Embed Size (px)
Citation preview

SROMS 1 VOLUME 16.6
RECOMBINANT HUMAN BONE MORPHOGENIC PROTEIN-2 (rhBMP-2) USE IN MAXILLOFACIAL SURGERY
Alan S. Herford, DDS, MD, FACS; Jeff Dean, DDS, MD, FACS
INTRODUCTION
Surgeons can now control osteogenesis through local application of BMP-2. BMP’s are osteoin-ductive proteins that are located in bone matrix and are responsible for embryonic skeletal formation and bone healing. Marshal Urist first coined the term “bone morphogenic protein” over 40 years ago. Recombinant human BMP-2 is an osteoinductive growth factor that has the potential to make autoge-nous bone grafting unnecessary.1 By demonstrating the capabilities of demineralized bone matrix to induce ectopic bone formation in a rat muscle pouch. Urist introduced the concept that growth factors can induce bone formation independent of a bone tissue environment.2
Recombinant human bone morphogenic proteins (rhBMPs) are cytokines belonging to the growth factor-B superfamily (TGF-b). There are over 20 types of bone morphogenic proteins cytokines (BMPS) with varying osteoinductive potential. rhBMP-2 is a genetically engineered version of BMP-2, a naturally occurring protein which is active in normal bone repair. The two most frequently studied include rhBMP-2 and rhBMP-7 (OP 1). These cytokines have the ability to bind to mesenchymal cells triggering differentiation into osteoblasts.
The availability of recombinant BMPs has allowed definitive tests of their osteoinductive activity in a variety of situations, including an-imal models of clinically relevant bone defects. Cheng et al, demonstrated the relative osteoin-ductivity of different BMPs at various stages of
differentiation in mesenchymal progenitor and osteoblastic cells infected by adenovirus-mediat-ed gene transfer of BMPs.3 BMP-2, 6, and 9 play an important role in the early phase of differen-tiation of the stem cells to preosteoblasts, while most BMPs promote the terminal differentiation of these preosteoblasts to osteoblasts.(Fig. 1) These findings may indicate that BMP-2, 6, and 9 may be more effective in locations where pluripotent cells are present (eg. autologous bone transplant or surrounding muscular tissue).4
The identification of the gene responsible for the production of rhBMP-2 led to its being cloned through recombinant technology. Oligo-nucleotide probes are used to create the human cDNA sequence that is then inserted into a viral vector (plasmid) which, in turn, is transfected into a carrier cell (recombination). These cells have the ability to produce large quantities of
rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 16 VOLUME 16.6
36. Carter TG, Brar PS, Tolas A, et al: Off-label use of recombinant human bone morphogenic protein-2 (rhBMP-2) for reconstruction of mandibular bone defects in humans. J Oral Maxillofac Surg 66:1417, 2008.
37. Clokie CM and Sandor GK: Reconstruction of 10 major mandibular defects using bioim-plants containing BMP-7. J Can Dent Assoc 74:67, 2008.
38. Kuklo TR, Groth AT, Anderson RC, et al: Recombinant human bone morphogenic protein-2 for grade III open segmental tib-ial fractures from combat injuries in Iraq. J Bone Joint Surg Br. 90:1068, 2008.
39. Schwartz ND and Hicks BM: Segmental bone defects treated using recombinant human bone morphogenic protein. J Orhopaedics 3(2) e2, 2006.
40. Herford AS, Boyne PJ, Rawson PR, et al: Bone morphogenic protein-induced repair of the premaxillary cleft. J Oral Maxillofac Surg 65:2136, 2007.
41. Jovanovic SA, Hunt DR, Bernard GW, et al: Long-term functional loading of dental implants in rhBMP-2 induced bone. A histo-logic study in the canine ridge augmentation model. Clin Oral Implants Res 793, 2003.
42. Boden, SD. The ABCs of BMPs. Othopaedic Nursing. 24:49, 2005.
43. Carreon LY, Glassman SD, Brock DC, et al: Adverse events in patients re-exposed to bone morphogenic protein for spine surgery. Spine 33:391, 2008.
