Embed Size (px)
Citation preview
79
mainly upon the rate of injection, and to a lesser extenton their position, and on their capacitance relative tothat of the main artery.
If the side-branches are collectively represented asone branch situated 55 cm. from the wrist (fig. 2), andthe flow-rate through the side-branches (Fb) is assumedto be at most 200 ml. per minute, the volume of fluid(V) which would have to be injected to reach the originof the vertebral artery at various rates of injection (Fs)may be calculated from the formula
(where Vi is the volume of the main arterial trunk fromwrist to side-branch and V2 is the volume fromside-branch to vertebral artery). The results were asfollows:
On the basis of the above assumptions it can be seenthat as little as 7 ml. would easily reach the vertebralartery at faster rates of injection.We have not been able to find any published reports
of cerebral damage complicating declotting of Scribnershunts. However, some workers 6 have observed theoccasional occurrence of transient cerebral symptomssuch as headaches, loss of consciousness, and con-vulsions. These episodes all occurred as a result of
declotting the arterial cannula of an upper-limb shunt.It is possible that most of these incidents were due tosmall cerebral emboli arising from the detached clot;the reversibility of the symptoms does not, of course,exclude such a possibility. However, cerebral embolismcannot be the only cause, for in some instances cerebralsymptoms followed the injection of only 1-2 ml. offluid. The possibility of cerebral arterial spasm wasconsidered, but its mechanism of production by theinjection of a small amount of fluid into the radialartery is difficult to explain and it has been suggestedthat an abnormally sensitive arterial system or theinadvertent use of very cold fluid might have beenresponsible.The clinical pictures of the two cases presented here
were ascribed to cerebral embolism, and this has beenconfirmed at necropsy in case 1. It is also the most
likely cause of the persistent hemianopia in case 2. Inboth cases the posterior part of the cerebral circulationwas affected, and this is presumably due to the clotreaching the vertebral artery from the subclavian trunk.The rarity of these incidents may be at least partly dueto the smaller percentage of patients requiring anupper-limb shunt, for no similar episodes have beenobserved with leg shunts.
In view of the potential risk and seriousness of theseincidents, we suggest that an attempt at de-clotting anarterial cannula should at first be made by aspiration ofthe clot or its dissolution with streptokinase. If thesemethods fail, an attempt at dislodging the thrombus bythe injection of isotonic saline solution may be justifi-able to save a vital shunt, but certain precautions mayhelp to diminish or abolish the risk of cerebralcomplications. The saline solution should be warmed
to body temperature, and injected firmly and slowly,using a 2 ml. syringe. Prior instillation of streptokinasesolution may help to detach the thrombus.We thank Prof. D. A. K. Black and Prof. H. Scarborough for
their permission to report their cases. Requests for reprintsshould be addressed to D. G., Stepping Hill Hospital, Stockport.
REFERENCES
1. Curtis, J. R., Eastwood, J. B., Smith, E. K. M., Storey, J. M.,Verroust, P. J., De Wardener, H. E., Wing, A. J., Wolfson, E. M.Q. Jl Med. 1969, 149, 49.
2. Hampers, C. L., Schupak, E. Long-term Hæmodialysis; p. 63.
London, 1967.3. Anderson, D. C., Martin, A. M., Clunie, G. J. A., Stewart, W. K.,
Robson, J. S. Proc. Eur. Dial. Transpl. Ass. 1967, 4, 55.4. Kjellstrand, C. M., Lindergard, B., Boijsen, E. ibid. p. 61.5. Shaw, A. B., Bazzard, F. J., Booth, E. M., Nilwarangkur, S.,
Berlyne, G. M. Q. Jl Med. 1965, 34, 237.6. Newsletter of the British Dialysis Group, August, 1968.
