Embed Size (px)
Citation preview

Recommendations for Professional Physical Therapy Curricula for the Foot and Ankle
Clinical Sciences Matrix
Primary Content
Terminal Behavioral
Objectives
After the completion of the
content, the student will be able
to…
Example Instructional
Objectives for the classroom
Example Instructional
Objectives for the Clinic
Screening
General Constitutional signs
Fatigue
Fever
Malaise
Weight change
Musculoskeletal
Fractures
Ottawa ankle
Rules
Avulsion
Severe pain with
weight bearing
Non-mechanical pain
Systemic arthritides
(i.e. gout)
Rheumatic Diseases
Neurological
• Dermatomal versus
non-dermatomal (i.e.
stocking glove)
o Sensation
Select appropriate screening
examination for the
integumentary, cardiopulmonary,
neurological and musculoskeletal
body systems to screen for
conditions beyond the scope of
PT practice that require a referral
to another health care provider.
Recall and identify the clinical
signs and patient response to
written and verbal questions
which indicate health
conditions beyond the scope of
PT practice.
Simulated case examples to
recognize selected
components.
Apply results of written and
verbal responses to a review of
systems with subjective and
objective clinical exam
findings to make the
determination that the patient
is:
1. appropriate for PT
2. is appropriate for PT
with referral
3. not appropriate for PT
and requires referral
elsewhere.
testing 5.07
monofilament
testing
o Vibration - 128
Hz
Myotomal patterns of
weakness versus
peripheral nerve
injuries (i.e. common
fibular nerve lesion)
Cardiopulmonary
DVT - screening
WELLS Criteria.
Riddle et
Peripheral vascular
disease
Integumentary
Infection
open wounds
post operative wounds
abnormal skin and nail
inspection
Psychosocial
depression
alcohol use
Examination

Patient/Client history and
review of medical record
utilizing the domains of the
ICF model
System reviews based on
patient/client needs
Use of Standard Tests and
measures from Guide to PT
Practice
Specific to the Foot and Ankle
Region:
Red flags (specific to F&A)
1. night sweats
2. sleep disturbance
3. change in neurologic
function
4. change in
neurological status -
progressive weakness
and/or sensatory
changes
Yellow flags
Diabetes - Charcot foot
Progressive neurologic
change - progressive
weakness and/or sensation
changes
Determine the Severity,
Irritability, Nature and Stage of
the complaint of the patient and
understand their relevance in the
domains of the ICF model.
recognize the components of the
subjective examination that may
be part of the medical diagnosis
and PT diagnosis to distinguish
the b ----- s______ f______
(BSF) impairments that require
assessment.
Select appropriate systems
examination techniques for the
integumentary, cardiopulmonary,
neurological, and
musculoskeletal systems to assist
in the progression to the specific
PT examination procedures,
diagnosis, prognosis, and
treatment plan
The student will describe the
components of the subjective
examination and how the
subjective examination
questions relate to the domains
of the ICF model.
The student will generate
(synthesis) a complete
subjective examination to
determine the local, remote,
referred, or systemic origins of
the patient’s complaint.
The student will recall the
components of the screening
examination and correctly
performs a screening
examination to determine the
local, remote, referred, or
systemic origins of the
patient’s complaint.
By the final clinical
experience, the student will
perform a subjective patient
examination rated at entry-
level by the clinical instructor
on the CPI
The student will compare and
contrast the findings of the
subjective examination to help
determine if the patient is:
4. appropriate for PT
5. is appropriate for PT
with referral
6. not appropriate for PT
and requires referral
elsewhere.
The student determines the
appropriate tests and measures
for the screening specific to
the foot and ankle.
Comment [S3]: Subjective exam alone will not be sufficient to make the tx
vs refer determination.
Comment [S2]: I believe in PT Guide terminology a systems review is
decidedly different than the regional MS screen
Comment [S1]: These are also noted under red flags. Should it be under just one heading?

DVT - screening WELLS
Criteria. Riddle et al
Inspection/Observation
Swelling - Figure 8 test,
circumference measures,
Pitting edema - yes or no
Integument -
Color and texture:. Noting
discoloration, shiny and or
ecchymosis.
Toe nails noting whether they
are dystrophic and thickened.
Temperature - hot or cold,
sweat response
Trophic changes - hair growth -
vascular problems
Calluses: formation or lack of
calluses, exostosis and boney
overgrowth
Perform an inspection of the feet
and ankles that includes noting
and assessing when appropriate:
1. swelling
2. integument
a. color texture
b. toe nails
c. temperature
d. trophic changes
e. calluses
Correlate inspection findings
with other exam findings when
determining assessment and plan
of care
The student will:
Identify clinical signs of
inflammation in the foot and
ankle.
Identify signs of a reduced
autonomic response in the foot
and ankle. (insert picture)
Identify signs of vascular
compromise (insert picture)
Identify signs of infection and
other integumentary problems
Determine when to refer
simulated patients to another
healthcare provider for
integumentary problems of the
foot and ankle
Interpret and integrate
inspection and observation
results into assessment and
plan of care of patients with
foot and ankle dysfunction
Comment [S4]: Patient first language is generally accepted but not required.

Foot Posture
Assessments/deformity
Foot Posture
Foot Posture Index
Weight bearing and non-
weight bearing visual
assessment of hindfoot
varus and valgus
Forefoot
Too many toes sign
Medial longitudinal arch height
(visual or navicular height)
Toe deformities:
Hallux valgus
Hammer toe
Claw toe
Mallet toe
Overlapping/crossover
Morton's foot structure (2nd toe
longer than the 1st)
Metatarsus adducts
explain, conduct, and interpret
measures of foot posture
including:
Foot Posture Index
Visual assessment of foot posture
(weight bearing and non-weight
bearing)
identify and explain the following
foot and ankle deformities:
• Hallux valgus
• Hammer toe
• Claw toe
• Mallet toe
• Overlapping/crossover
toes
• Morton's foot structure
(2nd toe longer than the
1st)
• Metatarsus adductus
Correlate foot posture assessment
findings with other exam findings
when determining assessment
and plan of care
The student will:
perform and apply the Foot
Posture Index to assess foot
posture
identify foot pronation and
supination postures in weight
bearing and non-weight
bearing
identify and describe various
foot deformities
The student will correctly
perform, interpret, and
integrate foot posture and
deformity clinical findings
with the assessment and plan
of care of patients with foot
and ankle dysfunction

Movement Analysis
Gait assessment
• Spatiotemporal
measures
• Specific Visual
Analysis Rancho Los
Amigos method
• Common gait
deviations related to the
ankle and foot (see
appendix Gait)
• Gait speed
• Stairs
Double Leg squats
• DF ROM
• Visual analysis
hindfoot, midfoot and
forefoot movement
Single leg squats
• LE alignment - note
femoral
adduction/internal
rotation vs. femoral
abduction/external
rotation
Perform a gait assessment
Determine demonstrated gait
deviations
Correctly identify normal vs.
abnormal motions of the ankle
and foot during the double leg
squat test
Correctly identify normal vs.
abnormal motions of the entire
LE during the single leg squat
test
Correlate movement analysis
findings with other exam findings
when determining assessment
and plan of care
The student will:
Describe key components of a
gait assessment
Identify and describe gait
deviations performed by a
simulated patient or patient
video
Perform gait assessment
efficiently with a classmate
Explain the rationale for
selection of various gait
assessment procedures based
on setting, severity, intensity,
nature and stage
Describe key components of
movement in the double and
single leg squat tests
Perform double and single leg
squat tests with a classmate
Identify deviations performed
by a simulated patient or
patient video during the
double and single leg squat
tests
The student will:
Perform gait assessment with a
patient
Identify and document gait
deviations demonstrated by a
patient
Select appropriate gait
assessment procedures specific
to the patient condition and
setting
integrate gait assessment
findings with other tests and
measures and patient
functional status
Discriminate patients
appropriate for double and
single leg squat testing
Perform double and/or single
leg squat test
Identify and document
movement patterns
demonstrated by a patient on
double and/or single leg squat
test

