Embed Size (px)
Citation preview
Rehabilitation for Rehabilitation for Amputation and Amputation and
Prosthetic Fitting Prosthetic Fitting after Burnafter Burn
Phase IPhase I
Characteristics of amputated limb Characteristics of amputated limb which can functional well in which can functional well in
prosthesisprosthesis Pain freePain free Well padded by soft tissueWell padded by soft tissue Non adherent scar Non adherent scar Cylindrical shapeCylindrical shape Greatest bone lengthGreatest bone length Normal sensationNormal sensation
Prosthetic Rehabilitation Prosthetic Rehabilitation Following Burn AmputationFollowing Burn Amputation
Phases of Rehabilitation
Acute Post Surgical Phase
Pre- Prosthetic Phase
Prosthetic Prescription and Fabrication Phase
Prosthetic Training Phase
Functional & follow up Phase

Time :Amputation Surgery to Suture
Removal
Promote wound healing
Control incisional and phantom pain
Maintain joint(s) ROM
Promote positive nitrogen balance
Goals
Mobilize entire body
Promote Wound Healing
1-A superficial skin defect can usually be closed adequately with a Split –thickness skin graft (STSG).2-Full –thickness defect over bony prominence is better handled with full –thickness coverage (either with local flap, pedicle flap, or free island flap).
Physical therapy can enhance wound healing and reduce associated complication (such as development of hypertrophic scar) through using low level laser therapy (LLLT) (Helium neon laser therapy and or Gl-Al-Ars), with following treatment protocol;
Incisional Pain:-Incisional Pain:- 1-It is a natural part of any surgical 1-It is a natural part of any surgical
procedure where skin subcutaneous tissue, procedure where skin subcutaneous tissue, nerve and muscles have been cut .It usually nerve and muscles have been cut .It usually goes away when swelling reduced and goes away when swelling reduced and healing occurs.healing occurs.
2-Incisional pain should be controlled with 2-Incisional pain should be controlled with adequate amounts of narcotic preferably adequate amounts of narcotic preferably given intravenously on regularly prescribed given intravenously on regularly prescribed dose basis. This is usually helpful for the first dose basis. This is usually helpful for the first three postoperative days. Subsequently oral three postoperative days. Subsequently oral analgesic should be adequate if there are no analgesic should be adequate if there are no other sources of significant painother sources of significant pain
Control Incisional and Phantom Pain
Phantom Pain:-Phantom Pain:- 1-This is a pain in the missing or amputated part of 1-This is a pain in the missing or amputated part of
the limb. It varies tremendously from person to the limb. It varies tremendously from person to person .It can include burning, tingling, squeezing person .It can include burning, tingling, squeezing and cramping, shocking, and shooting description.and cramping, shocking, and shooting description.
2-Phantom pain should be explained to the patients 2-Phantom pain should be explained to the patients since they occur in the early postoperative period.since they occur in the early postoperative period. 3-The patient should expect that phantom pain 3-The patient should expect that phantom pain sensation and phantom limb changes and usually sensation and phantom limb changes and usually
diminished, and may be become long term problem.diminished, and may be become long term problem. 4- Use of oral pain medication for significant phantom 4- Use of oral pain medication for significant phantom
pain has not usually produced adequate pain pain has not usually produced adequate pain reduction over period of time exceeding one week.reduction over period of time exceeding one week.
Control Incisional and Phantom Pain
Phantom Sensation:-Phantom Sensation:- This is sensation or feeling in the part of This is sensation or feeling in the part of
the limb that has been removed. it include the limb that has been removed. it include itching , tingling , warmth, cold, cramping , itching , tingling , warmth, cold, cramping , constriction , movement, and any other constriction , movement, and any other imaginable sensation , and all persons with imaginable sensation , and all persons with limb loss experience some phantom limb loss experience some phantom sensation.sensation.
Rresidual limb pain:-Rresidual limb pain:- This kind of pain occurs in what is left of This kind of pain occurs in what is left of
your natural limb after the amputation, as your natural limb after the amputation, as the residual limb always is more sensitive the residual limb always is more sensitive than other parts of body.than other parts of body.
