Embed Size (px)
Citation preview
Recurrent ischemia in the zone of prior myocardial infarction: Results of coronary angioplasty of the infarct-related artery
We studied the efficacy of coronary angioplasty (PTCA) of the infarct-related artery in 54
patients with recurrent myocardial ischemia in the zone of prior infarction. Our patients had recurrent ischemia 10 2 7 days after infarction, with 75% experiencing rest angina and 15%
having evidence of reinfarction. Angiography of the infarct-related artery demonstrated a critical stenosis in 35 of 54, a subtotal occlusion in 5 of 54, and a total occlusion in 14 of 54. PTCA was
successful in 94% of critical stenoses, 80% of subtotal occlusions, but in only 50% of total occlusions. Complications related to PTCA included a 3.7% rate of emergency surgery, but no
deaths or infarctions. During the clinical follow-up period of 11 f 7 months, there was one reinfarction and no deaths. Although 27% of our 44 patients with a successful initial PTCA
required a second revascularization procedure for recurrent angina, 40 patients (91%) remained symptomatically improved with angioplasty alone (including successful repeat PTCA in eight
patients). We conclude that PTCA of the infarct-related artery is beneficial for selected patients with recurrent ischemia in the zone of prior infarction. (AM HEART J lQ88;115:14.)
James Hopkins, M.D., Michael Savage, M.D., Andrew Zalewski, M.D., John P. Dervan, M.D., and Sheldon Goldberg, M.D. Philadelphia, Pa.
Recurrent angina following a myocardial infarction is due to either ischemia of viable myocardium within the zone of prior infarction or to myocardial ischemia in a vascular bed at a distance from the infarct zone. While patients with ischemia at a distance have the worst prognosis, patients with ischemia in the zone of prior infarction also have significant risk of reinfarction or sudden death.l Therefore, revascularization is generally recom- mended for patients with post infarction angina. Since patients with ischemia at a distance have multivessel disease, coronary artery surgery is usual- ly indicated and can now be performed with low morbidity and mortality. 2,3 In those patients with recurrent ischemia in the zone of prior infarction, percutaneous transluminal coronary angioplasty (PTCA) of the infarct-related artery is an alterna- tive mode of myocardial revascularization.
The initial outcome of PTCA of the infarct- related artery and the efficacy of a successful PTCA
From the Division of Cardiology, Department of Medicine, Thomas Jefferson University Hospital.
Supported in part by a grant from the Johnson and Johnson Family of Companies.
Received for publication March 2, 1987; accepted Aug. 3, 1987.
Reprint requests: Sheldon Goldberg, M.D., Cardiac Catheterization Labo- ratory, Thomas Jefferson University Hospital, 111 S. 11th St., Philadel- phia, PA 19107.
in preventing future adverse cardiac events associ- ated with the infarct-related artery have not been widely documented. Therefore, the goals of this study were (1) to describe the clinical and angio- graphic findings of patients who have recurrent ischemia in the zone of prior infarction and are candidates for PTCA; (2) to identify factors that affect the initial outcome of PTCA of the infarct- related artery; and (3) to assess whether successful PTCA improves the long-term prognosis of patients with recurrent ischemia in the zone of prior infarc- tion.
METHODS
Patient selection. We reviewed the data from 352 consecutive patients who underwent ?TCA at Thomas Jefferson University Hospital from January, 1984, to March, 1986. The study group consisted of 54 PTCA candidates who had had a recent myocardial infarction complicated by recurrent myocardial ischemia within the zone of prior infarction. Selection for PTCA was based on the presence of a critical stenosis in the infarct-related artery and the ability to achieve complete revasculariza- tion with PTCA. Patients with triple-vessel or left main disease were excluded from consideration for PTCA. Recurrent ischemia was defined as follows: at least one episode of rest angina more than 10 minutes in duration or aL least two episodes of exertional angina occurring within 30 days of prior myocardial infarction. The determination of ischemia localized to the infarct zone was made on the
14

Table 1. Clinical characteristics of 54 patients with recur- Table II. Electrocardiographic changes recorded in the rent ischemia after myocardial infarction leads of prior infarction during recurrent ischemia
Age Sex
Q wave MI Non-Q wave MI Infarct location
Clinical presentation
Interval between MI and ischemic event
Reinfarction
MI = myocardial infarction.
