Embed Size (px)
Citation preview
Registries for clinical research
Stefan James Professor of Cardiology Uppsala Clinical Research Centre Uppsala University Uppsala, Sweden
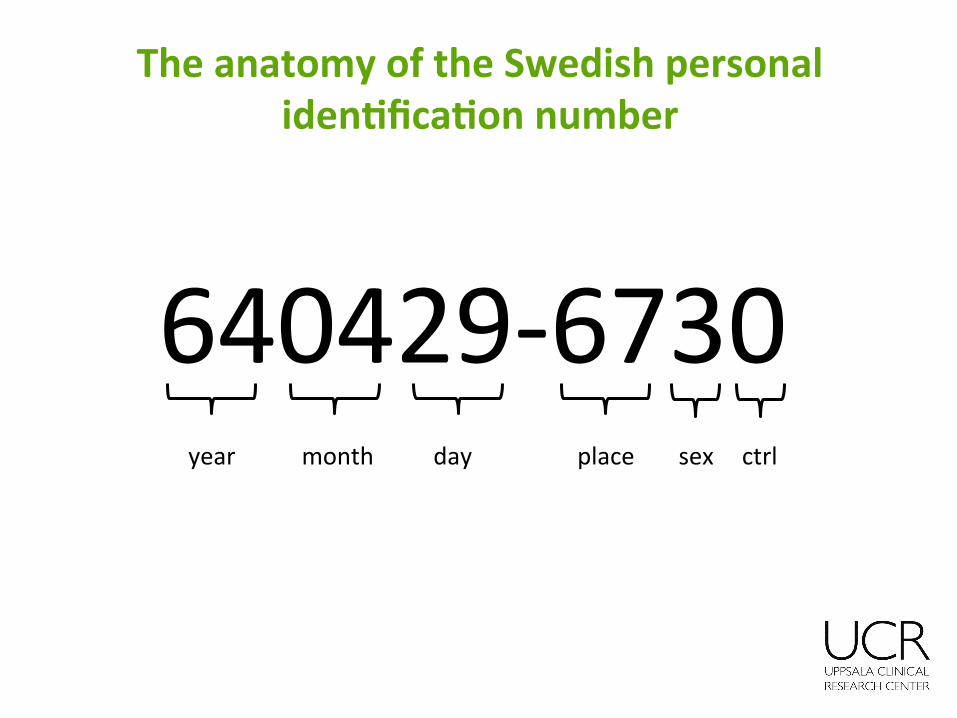
The anatomy of the Swedish personal iden4fica4on number
640429-‐6730 year month day place sex ctrl
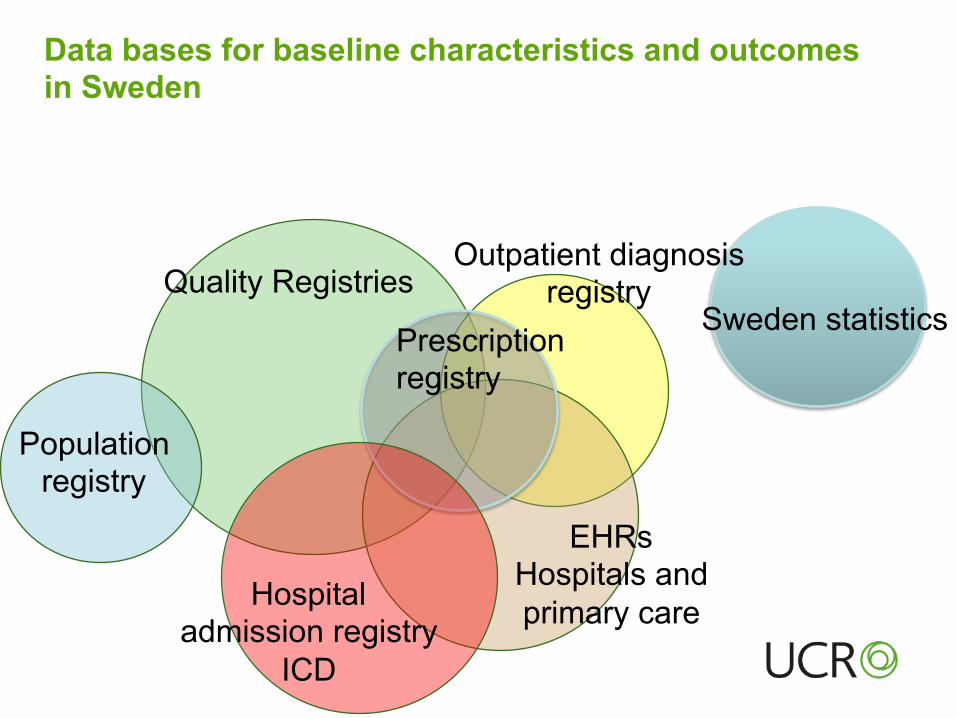
Quality Registries
EHRs Hospitals and primary care
Sweden statistics Prescription registry
Data bases for baseline characteristics and outcomes in Sweden
Hospital admission registry
ICD
Population registry
Outpatient diagnosis registry
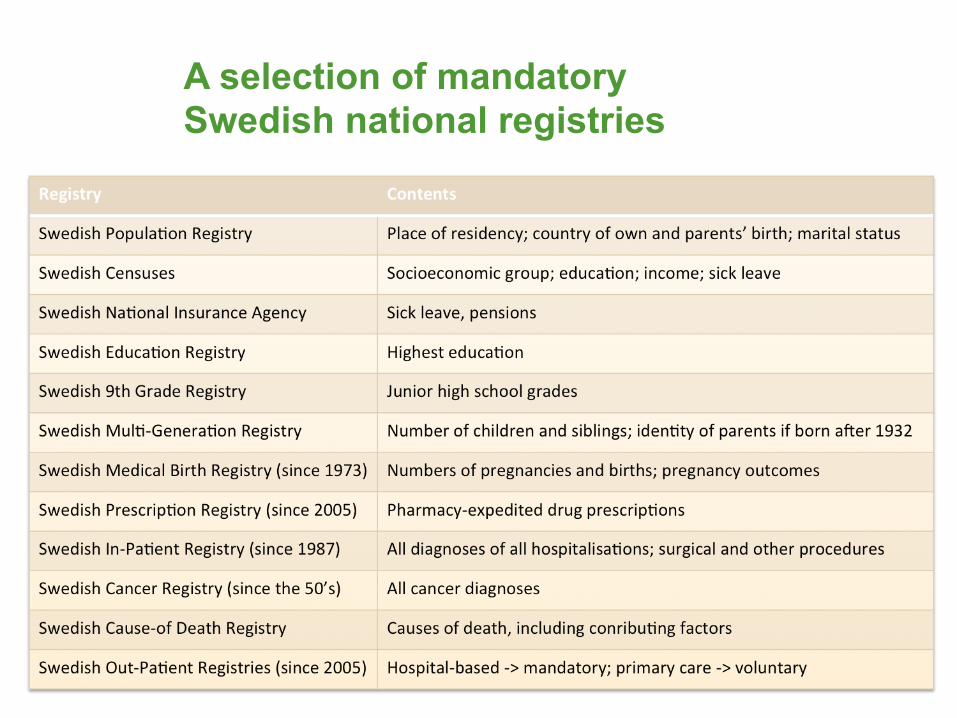
A selection of mandatory Swedish national registries
Olika typer av kvalitetsregister • ”Interventionsregister”, ex höftledsop
• ”Diagnos - vårdepisodsregister”, ex hjärtinfarkt
• ”Diagnos – långtidsregister”, ex diabetes
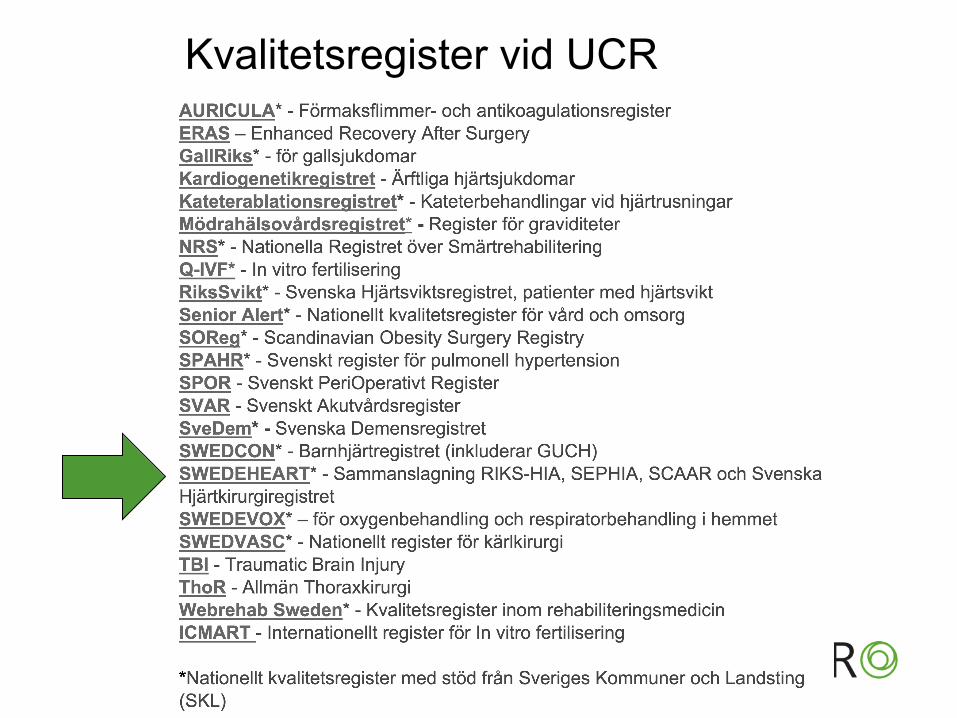
Kvalitetsregister vid UCR
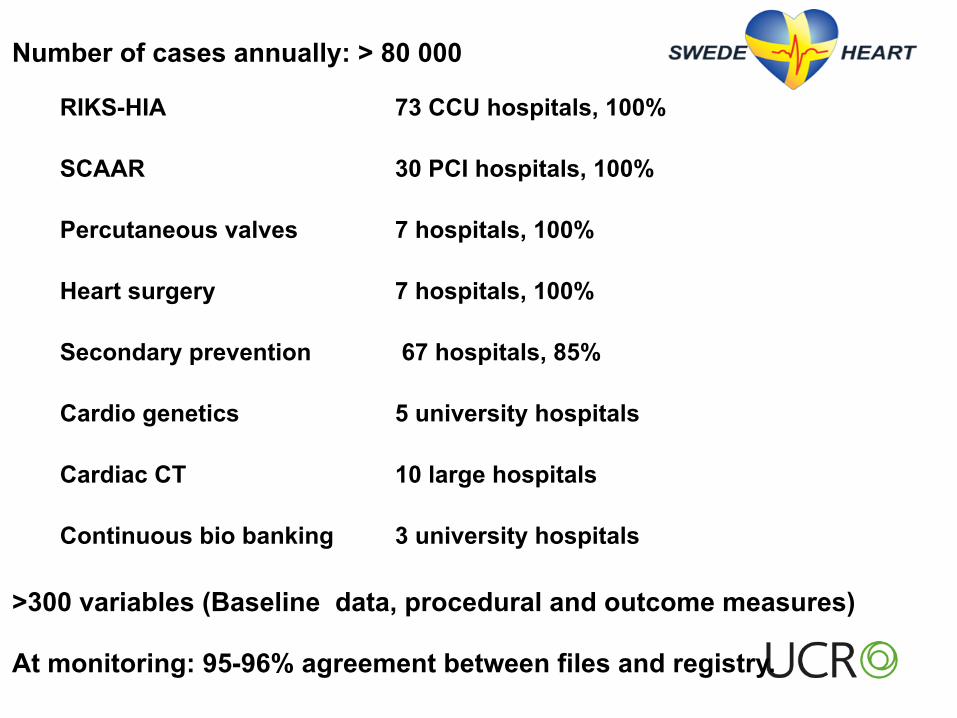
Number of cases annually: > 80 000
RIKS-HIA 73 CCU hospitals, 100%
SCAAR 30 PCI hospitals, 100%
Percutaneous valves 7 hospitals, 100%
Heart surgery 7 hospitals, 100%
Secondary prevention 67 hospitals, 85%
Cardio genetics 5 university hospitals
Cardiac CT 10 large hospitals
Continuous bio banking 3 university hospitals
>300 variables (Baseline data, procedural and outcome measures)
At monitoring: 95-96% agreement between files and registry.
Keys for success
• Simple registration process
• The users are highly motivated • The users have direct use of the system-
to print study reports and stats
• SCAAR is not just a registry - provides clinical information.
