.5) <0.0001‡ 20 60 (52.6) 45 (75.0)
Gedik E, et al. Relaparotomies: Why is Mortality Higher?
Eur J Trauma Emerg Surg 2009 Æ No. 6 549
cations that develop after abdominal surgery was 1.8%and the mortality rate was 48.2%, in accordance withdata previously reported in the literature [2–7, 12–14].The most common cause of RL after abdominal sur-gery was anastomotic leak and intra-abdominal infec-tion [2, 15]. In our study, uncontrolled passage of theintestinal contents into the abdominal cavity (leakagefrom intestinal repair or anastomosis and intestinalperforation) was found to be the most common causeof RL.
In our study, among the various causes of RL, in-tra-abdominal sepsis and intestinal necrosis were foundto have an effect on mortality. In patients undergoinglaparotomy due to intestinal obstruction, the presenceof retinal necrosis was reported to be a factor affectingmortality in many studies [16–18]. In a review by Dericiet al. [19] of surgery on incarcerated abdominal wallhernias, intestinal necrosis was the sole factor thatsignificantly affected mortality according to multivari-ate analysis. Intra-abdominal sepsis is different fromother infections with respect to severity of infectionand its wide range of causes. The mortality rate forintra-abdominal sepsis is quite high, and the prognosisis determined by the grade of contamination, theseverity of the underlying disease, the patient’s im-mune response and organ failure [20, 21]. The factorsaffecting prognosis in intra-abdominal sepsis: (1) thegrade of bacterial contamination, (2) the virulence ofthe bacterium causing contamination, (3) the adjuvanteffective medium for the bacteria inside the peritonealcavity, (4) the adequacy of the immune response of thehost, and (5) the adequacy of the baseline treatment[22]. A direct correlation was demonstrated betweenthe circulating cytokine concentration and the size ofthe septic response [23, 24]. The increased circulatingcytokine concentration is considered to be involved inthe clinical course, which progresses with systemicinflammatory response syndrome followed by organfailure [22]. Intra-abdominal sepsis after abdominalsurgery is associated with a mortality rate of 50–80%[3, 5, 25]. This rate was 72.2% in the current study.
The APACHE II score is suitable for comparingstudies with patients that have the same disease interms of severity of physiological derangement andrelated mortality rates. It is also possible to predictmortality rates in defined groups of patients using theAPACHE II score and diagnostic category weights [26,27]. However, a roughly accurate prediction of out-come for the individual patient is neither possible norjustified [26, 28–30]. For risk stratification in patientsundergoing emergency surgery, it is essential to eval-uate the APACHE II score before surgical treatment
Table 4. Predictors of relaparotomy-related mortality obtained by‘‘binary logistic regression.’’ (RL: Relaparotomy).
Variables Odds ratio 95% Confidenceinterval(lower–upper)
p value
APACHE II ‡ 20 0.137 (0.049–0.382) <0.0001a
Advanced age 0.966 (0.939–0.994) 0.017a
Presence of systemic disease 0.464 (0.152–1.417) 0.178Presence of peritonitis 0.506 (0.182–1.405) 0.191Multiple RL 0.326 (0.072–1.486) 0.148
aAPACHE II ‡ 20 and advanced age were significant independent riskfactors for relaparotomy-related mortality
5955N =
MORTALITY
AG
E
90
80
70
60
50
40
30
20
10
0
*
LivedDied
Figure 1. The correlation between mortality and age in relaparotomy.
MORTALITY
Num
ber
of p
atie
nts
50
40
30
20
10
0
APACHE II Score
<20
44
10
15
45
≥20
Died Lived
Figure 2. The correlation between mortality and APACHE II score inrelaparotomy.
Gedik E, et al. Relaparotomies: Why is Mortality Higher?
550 Eur J Trauma Emerg Surg 2009 Æ No. 6
[26]. A noticeable statistically significant relationshipwas reported between need for RL and APACHE IIscore > 20, level of serum albumin < 3 mg/dl in thepatients, age > 70 years old, and intra-abdominal sepsis[6]. Giangiuliani et al. [31] reported in their study,which included 512 patients, mainly those who had se-vere peritonitis, intra-abdominal sepsis, acute pancre-atitis, and bleeding esophageal varices, that there wasstatistical meaningful relationship between APACHEII score and obtained mortality ratio. We found that anAPACHE II score (which assesses the chronic health ofpatients, which is related to acute severity of disease,and patient age) of greater than 20 was an independentrisk factor that affected mortality in RL.