Control Incisional and Phantom Pain
1-Positioning is an important part of a patient's exercise 1-Positioning is an important part of a patient's exercise program. It is done to prevent shortening of soft tissue and program. It is done to prevent shortening of soft tissue and joint(s) contractures, that can result from ;joint(s) contractures, that can result from ;
(i) Soft tissue shortening .(i) Soft tissue shortening . (Ii) Muscle imbalance. (Ii) Muscle imbalance. (iii) Protective withdrawal reflex.(iii) Protective withdrawal reflex. (iv) Faulty position.(iv) Faulty position. 3-If possible patients with an amputation should lie prone 3-If possible patients with an amputation should lie prone
intermittently to enhance hip and knee extension, however intermittently to enhance hip and knee extension, however care should be taken to avoid over stress on cardiovascular care should be taken to avoid over stress on cardiovascular system during assuming this position.system during assuming this position.
4-The positioning program should emphasize active or 4-The positioning program should emphasize active or active assistive ROM of the joint (s) proximal to the active assistive ROM of the joint (s) proximal to the amputation.amputation.
5-Elevation of residual limb on a pillow can lead to the 5-Elevation of residual limb on a pillow can lead to the development of hip flexion contracture and so should be development of hip flexion contracture and so should be avoided.avoided.
Maintain Joint ROM &Strength
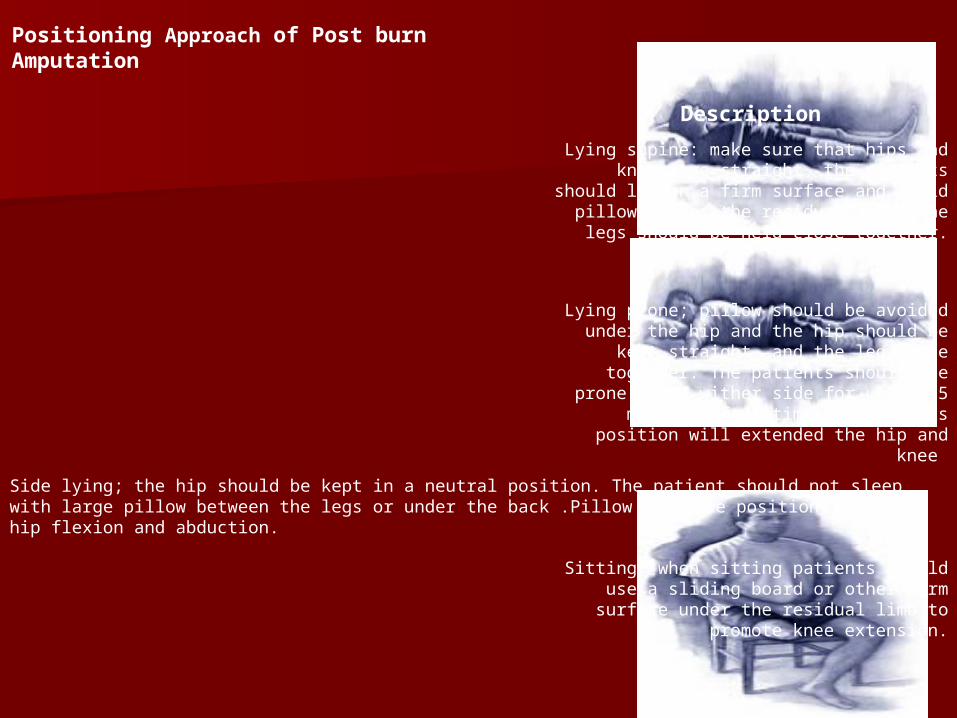
Positioning Approach of Post burn Amputation
Description
Lying supine: make sure that hips and knees are straight, the patients should lie on a firm surface
and avoid pillows under the residual limb. The legs should be held close together.
