Embed Size (px)
Citation preview

DRUG DISCOVERY
TODAY
DISEASEMODELS
Drug Discovery Today: Disease Models Vol. 1, No. 2 2004
Editors-in-Chief
Jan Tornell – AstraZeneca, Sweden
Denis Noble – University of Oxford, UK
Peripheral nervous system diseases
Regeneration and functional recoveryfollowing peripheral nerve injuryFrancisco J. Rodrıguez1,y, Antoni Valero-Cabre1,2,y, Xavier Navarro1,*1Department of Cell Biology, Physiology and Immunology, and Institute of Neurosciences, Universitat Autonoma de Barcelona,
Edif M Campus UAB, E-08193 Bellaterra, Spain2Department of Neurology, Harvard Medical School, Boston, MA 02155, USA
Peripheral nerve injuries result in loss of neural control
in denervated segments of the body, and severe dis-
abilities for the patients. Nerve regeneration usually
does not allow for adequate target reinnervation and
functional restitution. Neuronal response and axonal
regeneration imply a complex interaction of cell types
and changes in the expression of many molecules. Many
experimental models have been used to gain knowl-
edge on nerve regeneration and to develop strategies
to promote recovery.
*Corresponding author: (X. Navarro) [email protected] F.J. Rodrıguez and A. Valero-Cabre contributed equally to this paper and
both share first authorship.
1740-6757/$ � 2004 Elsevier Ltd. All rights reserved. DOI: 10.1016/j.ddmod.2004.09.008
Section Editor:Kathryn Albers – Department of Medicine, University ofPittsburgh, Pittsburgh, PA 15261, USA
Significant interest lies in determining how to efficiently restore motor,
sensory and autonomic nerve function following peripheral nerveinjury. In this review, Dr Xavier Navarro and colleagues provide a
comprehensive overview of current experimental models being used tostudy the regenerative response following peripheral nerve injury. Many
different injury paradigms are available that offer a wide range of
experimental approaches in which to test novel approaches for nerverepair, drug delivery and in vivo tissue engineering. These model systems
also provide a means in which to identify genes and signaling pathwaysimportant for functional nerve recovery.
Introduction
Injuries to peripheral nerves (PNs) result in partial or total loss
of motor, sensory and autonomic functions in the involved
segments of the body. Reinnervation (see Glossary) of dener-
vated targets can be achieved by regeneration of injured
axons or by collateral branching of undamaged axons in
the vicinity. Nevertheless, these mechanisms do not provide
for satisfactory functional recovery, especially after severe
injuries. PN problems are common and encompass a large
spectrum of traumatic injuries, diseases, tumors and iatro-
genic lesions. The incidence of traumatic injuries is estimated
as >500,000 new patients annually.
After injuries to PNs, axons and myelin sheaths distal to the
lesion are degraded. The degenerative products are elimi-
nated by the cooperative action of denervated Schwann cells
(SCs) and infiltrating macrophages. Wallerian degeneration
serves to create a microenvironment favoring axonal
regrowth. SCs within the endoneurial tubes of the distal
nerve dedifferentiate towards a non-myelinating proliferative
phenotype that over-express growth factors, cell adhesion
molecules and extracellular matrix. The axotomized neurons
shift from a ‘transmitter’ state to a ‘regenerative’ state, so their
axons generate growth cones that progress from the proximal
stump into the distal nerve. Axonal regeneration requires an
adequate substrate of trophic and tropic factors, provided by
reactive SCs, macrophages and the extracellular matrix
within the degenerated nerve. The regenerative process, how-
ever, does not usually reconstitute a normal nerve structure
neither allows for normal distal reconnection after severe
lesions.
Neuronal response and axonal regeneration require a com-
plex interaction of several cell types and changes in the
www.drugdiscoverytoday.com 177

Drug Discovery Today: Disease Models | Peripheral nervous system diseases Vol. 1, No. 2 2004
Glossary
Artificial nerve graft: device designed to repair nerve gaps, as a
substitute of a natural nerve grafts.
Axonal regeneration: regrowth and elongation of the cut axon tips.
Axotomy: rupture or section of the axon, leading to loss of continuity
and of impulse conduction through the distal axon.
Iatrogenic lesion: lesion or secondary complication due to medical or
surgical procedures.
Nerve fascicle: bundle of nerve fibers encircled by perineurial sheath.
Nerve graft repair: interposition of a nerve segment between the
stumps of a transected nerve.
Neuritogenesis: growth of neurites, thin dendrite-like prolongations
from neurons cultured in vitro.
Neuroma: enlargement of the proximal stump of a cut nerve composed
by twisting regenerating sprouts and connective tissue.
Neurotmesis: complete transection of a peripheral nerve.
Reinnervation accuracy: adequate reinnervation of a target end organ
by axons that originally served that organ.
Root avulsion: rupture by stretch of a spinal root at its entrance in the
spinal cord.
Tubulization or tube repair: implantation of a nerve guide to bridge a
gap created in the peripheral nerve.
Vibrissa: mystacial hair in the rodents, moved by piloerector muscles for
exploratory behavior.
