Embed Size (px)
Citation preview
445
REASSICNMENT OF TASKS IN PAEDIATRI,CS.*
By CHARLES McNEIL.
T H E subject - -" Reassignment of Tasks in P~ediatrics " - - i s a wide one, and in the limits of a single address can only be discussed on broad and general lines. P~ediatrics may be described as the
organised medical and social services whose object is the direct care of infants and children, and also the assistance of parents, and especially mothers, in their task of child care. These services include the great service of communal sanitation, hospitals of various kinds, the Materni ty Service, and the comparatively new Child Welfare Service. Later in the address these different services of child care will be briefly described ; but it is clear that a great and complicated apparatus of child care has been at work for many years to promote the health and well-being of children; and fortunately, in the infant death rate we have a numerical measure o~ child health which allows us to judge the total effect of these social and medical agencies. This measurement of child health by infant death rates has its limitations and errors. We shall see presently what these limitations are; but even giving them full allowance, the infant death rates have been of great value, in revealing the different causes of infant deaths, and in comparing the differing death rates between dis. tr icts and towns in the same country, and between different countries throughout the world. The outstanding fact about the behaviour of infant death rates all over the world is that, wherever child-care services have been established and infant deaths recorded, there has been a great reduction of infant death rates in the last 50 years. As an illustra- tion, the Scottish infant death rate in 1906 stood at 115 per 1,000 live births, and in 1952 it had fallen to 35. A similar fall has taken place in many other countries during the same period; in some it has been greater, in others less. Scotland has been taken as an example and will be used for other figures of infant deaths, because she is representative of many countries in the general structure of her services of child care, and has falling figures of infant deaths and will give information which can be applied to other countries as well as to Scotland.
The limitations and defects of the infant death rate are principally two-- the omission of stillbil~ths, and its failure to give the causes of death. When stillbirths are added to the infant deaths a f te r birth, we get an accurate total of the infant loss dur ing the first year. And with this addition, the massing of infant deaths dur ing birth and the four weeks that follow becomes obvious, and suggests a division of the total infant loss into two periods, the line of division being the end of the first month af ter birth. The rightness of this division is confirmed, when pathological and clinical diagnosis shows that quite different pathological processes are at work in one or the other of the two divisions.
With the addition of stillbirths, we get a more accurate picture of the decline of infant deaths in the last for ty or fifty years. The figures are for Scotland and are shown in the following table. The stillbirths for
*(Based on an address g iven to the I r i sh Pmdia t r ie Associa t ion on J u n e 12th, 1953.)
446 I R I S H JOURNAL OF MEDICAL SCIENCE
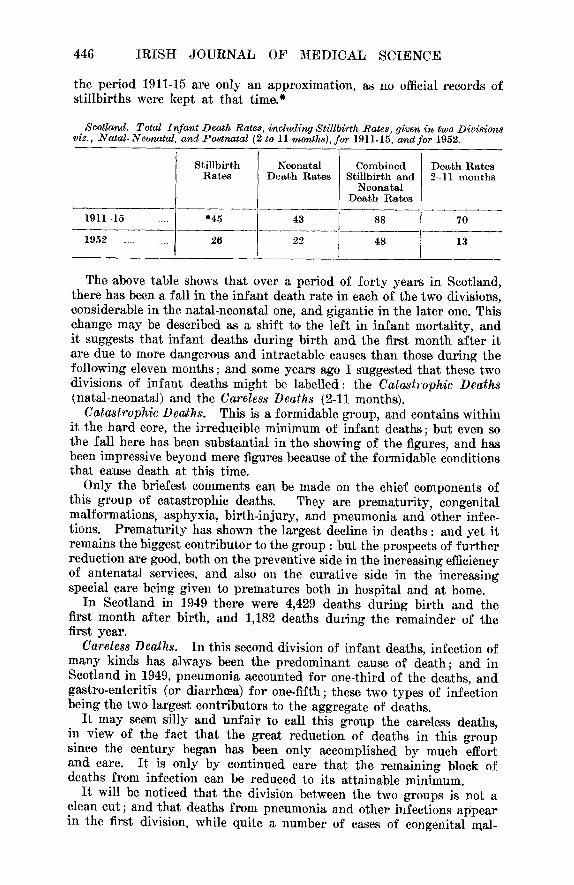
the period 1911-15 are only an approximation, as no official records of stillbirths were kept at tha£ time.*
Scotland. Total Iv, "ant Death Rates, including Stillbirth Rates, given in two Divisions viz., Natal-Neonatal and Postnatal (2 to l l months), ~or 1911-15. anal for 1952.
