Embed Size (px)
Citation preview

ARTÍCULO DE INVESTIGACIÓN REVISTA MEXICANA DE
INGENIERÍA BIOMÉDICAibVol. 37, No. 1, Ene-Abr 2016, pp. 49-61
dx.doi.org/10.17488/RMIB.37.1.6
Reference Equations for Impulse Oscillometricand Respiratory System Model Parametersin Anglo and Hispanic Children
E.G. Meraz1, H. Nazeran2, R. Edalatpour2, C. Rodriguez2, K. Montano2,C. Aguilar2, N. Avila2, J. O. Vidaña1, A. L. Portillo1
1Universidad Autónoma de Cd. Juárez, Cd. Juarez, México.2The University of Texas at El Paso, El Paso, Texas, USA.
ABSTRACTThe Impulse Oscillometry System (IOS) has been recognized as a useful diagnostic tool. Previous research
by our group has shown that R5 (Resistance at 5 Hz), R5-R20 (frequency dependence of resistance), AX (the“Goldman Triangle”) and the extended Resistor-Inductor-Capacitor (eRIC) model-derived parameter Cp (peripheralCompliance) are reliable measures that track respiratory system function. Here we determined the predictiveequations from 112 asthmatic and non-asthmatic Anglo and Hispanic children data, that were previously classifiedinto four groups: Normal, PSAI (Probable Small Airway Impairment), SAI (Small Airway Impairment), and Asthmaby using regression analysis of IOS and eRIC model parameters as dependent variables regressed against age, height,and weight. Height showed the greatest correlation with IOS and eRIC model parameters and provided the mostsignificant reference values for these measures in Anglo and Hispanic children. These values could serve as a usefulframework for diagnosis, early interventions, and treatment of respiratory diseases in this population.Keywords: reference equations, impulse oscillometry, asthma, children, small airway impairment.
Correspondencia:E. MerazUniversidad Autónoma de Cd. Juárez, Cd. Juarez, México.Correo electrónico: [email protected]
Fecha de recepción:19 de noviembre de 2015
Fecha de aceptación:29 de diciembre de 2015

50 Revista Mexicana de Ingeniería Biomédica · volumen 37 · número 1 · Ene-Abr, 2016
RESUMENEl Sistema de Oscilometría Impulsos (por sus siglas en Inglés: IOS) ha sido reconocido como una herramienta
de diagnóstico útil. Investigaciones previas realizadas por nuestro grupo han demostrado que R5 (Resistencia a5 Hz), R5-R20 (dependencia a la frecuencia de la resistencia), AX (el “Triángulo de Goldman”) y el párametroCp (Capacitancia periférica) derivado del modelo extendido Resistencia-inductor-condensador (eRIC) son medidasfiables que monitorean la función del sistema respiratorio. El presente estudio determina las ecuaciones de predicciónde 112 niños Anglo e Hispanos asmáticos y no asmáticos, que previamente clasificados en cuatro grupos: Normal,PSAI (por su nombre en inglés: Probable daño en las vías aéreas menores), SAI (por su nombre en inglés: Daño enlas vías aéreas menores), y Asma. Las ecuaciones de predicción se determinaron mediante análisis de regresión deparámetros del IOS y del modelo eRIC (variables dependientes) contra edad, estatura y peso. La estatura mostróla mejor correlación con los parámetros del IOS y del modelo eRIC, proporcionando los valores de referencia mássignificativos para estas medidas en niños Anglos e Hispanos. Estos valores podrían servir como un marco de refenciaútil para el diagnóstico, intervenciones tempranas, y tratamiento de las enfermedades respiratorias en esta población.Palabras clave: ecuaciones de referencia, oscilometría de impusos, asma, niños, daño en las vías aéreasmenores.
INTRODUCTION
Asthma is caused by a combination of geneticand environmental factors. It is a syndromecomprising different signs and symptoms suchas cough, wheezing, shortness of breath, andchest tightness (1). Asthma is one of themost common diseases of childhood, causingsubstantial morbidity (2). More than 10million children in the USA under age 18(14%) have been diagnosed with asthma (3).According to Dorland’s medical dictionarySmall Airway Impairment (SAI) is a chronicobstructive bronchitis with narrowing of thebronchioles and small bronchi.
Pulmonary Function Testing (PFT) isof great importance in the evaluation andtreatment of respiratory diseases. Theadvances in technology have culminatedin the development of easier to use andcommercially available PFT instruments thathave been simplified in order to requireminimal patient maneuvering and efforts (4).
