Embed Size (px)
Citation preview
Invited paper
Reducing workplace violence by creatinghealthy workplace environments
Bob Bowen, Michael R. Privitera and Vaughan Bowie
Abstract
Purpose – The purpose for writing this paper is to help develop and apply integrated models and
methods of best practice that can prevent and manage workplace incivility (WPI) and workplace
violence (WPV).
Design/methodology/approach – This approach uses the framework of the public health model to
integrate neurobiological, behavioural, organisational, mental health, and educational theory into a
holistic framework for the primary, secondary, and tertiary prevention of WPV. The key concepts built into
this model are those of organisational violence (OV), trauma-informed services, and positive behaviour
support (PBS). This approach is further illustrated by case studies from organisations that have
successfully implemented safety protocols that demonstrate the effectiveness of such an integrated
approach. This method is derived primarily from qualitative data based on the expertise and experience
of the authors in the areas of psychiatry, social work research, and instructional implementation as well
as reviews of the current literature.
Findings – This model suggests that understanding WPI and violence as reactions to a combination of
internal and external stressors is key to interrupting these violent responses. Responding to WPV
requires that organisations first take responsibility for their own role in generating WPV and recognize the
impact of organisationally generated trauma on staff and services users. In this behavioural model, WPV
and WPI have functions which require the teaching of replacement behaviours that help individuals to
escape from these stresses in ways that do not cause harm to themselves and/or others. Thus,
management must instruct staff how to teach and reinforce appropriate social and communicative
behaviours in order to replace those behaviours leading to WPV and WPI.
Practical implications – The practical implications of this paper are that it provides human service
practitioners with: an understanding of the functions of reactive violence at work; a methodology to
identify different types WPI and WPV; a framework to proactively teach violence replacement
behaviours, empowering people to address the causative factors in ways that do not cause harm to self
and/or others; skills that can be taught to management and staff individually or in group settings, as well
as to service users; and implementation models from various organisations that have achieved
significant reductions in WPV. Another important outcome demonstrated through the case studies is that
significant financial savings can be achieved through reduction of WPI and WPV which may in turn lead
to a related improvement in the quality of life for staff and service users through changes in workplace
practices. This outcome has implications for organisational practice and theory as well as human
services education and training.
Social implications – One key social implication of the model, if integrated into the company’s social
responsibility policies and practices, is the potential for improving the quality of life for staff and patients
in health care settings as well as employees, customers, and service users in other settings.
Originality/value – The originality shown in this paper is the way the three key concepts of OV,
trauma-informed services, and PBS are built into a public health model to prevent and mitigate WPV. This
paper is of particular value to boards of management, organisational directors, supervisors, HR and
training departments as well as direct care staff, service providers, and regulatory bodies.
Keywords Workplace, Violence, Workplace incivility, Positive behaviour support
Paper type Research paper
DOI 10.1108/17596591111187710 VOL. 3 NO. 4 2011, pp. 185-198,Q Emerald Group Publishing Limited, ISSN 1759-6599 j JOURNAL OFAGGRESSION, CONFLICTAND PEACERESEARCH j PAGE185
Bob Bowen is the CEO of
The Mandt System, Inc.,
Richardson, Texas, USA.
Michael R. Privitera is an
Associate Professor of
Psychiatry at the University
of Rochester Medical
Center, Rochester,
New York, USA.
Vaughan Bowie is an
Adjunct Fellow at the
University of Western
Sydney, Sydney, Australia.

Introduction
Workplace violence (WPV) between staff in organisations is estimated to cost organisations
in the US$4.2 billion per year in lost time and productivity (Tunajek, 2007). By understanding
the cumulative effect of workplace incivility (WPI), a low level form of WPV that could be
non-physical or physically deviant behaviour violating norms of mutual respect (Andersson
and Pearson, 1999), a behavioural model emerges. This model suggests that simply
educating staff about WPV and WPI is insufficient, and that understanding incivility and
violence as responses to a combination of internal and external stressors is key to
interrupting these violent responses. In this behavioural model, WPVandWPI have functions
which require the teaching of replacement behaviours that help individuals to escape from
these stresses in ways that do not cause harm to themselves and/or others. This requires that
organisations first take responsibility for their own role in generating WPV and then instruct
management staff how to teach and reinforce appropriate social and communicative
behaviours in order to replace those behaviours leading to WPV and WPI. Case examples
from organisations that have successfully implemented safety protocols will be presented
with specific training and leadership actions that can be replicated in other workplaces.
Violence in the workplace continues to escalate in the human service industry. According to
the US Bureau of Labor Statistics:
[. . .] a worker in health care and social assistance is nearly five timesmore likely to be the victim of
a nonfatal assault or violent act by person than the average worker in all industries combined.
At the same time that non-fatal declined in private industries, they increased slightly in
human services, according to this same report. Hospitals in the USA have 29.5 percent of
the employees in human services, but account for 40.1 percent of all non-fatal injuries
(Janocha and Smith, 2010). Whilst injuries to workers were decreasing in all other work
settings, health care workers risk of injury increased in the last ten years in the USA. Data in
the UKmirrors this trend, with 15.3 percent of life science and health professionals subjected
to WPV and 15.2 percent of health and social work employees reporting they have
experienced WPV (Paterson et al., 2008). As pervasive as these measurements of violence
are, most experts agree that the prevalence, intensity and effects of WPVare under-reported
(Privitera and Arnetz, 2011). The authors will focus on the presence of those positive aspects
of healthy organisational structures that give hope to the wounded persons who come to
health care settings in search of healing.
The International Labour Organisation has developed the following definition of WPV:
Any action, incident or behaviour that departs from reasonable conduct in which a person is
assaulted, threatened, harmed, injured in the course of, or as a direct result of, his or her work.
Internal workplace violence is that which takes place between workers, including managers and
supervisors. External workplace violence is that which takes place between workers (and
managers and supervisors) and any other person present at the workplace.
Whilst we go through the process of identifying violent behaviour, we must not lose sight of
the fact that some violence is a reaction to the culture of the organisation itself. What would
be a dysfunctional behaviour in a healthy and functional organisational climate can be seen
as a coping mechanism in an unhealthy, dysfunctional environment. It is not just ‘‘bad
apples’’ that must concern us, we must also focus on the possibility of a ‘‘bad barrel’’ (Bowie,
2010). When focusing on individuals (patients or staff in the health care system), such an
approach operates on a ‘‘bad apple’’ response to managing and preventing violence in the
workplace. However, there has been growing awareness of the role organisations may play
in creating oppressive and violent climates within their workplace, that may in turn trigger
violence by staff, patients, or others. This latter approach is the ‘‘bad barrel’’ approach to
managing WPV (Bowie, 2006).
Bowie (2011) expanded on this definition by adding the concept of organisational violence
(OV) in which ‘‘organizations knowingly and unnecessarily place their workers or clients in
dangerous or violent situations or allow a climate of abuse, bullying, or harassment to thrive
in the workplace’’. It is a relatively new construct to understand that the context of staff
PAGE 186 j JOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj VOL. 3 NO. 4 2011

behaviour includes the policies and procedures of an organisation, as well as their practices,
which constitute unwritten policies and procedures (Sims and Keon, 1999). OV can be a
causative factor in both staff to staff violence and client to staff violence, as well as other
types of WPV (Bowie, 2011).
