Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Reconstruction of lower lip with myomucosal advancement flap
Daghan Isik, MD,1* M. Fatih Garca, MD,2 Cengiz Durucu, MD,3 Ugur Goktas, MD,4 Bekir Atik, MD1
1Department of Plastic and Reconstructive Surgery, Medical School of Yuzuncu Yil University, Van, Turkey, 2Department of Otolaryngology, Medical School of Yuzuncu YilUniversity, Van, Turkey, 3Department of Otolaryngology, Medical School of Gaziantep University, Gaziantep, Turkey, 4Department of Anesthesiology, Medical School of YuzuncuYil University, Van, Turkey.
Accepted 6 September 2011
Published online 23 November 2011 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/hed.21957
ABSTRACT: Background. In this article, a new surgical procedure that canbe used for reconstruction of lower lip defects of any size is described.
Methods. In this prospective study, the surgical procedure was appliedin 16 patients. In this procedure, the mucosa and the orbicularis orismuscle of the lower lip are repaired with a composite flap, and the skindefect is closed using local skin flaps. The patients were assessed interms of complications, mouth opening, sphincter function of the mouth,and sensation in the lower lip.
Results. The aesthetic results obtained in all patients were satisfactory.Sufficient oral sphincter function was achieved in all patients.
Conclusion. Reconstruction of lower lip defects using the proceduredescribed here can be performed in patients with lower lip defects ofany size as long as the mucosal and skin repair lines are notsuperimposed. This procedure yielded good sphincter function andaesthetic results. VC 2011 Wiley Periodicals, Inc. Head Neck 34:1562–1569, 2012
KEY WORDS: lower lip reconstruction, myomucosal advancementflap, random flap, local flap, lower lip
The most important cause of lower lip defects is tumorablation.1,2 Full-thickness defects that are smaller than30% of the lower lip can be repaired primarily.3–5 Localflaps are used for lower lip defects involving between30% and 80% of the lower lip,5–11 whereas lower lipdefects with over 80% involvement are frequentlyrepaired with free flaps.12–16 The purpose of lower lipreconstruction is to achieve a sufficient oral orifice,appropriate muscle repair to restore oral functions, andreconstruction using a tissue with sensation and an aes-thetic outcome. Reconstructive surgeons have imple-mented repair procedures that mainly use adjacent tissuesbecause it is thought that these techniques provide recon-struction results that include all of the intended character-istics.3–11,17,18 Despite the significant number of proce-dures that have been described, new procedures areneeded that can be used for the reconstruction of lowerlip defects of all sizes. Furthermore, procedures that ena-ble the use of local tissues instead of free flaps aregreatly preferred, especially for extensive lower lipdefects. In general, almost all local reconstruction proce-dures aim at transferring lower lip mucosa, muscle, andskin tissue, collectively. In the procedure described inthis article, lower lip defects were considered to havebeen composed of 2 separate defects, namely a myomu-cosal defect and a skin defect; the myomucosal defectwas repaired with a myomucosal advancement flap
(MAF), while the skin defect was closed with local skinflaps. Reverse transposition flaps, rotation flaps, and bi-lobed flaps were used as local skin flaps.
PATIENTS AND METHODSIn this prospective study, the surgical procedure was
applied to all patients (16 patients; 4 women and 12 men)who were referred to our hospital with lower lip canceror with skin cancer around the mouth involving the lowerlip between June 2006 and December 2010. The patientswere between 35 and 72 years of age (mean age, 55.5years). In all of the patients, the lower lip defect devel-oped due to excision of squamous cell carcinoma. In 7patients, the lower lip defect was found to involve 30%to 60% of the lower lip; in 4 patients, it involved 60% to90%; and in the remaining 5 patients, it involved 90% ormore (total or near total). The maximum mouth orificewas measured in each patient at the sixth postoperativemonth. This value was obtained by measuring the maxi-mum distance between the lower and upper lip while thepatients opened their mouths maximally.
At the sixth postoperative month, a questionnaire wasgiven to the patients to assess their satisfaction with theresults of the surgery in terms of oral function and aes-thetics. In this questionnaire, the participants reportedtheir satisfaction with postoperative mouth opening, theposition of the lips during talking, the sensation in thelower lip, movements related to whistling and laughing,and esthetic satisfaction compared to the preoperativeconditions. The participants scored these items as verygood: 5, good: 4, moderate: 3, bad: 2, and very bad: 1.
