Embed Size (px)
Citation preview

Reassurance seeking and depression in adults with mildintellectual disability
S. L. Hartley,1 A. Hayes Lickel2 & W. E. MacLean Jr2
1 Waisman Center, University of Wisconsin-Madison, Madison,WI, USA2 University of Wyoming, Laramie,WI, USA
Abstract
Background Adults with intellectual disability (ID)experience a high prevalence of depression.Yet,little research has investigated interpersonal pro-cesses related to depression in this population. Inthe general population, depressed persons behavein ways that elicit negative and rejecting reactionsfrom others. In particular, excessive reassuranceseeking, defined as excessively and persistentlyseeking assurance from others that one is lovableand worthy, indirectly contributes to depressivesymptoms through evoking negative and rejectingsocial interactions. We examined the relationbetween excessive reassurance seeking, negative andrejecting social interactions and depression in adultswith mild ID.Method Eighty-seven adults with mild ID and staffcompleted the Glasgow Depression Scale for peoplewith a Learning Disorder and the Reassurance-Seeking Scale. In addition, adults with mild IDreported on their experience of negative social inter-actions, and staff rated their relative preference tointeract with the adult with mild ID. A meditationalmodel of the indirect effect of excessive reassurance
seeking on depressive symptoms via negative andrejecting social interactions was tested.Results Excessive reassurance seeking was posi-tively related to depressive symptoms. Negative andrejecting interactions partially mediated the relationbetween excessive reassurance seeking and depres-sive symptoms.Conclusions Findings identify an important inter-personal process in depression. Efforts to educatestaff and adults with mild ID about excessive reas-surance seeking and ways to alter it may be usefulin treating depression.
Keywords depression, intellectual disability,interpersonal, reassurance seeking, social skills
Introduction
Adults with intellectual disability (ID) experiencea higher rate of depression than their peers withaverage intelligence. Indeed, the point prevalence ofdepression in adults with ID is almost 4%, and theperiod prevalence is markedly higher (Deb et al.2001; Cooper et al. 2007).Yet, there has been littleinvestigation of the interpersonal pathways that con-tribute to depression in an ID population. In thegeneral population, interpersonal processes play animportant role in depression (e.g. Lewinsohn 1974;Coyne 1976a; Segrin & Abramson 1994). Dysphoricand depressed persons behave in ways that elicit
Correspondence: dr Sigan L. Hartley, Waisman Center, Rm 533,UW-Madison, 1500 Highland Avenue, Madison, WI 53705, USA(e-mail: [email protected]).
Journal of Intellectual Disability Research doi: 10.1111/j.1365-2788.2008.01126.x
volume 52 part 11 pp 917–929 november 2008917
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

negative and rejecting social interactions (Coyne1976a; Joiner 1994; Joiner & Schmidt 1998). In par-ticular, dysphoric and depressed children and adultsengage in excessive reassurance seeking, defined asexcessively and persistently seeking assurance fromothers that one is lovable and worthy (e.g. Potthoffet al. 1995; Joiner et al. 2001; Abela et al. 2005).When this assurance is given, however, its sincerityis doubted and the pattern is repeated. Eventuallyexcessive reassurance seeking leads to negative andrejecting reactions by others, which reduces the dys-phoric or depressed person’s social support andleads to interpersonal stress. In this way, excessivereassurance seeking is both a consequence ofdepression and indirect cause of further depressivesymptoms through the mediator of negative andrejecting social interactions (e.g. Joiner & Metalsky1995; Katz & Beach 1997; Joiner et al. 1999).
The few studies that have investigated interper-sonal processes in an ID population suggest thatdepressed adults with mild ID are vulnerable tonegative social interactions. The self-reportedfrequency and stress impact of negative socialinteractions of adults with mild ID is predictiveof concurrently assessed depressive symptoms anddepressive symptoms that are evident 6 monthslater (Lunsky & Benson 2001; Hartley & MacLean2005). Moreover, adults with mild ID diagnosedwith a depressive disorder report experiencing morenegative social interactions than non-depressedadults with mild ID matched on various subjectcharacteristics (Nezu et al. 1995). There is also evi-dence that caregivers reject depressed adults withmild ID, in that they minimise interactions withthese persons. In an early study, Schloss (1982)used an observational measure to record the socialinteractions of nine adults with moderate ID diag-nosed with a depressive disorder and nine adultswithout a depressive disorder with an equivalentchronological and mental age. As compared withthe non-depressed group, caregivers were less likelyto approach the depressed adults with moderateID when there was no specific purpose for theinteraction.
Studies have also shown a relation between inter-personal skill difficulties and depression in adultswith ID (Benson et al. 1985; Reiss & Benson 1985;Laman & Reiss 1987; Helsel & Matson 1988), sug-gesting that interpersonal processes may contribute
to this heightened experience of negative and reject-ing social interactions. However, these studiesfocused broadly on social skills without identifyingthe specific skill problems associated with depres-sion. Previous studies also neglected to examine thepathways through which interpersonal skill difficul-ties are related to depressive symptoms. Given theimportance of excessive reassurance seeking in typi-cally developing adults, who are similar to adultswith mild ID in everyday activities (e.g. hold jobs,do household chores and often have romantic rela-tionships) and children, who are developmentallysimilar to adults with mild ID (Joiner 1994; Joiner& Metalsky 1995; Joiner et al. 2001; Abela et al.2005), this may also be a key interpersonal behav-iour in depression in adults with mild ID. As in thetypically developing population, excessive reassur-ance seeking may be indirectly related to depressivesymptoms through evoking negative and rejectingsocial interactions.
Interestingly, excessive reassurance seeking iscurrently listed as one of several possible criterianeeded for a diagnosis of depressive episode in theDiagnostic Criteria for Psychiatric Disorders for usewith adults with Learning Disabilities/Mental Retar-dation (DC-LD; Royal College of Psychiatrists2001). It is also mentioned as a common behaviourevident in a Major Depressive Episode in adultswith mild ID in the Diagnostic Manual-IntellectualDisability (National Association for the DuallyDiagnosed 2007). However, there has not been asystematic investigation of whether depressed adultswith mild ID engage in more excessive reassuranceseeking than non-depressed adults with ID.
