Embed Size (px)
Citation preview

RECONSTRUCTIVE
Lower Third Nasal Reconstruction: When IsSkin Grafting an Appropriate Option?
Paul D. McCluskey, M.D.Fadi C. Constantine, M.D.James F. Thornton, M.D.
Dallas, Texas
Background: A full-thickness skin graft is generally not considered the idealreplacement for the thick, sebaceous skin of the nasal tip, ala, lower sidewalls,or dorsum. Instead, many clinicians prefer to reconstruct these defects with localor axial composite flaps that incorporate skin, subcutaneous tissue, and fat.Methods: The authors conducted a retrospective analysis of 55 consecutivepatients who underwent reconstruction of lower third nasal defects with full-thickness skin grafts between 2002 and 2007 performed by the senior author(J.F.T.). All of the patients in this review underwent skin cancer ablation bymeans of Mohs’ micrographic surgery.Results: Good aesthetic results, based on preoperative and postoperative pho-tographic analysis of contour and pigmentation, have been achieved in both therecipient and donor sites in 52 of 55 patients. Three patients, all of whom weresmokers, experienced loss of the skin graft requiring alternative reconstructivetechniques.Conclusions: Under certain conditions, skin grafting of defects of the caudalthird of the nose offers a viable reconstructive option that yields good contourand color match. Careful analysis of defect size, location, and depth and con-sideration of donor-site skin thickness and pigmentation are vital for accuratereplacement of the thick, pitted, sebaceous skin of the caudal nose. An evolutionin technique has revealed that the forehead donor skin often provides a moreconsistent color and contour match in such reconstructions. Secondary derm-abrasion of the graft provides a critical step for obtaining final aesthetic contourand color. (Plast. Reconstr. Surg. 124: 826, 2009.)
Defects of the lower third of the nose presenta special challenge to the reconstructivesurgeon. The unique character of the lower
third of the nose, with its interwoven concavities,convexities, and varying skin thicknesses, exacer-bates the difficult reconstruction of this region.
Well-defined flap algorithms are available forreconstruction of full-subunit alar or full-subunittip defects.1 The lower third nasal defects or de-fects larger than 1.5 cm in diameter can be reliablyreconstructed and repaired with nasolabial orforehead flaps using either a subunit or defect-only reconstruction.2 These techniques requiremultiple stages and allow for the replacement ofcartilage and lining if missing.
Paradoxically, acceptable results are more dif-ficult to achieve with smaller defects, most notablythose smaller than 1 cm. Local flaps applied forthese defects often result in violation of aestheticsubunits, worsening of the defect by alar notching,and frequent or unpredictable pincushioning.Likewise, the misapplication of skin grafts to largeor deep lower third defects often yields a de-pressed patchwork with unsuitable results.
In many cases of lower third nasal reconstruc-tion, particularly those arising from excision ofneoplasms by means of Mohs’ micrographic sur-gery, the defects are shallow and measure less than1 cm in diameter. These defects rarely encompassgreater than 50 percent of aesthetic subunits andare best treated as defect-only reconstructions.3
From the Department of Plastic Surgery, University of TexasSouthwestern Medical Center.Received for publication April 28, 2008; accepted March 12,2009.Presented at the Texas Society of Plastic Surgeons AnnualMeeting, in Austin, Texas, September of 2007.Copyright ©2009 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e3181b03749
Disclosure: None of the authors has any commer-cial association or financial relationships thatmight pose or create a conflict of interest with theinformation presented in this article.
www.PRSJournal.com826

Such defects can be successfully and reliablytreated with well-applied full-thickness skin graft-ing from the preauricular or more preferentialforehead donor site.
The evolution of the demonstrated skin graft-ing techniques started with the recognition of thefrustrating paradox in reconstructing small de-fects of the lower third. Larger defects could beeasily and reliably reconstructed with the well-es-tablished algorithms (i.e., nasolabial or foreheadflap reconstruction). Our institutional disappoint-ment with use of bilobed flaps from the upperthird of the nose to recreate defects on the lowerthird commonly results from the inherent designflaw of the bilobed flap (the design of the flapviolates a second or third aesthetic unit and oftencompletely distorts the alar groove) and the in-herent unpredictability of the final result becauseof its tendency to pincushion. We also have aninstitutional reluctance to advance skin from thenasal sidewall to reconstruct lower third defects, asthis destroys an aesthetic subunit that is very hardto reconstruct—the alar groove.