Wallerian: degeneration: process of degradation of axonal and myelin
debris after axotomy.
expression of many molecules with variable spatial and tem-
poral patterns. Therefore, a wide variety of methods are used
in experimental studies, depending on the specific goals of
each study. This review provides an overview of different
experimental models used to gain knowledge on the regen-
erative response after PN injuries and to assess repair strate-
gies to promote functional recovery (Table 1).
In vitro models of neuronal survival and
neuritogenesis
Neuronal cell cultures
The most simple and traditional in vitro model is the culture
of dissociated neuronal cells, mostly from dorsal root ganglia
(DRG) because of their easier access compared to other popu-
lations [1] (Fig. 1). This preparation, however, disrupts the
normal relationships between axons, glia and connective
tissue cells. Primary cell cultures need the sacrifice of a large
number of animals and allow for a limited number of cells. An
alternative model is cell lines, which are available from cell
banks (American Type Culture Collection, http://www.atc-
c.org), can be easily expanded, and provide a more homo-
genous cell population than primary neuronal cultures. One
cell line extensively used is PC12, a rat pheochromocytoma
line that when exposed to nerve growth factor (NGF) differ-
entiates into cells resembling adult sympathetic neurons.
However, because they are not real sympathetic neurons,
the genetic background – as with any cell line – can yield
results not representative of physiological roles in vivo. These
models are adequate to evaluate factors with direct impact on
178 www.drugdiscoverytoday.com
neurons for either survival or neuritogenesis, such as drugs,
growth factors or substrates, and, if co-cultured with other
cell types, such as SCs, to assess mechanisms of interaction.
Neuronal culture methods represent a suitable platform to
test strategies based on genetic manipulation of either neu-
rons or supporting cells. Ex vivo engineering of glial cells or in
vivo transduction of neurons by means of viral vectors are
becoming important tools to modulate the response after PN
injury [2,3].
Tissue-engineered 3-dimensional cultures
Tissue-engineered models of PN regeneration to study neurite
growth are generally based on the culture of dissociated
neurons on top of a 3-dimensional artificial tissue based on
extracellular matrix elements. Particular interest has received
the study of composition and geometry of the matrix and
addition of attachment peptides to investigate contact gui-
dance cues for neurite outgrowth [4,5].
In a recent study addressing how skin vasculature modu-
lates innervation by sensory neurons [6], the authors used an
artificial skin composed of a collagen–chitosan sponge filled
with human fibroblasts and endothelial cells. Endothelial
cells spontaneously formed a network of capillary-like tubes
that were followed by neurites. In addition, the 3-dimen-
sional structure of the construct allows for gradients of nutri-
ents and growth factors that might favor neurite outgrowth
from top to bottom of the sponge. The use of confocal
microscopy coupled to immunofluorescence permits visua-
lization of the neurite network and its interaction with other
components of the construct.
Organotypic cultures
Organotypic cultures have several advantages compared
with dissociated neuronal cultures. First, there is no need
for cell dissociation, a major cause of cell stress and death.
Second, the tissue cytoarchitecture and the interactions
between different cell types are both preserved, allowing
for a more physiological evaluation. Third, because the
culture preserves the whole anatomical structure it allows
for the generation of spatial interactions with other ele-
ments, such as a PN slice, or chemotropic interactions, such
as gradients for a growth factor from slow-releasing gels, or
an adjacent compartment filled with other unmodified or
engineered cell types.
Although the most commonly used structure is DRG, slices
of rodent spinal cord have also been successfully cultured.
Organotypic cultures of spinal cord have been mainly used to
investigate the effects of neuroprotective agents against
trauma or neurodegeneration [7,8]. Co-cultures of spinal
cord slices over a monolayer of muscle cells have been
applied to study neuromuscular innervation [9]. From the
several models described in the literature, the two described
below represent interesting examples for PN regeneration.

Vol. 1, No. 2 2004 Drug Discovery Today: Disease Models | Peripheral nervous system diseases
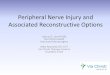
Figure 1. In vitro methods to study peripheral nerve regeneration. Primary cell cultures, neurons and glial cells can be used to evaluate factors expressed by
themselves or necessary to promote survival, neuritogenesis and/or proliferation. Also, if co-cultured they enable the study of cell–cell interactions. The
dissociated cells box shows a culture of embryonic spinal cord with neurons immunostained against b-Tubulin III (a) and Schwann cells immunopurified by
magnetic beads covered with p75-NGFr antibody (b). Chemotaxis chambers are used to evaluate the activity of soluble factors to promote cell migration
through a porous membrane. Tissue-engineered 3-dimensional cultures based on a sponge composed of extracellular matrix and cells that after culturing
neurons on top allows for the study of neurite growth. Organotypic cultures can be done from dorsal root ganglia, sympathetic ganglia, spinal cord slices and
peripheral nerve slices. Possibilities to manipulate the environment include placing gels containing cells or growth factors, a monolayer of unmodified or
engineered cells, and a growth-promoting substrate.
The co-culture of DRG with a whole nerve segment or a nerve
cryosection [10] enables the study, in vitro, of the interaction
between the neurites and their normal growth substrate in
vivo, with the advantage conferred by the option to modify
the culture medium. The development of artificial nerve
grafts based on 3-dimensional structures resembling the
distal denervated nerve to support axonal growth benefits
from the aligned distribution that collagen molecules adopt
when exposed to magnetic fields during polymerization.