The aims of this study are to: (1) determinewhether depression is related to excessive reassur-ance seeking; and (2) investigate the pathwaybetween excessive reassurance seeking, negative andrejecting interactions and depressive symptoms inadults with mild ID. We predicted that: (1) therewould be a positive association between excessivereassurance seeking and depressive symptoms; (2)adults with mild ID with a diagnosis of depressionwould engage in more excessive reassurance seekingthan those without a psychiatric disorder or thosewith a non-depressive psychiatric disorder; (3)excessive reassurance seeking would be positivelyrelated to negative and rejecting interactions; and(4) negative and rejecting interactions would
918Journal of Intellectual Disability Research volume 52 part 11 november 2008
S. L. Hartley et al. • Depression in intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

mediate the relationship between excessive reassur-ance seeking and depressive symptoms.
Method
Participants
Eighty-seven adults with mild ID (IQ 55–70 andconcomitant impairments in adaptive behaviour)and adequate oral communication skills (i.e. orallycommunicate without the aid of another person)aged 20–64 years were recruited from disabilityservice providers in the Rocky Mountain region ofthe USA to participate in the study. Participantswith a diagnosis of autism were excluded given thatimpaired social functioning is a core aspect of thisdisorder. In order to be consistent with previousstudies of depression in adults with mild ID (e.g.Lunsky & Havercamp 1999; Lunsky 2003; Hartley& MacLean 2005; Esbensen & Benson 2007), par-ticipants had various aetiologies for ID, with thelargest portion being of unknown aetiology.
Staff from participants’ disability service providerwho worked with each participant at least twice aweek were also recruited to complete measures.Staff, largely case managers, reported working withthe participants for an average of 3.7 years (range0.50–8.00 years). Forty-five of the staff were female,42 were male, and their average age was 25.6 years(SD = 5.32 years). One adult with mild ID wasunable to pass the pre-test procedure outlinedbelow and thus only staff-completed measures wereused for this participant. An additional four partici-pants did not appear to comprehend measurementquestions and thus only staff-completed measureswere used for these participants as well. Table 1
presents the subject characteristics of the 87 adultswith mild ID who participated in the study. Weintentionally recruited a large sample of participantswith a depressive disorder and thus 21 participants(24.1%) had a current depressive disorder diagnosisfrom their disability service provider. Twenty-twoparticipants (25.3%) had a non-depressive psychiat-ric disorder diagnosis by their disability service pro-vider. Of the 43 participants with a depressive ornon-depressive psychiatric disorder, 22 (51.2%) hadmore than one psychiatric disorder diagnosis. Theremaining 44 participants did not have a diagnosedpsychiatric disorder (see Table 1). The overall preva-
lence of psychiatric disorders in our sample is con-sistent with epidemiology research on co-occurringmental health disorders in the ID population(Borthwick-Duffy 1994; White et al. 2005).
Measures
Participant characteristics
IQ was assessed with the Kaufman Brief Intelli-gence Test-second Edition (K-BIT-2; Kaufman &Kaufman 2004), an individually administeredmeasure of verbal and non-verbal cognitive abilities.The K-BIT-2 IQ Composite score has satisfactoryinternal consistency (0.86–0.96), test–retest reliabil-ity (0.88–0.92) and concurrent validity (Kaufman &
Table 1 Subject characteristics of participants
Gender (n)Female 45Male 42
Age in years, M (SD) 40.1 (14.1)Ethnicity (n)
Caucasian 76Hispanic 3African-American 4Native American 2Asian 2
Living status (n)Alone or with 1 roommate 17Group home 64Family/host family 6
Composite IQ, M (SD) 62.9 (8.8)Adaptive GAC, M (SD) 63.0 (12.1)Psychiatric disorder (n)*
None 44Depressive disorder 21Other 22
Bipolar disorder 4Anxiety disorder 8Psychotic disorder 4Conduct disorder 4Personality disorder 5ADHD 4Adjustment 1Kleptomania 1Alcohol dependence/abuse 2Paedophilia 1
* Of the participants diagnosed with a psychiatric disorder, 51.2%had more than one diagnosed psychiatric disorder.GAC, General Adaptive Composite; ADHD, attention deficithyperactivity disorder.
919Journal of Intellectual Disability Research volume 52 part 11 november 2008
S. L. Hartley et al. • Depression in intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

Kaufman 2004). Staff reported on the age, gender,living status and ethnicity of the participants. Staffalso completed the Adaptive Behavior AssessmentSystem-second edition (ABAS-II; Harrison &Oakland 2006). The ABAS-II General AdaptiveComposite (GAC) score has adequate internal con-sistency (0.97–0.99), test–retest reliability (0.86–0.99) and concurrent validity (Harrison & Oakland2006).
Depressive symptoms
The Glasgow Depression Scale for people with aLearning Disorder (GDS; Cuthill et al. 2003), self-reported and caregiver supplement versions wereused. The 20-item self-report GDS and 16-itemGDS caregiver supplement are based on criteriafor depression in the DC-LD and use a 3-pointresponse set (‘Never/no’, ‘Sometimes’ and ‘Always/alot’). The self-reported version has adequate inter-nal consistency (0.97), test–retest reliability (0.97)and criterion validity (Cuthill et al. 2003). The car-egiver supplement also has satisfactory inter-raterreliability (0.93), internal consistency (0.88) andtest–retest reliability (0.98) (Cuthill et al. 2003). Inthis study, satisfactory internal consistency wasfound for both the self-reported GDS (0.84) andcaregiver supplement GDS (0.85).