56 years (range 35-70 years) 43/54 (80%) males 11/54 (20%) females 31/54 (57%) 23/54 (43%) 30 anterior 12 inferior 9 inferoposterolaterai 2 indeterminate
40/54 (75%) rest angina 14/54 (25 % ) exertion al angina 10 t 7 days (range 2-27 days) 7 k 5 days for rest angina
16 + 9 days for exertional angina S/54 (15%) patients
basis of ECG and/or angiographic criteria. 12atients who were included on the basis of ECG criteria ha.d at least a 1 mm ST segment shift from the isoelectric line or a T wave change during angina in the leads that demonstrated prior infarction. The angiographic criteria for inclusion was a 75% to 100% “culprit” stenosis of the infarct-related artery.
Clinical characteristics. The following descriptors were recorded: Q wave or non-Q wave infarction; infarct loca- tion; the time interval between myocardial infarction and post infarction angina; rest or exertional angina; ST segment shift or T wave change during angina; and the incidence of reinfarction. Non-Q wave infarction was defined by the presence of at least two of three criteria: 30 minutes of chest pain, elevation of the creatine phospho- kinase (CPK) to at least twice the top normal value, or new persistent ST or T wave changes on the ECG. A Q wave infarction was present if pathologic Q waves evolved in at least two limb leads or three precordial leads. Reinfarction was defined as recurrent ischemia after a myocardial infarction associated with a new elevation of the CPK to at least twice the top normal value, recurrent elevation of the CPK with a positive MB fraction, or new Q waves in two leads of the ECG.
Coronary arteriography and ventriculography. All cor- onary arteriograms were reviewed by two observers. The initial arteriogram of the infarct-related artery was evalu- ated for stenosis severity, morphology, thrombus, and collateral flow to the infarct vessel. Stenosis severity was assigned after reviewing an artery in two orthogonal views. Each stenosis was graded as (0 % to 49 % ), (50 % to 75 % ), (75 % to 99%), subtotal occlusion (loss of continuity of contrast at the stenosis with Thrombolysis in Myocardial Infarction trial [TIMI] grade 1 or 2 antegrade perfusion), or total occlusion (no antegrade flow). Stenosis morpholo- gy was judged by criteria similar to those of .4mbrose et al.? concentric (symmetric stenosis with a relatively smooth border), eccentric-smooth (asymmetric stenosis with a smooth border), eccentric-irregular (asymmetric
PTCA for post infarction angina 15
ST elevation ST depression T wave change
14 patients 12 patients 8 patients
stenosis with irregular or scalloped border), and diffuse (segmental disease or serial stenoses). Angiographic evi- dence of intracoronary thrombus was defined as delayed staining of contrast at the site of occlusion or an intracor- onary filling defect surrounded by contrast. Collaterals to the infarct-related artery were considered present if there was collateral filling of the infarct-related artery itself or a branch vessel. An ejection fraction and a subjective evalu- ation of the infarct segment systolic function were record- ed in 41 patients who had ventriculography performed.
Coronary angioplasty. PTCA was preformed by means of standard techniques.5 Inflation pressure was 80 to 140 psi. Inflation duration was 1 to 5 minutes. After dilatation, all patients received intravenous heparin for 6 to 24 hours, a calcium channel blocker, aspirin, dipyridamole, and nitrates. PTCA success was defined as less than a 50% diameter narrowing at completion of the procedure, a final trans-lesional gradient less than 20 mm Hg, and no in-hospital recurrent ischemic event.
During the follow-up period, patients and their physi- cians were questioned about the incidence of recurrent angina, reinfarction, sudden death, or an additional revas- cularization procedure. Repeat angiography was perform- ed in all symptomatic patients and was offered to all asymptomatic patients approximately 6 months after PTCA.