WPV can be present at various levels of intensity, and at its’ lower spectrum is known as WPI.
At all levels, these behaviours are used by staff in response to perceived stressors in their
work environments. WPI is defined as:
[. . .] low-intensity deviant behaviour with ambiguous intent to harm the target, in violation of
workplace norms for mutual respect. Uncivil behaviours are characteristically rude and
discourteous, displaying a lack of regard for others (Andersson and Pearson, 1999, p. 457).
WPI is calculated to cost $11,581 per nurse per year in lost productivity in the USA (Lewis
and Malecha, 2011).
Although causal factors for aggression range in the biological, psychological, and social
spectra of human experience (Ferns, 2007), often described collectively as biopsychosocial
causes, the two general types of aggression that more rapidly differentiate on basis of
motive are instrumental (sometimes referred to as predatory) and reactive (affective)
(Cornell et al., 1996; McElliskem, 2004). Instrumental aggression is goal directed and
planned aggression whereas reactive includes arousal such as hostility.
The authors understand that some models of violence postulate combinations of the two
types, and differentiate various causal factors mentioned here. However, the dichotomous
model provides staff with an ability to more easily understand in the moment that the violence
is not directed at them personally. By de-personalizing the behavioural interactions, staff is
empowered to analyze the behaviour instead of reacting to it, and consequently decreasing
the likelihood the interaction will escalate.
Table I, taken from the Society for Research in Child Development (2007), provides a
framework for assessing the two types of violence and in teaching staff how not to engage in
aggression, but to use other behaviours to achieve the same goals of violence.
Most episodes of WPV begin as reactive rather than instrumental forms of aggression
(Keashly, 2005) and hence are the focus of this paper. The effect of reactive aggression can
be lessened by teaching people who want to ‘‘get back’’ at the people or person who
harmed them in some way to respond using their cognitive analytical skills rather than to
react using primarily emotionally based behaviours. To do this, however, people must
de-escalate. An increase of 20 percent in pulse significantly decreases the ability of people
to use cognitive skills and as a result interactions, between people when they have
escalated, are often aggressive and conflictual (Gottman and Levenson, 1988).
After staff experience WPI and WPV, the natural human response may be to escalate into
reactive violence. In order to de-escalate in a healthy manner, one must affirm their feelings
after experiencingWPI and/orWPV, and then choose abehaviour that addresses the issues in
away that leads to resolutionof the conflict (Mandtet al., 2008). This approachalso empowers
staff to identify their feelings after a real or perceived event and affirm those feelings
Table I Understanding aggression to assist with responding
Feature Instrumental aggression Reactive aggression
Cue source/type Internal ExternalMotive Personal gain (acquisition) Harm the stimulus/antecedent (escape)Premeditation Yes NoImpulsivity Low HighEmotion Calm AngryMoral cognition Actions morally discounted Actions justified or deserved
Source: Society for Research in Child Development (2007)
VOL. 3 NO. 4 2011 jJOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj PAGE 187
in themselves. Choosing behaviours to address the issues in a way that leads to a positive
resolution of the conflict is the goal of programmes that address all forms of violence.
Separating the two types of violence in order to craft responses that are preventative and
incorporating the models described above allows us to view reactive aggression as an
attempt to escape from a perceived dysfunctional situation. Aggression can then be seen as
a coping mechanism to help people to escape from people or situations that cause them
stress (Ursin and Olff, 1995).
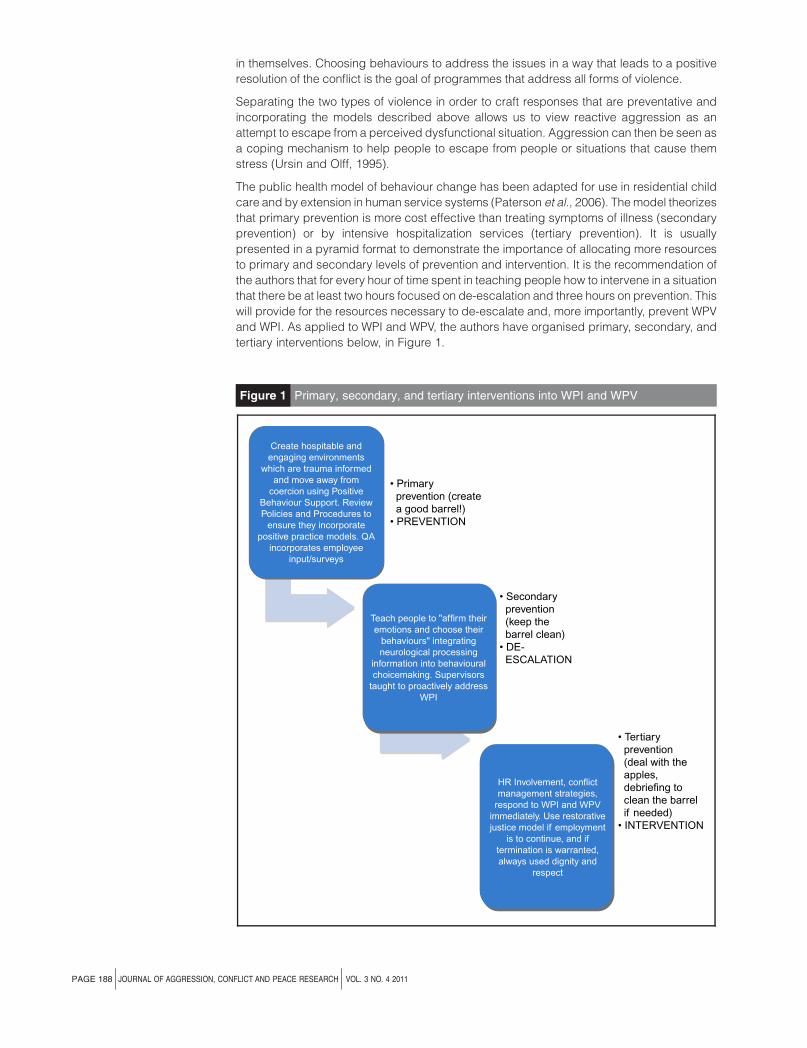
The public health model of behaviour change has been adapted for use in residential child
care and by extension in human service systems (Paterson et al., 2006). Themodel theorizes
that primary prevention is more cost effective than treating symptoms of illness (secondary
prevention) or by intensive hospitalization services (tertiary prevention). It is usually
presented in a pyramid format to demonstrate the importance of allocating more resources
to primary and secondary levels of prevention and intervention. It is the recommendation of
the authors that for every hour of time spent in teaching people how to intervene in a situation
that there be at least two hours focused on de-escalation and three hours on prevention. This
will provide for the resources necessary to de-escalate and, more importantly, prevent WPV
and WPI. As applied to WPI and WPV, the authors have organised primary, secondary, and
tertiary interventions below, in Figure 1.
