Embed Size (px)
Citation preview

Original Article
Reinforcing cerclage in the prevention of preterm birth in women athigh risk: a retrospective case–controlled study
Rachael SIMCOX and Andrew SHENNAN
Maternal and Fetal Research Unit, Division of Reproduction and Endocrinology, King’s College London, St. Thomas’ Hospital, London,UK
Background: Transvaginal ultrasound measurement of cervical length is useful after suture insertion in predictingpreterm delivery. However, there is little evidence to guide practice in the clinical scenario when fetal membranes are seenon ultrasound to be prolapsing distal to a cervical suture.Aim: To determine whether a reinforcing cerclage reduced preterm delivery in those women with ultrasound evidence offetal membranes prolapsing distal to the first suture.Methods: A retrospective cohort study was conducted on women with a cervical suture in situ plus ultrasound evidenceof fetal membranes prolapsing through the first suture. Exposed patients were those managed with a reinforcing cerclage.The unexposed group were women who were managed expectantly, without a reinforcing cerclage.Results: Those women with a reinforcing cerclage were significantly more likely to deliver at an earlier gestationcompared with those managed expectantly: 26+0 (±5+1) compared with 31+1 (±7+0) weeks, P = 0.047. More women inthe reinforcing cerclage group delivered at <32 completed weeks’ gestation: 12/13 (92%) versus 5/12 (42%), P = 0.01.There was no significant difference in the rate of second-trimester miscarriages between the expectant management groupand those with a reinforcing cerclage: 2/12 (17%) versus 5/13 (38%), P = 0.38.Conclusion: Our study found that a reinforcing cerclage following primary cerclage failure hastened preterm delivery.The role of transvaginal ultrasound measurement of cervical length postsuture is debatable if the possible intervention isnot beneficial and may be detrimental.
Key words: cervical cerclage, cervical length, preterm birth, reinforcing cerclage, transvaginal ultrasound.
Introduction
Cervical cerclage is a common prophylactic interventionthat has been used in the management of second-trimesterloss and preterm birth (PTB) for several decades, yet itremains one of the more controversial surgicalinterventions in obstetrics. Most sutures are insertedelectively based on a past obstetric history suggestive ofcervical insufficiency. To avoid potentially unnecessaryelective cerclage, transvaginal ultrasound assessment ofcervical length is frequently used to identify women witha short cervix to target for intervention (despite evidenceregarding the benefit of ultrasound-indicated cerclage
being inconsistent).1–3 Ultrasound measurement ofcervical length can also be useful after suture insertion inpredicting preterm delivery. An increase in cervical lengthis often seen postcerclage4 with the best predictor ofoutcome being length of closed cervix above the suture.5
Funnelling of the membranes to the level of the suture issignificantly associated with earlier preterm delivery,6,7
whereas lengths of 10 mm or greater above the suture areassociated with the best prognosis.5
Although a long closed cervix postcerclage isreassuring, with more clinicians choosing to measurecervical length posthistory-indicated and ultrasound-indicated cerclage, the clinical scenario is more likely toarise whereby a cervix already with a suture in place isseen to shorten further, with fetal membranes prolapsingdistal to the level of the suture. In such circumstances,some suggest a repeat of the cerclage procedure or a‘reinforcing’ cerclage; the hypothesis being that earlyevidence of suture failure can be identified with serialtransvaginal ultrasound and that repeat cerclage delaysdelivery.8 However, the benefits of such a repeat cerclage
Correspondence: Dr Rachael Simcox, Maternal and FetalResearch Unit, Division of Reproduction and Endocrinology,King’s College London, 10th Floor, North Wing,St. Thomas’ Hospital, London SE1 7EH, UK.Email: [email protected]
Received 18 July 2011; accepted 13 March 2012.
