Embed Size (px)
Citation preview

CONTINUING MEDICAL EDUCATION
Recognizing psoriatic arthritisin the dermatology clinic
Amit Garg, MD,a and Dafna Gladman, MDb
Boston, Massachusetts, and Toronto, Ontario, Canada
From
C
fo
W
Fund
Conf
re
re
ha
A
gr
ed
re
Repr
A
0190
ª 20
doi:1
Dermatologists care for patients with psoriasis in whom there exists an inherent risk of psoriatic arthritis, acondition with potential for causing joint damage and subsequent disability. Most patients have psoriasisfor years before the development of psoriatic arthritis, and there may be a significant proportion ofpsoriasis patients with joint involvement that are cared for by the dermatologist. With the absence of adiagnostic measure, the criterion standard for recognizing or monitoring psoriatic arthritis remains theclinical assessment. Recognition of psoriatic arthritis in the psoriasis patient—and the dermatologist’s abilityto differentiate it from other types of arthritis—provide an opportunity to improve patient outcomesthrough early recognition and facilitation of intervention in collaboration with a rheumatologist. ( J AmAcad Dermatol 2010;63:733-48.)
Learning objectives: After completing this learning activity, participants should be able to recognize thepresence of psoriatic arthritis among patients with psoriasis; distinguish psoriatic arthritis from reactivearthritis, osteoarthritis, gout, rheumatoid arthritis, and ankylosing spondylitis; and use appropriate laboratoryand imaging tests in the evaluation of patients with psoriasis and musculoskeletal complaints.
Key words: dermatologist; psoriatic arthritis; screening.
Dermatologists care for patients with psoria-sis in whom there exists an inherent risk ofcoupled morbidity, the most common
and well described of which is psoriatic arthritis(PsA). PsA may be defined as an inflammatoryarthritis which is seronegative for rheumatoid factor(RF) and enthesitis that is associated with psoriasis.1
It has been classified among the four main spondy-loarthropathies which, in addition to inflammatoryarthritis, share a spectrum of components includingenthesitis and dactylitis, axial involvement, RF
the Department of Dermatology,a Rheumatic Skin Disease
enter, Boston University School of Medicine, and the Centre
r Prognosis Studies in the Rheumatic Diseases,b Toronto
estern Hospital.
ing sources: None.
licts of interest: Dr Garg has been a consultant for Abbott, has
ceived honoraria from Abbott and Genentech, and has
ceived grants from Centocor and RegeneRx. Dr Gladman
s been a consultant for and received honoraria from Abbott,
mgen, BMS, Centocor, Schering, and Wyeth, and has received
ants from Abbott, Amgen, Schering, Pfizer, and Wyeth. The
itors, planners, and peer reviewers have no relevant financial
lationships.
int requests: Amit Garg, MD, Department of Dermatology, 609
lbany St, J207, Boston, MA 02118. E-mail: [email protected].
-9622/$36.00
10 by the American Academy of Dermatology, Inc.
0.1016/j.jaad.2010.02.061
seronegativity, presence of the human leukocyteantigen (HLA)*B27 allele and extraarticular features.2
Once described as a disease with a more mildprognosis,3,4 PsA is nowunderstood tohavepotentialfor joint damage with disability outcomes similar topatients with rheumatoid arthritis (RA).5-8 Up to 57%of PsA patients have erosive arthropathy,5,9 andfunctional disability occurs in 11% to 19% of pa-tients.5,9-11 PsA patients also have increasedmortalityrelative to the general population.12 Most patientshave psoriasis either for several years before thedevelopment of arthritis or simultaneously with it.5
As such, a significant proportion of psoriasis patientshave joint involvement without a diagnosis of PsA,13
and it is likely that many of these patients are underthe care of dermatologists. Accordingly, the recogni-tion of PsA in the psoriasis patient by the dermatol-ogist provides an opportunity to improve outcomesthrough early recognition and facilitation of inter-vention in collaboration with a rheumatologist.
The unpredictable, heterogeneous, and often in-sidious involvement of joints or juxtaarticular tendonsand ligaments can make clinical recognition of PsAand distinction from other types of arthritis a chal-lenge. Types of arthritis such as osteoarthritis (OA)and gout often coexist with psoriasis and mimicpresentations of PsA. Alternatively, patients withpsoriasis-like eruptions (ie, seborrhea) and concom-itant inflammatory arthritis, such as RA or ankylosing
733

J AM ACAD DERMATOL
NOVEMBER 2010734 Garg and Gladman
spondylitis (AS),maybemisdiagnosedwith PsA.Withthe absence of a diagnostic measure for PsA, thecriterion standard for diagnosis or monitoring re-mains the clinical assessment. With basic training, it ispossible for the dermatologist to recognize the pres-ence of PsA by appreciating disease demographicsand clinical features, asking the appropriate ques-
CAPSULE SUMMARY
d Dermatologists care for psoriasis patientsin whom there exists an inherent risk forcoupled morbidity, most commonlypsoriatic arthritis (PsA).
d Different types of arthritis coexist withpsoriasis and mimic presentations of PsA;in addition, patients with psoriasis-likeeruptions and concomitantinflammatory arthritis may bemisdiagnosed with PsA.
d The dermatologist may recognize thepresence of PsA by appreciating diseasedemographics and clinical features,asking the appropriate questions,performing simple targeted physicalassessments, and using the mostappropriate laboratory and imagingstudies.
d The recognition of PsA in psoriasispatients by the dermatologist providesan opportunity to improve outcomes
tions, performing simple tar-geted physical assessments,and using the appropriatelaboratory and imaging stud-ies. For a comprehensivegeneral overview of the diag-nostic and treatment chal-lenges of PsA as they relateto pathogenesis and burdenof disease, the reader is re-ferred to the January 2005continuing medical educa-tion article published in theJournal.14 The aim of thisreview is to provide the der-matologist with a practicalframework for recognizingthe clinical features of PsAand distinguishing these fea-tures from other commonforms of arthritis, thereby fa-cilitating more specific andtimely referral to rheumatol-ogy. PsA is contrasted withreactive arthritis (ReA), OA,gout, RA, and AS.
through early recognition and facilitationof intervention in collaboration with arheumatologist.
PSORIATIC ARTHRITISKey pointsd Psoriatic arthritis (PsA)
is a common condition in which psoriasisprecedes arthritis by years in most patientsd As an inflammatory arthritis, PsA is charac-terized by joint discomfort, swelling, andprolonged morning stiffness
d Patterns of joint involvement in PsA arevariable, and relying on patterns of involve-ment alone to distinguish PsA from otherforms of arthritis may be a pitfall
d Most common sites of entheseal involvementin PsA include the attachment of the Achillestendon or the plantar fascia to the calcaneus
d A visual inspection and targeted examina-tion of the joints and entheses may facilitaterecognition of PsA with greater sensitivitythan through patient-reported symptomsalone
d There are no laboratory tests that specify adiagnosis of PsA
d Thepresenceofmarginal andcentral erosions,periostitis, and bulky syndesmophytes onplain radiographic film distinguish PsA fromother forms of arthritis
EpidemiologyPsA has a worldwide prev-
alence among psoriasis pa-tients ranging from 6% to42%.15-23 Population hetero-geneity and varying methodsof disease classification anddata acquisition contribute tothedifficulty in establishing itstrue prevalence. Although theincidence of PsA among pa-tients with psoriasis variesamong epidemiologic stud-ies, it is apparent that it is acommon disorder.15-20 As arough estimate, if one-thirdof the 1% to 3% of the USpopulation with psoriasis hasPsA, then PsA may occur in0.3% to 1.0% of this group, aprevalence similar to thatseen in RA. In 70% of PsApatients, psoriasis precedesthe onset of arthritis by about10 years,5 and the likelihoodof developing PsA may alsocorrelate with duration andseverity of psoriasis.16 The si-multaneous onset of psoriasis
and arthritis is noted in approximately 10% to 15% ofcases,5 and arthritis may precede psoriasis by as manyas 10 to 15 years in the remaining 15% of cases. Inchildren, however, arthritis may precede psoriasis inas many as 50% of cases.24-26 PsA affects men andwomen equally, with a peak age of onset between 35and 45 years of age. In children, PsA has amean age ofonset of 9 to 10 years, and may have a femalepredominance.
With these epidemiologic considerations in mind,one may begin to classify patients among the varioustypes of arthritis. For example, a 30-year-old manwith psoriasis and pain of the distal interphalangeal(DIP) joint is more likely to have PsA than OA (seethe section on osteoarthritis). Similarly, a 35-year-oldman with psoriasis and diffuse swelling of the big toeis more likely to have PsA than gout (see the sectionon gout).

