-
8/12/2019 Registration of Stem Cell Based Clinical Trials
1/7
WORLD STEM CELL REPORT 2009 GENETICS POLICY INSTITUTE 501c3
2010 WORLD STEM CELL SUMMIT DETROIT, MI OCTOBER 4-6, 2010
WWW.WORLDSTEMCELLSUMMIT.COM WWW.GENPOL.ORG15
STEM CELLS, REGENERATIVE MEDICINE, AND SOCIETY
ubstantial progress in stem cell research hasbeen made since the
first report on thederivation of human embryonic stem (ES)
cells.1 As we celebrate the 10th anniversary of thislandmark
event, we also witness new scientific2
and policy3, 4
milestones that reinvigorate hopesfor moving forward the
clinical translation of stemcell-based interventions. Nevertheless,
stem cell-based therapies remain largely at theexperimental stages
and the road towards theclinical is still paved with major
scientific5, 6 andethical7 hurdles. A positive signpost though, is
therecent approval of what will be the worlds firstclinical trial
of a hESC-derived product by theUnited States Food and Drug
Administration
(FDA).
8
Geron Corporation has been grantedclearance for an
Investigational New Drug (IND)application for the clinical trial of
GRNOPC1 inpatients with acute spinal cord injury.
This article briefly addresses the rationale for establishing
clinicaltrial registries (CTR) and the challenges arising from
theirimplementation. A Clinical Trial Registry (CTR) is a
publiclyavailable database of all human interventional clinical
trials*regardless of the stage of development at inception, while
inprogress or after completion and of their publication status.
Theraison dtre for mandating the prospective registration of all
stem-cell based clinical trials will be discussed. It is beyond the
scope of this
paper to provide a comprehensive analysis of the wide range
ofpossible approaches, policy responses and their
implications.However, we want to provide a starting point for
discussionsurrounding key questions and challenges facing clinical
trialregistration, questions that go beyond a call for
voluntarypublication.
SMoving Towards the Clinic: Science,Policy and Ethics
Alongside these new scientific advances, important
policydevelopments have also taken place. The International Society
forStem Cell Research (ISSCR) adopted the first professional
guidelinessetting standards for the clinical translation of stem
cells9 in three
major areas: cell processing and manufacturing, pre-clinical
studiesand clinical research. The guidelines encompass
recommendationsand establish principles for the scientific,
clinical and ethical conductof translational stem cell researchers,
clinician-scientists, andregulators in the international
community.
In the context of medical research ethics in general,
anothersignificant policy development took place while we celebrate
a decadesince James Thomsons discovery. The World Medical
Associationamended the Helsinki Declaration,10 the primary source
and arbiterof research ethics worldwide.11While the Declaration is
addressedprimarily to physicians, the WMA intends for the
Declarations scopeto reach a full range of stakeholders.
Both the Helsinki Declaration and the ISSCR guidelines
recognize that authors, editors and publishers have ethical
obligationswith regard to the full publication of research results,
whethernegative, inconclusive or positive. Similarly, they
recognize the rightof research participants in particular and
society in general to haveaccess to this information. Moreover, the
Declaration of Helsinkitook the unprecedented move to call for the
registration of everyclinical trial in a publicly accessible
database before the recruitment ofthe first research subject
(Principle 19). In contrast, the ISSCRguidelines called only for
the publication of both positive andnegative results and adverse
events at professional scientificconferences or in peer-review
scientific journals before reporting theirresearch to the lay media
or to patient advocacy groups and
associations (Recommendation 33).The aforementioned policy
recommendations are of significantimportance as they establish
principles for strengthening transparencyin clinical research by
calling for the prospective publication ofresearch results. By
promoting transparency, they are encouragingscientific and ethical
integrity in clinical trials. They are also seeking
Registration of Stem Cell-BasedClinical Trials: A Scientific
and
Ethical ImperativeBy Rosario M. Isasi, J.D., M.P.H.
*The World Health Organization defines, for the purposes of
registration, a clinical trial as any research study that
prospectively assigns human participants or groups of humansto one
or more health-related interventions to evaluate the effects on
health outcomes. Clinical trials may also be referred to as
interventional trials. Interventions include but are
not restricted to drugs, cells and other biological products,
surgical procedures, radiologic procedures, devices, behavioural
treatments, process-of-care changes, preventive care, etc.
This definition includes Phase I to Phase IV trials.
http://www.who.int/ictrp/en/
http://www.worldstemcellsummit.com/http://www.genpol.org/http://www.genpol.org/http://www.genpol.org/http://www.worldstemcellsummit.com/
-
8/12/2019 Registration of Stem Cell Based Clinical Trials
2/7
WORLD STEM CELL REPORT 2009 GENETICS POLICY INSTITUTE 501c3
2010 WORLD STEM CELL SUMMIT DETROIT, MI OCTOBER 4-6, 2010
WWW.WORLDSTEMCELLSUMMIT.COM WWW.GENPOL.ORG16
trial results.23 It sought transparency and accountability in
scientificresearch with human participants.