ANATOMICAL CONSIDERATIONSThe lower third of the nose is defined by its
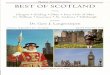
margins, which include the alar rims inferiorly,the nasolabial grooves laterally, and the alargroove, which forms the junction with the uppertwo-thirds of the nose.4,5 Any distortion of the alarrim or obliteration of the nasolabial groove is ex-ceedingly noticeable and difficult if not impossi-ble to correct secondarily. Classically, the lowerthird of the nose is composed of six subunits:bilateral ala and soft triangles, the central tip, andcolumella6 (Fig. 1). Importantly, the ala and tipare biconvex structures, and maintaining and re-storing the contour of these structures is essentialto aesthetic nasal reconstruction. The unique na-ture of the lower third skin, which is often thickand richly populated with sebaceous glands, com-plicates reconstructions, often rendering the skinstiff and difficult to rotate and form into localflaps.
PATIENTS AND METHODSThis is a retrospective review of 55 patients
who underwent reconstruction of lower third na-sal defects with full-thickness skin grafts between2002 and 2007, all performed by the senior author(J.F.T.). Only those patients with defects of thelower third, defined as the bilateral ala and softtriangles, tip, columella, lower dorsum, and nasalsidewalls were included in the review. All patientshad defects resulting from skin cancer ablation
using Mohs’ micrographic surgery performed by adermatologist. The reconstructions took placewithin 48 hours of excision, with the vast majorityoccurring on the same day as the Mohs’ proce-dure. All procedures were performed in an oper-ating room setting with either sedation supple-menting local anesthetic or local anesthesia alone.
Forehead or preauricular skin donor siteswere used in all cases, with primary closure of thedonor sites. The percentage of forehead skingrafts was greater in the later patients secondary tothe perception that these provided superior re-sults. Forehead skin was used in 65 percent, withthe remainder being preauricular skin. As a rule,the thicker nasal defects in younger patients werereconstructed with forehead skin, as this was anevolving technique. As the senior author began touse forehead skin more frequently as opposed topreauricular skin, a more consistent result wasachieved with regard to a normal appearing re-construction, with less irregularity in contour andcolor match.
RESULTSAverage defect size among all 55 patients was
8 mm, with a range of 5 to 17 mm. Sixty-eightpercent of the patients had greater than 3-monthfollow-up. Sixty-two percent underwent one derm-abrasion treatment, and 26 percent underwenttwo or more treatments. An aesthetic standard ofnot simply a healed wound but rather a normalappearance with good contour and color match asendpoints was used (Figs. 2 through 7). Patientswere evaluated for contour irregularities and hy-popigmentation or hyperpigmentation. Based on
Fig. 1. Illustration of the nasal subunits of the lower third. Thedorsum, tip, and paired soft triangles and alar lobules are shown.Note that the columella is not labeled.
Volume 124, Number 3 • Lower Third Nasal Reconstruction
827

postoperative photographs, 14 percent had minorcontour or color defects, with 8 percent havingmore pronounced color/contour changes (Figs. 8and 9). Of the 55 patients, there were only threecases (5 percent) of graft loss. All of these oc-curred in smokers [11 of 55 patients (20 percent)were active smokers], and among active smokers,the rate of graft failure was 27 percent (Fig. 10).There were no donor-site morbidities in this se-ries; however, most of the harvested grafts mea-sured less than or equal to 1 cm. There were noprimary failures of the bolster technique, and allbolsters were removed at 3 to 7 days postopera-
tively, with day 5 being the preferred time forbolster removal.
TechniqueAll procedures were performed under local
anesthesia with or without intravenous sedation inan operating room setting. A 1:1 mixture of 0.25%Marcaine (Hospira, Inc., Lake Forest, Ill.) with 1%lidocaine with epinephrine (mixed 1:1000 in 30 ccof lidocaine) was used for local anesthesia, vaso-constriction, and postoperative analgesia. Thismixture is injected subdermally at the site of the
Fig. 2. A 64-year-old man presented with an 8-mm nasal tip defect following Mohs’ excision of abasal cell carcinoma (left). There was exposed perichondrium in the base of the wound, although itwas a relatively thin defect. The patient underwent two rounds of postoperative dermabrasion afterskin graft placement (forehead donor site). (Right) Appearance at 3-month follow-up.