Figure 1 Primary, secondary, and tertiary interventions into WPI and WPV
Create hospitable andengaging environments
which are trauma informedand move away from
coercion using PositiveBehaviour Support. ReviewPolicies and Procedures to
ensure they incorporatepositive practice models. QA
incorporates employeeinput/surveys
Teach people to "affirm theiremotions and choose their
behaviours" integratingneurological processing
information into behaviouralchoicemaking. Supervisors
taught to proactively addressWPI
HR Involvement, conflictmanagement strategies,
respond to WPI and WPVimmediately. Use restorativejustice model if employment
is to continue, and iftermination is warranted,always used dignity and
respect
• Tertiary prevention (deal with the apples, debriefing to clean the barrel if needed)• INTERVENTION
• Secondary prevention (keep the barrel clean)• DE- ESCALATION
• Primary prevention (create a good barrel!)• PREVENTION
PAGE 188 j JOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj VOL. 3 NO. 4 2011
Primary prevention
Instead of focusing just on the ‘‘bad apples’’ (Rhodes et al., 2010) who are often blamed for
WPI and WPV, our focus is also on the barrel holding the apples. All behaviour occurs within
a social context and within organisations that context is the culture of the organisation. The
goal of intervention is to help organisations move from a toxic to a beneficial culture in which
staff can do their work more effectively (Bowie, 2010).
As WPV and WPI occur within complex workplace systems, Figure 1 shows how they can
associate with each other. Prevention of WPVandWPI must have systemic components, and
focus on all four of the major areas, not just one. For instance, organisation with ‘‘state of the
art’’ policies and procedures, trauma-informed leadership (having basic understanding of
how trauma affects the life of the individual-seeking services), and a non-coercive climate,
can still experience WPV and WPI because of situational stresses interacting with personal
traits. An important and often overlooked concept in understanding organisational cultures
and climates is the perceptions of employees within the organisation (Griffin et al., 2000). An
organisation that believes it has ‘‘state of the art’’ policies and procedures and Human
Resource functions that support employees only has them if the perception of employees
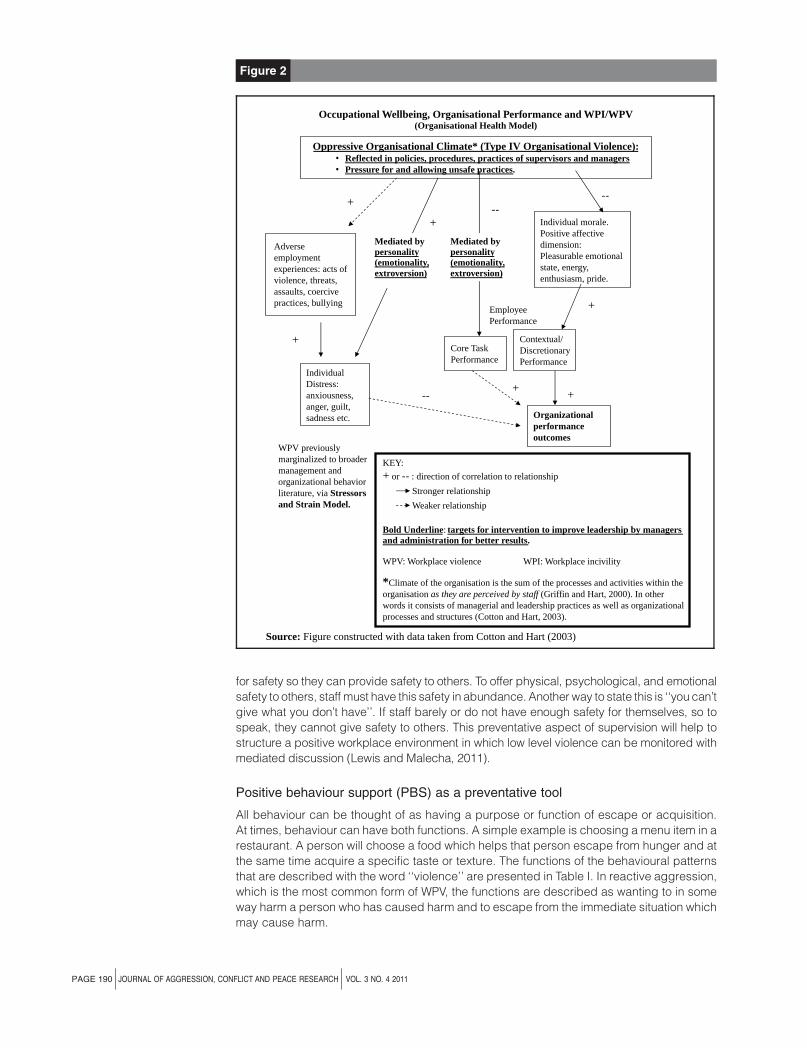
validates them. Figure 2, which shows a great deal of research, links together the concepts
of WPV/WPI, organisational wellbeing and organisational performance using an
organisational health model (Cotton and Hart, 2003). Previously, the stressors and strain
model, which dominated occupational stress research over 30 years, failed to link the stress
process with organisational performance. As such, occupational stress had been formerly
marginalised into the broader management and organisational behaviour literature, and had
been relegated to lower hierarchy of concern to organisational administration (Wright and
Cropanzano, 2000; Hart and Cooper, 2001).
In human service and health care settings, morale is suffering as a result of the increase in
WPI and WPV, reflected in the data from the US Bureau of Labor Statistics. Roger Fallott has
written extensively on the concept of ‘‘Trauma-informed Services,’’ (Fallot, 2011). By being
aware of the trauma histories of people, patients and staff alike, organisations can create a
service structure that is, in Fallott’s words, ‘‘hospitable and engaging’’. The process of
engaging staff is seen in the many examples of success in organisations that use a variety of
staff surveys to assess and address issues of OV and the cultures which inadvertently
support it (Cotton and Hart, 2003; Possibilities, 2008).
Hospitable environments are those which invite other people into the environment through an
admissions process with the promise of emotional, psychological, and physical safety.
These three levels of safety are seen in statutes on abuse, which prohibit physical abuse,
emotional abuse, and psychological abuse (CMS, 2006). Many organisations do a credible
job of providing this level of hospitality to individuals served, but less so to the staff who serve
them. Reducing WPI and WPV toward staff needs to be re-assessed as a quality of care
variable of interest to regulatory agencies, as mounting evidence show that WPV toward staff
ultimately affects quality of care provided to patients (Arnetz and Arnetz, 2001; Privitera and
Arnetz, 2011).
Engaging environments empower individuals served to direct the process of their own
recovery, habilitation or rehabilitation. This requires a shift from traditional behaviour
management models which focus on reinforcement and punishment to change behaviour to
the model of positive behaviour support (PBS). This shift in philosophy and belief has been
made in many health and social service settings as behaviour change theories are applied to
client behaviour. However, behaviour change efforts in addressing how staff interacts with
one other continue to use punishment-based models.
There is a common concept which states, ‘‘you can only give what you have in abundance’’.
Human service andhealth care environments are stressful andprovide services to apopulation
whose acuity needs are increasing. At the same time, the concept of ‘‘display rules’’
(Cropanzanoet al., 2004) states that when employees cannot display the emotionswithin them,
their stress level will increase. Supervisory and managerial staff must recognise this process
andoffer support to their staff inorder toprovide themwithenvironmentswhichmeet their needs
VOL. 3 NO. 4 2011 jJOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj PAGE 189
for safety so they can provide safety to others. To offer physical, psychological, and emotional
safety to others, staff must have this safety in abundance. Another way to state this is ‘‘you can’t
give what you don’t have’’. If staff barely or do not have enough safety for themselves, so to
speak, they cannot give safety to others. This preventative aspect of supervision will help to
structure a positive workplace environment in which low level violence can be monitored with
mediated discussion (Lewis and Malecha, 2011).