44. Shah MM, Smyth MD and Woo AS: Adverse facial edema associated with off-label use of recombinant human bone morphogen-
ic protein-2 in cranial reconstruction for craniosynostosis. J Neurosurg Pediatrics 1:255, 2008.
45. Akamaru T, Suh D, Boden S, et al: Simple carrier matrix modification can enhance delivery of recombinant human bone morphogenic protein-2 for posterolateral spine fusion. Spine 28:429, 2003.
RELATED ARTICLES FROM SELECTED READ-INGS IN ORAL AND MAXILLOFACIAL SURGERY
Bone Substitutes. Michael S. Buckley, DDS. Selected Readings in Oral and Maxillofacial Surgery, Vol. 4, #2, 1996.
Reconstruction of Maxillary Defects. Gregory J. Lutcavage, DDS; Siegfried J. Schaberg, DDS, PhD. Selected Readings in Oral and Maxillofacial Surgery, Vol. 5, #6, 1997.
Bone Graft Harvesting. A. Omar Abubaker, DMD, PhD; Mark A. Oghalai, DDS. Selected Readings in Oral and Maxillofacial Surgery, Vol.9, #6, 2001.
Management of Vertical Alveolar Defects for Implant Reconstruction. Leslie B. Heffez DMD, MS and Manuel Diaz DDS. Selected Readings in Oral and Maxillofacial Surgery, Vol.14, #3, 2006.
Outpatient Harvest of Bone Grafts. Alan S. Her-ford, DDS, MD and Brandon Brown, DDS. Selected Readings in Oral and Maxillofacial Surgery, Vol.15, #4, 2007.

rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 2 VOLUME 16.6
A
B
C
Figure 1. Activation of various BMP’s on bone forming cascade. (Courtesy Medtronics, Inc., Memphis, TN)
____________________________________
Figure 2. Recombinant technology used for creating rhBMP-2.(Courtesy Medtronics, Inc., Memphis, TN)
____________________________________
pure, disease-free rhBMP-2. (Fig. 2)
The emergence of rhBMP-2 as a viable alternative to traditional bone grafting is based on two important clinical challenges. The first is to eliminate the need to harvest bone from the iliac crest or other sites when performing maxillofacial reconstruction because increased morbidity is associated with these procedures.5 The second reason is to try to enhance the degree of new bone formation for placement of dental implants into an ideal location. Clinical applica-tion of BMP’s now includes defects of the facial skeleton,6,7 such as alveolar reconstruction, sinus augmentation, segmental defects and alveolar
rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 15 VOLUME 16.6
20. Banwart JC, Asher MA and Hassanein RS: Iliac crest bone graft harvest donor site morbidity: a statistical evaluation. Spine 20:1055, 1995.
21. Goulet JA, Senunas LE, DeSilva GL, et al: Autogenous iliac crest bone graft. Clin Or-thop 339:76, 1997.
22. Burkus JK. Heim SE, Gornet MF, et al: Is INFUSE bone grafts superior to autograft bone? An integrated analysis of clinical trials using the LT-CAGE lumbar tapered device. J Spinal Discord Tech. 16:113, 2003.
23. Itoh K, Udagawa N, Katagiri T, et al: Bone morphogenic protein-2 stimulates osteo-clast differentiation and survival supported by receptor activator of nuclear factor-kB ligand. Endocrinology 142:3656, 2001.
24. Wang EA, Rosen V, D’Alessandro JS, et al: Recombinant human bone morphogenic protein induces bone formation. Proc Natl Acad Sci USA 87:2220, 1990.
25. Bentz H, Nathan RM, Rosen DM, et al: Puri-fication and characterization of a unique osteoinductive factor from bovine bone. J Biol Chem 264:20805, 1989.
26. Johnson EE, Urist MR and Finerman GAM: Bone morphogenic protein augmentation grafting of resistant femoral nonunions: A preliminary report. Clin Orhtop Relat Res. 230:257, 1988.
27. Johnson EE, Urist MR and Finerman GAM: Repair of segmental defects of the tibia with cancellous bone grafts augmented with human bone morphogenic protein. A preliminary report. Clin Orthop Relat Res
236:249, 1988.
