Embed Size (px)
Citation preview
10/10/2015
1
Reducing Heart Failure Readmissions with Remote Pulmonary Arterial Pressure
Monitoring
Making Sense of the Sensor
Van Selby, MD
Amanda Schnell-Heringer, RN, MS, CNS
October 9, 2015
Disclosures
• Van Selby: None
• Amanda Schnell-Heringer: None
10/10/2015
2
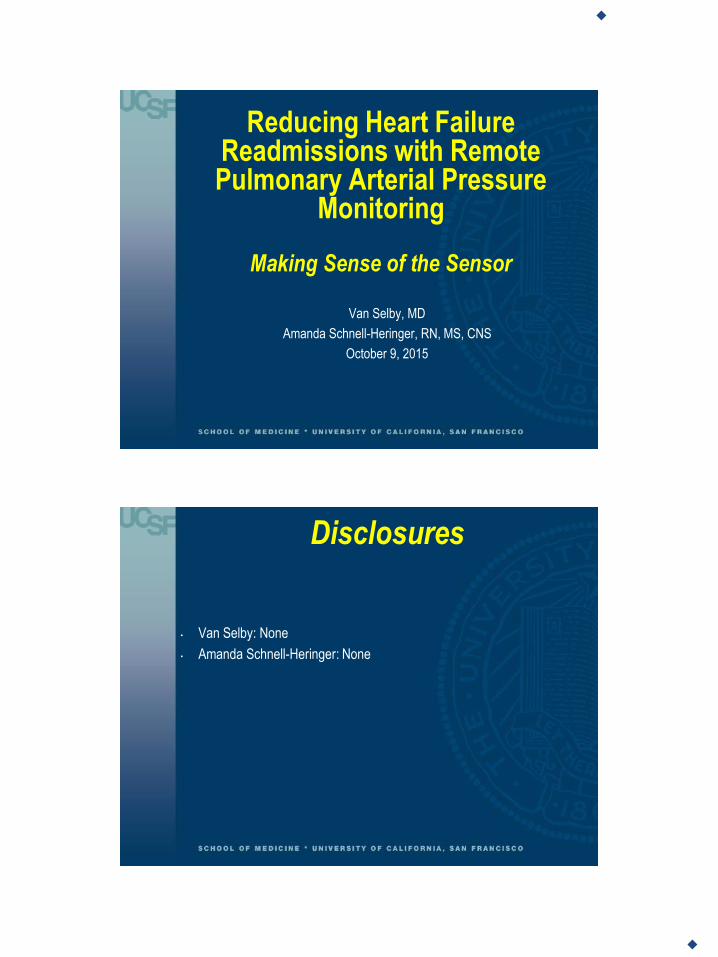
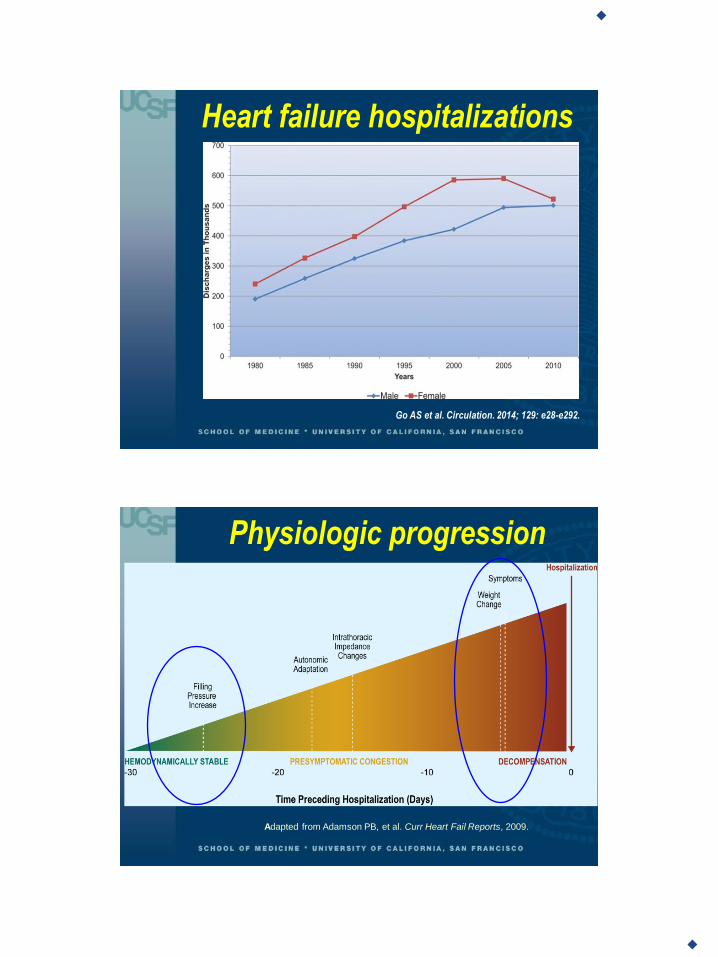
Heart failure hospitalizations
Go AS et al. Circulation. 2014; 129: e28-e292.
Physiologic progression
Adapted from Adamson PB, et al. Curr Heart Fail Reports, 2009.