Positive behaviour support (PBS) as a preventative tool
All behaviour can be thought of as having a purpose or function of escape or acquisition.
At times, behaviour can have both functions. A simple example is choosing a menu item in a
restaurant. A person will choose a food which helps that person escape from hunger and at
the same time acquire a specific taste or texture. The functions of the behavioural patterns
that are described with the word ‘‘violence’’ are presented in Table I. In reactive aggression,
which is the most common form of WPV, the functions are described as wanting to in some
way harm a person who has caused harm and to escape from the immediate situation which
may cause harm.
Figure 2
Source: Figure constructed with data taken from Cotton and Hart (2003)
Oppressive Organisational Climate* (Type IV Organisational Violence):• Reflected in policies, procedures, practices of supervisors and managers• Pressure for and allowing unsafe practices.
Adverseemploymentexperiences: acts ofviolence, threats,assaults, coercivepractices, bullying
IndividualDistress:anxiousness,anger, guilt,sadness etc.
Core TaskPerformance
Contextual/DiscretionaryPerformance
Individual morale.Positive affectivedimension:Pleasurable emotionalstate, energy,enthusiasm, pride.
WPV previouslymarginalized to broadermanagement andorganizational behaviorliterature, via Stressorsand Strain Model.
EmployeePerformance
Mediated bypersonality(emotionality,extroversion)
Mediated bypersonality(emotionality,extroversion)
- -
- -
- -
+
+
Organizationalperformanceoutcomes
+
+
+
+
KEY:
+ or - - : direction of correlation to relationship
Stronger relationship
Weaker relationship
Bold Underline: targets for intervention to improve leadership by managersand administration for better results.
WPV: Workplace violence WPI: Workplace incivility
*Climate of the organisation is the sum of the processes and activities within theorganisation as they are perceived by staff (Griffin and Hart, 2000). In otherwords it consists of managerial and leadership practices as well as organizationalprocesses and structures (Cotton and Hart, 2003).
Occupational Wellbeing, Organisational Performance and WPI/WPV(Organisational Health Model)
PAGE 190 j JOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj VOL. 3 NO. 4 2011

The concept of ‘‘escaping to safety’’ (Lindsay, 2000) rather than attacking the threat is a very
helpful construct in the prevention of WPI and WPV. In animal research, prey animals are not
stressed by the presence of a predator, but rather by an inability to detect their presence
(reduced predictability) and having escape routes to safety blocked. Using PBS to structure
personnel policies, teach supervisory and managerial skill and focus on creating an
organisational culture which teaches staff what to do (known as positive practice) can
provide a predictable environment in which emotional, psychological, and physical safety
can be established for staff and service users.
PBS can be described as a way to help people acquire the goals of their behaviour (the
antecedent) in ways that do not cause harm to themselves and/or others. By identifying the
antecedent events and using a structural analysis of the antecedent (Stichter et al., 2004),
prevention can be accomplished in a way that also teaches the individual to use different
behaviours the next time they encounter the same or similar event(s). Rather than focusing
on consequences to teach behaviour change, a structural analysis identifies the component
elements of the antecedent – ‘‘what do you really want – and then rearranges the antecedal
conditions’’. Using this approach to identify the variety of events that precede violent
behaviour will help individuals and organisations move from a reactive to a proactive
methodology of violence prevention.
Central to PBS is the understanding that staff who use PBS, ‘‘continually move away from
coercion’’ in all forms (NAU, 2005). Rather than seek compliance, PBS models invite people
to cooperate by building a relationship based on dignity and respect, and finding ways to
motivate people to change their behaviour through an invitational and collaborative process
rather than an externally imposed process of compliance (Bowen, 2009).
In the workplace, what this means is that the focus of the organisation must be one of taking
the lead in creating safe environments – physical, emotional, psychological. When people
feel safe they are free to focus on relationships, which in many cases are the foundation for
achievement. This approach is highlighted in the work of Maslow (1954), in which he
postulated that after the need for basic human sustenance, human beings needed safety.
The physical, psychological, and emotional safety of human beings is a pre-requisite
for healthy neurological development in children (Perry, 2000a) and to the continuing
development of those social structures that bind us together in human communities.
Thus, the leadership of the organisation must commit to this process of ‘‘continually moving
away from coercion’’ and restructure relationships at a level far deeper than simply reframing
the organisational chart. One example is the flexible matrix of relationships at the Treasure
Coast Forensic Treatment Center in the USA (Vanderberg and Bowen, 2011) which
incorporates security guards, psychiatric aides, nurses, therapists, psychologists and
psychiatrists into a holistic treatment team. Each member of the team is able to share their
perceptions of patient behaviour and be informed by the perceptions of other team
members. These relationships of equality of worth with a difference of roles (Bowen, 2006)
has led to the virtual elimination of seclusion and restraint with only two staff injuries resulting
in time lost from work at that organisation in 2010.
Personnel policies and procedures generally approach the question of changing employee
performance through punitive rather than positivemeasures, the ‘‘bad apple’’ approach. The
use of punitive responses such as unpaid suspension, letters of reprimand, employment
reviews, etc. are generally speaking, ineffective at changingbehaviour in the long-term (Mohr
andBowen, 2009). Theworddiscipline at its rootmeaning is supposed tobe teach, but no one
has ever looked forward to their next employee discipline meeting (Bowen, 2011). In the
creation of cultures that support instead of abuse employees, personnel policies must be
changed to reflect a continual move away from coercive practices in changing the behaviour
of people.
Secondary prevention – de-escalation
In their studies of organisational health in Australia, Cotton and Hart (2003) were concerned
with the relationship between occupational wellbeing and organisational performance. They
VOL. 3 NO. 4 2011 jJOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj PAGE 191
posited that for occupational wellbeing to be meaningful to the organisation, it must be tied
to organisational performance (Cotton and Hart, 2003). Distress on the job is a separate
concept from morale and makes independent contributions to overall employee wellbeing.
Organisational climate is a broader concept relating to how employees perceive the way in
which their workplace functions (Griffin et al., 2000), consisting of perceptions-concerning
leadership and managerial practices, as well as organisational structures and processes.
These organisational structures and processes consist of appraisal and recognition
processes, decision-making styles, clarity of roles and alignment of goals of the organisation,
etc. (James and McIntyre, 1996; Hart and Cooper, 2001). The emotional impact of these
organisational factorsonmoralearemore influential thanadverseemployment experiencesof
stress (Hart et al., 1997). This is true across different types of professions, regardless of the
adverse employment experiences (i.e. true for police and true for teachers, etc.). In other
words, positive practice models in which employees are directed towards ‘‘what to do’’
instead of ‘‘what not to do’’ will provide the individual and organisational morale needed to
overcome the effects of WPI and WPV.
Leaders who understand the power of participation through feedback systems such as
employee surveys and then utilise them, can mitigate much of the stress which is part of all
work environments. Leadership is the most critical factor in moving away from coercion and
towards creating hospitable and engaging organisations (Huckshorn, 2004). When leaders
create a vision and empower others to not only share it but also build on it, WPV has been
reduced dramatically. Examples include Pennsylvania’s psychiatric hospitals (Smith et al.,
2005) and reductions of violence in an adolescent unit in a psychiatric hospital in
Massachusetts (LeBel and Goldstein, 2005).
