Embed Size (px)
Citation preview
Regulatory Realities 2015: Changes that Impact Your Practice
Jennifer Kennedy, MA, BSN, RN, CHCNational Hospice and Palliative Care Organization
October 2015
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 2
FY 2016 Proposed Hospice Wage Index Rule
Rate Update
• 1.6%• Net effect: 1.1%– Adjustments for the final year of BNAF– Adjustments for wage index variations
• Effective October 1, 2015• Standard rate increase in effect for period
October 1, 2015 through December 31, 2015
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 3
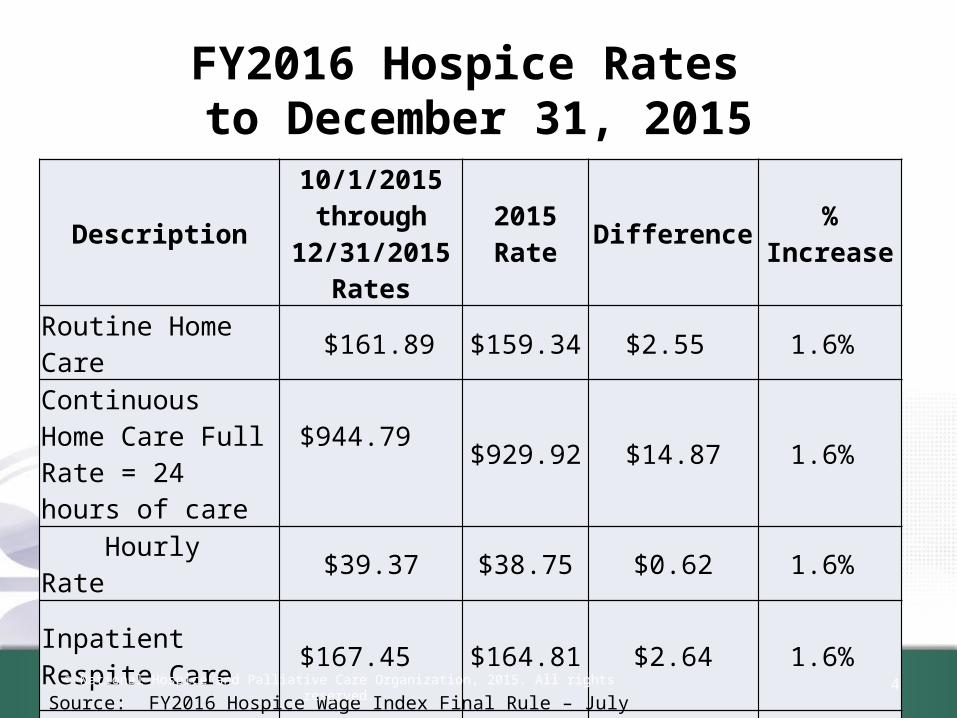
FY2016 Hospice Rates to December 31, 2015
Description10/1/2015
through 12/31/2015
Rates2015 Rate Difference % Increase
Routine Home Care $161.89 $159.34 $2.55 1.6%
Continuous Home Care Full Rate = 24 hours of care
$944.79 $929.92 $14.87 1.6%
Hourly Rate $39.37 $38.75 $0.62 1.6%
Inpatient Respite Care $167.45 $164.81 $2.64 1.6%
General Inpatient Care
$720.11 $708.77 $11.34 1.6%
4Source: FY2016 Hospice Wage Index Final Rule – July 31, 2015
© National Hospice and Palliative Care Organization, 2015. All rights reserved.
Hospice payment reform
• Implemented January 1, 2016• Two tiered routine home care rate– Based on length of stay– 1-60 days – 15% more than current rate– 61+ days -- -8% less than current rate
• Service Intensity Add-on– Last seven days of life– RN or social worker
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 5
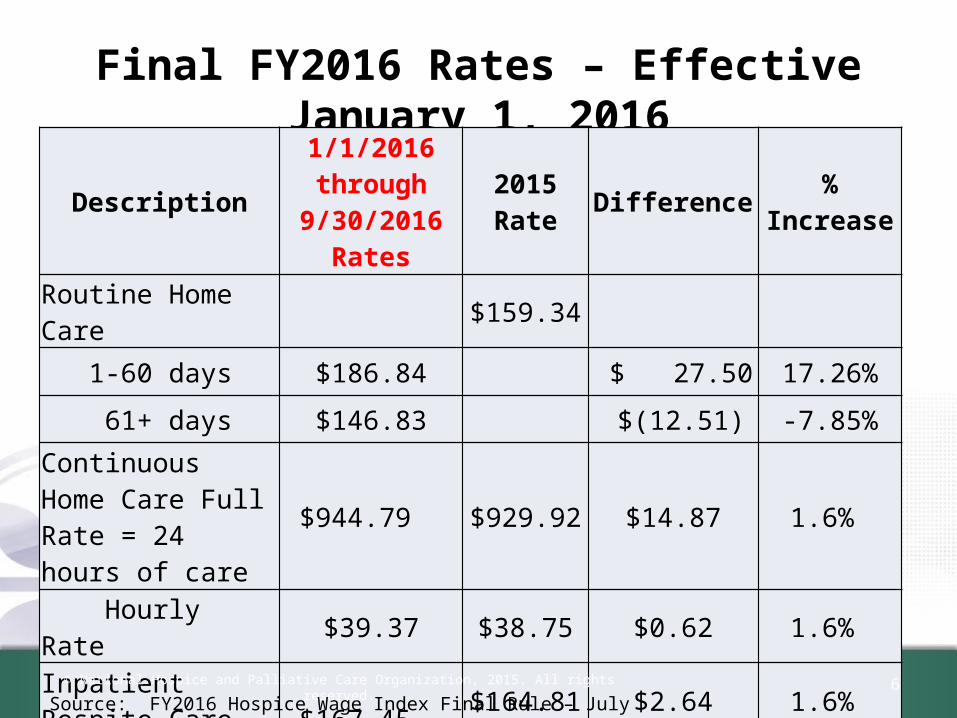
Final FY2016 Rates – Effective January 1, 2016
Description1/1/2016through
9/30/2016Rates
2015 Rate Difference % Increase
Routine Home Care $159.34
1-60 days $186.84 $ 27.50 17.26%
61+ days $146.83 $(12.51) -7.85%
Continuous Home Care Full Rate = 24 hours of care
$944.79 $929.92 $14.87 1.6%
Hourly Rate $39.37 $38.75 $0.62 1.6%
Inpatient Respite Care $167.45 $164.81 $2.64 1.6%
General Inpatient Care $720.11 $708.77 $11.34 1.6%
6Source: FY2016 Hospice Wage Index Final Rule – July 31, 2015
© National Hospice and Palliative Care Organization, 2015. All rights reserved.
Count of days follows the patient
• For patients who revoke their hospice benefit or are discharged and readmitted to hospice care within 60 days of their discharge, the patient’s prior days in hospice care will “continue to follow the patient and will count toward his or her patient days for the new hospice election.”
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 7
Count of days example 1-60 days
• Patients elects Medicare hospice benefit• Day 3 – revoke for additional curative
treatment• Day 10 – re-elect Medicare hospice benefit
• Count of daysAt re-election, the day count is 4
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 8
Count of days example61+ days
• Patient elects Medicare hospice benefit with hospice #1
• Day 55 – discharged by hospice for “no longer terminally ill”
