Embed Size (px)
Citation preview
Reflux Gastritis Following Gastric Surgery
THEODORE DRAPANAS, M.D., MORRISON BETHEA, M.D.
Reflux gastritis is a distinct clinical entity produced by thereflux of duodenal and proximal intestinal content into thestomach following operations which create a stoma betweenthe stomach and proximal intestine or following pyloroplasty.In 24 patients this clinical pattern was documented andthese findings were supported by gastroscopic demonstrationof reflux and the microscopic pattern of reflux gasritis. Di-version of proximal intestinal content from the stomach insuch patients uniformly led to relief of symptoms with dis-appearance of gastritis and postoperative weight gain. Thepossible role of bile, pancreatic juice and acid as an ex-planation for the mechanism of this entity is presented.
W ITH THE INCREASING UTILIZATON of fibroptic gas-
troscopy and with improved methods for determi-nation of gastric mucosal function, there has occurredwithin recent years an increased awareness of refluxgastritis. For many years it has been recognized thatgastritis to a varying degree may occur in any procedurewhich bypasses the pylorus or in which the pylorus isrendered incompetent. Nevertheless, a number of in-vestigators have begun documenting during the pasttwo decades the possible deleterious effects of reflux ofbile and/or pancreatic juice into the stomach followingsuch procedures.lal813-15,17,20,21,2,l227,29,31,a-5
In reviewing a large series of patients who had under-gone gastric procedures at Charity Hospital, we becameimpressed with a small but significant group of patientswho demonstrated a distressing symptom complex ofweight loss, vague, diffuse epigastric pain, and nauseawith emesis which was occasionally mixed with bile.Most of them had multiple hospital admissions. In al-most every instance their gastric juice was achlorhydricin both the fasting sample and following histamine stim-
Presented at the Annual Meeting of the Southern Surgical As-sociation, Hot Springs, Virginia, December 3-5, 1973.
Mailing Address: Theodore Drapanas, M.D., Department ofSurgery, Tulane University School of Medicine, 1430 TulaneAvenue, New Orleans, Louisiana.
From the Department of Surgery, Tulane University Schoolof Medicine and the Tulane Division, Charity Hospital ot
Louisiana, New Orleans, Louisiana
ulation. The impressive pattern of diffuse gastritis pres-ent on gastroscopy made us re-examine carefully theirproblems and the present report represents an extensivestudy of the 24 patients in whom the diagnosis of refluxgastritis was made and surgical intervention was under-taken during the past five years ( 1968-1973).
Clinical Material
Of the 24 patients who have undergone surgical cor-rection for reflux gastritis, 17 were males and 7 werefemales. They ranged in age between 33 and 70 years.All patients' initial surgery was for peptic ulcer diseaseand all had operations which either bypassed or createdan incompetent pylorus. Five of these patients had astheir original procedure a bilateral truncal vagotomy,antrectomy and gastroduodenostomy (Billroth I); eighthad a bilateral truncal vagotomy, antrectomy and gastro-jejunostomy (Billroth II); seven had a subtotal gastrec-tomy and gastrojejunostomy without vagotomy; twohad a bilateral truncal vagotomy and pyloroplasty; andthe remaining two had a simple gastrojejunostomy with-out vagotomy.
All of the patients except one presented with diffuseepigastric pain and associated nausea and vomiting(Table 1). Nineteen had bile present in the emesiswhich was not necessarily associated with meals. Nine-teen patients also presented with chronic weight lossranging from 5 to 60 pounds with a mean of 15 pounds.Nine patients had some evidence of upper gastrointes-tinal bleeding, two of whom had massive hematemesisrequiring immediate transfusion and admission to thesurgical service. Three patients in addition to reflux gas-tritis had dysphagia due to associated reflux esophagitis.
618

REFLUX GASTRI'I'IS
The interval between initial surgery for peptic ulcerdisease and the onset of symptomatic reflux gastritisranged from two months to almost 20 years. All patientsdemonstrated either a histamine fast achlorhydria or ahvpochlorhydria on gastric analysis. Upper gastroin-testinal x-rays were uniformly within normal limits ex-cept in one patient who demonstrated an ulcer on thegastric side of a gastrojejunostomy. This patient was alsoachlorhydric. Six patients had a microcytic, hypochromicaniemia secondary to chroniic gastric lhemorrhage. Allpatients were gastroscoped preoperatively and free re-flux of bile into the gastric remnant was demonstrated;this was associated with an extremely friable, atrophicgastric mucosa often covered with multiple small super-ficial ulcers.
All of these patients had beeni followed for a variableperiod and represented failures in medical managementconsisting of dietary controls, antacids and spasmodics.Four of these patients were also treated with Cholestyra-mine in an effort to remove bile salts from the stomach,but even these efforts were unsuccessful. Of further in-terest was the fact that three patients had additionalgastric procedures for the symptoms following theirinitial procedure and these procedures were also un-successful. Our indications for surgery in this group ofpatients were threefold; failure to improve on strict medi-cal management or gastric bleeding, gastroscopic docu-mentation of bilious reflux through the anastomosis or
619l'ABLF, 1. Reflux Gastritis Symptoms
No. Patients
Epigastric painNausea and vomitingBilious vomitingXVeight lossBleedingDysphagia
* 5-60 lbs. (meani = 15 lbs.)
23231919*93
pylorus and gross and microscopic evidence of diffusegastritis.
