Embed Size (px)
Citation preview

CASE REPORT
Recurrent Cushing's Disease Associated withNephrotic Syndrome
Tomohide Tatsumi, Toyohiko Morishima*, Takao Watarai*, Masashi Kubota*, Mineo Kodama*,Munehide Matsuhisa*, Eiichi Imano*, Masaaki Izumi*, Toshiro Takama*, SungHyo Shin**,
Kiyoshi Kawano***, Ryuzo Kawamori* and Takenobu Kamada*
A case of recurrent Cushing's disease with nephrotic syndrome due to membranoproliferativeglomerulonephritis (MPGN)is presented. Functional pituitary adenomarecurred 6 years aftertranssphenoidal pituitary adenomectomy. Due to infiltration into the surrounding tissues,transcranial surgery was performed. However, this failed to induce a remission and thus gammaknife therapy was applied. Histopathological evaluation revealed that the glomerular lesions hadprogressed to a rather advanced stage of MPGN.Although this association could be coincidental,the recurrence of pituitary macroadenomamight be induced by the cessation of steroid treatmentfor the nephrotic syndrome.(Internal Medicine 34: 10-14, 1995)
Key words: transsphenoidal adenomectomy, transcranial surgery, gammaknife, steroid therapy
Introduction
Wereport a case of Cushing's disease in association withnephrotic syndrome. To our knowledge, this appears to be thefirst report of the combination of these two diseases, althoughtwo cases of Cushing's syndrome associated with nephroticsyndrome have appeared in the literature in the last 30 years;one was caused by adrenal adenoma (1) and the otherby ectopiccorticotropin secreting pheochromocytoma (2), in both casesthe nephrotic syndrome was due to focal glomerulosclerosis.The present case displayed recurrent functional pituitary
adenomaand membranoproliferative glomerulonephritis(MPGN) with atypical histological findings.
Case ReportA 30-year-old male was admitted to Osaka University Hos-pital onJuly 23, 1992. In 1986, he hadbeen diagnosed as havingCushing ' s disease due to adrenocorticotropic hormone (ACTH)secreting pituitary adenoma; transsphenoidal pituitary micro-surgery (Hardy's operation) was performed in Osaka Univer-sity Hospital. After the surgery, supplementation withhydrocortisone (15-20 mg once daily) was continued for 6months; the endocrinological data improved and the physicalfindings characteristic of Cushing's disease (moonface and
central obesity etc.) were gradually resolved. Proteinuria wasfirst pointed out on routine examination in 1980. He was
referred to a hospital in 1982, where the diagnosis of chronicglomerulonephritis was made, but he was followed without anymedication thereafter. In 1989, he visited another hospital forfurther examination because of aggravation of the proteinuria,and renal biopsy revealed nephrotic syndrome due to MPGN.After almost one year of treatment with anticoagulants andnonsteroidal anti-inflammatory drugs, prednisolone was initi-ated at an initial dose of40 mg per day in 1990, since there wasno improvement observed in the histological examination ofthe kidney. In spite of steroid therapy, moderate proteinuriapersisted and the patient discontinued the treatment 6 monthslater. From the end of 1991, he gradually became aware ofgeneral fatigue, a moonface, central obesity and striae cutis. InJune 1 992, he visited Osaka University Hospital and recurrenceof the pituitary adenomawas suspected from the brain magneticresonance imaging (MRI) and an elevated plasma ACTHlevel.He was admitted to our hospital for further examination andtreatment.On admission, his height was 165.0 cm with body weight of63.5 kg. Bloodpressure was 124/88 mmHg, with aregularpulserate of 67/min. Physical examination revealed the stigmata ofCushing's disease such as truncal obesity, moon face, buffalohump and striae cutis. Laboratory data on admission and
From the Division of Gastroenterology, Osaka Minami National Hospital, Kawachinagano, *the First Department of Medicine, Osaka University School ofMedicine, Suita, **the Division of Internal Medicine, Osaka Seamen' s Insurance Hospital, Osaka and ***the Division of Clinical Pathology, Osaka Rosai
Hospital, Sakai
Received for publication February 24, 1994; Accepted for publication September 7, 1994Reprint requests should be addressed to Dr. Toyohiko Morishima, the First Department of Medicine, Osaka University School of Medicine, 2-2 Yamadaoka,
Suita565
10 Internal Medicine Vol. 34, No. 1 (January 1995)

Cushing's Disease with Nephrotic Syndrome
endocrinological findings are summarized in Table 1. Hypo-albuminemia (2.5 g/dl), hypercholestrolemia (440 mg/dl), andmoderate proteinuria (3.75 g/day) were all compatible with thediagnosis of nephrotic syndrome. The urine was negative forBence-Jones protein. The levels of serum creatinine and bloodurea nitrogen were normal, and creatinine clearance was withinthe normal range. There were no abnormalities either in theserological or immunological tests. Neurological examinationrevealed no apparent abnormalities except for atrophy andweaknessof the extremities.