10/10/2015
3
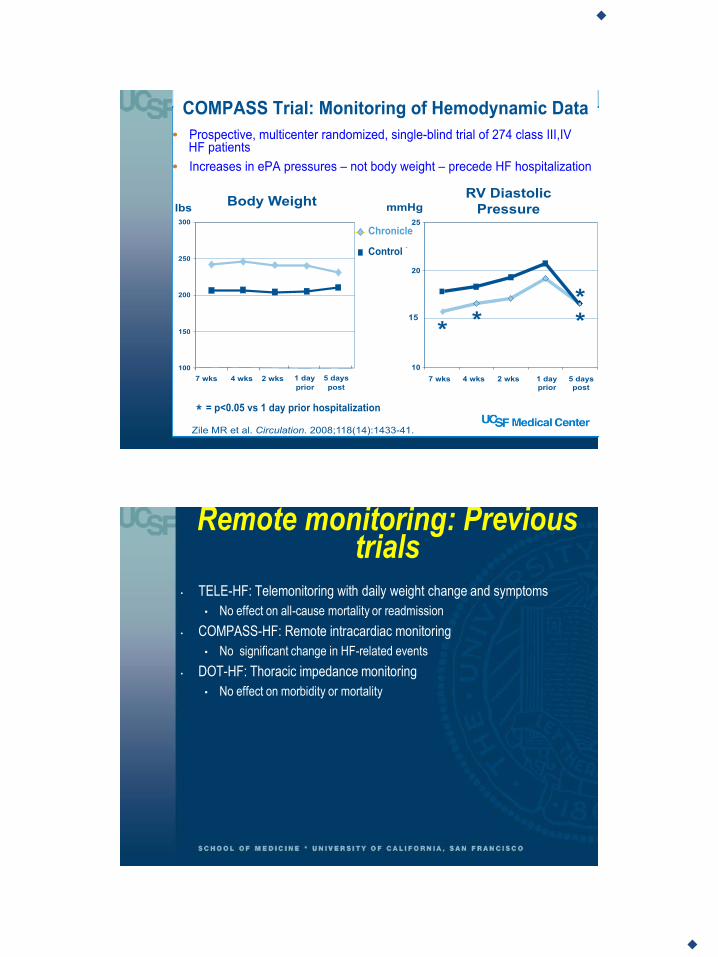
Remote monitoring: Previous trials
• TELE-HF: Telemonitoring with daily weight change and symptoms
• No effect on all-cause mortality or readmission
• COMPASS-HF: Remote intracardiac monitoring
• No significant change in HF-related events
• DOT-HF: Thoracic impedance monitoring
• No effect on morbidity or mortality
10/10/2015
4
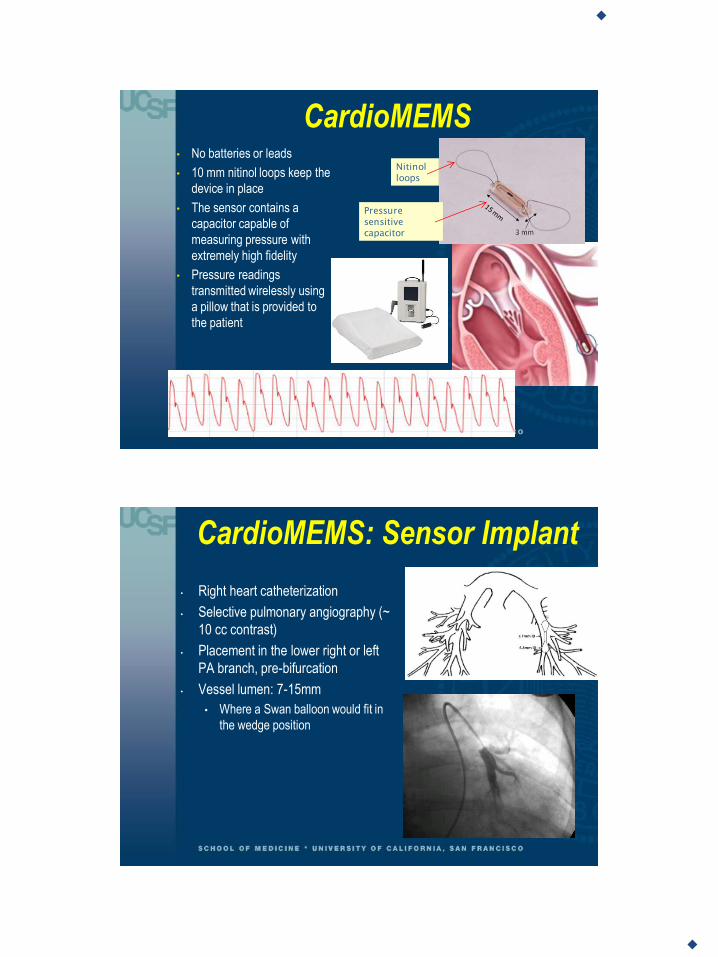
CardioMEMS
Nitinol
loops
Pressure
sensitive
capacitor
• No batteries or leads
• 10 mm nitinol loops keep the
device in place
• The sensor contains a
capacitor capable of
measuring pressure with
extremely high fidelity
• Pressure readings
transmitted wirelessly using
a pillow that is provided to
the patient
CardioMEMS: Sensor Implant
• Right heart catheterization
• Selective pulmonary angiography (~
10 cc contrast)
• Placement in the lower right or left
PA branch, pre-bifurcation
• Vessel lumen: 7-15mm
• Where a Swan balloon would fit in
the wedge position
10/10/2015
5
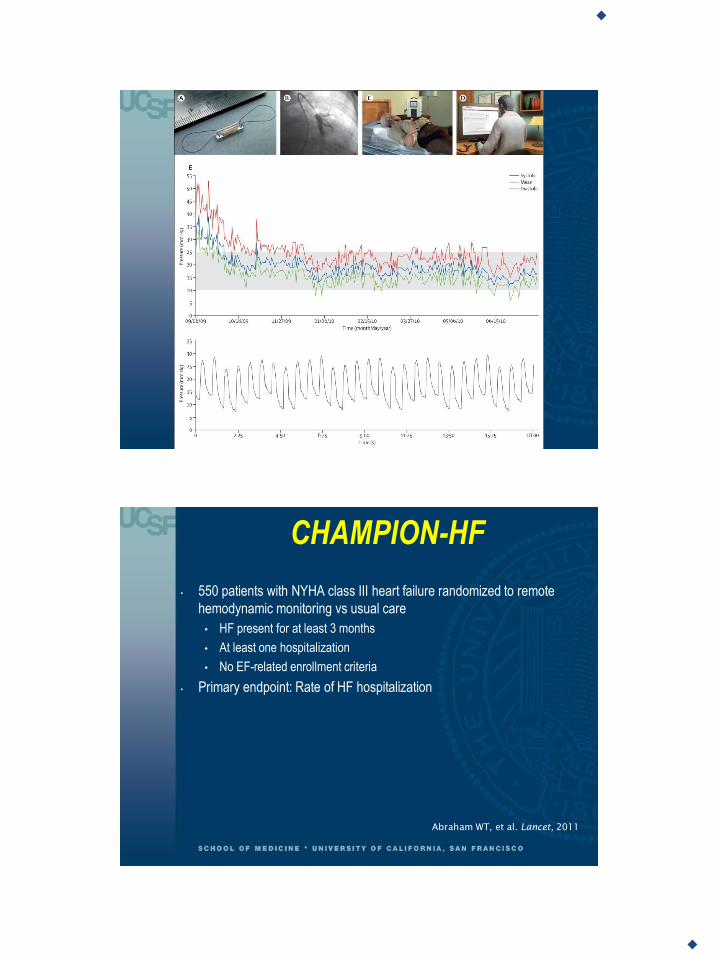
CHAMPION-HF
• 550 patients with NYHA class III heart failure randomized to remote