When proposing human clinical trials, ethics demandsevidence.24
Clinical trial registration aims to meet this ethical duty
byfacilitating access to the details of both clinical trials
protocol and itsinitiation (e.g. objectives, main design features,
sample size, and
tested treatments) and to results of key trial endpoints,25
in acomprehensive and objective manner. As stated in the
introduction,a Clinical Trial Registry (CTR) is a publicly
available database of allhuman interventional clinical trials
regardless of the stage ofdevelopment and of their publication
status.
In order to be effective, clinical trial registries must be
globalcomprehensive, accurate, and publicly accessible. In
addition, accessto a registry should be simple, inexpensive and
appropriate to theintended user population to allow for the
unrestricted disseminationof research results. All these should be
coupled with an independentverification of postings and compliance
mechanisms in order toensure that ethical standards in clinical
practice are respected.
The raison dtre for the establishment of a CTR is to serve as
a
vehicle for knowledge transfer by providing an unbiased public
recordon safety and effectiveness, which in turn is translated in
thefoundation of evidence-based medicine. Moreover, by requiring
theprospective registration of clinical trials at their inception,
theproblem of bias in the body of evidence could be largely
eliminated,as registration in a CTR would occur independently of
the ultimatefindings or publication status of a trial. (Table
1)
to maintain public trust, essential for the feasibility of any
scientificendeavor but even more so in an area that has elucidated
so muchpolitical, social and ethical controversy, that of stem cell
research.
Over the past decades, clinical trials of stem
cell-basedinterventions (e.g. transplantation) have been carried
out usingumbilical cord blood stem cells and autologous adult stem
cells (e.g.
hematopoietic stem cells or blood stem cells) to treat diseases
such asleukemia, lymphoma and several inherited blood disorders.
Thesafety and efficacy of these interventions has been well
established.Conversely, interventions using human embryonic stem
cells andfetal tissue are still in early experimental stages.
Controversial clinicaltrials using these same sources of stem cell
lines are reportedly beingconducted in several countries,12 some
with little scientific or otheroversight and no evaluation of
clinical outcomes and safety.
Indeed, unproven stem cell interventions outside a
clearlyregulated clinical trial are proliferating around the world,
facilitatedby loopholes in several national regulatory systems or
evenencouraged by government support.13 Confusion between
theseunproven interventions and scientifically sound and
rigorously
designed clinical trials puts at risk not only the safety of
researchparticipants, but also damages the integrity of the field
as it erodespublic trust.14 Similar negative effects arise from the
lack oftransparency in disclosing the protocol design and its
outcomes in anumber of legitimate stem cell-based clinical trials
and interventions.
In the field of stem cell research, the prospect of clinical
trialregistration has seldom been explored. This is inspite of a
globalconsensus15 that recognizes the need for prospective
registration of allinterventional trials as a scientific, ethical
and professional imperative(if not a legal obligation) for
scientists, governments and fundingorganizations.16 This duty is
grounded in the fundamental need todisseminate knowledge and
protect and respect research participantsand patients.17
Notwithstanding this consensual duty, a gap between
the number of trials conducted and the number for which results
arepublicly available persists and has been well-documented.18 To
addressthis problem, a wide variety of stakeholders have adopted a
broadrange of approaches.19, 20 They range from policies mandating
clinicaltrial registration as a pre-condition of publication,21 to
the creation ofnational registries* and an International Clinical
Trial RegistryPlatform by the World Health Organization
(WHO).**
Clinical Trial Registration and ItsRaison dtre
The movement towards establishing clinical trials
registrationemerged as a reaction to scandals surrounding
structural flaws in the
clinical trials enterprise22
that ranged from publication bias,regulatory lapses, to secrecy
and intentional misrepresentations of
STEM CELLS, REGENERATIVE MEDICINE, AND SOCIETY
*See for example the following national clinical trial
registries: USA Clinical Trials.gov, Australian New Zealand
Clinical Trials Registry (ANZCTR), Chinese Clinical Trial
Register(ChiCTR), Clinical Trials Registry India (CTRI), German
Clinical Trials Register (DRKS), Iranian Registry of Clinical
Trials (IRCT), Japan Primary Registries Network, The
Netherlands National, Trial Register (NTR), Sri Lanka Clinical
Trials Registry (SLCTR)
**The WHO International Clinical Trials Registry Platform
(ICTRP) overall objective is to ensure that a complete view of
research is accessible to all those involved in health caredecision
making. This will improve research transparency and will ultimately
strengthen the validity and value of the scientific evidence base.