• Flexibility, the users can influence the contents and create own variables
• Merging with other registries
SWEDE HEART
Data entry on line by the operator
Automatic linkage with population registry to provide name, sex
Automated data checks
Clinical background and prior CV disease
Angiographic background data
Administrative data
Name, personal ID number
Refered from
Date of procedure Type of registration
Office /call service Local hospital
Body length
Body length (cm)
S-creatinine (ug/L
Creatinine clearance (ml/min) Prior PCI Prior CABG
Diabetes Smoking
Auto populated fields from previous registrations
Calculated variables
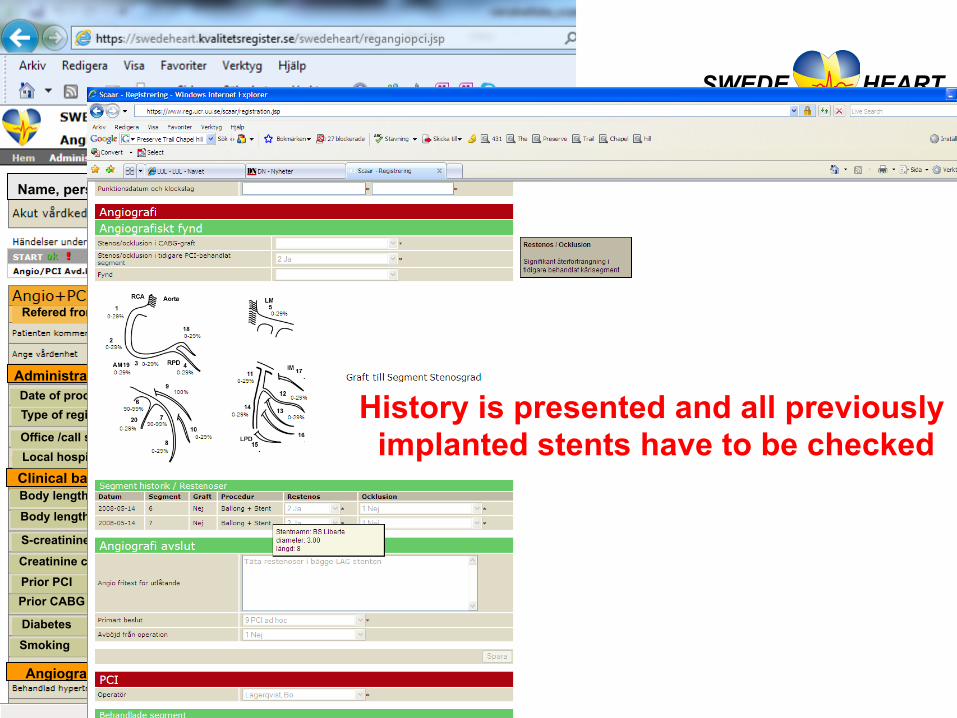
History is presented and all previously implanted stents have to be checked
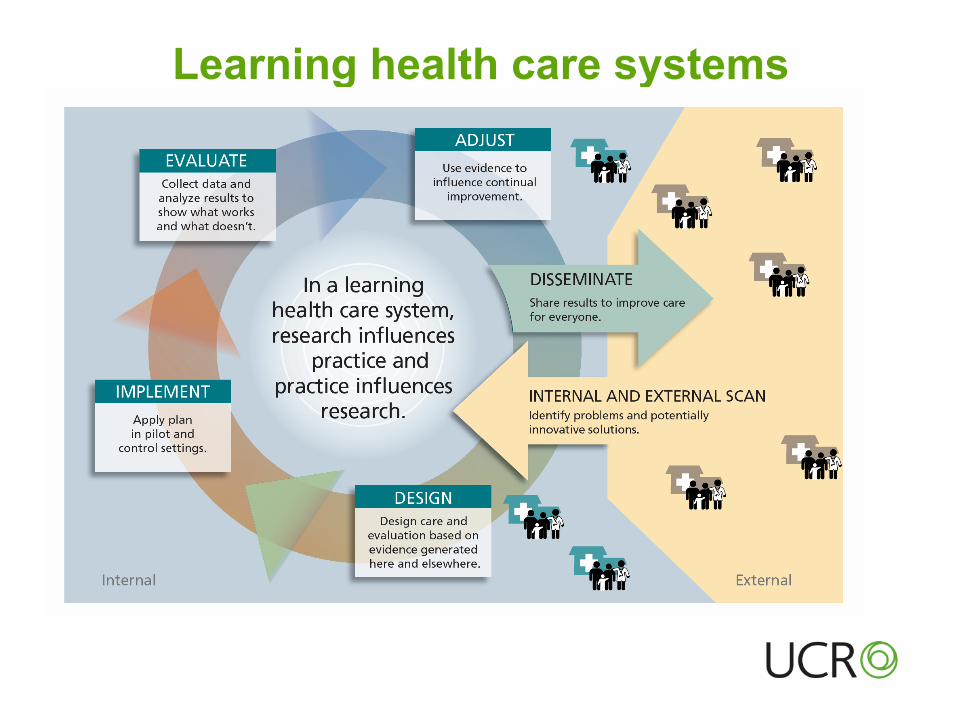
Learning health care systems
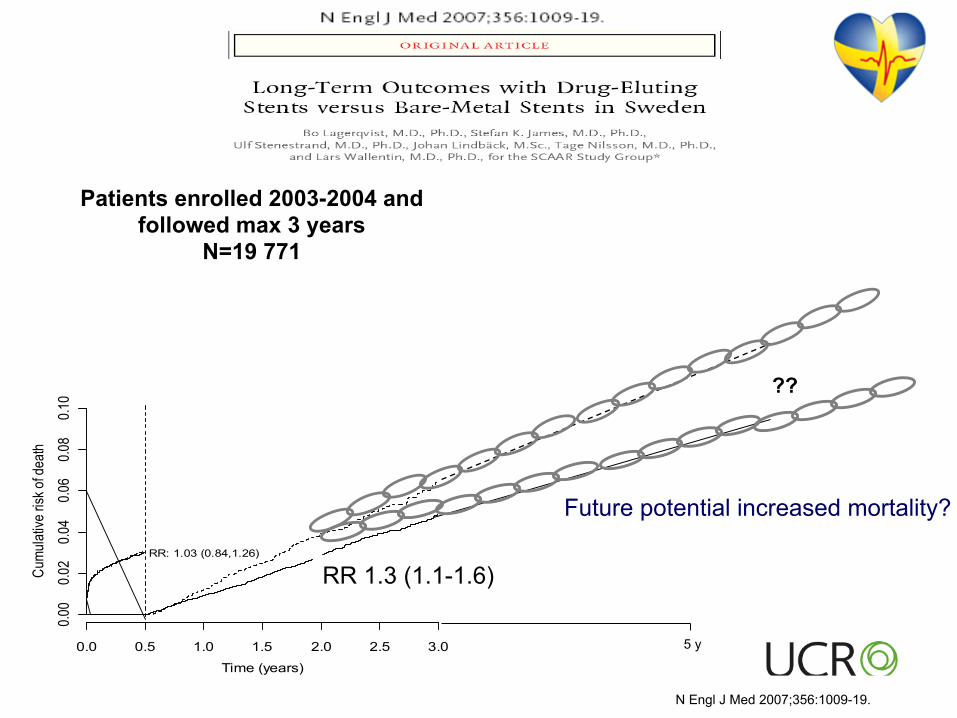
RR: 1.03 (0.84,1.26)
0.0 0.5 1.0 1.5 2.0 2.5 3.0
0.00
0.02
0.04
0.06
0.08
0.10
Time (years)
Cum
ulat
ive ri
sk o
f dea
th
RR: 1.32 (1.11,1.57)
BMS 12880 12473 12354 12228 9298 5966 3199DES 5770 5605 5541 5471 3434 1777 626
RR 1.3 (1.1-1.6)
Future potential increased mortality?
??
5 y
Patients enrolled 2003-2004 and followed max 3 years
N=19 771
N Engl J Med 2007;356:1009-19.
BMS vs DMS Bare metal stents vs. Death metal stents
“The SCAAR registry is contaminated with flaw data….” M Leon 2007
The SCAAR Scare
“This clearly shows how inappropriate registry studies are….” Kastrati 2007
“What is rotten in the kingdom of Sweden” P. Serruys 2008
Years after PCI
Cum
ulat
ive
rate
of d
efin
ite s
tent
thro
mbo
sis
(%)
2 1 0
2
1
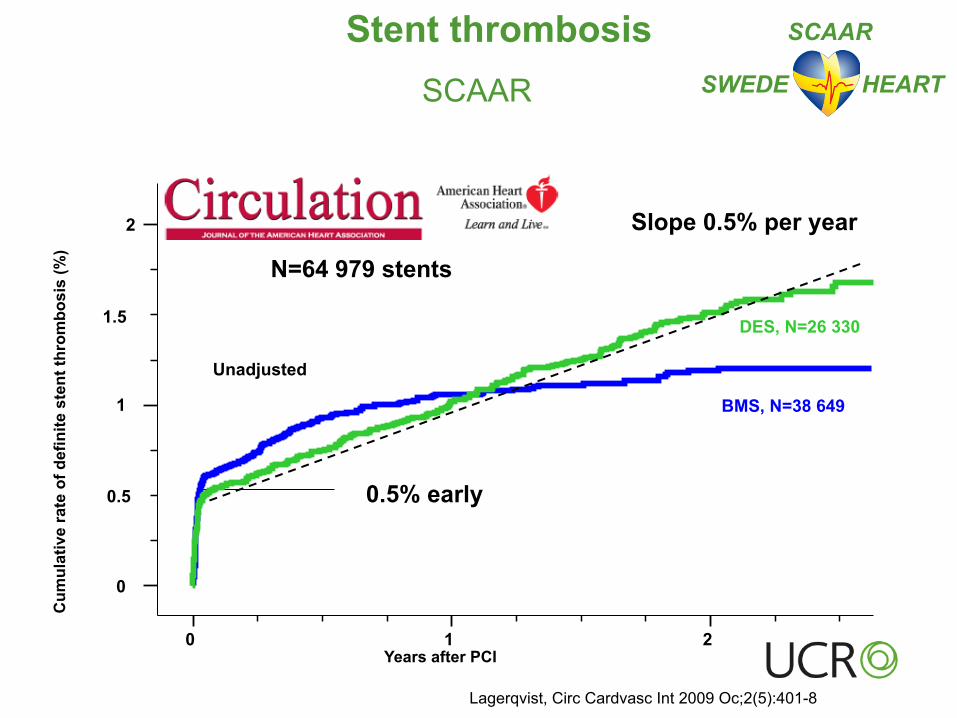
0.5 0.5% early
0
1.5
N=64 979 stents
Unadjusted BMS, N=38 649
Slope 0.5% per year
DES, N=26 330
Lagerqvist, Circ Cardvasc Int 2009 Oc;2(5):401-8
Stent thrombosis SCAAR SWEDE HEART
SCAAR
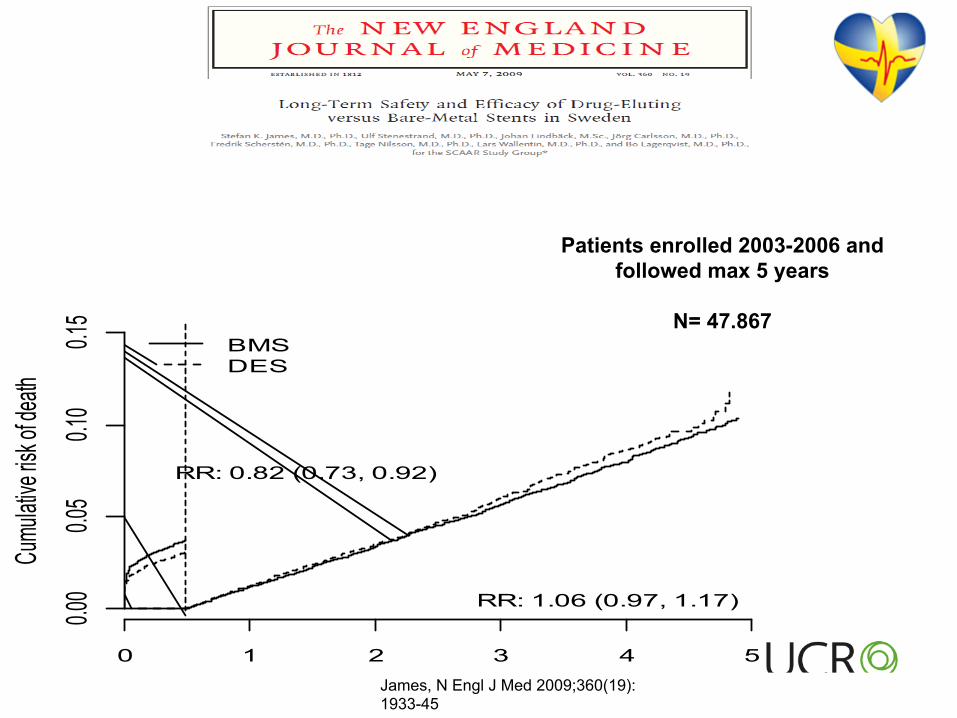
0 1 2 3 4 5
0.00
0.05
0.10
0.15
Time (years)
Cumu
lative
risk of
death
BMSDES
BMS 28286 26843 19429 13592 6682 7DES 19681 18893 12691 6065 1964 0
RR: 0.82 (0.73, 0.92)