Reassurance seeking
The Reassurance-Seeking Scale (RSS; Joiner &Metalsky 1995, 2001) was reworded for use withadults with mild ID (i.e. parents and friends waschanged to family, staff or friends) and consistedof four items: ‘I always need to ask my family, staffand friends if they like me’; ‘I always need to askmy family, staff or friends if they really care aboutme’; ‘Sometimes when I ask people if they like me,they tell me to stop asking’; and ‘Sometimes when Iask people if they like me, they get mad’. Responseoptions included ‘No/not at all’, ‘Sometimes’ andExtremely’. Among typically developing children(aged 6–14 years), the RSS has satisfactory internalconsistency (0.78), 1-year test–retest reliability(0.61) and concurrent and criterion validity (Joiner1999; Joiner et al. 2001; Abela et al. 2005; Abelaet al. 2006). In this study, the RSS had adequateinternal consistency (0.76) among adults withmild ID.
A staff-reported version of the RSS had a 7-pointresponse set (‘Not at all’ to ‘Extremely’) for fouritems: ‘Does the adult with mild ID often askothers how they truly feel about them?’; ‘Does theadult with mild ID frequently seek reassurancefrom others as to whether they really care aboutthem?’; ‘Do others sometimes become irritated withthe adult with mild ID for seeking reassuranceabout whether they really care about them?’; and‘Do others sometimes get “fed up” with the adultwith mild ID for seeking reassurance about whetherthey really care about them?’. By using theseresponse options, the RSS has adequate internalconsistency (0.85–0.95) and discriminant and con-current validity in the general population (Joineret al. 1992; Joiner 1994; Potthoff et al. 1995; Joiner& Metalsky 2001). In this study, satisfactory inter-nal consistency (0.84) was found for the staff-reported RSS, and there was a significant positivecorrelation between the staff-reported RSS and self-reported RSS (r = 0.33, P < 0.01).
Inventory of negative social interactions
The Inventory of Negative Social Interactions(INSI; Lakey et al. 1994) is a 40-item self-reportmeasure of a variety of negative social situations.Sample items include ‘Said bad things about you’and ‘Took something of yours without asking’.Among adults with mild ID, the INSI was found tohave adequate reliability and criterion validity andwas predictive of somatic complaints and depressivesymptoms reported 6 months later (Lunsky &Benson 2001; Lunsky & Bramston 2006). In thisstudy, the self-reported INSI had satisfactory inter-nal consistency (0.93).
Interpersonal rejection
In line with past measures of interpersonal rejection(e.g. Coyne 1976b; Gotlib & Robinson 1982; Joineret al. 1992; Joiner & Metalsky 1995), this constructwas operationalised as staff’s preference or desir-ability to interact with the adult with mild ID. Spe-cifically, staff rated their desirability to interact withthe adult with mild ID through nine questions (‘Ilook forward to working with this person more thanother clients’; ‘I would like to sit next to this personon a 3-hour bus trip’; ‘I would like to spend timewith this person outside of my job’; ‘I expect to
920Journal of Intellectual Disability Research volume 52 part 11 november 2008
S. L. Hartley et al. • Depression in intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

have a good time during my interactions with thisperson’; ‘I am excited to continue to work with thisperson in the future’; ‘I wish I could spend moretime working with this person than with otherclients’; ‘I would like to have this person as a neigh-bor’; ‘I would like to work with this person on atask or project’; ‘I would like to have this person asa close friend’.) using a 7-point scale (‘Not true’ to‘Very true’). These questions were adapted frommeasures used in the general population (Coyne1976b; Gotlib & Robinson 1982). Items on theinterpersonal rejection measure were thenreversely scored so that higher scores reflectedgreater interpersonal rejection. In this study,adequate internal consistency was achieved (0.91),and the interpersonal rejection measure wassignificantly positively correlated with the INSI(r = 0.23, P = 0.04).
Procedure
Staff were given a packet of materials including theABAS-II, GDS caregiver supplement, RSS staffrating and interpersonal rejection measure. Oncecompleted, the packets were returned to theresearchers via mail, and staff were paid $20. Adultswith mild ID were interviewed at their home or theheadquarters of their developmental disabilityservice provider. A pre-test was used to determinewhether adults with mild ID could reliably use a3-point Likert-type scale. In the pre-test, adultswith mild ID were required to assign size–orderrelations among a set of clear containers withvarying amounts of coloured water, match the con-tainers to written descriptors (‘No’ ‘Medium’ and‘A lot’) and a numerical scale of size (0–2), andcorrectly indicate where their favourite and leastfavourite food items fell using the containers,numbers or written descriptors. This pre-test hasbeen used in a previous study (Hartley & MacLean2005) and shown to result in minimal response biasduring actual testing. Participants who passed thepre-test were administered the K-BIT-2. Partici-pants were read the GDS self-report, INSI self-report and RSS self-report. In all, the proceduretook 40–60 min. Adults with mild ID werepaid $20 for their participation in thestudy.
Results
Data analysis plan
A one-way analysis of variance (ANOVA) was usedto identify differences in the GDS among partici-pants diagnosed with a depressive disorder, partici-pants diagnosed with a non-depressive psychiatricdisorder and participants without a psychiatric dis-order. The association between excessive reassur-ance seeking, negative and rejecting interactionsand depressive symptoms was examined. One-wayANOVAs were used to identify differences in exces-sive reassurance seeking and negative and rejectinginteractions among participants diagnosed with adepressive disorder, participants diagnosed with anon-depressive psychiatric disorder and participantswithout a psychiatric disorder diagnosis. Correla-tions, independent sample t-tests and one-wayANOVAs were used to identify subject characteris-tics related to depressive symptoms, excessive reas-surance seeking and negative and rejectinginteractions.