Spirometry has been one of the mostcommonly used methods of assessing lung
function in older children and adults(5). It has been demonstrated that bothpre-school and school-age children havedifficulty meeting some of the quality-controlcriteria outlined in the ATS/ERS guidelineswhen performing spirometry, and mostpediatricians may profess that the criticalperiod to evaluate pulmonary function is theinfantile period, since this is the age of onsetfor childhood asthma (6). Objective measuresfor diagnosis and treatment of childhoodasthma remain elusive (7), and the demandfor an index applicable in a clinical settingfor the evaluation of lung function in youngchildren had been specified (8).
Forced Oscillation Technique (FOT)is the general name for airway mechanicmeasurement using the noninvasivesuperimposition of pressure waves onthe subject’s airway during normal tidalbreathing. It has been noted however thata need for a practical FO index to defineairway obstruction exists (9).
Impulse Oscillometry is one type of FOT.It is a promising pulmonary function testing

Meraz et al. Reference equations for impulse oscillometric and respiratory system model parametersin anglo and hispanic children 51
method to diagnose and treat asthmaticpreschoolers, but there is a need for morestudies to be able to determine more preciselywhat IOS measures and what constitutesnormal values (6-7). Impulse Oscillometrymay be effectively employed in the diagnosisand management of diseases of the airways inchildren (10). IOS has also been recognizedto be a useful diagnostic tool in early asthmadevelopment and could generate objectiveoutcome measures of early interventions (11-12). IOS should be considered as bothan adjunct, and in some circumstances, asan alternative pulmonary function test tospirometry. It has been demonstrated thatIOS has greater sensitivity and specificityin comparison to spirometry in identifyingchildren with asthma and in determiningtheir improvement after treatment on thebasis of their bronchodilator responses (12-14). Other studies have established that IOScould be used to detect alterations in airwaymechanics over the course of therapy notreflected by spirometry and that IOS maybe capable of demonstrating airway growth-related changes over time (15-16).
Previous research by our groupdemonstrated that certain parameters of theequivalent electrical circuit models of thehuman respiratory system, the augmentedRIC (aRIC) and extended RIC (eRIC),along with those of the IOS parameters haveproven to be valuable in the diagnosis ofpatients with central and peripheral airwayobstruction (16-17).
Reference Equations offer concise andcompact quantitative means for evaluatingthe pulmonary function values of a singlepatient by comparing his or her data to thedistribution of measurements in a referencepopulation. Regression equations serveas effective and inexpensive alternatives todetermine expected values of respiratorysystem measures as a function of height,weight, and age (18).
The purpose of this study wasto determine predictive IOS Reference
Equations based upon data acquired from112 asthmatic and non-asthmatic Anglo andHispanic children, 5-17 years old, in orderto provide an original frame of reference fordifferent IOS and respiratory system modelparameters within this population.
The present article is the first inpublishing IOS Reference Equations forAnglo and Hispanic children 5 to 17 years oldas well as the first in calculating ReferenceEquations for IOS-based respiratory systemmodel parameters (eRIC-Rp and eRIC-Cp).
METHODS
Subjects
IOS pulmonary function testing wasperformed in Anglo and Hispanic children5-17 years old living in El Paso, Texas. Thedata were collected at Western Sky MedicalResearch Clinic and at a Health Fair heldat an elementary school located in the city’sSocorro school district in 2006. The acquireddata were then analyzed by our expertclinician and classified into four categories:Normal, Probable Small Airway Impairment(PSAI), Small Airway Impairment (SAI), andAsthma. A total of 112 children, 5 to 17years of age were tested: 52 females and60 males. The University of Texas at ElPaso (UTEP) Institutional Review Board(IRB) approved the research protocol. Aninformed consent form was given to everyparent and their child, providing them with adetailed description of the study. The study’spopulation demographics (Age, StandingHeight, and Weight) are shown in Table 1.
Table 1. Study PopulationTable 1. Study Population.
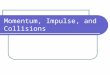
Figure 1. Histogram showing the distribution of the number of children with respect to their Heights.
Figure 2. eRIC model (17).
