Embed Size (px)
Citation preview

8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 1/15
W o r l d J . S u r g . 6, 10-24, 1 9 8 2
of Sdrgery
Major and Minor Segmentectomies "R6gl6es" in Liver Surgery
Henri Bismuth, M.D., Didier Houssin, M.D., and Denis Castaing, M.D.
Uni t~ de Ch i ru rg ie H~pa to -Bi l ia i re , F acu l t6 de M6dec ine P a r i s S ud , H6p i ta l P au l Brousse , Vi l le ju i f , F rance
I n d i v i d u a l i z a ti o n o f t h e s e g m e n t a s t h e f u n c t i o n a l a n a t o m i -
c a l u n i t o f t h e l iv e r p e r m i t s t h e p e r f o r m a n c e o f s u r g i c a l
s e g m e n t e c t o m i e s . T h e s e s e g m e n t a l r e s e c ti o n s a r e " r 6 g l 6 e s "
b e c a u s e t h e p l a n e o f c l e a v a g e o f t h e h e p a t i c p a r e n c h y m a
f o l lo w s t h e a n a t o m i c a l s c is s u r a e . F r o m t h e t e c h n i c a l p o i n t
o f v i e w , l i v e r s e g m e n t e c t o m i e s a r e c h a r a c t e r i z e d b y a n
e x c l u s i v e t r a n s p a r e n c h y m a t o u s a p p r o a c h t o t h e v a s c u l a r
p e d i c le s o f t h e s e g m e n t t o b e r e m o v e d . W e h a v e p e r f o r m e d
t h i s t y p e o f s u r g e r y i n 2 2 p a t i e n t s w i t h n o m o r t a l i t y . T h e s e
o p e r a t i o n s a r e i n d i c a t e d i n : ( 1 ) s o m e b e n i g n t u m o r s ; ( 2 )
s o m e l i v e r t r a u m a ; ( 3 ) b i l i a r y o p e r a t i o n s a b o v e t h e h i l u s ,
w h e r e a n t e r i o r r e s e c t i o n o f s e g m e n t I V c a n b e n e c e s s a r y ;
a n d ( 4 ) c a r c i n o m a s o f t h e g a l l b l a d d e r d i s c o v e r e d h i s t o l o g i -
c a l ly a f t e r c h o l e c y s t e c t o m y . L i v e r s e g m e n t e c t o m i e s c a n a l s o
b e i n d i c a te d f o r m a l i g n a n t t u m o r s w h e n t h e l i v e r is c i r r h o t -i c , o r w h e n a n e x t e n d e d r e s e c t i o n i s l ik e l y t o e x p o s e t h e
p a t i e n t t o t h e r i s k o f l i v e r f a i l u r e . I n d e e d , o n e o f t h e m a i n
a d v a n t a g e s o f l i v e r s e g m e n t e c t o m i e s i s t h a t t h e y p e r m i t
a n e c o n o m i c a l b u t s a f e s u r g i c a l r e s e c t i o n o f t h e h e p a t i c
p a r e n c h y m a .
There is some confusion in the world literatureregarding the definition of the anatomical divisionof the liver. Elsewhere in this symposium, thedifferent concepts are explained and a nomencla-ture, that of Couinaud [1], is chosen. According to
Couinaud, a segment is the smallest anatomical unitof the liver (Fig. 1). The segment described byCouinaud corresponds approximately to the sub-segment described by Goldsmith and Woodburne[2]. It is different from the area descr ibed by Hea ley
Reprint requests: Henri Bismuth, H6pitalBrousse, 94800 Villejuif, France.
0364-2313/82/0006-0010 $03.009 1982 Socidt6 Internationale de Chirurgie
Paul
and Schroy [3], which is based upon the biliary
distribution rather than up on the portal distribution.The resection of one of the 8 segments o f the liver
is called a segmentectomy: unisegmentectomywhen 1 segment is removed, plurisegmentectomy
when 2 or more segments are removed. Liversegmentectomies are intermediate procedures be-tween the 4 common hepatectomies and the smallatypical wedge resections. Segmentectomies are"r6gl6es" because they follow exclusively the ana-tomical liver scissurae that separate the differentsegments of the gland. Respect of these scissuraeduring segmental excisions prevents impairment of
the vascularization of the remaining parenchymaand excessive bleeding. A thorough knowledge ofthe anatomical structure of the liver is prerequisiteto the performance of liver segmentectomies.
Liver segmentectomies permit the anatomicalresection of hepatic lesions without the unneces-sary removal of a large amou nt of normal parenchy-ma. They are particularly useful in some benigntumors or posttraumatic lesions; for carcinomas ofthe gallbladder; more rarely for biliary surgeryabove the hilus; for removal of small centralhepatocarcinomas; and for liver resections in cir-rhotic patients.
The purpose of this report is to describe thetechnical aspects of the major and minor liversegmentectomies "r6gl6es." We shall also reviewour experience with various segmental resections in22 patients (Table 1) who underwent this type of
surgery at our hospital betw een 1970 and 1980. Thedifferent indications for operation are given in
Table 2.Liver segmentectomies "r6gl6es" are the best
illustration of the technique of primary intraparen-chymatous approach of the hepatic vessels de-scribed by Ton That Tung [4]. Indeed, since most ofthe left or right liver is conserved, there is no place
8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 2/15
H.B i sm uth e t a l . : Se gm e nte c tom i e s i n L i ve r Sur ge r y 11
,o,
B
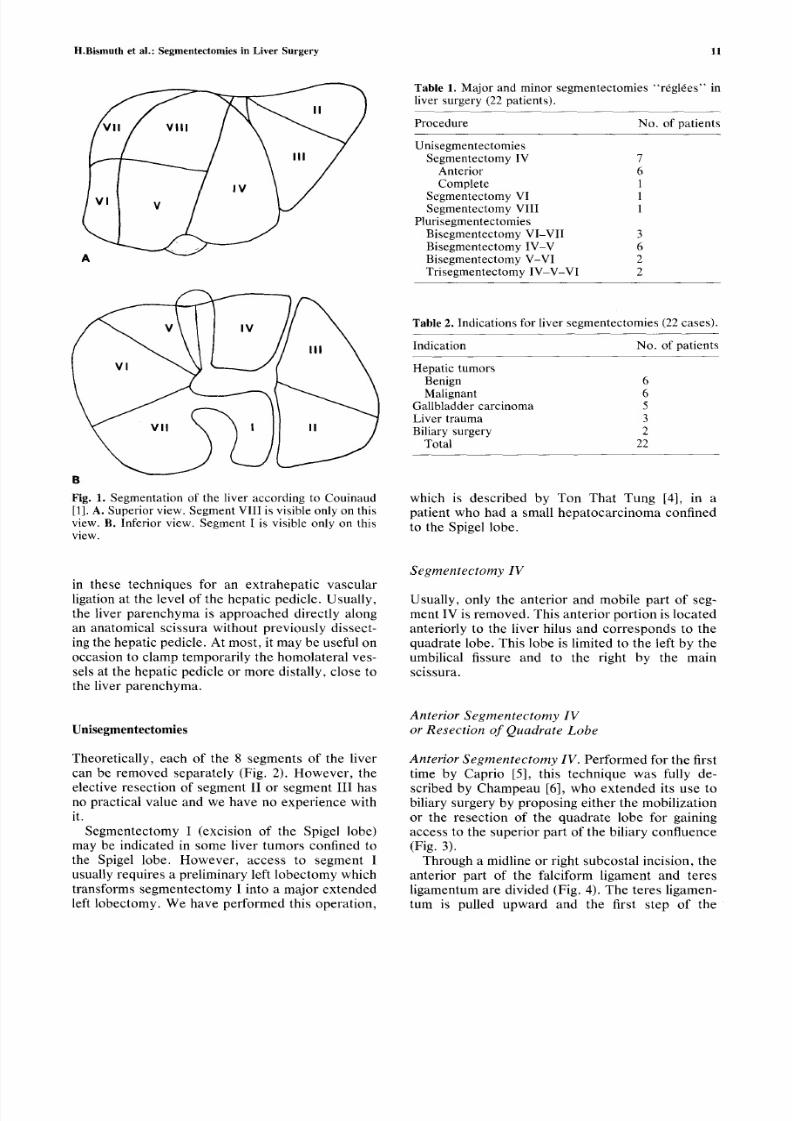
Fig. 1 . Segm enta t ion of the l ive r accord ing to Cou inaud[1]. A. Sup erior view. Segm ent VIII is visible only on thisview. B. Inferior view. Segment I is vis ible only on thisview.
Ta b l e 1. Major and minor s egmentec tomies " rdgl6es" inl iver su rgery (22 pat ients) .
P rocedure No. of pa t i en t s
Unisegmentec tomiesS e g m e n t e c t o m y I V 7
Ante r ior 6
Comple te 1S e g m e n t e c t o m y V I 1S e g m e n t e c t o m y V I I I 1
P lur i s egmentec tomiesB i s e g m e n t e c to m y V I - V I I 3B i s e g m e n t e c to m y I V - V 6B i s e g m e n t e c to m y V - V I 2T r i s e g m e n t ec t o m y I V - V - V I 2
Ta b l e 2. Indicat ions for l iver segmentectomies (22 cases) .
Indica t ion No. of pa t i en t s
Hepa t i c tumorsBenign 6Mal ignant 6
Gal lb ladder ca rc inom a 5L i v e r t r a u m a 3Bil iary surgery 2
Total 22
w h i c h i s d e s c r i b e d b y T o n T h a t T u n g [ 4 ] , i n a
p a t i e n t w h o h a d a s m a l l h e p a t o c a r c i n o m a c o n f i n e d
t o t h e S p i g e l l o b e .
i n t h e s e t e c h n i q u e s f o r a n e x t r a h e p a t i c v a s c u l a r
l i g a ti o n a t t h e l e v e l o f th e h e p a t i c p e d i c l e . U s u a l l y ,
t h e l i v e r p a r e n c h y m a i s a p p r o a c h e d d i r e c t l y a l o n g
a n a n a t o m i c a l s c i s s u r a w i t h o u t p r e v i o u s l y d i s s e c t -
i n g t h e h e p a t i c p e d i c l e . A t m o s t , i t m a y b e u s e f u l o n
o c c a s i o n to c l a m p t e m p o r a r i l y t h e h o m o l a t e r a l v e s -
s e ls a t t h e h e p a t i c p e d i c l e o r m o r e d i s t a l l y , c lo s e t o
t h e li v er p a r e n c h y m a .
U n i s e g m e n t e c t o m i e s
T h e o r e t i c a l ly , e a c h o f t h e 8 s e g m e n t s o f th e l i v e r
c a n b e r e m o v e d s e p a r a t e l y ( Fi g . 2 ). H o w e v e r , t h e
e l e ct iv e r e s e c t i o n o f s e g m e n t I I o r s e g m e n t I I I h a s
n o p r a ct i ca l v a l u e a n d w e h a v e n o e x p e r i e n c e w i t h
it .