Tranquillo and colleagues developed an in vitro model con-
sisting on a tube filled with collagen that allows for the
placement of a DRG on a small chamber located on one
side of the rod and the analysis of neurite growth extent
and direction [11]. The field is exploring the use of other
elements of the extracellular matrix, such as fibrin and
fibronectin [12], and the incorporation of neuritotropic
oligopeptides [13].
Glial cell cultures
The de-differentiation and migration of SCs is a crucial step
for regeneration after PN injury. Two to six months after
injury, denervated SCs become atrophic and lose their cap-
ability to promote axonal regeneration. When surgery is
delayed and/or the distance axons have to regrow is long,
the distal nerve stump might remain denervated for months.
SC cultures helped to characterize and to compare the mole-
cular phenotypes of acutely and chronically denervated cells
in vitro [14,15].
SC migration can be promoted by either gradients of
soluble chemotropic factors or contact-guidance substrates.
A common technique is the use of chemotaxis chambers, a
cell culture system designed to count the number of cells able
to migrate through a porous insert in response to soluble
factors. A recent study has shown that SCs increase their
kinetic activity when exposed to NGF, but not to brain-
www.drugdiscoverytoday.com 179

Drug Discovery Today: Disease Models | Peripheral nervous system diseases Vol. 1, No. 2 2004
Table 1. Comparison summary table
In vitro models In vivo models In silico models
Pros Simplicity Similar models to human lesions Combining experimental information
from molecular to organ levels
Short time studies Different types of models and injuries Multiple hypothesis testing
Testing of multiple factors Large experience in physiological and
pathological experiments
Available cell lines Available transgenic and knockout animals
Cons Physiological differences
with in vivo models
Cost and time consuming Results should be assessed on in vitro
and in vivo models
Missing influences from
host factors
Complexity Limited models available
Accurate methodologies for evaluation
Ethical considerations
Best use of model Initial testing of factors
and drugs
Developing and testing new
therapeutic strategies
Simulation modeling of multiple
variables influencing nerve regeneration
Preservation of cytoarchitecture
in organotypic cultures
How to get access
to the models
Literature Literature Literature
Cell banks
References [1–17] [18–44] [45–54]
derived neurotrophic factor (BDNF) or neurotrophin-3 (NT-3)
[16]. A second method is the determination of maximal
distance of migration of SCs dissociated in culture or from
a PN explant in response to factors added to the medium,
attached to the culture plate surface or secreted by engineered
cells in a confluent monolayer [17]. Finally, in vitro tests are
also used to assess the ability of extracellular matrices or nerve
guides to promote SC migration [12].
In vivo models of peripheral nerve regeneration and
recovery
A wide variety of animal and nerve models have been used in
PN regeneration research. Rodents, particularly mice and rats,
have become the most frequently utilized model. Their inex-
pensive housing costs, their distribution of nerve trunks
similar to humans, and the large availability of genetic,
cellular and system physiology data, makes them particularly
suitable. Furthermore, numerous transgenic and knockout
rodent models (not covered here) have been developed prov-
ing to be an essential approach to study regeneration-related
mechanisms and pathways. Non-human primates have been
occasionally used. In spite of their proximity to human
models, their high cost and sophisticated housing explains
its limited use. Unless long-term behavioral and electrophy-
siological assessment of fine motor and sensory functions are
carried out or drug and/or device testing is at final stages
preceding clinical application, the benefits of monkey over
rodent models are at least questionable.
In rodent models, lesions to a large variety of nerves have
been assayed. Sciatic, femoral, facial and median nerves, and
brachial and lumbar spinal roots are among the most fre-
quently found in the literature. Some of these models emu-
180 www.drugdiscoverytoday.com
late clinically relevant lesions occurring in the same or similar
nerves in humans. Others enable researchers to tackle specific
molecular, cellular or behavioral problems that might help to
expand knowledge in the field.
Sciatic nerve model
The sciatic nerve model is most commonly used in PN
regeneration studies. It provides a nerve trunk with adequate
length and space at the mid-thigh for surgical manipulation
and introduction of grafts or guides (see below). The sciatic
nerve divides above the popliteal fossa into three branches:
tibial, peroneal and sural nerves. Each of these branches
conveys different proportions of motor, sensory and auto-
nomic axons towards muscles, skin receptors and vessels or
sweat glands, located at defined territories of the hindlimb.
Injury in one but not other sciatic branches yields to paralysis
and anesthesia of particular regions. Motor and sensory
neurons are orderly distributed at different levels and depths
in the spinal cord and DRG [18,19]. Although sciatic nerve
injuries themselves are rare in humans, this model provides a
very realistic testing bench for lesions involving plurifasci-
cular mixed nerves with axons of different size and types
competing to reach distal endoneurial tubules and reinner-
vate targets. Comparisons with the normal distribution
enable the accuracy of reinnervation to be addressed through
electrophysiological and retrograde tracing methods (Fig. 2).
Behavioral recovery of walking has been extensively assessed
by detailed analysis of the paw prints during gait [20].