Running
Range of Movement
Ankle Dorsiflexion
Weight bearing
Knee to wall- Distance of
toe to wall or inclinometer
Knee straight - inclinometer,
(consider block for forefoot)
Non-weight bearing
Knee straight - Supine
Goniometry (Di Giovanni,
Norkin & White 2003)
Ankle Plantar flexion
Non Weight bearing
Supine goniometry with the
distal arm aligned with the
inferior aspect of calcaneus
Select the most appropriate
ROM measurement for
examination.
Correctly perform selected tests
and measures
Correctly interprets objective
measurement findings
Identifies the need for potential
test and measure modification
based on setting, severity,
intensity, nature and stage
Discriminates valid and reliable
The student will:
Identify various tests and
measures to thoroughly assess
patient impairments
Describe the procedural
components for measuring
range of motion
Relate the anatomic structures
being assessed by specific
ROM measures
Identify common procedural
errors when performing ROM
measurement
The student will:
Perform ROM examination
measures on a patient
Perform ROM tests and
measures efficiently
Provide rational for ROM tests
and measures selected
Conducts self assessments of
psycho-motor skills and
modifies performance based on
feedback

(old article Steve said)
Subtalar Inversion/Eversion
Non-weight bearing prone -
inversion/eversion observe
qualitatively and/or
goniometry.
Foot Inversion/eversion
Non-weight bearing supine -
supine distal arm aligned with
the 2nd metatarsal (citation
from Martin) (Norkin &
White)
Hallux dorsiflexion-
Non-weight bearing or
Weight bearing
(DNawoczenski, 200?)
Medial longitudinal arch -
Weight bearing - Navicular
drop test
Midfoot motion
(Calcaneocuboid and
talonavicular joints)
Non-weight bearing
- assess forefoot movement
when the rear foot is everted
and inverted. A normal test is
when the foot is inverted and
stability increases (i.e. less
ROM tests and measures
Correctly identifies joint end
feel / motion barriers with
passive motion assessment
Perform an examination of a
student in the classroom
simulating ROM restrictions
Provide a rational for choice of
ROM measures selected
Correlates findings of ROM
measures to identified
abnormal motion patterns
Conducts self assessments of
psycho-motor skills and
modifies performance based on
feedback.
Analyze and discuss a patient-
client video to identify
modifications to ROM testing
based on patient condition and
setting
Comment [S5]: Need reference
Comment [S6]: Reference

Strength Assessment
Manual Muscle testing(MMT)
Ankle plantar
flexion/dorsiflexion/inversion/e
version/toe flexion/extension
Hip/knee/trunk as indicated
by movement analysis
to demonstrate competence in
performing MMT of the foot
and ankle
demonstrate the ability to
conduct and interpret heel raise
tests (single leg and double leg).
describe and administer sports
The student will:
interpret MMT and correlate
findings with simulated foot
and ankle conditions
interpret heel raise test results in
video clips of patients with foot
and ankle dysfunction
The student will:
analyze MMT tests of the foot
and ankle in patients with foot
and ankle dysfunction
discriminate modifications to
assessment of muscle strength
based on a patient’s pathology,
irritability, and/or severity.
forefoot movement is noted).
Accessory Joint Movement
Talocrural - posterior glide
test,anterior/posterior glides
/distraction
Subtalar- medial/lateral/anterior
glides/distraction
Talonavicular joint -
dorsal/plantar gliding
Calcaneocuboid -
dorsal/plantar gliding
First Ray mobility - dorsal
/plantar movement
Distal tibiofibular -
anterior/posterior gliding
Interphalangeal and Metatarsal
phalangeal joints -
distraction/dorsal/plantar
gliding
Discriminate mobility findings
as hypomobile, hypermobile or
within normal limits.
Synthesize information from
ROM assessment and accessory
movement testing to identify
bony versus soft tissue
restrictions
Correlate ROM and mobility
assessment findings with other
exam findings when
determining assessment and
plan of care
Describe the relationship of
rear foot to forefoot
biomechanical axes and it
influence on joint mobility and
stability
Perform mobility testing for the
joints listed for hypomobility
/normal/hypermobility to
determine the potential for
manual therapy interventions
Correctly interpret findings of a
joint mobility assessment on a
classmate
Conducts self assessments of
psycho-motor skills and
modifies performance based on
feedback.
Perform accessory joint
mobility assessment measures
on a patient
Perform accessory motion
safely and efficiently
Provide rational for accessory
motion assessment.
Conducts self assessments of
psycho-motor skills and
modifies performance based on
feedback.

Heel Rise Test - assessed for
height, number of reps, rear
foot inversion or eversion
position, medial versus lateral
forefoot pressure, arch height,
and comparison to normative
data
Functional strength/return to
activity
specific tests for return to play
describe and administer
functional tests for return to
work
to describe and perform
functional tests associated with
the foot and ankle including:
1) squats
2) step ups
3) hopping
Correlate strength assessment
findings with other exam
findings when determining
assessment and plan of care
discuss when to apply various
MMT of the foot and ankle
depending patients pathology,
irritability, and/or severity
discuss the reliability and
validity issues associated with
MMT of the foot and ankle.
discuss the cause of muscle
weakness in conditions
associated with the foot and
ankle (secondary result of
disuse or direct result of injury).
generate hypotheses to address
the probability a detected
weakness is directly caused by
the pathology or is the result of
a secondary effect (i.e. disuse).
Special Tests
Ankle -
• Talocrural sprain
o anterior drawer
o talar tilt
• Syndesmotic sprain -
o dorsiflexion/ext
ernal rotation
o squeeze
Tinel sign
Windlass test
Ottawa(recent version) Foot
select, perform, and interpret
appropriate clinical special tests
to assist with assessment of foot
and ankle conditions
Correlate special test findings
with other exam findings when
determining assessment and
plan of care
The student will:
describe the procedural
components foot and ankle
clinical special tests
accurately perform foot and
ankle clinical special tests
discriminate validity and
reliability of selected clinical
special tests
identify common procedural
errors when performing selected
special tests
The student will:
perform clinical special tests
on a patient
interpret special test results for
integration into the assessment
and plan of care
conduct self assessments of
psycho-motor skills and
modifies performance based on
feedback.

and Ankle Rules
Thompson Test
Clinical Prediction Rule for
ankle instability
discriminate the appropriate use
of foot and ankle special tests
for simulated patients
Palpation of Relevant
Structures
NOTE: Connect to relevant
diagnoses
Lateral Structures:
Fibula head/neck/shaft
Fibularis longus/brevis mm
Lateral malleolus
Anterior inferior tibiofibular
joint
Anterior inferior tibiofibular
ligament
Calcaneus
Peroneal tubercle
Calcaneofibular ligament
Fibular tendons
(Longus/Brevis)
Cuboid
Styloid process 5th metatarsal
5th metatarsal base/shaft/head
Sinus Tarsi
Extensor digitorum brevis
Anterior talofibular ligament
Identify key surface anatomical
structures relevant to
patient/client presenting chief
complaint(s).
Prioritize and demonstrate the
ability to apply the basic
concepts of gross anatomy to
the analysis of patient/client
problems related to
musculoskeletal system of the
leg, ankle, and foot.
Differentiate normal vs.
abnormal findings obtained
from surface anatomy
palpation.
Correlate palpation findings
with other exam findings when
determining assessment and
plan of care
The student will:
Discuss normal and potentially
abnormal clinical findings
identified from a palpation
examination given selected
pathological scenarios.
Perform an examination of a
student in the classroom that
includes correct identification
and palpation of relevant
osseous, musculotendinous,
and/or neurovascular structures.
Perform an efficient
examination of a patient/client
with foot/ankle pathology or
complaint.
Conduct a physical
examination using palpation
techniques that contribute to
the formulation of the
differential diagnosis.
Provides written and verbal
communication utilizing
correct terminology and
description for accurate
recording of physical
examination findings.
Conducts self-assessments of
psycho-motor skills and
modifies performance based on
feedback.

