Embed Size (px)
Citation preview

Develop. Med. Child Neurol. 1970, 12, 565-571
Recovery of Motor and Intellectual Function in Children Sustaining Severe Head Injuries
Joyce D. Brink Alice L. Garrett William R. Hale James Woo-Sam Vernon L. Nickel
IN the United States there are an estimated one million children who sustain head injuries each year (Young 1969). In two large series of consecutive cases hospitalized with head trauma, the incidence of perma- nent neurological deficits is reported as 0.5 per cent and 5.9 per cent (Rickham 1961). When the child is comatose for over 24 hours, the incidence of these deficits rises sharply (Hendrick et al. 1962). Only a few articles in the pediatric literature have discussed the long-term residual effects of traumatic brain injuries (Robertson and Pollard 1955, Sedzimir 1959, Hjern and Nylander 1962, Ommaya 1966). To our knowledge, no previous study has dealt exclusively with a large number of children who have survived after a prolonged period of coma.
This paper describes 52 patients who sustained head injuries and were comatose for more than one week. Forty-six of these children were evaluated one to seven years after injury for assessment of motor function, degree of independence in walking and self-care, speech function, intelligence, school placement, and changes in personality and behavior.
Material and Methods During the years 1959 to 1966, 52
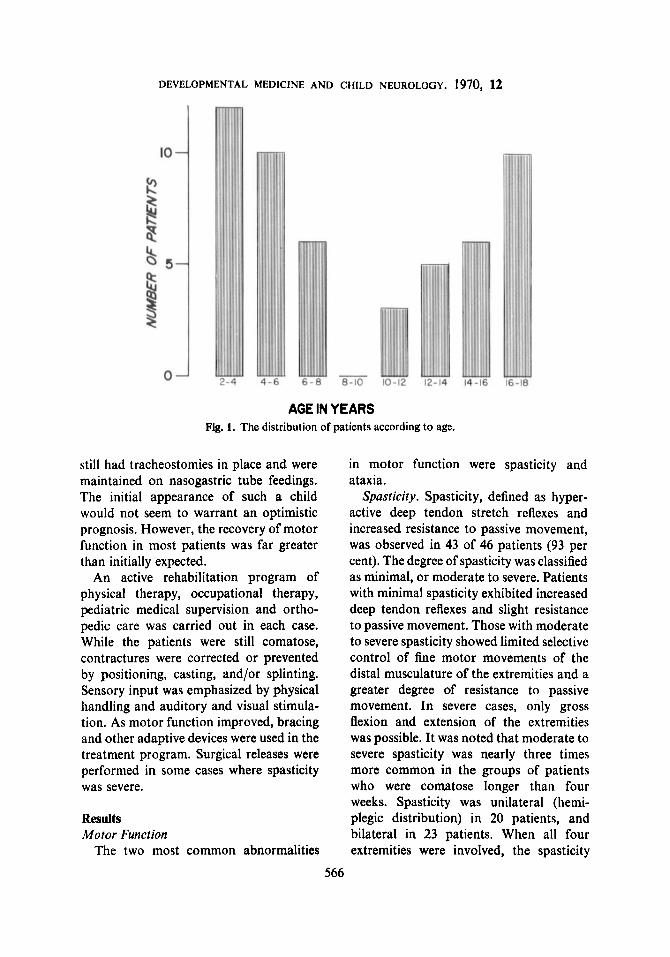
patients between 2 and 18 years (median age 8 years) were admitted to Rancho Los Amigos Hospital for rehabilitation follow- ing severe head trauma. Figure 1 shows the distribution of patients according to age: 28 were under the age of 8; 24 were over the age of 8. Males outnumbered females 39 to 13. All but 10 patients were injured in accidents involving motor vehicles.
The severity of initial brain injury is indicated by the length ofcoma, a minimum of one week in all cases. Seven weeks was the average duration of coma for patients who regained consciousness, with a median of four weeks. Three patients are still comatose after more than a year. There were three late deaths in our series; one 9 months, one 2 years, and one 4 i years following injury. Thirty-eight patients were decerebrate or decorticate initially; 21 had skull fractures; 28 underwent emergency craniotomies.