Lying prone; pillow should be avoided under the hip and the hip should be kept straight, and the leg
close together. The patients should lie prone or on wither side for up to 15 minutes, four times a day.
This position will extended the hip and knee
Side lying; the hip should be kept in a neutral position. The patient should not sleep with large pillow between the legs or under the back .Pillow in these positions enhance hip flexion and abduction.
Sitting: when sitting patients should use a sliding board or other firm surface under the residual limb
to promote knee extension.
ExercisesExercises
1-The exercises program is designed individually 1-The exercises program is designed individually and includes ROM, exercises, isometric, isotonic, and includes ROM, exercises, isometric, isotonic, and endurance activities, and these dependent and endurance activities, and these dependent largely on largely on
(i)-Postoperative healing.(i)-Postoperative healing.
(ii)-Postoperative pain(ii)-Postoperative pain
(iii)-Post-surgical dressing.(iii)-Post-surgical dressing. 2-This exercise should not produce more than 2-This exercise should not produce more than
mild discomfort and put less stress on suture mild discomfort and put less stress on suture line, otherwise stop exercises.line, otherwise stop exercises.
3-The hip extensor, abductors and knee extensor 3-The hip extensor, abductors and knee extensor and flexors are particularly important for and flexors are particularly important for prosthetic ambulation.prosthetic ambulation.
4-Strengthening exercise for upper extremity 4-Strengthening exercise for upper extremity muscles of shoulder depressor, elbow extensor, muscles of shoulder depressor, elbow extensor, wrist extensor, and hand flexor should wrist extensor, and hand flexor should encouraged, with general strengthening encouraged, with general strengthening program for trunk and abdominal muscles.program for trunk and abdominal muscles.
5-The program should emphasize active or 5-The program should emphasize active or active assistive ROM of the joint (s) proximal to active assistive ROM of the joint (s) proximal to the amputation, at 1st to 2nd day the amputation, at 1st to 2nd day postoperative.postoperative.
6- Active motion of all proximal joints through 6- Active motion of all proximal joints through the full ROM should be obtained by 10 -14 days the full ROM should be obtained by 10 -14 days following amputation unless grafting procedure following amputation unless grafting procedure precludes exercising.precludes exercising.
7-Gentle isometric exercises can be started at the 5th 7-Gentle isometric exercises can be started at the 5th postoperative day.postoperative day.
* A brief repetitive isometric exercises (BRIME), * A brief repetitive isometric exercises (BRIME), regimen is an extension of the original isometric .A regimen is an extension of the original isometric .A patient with an imputation may use this regiment which patient with an imputation may use this regiment which consists of up to 20 maximum contractions. consists of up to 20 maximum contractions.
Each held for 6 second Each held for 6 second (Why?).(Why?). A 20 seconds rest after each contraction is A 20 seconds rest after each contraction is
recommended recommended (Why?).(Why?). Rhythmic breathing during the contraction is Rhythmic breathing during the contraction is
recommended recommended (Why?).(Why?). * Multiple angle isometric exercises should be * Multiple angle isometric exercises should be
performed.performed. 8- Isotonic exercises can be encouraged at 7 -10 days 8- Isotonic exercises can be encouraged at 7 -10 days
postoperative.postoperative. 9-Program of muscle contraction and joint motion (8-10 9-Program of muscle contraction and joint motion (8-10
repetition for 3sets) should be repeated several time repetition for 3sets) should be repeated several time daily (4-6 times), and once when adequately performed daily (4-6 times), and once when adequately performed no need for supervision.no need for supervision.
