Embed Size (px)
Citation preview

Vol. 25, No. 8JOURNAL OF CLINICAL MICROBIOLOGY, Aug, 1987, p. 1421-14230095-1137/87/081421-03$02.00/0Copyright © 1987, American Society for Microbiology
Recovery of Blastomyces dermatitidis from Blood of a Patient withDisseminated Blastomycosis
CORA E. MUSIAL,1 WALTER R. WILSON,2 INA R. SINKELDAM,' AND GLENN D. ROBERTS'*Section of Clinical Microbiology, Department of Laboratory Medicine,l and Division of Infectious Diseases,2
Mayo Clinic and Mayo Foundation, Rochester, Minnesota 55905
Received 20 January 1987/Accepted 5 May 1987
This report describes the first well-documented reported case of the recovery of Blastomyces dermatitidis fromthe blood of a patient with disseminated blastomycosis. The isolate was recovered by using a lysis-centrifugationmethod and inhibitory mold agar after 6 days of incubation at 30°C. One of six blood samples collected yieldeda positive culture.
Blastomyces dermatitidis, a dimorphic fungus, causesblastomycosis, a systemic pyogranulomatous disease. Pri-mary infection is acquired through the lungs and produces anacute self-limiting disease or pulmonary disease usuallyfollowed by secondary hematogenous dissemination to theskin, skeletal, genitourinary, and central nervous systems(3). The organism has been recovered from numerous clini-cal specimen sources, including respiratory secretions, skinlesions, bone, urine, cerebrospinal fluid, and other tissues.Despite hematogenous dissemination of the organism, therecovery of B. dermatitidis from blood has not been welldocumented. This manuscript presents a detailed descriptionof a case of blastomycosis in which hematogenous dissem-ination led to a substantial recovery of B. dermatitidis fromblood.
CASE REPORT
A 75-year-old farm wife from Iowa experienced an acuteepisode of pain in the left lateral melleolus and great toeshortly after falling in her garden. Her local physician madea diagnosis of probable gout, and she was treated withindomethacin. Subsequently, she developed inflammationand swelling of the left foot; a diagnosis of cellulitis wasmade, and treatment with erythromycin was begun withoutimprovement. She later developed lymphangitis of the leftfoot and was admitted to a local hospital, where treatmentwith cefazolin and prednisone was administered. She im-proved but continued to have pain in the left foot on weightbearing and was noted to have a fourth metatarsophalangealfracture. She was discharged and treated on an outpatientbasis with cephalexin and prednisone, but during the next 48h a generalized pustular eruption developed in conjunctionwith anorexia, fever, chills, a nonproductive cough, andshortness of breath. She was readmitted to the local hospital2 days after her earlier discharge. Bacterial blood cultureswere negative, and the leukocyte count was 1.6 x 1010/liter.She was treated with chloramphenicol and transferred to theMayo Clinic 4 days later for further evaluation of her illness.Upon admission to the Mayo Clinic, she appeared ill and
slightly confused but conversational and had a constantcough. Vital signs included the following: temperature,38.3°C; pulse, 110/min; respiratory rate, 30/min; and bloodpressure, 160/82 mm Hg. A generalized pustular eruption ofthe face and extremities with relative sparing of the trunk
* Corresponding author.
and scalp was present (Fig. 1). The palms and soles haddiscrete 1- to 4-mm pustules (some were grouped) witherythematous bases, and many residual crusted papuleswere present. There were no discrete vesicles. She had mild
FIG. 1. Generalized pustular eruption of the knee of a patientwith disseminated blastomycosis showing some pustules witherythematous bases.