The ICTRP was developed in
collaboration with the International Standard Randomised
Controlled Trial Number (ISRCTN) register, based in the UK, and the
ClinicalTrials.gov registry, based in the US, theICTRP with the aim
to promote consensus regarding international norms and standards in
clinical trial registration. The ICTRP requires that clinical
trials are registered at inception
and proposes that a unique Universal Trial Reference Number be
given to each trial to prevent duplication. The ICTRP is not a
registry itself but a comprehensive search portal for
registries that exist worldwide.
http://www.who.int/ictrp/en/
Table 1: Clinical Trial Registry: Objectives
1. Respect the investigator-participant covenantto contribute to
biomedical knowledge by
making trial methods and findings public.2. Strengthen
protection and respect for research
participants
3. Foster accountability and transparency withregard to global
standards for ethical research.
4. Provide a foundation for evidence-basedmedicine
5. Serve as a vehicle for knowledge transfer byproviding an
unbiased public record on safetyand effectiveness
6. Advance innovation and acceleration of
research practice in clinical therapies
http://www.worldstemcellsummit.com/http://www.genpol.org/http://www.genpol.org/http://www.genpol.org/http://www.worldstemcellsummit.com/
-
8/12/2019 Registration of Stem Cell Based Clinical Trials
3/7
WORLD STEM CELL REPORT 2009 GENETICS POLICY INSTITUTE 501c3
2010 WORLD STEM CELL SUMMIT DETROIT, MI OCTOBER 4-6, 2010
WWW.WORLDSTEMCELLSUMMIT.COM WWW.GENPOL.ORG17
Transplantation of cells derived from pluripotent stem cells
isstill a highly innovative practice and consequently, a great
degree ofuncertainty exists with respect of weighing the
benefit/risk ratio forsuch interventions. The advantages that
pluripotent stem cells possessin terms of their capacity for
self-renewal and differentiation; arepaired with the immense
challenge of establishing mechanisms toadequately control them in
order to prevent negative effects such as
Furthermore, it is the goal of a CTR to enable to carry out
meta-analyses. Meta-analyses or quantitative overviews are the
primarymeans by which the safety and efficacy of new drugs and
otherinterventions are assessed. Often individual clinical trials
lackadequate statistical power to reliably adjudicate between
alternativetreatments strategies. It is therefore necessary in many
instances to
conduct meta-analyses or quantitative overviews of all relevant
trialsin order to draw conclusions about the efficacy of a
particulartreatment or procedure.26 To this date, the results of
meta-analysisstudies have improved clinical practice in many areas
of medicine.27
Stem cell research plays a key role in the increasingly
promisingarea of regenerative medicine, showing potential to
improve ourability to treat, prevent and cure disease by providing
a potentialunlimited source of cells for organ transplantation and
therapies.Stem cell research could also provide a successful model
system fordrug discovery, including the development of new testing
methodsfor efficacy, toxicity and safety. It will improve our
understanding ofthe processes of human cell differentiation and
development, withpossible positive consequences for the treatment
of diseases such as
cancer. Finally, research using induced pluripotent cell (IPs
cells) andsomatic cell nuclear transfer (SCNT) will create
patient-and-diseasespecific stem cell lines for research purposes
and eventually, for safeand effective therapies.28
STEM CELLS, REGENERATIVE MEDICINE, AND SOCIETY
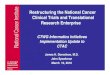
Table 2
The registration of all interventional trials is ascientific,
ethical and moral responsibility. WHOInternational Clinical Trials
Registry Platform (ICTRP)
A Snap-shot of Stem Cell-based Clinical Trialavailable through
WHOs ICTRP*
Key Word Number of Trials
Stem Cells 1837Hematopoietic Stem Cells 470Autologous Stem Cells
19Cord Blood Stem Cells 03Embryonic Stem Cells 03Adult Stem Cells
18Fetal Stem Cells 0IPs 03*The search was conducted on June 15th
2009.
http://www.who.int/ictrp/en/
tumor formation, excess proliferation, inappropriate
differentiation,improper localization, among other serious adverse
events. Thepotential for significant risks arising from these
interventions aredistinct from all other therapies. Accordingly,
they warrant particularscrutiny with regards to their protocol
design, conduct and analysis(e.g. type of cell, disease or
condition concerned, control cases,
participant enrollment, ethics approval, outcomes, follow-up,
etc.); tosay nothing about evidence of safety and efficacy.29 On
this latterpoint, the recommendations issued in ISSCR`s Clinical
Translationguidelines are illustrative. The guidelines call on
researchers topublish positive results, negative results, and
adverse events and thuspromote transparency, to prevent others from
being subjected tounnecessary risk in future clinical research and
to ensure thedevelopment of clinically effective and competitive
stem-cell basedtherapies.30
The impact of trial registration of cell-based
clinicalinterventions should not be taken lightly. The continuous
andcomprehensive registration of these interventions could
significantlyimpact the foundation of evidence-based medicine, and
even shape
clinical practice by supporting the translation of research from
thebench to the bedside through the development of best
practiceguidelines. To draft best practice guidelines such as those
adoptedby ISSCR -, professional organizations rely on the body of
scientificevidence; which in turn outlines the current standard of
careSimilarly, policy-makers often rely on such evidence when
draftinglaws and regulations dealing with scientific and medical
practice. Asa result, clinical trial registration could have a
great impact in shapingnot only public policy, but also medical or
product liability. The latteris of particular importance given the
already mentioned proliferationof scientifically unproven and
ethically problematic cell-basedinterventions.