RR: 1.06 (0.97, 1.17)
Patients enrolled 2003-2006 and followed max 5 years
N= 47.867
James, N Engl J Med 2009;360(19):1933-45
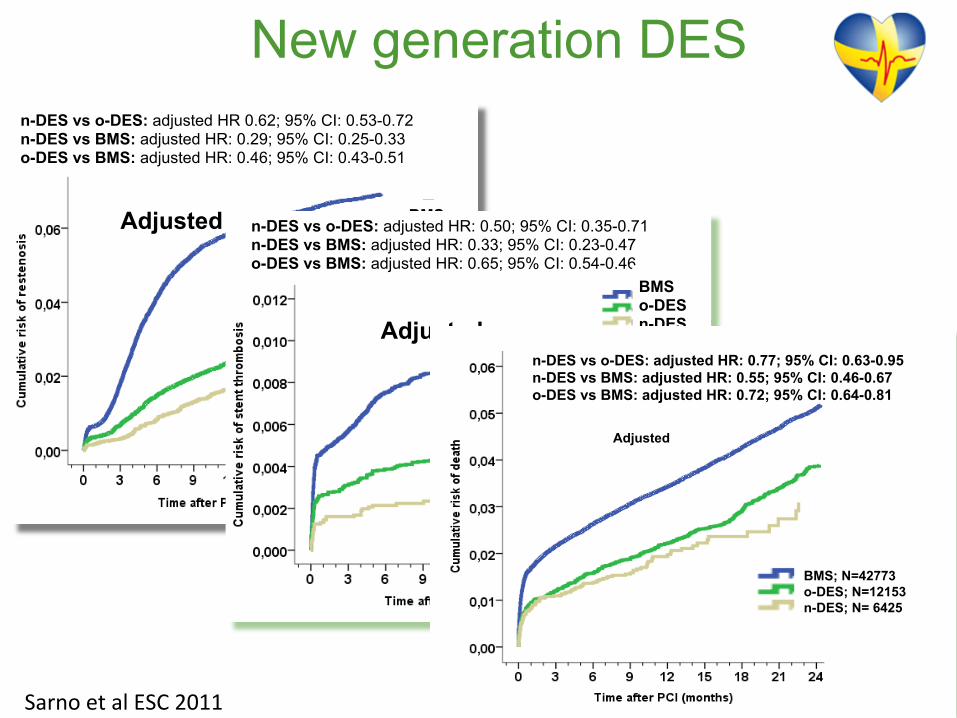
New generation DES n-DES vs o-DES: adjusted HR 0.62; 95% CI: 0.53-0.72 n-DES vs BMS: adjusted HR: 0.29; 95% CI: 0.25-0.33 o-DES vs BMS: adjusted HR: 0.46; 95% CI: 0.43-0.51
BMS o-DES n-DES
Adjusted
Sarno et al ESC 2011
n-DES vs o-DES: adjusted HR: 0.50; 95% CI: 0.35-0.71 n-DES vs BMS: adjusted HR: 0.33; 95% CI: 0.23-0.47 o-DES vs BMS: adjusted HR: 0.65; 95% CI: 0.54-0.46
BMS o-DES n-DES Adjusted
n-DES vs o-DES: adjusted HR: 0.77; 95% CI: 0.63-0.95 n-DES vs BMS: adjusted HR: 0.55; 95% CI: 0.46-0.67 o-DES vs BMS: adjusted HR: 0.72; 95% CI: 0.64-0.81
BMS; N=42773 o-DES; N=12153 n-DES; N= 6425
Adjusted
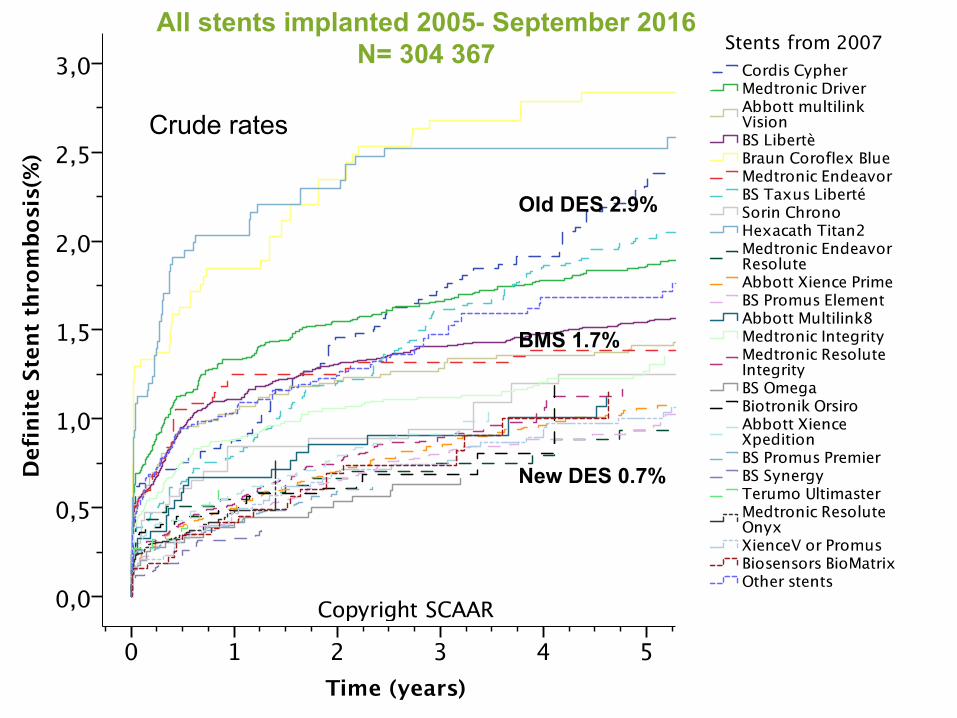
New DES 0.7%
BMS 1.7%
Old DES 2.9%
All stents implanted 2005- September 2016 N= 304 367
Crude rates
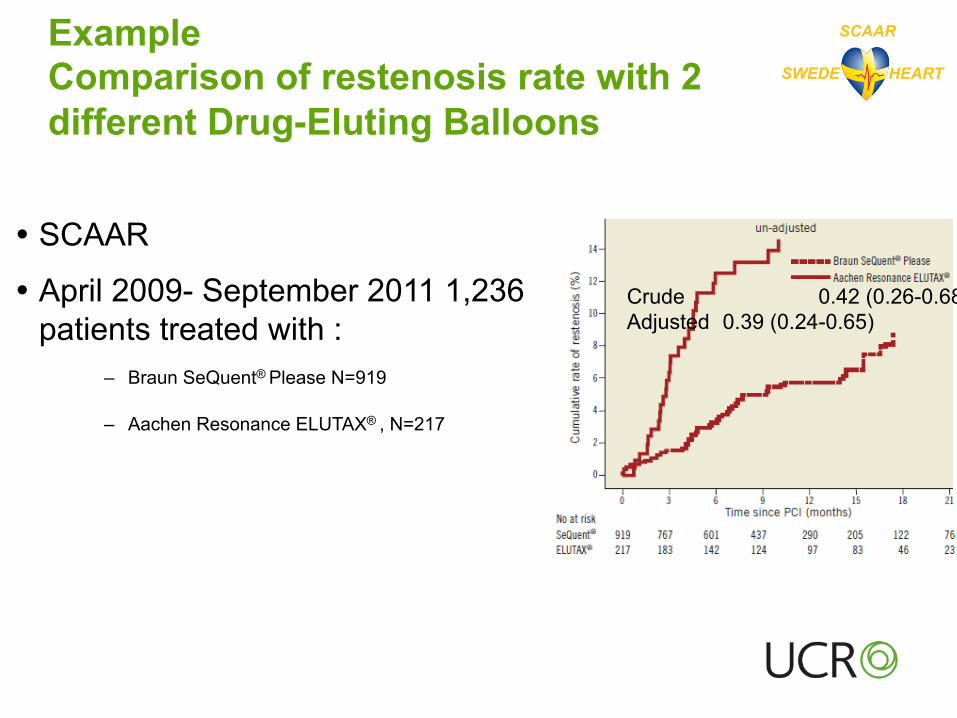
Example Comparison of restenosis rate with 2 different Drug-Eluting Balloons
� SCAAR
� April 2009- September 2011 1,236 patients treated with :
– Braun SeQuent® Please N=919
– Aachen Resonance ELUTAX® , N=217
SWEDE HEART
SCAAR
Crude 0.42 (0.26-0.68) Adjusted 0.39 (0.24-0.65)
Bondesson P. et al, Eurointervention 2012;8(4):444-9
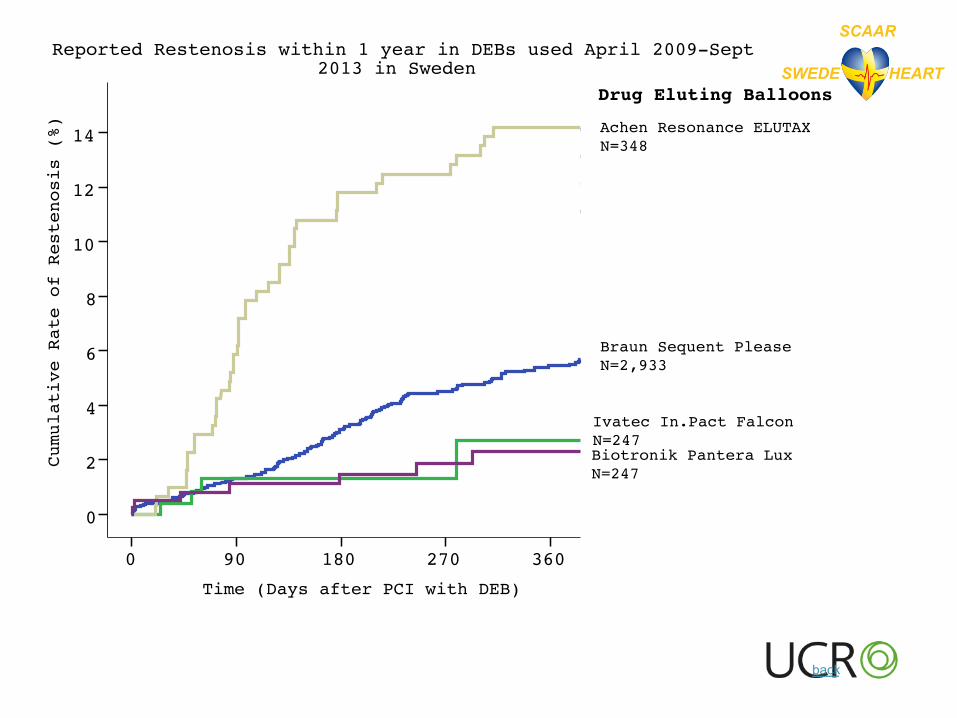
Time (Days after PCI with DEB)
360270180900
Cumulative Rate of Restenosis (%)
14
12
10
8
6
4
2
0
Reported Restenosis within 1 year in DEBs used April 2009-Septe2013 in Sweden
Biotronik Pantera N=382
Aachen Resonance Elutax N=308
Ivatec In.Pact FalN=247
Braun Sequent PleaN=2 933
Drug Eluting BaloDrug Eluting Balloons
Braun Sequent PleaseN=2,933
Ivatec In.Pact FalconN=247Biotronik Pantera LuxN=247
Achen Resonance ELUTAXN=348
SWEDE HEART
SCAAR
back
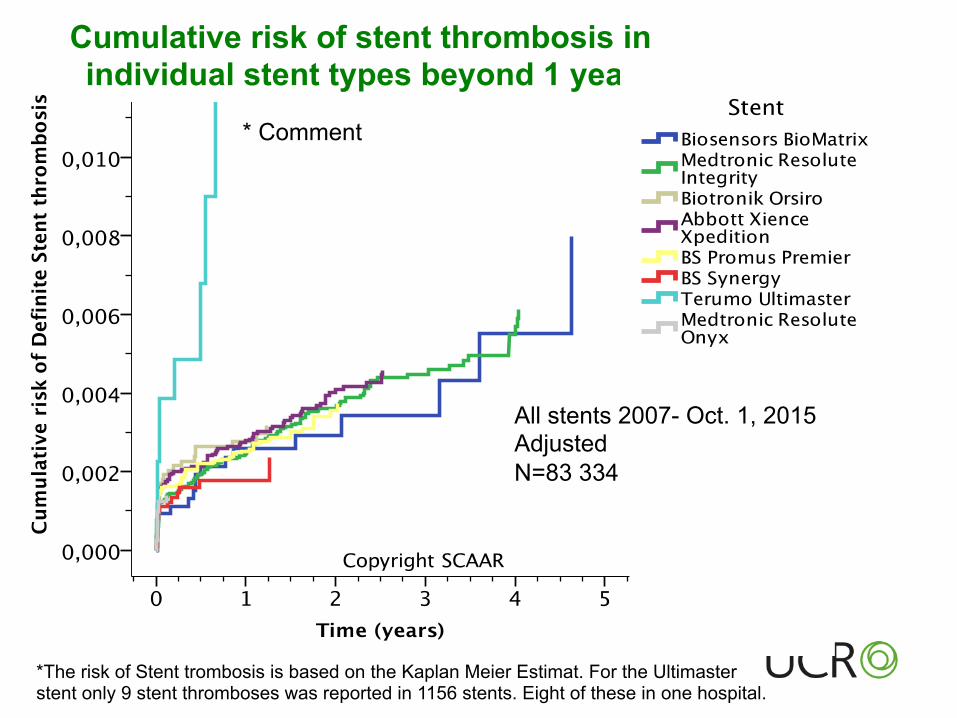
* Comment
*The risk of Stent trombosis is based on the Kaplan Meier Estimat. For the Ultimaster stent only 9 stent thromboses was reported in 1156 stents. Eight of these in one hospital.
