Embed Size (px)
Citation preview

Recurrent Protein-losing Enteropathy and Tricuspid ValveInsufficiency in a Transplanted Heart: A Causal Relationship?chd_557 10..13
Sanjeev Aggarwal, MD,* Ralph E. Delius, MD,† Henry L. Walters, MD,† andThomas J. L’Ecuyer, MD*
*Division of Pediatric Cardiology, †Department of Cardiovascular Surgery, Children’s Hospital of Michigan, Detroit, Mich,USA
A B S T R A C T
This case report describes a toddler who developed a protein-losing enteropathy (PLE) 4 years after orthotopic hearttransplantation (OHT). He was born with a hypoplastic left heart syndrome for which he underwent a successfulNorwood procedure, a Hemi–Fontan palliation, and a Fontan palliation at 18 months of age. Fifteen monthsfollowing the Fontan operation, he developed a PLE and Fontan failure requiring OHT. Four years after OHT, hedeveloped a severe tricuspid regurgitation and a PLE. His PLE improved after tricuspid valve replacement. It is now2 years since his tricuspid valve replacement and he remains clinically free of ascites and peripheral edema with anormal serum albumin level. His prosthetic tricuspid valve is functioning normally.
Key Words. Protein-losing Enteropathy; Heart Transplantation; Tricuspid Valve Regurgitation
Introduction
Protein-losing enteropathy (PLE) is a recog-nized complication of the Fontan procedure
for which cardiac transplantation is considereda rescue therapeutic option. Resolution of thePLE has been reported following an orthotopicheart transplantation (OHT). We report a case ofFontan palliation with PLE who has improvedfollowing a heart transplantation and subsequentlydeveloped a recurrence of PLE, which resolvedwith a tricuspid valve replacement.
Case Report
Our patient was antenatally diagnosed with ahypoplastic left heart syndrome with a mitral andan aortic atresia and underwent the first stage ofthe Norwood procedure at 8 days of age. He sub-sequently developed a moderate-to-severe tricus-pid regurgitation (TR) with a right ventriculardilatation. At 6 months of age, he underwent theHemi–Fontan procedure and the tricuspid valvu-loplasty with a marked improvement in his cardio-vascular status. On cardiac catheterization beforethe completion of Fontan palliation, the pulmo-nary arterial pressure was normal at 12 mm Hgand the pulmonary vascular resistance was1.2 WU/m. At 18 months of age, he underwent a
Fontan procedure with a 3-mm fenestration. Sub-sequently at 29 months of age, he developed asignificant right ventricular dysfunction, a moder-ate TR, ascites, and a PLE. Medical managementof PLE included intravenous albumin and lasixtherapy. In view of a significant gradient across thefenestration on echocardiogram, a balloon dilationof the atrial level fenestration was performed,which resulted in a reduction of central venouspressure from 16–17 mm Hg to 12 mm Hg.Oxygen saturations decreased from 92% to60–65% without any improvement with 100%oxygen and nitric oxide. He continued to requirepressors (milrinone 0.75 mg/kg/min and dob-utamine 10 mcg/kg/min) and developed ascitesand peripheral edema. Therefore, after 3 weeks adecision was made to list for an OHT for refrac-tory PLE.