Dorsal Structures:
Anterior compartment mm.
Anterior inferior tibiofibular
joint
Anterior inferior tibiofibular
ligament.
Anterior tibialis tendon
Extensor hallucis longus
tendon
Dorsalis pedis artery/pulse
Extensor digitorum longus
tendon
Extensor digitorum brevis m.
Talar neck
Navicular
1st, 2
nd, 3
rd cuneiforms
Metatarsals I-V base/shaft/head
1st metatarsal joint
Medial Structures:
Medial malleolus
Posterior tibialis tendon
Flexor digitorum longus
tendon
Posterior tibial artery/pulse
Deltoid ligament
Talus
Sustentaculum tali
Calcaneonavicular “Spring"
ligament
Navicular tuberosity
1st cuneiform
1st metatarsal base/shaft/head
Abductor hallucis m.
1st MTP joint
Posterior Structures:
Calcaneus
Achilles tendon
Retrocalcaneal bursa
Soleus m
Gastrocnemius m
Plantar Structures:
Calcaneus
Calcaneal fat pad
Calcaneal tubercle (medial)
Plantar fascia/aponeurosis
Metatarsal heads I-V
Sesamoids
Vascular:
-Popliteal Artery
-Posterior Tibial Artery
-Dorsalis Pedis Artery
-Capillary Refill
Link between palpation and
diagnosis. (Categorized above)
Confirmatory - should be done
at the end

Neurologic Examination
Reflexes
Myotome
Tinel's
Tarsal Tunnel Test-
dorsiflexion with eversion
inversion and plantar flexion
(space occupying lesion)
SLUMP/SLR to test for
proximal contribution to the
foot and ankle chief complaint
Understand the proper selection
of the tests and measures is
dependent on:
1. Chief
complaint/subjective
examination
2. Demographics
3. SINS
4. Functional level of
patient
The student will:
Discuss normal and potentially
abnormal clinical findings
identified from each of the tests
used in this area of examination
using clinical scenarios.
Perform these examination
tests correctly and safely
interpret whether neurologic
finding(s) is/are specific to the
foot and ankle condition or
related to another condition of
the LE or body systems .
The student will:
Perform neurologic
examination measures on a
patient
Perform test and measures
efficiently and correctly
interpret results.
Conducts self assessments
psycho-motor skills and
modifies performance based on
feedback.
Interpret and integrate the
results with the assessment and
plan of care.
Balance -
--Romberg – Sharpened
Romberg
--Single leg stance
-----Eyes closed eyes open
-----head neck rotation
-----Surfaces - foam no foam
-----assess for ankle, knee and
hip strategy
Modified Star Excursion
Hop to Stabilization
Understand the proper selection
of the tests and measures is
dependent on:
1. Chief
complaint/subjective
examination
2. Demographics
3. SINS
4. Functional level of
patient
Determines the need for a more
in- depth fall risk assessment in
The student will:
Discuss normal and potentially
abnormal clinical findings
identified from each of the tests
used in this area of examination
using clinical scenarios.
Perform these examination
tests correctly and safely
The student will:
Perform balance measures on a
patient
Perform test and measures
efficiently and correctly
interpret results.
Conducts self assessments of
psycho-motor skills and
modifies performance based on
feedback.

Assessment of falls risk -
BERG, TUG, Tinnetti,
Rickli and Jones
selected patients Interpret and integrate the
results with the assessment and
plan of care.
Lower Quarter Screen (LQS)
Recognize the potential for
referred pain into the foot and
ankle for means of specific
examination of other body
regions, diagnosis, or potential
referral to another healthcare
provider.
The student will:
correctly performthe
components of a lower quarter
screen with a classmate
recognize a referred pain
pattern based on LQS
examination results
The student will:
perform a lower quarter screen
on a patient to rule in /out
referred pain and the need for
specific examination of other
body regions
Evaluation
Diagnosis
PTTD
Describes the continuum of dysfunction
Discriminates between this diagnosis and
pertinent differential diagnoses (rules out
the following):
SPECIFICS?
Describes signs and symptoms,relevant
history and examination including:
• tenderness along the tendon
course
• reduced calcaneal inversion during
heel rise
• weak inversion/ PF
• Abnormal alignment and
Describes the location and
function of the TP and performs
MMT, and palpation of same.
Describes the associated
structural and movement
impairments including heel rise
test and gait deviations.
The student must have
experience practicing clinical
management of a tendinous
structure.
The student describes having
had exposure to an actual
patient, a case study,
simulation of a foot tendon
problem, or related hooked-
on- evidence case.
The student supports
Comment [S7]: Should this follow systems review earlier in the examination
matrix?

movement associated with
pronation
choosing examination items
consistent with severity and
nature of the problem
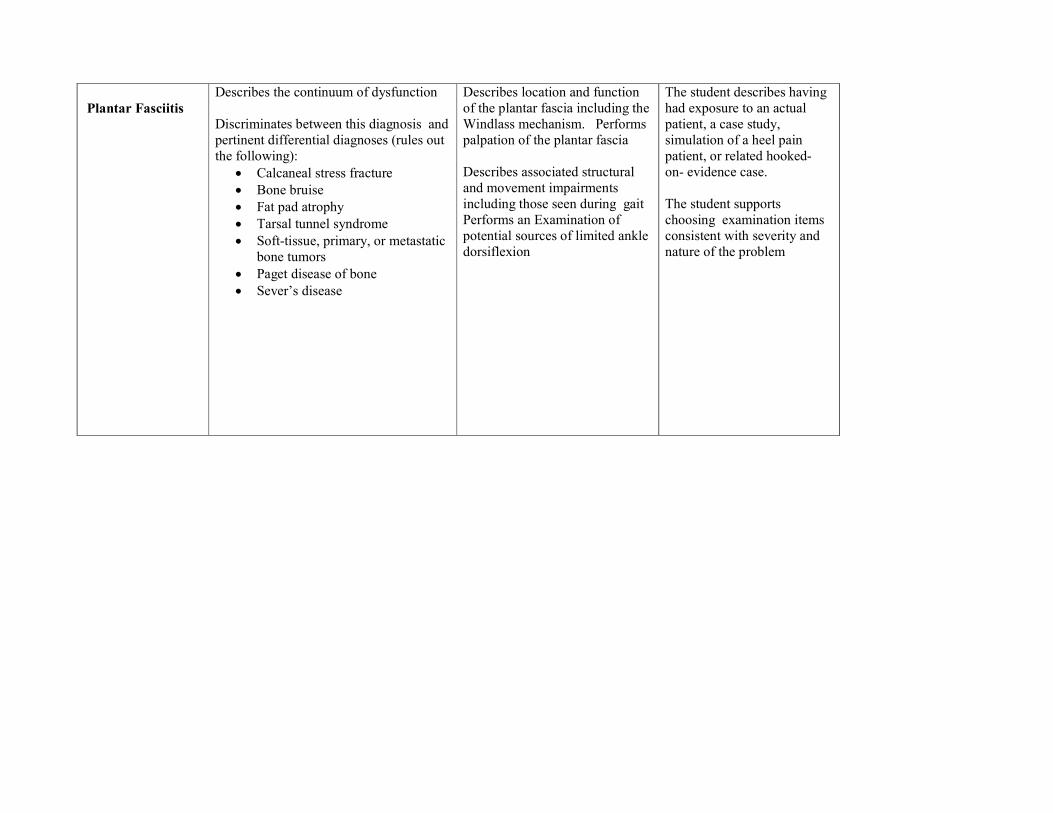
Plantar Fasciitis
Describes the continuum of dysfunction
Discriminates between this diagnosis and
pertinent differential diagnoses (rules out
the following):
• Calcaneal stress fracture
• Bone bruise
• Fat pad atrophy
• Tarsal tunnel syndrome
• Soft-tissue, primary, or metastatic
bone tumors
• Paget disease of bone
• Sever’s disease
Describes location and function
of the plantar fascia including the
Windlass mechanism. Performs
palpation of the plantar fascia
Describes associated structural
and movement impairments
including those seen during gait
Performs an Examination of
potential sources of limited ankle
dorsiflexion
The student describes having
had exposure to an actual
patient, a case study,
simulation of a heel pain
patient, or related hooked-
on- evidence case.
The student supports
choosing examination items
consistent with severity and
nature of the problem

• Referred pain as a result of an S1
radiculopathy
Describes signs and symptoms, relevant
history and examination including:
• Pain upon palpation of the
proximal plantar fascia attachment
• First step pain
1st Toe extension reproduces pain at the
proximal or distal attachment of ? ? PF?
Achilles
Tendinopathy
Describes the continuum of tendinopathy
and progression of symptoms.
Discriminates between this diagnosis and
pertinent differential diagnoses (rules out
the following):
• Acute achilles tendon rupture
• Partial tear of the Achilles tendon
• Retrocalcaneal bursitis
• Posterior ankle impingement
• Irritation or neuroma of the sural
nerve
• Os trigonum syndrome
Describes location and function
of the Achilles tendon. Performs
palpation and functional testing
(heel rise and manual muscle
testing ).
Performs palpation to determine
the anatomical location of the
tendinopathy
Describes the associated
structural and movement
impairments including deviations
The student describes having
had experience in clinical
management of a tendinous
structure
The student supports
choosing examination items
consistent with severity and
nature of the problem
for an actual or simulated
patient/ case study.
(attached. hooked- on-
evidence case)

