Embed Size (px)
Citation preview
Region 2 Annual Fall instituteJohn W. Gahan Jr.
1New York State Department of Health
AgendaPre-Reform Rates
Updates/timeframesReform Rates
4/1/201010/1/2010 – Blended Rates
Potentially Preventable Readmissions (PPR’s)New Psych MethodologyFMAP Payment ReductionsDSH Audit Update and ProcessQuestions and Answers
2New York State Department of Health
Pre-Reform RatesInitial 2009 rates:
General items included Capital 2007 volume, etc. Worker Retention reconciliation
Updates to 2009 rates2008 and 2009 volume
Including LOS relief and added bed appeals2008 and 2009 actual capitalWorker Retention reconciliation – 2008 and 2009
Retro publicationOld appeals
3New York State Department of Health
Reform Rates4/1/2010 Rates:
Updated statewide base price for some minor corrections
New Transition amounts Divided by 2008 paid claims
Workers Comp/No Fault Rates trended 2010-11 budget delinked items effective 4/1/2010 Rebasing adjustment in Medicaid rates not
applicable to WC/NF rates ($154.5M)
4New York State Department of Health
Blended Rates effective 10/1/2010
5New York State Department of Health
DOH has established a single statewide base price that combines Medicaid FFS and MC based on updated 2008 data.
The blended base price per discharge will be established based on targeted statewide Medicaid inpatient hospital expenditures from both Medicaid FFS and MC, and the new reform rate variables (i.e. GME, WEF, case mix, etc.)
Phase II – Blend FFS and MC Effective October 1, 2010 and forward
6New York State Department of Health
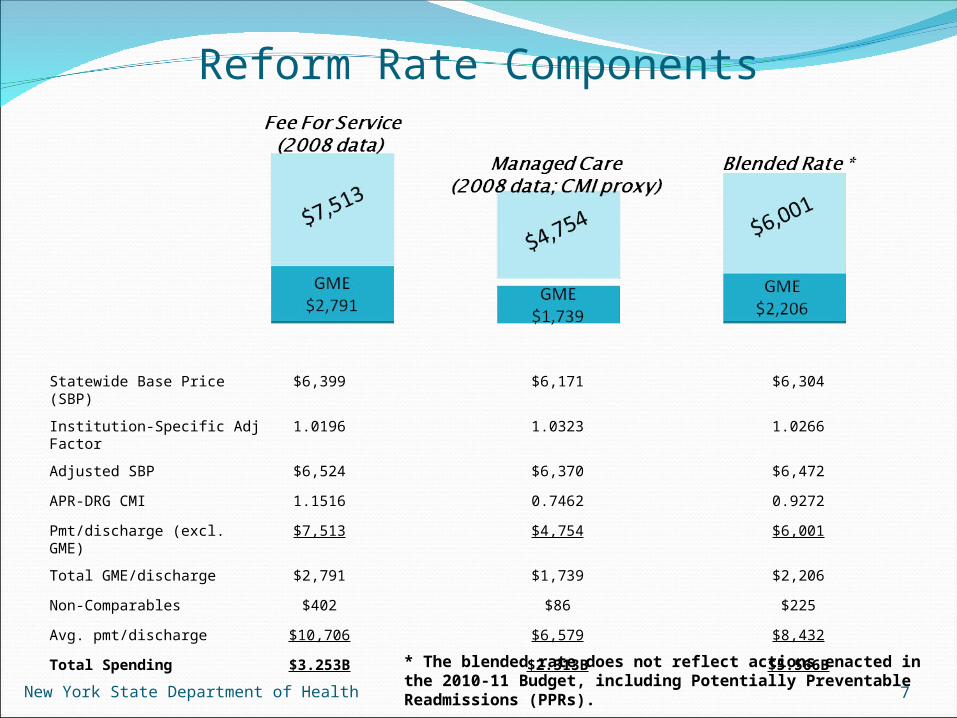
Reform Rate Components
Statewide Base Price (SBP) $6,399 $6,171 $6,304
Institution-Specific Adj Factor
1.0196 1.0323 1.0266
Adjusted SBP $6,524 $6,370 $6,472
APR-DRG CMI 1.1516 0.7462 0.9272
Pmt/discharge (excl. GME) $7,513 $4,754 $6,001
Total GME/discharge $2,791 $1,739 $2,206
Non-Comparables $402 $86 $225
Avg. pmt/discharge $10,706 $6,579 $8,432
Total Spending $3.253B $2.313B $5.566B
7
* The blended rate does not reflect actions enacted in the 2010-11 Budget, including Potentially Preventable Readmissions (PPRs).New York State Department of Health
The blended rate will result in increased FFS savings (from $225M) and increased payments to hospitals related to MC services, based on 2008 utilization (savings will still net to $225M).
$225 million (and the $154 million across-the-board reduction) in gross Medicaid savings will be retained across both FFS and MC sectors and does not “double-up”.
Funds will need to be shifted in the Budget to accommodate this dynamic.
8
Funding Reallocations
New York State Department of Health
A Transition II Pool will be established to provide an additional $150 million over 3 years ($75M/$50M/$25M) to further assist hospitals to adjust operations consistent with state health care priorities and revenue streams.
Additional $37.5M for the period 10/20/10 through 3/31/11
Transition funds will be phased out consistent with Transition Pool I, however, these monies will be reinvested back into the base price.
Allocation of these funds will be consistent with Transition Pool I (setting a threshold floor percentage – 10.45%) based on FFS losses and allocated through FFS claims only.
Hospital Transition II Pool (Continued)
9New York State Department of Health
In year one, the blended base price will be reduced to generate $75M in additional savings.
The new base price will be $6,202 (from $6,304).
Includes public facilities, who were previously excluded from receiving funds from Transition Pool I.