10-These exercises help to10-These exercises help to (i)-Reduce edema, and promote healing.(i)-Reduce edema, and promote healing. (ii)-Maintain joint ROM,(ii)-Maintain joint ROM, (iii)-Prevent contracture and correct (iii)-Prevent contracture and correct
existing contractureexisting contracture (iv)-Allow early mobility self care and (iv)-Allow early mobility self care and (v)-Maintain muscle strength, and (v)-Maintain muscle strength, and
kinesthetic sense of residual and phantom kinesthetic sense of residual and phantom limb, which can later be used in prosthetic limb, which can later be used in prosthetic trainingtraining
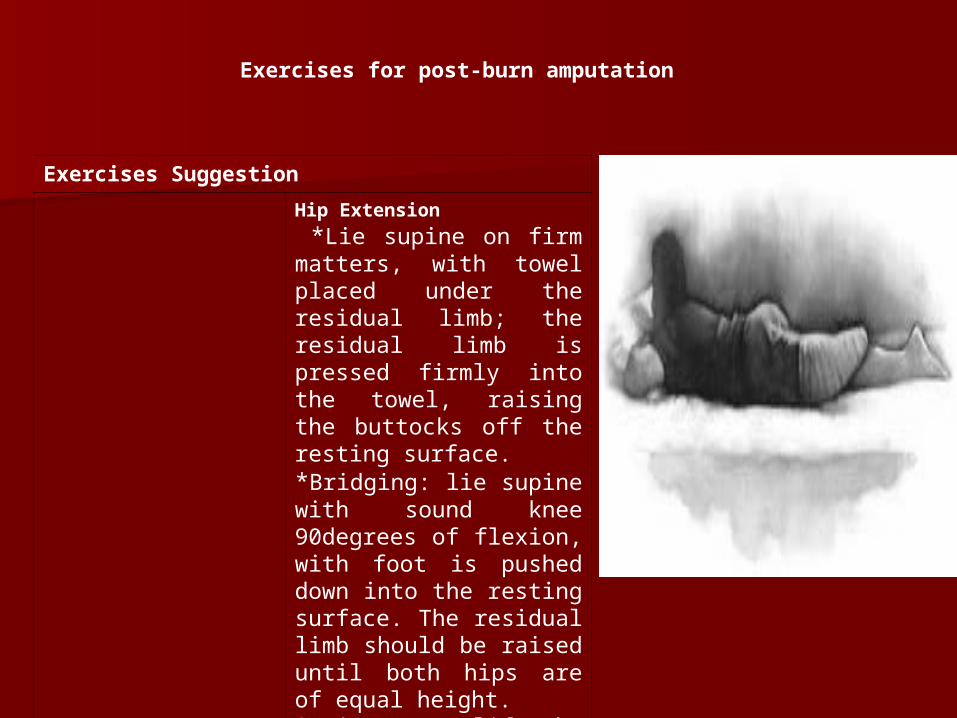
Exercises for post-burn amputation
Exercises Suggestion
Hip Extension
*Lie supine on firm matters, with towel placed under the residual limb; the residual limb is pressed firmly into the towel, raising the buttocks off the resting surface.*Bridging: lie supine with sound knee 90degrees of flexion, with foot is pushed down into the resting surface. The residual limb should be raised until both hips are of equal height.* Lie prone; lift the leg off the mat, at time with knee extended.