*Corresponding author: D. Isik, Department of Plastic and ReconstructiveSurgery, Medical School of Yuzuncu Yil University, Van, Turkey.E-mail: [email protected]
1562 HEAD & NECK—DOI 10.1002/HED NOVEMBER 2012

Surgical procedure
The myomucosal defect was repaired by MAF in allpatients, whereas in 1 patient with a total lower lip defect,the mucosa was reconstructed using MAF and a skingraft. For reconstruction of the skin defects, a rotationflap was used in 8 patients (a bilateral rotation flap wasused in 5 patients); in 7 patients, a reverse transpositionflap from the adjacent part of the lip was used (the bilat-eral was used in 2 patients); and in 1 patient, a bi-lobedflap was used (Table 1). All patients were operated onwhile they were under general anesthesia, except 4patients who were operated on while they were underlocal anesthesia. For reconstruction of the mucosa andorbicularis oris, an incision was made starting from 1 sideof the defect through the vermillion-skin border; this inci-sion passed through the modiolus and was continued hori-zontally 1.5 to 4 cm inside the mouth. A second mucosaincision was made inside the mouth, parallel to the firstincision, starting from the lower end of the lower lipdefect at the level of the lower lip vestibule, extending tothe cheek. While the incised rectangular advancementflap was harvested, especially around the modiolus, onlythe orbicularis oris muscle was included in the mucosalflap. To achieve this, other muscles in this area were notincluded in the flap and were left in their original posi-tions. If the orbicularis oris muscle is fully dissectedbetween the lower and upper lip lateral to the modioluswhile the MAF is harvested, sphincter functions may belost postoperatively; therefore, the orbicularis oris was notcompletely cut horizontally, and at least 0.5 cm of muscletissue was kept intact. In particular, the depressor anguli
oris muscles and other muscles responsible for movingthe modiolus were not included in the MAF. Anotherissue in harvesting the MAF was preserving the mentalnerve. The mental nerve was preserved in the advance-ment flap to prevent postsurgical sensory defects in thelower lip mucosa. The mucosal area innervated by themental nerve was excised together with the tumor. Thisexcision was bilateral in cases of extensive lower lipdefects and monolateral in tumors adjacent to the lowerlip commissura. In such cases, the mental nerve could notbe transferred with the mucosal flap, and it was preservedin its original position to maintain innervation in therelated skin area. Horizontal MAFs harvested from bothsides were sutured to each other in the midline, and thelower lip vestibule was regenerated inferior to the flaps.
Afterward, skin reconstruction was performed over thelower lip reconstruction in which the muscle and mucosarepair was completed. For lower lip skin reconstruction, atransposition flap harvested from the area adjacent to themouth with a superior pedicle, a rotation flap expandingto the mentum, or a bi-lobed flap including cervical skinwere used (Figures 1 and 2). When required, skin residue(dog ear) in the commissura area was excised in a sepa-rate session with the patient under local anesthesia.
RESULTSPatients were postoperatively followed for 3 months to
2 years (mean, 10.6 months). In all patients, lower lipreconstruction was successfully completed. The aestheticresults obtained in all patients were satisfactory. Oralfunction after the surgery was nearly normal in allpatients (Figures 3–7). The mean postoperative maximumoral orifice was 5.15 cm (range, 4.5–5.5 cm) and suffi-cient oral sphincter function was achieved in all patients.Deficits in quality-of-life parameters such as speech, abil-ity to retain food under lower lip, and salivation retentionwere not observed. Oral mucosa sensory functions wereintact in all patients at the postoperative follow-up.Except for 2 patients, no complications were seen. In 1patient with complications, wound dehiscence wasobserved along the mucosal repair line, and this area wasre-sutured with the patient under local anesthesia. In theother patient with complications, the skin defect had beenrepaired using the rotation flap, and superficial necrosisof 0.5 cm and scar dehiscence were seen on the repairline of the skin tissue. This was repaired by debridementand re-suturing. One patient with lip cancer involving thetotal lower lip died of primary pulmonary lung cancerapproximately 3 months after total lower lip reconstruc-tion with MAF and a bilateral transposition skin flap.