• Achilles tendon ossification
• Systemic inflammatory disease
• Insertional Achilles tendinopathy
• Boney enlargement on back of the
calcaneus (Haglunds deformity)
Describes signs and symptoms, relevant
history and examination including:
• Localized pain and stiffness
following periods of prolonged
inactivity
• Intermittent pain experienced
during activity and exercise
• Perceived tenderness
and pain upon palpation to the
Achilles tendon
• Positive Achilles Tendon
Palpation Test
• Decreased plantar flexor strength
with
associated either increased or
decreased dorsiflexion A? P?
range of motion
• limited ability to perform
repetitive unilateral heel raises
when compared to the
contralateral side
in: Gait, unilateral heel rise,
single limb hop, or ability to
descend stairs
The student discriminates
between a tendinous lesion
and pertinent differential
diagnoses (rules in/out
tendinous lesion)
Lateral ankle
sprain and
syndesmotic/high
ankle sprain
Describes continuum of dysfunction of
lateral ankle sprains and high
ankle/syndesmotic sprain
Describes the function of the
anterior talo-fibular and calcaneo-
fibular ligaments.
Performs palpation of the
The student describes having
had exposure to an actual
patient, a case study,
simulation of a patient with
ankle sprain or

Describes signs and symptoms, relevant
history and examination including:
- Pain with palpation of the
involved ligaments (ATFL, CFL,
Ant tib-fib lig)
- Mechanism of injury –
inversion/plantarflexion (lateral
ankle sprain) versus dorsiflexion
and eversion (high ankle
sprain/syndesmotic)
- Reproduction of ankle instability
or pain with special tests
Discriminates between this diagnosis and
pertinent differential diagnoses (rules out
the following):
• Peroneal tear
• Medial collateral ligament
ankle sprain
• Lisfranc
Fracture/Dislocation
• Subtalar sprain
• Achilles tendon rupture
• Lateral talar process injury
• Anterior process of the
calcaneus injury
calcaneal-fibular and the anterior
tib-fib ligaments.
Performs a measurement of
swelling of the ankle using the
figure of eight – in 20 degrees of
plantar flexion
Performs a combination of tests
to assess ligament stability
including: talar tilt, anterior
drawer for lateral ankle sprain
and external rotation and squeeze
test for high ankle
sprain/syndesmotic sprain
Describes the Ottawa Ankle
Rules and when to refer a patient
for radiograph
Supports choosing examination
items consistent with severity and
nature of the problem
syndesmotic/high ankle
sprain, or related hooked- on-
evidence case.
Hallux Abducto-
Valgus
Describes the continuum of dysfunction
that can be addressed by a PT
Discriminates between this diagnosis and
Describes the location function
and of the 1st MTP and 1st ray.
Describes the associated
The student describes having
had exposure to an actual
patient, a case study,
simulation of hallux valgus,

pertinent differential diagnoses (rules out
the following):
• sesamoid stress fracture,
• avascular necrosis,
• osteochondral fractures, and
chondromalacia,
• metatarsalgia, nerve impingement,
• infection,
• bursitis,
• sesamoiditis,
• bipartite sesamoids
(Hockenberry99, Dedmond 06).
Describes signs and symptoms, relevant
history and examination including:
• Palpation and observation
including medial eminence
tenderness,
• severity of HAV deformity,
• contribution of shoeware
• static foot type based on standing
alignment
• Gait pattern and weight
acceptance under 1st MTP
structural and movement
impairments including:
• Palpation
• Gait
• Static foot alignment
• 1st MTP ROM
or related hooked- on-
evidence case.
The student supports
choosing examination items
consistent with severity and
nature of the problem.
The student performs an
assessment of the stability of
an MTP joint.
Hallux Limitus
Describes the continuum and etiology of
this dysfunction
Describes signs and symptoms, relevant
history and examination including:
• Limited accessory motion of the
1st MTP and/or ray.
Describes the location function
and of the 1st MTP, sesamoids,
and 1st ray.
Describes the associated
structural and movement
impairments including results of
The student describes having
had exposure to an actual
patient, a case study, a
simulation of hallux limitus,
or related hooked- on-
evidence case.

• Associated proximal alignments
and compensations due to reduced
heel rise in gait and function.
• Atypical function and position of
the sesamoid apparatus
performing:
• palpation
• gait examination
• Static foot alignment
examination
• 1st MTP PROM
examination
• Flexor halluces longus
manual muscle testing
The student supports
choosing examination items
consistent with severity and
nature of the problem.
.
The student performs an
examination of the motion of
the 1st MTP joint.
Metatarsalgia Describes the continuum of dysfunction
and discriminates between this diagnosis
and pertinent differential diagnoses (rules
out the following):
• Interdigital neuroma,
• plantar keratosis,
• Frieberg’s disease,
• Metatarsal stress fracture,
inflammatory arthropathy(such as
rheumatoid arthritis, seronegative
spondyloarthropathy, or
crystalline-induced arthritis),
• tarsal coalition,
• vertical talus,
• or accessory navicular (Omey.
Glasoe 05)
Describes signs and symptoms, relevant
history and examination including:
• Pain upon palpation of the distal
Describes the location and
function of the distal plantar
fascia, FDL, MTP joint capsule,
interdigital nerve and fat pad.
Describes the associated
structural and movement
impairments including results of
performing:
• Palpation
• Gait examination
• Manual Muscle testing of
intrinsic foot muscle
strength
• Mulders test
• Tinel test
The student describes having
had exposure to either an
actual patient, a case study,
simulation of forefoot pain, or
related hooked- on- evidence
case.
The patient supports choosing
examination items consistent
with severity and nature of
the problem.

2-3rd metatarsal heads, plantar
MTP, and FDL.
• Special tests including digital
Lachman, Drawer, or Mulders test
• Pertinent gait abnormality
Shin Splints/Medial
Tibial Stress
Syndrome
Describes signs and symptoms, relevant
history and examination including:
• Pain in the front of the shin.
• A patient who has high use (high
BMI or activity level) and poor
foot alignment.
• Anterolateral lower leg pain is
often associated with the anterior
compartment muscles.
• Anteromedial lower leg pain is
indicative of stress fracture.
Discriminates between this diagnosis and
pertinent differential diagnoses (rules out
the following):
• Compartment Syndrome
• Performs palpation of
anterior compartment
muscles.
• Performs palpation of the
anterior tibia where there
is no muscle coverage.
• Describes and performs
demonstration ofthe
actions of the three
muscles in the anterior
compartment.
• Performs correct stretch
of each muscle in the
anterior compartment
including elongation over
all the joints each crosses.
• Describes when to refer
the patient to orthopaedics
for diagnosis and
management of a potential
stress fracture.
Ankle
Osteoarthritis
(OA)- Non-surgical
Post-op
Describes signs and symptoms, relevant
history and examination including for
Non-surgical ankle OA:
• Pain during and after activity
• Continuum of joint deformity and
loss of motion
Describes the associated
structural and movement
impairments including:
description that surgical
management of OA can include
The students describes having
had experience in the clinical
management of OA.