As a population ages, increasing numbers of el-derly people will present for surgery [32]. The in-creased percentage of operations in elderly patients isdue not only to the increasing number of older patientsbut also a reluctance to offer surgical treatment to theelderly [33]. Many studies have shown that the resultsof elective surgery in elderly patients seem largelyfavorable, while those of emergency surgery are not[34]. Emergency surgery carries a higher operative riskfor morbidity and mortality, threefold higher than therisk associated with elective surgery [35, 36]. Bunt et al.[5] reported that age was a significant factor in mor-tality in patients that underwent urgent relaparotomy,and stated that the mortality rate was 16% below50 years of age and 50% above 50 years of age. Elderlypatients are more vulnerable to mortality in emergencysurgery because of the overall decline in physiologicalreserves [33]. MOF was reported to develop mostcommonly in elderly patients [3]. In the current study,mortality was 68.6% in patients ‡ 50, and the multi-variant analysis revealed that advanced age was anindependent risk factor for mortality. The adverse ef-fect of the operation-complication–reoperation serieson the organ systems of the elderly due to complica-tions after recent abdominal surgery may explain thehigh rate of mortality in this patient population.
As indicated in the current study and previous re-views, the mortality rate is quite high (for both electiveand emergency surgery) relative to that for the initialoperation. Due to the high mortality rate, necessarycare should be taken to avoid complications that mayrequire RL. Determining the patient’s preoperativerisk factors, describing the disease in the most accurateway possible, and evaluating the surgical area andtechnique in association with the disease and diseasefactors would help to decrease the risk of complica-tions. Thus, we believe that the requirement for RLand thus mortality rates would be decreased.
In conclusion, we determined in our retrospectivestudy that advanced age and an APACHE II score of‡ 20 are independent risk factors affecting mortality. Webelieve that further prospective, multicenter, compre-hensive studies involving a large number of patients areneeded.
Conflict of interest statementThe authors declare that there is no actual or potential conflict of
interest in relation to this article.
References1. Parker MC, Ellis M, Moran BJ, Thompson JN, Wilson MS, Menzies
D. Postoperative adhesions: ten-year follow-up of 12584 patientundergoing lower abdominal surgery. Dis Colon Rectum 2001;44:822–30.
2. Unalp HR, Kamer E, Kar H, Bal A, Peskersoy M, Onal MA. Urgentabdominal re-explorations. World J Emerg Surg 2006;1:10.
3. Hutchins RR, Gunning P, Lucas DN, Allen-Mersh TG, Soni NC.Relaparotomy for suspected intraperitoneal sepsis afterabdominal surgery. World J Surg 2004;28:137–41.
4. Schein M. Planned reoperations and open management incritical intra-abdominal infections: prospective experience in 52cases. World J Surg 1991;15:537–45.
5. Bunt TJ. Urgent relaparotomy: the high-risk, no-choice opera-tion. Surgery 1985;98:555–60.
6. Kirk RM. Reoperative surgery for early complication for abdominaland abdominothoracic operations. J R Soc Med 1988; 81: 7–9.
7. Zer M, Dux S, Dintsman M. The timing of relaparotomy and itsinfluence on prognosis. A 10 year survey. Am J Surg 1980;139:338–43.
8. Knaus WA, Draper EA, Wagner DP, Zimmerman JE: APACHE II aseverity of disease classification system. Crit Care Med 1985; 13:818–29.
9. Wain MO, Sykes PA. Emergency abdominal re-exploration in adistrict general hospital. Ann R Coll Surg Engl 1987; 69: 169–74.
10. Hinsdale JG, Jaffe BM. Reoperations for intraabdominal sepsis.Ann Surg 1984;199:31–6.
11. Thompson JS, Baxter BT, Allison JG, Johnson FE, Lee KK, ParkWY. Temporal patterns of postoperative complications. ArchSurg 2003;138:596–603.
12. Kriger AG, Shurkalin BK, Glushkov PS, Andreitsev IL. Diagnosisand treatment of postoperative intraabdominal complications.Khirurgiia 2003;8:19–23.
13. Zavernyi LG, Poida AI, Melik VM, Bondarenko ND, Tarasov AA,Nadeev SS, Stepanik IVa. Prognosis in the outcome of relapar-otomy. Klin Khir 1992;8:12–6.
14. Rygachev GP, Nekhaev AN, Kerez PI, Kremen VE: Relaparotomyin the treatment of generalized postoperative peritonitis.Khirurgiia 1997;1:45–8.