Fig 1. Synovial fluid in psoriatic arthritis. Synovial fluidfrom a patient with psoriatic arthritis, an inflammatoryarthritis, contains a white blood cell count greater than2000, of which at least 75% are polymorphonuclear cells.This composition imparts a cloudy or opaque appearanceto the aspirate (right). Synovial fluid from a patient withnoninflammatory arthritis has a white cell count of lessthan 2000 and is transparent in appearance (left).
J AM ACAD DERMATOL
VOLUME 63, NUMBER 5Garg and Gladman 735
Clinical features. PsA is an inflammatory arthri-tis (Fig 1) in which initial musculoskeletal symptomsare more often insidious in onset, rather than acute.Joint discomfort, more often than pain, characterizesPsA. However, asymptomatic disease, even withevidence of radiographic damage of the involvedjoint, is not uncommon. While 100% of patients withRA and AS, for example, complain of morningstiffness, only about half of PsA patients give thesame complaint. Prolonged morning stiffness lastinglonger than 60 minutes results from inflammatoryinvolvement of entheses, the point at which tendonsor ligaments insert to bone. The stiffness in PsAcontinues to improve throughout the day withactivity, and it becomes more prominent with pe-riods of rest, such as overnight sleep.
Patterns of joint involvementThe patterns of joint involvement in PsA are
variable, and the natural course of disease andtreatment bear further influence on dynamic patternsof involvement over the course of disease. Whatbegins as oligoarthritis (4 or fewer joints) mayconvert to polyarticular (more than 4 joints) diseaseover years, and may revert once again to oligoar-thritis with treatment. Axial involvement may occurat onset, may develop later in the disease course, ormay be absent altogether. As such, relying onpatterns of involvement alone to distinguish amongdifferent forms of arthritis may be a pitfall.
Among the recognized patterns of PsA initiallydescribed by Moll and Wright,1 the DIP predominantpattern may be the most readily recognized becauseit is unique to PsA. However, this pattern occurs in
only 5% to 10% of patients, and primarily in men.27
An asymmetric oligoarthritis pattern occurs in about30% of patients. In this pattern, there is typicallyinvolvement of a large joint, such as the knee, and afew small joints of the hands or feet, often inassociation with dactylitis. However, several seriessuggest the polyarthritis pattern to be at least ascommon as the oligoarticular pattern in PsA, espe-cially among women.5,6,9,28,29 Polyarticular diseaseinvolves the fingers, wrists, toes, and ankles. Whilebearing similarity to the pattern observed in RA (seethe section on rheumatoid arthritis), the polyarthritispattern in PsA may be distinguished further byinvolvement of DIP joints and the relative asymmetryamong involved joints. Moreover, whereas PsA ismore likely to affect all of the joints in any one digit(RAY distribution) while others remain free of arthri-tis, RA affects the same joints in all of the digits.Occurring in about 5% of PsA patients, arthritismutilans of the hands and feet is not nearly ascommon as it is in RA.
Axial disease alone, in the form of spondylitis(inflammation of apophyseal joints of the spine)and/or sacroiliitis (inflammation of the sacroiliacjoint in the pelvis) occurs in 5% of patients withPsA and most often in males. More often though,axial disease occurs in conjunction with peripheralarthritis, and so in total, up to 40% of PsA patientshave some form of axial involvement. Spondylitis inPsA involves the cervical spine with relative sparingof the thoracolumbar spine. The atlantoaxial joint isat risk for subluxation with severe cervical disease.Vertebrae of the spine are affected dysynchronouslywith skipping in PsA. Notably, there may be discor-dant involvement of the spine without sacroiliacdisease, unlike axial disease in AS (see the section onankylosing spondylitis). When present, sacroiliitis inPsA is usually asymmetric, also in contrast to AS.
Enthesitis and dactylitis. Whereas synovitis isthe primary lesion in RA, synovitis along with enthe-sitis characterizes PsA. Ensthesitis, or inflammation atthe site of tendon or ligament insertion into bone, ispresent in up to 42% of patients.30 There are manyentheseal structures that serve to absorb and dissipatemechanical stress around joint structures, and inflam-mation of these structures results in clinically apparenttightness around joints, most notable after periods ofrest. Enthesitis may affect both peripheral and axialsites independently from inflammatory involvementof the joint. The most common sites of enthesealinvolvement in PsA include the attachment of theAchilles tendon or the plantar fascia to the calcaneus(heel), as well as the ligaments around the rib cage,pelvis, vertebral bodies, posterior tibial tendon, quad-riceps muscle, patellar tendon, and the elbow.

Table I. Comparison of clinical features among types of arthritis that may coexist with psoriasis or that mimicpsoriatic arthritis
Clinical feature PsA OA Gout RA AS ReA
Gender M=F MzF M[ F F[M M[[[F M[[FAge at onset (yrs) 35-45 [50 20-40 30-50 20-40 20-40Onset Gradual Gradual Acute Acute/gradual Acute/gradual AcuteQuality of jointsymptoms
Discomfort/painless than in RA
Discomfort Pain Pain Pain Pain
Morning stiffness(min)
[60, betterwith activity
\20, worsewith activity
None [60, betterwith activity
[60, betterwith activity
[60, betterwith activity
Extraarticularfeatures
Present Absent Absent Present Present Present
AS, Ankylosing spondylitis; F, female; M, male; OA, osteoarthritis; PsA, psoriatic arthritis; RA, rheumatoid arthritis; ReA, reactive arthritis.
J AM ACAD DERMATOL
NOVEMBER 2010736 Garg and Gladman
Enthesitis has been proposed as a common denom-inator between psoriatic nail changes and PsA.Magnetic resonance imaging coupled with histologicfindings suggest a connection between nail changesand the enthuses.31
Associated extraarticular symptoms. Inflam-matory arthritis is associated with extraarticularsymptoms, the frequency and extent of which de-pend on the type of arthritis involved. Similar topatients with other types of inflammatory arthritis,PsA patients experience constitutional symptoms,especially fatigue and sometimes anorexia, weightloss, and generalized weakness. PsA belongs to thespondyloarthritis group, which shares extraarticularfeatures different from those seen in seropositivedisease, of which RA is the prototype. For example,conjunctivitis or uveitis tends to occur in seronegativediseases, whereas scleritis and episcleritis are morelikely to occur in seropositive diseases. In PsA,conjunctivitis or uveitis resulting in pain, photopho-bia, and lacrimation may be present in 7% to 33% ofcases. Ocular involvement in PsA tends to be chronicand bilateral, and it may involve posterior chambers.Aortic insufficiency resulting in symptoms of conges-tive heart failure is a rare complication in PsA. Table Icompares the clinical features among types of arthri-tis that may coexist with psoriasis or that mimic PsA.
Physical examinationThe dermatologist is not expected to perform a
joint examination on a psoriasis patient routinely.However, a functional appreciation of signs sugges-tive of inflammatory arthritis and enthesitis mayallow the dermatologist to recognize PsA withgreater sensitivity than through patient reportedsymptoms alone, and to refer for rheumatologyconsultation with better specificity and timing. Ifhistory and a review of systems alone do not suggestthe presence of PsA, simple targeted physical
examination of the joints and entheses may facilitatereaching the threshold for the appropriate index ofsuspicion.
Important information is obtained through visualinspection of joints and through straightforwardexamination maneuvers. In the same way the integ-ument lends itself to visual diagnostic assessment, somay skin overlying peripheral joints and entheses.Erythema is often present overlying inflamed jointsof the hands and feet in PsA (Fig 2). Swelling aroundjoints may be appreciated through close visualinspection, although this feature may go unnoticedif overlying erythema is also subtle or absent.Contours of joints become less apparent with swell-ing, and this is more noticeable upon comparison touninvolved joints (Fig 3). Larger joints, such as theknee, may have overlying erythema when inflamed,and swelling is easier to visually appreciate in theselarger joints (Fig 4). In mutilating disease, hands withshortened fingers resulting from progressive osteol-ysis are readily apparent on visual inspection as acharacteristic deformity in PsA known as ‘‘opera-glass hands’’ (Fig 5). Mutilating PsA is more commonin men and it is more frequent with early onsetdisease, making early recognition of PsA in thissubset of patients essential. Ankylosis, or fusion, ofsmall joints, whichmaymanifest clinically with eitherfixed bent (contractures) or straight joints, is anothercommon deformity (Fig 5) noted through visualinspection.
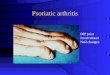
Uniform swelling of a finger or toe (Fig 6), or theappearance of a ‘‘sausage digit,’’ represents dactylitis,which occurs in up to 49% of those with PsA andresults from simultaneous inflammation of all threejoints and tenosynovitis of the involved digit.Because the toes are more commonly involved,32 itis essential to examine the feet with shoes and socksremoved when evaluating patients with psoriasis.Dactylitis of fingers is often accompanied by