S e g m e n t e c t o m y I ( e x c i si o n o f t h e S p i g e l lo b e )
m a y b e i n d i c a t e d in s o m e l i v e r t u m o r s c o n f i n e d t o
t h e S pi g el l o b e. H o w e v e r , a c c e s s t o s e g m e n t I
u s u a ll y r eq u i r e s a p r e l i m i n a r y l e f t l o b e c t o m y w h i c h
t r a n s f o r m s s e g m e n t e c t o m y I i n to a m a j o r e x t e n d e d
l e ft l o b e c t o m y . W e h a v e p e r f o r m e d t h i s o p e r a t io n ,
S e g m e n t e c t o m y I V
U s u a l l y , o n l y t h e a n t e r i o r a n d m o b i l e p a r t o f s eg -
m e n t I V i s r e m o v e d . T h i s a n t e r i o r p o r t i o n i s l o c a t e d
a n t e r i o r l y to t h e l i v e r h i l u s a n d c o r r e s p o n d s t o t h e
q u a d r a t e l o b e . T h i s l o b e i s l im i t e d t o t h e l e f t b y t h e
u m b i l ic a l f i s s u r e a n d t o t h e r i g h t b y t h e m a i n
s c i s s u r a .
A n t e r io r S e g m e n t e c t o m y I V
o r R e s e c t io n o f Q u a d r a t e L o b e
A n t e r i o r S e g m e n t e c t o m y I V . P e r f o r m e d f o r t h e f i rs t
t i m e b y C a p r i o [ 5], t h i s t e c h n i q u e w a s f u l l y d e -
s c r i b e d b y C h a m p e a u [ 6 ] , w h o e x t e n d e d i t s u s e t o
b i li a ry s u r g e r y b y p r o p o s i n g e i t h e r t h e m o b i l i z a t io n
o r t h e r e s e c t io n o f th e q u a d r a t e l o b e f o r g a i n in g
a c c e s s t o t h e s u p e r i o r p a r t o f t h e b i l i a ry c o n f l u e n c e
(Fig. 3) .
T h r o u g h a m i d l in e o r r i g h t s u b c o s t a l i n c i si o n , t h e
a n t e r io r p a r t o f t h e f a l c i f o r m l ig a m e n t a n d t e r e s
l i g a m e n t u m a r e d i v i d e d ( F i g . 4 ) . T h e t e r e s l i g a m e n -
t u r n i s p u l l e d u p w a r d a n d t h e f i r s t st e p o f t h e

8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 3/15
12 W o r ld J . S u rg . Vo l . 6 , No . 1 , Janu a ry 1982
A B
C D
Fig. 2. Unisegmentectomies. A and B. SegmentectomyIV: anterior, of the quadrate lobe (A), and complete (B).C. Segmentectomy VIII. D. Segmentectomy VI.
resection consists of dividing the bridge of paren-
chyma which frequently joins segments III and IV
below the teres ligamentum. This bridge of paren-
chyma is transected by crushing it down with a
Kelly clamp and by electrocoagulation or ligation of
the small vessels. Then, the peritoneum is divided
at the inferior part of the teres ligamentum and 2 or
3 arterial and portal pedicles are dissected to theright of the teres ligamentum. These pedicles are
not systematized and are directed toward the quad-
rate lobe.
The portal pedicles are behind the arterial pedi-
cles, which are superficial. In depth, there is a
fibrous tissue, which constitutes the superior limit
of the teres ligamentum and in which 2 biliary ducts
are usually present.
On the anterior side of the liver and along the
main scissura, the liver is transected up to the
vertex of the hilus. There are no portal branches in
this scissura and the only major vascular elements
requiring ligation are the left branches of the middle
hepatic vein. It is preferable to transect the liver a
little to the left of the main scissura to avoid the
middle hepatic vein.
Posteriorly, at the inferior part of the liver, the
capsule of Glisson is incised in fron t of the peritone-
um of the hilum and some small arterial and portal
branches of the quadrate lobe are ligated and divid-
ed.
Subsequently, a transverse incision of the cap-
sule of Glisson is made at the superior port ion of the
liver, which will join the posterior ends of the right
and left liver transections. This posterior liver tran-
section is performed progressively by crushing
down the parenchyma. During this transection, 3 to
5 branches of the middle hepatic vein are divided.
C o m p l e t e S e g m e n t e c t o m y I V . This procedure is
equivalent to the complete resection of the medial
part of the liver (Fig. 5). Segment IV is removed up
to the anterior part of the vena cava.
The first steps are similar to those performed for
the resection of the quadrate lobe. However, the 2
posteriorly directed parenchymatous transections
are extended up to the vena cava. The middle
hepatic vein, which is usually posteriorly located
close to the vena cava, is not divided during this
complete segmente ctomy IV. Howev er, when the
vein crosses transv ersely the po sterior part of seg-
ment IV to join more anteriorly the left hepatic
vein, it may be necessar y to ligate it, without risk tothe remaining parenchy ma.
As segment IV is just anterior to the Spigel lobe(segment I), the last step of the resection is to
separate these 2 segments. There is no visible
demarcation between the posterior and inferior
parts of segment IV and the anterior and superior
parts of segment I and, for this reason, this last step
can cause bleeding.
After complete resection of segment IV, the liver
is almost split into 2 parts and an approximation of
the 2 parts may be n ecessary to avoid the stomach
and duodenum occupying the wide space between
the right liver and the left lobe.
C a s e Rep o r t s . Patient no. 1 was a 33-year-old
female, on oral contraception for 8 years. During anoperation for an ovarian cyst, she was found to
have a large asymptomatic liver tumor. Angiogra-
phy revealed 2 hypervascu lar lesions: 1 in segment
IV (5 cm in diameter) and 1 in segment VIII (8 cm in
diameter). At reoperation the benign nature of the
tumor was established by frozen section. Because
of the benign character of the lesion and the risk
involved with a large resection, only the anterior
lesion was removed by an anterior segmentectomy
IV, principally for histological diagnosis. Definite
histology was focal nodular hyperplasia. Two years
later, liver ultrasound revealed no modification of
the segment VIII lesion.
Patient no. 2 was a 38-year-old female, on oral
contraception for 8 years, who had a large asymp-
tomatic tumor of segment IV discovered during an
operation for an ovarian cyst. Angiography re-
vealed a large hypervascular lesion in segment IV
and a smaller lesion in segment VIII. At reope ration
the tumor (15 cm in diameter), which was an
hemangioma, was surgically removed by an anteri-
or segmentec tomy IV. The other hemang ioma (7 cm
in diameter) was treated by intraoperative emboli-
zation of the right paramedian artery. One year
8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 4/15
H . Bi smut h e t a l . : Se g m e nt e c t o m i e s i n L i v e r Sur g e r y 1 3
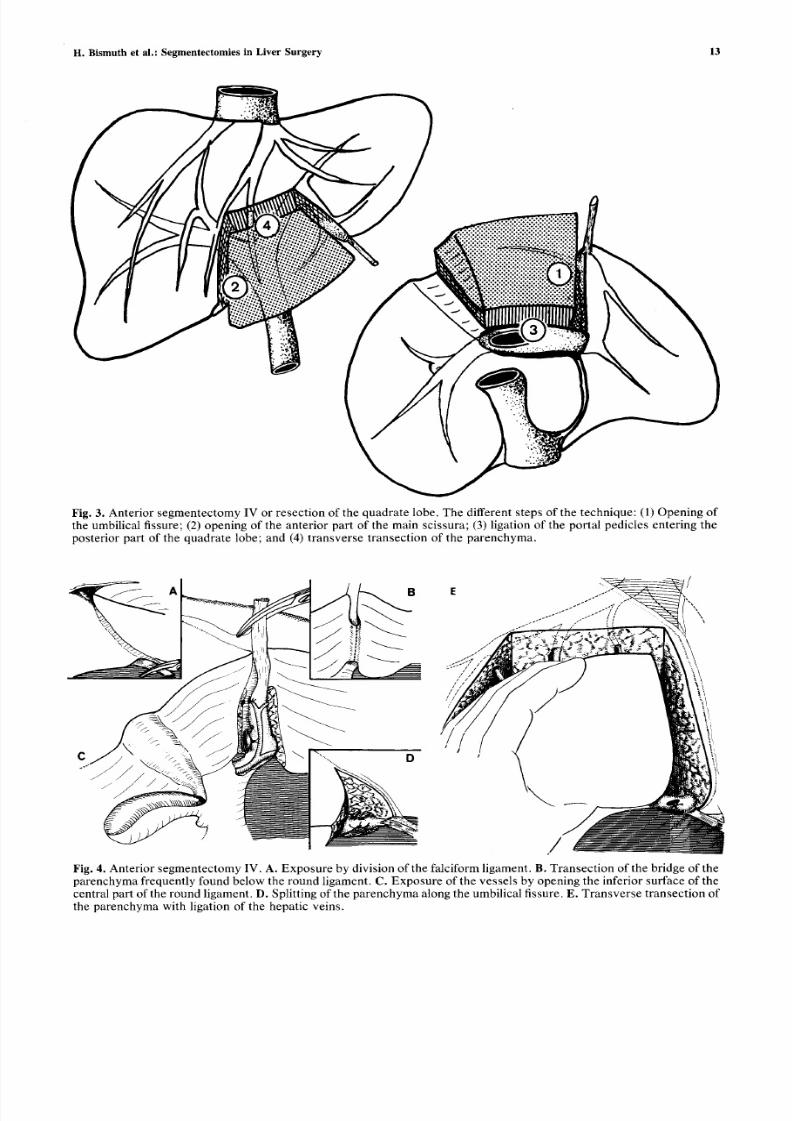
Fig. 3 . Ante r io r s egm entec tom y IV or re s ec t ion o f the quadra te lobe . T he d i f fe ren t s t eps o f the t echn ique : (1) Open ing o fthe umbi l i ca l f i s su re ; (2 ) open ing o f the an te r io r p a r t o f the m a in s c i s s u ra ; (3 ) liga t ion o f the por ta l p ed ic le s en te r ing thep o s t e r i o r p a r t o f th e q u a d r a t e l o b e ; a n d ( 4) t r a n s v e r s e t r a n s e c t io n o f th e p a r e n c h y m a .
Fig . 4 . Ante r io r s e gm ente c tom y IV. A . E xp os u re by d iv i s ion o f the fa lc i fo rm l igament . B . T rans ec t io n o f the b r idge o f thep a r e n c h y m a f re q u e n t l y f o u n d b e l o w t h e r o u n d l i ga m e n t . C . E x p o s u r e o f th e v e s s e l s b y o p e n i n g t h e i n f e r i o r s u r f a ce o f t h ecen t ra l pa r t o f the round l igament . D . Sp l i t t ing o f the pa re nch ym a a long the umbi l i ca l f i s s u re. E . T ra ns v e rs e t ran s ec t ion o fthe pa ren chy ma wi th l iga tion o f the hepa t i c ve ins .