All stents 2007- Oct. 1, 2015 Adjusted N=83 334
Cumulative risk of stent thrombosis in individual stent types beyond 1 year
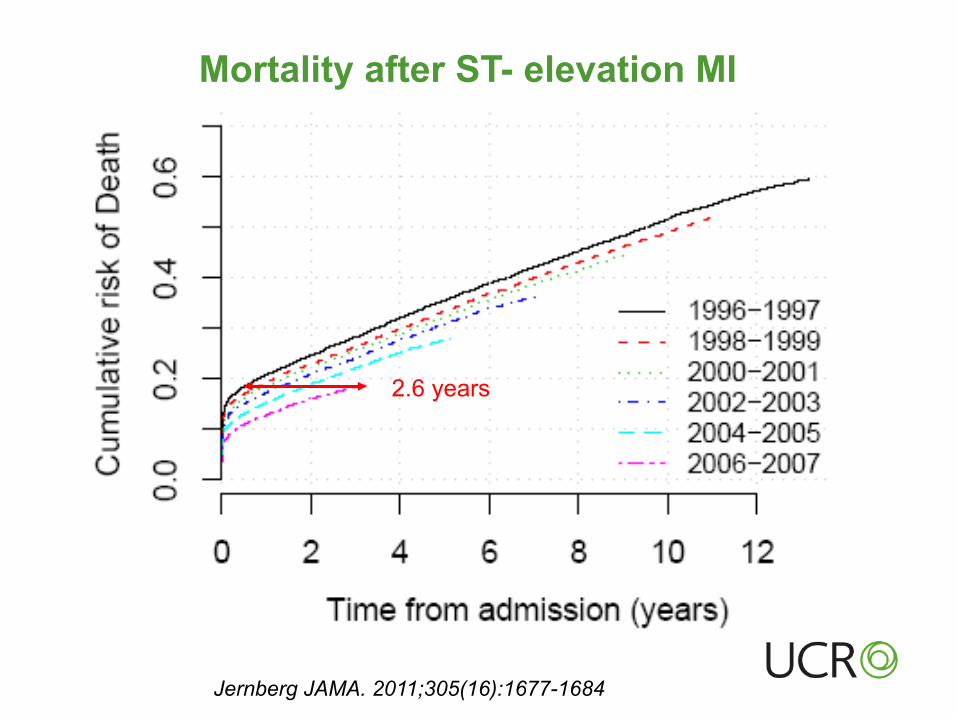
2.6 years
Jernberg JAMA. 2011;305(16):1677-1684
Mortality after ST- elevation MI
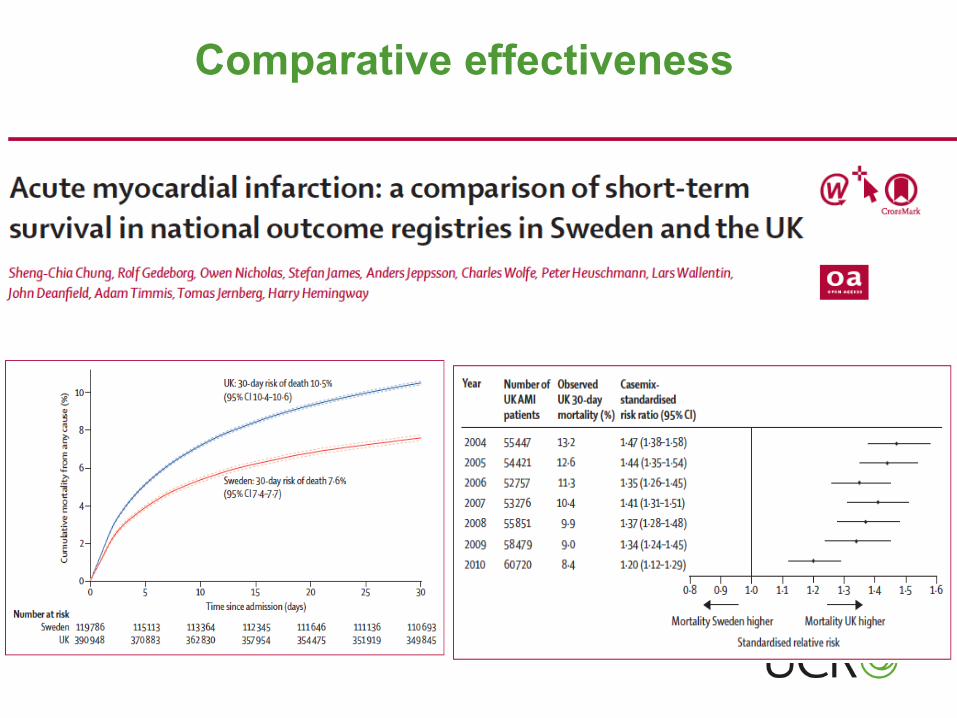
Comparative effectiveness
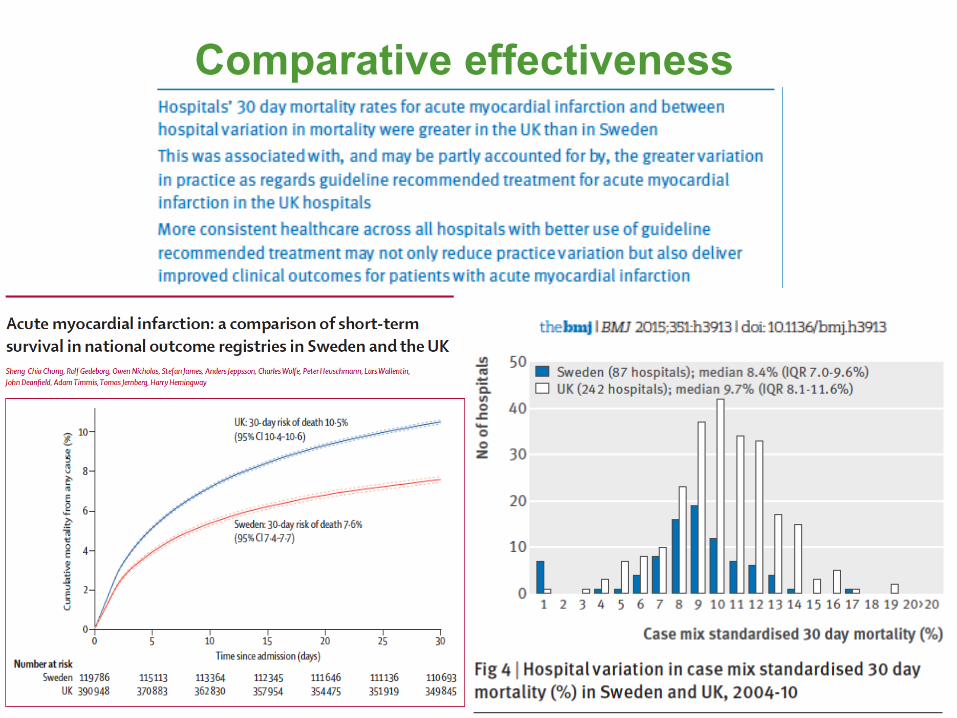
Comparative effectiveness
SWEDE HEART
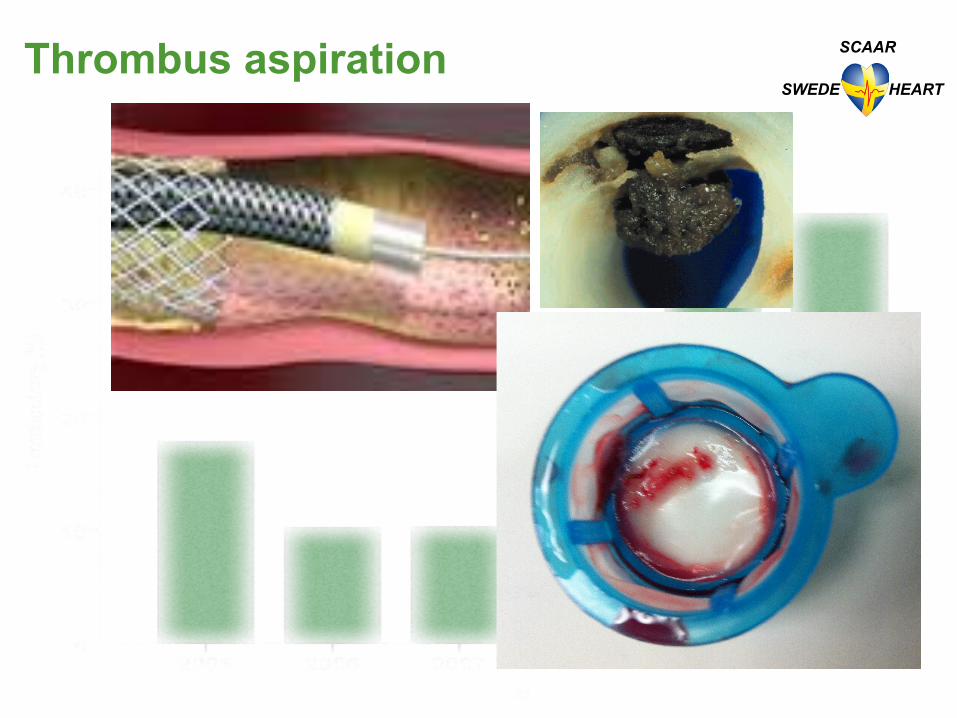
SCAAR Thrombus aspiration
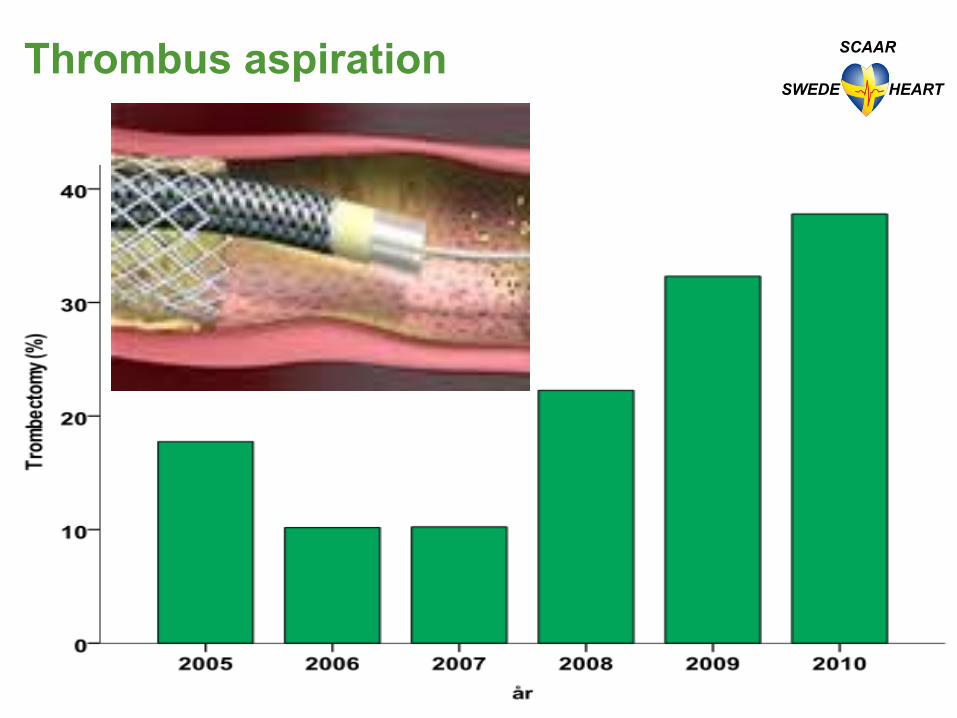
SWEDE HEART
SCAAR Thrombus aspiration
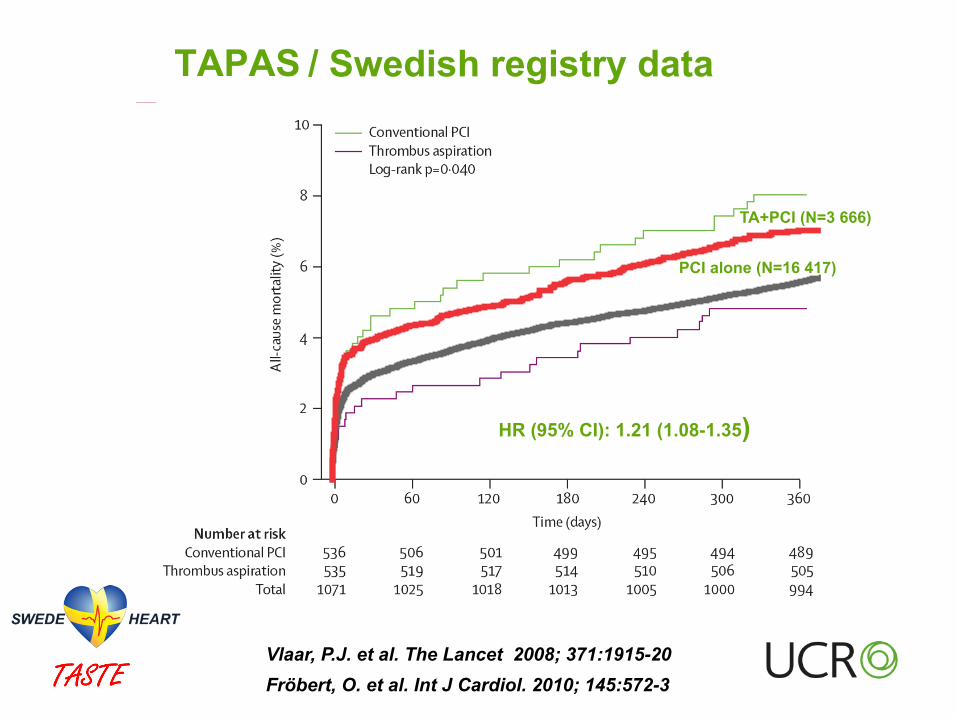
Vlaar, P.J. et al. The Lancet 2008; 371:1915-20
TAPAS
Fröbert, O. et al. Int J Cardiol. 2010; 145:572-3
HR (95% CI): 1.21 (1.08-1.35)
/ Swedish registry data
PCI alone (N=16 417)
TA+PCI (N=3 666)
Randomized Studies (RCT)
Non randomized Observational studies
Randomized Controlled/Clinical Trials - RCT
Weaknesses
Strengths
§ Correctly designed studies with adequate power are gold standard § Extinguishes confounding
§ Highly selected populations due to exclusion criteria § Often selected specialized study centers
§ Often surrogate endpoints
§ Long time to plan and complete § Expensive
§ Often sponsored by industry- only studies with economic interest will be performed
Randomized Clinical Trials- RCT
Strengths
• Data quality variable and questionable • Cannot be used for comparative outcomes research
• Confounding factors can not be adjusted for despite advanced statistical models
• Ideal for description of standars • Unselected patient populations –generalizable
• Large number of events – makes it possible to identify rare events
• Inexpensive
Weaknesses
Register studies Observational studies (Non-inverventional)
Prosective randomized trial that uses a clinical registry for one or several major functions for trial conduct and outcomes reporting.
Register based Randomized Clinical trials- R-RCT
� Iden>fy pa>ents � Randomize
� Collect baseline and procedure characteris>cs (CRF) � Assist with and collect consent forms
� Iden>fy clinical endpoints (endpoint detec>on) � Control clinical outcome events (adjudica>on, CEC)
Some or all parts of trial
What can a registry do?
Registry based Randomized Clinical trials - R-RCT
Strengths
• Correctly designed studies with adequate power are gold standard • Extinguishes confounding
• Unselected patient populations –generalizable
• Large number of events – makes it possible to identify rare events • Inexpensive
Challenges
• Data quality • Variable definition
§ Combines the advantages of a clinical registry and randomized study
§ Complement to classical RCT –No substitute
§ No formal definition
� RRCT
� Evaluation of therapeutic options available/used in
routine clinical care
RCT Approval of new
pharmaceutical agents and medical devices
R-RCT vs. classical RCT

RCT R-RCT
Strategy +
Device – CE mark, used +
Drugs approved/ used in clinical practise
+
Drugs for new indication + +
Device, first in man +
New drugs +
Study design
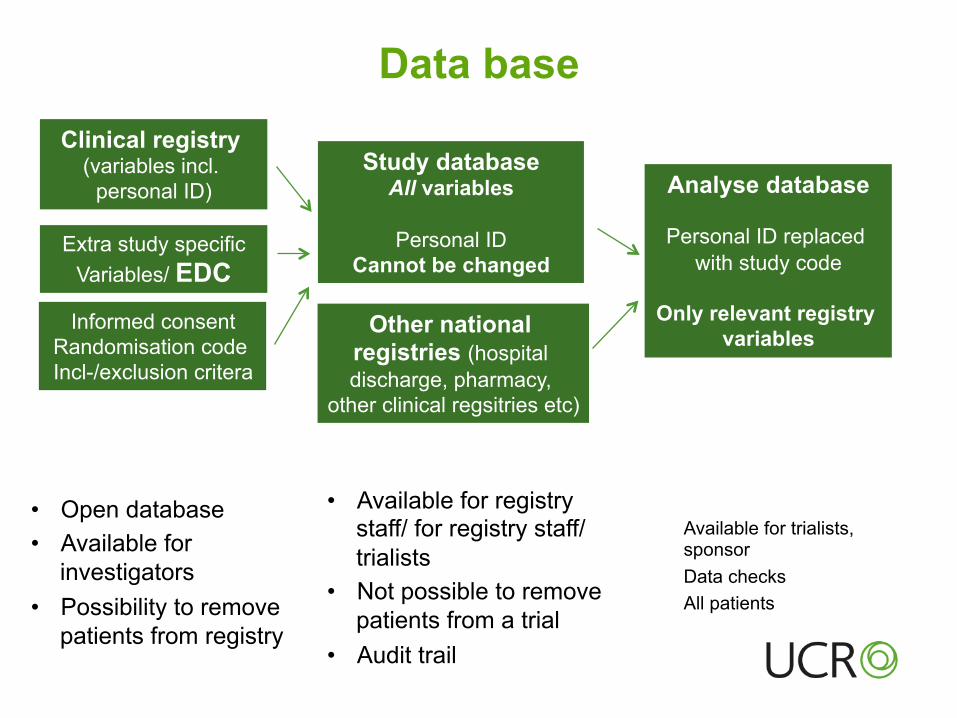
Data base
Informed consent
Randomisation code Incl-/exclusion critera
Extra study specific Variables/ EDC
Clinical registry (variables incl.
personal ID) Study database
All variables
Personal ID Cannot be changed
Analyse database
Personal ID replaced with study code
Only relevant registry
variables
• Open database • Available for
investigators • Possibility to remove
patients from registry
• Available for registry staff/ for registry staff/trialists
• Not possible to remove patients from a trial
• Audit trail
Available for trialists, sponsor Data checks All patients
Other national registries (hospital discharge, pharmacy,
other clinical regsitries etc)
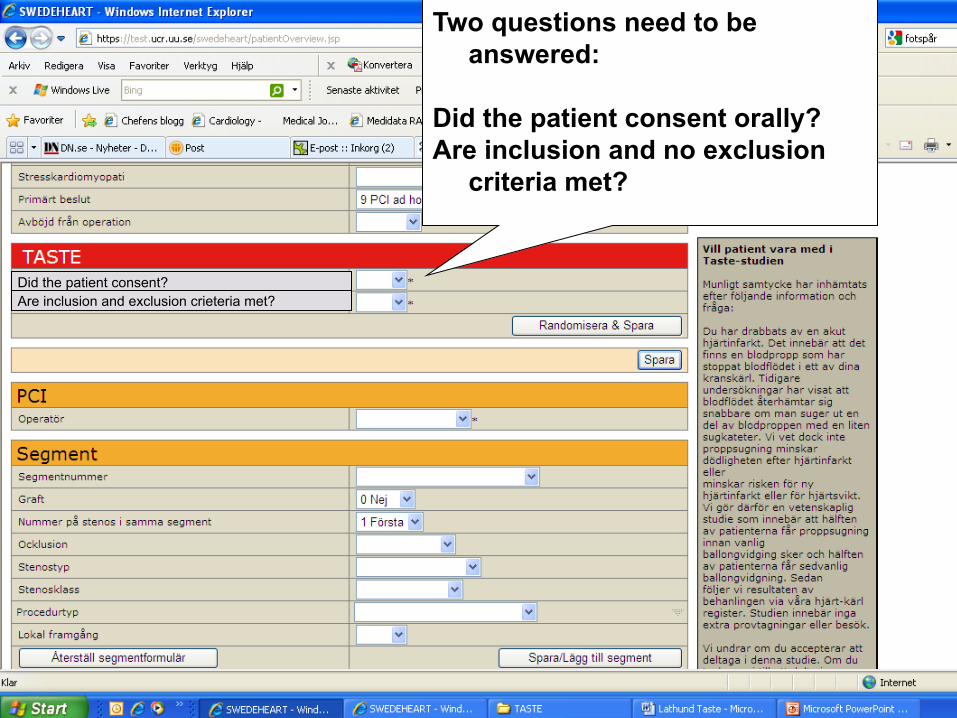
Two questions need to be answered:
Did the patient consent orally? Are inclusion and no exclusion
criteria met?