At 33 months of age, he underwent anOHT; his immediate postoperative course wascomplicated by a right ventricular dysfunction,requiring extracorporeal membrane oxygenation.He was discharged home 5 weeks after transplantand received a standard immunosupression includ-ing antithymocyte gamma globulin, steroids,imuran, and tacrolimus. Following the OHT, hehad a mild–to-moderate TR with normal rightventricular and pulmonary artery pressures and
E10
© 2011 Wiley Periodicals, Inc.Congenit Heart Dis. 2012;7:E10–E13

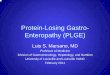
pulmonary vascular resistance on multiple cardiaccatheterizations. Around 2 years after the OHT,he developed a clinical rejection with the worsen-ing of the tricuspid valve regurgitation and a junc-tional rhythm with a rate of 120 bpm. Over thenext 2 years, the severe TR persisted (Figure 1)with the development of a significant dilatationof the right atrium and inferior vena cava andeasy fatigability. However, his right ventricularpressure and function remained normal. Fouryears after his OHT, he developed significantascites, hepatomegaly, and peripheral edemarequiring hospitalization. His cardiac catheteriza-tion revealed a mean capillary wedge pressure of10 mm Hg and a right atrial pressure of 15 mmof Hg. His endomyocardial biopsy was negativefor cellar rejection, although there was a posi-tive blood vessel Complemet 4 split product D(C4D) staining and had some detectable antidonorantibodies compatible with humoral rejection.Extensive hematology and chemistry evaluationswere normal except for a low serum albuminof 1.5 g/dL. Stool was positive for alpha1-antitrypsin. He was treated with intravenousimmunoglobulin and prednisolone for humoralrejection. He also received albumin infusions withlasix without any significant improvement in hisalbumin level. Even after treatment for humoralrejection with intravenous immunoglobulin(IVIG), he continued to have a low serum albuminwith signs of a right-sided heart failure. A repeatcatheterization performed 3 months after thishospitalization revealed a right atrial a wave of15 mm Hg, a mean right atrial pressure of11 mm Hg, a right ventricular end diastolic pres-sure of 7 mm Hg, a cardiac output of 3.4 L/min/
M2, and a pulmonary vascular resistance of 0.88Wood unit/m2. The endomyocardial biopsy per-formed was negative for both cellular rejection andhumoral rejection (negative for C4D staining). Anelectrophysiological study performed at the timedemonstrated a sick sinus syndrome with an inter-mittent sinus acceleration and deceleration, an evi-dence of atrioventricular (AV) node dysfunction, afirst degree AV block, and an accelerated junc-tional rhythm. No substrate site potentially ame-nable to radiofrequency ablation was uncovered.He continued to have a low albumin level, ascites,and a peripheral edema consistent with a recurrentPLE.
At this time, it was decided to repair the tricus-pid valve in an attempt to improve the hemody-namics and reduce the size of the right atrium andrestore the AV synchrony. During the surgery, thetricuspid valve was found to comprise three thindelicate leaflets with a very dysfunctional anteriorleaflet and a very slender papillary muscle, whichwas attached directly to the free margin of theleaflet. Therefore, the tricuspid valve replacementwith a 27-mm Carpentier-Edwards perimountbovine pericardial mitral bioprosthesis (EdwardsLifesciences, Irvine, Calif, USA) was performed.In the weeks following the procedure, there was asteady improvement of ascites, pedal edema, andhepatomegaly with an improvement in serumalbumin to 3.8 g/dL. Alpha 1-antitrypsin in stoolbecame negative. At the latest follow-up 2 yearsafter the tricuspid valve replacement, he remainsfree of ascites, peripheral edema, or PLE with asignificant improvement in the right atrial and theright ventricular size on echocardiogram, and animprovement in the right atrial pressure (mean8 mm Hg) on cardiac catheterization. His elec-trocardiogram continues to show a junctionalrhythm. He has persistent donor-specific antibod-ies in blood even after IVIG, plasmapheresis, andrituximab, and continues to receive antirejectionmedications. His latest serum albumin is 4.2 g/dL.Table 1 describes the serum albumin concentra-tions and the right and left atrial pressures at dif-ferent time points through the clinical course ofthe subject.
Discussion
Since 1971, when Fontan palliation was firstdescribed, it has been extensively used forcongenital heart defects with a single ventriclephysiology.1 The development of PLE is a recog-
Figure 1. Apical four-chamber view showing severe tricus-pid valve regurgitation and severely dilated right atrium.
