Embed Size (px)
Citation preview

CURRICULUM IN CARDIOLOGY
Reassessment of the effects of vasodilator drugs in primary pulmonary hypertension: Guidelines for determining a pulmonary vasodilator response
Stuart Rich, M.D., Jorge Martinez, M.D., Wilfred Lam, M.D., Paul S. Levy, Sc.D., and Kenneth M. Rosen, M.D. Chicago, Ill.
Patients with primary pulmonary hypertension develop hemodynamic changes characterized by an elevation in pulmonary artery pressure and pulmo- nary vascular resistance, and by a reduced cardiac output.’ There does not appear to be any relation- ship, however, between the magnitude of these changes and the duration of the illness.2 Conse- quently it becomes difficult to distinguish patients early in the course of their disease from those who have had the illness for many years. It has been suggested that the acute response to vasodilator drugs may be helpful in this regard.3 Upon making the diagnosis of primary pulmonary hypertension it is recommended practice to test the responsiveness of the pulmonary vasculature with vasodilator drugs given intravenously at the time of cardiac catheter- ization4 A substantial reduction in the pulmonary vascular resistance following drug administration has been interpreted as resulting from vasodilation within the pulmonary vascular bed,5*6 suggesting that patients who respond favorably are earlier in the course of their illness, still having reversible vasoconstriction.3
Recent successes in the use of vasodilator drugs for the treatment of essential hypertension have stimulated interest in the use of these drugs for patients with primary pulmonary hypertension as well. Demonstration of a fall in the pulmonary
From the Section of Cardiology, Department of Medicine, Abraham Lincoln School of Medicine, University of Illinois College of Medicine; and the Epidemiology and Biometry Program, School of Public Health.
Supported in part by National Heart, Lung and Blood Institute Training Grant HL 07387 and by United States Public Health Service Training Grant HL 07381 (for work done by Dr. Rich at the University of
Chicago).
Received for publication June 7, 1982; accepted July 27, 1982.
Reprint requests: Stuart Rich, M.D., Cardiology Section, University of Illinois Hospital, P.O. Box 6998, Chicago, IL 60680.
0002~8703/83/010119 + 09$00.90/O o 1983 The C. V. Mosby Co.
vascular resistance from acute drug administration has been used as a criterion to place these patients on chronic oral therapy.5 We analyzed the acute changes that a variety of vasodilator drugs produced on both the systemic and pulmonary vasculatures in five patients with primary pulmonary hypertension. Our current results, when viewed in light of previous results, allow us to make some new generalizations regarding drug responsiveness in this disease. In addition, our results suggest that some traditional beliefs regarding therapy need to be reexamined.
METHODOLOGY
Patients. The study population was a group of five patients, three females and two males, 19 to 47 years in age (mean = 34), who were evaluated between 1978 and 1981 (three at the University of Chicago and two at the University of Illinois). None of the patients had clinical signs of right heart failure, but four had significant dyspnea with effort and one had mild effort-related fatigue. The patients were off all medications at the time of study. All patients gave their informed consent to the drug testing.
Measurements. The patients were studied in the supine position either in the Coronary Care Unit (CCU) or in the cardiac catheterization laboratory. A right heart catheterization was performed with either a No. 7 French thermodilution Swan-Ganz flow directed catheter or a No. 7 French Cournand catheter. The radial artery was canulated with a short Teflon catheter. Pressures were monitored in the catheterization laboratory with a Gould-Sta- tham P23Db pressure transducer and a multichan- nel recorder (Electronics for Medicine VR-16), and in the CCU with a Gould-Statham P23Db pressure transducer and a two-channel recorder (Hewlett- Packard). An ECG lead was monitored continuously throughout each study.