• Day 56 – patient re-elects their Medicare hospice benefit with hospice #2
• How does the day count work?– First hospice – 55 days at higher RHC rate– Second hospice – 5 days at higher RHC rate, remaining
days at lower RHC rate© National Hospice and Palliative Care Organization, 2015. All rights reserved. 9
Day count and levels of care
• Day count includes all hospice days of care• All levels of care• Regardless of whether days of care were
billable or not– Days not billable because of a late face to face– Days not billable because of a NOE that RTPs
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 10
Breaks in Service
• If a hospice patient revokes or is discharged from hospice care and the break in service is 61 days or more, then the patient qualifies for the higher RHC rate.
• If the break in service is 60 days or less, the day count resumes and the patient’s RHC rate drops to the 61+ rate when the total days of care total 61 days or more.
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 11
Existing patients on January 1, 2016
• The calculation of days of care will start with the patient’s hospice election, even if that election started before January 1, 2016.
• Example– Patient elects Medicare hospice benefit on
December 1, 2015– New hospice payment rates begin January 1, 2016• Day count for higher RHC rate is day 32 on 1/1/2016
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 12
Transfer Day
• If a patient transfers from one hospice to another and there is no gap in care, the transfer day will be counted as 1 day, and both hospices will include the same date on their claim.
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 13
Episodes of care
• 2 counts of days will need to be tracked– Benefit (election) periods – 90/90/60s– Episode of care – Benefit period or series of
benefit periods applicable to a single patient, with no more than a 60 day gap in hospice care
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 14
Service Intensity Add-on
• For visits conducted by an RN or social worker• Any time in the last seven days of a hospice patient’s life, • If the following criteria are met:
– The day of care is a RHC day– The day occurs during the last 7 days of life– The patient’s discharge is due to death– Direct care is provided by an RN or social worker – Only in person visits count toward the payment; no social
worker phone calls• The total hours paid at the SIA cannot exceed 4 hours in
a day for the RN and social worker combined© National Hospice and Palliative Care Organization, 2015. All rights reserved. 15
SIA Payments
• The SIA payment equals the CHC hourly rate of $39.37, regionally adjusted
• Multiplied by the number of hours of RN and social worker direct patient care visit time, listed on the claim form in 15 minute increments.