1421
on June 5, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
1422 MUSIAL ET AL.
pulmonary infiltrates. She was intubated, and an open-lungbiopsy was performed on the right middle lobe 4 days after
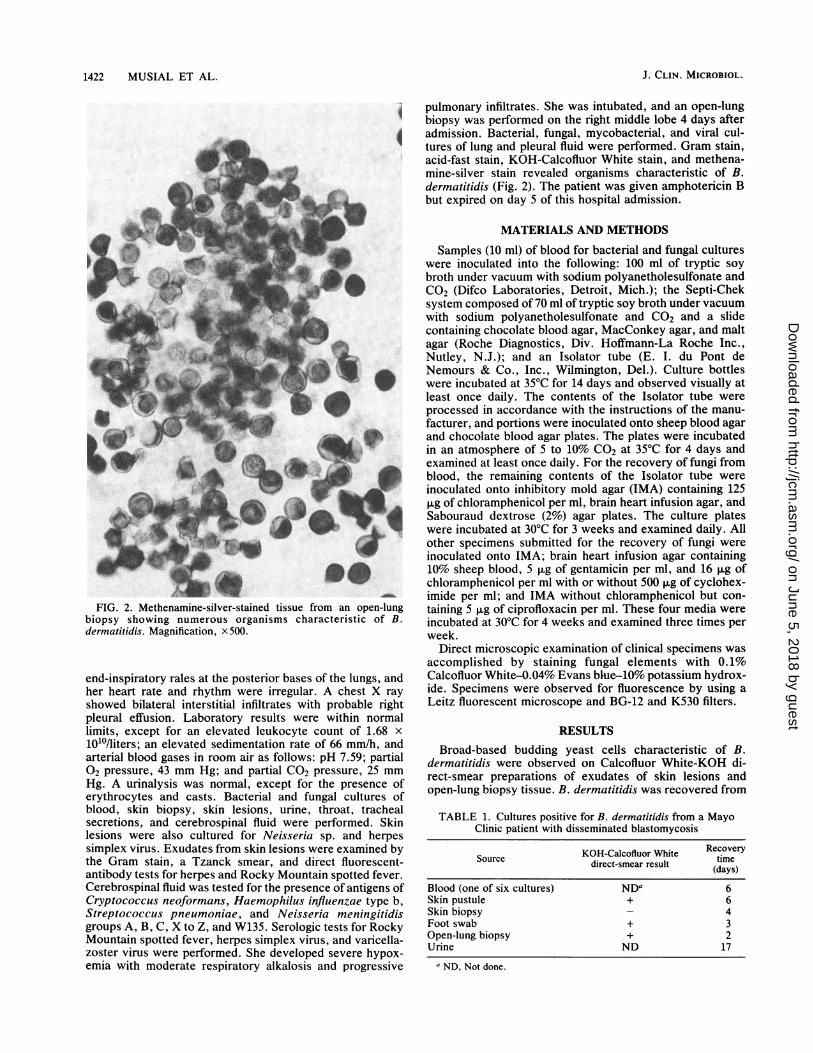
4 admission. Bacterial, fungal, mycobacterial, and viral cul-tures of lung and pleural fluid were performed. Gram stain,acid-fast stain, KOH-Calcofluor White stain, and methena-mine-silver stain revealed organisms characteristic of B.dermatitidis (Fig. 2). The patient was given amphotericin Bbut expired on day 5 of this hospital admission.
MATERIALS AND METHODS
._.
FIG. 2. Methenamine-silver-stained tissue from an open-lungbiopsy showing numerous organisms characteristic of B.dermatitidis. Magnification, x500.
end-inspiratory rales at the posterior bases of the lungs, andher heart rate and rhythm were irregular. A chest X rayshowed bilateral interstitial infiltrates with probable rightpleural effusion. Laboratory results were within normallimits, except for an elevated leukocyte count of 1.68 x
101'/liters; an elevated sedimentation rate of 66 mm/h, andarterial blood gases in room air as follows: pH 7.59; partial02 pressure, 43 mm Hg; and partial C02 pressure, 25 mmHg. A urinalysis was normal, except for the presence oferythrocytes and casts. Bacterial and fungal cultures ofblood, skin biopsy, skin lesions, urine, throat, trachealsecretions, and cerebrospinal fluid were performed. Skinlesions were also cultured for Neisseria sp. and herpessimplex virus. Exudates from skin lesions were examined bythe Gram stain, a Tzanck smear, and direct fluorescent-antibody tests for herpes and Rocky Mountain spotted fever.