224 © 2012 The Authors
ANZJOG © 2012 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists
Australian and New Zealand Journal of Obstetrics and Gynaecology 2012; 52: 224–228 DOI: 10.1111/j.1479-828X.2012.01440.x
Th e Australian and New Zealand Journal of Obstetrics and Gynaecology

procedure are not known, and it is possible that aprecarious situation with a short cervix could be worsenedby another surgical procedure involving further manipulationof the cervix.There is little information in the literature pertaining to
repeat cerclage for those identified as being at risk byshort cervical length measured on ultrasound. Oneretrospective study found reinforcing cerclage to delaydelivery,8 whereas another found the opposite to be true.9
As part of larger trials of cerclage, some recruits haverequired reinforcing second sutures, again with differingconclusions reached.2,10
The aim of this study was to determine whether areinforcing cerclage following membrane prolapse througha first suture reduced preterm delivery in those women athigh risk.
Materials and Methods
A retrospective cohort study was conducted on womenwith a cervical suture plus fetal membranes prolapsingdistal to the suture. Over 1500 pregnancies recorded inthe Preterm Prevention Clinics’ database of St. Thomas’Hospital and Queen Charlotte’s Hospital, London,between 2002 and 2006 were hand searched by RS. Allwomen who had ultrasonographical evidence ofmembranes prolapsing beyond the level of the cervicalsuture were included in the study. Exposed patients werethose with membranes prolapsing beyond the level of thecerclage who were managed with a reinforcing cerclage.The unexposed group were women who were managedexpectantly, without a reinforcing cerclage. As this clinicalscenario was rare, the management of each individual wasat the discretion of the lead clinician.All women were deemed high risk of preterm delivery
having had one or more of the following: past obstetrichistory of preterm birth or mid-trimester loss, previouscervical suture, significant cervical surgery or a uterineanomaly. Inclusion criteria were any woman with asingleton pregnancy who had ultrasonographical evidenceof membranes prolapsing beyond a cervical suture(irrespective of whether this initial suture was elective,ultrasound-indicated or transabdominal). Exclusion criteriaincluded those women with a multifetal pregnancy, thosewith incomplete records or those who did not fit thecriteria. Transvaginal ultrasound cervical assessment wasperformed on all women from presentation until26 weeks’ gestation on a fortnightly basis. All ultrasoundscans were performed by a research fellow trained inultrasound or by the lead consultant using a 7.5-MHztransvaginal probe. Reinforcing sutures followed thetechnique described by McDonald. Additional treatments,including antibiotics for abnormal vaginal flora,progesterone pessaries and bed rest, were arranged on anindividual basis, and these factors were not independentlyanalysed.Primary outcome was gestation at delivery, with
secondary outcomes being preterm birth at <32 weeks’
completed gestation, second-trimester miscarriage definedas previable birth at <24 weeks and neonatal outcome.Statistical analysis was performed using STATA 8 (version
9.1, StataCorp, College Station, TX, USA), Mann–Whitney U test, Student’s t-test and Fisher’s exact testwhere appropriate. Two-tailed probability values of <0.05were considered as statistically significant.
Results
During the 4-year period from 2002 to 2006, therewere 25 women identified as having ultrasonographicalevidence of membranes prolapsing through the firstsuture. Of these 25 women, 13 had a secondreinforcing suture inserted and 12 were managedexpectantly.
Demographic characteristics and past obstetrichistory
In the study cohort as a whole, 20 of 25 (80%) womenhad had at least one previous mid-trimester loss, and 8 of25 (32%) had had two or more. Regarding previouspreterm delivery at <32 weeks’ gestation, 11 of 25 (44%)women had had at least one previous preterm birth.There was no significant difference between thereinforcing cerclage group and the control group withrespect to past obstetric history. Similarly, there was nosignificant difference between the numbers of women whohad had either a successful or a failed cervical suture in aprevious pregnancy. Subject demographics were notsignificantly different between the two groups.The cervical length (CL) at which membranes were
seen to be prolapsing through the suture was the same forboth groups (7.2 mm). The mean gestational age atwhich this was diagnosed was 8 days earlier in the repeatcerclage group, but this was not significantly different.These details are summarised in Table 1.