• Minimum of 15 minutes, maximum of 4 hours per day
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 16
Claims processing
• RHC: Hospice will file claim for a routine home care day– CMS claims processing will determine 60 day or
61+ day payment rate• SIA: Hospice will report visits and visit times
as usual– CMS claims processing will determine which days
and visits will qualify for SIA payment
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 17
Service Intensity Add-on Payment
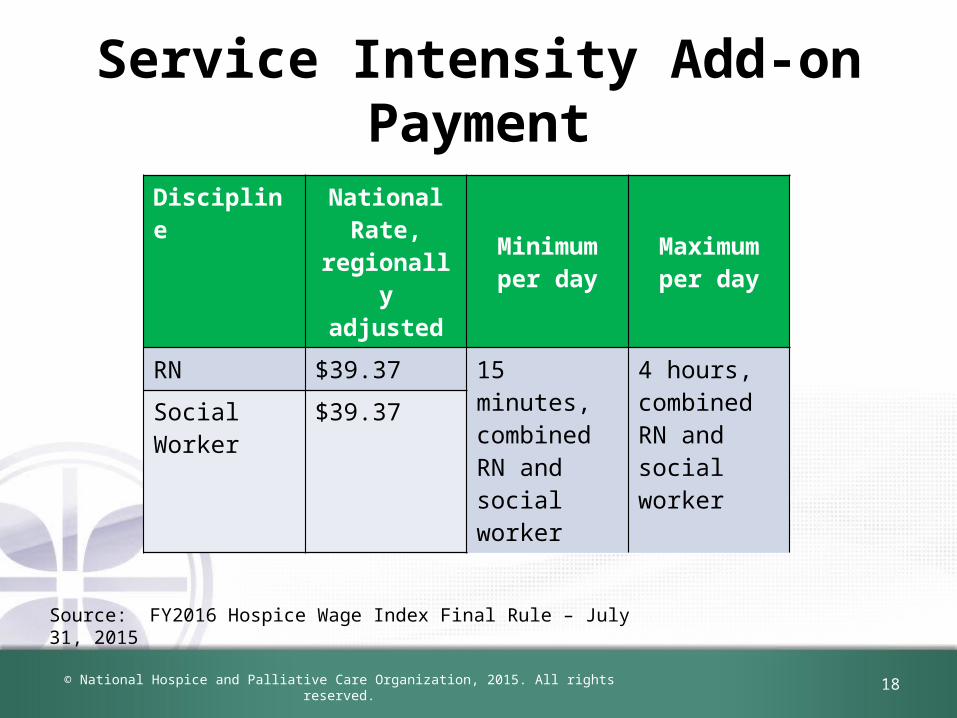
Discipline National Rate, regionally adjusted
Minimum per day
Maximum per day
RN $39.37 15 minutes, combined RN and social worker
4 hours, combined RN and social worker
Social Worker $39.37
Source: FY2016 Hospice Wage Index Final Rule – July 31, 2015
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 18
RN Visits
• Current visit reporting (G-codes) includes both RN and LPN/LVN
• CMS will create two separate G-codes to track RN and LPN visits separately to allow for SIA payments for RN visits
• Watch for a CMS transmittal and implementation date
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 19
Medicaid Implementation
• The Social Security Act requires that Medicaid “payment for hospice care be in amounts no lower than the amounts, using the same methodology,” used under Medicare
• Two-tiered RHC rate applies to both Medicare and Medicaid.
• CMS anticipates that state Medicaid agencies will need additional time to make the necessary systems and software changes in the RHC structure.
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 20
Memo to States from CMS
• Memo issued September 1, 2015.• CMS expects that:– Medicaid will comply with new rate structure– the state agencies share the Medicaid hospice
payment rates for FY 2016 with the hospice providers in their respective states
• http://www.medicaid.gov/medicaid-chip-program-information/by-topics/benefits/downloads/medicaid-hospice-rates-ffy-2016.pdf
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 21
Hospice Wage Index
• Last year of budget neutrality adjustment factor (BNAF)
• Hospice floor– If wage index is less than 0.8, a 15% increase to
the wage index is calculated– The result of the calculation is used, to a
maximum of 0.8
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 22
2010 Census and CBSA changes
• FY2016 wage index charts implement the changes in urban and rural areas based on the 2010 census
• Published by the Office of Management and Budget (OMB).
• One year transition to new CBSA or state designations– 50% at old wage/50% at new wage index
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 23
Cap amount
• 2015 Cap amount: $27,382.63 for the cap period November 1, 2014 through October 31, 2015.
• 2016 Cap amount: $27,820.75 for the cap period November 1, 2015 through October 31, 2016– 2016 cap amount updated by the FY2016 hospice
payment update of 1.6%
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 24
Proposed quality measures for future years
• No new measures are proposed for payment year FY2017• High priority concept areas are being considered,
including:– Patient reported pain outcome measure– Claims-based measures focused on care practice patterns
• skilled visits in the last days of life• burdensome transitions of care for patients in and out of the hospice
benefit• rates of live discharge from hospice
– Responsiveness of hospice to patient and family care needs– Hospice team communication and care coordination
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 25
CAHPS participation for 2018 Annual Payment Update
• Required to collect data using the CAHPS ® Hospice Survey • Must use CMS-approved third party vendors • Ongoing monthly participation is required January 1, 2016
through December 31, 2106 • Compliance will dictate the payment amounts for FY2018• Deadlines for data submission occur quarterly • Due second Wednesday of the submission months
– August– November– February– May
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 26
Quality Reporting Thresholds
• Data submission deadlines for HIS records thresholds: – January 1 – December 31, 2016: 70% of all related HIS records
will be submitted within the 30 day submission timeframe for the year or face the 2% reduction in the marketbasket update for 2018.