Endocrinological examination revealed an elevation in thebasal plasma ACTH level and in 24-hour urinary 17-
hydroxycorticosteroid ( 1 7-OHCS) excretion while the level ofserum cortisol was within the normal range. Although the 24-hour urinary 17-OHCSexcretion was not less than 50%of thebaseline value by low-dose dexamethasone (0.5 mg per os,every 6 hours), it was sufficiently suppressed with high-dosedexamethasone administration (2 mg per os, every 6 hours), asshown in Table 1. No abnormalities were detected in the
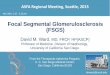
bilateral adrenal glands by abdominal X-ray computed tomog-raphy. Brain computed tomography and MRIrevealed a tumormass in the pituitary gland, which invaded the region aroundboth carotid arteries, especially to the left side (Fig. 1). Theresults of bilateral petrosal sinus sampling with corticotropin-
Table 1. Laboratory Data on Admission and Endocrinological Findings
Peripheral Blood Coagulation TestRed blood cells 487x 1 04/mm3 Activated partial thromboplastin time 23 secHemoglobin 1 5.0 g/dl Prothrombin time 1 03%Hematocrit 46.7 % Fibrinogen 268 mg/dlWhite blood cells 7,730/mm3 Hepaplastin test 1 40%Neutrophil 70. 1 % Fibrin/fibrinogen degradation products l.OO jig/ml
Eosinophil 0.7 % Antithrombin III 1 05 %Basophil 0.7% Plasminogen 86%
Lymphocyte 1 8.0% Serological TestPlatelet 24.7x 1 04/mm3 C-reactive protein (-)
Blood Chemistry Rheumatoid factor (-)Aspartate aminotransferase 1 5 U/l Anti-streptolysin-O (-)Alanine aminotransferase 26 UA Rapid plasma reagin (-)y-glutamyltranspeptidase 7 3 U/l Treponema pallidum hemagglutination (-)Alkaline phosphatase 67 UA Hepatitis B virus surface antigen (-)Total protein 4.4 g/dl Hepatitis B virus surface antibody (-)Albumin 2.5 g/dl Immunological TestGlobulin 1.9 g/dl C3 66 mg/dlA/G 1.3 C4 34 mg/dlThymol turbidity test 1 U CH50 39.3 U/mlZinc sulfate turbidity test 1 U Anti-nucl. Ab x40Total bilirubin 0.6 mg/dl Anti-DNA Ab x5Direct bilirubin 0. 1 mg/dl Serum ElectrophoresisCreatinine 0.8 mg/dl Albumin 55. 1 %Urea nitrogen 1 8 mg/dl arGlbulin 3.7%Total cholesterol 440 mg/dl oc2-Glbulin 2 1.0%Esterified cholesterol 324 mg/dl B-Glbulin 1 0.3 %Triglyceride 1 60 mg/dl y-Glbulin 9. 9%
Non-esterified free fatty acid 121 ueq/dl 75 g Oral glucose tolerance testLow density lipoprotein 1,067 mg/dl 0 30 60 120 (min)Very low density lipoprotein 381 mg/dl Plasmaglucose (mg/dl) 91 138 154 112Chylomicron 49 mg/dl Endocrinological TestLactate dehydrogenase 250 U/l - Basal state -Leucine aminopeptidase 34 UA ACTH[<50] 104 pg/mlCholinesterase 4032 UA Cortisol [4.5-24.0] 1 7.2 jig/dlCreative phosphokinase 60 UA Thyroid stimulating hormone [0.4-5.6] 1. 1 jLiU/mlFasting plasma glucose 86 mg/dl Growth hormone [<6.0] 0. 1 ng/mlHbAlc 6.3% 24-hr-Urinary 17-OHCS[3.4-1 2] 14.5 mg/dayUrine Test 24-hr-Urinary 1 7-KS [4.6-1 8] 8.8 mg/day
glucose (-)
protein 3.75 g/day - Circadian profile -occult blood (+) 8:00 1 6:00 22:00sediments ACTH (pg/ml) 1 10 57 83