Primary outcome
Those women with a reinforcing cerclage weresignificantly more likely to deliver at an earlier gestationcompared with those women who were managedexpectantly. The mean gestational age at delivery for the13 women treated with a double cerclage was 26+0
(+/- 5+1) weeks compared with 31+1 (±7+0) weeks forwomen treated expectantly, P = 0.047.
Secondary outcomes
Statistically, more women in the reinforcing cerclagegroup delivered at <32 completed weeks’ gestation whencompared with the control group: 12/13 (92%) versus5/12 (42%), P = 0.01. There were fewer second-trimestermiscarriages in the expectant management group, but thisdid not reach statistical significance: 2/12 (17%) versus5/13 (38%), P = 0.38.
© 2012 The Authors 225
ANZJOG © 2012 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists
Reinforcing cerclage in the prevention of PTB
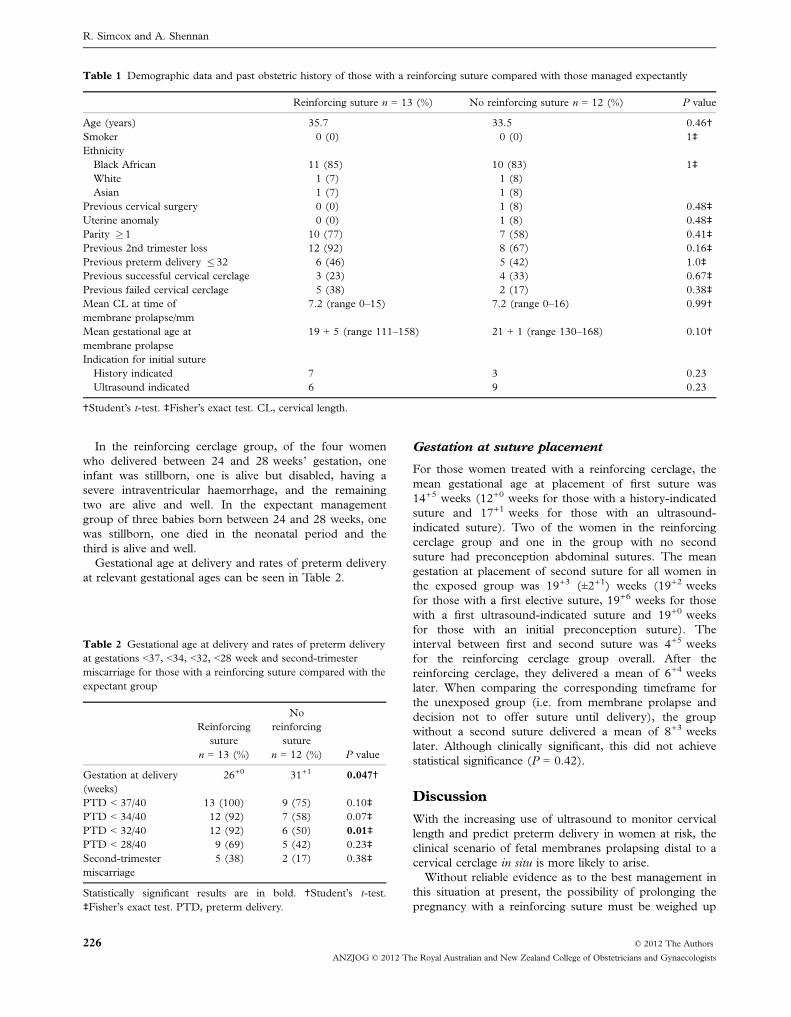
In the reinforcing cerclage group, of the four womenwho delivered between 24 and 28 weeks’ gestation, oneinfant was stillborn, one is alive but disabled, having asevere intraventricular haemorrhage, and the remainingtwo are alive and well. In the expectant managementgroup of three babies born between 24 and 28 weeks, onewas stillborn, one died in the neonatal period and thethird is alive and well.Gestational age at delivery and rates of preterm delivery
at relevant gestational ages can be seen in Table 2.