Stillbirth Neonatal Combined Death Rates Rates Death Rates Stillbirth and 2-11 months
Neonatal Death Rates
1911-15 .... *45 43 88 70
1952 . . . . . . . . 26 22 48 13
The above table shows that over a period of fo r ty years in Scotland, there has been a fall in the infan t death rate in each of the two divisions, considerable in the natal-neonatal one, and gigantic in the later one. This change may be described as a shift to the left in infant mortali ty, and i t suggests that infant deaths during birth and the first month af te r it are due to more dangerous and intractable canses than those during the following eleven months; and some years ago I suggested that these two divisions of infant deaths might be labelled: the Catastrophic Deaths (natal-neonatal) and the Careless Deaths (211 months).
Catastrophic Dea,ths. This is a formidable group, and contains within it the ha rd core, the irreducible minimum of infant deaths; but even so the fall here has been substantial in the showing of the figures, and has been impressive beyond mere figures because of the formidable conditions that cause death at this time.
Only the briefest comments can be made on the chief components of this group of catastrophic deaths. They are prematuri ty , congenital malformations, asphyxia, bir th-injury, and pneumonia and other infec- tions. Prematur i ty has shown the largest decline in deaths : and yet it remains the biggest contr ibutor to the group : but the prospects of fu r ther reduction are good, both on the preventive side in the increasing efficiency of antenatal services, and also on the curative side in the increasing special care being given to prematures both in hospital and at home.
In Scotland in 1949 there were 4,429 deaths dur ing birth and the first month af ter birth, and 1,182 deaths during the remainder of the first year.
Careless Deaths. In this second division of infant deaths, infection of many kinds has always been the predominant cause of death; and in Scotland in 1949, pneumonia accounted for one-third of the deaths, and gastro-enteritis (or diarrhoea) for one-fifth; these two types of infection being the two largest contributors to the aggregate of deaths.
I t may seem silly and unfa i r to call this group the careless deaths, in view of the fact that the great reduction of deaths in this group since the century began has been only accomplished by much effort and care. I t is only by continued care that the remaining block of deaths from infection can be reduced to its attainable minimum.
I t will be noticed that the division between the two groups is not a clean cut; and that deaths from pneumonia and other infections appear in the first division, while quite a number of cases of congenital n~al-
REASSIGNMENT OF TASKS IN P ~ D I A T R I C S 447
formation and birth injury overflow into the second division and appear there as deaths. This mixture does not impair the pathological sound- ness and the practical value of the separation of the two groups.
This great fall in infant deaths during birth and throughout the first years of life has been brought about, not by one agency, but by a chain of services of child care, some old, some fairly new. These social and medical services may be described as weapons of control and defence in the war against disease and death in children. We are now ready to name and describe these various weapons of control, noting in which of the two divisions of infant deaths they are used, and if any of them might be sharpened and made more effective in use. Such a discussion will be in keeping with the title of the address : " Readjustment of Tasks in P~ediatrics "
The Services of Child Care. The list of services of infant child care is as follows : The home service of mothers and fathers; communal sanitation; the Antenatal and Maternity Hospital Service ; the Children's and Fever Hospital Service ; the service of family doctors ; the Maternity and Child Welfare Service.
The Home Service. The oldest and the most important of all these services is given at home by the busy hands and loving hearts of fathers and mothers. The maternal care of the child at home is the foundation service, and round it are ranged all the others in our list. The require- ments of the mother for her many and incessant tasks of child care are many, and may be difficult to meet: wise and instructed women to teach her how to carry out these daily tasks at home; a family doctor to supervise; supervision of her own health, especially in pregnancy and parturition; a suitable and sanitary house,; and a husband whose work feeds and clothes his household, and who exercises his rule and influence in family life.
But at the centre of child care are the instructed mind of the mother, the conscience of the mother and the strength of her arms. They are the central and essential postulates of child health.
Communal and Home Sa.nitation. The great reduction in infant deaths that has taken place is the achievement of many forces and agencies working together to this end. When P~ediatries mfffles and preens her feathers in contemplating this grand achievement, one of these agencies is apt to be forgotten. This is the silent service of sanitation-- the immense communal service of sewers, drainage, water supplies, lighting, food inspection, refuse removal and housing. Let us remember this, nor forget that this great public enterprise of sanitation is not yet completed so long as there remain considerable numbers of insanitary and overcrowded houses.
Nor should we forget that mothers have their part to play in this service of sanitation. The sanitary inspector and the scavenger do not come inside the home, ~vhere these duties fall upon the mother. Family doctors and health visitors who know the sanitary conditions of homes are entitled to admonish mothers if they neglect their sanitary duties; and they ought to impress upon all mothers the great importance of keeping in cleanness and order the house and all its contents, material and personal. This side of the work of the Child Welfare Service in preaching the duty and the great reward of cleanness, decency and
448 IRISH JOURNAL OF MEDICAL SCIENCE
order within the home should be kept in the foreground of the pro- gramme of education. And the reward of cleanness and order is not confined to the physical plane of lives saved and better health; it flows over into the moral sphere and bears fruit in self-control and self- respect, and in serenity and harmony of spirit for all who are within a well-kept home.