The principle of benefit sharing provides an additional
justification for advocating for the prospective registration of
clinicaltrials. Clinical trials contribute to building societys
collectiveknowledge. The financial investments committed by
sponsors ofclinical research especially when obtained by public
funders demand for the resulting knowledge to be shared.31 by
informingpriority setting and the planning of future studies,
identifying trendsand gaps and avoiding unnecessary duplication
(which must bedistinguished from appropriate replication) of
research.
Of equal importance are the objectives of respecting
theinvestigator-participant covenant to contribute to
biomedicalknowledge by making trial methods and outcomes public.
Mostoften, the participation of healthy volunteers in a clinical
trial takesplace because such individuals believe they are
contributing to thegeneration of medical knowledge. However, when
the knowledgegained is never transferred, the trust between
investigators, researchparticipants and the public at large is
breached.
Fostering accountability and transparency with regard to
globalstandards for ethical research is also a goal of clinical
trial registration
A fundamental tenet of research ethics is respect for autonomy.
Forresearch participants to be respected as autonomous agents, they
mustprovide free, voluntary and informed consent. The latter can
only beachieved by publicly disclosing the body of evidence as
pertains totrial findings (inconclusive, negative or positive),
thus making explicit
http://www.worldstemcellsummit.com/http://www.genpol.org/http://www.genpol.org/http://www.genpol.org/http://www.worldstemcellsummit.com/
-
8/12/2019 Registration of Stem Cell Based Clinical Trials
4/7
WORLD STEM CELL REPORT 2009 GENETICS POLICY INSTITUTE 501c3
2010 WORLD STEM CELL SUMMIT DETROIT, MI OCTOBER 4-6, 2010
WWW.WORLDSTEMCELLSUMMIT.COM WWW.GENPOL.ORG18
STEM CELLS, REGENERATIVE MEDICINE, AND SOCIETY
the current standard of care .This public record empowers
researchparticipants, enabling them to make informed decisions,
especially
with respect to the balancing of the benefits and risks of
participation.It further mitigates the chances of therapeutic
misconception.Strengthening protections for research participants
in early stem cell-based clinical trials is necessary given the
highly innovative nature of
these interventions, and the likelihood that recruitment of
researchparticipants would be done from the most vulnerable
populations(e.g. the severely ill).32
Clinical Trial Registration: Challenges
At the present time, registration of clinical trials is
generallyvoluntary, making compliance mechanisms difficult to
enforce.However, some national jurisdictions and international
institutionspolicies have adopted policies making registration a
compulsoryrequirement (e.g. USA, India, Australia, Argentina,
EuropeanCommission, etc.). Unlike the World Health Organizations
ClinicalTrial Platform, which is based on voluntary registration,
theInternational Committee of Medical Journal Editors (ICMJE)33
mandates that any manuscript detailing clinical trial findings
must berecorded in a publicly accessed registry before it can be
published.The ICMJE, an organization which represents eleven
renownedmedical journals, has thus taken the initiative to prevent
publicationbias while giving researchers an incentive to register
their trials.
In the stem cell research context, as previously stated, the
ISSCRstopped short of calling for mandatory clinical trial
registration of allstem cell-based clinical trials. It opted
instead for calling for thepublication of research findings via
scientific conferences and peer-reviewed journals, thus confining
to a certain extent* thedissemination of knowledge to professional
circles. The timelypublication of research findings is particularly
important in a rapidlyevolving field that has elicited so much
hope, hype and polarizedpolitical, social and ethical debates.
Dissemination of researchfindings in scientific circles (e.g.
conference, journals) and trialregistration should not be
interpreted as excluding requirements butrather as having a
complementary role. A clinical trial registry ifadequately designed
targets not only the scientific audience but alsoto the lay public,
thus making information available to a wideraudience.
The success of a clinical trial registry relies on its ability
to meetthe needs of the primary intended users, patients and other
membersof the public. But ultimately it depends on a willingness to
contributeto a joint enterprise for the common good.34 In order to
ensurecompliance, institutional review boards should require
clinical trial
registration as a condition of approval35
and so institutionalresponsibility would be established.Aside
from implementing compliance mechanisms, the
auditing, monitoring and oversight of existing registries are
additionaldifficulties that must be overcome in order for clinical
trialregistration to be effective. Similarly, to maintain trust,
safeguards toprotect privacy and confidentiality of research
participants andproprietary information should be established. A
registry includes
extensive data coming from multiple sources; it requires
frequentupdating to remain thorough and correct. Therefore,
verificationprocedures must be enforced to ensure accuracy and
qualityassurance.