Femoral nerve model
The femoral nerve of the rat is a relevant model to study the
accuracy of reinnervation of motor and sensory axons onto

Vol. 1, No. 2 2004 Drug Discovery Today: Disease Models | Peripheral nervous system diseases
Figure 2. Schema of retrograde tracing of motoneurons in the sciatic nerve and its branches that can be applied after injury and regeneration to assess
topographic accuracy of muscle reinnervation. Different tracers are injected in different nerves near or at the entrance in the muscle. After a few days,
corresponding motor nuclei can be visualized on either transversal or longitudinal spinal cord sections, the numbers of motoneuron bodies counted, and the
outline and location of the motor nuclei calculated. Abbrevistions: GCm, gastrocnemius medialis muscle; GCl, gastrocnemius lateralis muscle; TA, tibialis
anterior muscle; PL, plantar muscles.
appropriate targets (i.e. muscle or skin receptors). It has
terminal division onto two different branches of similar size:
a muscular branch to the quadriceps muscle (containing
�300–500 motor axons), and a cutaneous branch conveying
sensory innervation to the skin of the anterolateral region of
the thigh (�1500 myelinated sensory axons). Preferential
motor or sensory reinnervation [21,22] has been demon-
strated using this particular model. Preferential reinnervation
refers to the higher probability of regenerating motor axons
to reinnervate muscle than skin, and vice versa for sensory
axons. The relevance of pathway-related guidance molecules
can be investigated in this model.
Median nerve model
Median nerve lesions are relevant in humans, particularly in
the context of carpal tunnel syndrome. The median nerve
provides a model in which motor and sensory axons segregate
in different nerve branches distal to the wrist. Rodent models
of median nerve injury are seldom used, due to limited
possibilities of testing fine finger motor or sensory functions
in small animals. The narrow space available in the forearm of
rodents makes surgery challenging. In spite of those difficul-
ties, electrophysiological assessment of median and ulnar
nerves and behavioral testing of grasping have been reported
after injuries and nerve graft repair [23,24]. In monkeys,
regeneration after different length resections of the median
nerve repaired by either direct suture, sural grafts or collagen
guides has been studied in detail [25,26]. Nerve gaps, com-
parable with those considered limiting in humans, can be
studied in the monkey model. Electrophysiological techni-
ques similar to those used in clinical evaluation to explore
reinnervation can be applied.
Facial nerve model
In rodents, as in humans, the facial nerve is a motor nerve
innervating face muscles. Its main trunk divides into the
marginal–mandibular and the buccal branches, the latter
innervating the rows of whisker muscles. Owing to its super-
ficial location, surgical access to the facial nerve is simple.
Highly variable numbers of motoneurons (3200–6500) have
been localized in the facial nucleus by retrograde tracers.
They are organized in three different regions, depending
on the vibrissa they innervate and the projecting branch.
Rodent facial nerve lesions have been primarily used to study
molecular and cellular aspects of degeneration and regenera-
tion of motoneurons [27]. Human facial nerve lesions are
www.drugdiscoverytoday.com 181

Drug Discovery Today: Disease Models | Peripheral nervous system diseases Vol. 1, No. 2 2004
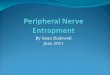
Figure 3. Micrographs of the mouse sciatic nerve exposed at the mid-
thigh and subjected to (a) a crush lesion, (b) a resection of 6 mm repaired
by autografting the same segment resected, and (c) a resection repaired
by tube implantation leaving a 6 mm gap.
common and have devastating effects, not only when no
regeneration occurs, but frequently as a result of exuberant
sprouting, hyperinnervation and misdirected reinnervation
leading to dyskinesiae [27]. To tackle this particular problem,
transections of the buccal branch in rats have been used for
testing therapies aimed to limit misdirected reinnervation
[28]. Multitracing studies, electrophysiology and behavioral
assessment of vibrissae movements during exploratory beha-
vior have been successfully implemented in this model.
Spinal root models
Depending on the level the roots are severed from the spinal
cord, plexus lesions can be classified as preganglionic or post-
ganglionic. The dorsal sensory root, the ventral motor root or
both can be involved. Ventral root avulsion results in signifi-
cant death of motoneurons in adult animals. A crush-traction
of the spinal nerves has similar effects but maintains the
continuity of the roots with the spinal cord. Surgical, pharma-
cological and gene transfer approaches have been considered
to rescue motoneurons and to promote axonal regeneration in
lesions at or close to the spinal cord interface [29,30]. Regard-
ing dorsal roots, preganglionic lesions induced by avulsion or
sectionhavea bad prognosis,because the centralaxons can not
penetrate the dorsal root entryzone into the spinal cord,which
exhibits a highly inhibitory ambiance for regeneration. Sever-
ing dorsal roots of lumbar or brachial plexuses has generated
rat models of dorsal root lesions. Local application of neuro-
trophic factors and cell transplantation combined with surgi-
cal repair has been found to overcome the central inhibition
and achieve regeneration and limited behavioral recovery in
some studies [31,32].