119

120 Rich et al. January, 1983
American Heart Journal
Table I. Hemodynamic effects of vasodilators in five patients with primary pulmonary hypertension -~
MW II Mean systemic puhunaq Syst+~mlc, ruscular Pulmonary c~a.scular
Cardiac output pFk?SSUF~ pres.sure rc.5 istanc e rcsistanc6~ (Llmin) (mm Hg) (mnl Hg) (dyws-.sw.cnlr ‘: id.yws-see -(‘72 .J
Patient Age/sex Drug Before After Before After Before After Before After reduction Before After reduction
1 47M HYD 3.4 3.6 120 116 48 46 2682 348” ;.,: 870 842 is.2 2 37F ISP 2.1 4.2 90 86 i-
;;I 65 3124 1494 52.2 1905 1069 43.5
2’ DIAZ 1.7 2.2 90 62 55 3859 1935 49.9 2023 1786 II 7 2t PHEN 2.6 2.7 88 79 6’) 62 2461 2066 16.0 1692 162:< .1. I 3 20F ISP 4.1 5.2 90 95 80 95 1580 1325 16.: 1405 1325 .i.; 3* TOL 3.3 7.6 88 85 70 80 1981 81 :I 59.0 1696 844 31.2 3t PHEN 3.3 3.7 90 88 70 65 2036 17K1 13.4 1478 1225 1’7.1 4 19F TOL 5.0 5.8 115 100 60 35 1760 1310 25.6 800 345 S6.9 4* HYD 4.6 5.1 87 80 60 65 1460 119’ 18.1 904 863 .I.,> 4t ISP 5.3 6.2 107 87 ;(J 80 1555 Ill70 31.2 906 890 i .x 5 46M TOL 3.5 4.5 104 90 64 58 2221 1493 32.8 1314 924 29.7 5* HYD 2.2 3.9 110 90 68 65 3706 1648 %55..5 2201 1160 47.3
Mean 3.4 4.9 98 88 63 64 2369 1549 34.6 1433 107.5 “4.9 rt SE 0.3 0.4 3 4 ‘! 4 238 134 140 I11 p value <O.Ol <O.Ol NS <U.OO! <O.Ol
____- - _..---_ .- Abbreviations and symbols: * = same patient, second drug; t = same patient, third drug; DIAZ = diazoxide; HYD = hydralazine; ISP = isoprotwznol;
PHEN = phentolamine; TOL = tolazoline.
Cardiac outputs were determined either by the thermodilution technique (Edwards 9150 C.O. com- puter), or by the Fick equation with simultaneous arterial and mixed venous samples collected in heparinized syringes and oxygen content deter- mined on a cooximeter (Instrument Laboratory 282), and exhaled gas collected in a paramagnetic oxygen analyzer (Beckman MMC). In every instance baseline measurements were made of the systemic arterial pressure (SAP), right atria1 pressure (RAP), pulmonary artery pressure (PAP), and pulmonary wedge pressure (PWP), all in millimeters of mercu- ry, and cardiac output (CO), in liters/minute, prior to the administration of each drug. Mean intravas- cular pressures were obtained by electronic integra- tion. Values for vascular resistances were calculated (in dynes-set-cma5) from the following formulas: systemic vascular resistance (SVR) = (SAP - RAP) CO) x 80; total systemic resistance (TSR) = (SAP/ CO) x 80; pulmonary vascular resistance (PVR) = (PAP - PWP) CO) x 80; and total pulmonary resis- tance (TPR) = (PAP/CO) X 80.
Drug administration. The administration of the various drugs given to each patient is summarized in Table I. Five different vasodilator drugs were used. Tolazoline was administered (three patients) as a 1 mg/kg intrapulmonary injection over 30 seconds with pressures and cardiac outputs measured after 15 minutes. Hydralazine was given (three patients) as a 0.3 mg/kg injection over 10 minutes with the
measurements of pressures and cardiac outputs made after 30 minutes. Isoproterenol was given (three patients) as a constant infusion up to 5 pg/kg for 10 minutes. Phentolamine was given (two patients) as a 5 mg slow intravenous injection with pressures and cardiac outputs measured after 10 minutes. Diazoxide was given (one patient) as an intravenous injection of 150 mg followed by 300 mg 5 minutes later. Measurements of pressures and cardi- ac outputs were made 15 minutes later.