hemodynamic monitoring vs usual care
• HF present for at least 3 months
• At least one hospitalization
• No EF-related enrollment criteria
• Primary endpoint: Rate of HF hospitalization
Abraham WT, et al. Lancet, 2011
10/10/2015
6
CHAMPION-HF: Treatment algorithm
• All patients took daily home pressure readings
• Pressures were reviewed at least once per week, and more frequently if
indicated for clinical reasons
• Target pressures:
• PA systolic pressure 15-35 mmHg
• PA diastolic pressure 8-20 mmHg
• PA mean pressure 10-25 mmHg
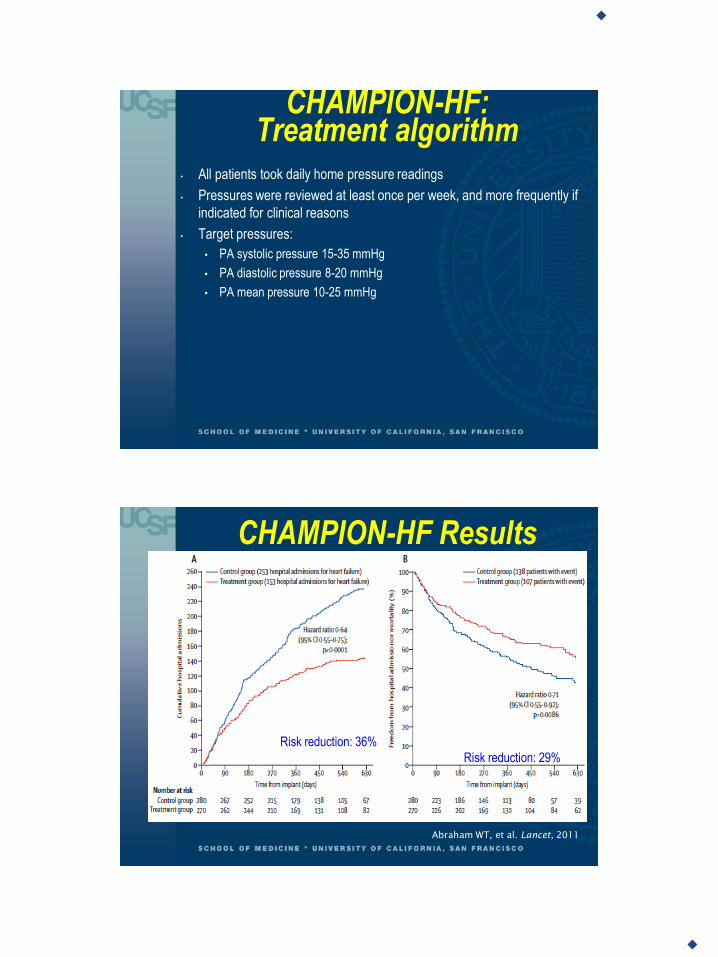
CHAMPION-HF Results
Risk reduction: 36%
Risk reduction: 29%
Abraham WT, et al. Lancet, 2011

10/10/2015
7
Hemodynamic monitoring leads to more medication changes
Abraham WT, et al. Lancet, 2011
CHAMPION: Safety endpoints
• 15 adverse events reported among 575 device implants
• 7 procedure-related
• 4 bleeding (groin, epistaxis, hemoptysis)
• 3 hospitalizations related to anticoagulation
• No pulmonary infarcts or embolism
• No events required removal of the sensor
• No significant differences in adverse events between the two groups.