Statistical analysis. Results were expressed as a mean f standard error of the mean. Values were com- pared within groups by means of Student’s paired t test and between groups by means of Student’s t test for group observations. Fisher’s exact test was used to evaluate the incidence of reinfarction in patients with and without ST elevation.
RESULTS
Clinical findings. The clinical characteristics of the 54 patients with post infarction ischemia who under- went PTCA are presented in Table I. Recurrent rest angina occurred in 75% (40 of 54) patients and culminated in reinfarction in 15% (8 of 54) of patients. The time interval between myocardial infarction and recurrent ischemia was 10 t 7 days (range 2 to 27 days). This interval was significantly shorter in patients with rest angina (7 + 5 days) as compared to patients with purely exertional angina (16 f 9 days, p < 0.05).
As demonstrated in Table II, ST segment shifts or T wave changes in the leads of the infarct zone were documented during post infarction angina in 34
16 Hopkins et al.
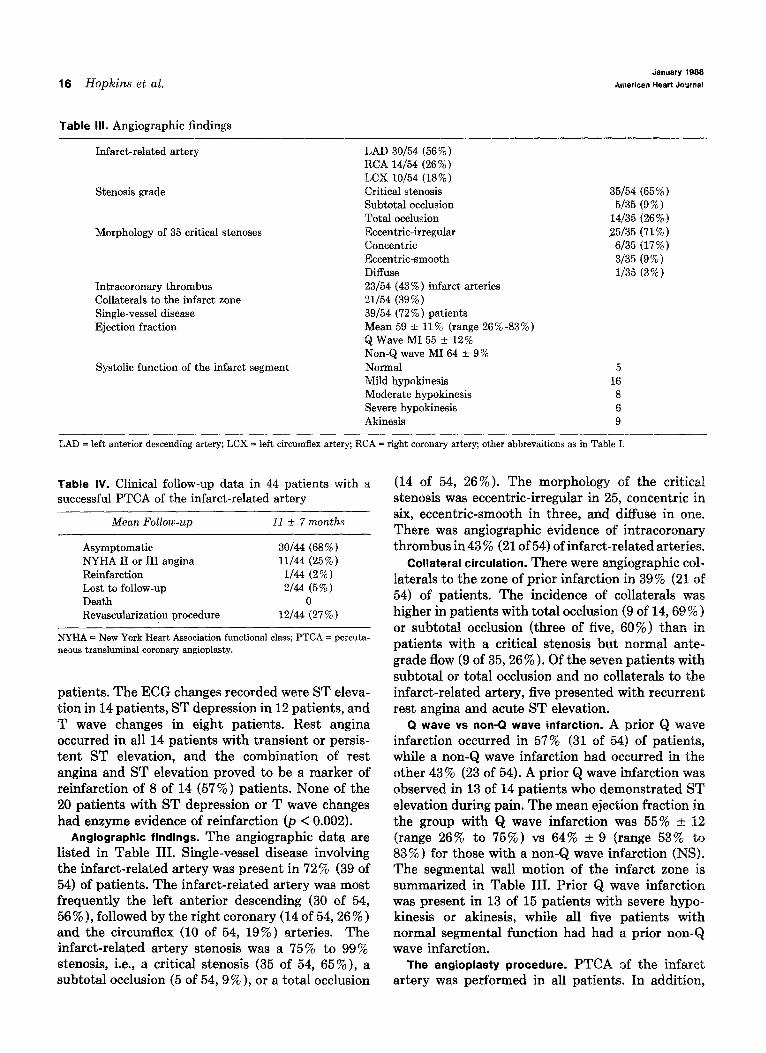
Table Ill. Angiographic findings
Infarct-related artery
Stenosis grade
Morphology of 35 critical stenoses
Intracoronary thrombus Collaterals to the infarct zone Single-vessel disease Ejection fraction
Systolic function of the infarct segment
LAD 30/54 (56%) RCA 14/54 (26%) LCX 10/54 (18%) Critical stenosis Subtotal occlusion Total occlusion Eccentric-irregular Concentric Eccentric-smooth Diffuse 23/54 (43%) infarct arteries u/54 (39%) 39/54 (72 % ) patients Mean 59 * 11% (range 26%-83%) QWaveM155 + 12% Non-Q wave MI 64 f 9% Normal Mild hypokinesis Moderate hypokinesis Severe hypokinesis Akinesis
35/54 (65%) 5/35 (9 % )
14/35 (26%) 25/35 (71%) 6/35 (17%) 3135 (9 % ) l/35 (3%)
5 16 8 6 9
LAD = left anterior descending artery; LCX = left circumflex artery; RCA = right coronary artery; other abbrevaitions as in Table I.