Fig. 3. A 43-year-old woman presented with a 7-mm alar defect, abutting but not crossing the alar rim.(Left) Appearance of the patient 1 week after skin grafting from a forehead donor site. Note the duskyappearance of the graft despite good take. (Right) The patient 3 months postoperatively. She has un-dergone two dermabrasion treatments.
Plastic and Reconstructive Surgery • September 2009
828

defect and the graft donor site. The operativeapproach to each defect followed a similar ca-dence beginning with reverticalization of thewound edges and sharp debridement of any fi-brinous tissue or debris in the base of the defect.This initial step is critical for normalizing any con-tour abnormalities in the defect and is performedunder loupe magnification with a straight, double-edged beaver blade. Further excisions were per-formed if required to place the borders withinaesthetic subunits; however, there was not strict
adherence to aesthetic subunit reconstruction,and these cases should be considered as defect-only reconstructions.
After reverticalization of the wound edges andnormalization of the contour, a foil pattern tem-plate was used. This template should be treated asa three-dimensional construct, accounting for therelative concavity or convexity of the tissue sur-rounding the defect. Based on the template, afull-thickness skin graft, either from the preauric-ular or preferentially from the forehead donor
Fig. 4. A 57-year-old man with thin nasal skin underwent Mohs’ excision of a basal cell carcinoma onhis nasal tip (left). (Right) Patient 3-month follow-up after full-thickness skin grafting from fore-head skin and one in-office dermabrasion treatment.
Fig. 5. A 54-year-old man had a 7-mm alar defect after excision of a basal cell carcinoma (left). (Right)Patient at the 3-month follow-up visit following preauricular skin grafting. He received one dermabra-sion treatment.
Volume 124, Number 3 • Lower Third Nasal Reconstruction
829

site, is harvested. The donor sites were all closedin a multilayer fashion with buried interruptedand continuous suture. The donor sites were fre-quently placed at the junction of the hair-bearingand non–hair-bearing scalp following the relaxedskin tension lines. Great care was taken to ensurethat the grafts harvested were identical sizematched to the donor site. This was accomplishedby using the foil pattern template and sharplyscoring the harvested graft within the ellipse of thedonor site to accurately reflect the size before graftharvest. This eliminates the distortion caused byblurry ink lines while harvesting the graft. There-fore, scoring the template before harvest repre-
sents a critical step in accurately designing thegraft to be the exact size of the defect. Care wastaken to handle the graft atraumatically through-out its harvest and inset.
In the initial 10 consecutive patients includedin this review, the skin grafts were sewn into thedefect with 4-0 or 5-0 chromic gut suture; however,secondary to an unsatisfactory inflammatory re-sponse from the chromic suture, the suture ma-terial has been changed to 5-0 fast-absorbing gut,which was used for the remainder of the cases. Thegrafts are precisely sewn into place with continu-ous opposing 4-0 or 5-0 plain gut sutures that runin a continuous fashion in opposite directions
Fig. 6. A 1-cm superficial alar defect was reconstructed with a full-thickness skin graft from a forehead donor sitein this 37-year-old woman (left). After two dermabrasion treatments, her contour and pigmentation at 3 monthsare very good (right).
Fig. 7. This 6-mm alar rim defect was reconstructed with a full-thickness skin graft using preauricular skin (left). (Center) Photographdemonstrates the degree of healing at 1 month postoperatively. After two dermabrasion treatments, no contour or color irregu-larities are visible (right).
Plastic and Reconstructive Surgery • September 2009
830

around the graft and are tied at the opposite side.This precisely insets the graft, providing a stableinset with no bunching or distortion, and is verytime saving (Fig. 11).
