Embed Size (px)
Citation preview

POSTER
N°67Regeneration in aesthetic area with Autologus Bone
Ring Technique: protocol, timing and work flow
1- Albrektsson, T., Zarb, G., Whortington, P. & Eriksson, A.R. (1986) The long term efficacy of currently used dental implants: a review and proposed criteria of success. International Journal of Oral and Maxillo- facial Implants 1: 1–25.
2- Buser, D., Bragger, U., Lang, N.P. & Nyman, S. (1990) Regeneration and enlargement of jaw bone using guided tissue regeneration. Clinical Oral Implants Research 1: 22–32.
3- Misch, C.M. (1997) Comparison of intraoral donor sites for onlay grafting prior to implant placement. International Journal of Oral and Maxillofacial Implants 12: 767–776.
4- Khoury F, Antoun A, Missika P. Bone Augmentation in Oral Implanto- logy. Berlin, London: Quintessenz, 2007.
5-Mark R. Stevens, Hany A, Mahmoud E, Mohamed S.Implant Bone Rings. One-Stage. Three-Dimensional Bone Transplant Technique: A Case Report. Journal of Implantology Vol xxxvi N. one 2010.
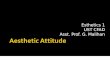
Image 1 shows the first quadrant sector after
extraction of tooth 1.4 which was fractured due
to overloading after trauma. The radiograph
shows a wide horizontal atrophy of the maxilla in
region 1.4. The patient had optimal conditions
for implant placement and bone augmentation.
One of the methods to achieve primary implant
stability is the "Bone Ring Technique". In this
case the palatal zone above the incisor was an
appropriate donor site. Premedication was
performed using antibiotics (Augmentin, 2 g,
GlaxoSmithkline) 2 hours before surgery and a
preoperative rinse with 0,2% chlorexidine
solution (Corsodyl, GlaxoSmithkline). After a
full-thickness flap was released, implant site
preparation was performed using conventional
twist drills. The bone ring was harvested from
the palatal region using a trephine bur. One
implant (external 4.1mm Shape1 hybrid, I-RES)
was placed together with the bone ring graft.
The coincident placement of the implant and the
bone ring graft stabilizes the implant and the
bone graft simultaneosly. The gap around the
bone ring was augmented with hydroxyapatite
particulate bone graft (Osbond Curasan) and
covered with resorbable porcine membrane. The
mucoperiosteal flap was sutured with horizontal
mattress and simple sutures using 4/0 PTFE.
CASE PRESENTATION
BIBLIOGRAPHY
CONCLUSIONS
In the present case, immediate implant
placement and simultaneous bone augmentation
was successfully achieved. This technique
reduced the period of therapeutic time from 12
to 6 months in comparison to classic bone
augmentation techniques. Furthermore, patient
morbidity and treatment costs can be reduced,
since less surgical procedures are required.
Further long-term controlled studies are needed
to confirm the benefits of the autologous "Bone
Ring Technique" in esthetic zone.
BACKGROUNDThe reconstruction of alveolar defects after
tooth loss is one of the major challenges in
implant dentistry. Autogenous bone grafts are
osteoinductive, osteogenic and osteoconductive
with significant higher regenerative capability in
comparison to all other grafts. This is why
autogenous bone, especially for larger lateral or
vertical defects, remains the gold standard for
augmentation.
*Vittorio Siro Leone Farina D.D.S. Adriano Azaripour D.D.S. PhD Department of Periodontology University of Mainz (Germany)
Foto 1: Show the initial situation after 2 month tooth
extraction and rx
Foto 2: After mucoperiosteal flap elevation,
before surgery Bone defect
Foto 3: Shape palatal Bone Ring by kit trephine
(Zept Germany)
Foto 4: Shape bone defect before insert bone ringFoto 5: Stabilize bone ring by implant (Shape1 Hybrid I-RES)
4.1 x 13mm
Foto 6: GBR with hydroxiapatite(Osbone, Curasan) and porcine
membrane(Osgide, Curasan)
Foto 7: After 3 month show new bone around implant
Foto 8: Prosthetic implant rehabilitation and finally
esthetic result after 1 yr and rx