RECOVERY FROM NON-TRAUMATIC
LOCALISED GAS GANGRENE AND
CLOSTRIDIAL SEPTICÆMIA
ALAN T. MARTY * ROBERT M. FILLER
Children’s Hospital Medical Center, Boston, Massachusetts
Summary Non-traumatic clostridial infections
present either as septicæmia or as a
metastatic localised lesion. Almost all such infectionsoccur in elderly debilitated patients with ulceratinglesions in the gastrointestinal, biliary, or genitourinarytracts. In addition, most cases have developed indiabetics or in patients receiving cancer chemothera-peutic agents. All eight reported cases of non-traumaticclostridial myonecrosis have died of overwhelmingclostridial infection, usually within 24 hours. The casedescribed here was recognised early and treated
promptly by debridement of necrotic muscle and byhyperbaric oxygen. This 74-year-old man recoveredcompletely from the gas gangrene, though he died3 weeks later with widespread gram-negative sepsis.
Introduction
NON-TRAUMATIC clostridial infections deserve moreattention because such cases will end fatally if not
recognised early and treated rapidly. These infectionspresent as septicaemia, or more rarely as a localisedlesion in muscle. In the past 5 years fifteen patientswith gas gangrene were sent to this hospital because ofthe availability of a hyperbaric oxygen treatment
chamber. i The artiology of 1 of these cases of gasgangrene was non-traumatic; this was in an elderlydiabetic man with arteriosclerosis and an ulceratedadenocarcinoma of the colon. Because of early diagnosisand prompt therapy, this man’s gas gangrene was
completely eradicated, thus representing the first
successfully treated case of non-traumatic metastaticclostridial myonecrosis.
Case-reportThis 74-year-old white male first entered another
hospital because of pain and crepitation in the right forearm.The patient had been a well-controlled mild diabetic for8 years, and 3 years ago was treated for a myocardial infarct.2 weeks before admission, the patient noted persistent* Present address: Peter Bent Brigham Hospital, Boston, Massachusetts
02115, U.S.A.
80
heaviness of, and difficulty in moving, the right upperextremity. 2 days before admission he experienced a suddenshaking chill, and the next morning awoke with severe rightforearm pain. He denied recent injections or trauma to thearm; his diabetes was controlled with oral hypoglycxmicagents and he received no insulin. Because of progressiveerythema, crepitation, and swelling extending to the rightanterior chest wall, the forearm was incised; gas gangrenewas diagnosed. He was transferred to the hyperbaric unitat this centre.
Physical examination on admission to this hospitalrevealed a somnolent, critically ill, non-icteric, elderly man.His blood-pressure was 120/80 mm. Hg, pulse-rate 104 perminute, and temperature 101 °F (38’2°C). His right forearm,arm, shoulder, and anterior chest wall were tender, swollen,crepitant, and reddish brown. Necrotic muscle and a
foul watery exudate were noted at the site of the
previous incision. The right radial pulse was faint but allother peripheral pulses were normal. Abdominal examina-tion revealed a slightly tender, somewhat mobile, rightupper quadrant mass, and the stool contained occult blood.