28. Fiorellini JP, Howell TH, Cochran D, et al: Randomized study evaluating recombinant human bone morphogenic protein-2 for ex-traction socket augmentation. J Periodontol 76:605, 2005.
29. Boyne PJ and James RA: Grafting of the max-illary sinus floor with autogenous marrow and bone. J Oral Surg 38:613, 1980.
30. Tatum H: Maxillary sinus and implant reconstruc-tion. Dental Clin North Am 30:107,1986.
31. Smiler DG, Johnson PW, Lozado JL, et al: Sinus lift grafts and endosseous implants. Treat-ment of the atrophic posterior maxilla. Dent Clin North Am 36:151, 1992.
32. Boyne PJ: Application of bone morphogenic proteins in the treatment of clinical oral and maxillofacial defects. J Bone Joint Surg Am 83-A (Suppl 1) S146, 2001.
33. Boyne PJ, Salina S, et al: Bone regeneration using rhBMP-2 induction in hemimandibulectomy type defects of elderly subhuman primates. Cell Tissue Bank 7:1, 2006.
34. Moghadam HG, Urist T, Sandor GK, et al: Suc-cessful mandibular reconstruction using a BMP bio-implant. J Craniofac Surg 12:119, 2001.
35. Herford AS and PJ Boyne: Reconstruction of mandibular continuity defects with bone morphogenic protein-2 (rhBMP-2). J Oral Maxillofac Surg 66:616, 2008.

rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 3 VOLUME 16.6
Figure 3. Mechanism of action of rhBMP-2. (Courtesy Medtronics, Inc., Memphis, TN)
Figure 4. Activation of intracellular signaling by rhBMP-2. (Courtesy Medtronics, Inc., Memphis, TN)
____________________________________
_____________________________________
cleft reconstruction.
MECHANISM OF ACTION
The osteoinductive cytokine rhBMP-2 induces the differentiation of pluripotential pre-cursor cells into new bone tissue at the site of implantation. Through signaling, it promotes the recruitment of the patient’s own adult mesen-chymal stem cells (AMS) to the surgical site, and proliferation of the recruited cells, and the dif-ferentiation of these cells into bone cell precur-sors.(Fig.3) The bone induced by rhBMP-2/ACS remodels and assumes the structure appropriate to its location and function as would be expected from host bone. Although the number of AMS decreases with age, studies have shown that bone formation and repair with BMP-2 is as effective in old animals and in elderly human patients as in young children with cleft palates.8,9
rhBMP-2 binds to specific receptors on the stem cell surface causing them to differentiate into bone-forming osteoblasts.(Fig. 4) Not all BMPs are capable of this binding. There are two types of transmembrane serine/threonine kinase receptors, BRI and BRII, which form heteromer-ic complexes prior to and after ligand binding. Within a BMP-bound receptor complex, BRII transphosphorylates and activates BRI-a for further signaling. Essentially, oligomerization of BMP receptors forms a signaling receptor complex.
Smads are signal transducers for the mem-bers of the TGF-β superfamily. Receptor-regu-lated Smads (R-Smads) are activated by BMP and translocate into the nucleus. Smad oligomers regulate the transcription of target genes through direct binding to DNA, DNA binding proteins, and transcription co-activators or co-repressors. The Smad pathway is regulated by common-me-diator Smads (Co-Smad 4 for BMPs), inhibitory Smads (I-Smad 6 and 7), Smad binding proteins,
rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 14 VOLUME 16.6
REFERENCES
1. Wozney JM: Overview of bone morphogenic proteins. Spine 27(16 Suppl 1):S2-8, 2002.
2. Urist MR: Bone. Formation by autoinduction. Science 150:893, 1965.
3. Cheng H, Jiang W, Phillips FM, et al: Osteogenic activity of the fourteen types of human bone morphogenic proteins (BMPs). J Bone Joint Surg Am 85:1544, 2003.
4. Termaat MF, Den Boer FC, Bakker P, et al: Bone morphogenic proteins. Development and clinical efficacy in the treatment of fractures and bone defects. J Bone Joint Surg Am 87:1367, 2005.
