Embed Size (px)
Citation preview

60 M A S S A G E & B O DY WO R K • D E C E M B E R / J A N U A RY 2 0 0 0
The human bodyis an intelligentliving organism
constantly re-creatingitself in response tostimuli. Some of thesestimuli are physicaltrauma and injury, someare emotional, and oth-ers are new and desir-able learnings acquiredthrough training or edu-cation. In this realm ofnew and desirable learn-ings, NeuroMuscularReprogramming®(NMR) can contribute agreat deal. It utilizes aform of positive kines-thetic conversation withthe body to imprint new learnings on themotor control center of the brain, replacingdamaged imprints created through trauma,injury, operations or repetitive strain fromergonomically inefficient use patterns.
Neurologic Patterns are Easily Disrupted
When a limb is broken or a jointwhiplashed or strained, the damage is not justto the tissues. There is also damage to theneuromuscular programs governing align-ment, movement and postural support. Afterthe bone has knit or the tissue tears have
healed, painful symp-toms often persist.These are a result ofanother kind of injury –dysfunctional move-ment patternsimpressed on the motorcoordination center atthe time of injurywhich do not changesimply because the tis-sue has repaired itself.There are also manyoccasions in life inwhich the body sustainssub-clinical injuries,namely, no tissue dam-age, but a definite dis-ruption of functionaccompanied by very
real pain. Those neurologic patterns can beeasily re-educated. Bodies require periodictune-ups of their motor coordination pro-grams. This is easily done with NMR.
Traditional Rehabilitation Falls Short
Here’s an example of NMR’s capabilities.After an operation to repin the tendons of arepeatedly dislocated shoulder, an orthopedicsurgeon compliments his patient on the 65%of normal range of motion that he hasregained post-rehab. After one session ofNMR, this same client leaves with 95% of hisoriginal range.
R E H A B I L I T A T I O NNEUROMUSCULAR REPROGRAMMING
B y J o c e l y n O l i v i e r
LINKTHE MISSING
LINK
&&Massage
BodyworkM A G A Z I N E

D E C E M B E R / J A N U A RY 2 0 0 0 • M A S S A G E & B O DY WO R K 61
During rehab, the patient performs exer-cises designed to re-build strength in hisshoulder muscles, but he is exercising mus-cles still inhibited from the shock of repeat-ed dislocation. In injuries such as these, themedical profession is concerned with therepair of disrupted tissue – broken bones,torn ligaments, sprains, etc. – and stabilizingthe situation until the body can heal itself.Physical therapy and occupational therapythen provide some brilliant support in theform of rehabilitative exercise. What is notrecognized is that the muscles performingthe exercises still use dysfunctional coordi-nation patterns formed at the time of theinjury. The client’s tonus improves, he feelsbetter, but his recovery is not complete.
Physical therapists want the patient to dothe job of re-building function through self-initiated activity, from the inside out. Hencerehab focuses strongly on exercise programsto strengthen unused neuromuscular path-ways. Unfortunately, the most disused path-ways have developed sensory motor amne-sia; they cannot feel themselves or respondto messages from the motor control center.When exercise is performed, those pathwaysare not accessible. Traditional rehab tends toreinforce the compensatory pathways estab-lished during the process of injury. In thecases where painful symptoms persist twomonths post-rehab, the body is telling usthere are still structural elements thatremain dysfunctional.1
I have observed that we can regain muchmore of our original neuromuscular claritythan is currently believed to be possible. Inthe short time the medical profession hasbeen exploring the field of rehabilitativetherapies, few practitioners have understoodfully what the human body is capable ofachieving. If we knew more results wereavailable to us, we would be more likely topursue them. The missing piece in rehabtherapy – preparing the muscles for newlearnings, re-creating the coordination pat-terns that can best benefit from repetitive
See Neuromuscular, p63
Dysfunction of the motor coordinationprograms governing movement, posturalsupport and alignment are the biggestsource of non-pathological body pain.
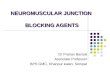
Here, Jocelyn Olivier is shown releasing the adductor brevis to facil-itate hamstring strength.