Fabrication of the skin graft bolster completesthe procedure. In the majority of cases, a double-armed 3-0 or 4-0 Prolene suture (Ethicon, Inc.,Somerville, N.J.) is placed at the center throughthe underlying tissue and then through the centerof the graft. Both arms of the suture are placed ina similar fashion and then left untied and sewndirectly into the bolster (Fig. 12). All bolsters inthis review were fashioned from dry surgical prep-aration sponges that had been preoperatively gas
sterilized. The surgical preparation sponge mate-rial provides adequate rebound and support. Thesponge bolsters are all coated with antibiotic oint-ment away from the operative field and thethrough-and-through 3-0 Prolene sutures are thenplaced in juxtaposition through the bolster andtied in place (Fig. 13). This technique obliteratescentral dead space and optimizes graft adherence.The remainder of the bolster was then securedwith 5-0 silk bolster sutures placed through thegraft and native skin edge, then tied at four toeight points around the graft, depending on graftsize. The closed donor-site incision and the edges
Fig. 8. A patient with a hypopigmented scar after full-thicknessskin grafting from preauricular skin to the nasal tip with postop-erative dermabrasion.
Fig. 9. This patient received a full-thickness skin graft from apreauricular donor site to his ala with postoperative dermabra-sion. He has a persistent contour defect at this site.
Fig. 10. An example of a failed alar graft from forehead skin in asmoker. This was successfully regrafted after the wound wasdebrided.
Fig. 11. An example of the fast-absorbing running suture at thegraft margin, and four-corner bolster sutures.
Volume 124, Number 3 • Lower Third Nasal Reconstruction
831

and exterior of the bolster were coated with an-tibiotic ointment.
Donor sites were dressed with Xeroform gauze(Sherwood Medical, St. Louis, Mo.), and the pa-tients were each given a set of written wound careinstructions. The patients are instructed to begin
showering on the second postoperative day withthe provision that they cover the graft bolsters witha vigorous coating of antibiotic ointment beforeshowering. The bolsters and the graft materialwere very well tolerated, as mentioned earlier, withno bolster failures.
Given the thickness of the forehead skin, it is notunusual for the most superficial portion of the graftto initially undergo a period of partial slough. Thiswas treated with continued application of antibioticointment and patient reassurance. Patients wereseen at weekly intervals until full graft survival wasensured. At this point, daily application of antibi-otic ointment was discontinued and patients wereoffered the opportunity to begin topical scarcream therapy with Mederma (Merz Pharmaceu-ticals, Greensboro, N.C.), Scar Zone (CCA Indus-tries, East Rutherford, N.J.), or more recently,Transdermis scar therapy (NFI Consumer Prod-ucts, Fayetteville, N.C.). No clinical science sup-ports the use of one scar cream over another;however, it has been our experience that the pa-tients strongly prefer applying a scar care product,and subjectively the Transdermis scar therapy re-sulted in a fairly rapid reduction in inflammatoryresponse. We also currently offer patients the op-portunity to apply silicone sheeting to both theskin graft and donor-site areas.
It should be noted that the postoperative rec-ommendations for scar therapy are based not onscience but on an evolving clinical practice withlessons learned from failures in scar therapy fromthe beginning of the practice. All of the patientswere offered dermabrasion beginning at 6 weeksafter grafting. Based on the behavior and appear-ance of the scar, up to three postoperative derm-abrasion treatments were offered at 6-week inter-vals. The dermabrasion itself was performed in theoffice setting, with only topical tetracaine creamfor anesthetic. The dermabrasion was performedwith a rotary dermabrader using the diamond cyl-inder wheel, and the endpoint was deep punctatebleeding. The goal of the dermabrasion proce-dure was to both improve the graft color and toblur or diminish the patch effect of the graft onthe surrounding nasal skin by essentially improv-ing the appearance of the surrounding scar. Theprocedure was confined to the graft and immedi-ate surrounding skin. Although dermabrading en-tire subunits has been advocated to provide aneven contour over the subunit, we have found thispractice largely unnecessary for smaller defects.7Entire subunit dermabrasion was not frequentlyoffered except for larger defects that encom-passed a majority of the subunit. An illustration of
Fig. 12. The through-and-through monofilament suture usedto provide additional stability and compression to the skin graftbolster. Both needles on the double-ended suture are thenpassed through the center of a piece of surgical sponge and tieddown.
Fig. 13. Illustration of the bolster technique used by the seniorauthor. Through-and-through 3-0 Prolene sutures are placed injuxtaposition through the bolster and tied in place. This tech-nique obliterates central dead space and optimizes graftadherence.
Plastic and Reconstructive Surgery • September 2009
832

the effects of dermabrasion is provided in sequen-tial photographs in Figure 6.8
DISCUSSIONHistorically, and often correctly, skin grafting
of defects of the lower third of the nose has beenconsidered to yield an inferior aesthetic result. Theinappropriate placement of large, poorly color-matched supraclavicular or postauricular skingrafts to replace the thick, often convex defects ofthe lower third can yield results that are poor andfrequently impossible to correct.
Achieving a well-contoured, aesthetically pleas-ing result begins with meticulous preoperative anal-ysis of the nasal defect. Criteria for selecting lowerthird nasal defects that can be acceptably treatedwith full-thickness grafts include defect location;size smaller than 1 cm; and a partial-thicknessdefect with underlying dermis, subcutaneous tis-sue, or perichondrium.
The basic concern with using a full-thicknessskin graft is the resultant patchwork appearancecaused by color mismatch and contour defects.Adhering to the concept of subunit reconstruc-tion alleviates concerns for a resultant patchworkappearance, regardless of the reconstructivemethod. The senior author, however, prefers adefect-only approach to nasal reconstructionwhen using full-thickness skin grafts. Acceptableresults were achieved in this study using full-thick-ness skin grafts to reconstruct lower third defectssmaller than 1 cm in diameter, with each caseperformed without excising an entire subunit.The decision to limit described reconstructions toless than 1 cm is not based on the inability toreconstruct larger defects; however, defects largerthan 1 cm, we feel, are reconstructed more suc-cessfully with entire subunit reconstructions usingmore standard reconstruction techniques (localor adjacent flap techniques). Contrasting defect-only versus subunit nasal reconstruction is beyondthe scope of this study; however, these conceptsare an important component of defect analysisand must always be considered. Again, a principle-based reconstruction, beginning with careful andmeticulous defect analysis and selection, will yieldan acceptable result regardless of the reconstruc-tive method.9
Adhering to the concept of replacing like withlike, the individual characteristics of skin graft do-nor sites must be considered. After analyzing thedefect and creating a like-sized template, the ap-propriate donor site must be selected based ontexture, thickness, color, and tendency toward hy-perpigmentation or hypopigmentation. Much of
our current knowledge of donor-site characteris-tics comes from the dermatology literature. Thesenior author prefers preauricular and more pref-erably forehead skin for lower third nasal recon-struction. Forehead sites offer thicker skin, with arelatively sebaceous, oily texture, and they sufferthe same degree of daily sun exposure and actinicdamage as the lower third of the nose. Other do-nor sites available to the reconstructive surgeoninclude the nasolabial fold, postauricular skin,and supraclavicular skin. Postauricular donor sitessuffer very little (if any) daily sun exposure andhave much thinner skin than the nasal lobule.Therefore, they are prone to pigmentationchanges and do not provide a good contour matchfor reconstructing the lower third of the nose.Likewise, the skin of the supraclavicular regioncontains very few sebaceous elements and is oftenhyperpigmented before harvest. The preauricularand forehead donor site grafts should be har-vested without including terminal hairs and de-signed along relaxed skin tension lines, allowing forprimary closure. Good results can be achieved with-out distorting the anterior hairline or sideburn.
Hubbard wrote a provocative article describ-ing 33 patients who had lower third defects re-constructed with nasolabial fat and/or partiallydefatted skin grafts harvested from the nasolabialfold.10 The illustrated results demonstrated per-fectly acceptable reconstructions, and his workserves as a useful description of a different tech-nique using the nasolabial donor site. Although adeparture from commonly preferred techniques,his results are a testament to the concept that askin graft can survive without being completelydefatted. Although his results are aesthetically ac-ceptable and associated with very few graft losses,most authors argue that leaving this fat impedesthe processes of imbibition and inosculation nec-essary for graft survival, thereby risking high ratesof graft loss. Contact between the graft dermis andthe recipient bed is of vital importance for estab-lishment of neovascularization. Therefore, we re-gard careful defatting of the graft and use of abolster indispensable technical components to en-sure survival or “take” of the full-thickness graft.
If a defect is of sufficient depth to require agraft that includes subcutaneous fat, using a full-thickness skin graft for such a defect represents abreak from principle-based reconstruction. Like-wise, when considering defects along or near thealar rim, one must carefully account for the po-tential for alar notching. Given appropriate defectanalysis, reconstructing a superficial alar defectwith a full-thickness skin graft may yield an ac-
Volume 124, Number 3 • Lower Third Nasal Reconstruction
833

ceptable result without resultant notching. Skingrafting for defects that abut the alar rim wereused with great caution in this series. Preferen-tially, skin grafts on the posterior aspect of the alaor defects in male patients with very thick seba-ceous skin could be grafted more safely withoutthe risk of alar retraction secondary to the inher-ent stability of anatomical position on the ala.9Deeper defects that extend into the subcutaneoustissue or to the perichondrium of the lateral crurademand a local flap or nasolabial flap with a non-anatomical alar contour graft.
It is frequently debated in both the dermato-logic and plastic surgery literature whether to har-vest a graft of identical size to the defect, or tocorrect for anticipated contraction and harvest alarger graft. The senior author’s technique in-volves creation of a template of equal size to thedefect. As discussed previously, this template isdesigned in three dimensions, taking concavity orconvexity into consideration. Full-thickness skingrafts primarily contract 10 to 15 percent afterexcision; however, insetting the graft under ap-propriate tension readily resolves this problem. Allof the defects presented in this study were recon-structed with grafts of equal size. Harvesting alarger graft to account for primary contractionpresents a number of issues. First, the donor sitemust be larger, and in keeping with an ellipticaldesign, increasing the diameter of the donor sitenecessitates an extension of its axial length. Thelarger donor graft, which represents an estimationof size to account for contraction, often requirestrimming before inset; this leads to an inexact sizeand shape that no longer resembles the templateor the defect. Harvesting a larger graft does notimprove these results but instead presents the con-founding morbidity of a larger donor site.
Graft loss is always a concern, and althoughresults are improved by careful defatting and bol-ster placement with through-and-through buttresssutures, other factors such as a history of smokingcome into play. All of the graft losses in this serieswere in smoking patients. It is impossible to de-velop and maintain a comprehensive reconstruc-tive practice without operating on smokers; how-ever, these patients must understand that they areat significantly higher risk of graft loss or flapnecrosis, and may ultimately be left with an un-acceptable result. The effects of nicotine are welldocumented as a potent vasoconstrictor that re-duces blood flow, leading to a hypoxic cascadethat impairs healing and increases platelet aggre-gation and adhesion. In the multicenter study ofrecipient-site complications of full-thickness skin
grafts, authors of the Australian Mohs Databaseshowed that “although the number of smokers wassmall, they had a mean graft survival of 2% on thesecond visit compared with 75.9% in the non-smoking group.” If the patients are seen preop-eratively, substantial benefit has been shown inpeople who are able to abstain from smoking forat least 4 weeks before reconstruction.
Patients are typically well informed and un-derstand the possibility of graft loss. They arehighly attuned to changes in graft appearance andwill often present in the early postoperative periodwith concerns over a pale or overly dark graft.Indeed, full-thickness skin grafts are less predict-able than nasolabial or local flaps. The healingperiod involves color and texture changes that canraise alarm before arriving at the final, aestheti-cally acceptable result. The graft is initially isch-emic, appearing white and pale. As it evolvesthrough the stages of revascularization, it will be-come edematous and then darken, resulting in acyanotic or hyperemic appearance. These colorchanges vary among patients and among graft sitesand sizes in an unpredictable manner, but overweeks to months, the living graft will approximate anormal color. In some cases, especially with a thickgraft, the epidermis will turn dark and slough. Thistissue will reepithelialize, given the presence of der-mal appendages, but both the patient and physicianwill have a justified concern that the graft has failed.Patients should be counseled to anticipate thesechanges in color and texture.
In keeping with the principles asserted byRohrich et al., good contour is the aesthetic end-point to all nasal reconstructions.9 To achieve this,the authors describe “complementary ablativeprocedures” to enhance final results. These pro-cedures include dermabrasion, thinning of flaps,breaking up trapdoor scar lines, and steroid injec-tions at sites of pincushioning. Primary dermabra-sion is not typically performed for full-thickness skingrafts because of the risk of trauma to the delicategraft and because of the unpredictable course ofhealing that the graft will follow. Dermabrasion ofskin grafts is instead performed at approximately 6weeks postoperatively. Depending on the size of thegraft, dermabrasion can be limited to the graft mar-gins or can include an entire subunit(s).
CONCLUSIONSThe following principles make skin grafting of
lower third subunits a viable reconstruction op-tion. Provided that these constraints are followed,skin grafting of the lower third of the nose is anappropriate part of the reconstructive algorithm.
Plastic and Reconstructive Surgery • September 2009
834

1. Rigorous defect selection to include onlysuperficial defects, and size-limited defects.Defects larger than 1 cm will be bettertreated with alternative reconstructions. De-fects that involve cartilage or deeper are bydefinition complex nasal defects that willrequire onlay cartilage grafting for satisfac-tory reconstruction. Skin grafting is not of-fered for these defects.
2. Caution in skin grafting defects abutting thealar rim.
3. Meticulous graft donor-site selection usingthe thicker and better color-matched fore-head skin in the majority of cases.
4. Meticulous size matching of the graft, usinga foil pattern template, and development ofa bolster material from a surgical spongethat provides ideal compression and han-dling qualities used in conjunction with athrough-and-through central Prolene sutureto minimize graft dead space.
5. Liberal use of postoperative dermabrasionto optimize the final color match.
James F. Thornton, M.D.Department of Plastic Surgery
University of Texas Southwestern Medical School1801 Inwood Road, 4th Floor
Dallas, Texas [email protected]
REFERENCES1. Hill TG. Contouring of donor skin in full-thickness skin
grafting. J Dermatol Surg Oncol. 1987;13:883–886.2. Barton FE Jr. Aesthetic aspects of partial nasal reconstruc-
tion. Clin Plast Surg. 1981;9:177–191.3. Dimitropolous V, Bichakjian CK, Johnson TM. Forehead
donor site full-thickness skin graft. Dermatol Surg. 2005;31:324–326.
4. Collins PS, Farber GA. Postsurgical dermabrasion of thenose. J Dermatol Surg Oncol. 1984;10:476–477.
5. Leibovitch I, Huilgol SC, Richards S, Paver R, Selva D. TheAustralian Mohs database: Short term recipient site compli-cations in full thickness skin grafts. Dermatol Surg. 2006;32:1364–1368.
6. Baker S, Swanson NA. Local Flaps in Facial Reconstruction. St.Louis: Mosby; 1995.
7. Adams DC, Ramsey ML. Grafts in dermatologic surgery: Re-view and update on full- and split-thickness skin grafts, freecartilage grafts, and composite grafts. J Dermatol Surg. 2005;31:1055–1067.
8. Kuijpers DI, Smeets NW, Lapiere K, Thissen MR, Krekels GA,Neumann HA. Do systemic antibiotics increase the survivalof a full-thickness graft of the nose? J Eur Acad DermatolVenereol. 2006;20:1296–1301.
9. Rohrich RJ, Griffin JR, Ansari M, Beran SJ, Potter JK. Nasalreconstruction: Beyond aesthetic subunits: A 15 year reviewof 1334 cases. Plast Reconstr Surg. 2004;114:1405–1416; dis-cussion 1417–1419.
10. Hubbard TJ. Leave the fat, skip the bolster: Thinking outsidethe box in lower third nasal reconstruction. Plast ReconstrSurg. 2004;114:1427–1435.
11. Menick FJ. Facial reconstruction with local and distant tissue:The interface of aesthetic and reconstructive surgery. PlastReconstr Surg. 1998;102:1424–1433.
Instructions for Authors: Key GuidelinesManuscript Length/Number of Figures
To enhance quality and readability and to be more competitve with other leading scientific journals, allmanuscripts must now conform to the new word-count standards for article length and limited number offigure pieces:
• Original Articles and Special Topics/Comprehensive Reviews are limited to 3000 words and 20 figurepieces.
• Case Reports, Ideas & Innovations, and Follow-Up Clinics are limited to 1000 words and 4 figure pieces.
• Letters and Viewpoints are limited to 500 words, 2 figure pieces, and 5 references.
Volume 124, Number 3 • Lower Third Nasal Reconstruction
835