• No pressure sensor failures in either group
10/10/2015
8
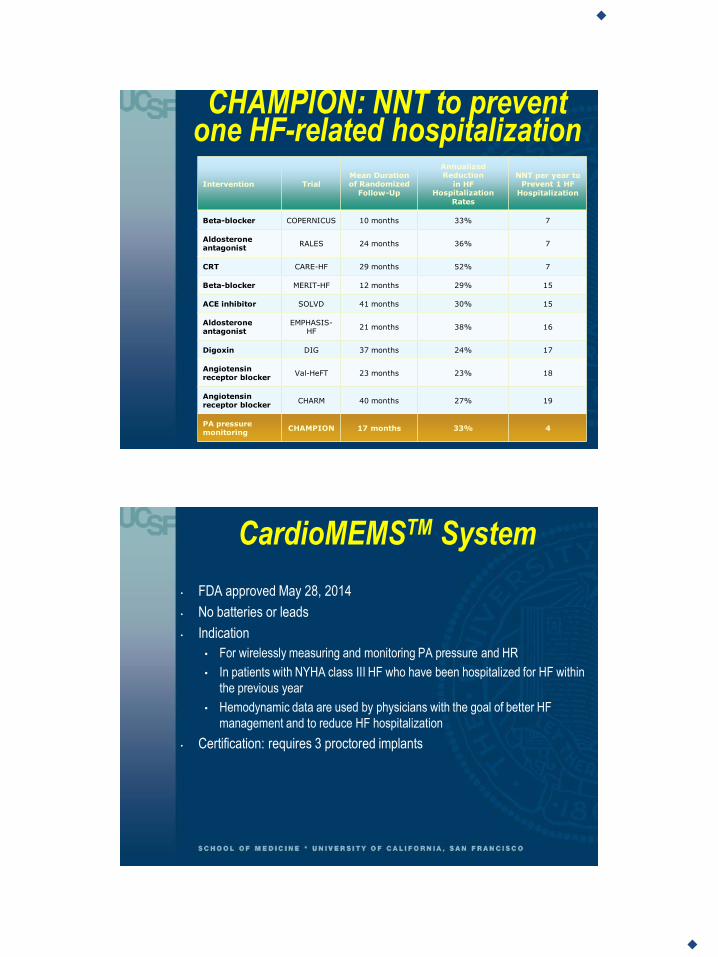
CHAMPION: NNT to prevent one HF-related hospitalization
Intervention Trial Mean Duration of Randomized
Follow-Up
Annualized Reduction
in HF Hospitalization
Rates
NNT per year to Prevent 1 HF
Hospitalization
Beta-blocker COPERNICUS 10 months 33% 7
Aldosterone antagonist
RALES 24 months 36% 7
CRT CARE-HF 29 months 52% 7
Beta-blocker MERIT-HF 12 months 29% 15
ACE inhibitor SOLVD 41 months 30% 15
Aldosterone antagonist
EMPHASIS-HF
21 months 38% 16
Digoxin DIG 37 months 24% 17
Angiotensin receptor blocker
Val-HeFT 23 months 23% 18
Angiotensin receptor blocker
CHARM 40 months 27% 19
PA pressure monitoring
CHAMPION 17 months 33% 4
CardioMEMSTM System
• FDA approved May 28, 2014
• No batteries or leads
• Indication
• For wirelessly measuring and monitoring PA pressure and HR
• In patients with NYHA class III HF who have been hospitalized for HF within
the previous year
• Hemodynamic data are used by physicians with the goal of better HF
management and to reduce HF hospitalization
• Certification: requires 3 proctored implants
10/10/2015
9
UCSF criteria/considerations for CardioMEMS
• At least one HF-related hospitalization in the past year
• No contraindication for DAPT
• Necessary adherence, as demonstrated by:
• Regular lab monitoring
• Able to take meds as instructed
• Attend MD appts regularly