Table IV. Clinical follow-up data in 44 patients with a successful PTCA of the infarct-related artery
Mean Follow-up 11 + 7 months
Asymptomatic 30/44 (68% ) NYHA II or III angina 11/44 (25 % ) Reinfarction l/44 (2 % ) Lost to follow-up 2/44 (5 % ) Death 0 Revascularization procedure 12/44 (27%)
NYHA = New York Heart Association functional class; PTCA = percuta- neous transluminal coronary angioplasty.
patients. The ECG changes recorded were ST eleva- tion in 14 patients, ST depression in 12 patients, and T wave changes in eight patients. Rest angina occurred in all 14 patients with transient or persis- tent ST elevation, and the combination of rest angina and ST elevation proved to be a marker of reinfarction of 8 of 14 (57 % ) patients. None of the 20 patients with ST depression or T wave changes had enzyme evidence of reinfarction (p < 0.002).
Angiographic findings. The angiographic data are listed in Table III. Single-vessel disease involving the infarct-related artery was present in 72% (39 of 54) of patients. The infarct-related artery was most frequently the left anterior descending (30 of 54, 56 % ), followed by the right coronary (14 of 54,26 % ) and the circumflex (10 of 54, 19%) arteries. The infarct-related artery stenosis was a 75% to 99% stenosis, i.e., a critical stenosis (35 of 54, 65%), a subtotal occlusion (5 of 54,9%), or a total occlusion
(14 of 54, 26%). The morphology of the critical stenosis was eccentric-irregular in 25, concentric in six, eccentric-smooth in three, and diffuse in one. There was angiographic evidence of intracoronary thrombus in 43 % (21 of 54) of infarct-related arteries.
Collateral circulation. There were angiographic col- laterals to the zone of prior infarction in 39% (21 of 54) of patients. The incidence of collaterals was higher in patients with total occlusion (9 of 14,69 % ) or subtotal occlusion (three of five, 60%) than in patients with a critical stenosis but normal ante- grade flow (9 of 35,26%). Of the seven patients with subtotal or total occlusion and no collaterals to the infarct-related artery, five presented with recurrent rest angina and acute ST elevation.
Q wave vs non-Q wave infarction. A prior Q wave infarction occurred in 57% (31 of 54) of patients, while a non-Q wave infarction had occurred in the other 43% (23 of 54). A prior Q wave infarction was observed in 13 of 14 patients who demonstrated ST elevation during pain. The mean ejection fraction in the group with Q wave infarction was 55% t 12 (range 26% to 75%) vs 64% k 9 (range 53% to 83 % ) for those with a non-Q wave infarction (NS). The segmental wall motion of the infarct zone is summarized in Table III. Prior Q wave infarction was present in 13 of 15 patients with severe hypo- kinesis or akinesis, while all five patients with normal segmental function had had a prior non- wave infarction.