In each patient with the exception of patient No. 3, successive drugs were administered after consid- erable time intervals (minimum 4 hours) to allow for adequate clearance of the preceding drug, and to have the patient in a restful state. Because of the rapid worsening symptoms in patient No. 3, three drugs were tested at one session in the catheteriza- tion laboratory. Isoproterenol was the first drug given, followed by phentolamine 35 minutes after the cessation of the isoproterenol infusion, when the patient’s heart rate and pulmonary and systemic pressures had returned to baseline. This was fol- lowed by diazoxide 40 minutes later, again after the heart rate and pressures had returned to the previ- ous baseline measurements.
Statistics. Mean levels of hemodynamic variables before and after administration of each drug were calculated, and the significance of the drug effect on each variable was evaluated by the t test for paired data. Patients were categorized into groups accord-

Volume 105
Number 1 Vasodilators in primary pulmonary hypertension 121
Table il. Changes in pulmonary pressure, pulmonary resistance, and cardiac output in five patients tested with vasodilator drugs (reported as percent increase [+] or percent decrease [-I)
Patient 1 2 3 4 5
Tolazoline
Hydralazine
Isoproterenol
Phentolamine
Diazoxide
PA co
PVR PA co
PVR PA co
PVR PA co
PVR PA co
PVR
-4 +6 -3
+14 +100
-44 0
+4 -4
+10 +26 -12
+14 i-130
-50
+19 +21
-6 -1
+13 -16
-38 -9 +16 +21 -57 -30
+8 -4 +11 t80
-5 -47 t14 +17
-2
CO = cardiac output; PA = mean pulmonary artery pressure; PVR = pulmonary vascular resistance.
ing to their levels of certain hemodynamic variables, and contingency table analysis was used to evaluate the significance of differences between groups with respect to the distribution of other categorical vari- ables. The Pearson product moment correlation coefficient was used to evaluate the association between mean pulmonary artery pressure and pul- monary vascular resistance, and between the change in cardiac output and vascular resistances following drug testing.
OBSERVATIONS
Overall effects of vasodilators. The results of the drug effects on these patients as a group are summa- rized in Table I. There are several features of note. Although these agents (as one would anticipate) lowered the systemic arterial pressures significantly, there was no significant change in the pulmonary artery pressure. In every study the cardiac output increased and both the systemic vascular resistance and pulmonary vascular resistance fell. There was no significant correlation, however, between the change in pulmonary artery pressure and the per- cent reduction in pulmonary vascular resistance after drug administration in these patients (r = 0.42, p < 0.1).
Effect of vasodilators in individual patients. The effect of the various vasodilators on the pulmonary artery pressure was varied and unpredictable (Table II). Some agents lowered the pressure in some patients and raised it in others. Patient No. 3 had a 7% reduction in mean pulmonary artery pressure with phentolamine, but a 14% increase in mean pulmonary pressure with tolazoline. Patient No. 4 had a 38% reduction in mean pulmonary artery
pressure with tolazoline but a 14% increase in mean pulmonary artery pressure with isoproterenol. Of the four patients given more than one drug, only one (patient No. 5) had the same direction of change in mean pulmonary artery pressure to all agents given.
The only drug that had a consistent effect was isoproterenol, which caused an increase in mean pulmonary artery pressure in all three patients to whom it was given. No drug caused the mean pulmonary artery pressure to be lowered in every case. Although tolazoline caused the largest reduc- tion in pulmonary pressure in one of the patients (patient No. 4), it caused a substantial increase in pulmonary artery pressure in another.
Review of the literature with statistical analysis. We compared our results to previously reported studies to see if our findings were representative. We attempted to review every known paper published on the effects of vasodilator drugs in patients with primary pulmonary hypertension and have included in this review each paper that (1) describes the effects of vasodilator type drugs in patients with primary pulmonary hypertension; (2) provides, as a minimum, the acute or short-term effects of the drugs on the cardiac output, pulmonary artery pres- sure, systemic and pulmonary resistances; and (3) provides data for both the control and treated states.
Between 1951 and 1981 there have been only 13 such published papers,5*6. 7-17 which describe the effects of seven different drugs on 33 different patients. Eight of these are case reports,6, g, I19 13-17 and one deals with only two patients.7 Most studies deal with the effects of one drug on one or more patients.