– January 1 – December 31, 2017: 80% of all related HIS records will be submitted within the 30 day submission timeframe or face the 2% reduction in the marketbasket update for 2019.
– January 1 – December 31, 2018: 90% of all related HIS records will be submitted within the 30 day submission timeframe for the year or face the 2% reduction in the marketbasket update for 2020.
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 27
Fewer than 50 survey-eligible caregivers for CAHPS survey
• If a hospice has fewer than 50 survey-eligible decedents/caregivers in the period January 1, 2016 to December 31, 2016, are exempt from the CAHPS ® Hospice Survey
• To qualify a hospice MUST submit an exemption request form, available in the first quarter of 2017
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 28
Notification of non-compliance
• CMS will begin using the QIES National System for Certification and Survey Provider Enhanced Reports (CASPER) system
• Can be accessed using the CASPER reporting application
• Letters will also be sent via regular USPS mail, beginning with the FY2017 payment determination
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 29
Public display of quality measures
• CMS will develop “the infrastructure for public reporting and method for hospices to preview their quality data prior to publicly reporting any such information”
• A timeframe for public reporting of quality measure data in hospice will be announced in future rulemaking
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 30
Quality Reporting Impact on Payments
• Beginning in FY 2014, hospices which fail to report quality data will have their market basket update reduced by 2 percentage points.
• For FY2016, the percentage increase is -0.4%
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 31
Diagnosis Reporting on Claim Form
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 32
Diagnosis Reporting on Hospice Claims
• Clarification: Hospices will report ALL diagnoses identified in the initial and comprehensive assessments on the hospice, whether related or unrelated to the terminal prognosis, effective October 1, 2015.
• Mental health conditions: This will include any mental health disorders or conditions that would affect the plan of care.
• “Virtually all”: CMS states that “hospices are required to provide virtually all the care that is needed by terminally ill individuals and we [CMS] would expect to see little being provided outside the benefit
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 33
Diagnosis Reporting on Claim Form
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 34
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 35
Four case studies on frequent hospice diagnoses
• Case studies presented for following diagnoses– chronic airway obstruction– congestive heart failure– cerebral degeneration– lung cancer
• Citation of :– Typical symptoms– Evidence-based practice interventions/ recommendations
• Comments on Medicare spending outside the hospice benefit
© National Hospice and Palliative Care Organization, 2015. All rights reserved.
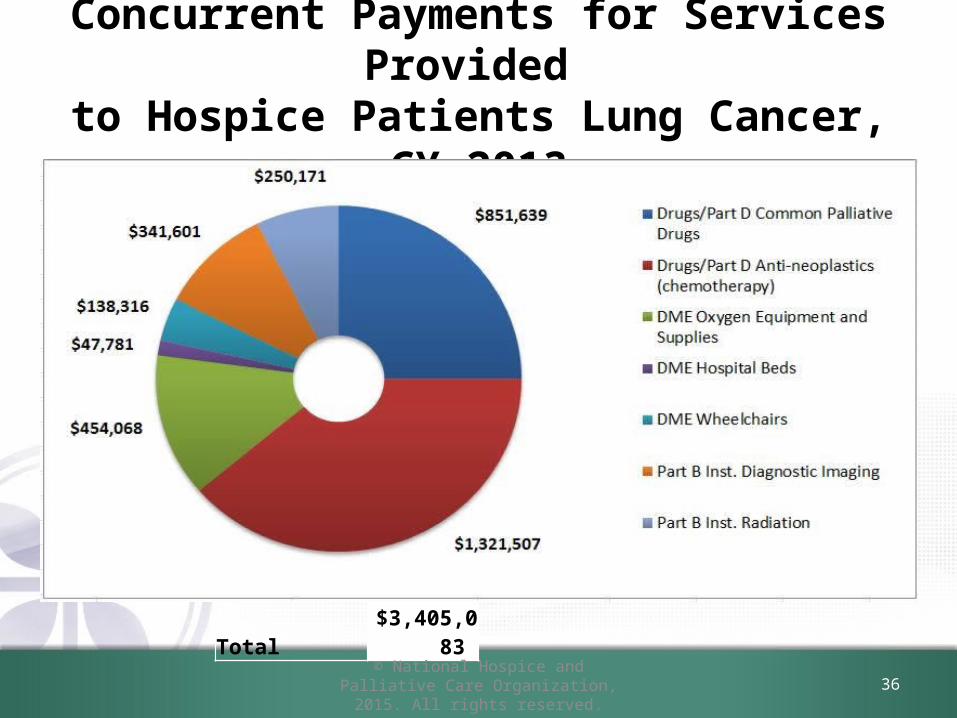