GastroesophagoscopyAll patients had at least one and often repeated gas-
troscopic studies in order to determine the effects ofmedical management and to document the course of theirdisease. A striking pattern appeared to evolve from thesestudies. First, was the almost continuous regurgitationreflux into the stonmach of a mixture of bile stained duo-denal content. Secondly, there was evidence of extremefriability of the gastric mucosa with multiple punctateulcerations and a granular, atrophic appearance. The mu-cosa appeared to bleed easily upon contact with thefibroptic gastroscope. In all cases, recurrent or marginalulcer was excluded. Biopsies were taken from numeroussites whenever possible and these were correlated withthe gastroscopic pattern.The typical changes are shown in Fig. 1 from a gastro-
FIG. 1. Typical changesin mild reflux gastritis.Gastroscopic biopsy ob-tained in this patient re-vealed chronic inflamma-tion, edema and mildulceration of the mucosalglands. There is elonga-tion and "corkscrewing"of the gastric glands ex-tending downwards to-wards the lamina muscu-laris mucosa. (45X )
N'ol. 179 * No. 5

Aniii. Surg. * May 1974
scopic biopsy in a patient with long standing symptomsof epigastric paini, nausea and vomitinig and weight losssix years following previous gastric surgery. We haveinterpreted the pattern in this figure as "nmild", butelongation of the gastric glands cani be clearly seen alongwith inflammatory changes presenit in the mucosa. Onlyrarely did the extent of gastritis penetrate the laminamuscularis mucosa. Small superficial ulcerations of thetips of the gastric glands are also evidenit.A more advanced fornm of reflux gastritis is shown in
Figs. 2a and b, takein from different areas of the stomachin the same patient. Denudation of the gastire inucosais clearly showni aloing with marked elonigatioin of the
FIG. 2a, b. A more advanced form of ieflux gastritis is depictedin these gastroscopic biopsies from another patient with biliousvomiting, epigastric pain and weight loss who had histamine fastachlorhydria. 2a (above) shows denudation of the gastric mucosawith an inflammnatory exudate on the surface. 2b (below) takenfrom another area of the stomach shows marked atrop)hic changesin the mucosa with diminution in the numiibers of chief and parietalcell. (45x )
gastric glands extendinig to the muscularis mucosa anda severe inflammiatory response and congestioin.The degree to which reflux nmay produce severe altera-
tioils in the gastric inucosa is showin in Fig. 3. Therecani be seein shallow ulcerationis with sloughing of thetips of the gastric glands, a diffuse fibrinous exudate aindnumerous inflaimnatory cells. This patient had disablingsymptoms and had lost 40 pounds of weight over theprevious five years.
Surgical ProceduresIn these 24 patients who were deemed surgical candi-
dates according to the previously mentioned criteria, avariety of procedures were performed, all aimed to pre-vent reflux of duodenal juice, including bile, into thestomach or gastric remnanit (Figs. 4-7). Fifteen patienitshad a Roux En-Y anastomosis (Fig. 4) in which at leasta 25 cin interposed jejunal limb was utilized. Of thesefifteen patients, five had had a previous vagotomy andantrectomy with gastroduodenostomy, four had a pre-vious vagotonmy, anitrectomy with gastrojejunostomy, fourhad a subtotal gastrectomy (Billroth 11) with nio vagot-olmny, one had a previous vagotoim-y and pyloroplasty aindone patient had a simple diverting gastrojejunostomy.
In five patients a Tanner 19 procedure was pelformedin which the afferent limb of the gastrojejunostomy wastransected and reimplanted into the efferent limb (Fig.5). This defunctionalized limb of jejunui- also ineasured25 c;n. Advantages of the Tanner 19 procedure includedthe ease with which it could be perfornmed by obviatinigthe need to dissect the entire anastomosis which in somneinstances was extremely high, particularly in patientswith more radical gastric resections. All five of thesepatients had had a previous gastrojejunostomy, four withvagotomy and antrectomy and one with a high subtotalgastrectomy alone.A 10 cm isoperistaltic loop of jejunium (Henley loop)
interposed between the gastric remnant and the duo-denum was utilized in three patients (Fig. 6). Two ofthese patients had a previous subtotal gastrectomy andone patient a previous vagotomy and pyloroplasty.Finally, in the remaining patient who had had a gastro-jejunostomy performed fifteen years previously for anobstructin-g duodenal ulcer which had healed, the anasto-mosis was taken down and normal intestinal continiuityrestored (Fig. 7). All patients except the last one men-tioned had a vagotomy added to the diversioniary pro-cedure.
ResultsT'he results of surgery in the entire group of 24 patienlts
are shown in Table 2. Thirteen of the fifteen patienits witha Roux-Y loop are classified as ail excellent result andremain asymptonmatic for periods ranginig from three
DRAPANAS AND BEI'HEA620

REFLUX GASTRITIS
FIG. 3. A severe form ofreflux gastritis is shownin this specimen obtainedfrom a patient who haddisabling symptoms. Thegastroscopic biopsy re-vealed ulceration of thegastric mucosa, elonga-tion of the gastric glands,severe inflammatory re-sponse and areas of hem-orrhage. The disease issuperficial to the muscu-laris mucosa. (45X)
months to four years following the definitive procedure.One additional patient is classified as a good result, fordespite the fact that his preoperative symptoms of ab-dominal pain and vomiting had ceased, he continuedto have mild dumping symptoms which existed preop-
eratively. Another patient, a 52-year-old male, was doing
ROUX Y15 patients
PREVIOUS SURGERY:
K25cm
5 Vagotomy; Antrectomy; Billroth I4 Vagotomy; Antrectomy; Billroth II
4 Subtotal Gastrectomy; Biliroth 11(no vagotomy in these)
1 Vagotomy; Pyloroplasty1 Gastrojejunostomy
Fit;. 4. Thie Roux-Y techinique of bypass of the anrastonmosis isshowmi. 25 cm limb of defunctionalized jejuinum was utilized in15 patients. In our experience 25 cm limb was adequate il pre-venting reflux. Vagotomy should be added if not previously per-formed in order to preveint recurrent ulceration.