Linear regressions were used to investigate thepotential indirect effect of negative social interac-tions and interpersonal rejection (mediators) on therelation between excessive reassurance seeking(independent variable) and depressive symptoms(dependent variable) by using the causal steps out-lined by Baron and Kenny (Judd & Kenny 1981;Baron & Kenny 1986). Regressions were run sepa-rately for the self-report and staff-rating measures.To establish a mediating effect, the following crite-ria must be met: (1) a significant associationbetween the independent variable and dependentvariable; (2) a significant association between theindependent variable and mediator; and (3) therelation between the independent variable anddependent variable decreases significantly with thepotential mediator in the model, while the associa-tion between the mediator and dependent variableremains. The Baron–Kenny method has severallimitations (e.g. low power, greater likelihood ofType I errors and an inability to address suppres-sion effects) and cannot determine whether indirecteffects are significantly different from zero. There-fore, we also employed the Sobel (1982) test, whichovercomes many of these limitations and can deter-mine whether the indirect effect of reassuranceseeking on depression via negative and rejecting
921Journal of Intellectual Disability Research volume 52 part 11 november 2008
S. L. Hartley et al. • Depression in intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

interactions was significantly different from zero.Bootstrapping was not used. The Sobel test wascalculated by running regression analyses in spss.Table 2 presents the internal consistencyvalues, means, standard deviations, inter-correlations and potential and actual rangesfor the measures.
Depressive symptoms
Table 3 presents the means and standard deviationsfor the participants diagnosed with a depressive dis-order (N = 21), with a non-depressive psychiatricdisorder (N = 22) and without a psychiatric disor-der (N = 41) on the GDS, RSS and negative and
Table 2 Intercorrelation, descriptive andinternal consistency values for studymeasures
1 2 3 4 5 6
GDS1. Caregiver supplement (0.85)2. Self-report 0.45** (0.84)
RSS3. Staff rating 0.46** 0.21* (0.84)4. Self-report 0.20 0.40** 0.33** (0.76)
Negative and rejectinginteractions5. INSI self-report 0.30** 0.55** 0.20 0.42** (0.93)6. Interpersonal rejection
staff report0.50** 0.25* 0.34** 0.20 0.23* (0.91)
Mean 9.45 15.01 7.08 3.29 31.01 29.52Standard deviation 6.14 6.56 5.81 2.36 21.32 11.91Potential range 0–32 0–40 0–24 0–8 0–80 0–54Actual range 0–28 1–29 0–22 0–8 0–74 4–54
GDS, Glasgow Depression Scale for people with a Learning Disorder; RSS, Reassurance-Seeking Scale; INSI, Inventory of Negative Social Interactions.* P � 0.05, ** P �0.01.
Table 3 Means and standard deviation in parentheses on measures for participants with a depressive disorder (N = 21), a non-depressivepsychiatric disorder (N = 22) and no psychiatric disorders (N = 44)
DepressionNon-depressivepsychiatric disorder
No psychiatricdisorders
GDSCaregiver supplement 12.50 (6.77)*† 9.70 (5.30) 6.54 (5.50)Self-report 19.92 (6.04)*† 15.73 (5.95) 12.14 (5.46)
RSSStaff rating 9.50 (6.11)*† 6.44 (5.30) 5.62 (5.58)Self-report 4.63 (1.79)† 3.96 (2.10) 2.71 (2.36)
Negative and rejecting interactionsINSI self-report 42.21 (18.48)† 37.00 (21.05) 20.28 (18.27)Interpersonal rejection staff rating 31.16 (13.28) 30.50 (10.29) 27.34 (12.12)
GDS, Glasgow Depression Scale for people with a Learning Disorder; RSS, Reassurance-Seeking Scale; INSI, Inventory of NegativeSocial Interactions.* Significantly higher at P < 0.05 than Non-Depressive Psychiatric Disorder group.† Significantly higher at P < 0.05 than No Psychiatric Disorder group.
922Journal of Intellectual Disability Research volume 52 part 11 november 2008
S. L. Hartley et al. • Depression in intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

rejecting interaction measures. A one-way ANOVAand follow-up Student–Newman–Keuls post hocanalyses indicated that the participants diagnosedwith a depressive disorder were significantly higheron the GDS caregiver supplement than the partici-pants with a non-depressive psychiatric disorderand the participants without a psychiatric disorder(F2,78 = 8.05, P < 0.01). Similarly, the participantsdiagnosed with a depressive disorder were signifi-cantly higher on the GDS self-report than the par-ticipants with a non-depressive psychiatric disorderand the participants without a psychiatric disorder(F2,78 = 14.43, P < 0.01).
Excessive reassurance seeking and depression
As shown in Table 2, there was a significant correla-tion between the RSS self-report, the RSS staffrating, the GDS self-report and the GDS caregiversupplement. Consistent with our prediction, therewas a significant correlation between the RSS self-report and GDS self-report and between the RSSstaff rating and GDS caregiver supplement. A one-way ANOVA and follow-up Student–Newman–Keuls post hoc analyses indicated that theparticipants diagnosed with a depressive disorder(M = 9.50, SD = 6.11) were significantly higher onthe RSS staff rating than the participants with anon-depressive psychiatric disorder and the partici-pants without a psychiatric disorder (F2,78 = 3.56,P = 0.03). There was also significant a difference forthe RSS self-report (F2,78 = 5.97, P < 0.01). The par-ticipants with a depressive disorder were signifi-cantly higher on the RSS self-report than theparticipants without a psychiatric disorder, but werenot significantly different from the participants witha non-depressive psychiatric disorder.
Negative and rejecting interactions and depression
As shown in Table 2, was a significant positive cor-relation between the INSI self-report, the GDS self-report and the GDS caregiver supplement. Therewas also a significant positive correlation betweenthe interpersonal rejection staff rating, the GDSself-report and the GDS caregiver supplement. Par-ticipants without a psychiatric disorder were signifi-cantly lower on the INSI self-report than theparticipants with a depressive disorder and the par-
ticipants with a non-depressive psychiatric disorder(F2,78 = 11.45, P < 0.01). There was not significantdifference on the INSI between the participantswith a depressive disorder and those with a non-depressive psychiatric disorder. There was not a sig-nificant a difference on the interpersonal rejectionstaff rating among the participants without a psy-chiatric disorder, those with a depressive disorderand those with a non-depressive psychiatric disorder(F2,78 = 0.68, P = 0.41).