Antenatal Ma, ternity and Newborn Service. This is a well-organised and powerful service to protect the health and safety of mother and child in three periods of pregnancy, parturition, and puerperium. Its success is shown by the falling maternal, stillbirth, and neonatal death rates. There has been a great extension in the antenatal branch of the service in the last thir ty years, and this expansion will continue. About the same time more attention began to be paid to the care of the new- born, and especially of premature babies, and also to the study of the physiological and pathological problems of the newborn. The whole ~r- vice in its three branches is already strong, and as it expands further is certain to increase its powerful control over the health of mothers and babies. This sphere of influence is well defined, and its service is of a fundamental and far-reaching kind. The task assigned to it in p~ediatrics is in good hands.
The Maternity and Child Welfare Servive. The following remarks will deal only with the Child Welfare Service. The maternity side of the Service is supplementary to the Antenatal and Maternity Service.
The baby, after months of hidden and protected life in the womb of the mother, and after two or three weeks in the nursery of the maternity hospital, now returns home and remains for years at home in the ca~"e of its mother. Once it is ,at home another great service of child care swings into action--the Child Welfare Service.
This is a new service, set up on a national scale in England and Wales, Scotland and Ireland about thirty years ago.
The routine tasks of the clinics and home visits of the Child Welfare Service are to give attention to many minor illnesses and disorder, the detection of more serious illness, the assessment of the general condition of the baby, and the instruction of the mother in the rules whereby health may be maintained and restored. In these tasks we see in operation curative and preventive medicine. The preventive side is a service of education of mothers, and as an orga~ised service is only at its begin- ning, and has been mainly occupied in the instruction of mothers in domestic hygiene and infant feeding.
In the early part of this address, we noted the great fall in infant deaths in many parts of the world in the last fifty years. Which of these two medical services has made the greater contribution to this result--the curative services of children's fever hospitals, or the pre- ventive education given to mothers by the Child Welfare Service? Without attempting argument or producing evidence, my belief is that the contribution of preventive medicine by education has been the greater. Mothers have acquired somehow, and have put to use, much knowledge about infant feeding and the hygiene of the home; they have learned this, not out of books and newspapers, nor from grandmothers and wise neighbours, but from the lips of the new teachers in the Child Welfare Service. It must be remembered that the aim and policy of the
REASSIGNMENT OF TASKS IN P.~]DIATRICS 449
Child Welfare Service is twofold : to reduce death in children to a maxi- mum degree, and to maintain the lives of the survivors at a high level. It was set up for this double purpose and what has been done so far is a good beginning, and the opening of a vista of new and greater ~chieve- ment in the future.
D~alectics of the CMld Welfare Service. When we examine side by side the preventive and the curative branches of child medicine in a critical analysis, and t ry to reveal their inner nature, their governing principles and the logic of their activities we shall see how much the one differs from the other; and we shall have a clearer idea of what the future assignment of the tasks of the Child Welfare Service should be. The single term " dialectics " expresses the results of such an analysis.
The Child Welfare Service on its preventive side is a service of educa- tion in child care. Its pupils are mothers actually engaged in the tasks of child care. Its teachers are specially appointed doctors and nurses, the medical officers and health visitors of the service.
The knowledge which is exchanged in this service of education is two- fold: (a) the knowledge and clinical recognition of the physical and mental states tha~ constitute health throughout infancy and childhood; and (b) the knowledge of the instruments (or agents) necessary for health, and of their right use, viz., communal and domestic sanitation; food, feeding, and digestion; air, sunshine, exercise and rest, muscle con- trol, dexterity and carriage; social habits and beha~iour, etc.
The material for the teaching and practice of child health is found in every home, in the, children and their mothers and in the environment of the home; and also, more conveniently although less completely, at the assembly points of mothers and children in the clinics.
The teachers of the Child Welfare Service, the doctors and nurses, do not use the ordinary methods of education. Their task is to tell mothers of the things that they alone can do for their children, and to teach them how to do them. In this special sphere of education, the teachers do not stand behind desks and use blackboards; nor do they give lectures, going through an ordered course of instruction. The method of teaching is a personal, intimate and friendly interview between the doctor or nurse and the mother, by question and answer; an examina- tion of the child; the detection of a fault or faults in child care and a simple explanation of how they may be corrected. It is not an easy method of education, for the knowledge that is dealt with is deep and intricate, and its application involves details of technique, a~d both must be translated into the simple language of the home.
The teachers must themselves acquire this knowledge of child health and the methods of its practice before they become fully qualified to teach mothers. The present training of the teachers is at present far short of what is needed. What is required is the provision of schools of study and training for those who choose a career in the Child Welfare Service. Later, I shall elaborate this proposal as the most important reassignment for the educational work of the Child Welfare Service.