5. Ahlmann E, Suh D, Boden S, et al: Comparison of anterior and posterior iliac crest bone grafts in terms of harvest-site morbidity and functional outcomes. J Bone and Joint Surg 84:716, 2002.
6. Herford AS, Boyne PJ and Williams RP: Clinical applications of rhBMP-2 in maxillofacial surgery. CDA Journal 35:335, 2007.
7. Warnke PH, Springer IN, Wiltfang J, et al: Growth and transplantation of a custom vascularized bone graft in a man. Lancet 364:766, 2004.
8. Bessho K and Iizuka T: Changes in bone inducing activity of bone morphogenic protein with aging. Ann Chir Gynaecol Suppl 207:49, 1993.
9. Poyton AR and Lane JM: Safety profile for the clinical use of bone morphogenic proteins in the spine. Spine 27:S40, 2002.
10. Itoh S, Itoh F, Goumans MJ, et al. Signaling of transforming growth factor-beta family
members through Smad proteins. Eur J Biochem 267:6954, 2000.
11. Von Bubnoff A and Cho KW: Intracellular BMP signaling regulation in vertebrates: pathway or network? Dev Biol 239:1, 2001.
12. Canalis E, Economides AN and Gazzerro E: Bone morphogenic proteins, their antagonists, and the skeleton. Endocr Rev 24:218, 2003.
13. Westerhuis RJ, van Bezooijen RL and Kloen P: Use of bone morphogenic proteins in trau-matology. Injury 36:1405, 2005.
14. Gornet M, Burkus J, Dickman C, et al: Recom-binant human bone morphogenic protein-2 with tapered cages: a prospective, random-ized lumbar fusion study. Spine J 2:8, 2002.
15. Boden S, Zdelblick T, Sandu H, et al: The use of rhBMP-2 in interbody fusion cages. Spine 25:376, 2000.
16. Burkus J, Gornet M, Dickman C, et al: Anterior lumbar interbody fusion using rhBMP-2 with tapered interbody cages. J Spinal Dis-cord Tech 15:337, 2002.
17. Boyne PJ, Lilly LC, Marx RE, et al: De novo bone induction by recombinant human bone morphogenic protein-2 (rhBMP-2) in maxillary sinus floor augmentation. J Oral Maxillofac Surg 63:1693, 2005.
18. Boyne PJ, Nath R and Nakmura A: Human recombinant BMP-2 in osseous reconstruc-tion of simulated cleft palate defects. Br J Oral Maxillofac Surg 36:84, 1998.
19. Arrington ED, Smith WJ, Chambers HG, et al: Complications of iliac crest bone graft har-vesting. Clin Orthop 329:300, 1996.

rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 4 VOLUME 16.6
and protein degradations.10,11
Growth and differentiation factors such as BMP-2 play essential role in cellular functioning but require a tempering of their signal for coor-dinated bone formation and remodeling. This is achieved by feedback mechanisms, extracellular antagonists (i.e., noggin, gremlin, DAN and cerberus) and intracellularly by inhibition and modulation of the Smad-signalling pathway.12,13
COMPARISON TO AUTOGRAFTS
Probably the greatest potential advantage for rhBMP-2 use is eliminating the need for graft harvest and its associated morbidity. Pro-spective studies have shown that rhBMP-2 is superior to autografts in obtaining successful lumbar fusion.14-16 Although it remains to be seen whether this will be true for maxillofacial reconstructions, studies thus far are promising. Cleft palate patients and patients undergoing a sinus lift procedure who received rhBMP-2 performed as well as patients receiving iliac crest autografts.17,18
Complications with harvest of iliac crest bone graft may occur in as many as 15% to 25% of patients.19-22 Harvesting iliac crest bone is associated with pain and carries the risk of sig-nificant morbidity. Graft harvest complications from an additional operative site include chronic donor site pain, increased operative time, and additional cost. For larger defects the quantity of bone available to harvest may be insufficient for large defects or in patients with previous graft harvests. (See also Selected Readings in Oral and Maxillofacial Surgery Vol. 15, #4; Vol. 14, #3; Vol. 9, #6; Vol. 5, #6; Vol. 4, #2)
Autogenous bone has long been considered the “gold standard”, but transplanted autogenous bone may need to be resorbed or remodeled before fusing. BMP has a role in the regulation of bone turnover via coupled osteoblastic and osteoclastic activity.9 Itoh et al. described how BMP mediated signals are involved in osteo-clastic resorption.23
Therefore, rhBMP-2 may accelerate the creeping substitution of an allograft by stimu-lating an osteoclastic response in concert with an ostoeblastic response. Because rhBMP-2 is osteoinductive and allografts are osteocon-duc-tive, it appears logical to combine the two in an effort to enhance the amount and rate of bone formation.