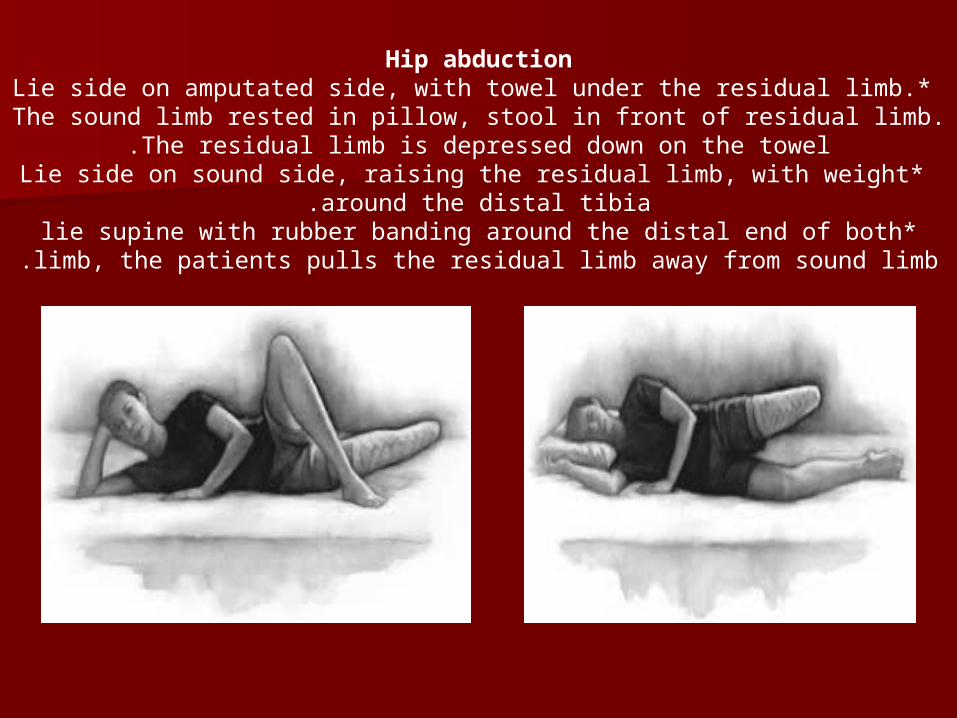
Hip abduction* Lie side on amputated side, with towel under the residual limb. The sound
limb rested in pillow, stool in front of residual limb. The residual limb is depressed down on the towel.
* Lie side on sound side, raising the residual limb, with weight around the distal tibia.
*lie supine with rubber banding around the distal end of both limb, the patients pulls the residual limb away from sound limb.
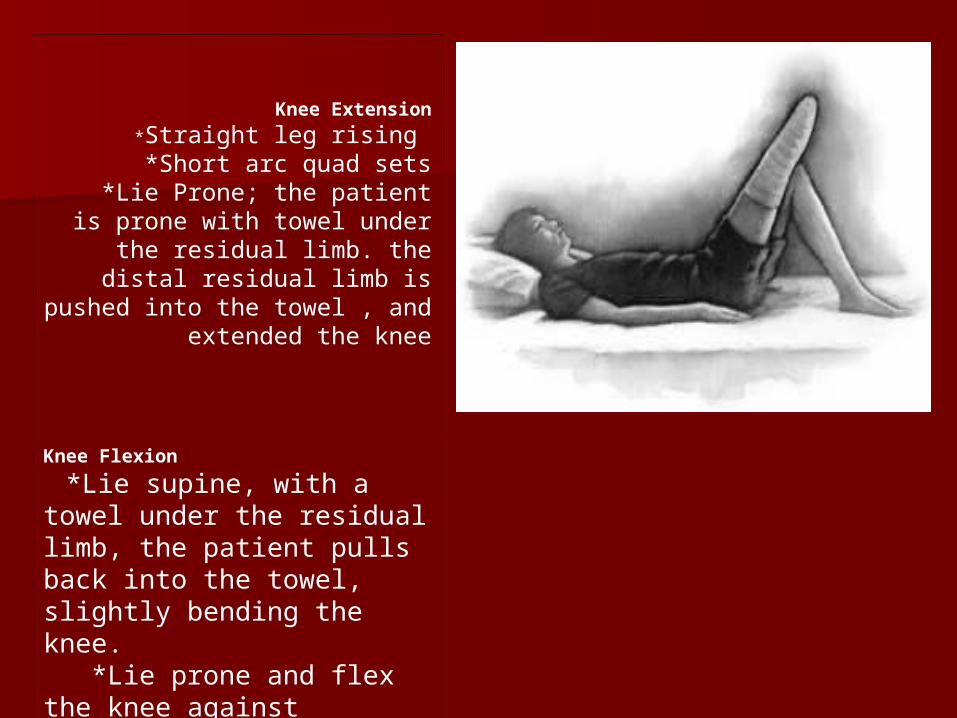
Knee Extension
*Straight leg rising *Short arc quad sets
*Lie Prone; the patient is prone with towel under the residual limb.
the distal residual limb is pushed into the towel , and extended the
knee
Knee Flexion
*Lie supine, with a towel under the residual limb, the patient pulls back into the towel, slightly bending the knee. *Lie prone and flex the knee against gravity.