well in the postoperative period until the 10th postop-erative day when he developed a sudden massive pul-monary embolism and expired.Of the 5 patients offered a Tanner 19 procedure, all
remain asymptomatic with excellent results. Sinmilarly,the three patients with a Henley loop also remaiin asymp-tomatic and are classified as excellenit; the patient withtakedowni of the gastrojejunostomy also reminainis asympto-inatic.
The relief of symptoms following these surgical pro-cedures was indeed strikinig. Abdomiiinal pain rapidly dis-appeared, in imiost instaniees during the iniirnediate post-operative period, voimitiing was no longer a problem andall patienits gaiined weight. The cliniical response was alsoaccompanied by a milarked imiiproveimienit in the gastro-scopic apearanice of the stomiiach in all of these patienits.A typical patient is presenited in the following case report:
FIG. 5. Tanner 19 techni(lueof reconstruction for refluxgastritis. Advantages of thistechinique include the limitedexposure necessaryr and implan-tation of the afferenrt limb intothe efferent limb as showvn.Five patienits were offered thisprocedure.
PREVIOUS SURGERY.4 Vagoto.y, Amrocto.y
Billroth 11
Subtotal Gastrecto.yBillrot1 11
621Vol. 179 * No. 5
DRAPANAS AND BETHEA
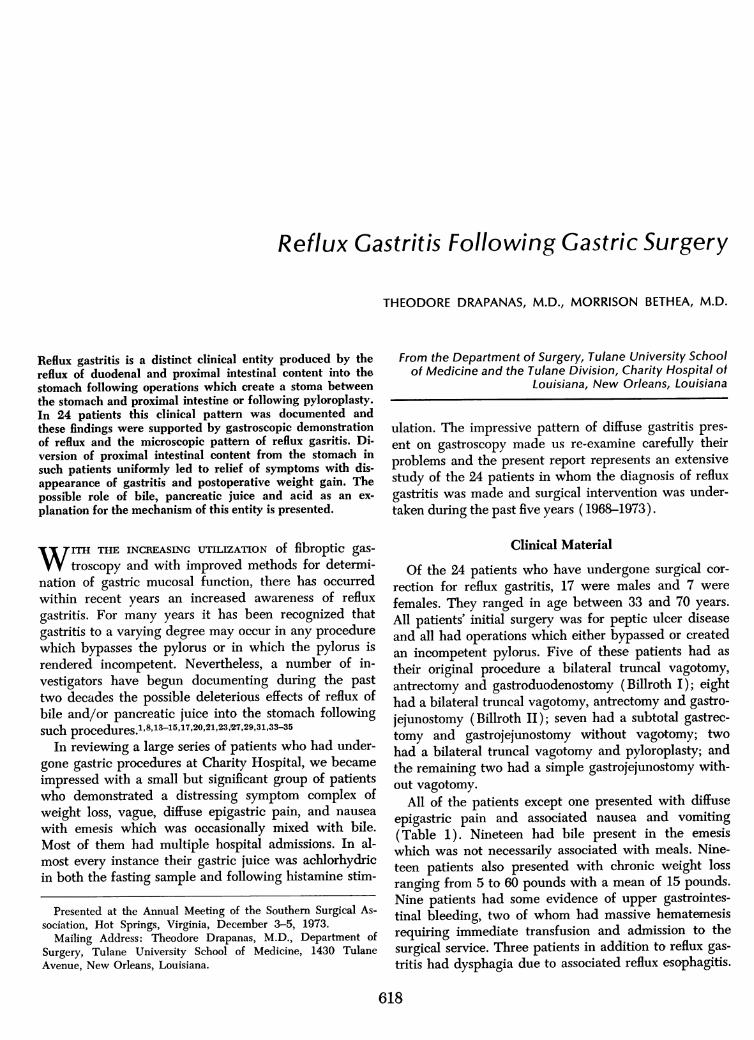
Fic.. 6. Henley loop recon-struction utilizing a 10 cminterposed loop of isoperistalicjejunum between the gastricremnant and the duodenum.Vagotomy was added in the 2p1atients in whom it had notbeen previously performed.Three patients were offered thisprocedure.
TABLIE 2. Resuilts of Sutrgery in Entire Grouip of 24 Patients
RestiltsNo.