At the time of transfer from acute neurosurgical wards after their medical condition was stable, the majority of patients were not fully responsive. Many
_____ Department of Pediatrics, Rancho Los Amigos Hospital, Downey, California 90242
565
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1970, 12
AGE IN YEARS Fig. 1. The distribution of patients according to age.
still had tracheostomies in place and were maintained on nasogastric tube feedings. The initial appearance of such a child would not seem to warrant an optimistic prognosis. However, the recovery of motor function in most patients was far greater than initially expected.
An active rehabilitation program of physical therapy, occupational therapy, pediatric medical supervision and ortho- pedic care was carried out in each case. While the patients were still comatose, contractures were corrected or prevented by positioning, casting, and/or splinting. Sensory input was emphasized by physical handling and auditory and visual stimula- tion. As motor function improved, bracing and other adaptive devices were used in the treatment program. Surgical releases were performed in some cases where spasticity was severe.
Results Motor Function
The two most common abnormalities
in motor function were spasticity and ataxia.
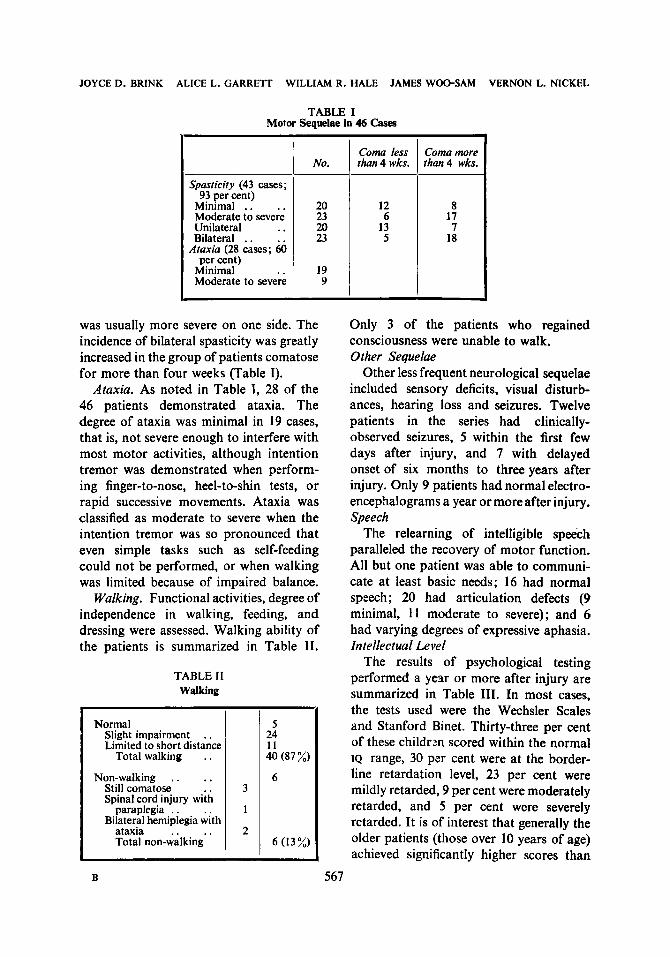
Spasticity. Spasticity, defined as hyper- active deep tendon stretch reflexes and increased resistance to passive movement, was observed in 43 of 46 patients (93 per cent). The degree of spasticity was classified as minimal, or moderate to severe. Patients with minimal spasticity exhibited increased deep tendon reflexes and slight resistance to passive movement. Those with moderate to severe spasticity showed limited selective control of fine motor movements of the distal musculature of the extremities and a greater degree of resistance to passive movement. In severe cases, only gross flexion and extension of the extremities was possible. It was noted that moderate to severe spasticity was nearly three times more common in the groups of patients who were comatose longer than four weeks. Spasticity was unilateral (hemi- plegic distribution) in 20 patients, and bilateral in 23 patients. When all four extremities were involved, the spasticity
566
JOYCE D. BRINK ALICE L. GARRETT WILLIAM R . HALE JAMES WOO-SAM VERNON L. NICKEL
TABLE I Motor Sequelae in 46 Casw
Spasticity (43 cases;
Minimal . . . . Moderate to severe Unilateral .. Bilateral . .
Ataxia (28 cases; 60 per cent)
Minimal Moderate to severe
93 per cent)
No.