15. Harbrecht PJ, Garrison RNl, Fry DE. Early urgent relaparotomy.Arch Surg 1984;119:369–74.
16. Mucha PJR. Small intestinal obstruction. Surg Clin North Am1987;67:597–620.
17. Fevang BT, Fevang JM, Stangeland L, Soreide O, Svanes K, VisteA. Complications and death after surgical treatment of smallbowel obstruction: a 35-year institutional experience. Ann Surg2000;231:529–37.
Gedik E, et al. Relaparotomies: Why is Mortality Higher?
Eur J Trauma Emerg Surg 2009 Æ No. 6 551
18. Uludag M, Akgün _I, Yetkin G, Kebudi A, _Isgör A, Sener A. Factorsaffecting morbidit and mortality in mechanical intestinalobstruction. Ulus Travma Acil Cerrahi Derg 2004;10:177–84.
19. Derici H, Unalp HR, Bozdag AD, Nazli O, Tansug T, Kamer E.Factors affecting morbidity and mortality in incarceratedabdominal wall hernias. Hernia 2007;11:341–6.
20. Berger D, Buttenschoen K. Management of abdominal sepsis.Langenbecks Arch Surg 1998;383:35–43.
21. Mulier S, Penninckx F, Verwaest C, Filez L, Aerts R, Fieuws S,Lauwers P. Factors affecting mortality in generalized postop-erative peritonitis: multivariate analysis in 96 patients. World JSurg 2003;27:379–84.
22. Malangoni M. Contributions to the management of intraab-dominal infections. Am J Surg 2005; 190: 255–9.
23. Ordonez CA, Puyana JC. Management of peritonitis in thecritically ill patient. Surg Clin N Am 2006; 86: 1323–49.
24. Baue AE. Multiple organ dysfunction syndrome. Arch Surg1997;132:703–7.
25. McCrory C, Crowley K. Is repeat laparotomy of value in patientswith suspected intraabdominal sepsis in the intensive careunit? Ir J Med Sci 1997;166:88–91.
26. Koperna T, Semmler D, Marian F. Risk stratification in emer-gency surgical patients. Arch Surg 2001;136:55–9.
27. Barie PS, Hydo LJ, Fiscer E. Development of multiple organdysfunction syndrome in critically ill patients with perforatedviscus: predictive value of APACHE severity scoring. Arch Surg1996;131:37–43.
28. Ohmann C, Hau T. Prognostic indices in peritonitis. Hepato-gastroenterology 1997;44:937–46.
29. Giebel GD, Troidl H. Möglichkeiten und grenzen von scores:theoretische überlegungen über scores. Langenbecks Arch Surg1996;381:59–62.
30. Berger MM, Marazzi A, Freeman J, Chiolero R. Evaluation of theconsistency of acute physiology and chronic healthy evaluation(APACHE II) scoring in the surgical intensive care unit. Crit CareMed 1992;20:1681–7.
31. Giangiuliani G, Mancini A, Gui D. Validation of a severity ofillness score (APACHE II) in a surgical intensive care unit.Intensive Care Med 1989;15:519–22.
32. Oskvig RM. Special problems in elderly. Chest 1999; 115: 158–64.33. Rosenthal RA, Zenilman ME. Surgery in elderly. In: Towsend CM,
Beauchamp RD, Evers MB, Mattox KL, eds. The biological basisof modern surgical practice, 16th ed. Philadelphia: WB Saun-ders, 2001:226–46.
34. Mclnytre R, Reinbach D, Cushuieri RJ. Emergency abdominalsurgery in the elderly. JR Coll Surg Edinb 1997; 42: 1738.
35. Karanikas ID, Liakakos TD, Koundourakis SS, Tzorakis SE,Dendrinos SS. Emergency operations in elderly: management ofoutcome. Int Surg 1996;81:158–62.
36. Rosenthal RA, Andersen DK. Physiologic considerations in theelderly surgical patient. In: Miller TA, ed. Modern surgical care,2nd ed. St Louis: Quality Medical Publishing Inc.; 1998;1362–84.
Address for CorrespondenceErcan GedikDepartment of General SurgeryDicle University21280, DiyarbakirTurkeyPhone (+90) 5322536030e-mail: [email protected]
Gedik E, et al. Relaparotomies: Why is Mortality Higher?
552 Eur J Trauma Emerg Surg 2009 Æ No. 6