Demographics
Males and Females
Subject Range Mean ± SD
Age (years) 5 to 17 9.88 ± 3.62
Height (cm) 101.6 to 183.4 139.8 ± 21.31
Weight (kg) 14.5 to 93.8 41.02 ± 19.94
C
p
R
c
Rp
I

52 Revista Mexicana de Ingeniería Biomédica · volumen 37 · número 1 · Ene-Abr, 2016
Table 1. Study Population.
Figure 1. Histogram showing the distribution of the number of children with respect to their Heights.
Figure 2. eRIC model (17).
Demographics
Males and Females
Subject Range Mean ± SD
Age (years) 5 to 17 9.88 ± 3.62
Height (cm) 101.6 to 183.4 139.8 ± 21.31
Weight (kg) 14.5 to 93.8 41.02 ± 19.94
C
p
R
c
Rp
I
Figure 1. Histogram showing the distribution of thenumber of children with respect to their Heights.
Figure 1 shows the frequency distributionof all the study population as a function ofHeight (cm).
Regression equations
Regression analysis was used in thedetermination of the Reference Equationsfor this population. The use of bivariatelinear regressions provided the bestprediction models with higher significanceof independent variables, better thanMultivariate linear equations.
One approach to perform regressionanalysis is to use separate simple regressionequations for several different age groups.The square of the correlation coefficient (r2)and the Standard Error of the Estimate(SEE) are the most common measures of howwell the regression equations fit the data theydescribe. The proportion of variation in theobserved data represented by the independentvariables is measured by r2. The SEE isthe average Standard Deviation (SD) of thedata around the regression line. As regressionmethods reduce the differences between thepredicted and observed pulmonary functionmeasures in the reference population, thevalues of SEE will decrease and r2 willincrease (18).
IOS measurements
Impulse Oscillometry measures PulmonaryImpedance (Zr) during normal tidalbreathing of a subject. Zr is comprisedof Resistance (R) and Reactance (X)components, which are 90 electrical degreesout of phase. Resistance is indicative of theenergy required to propagate the pressurewave through the airways and Reactance isreflective of the amount of recoil generatedagainst that pressure wave. The Reactancecomprises forces of inertia resulting from theair movement in the conducting airways andthe elastic recoil of the lung tissue. R and Xare measured in either units of cmH2O/L/s orKPa/L/s. IOS measures pulmonary functionover a range of frequencies from 5 to 25Hz (cycles/sec). Acoustic waves with loweroscillation frequencies, such as 5 Hz, travelfarther to the lung periphery and provideindices of the entire pulmonary system,whereas waves with higher frequencies, suchas 20 Hz, provide information primarilyrelated to the central airways. Increasingevidence shows that the peripheral airwayshave an important role in asthma control;however none of the traditional tests(e.g. Spirometry) specifically measures theperipheral airways. IOS is increasingly beingused to separately measure the degree ofcentral and peripheral airway obstruction.Resistance at 5Hz minus Resistance at 20Hz (R5-R20) has been used as an index offrequency dependence of resistance (fdR),representing peripheral airways obstruction.Frequency dependence of resistance isinversely proportional to age: the younger thechild, the greater the R5-R20 value (10, 19).The Resonant Frequency (Fres) is the point atwhich reactance is zero. The Reactance Area(AX), also called the “Goldman Triangle”,is the integrated low frequency respiratoryreactance magnitude between 5Hz (X5) andFres. AX is a single metric that reflectschanges in the degree of peripheral airwayobstruction and closely correlates with fdR(20).

Meraz et al. Reference equations for impulse oscillometric and respiratory system model parametersin anglo and hispanic children 53
For this study, a Jaeger MasterScreenIOS (Viasys Healthcare, Inc. Yorba Linda,CA, USA) was used. The system wascalibrated every day before data collectionusing a 3-L syringe for volume calibrationsand a reference resistance (0.2 kPa/L/s) forpressure calibrations. Children were asked towear a nose clip, while breathing normallythrough a mouthpiece, and were instructedto close their lips tightly around it to avoidair leakage. Three to five IOS test replicateswere performed on each subject to ensurereproducible tests without artifacts causedby air leaks, swallowing, breath-holding, orvocalization. In each IOS test impulses wereapplied for a period of 30 to 45 seconds.IOS data were carefully reviewed offline andquality assured by our group’s resident expertclinician who rejected segments affected byairflow leaks or swallowing artifacts.