• Able to lie flat
• No major psychosocial barriers to appropriate transmissions and follow-up
• Major exclusions:
• PE/DVT
• GFR<25, unresponsive to diuretics, HD
• Major cardiovascular event within 2 months
• Coagulopathy
• Hypersensitivity to ASA/Plavix
Patient Cases
10/10/2015
10
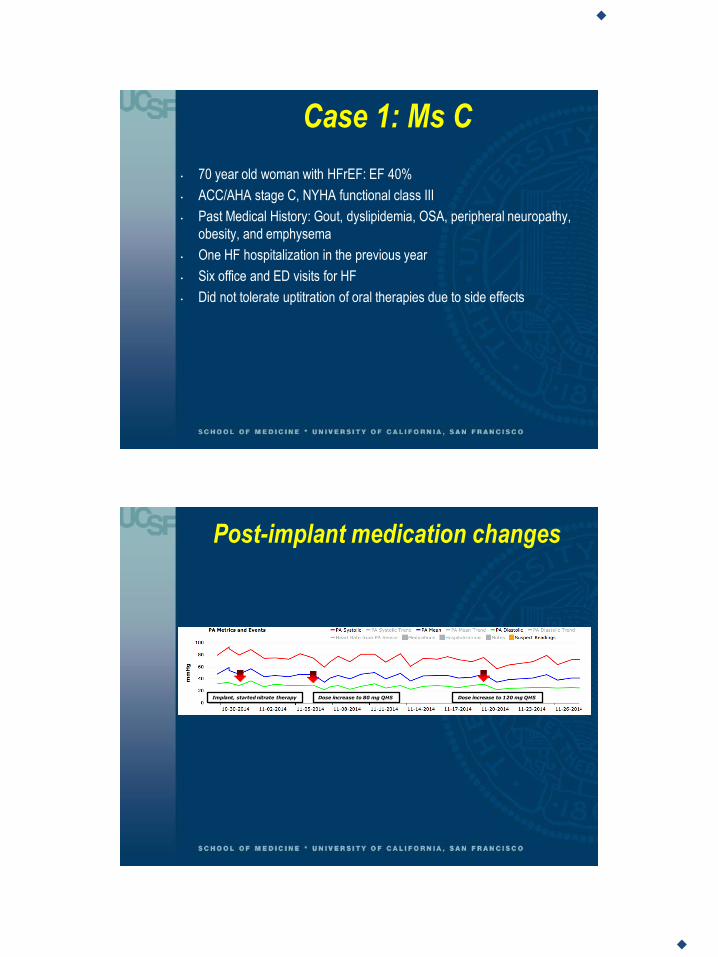
Case 1: Ms C
• 70 year old woman with HFrEF: EF 40%
• ACC/AHA stage C, NYHA functional class III
• Past Medical History: Gout, dyslipidemia, OSA, peripheral neuropathy,
obesity, and emphysema
• One HF hospitalization in the previous year
• Six office and ED visits for HF
• Did not tolerate uptitration of oral therapies due to side effects
Post-implant medication changes
Implant, started nitrate therapy Dose increase to 80 mg QHS Dose increase to 120 mg QHS
10/10/2015
11
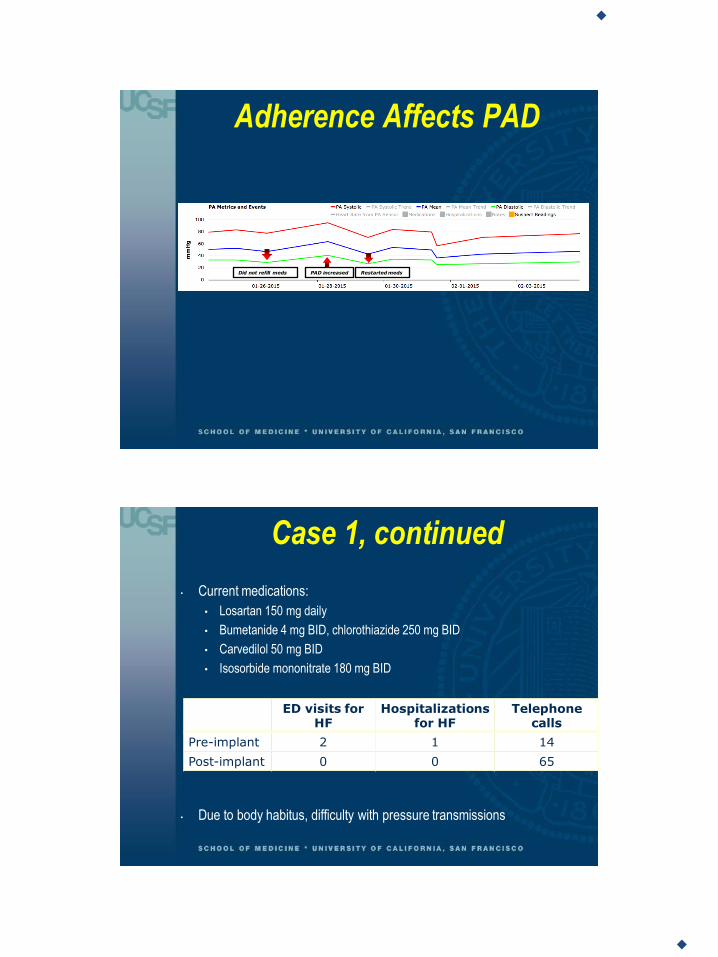
Adherence Affects PAD
Did not refill meds Restarted meds PAD increased
Case 1, continued
• Current medications:
• Losartan 150 mg daily
• Bumetanide 4 mg BID, chlorothiazide 250 mg BID
• Carvedilol 50 mg BID
• Isosorbide mononitrate 180 mg BID
• Due to body habitus, difficulty with pressure transmissions
ED visits for HF
Hospitalizations for HF
Telephone calls
Pre-implant 2 1 14
Post-implant 0 0 65
10/10/2015
12
Case 2: Mr F
• 60 y.o. male with NIDCM due to prior alcohol and cocaine use. Pt reports
no recent use of cocaine and minimal weekly ETOH use.