In vivo models of nerve injury and repair
After PN injuries the capability of severed axons to regenerate
and recover functional connections is dependent on the site,
type of lesion and the distance over which axons must regrow
to span the injury. The nerve trunk injured, the type and the
severity of the lesion determine the need for surgical repair
and the prognosis for functional return. This is why the
traditional classifications of nerve lesions in the clinical field
are based upon the morphology of the lesion and the extent
of nerve sheath damage. The most common types of injury
performed in the experimental setting are: focal crush or
freeze injury that induces axonal interruption preserving
connective sheaths (axonotmesis), complete transection dis-
rupting the whole nerve trunk (neurotmesis) and resection of
a nerve segment inducing a gap of certain length (Fig. 3).
After nerve crush regeneration is usually successful thanks
to the favorable terrain provided by reactive SCs and the
preservation in continuity of the endoneurial tubules. Both
facts enhance axonal elongation and facilitate adequate tar-
get reinnervation [19]. After a short (one to two days) latency
to cross the injury site, axons regenerate at linear rate along
182 www.drugdiscoverytoday.com
the distal nerve. Crush injuries are adequate to investigate the
intrinsic cellular and molecular events that intervene in PN
regeneration, and to assess factors, such as drugs [33] that
might enhance the speed of regeneration and the effective-
ness of reinnervation. Crush injuries exerted previously or
proximally to the nerve lesion site increase the rate of regen-
eration. The effect of conditioning injuries is explained by
accelerating the shift to the neuronal ‘regenerative’ state or
through early activation of SCs.
By contrast, axonal growth is limited across a gap imposed
after transection of a nerve. If left unrepaired, or if over-
imposing a nerve ligature or a capped tube, the abortive
regenerative growth leads to neuroma formation. The neu-
roma model has been mainly applied to investigate local and
neuronal changes that contribute to the development of
neuropathic pain after injury [34,35].
Surgical repair is needed for axonal regeneration to take
place after PN section. Epineurial suturing of stumps,
attempting to coapt individual nerve fascicles, has been
the most classical method of repair. In plurifascicular nerves
identification of cutaneous and muscular fascicles might be
possible by the use of neurophysiological stimulation or
histochemical staining. Long delayed repair results in a pro-
gressive reduction of the number of neurons that regenerate
and reinnervate denervated targets. Cross suture techniques
are useful to assess the consequences of either prolonged
axotomy or denervation of the distal stump. Thus, the tibial
nerve is cut, prevented to regenerate for months to prolong
axotomy, and thereafter the proximal stump is refreshed and
sutured to the freshly cut peroneal nerve. The converse
procedure is performed to prolong SC denervation. With
these models, it has been found that low-dose BDNF or glial
cell derived neurotrophic factor (GDNF) counteract the
effects of chronic axotomy [15].

Vol. 1, No. 2 2004 Drug Discovery Today: Disease Models | Peripheral nervous system diseases
The gold standard model for repairing a long nerve gap is
the autograft. Wallerian degeneration occurs more slowly in
the graft than in the distal stump, but autografts retain the
structure for long periods and do not show immunoreaction.
Autograft repair allows for similar number of regenerated
axons and functional recovery in contrast to direct suture
repair. The use of nerve allografts or xenografts is followed by
immune rejection, which is mainly directed against SCs and
myelin in the graft. Investigations on such graft models have
evaluated immunosuppressive therapies with limited second-
ary complications and procedures that reduce immunogeni-
city without affecting regeneration [36,37]. Different
procedures have been applied to make the graft acellular
but still maintain the connective sheaths. The resulting
allograft scaffolds can be repopulated by host SCs and support
axonal regeneration. Other tissue grafts, such as acellular
muscle tubes and blood vessels, have also been modeled as
a bridge for nerve gap repair [38].
Tubulization, the implantation of a tube or guide to bridge
a nerve gap, provides a useful model for studying and manip-
ulating cellular and biochemical events during PN regenera-
tion. Proximal and distal nerve stumps are fixed a few
millimeters within the ends of a tube, leaving a measured
gap in between. The silicone tube model has become the
standard for tubulization. In the past decades intense
research has focused on development of new polymeric
materials with intrinsic properties that enhance regeneration
[39]. Nerve guides offer a closed space, where neurotrophic
elements provided by the injured nerve accumulate and
support axonal growth. A limit to regeneration exists within
nerve guides depending upon the length of the gap, that is
species-dependent [40]. Therefore, tube repair offers a general
model to different approaches. Within a short or mid-length
gap, the guide constitutes a window to investigate the role of
different molecular factors and cell types in the regenerating
process [41,42]. With a long gap, above limiting length, tube
repair constitutes the basis for development of artificial grafts
that might substitute classical autologous nerve grafting.
Many works have assayed the introduction inside the tube
of neurotrophic factors, extracellular matrix components or
transplanted cells [39,40,43].
An interesting model described by Torigoe [44] is the film
model, in which the proximal stump of a transected nerve is
sandwiched between two sheets of thin plastic film and
remained in vivo for several days. The regenerating axons
and non-neuronal cells can be labeled and visualized on
the film and different strategies applied to investigate the
effects on early axonal growth and cell migration.