D E C E M B E R / J A N U A RY 2 0 0 0 • M A S S A G E & B O DY WO R K 63
exercise – comes before the exercise.NeuroMuscular Reprogrammingprovides that missing link.
Dysfunction of the motor coordi-nation programs governing move-ment, postural support and align-ment are the biggest source of non-pathological body pain. These mis-coordinations are easily repro-grammed in fundamentally healthybodies and the relief from pain isusually immediate.
Rehabilitating Disrupted Patterns is the Focus of NMR
NMR engages in a kinestheticconversation with the motor controlcenter of the brain to facilitate newlearnings. It bypasses the usual reflexspinal root circuits to address neuro-muscular problems at their source, themotor control center.
The difference between NMR andother neuromuscular therapies lies inits very specific use of muscle testingto bring to consciousness neuromus-cular dysfunction and cue the brainfor new learnings. We have repeated-ly explored and experimented, com-paring the value of simply releasingover-toned muscles through othermodalities. NeuroMuscularReprogramming adds somethingmore to the effectiveness of all thesetechniques. The results achievedwith the addition of muscle testingare longer lasting and truly re-educa-tional for the client. Involving theintelligence of the consciousbody/mind in the kinesthetic conver-sation of hands-on work far exceedsother release therapies in achievinglasting results. The practitioner testsand then facilitates the establishmentof new or more efficient coordinationpatterns using their choice of releaseand facilitation techniques.
How NMR Works A former football player has a
rotator cuff injury of unknown ori-gin; he cannot remember when thesymptoms started. The shoulder
resists passive movement toward theear and any external rotation causes ajab of pain. Taking the shoulder tothe limit of its comfort in externalrotation, we test the infraspinatus. Ittests weak. The subscapularis, on theother hand, tests strong. We releasethe subscapularis and then retest theinfraspinatus which is now able toresist easily. The client is amazed torealize that he can externally rotatehis shoulder as far back as it wouldnormally be expected to go withoutany pain whatsoever. This re-pro-gramming of the reciprocal inhibitorsof the internal and external rotatorsof the shoulder took five minutes tochange a pattern the client had beenliving with for many years.
Next we test the anterior deltoid.This is also weak. We release theoverly-contracted scalenes and theanterior deltoid can now respond tomotor messages with the appropriateresistance. This five-minute kines-thetic conversation resolves the inhi-bition pattern created by a fixationalong a line of force.
Sometimes muscles which normal-ly work in sequence with each otherwill exhibit “reactive” tendencies.One of the muscles of the “reactive”pair will work fine when tested alone,but test weak when used in sequencewith another. This can happen, asillustrated above, along a “line offorce” or in case of reciprocal inhibi-tion or even within two parts of thesame muscle system such as the ham-strings or the ilio-psoas. The NMRprotocol, which reveals all possiblereactives, performs three tests on twomuscles in sequence, testing first A,then B, then A again.
The patterns of relationship thatare revealed and resolved throughNMR include reciprocal inhibitionacross a joint, lines of force in asequencing of coordinated effort, par-allel structures performing secondarysupport for the disabled muscle, spi-raling patterns of movement, and theresulting weakness in the extremitiesresulting from overstabilization at the
core. More complex situations canalso express themselves as deep ten-sions resulting from superficial inhi-bitions, necessitating that the posturaland movement support be carriedsolely by the intrinsic muscles. Youmay be working with these patternsalready in your practice. NMR willgive you tools to speed up the work.
NMR involves the participation ofthe client. The muscle testing proto-cols serve as a biofeedback device tobring the body into sharp focus,increasing our conscious connectionwith it, revealing how the interrelat-ed parts move and feel coordinatedwith each other. Not only is the ther-apist able to be very detailed andthorough in the assessment process,but the client is thus made consciousof “what’s on” and “what’s off” atthe same time. Clients who are moresensitive to their bodies can feelimmediately the improvement inneuromuscular connectivity as theyparticipate in corrections and con-nections being made.