Operatioti Patients Excellent Good Poor
Roux Y 15 13 1* ItTanner- 19 5 5 0 0Henley loop 3 3 0 0Anastomlosis Takedowii 1 1 0 0
* Conitinued dumnping syndromet P'ost-op death, pulmonary embolus-10 days
Case Report
A 53-year-old Caucasian female underwent a bilateral truncalvagotomy, hemigastrectomy, and gastroduiodenostomy in 1957 forintractable peptic ulcer disease. Shc remained sym)tom free until1962 when she developed recurrenlt nausea, vomiting and severe
epigastric pain. Her symptoms were not relieved by antacids.Upper gastrointestinal x-rays demon.strated hypertrophy of thegastric mucosal folds. Gastroscopic examiniations revealed multiplesuperficial per-ianiastoinotic ulcerations and diffuse gastr-itis. Be-cause of these symptoms in 1963 a resection of the previousanastomosis andl conversion to a gastrojejunostomy (Billroth IL)were performed. She did well following this second procedureunitil 1971 when her nausea and abdominal pain recurred. Shehad multiple hospitalizations betwveen 1971 and 1973 but evalua-tion on each occasion revealed only gastritis anid she was dis-charged on medical therapy. In June, 1973 she was admittedto the Tulane Surgical Service at Charity Hospital with hema-
temesis, bilious vomiting, severe epigastric pain and chronic weightloss. Admission hematocrit was 24 cand stools were guaiac posi-tive. An SMA-12 profile was normal except for hypoalbuminemia.Upper gastrointestinal x-rays were interpreted unremarkable.Gastroscopy revealed a friable, atrophic gastric mucosa with super-
ficial punctate ulcerations (Fig. 8a). Bile freely refluxed into thegastric pouch. A 12-hour gastric analysis and histamine stimula-tion revealed ach]orhydria with a large quantity of bile in thegastric aspirate. After no improvement on medical managementshe was re-explored at which time there was no evidence ofloop obstructions or marginal ulcer. A Tanner 19 diverting pro-
cedure was performed and her postoperative course was unre-
markable. At five months following her revisional surgery she
remains completely asymptomatic. Repeat gastroscopy with biopsyrevealed an entirely normal gastric mucosa (Fig. 8b).
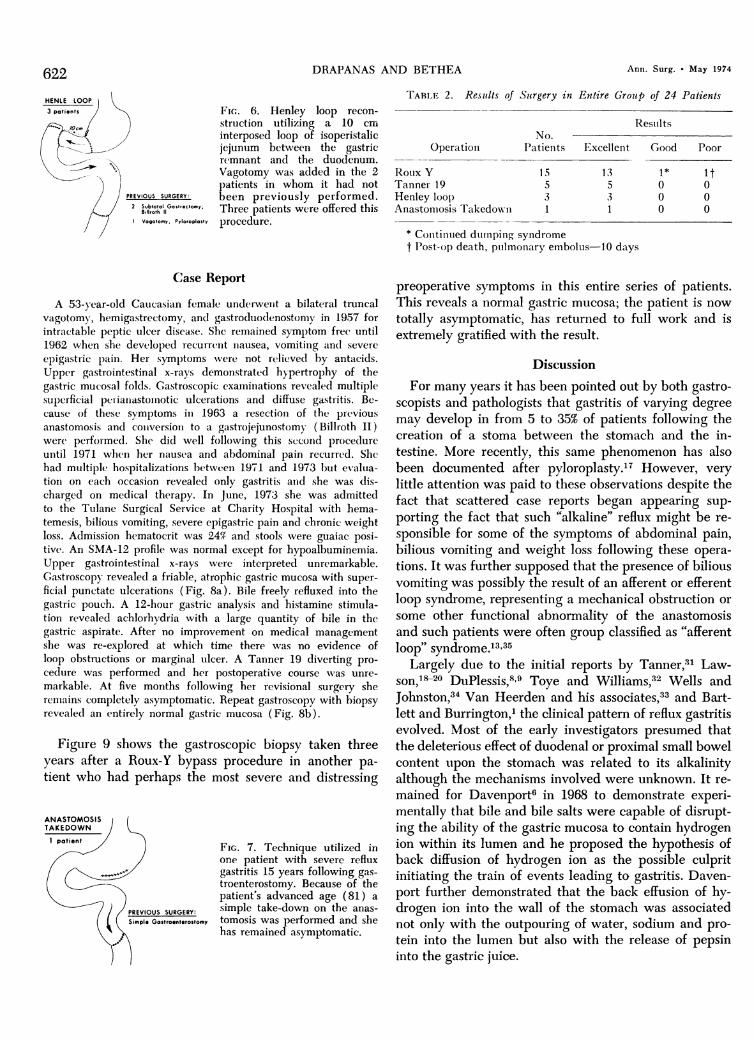
Figure 9 shows the gastroscopic biopsy taken threeyears after a Roux-Y bypass procedure in another pa-
tient who had perhaps the most severe and distressing
ANASTOMOSISTAKEDOWN
patient
FIG. 7. Technique utilized inone patient with severe refluxgastritis 15 years following gas-troenterostomy. Because of thepatient's advanced age (81) a
2JPREVIOUS SURGERY: simple take-down on the anas-Simple Gostroenterostomy tomosis was performed and she
has remained asymptomatic.
preoperative symptoms in this entire series of patients.This reveals a normal gastric mucosa; the patient is nowtotally asymptomatic, has returned to full work and isextremely gratified with the result.