CLINICAL USE OF rhBMP-2
Reports of clinical use of extracts of human BMP from allograft bone matrix began in the late 1980’s. In 1988 the DNA sequence for BMP was isolated from a purified extract, leading to the production of recombinant BMP. This recombinant process allows for the production of large quantities of highly purified BMP at a known concentration.24,25
In 2007, the FDA granted approval of rhBMP-2 (INFUSE Bone Graft®, Medtronics, Memphis, TN) as an alternative to autogenous bone grafts for sinus augmentations, and for localized alveolar ridge augmentation of defects associated with extraction sockets. This approval was based on data from 312 patients enrolled in a total of 5 clinical studies. However, rhBMP-2 is contraindicated for patients with a known hyper-sensitivity to rhBMP-2 or bovine type I collagen. It should not be used in the vicinity of a resected
rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 13 VOLUME 16.6
recognition for his research, much of which was completed in cooperation with Dr. Philip Boyne. Several of his research endeavors are related to growth factors and their use in facial reconstruction. Last May, 2008, Dr. Herford was named the inaugural Philip Boyne-Peter Geistlich Professor of Oral and Maxillofacial Surgery. He also recently was inducted into the American College of Surgeons.
Dr. Jeffrey S. Dean received his D.D.S. from Creighton University School of Dentist-ry and his M.D. from the University of Texas Southwestern Medical School in Dallas. Dr. Dean completed his training in oral and maxil-lofacial surgery at Parkland Memorial Hospital at the University of Texas Southwestern Medical Center in Dallas. Currently he is in private prac-tice with Facial and Oral Surgery Associates in Pocatello, Idaho and Assistant Professor in the Department of Oral and Maxillofacial Surgery at Loma Linda University. He has been involved in research and has multiple articles and book chapters. He is a fellow of the American College of Surgeons. Dr. Dean practices full-scope oral
and maxillofacial surgery with interests in facial flaps, facial reconstruction, cleft and craniofacial surgery.

rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 5 VOLUME 16.6
tumor, in patients with any active malignancy, in infected sites or in pregnant women.
The osteoinductive capabilities of rhBMP-2 have been widely studied in different bone healing environments. Preclinical and clinical research has demonstrated that rhBMP-2 com-bined with an absorbable collagen sponge (ACS) can induce new bone formation. Dose-dependant clinical studies have determined 1.5mg/cc as a safe and predictable dose for bone formation. rhBMP-2 has been show to heal critical-size bone defects both in animal models and clin-ically.
Using extracts of BMP, Johnson, et al. reported on a dozen nonunion patients.26 Union was obtained in 11 out of 12 nonunions, at an av-erage time of 4.7 months. This was followed by a report of BMP implanted along with autograft in six patients with traumatic 3 cm to 17 cm tibial defects.27 The tibia were stabilized with external fixation and all six patients regained function.
Because the half-life of rhBMP-2 is only minutes in the bloodstream, it must be adminis-tered locally to the bleeding bone over a period of time to stimulate with new bone formation. The absorbable collagen sponge (ACS) carri-er matrix provides a means of delivering and retaining rhBMP-2 at the surgical site.
It also helps prevent soft tissue prolapse into the defect, enabling bony vascular growth to occur during rhBMP-2 induced bone forma-tion. The ACS is type I collagen derived from highly purified bovine tendon. Because the ACS lacks structural stability the soft-tissue walls
of the defect can compress it. Development of future carriers with greater structural stability will better maintain the space for optimal bone formation.