In silico models of nerve regeneration
A few studies have been published using oligonucleotide and
cDNA arrays for the determination of changes in gene expres-
sion in lesioned sympathetic ganglia neurons [45], in the
distal nerve stump at different time points after axotomy
[46,47], and in the ventral horn after root avulsion [48]. A
large number of expressed genes, however, do not have a
known protein correlate, and their physiological role has to
be determined by adequate in vitro or in vivo approaches. It is
also important not to neglect the technical limitation of
microarrays to detect low-abundance genes, which become
diluted when the sample is composed of multiple cellular
types, and, because they are tightly regulated, can be the real
effectors for larger changes observed in other genes.
In silico models are computer-based simulations for the
study of biological interactions at different levels of complex-
ity ranging from genes and proteins to the whole organism.
The advantage of computer models of nerve regeneration is
the ease with which different variables can be altered to
explore the interactive temporal relationships of multiple
cellular and molecular factors during regeneration. A few
reports exist on mathematical models, based upon experi-
mental data, to model growth cone shape and motility [49],
to simulate nerve regeneration after crush and section fol-
lowed by tube repair [50] or to evaluate various nerve guide
designs [51]. As in silico models become more accurate and
incorporate the huge amount of data from gene arrays, they
might become indispensable for the initial design and further
optimization of new drugs or substrates.
Substrate patterning
This technology uses photolithography to generate surfaces
that combine one or more substrates on a predefined chemi-
cal, geometrical and spatial distribution. It serves to deter-
mine their ability to influence cell adhesion, proliferation,
apoptosis, migration and orientation [52]. An example of its
application is the prove that neuronal polarity depends on
the presence of substrates with different adhesive strength;
whereas neuronal soma and dendrites develop on the most
adhesive substrate, axons extend preferentially on weaker
adhesive substrates, grow faster if they find a different sub-
strate as the one at the soma, and its adhesiveness has a
decreasing gradient from it [53]. Similar technology has
shown that substrates microgrooved with adsorbed laminin
are effective in promoting the adhesion and alignment of SCs
in vitro, with optimal widths and spacing of 10–20 mm [54].
Because cells respond differently if disposed on two or three
dimensions, future directions should address the develop-
ment of 3-dimensional in vitro systems, based on materials
suitable for topographical modification such as hydrogel
scaffoldings or agarose gels.
Conclusions
In vitro models have been and will be important for expand-
ing knowledge at the cellular level. They also help paving the
way for initially developing new potential therapies to pro-
mote cell survival, enhance regeneration and guide neurite
www.drugdiscoverytoday.com 183

Drug Discovery Today: Disease Models | Peripheral nervous system diseases Vol. 1, No. 2 2004
Links
� http://www.atcc.org
� http://pns.ucsd.edu
� http://www.hand-surg.org
� http://www.vard.org/neural/neural.htm
� http://www.integra-ls.com
� http://biomed.brown.edu/Courses/BI108/BI108_2001_Groups/
Nerve_Regeneration
Outstanding issues
� Identification of genes related to axonal regeneration, Schwann cell
response and target denervation.
� Characterization of molecular cues that guide selective growth of
different types of nerve fibers to adequate targets.
� Development of clinically useful artificial nerve grafts.
� Treatment for secondary complications of nerve injuries
(neuropathic pain, hyperreflexia, atrophy).
� Neuroprotection and axonal regeneration in proximal nerve injuries.
� Enhancement of regeneration and recovery after chronic
denervation.
outgrowth. In silico models will develop in a near future andwill have a fundamental role by combining experimental
information from molecular to tissue levels. In vivo animal
models will continue to be essential for further development
of therapies and particularly for a safe and effective transfer to
human patients. Results on in vivo models might be condi-
tioned by delivery systems, pharmacokinetic and pharmaco-
dynamic profiles, adequacy of devices, and potential
biochemical and cellular interactions, which might modify
the effects found in vitro or simulated in silico. The transfer from
successful results on in vivo models to clinical treatment of
patients might be equally uncertain because of physiological
differences and distinctions of pathologies. Although experi-
mental models have provided an adequate benchmark for
assessing pharmacological agents aimed at improving regen-
eration, the applicabilityofbiochemical ormetabolic factors to
improve regeneration in human subjects remains still spec-
ulative in most instances. Nevertheless, there are good exam-
ples of successful translation from laboratory to clinic, such as
nerve tubulization repair that has been tested with success in
human patients [55], or treatment with immunophilin ligands
that, in addition to acting as immunosuppressant for accep-
tance of allografts, also enhance nerve regeneration [37].
Future research models will focus on refining strategies to
enhance PN regeneration, to counteract factors contributing
to poor functional recovery after severe injuries, such as
damage to neuronal cells due to axotomy, inability for axonal
growth due to the nerve lesion or to underlying diseases, poor
specificity of reinnervation by regenerating axonsand second-
ary plastic changes in central connections.