Respiratory Impedance Model
Extended RIC (eRIC) Model:This model was developed as an
improvement to the RIC model withan additional peripheral Resistance (Rp)connected in parallel with the Capacitance.Therefore, the eRIC model is composedof central (large airway) Resistance (Rc),large airway Inertance (I), peripheral (smallairway) Compliance (Cp), and peripheral(small airway) Resistance (Rp). This addedRp allows for the frequency dependenceof Resistance observed in impedance data.Figure 2 shows the eRIC model circuit.
Data analysis
The average values of the IOS and eRICmodel parameters were used in this studyto determine the Regression Equationsfor the four groups: Normal, ProbableSmall Airway Impairment (PSAI), SmallAirway Impairment (SAI), and Asthma.All of the statistical analyses in thisstudy were performed using SPSS 22Software (SPSS Inc., Chicago, IL, USA).
Table 1. Study Population.
Figure 1. Histogram showing the distribution of the number of children with respect to their Heights.
Figure 2. eRIC model (17).
Demographics
Males and Females
Subject Range Mean ± SD
Age (years) 5 to 17 9.88 ± 3.62
Height (cm) 101.6 to 183.4 139.8 ± 21.31
Weight (kg) 14.5 to 93.8 41.02 ± 19.94
Cp
Rc
Rp
I
Figure 2. eRIC model (17).
These equations were generated using simplelinear regression analysis with Height, Age,and Weight as independent variables.
RESULTS
Reference values are important indexesin establishing whether an individual’smeasured values fall within a range to beexpected for a healthy person with similarheight and age. Most of the previous studiesperformed to provide reference values forFOT and IOS parameters for children weredesigned for preschool children (21-28), asIOS has been proven to be of high significancein the assessment of the pulmonary system inthis population. Attractive practical featuressuch as: effort-free operation, minimalpassive cooperation from the subject wearinga nose clip while keeping tightly closed lipsaround a mouthpiece, and breathing normallythrough the mouth make the IOS a popularlung function test for small children who areunable to perform spirometry. Studies byother researchers have generated FOT andIOS Reference Equations for 2-20 year-oldchildren and young adults (29-33), whichare comparable to the results in the presentstudy.
Table 3 presents a summary of the studiesperformed using the Impulse Oscillometrytechnique to generate Reference Equationsfor children (23-28, 31-33).

54 Revista Mexicana de Ingeniería Biomédica · volumen 37 · número 1 · Ene-Abr, 2016
Table 2. Demographics for each classificationgroup.
Table 2. Demographics for each Classification Group
Table 3. Summary of IOS Reference Equations for children.
Table 3. Summary of IOS Reference Equations for children.
Table 2. Demographics for each Classification Group
Table 3. Summary of IOS Reference Equations for children.

Meraz et al. Reference equations for impulse oscillometric and respiratory system model parametersin anglo and hispanic children 55
A recent study by Hagiwara et al. (34)was published showing Reference Values forJapanese Children (6-15 years). In this studythe authors presented R5, R20 and R5-R25Reference values according to height in termsof standard deviation calculated with thelambda-mu-sigma (LMS) method. As onlyIOS Reference values and standard curves,for the mentioned parameters, were presentedand Reference Equations were not calculated,as in previous studies (21-33), it was notpossible for us to include that study in ourTable 3.
Also Santos Schivinski et al. (35) recentlyreported IOS Reference Equations forBrazilian Healthy children and adolescents.They tested 864 healthy school students aged6 to 14 years old. Only an abstract has beenpublished on this research and no ReferenceEquations were given.
In our previous work, we havedemonstrated that there are no significantdifferences between genders (36) and betweenethnic groups in this population (37). Wedid not observe gender or race significantdifferences in the same manner in ourinvestigation as it was demonstrated inprevious studies (24-25, 27).
In the present study Reference Equationsfor IOS and eRIC model parameters weregenerated based upon IOS data acquiredfrom 112 children, previously classified byour expert clinician, the late Dr. MichaelGoldman, into four groups: Normal, PSAI,SAI and Asthma. The Normal Groupwas composed of 11 children, PSAI of 17children, SAI of 54 children and Asthmaticof 30 children, respectively. In Table 2, thedemographics for each group are presented.
In Table 3 the following informationis presented: r = correlation coefficient,r2=coefficient of determination (the fractionof the data that is the closest to the lineof best fit), R = Resistance (kPa/L/s),X = Reactance (kPa/L/s), AX = theGoldman Triangle (kPa/L), Height (metersor centimeters), Age (years or months), and
Table 4. Regression equations for normal group.Table 4. Regression Equations for Normal Group.