Did the patient consent? Are inclusion and exclusion crieteria met?
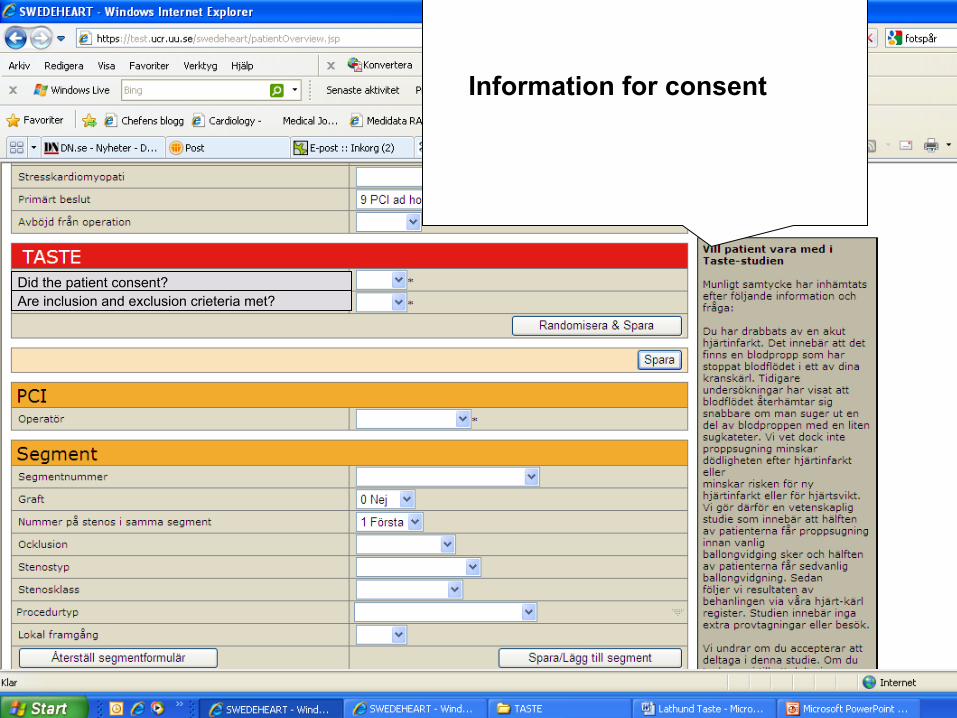
Information for consent
Did the patient consent? Are inclusion and exclusion crieteria met?
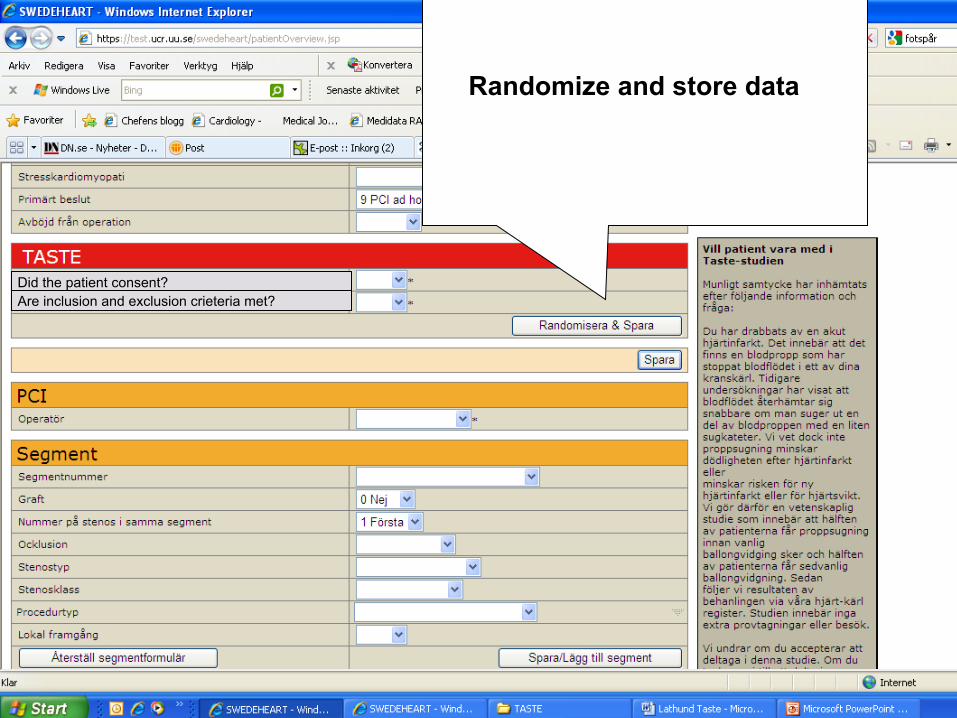
Randomize and store data
Did the patient consent? Are inclusion and exclusion crieteria met?
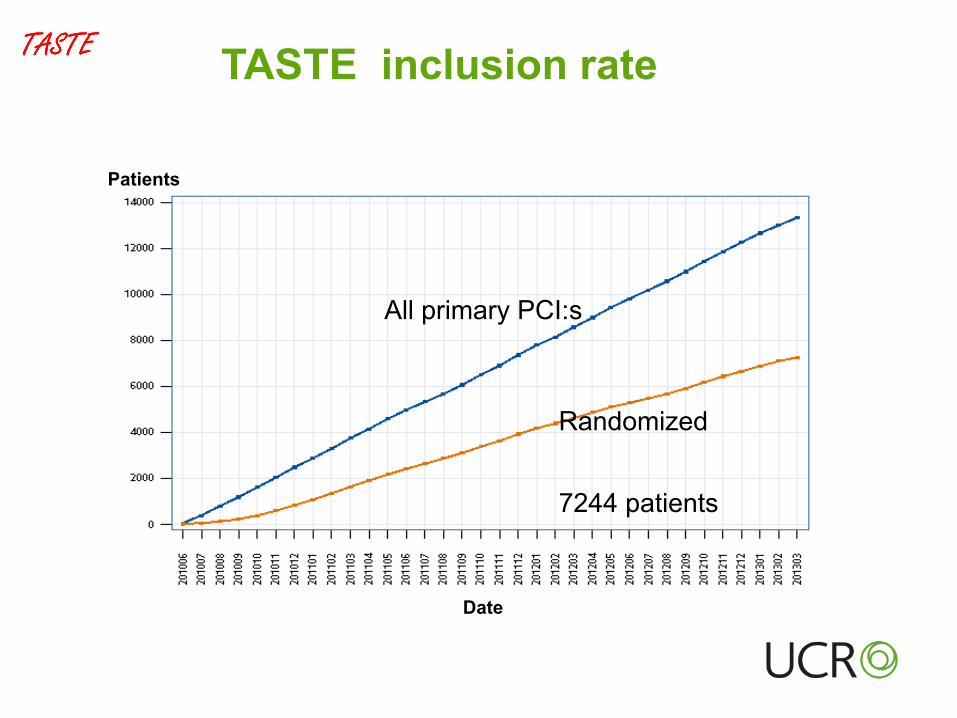
Randomized
All primary PCI:s
7244 patients
Date
Patients
TASTE inclusion rate
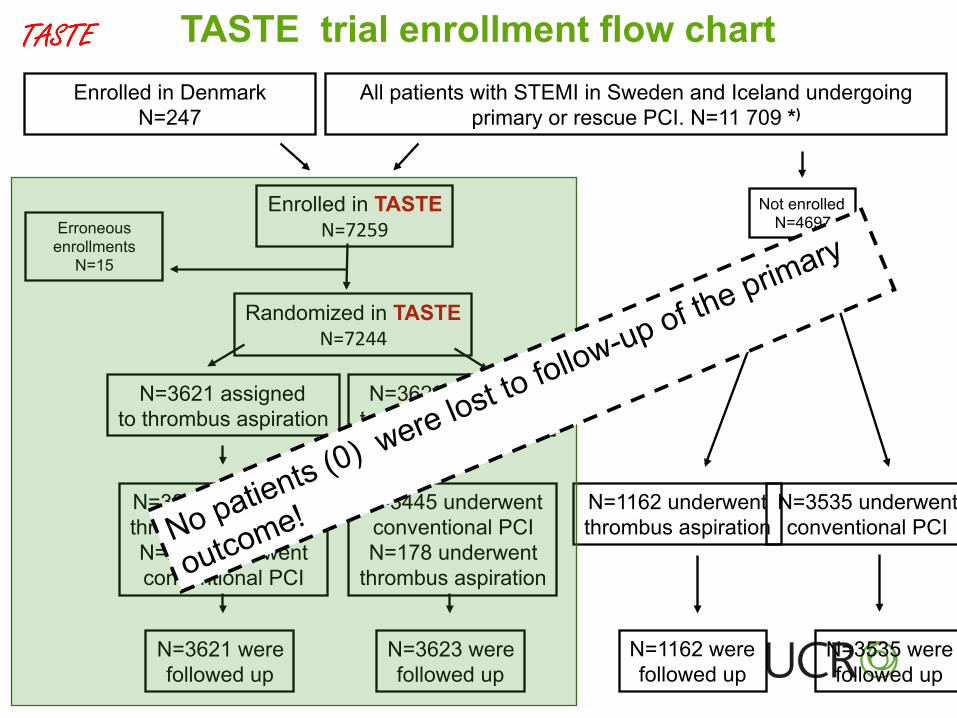
All patients with STEMI in Sweden and Iceland undergoing primary or rescue PCI. N=11 709 *)
Enrolled in TASTE N=7259
N=3621 assigned to thrombus aspiration
N=3399 underwent thrombus aspiration N=222 underwent conventional PCI
TASTE trial enrollment flow chart
Not enrolled N=4697
N=3623 assigned to conventional PCI
N=3535 underwent conventional PCI
N=1162 underwent thrombus aspiration
N=3445 underwent conventional PCI N=178 underwent
thrombus aspiration
N=3621 were followed up
N=3623 were followed up
N=1162 were followed up
N=3535 were followed up
Enrolled in Denmark N=247
Erroneous enrollments
N=15
Randomized in TASTE N=7244
� � � � � �� �����
���
���
��
���
��
���
�� �������������������������������������������������������������������������������������������������������������������������� �������������������������������������������������������������������������������������������������������������������������������
�����������
�� ���
��
���
����
����
����
�!�"
���#
�$%&
'�(�#�
���
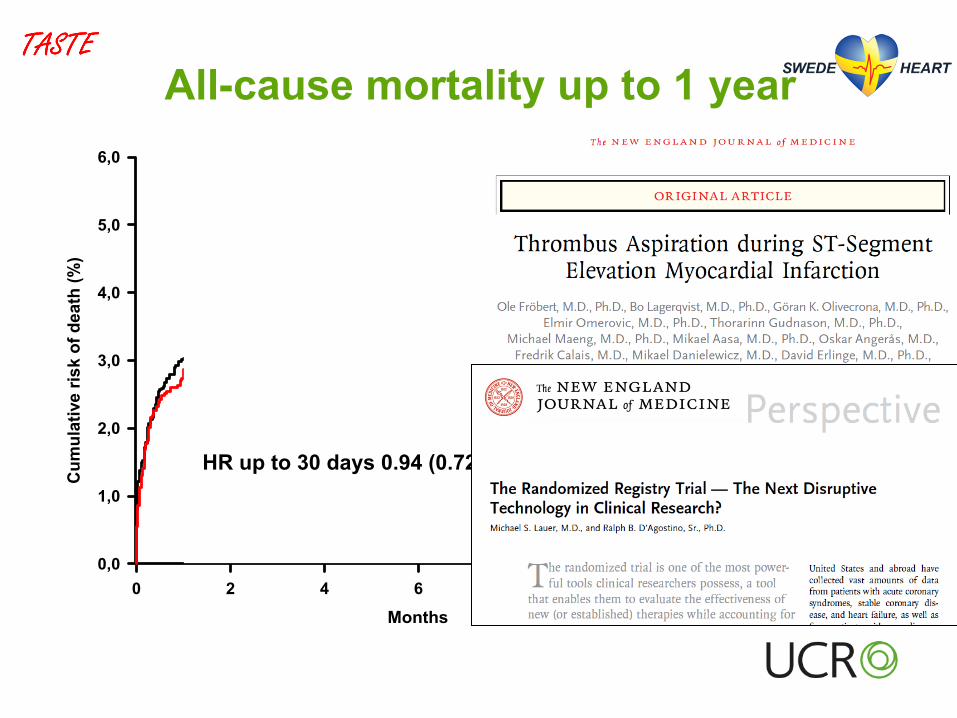
All-cause mortality up to 1 year
HR up to 1 year 0.94 (0.78 – 1.15), P=0.57
HR up to 30 days 0.94 (0.72 - 1.22), P=0.63
� � � � � �� �����
���
���
��
���
��
���
�� �������������������������������������������������������������������������������������������������������������������������� �������������������������������������������������������������������������������������������������������������������������������
�����������
�� ���
��
���
����
����
����
�!�"
���#
�$%&
'�(�#�
���
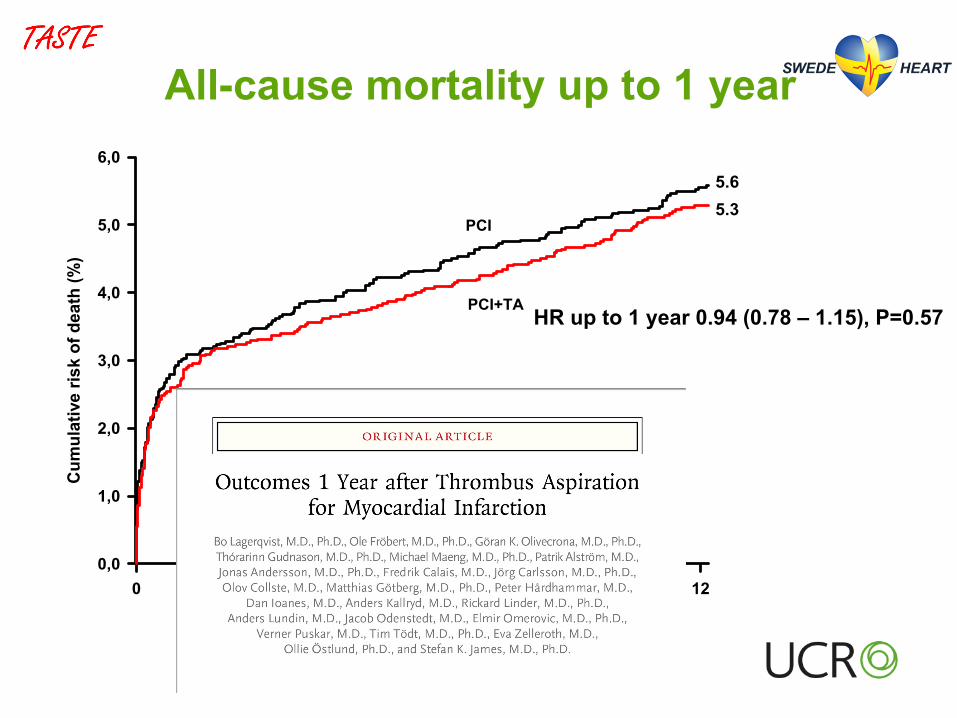
All-cause mortality up to 1 year
HR up to 1 year 0.94 (0.78 – 1.15), P=0.57
HR up to 30 days 0.94 (0.72 - 1.22), P=0.63
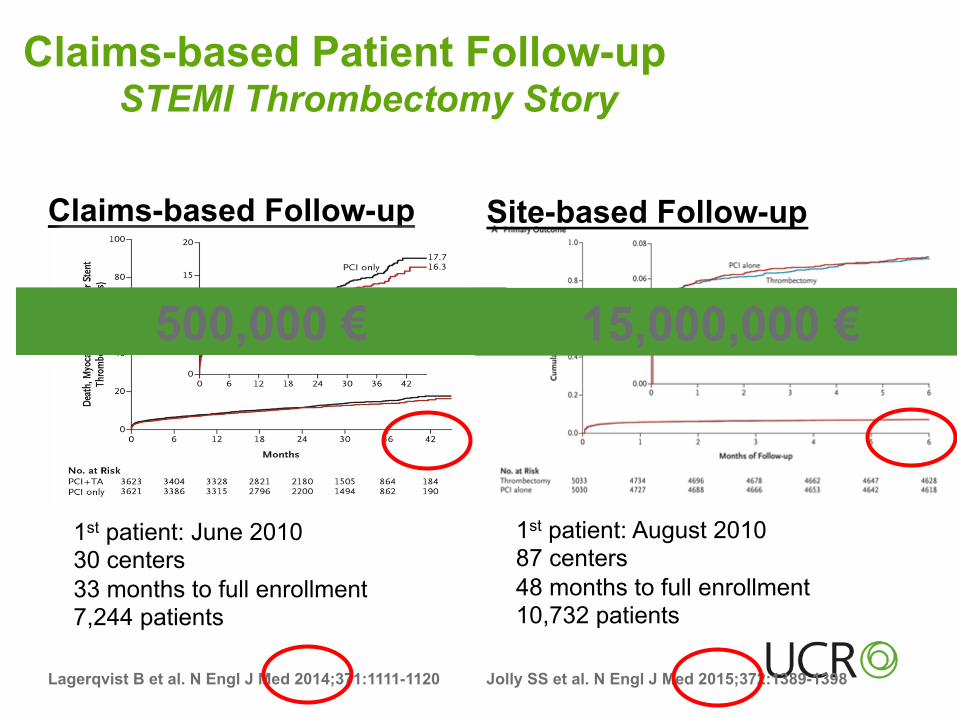
Claims-based Patient Follow-up STEMI Thrombectomy Story
Claims-based Follow-up
Lagerqvist B et al. N Engl J Med 2014;371:1111-1120 Jolly SS et al. N Engl J Med 2015;372:1389-1398
1st patient: June 2010 30 centers 33 months to full enrollment 7,244 patients
1st patient: August 2010 87 centers 48 months to full enrollment 10,732 patients
Site-based Follow-up
500,000 € 15,000,000 €
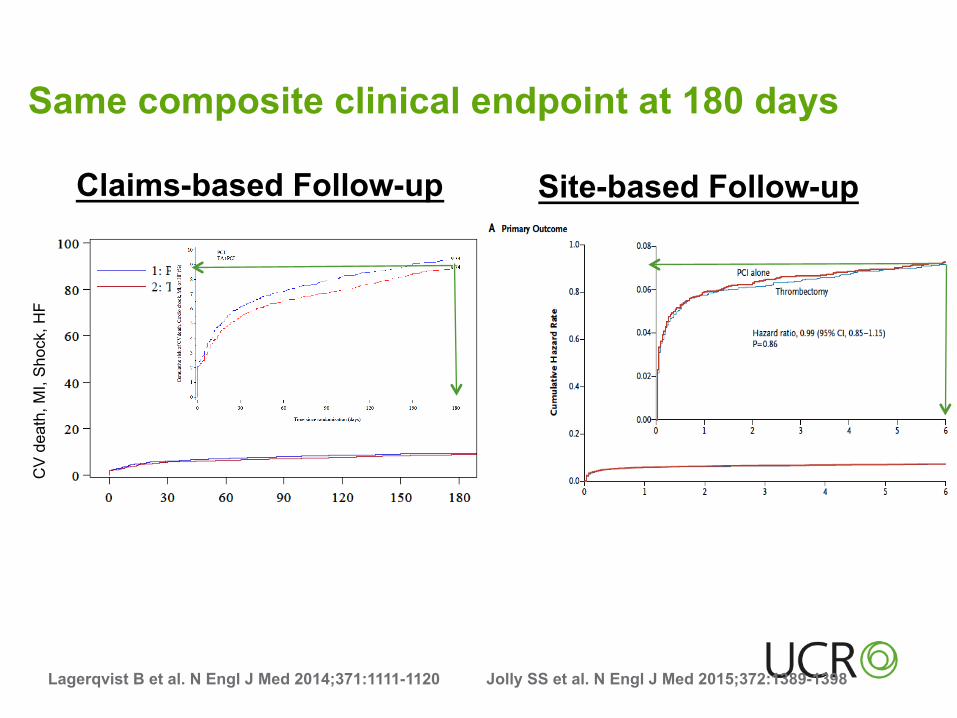
Same composite clinical endpoint at 180 days
Claims-based Follow-up
Lagerqvist B et al. N Engl J Med 2014;371:1111-1120 Jolly SS et al. N Engl J Med 2015;372:1389-1398