Related articles
Boyd, J.G. and Gordon, T. (2003) Neurotrophic factors and their
receptors in axonal regeneration and functional recovery after
peripheral nerve injury. Mol. Neurobiol. 27, 277–323
Fu, S.Y. and Gordon, T. (1997) The cellular and molecular basis of
peripheral nerve regeneration. Mol. Neurobiol. 14, 67–116
Hall, S. (2001) Nerve repair: a neurobiologist’s view. J. Hand Surg. 26B,
129–136
Stoll, G. and Muller, H.W. (1999) Nerve injury, axonal degeneration and
neural regeneration: basic insights. Brain Pathol. 9, 313–325
Verdu, E. and Navarro, X. (1998) The role of Schwann cell in nerve
regeneration. In Understanding Glial Cells (Castellano, B., Gonzalez, B.,
Nieto-Sampedro, M., eds), pp. 319–359, Kluwer Academic Publishers
184 www.drugdiscoverytoday.com
References1 Fedoroff, S. and Richardson, A. (2001) Protocols for Neural Cell Culture.
Humana Press
2 Washbourne, P. and McAllister, A.K. (2002) Techniques for gene transfer
into neurons. Curr. Opin. Neurobiol. 12, 566–573
3 Glorioso, J.C. et al. (2003) Therapeutic gene transfer to the nervous system
using viral vectors. J. Virol. 9, 165–172
4 Bellamkonda, R. et al. (1995) Laminin oligopeptide derivatized agarose
gels allow three-dimensional neurite extension in vitro. J. Neurosci. Res.
41, 501–509
5 Ahmed, Z. and Brown, R.A. (1999) Adhesion, alignment, and migration of
cultured Schwann cells on ultrathin fibronectin fibres. Cell Motil. Cytos-
keleton 42, 331–343
6 Gingras, M. et al. (2003) In vitro development of a tissue-engineered model
of peripheral nerve regeneration to study neurite growth. FASEB J. 17,
2124–2126
7 Drachman, D.B. and Rothstein, J.D. (2000) Inhibition of cyclooxygenase-2
protects motor neurons in an organotypic model of amyotrophic lateral
sclerosis. Ann. Neurol. 48, 792–795
8 Krassioukov, A.V. et al. (2002) An in vitro model of neurotrauma in
organotypic spinal cord cultures from adult mice. Brain Res. Protocols 10,
60–68
9 Wagner, S. et al. (2003) Functional maturation of nicotinic acetylcholine
receptors as an indicator of murine muscular differentiation in a new nerve-
muscle co-culture system. Pflugers Arch. 447, 14–22
10 Luk, H.W. et al. (2003) Macrophages contribute to the maintenance of
stable regenerating neurites following peripheral nerve injury. J. Neurosci.
Res. 73, 644–658
11 Dubey, N. et al. (1999) Guided neurite elongation and Schwann cell
invasion into magnetically aligned collagen in simulated peripheral nerve
regeneration. Exp. Neurol. 158, 338–350
12 Ahmed, Z. et al. (2003) Nerve guide material made from fibronectin:
assessment of in vitro properties. Tissue Eng. 9, 219–231
13 Schense, J.C. et al. (2000) Enzymatic incorporation of bioactive peptides
into fibrin matrices enhances neurite extension. Nat. Biotechnol. 18,
415–419
14 Hall, S.M. (1999) The biology of chronically denervated Schwann cells.
Ann. N. Y. Acad. Sci. 883, 215–233
15 Gordon, T. et al. (2003) Experimental strategies to promote functional
recovery after peripheral nerve injuries. J. Peripher. Nerv. Syst. 8, 236–250
16 Maniwa, S. et al. (2003) Effects of neurotrophic factors on chemokinesis of
Schwann cells in culture. Scand. J. Plast. Reconstr. Surg. Hand Surg. 37,
14–17
17 Paratcha, G. et al. (2003) The neural cell adhesion molecule NCAM is an
alternative signaling receptor for GDNF family ligands. Cell 113, 867–879
18 Valero-Cabre, A. and Navarro, X. (2002) Functional impact of axonal
misdirection on muscle reinnervation after peripheral nerve resection and
graft or tube repair. J. Neurotrauma 19, 1475–1485
19 Valero-Cabre, A. et al. (2004) Peripheral and spinal motor reorganization
after nerve injury and repair. J. Neurotrauma 21, 95–108
20 Varejao, A.S. et al. (2001) Functional evaluation of peripheral nerve
regeneration in the rat: walking track analysis. J. Neurosci. Methods
108, 1–9

Vol. 1, No. 2 2004 Drug Discovery Today: Disease Models | Peripheral nervous system diseases
21 Brushart, T.M. et al. (1998) Contributions of pathway and neuron to
preferential motor reinnervation. J. Neurosci. 18, 8674–8681
22 Madison, R.D. et al. (1996) Reinnervation accuracy of the rat femoral
nerve by motor and sensory neurons. J. Neurosci. 16, 5698–5703
23 Bertelli, J.A. et al. (2004) Long interpositional nerve graft consistently
induces incomplete motor and sensory recovery in the rat. An experimental
model to test nerve repair. J. Neurosci. Methods 134, 75–80
24 Papalia, I. et al. (2003) On the use of grasping test in the rat median nerve
model: A reappraisal of its efficacy for quantitative assessment of motor
function recovery. J. Neurosci. Methods 127, 43–47
25 Archibald, S.J. et al. (1995) Monkey median nerve repaired by nerve graft
or collagen nerve guide tube. J. Neurosci. 15, 4109–4123
26 Krarup, C. et al. (2002) Factors that influence peripheral nerve regenera-
tion: an electrophysiological study of the monkey median nerve. Ann.