Hospital Transition II Pool (Continued)
10New York State Department of Health
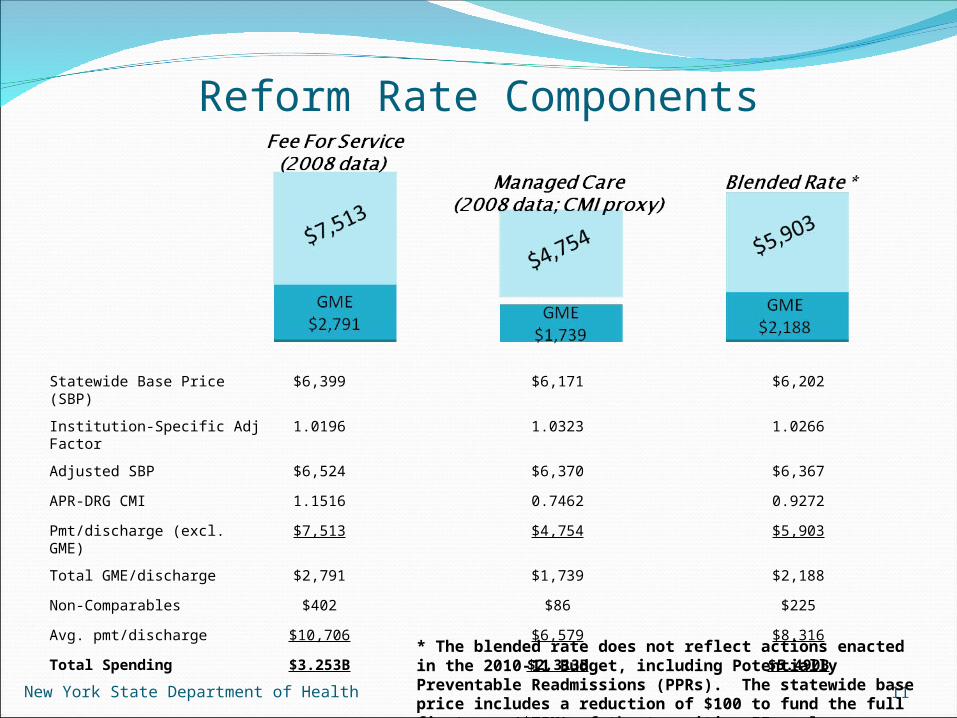
Reform Rate Components
Statewide Base Price (SBP) $6,399 $6,171 $6,202
Institution-Specific Adj Factor
1.0196 1.0323 1.0266
Adjusted SBP $6,524 $6,370 $6,367
APR-DRG CMI 1.1516 0.7462 0.9272
Pmt/discharge (excl. GME) $7,513 $4,754 $5,903
Total GME/discharge $2,791 $1,739 $2,188
Non-Comparables $402 $86 $225
Avg. pmt/discharge $10,706 $6,579 $8,316
Total Spending $3.253B $2.313B $5.490B
11
* The blended rate does not reflect actions enacted in the 2010-11 Budget, including Potentially Preventable Readmissions (PPRs). The statewide base price includes a reduction of $100 to fund the full first yr. ($75M) of the transition II pool.
New York State Department of Health
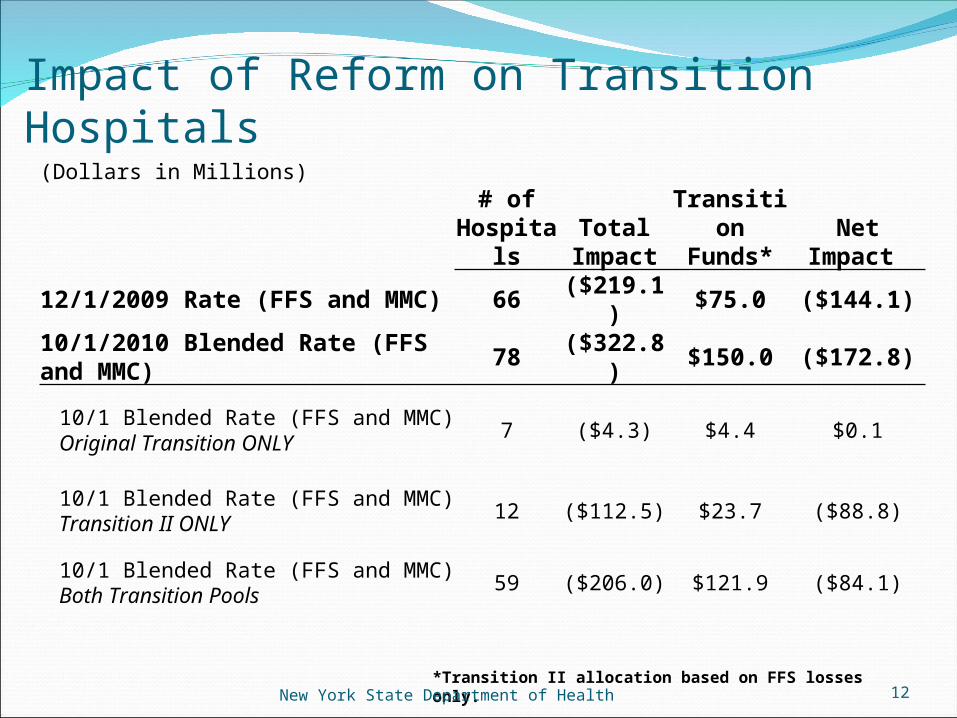
Impact of Reform on Transition Hospitals
12
(Dollars in Millions)# of
HospitalsTotal
ImpactTransition
Funds* Net Impact
12/1/2009 Rate (FFS and MMC) 66 ($219.1) $75.0 ($144.1)
10/1/2010 Blended Rate (FFS and MMC) 78 ($322.8) $150.0 ($172.8)
10/1 Blended Rate (FFS and MMC) Original Transition ONLY 7 ($4.3) $4.4 $0.1
10/1 Blended Rate (FFS and MMC) Transition II ONLY 12 ($112.5) $23.7 ($88.8)
10/1 Blended Rate (FFS and MMC) Both Transition Pools 59 ($206.0) $121.9 ($84.1)
*Transition II allocation based on FFS losses only.New York State Department of Health
A Potentially Preventable Readmission (PPR) is a readmission within 15 days that is clinically related to the initial hospital admission
Excludes behavioral health at the initial admission; major or metastic malignancies; multiple trauma; burns; neonatal; obstetrical; and discharges with a status of “left against medical advice”
Includes readmissions for fee-for-service and Medicaid managed care
Will begin discussions with stakeholders to incorporate behavioral health PPRs beginning 4/1/12
Potentially Preventable Readmissions (10 NYCRR 86-1.37)
13New York State Department of Health
2010-11 Budget requires this proposal to generate $47M in full annual, gross, savings (in 2011-12)
$37.1M related to FFS readmissions; $9.9M related to MMC readmissions
To generate these savings, the following method is used:
Using 2007 data, a risk adjusted model identifies hospital specific “excess readmissions” (observed rate is in excess to the expected rate)
A readmission adjustment factor is computed using the ratio of aggregate payments related to the excess readmissions to the aggregate payments for all non-behavioral health discharges
This adjustment factor is prospectively applied to the applicable hospital’s case payment and per diem rates on discharges beginning 7/1/10; implemented in 10/1/2010 rates.