From the questionnaire, the mean score for mouthopening was 4.00 points, the mean score for the lower lipposition during talking was 4.26 points, the mean scorefor sensation in the lower lip was 3.93 points, the meanscore for movement related to whistling was 3.26 points,the mean score for movement related to laughing was3.33 points, and the mean score for the esthetic result was3.53 points.
DISCUSSIONMany procedures have been described for the recon-
struction of lower lip defects, although new techniques
TABLE 1. Characteristics of patients with lower lip cancer treated withlower lip reconstruction.
Patientno.
Sex/age
Lower lipdefect, % Skin flap Complication
1 M / 50 40 Rotation (unilateral) None2 M / 64 100 Interpolation (bilateral) None*3 M / 63 95 Rotation (bilateral) None4 M / 57 50 Interpolation
(unilateral)Dehiscencein mucosa
5 F / 72 40 Interpolation(unilateral)
None
6 M / 46 70 Rotation (unilateral) None7 M / 65 40 Interpolation
(unilateral)None
8 M / 71 90 Rotation (bilateral) None9 M / 68 50 Rotation (unilateral) None10 M / 38 90 Rotation
(bilateral)Marginalnecrosisin skin flap
11 F / 62 50 Bi-lobed flap None12 M / 35 50 Interpolation
(unilateral)None
13 F / 43 80 Interpolation(bilateral)
None
14 M / 54 75 Rotation (bilateral) None15 M / 57 95 Rotation (bilateral) None16 F / 43 70 Interpolation
(unilateral)None
Abbreviations: M, male; F, female.* The patient died at the third postoperative month from the primary pulmonary cancer.
MYOMUCOSAL ADVANCEMENT FLAP
HEAD & NECK—DOI 10.1002/HED NOVEMBER 2012 1563

are still required to close extensive defects with localflaps. In an ideal procedure for total lower lip defects, thesurgical technique should be performed using local flaps;satisfactory functional and aesthetic results should beachieved; the risk of complications such as full-thicknesswound dehiscence, scar contracture along the repair line,or notching should be low; and donor region morbidityshould be limited. Defects involving less than one thirdof the lower lip can be reconstructed primarily3–5; lowerlip defects involving between 30% and 80% of the lowerlip can be reconstructed with Karapandzic, Abbe, Est-lander, McGregor, or Gillies fan flaps, and Nakajimaflaps or Schuchardt flaps.5,6,11,19 Until now, the mostappropriate reconstruction method for total or near-totallower lip defects has been the use of free flaps. In proce-dures described for lower lip reconstruction with localflaps, the upper lip, cheek, mentum, and lower lip havebeen used as donors.5,6,11,19 In all of these conventionaltechniques, which have been reported to provide positiveresults, the lower lip mucosa is transferred together withmuscles and skin, and lower lip reconstruction isattempted. In our opinion, the most important step inlower lip reconstruction is myomucosal reconstruction.On the other hand, attempting to perform myomucosalreconstruction together with a skin area and through askin flap maneuver, as is done in conventional proce-dures, limits the extension and mobility of the muscleand the mucosa to be transferred. The MAF used to
reconstruct lower lip defects in this study was first usedby Mutaf et al20 in 1993 to treat lower lip sinuses.Because lower lip sinuses are present in the red region(mucosa) of the inner lip, mucosa reconstruction alone issufficient, and MAF is an appropriate choice for thisreconstruction. Other studies using myomucosal flapsinclude a unilateral vermillion flap designed by Lane andKent21 in 2007 for small mucosal defects of the lower lipand myomucosal vermillion flaps harvested from lowerand upper lips by Robotti et al22 for commissura defects.The possibility of restoring myomucosal and skin regionswith separate flaps during lower lip reconstruction withlocal flaps was proposed by Ducic et al23 in 2005. Inpatients with lower lip defects involving between 50%and 80% of the tissue, Ducic et al23 used a split myomu-cosal flap for muscle and mucosa reconstruction, whileprimary repair of the skin defect was performed. In