122 Rich et al. January. 1983
American Heart Jownai
Table III. Hemodynamic effects of vasodilator drugs in patients with primary pulmonary hypertension as reported in the literature
Ref. Patient
no. Dose
C‘ardiac output
(L/mini
Before After
Mean systemic pressuw (mm Hg) -~ -__-..
Before After
Mean pulmonar>
pressure (mm Hg)
Reforr After
‘, fall In systemic
resistance
; /-a/l 1n pulmonary resistance
Acetylcholine (i.v. infusion) (8) 1 0.5 mg/min
(15) 2 4.25 Fg/min (17) 3 3 pg/min
Tolazoline (i.v.) (17) 3 75 mg
(7) 4 25 mg (7) 5 50 mg
(13) 6 10 mg (16) 7 50 mg
Isoproterenol (i.v. infusion) (10) 8 1 rg/min 3.1 4.8 83 82 53 50 :<6 67 (10) 9 2 pglmin 3.6 5.1 90 92 56 60 28 24 (10) 10 2 pg/min 2.5 3.5 127 118 90 110 43 12 (10) 11 1 rg/min 3.6 4.4 88 84 40 45 22 11 (10) 12 1 pg/min 2.2 3.4 86 82 68 80 38 23
(10) 13 1 fig/min 3.2 5.0 82 72 64 85 45 I 8 (10) 14 2 rg/min 2.1 3.2 99 118 57 HO 22 8
Hydralazine (oral) (5) 15 (5) 16 (5) 17 (5) 18
50 mg 3.5 8.6 135 110 78 47 67 76 50 mg 3.3 5.4 110 102 -56 34 43 63
50 mg 4.9 8.8 110 110 68 75 44 40 50 mg 3.6 5.6 76 80 61 60 34 37
Diazoxide (i.v.) (12) 19 (12) 20 (12) 21 (12) 22 (12) 23 (12) 24 (12) 25 (12) 26 (12) 27
(6) 28 (6) 29 (6) 30 (6) 31 (9) 32
300 mg 4.1 5.6 82 73 73 70 53 1.17 300 mg 2.9 4.5 107 86 71 83 49 23 300 mg 2.5 5.5 110 82 73 68 66 57
480 mg 2.2 4.9 84 63 69 56 66 64 480 mg 2.1 3.3 123 71 60 60 61 36 480 mg 4.2 7.4 87 68 65 48 57 58 480 mg 4.4 7.5 85 51 52 55 63 38 600 mg 3.2 4.4 86 68 86 86 44 27
600 mg 2.5 5.5 88 68 60 62 66 53 515 mg 2.4 4.8 92 67 71 67 68 54 515 mg 3.3 5.3 113 83 76 63 53 48 515 mg 2.8 4.9 84 72 7” d .? 59 50 54 515 mg 2.8 3.8 83 87 64 89 23 0 300 mg 2.6 3.9 78 70 54 52 41 :i6
Nifedipine (sublingual) (9) 32 20 mg
Phentolamine (i.v.) (14) 93 5 mg
Mean 3 SE p value
3.42 5.28 94.3 84.8 64.1 61.8 40.8 37.8 0.20 0.26 2.84 3.09 2.16 3.20 3.01 3.27
0.0001 0.0001 NS 0.0001 0.0001
‘Refers to cases in which cardiac index was given instead of cardiac output. The values of these two cases were excluded from the statistical analyses.
4.7 5.2 122 130 74 35 4 60 1.72 1.87* 101 96 39 30 13 30 4.19 5.05 62 64 8” 88 15 ii
3.44 4.18 72 68 82 80 26 “2 2.72 3.85 95 93 48 35 31 5(! 3.53 5.85 102 106 47 46 37 4 1 6.7 8.0 100 98 52 45 18 :14 3.73 4.98* 85 81 72 68 28 29
2.23 5.16 73 76 58 55 60
6.7 8.0 100 98
63
45 35 18 a3

Volume 105
Number 1
Two studies deal with the effects of two drugs on a single patient.gr’7 Thus we have obtained hemody- namic information about the results of 35 drug challenges in 33 patients with primary pulmonary hypertension; the results of these studies are listed in Table III.