20 23 20 23
19 9
was usually more severe on one side. The incidence of bilateral spasticity was greatly increased in the group of patients comatose for more than four weeks (Table I).
Ataxia. As noted in Table I, 28 of the 46 patients demonstrated ataxia. The degree of ataxia was minimal in 19 cases, that is, not severe enough to interfere with most motor activities, although intention tremor was demonstrated when perform- ing finger-to-nose, heel-to-shin tests, or rapid successive movements. Ataxia was classified as moderate to severe when the intention tremor was so pronounced that even simple tasks such as self-feeding could not be performed, or when walking was limited because of impaired balance.
Walking. Functional activities, degree of independence in walking, feeding, and dressing were assessed. Walking ability of the patients is summarized in Table 11.
TABLE I1 Walking
Normal Slight impairment . . Limited to short distance
Total walking . . Non-walking . . . .
Still comatose .. Spinal cord injury with
paraplegia . . Bilateral hemiplegia with
ataxia . . .. Total non-walking
B
Coma less than 4 wks.
12 6
13 5
Coma more than4 wks.
8 17 7
18
Only 3 of the patients who regained consciousness were unable to walk. Other Sequelae
Other less frequent neurological sequelae included sensory deficits, visual disturb- ances, hearing loss and seizures. Twelve patients in the series had clinically- observed seizures, 5 within the first few days after injury, and 7 with delayed onset of six months to three years after injury. Only 9 patients had normal electro- encephalograms a year or more after injury. Speech
The relearning of intelligible speech paralleled the recovery of motor function. All but one patient was able to communi- cate at least basic needs; 16 had normal speech; 20 had articulation defects (9 minimal, 11 moderate to severe); and 6 had varying degrees of expressive aphasia. Intellectual Level
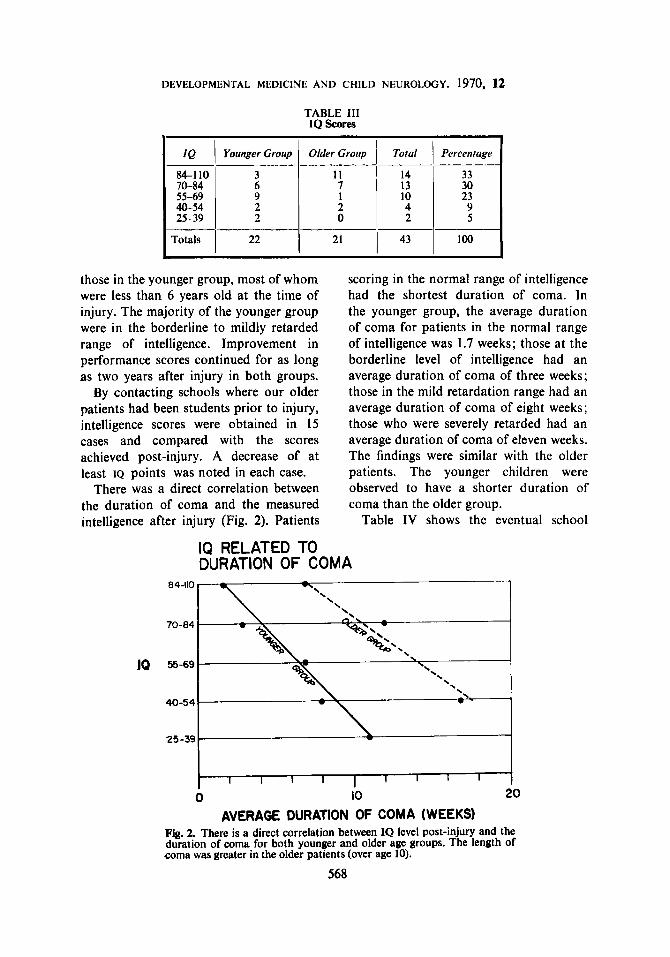
The results of psychological testing performed a year or more after injury are summarized in Table 111. In most cases, the tests used were the Wechsler Scales and Stanford Binet. Thirty-three per cent of these childrm scored within the normal IQ range, 30 per cent were at the border- line retardation level, 23 per cent were mildly retarded, 9 per cent were moderately retarded, and 5 per cent were severely retarded. It is of interest that generally the older patients (those over 10 years of age) achieved significantly higher scores than
567
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1970, 12
TABLE 111 IQ Scores
70-84 55-69 10 23 40-54 2 2 9 25-39 2 0
I Totals I 22 1 21 I 43 I 100
those in the younger group, most of whom were less than 6 years old at the time of injury. The majority of the younger group were in the borderline to mildly retarded range of intelligence. Improvement in performance scores continued for as long as two years after injury in both groups.