RBCs 3-5/HF Cortisol ((ig/dl) 1 5.7 1 1.3 10.4WB Cs 1 -0/HFoval fat bodies (+) - Dexamethasonesuppression test -
Erythrocyte sedimentation rate Pre 2 mg 8 mg1 hr 20 mm, 2 hr 50 mm Urinary 17-OHCS(mg/day) 15.7 1 1 3.4
Values in brackets represent the normal range.
Internal Medicine Vol. 34, No. 1 (January 1995) ll

Tatsumi et al
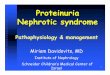
releasing hormone (CRH) administration are illustrated in Fig.2. ACTHlevel in the plasma obtained from the left inferiorpetrosal sinus (lt-IPS) in the basal state was much higher thanthat from the right inferior petrosal sinus (rt-IPS) or peripheralvein (195 pg/ml, 49 pg/ml and 76 pg/ml, respectively). Therewas a remarkable increase in ACTHlevels in the plasma fromlt-IPS following CRHadministration, while those from rt-IPSand the peripheral vein showed almost no changes. Accordingto a recent report by Old field et al, as in the present case, the
Fig. 1. Brain magnetic resonance imaging (MRI) beforetranscranial surgery: sagittal plane (A) and coronal plane (B).
response of functioning pituitary adenoma to CRHadministra-tion is not necessarily reflected in the plasma ACTHlevels inthe peripheral vein (3). Thus, simultaneous sampling from
bilateral petrosal sinus and the peripheral vein could be quiteuseful not only for the differential diagnosis but also for
evaluating the responsiveness of the pituitary adenoma to CRHstimulation. From these endocrinological results and the find-ings of imaging techniques, the diagnosis was recurrence ofACTHsecreting pituitary adenoma (3, 4).Because the tumor was infiltrating the region around bothinternal carotid arteries, hypophysectomy by the transcranialapproach was performed and over 70%of the tumor mass wasresected except for the part around the left carotid artery (Fig.
600-
- CRH O.lmgiv.
500- I
g 400- /
13 /3 3oo- / -à"-lt-IPS
H - / -*-rt-IPS
< I« 200 - 0 -à"-- Peripheral
100 - **å '--*à"-.#>«=^===^-å
QI J 1 | | | | | |
0 5 10 15 20 25 30 35
Time (min)
Fig. 2. Results of bilateral petrosal sinus sampling with corticotropin-releasing hormone (CRH) administration.
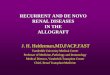
Fig. 3. Brain magnetic resonance imaging (MRI) one week aftertranscranial surgery.
12Internal Medicine Vol. 34, No. 1 (January 1995)

Cushing's Disease with Nephrotic Syndrome
3). Histological examination revealed chromophobeadenoma.Although the plasma ACTHlevel returned to the normal range(41 pg/ml) 3 days after surgery, it gradually increased onemonth later and enlargement in tumor size was revealed by
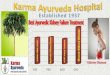
Fig. 4. Lightmicroscopy. Markedmesangialexpansionis visible, mainlydue to matrix enlargement with a lesser degree of endocapillary cellularproliferation (x250).
brain MRI. The patient was referred to another hospital, wherestereotactic radiosurgery with a gammaknife was performed.