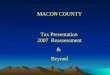
We found that the findings of these studies paralleled our own experience. The cardiac output rose in every patient in every case, and both the systemic and pulmonary resistances fell in every patient with every drug. There was no correlation between the mean pulmonary artery pressure in the control state and the fall in pulmonary vascular resistance after drug administration (Fig. 1). The mean fall in pulmonary vascular resistance after drug administration was 37.8 % , while the mean fall in pulmonary artery pressure was 5.9 % . The pulmo- nary artery pressure fell in only 21 of the 35 trials, and in seven of these cases the fall in pulmonary artery pressure was less than 5 mm Hg.
Relative effects of the different vasodiiators (Table
IV). We checked to determine if any of the particular drugs used had significantly different effects in these patients. In light of the small numbers of patients tested with each drug, we chose to compare the four drugs with the greatest use: tolazoline (five patients), isoproterenol (seven patients), hydral- azine (four patients), and diazoxide (14 patients). The administration of each of these individual drugs resulted in significant increases in the cardiac out- puts and significant reductions in the systemic and pulmonary resistances in all patients. There were some differences between the drugs as well. Tolazo- line was the only agent that caused a significant reduction in the mean pulmonary artery pressure. Conversely, isoproterenol caused a significant increase in the pulmonary artery pressure in the patients tested. Neither diazoxide nor hydrala- zine caused significant changes in the pulmonary artery pressure, but diazoxide was the only drug that caused a significant fall in the systemic pres- sure.
Characterization of the hemodynamic response to vasodilators. Since vasodilators acutely lowered the pulmonary vascular resistance in every patient with primary pulmonary hypertension in our review, a fall in pulmonary resistance did not discriminate between a beneficial and an adverse drug effect (i.e., patients in whom the pulmonary artery pressure is lowered compared to those who have an increase). The fall in the systemic and pulmonary vascular resistances that occurred were largely a manifesta- tion of the increase in cardiac output that resulted from the vasodilator drugs. However, the changes in
Vasodilators in primary pulmonary hypertension 123
3-
3-
3-
3-
3-
3-
3-
3-
4
n = 35 r = 0.035
p = NS
.
l
.
.
. .
l .
. 0.
.
.
. . .
l : .
.
. .
. .
. .
. . . .
zr- 50 I 60 1 . 70 I 80 I 90 1 MEAN PULMONARY ARTERY PRESSURE
(mm Hg at baseline)
Fig. 1. Relationship between the baseline mean pulmo- nary artery pressure and the percent fall in pulmonary vascular resistance in the 33 patients challenged with various vasodilator drugs as reported in the literature. No significant correlation could be established between the fall in pulmonary vascular resistance and the severity of the pulmonary hypertension.
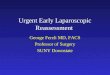
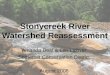
the systemic and pulmonary vascular resistances were not identical. We looked at the association be- tween the change in cardiac output against the changes in systemic and pulmonary resistance inde- pendently (Figs. 2 and 3). Although as one would expect there was a correlation between both, the change in cardiac output that occurred correlated more with the change in systemic vascular resistance than it did with the pulmonary vascular resistance.
In an attempt to identify a pulmonary vasodilator response, we looked at those patients in whom the change in pulmonary vascular resistance was greater than the change in systemic vascular resistance. There were 16 such patients in our series. A closer look at their hemodynamic response to the drug challenge showed that they had a significant reduc- tion in pulmonary artery pressure without a fall in

124 Rich et al. January, 1983
American Heart Journal
% 60-
+ 2 50-
4 & 40-
2 30- 8 j zo- a
z IO-
.
. . n = 35 -
r = 0.62
% INCREASE IN CARDIAC OUTPUT
Fig. 2. The relationship between the percent fall in pulmonary vascular resistance and the percent increase in cardiac output (see text).
Y 2 5 70- . ’ I .
60- .
3 . . .
=j 50- . .
t: l * . . .
p 40- . . . . 0 . r 30- i+
. . . n = 35
; . . .