DiscussionFor many years it has been pointed out by both gastro-
scopists and pathologists that gastritis of varying degreemay develop in from 5 to 35% of patients following thecreation of a stoma between the stomach and the in-testine. More recently, this same phenomenon has alsobeen documented after pyloroplasty.'T However, very
little attention was paid to these observations despite thefact that scattered case reports began appearing sup-
porting the fact that such "alkaline" reflux might be re-
sponsible for some of the symptoms of abdominal pain,bilious vomiting and weight loss following these opera-tions. It was further supposed that the presence of biliousvomiting was possibly the result of an afferent or efferentloop syndrome, representing a mechanical obstruction or
some other functional abnormality of the anastomosisand such patients were often group classified as "afferentloop" syndrome.13 35
Largely due to the initial reports by Tanner,31 Law-son, 20 DuPlessis,89 Toye and Williams,32 Wells andJohnston,34 Van Heerden and his associates,33 and Bart-lett and Burrington,' the clinical pattern of reflux gastritisevolved. Most of the early investigators presumed thatthe deleterious effect of duodenal or proximal small bowelcontent upon the stomach was related to its alkalinityalthough the mechanisms involved were unknown. It re-
mained for Davenport6 in 1968 to demonstrate experi-mentally that bile and bile salts were capable of disrupt-ing the ability of the gastric mucosa to contain hydrogenion within its lumen and he proposed the hypothesis ofback diffusion of hydrogen ion as the possible culpritinitiating the train of events leading to gastritis. Daven-port further demonstrated that the back effusion of hy-drogen ion into the wall of the stomach was associatednot only with the outpouring of water, sodium and pro-tein into the lumen but also with the release of pepsininto the gastric juice.
622
PREVIOUS SURGERY:
2 Subtotal Gost,.ctomy,Billioth 11
Vogotomy, Pyloaoplasty
Ann. Surg. * May 1974

REFLUX GASTRITIS 623
FIG. 8a, b 8a (left) shows preoperative gastric biopsy in 53-year -old female with reflux gastritis. The inflammatory and ulcerativechanges in the mucosa are well shown. 8b (right) shows repeat gastric biopsy five months following Tanner 19 diverting procedure.
The gastric mucosa appears normal and patient is asymptomatic. (45x )
Since these initial observations numerous investigatorshave studied experimentally the possible mechanisms in-volved in the production of diffuse and/or atrophicgastritis in these patients. DuPlessis9 measured bile acidconjugates in gastric aspirates and found that patientswith gastric ulcer had considerably larger amounts ofbile acids in overnight gastric juice collections compared
FIG. 9. Gastric biopsy ob-tained three years follow-ing Tanner 19 divertingprocedure for reflux gas-tritis. This patient hadsymptoms of reflux gastri-tis for 8 years followingtruncal vagotomy, hemi-gastrectomy and BillrothII reconstruction. He be-came asymptomaticwithin a few days fol-lowing surgery and hasremained asymptomatic.The biopsy at three yearsreveals normal gastricmucosa. (45x)
to normal individuals or even patients with duodenalulcer.Rhodes and his group were able to document by an
ingenious technique utilizing an intravenous dose of car-bon14 tagged bile salts and measuring the concentrationof radioactive bile salts in the gastric aspirate that re-gurgitation of duodenal contents through the pylorus into
Vol. 179 * No. S
-A

Ann. Siirg. . May 1974DRAPANAS AND BETIHEAPYLORIC INCOMPETENCE or BYPASS
BILE REFLUX
DISRUPTION of GASTRIN RELEASEMUCOSAL BARRIER
H SECRETION
H BACK DIFFUSION
Fic.. 10. Postulated mechanism of pathogenesis of reflux gastritis.
the stomach was considerably higher in patients withgastric ulcer as compared to patients with normal stom-achs or with duodenal ulcer.23Van Geertruyden'0"1' demonstrated that following the
partial gastrectomy with Billroth II reconstruction inhumans, the residual gastric pouch showed a progres-sive diminution in its ability to secrete acid and this cor-
related well with the pathoiogic finding of gastritis. Law-son fuirther demonstrated that in dogs with Billroth II
reconstruction extensive gastritis could be fouind in thegastric pouich whereas following a Billroth I reconstruc-tion the gastritis appeared to be limited to the area sur-
rounding the anatomosis.'8Ritchie and his associates24-26 measured the parietal
and chief cell population of the residual gastric pouch
after antrectomy with a Billroth I type of reconstructionand found that these are unchanged up to one year fol-lowing the procedure. Howvever, after a Billroth II recon-
struction, there was a progressive diminution in the num-hers of parietal and chief cells and there appearedcharacteristic changes of atrophic gastritis in the area ad-jacent to the gastric jejunostomy. In subsequent studiesDelaney, Ritchie and their associates7 reported an in-genious series of experiments in which. a tube of gastricwall was reconstructed from the greater curvature of thedog's stomach, pedicled upon the short gastric vessels,interposed at various sites in the gastrointestinal tractand biopsied. They were able clearly to show that ex-
posure to jejunal content led to rapid and profoundmucosal changes consisting of round-cell infiltration, theappearance of mucous cells deep in the gastric crypts,diminuition of parietal and chief cells, and eystic dilata-tion of the glands. On the other hand, tubes of gastricmucosa exposed to pure bile did not demonstrate thesechanges whereas tuibes exposed to pancreatic juice alonedid show changes, although they were mi.lder and slowerto develop.The apparent lack of the ability of bile alonie to pro-
duce suich changes was also supported by Byers andJordan4 who implanted vascularized patches of gastricmucosa into the wall of the gall bladder in dogs. Evenafter one year the mucosa appeared normal and theyconcluded that bile alone was incapable of inducinggastritis but theorized that something additional wasneeded, possibly acid. Nevertheless, a considerable con-troversy arose concerning whether or not bile alone, incombination with pancreatic juice, or the combination ofbile, pancreatic juice and acid were needed to produicethis pattern of gastritis.