• Prior history of ankle instability or
trauma
Describes signs and symptoms, relevant
history and examination including for
Post-op OA:
• Obtains relevant information
about surgical or medical
management to identify
indications/contraindications for
examination and intervention
Osteochondral procedures, ankle
replacement, or ankle fusion
(while the current standard of
care is ankle fusion for end stage
OA)
Post-op –Describes and examines
the tissues involved in the injury
and/or surgery including the
influence of time on return to
function
Neuropathic
(Diabetic) Foot • Describes signs and symptoms,
relevant history and examination
including: Loss of protective
sensation on at least on aspect of
the plantar surface of the foot
(generally stocking/glove)
• Signs autonomic system
dysfunction (e.g. hair loss, loss of
sweating)
• Diagnosis that can result in loss of
peripheral sensation (diabetes,
heavy metal, alcohol, idiopathic)
Associated complications:
• Ulcer formation
• Neuropathic Charcot Arthropathy
• Joint deformity
• Impaired balance
• Peripheral vascular
disease/ischemia
• Loss of joint mobility
• Loss of foot bone mineral density
• Delayed bone and tissue healing
Performs the following
examination items in the foot:
• Visual exam of skin and
nails
• Sensory examination of
the foot
• Palpation of pulses
• Passive and active range
of motion
Performs a footwear examination
discriminating between
appropriate and inappropriate
footwear and orthosis
components
Describes deformity and potential
consequences of each deformity
in people with this diagnosis (e.g.
hammer/claw toe, medial and
lateral midfoot and hindfoot
deformity)
The student performs a screen
for diabetes during the history
The student describes and as
appropriate performs
precautions for insensate feet
during examination and
treatment.
The student describes having
had exposure to an actual
patient, a case study,
simulation, or in class patient
lab of an individual with a
neuropathic foot.

Perform examination of need for
assistive device
Calcaneal
Apophysitis
(Sever’s
Disease)/calcaneal
epiphyseal fracture
Describes the continuum and etiology of
this dysfunction
from apophysitis through
epiphyseal fracture
• Explains that this type of
fracture cannot be diagnosed
through x ray, but rather is
made through signs and
symptoms and responses to
management.
• Describes signs and symptoms,
relevant history and examination
including: Pain at the heel;
usually right at the posterior most
tip
• Patient is a child of an age when
their calcaneus has not fully fused
(5-10 years)
• History of high activity level
and/or growth spirt
• Patient stands with heels in
eversion relative to subtalar
neutral
• Describes that this
problem warrants
intervention and that if it
is a fracture it may require
immobilization for eight
weeks followed by rehab
(stretching, strengthening,
balance work etc )
• Describes that the
mechanism of injury is
that the heel cord is tight
and pulls the calcaneal
epiphysis apart.
• Performs appropriate
secondary tests to address
force distribution and
aberrant motion including
fabrication/adaptation of
temporary foot orthoses
and heel lifts to support
medial arch and/or
hindfoot.
Student describes having had
exposure to an actual patient
or a case study of Sever’s
disease that includes its PT
management.

and associated dysfunctions
functional leg length discrepancy
shin splints
proximal compensations and
associated pains and dysfunctions
Fracture (5th
metatarsal,
navicular, midfoot)
Describes signs and symptoms, relevant
history and screening examination
including:
• Pain with palpation
• Inability weight bear for 4 steps
• High incidence of non-union
Describes signs and symptoms, relevant
history and examination related to
medical management including: :
• Obtain relevant information about
surgical or medical management
to identify indications/
contraindications for PT
examination, intervention
Describes signs and symptoms,
relevant history and examination
of fracture when performing
Palpation of boney
structures of the foot and
ankle
Student will describe a timeline
to guide progression of care
following the medical or surgical
management of a fracture.
The student describes having
had experience with the PT
clinical management of a
fracture.
Chronic Ankle
instability/
functional and
mechanical
Describes signs and symptoms, relevant
history and examination related to chronic
(functional and mechanical) ankle
instability including including:
• patients with feelings of
instability,
• impaired balance and
proprioception,
• decreased passive or active range
of motion.
Discriminates between this diagnosis and
Performs balance and
proprioception testing.
Performs a group of tests to
assess stability of ankle
ligaments.
The student describes having
had exposure to either an
actual patient with ankle
instability, a case study, or
simulation of a patient with
chronic ankle instability.
The student supports
choosing examination items
consistent with severity and
nature of the problem.

pertinent differential diagnoses (rules out
the following):
• Peronal tendon pathology
• Accessory ossicles
• Tarsal coalition
• Sinus tarsi syndrome
• Subtalar sprains with or
without instability
• Spring or bifurcate
ligament damage
• Peronal tendon pathology
• Accessory ossicles
• Tarsal coalition
• Sinus tarsi syndrome
• Subtalar sprains with or
without instability
• Spring or bifurcate
ligament damage
• Ankle impingement
Tarsal Tunnel
Discriminates between this diagnosis and
pertinent differential diagnoses (rules out
the following):
• Plantar fasciitis
• Describes signs and symptoms,
relevant history and examination
related to medical management
including: Distal production of
symptoms with tapping (Tinel’s)
of the posterior tibial nerve
pathway.
Performs palpation of posterior
tibial nerve
Performs the Tinel’s and
Provocative Tinel’s tests
The student describes having
had exposure to either an
actual patient, a case study, or
simulation of a foot and ankle
case in which they must
choose to rule out
involvement of the posterior
tibial nerve as a source of
symptoms.

• Symptoms reproduced
with sustained dorsiflexion-
eversion of the foot
• Provocative Tinel’s:
symptoms reproduced during
tapping of the nerve pathway with
the foot in dorsiflexion, maximal
calcaneal eversion, and toes
extended. (Kinoshita M, Okuda
R, Morikawa J et al. The
Dorsiflexion-Eversion Test for
Diagnosis of Tarsal Tunnel
Syndrome. J Bone Joint Surg Am.
2001; 83(12):1835-1839.)
Do we need this first and last bullet?
Equinus related to
any or all of the
following:
• Passive
tightness of
PF
• Dynamic
tightness of
PFors
(spasticity)
• Poorly timed
dorsiflexion
activity
• Weak or
absent
dorsiflexors
Describes signs and symptoms, relevant
history and examination related to medical
management including:
• PROM DF less than 10 with the
knee extended avoiding pronation
• Lack of heel strike during gait
• Early heel off during gait (mild)
• Stands with heels on ground and
pronation or supination, walks on
toes (moderate)
• Stands and walks on toes. (severe)
Discriminates between those
that do, and do not, attain heel
strike during gait.
Describes all the plantar flexor
muscles that could be tight,
active at the wrong time, or
overly shortened.
Performs PROM measurements
of dorsiflexion with and without
pronation, with and without
knee flexion
Describes the likely presence of
initial resistance (R1), verses
ultimate PROM (R2) in patients
The student
describes having
had exposure to an
actual patient or a
case study
involving clinical
management
of an equinus foot
problem including
discriminating
between origins of
the equinus. This
involves
performing,
or describing, an
examination that
discriminates

with spasticity.
between tight
plantar flexor
muscle(s), joint
limitation (s),
poorly timed
plantar or
dorsiflexion, or
excessive plantar
flexion activity.
The student will
discriminate
between
specific situations
when referral is
warranted being
specific as to the
type of referral (PT
with neurological
expertise, to
physiatry
or other MD skilled
in medical
management of
spasticity including
botulinum toxin
injections,
orthopaedic
surgeon,
neurosurgeon,
or orthotist).
Hence, the student

will describe that
which discriminates
a patient with
plantar flexor
spasticity from
other patients.
Foot Supination
Syndrome
• Describes signs and symptoms,
relevant history and examination
including: Related source
diagnosis including tibial stress
fracture, plantar fasciitis,
metatarsal (MT) stress
fracture/Metatarsalgia 1and 5,
sesamoiditis, fibularis
tendinopathy/tear, achilles
tendinopathy, Hallux abducto-
valgus, bunionette, Hallux limitus
• Hindfoot inversion, talo-navicular
elevated, forefoot adduction,
plantarflexion first ray, reduced
lateral arch height, during gait,
hopping, running, and stepping
• Callus formation at 1st and 5
th
metatarsal heads
• Footwear worn on lateral border
• Force distribution and/or
addressing aberrant motion
identified reduces signs and
Descriminates supination during
the stated movements from other
motions
Performs appropriate secondary
tests to address force distribution
and aberrant motion
(verbal/tactile cueing, taping, and
orthosis fabrication and/or use).
The student supports
choosing examination items
consistent with severity and
nature of the problem.
The student discriminates
excessive or poorly timed
foot supination from other
motions during gait in a
patient.
The student must describe
having had exposure to
actual, simulated and/or a
relevant case study of foot
supination syndrome.