“Corrections” describes the processan NMR practitioner uses to createchanges in the movement coordina-tion center of the cerebrum wherenew motor skill learnings take place.Testing a muscle in sequence withothers that are involved in a compen-satory pattern cues the brain forreprogramming. It initiates a kines-thetic conversation with the motorcontrol center in the forebrain, bring-ing up a stored pattern from the cere-bellum for conscious re-learning inthe cerebrum. The therapist canchoose any of their own bodyworktechniques to release the inhibitions.Retesting them anchors the new usepattern and causes a rewriting ofthe programs which are then storedin the motor coordination center inthe cerebellum. These new pro-grams become your body’s automat-ic response.
This kinesthetic conversation asan aspect of therapy is fast and thor-ough and usually painless as it doesnot require force. It engages with
Neuromuscular, from p61
n e u r o m u s c u l a r r e p r o g r a m m i n g
See Neuromuscular, p64

64 M A S S A G E & B O DY WO R K • D E C E M B E R / J A N U A RY 2 0 0 0
the body’s intelligence to restore theoptimal patterns for movement lostthrough disuse, misuse or trauma.
What is Muscle Testing?Asking a muscle to resist the
application of a 5-15 pound pressurereveals the clarity of the neuromus-cular connections facilitating thatmuscle. When a muscle has becomedisabled, the body cannot find theneurological connection to respondto the task of resistance againstpressure. One of the beauties ofNMR lies in its ability to be so spe-cific. Muscle testing can give you adetailed assessment of the actionand functional range of a joint.Since joints work in complex varia-tions of alignment with neighboringstructures, careful positioning whilemuscle testing can duplicate anyneuromuscular task and reveal intotal detail which functions areworking and which are not.
Results When All Else has FailedNMR can provide the missing
link in learning for conditions whichhave not previously responded totherapy. We often see clients whohave been to many other kinds ofhealth professionals without gainingrelief from symptoms. Even injuriesyears old can be alleviated with thisessential piece of rehabilitation.
A new NMR graduate is seeing aclient who sustained two whiplashes20 years ago. Since then, the clienthas been unable to raise her headfrom the bed without using herhands to lift her head. She has con-stant pain between her shoulderblades, and the area of her rightdiaphragm is also painful and “hardas a rock.” She has great difficultyworking at her desk, as her armsbecome exhausted after a short timefrom holding them up to her key-board. She has seen orthopedists,chiropractors, Rolfers and osteopathsover the years without success.
Muscle testing reveals no connec-tivity at all in her sternocleidomas-toid muscles (they are completelyunable to respond), and weakness inher quadratus lumborum and glu-teus maximus. After three sessionsof two hours each, including NMRas one of the strategies, the client isnow ecstatic to be moving her headfreely for the first time in 20 years,and is able to lift it unaided from asupine position. After the muscleshave been re-educated throughNMR, the client’s own daily activi-ties continue to strengthen her previ-ously emaciated sternocleidomastoidmuscles. Sometimes the integrationof new information introduced in asession continues to happen over aperiod of the next few days. The cor-rections will continue to evolve andthe client will have regained evenmore functionality by the next visit.
NMR – The Sherlock Holmes ofNeuro-Muscular Problems
In a NeuroMuscular Reprogram-ming class you learn solutions to typ-ical alignment problems and aretaught the principles which enableyou to figure out solutions for theidiosyncratic patterns you find. NMRdoes not replace other bodyworkmodalities; it simply adds a missingtool to your tool kit.
A client came to see me who hadbeen receiving bodywork for yearsfor a gradually decreasing mobility inthe range of movement of her righthip joint and constant pain travelingthrough her right buttock. Walkingproduced a painful “catch” in thearea of the hip joint. Previous yearsof bodywork sessions had helped, butnot resolved, the problem.