Congenit Heart Dis. 2012;7:E10–E13
Protein-Losing Enteropathy E11

nized long-term complication of Fontan pallia-tion, reported to occur in 5–13% of cases.2,3
Patients with PLE have generalized edema,ascites, and diarrhea, and a dismal prognosis with areported 5-year survival of 46–59%.2 Althoughthere is no consensus on management strategies,therapeutic options include medications such asdiuretics, afterload reducers, steroids, and heparin;interventional options include fenestration of theatrial septum, balloon dilatation of obstructedpathways, or surgical conversion to lateraltunnel.2–6 OHT is considered a rescue modalityfor patients with refractory PLE following aFontan repair.7–9 At least two case reports describean improvement or reversal of PLE after thetransplantation in children who had undergone aFontan palliation.8,9 Bernstein et al. reported thatPLE resolved in 19 out of 34 failed Fontanpatients who survived >30 days after the OHT.7 Inour patient, PLE resolved and right ventricularfunction remained normal for nearly 4 years fol-lowing the OHT.
Holmgren et al. noted an inverse correlationbetween inferior vena caval pressures and serumalbumin concentrations in a 10-year-old boy.Gradual resolution of PLE after OHT correlatedwith a decrease in inferior vena caval pressures tonormal values. In our case, a gradual increase inthe right atrial pressure following the OHT wasassociated with recurrence of the PLE and itsimprovement with decrease in the right atrialpressure after tricuspid valve replacement. It ispossible that thresholds of right atrial pressurethat are associated with clinical PLE may vary inindividual cases.
Our patient developed a severe TR, an elevatedright atrial pressure, and a severe dilation of theright atrium and a recurrence of the PLE post-OHT. Tricuspid valve replacement resulted in an
improvement in the right atrial pressure and aresolution of the PLE. Scattered case reports havepreviously described an association betweensevere TR (traumatic or rheumatic in etiology)and PLE.10,11 In one case report, PLE secondaryto severe TR led to a lymphopenia and an immu-nological deficiency.12 Improvement in PLE afterthe repair of tricuspid valve has been reported inone previous patient with a TR related to rheu-matic heart disease.10 The mechanistic explana-tion for the association between triscuspid valveregurgitation and PLE remains speculative. Onemechanism could be a poor cardiac output sec-ondary to TR, causing poor intestinal mucosalperfusion, mucosal damage, and consequentlyPLE. Another plausible explanation is that anelevated venous pressure causes impairment of thelymphatic drainage from the intestinal mucosa,lymphangiectasia, and PLE. A third postulatedmechanism is an inflammation and infection ofenteral mucosa secondary to autoimmune disease.In fact, immunosuppression has been used tomanage some cases of PLE. This is the first casereport that we are aware of, where PLE wasobserved in association with TR in a transplantedheart.
In conclusion, a refractory PLE following aFontan repair can resolve after the OHT. PLEmay recur with a hemodynamic derangement anda correction of the hemodynamic derangementresulted in PLE resolution. We speculate that theprior PLE with a Fontan circulation may havealtered the lymphatic circulation and somehowpredisposed to the redevelopment of PLE inassociation with the TR. TR in our patient wasthought to be secondary to right ventricular dys-function, although endomyocardial biopsies mayplausibly have contributed to its progression. Afterexcluding hepatic and infectious causes of protein
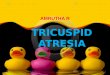
Table 1. Serum Albumin Concentrations and Right and Left Atrial Pressures on Cardiac Catheterization at Different TimePoints through the Clinical Course of the Subject
Time Points during Clinical Course AgeMean CVP/RAPressure (mmHg)
Mean LA /wedgePressure (mmHg)
Serum Albumin(mg/dl)
Pre-Hemi–Fontan palliation 4 months 18 10 NAPre-Fontan palliation 18 months 12 6 NAPost-Fontan, severe PLE 30 months 17 12 1.2-2.8Post-OHT 32 months 16 20 2.81 month after OHT 33 months 11 12 3.21 year after OHT 42 months 8 13 3.83 years after OHT 6 years 12 10 4.24 years after OHT, PLE 7 years 15 10 1.5–2.26 months after tricuspid valve replacement 7.5 years 9 13 3.91 year after tricuspid valve replacement 8 years 10 14 4.42 years after tricuspid valve replacement 9 years 8 13 4.6
CVP, central venous pressure; LA, left atrial; RA, right atrial; NA, not applicable; PLE, protein-losing enteropathy; OHT, orthotopic heart transplantation.