Gestation at suture placement
For those women treated with a reinforcing cerclage, themean gestational age at placement of first suture was14+5 weeks (12+0 weeks for those with a history-indicatedsuture and 17+1 weeks for those with an ultrasound-indicated suture). Two of the women in the reinforcingcerclage group and one in the group with no secondsuture had preconception abdominal sutures. The meangestation at placement of second suture for all women inthe exposed group was 19+3 (±2+1) weeks (19+2 weeksfor those with a first elective suture, 19+6 weeks for thosewith a first ultrasound-indicated suture and 19+0 weeksfor those with an initial preconception suture). Theinterval between first and second suture was 4+5 weeksfor the reinforcing cerclage group overall. After thereinforcing cerclage, they delivered a mean of 6+4 weekslater. When comparing the corresponding timeframe forthe unexposed group (i.e. from membrane prolapse anddecision not to offer suture until delivery), the groupwithout a second suture delivered a mean of 8+3 weekslater. Although clinically significant, this did not achievestatistical significance (P = 0.42).
Discussion
With the increasing use of ultrasound to monitor cervicallength and predict preterm delivery in women at risk, theclinical scenario of fetal membranes prolapsing distal to acervical cerclage in situ is more likely to arise.Without reliable evidence as to the best management in
this situation at present, the possibility of prolonging thepregnancy with a reinforcing suture must be weighed up
Table 1 Demographic data and past obstetric history of those with a reinforcing suture compared with those managed expectantly
Reinforcing suture n = 13 (%) No reinforcing suture n = 12 (%) P value
Age (years) 35.7 33.5 0.46†Smoker 0 (0) 0 (0) 1‡EthnicityBlack African 11 (85) 10 (83) 1‡White 1 (7) 1 (8)Asian 1 (7) 1 (8)
Previous cervical surgery 0 (0) 1 (8) 0.48‡Uterine anomaly 0 (0) 1 (8) 0.48‡Parity �1 10 (77) 7 (58) 0.41‡Previous 2nd trimester loss 12 (92) 8 (67) 0.16‡Previous preterm delivery �32 6 (46) 5 (42) 1.0‡Previous successful cervical cerclage 3 (23) 4 (33) 0.67‡Previous failed cervical cerclage 5 (38) 2 (17) 0.38‡Mean CL at time ofmembrane prolapse/mm
7.2 (range 0–15) 7.2 (range 0–16) 0.99†
Mean gestational age atmembrane prolapse
19 + 5 (range 111–158) 21 + 1 (range 130–168) 0.10†
Indication for initial sutureHistory indicated 7 3 0.23Ultrasound indicated 6 9 0.23
†Student’s t-test. ‡Fisher’s exact test. CL, cervical length.
Table 2 Gestational age at delivery and rates of preterm deliveryat gestations <37, <34, <32, <28 week and second-trimestermiscarriage for those with a reinforcing suture compared with theexpectant group
Reinforcingsuture
n = 13 (%)
Noreinforcing
suturen = 12 (%) P value
Gestation at delivery(weeks)
26+0 31+1 0.047†
PTD < 37/40 13 (100) 9 (75) 0.10‡PTD < 34/40 12 (92) 7 (58) 0.07‡PTD < 32/40 12 (92) 6 (50) 0.01‡
PTD < 28/40 9 (69) 5 (42) 0.23‡Second-trimestermiscarriage
5 (38) 2 (17) 0.38‡
Statistically significant results are in bold. †Student’s t-test.‡Fisher’s exact test. PTD, preterm delivery.