Subject characteristics and GDS, RSS, and negativeand rejecting interactions
Correlations were conducted between the GDScaregiver supplement and age (years), IQ, (K-BIT-2Composite standard score) and adaptive behaviour(ABAS-II GAC standard score). There was not asignificant correlation between the GDS caregiversupplement and age (r = 0.12, P = 0.23), IQ(r = -0.07, P = 0.50) or adaptive behaviour(r = -0.13, P = 0.24). Independent samples t-testsindicated that the GDS caregiver supplement didnot significantly differ by gender [t(86) = 0.96,P = 0.34] or Caucasian versus non-Caucasian eth-nicity [t(86) = -0.21, P = 0.83]. A one-way ANOVAindicated that the GDS caregiver supplement didnot significantly differ by living status (group home,alone or with one other, and family) (F2,79 = 0.56,P = 0.58). Similarly, there was not a significant cor-relation between the GDS self-report and age(r = -0.08, P = 0.47), IQ (r = -0.08, P = 0.47), oradaptive behaviour (r = -0.09, P = 0.42). The GDSself-report did not significantly differ by gender[t(86) = 1.41, P = 0.16] or Caucasian versus non-Caucasian ethnicity [t(86) = -0.25, P = 0.88]. TheGDS self-report did not significantly differ by livingstatus (F2,79 = 1.08, P = 0.32).
There was not a significant correlation betweenthe RSS staff rating and age (r = -0.06, P = 0.58),IQ (r = 0.15, P = 0.16) or adaptive behaviour(r = 0.01, P = 0.99). The RSS staff rating did notsignificantly differ by gender [t(86) = 1.45, P = 0.16]or Caucasian versus non-Caucasian ethnicity[t(86) = 0.95, P = 0.35]. The RSS staff rating alsodid not significantly differ by living status(F2,79 = 0.05, P = 0.95). Similarly, there was not asignificant correlation between the RSS self-reportand age (r = -0.06, P = 0.59), IQ (r = -0.15,
923Journal of Intellectual Disability Research volume 52 part 11 november 2008
S. L. Hartley et al. • Depression in intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

P = 0.17) or adaptive behaviour (r = -0.08,P = 0.50). The RSS self-report did not significantlydiffer by gender [t(86) = 0.86, p = 0.39] or Cauca-sian versus non-Caucasian ethnicity [t(86) = 0.15,P = 0.88]. The RSS self-report also did notsignificantly differ by living status (F2,79 = 0.02,P = 0.98).
There was not a significant correlation betweenthe INSI self-report and age (r = -0.20, P = 0.08),IQ (r = -0.09, P = 0.42) or adaptive behaviour(r = -0.06, P = 0.59). The INSI self-report did notsignificantly differ by gender [t(86) = 1.13, P = 0.26]or Caucasian versus non-Caucasian ethnicity[t(86) = 0.55, P = 0.58]. The INSI self-reportalso did not significantly differ by living status(F2,79 = 1.24, P = 0.30). Similarly, there was not asignificant correlation between the interpersonalrejection staff rating and age (r = -0.08, P = 0.59),IQ (r = -0.12, P = 0.27) or adaptive behaviour(r = -0.05, P = 0.67). The interpersonal rejectionstaff report did not significantly differ by gender[t(86) = 0.90, P = 0.37] or Caucasian versus non-Caucasian ethnicity [t(86) = 1.19, P = 0.24]. Theinterpersonal rejection staff rating also did notsignificantly differ by living status (F2,79 = 0.83,P = 0.44).
Mediation analyses
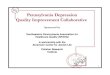
As shown in Table 2, there was a significant positiveassociation between the RSS staff rating and theinterpersonal rejection staff rating. There was alsoa significant positive association between the RSSself-report and the INSI self-report. Table 4 pre-sents the results of the regression analyses for theassociations among the RSS, INSI, interpersonalrejection and GDS. The RSS self-report was signifi-cantly associated with the GDS self-report, therewas a significant association between the RSS self-report and the INSI self-report, and the INSI self-report was significantly associated with the GDSself-report. In addition, the relation between theRSS self-report and the GDS self-report decreasedwhen the INSI self-report was entered into themodel, while the association between the INSI self-report and the GDS self-report remained (Fig. 1).The Sobel test for mediation yielded a significantresult, indicating that the association between self-reported reassurance seeking and depressive symp-toms was significantly reduced by the inclusion ofnegative social interactions (Sobel = 3.32, P < 0.01).Negative social interactions are considered to be apartial mediator of depressive symptoms given that
Table 4 Mediation analyses
Regression model Mean square d.f. B SE b b Sobel test
Self-report measuresGDSModel 1 619.30 1
RSS 1.14 0.28 0.40**Model 2 680.50 2 3.32**
RSS 0.57 0.28 0.20*INSI 0.16 0.03 0.48**
Staff-report measuresGDSModel 1 708.33 1
RSS 0.49 0.10 0.46**Model 2 529.12 2 2.54**
RSS 0.33 0.10 0.31**Interpersonal rejection 0.20 0.05 0.39**
GDS, Glasgow Depression Scale for people with a Learning Disorder; INSI, Inventory of Negative Social Interactions; RSS, Reassurance-Seeking Scale; SE, standard error.* P � 0.05, ** P � 0.01.
924Journal of Intellectual Disability Research volume 52 part 11 november 2008
S. L. Hartley et al. • Depression in intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

the RSS self-report was still significantly associatedwith the GDS self-report when controlling forINSI.
The RSS staff rating was also significantly associ-ated with interpersonal rejection staff rating, andinterpersonal rejection staff rating was significantlyassociated with the GDS caregiver supplement.Finally, the relation between the RSS staff ratingand the GDS caregiver supplement decreased wheninterpersonal rejection staff rating was entered intothe model, while the association between the RSSstaff rating and the GDS caregiver supplementremained (Fig. 2). The Sobel test for mediationyielded a significant result, indicating that the asso-ciation between reassurance seeking and depressionwas significantly reduced by the inclusion of inter-personal rejection (Sobel = 2.54, P = 0.01). Inter-personal rejection is considered to be a partialmediator of depressive symptoms given that the
RSS staff rating was still significantly associatedwith the GDS caregiver supplement when control-ling for interpersonal rejection.