Site-based Follow-up
CV
dea
th, M
I, S
hock
, HF
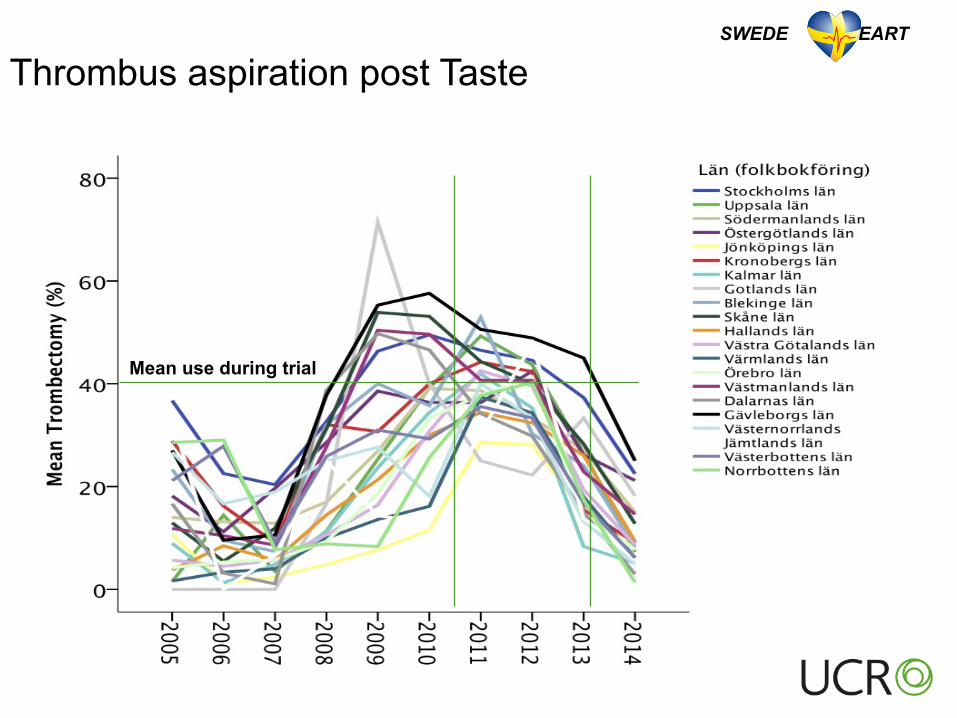
Thrombus aspiration post Taste
Mean use during trial
SWEDE HEART
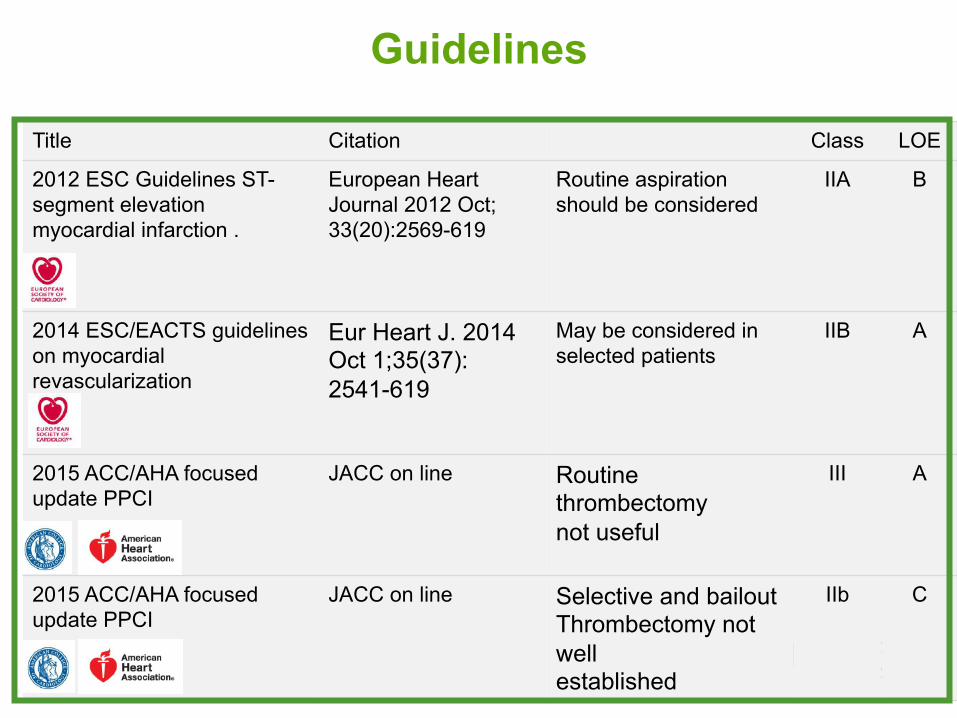
Title Citation Class LOE
2012 ESC Guidelines ST-segment elevation myocardial infarction .
European Heart Journal 2012 Oct;33(20):2569-619
Routine aspiration should be considered
IIA B
2014 ESC/EACTS guidelines on myocardial revascularization
Eur Heart J. 2014 Oct 1;35(37):2541-619
May be considered in selected patients
IIB A
2015 ACC/AHA focused update PPCI
JACC on line Routine thrombectomy not useful
III A
2015 ACC/AHA focused update PPCI
JACC on line Selective and bailout Thrombectomy not well established
IIb C
Guidelines
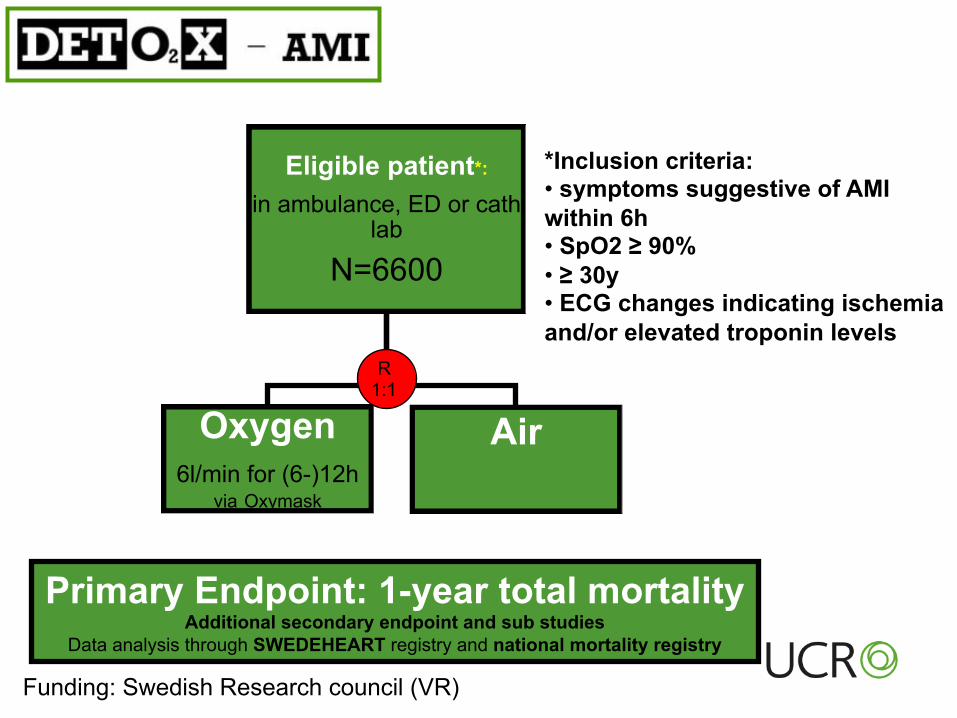
Eligible patient*:
in ambulance, ED or cath lab
N=6600
Oxygen 6l/min for (6-)12h
via Oxymask
Air
Primary Endpoint: 1-year total mortality Additional secondary endpoint and sub studies
Data analysis through SWEDEHEART registry and national mortality registry
*Inclusion criteria: • symptoms suggestive of AMI within 6h • SpO2 ≥ 90% • ≥ 30y • ECG changes indicating ischemia and/or elevated troponin levels
R 1:1
Funding: Swedish Research council (VR)
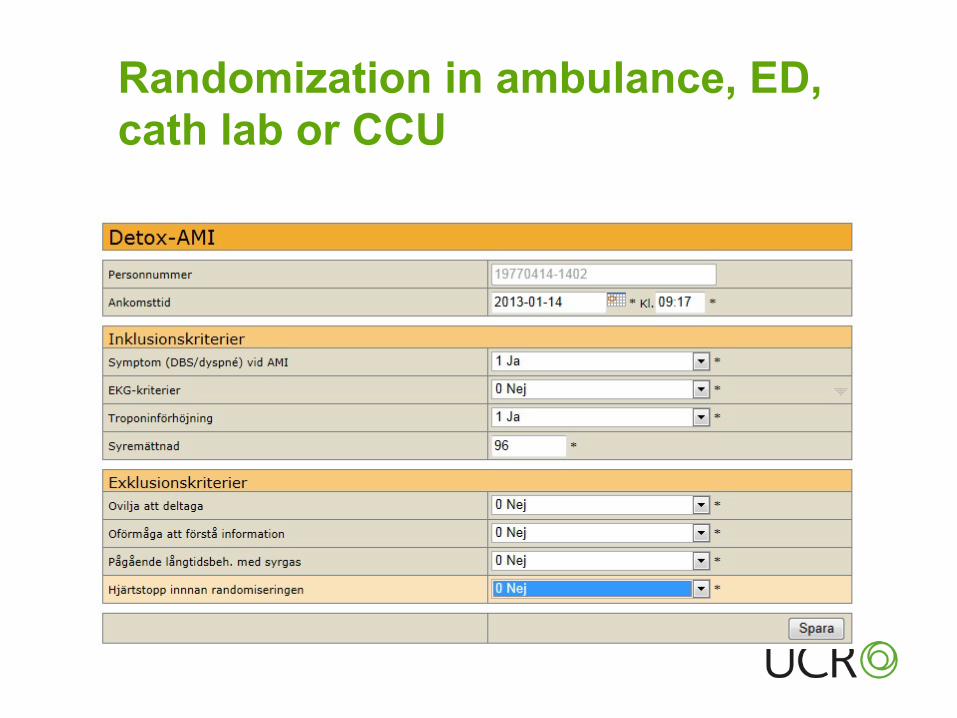
Randomization in ambulance, ED, cath lab or CCU
Inklud
erad
e pa
tienter
0
1000
2000
3000
4000
5000
6000
Datum
2013-‐01-‐01 2013-‐07-‐01 2014-‐01-‐01 2014-‐07-‐01 2015-‐01-‐01 2015-‐07-‐01 2016-‐01-‐01
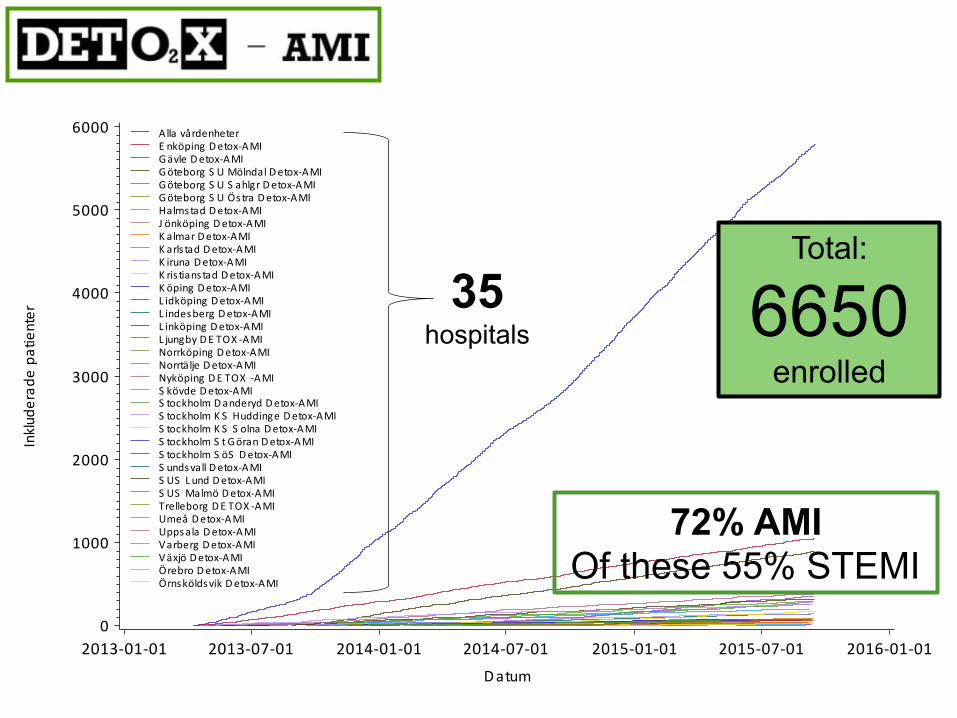
Alla vårdenheterE nköping Detox-‐AMIGävle Detox-‐AMIGöteborg S U Mölndal Detox-‐AMIGöteborg S U S ahlgr Detox-‐AMIGöteborg S U Östra Detox-‐AMIHalmstad Detox-‐AMIJ önköping Detox-‐AMIK almar Detox-‐AMIK arls tad Detox-‐AMIK iruna Detox-‐AMIK ris tianstad Detox-‐AMIK öping Detox-‐AMIL idköping Detox-‐AMIL indesberg Detox-‐AMIL inköping Detox-‐AMIL jungby DE TOX -‐AMINorrköping Detox-‐AMINorrtälje Detox-‐AMINyköping DE TOX -‐AMIS kövde Detox-‐AMIS tockholm Danderyd Detox-‐AMIS tockholm K S Huddinge Detox-‐AMIS tockholm K S S olna Detox-‐AMIS tockholm S t Göran Detox-‐AMIS tockholm S öS Detox-‐AMIS undsvall Detox-‐AMIS US L und Detox-‐AMIS US Malmö Detox-‐AMITrelleborg DE TOX -‐AMIUmeå Detox-‐AMIUppsala Detox-‐AMIVarberg Detox-‐AMIVäxjö Detox-‐AMIÖrebro Detox-‐AMIÖrnsköldsvik Detox-‐AMI