There was a lack of elasticitythroughout the hip joint. Externalrotation and extension were severelylimited and muscle testing revealedher psoas and piriformis were weak.This weakness in the psoas wasbeing compensated for by overdevel-oped iliacus muscles. All walkingaggravated a hip joint that was in a
state of contraction throughout, notsupported by the psoas or the exter-nal rotators and over-stabilized bythe internal rotators. Releasing theiliacus and pectinius improved piri-formis strength, but thorough worktesting and re-balancing all the mus-cular elements in the hip, low backand pelvis did nothing to improve thestrength and elasticity of the psoas.The source of the problem involvedanother principle of neuromuscularcoordination, inhibitions along a lineof force – muscles running in thesame direction that sequence to per-form complex actions such as liftingyour food to your mouth.
Work in the area of the scalenesrevealed rigid muscle. This rigiditycaused a locked right rotation of C3,C4 and C5 with so little movement itappeared to have splinted into onebony mass. Bone spurs were develop-ing along the anterior border of thetransverse processes and the wholearea of the scalenes was emaciated.She also experienced limited andpainful range of motion in her rightshoulder.
This unremitting tension in thescalenes caused a shutdown of the“line of force” through the whole rightside of her body, inhibiting her psoasand ankle dorsiflexors. Testing thepsoas in sequence with the scalenesand then releasing the scalenes finallyfacilitated the strengthening of thepsoas. This example illustrates how,when any of the elements along theline of muscles that work in sequenceto perform a function – such as later-al bending or forward flexion –become fixated, they cause inhibitorymessages further down (or up) theline of force.
After one session, the clientreported enormous reduction ofpain through the right hip area andincreased range of motion in theshoulder. After two sessions, herneck no longer had a preferred rightrotation and had regained flexibility.Finally, after five sessions, the righthip pain was completely gone, she
n e u r o m u s c u l a r r e p r o g r a m m i n g
Neuromuscular, from p63

D E C E M B E R / J A N U A RY 2 0 0 0 • M A S S A G E & B O DY WO R K 65
had resumed walking for pleasure and exercise, andshe reported that her energy had returned to levels shehadn’t experienced in years.
Rehabilitating Wrist and Hand ConditionsWhen the scalenes or the anterior deltoid and superi-
or fibers of the serratus attaching to the anterior bor-der of the scapula become chronically contracted, theyinhibit full function of bracchio-radialis and the lateralwrist extensors, and are the source of many discourag-ing symptoms for massage practitioners, causing elbowor wrist strain. How do you go about using NMR tocorrect these imbalances? First, test the bracchio-radi-alis. Then test the scalenes or anterior deltoid. Nowtest the bracchio-radialis again. If the bracchio-radialistests weak either initially or after using it in sequencewith the scalenes, release the scalenes. Then retest thebracchio-radialis again. This anchors the correction.Now the body becomes aware that it is easy to get mes-sages through to a muscle that was kinesthetically“blind” only a few moments earlier.
A Complementary TherapyNMR complements the work of other health profes-
sionals. This work belongs in chiropractor’s offices,physical therapy departments and sports training cen-ters. For example, an NMR practitioner worked con-jointly with a physical therapist on a client who, as aresult of a “tummy tuck,” lost the range of motion inher hips and couldn’t stand up straight or lie on herstomach. The physical therapist worked to stretch thefascia of the lower abdomen, which helped a little, andgave strengthening exercises for the client’s back whichdidn’t help at all. The NMR practitioner tested allfunctions of extension and flexion through the lowerback and abdomen and found the insertion of thepsoas “reactive” to the origin. The psoas was strong atone end and weak at the other. It tested strong in oneposition and weak in another. The tension in the ori-gin of the psoas was also inhibiting the hip extensors.When the origin of the psoas and the internal obliqueswere released after testing the extensors of the hip andback, the client could immediately stand straighter.
The BenefitsThe unexpected benefits of reducing the energy
demand from the support and movement system byimproving neuromuscular efficiency are more energy,clearer vision, increase in muscle definition throughnormal activity levels, a normalization of tissue metab-olism, and more energy available for the higher brainfunctions of creative thought and problem-solving.Psychologically, it means a general sense of greater
See Neuromuscular, p66