226 © 2012 The Authors
ANZJOG © 2012 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists
R. Simcox and A. Shennan

with the potential risks of membrane rupture, infectionand precipitating a preterm delivery. At our institution, ofthose 25 women with ultrasonographical evidence of fetalmembranes prolapsing distal to the cervical suture, areinforcing suture was associated with a significantlyearlier gestation at delivery compared with those womenwho were managed expectantly.Our findings broadly agree with those found by Baxter
et al.9 who found a reinforcing cerclage to be associatedwith a significantly earlier gestational age at delivery aswell as higher rates of both preterm delivery <35 weeksand previable delivery <24 weeks. The design of ourretrospective analysis differed from that of Baxter et al. inthat their criteria for a reinforcing cerclage was based oncervical length of � 25 mm.Fox et al.8 retrospectively analysed outcomes in 26
women with cervical sutures in situ whom were allscanned. Of these, 12 required repeat cerclage formembrane prolapse through the suture or significantcervical shortening. The authors proposed that theirpolicy of repeat cerclage might delay delivery by sevenadditional weeks as the median interval between firstcervical change and delivery was 13 weeks. However, thecomparison between the single cerclage group andthe repeat cerclage group is not a meaningful one as theformer group did not have the significant cervical changeas the latter group.We acknowledge there are several limitations to our
study. The sample size is small and selection bias cannotbe eliminated because of the retrospective design of thestudy. However, the groups were not significantly differentwith respect to their demographic or past obstetrichistory. Certain measures with the potential to influenceoutcome such as bed rest, antibiotics and progesteronewere not controlled for, but the protocol at the twohospitals contributing to the database were similar, andthe variable of clinician preference was minimal as bothclinics were serviced by one research fellow and the leadconsultant clinician for each clinic did not changethroughout the duration of this analysis.As with any surgical procedure, cervical cerclage is
operator dependent, and if the initial suture appeared onultrasound to be inadequately placed (i.e. not approximateto the bladder neck), a reinforcing cerclage may havebeen favoured. This theory is not obviously supported bythe data presented here, as the cervical length at whichmembranes were seen to be prolapsing through the firstsuture was no different between the exposed and controlgroup. Also, the policy of both hospitals was for a seniorclinician to insert the cerclage, and in cases of areinforcing cerclage, the consultant lead for the clinicperformed the procedure.The interval between first suture and membranes
prolapsing through the stitch was shorter for thosewomen who had had an ultrasound-indicated first suture,which would be expected as ultrasound-indicated suturesare generally placed at a later gestational age than electivesutures.11 There were more women with a history-
indicated first stitch in the group who received a secondcerclage (7 versus 3), and similarly more women with anultrasound-indicated first suture in the expectantmanagement group (9 versus 6). However, this was notstatistically significant, and the ultrasonographical cervicallength at the time of membrane prolapse was the same inboth groups. It is possible there was an unrealisedreluctance to offer a repeat cerclage to those who hadonly recently had a suture (i.e. those with an ultrasound-indicated suture), or it may have been the patient’spreference to have or refuse a repeat procedure.The authors recognise that the type of initial first suturemay be a confounder if outcomes of pregnancies withhistory-indicated sutures are different from those withultrasound-indicated sutures. However, as there is nodefinitive agreed criteria as to whom should receive ahistory-indicated suture, we were pragmatic in ourdecision to include all types of suture in the trial.The gestation at which the membranes were seen
prolapsing through the first stitch was 10 days earlier inthe group who received a second suture. This was notstatistically significant, although in a clinical setting theremay have been more inclination to offer a repeat suture atthe earlier gestation.Ideally to make the strongest comparison between
reinforcing cerclage and expectant management, theclinical situation would have been the same for eachwoman (i.e. all elective first sutures). However, the studywas a pragmatic one, and the question as to whether areinforcing suture is beneficial when membranes are seenprolapsing through the suture still remains, whether theinitial suture was elective, ultrasound indicated orpreconception.It is not apparent why a reinforcing cerclage would be
detrimental in preventing preterm delivery in thesewomen with an apparently failing first suture. It may bethat further manipulation and instrumentation of thecervix worsens an already precarious scenario. Faced withthis dire clinical situation and in a woman with a poorpast obstetric history, the possibility of salvaging thepregnancy with a reinforcing cerclage would appear theonly option. However, in our small study, furtherintervention worsened the outcome. Uterine activity maybe exacerbated by the process of further surgery, and ifclinically silent inflammation and/or infection haveoccurred, then mechanical support with another stitchmay be too late.The role of transvaginal ultrasound measurement of
cervical length postsuture is debatable if the possibleintervention is not beneficial and may be detrimental.Large multicentre trials are needed to further confirmthese findings.