The reduction % will be applied to the statewide base price, DME, and non-comparables
PPRs - Methodology
14New York State Department of Health
15New York State Department of Health
Background Legislation
A new inpatient psychiatric reimbursement methodology was passed in the 2009-10 Medicaid reform legislation
Implementation date Initially planned for December 1, 2009 The executive budget delayed it to April 1, 2010 Revised start date is October 20, 2010
Task Force The psychiatric payment methodology was developed through a joint
initiative with representatives from DOH, OMH, GNYHA, HANYS Goal
Utilizing a Medicare-like approach, develop a reimbursement strategy to pay more appropriately for inpatient psychiatric admissions and address length of stay
Maintain Budget Neutrality The operating payments for inpatient psychiatric services under the
current system and under the new methodology will be budget neutral Transition
A $25 Million annual investment as a result of rebasing to 2005 costs will be used for transitioning to the new methodology
New York State Department of Health
16
Impetus for Change:Current System’s Weaknesses
New York State Department of Health
17
Cost base is 1981, non-Medicare payers Outdated Inpatient costs attributable to Medicaid patients not
recognizedSame per diem rate throughout the stay
Higher costs for initial work up, and lower costs later in the stay not recognized
No incentives for length of stay reduction (NYS is twice the national average)
Doesn’t recognize different levels of mental health care service provided
Doesn’t recognize observable , systematic cost differences in Office of Mental Health’s priority areas Rural hospitals, adolescents, presence of mental retardation,
and physical comorbiditiesPayments based on hospital-specific costs do not encourage
efficiency
New Methodology:Highlights
New York State Department of Health
18
Applicable to Article 28 exempt psychiatric inpatient hospitals and exempt units
Major constructive change in the way inpatient psychiatric rates are calculated and how Medicaid claims are paid after October 1, 2010
A modernized approach making reimbursement more adequate and equitable
New system will pay for the level of service rendered, address length of stay variance, and will be more consistent with how Medicare reimburses for this service
Inpatient psychiatric per diem rates will be based on 2005 Medicaid operating costs (per statute)