Table 5. Regression Equations for PSAI Group.
Table 5. Regression equations for PSAI group.
Table 4. Regression Equations for Normal Group.
Table 5. Regression Equations for PSAI Group.
Weight (kilograms) for the mentioned studiesusing IOS (23-28, 31-33).
Our linear regression analysis indicatedthat IOS variables were well correlated withboth Height and Age, as found by Amra (31)and Gochioca-Rangel (33), but most stronglyassociated with Height as has been shown inprevious studies (23-29, 32). The ReferenceEquations generated in the present study asa function of Height are presented in Table

56 Revista Mexicana de Ingeniería Biomédica · volumen 37 · número 1 · Ene-Abr, 2016
Table 6. Regression equations for SAI group.Table 6. Regression Equations for SAI Group.
Table 7. Regression Equations for Asthma Group.
Table 7. Regression equations for asthma group.
Table 6. Regression Equations for SAI Group.
Table 7. Regression Equations for Asthma Group.
4 for Normal, Table 5 for PSAI, Table 6for SAI, and Table 7 for Asthmatic childrenrespectively; where r2 = the coefficient ofdetermination and SEE = the Standard Errorof the Estimate.
DISCUSSION
In contrast to our research, the studyperformed by Frei et al. (24), presented
Figure 3. R5 as function of Height for all children.
Figure 4. X5 as function of Height for all children.
Figure 3. R5 as function of Height for all children.
Figure 3. R5 as function of Height for all children.
Figure 4. X5 as function of Height for all children.
Figure 4. X5 as function of height for all children.
Reference Equations for solely white NorthAmerican children (3-10 years) with twowhite parents.
Our study is the first in publishingIOS Reference Equations for Anglo andHispanic children 5 to 17 years old. Alsois the first study in calculating ReferenceEquations for IOS-based respiratory systemmodel parameters (eRIC-Rp and eRIC-Cp).One of the advantages of our ReferenceEquations is that most of the significant IOSand model parameters resulted in r2 values

Meraz et al. Reference equations for impulse oscillometric and respiratory system model parametersin anglo and hispanic children 57
higher than 30%, with some of them reachingup to 60% and even to 80%, whereas previousstudies reported r2 values lower than 20%(26-27).
The regression equations with r2 valueshigher than 0.4 are highlighted in bold inTables 4 to 7. In the Normal Group,it can be observed that the resistancevalues R5 to R20 and R5-R20 present thehighest r2 values, showing these to be goodpredictors of normal parameters. In thePSAI, SAI, and Asthma Groups R5, X5,X10, X15, R5-R20, AX eRIC-Rp and eRIC-Cp have the greatest r2 values which seemto indicate that these parameters are thebest predictors for children with respiratoryimpairments. These results seem to confirmwhat Nowowiejska et al. have previouslyconcluded (32) by showing that reactancesmanifested greater specificity compared toresistances in assessing bronchial obstructionin children.
One of the limitations of our studywas that the Normal Group included solelysample data from children 11-17 yearsold. This could be the reason why ourR5 regression coefficient was lower thanthose reported in previous studies by otherresearchers (24-27). However, in spite of thislimitation, it is clear that Resistance valuesdecrease with Height and Age as expected.
In Figure 5, the reference equation for R5as a function of Height was compared withthose generated in previous studies, whichutilized simple linear regression equations torepresent their data. Our data are close tothose acquired by Nowowiejska et al. (32),who utilized a wider age range than the onesused in other studies, and it seems that theequations generated by Frei et al. (24), Parket al. (26), and Lai et al. (28) could have beensimilar to ours if we would have been ableto include data from younger normal childrenwith lower heights.
It can be observed in Figures 6 and 7 thatR5 increases with respiratory impairmentseverity, from normal to PSAI to SAI and
Figure 5. A comparison of the relationship between R5 and Height in our study and those of Frei, Park,
Lai and Nowowiejska(24, 26, 28, 32).
Figure 6. R5 Boxplot for the four groups in our study population
Figure 5. A comparison of the relationship betweenR5 and Height in our study and those of Frei, Park,Lai and Nowowiejska(24, 26, 28, 32).
Figure 5. A comparison of the relationship between R5 and Height in our study and those of Frei, Park,
Lai and Nowowiejska(24, 26, 28, 32).
Figure 6. R5 Boxplot for the four groups in our study population
Figure 6. R5 Boxplot for the four groups in ourstudy population.