Fig 2. Erythema overlying joints in psoriatic arthritis. Dullred erythema overlying inflamed joints of the foot.
Fig 3. Swollen joints in psoriatic arthritis over the secondand third metacarpophalangeal joints of the hands.
Fig 4. Swelling of the right knee in psoriatic arthritis.Swelling of larger joints such as the knee may be appre-ciated by visual inspection.
Fig 5. Opera glass hands in psoriatic arthritis. Mutilatingpsoriatic arthritis in which shortened fingers result fromprogressive erosive disease and osteolysis, leading tocollapse of the involved joints and telescoping of digits.Anykylosis or bending of the digits is also apparent.
J AM ACAD DERMATOL
VOLUME 63, NUMBER 5Garg and Gladman 737
psoriatic nail disease, which has been identified inmore than 80% of patients with PsA and less than50% of patients with psoriasis without arthritis.33,34 Inaddition, superficial tendons, such as the Achillestendon, may appear visibly swollen, especially whencompared to the contralateral tendon. While thereare specific measures to assess enthesitis,35 it is notexpected that the dermatologist would perform suchevaluations.
When joint and entheseal symptoms in PsA arepresent without obvious visual clues, targeted ex-amination maneuvers may facilitate the recognitionof skeletal involvement. Activation of range of mo-tion of the neck, shoulders, elbows, wrists, fingers,knees, ankles, and toes may elicit stiffness or pain.Specifically, one might stress the wrists, shoulders,elbows, finger joints, and toe joints to elicit pain.Dermatologists and rheumatologists have showntheir ability to elicit joint tenderness in a reliableway.36 It may also be possible for a dermatologist toelicit tenderness at the insertion of the Achillestendon and the plantar fascia.
Axial disease in PsA is easilymissed, partly becausethe examination of axial joints is fraught with poor
sensitivity and specificity because of the relativeinaccessibility of these joints. Such maneuvers havelimited roles, even in rheumatologypractice. Apatientoccasionally presents with obvious difficulties withspinal mobility. In some, range of motion or maneu-vers that stress the sacroiliac joint may elicit pain orstiffness. The loss of spinal mobility may be notedthrough simple attempts at anterior and lateral flex-ion. If axial disease is ultimately suspected, plain filmor magnetic resonance imaging (MRI) with fat sup-pressed signal (STIR images) in anticipation of therheumatology consultation may be considered. TableII compares the physical examination features in PsAwith other types of arthritis that may coexist withpsoriasis or that mimic PsA.
Laboratory tests. There are no laboratory teststhat specify a diagnosis of PsA. Erythrocyte sedimen-tation rate (ESR) and C-reactive protein (CRP) areunreliable in detecting the presence of PsA,5 andthey are more often elevated in RA, AS, and ReA.While not diagnostic for PsA, acute phase reactantsare prognostic for both joint destruction and survival

Fig 6. Dactylitis in psoriatic arthritis. Fusiform swelling ofa right thumb (A) and the fourth left toe (B) as a result ofinflammation of phalangeal joints along with entheses.
J AM ACAD DERMATOL
NOVEMBER 2010738 Garg and Gladman
and thus warrant evaluation for the PsA patient. HLA-B*27, present in 7% of North American whites, is alsonoted in 50% to 70% of patients with axial diseaseand less than 15% of those with peripheral disease inPsA, and its presence is independent of diseaseseverity.23 Although also not diagnostic of PsA,HLA-B*27, particularly in the presence of HLA-DR*07, is prognostic for the progression of jointdamage in PsA.37 Table III compares laboratoryevaluations in PsA with other types of arthritis thatmay coexist with psoriasis or that mimic PsA.
Imaging findingsJust as dermatologists apply the descriptive por-
tion of a histopathology report to the patient’spresentation for clinical pathologic correlation, theknowledgeable dermatologist may also analyze thedescription of the radiology report to assess if find-ings in psoriasis patients are consistent with PsA. Onplain radiographs, type of erosion and deformity, thepresence of periostitis, and the pattern of involve-ment assist in distinguishing PsA from other forms ofarthritis.
New bony proliferation, or periostitis, that isobserved adjacent to erosions and at sites of
entheseal attachments is an identifying featureunique to PsA among inflammatory arthropathies.Radiographically, it manifests as juxtaarticular fluffywhitening. Marginal surfaces of bone, which are lesswell protected by articular cartilage, are susceptibleto erosive changes early on in PsA (Fig 7, A).Marginal erosions in PsA may progress further toinvolve the central articular surface, resulting in thecharacteristic ‘‘pencil in cup’’ finding (Fig 7, B). Thistype of progressive osteolysis, or bone resorption,leads to dissolution of the joint and collapse of thephalanges and metacarpal bone, resulting in anopera glass or telescoping deformity of the digit.This type of deformity is unique to PsA. Deformitiesin PsA are distinguished by the presence of both lysisand ankylosis, which may occur in different joints ofthe same digit. Occasionally, bone loss from erosivedisease may be extensive enough to also causesubluxations.
The correlation between symptoms and radio-logic evidence of spondylitis and sacroiliitis may bepoor, and symptoms of morning stiffness in thelower back or buttocks may not be further substan-tiated with findings on plain radiographic film. Thispoor sensitivity also accounts for one of the reasonsthat axial disease in PsA is easily missed. Erosions atthe sacroiliac joint in PsA are typically asymmetricand unilateral. With time, the joint space between thesacrum and the ilium becomes obliterated because ofsclerosis of the bone. With spinal disease in PsA,inflammatory granulation tissue at the junction of thedisk cartilage and the margin of the vertebral body isreplaced by bony structures called syndesmo-phytes—which ultimately bridge adjacent vertebralbodies, resulting in ankylosis of the spine. In PsA,syndesmophytes are bulky, they may involve oneside of the vertebral body and not the other at anygiven level (asymmetric), and they may affect thespine intermittently with skip areas. This is in con-trast to syndesmophytes in AS, which are thin,symmetric, and continuous (Fig 8). Other commonaxial radiographic findings in PsA include paraver-tebral ossification and, in advanced disease, verte-bral fusion with disk calcification.
Enthesitis may be difficult to assess with plainradiographs, especially early in the course of disease.Erosion and periostitis may be noted at the site ofinsertion of tendons to bone, such as at the site ofinsertion of the Achilles tendon to the calcaneus. MRIand ultrasound are of greater value than plainradiographic film when evaluating for the presenceof enthesitis. T1-weighted MRI is useful in definingthe anatomic detail of soft tissue. In this sequence, fatand bone marrow have a bright signal and appearwhite in color, muscle has an intermediate signal