• HFrEF: EF 20%
• ACC/AHA Stage C, NYHA Class III
• CRT-D, cirrhosis, paroxysmal atrial fibrillation, sleep apnea, COPD.
• Worsening HF symptoms despite maximal treatment.
• Two HF admissions in the previous year
10/10/2015
13
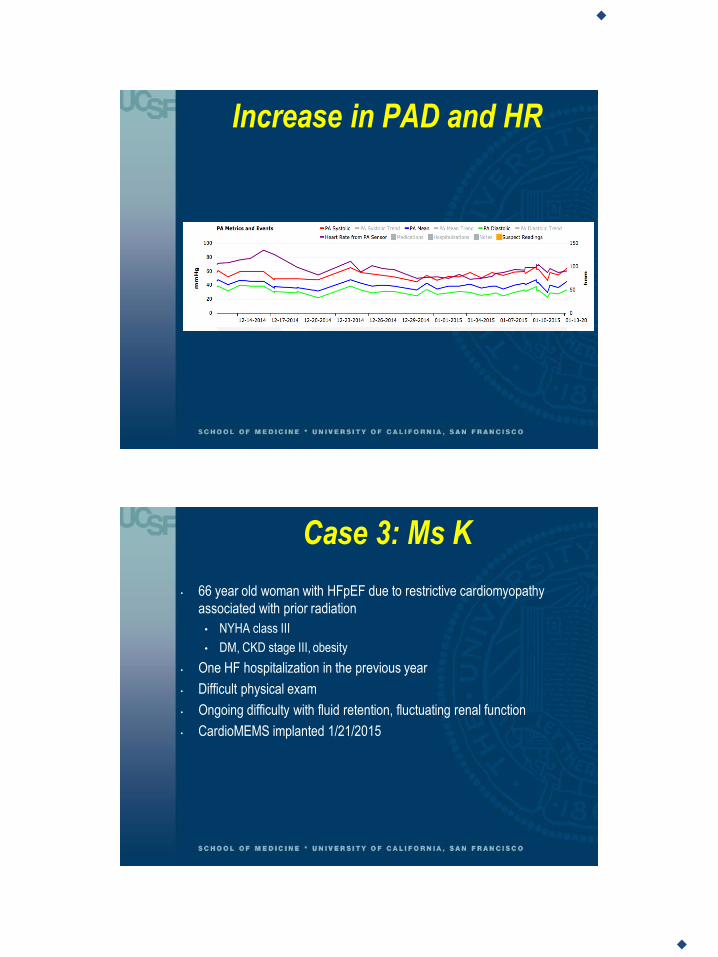
Increase in PAD and HR
Case 3: Ms K
• 66 year old woman with HFpEF due to restrictive cardiomyopathy
associated with prior radiation
• NYHA class III
• DM, CKD stage III, obesity
• One HF hospitalization in the previous year
• Difficult physical exam
• Ongoing difficulty with fluid retention, fluctuating renal function
• CardioMEMS implanted 1/21/2015
10/10/2015
14
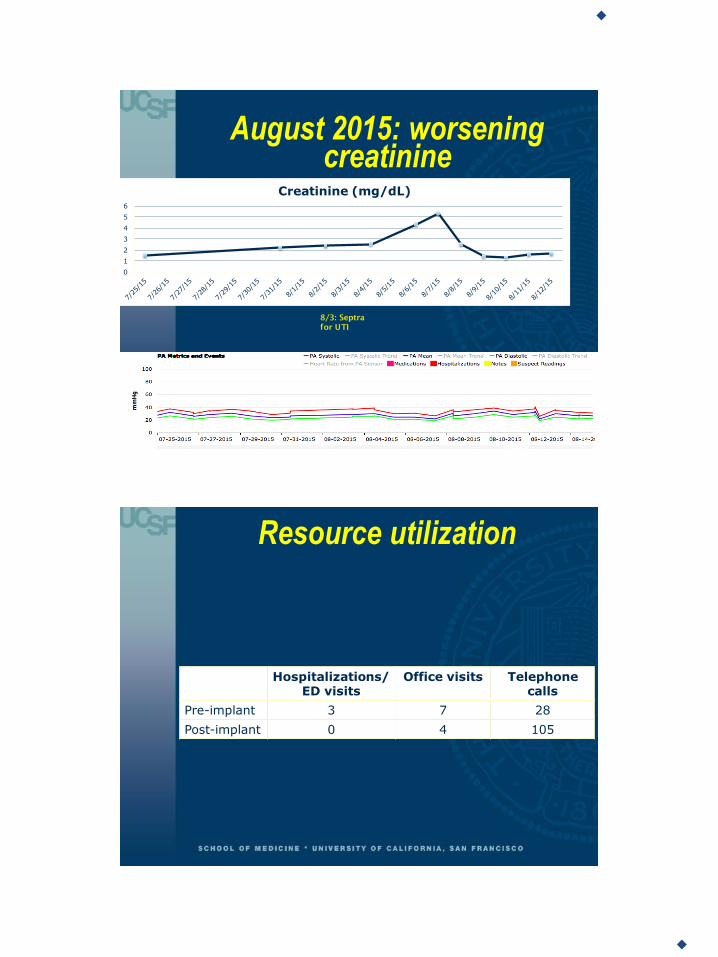
August 2015: worsening creatinine
0
1
2
3
4
5
6
Creatinine (mg/dL)
8/3: Septra
for UTI
Resource utilization