Asthma. It can also be noticed that X5decreases with SAI and Asthma severity, inthe same progression as expected. In a similarmanner, Figure 8 shows that AX increaseswith respiratory impairment severity.

58 Revista Mexicana de Ingeniería Biomédica · volumen 37 · número 1 · Ene-Abr, 2016
Figure 7. X5 Boxplot for the four groups in our study population.
Figure 8. AX Boxplot for the four groups in our study population.
Figure 7. X5 Boxplot for the four groups in ourstudy population.
Figure 7. X5 Boxplot for the four groups in our study population.
Figure 8. AX Boxplot for the four groups in our study population.
Figure 8. AX Boxplot for the four groups in ourstudy population.
CONCLUSIONS
Impulse Oscillometry can serve as asensitive pulmonary function test performedin younger and older children todiagnose asthma and other pulmonaryconditions with relative ease and withoutrequiring extreme breathing maneuvers and
bronchoprovocation. It has been proven tobe useful in the assessment of respiratoryimpairments. Our investigation reported hereprovided IOS and eRIC model parameterReference Equations for four groups ofHispanic and Anglo children: Normal,PSAI, SAI and Asthma. These equationscould be used in the future to provide aquantitative framework for indication ofillness progression, or as a reference tool todiagnose the degree of respiratory systemimpairments in children in the 5 - 17 year-oldage group.
This work showed and validated thatHeight was the best determinant of IOSvariables. Resistance (R) correlatednegatively with Height, while Reactance (X)correlated positively as previously seen in theliterature.
Acknowledgements
The data collection for this research wassupported by NIH grant #1 S11 ES0133390-01 A 1: UTEP-UNM HSC ARCH Programon Border Asthma. HN and EGM wouldlike to dedicate this contribution to the lovingmemory of Dr. Michael Goldman, Professorof Medicine at the UCLA Medical School.We will remain eternally thankful for hismentoring in Pulmonary Physiology, FOTand IOS testing, for his collaboration, andfriendship. He will always be present in ourwork and our hearts.
REFERENCES
1. Panettieri R.A. Jr, Covar R, GrantE, Hillyer E.V., Bacharier L. “Naturalhistory of asthma: Persistence versusprogression - does the beginning predictthe end?” American Academy ofAllergy, Asthma & Immunology, vol.121, no. 3, pp. 607-613.
2. Asher M.I., Keil U., Anderson H.R.,Beasley R., Crane J., Martinez F.,

Meraz et al. Reference equations for impulse oscillometric and respiratory system model parametersin anglo and hispanic children 59
Mitchell E.A., Pearce N., Sibbald B.,Stewart A.W., Strachan D., WeilandS.K., Williams H.C. “Internationalstudy of asthma and allergies inchildhood (ISAAC): rationale andmethods.” European RespiratoryJournal, vol. 8, pp. 483-491.
3. Bloom B, Jones LI, Freeman G.“Summary health statistics for U.S.children: National Health InterviewSurvey 2012,” National Center forHealth Statistics, Vital Health Stat vol.10, no. 258, Hyattsville, Maryland,2013.
4. Escobar H., Carver T.W. “Pulmonaryfunction testing in young children.”Current Allergy and Asthma Reports,vol. 11, pp. 473- 481, 2011.
5. Larsen G.L., Brian Kang J-K., Guildbert T., Morgan W.“Assessing respiratory function inyoung children: Developmentalconsiderations.” American Academy ofAllergy, Asthma and Immunology, vol.115, no. 4, pp. 657-666, 2005.
6. Mochizuki H, Hirai K, Tabata H.“Forced oscillation technique andchildhood asthma.” AllergologyInternational, vol. 61, pp. 373-383,2012.
7. Galant SP, Nickerson B. “Lung functionmeasurement in the assessment ofchildhood asthma: recent importantdevelopments.” Current Opinion inAllergy and Clinical Immunology, vol.10, pp. 149-154, 2010.
8. Bisgaard H, Klug B. Lung functionmeasurement in awake young children.”Eur Respir J, vol. 8, pp. 2067-2075,1995.
9. Oostveen E, MacLeod D, LorinoH, Farre R, Hantos Z, DesagerK, Marchal F, “On behalf of the
ERS Task Force on RespiratoryImpedance Measurements. The forcedoscillation technique in clinical practice:methodology, recommendations andfuture developments.” Eur Respir J,vol. 22, pp. 1026-1041, 2003.