8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 5/15
14
I I
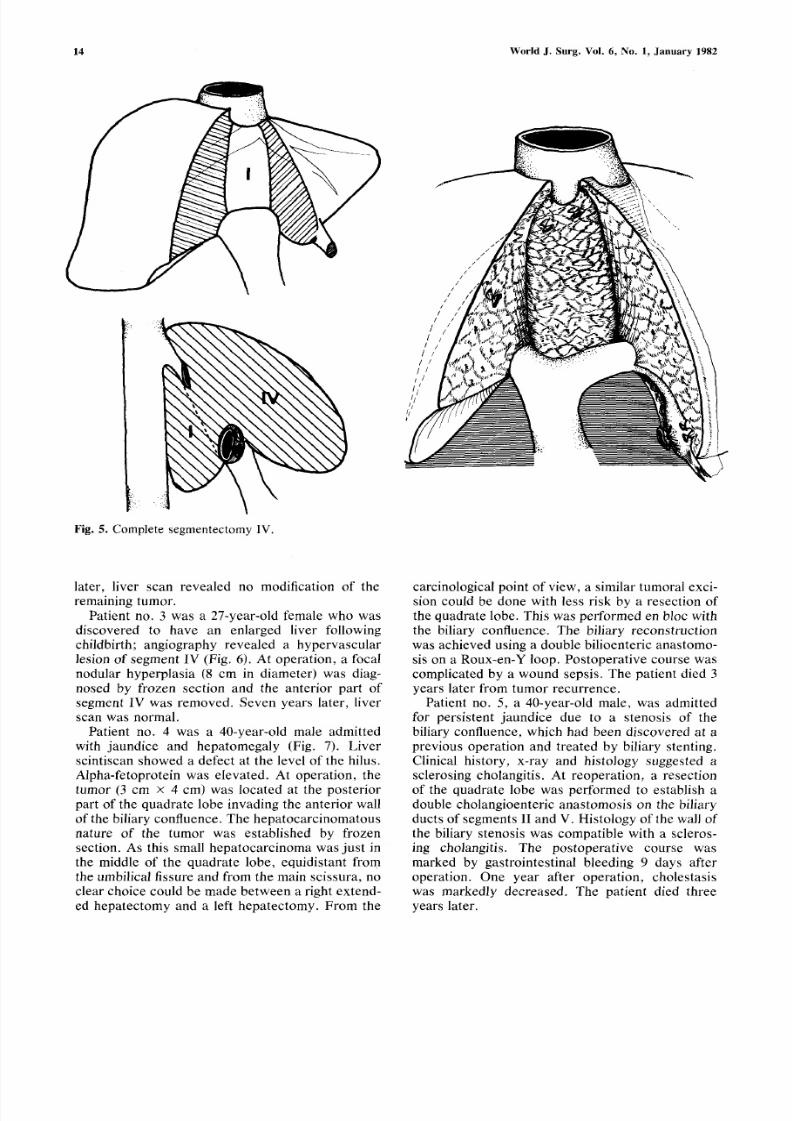
F i g . 5. Complete segmentectomy IV.
W o r l d J . S u r g . V o l . 6, N o . 1 , J a n u a r y 1 9 8 2
later, liver scan revealed no modification of the
remaining tumor.
Patient no. 3 was a 27-year-old female who was
discovered to have an enlarged liver following
childbirth; angiography revealed a hypervascular
lesion of segment IV (Fig. 6). At operation, a focal
nodular hyperplasia (8 cm in diameter) was diag-
nosed by frozen section and the anterior part of
segment IV was removed. Seven years later, liver
scan was normal.
Patient no. 4 was a 40-year-old male admittedwith jaundice and hepato megaly (Fig. 7). Liver
scintiscan showed a defect at the level of the hilus.
Alpha-fetoprotein was elevated. At operation, the
tumor (3 cm • 4 cm) was located at the posterior
part of the quadrate lobe invading the anterior wall
of the biliary confluence. The hepatoca rcinomato us
nature of the tumor was established by frozen
section. As this small hepatocarcino ma was just in
the middle of the quadrate lobe, equidistant from
the umbilical fissure and from the main scissura, no
clear choice could be made between a right extend-
ed hepatectomy and a left hepatectomy. From the
carcinological point of view, a similar tumoral exci-
sion could be done with less risk by a resection of
the quadrate lobe. This was performed en bloc with
the biliary confluence. The biliary reconstruction
was achieved using a double bilioenteric anastomo-
sis on a Roux-en-Y loop. Postoperative course was
complicated by a wound sepsis. The patient died 3
years later from tumor recurrence.
Patient no. 5, a 40-year-old male, was admitted
for persistent jaundice due to a stenosis of the
biliary confluence, which had been discovered at aprevious operation and treated by biliary stenting.
Clinical history, x-ray and histology suggested a
sclerosing cholangitis. At reoperation, a resection
of the quadrate lobe was performed to establish a
double cholangioenteric anastomosis on the b i l i a ryducts of segments II and V. Histo logy of the wall of
the biliary stenosis was compatible with a scleros-
ing cholangitis. The postoperative course was
marked by gastrointestinal bleeding 9 days after
operation. One year after operation, cholestasis
was markedly decreased. The patient died three
years later.
8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 6/15
H. Bismuth et al.: Segmentectomies in Liver Surgery 15
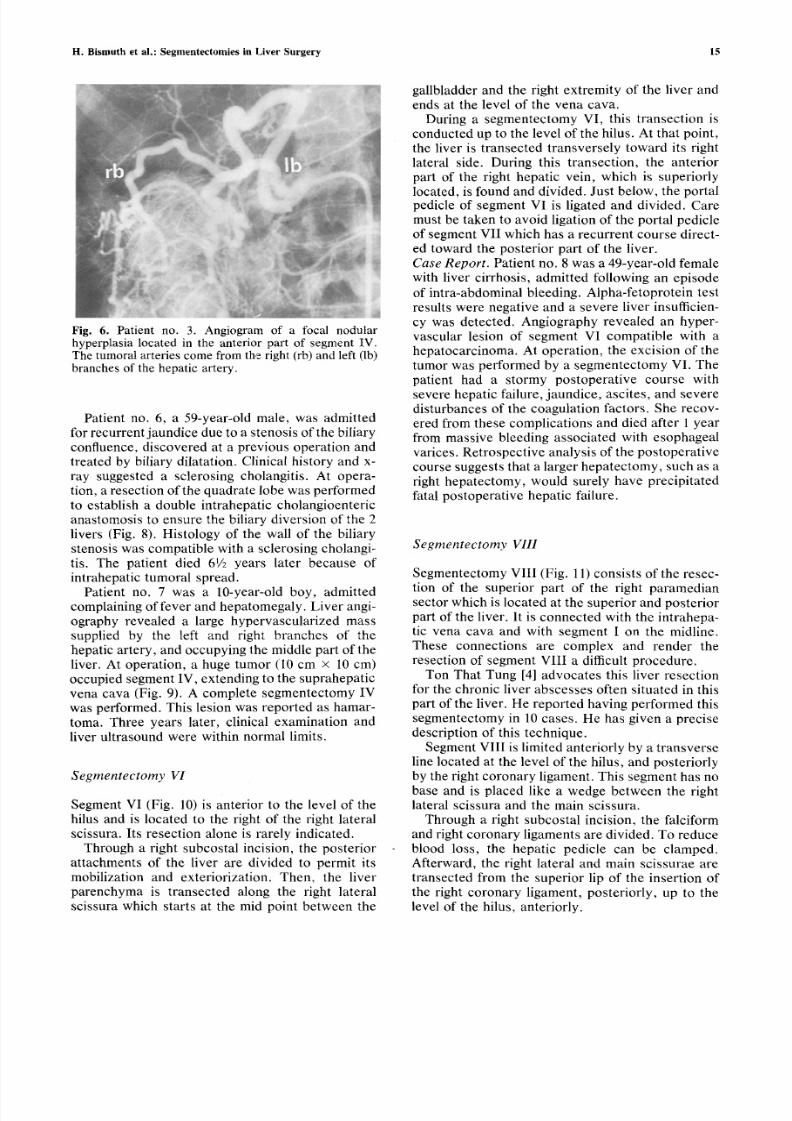
Fig. 6. Patient no. 3. Angiogram of a focal nodularhyperplasia located in the anterior part of segment IV.The tumoral arteries come from the right (rb) and left (lb)
branches of the hepatic artery.
Patient no. 6, a 59-year-old male, was admitted
for recurrent jaundice due to a stenosis of the biliary
confluence, discovered at a previous operation and
treated by biliary dilatation. Clinical history and x-
ray suggested a sclerosing cholangitis. At opera-
tion, a resection of the quadrate lobe was perfor med
to establish a double intrahepatic cholangioenteric
anastomosis to ensure the biliary diversion of the 2
livers (Fig. 8). Histology of the wall of the biliary
stenosis was compatible with a sclerosing cholangi-tis. The patient died 61/2 years later because of
intrahepatic tumoral spread.
Patient no. 7 was a 10-year-old boy, admitted
complaining of fever and h epatomegaly. Liver angi-
ography revealed a large hypervascularized mass
supplied by the left and right branches of the
hepatic artery, and occupying the middle part of the
liver. At operation, a huge tumor (10 cm • I0 cm)occupied segment IV, extending to the suprahepatic
vena cava (Fig. 9). A complete segmentectomy IV
was performed. This lesion was reported as hamar-
toma. Three years later, clinical examination and
liver ultrasound were within normal limits.
Segmentectomy VI
Segment VI (Fig. 10) is anterior to the level of the
hilus and is located to the right of the right lateral
scissura. Its resection alone is rarely indicated.
Through a right subcostal incision, the posterior
attachments of the liver are divided to permit its
mobilization and exteriorization. Then, the liver
parenchyma is transected along the right lateral
scissura which starts at the mid point between the
gallbladder and the right extremity of the liver and
ends at the level of the vena cava.
During a segmentectomy VI, this transection is
conducted up to the level of the hilus. At that point,
the liver is transected transversely toward its right
lateral side. During this transection, the anterior
part of the right hepatic vein, which is superiorlylocated, is found and divided. Just below, the portalpedicle of segment VI is ligated and divided. Care
must be taken to avoid ligation of the portal pedicle
of segment VII which has a recurrent course direct-
ed toward the posterior part of the liver.
Case Report. Patient no. 8 was a 49-year-old female
with liver cirrhosis, admitted following an episode
of intra-abdominal bleeding. Alpha-fetoprotein test
results were negative and a severe liver insufficien-
cy was detected. Angiography revealed an hyper-
vascular lesion of segment VI compatible with a
hepatocarcinoma. At operation, the excision of the
tumor was performed by a segmentectomy VI. Thepatient had a stormy postoperative course with
severe hepatic failure, jaundi ce, ascites, and severe
disturbances of the coagulation factors. She recov-
ered from these complications and died after 1 year
from massive bleeding associated with esophageal
varices. Retrospective analysis of the postoper ative
course suggests that a larger hepatect omy, such as a
right hepatectomy, would surely have precipitated
fatal postoperative hepatic failure.
Segmentectomy VIII
Segmentectomy VIII (Fig. 11) consists of the resec-
tion of the superior part of the right paramedian
sector which is located at the superior and posterior
part of the liver. It is connected with the intrahepa-
tic vena cava and with segment I on the midline.
These connections are complex and render the
resection of segment VIII a difficult procedure.
Ton That Tung [4] advocates this liver resection
for the chronic liver abscesses often situated in this
part of the liver. He reported having performed this
segmentectomy in 10 cases. He has given a precise
description of this technique.Segment VIII is limited anteriorly by a tr ansverse
line located at the level of the hilus, and posteriorly
by the right coronary ligament. This segment has no
base and is placed like a wedge between the right
lateral scissura and the main scissura.