It is argued that clinical trials should be registered at all
phases,even at inception, in order to ensure full disclosure.
Without the
registration of clinical trials at all phases, it would be
impossible eitherto know adverse reactions or to assess safety and
efficacy. Theregistration of early-phase clinical trials would
ensure then that therisks related to new interventions or
treatments are publicly known,36
thus preventing ineffective or harmful interventions from
continuingIf clinical trials are registered only after they have
been completed andfound to be favourable, or published, publication
bias will result.Furthermore, requiring that clinical trials be
registered at inception
would prevent the loss of potentially valuable scientific
informationdue to early trials that are often terminated for
economic reasons. 37
Particular challenges relate to the design and scope of a
clinicaltrial registry for stem cell lines, especially concerning
theestablishment of a minimum data set as it would require
agreement
on standard data elements. A mandatory, minimum data set
fosterstransparency and accountability by providing a comprehensive
andtransparent (non-promotional) posting of methodology and
resultsThe currency and accuracy of the information in a
prospectiveregistry is of paramount importance. In the case of stem
cell clinicaltrials, data must include information regarding the
origin of thehuman stem cell lines, their derivation and culture
methods andconditions, traceability requirements as well as their
bankingprocedures.
Clinical trial registration still faces unyielding resistance
from thepharmaceutical and biomedical industries. As these
industriesaccount for the majority of clinical trials sponsors, it
is essential thatthese industries participate and comply with
registration and
publication standards. Their reluctance steams on the alleged
adverseeffects of trial registration on their intellectual property
rightscommercial or academic competitive advantage; as well as on
thedangers of international piracy and/or the disclosure of trade
secrets.3
All of these factors could negatively target their
therapeuticdevelopment and regulatory strategies, potentially
damaging investorinterests and stock value.39
The pharmaceutical and biotechnological industries concedethat
the dissemination of knowledge and the protection of the rightsand
the safety of patients (and research participants) should
triumphover concerns for the confidentiality of proprietary
interests, theprotection of academic freedom and the exclusivity of
research ideas.40
However, they argue that clinical trial registration would not
have theeffect of increasing safety or protections for
researchparticipants/patients nor of diminishing publication bias.
It remainsto be seen if a balance between those conflicting
interests could beachieved in order to serve the public interest.
As pointed out byRennie, the financial cost of an effective,
independent andtransparent clinical trial register would amount to
a tiny fraction ofthe costs of the trials themselves, or the costs
of not knowing their
*ISSCR published along to the Guidelines for the Clinical
Translation of Stem Cell, a Patient Handbook on Stem Cell Therapies
(December 2008), providing valuable scientificinformation for
patients and their doctors evaluating a stem cell therapy.
http://www.worldstemcellsummit.com/http://www.genpol.org/http://www.genpol.org/http://www.genpol.org/http://www.worldstemcellsummit.com/
-
8/12/2019 Registration of Stem Cell Based Clinical Trials
5/7
WORLD STEM CELL REPORT 2009 GENETICS POLICY INSTITUTE 501c3
2010 WORLD STEM CELL SUMMIT DETROIT, MI OCTOBER 4-6, 2010
WWW.WORLDSTEMCELLSUMMIT.COM WWW.GENPOL.ORG19
STEM CELLS, REGENERATIVE MEDICINE, AND SOCIETY
results, while the personal costs of allowing the present
chaotic systemto continue are incalculable.41
Conclusion
History has taught us many cautionary lessons of
significantharms arising from moving forward with a scientific
field of inquiry
without transparency and accountability. These harms go
beyondphysical harms to research participants, but they extend to
ethical andmoral ones that reach society and science itself,
eroding public trust.Scientific research holds out much promise for
potential socialbenefits for funders, research participants and
society in general.However, this promise cannot be realized if
research findings areconcealed, selectively reported or
misrepresented. The globalconsensus declaring the prospective
registration of clinical trials ascientific, ethical and
professional obligation is a major milestone.
Yet, this recognition is insufficient in the absence of
compliance. To
date, voluntary schemes calling for publication and registration
havemet with limited success.
Prospective disclosure of research findings and clinical
trialresults fosters innovation and scientific rigor. As stem cell
researchrapidly evolves, bringing us one step closer to the clinic,
the time isripe to remind us all of the ethical duties we owe to
society, to science
and to ourselves. Hence, this renewed call for making clinical
trialregistration a mandatory requirement.