Renal biopsy was performed to reevaluate histologicalchanges in the kidney 2 months after transcranial hypo-physectomy. Light microscopic examination revealed markedmesangial expansion, mainly due to matrix enlargement with alesser degree of endocapillary cellular proliferation (Fig. 4),suggesting a rather advanced stage of MPGN.These histologi-cal findings, however, are not specific for idiopathic MPGN,and can be associated with other diseases such as diabetesmellitus, amyloidosis, cryoimmunoglobulinemia or immuno-tactoid glomerulonephritis (5-7). The diagnosis of diabeticnephropathy was unlikely because of normal glucose toleranceto 75 g oral glucose challenge and a negative history of diabetes.Amyloidosis was excluded by negative Congo red stain, andcirculating cryoimmunoglobulins were not detected in thispatient. For further exploration, electron microscopic examina-tion was performed. As shown in Fig. 5, there was a large andamorphous deposit under the epithelium, but no coarse fibrils inthe glomerular mesangia or capillary walls, distinctive ultra-structural features of immunotactoid glomerulopathy, weredetected (6, 7). Because of these histopathological findings, thediagnosis was idiopathic MPGNwith atypical histological
Fig. 5. Electron microscopy.. A large and amorphous deposit is visible under the epithelium; no coarse fibrils in glomerular mesangia or in capillarywalls are found (x10,000).
Internal Medicine Vol. 34, No. 1 (January 1995) 13

Tatsumi et al
lesions, and combination therapy was initiated using cyclo-phosphamide, dipyridamole, warfarin and angiotensin convert-ing enzyme inhibitor. After l O months, the treatment showed nobeneficial effect on the proteinuria.
Discussion
This case appears to be the first report of Cushing's diseaseassociated with nephrotic syndrome. Because proteinuria wasfirst pointed out 6 years before the onset of the first episode ofCushing's disease, the renal lesion seemed to have precededpituitary adenoma in the present case. After the transsphenoidalsurgery in 1986, the patient had regularly visited our hospitaluntil the end of 1 988, and no progression in proteinuria had beendetected during this period. Therefore, it seems unlikely thatcessation of a rather short-term supplementation with hydro-cortisone may trigger the emergence of the nephrotic syn-drome. Light microscopic examination done in our hospital
revealed that matrix enlargement was more distinct, butendocapillary hypercellularity was much less compared to thebiopsy specimens of 1989. Although electron microscopicexamination was not performed previously in this patient, thepresent findings from light and electron microscopic examina-tions suggested that glomerular lesions had progressed to arather advanced stage ofMPGN.The pathogenesis ofMPGNispoorly understood but an immunecomplex-mediated mecha-nism is suggested on the basis of clinicopathologic associa-tions. At the time of diagnosis, a considerable percentage ofpatients show low concentrations of C3 and CH50. Duringfollow-up observations, however, serum complement levelsmay vary considerably, remaining low in most patients but alsonormalizing as in the present case. In previous reports in whichfocal glomerulosclerosis was associated with functional adre-nal adenoma ( 1 ) or ectopic ACTHsecreting pheochromocytoma
(2), it was suggested that co-existing hypertension due tohypersecretion of cortisol or catecholamines had a deleteriouseffect on the renal lesion, since the nephrotic syndrome wasmarkedly ameliorated after antihypertensive treatment ( 1 ) orsurgical resection of the tumor mass (2). In the present case,however, there was no hypertension and the nephrotic syn-drome was caused by MPGN,for which glucocorticoid isconsidered to be useful in combination drug therapy (5). Thus,the possibility is slight that hypercortisolemia due to the recur-rence of functional pituitary adenomahas any deleterious
effects on the course of MPGN.In the present case, serum totalcortisol levels were within the normal range in spite of elevatedplasma ACTHlevels and the presence of clinical features ofCushing's disease. This is probably attributed to urinary loss ofcortisol binding globulin due to the nephrotic syndrome (8).Transsphenoidal pituitary adenomectomywas performed
on this patient when Cushing ' s disease was first diagnosed. Thissurgery has been considered the procedure of choice in treatingCushing's disease, with remission rates ranging from 74%to
84% (9-ll). In the present case, this procedure brought anormalization of the endocrinological findings for about 5
years. According to a recent report by Tindall et al, the recur-
rence rate after selective adenomectomyseems slightly highercompared with other operative procedures such as subtotal ortotal hypophysectomy (12). It is of interest to note that therecurrence of pituitary macroadenoma occurred within 1 yearof cessation of steroid treatment for the nephrotic syndrome inthe present case. Twocases ofTSH-secreting pituitary adenomawere reported in the literature in which relatively rapid growthof the adenomamight have been induced by normalization ofserum T3 and T4 (13). Thus, in a similar way, the release ofnegative feedback after cessation of steroid therapy mightaccelerate the growth of pituitary adenoma and contribute to therecurrence.