Laboratory data on admission disclosed a hzematocrit of35%, and a white-blood-cell (w.B.c.) count of 12,000 perc.mm.; urine showed 4+ sugar, 2+ protein, and 20 w.B.c.per high-power field. Many gram-positive rods were seenon a gram stain of the wound exudate. Blood-urea-
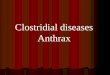
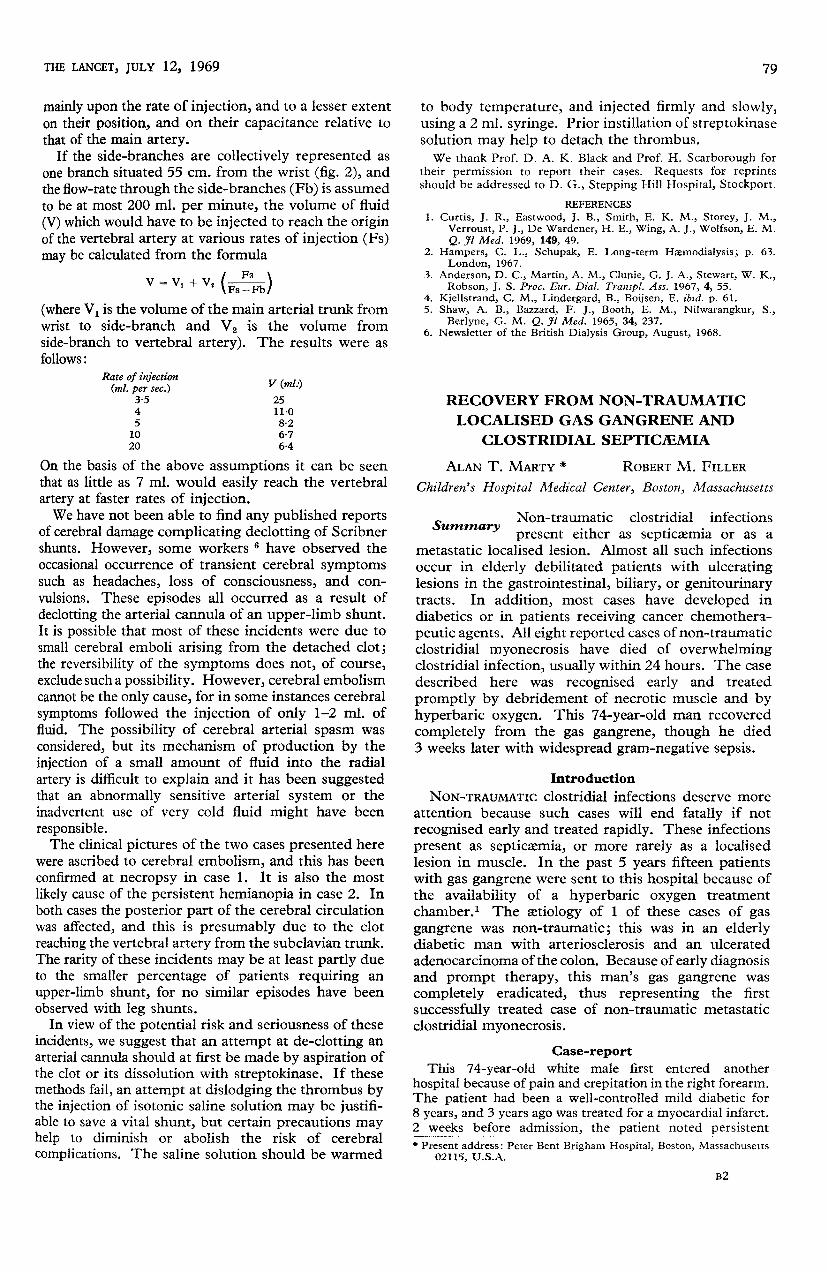
nitrogen 10 mg. per 110 ml.; electrolytes (meq. per litre)sodium 133, chloride 95, potassium 4-9, total carbon dioxide33. X-rays confirmed the presence of soft-tissue gas in theright forearm, arm, and shoulder (fig. 1).
Shortly after admission the patient was taken to theoperating-room in the hyperbaric chamber. Extensivedebridement of necrotic muscle was necessary, and this wasdone in conjunction with controlled ventilation with 100%oxygen at three atmospheres of pressure for 90 minutes. Theentire extensor compartment of the forearm was excised,and thrombosis of many small vessels was noted. 12 hourslater another 90-minute hyperbaric-oxygen treatment wasgiven, and re-examination of his wound at that time showedno residual myonecrosis. Clostridia perfrinnens and Proteus
Fig. 1-X-ray of right arm on admission demonstrating exten-sive intramuscular gas and oedema extending on to the chestwall-i.e., the typical X-ray signs of gas gangrene.