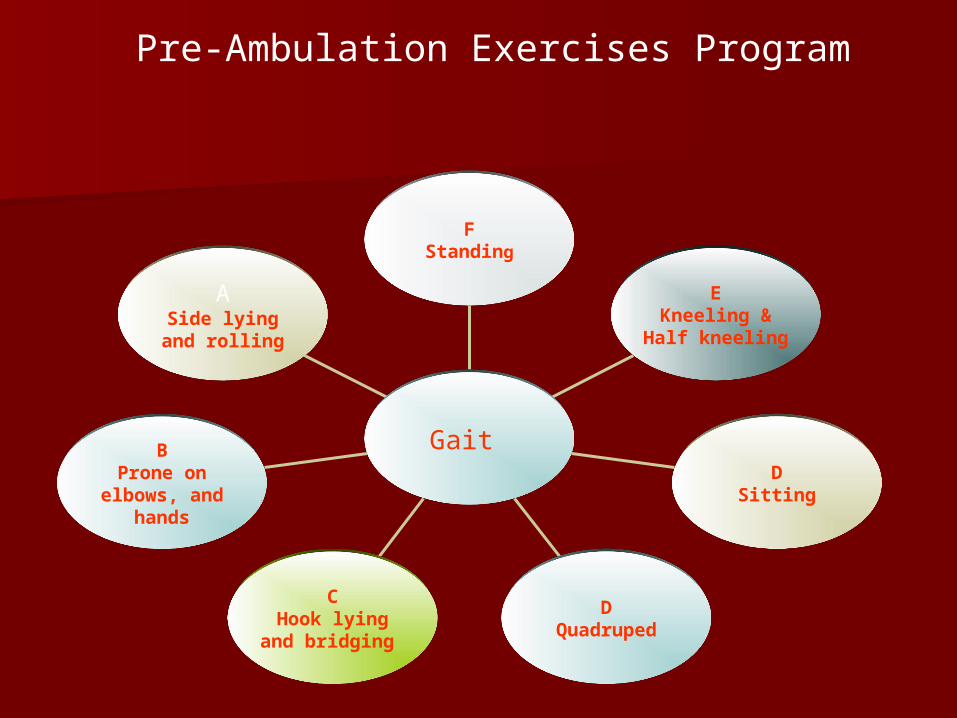
Pre-Ambulation Exercises Program
ASide lying and
rolling
BProne on
elbows, and hands
CHook lying and
bridging
DQuadruped
DSitting
EKneeling &
Half kneeling
FStanding
Gait
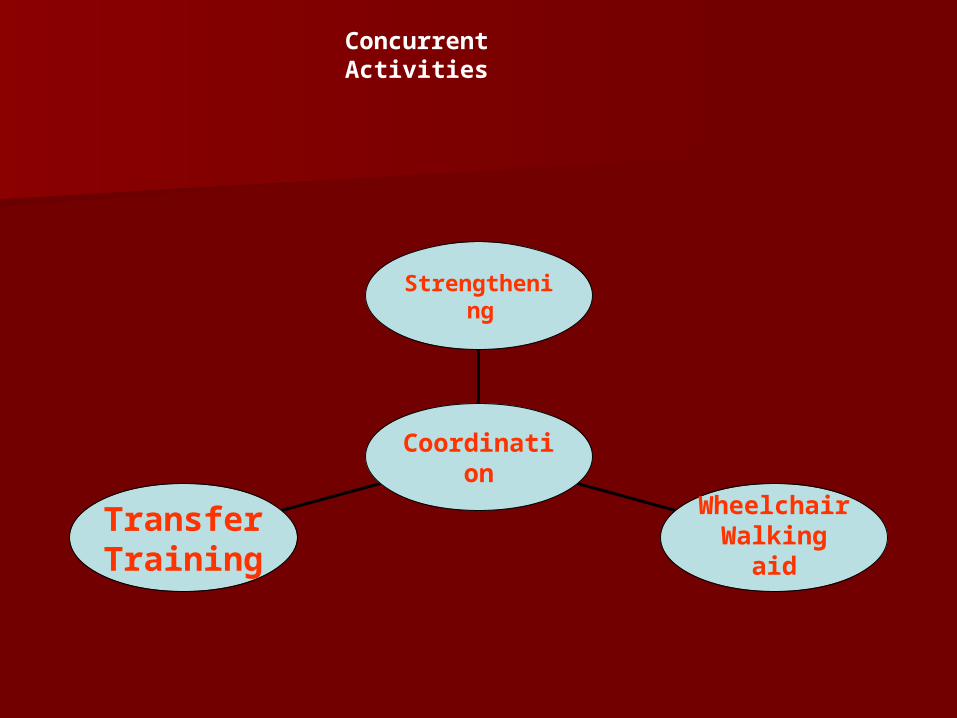
Concurrent Activities
Transfer Training
WheelchairWalking aid
Strengthening
Coordination
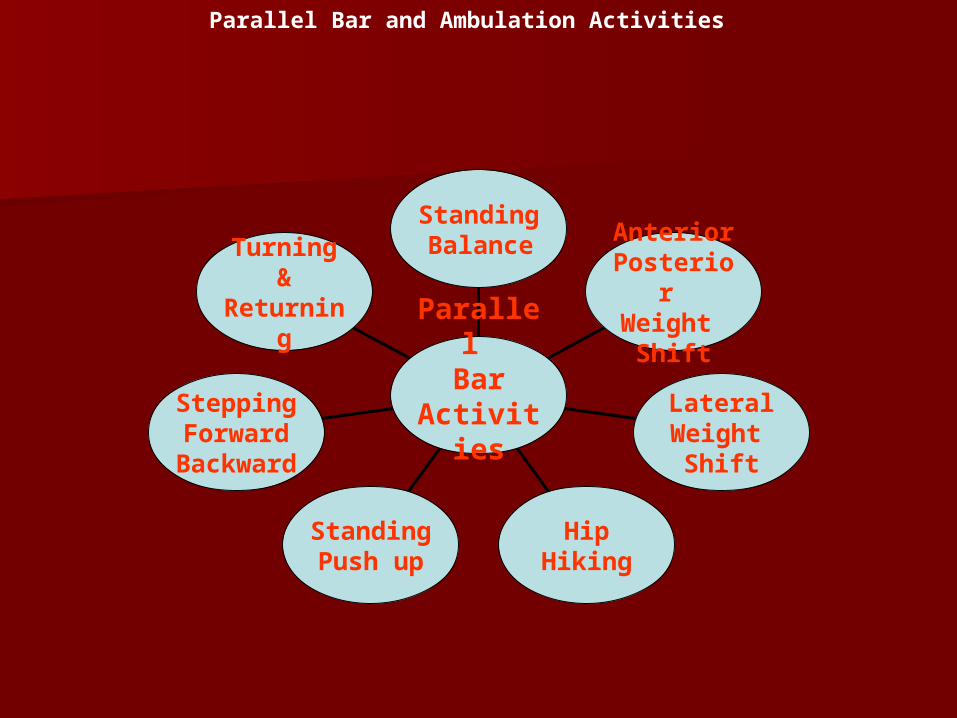
Parallel Bar and Ambulation Activities
Turning&
Returning
SteppingForward
Backward
Standing Push up
HipHiking
Lateral Weight
Shift
AnteriorPosterior Weight
Shift
Standing Balance
Parallel Bar
Activities
Walking with crutches (For persons with single leg amputations
only):
First move the crutches forward about (30 cm). Step forward with your residual
limb/prosthesis. Land it between your crutches. Lift your natural limb and step to, or past the
crutches.
Going up stairs:
Step up with your natural limb first. Then bring your crutches and residual limb/prosthesis up.
Going down stairs:
Don’t hop. Move your crutches down first, then step down with your residual limb/ prosthesis.
Lastly, step down with your natural limb.