The angioplasty procedure. PTCA of the infarct artery was performed in all patients. In addition,
Volume 115
Number 1, Part 1 PTCA for post infarction angina 17
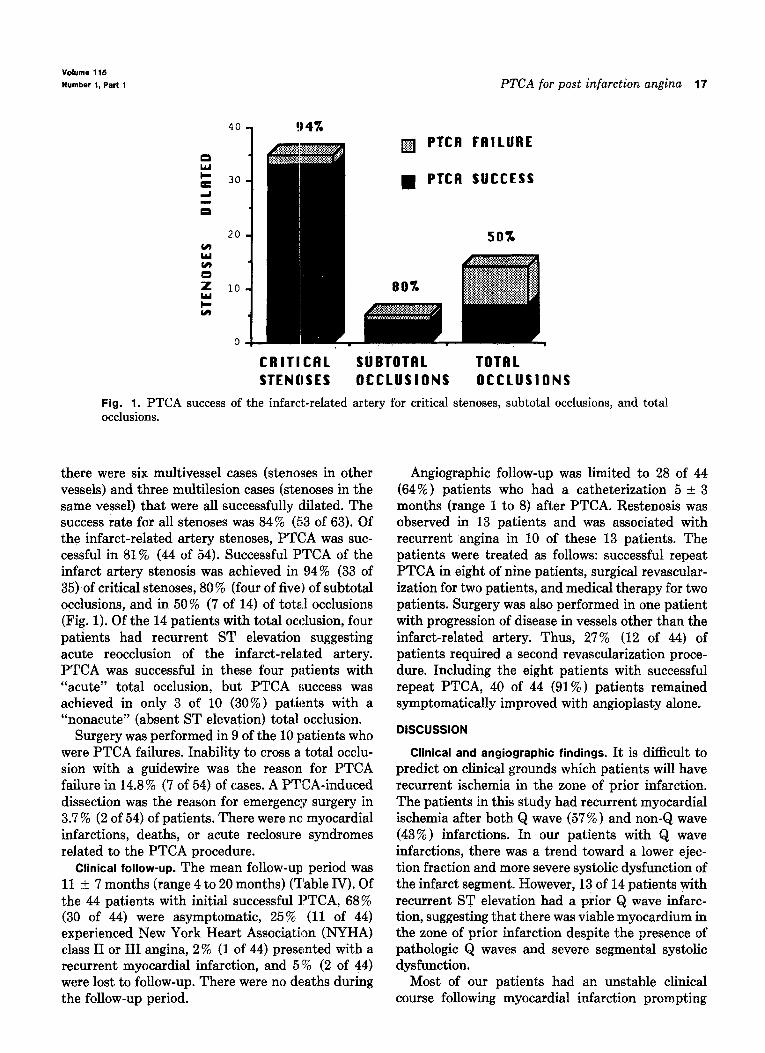
q PTCB FAILURE
n PTCB SUCCESS
CRITICAL SUBTOTAL TOTBL STENUSES OCCLUSIONS OCCLUSIONS
Fig. 1. PTCA success of the infarct-related artery for critical stenoses, subtotal occlusions, and total occlusions.
there were six multivessel cases (&noses in other vessels) and three multilesion cases (stenoses in the same vessel) that were all successfully dilated. The success rate for all stenoses was 84% (53 of 63). Of the infarct-related artery stenoses, PTCA was suc- cessful in 81% (44 of 54). Successful PTCA of the infarct artery stenosis was achieved in 94% (33 of 35) of critical stenoses, 80 % (four of five) of subtotal occlusions, and in 50% (7 of 14) of total occlusions (Fig. 1). Of the 14 patients with total occlusion, four patients had recurrent ST elevation suggesting acute reocclusion of the infarct-rela.ted artery. PTCA was successful in these four patients with “acute” total occlusion, but PTCA success was achieved in only 3 of 10 (30%) patients with a “nonacute” (absent ST elevation) total occlusion.
Surgery was performed in 9 of the 10 patients who were PTCA failures. Inability to cross a total occlu- sion with a guidewire was the reason for PTCA failure in 14.8% (7 of 54) of cases. A PTCA-induced dissection was the reason for emergency surgery in 3.7 % (2 of 54) of patients. There were no myocardial infarctions, deaths, or acute reclosure syndromes related to the PTCA procedure.