Table II. Physical examination in psoriatic arthritis and in types of arthritis that may coexist with psoriasis orthat mimic psoriatic arthritis
Physical
examination PsA OA Gout RA AS ReA
Pattern of jointinvolvement
Oligoarthritis,polyarthritis,axial
Monoarthritis,oligoarthritis
Monoarthritis,oligoarthritis,polyarthritis
Polyarthritis Axial plus largeperipheral joints,asymmetric
Oligoarthritis,polyarthritis.axial
Distribution Peripheral(includingDIP) and axial
Peripheral(includingDIP) and axial
Peripheral Peripheral(includingMCP)
Axial[[Peripheral Peripheral(includingDIP) and axial
Symmetry Asymmetric Asymmetric Asymmetric Symmetric Symmetric AsymmetricSwelling andoverlyingerythemaof joints
Present Absent Present Present Absent Present
Enthesitis Present Absent Absent Absent Present PresentDactylitis 48% Absent Absent Absent Absent OccasionalSynovitis Present Absent Absent Present Present in some PresentTypicaldeformity
Opera glass(telescoping)digit
Heberden andBouchardnodes
Tophi Swan neck,boutonniere,zig zag
Spinal ankylosis Spinal ankylosis
AS, Ankylosing spondylitis; DIP, distal interphalangeal; MCP, metacarpophalangeal; OA, osteoarthritis; PsA, psoriatic arthritis; RA, rheumatoid
arthritis; ReA, reactive arthritis.
Table III. Laboratory evaluations in psoriatic arthritis and in types of arthritis that may coexist with psoriasis orthat mimic psoriatic arthritis
Laboratory test PsA OA Gout RA AS ReA
ESR 1/� Normal Normal (elevatedduring attack)
Elevated 1/� 1/�
CRP 1/� Normal Normal Elevated 1/� 1/�RF Usually absent Usually absent Absent Usually present Usually absent Usually absentCCP Ab Usually absent Absent Absent Present Usually absent Usually absentHLA*B27 15-70% 4-8% 4-8% 4-8% 90% 50-85%Synovialaspirate
Inflammatory Noninflammatory Inflammatory Inflammatory Inflammatory Inflammatory
AS, Ankylosing spondylitis; CCP, citrullinated-containing proteins; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; HLA, human
leukocyte antigen; OA, osteoarthritis; PsA, psoriatic arthritis; RA, rheumatoid arthritis; ReA, reactive arthritis; RF, rheumatoid arthritis.
J AM ACAD DERMATOL
VOLUME 63, NUMBER 5Garg and Gladman 739
intensity and appears dark, while the tendons andligaments appear black in color. As noted on T1-weighted MRI, thickening of the plantar fascia in thecontext of plantar stiffness is suggestive of plantarenthesitis (Fig 9, A). T1-weighted MRI may also makeapparent edema and fluid collections near sites ofattachment of tendon to bone. Fat and marrow sharethe same signal intensity as fluid or edema. Bysuppressing the fat and marrow signal through aT2-weighted STIR signal, fluid and edema are iso-lated for improved visualization (Fig 9, B). The use ofultrasound for the detection of enthesitis has recentlybeen proposed. Indeed, enthesitis was detectedcommonly among patients with psoriasis who havenot been diagnosed with PsA.38,39
Table IV compares imaging findings in PsA withother types of arthritis that may coexist with psoriasisor mimic PsA.
REACTIVE ARTHRITISKey pointsd Reactive arthritis (ReA) is distinguished frompsoriatic arthritis (PsA) by its acute onset ofarthritis and enthesitis, and by the additiveinvolvement of new joints over days
d While ReA and PsA share extraarticularsymptoms, urethritis, cervicitis, and bowelsymptoms are also features that distinguishReA

Fig 7. Marginal erosion and periostitis in psoriatic arthritis. Characteristic radiographic changesin psoriatic arthritis include marginal erosions at several joints of the hands and best noted atthe second, third, and fourth metacarpophalangeal joints in this patient. Juxtaarticular fluffywhitening, known as periostitis, also occurs at several joints and may be best appreciated at thesecond, third, and fourth proximal interphalangeal joints in this patient (A). B, Pencil in cupdeformity. Marginal erosions progressing centrally give rise to the ‘‘pencil in cup’’ deformitynoted on the fifth metatarsophalangeal joint. (Photographs courtesy of Eugene Kissin, MD,Boston Medical Center.)
J AM ACAD DERMATOL
NOVEMBER 2010740 Garg and Gladman
d Patterns of asymmetric peripheral and axialjoint involvement are similar in ReA and PsA
d Physical examination, laboratory testing,and imaging findings may not distinguishReA from PsA
EpidemiologyReA affects individuals 20 to 40 years of age,
similar to the range in PsA. Men and women areaffected equally by the foodborne enteric form ofReA, while the veneral form affects men nine times asoften as women.
Clinical features. Although ReA shares a num-ber of features with PsA, it is distinguished by itsrelative acute onset of arthritis and enthesitis, whichtends to occur within days of a triggering infection. Ingeneral, although stiffness in ReA may be indistin-guishable from that in PsA, pain and limitation inmovement tend to be more severe in ReA. In bothPsA and ReA, swelling and overlying erythema of theinvolved joints are apparent.
Patterns of joint involvement. ReA affectslower extremity and foot joints more commonly,whereas PsA often involves peripheral joints ofthe upper extremities. Both PsA and ReA involvethe peripheral joints asymmetrically. Unlike PsA
however, there is additive involvement of new jointsover the course of days in ReA. Sacroiliitis occurs inless than 10% of acute cases of ReA, but it is presentin half of patients with chronic disease. Severeankylosing disease of the spine occurs in only 5%of patients with ReA.
Enthesitis and dactylitis. Enthesitis is a fre-quent occurrence in ReA. Furthermore, sites ofenthesial involvement are similar in ReA and PsA,and both often develop dactylitis of toes (Fig 10) andfingers with Achilles tendonitis and plantar fasciitis.
Associated extraarticular symptoms. In ReA,conjunctivitis or uveitis is typically bilateral.Urethritis or cervicitis along with bowel symptomsfurther characterize ReA but not PsA.
Physical examination. Axial and peripheralassessments in ReA are similar to those in PsA, anddistinction by physical examination alone betweenPsA with limited or inconspicuous psoriasis and ReAwith psoriasiform dermatitis may be difficult.
Laboratory tests. While HLA-B*27 is present in50% to 85% of ReA patients, it is neither necessarynor sufficient for the diagnosis, as is the case in PsA.
Imaging findings. The appearance of joint ero-sions and enthesitis, whether peripheral or axial, inReA may be indistinguishable from those in PsA.