When de-escalation is necessary, it is often because the preventative steps were ineffective.
Organisations sometimes look at escalation into WPI andWPVas symptomatic only of issues
amongst staff. It is critical, however, that the organisational culturebeassessed todetermine if
there was a causative factor, or setting event within policies and procedures, supervisory
practices, etc.
Teaching people to ‘‘affirm their emotions and choose their behaviours’’ (Mandt et al., 2008)
empowers them to affirm the validity of their emotions, whilst at the same time choosing
behavioural responses that are not violent. This approach can decrease impulsivity and
move people away from reactive violence and towards a cognitively driven model in which
we choose to act in a rational and not emotive manner. By affirming the underlying emotions,
we do not denigrate or deny emotion; rather we validate the feeling and choose the
behaviour that helps us achieve our goals.
However, in order toprevent violence fromoccurring, the antecedent events, including setting
events, must be identified (Crone and Horner, 2003). When people respond to a behaviour
without any clear understanding of its preceding events, they will most likely form part of a
power struggle with the individual because they do not know what the individual wanted to
accomplish through their behaviour. The first step of prevention in cases of client on staff and
staff on staff violence must, therefore, be the identification of the antecedent events.
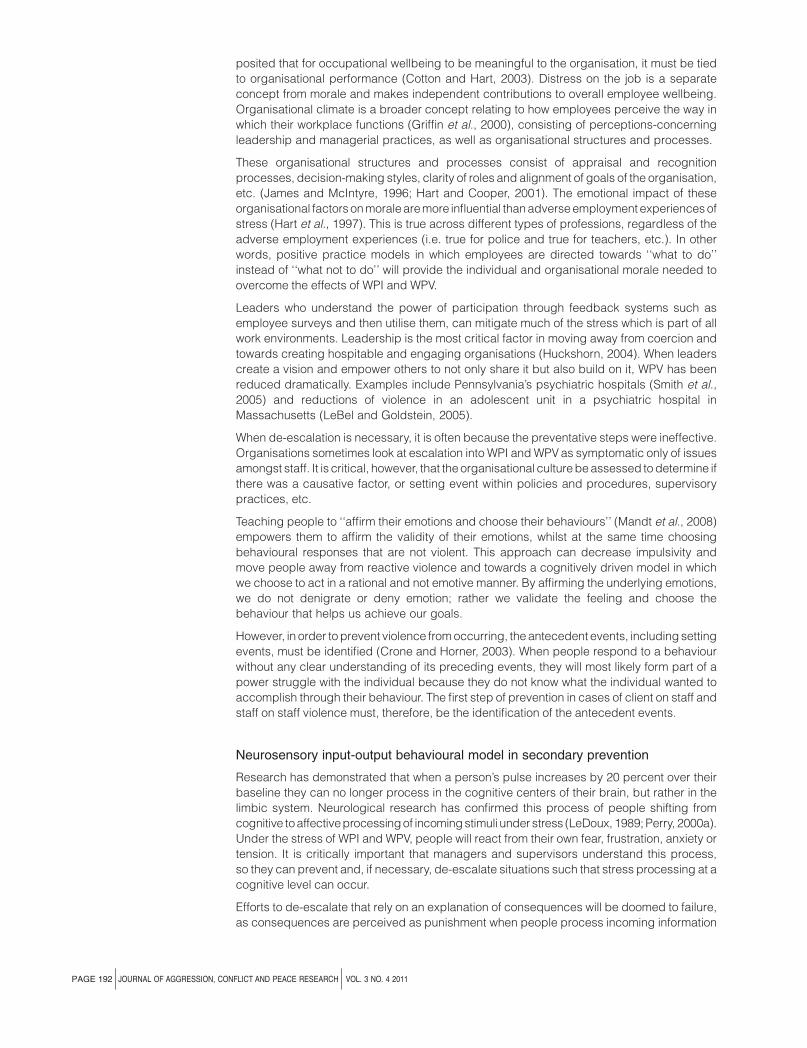
Neurosensory input-output behavioural model in secondary prevention
Research has demonstrated that when a person’s pulse increases by 20 percent over their
baseline they can no longer process in the cognitive centers of their brain, but rather in the
limbic system. Neurological research has confirmed this process of people shifting from
cognitive toaffectiveprocessingof incomingstimuli under stress (LeDoux, 1989;Perry, 2000a).
Under the stress of WPI and WPV, people will react from their own fear, frustration, anxiety or
tension. It is critically important that managers and supervisors understand this process,
so they can prevent and, if necessary, de-escalate situations such that stress processing at a
cognitive level can occur.
Efforts to de-escalate that rely on an explanation of consequences will be doomed to failure,
as consequences are perceived as punishment when people process incoming information
PAGE 192 j JOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj VOL. 3 NO. 4 2011
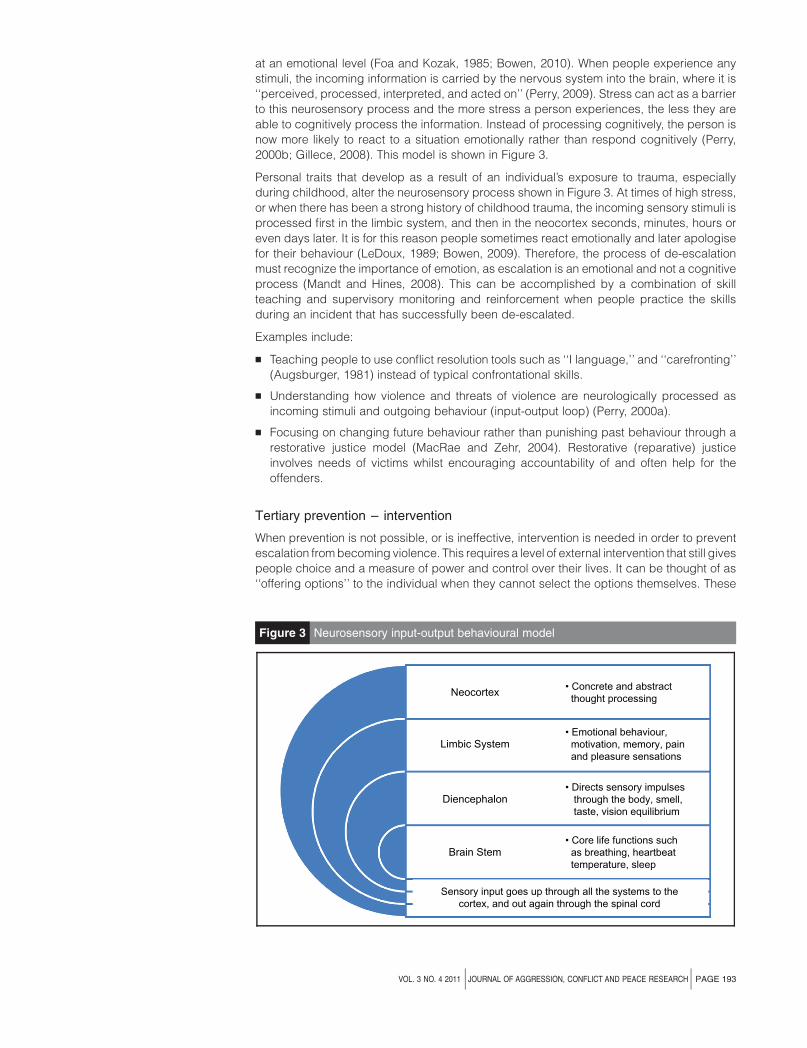
at an emotional level (Foa and Kozak, 1985; Bowen, 2010). When people experience any
stimuli, the incoming information is carried by the nervous system into the brain, where it is
‘‘perceived, processed, interpreted, and acted on’’ (Perry, 2009). Stress can act as a barrier
to this neurosensory process and the more stress a person experiences, the less they are
able to cognitively process the information. Instead of processing cognitively, the person is
now more likely to react to a situation emotionally rather than respond cognitively (Perry,
2000b; Gillece, 2008). This model is shown in Figure 3.