Through a right subcostal incision, the falciform
and right coronary ligaments are divided. To reduce
blood loss, the hepatic pedicle can be clamped.
Afterward, the right lateral and main scissurae are
transected from the superior lip of the insertion of
the right coronary ligament, posteriorly, up to the
level of the hilus, anteriorly.
8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 7/15
16 World J. Surg. Vol. 6, No. 1, January 1982
umbilicalcissure
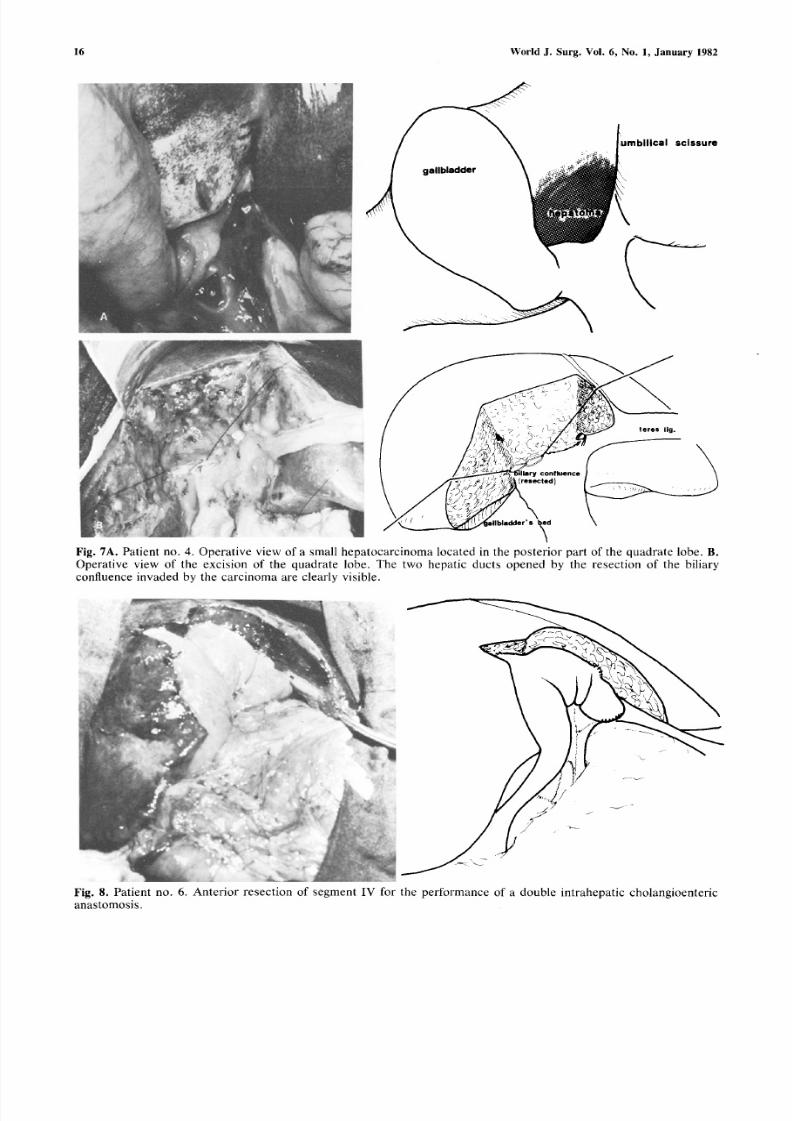
Fig . 7A. Pa t i en t no . 4 . Ope ra t iv e v iew o f a sma l l hepa toca rc ino ma loca ted in the pos te r io r pa r t o f the quadra te lobe . B .Ope ra t ive v iew o f the exc i s ion o f the quadra te lobe . T he two he pa t i c duc t s opene d by the re s e c t ion o f the b i l i a ry
conf luence invaded by the ca rc inoma a re c l ea r ly v i s ib le .
J
Fig . 8 . Pa t i en t no. 6 . An te r io r re s ec t ion o f s egmen t IV fo r the pe r fo rmanc e o f a doub le in t rahepa t i c cho la ng ioen te r i c
anas tomos i s .
8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 8/15
H . Bismuthet a l.: Segmentectomies n Liver Surgery 17
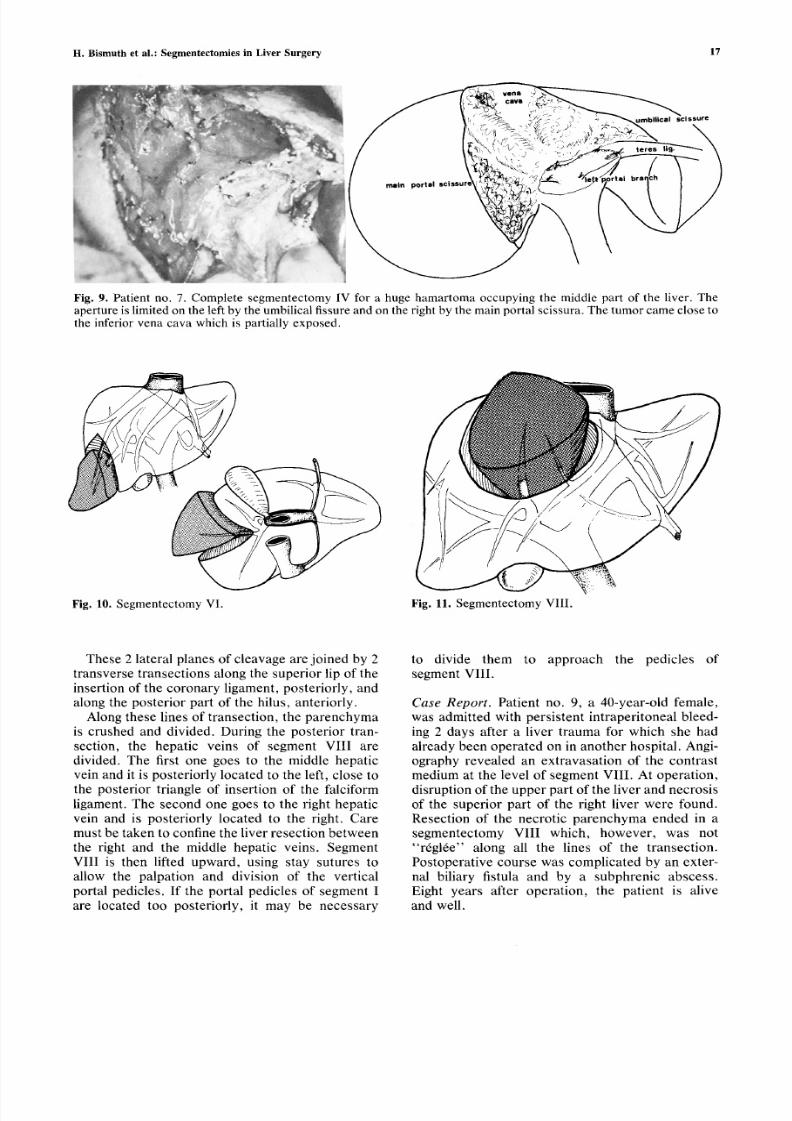
Fig. 9. Patient no. 7. Complete segmentectomy IV for a huge hamartoma occupying the middle part of the liver. Theaperture is limited on the left by the umbilical fissure and on the right by the main portal scissura. The tumor came close tothe inferior vena cava which is partially exposed.
~ b
!~:~:~::::::~:
i : : : : ~ : ~
Fig. 10. Segmentectomy VI. Fig. 11. Segmentectomy VIII.
These 2 lateral planes of cleavage are joined by 2
transverse transections along the superior lip of the
insertion of the coron ary ligament, posteriorly, and
along the posterior part of the hilus, anteriorly.
Along these lines of transection, the par enchy ma
is crushed and divided. During the posterior tran-section, the hepatic veins of segment VIII are
divided. The first one goes to the middle hepatic
vein and it is posteriorly located to the left, close to
the posterior triangle of insertion of the falciform
ligament. The second one goes to the right hepatic
vein and is posteriorly located to the right. Care
must be taken to confine the liver resection betwe en
the right and the middle hepatic veins. Segment
VIII is then lifted upward, using stay sutures to
allow the palpation and division of the vertical
portal pedicles. If the portal pedicles of segment I
are located too posteriorly, it may be necessary
to divide them to approach the pedicles of
segment VIII.
Case Report. Patient no. 9, a 40-year-old female,
was admitted with persistent intraperitoneal bleed-
ing 2 days after a liver trauma for which she hadalready been operated on in an other hospital. Angi-
ography revealed an extravasation of the contrast
medium at the level of segment VIII. At operation,
disruption of the upper part of the liver and necrosis
of the superior part of the right liver were found.
Resection of the necrotic parenchyma ended in a
segmentectomy VIII which, howeve r, was not
"rdglde" along all the lines of the transection.
Postoperative course was complicated by an exter-
nal biliary fistula and by a subphrenic abscess.
Eight years after operation, the patient is alive
and well.
8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 9/15
1 8 W o r l d J . S u r g . V o l . 6 , N o . 1 , J a n u a r y 1 98 2
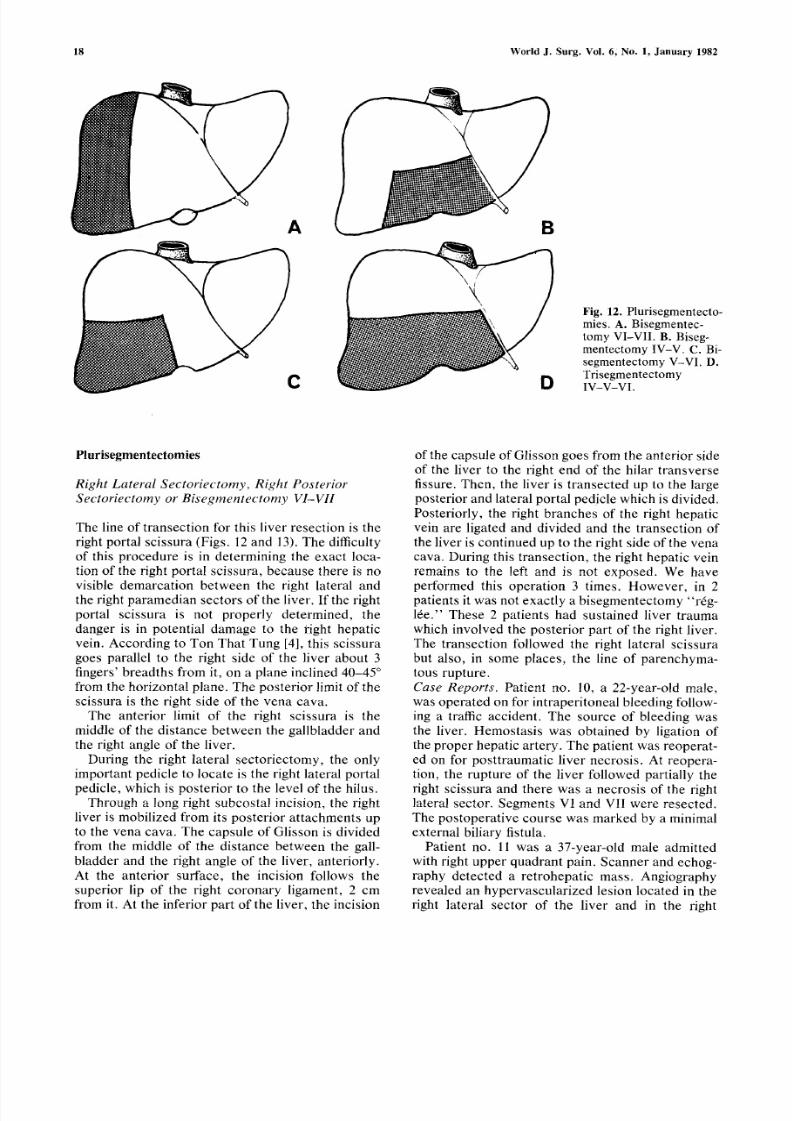
lFig. 12. Plurisegmentecto-mies. A. Bisegmentec-tomy VI-VII. B. Biseg-mentectomy IV-V. C. Bi-
segmentectomy V-VI. D.TrisegmentectomyIV-V-VI.