Additional investment of $25M annually over existing inpatient psychiatric expenditures as provided for in the 2009-10 budget to assist hospitals to transition to the new methodology
Transition will gradually be phased into the statewide price over the period 10/20/2010-12/31/2014
Data Overview
New York State Department of Health
19
Legislation requires use of 2005 Medicaid costsICR: Best source for provider costSPARCS: Best source for all-payer case-level data
Basis to match case-level charges to ICRDevelopment of departmental ratios of cost to charges (RCCs)More complete reporting of charges compared to 2005 MMISMore secondary diagnoses reported compared to 2005 MMIS
MMIS: Best source to determine psychiatric casesOne year’s worth of data not reliable enough to estimate systematic determinants of cost
Model Development:Operating Payment Adjustments
New York State Department of Health
20
Facility-level adjustment: WEFTo account for wage differences in hospitals’ labor
marketsFor Oct. 1st: same as acute care Medicaid payment system
ECT rateUse the federal rate in effect during the first half of 2010:
$281Severity of illness:
Based on DRG relative weights Calculated specifically for psychiatric patients Uses hospital-specific relative value (HSRV) method
APR-DRGs to account for four severity levelsConsistent with acute care weight methodology
All other adjustments:Regression based
DRGs for Medicaid Psych Patientswith Cost Estimates, 2005-2006
New York State Department of Health
21
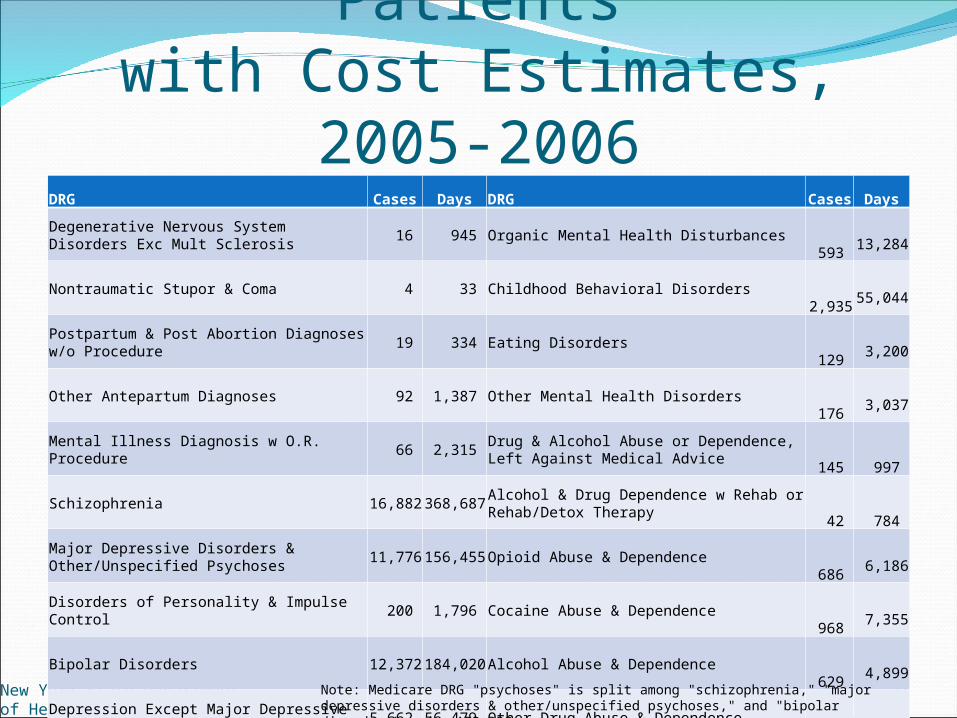
DRG Cases Days DRG Cases DaysDegenerative Nervous System Disorders Exc Mult Sclerosis 16 945 Organic Mental Health Disturbances
593
13,284
Nontraumatic Stupor & Coma 4 33 Childhood Behavioral Disorders 2,935
55,044
Postpartum & Post Abortion Diagnoses w/o Procedure 19 334 Eating Disorders
129
3,200
Other Antepartum Diagnoses 92 1,387 Other Mental Health Disorders 176
3,037
Mental Illness Diagnosis w O.R. Procedure 66 2,315 Drug & Alcohol Abuse or Dependence, Left Against Medical Advice
145
997
Schizophrenia 16,882 368,687 Alcohol & Drug Dependence w Rehab or Rehab/Detox Therapy
42
784
Major Depressive Disorders & Other/Unspecified Psychoses 11,776 156,455 Opioid Abuse & Dependence
686
6,186
Disorders of Personality & Impulse Control 200 1,796 Cocaine Abuse & Dependence 968
7,355
Bipolar Disorders 12,372 184,020 Alcohol Abuse & Dependence 629
4,899
Depression Except Major Depressive Disorder 5,662 56,479 Other Drug Abuse & Dependence 420