theirtechnique, primary repair of the lower lip skin may causemicrostomia in lower lip defects involving 80%. Addi-tionally, the suture line of the myomucosal flap is super-imposed on the skin suture line. Similarly, in techniquessuch as Karapandzic, Abbe, Estlander, McGregor, andGillies fan flaps, or in the procedures of Nakajima orSchuchardt, where lower lip reconstruction is performedwith composite flaps containing mucosa, muscle, andskin tissues, the lower lip mucosa suture line is superim-posed by the skin repair suture line. As a result, evenvery small healing scar defects along the lower lip repair
FIGURE 1. Schematic diagram of lower lip reconstruction with a bilateral rotation flap and myomucosal advancement flap (MAF). (A) Preoperativeanatomy of the lip, (B) appearance of the near-total lower lip defect and planning of the MAF (dotted lines indicate the MAF), (C) view of themyomucosal flap advancement, preserving at least a 0.5 cm of the lateral portion of the orbicularis oris muscle after MAF harvesting, (D) suturationof the myomucosal flaps, (E) planning of the rotation flaps on the mentum, (F) appearance of the harvested rotation flaps, (G) view of the suturedskin flap and cutting of the excess skin, (H) postoperative final view of the patient, (I) appearance of the anatomic placement of the orbicularis orismuscle and mucosa innervation at the end of the surgery. [Color figure can be viewed in the online issue, which is available atwileyonlinelibrary.com.]
ISIK ET AL.
1564 HEAD & NECK—DOI 10.1002/HED NOVEMBER 2012

FIGURE 2. Diagram of lower lip cancer reconstruction with a unilateral transposition flap and myomucosal advancement flap (MAF) application. (A)Preoperative anatomy of the lip, (B) appearance of the lower lip defect and planning of the operation (dotted lines indicate the MAF, straight linesindicate the skin flap), (C) view of the myomucosal flap advancement, preserving at least a 0.5 cm lateral portion of the orbicularis oris muscleafter MAF harvesting, (D) suturation of the myomucosal flaps, (E) suturation of the transposition flap onto the defect region, (F) postoperativeappearance, (G) postoperative anatomic appearance of the orbicularis oris muscles and mental nerve. [Color figure can be viewed in the onlineissue, which is available at wileyonlinelibrary.com.]
FIGURE 3. Lower lip reconstruction with myomucosal advancement flap (MAF) and a bilateral rotation flap in a patient with lower lip cancer. (A)Appearance of preoperative lower lip cancer in a patient (line indicates the planned excision; mucosal invasion is seen in the small photo), (B) viewof the near-total lower lip defect, (C and D) appearance of the left and right harvested MAF with total cancer excision consisting of mandibularperiosteum, (E and F) suturation of the myomucosal flaps to each other and testing of the vermillion reconstruction, (G) appearance of the keysuture in the skin rotation flaps (the dotted line shows the planned excision of the excess skin in the skin flaps), (H) final appearance of thereconstructed lower lip at end of the surgery. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
MYOMUCOSAL ADVANCEMENT FLAP
HEAD & NECK—DOI 10.1002/HED NOVEMBER 2012 1565

line may lead to full-thickness wound dehiscence or oro-cutaneous fistula formation. Another disadvantage of thisapproach is the risk of causing a vertical scar on thelower lip, which, in time, has the potential to lead to acontracture or notching at the midline. In 2007, Koc etal24 performed lower lip repair with z-plasty to preventscar contracture. In the technique described in the presentarticle, mucosa and skin repair lines did not superimpose,and the risk of postoperative fistulization and scar con-tracture after lower lip reconstruction was decreased.Accordingly, in this trial, wound dehiscence was seenalong the skin repair line in 1 patient with complicationsand along the mucosal repair line in the other, but thesecomplications did not lead to complete dehiscence alongthe repair line.