Dialectics of the Children's Hospital Servive (including Fevers). The nature of the medical work in children's hospitals is radically different from that in the Child Welfare Service.
The work of a children's hospital is the care of children suffering from
450 IRISH JOURNAL OF MEDICAL SCIENCE
disease. The material of this study and practice is provided by children suffering from disease of many kinds. The immediate and main object of study is not the whole body, but a part of it which may be large or small; when the disease in this fraction of disordered life is located and put right, and the child restored to health, the work of the hospital is done. The child leaves hospital, goes home, and remains outside the hospital service so long as health remains.
The composite body of knowledge which is gathered together in a children's hospital is of disease in children, the sum of hundreds of diseases, each a separate entity with its ewn cause, pathology, diagnosis and treatment. The preventive work of the welfare clinic deals not with fractions but with integers of life, and tries to establish and maintain that integral condition of life that we call health.
The education given in teaching children's hospitals is to medical students and nurses, and is in diseases of children, the material being provided by the child patients. From these two schools of training there proceed doctors and nurses who practise their skills in children suffering from disease. In a children's hospital, education in child health may be attempted; but it cannot be properly given, from the lack of the clinical materials of mothers and healthy children, and from the lack of experience of the staff in the clinical problems of child health.
Schoois of Study and Training in Child Health. Reassignment of Tazks in Peediatrics. Of all the services engaged in
child care, the Child Welfare Service is the youngest, and the weakest in organisation and prestige; but already it has done good work in reducing infant deaths, and the much greater work of assuring a higher quality of life throughout childhood lies in its hands. This programme of health in children by the education of mothers can be advanced by the provision of schools of study and training in child health, where the teachers of mothers can tm trained in its theory and practice.
This programme of study and tralning is wide and deep and covers the whole life of the child; but a modest beginning can bo made with domestic sanitation and dietetics.
The material for this study will be found in a selected child welfare centre; and the best is a clinic attached to a maternity hospital, where child life at its beginning is found in the nurseries of the newborn, and where the newborn on leaving hospital return to the welfare clinic and in this continuing attendance furnish an unbroken record of life from birth. Less suitable would be a welfare clinic at a children's hospital, where the members of the staff as they work in the clinic would tend to have a bias of mind and a ruling interest in disease rather than in health.
But these details of locus of the new training eentres, and even of their programmes, are of less importance. The, important thing is the firm acceptance of the principle, and its embodiment in experimental centres. When the Child Welfare Service has established in every large area a school of study and training in child health, it will find its work powerfully reinforced, and its authority, dignity and prestige increased.
The Antenatal, Maternity and Newborn Service. This triple service has in recent years been steadily increasing in the organisation and efficiency of its three branches. Its expansion will continue, and it is
REASSIGNMENT OF TASKS IN P2EDIATRICS 451
bound to make an important and perhaps a decisive contribution to the reduction of the catastrophic deaths, reaching the irreducible minimum of deaths among mothers and infants.
Children's a,nd Fever Hospital Services. These services have their preventive as well as their curative sides. On the curative side their power has been increased by the new drugs; and this will be increased by deeper exploration into the many unsolved problems of disease in children.
Sanitatiom The present high standards of communaI sanitation have been reached by a century of public effort, and can only be maintained by continued effort and vigilance. There remains a lag in the building of new houses, but that work is in hand. It must not be forgotten that domestic sanitation is largely the responsibility of mothers and of their advisers in the Child Welfare Service. Good houses must be accompanied by good housekeeping.
Panoraona. Our subject has been child care, with its aim of child health. Its
centre is the mother's care of her children at home. Round about these persons and this place are ranged great organised services, social and medical; these were begun about a hundred years ago and have now been brought to great efficiency and power. They can hardly be called auxiliary services for they are essential to the success of the whole enterprise.
These services in aid of the, mother have built up round the home a shield of defence, getting ever stronger, against disease and death in children, but they do not directly ensure a high level of health among children.
The latest of these services---the Child Welfare Service--is different from all the others. For it includes as an essential part a service of education that sets itself to teach the mother, not about disease, but knowledge of child care and its practice. This education in child health is the unique assigq~ment of the Child Welfare Service, by means of it the level of health in children can be progressively raised.
A high level of health in children cannot be reached unless mothers are given the instruments of child health and know how to use them. But they do not have this knowledge and must be taught it, and the teachers themselves must be well trained in the theory and practice of child health.
One part of the general aim of child care is the reduction of disease and death to its minimum; and in some countries this aim, if not yet reached, is not far off. The other part of the grand aim is optimum health in child life; this lies on the distant horizon, but it has now become a social idea and ideal. The time of its attainment, will largely depend upon the work of the Child Welfare Service, and upon the training of the doctors and nurses who are engaged in this great educa- tional service of child health.





