symptoms
• Associated proximal alignments
and compensations (functional leg
length discrepancies, lateral
femoral rotation)
Foot Pronation
Syndrome
• Describes signs and symptoms,
relevant history and examination
including: Related source
diagnosis including Medial tibial
stress syndrome , plantar fasciitis,
metatarsal stress
fracture/Metatarsalgia 2/3,
Neuroma, PTTD, Achilles
tendinopathy, Hallux Abducto-
valgus, Hallux Limitus, Fibularis
• Hindfoot eversion, talo-navicular
descent, and forefoot abduction
during gait, hopping, running, and
stepping
• Callus formation at metatarsal
heads 2nd and 3
rd, and medial side
of hallux
• Footwear worn on medial border
of the shoe and under 2nd and 3
rd
metatarsal.
• Correction of abberant motion
identified reduces signs and
symptoms
• Associated proximal alignments
and compensations (functional leg
length discrepancies, medial tibial
and femoral rotation, ?ipselateral
Discriminates pronation during
the stated movements from other
motions.
Performs appropriate secondary
tests to reduce aberrant motion
(verbal/tactile cueing, taping, and
orthosis fabrication and/or use).
The student supports
choosing examination items
consistent with severity and
nature of the problem.
The student discriminates
excessive or poorly timed
foot pronation from other
motions during gait in a
patient
The student describes having
had exposure to actual,
simulated and/or a relevant
case study of foot pronation
syndrome.

pelvic drop)
Prognosis
Plan of Care
Intervention
Therapeutic Exercises
• Balance
• Strengthening
• Stretching
• Endurance
• Select and perform
appropriate therapeutic
exercises
• Demonstrate strategies
for the interventions
• Apply principles of safe
practice to patient/client
care
• Deliver interventions
based on the best
evidence available and
practice guidelines
• Discuss rationale for
selecting specific
therapeutic exercises,
including dosage,
• Demonstrate the ability
to instruct or perform
selected interventions
• Discuss the principles of
exercise progression
• Recognize and be able
to instruct patient on
special interventions for
the foot/ankle, including
(but not limited to):
o Plantar fascia
stretching
o Gastroc stretching,
protecting the mid-
foot
o Foot intrinsic
strengthening
exercises
o Proximal muscle
strengthening
including core, pelvis
• Design, implement, and
progress an appropriate
treatment program
• Monitor patient
response to
interventions and
modify as appropriate
•
and LE
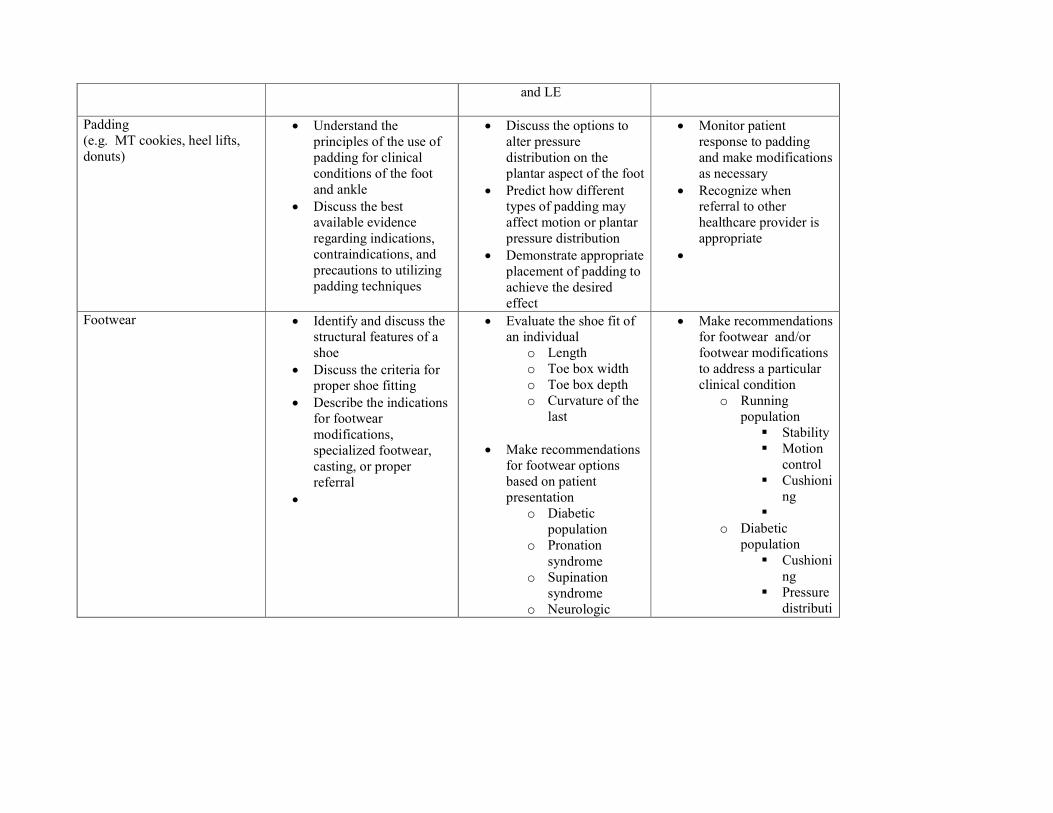
Padding
(e.g. MT cookies, heel lifts,
donuts)
• Understand the
principles of the use of
padding for clinical
conditions of the foot
and ankle
• Discuss the best
available evidence
regarding indications,
contraindications, and
precautions to utilizing
padding techniques
• Discuss the options to
alter pressure
distribution on the
plantar aspect of the foot
• Predict how different
types of padding may
affect motion or plantar
pressure distribution
• Demonstrate appropriate
placement of padding to
achieve the desired
effect
• Monitor patient
response to padding
and make modifications
as necessary
• Recognize when
referral to other
healthcare provider is
appropriate
•
Footwear • Identify and discuss the
structural features of a
shoe
• Discuss the criteria for
proper shoe fitting
• Describe the indications
for footwear
modifications,
specialized footwear,
casting, or proper
referral
•
• Evaluate the shoe fit of
an individual
o Length
o Toe box width
o Toe box depth
o Curvature of the
last
• Make recommendations
for footwear options
based on patient
presentation
o Diabetic
population
o Pronation
syndrome
o Supination
syndrome
o Neurologic
• Make recommendations
for footwear and/or
footwear modifications
to address a particular
clinical condition
o Running
population
� Stability
� Motion
control
� Cushioni
ng
�
o Diabetic
population
� Cushioni
ng
� Pressure
distributi

population
o Arthritic
population
o
• Discuss the rationale for
various features of a
shoe
• Identify the specific
components of a shoe
o Toe box
o Heel counter
o Vamp
o Mid-sole
o Sock liner
on
� Adequat
e toe box
width/
depth
�
• Refer to appropriate
healthcare provider as
necessary
Abnormal Motion
• Excessive Motion
o Bracing
o Strapping
o Foot Orthoses
• Limited Motion
o Mobilization
o Manipulation
• Discuss the rationale
and best available
evidence for each of the
interventions utilized to
control motion
• Discuss indications and
contraindications for
motion control,
including bracing and
strapping
• Recognize the
implications of
interventions on the
various components of
the kinetic chain
• Select and perform
appropriate joint
mobilization techniques
related to limited motion
Excessive Motion
• Describe the indications
and recommendations
for bracing of the foot
and ankle
o AFO
o KAFO
o Boot
o Stirrup
o Lace-up
• Describe the indications
and recommendations
for strapping of the foot
and ankle
o Ankle Instability
� Stirrup
� Basketwe
ave
o
• As available, observe or
participate in the
prescription,
fabrication,
modification, or
dispensing of bracing:
o AFO
o KAFO
o Boot
o Stirrup
o Lace-up