The delivery of rhBMP-2 to a surgical site on an absorbable collagen sponge has been investigated in preclinical and clinical studies of localized alveolar grafting as well as sinus floor augmentations prior to implants. A pivotal study indicated that rhBMP-2 provides clinical and radiographic outcomes that are equivalent to those after autogenous grafting.17
Localized Alveolar Defects
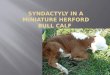
rhBMP-2 can be used for localized ridge augmentation procedures. A randomized pro-spective study evaluating the use of rhBMP-2 for extraction socket augmentation showed that rhBMP-2 could predictably form de novo bone.28 Eighty patients requiring local alveolar aug-mentation for bucal wall defects in the anterior maxilla were evaluated. Patients who received 1.5 mg/cc rhBMP-2/ACS had significantly greater bone augmentation compared to controls (p<0.05). The adequacy of bone for placement of a dental implant was approximately twice as great in the rhBMP-2/ACS group.(Fig. 5)
Maxillary Sinus Lift
The maxillay sinus lift can reliably pro-vide sufficient bone for placement of dental implants.29-31 Boyne, et al, reported the results of bone induction by rhBMP-2/ACS in maxillary sinus floor augmentation.17 They found that rhB-
rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 12 VOLUME 16.6
reoperation were all improved with rhBMP-2 in their large series of patients.38
Despite the extent of bone formation, there has been no evidence of bone formation extend-ing beyond the boundaries of the defect. The process of induced bone formation appears to be a controlled response to highly concentrated levels of rhBMP-2. Because this bone-inducing protein is normally present endogenously in the body it is likely that normal growth regulating genes control the growth process and prevent overgrowth.
QUESTIONS FOR THE FUTURE
Still unanswered are questions such as:
· What is the ideal grafting material to combine with BMP to enhance bone for-mation in a specific defect?
· Does the addition of BMP to autogenous bone improve the “gold standard”?
· Will alloplastic, allogenic, or xenogenic graft material in combination with rhB-MP-2 prove to be superior than rhBMP-2/ACS alone?
· Are there other cytokines that will enhance the activity of BMP-2?
Future studies will help us continue to shed light on these questions and many more as we strive to improve our understanding of bone healing.
CONCLUSIONS
The published literature suggests that rhB-MP-2 is clinically effective in treatment of criti-cal-size defects in both extremities as well as in the maxillofacial region by predictably inducing new bone formation at the site of implantation. Further study will be needed to support this conclusion and offer definitive proof that rhB-MP-2ACS can be as safe an alternative to the harvest of autografts in maxillofacial trauma as it has proved to be in orthopedic applications. The advantages of rhBMP-2 repair to the patient include a shorter hospital stay, avoidance of gait and sensory disturbance, as well as decreased sites for scar formation and possible infection. Surgical time is reduced because the surgeon does not have to harvest autogenous bone from a secondary site. In the future, the use of exog-enous cytokines, particularly those in the BMP series will become common and the regeneration of osseous defects will likely be brought about through a clinical outpatient procedure.
Dr. Alan Herford received his Doctor of Dental Surgery from Loma Linda University School of Dentistry in 1994. He then moved to Dallas where he attended the University of Texas Southwestern Medical Center, earning his MD degree in 1997 and completing the Advanced Eeducation Program in Oral and Maxillofacial Surgery at Parkland Hospital. Following his return to LLU in 2000, he was appointed chair of the OMFS Department and advanced program director in 2002. During his tenure at Loma Lin-da the residency program has tripled in size and has integrated with the Loma Linda University School of Medicine. Dr. Herford has achieved distinction as a leader in surgery, receiving

rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 6 VOLUME 16.6
A B
CD
Figure 5. A. Failed tooth with loss of buccal plate of bone, B. Implant and rhBMP-2 placed, C. Radiograph showing implant in place, D. Postoperative result.
________________________________________________________________________________
MP-2 predictably and safely induced adequate loading of endosseous dental implants in patients requiring staged maxillary floor augmentation.23 The proportion of patients who received dental implants that were functionally loaded and re-mained functional at 36 months post-functional loading was 62% and 76% in the bone graft and 1.5 mg/ml rhBMP-2/ACS treatment groups, respectively.