Cerebrospinal fluid was tested for the presence of antigens ofCryptococcus neoformans, Haemophilus influenza type b,Streptococcus pneumoniae, and Neisseria meningitidisgroups A, B, C, X to Z, and W135. Serologic tests for RockyMountain spotted fever, herpes simplex virus, and varicella-zoster virus were performed. She developed severe hypox-emia with moderate respiratory alkalosis and progressive
Samples (10 ml) of blood for bacterial and fungal cultureswere inoculated into the following: 100 ml of tryptic soybroth under vacuum with sodium polyanetholesulfonate andC02 (Difco Laboratories, Detroit, Mich.); the Septi-Cheksystem composed of 70 ml of tryptic soy broth under vacuumwith sodium polyanetholesulfonate and C02 and a slidecontaining chocolate blood agar, MacConkey agar, and maltagar (Roche Diagnostics, Div. Hoffmann-La Roche Inc.,Nutley, N.J.); and an Isolator tube (E. I. du Pont deNemours & Co., Inc., Wilmington, Del.). Culture bottleswere incubated at 35°C for 14 days and observed visually atleast once daily. The contents of the Isolator tube were
processed in accordance with the instructions of the manu-
facturer, and portions were inoculated onto sheep blood agarand chocolate blood agar plates. The plates were incubatedin an atmosphere of 5 to 10% C02 at 35°C for 4 days andexamined at least once daily. For the recovery of fungi fromblood, the remaining contents of the Isolator tube were
inoculated onto inhibitory mold agar (IMA) containing 125,ug of chloramphenicol per ml, brain heart infusion agar, andSabouraud dextrose (2%) agar plates. The culture plateswere incubated at 30°C for 3 weeks and examined daily. Allother specimens submitted for the recovery of fungi were
inoculated onto IMA; brain heart infusion agar containing10% sheep blood, 5 ,ug of gentamicin per ml, and 16 ,ug ofchloramphenicol per ml with or without 500 ,ug of cyclohex-imide per ml; and IMA without chloramphenicol but con-taining 5 ,ug of ciprofloxacin per ml. These four media were
incubated at 30°C for 4 weeks and examined three times perweek.
Direct microscopic examination of clinical specimens was
accomplished by staining fungal elements with 0.1%Calcofluor White-0.04% Evans blue-10% potassium hydrox-ide. Specimens were observed for fluorescence by using aLeitz fluorescent microscope and BG-12 and K530 filters.
RESULTSBroad-based budding yeast cells characteristic of B.
dermatitidis were observed on Calcofluor White-KOH di-rect-smear preparations of exudates of skin lesions andopen-lung biopsy tissue. B. dermatitidis was recovered from
TABLE 1. Cultures positive for B. dermatitidis from a MayoClinic patient with disseminated blastomycosis
KOH-Calcofluor White RecoverySource direct-smear result tisme
Blood (one of six cultures) NDa 6Skin pustule + 6Skin biopsy 4Foot swab + 3Open-lung biopsy + 2Urine ND 17
a ND, Not done.
J. CLIN. MICROBIOL.
on June 5, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

RECOVERY OF B. DERMATITIDIS FROM BLOOD 1423
TABLE 2. Distribution of 167 isolates of B. dermatitidisrecovered from clinical specimens from 1976 to 1986
Specimen No. of positivecultures
Sputum .......................................... 40Induced sputum.......................................... 30Gastric washings ......................................... 20Bronchial washings ..................................... . 16Lung.......................................... 15Urine .......................................... 5Skin .......................................... 5Ankle .......................................... 4Mediastinum .......................................... 3Foot .......................................... 3Ischium .......................................... 3Tibia.......................................... 3Hand .......................................... 3Prostate.......................................... 2Wrist .......................................... 2Back .......................................... 2Thigh, knee .......................................... 2Face .......................................... 1Lip .......................................... 1Throat .......................................... 1Shoulder .......................................... 1Blood .......................................... 1Chest .......................................... 1Groin .......................................... 1Scrotum .......................................... 1Leg .......................................... 1
one of six blood cultures, urine, skin lesions, skin biopsytissue, and open-lung biopsy tissue. A summary of culturespositive for B. dermatitidis and their recovery times ispresented in Table 1.Four separate blood samples were collected on the day of
admission to the Mayo Clinic, and two additional sampleswere collected on the following day. One of the first fourcultures became positive after 6 days of incubation. White,filamentous colonies were observed on IMA with chloram-phenicol only. The filamentous form was converted to thecharacteristic yeast form on cottonseed agar incubated at35°C after 19 days.