Acknowledgements
We would like to thank Professor Bennett, the leadclinician of the Preterm Prevention Clinic at QueenCharlotte’s Hospital and previous research fellows Dr
© 2012 The Authors 227
ANZJOG © 2012 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists
Reinforcing cerclage in the prevention of PTB

Katie Groom and Dr Bryony Jones, who have beeninvolved in the management of these women.
References
1 Althuisius SM, Dekker GA, Hummel P et al. Final resultsof the cervical incompetence prevention randomizedcerclage trial (CIPRACT): therapeutic cerclage with bed restversus bed rest alone. Am J Obstet Gynecol 2001; 185: 1106–1112.
2 Rust OA, Atlas RO, Reed J et al. Revisiting the short cervixdetected by transvaginal ultrasound in the second trimester:why cerclage therapy may not help. Am J Obstet Gynecol2001; 185: 1098–1105.
3 Drakeley AJ, Roberts D, Alfirevic Z. Cervical stitch (cerclage)for preventing pregnancy loss in women. Cochrane DatabaseSystem Rev 2003; (1): CD003253. DOI: 10.1002/14651858.CD003253.
4 O’Connell MP, Lindow SW. Reversal of asymptomaticcervical length shortening with cervical cerclage: a preliminarystudy. Hum Reprod 2001; 16: 172–173.
5 Groom KM, Shennan AH, Bennett PR. Ultrasound-indicatedcervical cerclage: outcome depends on preoperative cervical
length and presence of visible membranes at time of cerclage.Am J Obstet Gynecol 2002; 187: 445–449.
6 O’Brien JM, Hill AL, Barton JR. Funneling to the stitch: aninformative ultrasonographic finding after cervical cerclage.Ultrasound Obstet Gynecol 2002; 20: 252–255.
7 Guzman ER, Houlihan C, Vintzileos A et al. The significanceof transvaginal ultrasonographic evaluation of the cervix inwomen treated with emergency cerclage. Am J Obstet Gynecol1996; 175: 471–476.
8 Fox R, Holmes R, James M et al. Serial transvaginalultrasonography following McDonald cerclage and repeatsuture insertion. Aust N Z J Obstet Gynaecol 1998; 38: 27–30.
9 Baxter JK, Airoldi J, Berghella V. Short cervical length afterhistory-indicated cerclage: is a reinforcing cerclage beneficial?Am J Obstet Gynecol 2005; 193: 1204–1207.
10 Althuisius SM, Dekker GA, van Geijn HP et al. Cervicalincompetence prevention randomized cerclage trial(CIPRACT): study design and preliminary results. Am JObstet Gynecol 2000; 183: 823–829.
11 Groom KM, Bennett PR, Golara M et al. Elective cervicalcerclage versus serial ultrasound surveillance of cervical lengthin a population at high risk for preterm delivery. Eur J ObstetGynecol Reprod Biol 2004; 112: 158–161.
228 © 2012 The Authors
ANZJOG © 2012 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists
R. Simcox and A. Shennan







![Preconception Laparoscopic Cervical Cerclage: The ... · 1965 [5], trans-abdominal cervical cerclage prior to pregnancy has emerged as a safe and effective intervention for improving](https://img.pdfslide.us/doc/110x75/5f8851cdb723447a244bb50e/preconception-laparoscopic-cervical-cerclage-the-1965-5-trans-abdominal.jpg)











![Cervicalstitch(cerclage)forpreventingpretermbirthin ... › download › pdf › 131165057.pdf · [Intervention Review] Cervical stitch (cerclage) for preventing preterm birth in](https://img.pdfslide.us/doc/110x75/5f03a1417e708231d409ff53/cervicalstitchcerclageforpreventingpretermbirthin-a-download-a-pdf-a.jpg)