P l u r i s e g m e n t e c t o m i e s
Right Lateral Sectoriectomy, Right Posterior
Sectoriectomy or Bisegmentectomy V1-VII
The line of transection for this liver resection is the
right portal scissura (Figs. 12 and 13). The difficulty
of this procedure is in determining the exact loca-
tion of the right portal scissura, because there is no
visible demarcation between the right lateral and
the right paramedian sectors of the liver. If the right
portal scissura is not properly determined, the
danger is in potential damage to the right hepatic
vein. According to Ton That Tung [4], this scissura
goes parallel to the right side of the liver about 3
fingers' breadths from it, on a plane inclined 40-45 ~
from the horizontal plane. The posterior limit of the
scissura is the right side of the vena cava.
The anterior limit of the right scissura is the
middle of the distance between the gallbladder andthe right angle of the liver.
During the right lateral sectoriectomy, the only
important pedicle to locate is the right lateral portal
pedicle, which is posterior to the level of the hilus.
Through a long right subcostal incision, the right
liver is mobilized from its posterior attachmen ts up
to the vena cava. The capsule of Glisson is divided
from the middle of the distance between the gall-
bladder and the right angle of the liver, anteriorly.
At the anterior surface, the incision follows the
superior lip of the right coronary ligament, 2 cm
from it. At the inferior part of the liver, the incision
of the capsule of Glisson goes from the anterior side
of the liver to the right end of the hilar transverse
fissure. Then, the liver is transected up to the large
posterior and lateral portal pedicle which is divided.
Posteriorly, the right branches of the right hepatic
vein are ligated and divided and the transection of
the liver is continued up to the right side of the vena
cava. During this transection, the right hepatic vein
remains to the left and is not exposed. We have
performed this operation 3 times. However, in 2
patients it was not exact ly a bisegmente ctomy "r6g-
16e." These 2 patients had sustained liver trauma
which involved the posterior part of the right liver.
The transection followed the right lateral scissura
but also, in some places, the line of parenchyma-
tous rupture.
Case Reports. Patient no. 10, a 22-year-old male,
was operated on for intraperitoneal bleeding follow-
ing a traffic accident. The source of bleeding was
the liver. Hemostasis was obtained by ligation ofthe proper hepatic artery. The patient was reoperat-
ed on for posttraumatic liver necrosis. At reopera-
tion, the rupture of the liver followed partially the
right scissura and there was a necrosis of the right
lateral sector. Segments VI and VII were resected.
The postoperative course was marke d by a minimal
external biliary fistula.
Patient no. 11 was a 37-year-old male admitted
with right upper quadrant pain. Scanner and echog-
raphy detected a retrohepatic mass. Angiography
revealed an hypervascular ized lesion located in the
right lateral sector of the liver and in the right
8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 10/15
H. B i sm uth e t a l . : Se gm e nte c tom i e s i n L i ve r Sur ge r y 19
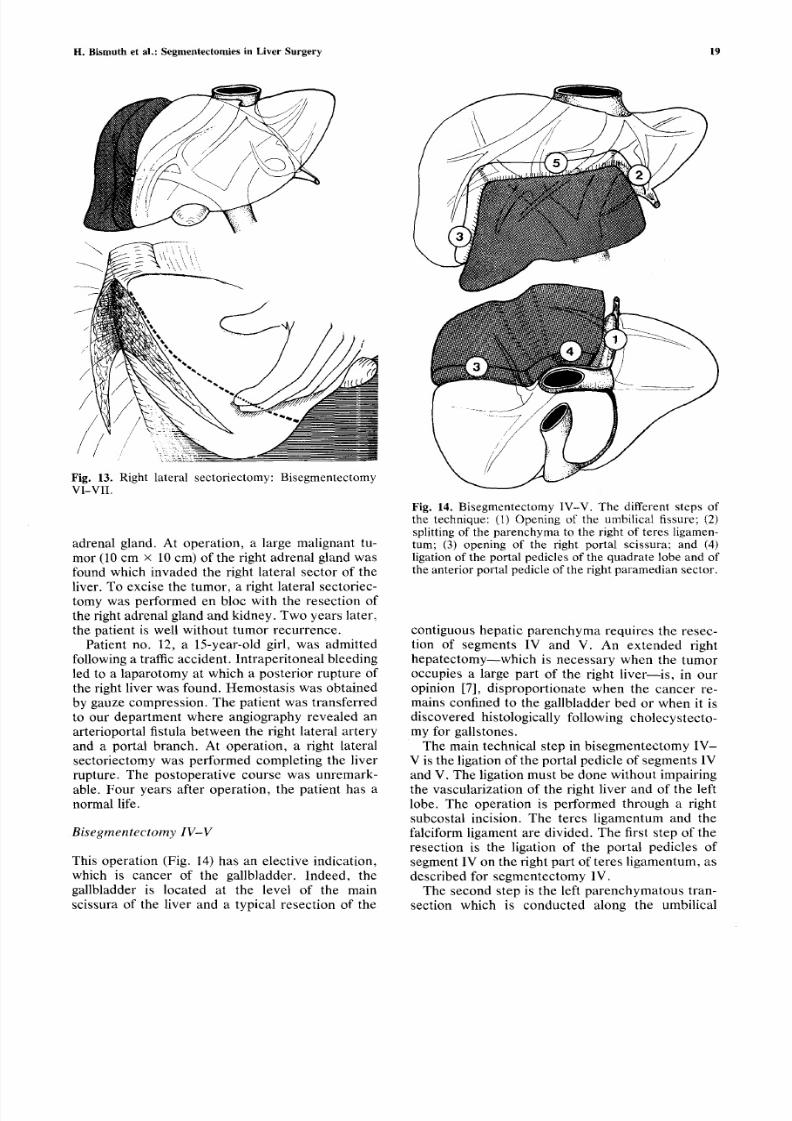
Fig. 13. Right la teral sectoriectomy: BisegrnentectomyV I - V I I .
a d r e n a l g l a n d . A t o p e r a t i o n , a l a rg e m a l i g n a n t t u -
m o r (1 0 c m • 1 0 c m ) o f th e r i g h t a d r e n a l g l a n d w a s
f o u n d w h i c h i n v a d e d t h e r i g h t l at e r al s e c t o r o f t h e
l iv e r . T o e x c i s e t h e t u m o r , a r i g h t l a t e r a l s e c t o r i e c -
t o m y w a s p e r f o r m e d e n b l o c w i t h t h e r e s e c t io n o f
t h e r ig h t a d r e n a l g la n d a n d k i d n e y . T w o y e a r s l a t e r,
t h e p a t i e n t is w e l l w i t h o u t t u m o r r e c u r r e n c e .
P a t i e n t n o . 1 2 , a 1 5 - y e a r - o l d g i r l, w a s a d m i t t e d
f o l l o w i n g a tr a f fi c a c c i d e n t , l n t r a p e r i t o n e a l b l e e d i n g
l e d t o a l a p a r o t o m y a t w h i c h a p o s t e r io r r u p t u r e o f
t h e ri g h t l iv e r w a s f o u n d . H e m o s t a s i s w a s o b t a i n e d
b y g a u z e c o m p r e s s i o n . T h e p a t i e n t w a s t r a n s f e r r e d
t o o u r d e p a r t m e n t w h e r e a n g i o g r a p h y r e v e a l e d a n
a r t e r i o p o r t a l f i s tu l a b e t w e e n t h e r i g h t l a t e r a l a r t e r ya n d a p o r t a l b r a n c h . A t o p e r a t i o n , a r i g h t l a t e r a l
s e c t o r i e c t o m y w a s p e r f o r m e d c o m p l e t i n g th e l i v er
r u p t u r e . T h e p o s t o p e r a t i v e c o u r s e w a s u n r e m a r k -
a b l e . F o u r y e a r s a f t e r o p e r a t i o n , t h e p a t i e n t h a s a
n o r m a l l i f e .
Bisegmentectomy IV-V
T h i s o p e r a t i o n ( F i g . 1 4 ) h a s a n e l e c t i v e i n d i c a t i o n ,
w h i c h i s c a n c e r o f t h e g a l l b l a d d e r . I n d e e d , t h e
g a l l b l a d d e r is l o c a t e d a t t h e l e v e l o f t h e m a i n
s c i s s u r a o f th e l i v e r a n d a t y p i c a l r e s e c t i o n o f t h e
Fig. 14. Bisegrnen tectorny IV-V . T he different s teps ofthe technique: (1) Opening of the umbil ical f issure; (2)spl i t t ing of the parenchyma to the r ight of teres l igamen-turn; (3) opening of the r ight portal scissura; and (4)l iga tion of the por ta l pedic les of the qu adra te lobe and ofthe an te r ior por t a l pedic le of the r ight pa ram edian sec tor .
c o n t i g u o u s h e p a t i c p a r e n c h y m a r e q u i r e s t h e r e s e c -
t io n o f s e g m e n t s I V a n d V . A n e x t e n d e d r i g h t
h e p a t e c t o m y - - w h i c h i s n e c e s s a r y w h e n t h e t u m o r
o c c u p i e s a la r g e p a r t o f t h e r i g h t l i v e r - - i s , i n o u r
o p i n i o n [7 ], d i s p r o p o r t i o n a t e w h e n t h e c a n c e r r e -
m a i n s c o n f i n e d to t h e g a l l b l a d d e r b e d o r w h e n i t is
d i s c o v e r e d h i s to l o g i c a ll y f o ll o w i n g c h o l e c y s t e c t o -
m y f o r g a l l s to n e s .T h e m a i n te c h n i ca l s t ep i n b i s e g m e n t e c t o m y I V -
V i s t h e l i g a t io n o f t h e p o r t a l p e d i c l e o f s e g m e n t s I V
a n d V . T h e l ig a t io n m u s t b e d o n e w i t h o u t i m p a i r i n g
t h e v a s c u l a r i z a t i o n o f t h e r i g h t li v e r a n d o f t h e l e f t
l o b e . T h e o p e r a t i o n i s p e r f o r m e d t h r o u g h a r i g h t
s u b c o s t a l i n c i s i o n . T h e t e r e s l i g a m e n t u m a n d t h e
f a l c i f o r m l i g a m e n t a r e d i v i d e d . T h e f i rs t s te p o f t h e
r e s e c t i o n i s t h e l i g a t io n o f th e p o r t a l p e d i c l e s o f
s e g m e n t I V o n t h e r i g h t p a r t o f t e re s l i g a m e n t u m , a s
d e s cr i be d f o r s e g m e n t e c t o m y I V .