Hospitalizations/ED visits
Office visits Telephone calls
Pre-implant 3 7 28
Post-implant 0 4 105
10/10/2015
15
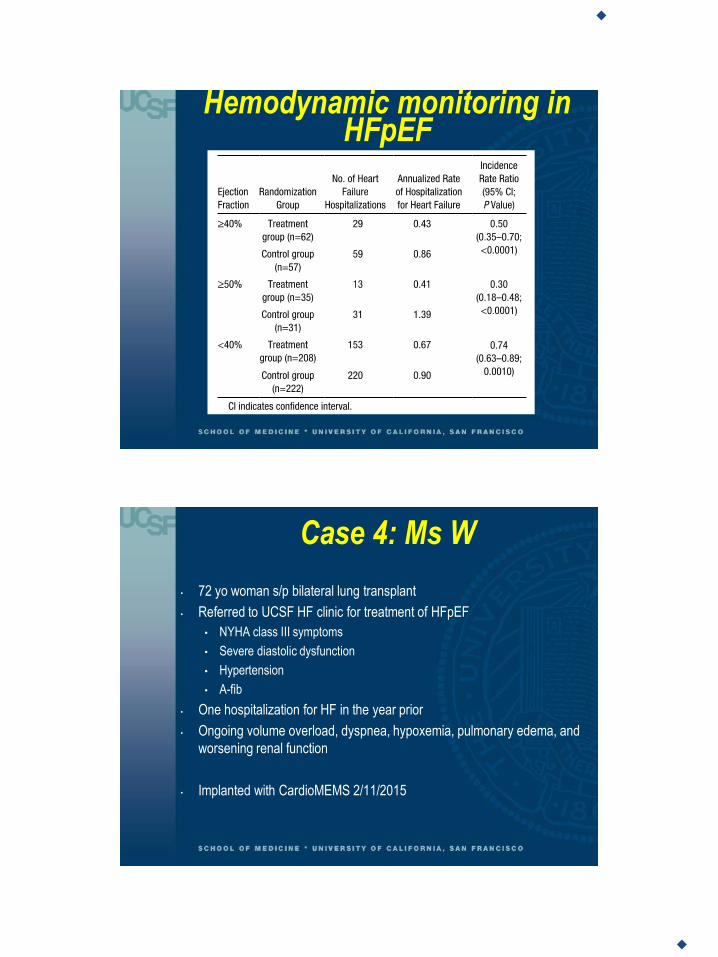
Hemodynamic monitoring in HFpEF
Case 4: Ms W
• 72 yo woman s/p bilateral lung transplant
• Referred to UCSF HF clinic for treatment of HFpEF
• NYHA class III symptoms
• Severe diastolic dysfunction
• Hypertension
• A-fib
• One hospitalization for HF in the year prior
• Ongoing volume overload, dyspnea, hypoxemia, pulmonary edema, and
worsening renal function
• Implanted with CardioMEMS 2/11/2015
10/10/2015
16
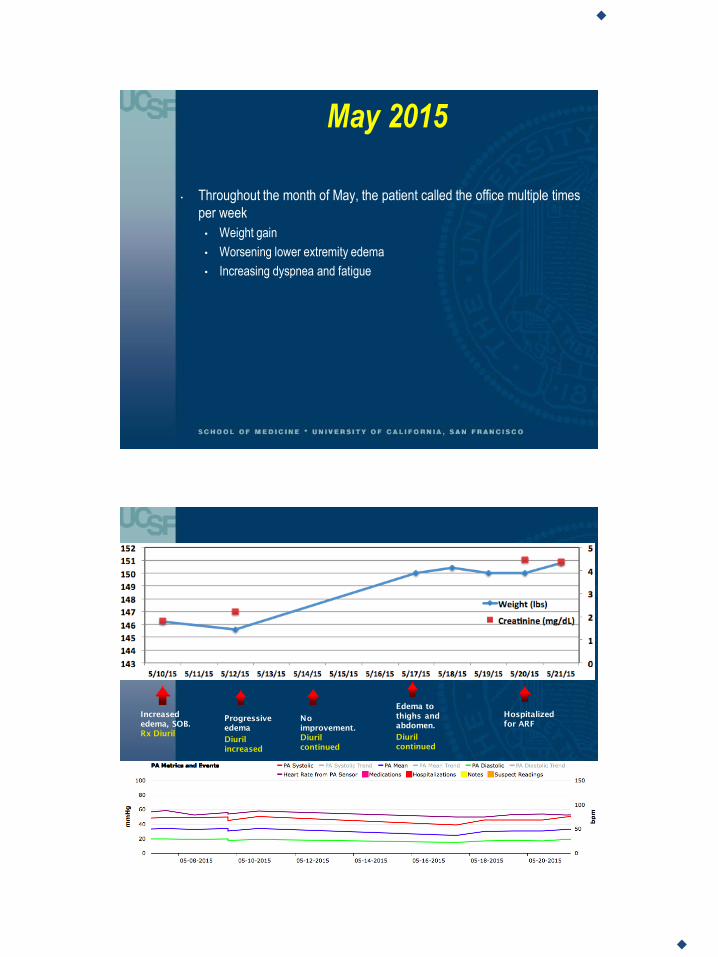
May 2015
• Throughout the month of May, the patient called the office multiple times
per week
• Weight gain
• Worsening lower extremity edema
• Increasing dyspnea and fatigue
Increased
edema, SOB.