• Discuss the rationale,
indications, and
contraindications for
manipulation
� Heel lock
o Medial Arch
� Low-Dye
� Cross X
� Reverse
Six
o Edema:
Compression
wrap with
pressure gradient
o Musculotendino
us
o support
(Achilles)
• Recognize a patient
(case) where foot
orthotic management
would be appropriate
• Understands the
mechanism by which a
foot orthosis restrains or
encourages motion
• Observe the fabrication,
modification, or fitting
of a foot orthotic
Limited Motion
• Demonstrates correct
hand placement and
technique when
providing grade I-IV
joint mobilizations to all
• As available, observe or
participate in the
prescription,
fabrication,
modification, or
dispensing of a foot
orthosis
o Custom
o Prefabricated
o Accomodative
• Demonstrate proper
technique when
performing at least one
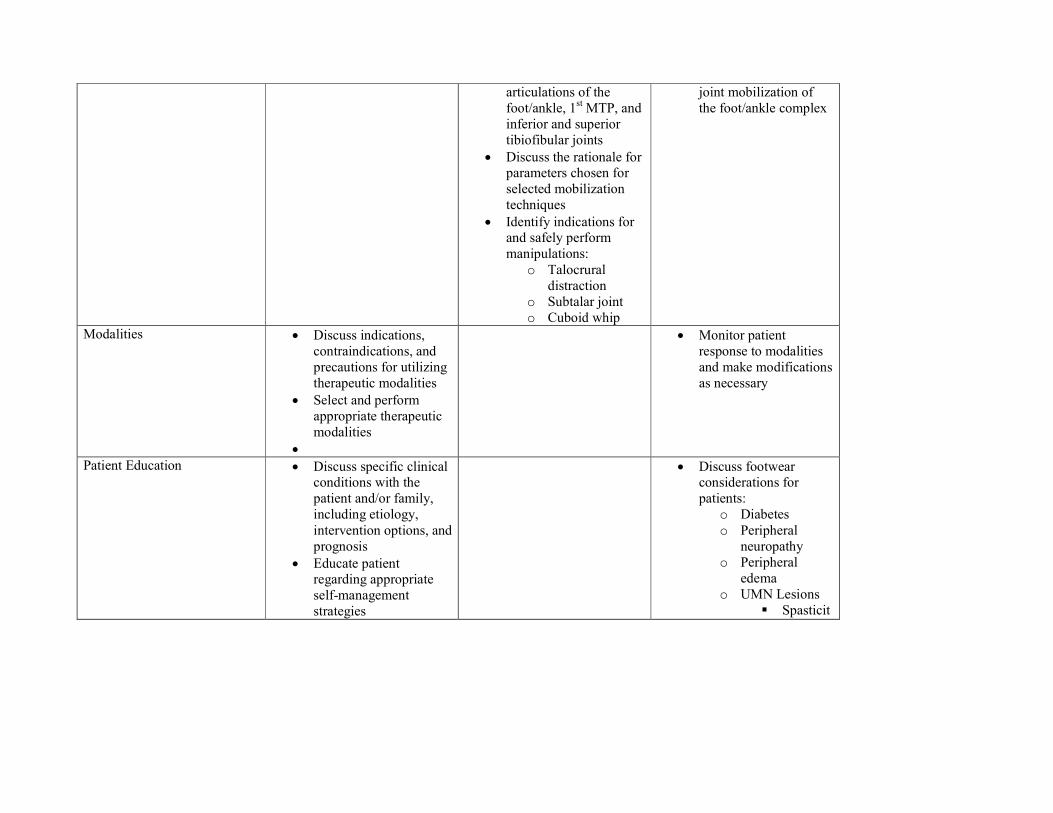
articulations of the
foot/ankle, 1st MTP, and
inferior and superior
tibiofibular joints
• Discuss the rationale for
parameters chosen for
selected mobilization
techniques
• Identify indications for
and safely perform
manipulations:
o Talocrural
distraction
o Subtalar joint
o Cuboid whip
joint mobilization of
the foot/ankle complex
Modalities • Discuss indications,
contraindications, and
precautions for utilizing
therapeutic modalities
• Select and perform
appropriate therapeutic
modalities
•
• Monitor patient
response to modalities
and make modifications
as necessary
Patient Education • Discuss specific clinical
conditions with the
patient and/or family,
including etiology,
intervention options, and
prognosis
• Educate patient
regarding appropriate
self-management
strategies
• Discuss footwear
considerations for
patients:
o Diabetes
o Peripheral
neuropathy
o Peripheral
edema
o UMN Lesions
� Spasticit

• Identify and discuss risk
factors and strategies for
injury prevention
y
� Flaccidit
y
o Trauma
o Arthritic
Conditions
� OA
� RA
o Athletes
Functional Training • •

APPENDICES
Appendix A
Table 18. Average values from various studies for a single heel rise test
Author Sample Average
Repetitions
Technique
Madeley,
2006199
Young athletes
(n = 30)
(mean age 24 ±
5.7 years old)
39 ± 11.7 Strings were used to document heel height and trunk
position. The test was terminated if the participant
leaned forward touching the string at the level of their
pectorals three times, the ipsilateral knee flexed, the
dorsal aspect of the foot did not contact the string for
three consecutive repetitions or the participant could no
longer continue. At this point, the number of heel-rise
repetitions that were performed was documented. One
trial was used for this test.
Lunsford,
1995199
Adults (n =
203)
(mean age men
= 34.7 ± 8.5,
women = 29.3 ±
5.0 years old)
27.9 ± 11.1
Each subject was allowed to touch the examiner with a
single finger for balance. The test was terminated if
the subject leaned or pushed down on the examiner, the
subject's knee flexed, the plantar-flexion range of
motion decreased by more than 50% of the starting
range of motion (measured quantitatively), or the
subject quit or asked to stop.
Jan,
2005143
Adults (n =
180)
(21- 80 years
old)
Male
21- 40 = 22.1 ± 9.8
41- 60 = 12.1 ± 6.6
61- 80 = 4.1 ± 1.9
Female
21- 40 = 16.1 ± 6.7
41- 60 = 9.3 ± 3.6
61- 80 = 2.7 ± 1.5
One examiner provided the finger-touch
support and counted the total number heel rises
accomplished. Another examiner observed the
participant laterally for any extraneous trunk lean or
knee flexion. The third examiner read the
electrogoniometer output on the monitor and
terminated the test if the plantar flexion angle became
less than 50% of the maximum angle.

Appendix B
Gait Velocity:
Normal or
Abnormal
Cause:
NOTES Stride length:
Equal? Yes----NO
If no, what is
cause?
NOTES Cadence:
Normal or
Abnormal
Cause:
NOTES
Task of Gait Weight
Acceptance
Single Limb
Support
Single Limb
Support
Limb
Advancement
Limb
Advancement
Phase of Gait
Reference Limb
Initial Contact
Loading Response
Mid Stance Terminal Stance Pre Swing Initial, Mid,
Terminal Swing
Contralateral
Limb
Pre Swing Initial to Mid
Swing
Mid to Terminal
Swing
Initial Contact
Loading Response
Mid and Terminal
Stance
ROCKER Heel rocker Ankle Rocker Forefoot rocker Forefoot rocker
Ankle: Normal Strikes in relative
DF moves into PF
via foot to ground
faster than tibia
moves forward
From PF into DF of
ankle
DF of ankle reaches
peak of 5-10
degrees
DF to 25 degrees of
PF to assist knee to
flex to shorten limb
Ankle remains in PF
during initial swing,
need knee flexion to
clear the limb
Ankle Abnormal
Common
Findings
1. Uncontrolled PF
2. Low Foot
Contact
3. Forefoot Contact
1. Excessive DF
(knee flexion in
mid stance)
2. Early Heel Rise
3. No forward tibial
progression
1. No heel rise prior
to C/L contact
2. Contact area
more lateral
Lack of PF
KEY: Decreased
knee flexion
Loss of FF rocker
Toe drag Int. Swing
Failure to achieve
neutral ankle for IC
Foot: Normal Foot pronation best
seen with calcaneal
eversion and unlock
of midtarsal joints
Early mid stance
pronation may
continue, should
see pronation cease
late mid stance and
supination begin
Rise of heel off the
ground should see
supination to allow
the foot to be rigid
with decrease WB
contact
Windlass
Mechanism
MTP joints continue
to extend, weight
should progress over
the 1st MTP joint,
supination is
maintained
Foot comes off the
ground in the
position it
maintained in pre
swing. Good place
to look for excessive
pronation
Foot: Abnormal 1. Excessive 1. Midtarsal joints 1. Midtarsal joints 1. Lack MTP joint 1. Foot comes off