Concurrent Payments for Services Provided to Hospice Patients Lung Cancer, CY 2013
Total $3,405,083
36
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 37
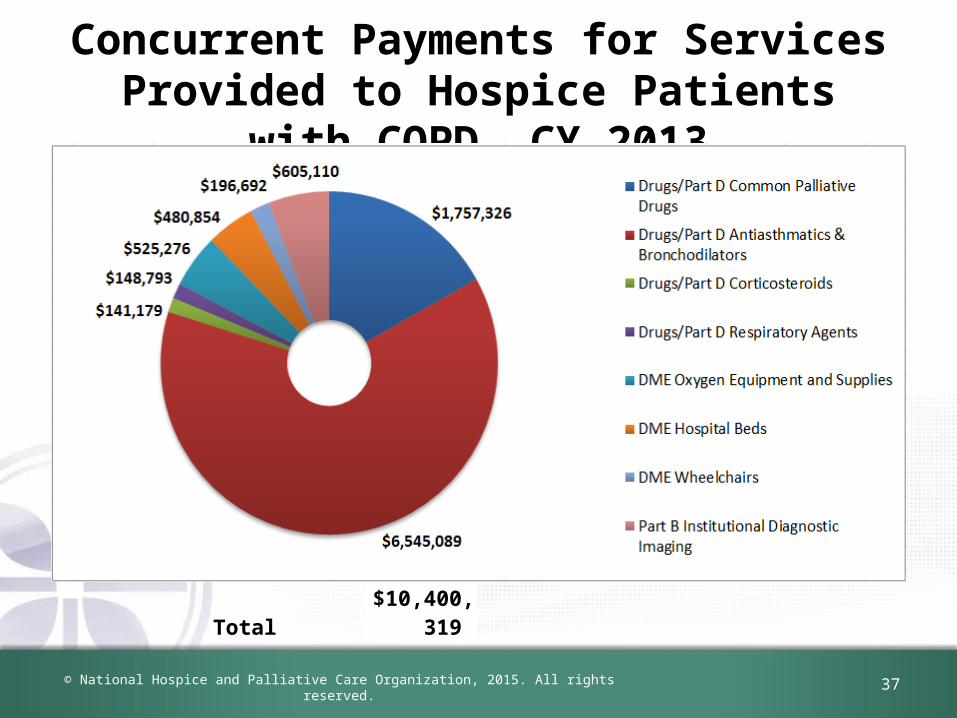
Concurrent Payments for Services Provided to Hospice Patients with COPD, CY 2013
Total $10,400,319
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 38
CMS Concern
• Analysis reveals:– Clinical based practices are not being covered
under the Medicare hospice benefit. – Potential systematic unbundling of the Medicare
hospice benefit – May be valuable analysis to inform policy
stakeholders
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 39
NHPCO Comments to CMS• NHPCO is concerned that CMS is holding hospice providers
alone solely responsible for all claims filed on behalf of beneficiaries who have elected hospice, and yet hospices often do not know, and are not in control of, whether or how other providers bill, and for what services, nor can hospices control whether and when a beneficiary sees a non-hospice provider.
• We encourage CMS to establish systems in claims processing so that other providers are immediately aware of the patient’s hospice election and are guided to coordinate with the hospice and to bill appropriately.
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 40
Assessment of Conditions and Comorbidities Required by Regulation
• We (CMS) continue to state that those circumstances would be “exceptional and unusual” and that hospices continue to be required to provide virtually all the care that is needed by terminally ill patients.
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 41
Assessment of Conditions and Comorbidities Required by Regulation
• Comorbidities are recognized as important factors – Contributing to the overall status of an individual – Should be considered when determining terminal
prognosis.• Mental health comorbidities must also be
considered. – Not uncommon for terminally ill individuals to have
underlying mental health conditions– Could contribute to their prognosis and/or affect the
plan of care
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 42
NHPCO Comments to CMS
• The cause and impact of a mental health (or any other) diagnosis has to be determined on a case by case basis, and expecting global adherence to general rules is unreasonable.
• In addition, the impact of any comorbid diagnosis may vary based on the individual length of prognosis.
• A hospice physician needs to make the determination of what is related to the terminal prognosis based on each individual patient’s clinical condition.
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 43
NHPCO Comments to CMS
• “Virtually all”– NHPCO strongly asserts that determinations of
“relatedness” must be made on a case by case basis, as CMS has stated previously, and it is the role and responsibility of the hospice medical director or hospice physician to determine what is related to the terminal prognosis, and what is not.
– We urge CMS to avoid blanket assertions or assumptions about which services are always related to a patient’s terminal prognosis.