35 hospitals
Total:
6650 enrolled
72% AMI Of these 55% STEMI
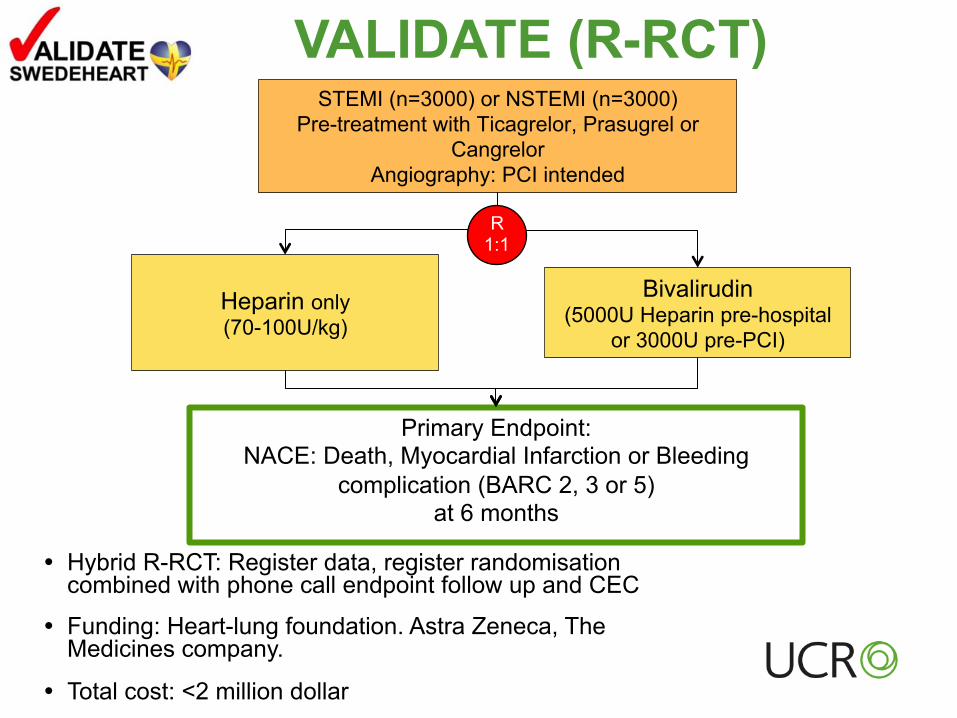
VALIDATE (R-RCT)
� Hybrid R-RCT: Register data, register randomisation combined with phone call endpoint follow up and CEC
� Funding: Heart-lung foundation. Astra Zeneca, The Medicines company.
� Total cost: <2 million dollar
STEMI (n=3000) or NSTEMI (n=3000) Pre-treatment with Ticagrelor, Prasugrel or
Cangrelor Angiography: PCI intended
Primary Endpoint: NACE: Death, Myocardial Infarction or Bleeding
complication (BARC 2, 3 or 5) at 6 months
Heparin only (70-100U/kg)
Bivalirudin (5000U Heparin pre-hospital
or 3000U pre-PCI)
R 1:1
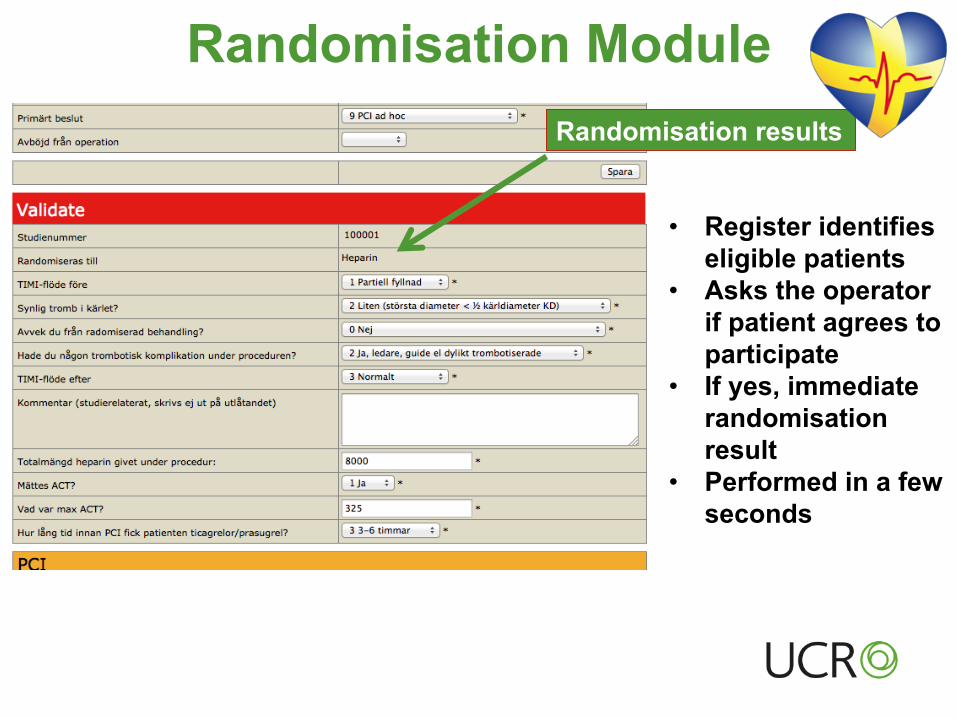
Randomisation Module
• Register identifies eligible patients
• Asks the operator if patient agrees to participate
• If yes, immediate randomisation result
• Performed in a few seconds
Randomisation results
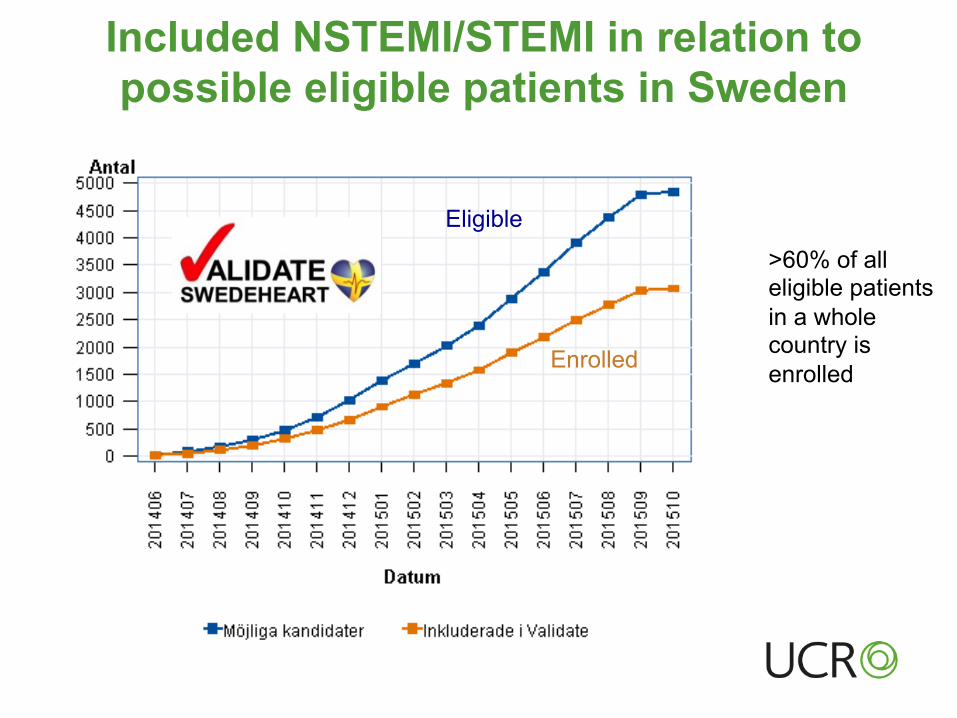
Included NSTEMI/STEMI in relation to possible eligible patients in Sweden
Eligible
Enrolled
>60% of all eligible patients in a whole country is enrolled
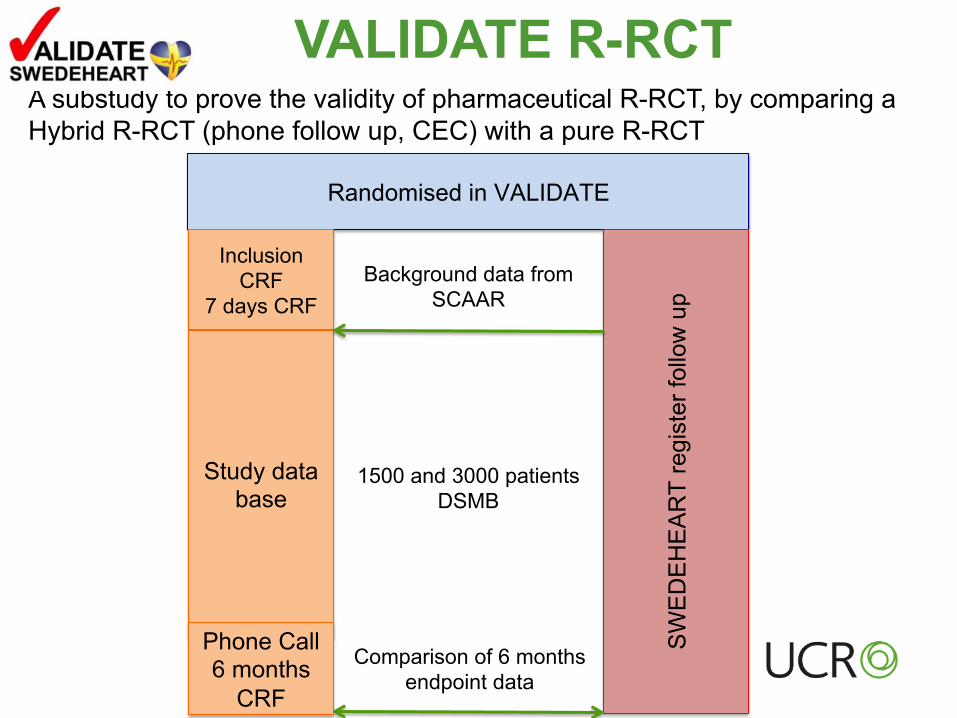
Randomised in VALIDATE
Inclusion CRF
7 days CRF
SW
ED
EH
EA
RT
regi
ster
follo
w u
p
Study data base
1500 and 3000 patients DSMB
Comparison of 6 months endpoint data
Phone Call 6 months
CRF
A substudy to prove the validity of pharmaceutical R-RCT, by comparing a Hybrid R-RCT (phone follow up, CEC) with a pure R-RCT
Background data from SCAAR
VALIDATE R-RCT
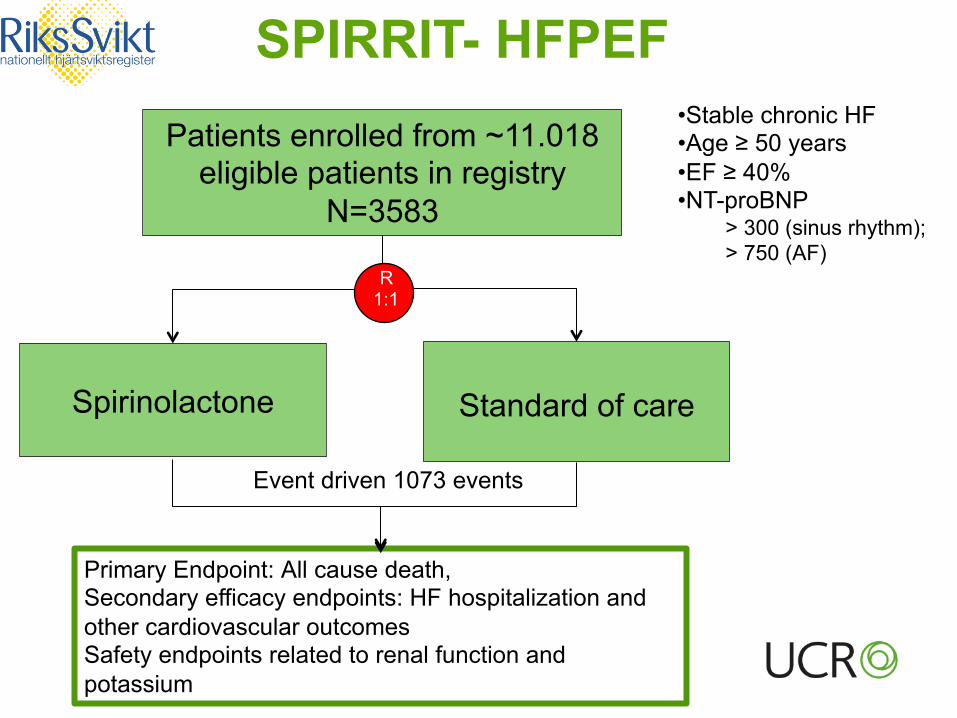
SPIRRIT- HFPEF
Patients enrolled from ~11.018 eligible patients in registry
N=3583
Primary Endpoint: All cause death, Secondary efficacy endpoints: HF hospitalization and other cardiovascular outcomes Safety endpoints related to renal function and potassium
Spirinolactone
Standard of care
R 1:1
• Stable chronic HF • Age ≥ 50 years • EF ≥ 40% • NT-proBNP
> 300 (sinus rhythm); > 750 (AF)
Event driven 1073 events
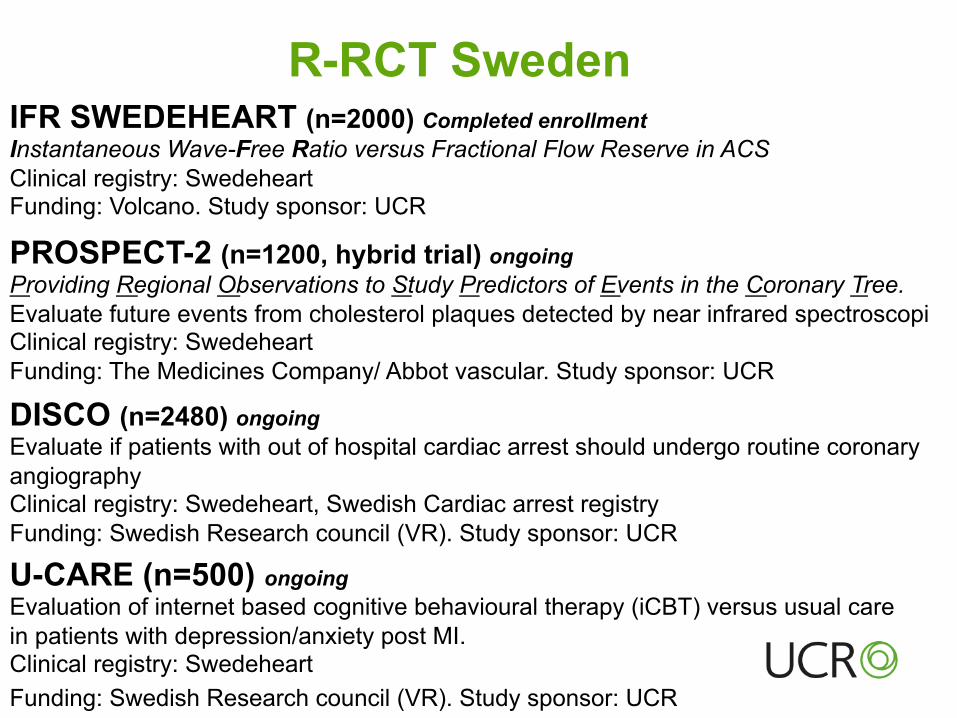
IFR SWEDEHEART (n=2000) Completed enrollment Instantaneous Wave-Free Ratio versus Fractional Flow Reserve in ACS Clinical registry: Swedeheart Funding: Volcano. Study sponsor: UCR