3,225
Adjustment Disorders & Neuroses Except Depressive Diagnoses 1,539 12,967 Non-Psychiatric DRGs
209
2,512
Acute Anxiety & Delirium States 541 3,896
Note: Medicare DRG "psychoses" is split among "schizophrenia," "major depressive disorders & other/unspecified psychoses," and "bipolar disorders" under APR-DRG system.
Adjustment Factors for Day Intervals & Interrupted stays
New York State Department of Health
22
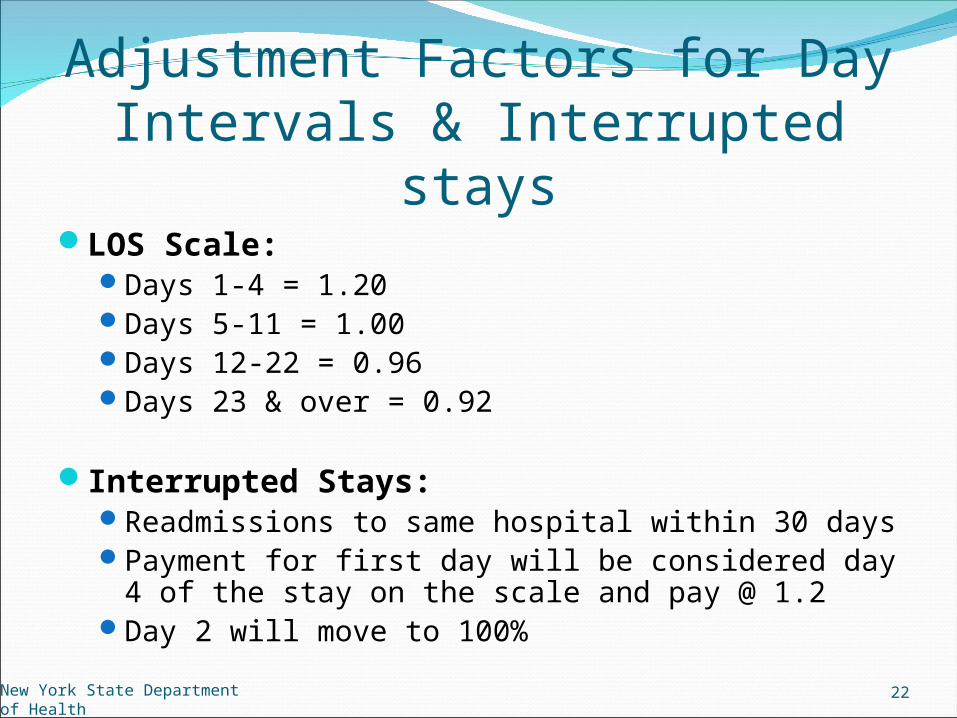
LOS Scale:Days 1-4 = 1.20Days 5-11 = 1.00Days 12-22 = 0.96Days 23 & over = 0.92
Interrupted Stays:Readmissions to same hospital within 30 daysPayment for first day will be considered day 4 of the
stay on the scale and pay @ 1.2Day 2 will move to 100%
Comorbidity Adjustment Factors
New York State Department of Health
23
Mental retardation as a secondary diagnosisAdjustment factor = 1.06
One other medial/physical comorbidityUses ICD-9-CM codes reported on the patient billConsiders secondary diagnoses that are
complicating conditions (CC/Major CC) under the MS-DRG system
Based on hierarchical condition categories (HCCs) used by various Medicare risk-adjustment methodologies
18 comorbidity groupsApplies the highest adjustment factor if there are
more than one comorbidity present
Comorbidity Categories
New York State Department of Health
24
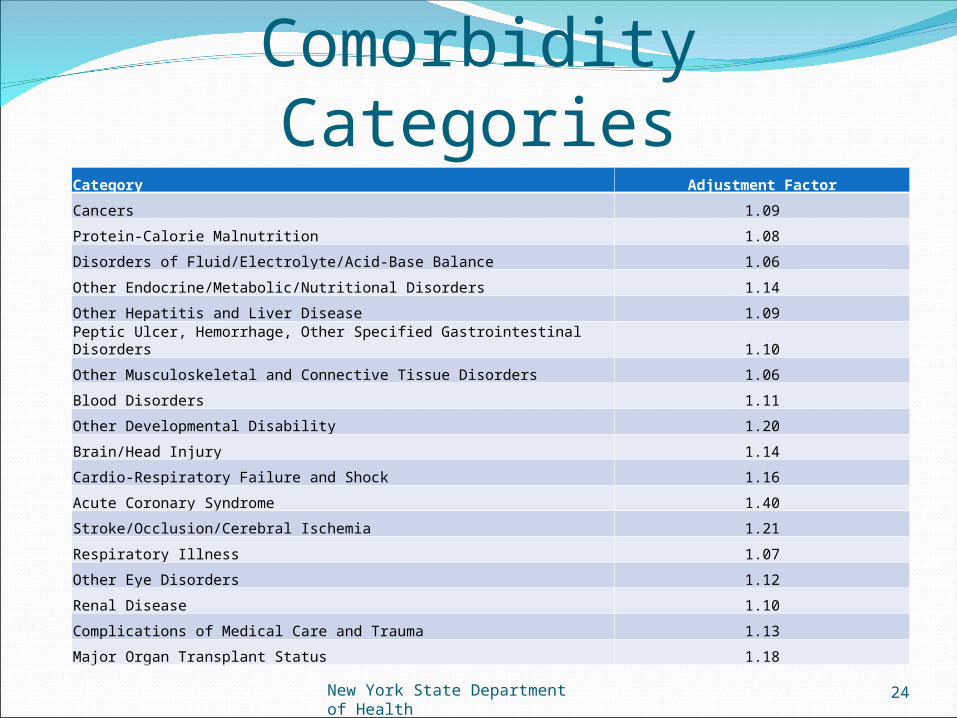
Category Adjustment Factor
Cancers 1.09
Protein-Calorie Malnutrition 1.08
Disorders of Fluid/Electrolyte/Acid-Base Balance 1.06
Other Endocrine/Metabolic/Nutritional Disorders 1.14
Other Hepatitis and Liver Disease 1.09
Peptic Ulcer, Hemorrhage, Other Specified Gastrointestinal Disorders 1.10
Other Musculoskeletal and Connective Tissue Disorders 1.06
Blood Disorders 1.11
Other Developmental Disability 1.20
Brain/Head Injury 1.14
Cardio-Respiratory Failure and Shock 1.16
Acute Coronary Syndrome 1.40
Stroke/Occlusion/Cerebral Ischemia 1.21
Respiratory Illness 1.07
Other Eye Disorders 1.12
Renal Disease 1.10
Complications of Medical Care and Trauma 1.13
Major Organ Transplant Status 1.18
New York State Department of Health
25
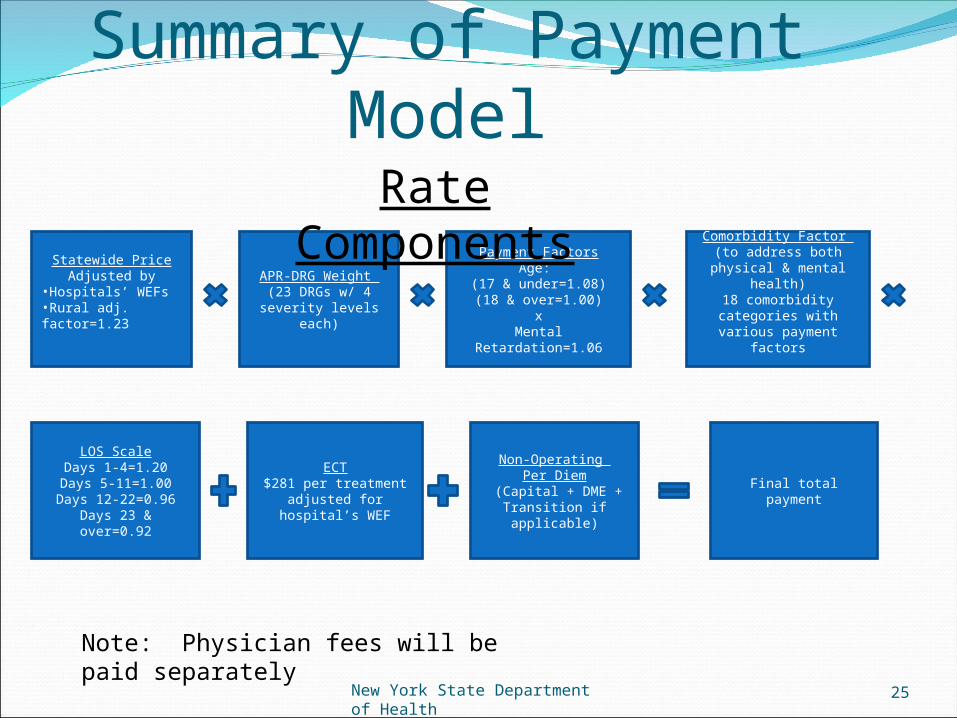
Summary of Payment Model
Statewide Price Adjusted by
•Hospitals’ WEFs•Rural adj. factor=1.23
APR-DRG Weight (23 DRGs w/ 4
severity levels each)
LOS ScaleDays 1-4=1.20
Days 5-11=1.00Days 12-22=0.96
Days 23 & over=0.92
Comorbidity Factor (to address both
physical & mental health)
18 comorbidity categories with various
payment factors