Clinical follow-up. The mean follow-up period was 11 f 7 months (range 4 to 20 months) (Table IV). Of the 44 patients with initial successful PTCA, 68% (30 of 44) were asymptomatic, 25 % (11 of 44) experienced New York Heart Association (NYHA) class II or III angina, 2% (1 of 44) presented with a recurrent myocardial infarction, and 5’% (2 of 44) were lost to follow-up. There were no deaths during the follow-up period.
Angiographic follow-up was limited to 28 of 44 (64%) patients who had a catheterization 5 t 3 months (range 1 to 8) after PTCA. Restenosis was observed in 13 patients and was associated with recurrent angina in 10 of these 13 patients. The patients were treated as follows: successful repeat PTCA in eight of nine patients, surgical revascular- ization for two patients, and medical therapy for two patients. Surgery was also performed in one patient with progression of disease in vessels other than the infarct-related artery. Thus, 27% (12 of 44) of patients required a second revascularization proce- dure. Including the eight patients with successful repeat PTCA, 40 of 44 (91% ) patients remained symptomatically improved with angioplasty alone.
DISCUSSION
Clinical and angiographic findings. It is difficult to predict on clinical grounds which patients will have recurrent ischemia in the zone of prior infarction. The patients in this study had recurrent myocardial ischemia after both Q wave (57 % ) and non-Q wave (43%) infarctions. In our patients with Q wave infarctions, there was a trend toward a lower ejec- tion fraction and more severe systolic dysfunction of the infarct segment. However, 13 of 14 patients with recurrent ST elevation had a prior Q wave infarc- tion, suggesting that there was viable myocardium in the zone of prior infarction despite the presence of pathologic Q waves and severe segmental systolic dysfunction.
Most of our patients had an unstable clinical course following myocardial infarction prompting

18 Hopkins et al.
immediate angiographic evaluation of coronary plaques.15 Despite the fact that angiographic evi- anatomy. Early recurrent rest angina occurred in dence of intracoronary thrombus was present in 75% of patients. Rest angina with recurrent ST 43% of our patients and an eccentric, irregular elevation and evidence of reinfarction was present in plaque was observed in the majority of patients, 15% of patients. acute closures were not observed.
Arteriography of the infarct-related artery most frequently demonstrated a critically stenosed but patent artery with normal antegrade flow. The most common stenosis morphology was an eccentric, irregular lesion, which has been previously charac- terized as an “active, unstable” plaque.6 There was a smaller group of patients with a subtotal or total occlusion of the infarct-related artery. These pat,ients had poor or absent antegrade flow, so that perfusion of the infarct zone was largely dependent on collateral circulation. As reported by Freedman et a1.,7 angiographic collaterals were more common in patients with an occlusion of the infarct-related artery. The physiologic importance of these collater- als was demonstrated by the five of seven patients with subtotal or total occlusion and no angiographic collaterals, who presented with acute recurrent ST elevation and evidence of reinfarction.3
Long-term efficacy of PTCA. Previous reports16-1s documented recurrent angina in 8% to 57 % of patients following myocardial infarction. The pres- ence of post infarction angina is associated with a 17% to 34% incidence of reinfarction and an increased risk of sudden death in the first year after myocardial infarction 1,18,1g Gleckel et aLzO reported that even patients with single-vessel disease and post infarction angina have a 20% incidence of death or reinfarction during a 39-month follow-up,
The prognosis of our patients who had a success- ful PTCA was good. There was only one reinfarction and no deaths during a mean follow-up period of 11 months. However, restenosis did limit the long-term efficacy of the procedure in 27 % of our patients who required a second revascularization procedure.