calcaneal eversion
2. Limited calcaneal
eversion
3. Excessive MTJ
unlock
4. Limited MTJ
unlock
remain unlocked
2. Midtarsal joints
remain locked
3. Excessive
inversion of
hindfoot continues
4. Excessive
eversion of
hindfoot continues
remain unlocked
2. 1st Ray does not
PF
3. Midtarsal joints
remain locked
4. 1st ray in too
much PF
extension
2. Excessive MTP
extension
3. Roll off the side
of 1st MTP jt.
4. Roll off lateral
forefoot
ground in excessive
pronation
2. Foot comes off
the ground in
excessive supination
Gait Velocity:
Normal or
Abnormal
Cause:
NOTES Stride length:
Equal? Yes----NO
If no, what is
cause?
NOTES Cadence:
Normal or
Abnormal
Cause:
NOTES
Task of Gait Weight
Acceptance
Single Limb
Support
Single Limb
Support
Limb
Advancement
Limb
Advancement
Phase of Gait
Reference Limb
Initial Contact
Loading Response
Mid Stance Terminal Stance Pre Swing Initial, Mid,
Terminal Swing
Contralateral
Limb
Pre Swing Initial to Mid
Swing
Mid to Terminal
Swing
Initial Contact
Loading Response
Mid and Terminal
Stance
ROCKER Heel rocker Ankle Rocker Forefoot rocker Forefoot rocker
Normal Yes---NO Yes---NO Yes---NO Yes---NO Yes---NO
ANKLE JOINT
Normal Yes---NO Yes---NO Yes---NO Yes---NO Yes---NO
If NO what is
deviation?
What are possible
causes for the
deviation from
normal?
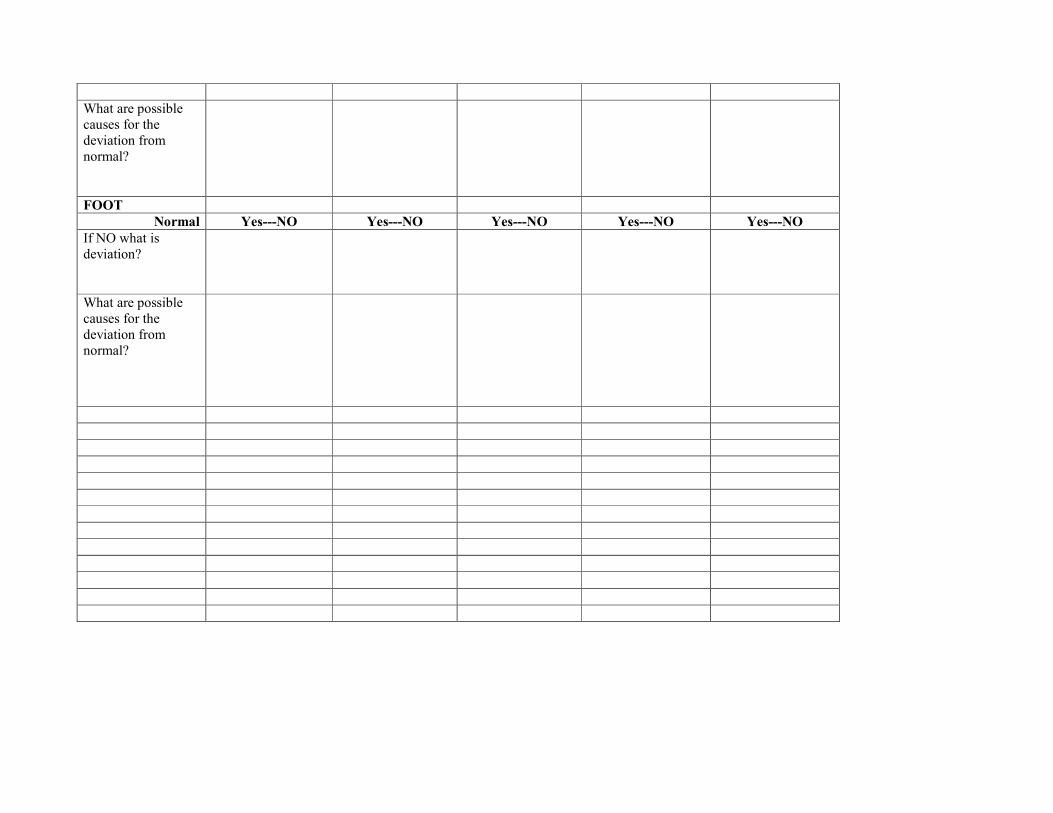
FOOT
Normal Yes---NO Yes---NO Yes---NO Yes---NO Yes---NO
If NO what is
deviation?
What are possible
causes for the
deviation from
normal?

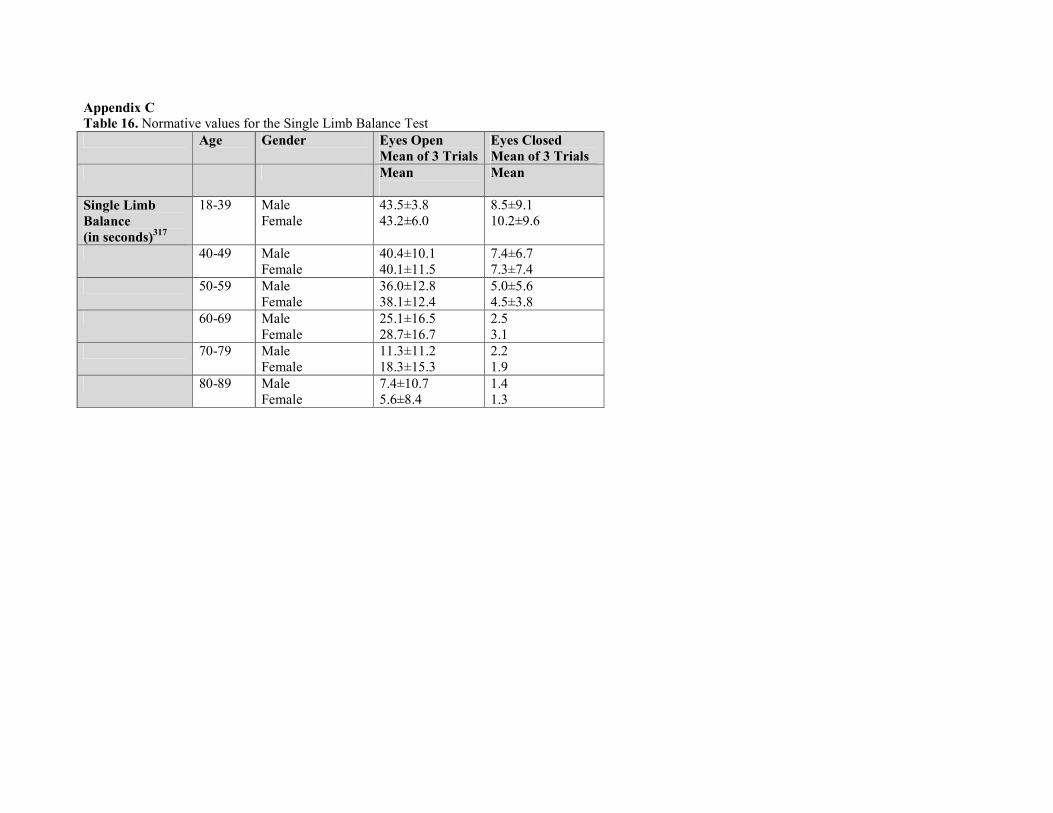
Appendix C
Table 16. Normative values for the Single Limb Balance Test
Age Gender Eyes Open
Mean of 3 Trials
Eyes Closed
Mean of 3 Trials
Mean
Mean
Single Limb
Balance
(in seconds)317
18-39 Male
Female
43.5±3.8
43.2±6.0
8.5±9.1
10.2±9.6
40-49 Male
Female
40.4±10.1
40.1±11.5
7.4±6.7
7.3±7.4
50-59 Male
Female
36.0±12.8
38.1±12.4
5.0±5.6
4.5±3.8
60-69 Male
Female
25.1±16.5
28.7±16.7
2.5
3.1
70-79 Male
Female
11.3±11.2
18.3±15.3
2.2
1.9
80-89 Male
Female
7.4±10.7
5.6±8.4
1.4
1.3






















![Physical education professional development 2012[1]](https://img.pdfslide.us/doc/110x75/545c0872b0af9f12318b4619/physical-education-professional-development-20121.jpg)



![Physical education professional development 2012[3]](https://img.pdfslide.us/doc/110x75/545c0885b1af9f3c0a8b4601/physical-education-professional-development-20123.jpg)