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 44
Parts A, B And D: “Leakage”Non Hospice Spending In Medicare
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 45
Part A and B Expenditures During a Hospice Stay
• FY2013– Paid by Medicare: $697.1 million– Paid by beneficiaries: $132.5 million
Source: FY2016 Hospice Wage Index proposed rule, April 30, 2015
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 46
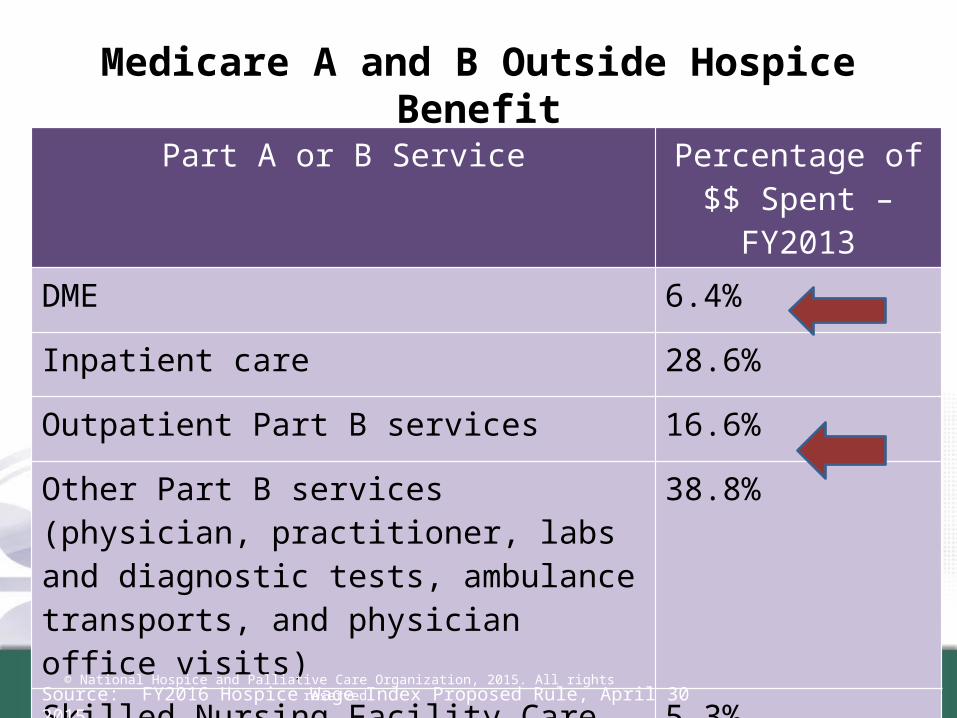
Medicare A and B Outside Hospice BenefitPart A or B Service Percentage of $$
Spent – FY2013DME 6.4%
Inpatient care 28.6%
Outpatient Part B services 16.6%
Other Part B services (physician, practitioner, labs and diagnostic tests, ambulance transports, and physician office visits)
38.8%
Skilled Nursing Facility Care 5.3%
Home Health Care 4.3%
Source: FY2016 Hospice Wage Index Proposed Rule, April 30 2015
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 47
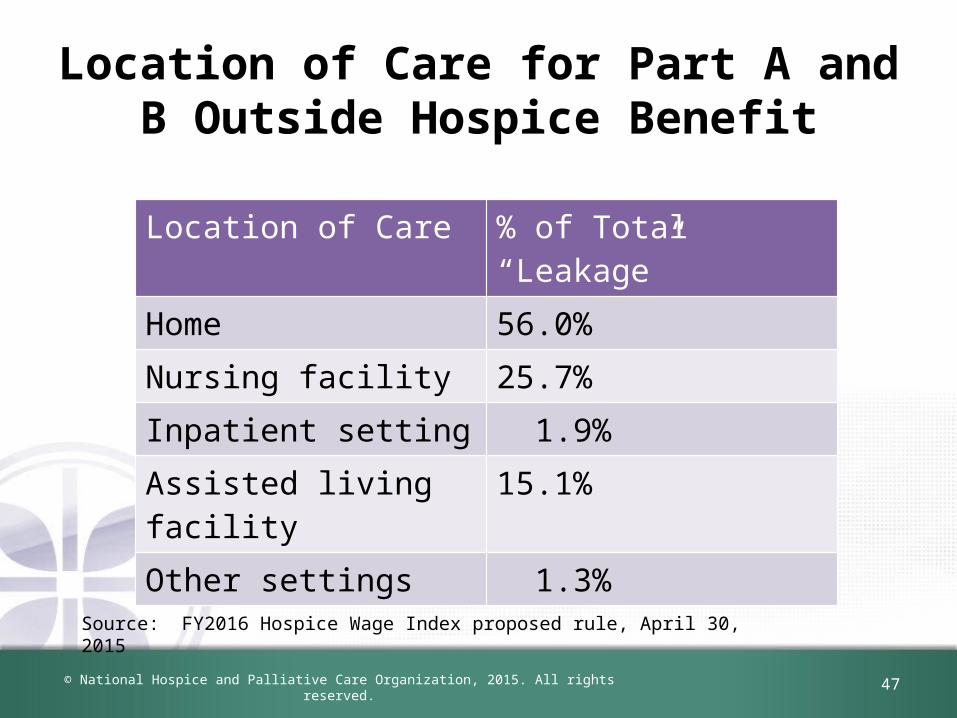
Location of Care for Part A and B Outside Hospice Benefit
Location of Care % of Total “Leakage”Home 56.0%Nursing facility 25.7%Inpatient setting 1.9%Assisted living facility 15.1%Other settings 1.3%
Source: FY2016 Hospice Wage Index proposed rule, April 30, 2015
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 48