Fig 9. Plantar thickening and edema in a patient withpsoriatic arthritis. A, T1-weighted magnetic resonanceimaging reveals thickened ([4 mm) plantar fascia (arrow).B, T2-weighted fat suppressed signal highlights edema(arrow) in the bone marrow of the calcaneus close to thesite of attachment of the plantar fascia.
Fig 8. Syndesmophytes in psoriatic arthritis. Syndesmo-phytes (arrows) are bulky, asymmetric, and affect thespine intermittently with skip areas, which is in contrast toankylosing spondylitis, in which syndesmophytes are thin,symmetrical, and continuous.
J AM ACAD DERMATOL
VOLUME 63, NUMBER 5Garg and Gladman 741
OSTEOARTHRITISKey pointsd Osteoarthritis (OA) occurs in older individ-uals as compared with psoriatic arthritis(PsA)
d Onset, quality of discomfort, and pattern ofjoint involvement are similar in OA and PsA
d Identification of Heberden and Bouchardnodes may distinguish OA from distal pha-langeal (DIP) and proximal interphalangeal(PIP) involvement, respectively, in PsA
d Enthesitis and extraarticular symptoms arenot features of OA
d Osteophyte formation, joint space narrow-ing, and the absence of erosions distinguishOA from PsA on plain radiographic film
EpidemiologyOA occurs in 30% of individuals between 45 and
65 years of age, but it affects 80% of people by theireighth decade of life. Symptomatic OA before 45years of age andwithout predisposing factors such asobesity is rare. As such, OA occurs in an olderpopulation than does PsA. The disease is equallycommon among men and women 45 to 55 years ofage, after which OA becomes more common amongwomen. In addition to age and obesity, trauma to ajoint is a risk factor for the development of OA, andthis has also been postulated as a triggering factor inPsA.40,41
Clinical features. The onset of symptoms in OAis somewhat gradual, as it is in PsA. The quality of
discomfort in OA, which may be similar to that inPsA, is a deep, dull pain localized to the involvedjoints, although hip pain in OA is often referred toinguinal area, buttocks, or the proximal thigh. Unlikein PsA, discomfort in OA becomes worse withactivity, is relieved by rest, and may become persis-tent with nocturnal exacerbations in advanceddisease. Although traditionally considered nonin-flammatory, OA may also cause morning stiffness,especially in older individuals. Morning stiffness inOA, unlike in PsA, is typically short lived, lasting 30minutes or less.
Patterns of joint involvement. Patterns ofperipheral joint involvement in OA may be similarto PsA, making the two a challenge to distinguish inthe patient with psoriasis. OA typically involves DIPand proximal interphalangeal (PIP) joints, the base

Table IV. Radiographic findings in psoriatic arthritis and in types of arthritis that may coexist with psoriasis orthat mimic psoriatic arthritis
Plain film finding PsA OA Gout RA AS ReA
Periostitis Present Absent Absent Absent Absent AbsentOsteopenia Absent Absent Absent Present Absent AbsentJoint spacenarrowing
Late manifestations Present Absent Present Late manifestation Late manifestation
Erosion Marginal and central Absent C- shaped Marginal Marginal MarginalSacroilitis Present Absent Absent Absent Present Present
AS, Ankylosing spondylitis; OA, osteoarthritis; PsA, psoriatic arthritis; RA, rheumatoid arthritis; ReA, reactive arthritis.
J AM ACAD DERMATOL
NOVEMBER 2010742 Garg and Gladman
of the thumb, and large weight-bearing joints, suchas the knees or hips. As with PsA, OA may affectany part of the axial skeleton independently ofperipheral joints.
Enthesitis and dactylitis. Enthesitis is not afeature of OA. MRI studies assessing enthesitiswere able to distinguish patients with PsA from thosewith OA.42 As such, patients with OA do not developdactylitis of fingers and toes, Achilles tendonitis, orplantar fasciitis, as might patients with PsA. It shouldbe noted, however, that patients with OA—particu-larly those who have diffuse idiopathic skeletalhyperostosis (DISH)—may have heel spurs.
Associated extraarticular symptoms. There isan absence of extraarticular systemic features in OA.
Physical examination. In OA, the DIP, PIP, andother weight-bearing joints may have tendernesslocalized to the involved joint. These joints, andespecially the knee, may also demonstrate creptius,the sensation of bone on bone rubbing with move-ment. Firm bony enlargements over the DIP(Heberden nodes) and PIP (Bouchard nodes) joints(Fig 11) are often readily apparent as characteristicclinical features in OA and should be differentiatedfrom the soft swelling resulting from effusion orproliferated synovium in inflammatory arthritis, in-cluding PsA.
Laboratory tests. Laboratory analyses in OA arenormal. There is no strong association with any HLAalleles.
Imaging findings. Although there is bony pro-liferation in the form of an osteophyte (bone spur) inOA, periostitis typical of PsA is absent. Erosions arealso absent in typical OA. An uncommon erosivevariant of OA may be more difficult to distinguish onthe basis of erosions alone. In erosive OA, ‘‘seagull’’shaped erosions are noted on the central articularsurfaces along with osteophytes, both of which helpdistinguish this rare variety of OA from PsA. OA ofthe spine may also be readily distinguished bypresence of joint space narrowing and osteophytesrather than syndesmophytes.
GOUTKey pointsd Gout occurs in older individuals as com-pared with psoriatic arthritis (PsA)
d In contrast to PsA, an attack of gout isabrupt, causes severe pain, and is followedby an obligatory period of remission
d While monoarticular gout may be distin-guished from the pattern of involvement inPsA, polyarticular gout in a patient withpsoriasis bears resemblance to PsA
d Although a swollen toe in gout may resembledactylitis in PsA, enthesitis is not a feature ofgout
d The presence of tophi is the best physicalclue to the diagnosis of gout
d Elevated serum uric acid may be noted inpatients with either gout or PSA
d On plain radiographic film, gout is distin-guished fromPsAby thepresence of C-shapederosions and absence of periostitis
EpidemiologyGout affects men about twice as often as women.
Men are afflicted between the ages of 30 and 50 yearsof age, a range that includes the peak age of onset inPsA. Because estrogenic hormones have a uricosuriceffect, women do not become affected by gout untilafter menopause, with peak age of onset between 50and 70 years of age—an age onset range less typicalthan that of PsA.
Clinical features. In stark contrast to PsA, ar-thropathy in early gout has an abrupt onset. Gout isalso distinguished from PsA by causing intense jointpain that is further aggravated by movement. Patientsoften cannot tolerate bed sheets over the affectedarea. In simple gout, painful episodes last up to 10days, after which time there is a unique period ofsymptom-free ‘‘intercritical remission’’ that does notoccur in PsA.Morning stiffness is not a feature of gout.
Patterns of joint involvement. In gout, it ismost common for a single metatarsophalangeal