Since transcranial surgery of the recurrent pituitary adenomafailed to induce a remission, gammaknife therapy was used forthis patient. This modality of stereotactic radiosurgery has beenused especially for treating arterio-venous malformations withconsiderably successful outcomes (14). Although there is notenough data available to predict the effect of gammaknifetherapy on pituitary adenoma, the present patient has shown nosigns of aggravation in plasma ACTHlevels or in tumor size at12 months after receiving the therapy.
References
1) Hiraiwa Y, Kusunoki N, Araki I, et al. A case report ofCushing syndromeassociated with nephrotic syndrome. Nippon Naika Gakkai Zasshi 77:1099, 1988 (in Japanese).
2) Chan R, Michelis MF. Pheochromocytoma and the ectopic corticotropinsyndrome in association with focal segmental glomerulosclerosis and thenephrotic syndrome. AmJ Kidney Dis 19: 289, 1992.
3) Old field EH, Doppman JL, Nieman LK, et al. Petrosal sinus samplingwith and without corticotropin-releasing hormone for the differentialdiagnosis of Cushing's syndrome. N Engl J Med 325: 897, 1991.
4) Carsin M, Carsin NB, Rolland Y, et al. Contribution of MRI to thediagnosis of ACTH-secreting pituitary adenomas. Exploration of 9 pa-tients with Cushing's disease. J Neuroradiol 17: 255, 1990.
5) Donadio JV Jr. Membranoproliferative glomerulonephritis. in: Diseasesin the Kidney, Schrier RW, Gottschalk CW, Eds. Little, Brown andCompany, Boston, 1993, p.1815.
6) Esparza AR, Chazan JA, Nayak RN, Cavallo T. Fibrillary (immunotactoid)glomerulopathy. AmJ Surg Pathol 15: 632, 1991.
7) Alpers CE. Immunotactoid (microtubular) glomerulopathy. AmJ KidneyDis 19: 185, 1992.
8) Doe RP. Excretion of corticosteroid-binding globulin in man. J ClinEndocr 24: 1029, 1964.
9) Hardy J. Cushing's disease: 50 years later. Presidential address: XVIICanadian Congress of Neurological Sciences. Can J Neurol Sci 9: 375,
1982.
10) Mampalam TJ, Tyrrel JB, Wikson CB. Transsphenoidal microsurgery forCushing disease. A report of 216 cases. Ann Intern Med 109: 487, 1988.
1 1) Tagliaferri M, Berselli ME, Loli P. Transsphenoidal microsurgery forCushing's disease. Acta Endocrinol 113: 5, 1986.
12) Tindall GT, Herring CJ, Clark RV, et al. Cushing's disease: Results oftranssphenoidal microsurgery with emphasis on surgical failures. J
Neurosurg 72: 363, 1990.13) Higuchi M, Mori S, Arita N, et al. Two cases ofTSH-secreting pituitary
adenoma; Endocrinological, diagnostic and therapeutic approach to thedisease. Neurological Surgery 19: 883, 1991 (in Japanese).
14) Luxton G, Petrovich Z, Jozsef G, Nedzi LA, Apuzzo MLJ. Stereotacticradiosurgery: Principles and comparison of treatment methods. Neuro-surgery 32: 241, 1993.
14 Internal Medicine Vol. 34, No. 1 (January 1995)