Personal traits that develop as a result of an individual’s exposure to trauma, especially
during childhood, alter the neurosensory process shown in Figure 3. At times of high stress,
or when there has been a strong history of childhood trauma, the incoming sensory stimuli is
processed first in the limbic system, and then in the neocortex seconds, minutes, hours or
even days later. It is for this reason people sometimes react emotionally and later apologise
for their behaviour (LeDoux, 1989; Bowen, 2009). Therefore, the process of de-escalation
must recognize the importance of emotion, as escalation is an emotional and not a cognitive
process (Mandt and Hines, 2008). This can be accomplished by a combination of skill
teaching and supervisory monitoring and reinforcement when people practice the skills
during an incident that has successfully been de-escalated.
Examples include:
B Teaching people to use conflict resolution tools such as ‘‘I language,’’ and ‘‘carefronting’’
(Augsburger, 1981) instead of typical confrontational skills.
B Understanding how violence and threats of violence are neurologically processed as
incoming stimuli and outgoing behaviour (input-output loop) (Perry, 2000a).
B Focusing on changing future behaviour rather than punishing past behaviour through a
restorative justice model (MacRae and Zehr, 2004). Restorative (reparative) justice
involves needs of victims whilst encouraging accountability of and often help for the
offenders.
Tertiary prevention – intervention
When prevention is not possible, or is ineffective, intervention is needed in order to prevent
escalation frombecoming violence. This requires a level of external intervention that still gives
people choice and a measure of power and control over their lives. It can be thought of as
‘‘offering options’’ to the individual when they cannot select the options themselves. These
Figure 3 Neurosensory input-output behavioural model
• Emotional behaviour, motivation, memory, pain and pleasure sensations
• Directs sensory impulses through the body, smell, taste, vision equilibrium
• Core life functions such as breathing, heartbeat temperature, sleep
• Concrete and abstract thought processing
Neocortex
Limbic System
Diencephalon
Brain Stem
Sensory input goes up through all the systems to thecortex, and out again through the spinal cord
VOL. 3 NO. 4 2011 jJOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj PAGE 193

external controls can be systemic in nature, such as policies and procedures identifying
specificmeasures to take in case of violence, or they can be protective responses to address
specific threats on a case by case basis.
It is at thepoint of intervention that organisations often resort to punitivepractices that become
part of the oppressive culture. It is important to hold true to the valueswe hold especially aswe
intervene. The models of Restorative Justice and PBS (Ross, 2009) also work during the
intervention process. At the University of Rochester Medical Center (Farley-Toombs, 2011),
administrators demonstrated their belief in a multidisciplinary process by clarifying roles and
staff procedures allowed with violent patients. As a result, there was a marked reduction in
patient to staff assaults and patient on patient assaults. These same principles have been
shown to work in reducing WPV between staff as an intervention protocol (International
Institute for Restorative Practices, 2011).
In the opinion of the authors, the path towards reduction in WPI andWPV involves continually
moving away from coercion and applying the same principles of non-coercive behaviour
change used with service recipients to the service providers, and thus changing
organisational cultures. This systems level approach has resulted in significant savings in
many organisations, including:
1. Grafton (Sanders and Gaynor, 2010) which was able, over a 4 year period, to:
B Reduce physical restraint by 99.7 percent.
B Reduce client-related injuries to staff by 41.2 percent.
B Reduce lost time expenses from client-related injuries by 94 percent.
B Save $5,785,437 in costs over a five-year period.
2. Community Memorial Hospital in Menominee Falls, Wisconsin was able to work with all
stakeholders to eliminate workers compensation costs due to patient aggression, and
has continued to focus on reducing all types of violence within the hospital.
3. Developmental Services of Nebraska, a provider of residential services for people
affected by intellectual and developmental disabilities, worked with their staff to virtually
eliminate restraint, and is now moving towards a system of ‘‘coercion free services’’
(Possibilities, 2008).
Conclusion
The authors started this paper with data on increases in injuries in human service and health
care settings. Despite prevention efforts over the last several decades, and individual
instances of significant reduction in the use of restraint, WPI andWPVare increasing. A study
presented at the 7th European Congress on Violence in Clinical Psychiatry (Putkonen et al.,
2011) showed that in a randomized study, the use of restraint and seclusion was dramatically
reduced during the study, but after the study ended, seclusion and restraint rates returned to
their previous levels. Rather than focus on the causative factors of what causes OV, WPI and
WPV, the authors focused on those positive aspects of organisational structures that give
hope to the wounded persons who come to health care settings in search of healing. This
hope is reflected in stories of success from Australia, the UK, the USA and elsewhere.
Because WPV and WPI occur within the context of large systems of care, a systems theory
model focusing on prevention, de-escalation, and intervention is needed upon which to base
other necessary programmes. Integrating a behavioural model to understand WPV and WPI
with a neurosensory model to conceptualize a dichotomous understanding of WPV and WPI
will greatly reduce WPV and its lower spectrum WPI, leading to more positive healing
environments and more positive work environments for staff. Further research is needed to
more fully integrate the models presented in this paper and increase the safety of all
stakeholders in human service settings.
PAGE 194 j JOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj VOL. 3 NO. 4 2011

References
Andersson, L.M. and Pearson, C.M. (1999), ‘‘Tit for tat? The spiraling effect of incivility in the workplace’’,
The Academy of Management Review, Vol. 24 No. 3, pp. 452-71.
Arnetz, J.E. and Arnetz, B. (2001), ‘‘Violence towards health care staff and possible effects on the quality
of care’’, Social Science & Medicine, Vol. 52, pp. 417-27.
Augsburger, D. (1981), Caring Enough to Confront: How to Understand and Express Your Deepest
Feelings Towards Others, Regal Books, Ventura, CA.
Bowen, B. (2006), ‘‘Supporting people, not just their behavior’’, paper presented at the International
Association for Positive Behavior Support Conference, Orlando, FL, December.
Bowen, B. (2009), ‘‘Applying invitational theory to human service settings’’, presented at the
International Alliance for Invitational Education World Conference, Rochester, NY, October 2009.
Bowen, B. (2010), ‘‘Incorporating traumagenic neurodevelopmental information into positive behaviour
support plans’’, paper presented at the International Research and Practice Conference, British Institute
of Learning Disabilities, Dublin.