DISCUSSION
A search of the literature, including several review articles(2, 4-7; C. E. Musial, D. M. Ilstrup, and G. D. Roberts,Abstr. Annu. Meet. Am. Soc. Microbiol. 1986, F53, 1986),revealed that the recovery of B. dermatitidis from blood hasnot previously been reported. Possible explanations, amongothers, responsible for the failure of laboratories to detectthis organism in blood include the following: (i) small num-
bers of organisms present in blood during fungemia; (ài)inappropriate timing of the collection of samples, perhaps
related to transient fungemia; (iii) lack of a sensitive bloodculture system and/or culture media; and (iv) failure toperform blood cultures for patients with disseminated blas-tomycosis.While it cannot be documented why B. dermatitidis was
recovered from this patient, we feel it was related either tothe blood culture system and media used for recovery andperhaps the large numbers of organisms present during acuteinfection or to prior corticosteroid treatment. With the use ofthe lysis-centrifugation blood culture system (Isolator) forthe recovery of bacteria and fungi from blood, fungemia hasbeen detected more rapidly and with a higher rate of sensi-tivity than with the use of other systems (1). Other filamen-tous fungi, including Histoplasma capsulatum andCoccidioides immitis, have been recovered from blood withthe lysis-centrifugation system. It appears that the combina-tion of media used with the Isolator system is necessary forthe optimal detection of fungemia (Musial et al., Abstr.Annu. Meet. Am. Soc. Microbiol. 1986). This report de-scribes the recovery of B. dermatitidis from blood with thisculture system.During the 10-year period from 1976 to 1986, 167 isolates
of B. dermatitidis were recovered from 56 patients by theMayo Clinic Clinical Mycology Laboratory. The specimendistribution is shown in Table 2 and includes this reportedsource.
In summary, the present report describes the first well-documented recovery of B. dermatitidis from the blood of apatient with disseminated blastomycosis. The isolate wasrecovered from an IMA plate 6 days after the blood had beenprocessed with the Isolator system. Because of the highersensitivity of the Isolator system for the detection offungemia and its increasing use, it is likely that additionalisolates of the dimorphic fungi will be detected in the bloodof patients with disseminated fungal disease.
LITERATURE CITED1. Bille, J., L. Stockman, G. D. Roberts, C. D. Horstmeier, and
D. M. Ilstrup. 1983. Evaluation of a lysis-centrifugation systemfor recovery of yeasts and filamentous fungi from blood. J. Clin.Microbiol. 18:469-471.
2. Busey, J. F. 1964. Blastomycosis. I. A review of 198 collectedcases in Veterans Administration hospitals. Am. Rev. Respir.Dis. 89:659-672.
3. Chapman, S. W. 1985. Blastomyces dermatitidis, p. 1477-1485.In G. L. Mandell, R. G. Douglas, Jr., and J. E. Bennett (ed.),Principles and practice of infectious diseases. John Wiley &Sons, Inc., New York.
4. Cockerill, F. R., G. D. Roberts, J. E. Rosenblatt, J. P. Utz, andD. C. Utz. 1984. Epidemic of pulmonary blastomycosis(Namekagon fever) in Wisconsin canoeists. Chest 86:688-692.
5. Drake, R. G., Jr. 1985. North American blastomycosis, a review.J. Ky. Med. Assoc. 83:77-82.
6. Sarosi, G. A., and S. F. Davies. 1979. Blastomycosis. Am. Rev.Respir. Dis. 120:911-942.
7. Schwarz, J., and K. Salfelder. 1977. Blastomycosis. A review of152 cases. Curr. Top. Pathol. 65:166-200.
VOL. 25, 1987
on June 5, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from












![PUSTULAR PSORIASIS RESPONDING TO PROBIOTICS – A NEW … 4/9... · 2012-11-22 · With anecdotal reference [4] of probiotics helping ... PUSTULAR PSORIASIS RESPONDING TO PROBIOTICS](https://img.pdfslide.us/doc/110x75/5e63831b9667476f8503b6bc/pustular-psoriasis-responding-to-probiotics-a-a-new-49-2012-11-22-with.jpg)
