ECT$281 per treatment
adjusted for hospital’s WEF
Final total payment
Non-Operating Per Diem
(Capital + DME + Transition if applicable)
Payment FactorsAge:
(17 & under=1.08)(18 & over=1.00)
xMental
Retardation=1.06
Rate Components
Note: Physician fees will be paid separately
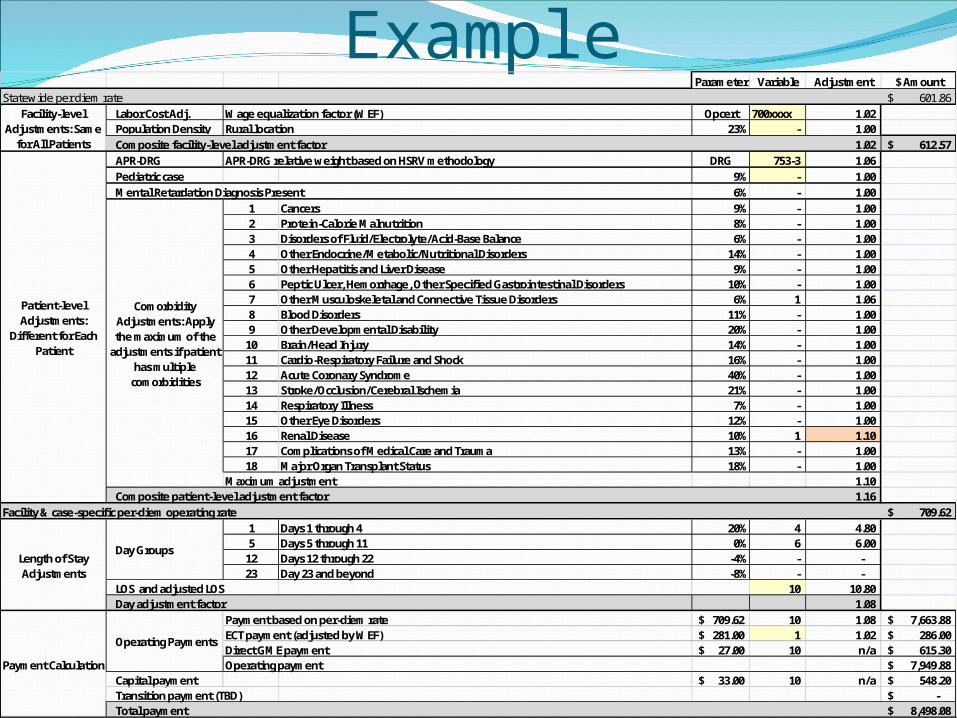
Payment Calculation ExampleParameter Variable Adjustment $ Amount
Statewide per diem rate 601.86$ Labor Cost Adj. Wage equalization factor (WEF) Opcert 700xxxx 1.02 Population Density Rural location 23% - 1.00 Composite facility-level adjustment factor 1.02 612.57$ APR-DRG APR-DRG relative weight based on HSRV methodology DRG 753-3 1.06 Pediatric case 9% - 1.00 Mental Retardation Diagnosis Present 6% - 1.00
1 Cancers 9% - 1.00 2 Protein-Calorie Malnutrition 8% - 1.00 3 Disorders of Fluid/Electrolyte/Acid-Base Balance 6% - 1.00 4 Other Endocrine/Metabolic/Nutritional Disorders 14% - 1.00 5 Other Hepatitis and Liver Disease 9% - 1.00 6 Peptic Ulcer, Hemorrhage, Other Specified Gastrointestinal Disorders 10% - 1.00 7 Other Musculoskeletal and Connective Tissue Disorders 6% 1 1.06 8 Blood Disorders 11% - 1.00 9 Other Developmental Disability 20% - 1.00
10 Brain/Head Injury 14% - 1.00 11 Cardio-Respiratory Failure and Shock 16% - 1.00 12 Acute Coronary Syndrome 40% - 1.00 13 Stroke/Occlusion/Cerebral Ischemia 21% - 1.00 14 Respiratory Illness 7% - 1.00 15 Other Eye Disorders 12% - 1.00 16 Renal Disease 10% 1 1.10 17 Complications of Medical Care and Trauma 13% - 1.00 18 Major Organ Transplant Status 18% - 1.00
Maximum adjustment 1.10 Composite patient-level adjustment factor 1.16
Facility & case-specific per-diem operating rate 709.62$ 1 Days 1 through 4 20% 4 4.80 5 Days 5 through 11 0% 6 6.00
12 Days 12 through 22 -4% - - 23 Day 23 and beyond -8% - -
LOS and adjusted LOS 10 10.80 Day adjustment factor 1.08
Payment based on per-diem rate 709.62$ 10 1.08 7,663.88$ ECT payment (adjusted by WEF) 281.00$ 1 1.02 286.00$ Direct GME payment 27.00$ 10 n/a 615.30$ Operating payment 7,949.88$
Capital payment 33.00$ 10 n/a 548.20$ Transition payment (TBD) -$ Total payment 8,498.08$
Payment Calculation
Operating Payments
Facility-level Adjustments: Same
for All Patients
Patient-level Adjustments:
Different for Each Patient
Comorbidity Adjustments: Apply the maximum of the
adjustments if patient has multiple
comorbidities
Length of Stay Adjustments
Day Groups
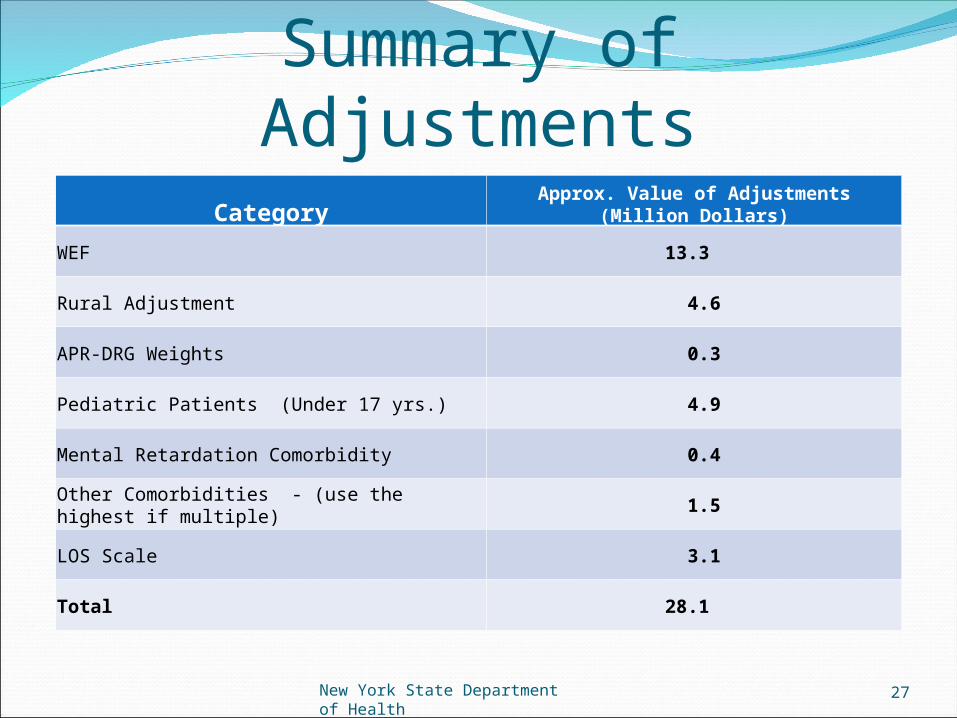
Summary of Adjustments