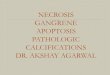
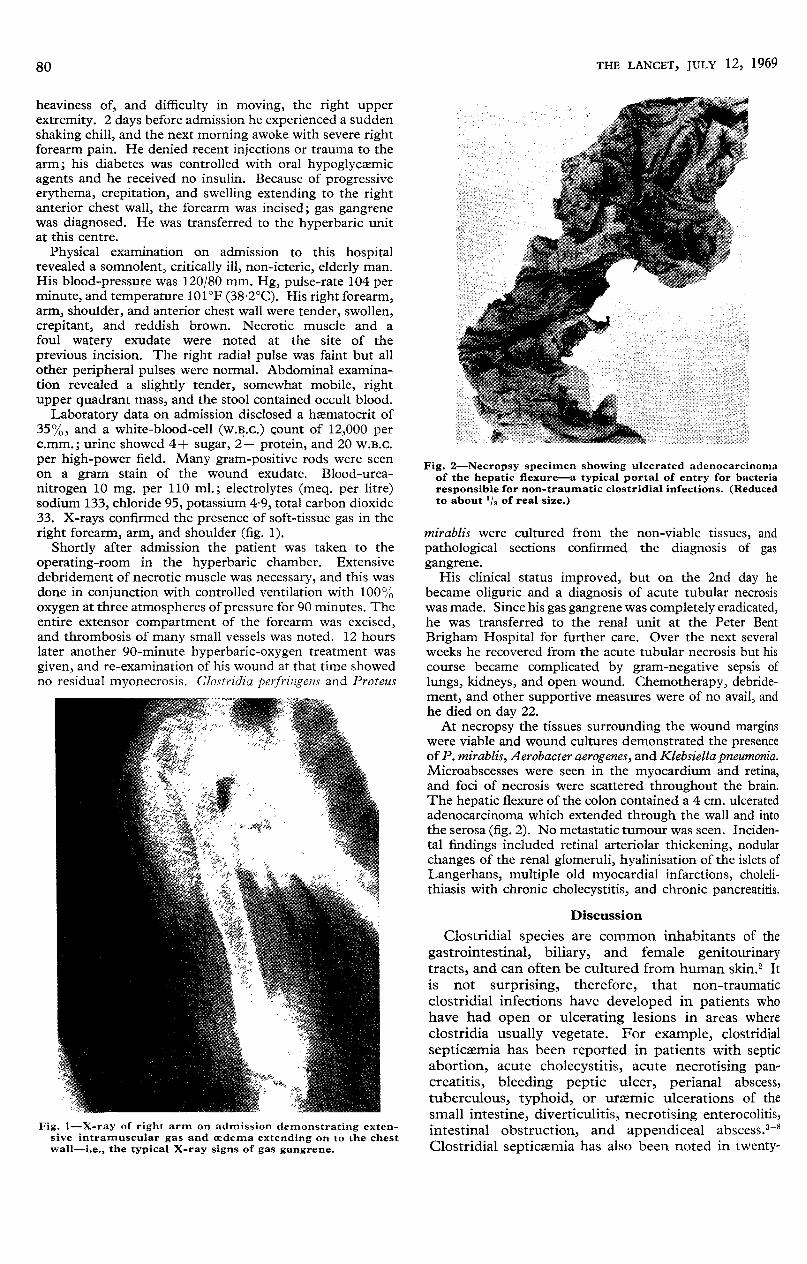
Fig. 2-Necropsy specimen showing ulcerated adenocarcinomaof the hepatic flexure-a typical portal of entry for bacteriaresponsible for non-traumatic clostridial infections. (Reducedto about ’/3 of real size.)
mirablis were cultured from the non-viable tissues, andpathological sections confirmed the diagnosis of gasgangrene.