. r = 20- 0.84 .
z .
IO- i . i-2 I L I 1 I I 1 I 1 8 I 1
8 20 40 60 80 loo I20
% INCREASE IN CARDIAC OUTPUT
Fig. 3. The relationship between the percent fall in systemic vascular resistance and the percent increase in cardiac output (see text).
systemic pressure, in addition to the rise in cardiac output that occurred (Fig. 4). All of these changes would be considered to be beneficial in patients with primary pulmonary hypertension.
COMMENTS
There has been renewed interest on the use of vasodilator drugs in the treatment of primary pul-
monary hypertension, owing to the success enjoyed from using these drugs in patients with essential hypertension by creating a sustained reduction in blood pressurei and congestive heart failure where they result in an increase in cardiac output.lg It is not clear, however, what constitutes a beneficial effect in patients with primary pulmonary hyperten- sion, who often have both elevated pulmonary arte-

Volume 105
Number 1 Vasodilators in primary pulmonary hypertension 125
B A SYSTEMIC PULMONARY
Fig. 4. The mean systemic and pulmonary arterial pressure before and after drug administration in the patients in whom the pulmonary vascular resistance fell more than the systemic vascular resistance. There was no significant fall in the systemic pressure in this group, while the pulmonary pressure fell in every case. B = before; A = after.
Table IV. Comparison of effects of different vasodilators on the systemic and pulmonary circulations
Cardiac output Mean systemic (Llmin) pressure (mm Hg)
Before After Before After
Mean pulmonary pressure (mm Hg)
Before After
% fall in
systemic resistance
% fall in pulmonary resistance
Tolazoline
Mean 4.35 5.47 90.8 89.2 60.2 54.8 28.0 35.2
f SE 0.79 0.95 5.54 6.67 7.09 8.29 3.11 4.83
P < 0.05 NS < 0.05 < 0.001 < 0.001 Isoproterenol
Mean 2.90 4.20 93.6 92.6 61.1 72.9 33.4 22.6
SE 0.24 0.31 5.96 6.92 5.87 10.15 3.60 7.75
P <O.OOl NS <0.025 <O.OOl <O.OOl Hydralazine
Mean 3.83 7.10 107.7 100.5 65.7 54.0 47.0 54.0 SE 0.36 0.93 12.1 7.09 4.77 8.78 7.04 9.35
P <0.05 NS NS <O.OOl <O.OOl Diazoride
Mean 3.0 5.09 93.0 72.1 67.6 65.6 54.3 41.3
SE 0.20 0.32 3.76 2.61 2.44 3.39 3.35 4.68
P <O.OOl <O.OOl NS <O.OOl <O.OOl
rial pressures and low cardiac outputs. Intuitively, a fall in the pulmonary arterial pressure would seem to be the most appropriate parameter to gauge a beneficial response. If normalization of the pulmo- nary artery pressure were chosen as the standard for gauging successful drug therapy, as it is with system- ic hypertension, then no patient with primary pul- monary hypertension in our review would be consid- ered to have successful therapy with vasodilator drugs.
Some investigators have claimed favorable results from vasodilator drugs by demonstrating a fall in the pulmonary vascular resistance, even when the pulmonary arterial pressure remained unchanged or became elevated.5 There are several objections to using a change in pulmonary vascular resistance as
the guide to drug therapy. The relationship between pulmonary resistance and pulmonary blood flow is based on assumptions made using Poiseuille’s law which are not entirely correct.22 Firstly, it has been shown that the relationship between pulmonary flow and pressure is curvilinear rather than along a straight line.‘l Since we cannot measure pulmonary resistance directly but rather calculate it from mea- surements of flow and pressure, the implicit changes that we seem to be seeing in resistance may be misleading. In addition, since the pulmonary vascu- lar bed is not a true closed system, increases in pulmonary blood flow could occur by recruitment of unused vascular channels rather than by vasodila- tion.22 Finally, it appears that the pulmonary vascu- lar resistance falls predictably in all patients with

126 Rich et al. January. 1983
American Heart Journal
primary pulmonary hypertension given vasodilator drugs, regardless of the severity of the pulmonary hypertension, thus making a reduction in pulmo- nary resistance alone an inadequate discriminator between a beneficial and an adverse drug effect. Presently there exist no accepted standards by which beneficial drug effects are measured in treat- ing primary pulmonary hypertension.