10. Komarow HD, Myles IA, Uzzaman A,Metcalfe DD. “Impulse oscillometry inthe evaluation of diseases of the airwaysin children.” Ann Allergy AsthmaImmunol, vol. 106, no. 3, pp. 191-199,2011.
11. Marota A, Klinnert MD, PriceMR, Larsen GL, Liy AH. “Impulseoscillometry provides an effectivemeasure of lung dysfunction in 4-year-old children at risk for persistentasthma.” J Allergy Clin Immunol, vol.112, no. 2, pp. 317-321, 2003.
12. Song TW, Kim KW, Kim ES, ParkJ-W, Sohn MH, Kim K-E. “Utility ofimpulse oscillometry in young childrenwith asthma.” Pediatr Allergy Immunol,vol. 19, pp. 763-768, 2008.
13. Gaylor PB, Saadeh CK, Goldman MD,Malacara JM, McGee MN. “Forcedoscilation using Impulse Oscillometry(IOS) provides objective responsesto Inhaled Corticosteroid (ICS) inasthmatic patients when FEV1 fails toimprove.” J Allergy and Clin Immun,vol. 111, art. S135, 2003.
14. Komarow HD, Skinner J, Young M,Gaskins D, Nelson C, Gergen PJ,Metcalfe DD. “A study of the use ofimpulse oscillometry in the evaluation ofchildren with asthma: analysis of lungparameters, order effect, and utilitycompared with spirometry.” PediatrPulmonol, vol. 47, no. 1, pp. 18-26,2012.
15. Larsen GL, Morgan W, Heldt GP,Mauger DT, Boehmer SJ, ChinchilliVM, Lemanske RF, Martinez F, Strunk

60 Revista Mexicana de Ingeniería Biomédica · volumen 37 · número 1 · Ene-Abr, 2016
RC, Szefler SJ, Zeiger RS, Taussig LM,Bacharier LB, Guilber TW, RadfordS, Sorkness CA. “Impulse oscillometryversus spirometry in a long-term studyof controller therapy for pediatricasthma.” J Allergy Clin Immunol, vol.123, no. 4, pp. 861-867, 2009.
16. Meraz EG, Nazeran H, Ramos CD,Nava P, Diong B, Goldman MD.“Analysis of impulse oscillometricmeasures of lung function andrespiratory system model parametersin small airway-impared and healthychildren over a 2 year period.”Biomedical Engineering Online Journal,vol. 10, pp. 1-21, 2011.
17. Diong B., Nazeran H., Nava P.,Goldman M.D. “Modeling humanrespiratory impedance.” IEEEEngineering in Medicine and BiologyMagazine, vol. 26, no. 1, pp. 48-55,2007.
18. American Thoracic Society. “Lungfunction testing: selection of referencevalues and interpretative strategies.”American Review of RespiratoryDisease, vol. 144, no. 5, pp. 1202-1218,1991.
19. Yixin S., Aledia A.S., GalantS.P., George S.C. “Peipheral airwayimpairment measured by oscillometrypredicts loss of asthma control inchildren.” American Academy ofAllergy, Asthma & Immunology, vol.131, no. 3, pp. 718-723, 2012.
20. Smith H.J., Reinhold P. GoldmanM.D. “Forced oscillation technique andimpulse oscillometry.” Eur Respir Mon,vol. 31, pp. 72-105, 2005.
21. Klug B, Bisgaard H. “Specific airwayresistance, interrupter resistance, andrespiratory impedance in healthychildren aged 2-7 years.” PediatrPulmonol, vol. 25, pp. 322-331, 1998.
22. Hellinckx J, De Boeck K, Bande-Knops J, van der Poel M, DemedtsM. “Bronchodilator response in 3-6.5year old healthy and stable asthmaticchildren.” Eur Respir J, vol. 12, pp.438-443, 1998.
23. Malmberg LP, Pelkonen A, Poussa T,Pohjanpalo A, Haahtela T, TurpeinenM. “Determinants of respiratory systeminput impedance and bronchodilatorresponse in healthy Finnish preschoolchildren.” Clin Physiol & Func Im, vol.22, pp. 64-71, 2002.
24. Frei J, Jutla J, Kramer G, Hatzakis GE,Ducharme FM, Davis GM. “Impulseoscillometry reference values in children100 to 150 cm in height and 3 to 10 yearsof age.” CHEST, vol. 128, pp. 1266-1273, 2005.