New York State Department of Health
27
Category Approx. Value of Adjustments (Million Dollars)
WEF 13.3
Rural Adjustment 4.6
APR-DRG Weights 0.3
Pediatric Patients (Under 17 yrs.) 4.9
Mental Retardation Comorbidity 0.4
Other Comorbidities - (use the highest if multiple) 1.5
LOS Scale 3.1
Total 28.1
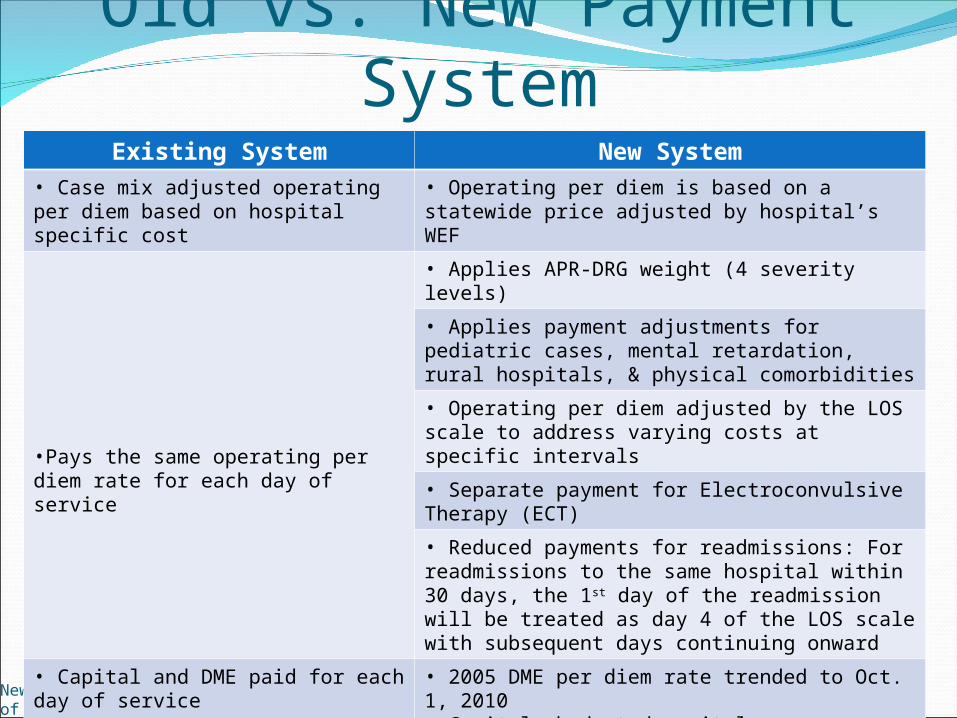
Old vs. New Payment System
New York State Department of Health
28
Existing System New System• Case mix adjusted operating per diem based on hospital specific cost
• Operating per diem is based on a statewide price adjusted by hospital’s WEF
•Pays the same operating per diem rate for each day of service
• Applies APR-DRG weight (4 severity levels)
• Applies payment adjustments for pediatric cases, mental retardation, rural hospitals, & physical comorbidities
• Operating per diem adjusted by the LOS scale to address varying costs at specific intervals
• Separate payment for Electroconvulsive Therapy (ECT)
• Reduced payments for readmissions: For readmissions to the same hospital within 30 days, the 1st day of the readmission will be treated as day 4 of the LOS scale with subsequent days continuing onward
• Capital and DME paid for each day of service
• 2005 DME per diem rate trended to Oct. 1, 2010• Capital: budgeted capital expenses divided by expected days for the rate year
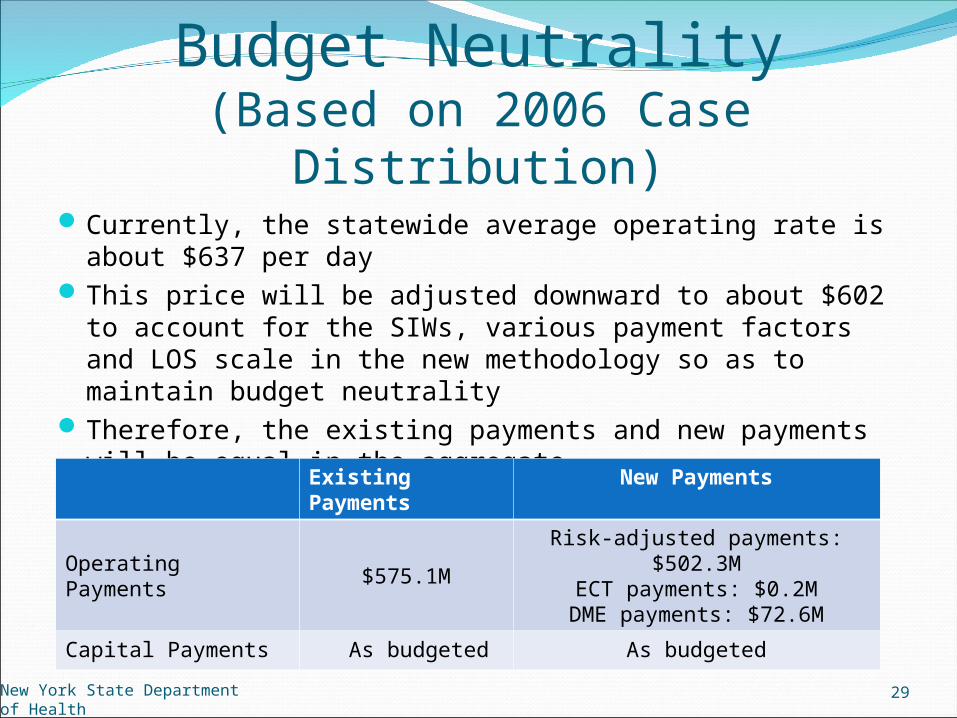
Budget Neutrality(Based on 2006 Case Distribution)
Currently, the statewide average operating rate is about $637 per day
This price will be adjusted downward to about $602 to account for the SIWs, various payment factors and LOS scale in the new methodology so as to maintain budget neutrality
Therefore, the existing payments and new payments will be equal in the aggregate
New York State Department of Health
29
Existing Payments
New Payments
Operating Payments $575.1M
Risk-adjusted payments: $502.3M
ECT payments: $0.2MDME payments: $72.6M
Capital Payments As budgeted As budgeted
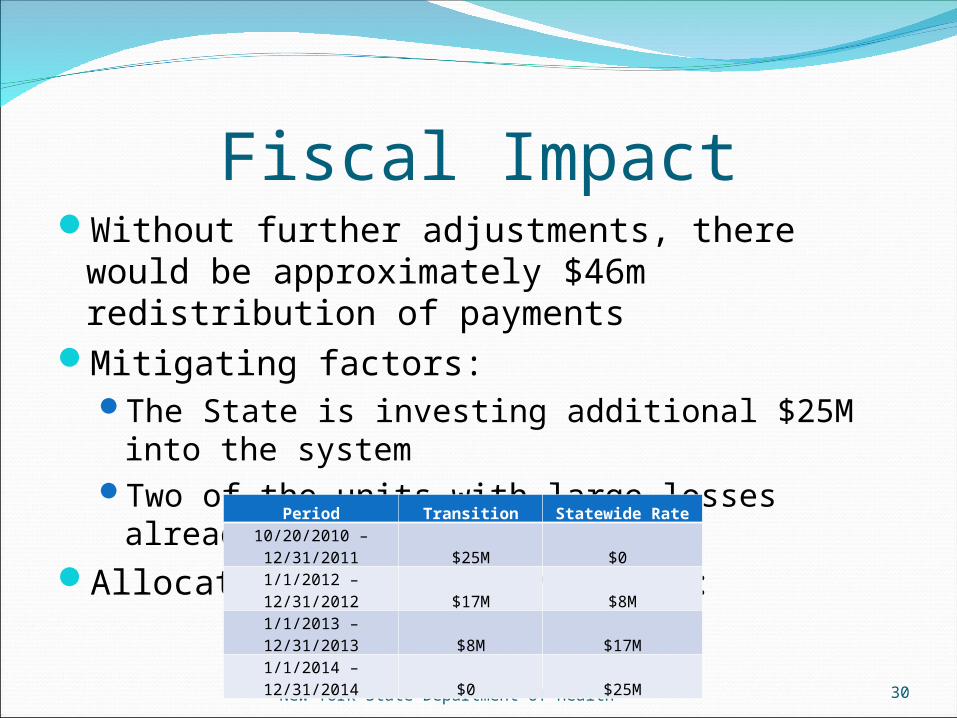
Fiscal ImpactWithout further adjustments, there would be
approximately $46m redistribution of payments
Mitigating factors:The State is investing additional $25M into the
systemTwo of the units with large losses already
closedAllocation of $25M investment:
New York State Department of Health 30
Period Transition Statewide Rate10/20/2010 – 12/31/2011 $25M $0
1/1/2012 – 12/31/2012 $17M $8M
1/1/2013 – 12/31/2013 $8M $17M
1/1/2014 – 12/31/2014 $0 $25M
Distribution Method of$25M Transition Fund