Patients with recurrent ischemia were selected for PTCA on the basis of the arteriogram of the infarct-related artery and the absence of triple- vessel or left main disease. Single-vessel disease of the infarct-related artery was present in 72% of our patients. Other than six carefully selected cases, patients with multivessel disease were not offered PTCA because of the possible complications associ- ated with multivessel PTCAg and the potential for causing severe myocardial dysfunction when dilat- ing a vessel that supplies myocardium at a distance from the infarct zone.lO
Resutts of coronary angioplasty. PTCA of the infarct-related artery had a high initial success rate for patients exhibiting a critical stenosis, subtotal occlusion, or total occlusion with acute ST elevation. The procedure had limited efficacy in those patients with a “nonacute” total occlusion. Inability to cross the occlusion with any available guidewire was the reason for PTCA failure. Thus, the success rate for PTCA of the infarct-related artery is similar to the results of PTCA previously reported for nontota111*12 and totall coronary artery occlusions.
Limitations of present study. Any comparison of the clinical course of our patients to a surgical or medical series is limited because of bias introduced by the use of historic controls. Furthermore, our patients were neither prospectively evaluated nor randomized to therapy. However, the majority of patients in this series had angina that was refractory to maximal medical therapy. Rad they participated in a randomized trial of PTCA vs medical therapy, the majority of patients assigned to medical therapy would have “crossed over” to PTCA. This study reflects the experience of applying PTCA to patients with recurrent ischemia in the same zone as prior infarction, and therefore provides information on the expected clinical course following PTCA in this high-risk group.
Complications related to PTCA were uncommon. A PTCA-induced dissection was the reason for emergency surgery in 3.7% (2 of 54) of patients. There were no deaths or myocardial infarctions associated with the PTCA procedure. Prior studies have reported an increased incidence of acute clo- sure syndrome after PTCA is performed in arteries with intracoronary thrombus14 or eccentric
Previous studies. Although the indications for PTCA have expanded, there are few reports of applying the technique in the setting of post infarc- tion angina. Gottlieb et al.“l reported a 91% success rate in 46 infarct-related arteries and nine nonin- farct-related arteries. Recurrent angina occurred in 22 % during follow-up. Holt et a1.22 reported an 80 % PTCA success rate in 69 patients. There was one death associated with PTCA, two patients experi- enced reinfarction during follow-up, and 24% of patients required a second revascularization proce- dure. DeFeyter et al. 23 have also reported their experience with the application of PTCA in 53 patients with post infarction angina. PTCA for ischemia at a distance was performed in 16% of patients and PTCA success was achieved in 89 % (47 of 53) of all cases. There were two reinfarctions and

Volume 115
Number 1, Part 1 PTCA for post infarction angina 19
26 % of patients had recurrent angina during follow- up.23
clinical implications. Recurrent angina after a myo- cardial infarction carries a poor prognosis, and early revascularization should be considered, In patients with ischemia in the zone of prior infarction, PTCA of the infarct-related artery is an attractive thera- peutic modality for improving perfusion of the infarct zone. While technical factors compromised PTCA success for “nonacute” total occlusions, PTCA of the infarct-related artery was an angio- graphic and clinical success in most patients with myocardial ischemia in the zone of prior infarction. Although a substantial minority of patients required a second revascularization procedure, the long-term prognosis was good. Additional prospective studies are required to determine if PTCA of the infarct- related artery decreases the incidence of reinfarction and sudden death during follow-up.
REFERENCES
1. Schuster EH, Bulkley BH. Early post-infarction angina. Ischemia at a distance and ischemia in the infarct zone. N Engl J Med 1981;305:1101.
3.
4.
5.
2. Jones EL, Waites TF, Craver JM, Bradford JM, Douglas JS. King SB, Bove DK, Dowey ER, Clements SD: Thompkins T; Hatcher CR. Coronary bypass for relief of persistent pain following acute myocardial infarction. Ann Thorac Surg 1981;32:33. Williams DB, Ivey TD, Bailey WW, Ivey SH, Rideout JZ, Douglas S. Postinfarction angina: results of early revascular- ization. J Am Co11 Cardiol 1983;2:859. TIM1 Study Group. The thrombolysis in myscardial infarc- tion (TIMI) trial. N Engl J Med 1985;312:91!j, 932. Gruentzig AR, Senning A, Siegenthaler WE. Nonoperative dilatation of coronary artery stenosis. N Engl J Med 1979;301:61. Ambrose JA, Winters SL, Arora RR, Eng A, Riccio A, Gorlin R. Fuster V. Angiographic evolution of coronary artery morphology in unstable angina. J Am Co11 Cardiol 1986; 7~472. Freedman SB, Dunn RF, Bernstein L, Morris J, Kelly DT. Influence of coronary collateral blood flow on the develop- ment of exertional ischemia and Q wave infarction in oatients with severe single-vessel disease. -Circulation 1985;71‘681. Fuster V, Frve RL. Kennedv MA. The ro1.e of collateral
6.