His clinical status improved, but on the 2nd day hebecame oliguric and a diagnosis of acute tubular necrosiswas made. Since his gas gangrene was completely eradicated,he was transferred to the renal unit at the Peter Bent
Brigham Hospital for further care. Over the next severalweeks he recovered from the acute tubular necrosis but hiscourse became complicated by gram-negative sepsis of
lungs, kidneys, and open wound. Chemotherapy, debride-ment, and other supportive measures were of no avail, andhe died on day 22.At necropsy the tissues surrounding the wound margins
were viable and wound cultures demonstrated the presenceof P. mirablis, Aerobacter aerogenes, and Klebsiella pneumonia.Microabscesses were seen in the myocardium and retina,and foci of necrosis were scattered throughout the brain.The hepatic flexure of the colon contained a 4 cm. ulceratedadenocarcinoma which extended through the wall and intothe serosa (fig. 2). No metastatic tumour was seen. Inciden-tal findings included retinal arteriolar thickening, nodularchanges of the renal glomeruli, hyalinisation of the islets ofLangerhans, multiple old myocardial infarctions, choleli-thiasis with chronic cholecystitis, and chronic pancreatitis.
Discussion
Clostridial species are common inhabitants of thegastrointestinal, biliary, and female genitourinarytracts, and can often be cultured from human skin.2 Itis not surprising, therefore, that non-traumaticclostridial infections have developed in patients whohave had open or ulcerating lesions in areas whereclostridia usually vegetate. For example, clostridialsepticxmia has been reported in patients with septicabortion, acute cholecystitis, acute necrotising pan-creatitis, bleeding peptic ulcer, perianal abscess,tuberculous, typhoid, or uraemic ulcerations of thesmall intestine, diverticulitis, necrotising enterocolitis,intestinal obstruction, and appendiceal abscess.3-8Clostridial septicaemia has also been noted in twenty-

81
one of over four thousand necropsy records of patientsdying with cancer, most of whom had ulceratinglesions of the gastrointestinal tract.9 9
Of the eight reported cases of non-traumatic clos-tridial gas gangrene localised to an extremity, one hadacute cholecystitis and necrotising pancreatitis, onehad a rectal abscess, two had perforated duodenalulcers, and four had an ulcerated adenocarcinoma of thecolon.4 6-8 10 11 i2 Our patient also had an ulceratedcarcinoma of the colon.Local factors are usually responsible for the patho-
genesis of clostridial gas gangrene after trauma. Thesefactors include decrease in oxygen tension in muscledue to failure of local blood-supply, presence of foreignbodies, presence of necrotic tissue and haemorrhage,and multiplication of synergistic pyogenic bacteria inthe wound. 2
Systemic factors seem to be very important in thepathogenesis of non-traumatic clostridial infections.For example, Samson and Gruhn’s two cases of
spontaneous clostridial septicaemia were debilitatedwith diabetes or nitrogen-mustard therapy.J3 All
twenty-one patients with clostridial septicxmia com-plicating carcinoma noted above were being treatedwith cancer chemotherapeutic agents.9 Jones’ case 3 ofclostridial septicaemia seeded from a small ulceratedadenocarcinoma of the ascending colon, presented ina patient receiving 6-mercaptopurine for chronic
granulocytic leukxmia. Nine of forty-two clostridialinfections in one community hospital were listed as"
complicating terminal carcinoma ".14A review of the eight cases of localised non-traumatic
clostridial gas gangrene which have been reportedreveals that five were over 70 years of age, three haddiabetes, and one had liver failure.6-1 10 11 i3 Our
patient was a 74-year-old diabetic man with severegeneralised arteriosclerosis.MacLennan suggested that slight local tissue injury
might be the factor which determines the metastaticsite of clostridial myonecrosis once the bacteria seedthe bloodstream. For example, Valentine’s 15 case ofmetastatic gas gangrene associated with an ulceratedadenocarcinoma of the colon arose in a patient whohad had recent blunt muscular trauma to the affected
extremity. Although our patient denied local traumato his arm or forearm, the fact that he awoke with theforearm pain suggests that he could have injured oroccluded local blood-supply in the affected extremitywhile he was asleep.Non-traumatic clostridial infections should be sus-
pected in elderly debilitated patients with lesions in thegastrointestinal, biliary, or genitourinary tracts. Theirprompt recognition and treatment are essential.