Acknowledgements
The author thanks the Canadian Stem Cell Network and
theInternational Stem Cell Forum for their funding support. The
author isespecially grateful to Maya Shukairy for providing expert
researchassistance and valuable comments. The opinions are those of
the authoralone.
Rosario Isasi is currently a Researcher theCentre of Genomics
and Policy, Faculty ofMedicine, Department of HumanGenetics, Mc
Gill University.
Her research interests intersect publichealth, ethics, law and
science. She hasparticular expertise in the area of
comparative law and international governance issues
surroundingregenerative medicine and stem cell research. She has
published inScience, Human Reproduction, Cell Stem Cell, Stem Cell
Research,
AJLM, JLME among other journals.
Closely related to her academic work is her role as a policy
adviser togovernment, professional and international bodies, such
as theUnited Nations, where she played an active role in the
adoption of
the UN Declaration on Human Cloning. Most recently, she
hascontributed to the Bioethics Education Project of the Royal
Collegeof Physicians and Surgeons of Canada.
Rosario Isasi is the Academic Secretary of the International
StemCell Forum Ethics Working Party and a member of the
HinxtonGroup, an international Consortium on Stem Cells, Ethics
andLaw. She is also a member of the Legal and Human Rights
AdvisoryBoard of the Genetics Policy Institute; and member of the
advisoryboard of Global Lawyers and Physicians, a
transnationalprofessional association of lawyers and physicians
working together
to promote human rights and health.
She holds her J.D. from the Pontifical Catholic University of
Peru,where she practiced corporate and health law. She received
herMasters of Public Health from Boston University, USA.
Rosario M. Isasi, J.D., M.P.H.
References1. Thomson, J.A., Itskovitz-Eldor, J., Shapiro, S.S.,
et al. (1998).
Embryonic stem cell lines derived from human blastocysts.
Science,282, 1145-1147.
2. Ohnuki, M., Takahashi, K., & Yamanaka, S. (2009).
Generation and
characterization of human induced pluripotent stem cells.
CurrProtoc Stem Cell Biol, 9, 4A.2.1-4A.2.25.
3. International Society for Stem Cell Research. Guidelines for
theClinical Translation of Stem Cells. (December 3, 2008).
4. World Medical Association. Declaration of Helsinki:
EthicalPrinciples for Medical Research Involving Human
Subjects.(Amended October 2008).
5. Bongso, A., Fong, C-Y., & Gauthaman, K. (2008). Taking
Stem Cellsto the Clinic: Major Challenges. Journal of Cellular
Biochemistry,105, 1352-1360.
6. Amariglio, N., Hirshberg, A., et. al. (2009). Donor-Derived
BrainTumor Following Neural Stem Cell Transplantation in an
AtaxiaTelangiectasia Patient. PLOs Medicine, 6(2), 0222-0231.
7. Lo, B., Kriestein, A., & Grady, D. (2008). Clinical
Trials in Stem Cell
Transplantation: Guidelines for Scientific and Ethical Review.
ClinicaTrials, 5, 517-522.
8. Geron Corporation (2009). Worlds First Clinical Trial of
HumanEmbryonic Stem Cell Therapy Cleared. Regen Med, 4(2), 161.
9. International Society for Stem Cell Research. Guidelines for
theClinical Translation of Stem Cells. (December 3, 2008).
10. World Medical Association. Declaration of Helsinki:
EthicalPrinciples for Medical Research Involving Human
Subjects.(Amended October 2008).
http://www.worldstemcellsummit.com/http://www.genpol.org/http://www.genpol.org/http://www.genpol.org/http://www.worldstemcellsummit.com/
-
8/12/2019 Registration of Stem Cell Based Clinical Trials
6/7
WORLD STEM CELL REPORT 2009 GENETICS POLICY INSTITUTE 501c3
2010 WORLD STEM CELL SUMMIT DETROIT, MI OCTOBER 4-6, 2010
WWW.WORLDSTEMCELLSUMMIT.COM WWW.GENPOL.ORG20
STEM CELLS, REGENERATIVE MEDICINE, AND SOCIETY
11. Goodyear, M.D., Lemmens, T., Sprumont, D., et.al. (2009).
The FDAand the Declaration of Helsinki. BMJ, 338(7704),
1157-58.
12. Kiatpongsan, S., & Sipp, D. (2009). Monitoring and
RegulatingOffshore Stem Cell Clinics. Science, 323, 1564-65.
13. MacReady, N. (April 2009). Special Report: The Murky Ethics
ofStem-Cell Tourism. The Lancet,10, 317-18.
14. Jayaraman, K. (June 2009). Indias First True Stem Cell
Trials. NatureBiotechnology. 27(6): 498.
15. Sim I. Trial Registration for Public Trust: Making the Case
forMedical Devices. J Gen Inter Med(2007) 23(Suppl 1):64-68.
16. Isasi, R., Nguyen, T. M. (2008). The rationale for a
registry ofclinical trials involving human stem cell therapies.