The most important indicator of a functional lower lipreconstruction is restoration of the oral sphincter function.In patients with lower lip defects involving less than 70%of the lower lip, this function can be restored by a num-ber of techniques, but in extensive defects, the number ofsurgical techniques restoring oral sphincter function islimited. Tobin25 tried to restore oral functions by using
the bilateral depressor anguli oris muscle in near-totallower lip defects. However, in the procedure described byTobin,25 a mimic muscle that has a key role in oral func-tions is sacrificed. In lower lip skin reconstructions per-formed either by using free flaps, by transferring freemuscle flaps together with skin flaps,12,13 or through re-position of adjacent muscles,26–28 restoration of oralsphincter function is attempted. Despite the fact thatlower lip reconstruction with free flaps is an importantoption in total lower lip defects, at sites further awayfrom the peripheral tissue, the color, thickness, and hairi-ness of the transferred tissue may be different, and theaesthetic result of reconstruction is poor. However, syn-chronization between the oral muscles and the musclestransferred as free flaps is not clear. Unsatisfactory aes-thetic and functional results and the need for microsur-gery equipment and an experienced team are serious dis-advantages of the techniques involving free flaps. In thisarticle, a local reconstruction option has been presentedfor near-total or total lower lip defects. In terms of aes-thetic and functional outcomes, this novel techniqueseems to be superior to total or near-total reconstruction
FIGURE 4. (A) Postoperative photo of the patient in Figure 3 1 year after the surgery with acceptable neutral positioning, (B) sphincter function, (C)and maximal mouth opening. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
FIGURE 5. Diagram showing lower lip reconstruction with a unilateral transposition flap and myomucosal advancement flap (MAF). (A) Planning ofthe operation and the appearance of the cancer, (B) appearance of a 50% defect in the lower lip after cancer removal, (C) view of the harvestedMAFs, (D) final appearance of the reconstructed lower lip at the end of the surgical operation, (E, F, G and H) photos of the patient 6 months afterthe surgery show normal function of the lip. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
ISIK ET AL.
1566 HEAD & NECK—DOI 10.1002/HED NOVEMBER 2012
involving free flaps. On the other hand, in very extensivetissue defects where the peripheral anatomic regions ofthe cheek or the mentum are also affected, it seems thatdistant tissue transfer remains the best reconstructionoption.
An MAF is a horizontal musculomucosal advancementflap that is prepared from the lower lip mucosa with thepedicle portion in the cheek mucosa. While the orbicula-ris oris muscle is advanced, a maximum of 1 cm of thismuscle is excised between the upper and lower lip withan incision in the modiolus. Although the internal musclefibers of the orbicularis oris adjacent to the vermillion areexcised, the external fibers remain intact; therefore, theoral sphincter function can be restored. Mucosal recon-struction with an MAF and closing of the skin using askin flap prevents microstomia in these patients. Espe-cially in extensive lower lip defects, if the modiolus mu-
cosa is not included in the advancement flap while themucosa is advanced or skin defect is primarily restored,the risk of microstomia is increased. In the current study,the patients gave a score of 4 of 5 points to the postoper-ative mouth opening compared to preoperative mouthopening. According to this result, mouth opening afterthis surgery is sufficient.