It appears that vasodilators act predominantly on the systemic circulation in most patients with pri- mary pulmonary hypertension. The change in pul- monary vascular resistance that occurs is probably a passive manifestation of the change in cardiac out- put. There are some patients, however, who do appear to have a beneficial response to these drugs. We have characterized them as having a fall in pulmonary resistance of a greater magnitude than the fall in systemic resistance, which is accompanied by a significant fall in pulmonary artery pressure without a significant change in systemic pressure, suggesting a pulmonary vasodilator effect.
Our series of five patients does not represent a new therapeutic approach to the drug testing of patients with primary pulmonary hypertension. However, the five patients that we have studied illustrate how a given patient could respond quite differently to a variety of drugs, and how a given drug can cause varied responses. Consequently, we feel that statements that are made about the irre- versibility of the pulmonary hypertension based on a single drug challenge are inaccurate. In fact, such statements may lead to an erroneous conclusion about the pulmonary vascular reactivity in a patient who might otherwise benefit from a different drug. We are also uncertain of the usefulness in testing patients having primary pulmonary hypertension for the purpose of selecting agents for chronic therapy with agents that have no suitable oral counterpart, since the response to any one given agent does not appear to predict the response to another, and affords no insight into the severity of the illness.
We compared the data in the literature to see if we could identify any of the drugs as being superior to the others for the therapy of primary pulmonary hypertension. Unfortunately, the number of patients tested with each of the drugs is relatively small. It appears, however, that isoproterenol has the least favorable effects, and that tolazoline has the most favorable effects. Neither agent is suitable for chronic oral therapy. Since no drug with pure pulmonary vasodilator properties has been identi- fied-i.e., an agent that will cause the pulmonary artery pressure to fall without changing the cardiac
output or systemic pressure--we feel that it is unlikely that any one of the existing vasodilator drugs will prove superior to the others for primary pulmonary hypertension. It should also be appreci- ated that the results of our literature review likely are skewed toward favorable results. Unfavorable drug responses in patients with primary pulmonary hypertension probably occur more commonly but go unreported.
In summary, we have shown that demonstrating a fall in the pulmonary vascular resistance with vaso- dilators in patients with primary pulmonary hyper- tension does not provide evidence of a beneficial drug effect, since a fall in pulmonary vascular resistance seems to occur in all patients, regardless of the severity of the pulmonary hypertension. In addition, there is no relationship between the fall in pulmonary resistance and the change in pulmonary artery pressure that occurs. As these drugs appear to work predominantly on the systemic circulation in most cases, we suggest that patients in whom the fall in pulmonary vascular resistance exceeds that of the systemic vascular resistance are manifesting a pul- monary vasodilator effect, which might be of bene- fit. Ideally, one would like to see normalization of the pulmonary artery pressure, but this seems to be a rare event.