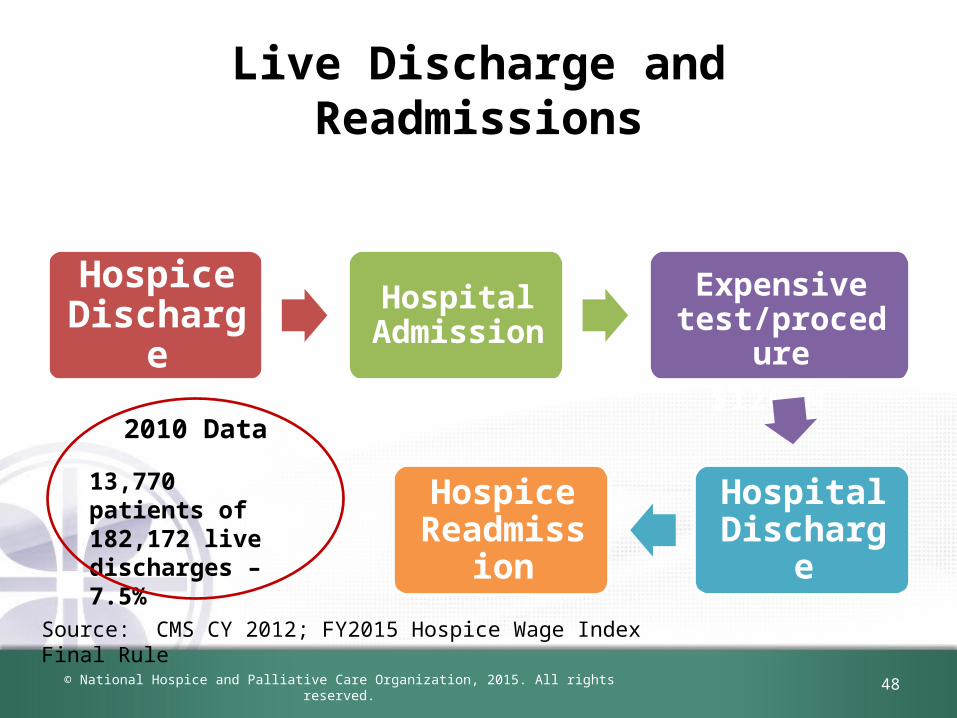
Live Discharge and Readmissions
Hospice Discharge
Hospital Admission
Expensive test/procedure$126 M
Hospital Discharge
Hospice Readmission
Source: CMS CY 2012; FY2015 Hospice Wage Index Final Rule
2010 Data
13,770 patients of 182,172 live discharges – 7.5%
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 49
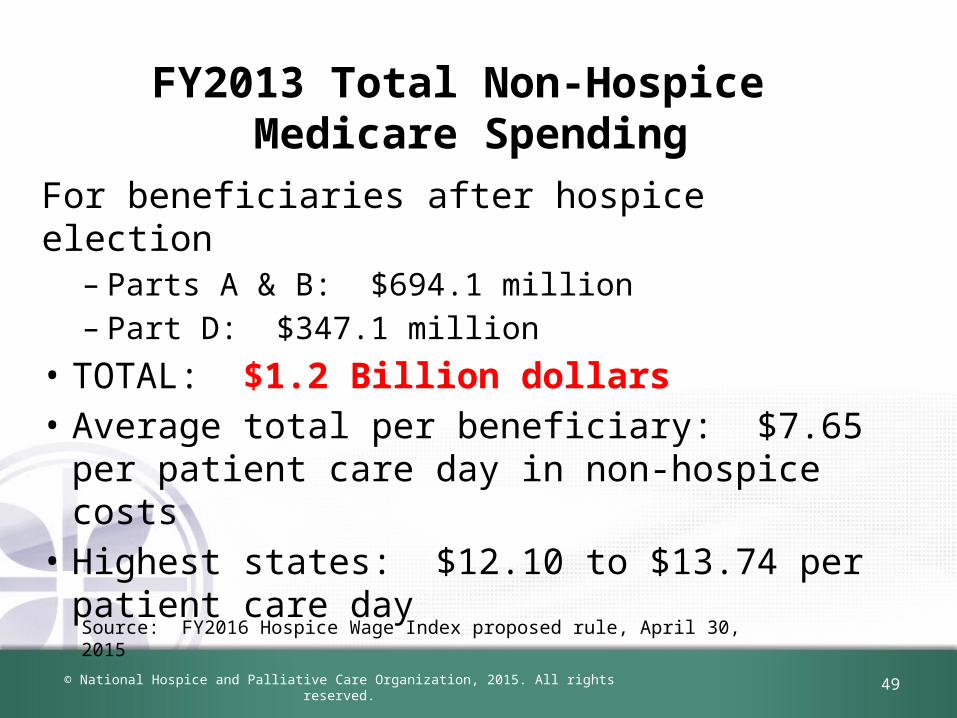
FY2013 Total Non-Hospice Medicare Spending
For beneficiaries after hospice election– Parts A & B: $694.1 million – Part D: $347.1 million
• TOTAL: $1.2 Billion dollars• Average total per beneficiary: $7.65 per
patient care day in non-hospice costs• Highest states: $12.10 to $13.74 per patient
care daySource: FY2016 Hospice Wage Index proposed rule, April 30, 2015
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 50
CMS Commentary
• We further examined hospice utilization data and developed a provider-level file to identify aberrant hospice behavior. The provider level file contains information on beneficiaries who were discharged (alive or deceased) in Calendar Year (CY) 2012 and includes claims data from January 1, 2010 through December 31, 2012.
© National Hospice and Palliative Care Organization, 2015. All rights reserved.