Discussion
Depression is one of the most prevalent psychiatricdisorders among adults with ID (Deb et al. 2001;Cooper et al. 2007), yet there is little researchregarding interpersonal processes contributing todepression. We investigated the relation betweenexcessive reassurance seeking, depressive symptomsand the negative and rejecting interactions of adultswith mild ID. Excessive reassurance seeking,assessed through both self- and staff-rated mea-sures, was positively associated with depressivesymptoms. Moreover, adults with mild ID diag-nosed with a depressive disorder engaged in moreexcessive reassurance seeking than adults with mildID without a psychiatric disorder. When rated bystaff, excessive reassurance seeking also distin-guished adults with mild ID who had a depressivedisorder from those with other types of psychiatricdisorders. Thus, as in typically developing adultsand children (Joiner & Metalsky 1995; Joiner &Schmidt 1998; Joiner et al. 2001; Abela et al. 2005),excessive reassurance seeking appears to be part ofthe depressive presentation in adults with mild ID.These findings add support for the current inclu-sion of excessive reassurance seeking in the diagnos-tic criteria for depressive disorders in the DC-LDand Diagnostic Manual-Intellectual Disability.However, additional research using alternative mea-sures of depression and samples of adults with mildID is needed before strong conclusions regardingthe appropriateness of this criterion for depressivedisorders can be reached.
In support of previous studies (Schloss 1982;Nezu et al. 1995; Lunsky & Benson 2001; Hartley &MacLean 2005), experiencing negative and rejectinginteractions was positively related to depressivesymptoms, and adults with mild ID who had adepressive disorder experienced more negativesocial interactions than adults without a psychiatricdisorder. Mediation analyses indicated that therelation between excessive reassurance seeking anddepressive symptoms was partially mediated bynegative and rejecting social interactions in adults
β = .20*
β = .40**
β = .55**b = .42**
GDS self-report
RSS self-report
INSI
Figure 1 Mediation model of the Reassurance-Seeking Scale(RSS), Inventory of Negative Social Interactions (INSI) and theGlasgow Depression Scale for People with a Learning Disorder(GDS) by using self-report measures. The two bs at the bottomrepresent the b before (above line) and after (below line) theintroduction of the mediator into the regression model. *P � 0.05,**P � 0.01.
β = .50**b = .34**
β = .31**
GDScaregiver
supplement
RSSstaff rating
β = .46**
Interpersonal rejection
Figure 2 Mediation model of the Reassurance-Seeking Scale(RSS), interpersonal rejection and the Glasgow Depression Scalefor People with a Learning Disorder (GDS) by using staff-reportedmeasures. The two bs at the bottom of each figure represent the bbefore (above line) and after (below line) the introduction of themediator into the regression model. **P � 0.01.
925Journal of Intellectual Disability Research volume 52 part 11 november 2008
S. L. Hartley et al. • Depression in intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

with mild ID. This is consistent with findings inthe general population (Joiner & Metalsky 1995;Potthoff et al. 1995; Katz & Beach 1997; Joineret al.1999) and suggests that excessive reassuranceseeking is a critical behaviour in creating negativeand rejecting interactions, which reduce the positivesocial support and increase the interpersonal stressof dysphoric and depressed adults with mild ID. Inthis way, excessive reassurance seeking may be animportant interpersonal process through whichdepression is maintained over time in adults withmild ID.
It is interesting to note that the associationbetween depressive symptoms and excessive reassur-ance seeking was relatively high when both wererated by self-report or both by staff rating. In con-trast, self-report and staff ratings of depressive symp-toms and excessive reassurance seeking had small,albeit often significant, associations. Previousresearch of both typically developing children andadults with mild ID has also found small associa-tions between self-report and informant ratings ofemotional and behavioural problems (e.g. Lunsky &Bramston 2006; Vierhaus & Lohaus 2008; Zimmer-man & Enderman 2008).The lack of a strong asso-ciation between self-report and informant ratings isoften attributed to differences in the experience ofthese problems.The subjective experience of depres-sion or excessive reassurance seeking as rated byadults with mild ID likely differs from the experienceof staff who observe these problems. However, bothexperiences add meaningful information for under-standing the interpersonal behaviours of depressedadults with mild ID. A strength of this study is thatrelation between excessive reassurance seeking anddepressive symptoms was partially mediated bynegative and rejecting social interactions by usingboth self-report and staff-rating measures.
Findings from this study have important implica-tions for designing intervention strategies to treatdepression in an ID population. Adults with mildID receiving disability services have frequent andoften intimate interactions with staff at their dayprogrammes, jobs or group homes. They are there-fore likely to seek reassurance from staff, and staffare likely to react in negative and rejecting ways.This provides a unique opportunity to train staff atdisability service providers about this interpersonalprocess. Interventions aimed at educating staff
about excessive reassurance seeking and teachingstrategies for not getting frustrated or aggravated bythis behaviour (e.g. taking a break, reminding your-self that this behaviour is common among peoplewho are depressed or using reassurance seeking as acue to give the client more positive support) may behelpful in treating depression in adults with mildID. Similarly, it may be feasible to develop interven-tions aimed at altering the interpersonal behavioursof dysphoric or depressed adults with mild ID.Such interventions could educate adults with mildID about the ill effect of excessive reassuranceseeking and teach them alternative strategies formanaging their self-doubt.
There are several limitations to this study. Across-sectional approach was used to investigate theassociation between excessive reassurance seeking,negative and rejecting interactions and depressivesymptoms at one time point. This methodologycannot provide direct evidence on causal processesor determine the direction of the relation betweenexcessive reassurance seeking, negative and rejectinginteractions and depressive symptoms. A longitudi-nal study of the time–order relation between thesevariables is needed to determine whether reassur-ance seeking precedes negative and rejecting inter-actions, and the experience of negative and rejectinginteractions then causes an increase in depressivesymptoms, as is described in the typically develop-ing literature. Alternatively, it may be that negativeand rejecting interactions occur first and cause anincrease in both excessive reassurance seeking anddepressive symptoms. Further research is needed torule out this possibility.