7.
8. .” circulation in the various coronary syndromes. Circulation 1979;59:1137.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
Cowley MJ, Vetrovec GW, DiSciascio G, Lewis SA, Hirsh PD, Wolfgang TC. Coronary angioplasty of multiple vessels: short and long term results. Circulation 1985;72:1314. Murphy DA, Craver JM, Jones EL, King SB, Curling PE, Douglas JS. Hemodynamic deterioration after coronary angioplasty in the presence of previous left ventricular infarc- tion. Am J Cardiol 1984;54:448. Anderson VA, Roubin GS, Leimgruber PP, Douglas JS, King SB, Gruentzig AR. Primary angiographic success rates of percutaneous transluminal coronary angioplasty. Am J Car- diol 1985;56:712. Bredlau C, Roubin G, Leimgruber P, Douglas J, King S, Gruentzig A. In-hospital morbidity and mortality in elective coronary angioplasty. Circulation 1985;72:1044. Kereiakes DJ, Selmov MR, McAuley BJ, McAuley DB, Sheenan DJ, Simpson JB. Angioplasty in total coronary occlusion: experience in 76 consecutive patients. J Am Co11 Cardiol 1985;6:526. Mabin TA, Holmes DR, Smith WC, Vlietstra RE, Bove AA, Reeder GS, Ctcseboro JH, Bresnaham JR, Orsguhk TA. Intracoronary thrombus: role in coronary occlusion compli- cating percutaneous transluminal angioplasty. J Am Co11 Cardiol 1985;5:198. Ischinger T, Gruentzig AR, Meier B, Galan K. Coronary dissection and total coronary occlusion associated with percu- taneous transluminal coronary angioplasty: significance of initial angiographic morphology of coronary stenoses. Circu- lation 1986;74:1371. Stenson RE, Flamm MD, Zaret BL, McGowan RL. Transient ST-segment elevation with postmyocardial infarction angina: prognostic significance. AM HEART J 1975;89:449. Shapiro EP. Management of the patient with post-infarction angina. In: Plotnick GD, editor. Unstable angina: a clinical approach. Mount Kisco, N.Y.: Futura Publishing Co, 1985. Marmor W, Sobel BE, Roberts R. Factors presaging early recurrent myocardial infarction (“extension”). Am J Cardiol 1981;48:603. Singer DE, Mulley AG, Thibault GE, Barnett GO. Unexpect- ed readmissions to the coronary-care unit during recovery from acute mvocardial infarction. N Enal J Med 1981: 3041625. - Gleckel L, Walkam S, Ross JH, Bodenheimer MM. Signiti- cance of postinfarction angina in patients with single vessel disease. J Am Co11 Cardiol 1986;7:208A. Gottlieb SO, Brin KP, Walford GD, McGaughey M, Riegel MB, Brinker JA. Percutaneous transluminal coronary angio- plasty for early postinfarction unstable angina; results and follow-up. J Am Co11 Cardiol 1986;7:20A. Holt GW, Gersh BJ, Holmes DR, Vlietlstra MB, Reeder GS, Bresnaham JR, Smith HC. The results of percutaneous transluminal angioplasty in postinfarction angina pectoris. J Am Co11 Cardiol 1986;7:62A. DeFeyter PJ, Serruys PW, Brand M, Hugenholtz P. Coronary angioplasty for early postinfarction angina. Circulation 1986:74:1365.





