Fig 10. Dactylitis in reactive arthritis. Uniform swelling ofthe right fourth toe in a patient with a psoriasiformdermatitis that mimics psoriasis. This presentation bearsa similarity to psoriatic arthritis.
Fig 11. Heberden and Bouchard nodes in osteoarthritis.Psoriasis patient with bony enlargements overlying thedistal interphalangeal (Heberden nodes, red arrows)and proximal interphalangeal (Bouchard nodes, yellowarrows) joints suggestive of osteoarthritis and not psoriaticarthritis.
J AM ACAD DERMATOL
VOLUME 63, NUMBER 5Garg and Gladman 743
(MTP) joint of the first toe to be involved in initialacute episodes, although other tarsal, ankle, andknee joints may be affected instead. Early on ingout, one joint is involved. With uric acid elevationand after several attacks, gout patients may developan asymmetric polyarticular arthritis involving sev-eral joints of the fingers (Fig 12), wrists, elbows,knees, ankles, and heels, a pattern that bearssimilarity to polyarticular disease in PsA. The pol-yarticular variety of gout is more common inpostmenopausal women with renal insufficiencywho are taking a diuretic, and in men with hyper-tension and a significant alcohol intake history.Even when multiple joints are affected, gout doesnot tend to involve the axial skeleton, which is arather common occurrence in PsA. By the timepatients develop polyarticular gout, they often havetophi, which are deposits of uric acid crystals in thetissues. These occur in the ears, the olecranonbursa, and other extensor surfaces, or over thejoints themselves.
Enthesitis and dactylitis. Enthesitis is not afeature of gout. Although an entire finger or toemay be swollen in the course of a gouty attackinvolving the small joints of hands or feet, it is notdescribed as dactylitis.
Associated extraarticular symptoms. In gout,there is an absence of extraarticular systemicfeatures.
Physical examination. The presence of tophi,more common in patients with polyarticular disease,is the best physical clue to the diagnosis of gout.A gouty joint that is active has intense overlying rederythema and swelling, and it is warm to touch andexquisitely tender. The joint affected by PsA, bycomparison, tends to be less impressive. However,the distinction between a joint chronically affected
by gout and dactylitis may be difficult in the patientwith psoriasis suspected to have PsA (Fig 13).
Laboratory tests. Patients with gout usuallyhave elevated serum uric acid, although the samemay be apparent in patients with psoriasis. Thecriterion standard for diagnosis of gout and distinc-tion from PsA involves analysis of the synovialaspirate, which shows birefringent needle-shapedmonosodium urate intracellular crystals and elevatedcell counts.
Imaging findings. In gout, erosions have acharacteristic well defined punched-out C-shapewith overhanging margins (Marte sign) that appeardistinct frommarginal or central erosions in PsA. Softtissue swelling and calcifications representing goutytophi may also result in subluxation of the joint.Periostitis is absent in joints affected by gout.
RHEUMATOID ARTHRITISKey pointsd Rheumatoid arthritis (RA) is an inflamma-tory arthritis with features similar to psori-atic arthritis (PsA), including pain, swelling,morning stiffness, pattern of joint involve-ment, and extraarticular features
d Enthesitis is not a feature of RAd Swan neck, Boutonniere, and zig-zag defor-mities characterize RA and may distinguish itfrom PsA
d Serologic markers in the appropriate clinicalcontext are useful in establishing a diagnosisof RA and distinguishing it from PsA
d Symmetry of marginal erosions and absenceof periostitis noted on plain radiographicfilm serve to distinguish RA from PsA

Fig 12. Polyarticular gout. A psoriasis patient with asym-metric polyarticular gout involving several joints of thefingers, a presentation which may be mistaken for psori-atic arthritis.
Fig 13. Tophaceous gout in a patient with psoriasis.Psoriasis patient with gout involving the fourth toe, apresentation that may be mistaken for dactylitis in psoriaticarthritis.
J AM ACAD DERMATOL
NOVEMBER 2010744 Garg and Gladman
EpidemiologyRA affects individuals in their fourth and fifth
decades of life. However, unlike PsA, RA increases inincidence with age and affects women three timesmore often than men.
Clinical features. Although RA begins some-what insidiously, it tends to be unremittingly pro-gressive soon after onset. RA is distinguished bycausing intense joint pain that is improved withactivity and exercise and aggravated by rest. While allpatients with RA complain of morning stiffness, onlyabout half of PsA patients give the same complaint.The stiffness in RA is alsomore severe and prolongedthan most patients with PsA. Although involvedjoints in RA demonstrate swelling as a result ofsynovitis and effusion, there is usually no erythemaoverlying them, as is often the case in PsA.
Patterns of joint involvementIn RA, there is inflammatory polyarthritis affecting
the hands, wrists, and knees that is uniformly sym-metric, whereas joint involvement in PsA tends not tobe. Involvement of metacarpophalangeal (MCP) andPIP joints of both hands and the MTP joints of bothfeet with sparing of DIP joints of the hands and feetare characteristic of RA. In PsA, DIP joints arefrequently involved in oligoarticular and polyarticu-lar disease and MCP joints are usually involved in thepolyarticular form of the disease. RA tends to affectthe same joint in all of the digits, whereas PsA is morelikely to affect all of the joints in any one digit. ThisPsA pattern is referred to as the Ray distribution.
Axial involvement in RA is typically limited tocervical spine disease and is related to inflammatorydisease in the atlantoaxial joint with subluxation.There is usually sparing of lumbar spine and sacrumin RA, whereas in PsA, the sacrum and lumbar spineare frequently involved.
Enthesitis and dactylitis. Entheseal involve-ment is not a feature of RA.
Associated extraarticular symptoms. Ocularinvolvement is infrequent in both RA and PsA. Siccasymptoms (epicleritis or scleritis) rather than theuveitis that occurs with PsA is more typical in RA.Patients with RA may have a number of additionalextraarticular features that are usually absent in PsA,most notably rheumatoid nodules which occur in atleast 20% of RA patients. Other extraarticular featuresinclude cutaneous vasculitis, pericarditis, pleuritis,pneumonitis, and interstitial fibrosis of the lungs.
Physical examination. Joints in RA are moreswollen and tender than joints in PsA. Althoughinflamed, joints affected by RA tend not to haveoverlying erythema, unlike the joints in PsA. Whilethe opera glass hand deformity is unique to PsA,the swan neck (hyperextension of PIP joint andcompensatory flexion at DIP joint; Fig 14) andBoutonniere (flexion contracture at PIP joint andextension at DIP joint) deformities characterize RA.Zig-zag deformity, in which there is radial deviationof the wrist with ulnar deviation of fingers, is alsocharacteristic in RA (Fig 15).
Laboratory tests. Present in more than twothirds of RA patients, RF helps to confirm the diag-nosis in an individual with clinical presentation

Fig 15. Z deformity in rheumatoid arthritis. Z deformity,with radial deviation of the wrist and ulnar deviation of thefingers, is suggestive of rheumatoid arthritis.
Fig 14. Swan neck deformity in rheumatoid arthritis.Hyperextension of the proximal interphalangeal jointand hyperflexion of the distal interphalangeal joint resultsin a deformity that characterizes rheumatoid arthritis.
J AM ACAD DERMATOL
VOLUME 63, NUMBER 5Garg and Gladman 745
suggestive of RA. However, RF is also noted in 5% ofhealthy adults. Moreover, its frequency increasesfurther with age, and up to 20% of individuals over65 years of age are seropositive. The serologicpresence of RF is also noted in a number of otherchronic infectious and autoimmune and inflamma-tory conditions, including up to 5% to 10% ofindividuals with PsA.5,43 Antibody to citrullinated-containing proteins has significantly improved sen-sitivity and specificity over RF for establishing thediagnosis of RA. Present in less than 7% of PsApatients,43 citrullinated-containing proteins antibodyis a better serologic test than RF to characterize an RApatient with inflammatory polyarthritis and a derma-titis that may mimic psoriasis (ie, seborrheic derma-titis) and to distinguish this presentation from PsA.
Imaging findings. In RA, erosions appear earlyand involve the MCP and MTP joints almost uni-formly and symmetrically. This is in contrast topolyarticular PsA, in which some but not all MCPand MTP joints are involved asymmetrically.Erosions in RA tend to stay marginal, whereas inPsA they also move away from the margin towardsthe center of the joint. Moreover, radiographs ofhands affected by RA will feature the Z deformity,showing radial deviation of the wrist and ulnardeviation of fingers. While there is juxtaarticularnew bone formation in PsA, bone loss, or osteope-nia, is the rule in RA.
ANKYLOSING SPONDYLITISKey pointsd Ankylosing spondylitis (AS) has earlier onsetof disease than psoriatic arthritis (PsA)
d AS is largely a disease of the axial skeletonwith bilateral sacroiliitis and ascending con-tinuous involvement of the spine
d AS is unremittingly progressive, with moresevere pain, stiffness, and limitation in axialmovement than PsA
d Extraarticular symptoms, including iritis,urethritis, and inflammatory bowel disease,are more common in AS than PsA
d Human leukocyte antigeneB*27 is present in90% of AS patients, but the allele is alsocommon among patients with PsA
d Bilateral and symmetrical erosions and scle-rosis of the sacroiliac joints, as well as con-tinuous ascending ankylosis of the spine, isnoted on plain radiographic film in AS, un-like in most cases of axial PsA
EpidemiologyAS, occurring in the second or third decade of life,
has an earlier onset of disease than PsA. Also incontrast to PsA, AS affects men at a rate of four to 10times that of women.
Clinical features. AS begins somewhat gradu-ally. In contrast to PsA, AS tends to be more painfuland progressive soon after onset. Patients with ASmore often progress to full axial ankylosis withinyears of diagnosis.44 While all patients with AScomplain of morning stiffness, only about half ofPsA patients give the same complaint. The pain andstiffness in AS tends to be more severe and pro-longed, and consequently the limitation in move-ment is also more restricted in AS as compared withPsA.
Patterns of joint involvement. AS is largely adisease of the axial skeleton. As a rule in AS, there isbilateral sacroiliitis, from which ascending involve-ment of the spine affects vertebrae continuouslywithout skipping. The presence of spondylitis in theabsence of sacroiliitis is highly unusual. This is incontrast to PsA, in which spondylitis may occur in the

