Embed Size (px)
Citation preview

Medical liability claim. These are three devastatingand costly words for America’s doctors—and an influen-tial factor in many physicians’ career choices. A new re-port by the American Medical Association reveals why:just over 42% of all physicians and an astonishing 57% ofphysicians in surgical subspecialties have been sued.Nearly 61% of physicians aged 55 or older have faced theordeal of a lawsuit (73% for those physicians in the surgi-cal subspecialties).1
Even those who have not been sued feel the effectsof this litigious environment. There are many proceduresthat I would like to perform but choose not to becauseof the risks of litigation. Treating retinopathy of prema-turity is a prime example in my own specialty. As an eyesurgeon, I have found that I am most comfortable limit-ing my practice to elective cataract and refractive proce-dures, although these procedures have their own liabilityrisks. In limiting the scope of my practice, I recognizehow liability risk forces many physicians toward more con-servative career choices.
But what if the specter of litigation could be re-duced through better, more documented patient com-munication? The idea might sound overly simplistic, butas a colleague once aptly noted, “Frustration is the dif-ference between expectation and reality.”
The level of patient frustration that results in law-suits often is rooted in an expectation of clinical resultsthat does not match actual outcomes. The concept is sup-ported by the fact that most legal cases are not aboutmedical errors; roughly 90% of those that go to trial aredecided in favor of the physician.2
Yet even so, defending against lawsuits takes atremendous emotional and financial toll. Eliminating mis-communication problems before they start, therefore, isof paramount importance. At Bluegrass Eye Surgery, thisis done through a standardized and well-documented in-formed consent process.
THE INFORMED CONSENTCONVERSATION
The term “informed consent” typically conjuresthoughts of a documentation requirement that carries
Reducing Liability Risk throughInformed Consent
Gary Wortz, MD*
new report by the American Medical Association reveals whymedical liability claims are so devastating and costly forAmerica’s doctors: just over 42% of all physicians and an as-tonishing 57% of physicians in surgical subspecialties have beensued. Nearly 61% of physicians aged 55 or older have facedthe ordeal of a lawsuit. But what if the specter of litigationcould be reduced through better, more documented patient com-
munication? One Kentucky ophthalmologist believes patient frustration of-ten is rooted in an expectation of clinical results that does not match actualoutcomes. To alleviate the disparity, he uses a standardized informed consentprocess to ensure patients thoroughly understand the procedure and possibleoutcomes. This article will explain in detail his three-pronged approach, fo-cused on procedure-specific counseling, education, and documentation.
Key words: Medical liability claims; liability risk; informed consent; patientsatisfaction; patient education; documentation.
A
*Board-certified ophthalmologist in private practice at Bluegrass EyeSurgery in Lebanon, KY.Copyright © 2011 by Greenbranch Publishing LLC.
www.greenbranch.com • 800-933-3711 203

legal liability if signatures are not obtained properly. Butit is much more than mere paperwork. It is a vital com-munication process that allows physicians to fully engagepatients in their own care decisions.
A recent study published in the Journal of theAmerican College of Surgeons concludes that total timespent on the informed consent process is the strongestpredictor of patient comprehension. It notes, “Affordingadequate time for informed consent discussions and us-ing informed consent adjuncts such as [repeat back] mayenhance comprehension . . .”3
The informed consent process, in fact, is designedto help prevent disparity between patient expectations andthe reality of typical surgical results through careful re-view of diagnosis; recommended and alternative treat-ments; and the potential benefits, risks, and complicationsof each treatment option. Unfortunately, however, a va-riety of factors often interfere with a patient’s ability toremember key details of this crucial discussion.
For this reason, I have standardized my informedconsent conversation to ensure each patient thoroughlyunderstands his or her surgical procedure and all possibleoutcomes. It is a three-pronged approach focused on pro-cedure-specific counseling, education, and documentation.
COUNSELING: OPENING THE DIALOG
As a board-certified ophthalmologist specializing incataract and refractive surgery, I sometimes see patientswho have never worn corrective lenses in their lives. Theyunderstand they have cataracts, but think that once thosecataracts are removed they automatically will enjoy thesame vision they had in their younger years.
Successful cataract surgery involves the uncompli-cated removal of the cataract and placement of an in-traocular lens that restores the correctable vision back tothe patient’s full potential. For many patients to enjoy afull range of clear vision, they will need to wear correc-
tive lenses. However, many patients do not understandthe difference between cataract surgery and LASIK re-fractive surgery and expect to have perfect vision withoutglasses starting the first day after surgery.
While many patients do experience great resultsfrom cataract surgery, including great vision withoutglasses, it is a mistake to set this as the standard expecta-tion unless you have the tools to deliver on it. The realityis that sometimes patients will need to wear glasses aftersurgery. A patient who does not fully comprehend thispossibility might perceive the outcome as a surgical fail-ure—or even surgical error—should it occur. Thus whatI consider a surgical success could be viewed with acri-mony and frustration on the part of the patient. That isone reason why the counseling and education process atBluegrass begins before I ever step into the exam room.
Most patients come to us by referral from otherproviders who already have made a preliminary cataractdiagnosis. Upon arrival, a technician checks the patient’svision, performs preliminary studies, and dilates the eyes.
Counseling and education begin during the 15 to 20minutes it takes for eyes to become fully dilated, when thetechnician plays a 17-minute video (Patient EducationConcepts, Houston, Texas) that explains: cataract surgery;intraocular lens technology; and surgical risks, benefits, andalternatives. Patients can take a true/false quiz at the end.
Ideally, every patient would fill in the quiz answersheet for inclusion in his or her chart; in reality, of course,that does not happen all of the time. Nevertheless, the video
www.greenbranch.com • 800-933-3711
204 Medical Practice Management • January/February 2011
Do’s and Don’ts Regarding InformedConsent Documentation
• Don’t execute the consent form on the first visitwhile the patient is still learning about the procedure.
• Don’t execute the form on the day of surgery.• Do execute the form in the office setting when the
patient is comfortable and has ample time to askquestions.
• Do offer the patient a copy of the form that he orshe has signed.
• Do consider a professional source of detailed, easy-to-understand, procedure-specific forms that arecontinuously updated and reviewed by a reputablevendor.
Three Best Practices for ManagingPatient Expectations
1. Use multiple strategies for educating patients.• Use personal discussion by the physician.• Show a video depicting the procedure.• Provide a comprehensive handout.• Create a detailed, procedure-specific informed
consent form.2. Ensure that patients are active participants in the
informed consent process.• Challenge them to pay attention.• Confirm understanding.
3. Be very specific about the risks of procedures andpossible complications.• If a patient appears unwilling to acknowledge
those risks, postpone the procedure until he orshe is ready to do so, or refer the patient else-where.
• If a patient declines a procedure after under-standing risks that he or she deems unacceptable,then you have done an admirable job of inform-ing and considering your patient’s interests.

and quiz still prime patients for a meaningful conversationonce I have met them and completed their exams.
During the course of that conversation, I always tellpatients the great thing about cataract surgery: it is anelective procedure. I am not a surgical salesman. My jobis not to talk patients into surgery, but to counsel themabout their options and offer them my service if they de-cide they want it. Putting patients in control of their treat-ment choice—even if that choice is to do nothing atall—is imperative to the informed consent process.
EDUCATION: LAYING FACTSON THE TABLE
Patients tend to approach informed consent from adifferent perspective than we do as physicians. They puttheir trust in a physician expecting a problem-free out-come, so at times it is an uphill battle to get them to takerisks seriously. Sometimes they simply do not want toknow about potential problems.
In truth, you can only inform patients to the degreethey desire. But the informed consent process gives patientsthe opportunity to know as much as they want to know.That is why, after counseling patients about their treatmentoptions, my conversation turns to a five-point informa-tional discussion. The five key elements of my review:1. Describe the surgery. Discuss what the procedure en-
tails and what the patient should expect. For instance,I explain that cataract surgery is a 10-minute, same-day procedure performed at a surgery center with se-dation, but no general anesthesia.
2. Review the key risks associated with the procedure.While my success rate for cataract surgery is more than99%, patients tend to expect a 100% guarantee—whichno surgeon can truthfully provide. I let patients knowthat while small, the risk of a complication that cannotbe fixed—including loss of vision or loss of the eye—does exist. Patients must be comfortable with this riskbefore I will proceed with surgery.
Figure 1. Selection of a cataract procedure consent.
www.greenbranch.com • 800-933-3711
Wortz/Informed Consent 205

3. Discuss the patient’s post-procedure responsibil-ities. These are the actions a patient must take to en-able an optimal outcome. Whether it is using eyedrops on schedule or attending all follow-up visits,patients must assume full responsibility for optimizingtheir outcomes, too.
4. Explain the patient’s alternatives and surgical op-tions associated with a planned procedure. This isperhaps the most important of the five points atBluegrass, and where expectation must be aligned withreality. We engage in a lengthy discussion of differentartificial lenses and what the lens choice could meanfor future vision. Cataract surgery is a modern-day mir-acle, yet patients must understand the limits of tech-nology. Despite everyone’s best efforts, glasses orcontact lenses sometimes are necessary after surgery—even for patients who have never worn them before.Some patients have asked me to provide 100% assur-
ance they would not need glasses. After reiterating thatno 100% guarantee is truthful, I tell these patients thatit is okay to postpone the surgery until they feel morecomfortable with the idea that glasses may be a po-tential necessity for visual correction after surgery.
5. Review the patient’s long-term prognosis. In thecase of an intraocular lens (IOL) implant, I clarify thatcataracts do not grow back. It is a common concern,and also one that affects a patient’s treatment deci-sion. Because they do not grow back, the sooner thesurgery is performed, the longer a patient can enjoythe results.
Following the discussion, patients are given a 12-page brochure I created that includes a description of myprofessional experience; a letter from me about cataractsurgery; and further information about lenses and op-tions, possible vision outcomes, answers to frequentlyasked questions, pre- and postoperative surgical instruc-
Figure 2. Consent screenshot showing the risks.
www.greenbranch.com • 800-933-3711
206 Medical Practice Management • January/February 2011

Figure 3. Consent ready for review.
www.greenbranch.com • 800-933-3711
Wortz/Informed Consent 207
tions, an eye-drop schedule, and an appointment re-minder that includes my personal cell phone number.
With information in hand, patients are asked to gohome, think through our conversation, read the brochure,consider the available treatment options, and arrive attheir treatment choices. They are encouraged to call mewith any questions. If they wish, we offer them our in-formed consent document to take home, but they arenever asked to sign it until they come back into the of-fice for their next visit.
DOCUMENTATION: INDICATING FULLUNDERSTANDING AND CONSENT
Once patients decide they want to proceed withsurgery, they come back into the office, and a technicianprovides surgery instructions, performs the lens calcula-tion, and walks through the informed consent documen-
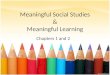
tation. A comprehensive, procedure-specific consentform—available via a software application (Figure 1)—allows me to delegate the task of executing the form toassistive personnel without hesitation.
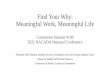
A thorough, easy-to-understand list of potentialcomplications (Figure 2) is the cornerstone of any solidconsent documentation. Everything that could possiblygo wrong should be mentioned. In our case, for instance,“droopy eyelid” is a complication commonly forgottenabout and left off of consent forms. While rare, the wirespeculum used during surgery can cause the eyelid mus-cle to stretch. This very uncommon—but not unknown—risk is listed on our consent documents.
When Bluegrass first opened, we used some tem-plate forms that had been developed by an insurance firm.However, as a resident at the Veterans Administration fa-cility in Lexington, Kentucky, I had become familiar withan automated informed consent and patient education

application (iMedConsent, Dialog Medical, Atlanta,Georgia) with which I was very comfortable because ofits professional, in-depth list of potential complications(including the aforementioned droopy eyelid).
Printing out a copy of the consent provides an ed-ucational tool for patients—a way to better remember andunderstand the conversation and their choices (Figure 3).Libraries of procedure-specific educational material canfurther augment the process. After patients sign the con-sent documentation, they are always offered a copy.
The well-thought-out, inclusive list of complicationson our cataract surgery consent form also makes it diffi-cult for those patients who suffer complications to laterclaim they did not realize that their particular complica-tion was a possibility. If ever my consent process werequestioned, I am comfortable that it would stand upagainst scrutiny.
STRENGTHENING OPERATIONS
At Bluegrass Eye Surgery, I am the sole ophthal-mologist working out of three locations that span 140miles across Kentucky. Last year, I performed more than1000 cataract procedures. Smooth operations dependon my ability to delegate key tasks to technicians andother staff.
Prompts throughout our informed consent processhelp make sure technicians consistently discuss all vitalrisk elements. Without that consistency and the compre-hensive nature of the documents themselves, delegationof that task would not be possible. As it is, however, it of-fers a tremendous “best practices” advantage.
Meanwhile, patients gain a clear perception of boththe benefits and risks associated with their care decisions.In the end, some patients have reviewed the documenta-tion, thought about the risks, and decided not to go for-ward with surgery. That in itself, I believe, speaks tohaving truly informed patients.
As the Journal of the American College of Surgeonsstudy3 reveals, patients are more likely to understand notonly the benefits, but also the risks and choices associatedwith the procedures we offer if we extend the amount oftime spent on informed consent discussions.
The standardized discussion at Bluegrass is only en-hanced through comprehensive educational tools—whichincludes the consent form itself.
“Frustration is the difference between expectationand reality.” It is a profound statement. But it also holdsa promise: Patients can be satisfied when their expecta-tions are balanced with the outcomes that are delivered.The potential for dissatisfaction that leads to lawsuits canbe diminished.
Ultimately, using the informed consentprocess to carefully align hopes withpotential outcomes is what keeps patientssatisfied with their care—and outof the courtroom.
The informed consent process can help gain well-educated patients and strengthen the patient/physicianrelationship. Ultimately, using it to carefully align hopeswith potential outcomes is what keeps patients satisfiedwith their care—and out of the courtroom. ■
REFERENCES
1. Kane CK. Medical Liability Claim Frequency: A 2007-2008Snapshot of Physicians. American Medical Association; August2010; www.ama-assn.org/ama1/pub/upload/mm/363/prp-201001-claim-freq.pdf.
2. New AMA Report Finds 95 Medical Liability Claims Filed forEvery 100 Physicians. American Medical Association; August 3,2010; www.ama-assn.org/ama/pub/news/news/medical-liability-report.shtml.
3. Fink AS, Prochazka AV, Henderson WG, et al. Predictors of com-prehension during surgical informed consent. J Am Coll Surg.2010;210;919-926.
208 Medical Practice Management • January/February 2011
www.greenbranch.com • 800-933-3711