Rx Diuril
Hospitalized
for ARF Progressive
edema
Diuril
increased
No
improvement.
Diuril
continued
Edema to
thighs and
abdomen.
Diuril
continued

10/10/2015
17
Ms W, conclusion
• Creatinine peaked at 4.7
• Hospitalized for acute renal failure
• Discharged, but continued to have problems with edema and dyspnea
Hemodynamic vs clinical management strategies
! Search Results
AB36-02 - Pressure for Action: ImplantablePulmonary Artery Pressure SensorMeasurements Alone Beat Clinical Signs toGuide Prevention of Heart FailureHospitalizations
" May 15, 2015, 1:45 - 2:00 PM #
Authors
Lee R. Goldberg, MD, MPH, Akshay S. Desai, MD, MPH, Maria Rosa Costanzo, MD, Lynne W. Stevenson, MD, Philip B.
Adamson, MD, J. Thomas Heywood, MD and William T. Abraham, MD. University of Pennsylvania, Philadelphia, PA,
Brigham and Women's Hospital, Boston, MA, Midwest Heart Specialists - Advocate Medical Group, Naperville, IL,
Oklahoma Heart Hospital, Oklahoma City, OK, Scripps Clinic, La Jolla, CA, Ohio State University Heart Center,
Columbus, OH
Disclosures
L.R. Goldberg: A - Consulting Fees/Honoraria; 1; St. Jude Medical, Boston Scientific Corp., Respicardia. I -
Research Grants; 2; CardioMEMS. A.S. Desai: A - Consulting Fees/Honoraria; 1; CardioMEMS, St. Jude Medical. M.
Costanzo: I - Research Grants; 1; CardioMEMS, St. Jude Medical. L.W. Stevenson: I - Research Grants; 1;
CardioMEMS, St. Jude Medical. P.B. Adamson: A - Consulting Fees/Honoraria; 1; CardioMEMS, St. Jude Medical. J.
Heywood: A - Consulting Fees/Honoraria; 1; CardioMEMS, St. Jude Medical. W.T. Abraham: A - Consulting
Fees/Honoraria; 1; St. Jude Medical.
Abstract
Introduction: Ambulatory hemodynamic monitoring of pulmonary artery pressures (PAP) decreased heart failure
hospitalizations (HFH) when pressure information was available to treating physicians in the CHAMPION trial.
However, it has not been determined how this PAP information was useful in addition to traditional clinical findings
related to congestion and fluid balance.
Methods: In the CHAMPION trial, 550 patients with NYHA class III HF and a HFH in the previous year were
randomized to Control (280) or PAP management (270). All interventions for patients in the PAP managed group
were characterized prospectively by investigators as triggered primarily by clinical findings OR by changes in PAP. All
interventions in the Control group were based only on clinical findings including changes in weight, symptoms or
physical findings.
Results: During the 6 month primary endpoint period, there were 585 changes in diuretic therapy in the Control
group and similar 594 triggered by clinical changes in the PAP managed group, in which an additional 953 were
triggered by PAP. HFH rates remained high in the PAP managed group if diuretic interventions were made only for
clinical changes. HFH rates were lowest in the patients for whom all diuretic interventions were triggered by PAP,
despite this cohort having the highest baseline PAP.
Conclusions: Heart failure hospitalization rates were most effectively reduced by a management strategy based
on pulmonary artery pressures without reliance upon clinical changes. This supports the strategy of early
intervention prior to clinical signs to avert clinical decompensation and heart failure readmissions.
(http://files.abstractsonline.com/CTRL/ff/4/450/68f/ac9/47a/78f/fad/6dd/227/163/0b/g7186_1.jpg)
$ Add To Itinerary
Goldberg LR et al, HRS 2015

10/10/2015
18
Conclusions
• Most HF hospitalizations are due to congestion
• Monitoring PAP/PAWP can identify impending events prior to weight gain
or worsening symptoms
• CardioMEMS can effectively reduce hospitalizations for heart failure when:
• Patients are well-selected
• The office is equipped to handle the increased volume
• A clear treatment algorithm based on hemodynamic data is used
• Don’t just go by clinical signs/symptoms, use the complete picture
• Ongoing post-approval CardioMEMS registry will provide valuable insights
to real world benefits and limitations of hemodynamic monitoring