Table V. Classification Criteria for Psoriatic Arthritis(CASPAR) criteria for the diagnosis of psoriaticarthritis
The Classification Criteria for Psoriatic Arthritis (CASPAR)criteria consist of established inflammatory articulardisease* with at least 3 points from the followingfeatures:
A. Current psoriasis (assigned a score of 2; all otherfeatures are assigned a score of 1)
B. A personal history of psoriasis (unless current pso-riasis is present)
C. A family history of psoriasis (unless current psori-asis is present or there is a personal history ofpsoriasis)
D. Current dactylitis or history of dactylitis recorded bya rheumatologist
E. Juxtaarticular new bone formationF. Rheumatoid factor negativityG. Typical psoriatic nail dystrophy including onycholy-
sis, pitting, and hyperkeratosis
*Prolonged morning or immobility-induced stiffness and tender
and swollen joints suggest an inflammatory joint disease.
J AM ACAD DERMATOL
NOVEMBER 2010746 Garg and Gladman
absence of sacroiliitis or in which spondylitis mayoccur before the onset of sacroiliitis. Involvement ofperipheral joints in AS, although infrequent, maybear resemblance to patterns in PsA with involve-ment of larger lower extremity joints such as theknees. Peripheral joint involvement is unusual inprimary AS.
Enthesitis and dactylitis. Enthesial inflamma-tion is most common in AS with the pelvis andspine as primary sites of involvement, as opposedto both axial and peripheral involvement in pa-tients with PsA. Enthesitis in AS is also continuousfrom sacrum to cervical spine which contrasts withPsA in which the sacroiliac joint is involved asym-metrically and in which spinal enthuses may beinvolved discontinuously. Dactylitis is not a featureof AS.
Associated extraarticular symptoms. AS isassociated with extraarticular features that aretypical to the spondyloarthropathies. These in-clude iritis, urethritis, and inflammatory boweldisease. About 10% of patients with AS also havepsoriasis without the additional clinical features ofpsoriatic arthritis. Patients with AS are also suscep-tible to dilatation of the base of the aorta becauseof aortitis, and this may also result in cardiacconduction abnormalities.
Laboratory tests. HLA-B*27 is present in 90%of AS patients. While it is neither necessary norsufficient for the diagnosis, the recently publishedAnkylosing Spondylitis Assessment (ASAS) groupcriteria for spondyloarthritis relies on the pres-ence of HLA-B*27. CRP is elevated in half thepatients with AS making it an unreliable bio-marker to detect disease, similar to its applicationto PsA.
Imaging findings. AS results in bilateral andsymmetrical erosions and sclerosis of the sacroiliacjoints, as well as continuous ascending ankylosis ofthe spine. In PsA, there may be cervical spineinvolvement with relative sparing of thoracolumbarspine, and even the sacroiliac joints. Because of this,axial function and mobility are more restricted in AScompared with PsA. Syndesmophytes in AS are moredelicate but affect the vertebrae continuously, whilesyndesmophytes in PsA are bulky and affect thespine asynchronously. Peripheral joint erosions inAS, when present, are indistinguishable from ero-sions in PsA, although periosteal reaction is nottypically noted in AS.
CONCLUSIONIn general, PsA may be suspected in a 30- to 40-
year-old man or woman with psoriasis and an
asymmetric inflammatory peripheral and/or axialarthritis with enthesitis and dactylitis, prolongedmorning stiffness, joint discomfort, erythema andswelling of the involved joints, and periostitis, mar-ginal or central erosions, and characteristic jointdeformities.
PsA is a disease in which some degree ofdiagnostic uncertainty for difficult cases existseven among rheumatologists. Although no diag-nostic criteria exist, the Group for Research andAssessment of Psoriasis and Psoriatic Arthritis(GRAPPA) has developed sensitive and specificcriteria, known as CASPAR (Classification Criteriafor Psoriatic Arthritis43; Table V), which has beenvalidated among rheumatologists and also in afamily practice setting.45 The development andvalidation of classification criteria for use amongdermatologists will be a focus of investigation forGRAPPA. In the interim, dermatologists shouldremain observant of symptoms and signs thatmight suggest musculoskeletal involvement, espe-cially given the established morbidities affectingPsA patients.46 It is becoming more evident thatthe paradigm of managing patients with psoriasisis shifting towards a multidisciplinary approach,and it is important that dermatologists, as earlycaretakers of psoriasis patients, are attentivelyaware of signs of comorbidities, especially PsA.
We thank Ms Daniella Adrien for her assistance in thepreparation of this manuscript and Dr Alpa G. Garg for herexpert guidance of our use of radiographic images.