OFFICE OF INSPECTOR GENERAL ACTIVITIES
51
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 52
Hospice care in assisted living
• Report released January 2015• Payments in ALFs more than doubled in 5 years,
totaling $2.1 billion in 2012. • Hospice beneficiaries in ALFs often had
diagnoses that usually require less complex care.
• Hospices typically provided fewer than 5 hours of visits per week
• Visit mix was heavily hospice aides
© National Hospice and Palliative Care Organization, 2015. All rights reserved.
53
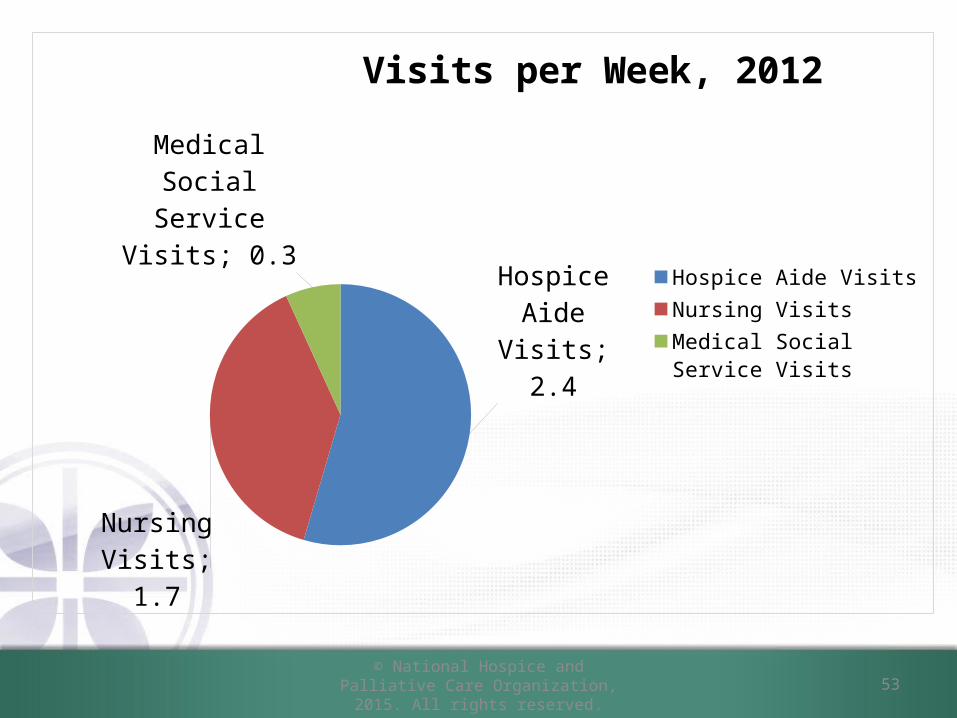
Hospice Aide Visits;
2.4
Nursing Vis-its; 1.7
Medical Social Service Visits; 0.3
Visits per Week, 2012
Hospice Aide VisitsNursing VisitsMedical Social Service Visits
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 54
OIG Areas of Concern
• 25 hospices reported no visits to their patients in ALFs in 2012 -- $2.3 million in Medicare $$
• 97 hospices relied on ALFs for most of their Medicare patients. More than ½ of Medicare payments they received in 2012
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 55
Additional OIG Hospice Focus in 2015
• Review of Hospice GIP – Assess the appropriateness of hospices’ general
inpatient care claims – Review content of election statements for
hospice beneficiaries who receive general inpatient care
– Review hospice medical records to address concerns that this level of hospice care is being misused or overused
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 56
Medicare Care Choices Model
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 57
Medicare Care Choices Model
• CMS sent letters to more than 125 providers• Huge expansion of grantee pool• Formal announcement with the list of
grantees will be made by CMS soon• Two start date cycles for 5 year project– January 1, 2016– January 1, 2018
• Awardees randomly selected
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 58
Physician Fee Schedule (PFS) Proposed Rule
© National Hospice and Palliative Care Organization, 2015. All rights reserved. 59
CY2016 Medicare Physician Fee Schedule
• Posted July 8, 2015• Two codes for Advance Care Planning
“activated” for 2016– CPT code 99497: 1st 30 minutes– CPT code 99498: each additional 30 minutes
• Scheduled to begin January 1, 2016• Comments due: September 8, 2015
Questions
60
NHPCO members enjoy unlimited access to Regulatory AssistanceFeel free to email questions to [email protected]
© National Hospice and Palliative Care Organization, 2015. All rights reserved.
© National Hospice and Palliative Care Organization, 2015. All rights reserved.
Regulatory and Compliance Team at NHPCO
Jennifer Kennedy, MA, BSN, RN, CHCDirector, Regulatory and Compliance
Judi Lund Person, MPHVice President, Regulatory and Compliance
Email us at: [email protected]
61
References
CMS Hospice Centerhttp://www.cms.hhs.gov/center/hospice.asp
Conditions of Participation HospiceFY 2016 Hospice Wage Index Final RuleMedicare Benefit Policy Manual; Chapter 9 - Coverage of
Hospice Services
NHPCO Regulatory Pagehttp://www.nhpco.org/resources/regulatory
62© National Hospice and Palliative Care Organization, 2015. All rights reserved.