Iveyt4,"5 and his associates demonstrated that thehigh concentration of bile salts found in the stomach ofpatients with gastric ulceration were possibly responsiblefor the marked increase in back diffusion of hydrogen ionin the human stomach. Johnson'6 in a very sophisticatedseries of experiments showed conclusively the definitedisrulption of the gastric muicosal barrier to hydrogenion cauising release of large quantities of pepsin, thusproviding another link in the chain of processes causedby back diffusion as previously postulated by Davenport.Disruption of the gastric mucosal barrier to hydrogenion with consequent back diffusion has also been re-cently implicated in the development of stress ulcera-tions by Skillman, Silen and their associates in a largepercentage of seriouisly ill sturgical patients.29'30 Simi-larly, Hamza and DenBesten have incriminated bile andbile salts in the destruction of the gastric mucosal bar-rier.t2Nahrwald in another significant series of experiments
demonstrated that bile and bile salts were able to releasegastrin from the denervated antrum.22 This demonstrationadded another dimension to our knowledge of the pathbo-genesis of reflux gastritis, for not only could direct in-jury to the gastric mucosa by bile, bile salts and pan-creatic juice be postulated but also the stimu-lation ofgastrin release by these substances might further agra-vate the mucosal destruction by added prodtuction ofhydrogen ion and back diffusion through the mucousblanket producing a vicious cycle. Bedi and his associ-ates have also confirmed the release of antral gastrin bybile salts.2
Regardless of the mechanism involved, in patients inwhom free reflux of bile and duodenal juice can be dem-onstrated along with the presence of diffuise gastritis andsvmptoms of vomiting, abdominal pain and weight loss,the salutary effect of bypass of the secretions from thegastric remnant has been amply demonstrated by Bart-lett,' DuPlessis,8 Joseph,'7 Lawson,20 Mackman,2' Rut-ledge,27 Tanner,31 Toye,32 Van Heerden,3' and Wells.34The present series of 24 patients in which every pa-
tient had gastroscopic evidence of gastritis, and the fur-ther documentation that in every one of these patientsrelief of this pattern could be accomplished by diversion
624

Vol. 179 - No. 5 REFIUX GASTRITIS 625
ot duiodenal and/or proximal jejuinal contents from thestomach lends overwhelming support to the observa-tions previously cited by others. In fact, the responsesof our patients to such surgery were so prompt and sogratifying to the patients that, in our opinion, little needexists at the present time to continue to procrastinatewith other forms of therapy in suich patients.We continuie to favor either the Rouix-Y reconstruction
in suich patients or the Tanner 1.9 procedure which rep-resents a modification of the Roux-Y technique buit issimpler and more quiickly performed for the anastomosisdoes not have to be dissected free completely. Neverthe-less, cau-tion muist be raised in recommending such pro-ceduires, particuilarly in patients who have a large gastricremnant or in whom the antruim is present for it has beenaptly demonstrated by many surgeons during the pastthree decades that diversion of duodenal contents fromthe anastomosis in suich patients may lead to recuirrenceof the uilcer diathesis. We therefore feel, as does Dii-Plessis, that it is important to perform a vagotomy in allpatients in whom it had not previously been performed.
Although the results with the interposed, isoperistaltic,10 cm Henley loop in three of ouir patients are similarto those in which the Roux-Y bypass or the Tanner 19loop was uitilized, we do not see any advantages in theHenley loop and it is considerably more difficult to per-form.
Fturther cauition muist be instilled, lest the unwarysurgeon begins to ascribe all symptoms of pain, vomitingand weight loss after gastric operations to reflux gastritis.In ouir experience, the majoritv of patients with suchsvmptoms still have other cau-.ses responsible for thesesymptoms, including afferent loop syndrome and recuir-rent marginal ulcer. For these reasons we feel stronglvthat a complete work-tip shouild be performed in allsuich patients incluiding carefuil roentgenologic studies,gastroscopy and biopsy along with studies of the gastricsecretion. If other causes can be ruled ovut, and if thetypical pattern of gastritis as shown in gastroscopicbiopsies is present along with svmptoms of abdominalpain, weight loss and the demonstration of free refluixof bile into the stomach, then the diagnosis of refluxgastritis can be firmly established.
References1. Bartlett, M. K. and Burrington, J. D.: Biliouis Vomiting After
G-astric Sturgery. Arch. Surg., 79:34, 1968.2. Bedi, B. S., Debas, H. T., CGillespie, C. and Gillespie, T. F.:
Effect of Bile Salts on Antral Castrin Release. Gastroen-terology, 60:256, 1971.
3. Belowski, H.: Does the Duodlenal Content Exert a HarmfulEffect on the Gastric Muicosa? C(astroenterologia, 98:233,1962.
4. Byers, F. M. Jr. and Jor(lan, P. H.: Effect of Bile UponGastric Mucosa. Proc. Soc. Exp. Biol. Med., 110:864, 1962.
5. Cheng, J., Ritchie, W., Jr. and Delaney, J.: Atrophic Gastritis:An Experimental Mo(lel. Fed. Proc., 28:513, 1969.
6. Davenport, H. WV.: Destruiction of the Gastric Mlucosal Bar-rier hy Detergents an(d Urea. Gastroenterology, 54:175,1.968.
7. Delaney, J. P., Cheng, J. WV. B., Butler, B. A. and Ritehie,XV. P., Jr.: Gastric Ulcer and Regirgitation Gastritis. Gut,11:715, 1970.