Health Law Rev,16(2), 56-68.
17. I. Chalmers, Underreporting research is scientific
misconduct(1990) 263 JAMA 1405.
18. Zarin D. A., Tse T. Moving Towards Transparency of Clinical
Trials.Science (March 2008) 319:1340-42.
19. Karmela Krle_a-Jeri_ et al., eds., Principles for
internationalregistration of protocol information and results from
human trials ofhealth related interventions: Ottawa Statement (part
1) (2005) 330BMJ 956.
20. International Federation of Pharmaceutical Manufacturers
andAssociations, Joint Position on the Disclosure of Clinical
TrialInformation via Clinical Trial Registries and Databases
(November2008).http://clinicaltrials.ifpma.org/fileadmin/files/pdfs/EN/Revised_Joint_Industry_Position_Nov_2008.pdf
21. International Committee of Medical Journal Editors.
UniformRequirements for Manuscripts Submitted to Biomedical
Journals:Writing and Editing for Biomedical Publication (October
2008)http://www.icmje.org/icmje.pdf
22. Wilson, J.M. (May 2009). A History Lesson for Stem Cells.
Science,
324, 727-28.23. Isasi, R., & Nguyen, T.M. (2008). The
rationale for a registry of
clinical trials involving human stem cell therapies. Health Law
Rev,16(2), 56-68.
24. Scott, C.T. (December 2008). Weighing Risks and Rewards en
Routeto the Clinic. Nature Reports Stem
Cells,doi:10.1038/stemcells.20008.158
25. Zarin, D.A., & Tse, T. (March 2008). Moving Towards
Transparency ofClinical Trials. Science,319, 1340-42.
26. Tumber, M.B., & Dickersin, K. (2004). Publication of
Clinical Trials:Accountability and Accessibility. J Intern Med,
256, 271.
27. Alexa, T, & Mc Cray (2000). Better Access to Information
aboutClinical Trials. Ann Intern Med, 133, 609.
28. Bongso, A., Fong, C-Y., & Gauthaman, K. (2008). Taking
Stem Cellsto the Clinic: Major Challenges. Journal of Cellular
Biochemistry,105, 1352-1360.
29. Lo, B., Kriestein, A., & Grady, D. (2008). Clinical
Trials in Stem CellTransplantation: Guidelines for Scientific and
Ethical Review. Clinica
Trials, 5, 517-522.30. Hyun, I., Lindvall, O., hrlund-Richter,
L., Cattaneo, E. et. al. (2008).
New ISSCR Guidelines Underscore Major Principles for
ResponsibleTranslational Stem Cell Research. Cell Stem Cell, 3,
607-610.
31. Krle_a-Jeri_, K., et al. (2005). Principles for
international registrationof protocol information and results from
human trials of healthrelated interventions: Ottawa statement (part
1). BMJ, 330, 956.
32. Sun-Wei Guo, Lone Hummelshoj, David L. Olive, et. al. A call
formore transparency of registered clinical trials on
endometriosis.Human Reproduction 2009 24(6):1247-1254.
33. International Committee of Medical Journal Editors.
UniformRequirements for Manuscripts Submitted to Biomedical
Journals:Writing and Editing for Biomedical Publication (October
2008)
34. Alexa, T., McCray & Nicholas, C. (2007). Design
andImplementation of a National Clinical Trials Registry. J Am
MedInform Assoc, 7, 313.
35. Levin, L.A., & Gage Palmer, J. (2007). Institutional
Review BoardsShould Require Clinical Trial Registration. Arch
Intern Med, 167(15),1577-80.
36. Alastair Wood, J.J. & J. Darbyshire (2006). Injury to
researchvolunteers the clinical research nightmar. N Engl J Med,
354,1869.
37. Dimasi, J.A. (2001). Risks in new drug development:
approvalsuccess rates for investigational drugs. Clin Pharmacol
Ther, 69,297.
38. Ida Sim et al., (2006). Clinical trial registration:
transparency is thewatchword. Lancet 367, 1631.
39. Somberg, J. (2003). Clinical Trials Registries. Editorial,
Am J Ther,10, 309.
40. International Federation of Pharmaceutical Manufacturers
andAssociations, Joint Position on the Disclosure of Clinical
TrialInformation via Clinical Trial Registries and
Databases(November 2008). Available
at:http://clinicaltrials.ifpma.org/fileadmin/files/pdfs/EN/Revised_Joint_Industry_Position_Nov_2008.pdf
41. Drummond, R. (2004). Trial Registration: A Great Idea
SwitchesFrom Ignored To Irresistible. JAMA, 292, 1359.