Bowen, B. (2011), ‘‘Moving away from coercion and enhancing patient dignity and respect’’,
in Privitera, M.R. (Ed.), Workplace Violence in Mental and General Health Care Setting, Jones and
Bartlett, Sudbury, MA, pp. 135-50.
Bowie, V. (2006), ‘‘Organizational management and culture as key triggers of workplace violence’’,
paper presented at the Reaching for the Light High Risk Interventions in Human Services Symposium,
University of Stirling, Stirling.
Bowie, V. (2010), ‘‘Individuals, organizations and workplace violence’’, paper presented at the
Transforming Your Organization from ‘‘Toxic’’ to ‘‘Welcoming’’ Social Justice Social Change Centre
Seminar, September 29, Social Change Social Research Centre, University of Western Sydney, Penrith,
Australia.
Bowie, V. (2011), ‘‘An emerging awareness of the role organizational culture and management style can
play in triggering workplace violence’’, in Privitera, M.R. (Ed.), Workplace Violence in Mental and
General Health Care Setting, Jones and Bartlett, Sudbury, MA, pp. 43-58.
CMS (2006), Centers for Medicaid and Medicare Services, Code of Federal Regulations Part 482,
Section 482.13, Federal Register, Centers for Medicaid and Medicare Services, Baltimore, MD,
December 8.
Cornell, D.G., Warren, J., Hawk, G., Stafford, E., Oram, G. and Pine, D. (1996), ‘‘Psychopathy in
instrumental and reactive violent offenders’’, Journal of Consulting and Clinical Psychology, Vol. 64 No. 4,
pp. 783-90.
Cotton, P. and Hart, P.M. (2003), ‘‘Occupational wellbeing and performance: a review of organisational
health research’’, Australian Psychologist, Vol. 38 No. 2, pp. 118-27.
Crone, D.A. and Horner, R.H. (2003), Building Positive Behavior Support Systems in Schools: Functional
Behavioral Assessments, Guilford Press, New York, NY.
Cropanzano, R., Weiss, H.M. and Elias, S.M. (2004), ‘‘The impact of display rules and emotional labor on
psychological well-being at work’’, Research in Occupational Stress and Well Being, Vol. 3, pp. 45-89.
Implications for practice
Understanding the functions of violence provides practitioners with:
B A methodology to assess WPI and WPV.
B A framework to proactively teach replacement behaviours, empowering people to address the
causative factors in ways that do not cause harm to self and/or others.
B Models of implementation at various organisations that have achieved significant reductions in
violence.
B Skills that can be taught to staff individually or in group settings, as well as to most individuals
served.
VOL. 3 NO. 4 2011 jJOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj PAGE 195
Fallot, R.D. (2011), ‘‘Trauma informed care: a values based context for social empowerment’’, paper
presented at the Workshop on Preventing Violence to Women and Children, Institute of Medicine,
Washington, DC, January 28.
Farley-Toombs, C. (2011), ‘‘Reducing episodes of patient assaults in acute adult psychiatric units:
an interdisciplinary approach’’, in Privitera, M.R. (Ed.), Workplace Violence in Mental and General Health
Care Setting, Jones and Bartlett, Sudbury, MA, pp. 105-12.
Ferns, T. (2007), ‘‘Considering theories of aggression in an emergency department context’’, Accident
and Emergency Nursing, Vol. 15, pp. 193-200.
Foa, E.B. and Kozak, M.J. (1985), ‘‘Emotional processing of fear: exposure to corrective action’’,
Psychological Bulletin, Vol. 99 No. 1, pp. 20-35.
Gillece, J. (2008), Understanding the Effects of Trauma, PowerPointe Presentation, National Technical
Assistance Center, Washington, DC.
Gottman, J.M. and Levenson, R.W. (1988), ‘‘The social psychology of marriage’’, in Noeller, P. and
Patrick, M.A. (Eds), Perspectives on Marital Interaction, Clevedon, England, pp. 182-99.
Griffin, M.A., Hart, P.M. and Wilson-Evered, E. (2000), ‘‘Using employee opinion surveys to improve
organizational health’’, in Murphy, L.R. and Cooper, C.L. (Eds), Health and Productive Work: An
International Perspective, Taylor and Francis, London, pp. 15-36.
Hart, P.M. and Cooper, C.L. (2001), ‘‘Occupational stress: toward a more integrated framework’’, in
Anderson, N., Ones, D.S., Sinangil, H.K. and Viswesvaran (Eds), Handbook of Industrial, Work, and
Organisational Psychology, Vol.1, pp. 93-114.
Hart, P.M., Wearing, A.J., Liepens, I. and Grin, M.A. (1997), ‘‘Linking organizational climate to employee
well-being and performance: a covariance structure approach’’, paper presented at the 12th Annual
Conference for the Society for Industrial and Organizational Psychology, St Louis, MO.
Huckshorn, K.A. (2004), ‘‘Reducing seclusion and restraint in mental health use settings’’, Journal of
Psychosocial Nursing Mental Health Service, Vol. 42, pp. 22-33.
International Institute for Restorative Practices (2011), ‘‘Toxic talk: from betrayal to trust in a workplace’’,
Training video, available at: www.iirp.org/books_n_videos_info/toxictalk.php
James, L.R. and McIntyre, M.D. (1996), ‘‘Perceptions of organizational climate’’, in Murphy, K. (Ed.),
Individual Differences and Behavior in Organizations, Jossey-Bass, San Francisco, CA.
Janocha, J.A. and Smith, R.T. (2010), Workplace Safety and Health in the Health care and Social
Assistance Industry, US Department of Labor, Bureau of Labor Statistics, Washington, DC.
LeBel, J. and Goldstein, R. (2005), ‘‘The economic cost of restraint and the value added by restraint
reduction or elimination’’, Psychiatric Services, Vol. 56, pp. 1109-14.
LeDoux, J. (1989), ‘‘Cognitive and emotional interactions in the brain’’, Cognition and Emotion, Vol. 3
No. 4, pp. 267-89.
Lewis, P.S. and Malecha, A. (2011), ‘‘The impact of workplace incivility on the work environment,
manager skill, and productivity’’, Journal of Nursing Administration, Vol. 41 No. 1, pp. 41-7.
Lindsay, S.R. (2000), Handbook of Applied Dog Behavior and Training, Wiley-Blackwell, Hoboken, NJ,
p. 455.
McElliskem, J.E. (2004), ‘‘Affective and predatory violence: a bimodal classification system of human
aggression and violence’’, Aggression and violent behavior, Vol. 10, pp. 1-30.
MacRae, A. and Zehr, H. (2004), The Little Book of Family Group Conferences: New Zealand Style, Good
Books, Intercourse, PA.
Mandt, D.H. and Hines, R.G. (2008), Advanced Technical Training: The Mandt Systemw, unpublished
training manual, Dallas, TX.
Mandt, D.H., Hines, R.G. and Bowen, B. (2008), ‘‘The Mandt Systemw: putting people first’’,
unpublished training manual, Mandt System, Richardson, TX.
Maslow, A. (1954), Motivation and Personality, Harper and Row, New York, NY.