8. Duplessis, D. J.: Gastric Mucosal Changes After Operationson the Stomach. S. Afr. Mled., J., 36:471, 1962.
9. Du.iPlessis, D. J.: Pathogenesis of Gastric ITlceration. Lancet,1:974, 1965.
10. Ceertniyden, J. van, Colard, MI., XVissocq and Dejardin, N.:Mode d'Action de la Bile stur la Secretion Castrique,Etude Chez le Rat a Pylore Ligatuire. C. S. Biol. (Paris),154:418, 1960.
11. Geertruiyden, J. van: Alterations dle la Physiologic GastriquesoIis l'Influience de la Bile. Leur Importanee Pour laPathogenie de l'Ulcere Peytique Recidivant Apres Cas-trectomie. Bull. Acad. Roy. Mied. Belg., 7 Ser., 1:53, 1961.
12. Hamza, K. N. and DenBesten, L.: Bile Salts Produicing StressUlcers Duiring Experimental Shock. Surgery, 71:161, 1972.
13. Herrington, J. L.: Remedial Operations for PostgastrectomySyn(dromes. Curr. Probl. Sturg., April 1970.
14. Ivey, K., DenBesten, L. and Bell, S.: Absorption of Bile SaltsFrom the Human Castric Mucosa. J. Appl. Physiol., 29:806, 1970.
1.5. Ivey, K., DenBesten, L.. and Clifton, J. A.: The Effects ofBile Salts on Ionic Movement Across the Human GastricNMlucosa. Gastroenterology, 59:683, 1970.
16. Johnson, L. R.: Pepsin Secretion During Damage by Acid andAlcohol to the Canine Gastric Mlucosa. Castroenterology,60:679, 1971.
17. Joseph, W. 1.., Ribera, R. A., O'Kieffe, D. A., Geeohoed,G. XV. and M1eCuine, W. S.: Mlanagement of Postopera-tive Alkaline Reflux Gastritis. Ann. Surg., 177:655, 1973.
18. Lawson, H, H.: Effect of Daodenal Contents on the GastricM1ucosa Tinder Fxperimental Conditions. ILancet, 1:469,1964.
19. Lawson H: H.: Castritis and Gastric UTlceration. Br. J. Surg.,5.3:493, 1966.
20. Lawson, H. H.: The Reversibility of Postgastrectomy AlkalineRefluix G-astritis by a Rouix En-Y Loop. Br. J. Suirg., 59:13,1972.
21. Mackman, S., Lremmer, K. E. and NMorrissey, J. F.: Postopera-tive Reflux Alkali Castritis ancl Esophagitis. Am. J. Surg.,121:694, 1971.
22. Nahrwald, D. L.: Bile as a Gastric Secretory Stimulant. Sur-gery, 71:157, 1972.
23. Rhodes. J., Barnardo, D., Phillips, S. F., Rovelstad, R. A. andHoffman, A. F.: Increased Reflux of Bile Into the Stomachin Patients With CGastric Ulcer. Gastroenterology, 57:241,1969.
24. Ritchie, W. P., Jr., Btleter, B. and Delaney, J. P.: Stuidies onthe Pathogenesis of Benign Gastric Ulcer: increased BackDiffusion of [H+] in Experimental Atrophic Gastritis. Suirg.Forum, 22:330, 1971.
25. Ritchie, W., Jr., Cheng, J. W. B. and Delaney, J.: Changesin Parietal and Chief Cell Populations Following Va-gotomy and Antrectomy. Surg. Forum, 20:319, 1969.
26. Bitchie, W. P., Jr. and Delaney, J. P.: The Susceptibility ofExperimental Atrophic G-astritis to UlTceration. Castro-enterology, 60:554, 1971.
27. Rutledge, B. H.: Jejunal Segments for the PostgastrectomySyndromes. Ann. Surg., 169:810, 19.69.

626 DRAPANAS AND BETHEA Ann. Surg. * May 1974
28. Sander, S., Myren, J. and Helsingen, N.: The Effect of BileReflux on the Gastric Mucosa. Gastroenterologia, 101:3,1964.
29. Silen, W.: Malevolent Gall (Editorial). Surgery, 71:311, 1972.30. Skillman, J. J., Gould, S. A., Chung, R. S. K. and Silen, W.:
The Gastric Mucosal Barrier: Clinical and ExperimentalStudies in Critically Ill and Normal Man and in the Rabbit.Ann. Surg., 172:564, 1970.
31. Tanner, N. C.: Disabilities Which May Follow the PepticUlcer Operation. Proe. Royal Soc. Med., 59:362, 1966.
32. Toye, D. K. M. and Williams, J. A.: Postgastrectomy BileVomiting. Lancet, 2:524, 1965.
33. Van Heerden, J. A., Priestley, J. T., Farrow, C. M. and Phil-lips, S. F.: Postoperative Alkaline Reflux Castritis. Am. J.Surg., 118:427, 1969.
34. Wells, C. and Johnston, J. H.: Revision to the Roux-En-YAnastomosis for Postgastrectomy Syndromes. Lancet, 2:479,1956.
35. Woodward, E. R.: The Postgastrectomy Syndromes. Spring-field, Ill., Charles C Thomas, pub.. 1963.
DiscussION
DR. J. LYNWOOD HERRINGTON, JR. (Nashville): As all of youknow, bilious vomiting was recognized even before the turn ofthe century, shortly after Anton Wolfler performed the first gas-troenterostomy in 1881. As a result, surgeons over the followingdecades have used various modifications of gastric resection andvarious modifications of gastroenterostomy with hopes of allevatingthis distressing problem. As Dr. Drapanas stated, it is, however,only within the last few years that these cases have been docu-mented as the result of the use of the fibreoptic gastroscope andbiopsy examinations.