Aggarwal et al.E12
Congenit Heart Dis. 2012;7:E10–E13

loss, elevated right atrial pressure should be con-sidered as a causative factor in PLE in transplantedpatients. Surgical repair of the tricuspid valve andimprovement in the right-sided pressures may becurative in such cases.
Corresponding Author: Sanjeev Aggarwal, MD,Division of Pediatric Cardiology, Department of Pedi-atrics, Children’s Hospital of Michigan, 3901 BeaubienBlvd, Detroit, MI 48201, USA. Tel: 313-745-6105;Fax: 313 993 0894; E-mail: [email protected]
Conflict of interest: There is no financial support or grant.
Accepted in final form: June 7, 2011.
References
1 Fontan F, Baudet E. Surgical repair of tricuspidatresia. Thorax. 1971;26:240–248.
2 Mertens L, Hagler DJ, Sauer U, Somerville J,Gewillig M. Protein-losing enteropathy after theFontan operation: an international multicenterstudy. PLE study group. J Thorac Cardiovasc Surg.1998;115:1063–1073.
3 Therrien J, Webb GD, Gatzoulis MA. Reversal ofprotein losing enteropathy with prednisone in adultswith modified Fontan operations: long term pallia-tion or bridge to cardiac transplantation? Heart.1999;82:241–243.
4 Feldt RH, Driscoll DJ, Offord KP, et al. Protein-losing enteropathy after the Fontan operation.J Thorac Cardiovasc Surg. 1996;112:672–680.
5 Jacobs ML, Rychik J, Byrum CJ, Norwood WI, Jr.Protein-losing enteropathy after Fontan operation:resolution after baffle fenestration. Ann Thorac Surg.1996;61:206–208.
6 Van Dellen RG, Lewis JC. Oral administration ofcromolyn in a patient with protein-losing enteropa-thy, food allergy, and eosinophilic gastroenteritis.Mayo Clin Proc. 1994;69:441–444.
7 Bernstein D, Naftel D, Chin C, et al. Outcome oflisting for cardiac transplantation for failed Fontan:a multi-institutional study. Circulation. 2006;114:273–280.
8 Brancaccio G, Carotti A, D’Argenio P, MichielonG, Parisi F. Protein-losing enteropathy after Fontansurgery: resolution after cardiac transplantation.J Heart Lung Transplant. 2003;22:484–486.
9 Holmgren D, Berggren H, Wahlander H, HallbergM, Myrdal U. Reversal of protein-losing enteropa-thy in a child with Fontan circulation is correlatedwith central venous pressure after heart transplan-tation. Pediatr Transplant. 2001;5:135–137.
10 Hiew C, Collins N, Foy A, Thomson D, Bastian B.Successful surgical treatment of protein-losingenteropathy complicating rheumatic tricuspidregurgitation. Heart Lung Circ. 2008;17:73–75.
11 Lin CH. Traumatic tricuspid regurgitation resultingin protein-losing enteropathy: a case report. J HeartValve Dis. 2005;14:852–854.
12 Strober W, Cohen LS, Waldmann TA, BraunwaldE. Tricuspid regurgitation. A newly recognizedcause of protein-losing enteropathy, lymphocyto-penia and immunologic deficiency. Am J Med.1968;44:842–850.
Congenit Heart Dis. 2012;7:E10–E13
Protein-Losing Enteropathy E13