This work was supported in part by a grant from the John A.Hartford Foundation.
Requests for reprints should be addressed to A. T. M.
REFERENCES
1. Eraklis, A. J., Filler, R. M., Pappas, A. M., Bernhard, W. F.
Am. J. Surg. (in the press).2. MacLennan, J. D. Bact. Rev. 1962, 26, 177.3. Jones, L. E., Wirth, W. A., Farrow, C. C. South. med. J. 1960,
53, 863.4. Rose, H. D., Bukosly, R. J. J. Am. med. Ass. 1966, 198, 1368.5. Smucker, E. E., Reid, S. E., Harding, H. B. ibid. 1960, 174, 898.6. Soscia, J., Grace, W. J. Am. J. dig. Dis. 1965, 10, 625.
References continued at foot of next column
7. Trippel, O. H., Ruggie, A. N., Staley, C. J., Elk, J. V. Surg. ClinsN. Am. 1967, 47, 17.
8. Whyland, W. A., Levin, M. N. Am. J. Surg. 1960, 99, 77.9. Cabrera, A., Tsukada, Y., Pickren, J. W. Cancer, N. Y. 1965, 18, 800.
10. Gazzaniga, A. B. Dis. Colon Rectum, 1967, 10, 298.11. Kimball, H. W., Rawson, A. J. Va med. Mon. 1952, 79, 269.12. Wyman, A. L. Br. med. J. 1949, i, 266.13. Samson, J., Gruhn, J. Chicago med. Sch. Q. 1964, 24, 12.14. Pyrtek, L. J., Bartus, S. H. New Engl. J. Med. 1962, 26, 698.15. Valentine, J. C. Br. J. Surg. 1957, 44, 630.
Preliminary Communications
A TRANSMISSIBLE AGENT FROM
SARCOID TISSUE
D. N. MITCHELL
Medical Research Council Tuberculosis and Chest Diseases
Unit, Brompton Hospital, London S.W.3R. J. W. REES
National Institute for Medical Research, London N.W.7
Summary The results of a controlled experimentin which an attempt was made to
transmit sarcoidosis by inoculation of sarcoid andnon-sarcoid lymph-node homogenates into the foot-pads of normal and immunologically deficient mice, arereported. The early and late changes in the footpadswere assessed microscopically. A substantial proportionof the footpads of mice receiving sarcoid homogenateshowed the histological characteristics typical ofsarcoidosis in man and evolved fully only after 6-8months following inoculation. Moreover, positiveKveim tests were confined to a proportion of thosemice given sarcoid homogenates and were all associatedwith a sarcoid granuloma in the footpad. Conversely,the inflammatory lesions seen in the early histology ofthe footpads of mice inoculated with non-sarcoidhomogenate were no longer apparent in the late
histology and Kveim tests in all mice given non-sarcoidhomogenate were negative.
INTRODUCTION
THE cause of sarcoidosis is unknown. Althoughthere have been many claims implicating bacteria,viruses, fungi, protozoa, or plant and chemical sub-stances, none of these have been substantiated. More-
over, because the general histological picture ofsarcoidosis is that of a non-caseating epithelioid-cellgranuloma and because a wide variety of micro-
organisms or their degredation products or chemicalsubstances can, in man and animals, produce suchgranulomas, animals have been used to demonstratethese features without, unfortunately, proving theirconnection with the disease in man. There is also goodevidence that patients with sarcoidosis have some
immunological defect, especially in their delayed-hypersensitivity response. Therefore, because no
specific astiological agent has been demonstrated, it hasbeen suggested that sarcoidosis represents an abnormalresponse of the host to non-specific agents or antigens.Against this background we report here our attemptsto transmit sarcoidosis to mice by inoculating homo-genates of human sarcoid tissue using both normal and