R-RCT Sweden
PROSPECT-2 (n=1200, hybrid trial) ongoing Providing Regional Observations to Study Predictors of Events in the Coronary Tree. Evaluate future events from cholesterol plaques detected by near infrared spectroscopi Clinical registry: Swedeheart Funding: The Medicines Company/ Abbot vascular. Study sponsor: UCR DISCO (n=2480) ongoing Evaluate if patients with out of hospital cardiac arrest should undergo routine coronary angiography Clinical registry: Swedeheart, Swedish Cardiac arrest registry Funding: Swedish Research council (VR). Study sponsor: UCR
U-CARE (n=500) ongoing Evaluation of internet based cognitive behavioural therapy (iCBT) versus usual care in patients with depression/anxiety post MI. Clinical registry: Swedeheart Funding: Swedish Research council (VR). Study sponsor: UCR
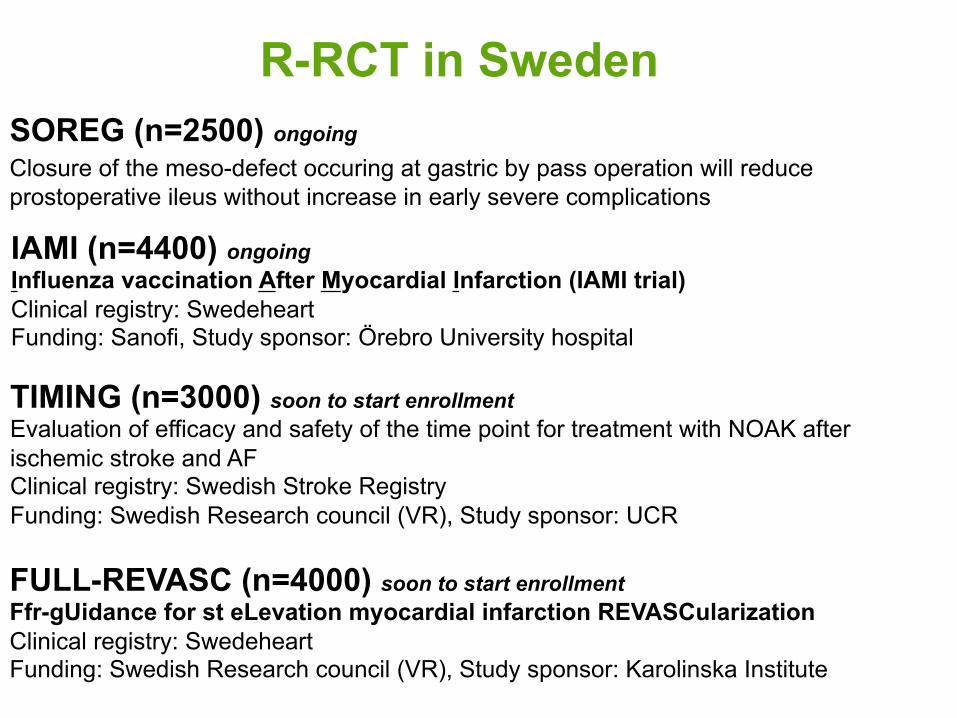
R-RCT in Sweden SOREG (n=2500) ongoing Closure of the meso-defect occuring at gastric by pass operation will reduce prostoperative ileus without increase in early severe complications
IAMI (n=4400) ongoing Influenza vaccination After Myocardial Infarction (IAMI trial) Clinical registry: Swedeheart Funding: Sanofi, Study sponsor: Örebro University hospital
TIMING (n=3000) soon to start enrollment Evaluation of efficacy and safety of the time point for treatment with NOAK after ischemic stroke and AF Clinical registry: Swedish Stroke Registry Funding: Swedish Research council (VR), Study sponsor: UCR
FULL-REVASC (n=4000) soon to start enrollment Ffr-gUidance for st eLevation myocardial infarction REVASCularization Clinical registry: Swedeheart Funding: Swedish Research council (VR), Study sponsor: Karolinska Institute
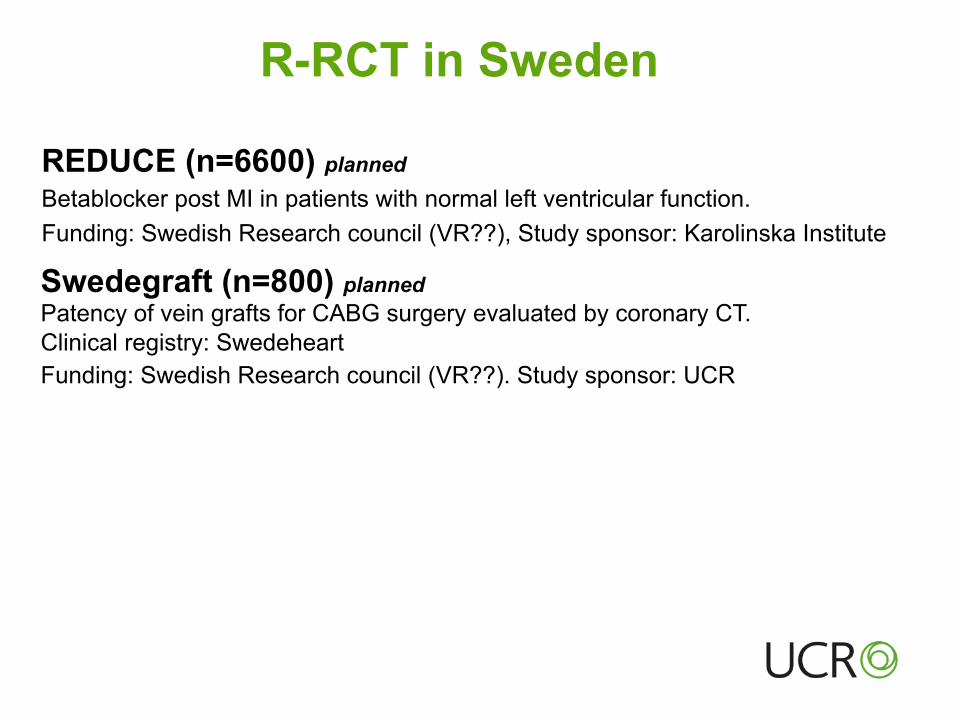
R-RCT in Sweden
Swedegraft (n=800) planned Patency of vein grafts for CABG surgery evaluated by coronary CT. Clinical registry: Swedeheart Funding: Swedish Research council (VR??). Study sponsor: UCR
REDUCE (n=6600) planned Betablocker post MI in patients with normal left ventricular function. Funding: Swedish Research council (VR??), Study sponsor: Karolinska Institute