The technique is similar to the standard maxillary sinus lift procedure described by Boyne and James.29 After elevating the Sneide-rian membrane, the rhBMP-2 soaked collagen
sponges are placed.(Fig. 6) Care is taken to effectively pack the floor of the sinus.
OFF-LABEL USE OF rhBMP-2
rhBMP-2 has been used successfully in non-human primates and humans to restore large critical-sized defects including continuity defects, alveolar clefts, and extensive vertical bone defects (preprosthetic defects).32,33
Continuity Defects
rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 11 VOLUME 16.6
maintaining space for these defects. (Fig. 9) The use of occlusive membranes (resorbable or non-resorbable) may impede vascular ingrowth and decrease the available AMS.
Poor Bone Healing Environments
Radiation and bisphosphonates are examples of factors that have the potential to impair bone and soft tissue healing. Chronic osteomyelitis is another example of a site as-sociated with impaired healing. Because of the angiogenic response to the BMP, this factor may have a role in poor bone healing environments such as those with inhibited healing due to radiation or bisphosphonates.
RISKS OF USING BMPs
Both rhBMP-2 and rhBMP-7 have been studied in thousands of patients and tens of thou-sands of animals with a high safety profile.42 It is estimated that over 500,000 patients have been treated with rhBMP-2. A low risk, similar to that in clinical trials leading to approval, can be expected with “on-label” use. Transient increas-es in antibodies to BMP develop in 5% to 10% of patients, but this does not affect bone healing on first exposure. However, less is known about the effects of multiple exposures.
Carreon, et al, studied patients who were re-exposed to rhBMP for spine surgery.43 They found no significant difference in the number of complications between first and second spine surgeries of the 96 patients using rhBMP-2. There were no wound problems or allergic reactions among the twelve patients who had a third surgery with rhBMP-2. They concluded that multiple exposures to rhBMP-2 does not increase the risk of wound infections or other
problems and does not result in clinically de-tectable allergic reactions.
When used “off-label”, there are possible adverse outcomes that must be balanced against the benefit of using rhBMP-2. Changing the recommended concentration of the BMP or the carrier material could risk inconsistent bone for-mation. If a higher concentration is used, local edema or fluid collection can occur; as has been reported after some cases of anterior cervical discectomy and fusion using BMP instead of autogenous bone.9 Adverse facial edema has also been noted when rhBMP-2 was used for cranial reconstruction to treat craniosynostosis.44 Because BMP can accelerate bone resorption in addition to bone formation, using more resorb-able carriers, that have not been carefully tested with BMP, can result in accelerated resorption of the bone.
The absorbable collagen sponge is suscep-tible to compression from the overlying tissue. This compressibility problem has led to the con-sideration of ways to maintain space, including engineering an alternative carrier, addition of compressive resistant osteoconductive materi-al, supporting the space with a membrane or mesh, or using screws or implants to “tent up” the tissue. Combining the rhBMP-2 with a graft extender may improve the economic feasibility of BMP-2 by reducing the required dose of the protein.45
As with any new technology, concerns over additional costs of such interventions should be considered. As discussed by Kuklo, et al. there is a compelling argument for the continued use of such technologies, because the primary outcome measures of bone union, rate of infection, and

rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 7 VOLUME 16.6
Figure 6. A.Lifting up of maxillary sinus membrane, B. Packing of rhBMP-2/ACS into created space, C. Implant placed in de novo bone.
A
B
C
Mandibular continuity defects secondary to trauma or tumor resection are common and often present reconstruction challenges. Pre-clinical animal studies have demonstrated that rhBMP-2/ACS can induce bone formation and repair large, critical-size segmental defects in rat femora, rabbit radii and ulnae, dog radii, and nonhuman primate radii.4 Boyne, et al, showed that rhBMP-2 could heal critical-size oral and maxilla-facial defects in a nonhuman primate model.16
The first reported human application of BMP in the mandible was by Moghaden et al. in 2001.34 In 2004, Warnke et al. used BMP-7 and bone mineral blocks (xenografts) to create a custom vascularized bone graft.7 The engineered graft was allowed to heal in the trapezius mus-cle and was subsequently transplanted into the recipient site using microvascular anastomosis.