I think, also we are indebted to our British and European friendsfor bringing this problem to our attention. They were fully awareof this entity 20 years ago. As a matter of fact, Frank Henley inLondon, and Professor Stauve Haddenstedt in Stockholm, wereadvocating isoperistaltic jejunal segments and Roux-en-Y recon-structions, in addition to vagotomy and gastric resection, as theprimary surgical procedure for the complications of duodenal ul-cer in order to avoid this distressing long-range complication.
I certainly agree wih Dr. Drapanas that bile reflux is not in-frequent and it is by no means rare after gastric operations. Itis like the dumping syndrome; if we question our patients, wewill detect it and I think we will find it to occur to some degreein from 5 to 35% of the cases. In the past we were simply over-looking this problem, and were labeling these patients variantsof the afferent loop problem, or else calling them neurotics.
During the past 10 months we have operated upon 11 docu-mented cases of reflux gastritis. In the past few years prior tothat, we had 17 additional cases, but they were not completelydocumented. We have treated these patients with either a Roux-en-Y reconstruction or a Henley loop. We have made the Henleyloop a little longer than Dr. Drapanas, usually about 15-20 cm.However, Dr. Sawyers and I both prefer the Roux-en-Y recon-struction, as does Dr. Drapanas, because it is easier to carry out.The 11 patients encountered with this entity during the past
10 months experienced symptoms which were really crippling.There were six males and five females in the group.
(Slide) They had the same set of symptomatology as Dr.Drapanas' patients: epigastric pain, nausea, and vomiting, andweight loss. Weight loss was appreciable in four patients; anemiawas a striking feature in several, and two patients had uppergastrointestinal bleeding.
(Slide) This slide shows you the 11 patients, and the type ofprocedure used. The Roux-en-Y reconstruction was carried out inall but one and in this case we used the Henley loop. As youcan see, the original operation was either a Billroth I or Billroth IItype reconstruction with vagotomy or else vagotomy and pyloro-plasty. In patients undergoing pyloroplasty we have always re-moved the antrum in carrying out the Henley loop or Roux-en-Yreconstruction. Four of the patients who had the Roux-en-Y re-construction also had in addition a Hunt-Lawrence pouch con-structed below the gastric remnant because these four patientshad lost considerable weight and were malnourished. This latterproblem is not unique.One of our 11 patients had not undergone a previous gastric
operation. On endoscopic study he had a wide, relaxed, patulous
pylorus with regurgiation of bile and duodenal contents and dif-fuse gastritis with ulceration throughout the stomach.
(Slide) This is a photograph showing the mucosal ulcerationand nodular hyperplasia with areas of intervening atrophic gas-tritis. This is a gross picture of the typical far advanced case.
I would like to ask Dr. Drapanas if he has any explanationwhy these patients sometimes get along for months or yearsfollowing the original gastric surgery before developing symp-toms of reflux gastritis. Also, would you comment on the post-operative correlations comparing your subsequent gastroscopicexaminations with the clinical appraisal of the patient's result. Inother words, have all your patients with excellent results had dis-appearance of the gastritis on endoscopic study, or have youseen some degree of gastritis with bile reflux persisting but nowyour patient is asymptomatic. From my perusal of the litera-ture on this matter it is my impression that patients have beensubjectively improved, but yet areas of gastrititis have persisted.
Lastly, I would like to exert a word of caution. The presence ofbile reflux after any definitive gastric operation is a common find-ing. We should not go overboard in diagnosing this problem andshould not subject patients to a remedial operation unless thesymptoms are severe and unresponsipe to conservative treatment.
DR. JOHN A. VAN HEERDEN (Rochester, Minnesota): Our initialinterest in Rochester, in reflux gastritis, was stimulated by Dr. JimPriestley, who, I am sure, is well known to all members of thissociety.Our management of this problem (slide) has essentially been
the same as that so adequately outlined by Dr. Drapanas today.Roux-en-Y, in our group, with vagectomy is still the most im-portant mode of therapy. Early in our experience with this syn-drome, a number of cases underwent either jejunal interpositionor conversion to a gastroduodenostomy. We feel that neither ofthese procedures are indicated today in the management of re-flux gastritis.
(Slide) Of the 31 patients, we achieved excellent results in83% of the Roux-en-Y's; and in approximately 72%1 of the interpo-sition procedures.
(Slide) Our surgical treatment has been essentially the sameas outlined by Dr. Drapanas; Roux-en-Y being by far the mostcommon, and certainly the easiest to perform.
Certain facets of this syndrome, however, continue to fascinateand frustrate our group.
1. The difficulty in correlating symptoms with objective find-ings. I think we have all seen gross reflux in an asymptomatic pa-tient, and in contrast, a patient who is severely symptomatic,with minimal reflux.
2. The difficulty in sorting out functional symptoms from thosethat are truly organic. So many of these patients are labeled ascrocks. Twenty-five per cent of the patients in our series hadhighly abnormal MMPI's-Minnesota Multiphasic Personality In-dexes. Yet this in no way correlated with good or bad postopera-tive results. Some of the patients who had the worst MMPI's didthe best.
3. Why is the pylorus incompetent in the primary case andin stress ulceration? Is this the primary defect, I think continuedinvestigation of the role of the pylorus may well prove most re-warding.





