25. Denker M, Malmber LP, Valind S,Thorsson O, Karlsson MK, Pelkonen A,Pohjanpalo A, Haahtela T, TurpeinenM, Wollmer P. “Reference values forrespiratory system impedance by usingimpulse oscillometry in children aged 2-11 years.” Clin Physiol Funct Imaging,vol. 26, pp. 247-250, 2006.
26. Park JH, Yoon JW, Shin YH, JeeHM, Wee YS, Chang SJ, Sim JH,Yum HY, Han MY. “Reference valuesfor respiratory system impedanceusing impulse oscillometry in healthypreschool children.” Korean J Pediatr,vol. 2, pp. 64-68, 2011.
27. Lee JY, Seo J-H, Kim HY, Jung YH,Kwon J-W, Kim B-J, Kim HB, Lee S-Y,Jang GC, Song DJ, Kim WK, Shim JY,Kim H-J, Shin Y-J, Park J-W, Cho S-H, Lee J-S, Hong S-J. “Reference valuesof impulse oscillometry and its utility inthe diagnosis of asthma in young Koreanchildren.” Journal of Asthma, vol. 49,no. 8, pp. 811-816, 2012.

Meraz et al. Reference equations for impulse oscillometric and respiratory system model parametersin anglo and hispanic children 61
28. Lai SH, Yao TC, Liao SL, TsaiMH, Hua MC, Yeh KW, HuangJL. “Reference Values of ImpulseOscillometry in Taiwanese PreschoolChildren.” Pediatrics and Neonatology,vol. 56, pp. 165-170, 2015.
29. Ducharme FM, David M, DucharmeGR. “Pediatric reference values forrespiratory resistance measured byforced oscillation.” CHEST, vol. 113,pp. 1322-1328, 1998.
30. Clement J, Dumoulin B, GubbelmansR, Hendriks S, van de Woestijne KP.“Reference values of total respiratoryresistance and reactance between 4 and26 Hz in children and adolescents aged4-20 years.” Bull Eur PhysiopatholRespir, vol. 23, pp. 441-448, 1987.
31. Amra B, Soltaninejad F, GolshanM. “Respiratory resistance by impulseoscillometry in healthy Iranian childrenaged 5-19.” Iran J Allergy AsthmaImmunol, vol. 7, no. 1, pp. 25-29, 2008.
32. Nowowiejska B, Tomalak W, RadlinskiJ, Siergiejko G, Latawiec W,Kackzmarski M. Transient referencevalues for impulse oscillometry forchildren aged 3-18 Years.” PediatricPulmonology, vol. 43, pp. 1193-1197,2008.
33. Gochicoa-Rangel L, Torre-BouscouletL, Martínez-Briseño D, Rodríguez-Moreno L, Cantú-González G, VargasMH. “Values of impulse oscillometryin healthy Mexican children and
adolescents.” Respiratory Care, vol. 60,no. 1, pp. 119-127, 2015.
34. Hagiwara S, Mochizuki H, MuramatsuR, Koyama H, Yagi H, NishidaY, Kobayashi T, Sakamoto N.“Reference values for Japanesechildren’s respiratory resistance usingthe LMS Method.” AllergologyInternational, vol. 63, pp. 113-119,2014.
35. Santos Schivinski CI, Seabra deAssumpcao M, Maba Goncalves R,Martins R, Godoy Bobbio T. “Referenceequations for impulse oscillometrysystem parameters in Brazilianhealthy children and adolescents.”Physiotherapy vol. 101, no. 1, pp.eS645-eS646, 2015.
36. Meraz E, Nazeran H, Diong B, GoldmanM. “Modeling human respiratoryimpedance in anglo asthmaticchildren.” Biomedical EngineeringRecent Developments, Proceeding ofthe Twenty Third Southern BiomedicalEngineering Conference, pp. 108-113,2007.
37. Meraz E, Nazeran H, Diong B, NavaP, Goldman M. “Normal ImpulseOscillometry (IOS) lung functionparameters in adolescents residing inEl Paso, TX.” Biomedical EngineeringRecent Developments, Proceedings ofthe Twenty Third Southern BiomedicalEngineering Conference, vol. 18, no. 9,pp. 72, 2008.
ib

62 Revista Mexicana de Ingeniería Biomédica · volumen 37 · número 1 · Ene-Abr, 2016