By contacting schools where our older patients had been students prior to injury, intelligence scores were obtained in 15 cases and compared with the scores achieved post-injury. A decrease of at least IQ points was noted in each case.
There was a direct correlation between the duration of coma and the measured intelligence after injury (Fig. 2). Patients
scoring in the normal range of intelligence had the shortest duration of coma. In the younger group, the average duration of coma for patients in the normal range of intelligence was 1.7 weeks; those at the borderline level of intelligence had an average duration of coma of three weeks; those in the mild retardation range had an average duration of coma of eight weeks; those who were severely retarded had an average duration of coma of eleven weeks. The findings were similar with the older patients. The younger children were observed to have a shorter duration of coma than the older group.
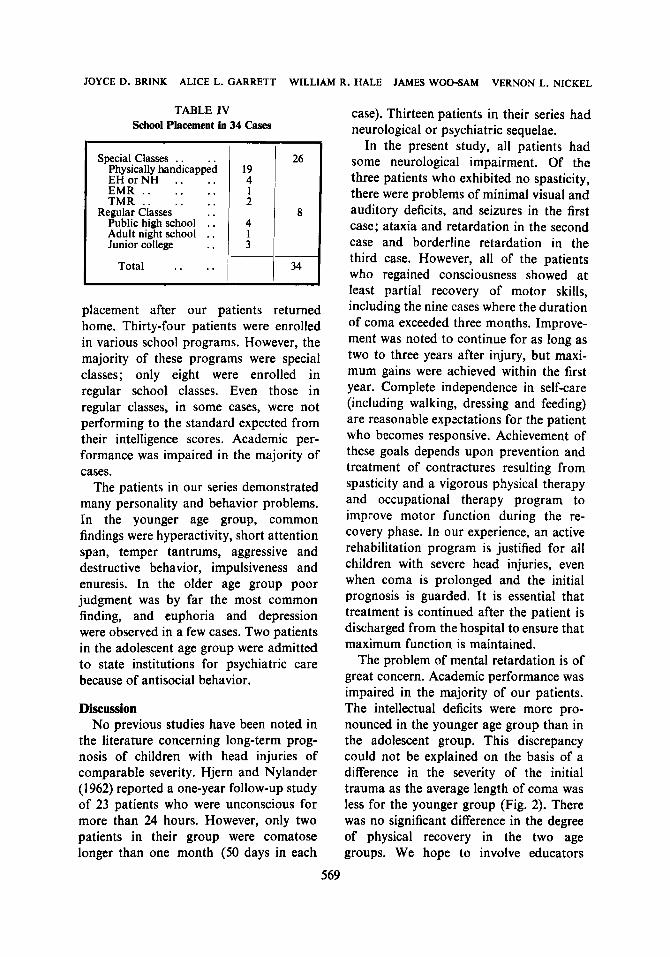
Table IV shows the eventual school
IQ RELATED TO DURATION OF COMA
0 10 20
AVERAGE DURATION OF COMA (WEEKS) Fig. 2. There is a direct correlation between IQ level post-injury and the duration of coma for both younger and older age groups. The length of coma was greater in the older patients (over age 10).
568
JOYCE D. BRINK ALICE L. GARRETT WILLIAM R. HALE JAMES WOO-SAM VERNON L. NICKEL
4 I
TABLE IV School Placement in 34 Cases
Special Classes . . Physically handicapped EHorNH .. .. EMR .. .. .. TMR .. .. ..
Regular Classes .. Public high school . . Adult night school . . Junior college . .
Total . . ..
placement after our patients returned home. Thirty-four patients were enrolled in various school programs. However, the majority of these programs were special classes; only eight were enrolled in regular school classes. Even those in regular classes, in some cases, were not performing to the standard expected from their intelligence scores. Academic per- formance was impaired in the majority of cases.