Herford and Boyne used rhBMP-2 to treat mandibular continuity defects.35 All 14 patients demonstrated successful osseous restoration of the missing bone when rhBMP/ACS was used without concomitant bone grafting materials. The authors described the importance of main-taining the periosteal envelope. This can be accomplished with either a superiorly placed titanium miniplate or titanium mesh.(Fig. 7) This metallic tenting up of the mucosa and periosteum is thought to be necessary to maintain the space for osseous regeneration.
Carter et al. used either rhBMP-2 alone or in combination with bone marrow cells and allogenic bone.36 In 2 out of 5 patients their continuity defect failed to proceed to union. They suggested that the failures were due to
rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 10 VOLUME 16.6
Figure 9. A. Radiograph showing extensive bone loss, B. Exposure of underlying alveolar ridge, C. Placement of a titanium mesh to maintain rhBMP-2 in place, D. Postoperative radiograph, E. Placement of dental implants into regenerated bone.
A
B
C D
E

rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 8 VOLUME 16.6
Figure 7. A. Mandibular tumor involving the right mandible, B. Immediate reconstruction with rhBMP-2/ACS combined with demineralized bone. Note the mesh superiorly to provide for space maintenance, C. Implants placed 8 months later.
________________________________________________________________________________
A
C B
chronic infection or lack of space maintenance by the graft.
Clokie and Sandor recently used bioim-plants containing BMP-7 for mandibular defects in a series of 10 patients.37 They reported suc-cessful restoration of critical size defects in 10 patients, with decreased operating room time and shorter hospital stays, thus saving health care system costs.
A recent study of 129 soldiers with type III open segmental tibia fractures and segmental cortical bone loss (2 cm to 10 cm) compared fix-ation with supplemental bone grafting (Group 1) or rhBMP-2/ACS and allograft bone (Group 2).38 There was a lower rate of infection in Group 2 (3.2%) compared to Group 1 (14.9%). Definitive
union was observed in 76% of Group 1 patients and 92% for Group 2 patients.
Another study evaluated the use of rhB-MP-2 with two different bone substitutes (calci-um sulfate or calcium phosphate) to repair seg-mental bone defects involving the extremities.39 Defects averaged 4.75 cm (ranging from 1.5 to 8.0 cm). In this group of patients, rhBMP-2/ACS healed of 84% critical-size defects.
Alveolar Clefts
Growth factors have shown promise in con-genital defects. (Fig. 8) In a non-human primate study using a simulated cleft model, Boyne, et al, found that rhBMP-2 could form bone in a cleft that was similar to that of autografts.18 Another study compared rhBMP-2 to anterior iliac crest
rhBMP-2 in Maxillofacial Surgery A.S. Herford, DDS, MD, FACS; J. Dean, DDS, MD,
SROMS 9 VOLUME 16.6
bone graft for treatment of alveolar clefts.40 They found that rhBMP-2 was an effective alternative to conventional anterior iliac particulate cancel-lous grafts in that series of patients.
Preprosthetic Defects
Preprosthetic augmentation procedures using bone grafts, such as ridge augmentation, are commonplace. Jovanovic, et al, performed a histologic study of a canine ridge augmented with BMP.41 They found no significant differ-ences between implants with rhBMP-2-induced bone and the resident bone. They concluded that rhBMP-2 allows installation, osseointe-gration, and long-term functional loading of dental implants. Titanium mesh is helpful in
Figure 8. A. Isolated left maxillary cleft, B. Radiograph showing extent of cleft, C. Closure of nasal floor, D. Placement of rhBMP-2/ACS into defect, E. Postoper-ative radiograph showing bone regeneration in area.
_____________________________________
AB
C D
E


























![[1919] Herford, C. H. - Norse Myth in English Poetry](https://img.pdfslide.us/doc/110x75/577d2c4d1a28ab4e1eabda3a/1919-herford-c-h-norse-myth-in-english-poetry.jpg)