CONCLUSIONS
Primary pulmonary hypertension is an illness in which a sustained elevation in pulmonary artery pressure leads to an increased pulmonary vascular resistance and a reduced cardiac output. Although the condition had been considered untreatable, vasodilator drugs are now being employed with the hope of arresting or reversing these hemodynamic changes. We report our experience in testing five patients with primary pulmonary hypertension with five different vasodilator agents. We also reviewed the literature and analyzed previously published results on the use of vasodilator drugs in patients with primary pulmonary hypertension. We found that all vasodilator agents cause an increase in cardiac output and a fall in pulmonary vascular resistance, regardless of the severity of the pulmo- nary hypertension. In only a few patients, however, is there a lowering in the pulmonary artery pressure. By comparing the percent fall in pulmonary vascular resistance to the percent fall in systemic vascular resistance produced by these drugs, we were able to identify a group of patients who not only had an increase in cardiac output and a fall in pulmonary vascular resistance, but who had a lowering of pulmonary artery pressure in each case as well. Thus

Volume 105 Number 1 Vasodilators in primary pulmonary hypertension 127
since a fall in the pulmonary vascular resistance is not necessarily accompanied by a fall in the pulmo- nary artery pressure, using the change in pulmonary vascular resistance alone as an indicator of benefi- cial drug effect can be misleading. One should rather assess the relative drug effects on both the systemic and pulmonary circulations in these patients to help identify drugs that might be beneficial.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Fishman AP, Pietra GG: Primary pulmonary hypertension. Ann Rev Med 31:421, 1980. Kanemoto N, Sasamoto H: Pulmonary hemodynamics in primary pulmonary hypertension. Jpn Heart J 20:395, 1979. Samet P, Bernstein WH: Loss of reactivity of the pulmonary vascular bed in primary pulmonary hypertension. AM HEART J 66:197, 1963. Grossman W: Cardiac catheterization and angiography. 2nd ed. Philadelphia, 1980, Lea & Febiger, p 119. Rubin LJ. Peter RH: Oral hvdralazine theranv for nrimarv pulmonary hypertension. N Engl J Med 302:69, 1980. - Wang SWS, Pohl JEF, Rowlands DJ, Wade EG: Diazoxide in treatment of primary pulmonary hypertension. Br Heart J 40:572, 1978. Gardiner JM: The effect of “priscol” in pulmonary hyperten- sion. Aust Ann Med 3:59, 1954. Charms BL: Primary pulmonary hypertension. Effect of unilateral pulmonary artery occlusion and infusion of acetyl- choline. Am J Cardiol 8:94, 1961. Camerine F, Alberti E, Klugmann S, Salve A: Primary pulmonary hypertension: Effects of nifedipine. Br Heart J 44:352, 1980. Daoud FS, Kelly DB, Reeves JT: Isoproterenol as a potential pulmonary vasodilator in primary pulmonary hypertension. Am J Cardiol 42:817, 1978.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
ElKayam U, Frishman WH, Yoran C, Strom J, Sonnenblick EH, Cohen MN: Unfavorable hemodynamic and clinical effects of isoproterenol in primary pulmonary hypertension. Cardiovasc Med 3:117, 1978. Honev M. Cohen L. Davies N. Denison D: Clinical and hemodynamic effects of diazoxide in primary pulmonary hypertension. Thorax 35:269, 1980. Rudolph AM, Paul MH, Sommer LS, Nadas AS: Effects of tolazoline hydrochloride (Priscoline) on circulatory dynamics of patients with pulmonary hypertension. AM HEART J 55:424, 1979. Ruskin JN, Hutter AM: Primary pulmonary hypertension treated with oral phentolamine. Ann Intern Med 90:772, 1979. Samet P, Bernstein WH, Widrich J: Intracardiac infusion of acetylcholine in primary pulmonary hypertension. AM HEART J 60:433, 1960. Yu PN: Primary pulmonary hypertension: Report of six cases and review of literature. Ann Intern Med 49:1138. 1958. Yuceoglu YZ, Dresdale DT, Valensi QJ, Narvas RM, Gottlieb NT: Primary pulmonary hypertension with hoarseness and massive (fatal) hemoptysis. Vascular Dis 4:290, 1967. Chidsey CA III, Gottlieb TB: The pharmacologic basis of antihypertensive therapy: The role of vasodilator drugs. Prog Cardiovasc Dis 17:99, 1974. Chatterjee K, Parmely W: The role of vasodilator therapy in heart failure. Prog Cardiovasc Dis 19:301, 1977. Burton AC: Physiology and biophysics of the circulation. Chicago, 1972, Year Book Medical Publishers, Inc, p 90. Fishman AP: Dynamics of the pulmonary circulation. In Hamilton WF, Dow P, editors: Handbook of physiology, section 2: Circulation. Vol 2. Washington, D.C., 1963, Ameri- can Physiological Society, p 1167. Maseri A, Caldini P, Howard P, Joshir C, Permutt S, Zierler KL: Determinants of pulmonary vascular volume-Recruit- ment versus distensibility. Circ Res 31:218, 1972.