T h e s e c o n d s t e p i s t h e l e ft p a r e n c h y m a t o u s t r a n -
s e c t i o n w h i c h i s c o n d u c t e d a l o n g t h e u m b i l i c a l

8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 11/15
2 0 W o r l d J . S u r g . V o l . 6 , N o . 1 , January 1982
fissure. The third step is the right liver transection,
which is conducted following a line parallel to the
right lateral scis sura 2 cm on its right. At the inferior
part of the liver, this tran section is directed toward
the right portal pedicle. During this transection, the
large inferior and posterior right paramedian portal
pedicle is found and its anterior branch is ligated.The fourth step is the ligation of the portal branches
on the posterior part of the quadrate lobe. The fifth
step is the posterior parenchymatous transection
which joins the left and right transections in front of
the hilus. During this transverse transection, the
large middle hepatic vein is ligated and divided.
Cas e Repor t s . Patient no. 13, a 42-year-old male,
was admitted with right upper quadrant pain. A1-
pha-fetoprotein levels were elevated and angiogra-
phy revealed a small hypervascular lesion (5 cm in
diameter) in segment IV. At operation, a small,
well-circumscribed hepatocarcinoma was located insegment IV, close to segment V. T he left lobe of the
liver was small. Segments IV and V were resected.
The postoperative course was unremarkable and
the patient is alive and well 2 years after operation.
Patient no. 14 was a 39-year-old female operated
on for gallstones. Histological examination of the
gallbladder revealed a carcinoma of the gallbladder
invading the adventitia. The patient was reop erated
on at our hospital and a resection of segments IV
and V was performed. Histological examination of
these 2 segments revealed no sign of malignancy.
Two years after operation, the patient is alive and
well. Biological and morphologic examinations of
the liver are normal.
Patient no. 15, a 57-year-old male, was operated
on for gallstones. Intraoperatively, a carcinoma of
the gallbladder, which extend ed beyond the serosa,
was discovered. This patient was treated by chole-
cystect omy and then transferred to our department.
Angiography revealed some irregularities of the
branches of the right hepatic artery. The patient
was reoperated on and a segmentectomy IV-V was
performed. Histologically, there was some residual
tumoral tissue in the gallbladder bed. The postoper-
ative course was uncomplicated. Two years afteroperation, the patient died with a tumor recurrenceinvading the duodenum .
Patient no. 16, a 29-year-old female, was operat-
ed on for right upper qu adrant pain associated with
an absence of opacification of the gallbladder. At
operation, a carc inoma of the gallbladder, invading
the gallbladder bed, was found and a chol ecystecto-
my was performed. Postoperatively, the patient
was transferred to our departmen t. The patient was
reoperated on and a bisegmentectom y IV-V was
performed. Histology revealed a tumoral extension
limited to the gallbladder bed. The postoperative
course was uncomplicated and the patient is alive
and well after 2 years. Recently, a second-look
operation was performed which did not disclose any
tumoral recurrence.
Patient no. 17, a 60-year-old female, unde rwen t a
cholecystectomy for gallstones. Histology of the
gallbladder revealed a carcinoma confined to thegallbladder. For this reason, the patient was trans-
ferred to our department. Angiography of the liver
was normal. The patient was reoperated on and a
bisegmentectomy IV-V was performed. Histology
revealed no sign of tumoral extension in the 2
resected segments. The postoperative course was
uncomplicated and the patient is alive and well 2
years after operation.
Patient no. 18, a 71-year-old male, was admitted
to our department for right upper quadrant pain.
Liver scintiscan revealed a defect in the right liver.
Angiography showed an hypervascular lesion locat-
ed at the level of the gallbladder bed. At operation,the mass was removed by performing a bisegmen-
tectomy IV-V. Histology revealed a small carcino-
ma of the gallbladder penetrating into the liver. The
postoperative course was uncomplicated and the
patient is alive and well 10 months after operation,
with no sign of tumor recurrence.
B i s e g m e n t e c t o m y V - V I
Proposed by Mancuso et al. [8], this bisegmentec-tomy is rarely performed (Fig. 15).
Just as in resection of the quadrate lobe, a
cholecyst ectomy is performed and the liver is tran-
sected along the main scissura. Contrary to what is
done during the resection of the quadr ate lobe, the
incision of the capsule of Glisson should be slightly
displaced to the right of the main scissura to avoid
the middle hepatic vein during the transection. The
transection is conducted up to the level of the hilus,
and then the liver is transected transversely toward
its right lateral side. This transection is no different
from that described for bisegmente ctomy IV-V and
for segment ectomy VI.
Cas e Repor t s . Patient no. 19 was a 2-year-oldfemale admitted to our department with hepatomeg-
aly. Angiography revealed a huge hypervascular
tumor of the right liver. The lesion, which was a
capsulated hamartoma, was resected by performing
a bisegmentectomy V-VI. The postoperative course
was uneventful and the patient is alive and well 4years later.
Patient no. 20, a 58-year-old male, was admittedfor right upper quadrant pain and hepatomegaly.
Angiography revealed an hypervascularized lesion
located inside the right part of the liver. At opera-
tion, the liver was cirrhotic and the tumor proved to
8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 12/15
H. Bismuth et al.: Segmentectomies in Liver Surgery 21
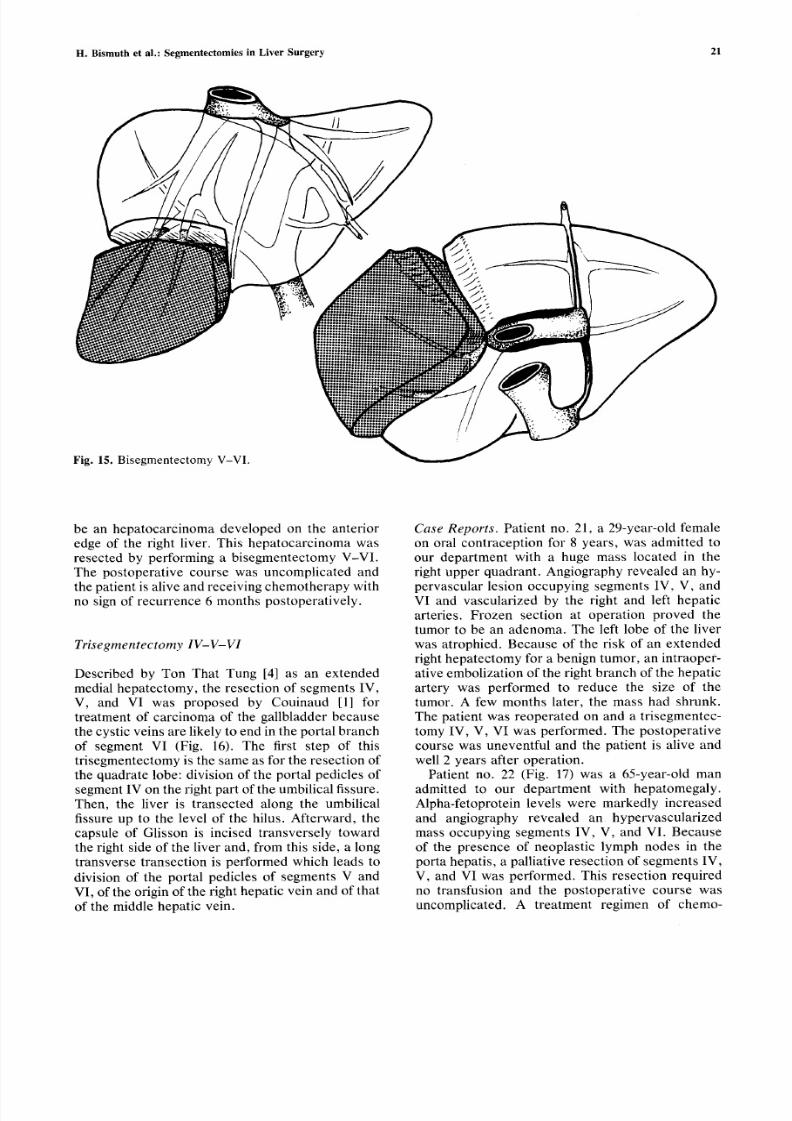
F i g . 1 5 . B i s e g m e n t e c t o m y V - V I .
J .
U lii! Iii" " ' ,
be an hepatocarcinoma developed on the anterior
edge of the right liver. This hepatocarcinoma was
resected by performing a bisegmentectomy V-VI.
The postoperative course was uncomplicated and
the patient is alive and receiving chemo therap y with
no sign of recurrence 6 months postoperatively.
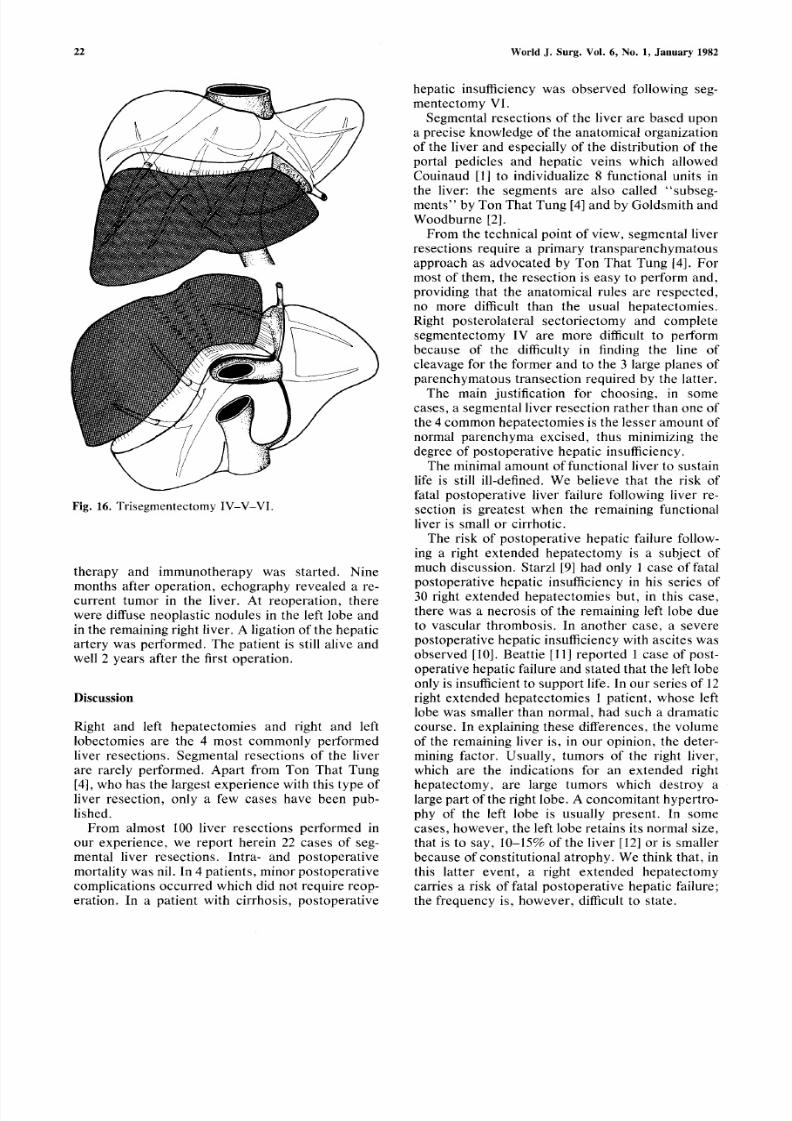
T r i s e g m e n t e c t o m y I V - V - V I
Described by Ton That Tung [4] as an extended
medial hepatectom y, the resection o f segments IV,
V, and VI was proposed by Couinaud [1] for
treatment of carcinoma of the gallbladder because
the cystic veins are likely to end in the portal b ranchof segment VI (Fig. 16). The first step of this
trisegmentectomy is the same as for the resection of
the quadrate lobe: division of the portal pedicles of
segment IV on the right part o f the umbilical fissure.