J AM ACAD DERMATOL
VOLUME 63, NUMBER 5Garg and Gladman 747
REFERENCES
1. Wright V, Moll JMH. Psoriatic arthritis. In: Seronegative poly-
arthritis. Amsterdam: Elsevier Scientific Publishing; 1976.
2. Gladman DD. Psoriatic arthritis. Dermatol Ther 2004;17:
350-63.
3. Wright V. Psoriatic arthritis. A comparative radiographic study
of rheumatoid arthritis and arthritis associated with psoriasis.
Ann Rheum Dis 1961;20:123-32.
4. Coulton BL, Thomson K, Symmons DP, Popert AJ. Outcome in
patients hospitalised for psoriatic arthritis. Clin Rheumatol
1989;8:261-5.
5. Gladman DD, Shuckett R, Russell ML, Thorne JC, Schachter RK.
Psoriatic arthritis (PSA)—an analysis of 220 patients. Q J Med
1987;62:127-41.
6. Kane D, Stafford L, Bresnihan B, FitzGerald O. A prospective,
clinical and radiological study of early psoriatic arthritis: an
early synovitis clinic experience. Rheumatology (Oxford) 2003;
42:1460-8.
7. McHugh NJ, Balachrishnan C, Jones SM. Progression of
peripheral joint disease in psoriatic arthritis: a 5-yr prospective
study. Rheumatology (Oxford) 2003;42:778-83.
8. Setty AR, Choi HK. Psoriatic arthritis epidemiology. Curr
Rheumatol Rep 2007;9:449-54.
9. Torre Alonso JC, Rodriguez Perez A, Arribas Castrillo JM, Ballina
Garcia J, Riestra Noriega JL, Lopez Larrea C. Psoriatic arthritis
(PA): a clinical, immunological and radiological study of 180
patients. Br J Rheumatol 1991;30:245-50.
10. Sokoll KB, Helliwell PS. Comparison of disability and quality of
life in rheumatoid and psoriatic arthritis. J Rheumatol 2001;28:
1842-6.
11. Husted JA, Tom BD, Farewell VT, Schentag CT, Gladman DD. A
longitudinal study of the effect of disease activity and clinical
damage on physical function over the course of psoriatic
arthritis: does the effect change over time? Arthritis Rheum
2007;56:840-9.
12. Gladman DD. Mortality in psoriatic arthritis. Clin Exp Rheuma-
tol 2008;26(5 suppl. 51):S62-5.
13. Radtke MA, Reich K, Blome C, Rustenbach S, Augustin M.
Prevalence and clinical features of psoriatic arthritis and joint
complaints in 2009 patients with psoriasis: results of a German
national survey. J Eur Acad Dermatol Venereol 2009;23:683-91.
14. Mease P, Goffe BS. Diagnosis and treatment of psoriatic
arthritis. J Am Acad Dermatol 2005;52:1-19.
15. Gladman DD. Psoriatic arthritis. Baillieres Clin Rheumatol 1995;
9:319-29.
16. Gelfand JM, Gladman DD, Mease PJ, Smith N, Margolis DJ,
Nijsten T, et al. Epidemiology of psoriatic arthritis in the
population of the United States. J Am Acad Dermatol Oct
2005;53:573.
17. Scarpa R, Oriente P, Pucino A, Torella M, Vignone L, Riccio A,
et al. Psoriatic arthritis in psoriatic patients. Br J Rheumatol
1984;23:246-50.
18. Zachariae H. Prevalence of joint disease in patients with
psoriasis: implications for therapy. Am J Clin Dermatol 2003;4:
441-7.
19. Leonard DG, O’Duffy JD, Rogers RS. Prospective analysis of
psoriatic arthritis in patients hospitalized for psoriasis. Mayo
Clin Proc 1978;53:511-8.
20. Alamanos Y, Voulgari PV, Drosos AA. Incidence and prevalence
of psoriatic arthritis: a systematic review. J Rheumatol 2008;35:
1354-8.
21. Reich K, Kruger K, Mossner R, Augustin M. Epidemiology and
clinical pattern of psoriatic arthritis in Germany: a prospective
interdisciplinary epidemiological study of 1511 patients with
plaque-type psoriasis. Br J Dermatol 2009;160:1040-7.
22. Wilson FC, Icen M, Crowson CS, McEvoy MT, Gabriel SE,
Kremers HM. Time trends in epidemiology and characteristics
of psoriatic arthritis over 3 decades: a population-based study.
J Rheumatol 2009;36:361-7.
23. Chandran V. Epidemiology of psoriatic arthritis. J Rheumatol
2009;36:213-5.
24. Stoll ML, Lio P, Sundel RP, Nigrovic PA. Comparison of
Vancouver and International League of Associations for rheu-
matology classification criteria for juvenile psoriatic arthritis.
Arthritis Rheum 2008;59:51-8.
25. Shore A, Ansell BM. Juvenile psoriatic arthritis—an analysis of
60 cases. J Pediatr 1982;100:529-35.
26. Southwood TR, Petty RE, Malleson PN, Delgado EA, Hunt DW,
Wood B, et al. Psoriatic arthritis in children. Arthritis Rheum
1989;32:1007-13.
27. Khan M, Schentag C, Gladman DD. Clinical and radiological
changes during psoriatic arthritis disease progression.
J Rheumatol 2003;30:1022-6.
28. Jones SM, Armas JB, Cohen MG, Lovell CR, Evison G, McHugh
NJ. Psoriatic arthritis: outcome of disease subsets and rela-
tionship of joint disease to nail and skin disease. Br J
Rheumatol 1994;33:834-9.
29. Veale D, Rogers S, Fitzgerald O. Classification of clinical subsets
in psoriatic arthritis. Br J Rheumatol 1994;33:133-8.
30. Fernandez-Sueiro JL, Willisch A, Pertega-Dıaz S, Tasende JA,
Fernandez-Lopez C, Galdo F, et al. Evaluation of ankylosing spon-
dylitis spinal mobility measurements in the assessment of spinal
involvement in psoriatic arthritis. Arthritis Rheum 2009;61:386-92.
31. McGonagle D. Enthesitis: an autoinflammatory lesion linking
nail and joint involvement in psoriatic disease. J Eur Acad
Dermatol Venereol 2009;23(suppl 1):9-13.
32. Brockbank JE, Stein M, Schentag CT, Gladman DD. Dactylitis in
psoriatic arthritis: a marker for disease severity? Ann Rheum
Dis 2005;64:188-90.
33. Gladman DD, Anhorn KA, Schachter RK, Mervart H. HLA
antigens in psoriatic arthritis. J Rheumatol 1986;13:586-92.
34. Griffiths CE, Barker JN. Pathogenesis and clinical features of
psoriasis. Lancet 2007;370:263-71.
35. Gladman DD, Inman RD, Cook RJ, van der Heijde D, Landewe
RB, Braun J, et al. International spondyloarthritis interobserver
reliability exercise—the INSPIRE study: I. Assessment of spinal
measures. J Rheumatol 2007;34:1733-9.
36. Chandran V, Gottlieb A, Cook RJ, Duffin KC, Garg A, Helliwell P,
et al. International multicenter psoriasis and psoriatic arthritis
reliability trial for the assessment of skin, joints, nails, and
dactylitis. Arthritis Rheum 2009;61:1235-42.
37. Gladman DD, Farewell VT, Kopciuk KA, Cook RJ. HLA markers
and progression in psoriatic arthritis. J Rheumatol 1998;25:730-3.
38. Gisondi P, Tinazzi I, El-Dalati G, Gallo M, Biasi D, Barbara LM,
et al. Lower limb enthesopathy in patients with psoriasis
without clinical signs of arthropathy: a hospital-based case-
control study. Ann Rheum Dis 2008;67:26-30.
39. Girolomoni G, Gisondi P. Psoriasis and systemic inflammation:
underdiagnosed enthesopathy. J Eur Acad Dermatol Venereol
2009;23(suppl 1):3-8.
40. Olivieri I, Padula A, D’Angelo S, Scarpa R. Role of trauma in
psoriatic arthritis. J Rheumatol 2008;35:2085-7.
41. Pattison E, Harrison BJ, Griffiths CE, Silman AJ, Bruce IN. Environ-
mental risk factors for the development of psoriatic arthritis:
results from a case-control study. Ann RheumDis 2008;67:672-6.
42. Tan AL, Benjamin M, Toumi H, Grainger AJ, Tanner SF, Emery P,
et al. The relationship between the extensor tendon enthesis
and the nail in distal interphalangeal joint disease in psoriatic
arthritis—a high-resolution MRI and histological study. Rheu-
matology (Oxford) 2007;46:253-6.

J AM ACAD DERMATOL
NOVEMBER 2010748 Garg and Gladman
43. Taylor W, Gladman D, Helliwell P, Marchesoni A, Mease P,
Mielants H. Classification criteria for psoriatic arthritis: devel-
opment of new criteria from a large international study.
Arthritis Rheum 2006;54:2665-73.
44. Gladman DD. Clinical aspects of the spondyloarthropathies.
Am J Med Sci 1998;316:234-8.
45. Chandran V, Schentag CT, Gladman DD. Sensitivity and
specificity of the CASPAR criteria for psoriatic arthritis in a
family medicine clinic setting. J Rheumatol 2008;35:2069-70.
46. Gladman DD, Ang M, Su L, Tom BD, Schentag CT, Farewell VT.
Cardiovascular morbidity in psoriatic arthritis. Ann Rheum Dis
2009;68:1131-5.