Neurol. 51, 69–81
27 Moran, L.B. and Graeber, M.B. (2004) The facial nerve axotomy model.
Brain Res. Rev. 44, 154–178
28 Streppel, M. et al. (2002) Focal application of neutralizing antibodies to
soluble neurotrophic factors reduces collateral axonal branching after
peripheral nerve lesion. Eur. J. Neurosci. 15, 1327–1342
29 Cullheim, S. et al. (2002) Properties of motoneurons underlying their
regenerative capacity after axon lesions in the ventral funiculus or at the
surface of the spinal cord. Brain Res. Rev. 40, 309–316
30 Natsume, A. et al. (2003) Enhanced functional recovery after proximal
nerve root injury by vector-mediated gene transfer. Exp. Neurol. 184,
878–886
31 Navarro, X. et al. (1999) Ensheathing glia transplants promote dorsal root
regeneration and spinal reflex restitution after multiple lumbar rhizotomy.
Ann. Neurol. 45, 207–215
32 Lee, L.M. et al. (2004) Acidic FGF enhances functional regeneration of
adult dorsal roots. Life Sci. 74, 1937–1943
33 Udina, E. et al. (2003) FK506 enhances reinnervation by regeneration and by
collateral sprouting of peripheral nerve fibers. Exp. Neurol. 183, 220–231
34 England, J. et al. (1998) Abnormal distributions of potassium channels in
human neuromas. Neurosci. Lett. 255, 37–40
35 Black, J.A. et al. (1999) Upregulation of a silent sodium channel after
peripheral, but not central, nerve injury in DRG neurons. J. Neurophysiol.
82, 2776–2785
36 Evans, P.J. et al. (1994) The peripheral nerve allograft: a comprehensive
review of regeneration and neuroimmunology. Prog. Neurobiol. 43, 187–
233
37 Gold, B.G. et al. (2004) Neuroregenerative and neuroprotective actions of
neuroimmunophilin compounds in traumatic and inflammatory neuropa-
thies. Neurol. Res. 26, 371–380
38 Fansa, H. et al. (2002) Host responses after acellular muscle basal lamina
allografting used as a matrix for tissue engineered nerve grafts. Trans-
plantation 74, 381–387
39 Schmidt, C.E. and Leach, J.B. et al. (2003) Neural tissue engineering:
strategies for repair and regeneration. Annu. Rev. Biomed. Eng. 5, 293–347
40 Yannas, I.V. (2001) Tissue and Organ Regeneration in Adults. Springer-
Verlag, New York
41 Fields, R.D. et al. (1989) Nerve regeneration through artificial tubular
implants. Prog. Neurobiol. 33, 87–134
42 Liu, H.M. (1996) Growth factors and extracellular matrix in peripheral
nerve regeneration, studied with a nerve chamber. J. Peripher. Nerv. Syst. 1,
97–110
43 Navarro, X. et al. (2003) Engineering an artificial nerve graft for the repair
of severe nerve injuries. Med. Biol. Eng. Comput. 41, 220–226
44 Torigoe, K. (1997) The role of migratory Schwann cells in nerve regen-
eration as studied by the film model. J. Peripher. Nerv. Syst. 2, 227–231
45 Boeshore, K.L. et al. (2004) Novel changes in gene expression following
axotomy of a sympathetic ganglion: a microarray analysis. J. Neurobiol.
59, 216–235
46 Bosse, F. et al. (2001) Gene expression profiling and molecular aspects in
peripheral nerve regeneration. Restor. Neurol. Neurosci. 19, 5–18
47 Kubo, T. et al. (2002) Analysis of genes induced in peripheral nerve after
axotomy using cDNA microarrays. J. Neurochem. 82, 1129–1136
48 Hu, J. et al. (2002) Microarray analysis suggests the involvement of
proteasomes, lysosomes, and matrix metalloproteinases in the response
of motor neurons to root avulsion. Eur. J. Neurosci. 16, 1409–1416
49 Buettner, H.M. (1995) Computer simulation of nerve growth cone filopo-
dial dynamics for visualization and analysis. Cell Motil. Cytoskeleton 32,
187–204
50 Podhajsky, R.J. and Myers, R.R. (1995) A diffusion-reaction model of
nerve regeneration. J. Neurosci. Methods 60, 79–88
51 Rutkowski, G.E. and Heath, C.A. (2002) Development of a bioartificial
nerve graft. I. Design based on a reaction-diffusion model. Biotechnol.
Prog. 18, 362–372
52 Corey, J.M. and Feldman, E.L. (2003) Substrate patterning: an
emerging technology for the study of neuronal behavior. Exp. Neurol.
184, S89–S96
53 Esch, T. et al. (1999) Local presentation of substrate molecules directs
axon specification by cultured hippocampal neurons. J. Neurosci. 19,
6417–6426
54 Miller, C. et al. (2001) Oriented Schwann cell growth on micropatterned
biodegradable polymer substrates. Biomaterials 22, 1263–1269
55 Lundborg, G. et al. (2004) Tubular repair of the median or ulnar nerve in
the human forearm: a 5-year follow-up. J. Hand Surg. 29B, 100–107
www.drugdiscoverytoday.com 185