Then, the liver is transected along the umbilical
fissure up to the level of the hilus. Afterward, the
capsule of Glisson is incised transversely toward
the right side of the liver and, from this side, a long
transverse transection is performed which leads to
division of the portal pedicles of segments V and
VI, of the origin of the right hepatic vein and of that
of the middle hepatic vein.
Cas e Repor t s . Patient no. 21, a 29-year-old female
on oral contraception for 8 years, was admitted to
our department with a huge mass located in the
right upper quadrant. Angiography revealed an hy-
pervascular lesion occupying segments IV, V, and
VI and vascularized by the right and left hepatic
arteries. Frozen section at operation proved the
tumor to be an adenoma. The left lobe of the liver
was atrophied. Because of the risk of an extended
right hepate ctomy for a benign tumor , an intraopex'-
ative embolization of the right branch of the hepatic
artery was performed to reduce the size of the
tumor. A few months later, the mass had shrunk.
The patient was reoperated on and a trisegmentec-
tomy IV, V, VI was performed. The postoperativecourse was uneventful and the patient is alive and
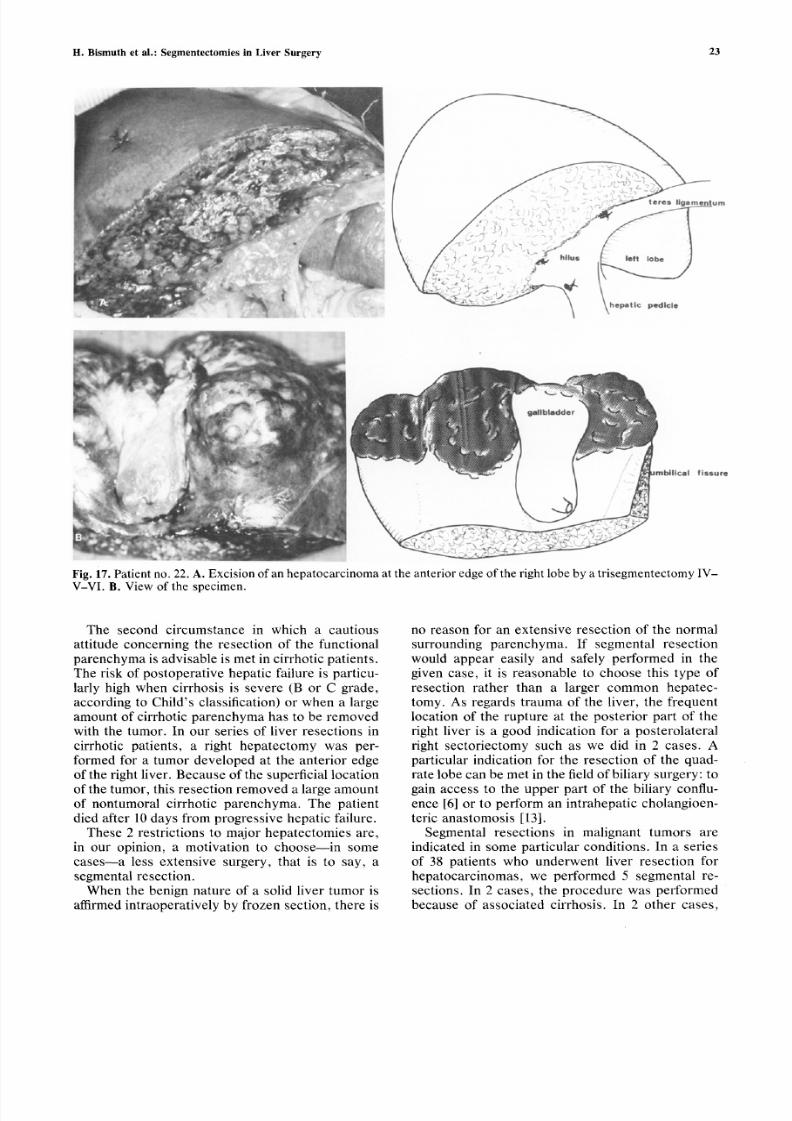
well 2 years after operation.Patient no. 22 (Fig. 17) was a 65-year-old man
admitted to our department with hepatomegaly.
Alpha-fetoprotein levels were markedly increased
and angiography revealed an hypervascularized
mass occupying segments IV, V, and VI. Because
of the presence of neoplastic lymph nodes in the
porta hepatis, a palliative resection of segments IV,
V, and VI was performed. This resection required
no transfusion and the postoperative course was
uncomplicated. A treatment regimen of chemo-
8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 13/15
2 2 W o r l d J . S u r g . V o l . 6 , N o . 1 , J a n u a r y 1 9 82
Fig. 16. Trisegmentectomy IV-V-VI.
therapy and immunotherapy was started. Nine
months after operation, echography revealed a re-
current tumor in the liver. At reoperation, there
were diffuse neoplastic nodules in the left lobe and
in the remaining right liver. A ligation of the hepatic
artery was performed. The patient is still alive and
well 2 years after the first operation.
Discuss ion
Right and left hepatectomies and right and left
lobectomies are the 4 most commonly performed
liver resections. Segmental resections of the liver
are rarely performed. Apart from Ton That Tung
[4], who has the largest experience with this type of
liver resection, only a few cases have been pub-
lished.
From almost 100 liver resections performed in
our experience, we report herein 22 cases of seg-
mental liver resections. Intra- and postoperative
mortality was nil. In 4 patients, minor po stoperative
complications occurred which did not require reop-
eration. In a patient with cirrhosis, postoperative
hepatic insufficiency was observed following seg-
mentectomy VI.
Segmental resections of the liver are based upon
a precise knowledge of the anatomical organization
of the liver and especially of the distribution of the
portal pedicles and hepatic veins which allowed
Couinaud [1] to individualize 8 functional units in
the liver: the segments are also called "subseg-
merits" by Ton That Tung [4] and by Goldsmith and
Woodburne [2].
From the technical point of view, segmental liver
resections require a primary transparenchymatous
approach as advocated by Ton That Tung [4]. For
most of them, the resection is easy to perform and,
providing that the anatomical rules are respected,
no more difficult than the usual hepatectomies.
Right posterolateral sectoriectomy and complete
segmentectomy IV are more difficult to perform
because of the difficulty in finding the line of
cleavage for the former and to the 3 large planes ofparenchymatous transection required by the latter.
The main justification for choosing, in some
cases, a segmental liver resection rather than one of
the 4 common hepatectomies is the lesser amount of
normal parenchyma excised, thus minimizing the
degree of postoperative hepatic insufficiency.
The minimal amount of functional liver to sustain
life is still ill-defined. We believe that the risk of
fatal postoperative liver failure following fiver re-
section is greatest when the remaining functional
liver is small or cirrhotic.
The risk of postoperative hepatic failure follow-
ing a right extended hepatectomy is a subject ofmuch discussion. Starzl [9] had only 1 case o f fatal
postopera tive hepatic insufficiency in his series of
30 right extended hepatectomies but, in this case,
there was a necrosis of the remaining left lobe due
to vascular thrombosis. In another case, a severe
postoperative hepatic insufficiency with ascites was
observed [10]. Beattie [I 1] reported 1 case of post-
operative hepatic failure and st ated tha t the left lobe
only is insufficient to support life. In our series of 12
right extended hepatectomies 1 patient, whose left
lobe was smaller than normal, had such a dramatic
course. In explaining these differences, the volume
of the remaining liver is, in our opinion, the deter-
mining factor. Usually, tumors of the right liver,
which are the indications for an extended right
hepatectomy, are large tumors which destroy a
large part o f the right lobe. A conc omitant hypertro-
phy of the left lobe is usually present. In some
cases, however, the left lobe retains its normal size,
that is to say, 10-15% of the liver [12] or is smaller
because o f constitutional atrophy. We think that, in
this latter event, a right extended hepatectomy
carries a risk of fatal postoperative hepatic failure;
the frequency is, however, difficult to state.
8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 14/15
H. Bismuth et al.: Segmentectomies in Liver Surgery 23
Fig. 17. Patient no. 22. A. Excision of an hepato carc inom a at the anter ior edge of the right lobe by a trisegm entec tomy IV -V-V I. B. View of the specimen.
T h e s eco n d c i r cu m s t an ce i n w h i ch a cau t i o u s
a t t i tu d e co n c e rn i n g t h e r e s ec t i o n o f t h e fu n c t i o n a l
p a r en ch y m a i s ad v i s ab l e i s m e t i n c i r rh o t i c p a t i en t s .
T h e r i s k o f p o s t o p e ra t i v e h ep a t i c f a i l u r e i s p a r t i cu -
l a r l y h i g h w h en c i r rh o s i s i s s ev e re (B o r C g rad e ,
acco rd i n g t o Ch i l d ' s c l a s s i f i ca t i o n ) o r w h en a l a rg e
a m o u n t o f c ir r h o ti c p a r e n c h y m a h a s t o b e r e m o v e d
w i t h t h e t u m o r . I n o u r s e r i e s o f l i v e r r e s ec t i o n s i nc i r rh o t i c p a t i en t s , a r i g h t h ep a t ec t o m y w as p e r -
f o r m e d f o r a t u m o r d e v e l o p e d a t t h e a n t e r i o r e d g e
o f th e r i g h t l iv e r . B ecau s e o f t h e s u p e r f i c ia l l o ca t i o n
o f t h e t u m o r , t h i s r e s ec t i o n r em o v e d a la rg e am o u n t
o f n o n t u m o r a l c i r r h o ti c p a r e n c h y m a . T h e p a t i e n t
d i ed a l t e r 1 0 d ay s f ro m p ro g r es s i v e h ep a t i c f a i l u r e .
T h es e 2 r e s t r i c t i o n s t o m a j o r h ep a t ec t o m i es a r e ,
i n o u r o p i n i o n , a m o t i v a t i o n t o ch o o s e - - i n s o m e
cas es - - a l e s s ex t en s i v e s u rg e ry , t h a t i s t o s ay , a
s eg m en t a l r e s ec t i o n .