References (continued)
http://www.worldstemcellsummit.com/http://www.genpol.org/http://www.genpol.org/http://www.genpol.org/http://www.worldstemcellsummit.com/
-
8/12/2019 Registration of Stem Cell Based Clinical Trials
7/7
WORLD STEM CELL REPORT 2009 GENETICS POLICY INSTITUTE 501c3
2010 WORLD STEM CELL SUMMIT DETROIT, MI OCTOBER 4-6, 2010
WWW.WORLDSTEMCELLSUMMIT.COM WWW.GENPOL.ORG22
STEM CELLS, REGENERATIVE MEDICINE, AND SOCIETY
n March 9, 2009 President Barack Obamasigned an Executive Order
expandingfederal funding for research using
embryonic stem cells in a White House signingceremony packed
with legislators, scientists, andpeople who have suffered from a
range ofdiseases and medical conditions that couldbenefit from the
research. The Presidents
executive order was a major milestone in the 10-year effort by
those patients, scientists,academics, and others who have argued
insupport of a broader federal stem cell policy.1
In some ways, the most telling aspect of the ceremony was
thatwhen President Obama signed the Executive Order,
numerousmembers of Congress were in attendance. Their presence
signaled asignificant shift in public opinion regarding the use of
federal fundingfor embryonic stem cell research; further, it
demonstrated theattitudinal changes regarding stem cell science
that have taken placesince 1998, when embryonic stem cells were
first derived.
Today, for many Americans, stem cell science is viewed
aspotentially beneficial not just for people suffering from
disease
but in maintaining the countrys prominence and preeminence
inscientific leadership. In a remarkably short timeframe, stem
cellscience has made the unusual transformation from a non-issue to
apolitical hot button and to an issue that transcends politics.
Background
Embryonic stem cells were first discovered in 1998 by Dr.
JamieThomson of the University of Wisconsin and Dr. John Gearhart
ofthe Johns Hopkins University.2, 3 While widely applauded for
itspotential in the scientific community, their discoveries very
quicklyset off a firestorm affecting researchers, ethicists,
politicians and, mostimportantly, patients in the United States
(US) and around the
world. In fact, the first series of congressional hearings on
the sciencefollowed quickly, beginning in January 1999, when the
SenateCommittee on Health, Education, Labor, and Pensions
convenedsessions involving a series of top researchers and
ethicists. 4
What became clear at the outset was that most US policymakersdid
not have an understanding of stem cell research and therefore
were uncomfortable with the concept. Almost immediately,
thesource of embryonic stem cells became a key issue in the
discussionand debate and initially there were broad
misunderstandings aboutthe origin of stem cells with many assuming
the issue to be
Oassociated with abortion.
At the time, relatively few legislators had a clear
understandingof the reality; the stem cells at the center of the
issue were cells derivedfrom embryos created for in vitro
fertilization (IVF) procedures. Infact, the cells in question were
not going to be used and were slatedto be discarded.
More often than not, the creation of embryonic stem cells
waserroneously linked to abortion, and the corresponding
political,moral, and religious issues that it entailed. To compound
theproblem, there were a handful of legislators and others that
might
have understood that abortion was not tied to stem cells, but
did nothave a detailed understanding of or were uncomfortable with
the IVFprocess itself. As a result, the immediate political
reaction to the 1998Thomson/Gearhart discoveries leaned toward a
ban on the research.
The Role of Patient Advocacy
In response to initial fears and negative reactions (often based
onmisunderstanding), an organized effort was launched on the part
ofpatient advocacy groups to delay any potential federal ban
onembryonic stem cell research. The aim was to provide education
onthe role of stem cells, the science, and their potential for
therapies andcures for leading conditions. In addition, time was
needed to enablediscussion and debate related to surrounding
ethical and religiousimplications. This effort started with
Patients Cure, originally formedby Dan Perry, who was the Executive
Director of the Alliance for
Aging Research. Patients Cures major focus was to slow
themomentum of any amendments that might surface in
Congressrestricting federal funding and support for stem cell
research.
Patient advocacy in the area of stem cell research emerged
amongthe campaign promises made by then Presidential candidate
George
W. Bush, who pledged to impose a ban on federal funding
forembryonic stem cell research. Once elected, it was clear that a
largerscale and more comprehensive effort would be required to
preservefederal funding for the research if not the ability to
conduct stemcell research itself.
Formation of the Coalition for theAdvancement of Medical
Research (CAMR)
The result was the creation of the Coalition for theAdvancement
of Medical Research (CAMR). Today, CAMRcomprises more than 100
nationally recognized patient organizations,universities,
scientific societies, and foundations, and conductsadvocacy and
education outreach focused on developing bettertreatments and cures
for people with life-threatening illnesses anddisorders.
Federal Funding of Stem CellResearch: Past, Present and FutureBy
Lawrence A. Soler, J.D.
http://www.worldstemcellsummit.com/http://www.genpol.org/http://www.genpol.org/http://www.genpol.org/http://www.worldstemcellsummit.com/