The patients in our series demonstrated many personality and behavior problems. In the younger age group, common findings were hyperactivity, short attention span, temper tantrums, aggressive and destructive behavior, impulsiveness and enuresis. In the older age group poor judgment was by far the most common finding, and euphoria and depression were observed in a few cases. Two patients in the adolescent age group were admitted to state institutions for psychiatric care because of antisocial behavior.
Discussion No previous studies have been noted in
the literature concerning long-term prog- nosis of children with head injuries of comparable severity. Hjern and Nylander (1962) reported a one-year follow-up study of 23 patients who were unconscious for more than 24 hours. However, only two patients in their group were comatose longer than one month (50 days in each
case). Thirteen patients in their series had neurological or psychiatric sequelae.
In the present study, all patients had some neurological impairment. Of the three patients who exhibited no spasticity, there were problems of minimal visual and auditory deficits, and seizures in the first case; ataxia and retardation in the second case and borderline retardation in the third case. However, all of the patients who regained consciousness showed a t least partial recovery of motor skills, including the nine cases where the duration of coma exceeded three months. Improve- ment was noted to continue for as long as two to three years after injury, but maxi- mum gains were achieved within the first year. Complete independence in self-care (including walking, dressing and feeding) are reasonable expxtations for the patient who becomes responsive. Achievement of these goals depends upon prevention and treatment of contractures resulting from spasticity and a vigorous physical therapy and occupational therapy program to improve motor function during the re- covery phase. In our experience, an active rehabilitation program is justified for all children with severe head injuries, even when coma is prolonged and the initial prognosis is guarded. I t is essential that treatment is continued after the patient is discharged from the hospital to ensure that maximum function is maintained.
The problem of mental retardation is of great concern. Academic performance was impaired in the majority of our patients. The intellectual deficits were more pro- nounced in the younger age group than in the adolescent group. This discrepancy could not be explained on the basis of a difference in the severity of the initial trauma as the average length of coma was less for the younger group (Fig. 2). There was no significant difference in the degree of physical recovery in the two age groups. We hope to involve educators
569
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1970, 12
more actively in the rehabilitation pro- injuries in their series were much less gram and follow-up of these patients so severe; only two children were unconscious that more attention can be given to the more than 24 hours. The aggressive, evaluation and management of the learn- impulsive, and sometimes destructive be- ing disabilities which are so common havior exhibited by our patients was very following head trauma. often more difficult for the families to
A study by Dillon and Leopold (1961) manage than the residual physical dis- discussed the personality and behaviour ability. In the adolescent group of patients, aberrations which occur as a result of head a common finding of poor judgment will injury. In their group of 50 cases, 47 limit vocational potential and thus the children showed psychological changes as achievement of financial independence in a result of trauma. In comparison with the adult life. group of patients in our study, the
SUMMARY Forty-six patients aged from 2 to 18 years were evaluated 1-7 years after sustaining
severe head trauma. The average duration of coma in this series was 7 weeks. Significant recovery of motor function was observed in the majority of cases. Indepen-
dence in ambulation and self-care were achieved by 87 per cent of these patients after completion of a comprehensive rehabilitation program which was continued throughout the recovery phase.
However, severe deficits were observed in the intellectual level measured by intelligence test scores. Children in the younger age group showed significantly greater impairment than the adolescents. The eventual degree of recovery of both motor function and intellec- tual ability were related to the duration of coma. In some cases, improvement in physical and psychological performance continued for as long as 3 years after injury.
RESUMB RCcupkration des fonctions motrice et intellectuelle
d’enfants ayant souflert de blessures graves de la fete 46 sujets lgCs de 2 B 18 ans ont CtC examints de un h sept ans apres un traumatisme
cranio-cbribral sCv6re. La durCe moyenne du coma post-traumatique ttait de sept semaines. Une rCcupCration significative de la fonction motrice a pu &re observ6e dans la majorit6
des cas. L‘indCpendance des deplacements et I’autonomie sociale a CtC rCaliste dans 87 des cas h la fin d’un programme de rCCducation adaptt, prolong6 tout au long de la ptriode de ricupiration.