Another limitation to this study is that wefocused on one potential mediator of the associa-tion between negative and rejecting interactions anddepression. Other maladaptive interpersonal behav-iours (e.g. poor eye contact, talking about negativecontent, self-focused talk or lack of intonation inspeech) seen in the typically developing population(e.g. for review see Segrin 2000) may also bepresent in adults with mild ID and indirectly con-tribute to depressive symptoms via evoking negativeor rejecting responses by others. Future research isneeded to determine whether depressed adults withmild ID also demonstrate these interpersonalbehaviours and, if so, their relation to perpetuatingdepression.
926Journal of Intellectual Disability Research volume 52 part 11 november 2008
S. L. Hartley et al. • Depression in intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

For many adults with mild ID family or friendsmay be more important and familiar than staff andthus a study of excessive reassurance seeking byusing alternative categories of important others isalso needed. In line with research in the typicallydeveloping population (Coyne 1976b; Joiner et al.1992), interpersonal rejection was assessed throughstaff ratings of desirability or preference to interactwith the adult with mild ID. Further studies areneeded to determine whether staff behaviour is con-sistent with their stated preferences (i.e. interact lesswith depressed than non-depressed adults with mildID). To date, only one study has used an observa-tional measure of staff’s interaction with depressedand non-depressed adults with mild ID (Schloss1982); however, this study did not include staffratings of their desirability to interact withdepressed and non-depressed adults with ID. Giventhat staff are employed to care for the adult withmild ID, their desirability ratings may not matchtheir actual interaction patterns to the same extentas in the general population.
Overall, this study broadens our understanding ofthe role of interpersonal behaviours, and specificallyexcessive reassurance seeking, in depression inadults with mild ID. This study also illuminated thepotential pathway between excessive reassuranceseeking and depressive symptoms to provide a basisfor understanding how this social behaviour maymaintain or exacerbate depression over time. Find-ings have relevance for directing future researchstudies of interpersonal pathways contributing todepression and designing interventions to treatdepression in an ID population. Efforts to educatestaff and adults with mild ID about the interper-sonal pattern of excessive reassurance seeking andways to alter it may be helpful in treatingdepression.
References
Abela J. R. Z., Hankin B. L., Haigh E. A., Adams P.,Vinokuroff T. & Trayhern L. (2005) Interpersonal vul-nerability to depression in high-risk children: the role ofinsecure attachment and reassurance seeking. Journal ofClinical Child and Adolescent Psychology 34, 182–92.
Abela J. R., Zuroff D. C., Ho M-H, Adams P. & HankinB. L. (2006) Excessive reassurance-seeking, hassles,and depressive symptoms in children of affectively ill
parents: A multiwave longitudinal study. Journal ofAbnormal Child Psychology 34, 171–87.
Baron R. M. & Kenny D. A. (1986) The moderator-mediator variable distinction in social psychologicalresearch: conceptual, strategic, and statistical consider-ations. Journal of Personality and Social Psychology 51,1173–82.
Benson B. A., Reiss S., Smith D. C. & Laman D. S.(1985) Psychosocial correlates of depression in mentallyretarded adults: II. Poor social skills. American Journal ofMental Deficiency 89, 657–9.
Borthwick-Duffy S. A. (1994) Epidemiology and preva-lence of psychopathology in people with mental retarda-tion. Journal of Consulting and Clinical Psychology 62,17–27.
Cooper S.-A., Smiley E., Morrison J., Williamson A. &Allan L. (2007) An epidemiological investigation ofaffective disorders with a population-based cohort of1023 adults with intellectual disabilities. PsychologicalMedicine 37, 873–82.
Coyne J. C. (1976a) Toward an interactional descriptionof depression. Psychiatry 39, 28–40.
Coyne J. C. (1976b) Depression and the responses ofothers. Journal of Abnormal Psychology 85, 186–93.
Cuthill F. M., Espie C. A. & Cooper S.-A. (2003) Devel-opment and psychometric properties of the GlasgowDepression Scale for people with a learning disability.British Journal of Psychiatry 182, 347–53.
Deb S., Thomas M. & Bright C. (2001) Mental disorderin adults with intellectual disability I: prevalence offunctional psychiatric illness among a community-based population aged between 16 and 64 years.Journal of Intellectual Disability Research 45, 495–505.
Esbensen A. J. & Benson B. A. (2007) An evaluation ofBeck’s cognitive therapy of depression in adults withintellectual disability. Journal of Intellectual DisabilityResearch 51, 14–24.
Gotlib I. H. & Robinson L. A. (1982) Responses todepressed individuals: discrepancies between self-reportand observer-rated behavior. Journal of Abnormal Psy-chology 91, 231–40.
Harrison P. & Oakland R. (2006) Adaptive Behavior Assess-ment System-Second Edition (ABAS-II.). HarcourtAssessment, Inc., San Antonio, TX.
Hartley S. L. & MacLean W. E., Jr (2005) Perceptions ofstress and coping strategies among adults with mildmental retardation: insight into psychological adjust-ment. American Journal on Mental Retardation 110, 285–97.
Helsel W. J. & Matson J. L. (1988) The relationship ofdepression to social skills and intellectual functioning inmentally retarded adults. Journal of Mental DeficiencyResearch 32, 411–8.
927Journal of Intellectual Disability Research volume 52 part 11 november 2008
S. L. Hartley et al. • Depression in intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

Joiner T. E., Jr (1994) Contagious depression: existence,specificity to depressed symptoms, and the role of reas-surance seeking. Journal of Personality and Social Psychol-ogy 67, 287–96.
Joiner T. E., Jr (1999) A test of interpersonal theory ofdepression in youth psychiatric inpatients. Journal ofAbnormal Child Psychology 27, 77–85.