The modiolus is a functional and aesthetic unit of themouth to which a number of mimic muscles providing upper,lower, and lateral movements are attached. In a number oflower lip reconstruction techniques, destruction of the ana-tomic features of the modiolus is avoided. On the other hand,in techniques involving Karapandzic and Gillies fan flaps andEstlander flaps, the anatomic localization of the modiolus isdisplaced.5,9,11 Additional interventions are required in theseprocedures to restore the localization of the modiolus. DuringMAF, the mucosa of the modiolus is transferred with the
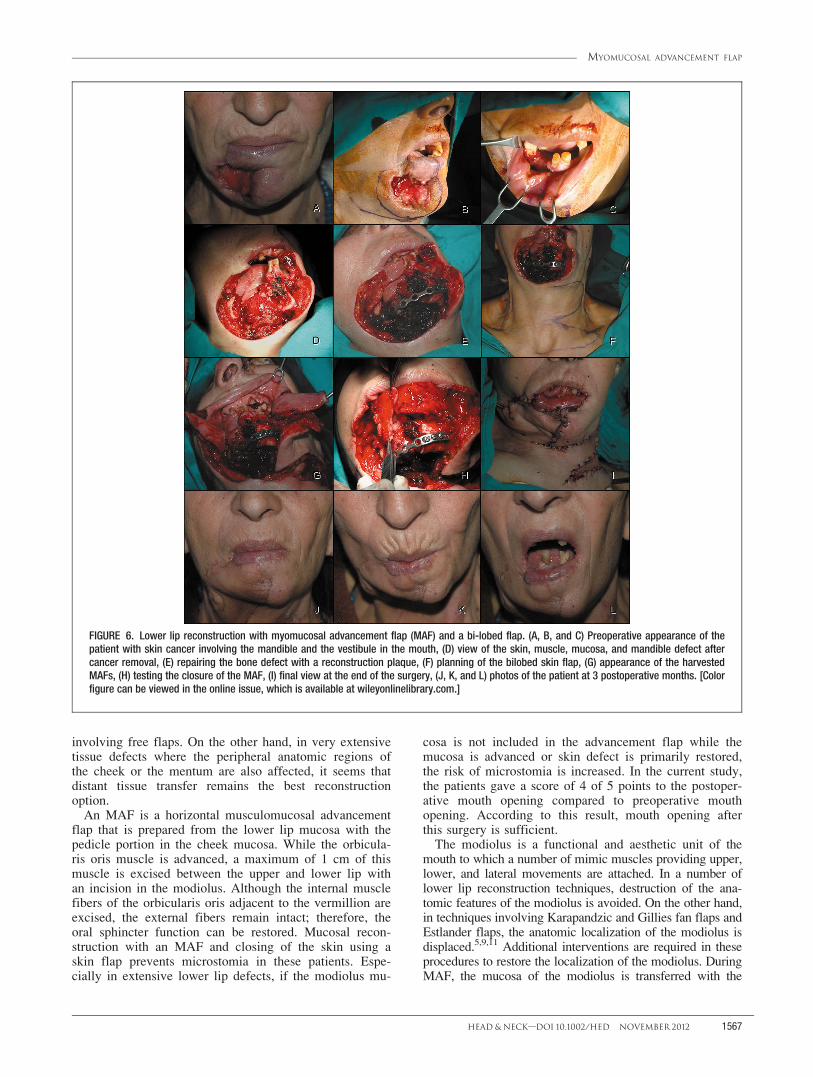
FIGURE 6. Lower lip reconstruction with myomucosal advancement flap (MAF) and a bi-lobed flap. (A, B, and C) Preoperative appearance of thepatient with skin cancer involving the mandible and the vestibule in the mouth, (D) view of the skin, muscle, mucosa, and mandible defect aftercancer removal, (E) repairing the bone defect with a reconstruction plaque, (F) planning of the bilobed skin flap, (G) appearance of the harvestedMAFs, (H) testing the closure of the MAF, (I) final view at the end of the surgery, (J, K, and L) photos of the patient at 3 postoperative months. [Colorfigure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
MYOMUCOSAL ADVANCEMENT FLAP
HEAD & NECK—DOI 10.1002/HED NOVEMBER 2012 1567

orbicularis oris muscle, but the depressor anguli oris muscleis dissected from the modiolus and left in place. Othermuscles providing motility to the modiolus with lateral andsuperior localization are outside the surgical intervention areaand therefore not affected. As a result, in this technique, allmuscles providing motility to the modiolus are preserved intheir anatomic localizations. In this study, the patientsreported that their oral functions (talking, whistling, andlaughing) and aesthetic results were sufficient; lip movementassociated with talking was given the highest score (4.26points).
Another important issue in lower lip reconstruction isthe innervation of the lower lip mucosa. Uninnervatedlips are prone to trauma caused by teeth. In the local neu-romusculocutaneous advancement flap described forlower lip reconstruction described by Turgut et al,4 theauthors created an incision in the mucosa starting fromthe lower lip vestibule, and they advanced the skin, mus-cle, and mucosa as a composite flap along the midlinewhile preserving the mental nerve. As a result, they pro-vided sensorial innervation of the newly formed lowerlip. Moschella and Cordova29 reported that preserving themental nerve is required in lower lip reconstruction; incases in which it cannot be preserved, lower lip innerva-tion may be provided by the buccal nerve. The mentalnerve innervates the vermillion and the lower lip mucosain the oral mucosa, while the commissura region and themucosa of the cheek are innervated by the buccal nerve.30
In the technique described in this article, the mental nervethat innervates the lower lip mucosa is preserved. Themucosa region is only innervated by bilateral excision ofthe mental nerve in patients with extensive defects. Inthese patients, sensorial innervation of a random patternof myomucosal flaps harvested from both cheeks forlower lip mucosal reconstruction is provided by the buc-cal nerve instead of the mental nerve; therefore, no senso-
rial innervation deficiency is observed in the newlyformed lower lip mucosa. In the presented study, thepatients gave a mean score of 3.93 points out of 5 topostoperative lower lip sensation. In patients with lowerlip cancer adjacent to 1 of the lip commissures, the lowerlip mucosa innervated by the mental nerve is excised uni-laterally. In these cases, the myomucosal flap harvestedfrom the cheek adjacent to the defect is innervated by thebuccal nerve, whereas the myomucosal flap harvestedfrom the healthy side of the mouth is innervated by themental nerve. As a result, sensorial innervation of thelower lip is restored.
CONCLUSIONA lower lip reconstruction technique that can be used
to repair lower lip defects of any size has been describedin this study. In this technique, the myomucosal regionand the skin of the lower lip are reconstructed with sepa-
rate flaps. During the transfer of these flaps to the recipi-
ent area, suture lines are not superimposed, reducing the
risk of complications such as orocutaneous fistula, full-
thickness wound dehiscence, scar contracture, and notch-
ing. We believe that this technique is a promising option
for aesthetic and functional lower lip reconstruction.
REFERENCES1. Cruse CW, Radocha RF. Squamous cell carcinoma of the lip. Plast
Reconstr Surg 1987;80:787–791.2. Wechselberger G, Gurunluoglu R, Bauer T, Piza–Katzer H, Schoeller T.
Functional lower lip reconstruction with bilateral cheek advancementflaps: revisitation of Webster method with a minor modification in thetechnique. Aesthetic Plast Surg 2002;26:423–428.
3. Mazzola RF, Lupo G. Evolving concept in lip reconstruction. Clin PlastSurg 1984;11:583–617.
4. Turgut G, Ozkaya O, Kayali MU, Tatlidede S, Huthut I, Bas L. Lower lipreconstruction with local neuromusculocutaneous advancement flap. JPlast Reconstr Aesthet Surg 2009;62: 1196–1201.
5. Lesavoy MA, Smith AD. Lower third face and lip reconstruction. In:Mathes SJ, editor. Plastic Surgery. Philadelphia: Saunders Elsevier; 2006.pp 799–858.
6. Faulhaber J, G�eraud C, Goerdt S, Koenen W. Functional and aestheticreconstruction of full-thickness defects of the lower lip after tumor resec-tion: analysis of 59 cases and discussion of a surgical approach. DermatolSurg 2010;36:859–867.
7. Johanson B, Aspelund E, Breine U, Holmstrom H. Surgical treatment ofnon-traumatic lower lip lesions with special reference to the step tech-nique. A follow-up on 149 patients. Scand J Plast Reconstr Surg 1974;8:232–240.
8. Andrews EB. Repair of lower lip defects by the Hagedorn rectangular flapmethod. Plast Reconstr Surg 1964;34:27–33.
9. Karapandzic M. Reconstruction of lip defects by local arterial flaps. Br JPlast Surg 1974;27:93–97.
10. Webster RC, Coffey RJ, Kelleher RE. Total and partial reconstruction ofthe lower lip with innervated musclebearing flaps. Plast Reconstr SurgTransplant Bull 1960;25:360–371.
11. Boutros S. Reconstruction of the lips. In: Thorne CH, editor. Grabb &Smith’s Plastic surgery. Philadelphia: Lippincott Williams & Wilkins;2007. pp 367–374.
12. Ueda K, Oba S, Ohtani K, Amano N, Fumiyama Y. Functional lower lipreconstruction with a forearm flap combined with a free gracilis muscletransfer. J Plast Reconstr Aesthet Surg 2006;59:867–870.
13. Ninkovic M, Spilimbergo SS, Ninkovic M. Lower lip reconstruction:introduction of a new procedure using a functioning gracilis muscle freeflap. Plast Reconstr Surg 2007;119:1472–1480.
14. Serletti JM, Tavin E, Moran SL, Coniglio JU. Total lower lip reconstruc-tion with a sensate composite radial forearm-palmaris longus free flap anda tongue flap. Plast Reconstr Surg 1997; 99:559–561.
15. Vaughan ED. The radial forearm free flap in orofacial reconstruction. Per-sonal experience in 120 consecutive cases. J Craniomaxillofac Surg 1990;18:2–7.
16. Yildirim S, Gideroglu K, Aydogdu E, Avci G, Akan M, Ak€oz T. Compos-ite anterolateral thigh-fascia lata flap: a good alternative to radial forearm-palmaris longus flap for total lower lip reconstruction. Plast Reconstr Surg2006;117:2033–2041.
FIGURE 7. Application of the myomucosal advancement flap(MAF) and bilateral transposition technique in a patient with lipcancer involving the total lower lip. [Color figure can be viewed inthe online issue, which is available at wileyonlinelibrary.com.]
ISIK ET AL.
1568 HEAD & NECK—DOI 10.1002/HED NOVEMBER 2012

17. Cruse CW, Radocha RF. Squamous cell carcinoma of the lip. PlastReconstr Surg 1987;80:787–791.
18. Wechselberger G, Gurunluoglu R, Bauer T, Piza–Katzer H, Schoeller T.Functional lower lip reconstruction with bilateral cheek advancementflaps: revisitation of Webster method with a minor modification in thetechnique. Aesthetic Plast Surg 2002;26: 423–428.
19. Roldan JC, Teschke M, Fritzer E, et al. Reconstruction of the lower lip: ra-tionale to preserve the aesthetic units of the face. Plast Reconstr Surg2007;120:1231–1239.
20. Mutaf M, Sens€oz O, Ustuner ET. The split-lip advancement technique(SLAT) for the treatment of congenital sinuses of the lower lip. PlastReconstr Surg 1993;92:615–620.
21. Lane JE, Kent DE. Repair of vermilion Mohs defect with unilateralaxial myocutaneous advancement flap. Dermatol Surg 2007; 33:1502–1504.
22. Robotti E, Righi B, Carminati M, et al. Oral commissure reconstructionwith orbicularis oris elastic musculomucosal flaps. J Plast Reconstr Aes-thet Surg 2010;63:431–439.
23. Ducic Y, Athre R, Cochran CS. The split orbicularis myomucosal flap forlower lip reconstruction. Arch Facial Plast Surg 2005;7: 347–352.
24. Koc MN, Orbay H, Uysal AC, Unlu RE, Sensoz O. Z plasty closure of lowerlip defects after tumor excision J Craniofac Surg 2007;18:1120–1124.
25. Tobin GR. Functional lower lip and oral sphincter reconstruction with in-nervated depressor anguli oris flaps. In: Strauch B, Vasconez LO,Hall–Findlay EJ, editors. Grabb’s Encyclopedia of Flaps. Boston: Little,Brown and Company; 1990. pp 665–669.
26. Yamauchi M, Yotsuyanagi T, Yokoi K, Urushidate S, Yamashita K,Higuma Y. One-stage reconstruction of a large defect of the lower lip andoral commissure. Br J Plast Surg 2005;58:614–618.
27. Shinohara H, Iwasawa M, Kitazawa T, Kushima H. Functional lip recon-struction with a radial forearm free flap combined with a masseter muscletransfer after wide total excision of the chin. Ann Plast Surg 2000;45:71–73.
28. Kushima H, Iwasawa M, Kiyono M, Ohtsuka Y, Hataya Y. Functionalreconstruction of total lower lip defects with a radial forearm free flapcombined with a depressor anguli oris muscle transfer. Ann Plast Surg1997;39:182–185.
29. Moschella F, Cordova A. ‘‘Depressor flaps’’ for large defects of the lowerlip and mental region. Plast Reconstr Surg 2005;115: 252–256.
30. Larrabee WF Jr, Makielski KH, Henderson JL. Surgical anatomy of theface. Philadelphia: Lippincott Williams & Wilkins; 2004.
MYOMUCOSAL ADVANCEMENT FLAP
HEAD & NECK—DOI 10.1002/HED NOVEMBER 2012 1569





