Cependant, des dtficits intellectuels graves ont it6 observts griice h des tests d’intelligence. Les troubles Ctaient significativement plus s6vkes chez les enfants jeunes que chez les adolescents. L‘importance de la r6cupCration de la fonction motrice comme celle de I’effi- cience intellectuelle apparait lit% h la durCe du coma. Dans quelques cas, les progrbs physiques et psychologiques se sont prolongis jusqu’h trois ans a p r h I’accident.
ZUSAMMENFASSUNG Die Erholung der motorischen und geistigen Funktionen
bei Kindern nach schweren Schadelverletzungen 47 Patienten von 2 bis 18 Jahren wurden 1 bis 7 Jahre nach schweren Schadelverletzungen
beobachtet. Die durchschnittliche Dauer der BewuBtlosigkeit betrug in dieser Serie 7 Wochen.
570
JOYCE D. BRINK ALICE L. GARRETT WILLIAM R. HALE JAMES WOO-SAM VERNON L. NICKEL
Eine signifikante Erholung der motorischen Funktionen wurde in der Mehrzahl der Falle beobachtet. Nach Abschlu 0 eines umfassenden Rehabilitationsprogrammes, das auch wahrend der Erholungsphase weitergefuhrt wurde, konnten 87 % der Patienten ohne Hilfe gehen und fur sich selbst sorgen.
Schwere Mangel wurden allerdings in der intellektuellen Leistungskraft gefunden, die mit Intelligenztests gepruft wurde. Die jiingeren Kinder zeigten eine signifikant gro Bere Schadi- gung als die heranwachsenden Kinder. Die voraussichtliche Wiederherstellung der motori- schen Funktionen und der geistigen Fahigkeiten stand in Beziehung zu der Dauer der BewuDtlosigkeit. In manchen Fallen hielt die Besserung des physischen und psychologischen Zustandes bis zu drei Jahren nach dem Unfall an.
RESUMEN Recuperacibn de las funciones motora e intelectual en nirios con
traumas craneales graves Cuarenta y seis pacientes de 2 a 18 aiios fueron examinados de 1 a 7 aiios despuis de
haber sufrido un grave trauma craneal. La duracibn media del coma en estos casos fue de 7 semanas.
Se observo una recuperacibn significativa de la funcibn motora en la mayoria de 10s casos. Una independencia en la deambulacibn y en la capacidad de cuidarse de s l mismos se consiguib en el 87% despuis de completar un programa de rehabilitacibn que se continub durante toda la fase de recuperacibn.
Sin embargo se observaron graves deficits en el nivel intelectual medidos post-tests de inteligencia. Los niiios del grupo mhs joven demostraron una alteracibn significativamente mayor que 10s adolescentes. El eventual grado de recupsracibn de las funciones motora e intelectual estaba en relacibn con la duracibn del coma. En algunos casos la m?joria flsica y psicolbgica continub durante un period0 de 3 aiios despuis del trauma.
REFERENCES Dillon, H., Leopold, R. L. (1961) ‘Childrsn and the pxt-concussioi syndroms.’J. Amer. med. Ass., 175, 86. Hendrick, E. B. Harwood-Nash, D. C., Hudson, A. R. (1962) ‘Head injuries in children: a survey of 4,465
Hjern, B., Nylander, I. (1962) ‘Late prognosis of severe head injaries in childhood.’ Arch. Dis. Childh., 37,
Ommaya, A. K. (1966) ‘Trauma to the nervous system.’ Ann. roy. Colf. Surg. Engl., 39,317. Rickham, P. P. (1961) ‘Head injuries in childhood.’ Helv. chir. Actu., 28,560. Robertson, R. C., Pollard, C. (1955) ‘Decerebrate state in children and adolescents.’ J. Neurosurg., 12, 13. Sedzimir, C. B. (1959) Therapeutic hyp3thermia.h cases of head injury.’J. Nworurg., 16.497. Young, W. M. (1969) ‘Poverty, intelli.@m% and life in the inner city.’ Ment. Retard., 7, (2), 21.
consecutive cases at the Hospital far Sick Children, Toronto Canada.’ Clin. Ncurosurg., lI ,45.
113.
571





