50% (12.5M) based on revenue lossTransition dollars will be allocated such that hospitals
will not lose more than approximately 5% revenue from the existing payments to the new payments in year 1
Same method as acute transition50% (12.5M) based on payment to cost ratio
Transition dollars will be allocated to hospitals whose costs are well above their revenues under the new methodology based on 2006 data
Thresholds for distribution will be published when final statewide rate is determined
Transition funds will be paid through rate adjustments
New York State Department of Health
31
Future UpdatesRebasing
There will be more frequent rebasing of cost data in the future, similar to the acute methodology, including updating the base year, service intensity weights, the payment factors, the LOS scale, and the ECT rate
Wage Equalization Factor (WEF)In the future, DOH will consider recalculating WEFs
for the inpatient psychiatric rates that will be based on psychiatric data only.
If psychiatric only WEFs are implemented, DOH will simultaneously recalculate and implement the acute WEFs to exclude the psychiatric wage and fringe data.
New York State Department of Health
32
FMAP Contingency ReductionsSection 313 of the Laws of 2010Gross amount of reduction for local shares @
$282MAll Medicaid payments to be reduced for claims
processed on or after 9/16/10 – 3/31/2011Cycle 727Check dated 9/27/10Released on 10/13/10
Exemptions:HEAL $’sFQHC’s Other Federal mandated payments (IHS, Refugees,
etc.)Reconciliation
33New York State Department of Health
DSH Audit UpdateProcess:Questionnaire:
Asking for data related and supporting the DSH assessment
Desk vs. Field AuditsHospitals selected for field audits have been
notifiedKPMG will schedule time at facility to review
more details of dataDeadlines are critical to meet
34New York State Department of Health
DSH Audit UpdateTimeframes for future years:
2008: Data to be provided before end of year – What should that
include? Information due by March 31, 2008 Working with KPMG to develop tool to collect Audits due to be completed 9/30/2011 Report due 12/31/2011
2009 – 2010 Similar time frames as 2008
2011 – Initial year which new method will actually apply Data issues at hospital level need to be corrected:
Charges on claims – critical to capture all costs related to Medicaid, Medicaid managed care and uninsured
35New York State Department of Health
New York State Department of Health 36