Wh en t h e b en i g n n a t u re o f a s ol i d li v e r t u m o r i s
a f f irm ed i n t r ao p e ra t i v e l y b y f ro ze n s ec t i o n , t h e re i s
n o r e a s o n f o r a n e x t e n s i v e r e s e c t i o n o f t h e n o r m a l
s u r r ou n d i n g p a r e n c h y m a . I f se g m e n t a l r e s e c t i o n
w o u l d ap p ea r ea s i l y an d s a f e l y p e r fo rm ed i n t h e
g i v en cas e , i t i s r ea s o n ab l e t o ch o o s e t h i s t y p e o f
r e s e c t i o n r a t h e r t h a n a l a r g e r c o m m o n h e p a t e c -
t o m y . A s r eg a rd s t r au m a o f t h e l i ve r , t h e f r eq u en t
l o ca t i o n o f t h e ru p t u r e a t t h e p o s t e r i o r p a r t o f t h e
r i g h t l i v e r i s a g o o d i n d i ca t i o n fo r a p o s t e ro l a t e r a lr i g h t s ec t o r i ec t o m y s u ch a s w e d i d i n 2 ca s es . A
p a r t i cu l a r i n d i ca t i o n fo r t h e r e s e c t i o n o f t h e q u ad -
ra te lobe can be m et in the f ie ld o f b i li ary surg ery : to
g a i n acces s t o t h e u p p e r p a r t o f th e b i l i a ry co n f lu -
en ce [6 ] o r t o p e r fo rm an i n t r ah ep a t i c ch o l an g i o en -
ter ic ana s tom os is [13] .
Seg m en t a l r e s ec t i o n s i n m a l i g n an t t u m o rs a r e
i n d i ca t ed i n s o m e p a r t i cu l a r co n d i t i o n s . I n a s e r i e s
o f 38 p a ti e n ts w h o u n d e r w e n t l i v er r e s e c t i o n f o r
h e p a t o c a r c i n o m a s , w e p e r f o r m e d 5 s e g m e n t a l r e -
s ec t i o n s . I n 2 ca s es , t h e p ro ced u re w as p e r fo rm ed
b ecau s e o f a s s o c i a t ed c i r rh o s i s , i n 2 o t h e r ca s es ,

8/3/2019 Reglas de Hepatectomias
http://slidepdf.com/reader/full/reglas-de-hepatectomias 15/15
2 4 W o r l d J . S u r g . V o l . 6 , N o . 1 , J a n u a r y 1 9 8 2
t h e h e p a t o c a r c i n o m a w a s s m a l l a n d l o c a t e d i n t h e
q u a d r a t e l o b e , e q u i d i s t a n t f r o m t h e m a i n s c i s s u r a
a n d t h e u m b i l i c a l f i s s u r e . F r o m t h e c a r c i n o l o g i c a l
p o i n t o f v ie w , a r i gh t e x t e n d e d h e p a t e c t o m y o r a
l ef t h e p a t e c t o m y h a s n o a d v a n t a g e w h e n c o m p a r e d
t o a s e g m e n t e c t o m y I V w h i c h f o l l o w s t h e s a m e
s c i s s u r a e . I n t h e l a s t c a s e , t h e r e s e c t i o n w a s p a l l ia -
t i v e .
A n o t h e r i n d i c a t i o n f o r s e g m e n t a l l i v e r r e s e c t io n
is c a r c i n o m a o f th e g a l l b l a d d e r w h e n m a l i g n a n c y i s
d i s c o v e r e d b y h i s t o l o g i c a l e x a m i n a t i o n o f a ga l l-
b l a d d e r s p e c i m e n r e m o v e d f o r g a l l s to n e s . I f h i st o l o-
g y r ev e a l s t h at t h e c a r c i n o m a h a s e x t e n d e d b e y o n d
t h e w a l l o f t h e g a l l b l a d d e r , w e t h i n k t h a t t h e r e i s a n
i n d i ca t io n f o r a c o m p l e m e n t a r y l i v er r e s e c t io n . T h i s
r e s e c t i o n s h o u l d r e m o v e t h e c o n t i g u o u s l i v e r p a r e n -
c h y m a : s e g m e n t s I V a n d V . T h e r i g h t e x t e n d e d
h e p a t e c t o m y , w h i c h i s o f t e n p r o p o s e d , is in o u r
o p i n i o n d i s p r o p o r t i o n a t e [7 ] s i n c e i t r e m o v e s a n
a l m o s t e n t i r e l y n o r m a l r i g h t l o b e . T h r e e o f o u rp a t i e n t s o p e r a t e d o n b y a b i s e g m e n t e c t o m y I V - V
a f t e r h i s to l o g ic a l d i s c o v e r y o f a c a r c i n o m a o f t h e
g a l l b l a d d e r a r e p r e s e n t l y a l i v e a f t e r m o r e t h a n 2
y e a r s w i t h n o s ig n o f t u m o r r e c u r r e n c e .
I n c o n c l u s io n , m a j o r a n d m i n o r h e p a t i c s e g m e n -
t e c t o m i e s " r d g l d e s " a r e o n e o f t h e b e s t i ll u s t r a ti o n s
o f th e a n a t o m i c a l s u r g e r y o f t h e l iv e r . T h e y a r e n o t
t e c h n i q u e s " d e f a c i l i t6 " w h i c h c a n b e c h o s e n f o r a
r a p i d a n d e x p e d i t i o u s s u r g e r y . T h e y a r e i n t e r e s t i n g
a l t e r n a t i v e s t o t h e c o m m o n h e p a t e c t o m i e s w h e n a
m o r e e c o n o m i c a l r e s e c t i o n i s p e r m i t t e d b y t h e
l o c a ti o n a n d t h e n a t u r e o f th e l e s i o n , o r w h e n a
m a j o r h e p a t e c t o m y i s l ik e l y to e x p o s e t h e p a t i en t t ot h e r is k o f p o s t o p e r a t i v e h e p a t i c f a i l u r e .
R~sum~
L ' i n d i v id u a l i s a t io n d u s e g m e n t c o m m e u n i t6 a n a t o -
m i q u e f o n c t i o n n e l l e h 6 p a t i q u e p e r m e t l a r 6 a l is a t io n
d e s e g m e n t e c t o m i e s . E l l e s s o n t r d g l d e s p a r c e q u e
l e s p l a n s d e s e c t i o n d u p a r e n c h y m e h ~ p a t i q u e s u i -
v e n t d es s c i s s u r es a n a t o m i q u e s . D u p o i n t d e v u e
t e c h n i q u e , l e s s e g m e n t e c t o m i e s h 6 p a t i q u e s s e c a r -
a c t d r is e n t p a r u n a b o r d t r a n s p a r e n c h y m a t e u x e x -c l u s i f d e s p d d i c u l e s v a s c u l a i r e s . N o u s a v o n s r d a l is 6
c e t y p e d ' i n t e r v e n t i o n c h e z 2 2 m a l a d e s s a n s m o r t a l -
i t 6 . L e s i n d i c a t i o n s p r i n c i p a l e s s o n t : ( 1 ) q u e l q u e s
t u m e u r s b d n i g n e s , ( 2) c e r t a i n s t r a u m a t i s m e s d u
f o i e , ( 3 ) l a c h i r u r g i e b i l i a i r e s u s - h i l a i r e o i l u n e
r d s e c t i o n d e l a p a r t i e a n t 6 r i e u r e d u s e g m e n t I V p e u t
~ t r e n d c e s s a i r e , e t ( 4 ) l e c a n c e r v d s i c u l a i r e l o r s q u ' i l
a ~t~ d d c o u v e r t s u r u n e p i 6 c e d e c h o l e c y s t e c t o m i e .
L e s s e g m e n t e c t o m i e s h 6 p a t i q u e s p e u v e n t f i tr e i nd i-
q u 6 e s 6 g a l e m e n t d a n s c e r t a i n e s t u m e u r s m a l i g n e s
l o r s q u e le f o ie e s t c i r r h o t i q u e o u l o r s q u ' u n e e x 6 r 6 s e
6 1 ar gi e f a i t c o u r i r u n r i s q u e d ' i n s u f f i s a n c e h 6 p a -
t iq u e . L ' u n d e s a v a n t a g e s p r i n c i p a u x d e s r d s e c t i o n s
s e g m e n t a i r e s d u f o i e e s t e n e f f e t d e p e r m e t t r e u n e
e x d r ~ s e 6 c o n o m i q u e d u p a r e n c h y m e h d p a t i q u e .
References
1 . Cou inaud , C . : Le Fo ie . E tudes A na tomiques e t Ch i r-urgica les. Par is , Masson, 1957
2 . Go ldsmi th , N .A. , Woodburne , R .T . : The su rg i ca lana tom y pe r t a in ing t o l i ve r r e sec t i on . Surg . G yneco l .Obste t . 195:310, 1957
3 . Hea l ey , J .E . , Schroy , P .C . : Ana to my o f t he b il i aryducts wi thin the human l iver . Arch. Surg. 66:599,1953
4 . Ton Tha t Tung : Les Rdsec t i ons Ma jeure s e t Min-eures du Foie . Par is , Masson, 1979
5. Caprio , G. : Un caso de ext i rpacion del Iobulo iz -quierdo del higado. Bul l . Soc . Cir . Urug. Montevideo2:159, 1931
6. Cham peau, M ., Pineau, P. : V oie d 'abord 61argiet rans-hdpat ique du canal hdpat ique gauche. Mere .Acad. Chir. 90:602, 1964
7. Bism uth, H. , Mal t , R. : Carc in om a of the bi lia ry t rac t .N. Engl . J . Med. 301:704, 1979
8 . Mancu so , M. , Na ta l i n i, E . , De l Grande , G. : Con t r i b -uto a l la conoscenza del la s t rut tura segmentar ia de lfegato in rapporto a l problema del la resez ione epat i -ca. Policlinico. Sez. Chir. 72:1955
9. Starz l , T .E . , K oep , L .J . , Wei ll , R. , I I I , Li l ly , J .R. ,Pu tnam, C .W. , Ald re t e , J .A . : R igh t t r i segmentec -tomy fo r hepa t ic neop la sms . Surg . Gyn eco l . Obs t e t .150:208, 1980
10 . S t a rz l , T .E . , Pu tnam, C .W. , Gro th , C .G. , Corman ,J .L . , Taubm an , J . : Alopec i a , a sc it e s , and i ncomple t eregene ra t i on a f t e r 85 t o 90 pe r cen t l i ve r r e sec t i on .Am. J . Surg. 129:587, 1975
11. Beat t ie , E .G. : Discussion in McBride , C.M., Wal-lace , C. : C ance r of the r ight lobe o f the l iver . Ava r i e ty o f ope ra t i ve p rocedure s . A rch . Surg . 105:289,
1972
12. S tone , H.H . , Lo ng , W.D. , S mi th , R .B . , Hayn es ,C .D. : Phys io log i ca l cons ide ra t i ons i n m a jo r hepa t icre sec t i ons . Am. J . Surg . 117:78, 1969
13. Bismuth, H. , Corle t te , M.B.: Int ra-hepat ic cholan-g io -en t er i c anas tomos i s i n ca rc inom a o f t he h il us o fthe l iver . Surg. Gynecol . Obste t . 140:170, 1975