PAGE 196 j JOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj VOL. 3 NO. 4 2011

Mohr, W. and Bowen, B. (2009), ‘‘Decreasing workplace violence means increasing workplace safety
through positive behaviour support’’, Proceedings of the 6th European Congress on Violence in Clinical
Psychiatry, Kavanah, Dwingeloo and Oud Consultancy, Amsterdam, pp. 250-3.
NAU (2005), ‘‘Northern Arizona University: an overview of positive behavior support’’, available at:
www4.nau.edu/ihd/PBS/PBS_overview.asp (accessed October 12, 2005).
Paterson, B., Leadbetter, D. and Miller, G. (2006), ‘‘Preventing violence in residential care: a public
health perspective’’, Residential Group Care Quarterly, Vol. 7 No. 1, pp. 11-13.
Paterson, B., Ryan, D. and McConish, S. (2008), Research and Best Practice Associated with the
Protection of Staff from Third Party Violence and Aggression in the Workplace – A Literature Review, NHS
Health Scotland, Edinburg.
Perry, B. (2000a), ‘‘Brain structure and function I: basics of organization’’, Child Trauma Academy
Interdisciplinary Series, Vol. 2 No. 3.
Perry, B. (2000b), ‘‘The neuroarcheology of childhood maltreatment’’, available at: www.childtrauma.
org/ctmaterials/Neuroarcheology.asp (accessed July 14, 2007).
Perry, B. (2009), ‘‘Examining child maltreatment through a neurodevelopmental lens: clinical
applications of the neurosequential model of therapeutics’’, Journal of Loss and Trauma, Vol. 14,
pp. 240-55.
Possibilities (2008), ‘‘Developmental services of Nebraska newsletter’’, March 2008 newsletter, available
at: www.dsnonline.org/PDF/220008/pdf (accessed October 28, 2009).
Privitera, M.R. and Arnetz, J. (2011), ‘‘Effect of workplace violence on staff, institution and quality of
patient care’’, in Privitera, M.R. (Ed.), Workplace Violence in Mental and General Health Care Setting,
Jones and Bartlett, Sudbury, MA, pp. 29-42.
Putkonen, A., Kuivalainen, S., Louheranta, O., Repo-Tiihonen, E., Kiviniemi, V. and Tiihonen, J. (2011),
‘‘A cluster randomized controlled study of seclusion and restraint reduction in high security psychiatric
care’’, presented at the 7th European Congress on Violence in Clinical Psychiatry, 21 October, 2011.
Rhodes, C., Pullen, A., Vickers, M.H., Clegg, S.R. and Pitsis, A. (2010), ‘‘Violence and workplace
bullying: what are an organization’s ethical responsibilities?’’, Administrative Theory & Praxis, Vol. 32
No. 1, pp. 96-115.
Ross, S.W. (2009), ‘‘Bully prevention in positive behavior support’’, doctoral dissertation, University of
Oregon, Eugene, OR.
Sanders, K. and Gaynor, J. (2010), ‘‘The Grafton experience: the minimization of restraint initiative’’,
paper presented at the International Research and Practice Conference, British Institute of Learning
Disabilities, Dublin.
Sims, R.L. and Keon, T.L. (1999), ‘‘Determinants of ethical decision making: the relationship of the
perceived organizational environment’’, Journal of Business Ethics, Vol. 19 No. 4, pp. 393-401.
Smith, G., Davis, R., Bixler, E., Lin, H., Altenor, A., Altenor, R., Hardenstine, B. and Kopchick, G. (2005),
‘‘Pennsylvania State Hospital system’s seclusion and restraint reduction program’’, Psychiatric Services,
Vol. 56 No. 9, pp. 1115-22.
Society for Research in Child Development (2007), ‘‘Revisiting the instrumental versus reactive
aggression distinction in child development’’, Roundtable Symposium presented at the Biennial
Meeting of Society for Research in Child Development, Boston, MA, March 31.
Stichter, J.P., Lewis, T.J., Johnson, N. and Trussel, R. (2004), ‘‘Toward a structural assessment: analyzing
the merits of an assessment tool for a student with E/BD’’, Assessment for Effective Intervention, Vol. 30
No. 1, pp. 25-40.
Tunajek, S. (2007), ‘‘Workplace incivility – part I: anger, harassment, and organizational violence’’, AANA
New Bulletin, March, pp. 30-1.
Ursin, H. and Olff, M. (1995), ‘‘Aggression, defense, and coping in humans’’, Aggressive Behavior,
Vol. 21 No. 1, pp. 13-19.
Vanderberg, J. and Bowen, B. (2011), ‘‘Security officers: structuring prevention, not just intervention’’,
paper presented at the 7th European Congress on Violence in Clinical Psychiatry, Prague, Czech
Republic, 19-22 October.
VOL. 3 NO. 4 2011 jJOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj PAGE 197

Wright, T.A. and Cropanzano, R. (2000), ‘‘Psychological wellbeing and job satisfaction as predictors of
job performance’’, Journal of Occupational Health Psychology, Vol. 5, pp. 84-94.
Further reading
Bloom, S.L. and Farragher, B. (2011), Destroying Sanctuary: The Crisis in Human Service Delivery
Systems, Oxford University Press, New York, NY.
Bowie, V. (2002), ‘‘Defining violence at work: a new typology’’, in Gill, M., Fisher, B. and Bowie, V. (Eds),
Violence at Work: Causes, Patterns, and Prevention, Willan, Portland, OR, pp. 1-20.
Gottman, J.M. and Katz, L. (1989), ‘‘Effects of marital discord on young children’s peer interaction and
health’’, Developmental Psychology, Vol. 25, pp. 373-81.
Greenberg, J. (1990), ‘‘Employee theft as a reaction to underpayment inequity: the hidden cost of pay
cuts’’, Journal of Applied Psychology, Vol. 75 No. 5, pp. 561-8.
Kessler, S.R., Spector, P.E., Chang, C.-H. and Parr, A.D. (2008), ‘‘Organizational violence and
aggression: development of the three factor violence climate survey’’, Work & Stress, Vol. 22 No. 2,
pp. 108-24.
Kumar, M., Jha, V. and Vaidya, S.D. (2007), ‘‘Empirical investigation of impact of organizational culture,
prosocial behavior and organizational trust on sharing mistakes in knowledge management systems’’,
Proceedings of the Pacific Asia Conference on Information Systems (PACIS 2007), Auckland, Paper
146, 3-6 July, available at: http://aisel.aisnet.org/pacis2007/146
Pollack, D.A. (2004), ‘‘Moving from coercion to collaboration in mental health services’’, DHHS
Publication No. (SMA) 04-3869, Center for Mental Health Services, Substance Abuse and Mental Health
Services Administration, Rockville, MD.
Purkey, W.W. and Strahan, D. (1995), ‘‘School transformation through invitational education’’,
Researching in the Schools, Vol. 2, pp. 1-6.
Wells, R. (2006), ‘‘Team leadership and patient outcomes in US psychiatric treatment settings’’, Social
Science & Medicine, Vol. 62 No. 8, pp. 1840-52.
Corresponding author
Bob Bowen can be contacted at: [email protected]
To purchase reprints of this article please e-mail: [email protected]
Or visit our web site for further details: www.emeraldinsight.com/reprints
PAGE 198 j JOURNAL OF AGGRESSION, CONFLICT AND PEACE RESEARCHj VOL. 3 NO. 4 2011