Joiner T. E., Jr & Metalsky G. I. (1995) A prospective testof an integrative interpersonal theory of depression:a naturalistic study of college roommates. Journal ofPersonality and Social Psychology 69, 778–88.
Joiner T. E., Jr & Metalsky G. I. (2001) Excessivereassurance-seeking: delineating a risk factor involved inthe development of depressive symptoms. PsychologicalScience 12, 371–9.
Joiner T. E., Jr & Schmidt N. B. (1998) Excessivereassurance-seeking predicts depressive but not anxiousreactions to acute stress. Journal of Abnormal Psychology107, 533–7.
Joiner T. E.Jr, , Alfano, M. S. & Metalsky G. I. (1992)When depression breeds contempt: reassurance-seeking,self-esteem and rejection of depressed college studentsby their roommates. Journal of Abnormal Psychology 101,165–73.
Joiner T. E., Jr, Metalsky G. I., Katz J. & Beach S. R. H.(1999) Depression and excessive reassurance-seeking.Psychology Inquiry 10, 269–79.
Joiner T. E., Jr, Gencoz G. I., Metalsky F. & Gencoz T.(2001) The relative specificity of excessive reassurance-seeking to depressive symptoms and diagnoses amongclinical samples of adults and youth. Journal of Psycho-pathology and Behavioral Assessment 23, 35–41.
Judd C. M. & Kenny D. A. (1981) Estimating the Effects ofSocial Interventions. Cambridge University Press, NewYork.
Katz J. & Beach S. R. H. (1997) Romance in the crossfire:when do women’s depressive symptoms predict partnerrelationship dissatisfaction? Journal of Social and ClinicalPsychology 16, 243–58.
Kaufman A. S. & Kaufman N. L. (2004) KBIT-2:Kaufman Brief Intelligence Test, 2nd edn. AGS Publish-ing, Minneapolis, MN.
Lakey B., Tardiff T. A. & Drew J. B. (1994) Negativesocial interactions: assessment and relations to socialsupport, cognitions, and psychological distress. Journalof Social and Clinical Psychology 13, 42–62.
Laman D. S. & Reiss S. (1987) Social skills deficienciesassociated with depressed moods of mentally retardedadults. American Journal of Mental Deficiency 92,224–9.
Lewinsohn P. M. (1974) A behavioral approach to depres-sion. In: The Psychology of Depression: ContemporaryTheory and Research (eds R. J. Friedman & M. M.Katz), pp. 157–78. Winston-Wiley, Washington,DC.
Lunsky Y. (2003) Depressive symptoms in intellectual dis-ability: does gender play a role? Journal of IntellectualDisability Research 47, 417–28.
Lunsky Y. & Benson B. A. (2001) Association betweenperceived social support and strain, and positive andnegative outcomes for adults with mild intellectual dis-ability. Journal of Intellectual Disability Research 45, 106–14.
Lunsky Y. & Bramston P. (2006) A preliminary study ofperceived stress in adults with intellectual disabilityaccording to self-report and informant ratings. Journalof Intellectual and Developmental Disability 31, 20–7.
Lunsky Y. & Havercamp S. M. (1999) Distinguishing lowlevels of social support and social strain: implications fordual diagnosis. American Journal on Mental Retardation104, 200–4.
National Association for the Dually Diagnosed (2007)Diagnostic Manual- Intellectual Disability: A Textbook ofDiagnosis of Mental Disorders in Persons with IntellectualDisability. NADD Press, Kingston, NY.
Nezu C. M., Nezu A. M., Rothenberg J. L., DelliCarpiniL. & Groag I. (1995) Depression in adults with mildmental retardation: are cognitive variables involved?Cognitive Therapy and Research 19, 227–39.
Potthoff J. G., Holahan C. J. & Joiner T. E., Jr (1995)Reassurance seeking, stress generation, and depressivesymptoms: an integrative model. Journal of Personalityand Social Psychology 68, 664–70.
Reiss S. & Benson B. A. (1985) Psychosocial correlates ofdepression in mentally retarded adults. I: Minimal socialsupport and stigmatization. American Journal of MentalDeficiency 89, 331–7.
Royal College of Psychiatrists (2001). DC-LD [DiagnosticCriteria for Psychiatric Disorders for Use with Adults withLearning Disabilities/Mental Retardation]. Gaskell Press,London.
Schloss P. (1982) Verbal interaction pattern of depressedand nondepressed institutionalized mentally retardedadults. Applied Research in Mental Retardation 3, 1–12.
Segrin C. (2000) Social skills deficits associated withdepression. Clinical Psychology Review 20, 379–403.
Segrin C. & Abramson L.Y. (1994) Negative reaction todepressive behaviors: a communication theories analysis.Journal of Abnormal Psychology 103, 655–68.
Sobel M. E. (1982) Asymptotic intervals for indirecteffects in structural equations models. In: SociologicalMethodology (ed. S. Leinhart), pp. 290–312. Jossey-Bass,San Francisco, CA.
Vierhaus M. & Lohaus A. (2008) Children and parents asinformants of emotional and behavioral problems pre-dicting female and male adolescent risk behaviors: alongitudinal cross-informant study. Journal ofYouth andAdolescence 37, 211–24.
928Journal of Intellectual Disability Research volume 52 part 11 november 2008
S. L. Hartley et al. • Depression in intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

White P., Chant D., Edwards N., Townsend C. &Waghorn G. (2005) The prevalence of intellectualdisability and comorbid mental illness in anAustralian community sample. The Australianand New Zealand Journal of Psychiatry 39, 395–400.
Zimmerman F. & Enderman M. (2008) Self-proxy agree-ment and correlates of health-related quality of life inyoung adults with epilepsy and mild intellectual disabili-ties. Epilepsy and Behavior 13, 202–11.
Accepted 11 August 2008
929Journal of Intellectual Disability Research volume 52 part 11 november 2008
S. L. Hartley et al. • Depression in intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd