Embed Size (px)
Citation preview
Accreditation Council for Graduate Medical Education
© 2014 Accreditation Council for Graduate Medical Education
Realizing the Promise of CBME for Patients and Professionals
© 2014 Accreditation Council for Graduate Medical Education
• Where we are and where we need to go • Why CBME and why now?
• What is needed to realize the “promise”
Outline
© 2014 Accreditation Council for Graduate Medical Education
“The Journey of a 1,000 Miles Begins with a Single Step”
© 2014 Accreditation Council for Graduate Medical Education
Where We Are As a Country
© 2014 Accreditation Council for Graduate Medical Education
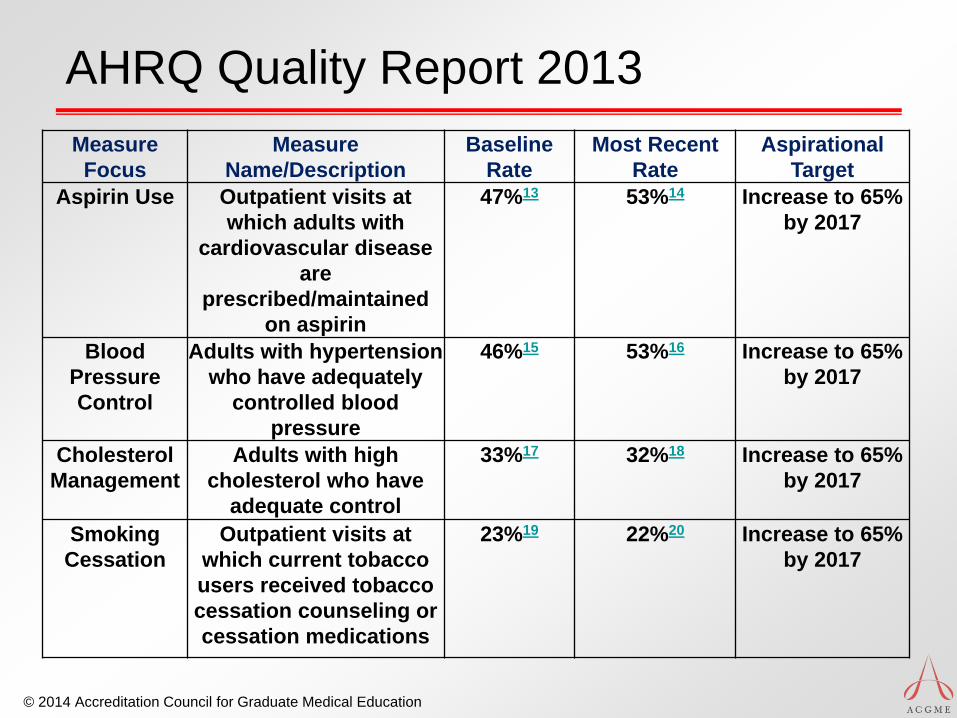
AHRQ Quality Report 2013 Measure Focus
Measure Name/Description
Baseline Rate
Most Recent Rate
Aspirational Target
Aspirin Use Outpatient visits at which adults with
cardiovascular disease are
prescribed/maintained on aspirin
47%13 53%14 Increase to 65% by 2017
Blood Pressure Control
Adults with hypertension who have adequately
controlled blood pressure
46%15 53%16 Increase to 65% by 2017
Cholesterol Management
Adults with high cholesterol who have
adequate control
33%17 32%18 Increase to 65% by 2017
Smoking Cessation
Outpatient visits at which current tobacco users received tobacco cessation counseling or cessation medications
23%19 22%20 Increase to 65% by 2017
© 2014 Accreditation Council for Graduate Medical Education
© 2014 Accreditation Council for Graduate Medical Education
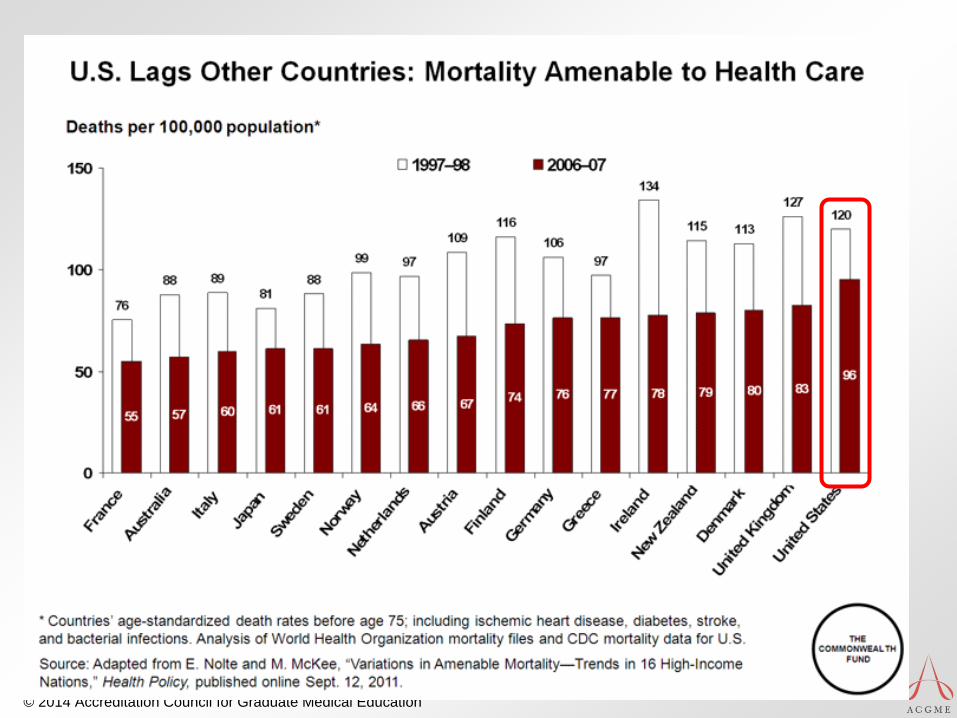
Arnie Milstein: ABIMF Forum 2010 “Since physician graduates of American medical education organizations typically lead or heavily influence US health care delivery, one source of indirect, broad, outcome-based evidence [of the effectiveness of the medical education enterprise] is the overall performance of the US health care system. The width of the performance gaps on the aims of effectiveness, safety and efficiency understandably reduces society’s confidence that physicians are adequately honoring their Hippocratic promises.”
Milstein A. Trailing Winds and Personal Risk Tolerance: An External Perspective on the Opportunity for Medical Educators to Fulfill Their Social Contract Permanently.
© 2014 Accreditation Council for Graduate Medical Education
Who is Raising Concern? • Institute of Medicine (2008)
• Resident Duty Hours: Enhancing Sleep, Supervision, and Safety
• Retooling for an Aging America • Congress (2011-12)
• Reductions in GME funding • Request to IOM to review GME regulation
• MedPAC • June 2009 Report • October 2009 Hearing • June 2010 Report
• IOM Financing/Regulation report pending
© 2014 Accreditation Council for Graduate Medical Education
Do We Have A
“Design Problem”?
© 2014 Accreditation Council for Graduate Medical Education
Ghost of Donabedian…
In Medical Education…
Structure X Process ≠ Outcome
© 2014 Accreditation Council for Graduate Medical Education
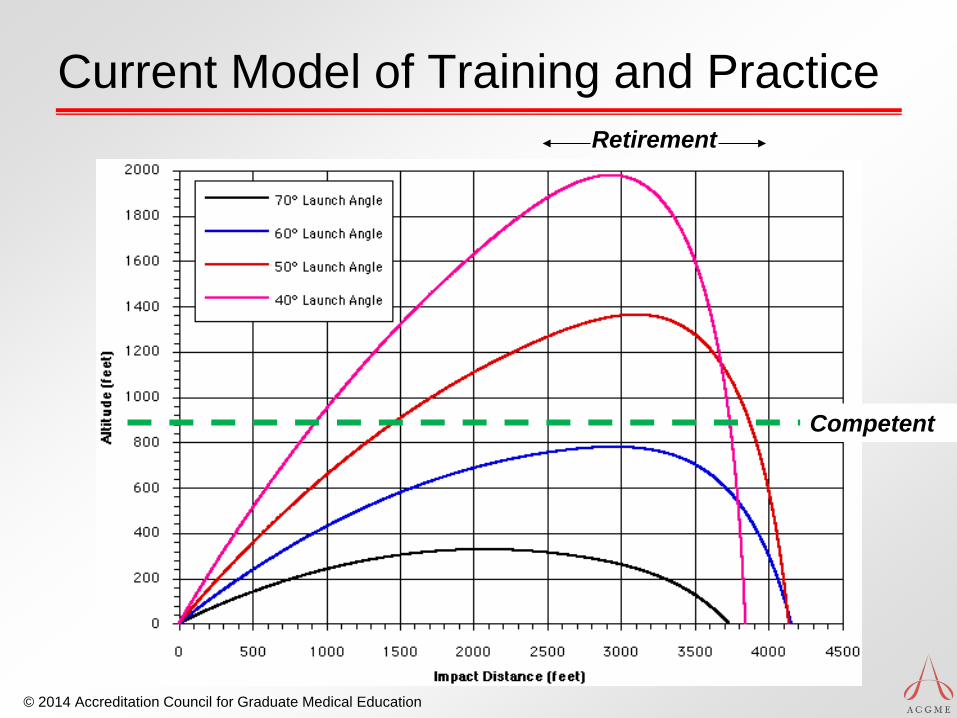
Current Model of Training and Practice Retirement
Competent
© 2014 Accreditation Council for Graduate Medical Education
Training Requirements for Endo
Train in an accredited program: http://www.acgme.org/acgmeweb/Portals/0/PFAssets/2013-PR-FAQPIF/143_endocrinology_diab_metab_int_med_07132013.pdf
24 months total 12 months clinical Rate the six general
competencies and overall competence
Take a test at the end
© 2014 Accreditation Council for Graduate Medical Education
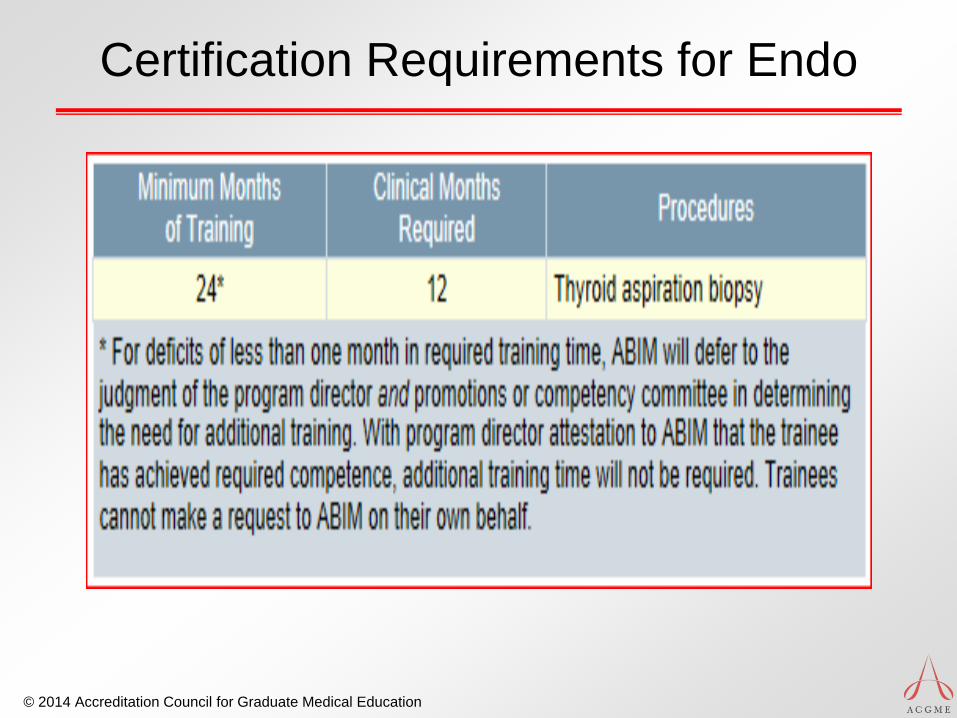
Certification Requirements for Endo
© 2014 Accreditation Council for Graduate Medical Education
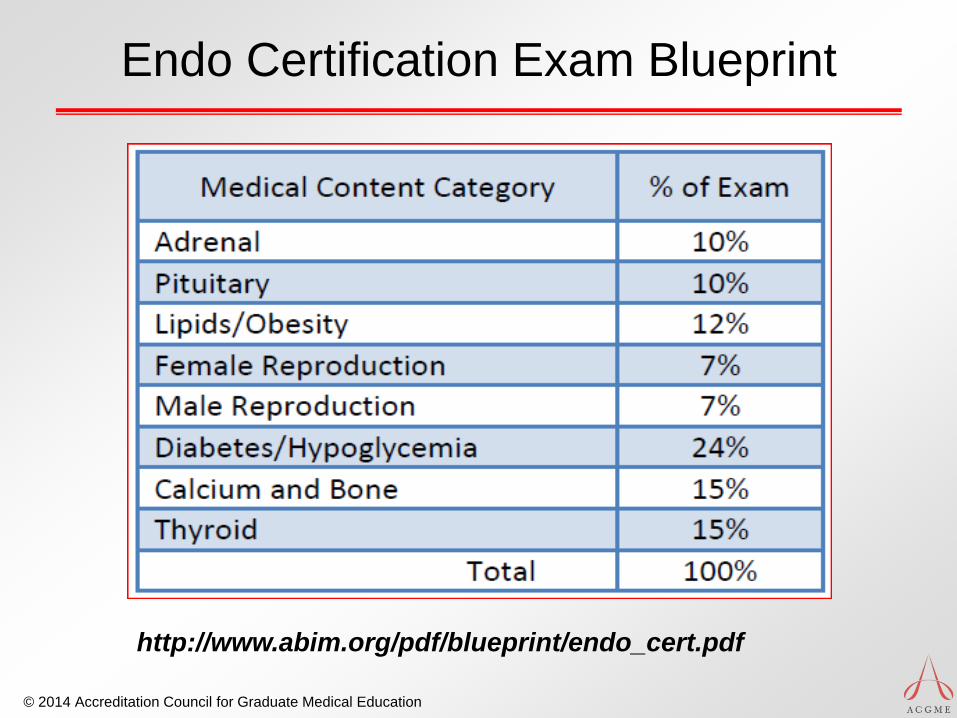
Endo Certification Exam Blueprint
http://www.abim.org/pdf/blueprint/endo_cert.pdf
© 2014 Accreditation Council for Graduate Medical Education
What About Patients?
© 2014 Accreditation Council for Graduate Medical Education
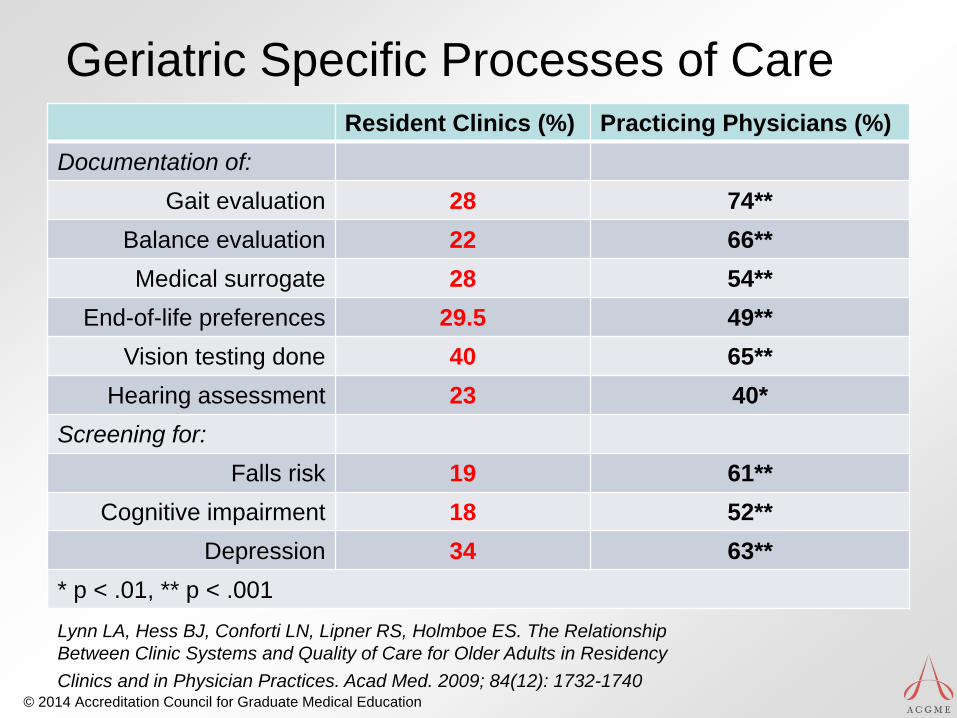
Geriatric Specific Processes of Care Resident Clinics (%) Practicing Physicians (%)
Documentation of: Gait evaluation 28 74**
Balance evaluation 22 66** Medical surrogate 28 54**
End-of-life preferences 29.5 49** Vision testing done 40 65**
Hearing assessment 23 40* Screening for:
Falls risk 19 61** Cognitive impairment 18 52**
Depression 34 63** * p < .01, ** p < .001 Lynn LA, Hess BJ, Conforti LN, Lipner RS, Holmboe ES. The Relationship Between Clinic Systems and Quality of Care for Older Adults in Residency Clinics and in Physician Practices. Acad Med. 2009; 84(12): 1732-1740
© 2014 Accreditation Council for Graduate Medical Education
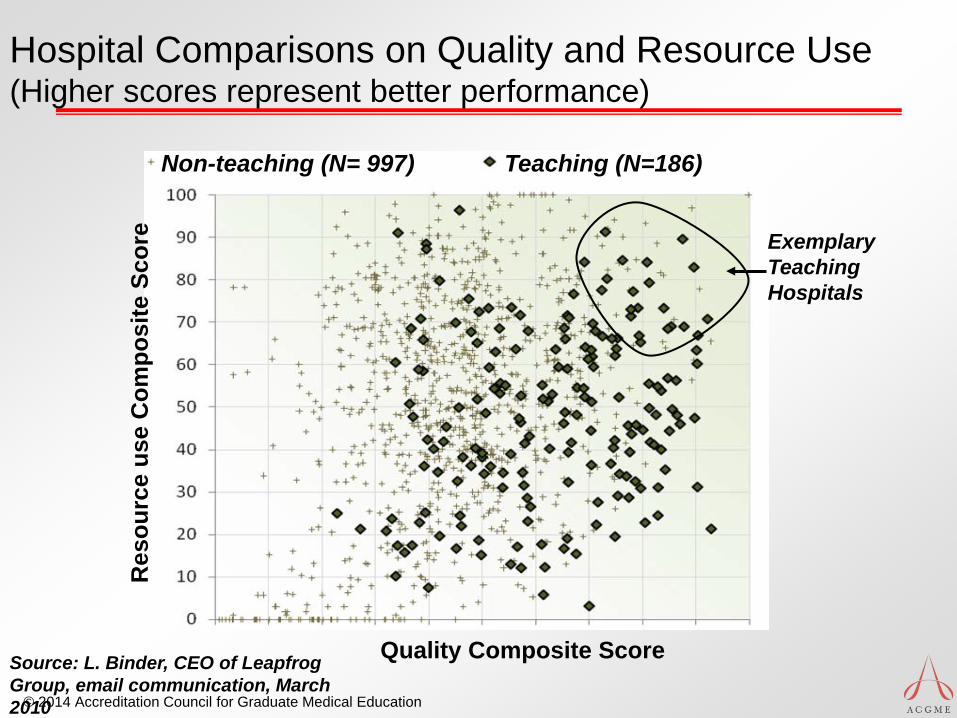
Hospital Comparisons on Quality and Resource Use (Higher scores represent better performance)
Non-teaching (N= 997) Teaching (N=186)
Quality Composite Score
Res
ourc
e us
e C
ompo
site
Sco
re
Exemplary Teaching Hospitals
Source: L. Binder, CEO of Leapfrog Group, email communication, March 2010
© 2014 Accreditation Council for Graduate Medical Education
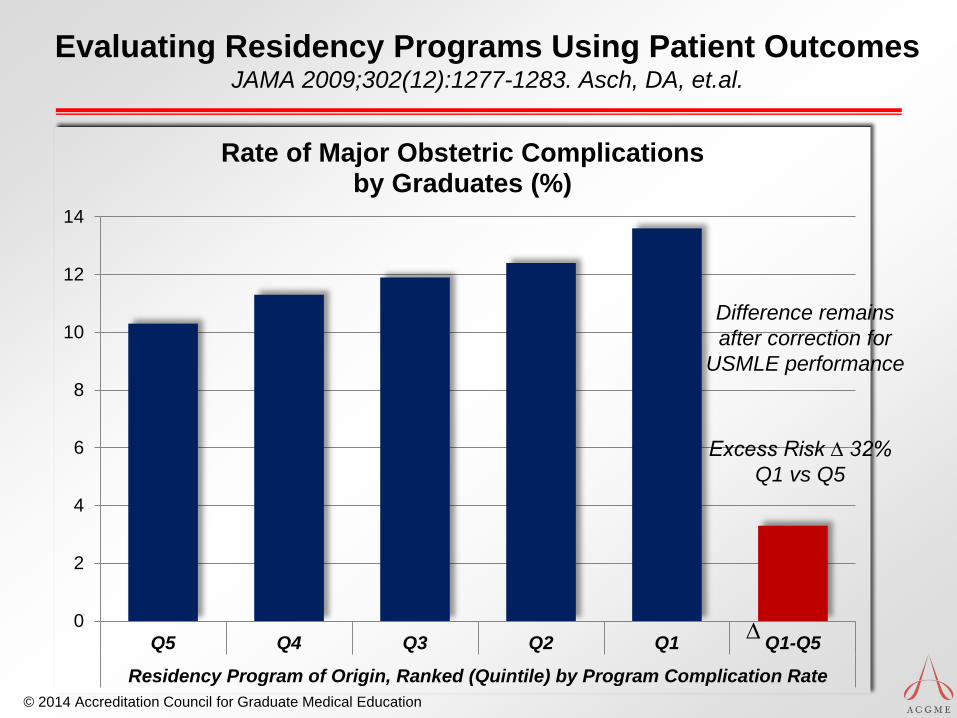
Evaluating Residency Programs Using Patient Outcomes JAMA 2009;302(12):1277-1283. Asch, DA, et.al.
0
2
4
6
8
10
12
14
Q5 Q4 Q3 Q2 Q1 Q1-Q5
Residency Program of Origin, Ranked (Quintile) by Program Complication Rate
Rate of Major Obstetric Complications by Graduates (%)
∆
Difference remains after correction for
USMLE performance
Excess Risk ∆ 32% Q1 vs Q5
© 2014 Accreditation Council for Graduate Medical Education
Office-based Practice Competencies • Inter-Professional team skills • Clinical IT Meaningful Use skills • Population management skills • Reflective practice and CQI skills
• Care Coordination • Continuity of Care • Leadership and management skills • Systems thinking • Procedural Skills
Individual Physician Readiness: Gaps
Crosson Health Affairs 2011
© 2014 Accreditation Council for Graduate Medical Education
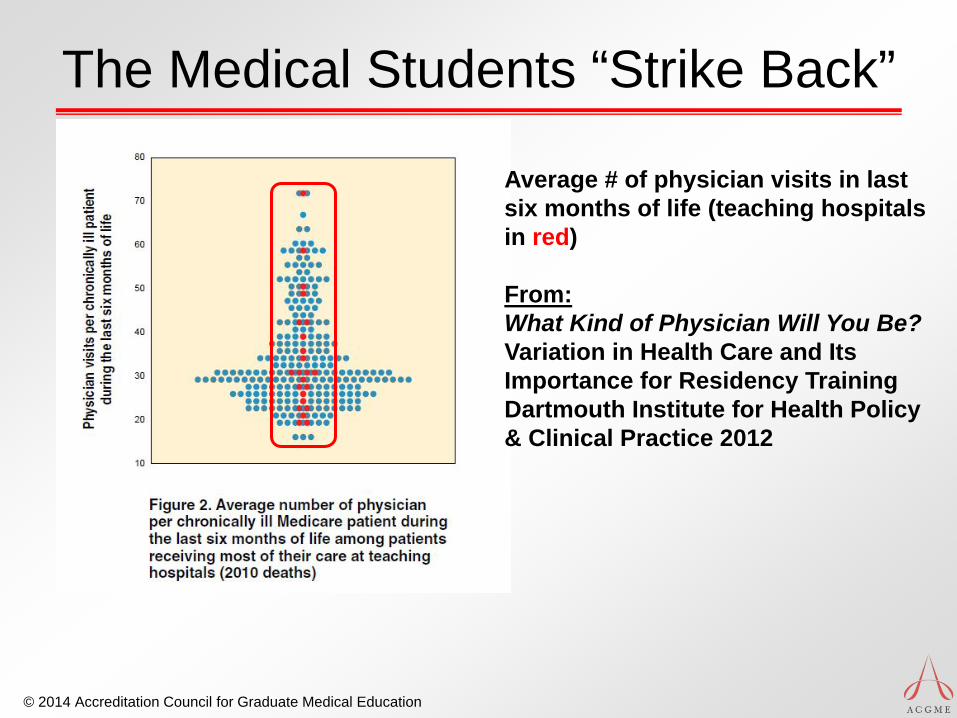
The Medical Students “Strike Back”
Average # of physician visits in last six months of life (teaching hospitals in red) From: What Kind of Physician Will You Be? Variation in Health Care and Its Importance for Residency Training Dartmouth Institute for Health Policy & Clinical Practice 2012
© 2014 Accreditation Council for Graduate Medical Education
How well do you understand the quality and safety of endocrinologic care or related care delivered in your
institution?
Where is Endocrinology today?
© 2014 Accreditation Council for Graduate Medical Education
“Every system is perfectly designed to achieve the results it gets.”
Paul Batalden
© 2014 Accreditation Council for Graduate Medical Education
Where We Are Trying to Go
Competency-based Medical Education
© 2014 Accreditation Council for Graduate Medical Education
Educating Physicians1
• “Can medical education’s illustrious past serve as an adequate guide to a future of excellence? Flexner asserted that scientific inquiry and discovery, not past traditions and practices, should point the way to the future in both medicine and medical education…”
1Cooke M, Irby DM and O’Brien BC. Educating Physicians. 2010.
© 2014 Accreditation Council for Graduate Medical Education
Educating Physicians • “…Medical training is inflexible, excessively long,
and not learner-centered. We found that clinical education is overly focused on inpatient clinical experience, supervised by clinical faculty who have less and less time to teach and who have ceded much of their teaching responsibilities to residents, and situated in hospitals with marginal capacity to support their teaching mission.”
© 2014 Accreditation Council for Graduate Medical Education
Carnegie: Reforms Recommended
• Standardize learning outcomes • Individualize learning while allowing flexibility and
the opportunity to progress as learners achieve competency milestones
• Establish rigorous and progressively higher levels of competency across the continuum of medical education
• Develop a coherent framework for the continuum of medical education and establish effective mechanisms to coordinate standards Carnegie Foundation: Acad Med, Vol. 85 (2) 2010
© 2014 Accreditation Council for Graduate Medical Education
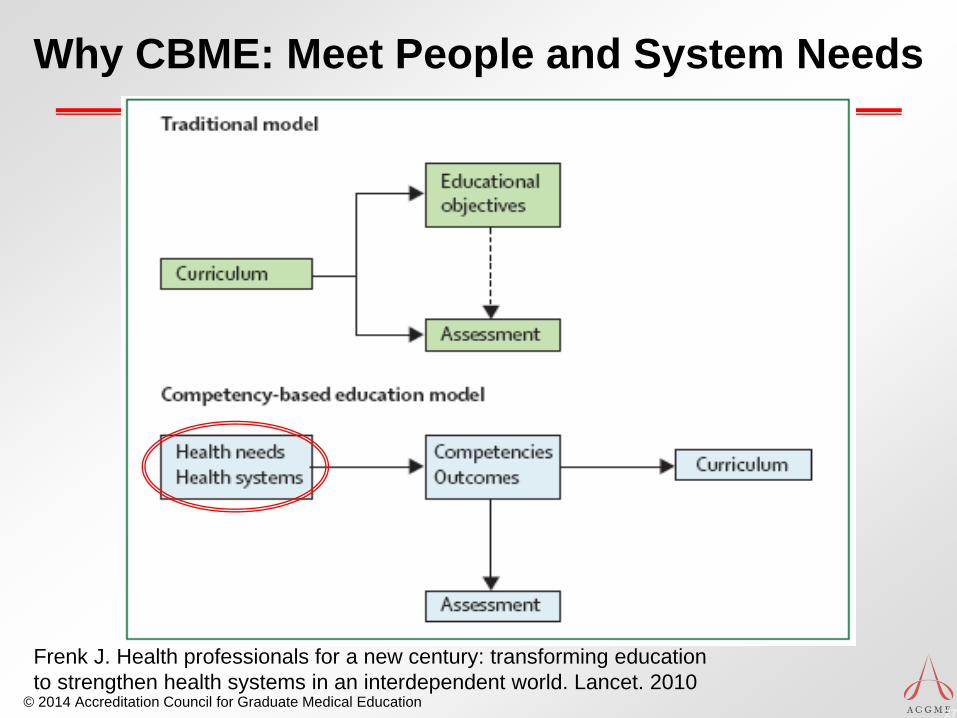
Why CBME: Meet People and System Needs
27
Frenk J. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010
© 2014 Accreditation Council for Graduate Medical Education
Early Principles: CBME
• World Health Organization (1978): • “The intended output of a competency-
based programme is a health professional who can practise medicine at a defined level of proficiency, in accord with local conditions, to meet local needs.”
McGaghie WC, Miller GE, Sajid AW, Telder TV. Competency-based Curriculum Development in Medical Education. World Health Organization, Switzerland, 1978.
© 2014 Accreditation Council for Graduate Medical Education
When I say “Milestone”…
…What first comes to mind?
© 2014 Accreditation Council for Graduate Medical Education
What Are Milestones for GME? • Elements of Resident Performance (Work Place)
• described as important by the literature and/or expert opinion
• Behaviorally Described in a Developmental Framework
• (Describe Aspirational Goals)
• Are a Subset of the elements of the Six Domains of Clinical Competency • designed to be markers of progress
• Are a potential framework for evaluation of progress along the continuum
• A tool to introduce new elements of the Competencies
© 2014 Accreditation Council for Graduate Medical Education
Entrustable Professional Activities
• EPAs represent the routine professional-life activities of physicians based on their specialty and subspecialty
• The concept of “entrustable” means: • ‘‘a practitioner has demonstrated the necessary
knowledge, skills and attitudes to be trusted to perform this activity [unsupervised].’’1
1Ten Cate O, Scheele F. Competency-based postgraduate training: can we bridge the gap between theory and
clinical practice? Acad Med. 2007; 82(6):542–547.
© 2014 Accreditation Council for Graduate Medical Education
An Entrustable Professional Activity • Part of essential work for a qualified professional • Requires specific knowledge, skill, attitude • Acquired through training • Leads to recognized output • Observable and measureable, leading to a
conclusion • Reflects the competencies expected
• EPA’s together constitute the core of the profession
ten Cate et al. Acad Med 2007
© 2014 Accreditation Council for Graduate Medical Education
Milestones and EPAs as Roadmap
Observations:
1) Journey not a straight line
2) More than one path (but not infinite paths)
3) “If you don’t know where you are going, any road will get you there”
© 2014 Accreditation Council for Graduate Medical Education
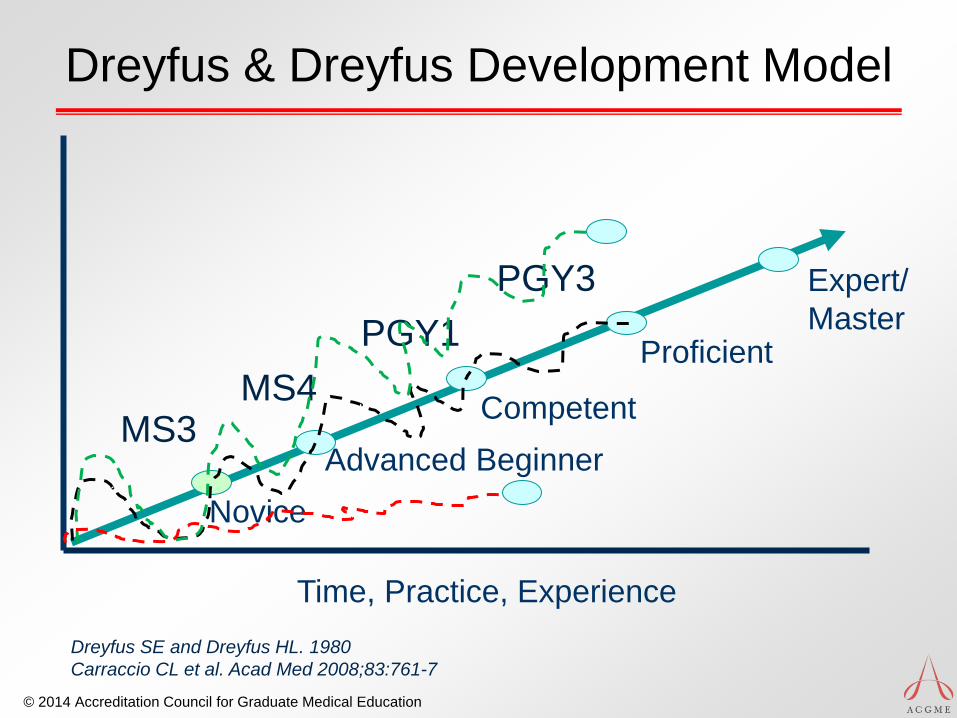
Dreyfus & Dreyfus Development Model
Dreyfus SE and Dreyfus HL. 1980 Carraccio CL et al. Acad Med 2008;83:761-7
Time, Practice, Experience
Novice Advanced Beginner
Competent
Proficient
Expert/ Master
MS3 MS4
PGY1 PGY3
© 2014 Accreditation Council for Graduate Medical Education
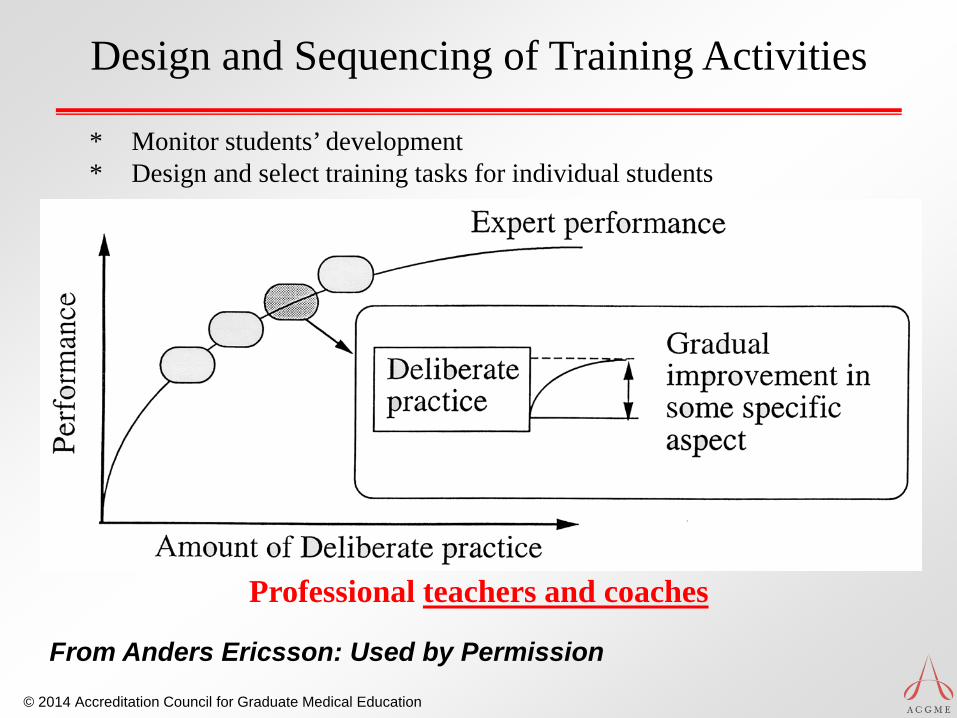
Design and Sequencing of Training Activities
Professional teachers and coaches
* Monitor students’ development * Design and select training tasks for individual students
From Anders Ericsson: Used by Permission
© 2014 Accreditation Council for Graduate Medical Education
Self Assessment Conundrum
Individually generated summary judgment of one’s skill level
Inaccurate Poor performers overestimate Outstanding performers underestimate
Davis D et al. JAMA 2006; 296:1094-1102 Eva KW et al. Acad Med. 2005;80:S46-54
© 2014 Accreditation Council for Graduate Medical Education
Boud and Molloy (2013)
“Feedback is seen not only as having influence on immediate tasks but of building students’ capability for making judgments about their subsequent work.” • Key concept: Think of feedback as part of
a series of PDSA/Kolb learning cycles
Boud D and Molloy E. Feedback in Higher and Professional Education. Routledge 2013.

© 2014 Accreditation Council for Graduate Medical Education
What is Needed to Realize the Promise
© 2014 Accreditation Council for Graduate Medical Education
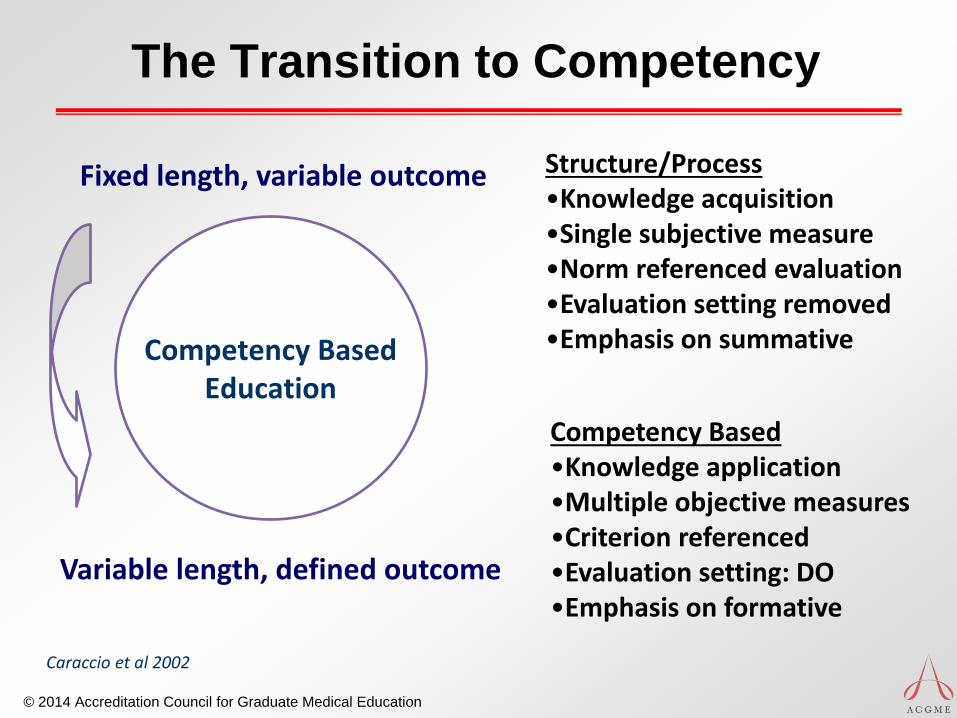
Competency Based Education
Fixed length, variable outcome
Variable length, defined outcome
Structure/Process •Knowledge acquisition •Single subjective measure •Norm referenced evaluation •Evaluation setting removed •Emphasis on summative
Competency Based •Knowledge application •Multiple objective measures •Criterion referenced •Evaluation setting: DO •Emphasis on formative
Caraccio et al 2002
The Transition to Competency
© 2014 Accreditation Council for Graduate Medical Education
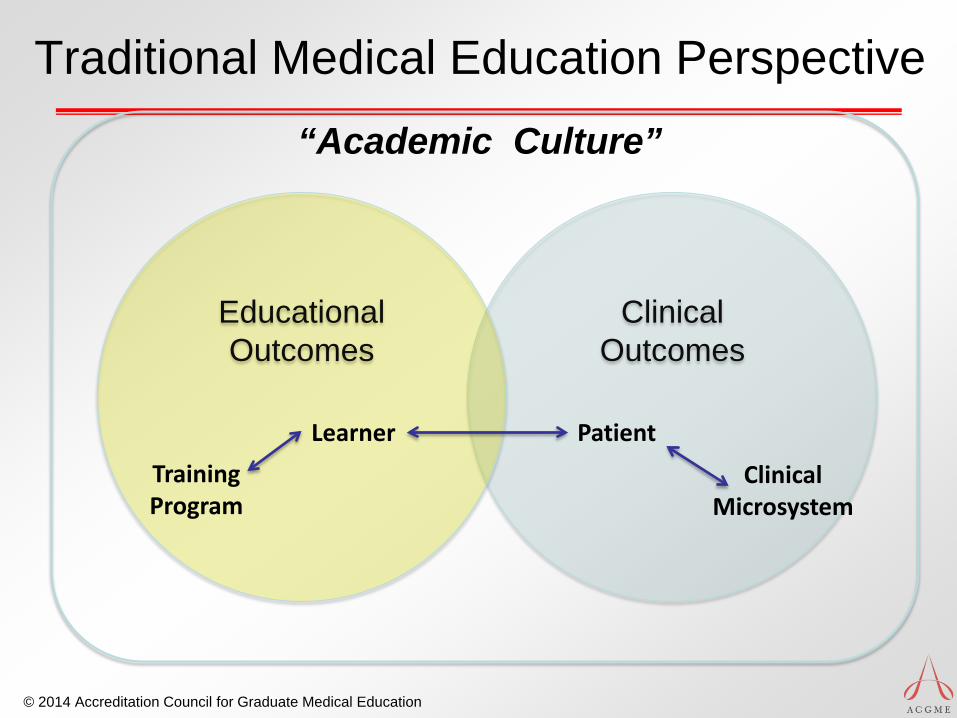
Clinical Outcomes
Educational Outcomes
Learner Patient
Clinical Microsystem
Training Program
Traditional Medical Education Perspective
“Academic Culture”
© 2014 Accreditation Council for Graduate Medical Education
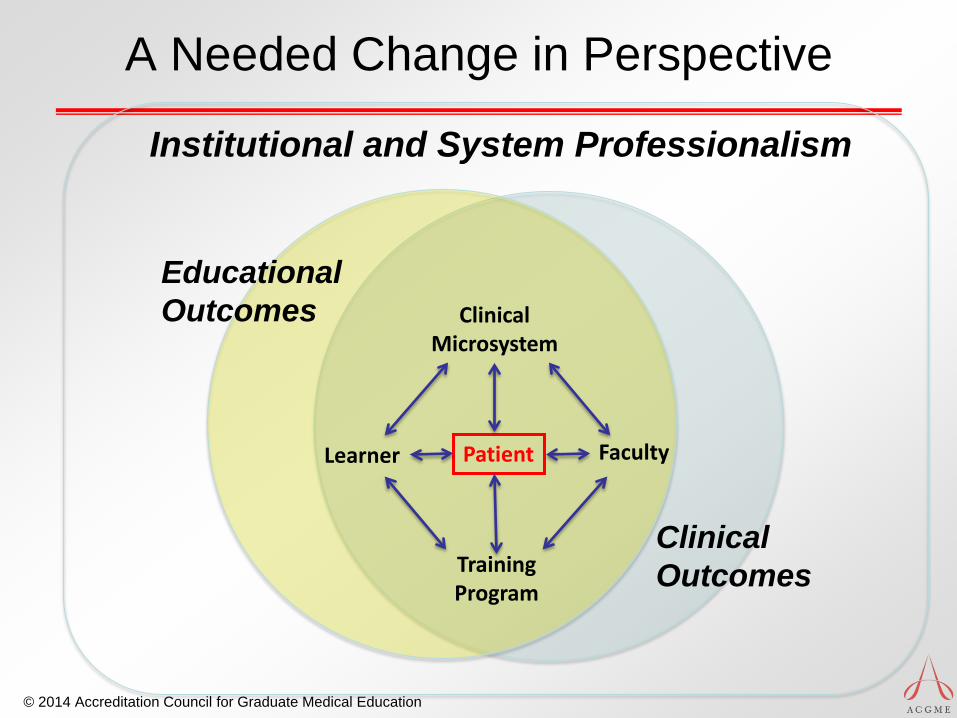
Learner Patient
Clinical Microsystem
Training Program
A Needed Change in Perspective
Faculty
Institutional and System Professionalism
Educational Outcomes
Clinical Outcomes
© 2014 Accreditation Council for Graduate Medical Education
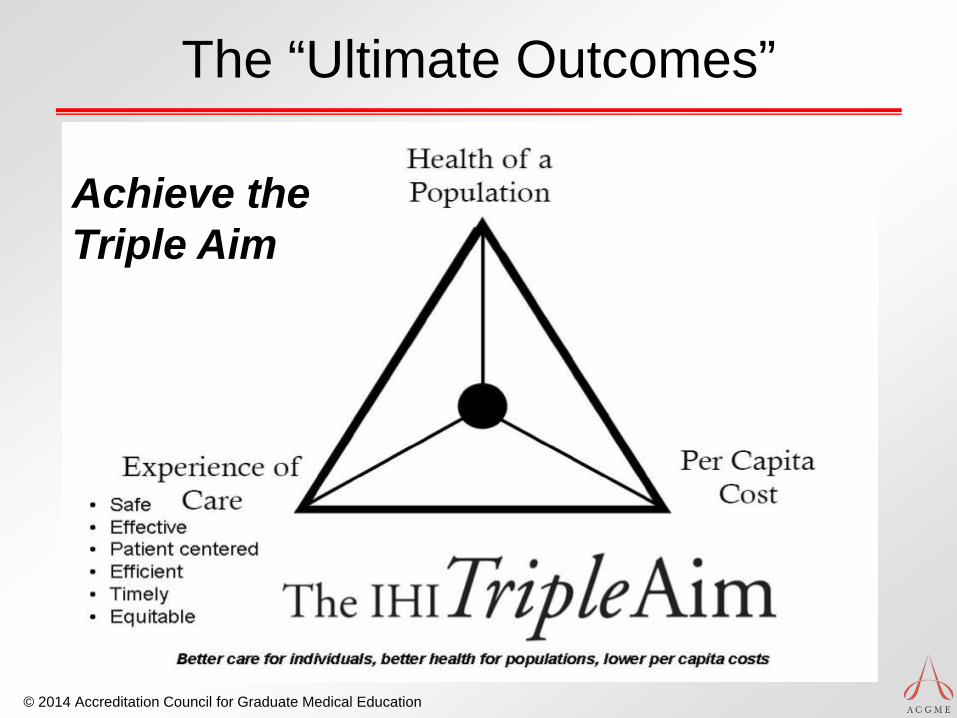
The “Ultimate Outcomes”
• A competent (at a minimum) practitioner aligned with:
CMS Triple Aim
Achieve the Triple Aim
© 2014 Accreditation Council for Graduate Medical Education
Observation and Safe Patient Care
Importance of appropriate supervision Entrustment
Trainee performance* X Appropriate level of supervision**
Must = Safe, effective patient-centered care
* a function of level of competence in context **a function of attending competence in context
Kogan JR, Conforti LN, Iobst WF, Holmboe ES. Reconceptualizing variable rater assessments as both an educational and clinical care problem. Acad Med. 2014; 89(5):721-7

© 2014 Accreditation Council for Graduate Medical Education
Effective Professional Development: Must Align Curriculum with Assessment
Dreyfus SE and Dreyfus HL. 1980 Carraccio CL et al. Acad Med 2008;83:761-7
Time, Practice, Experience
Novice Advanced Beginner
Competent
Proficient
Expert/ Master
MILESTONES Curriculum
Assessment
Curriculum
Assessment
Curriculum
Assessment
Curriculum
Assessment
Curriculum
Assessment
© 2014 Accreditation Council for Graduate Medical Education
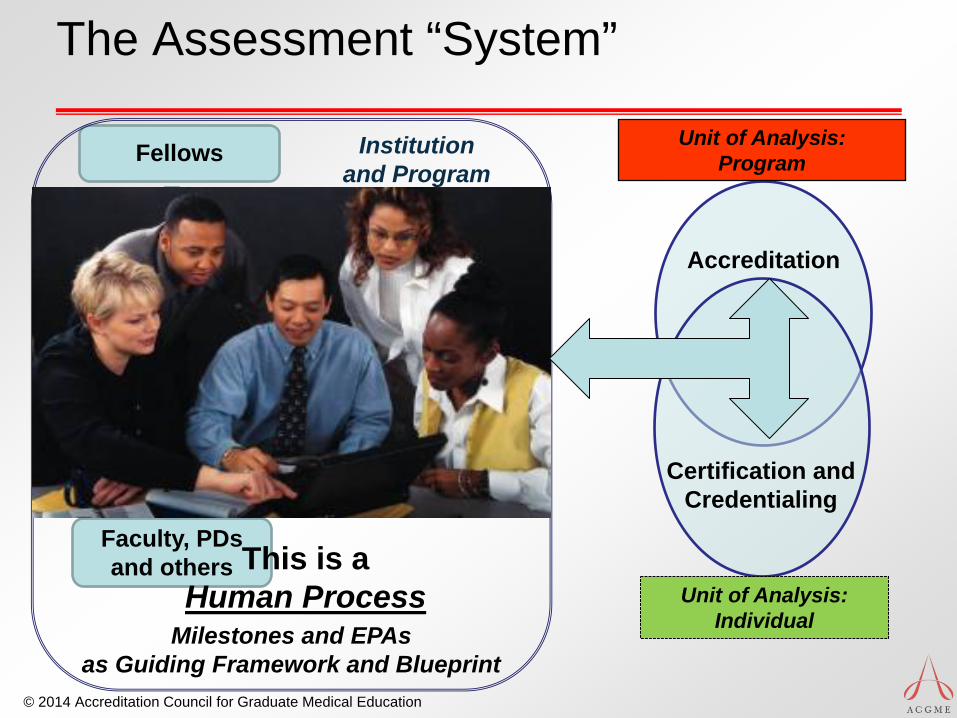
The Assessment “System”
Assessments within Program:
• Direct observations • Audit and
performance data • Multi-source FB
• Simulation • ITExam
Judgment and Synthesis: Committee
Fellows
Faculty, PDs and others
Milestones and EPAs as Guiding Framework and Blueprint
Accreditation
Unit of Analysis: Program
Certification and Credentialing
Unit of Analysis: Individual
Institution and Program
This is a Human Process
© 2014 Accreditation Council for Graduate Medical Education
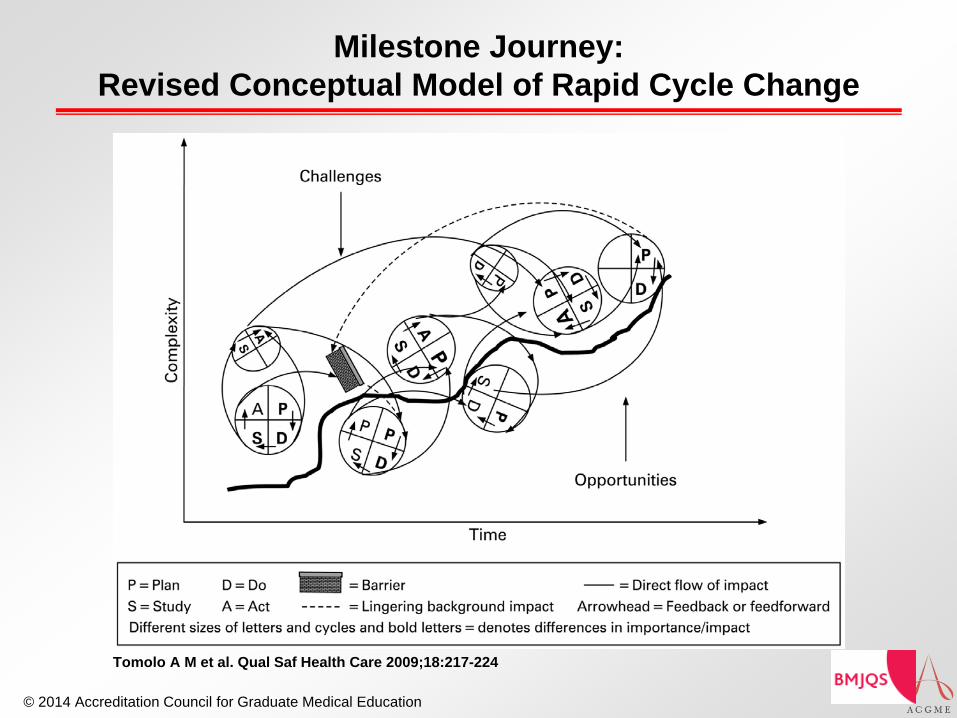
Milestone Journey: Revised Conceptual Model of Rapid Cycle Change
Tomolo A M et al. Qual Saf Health Care 2009;18:217-224
© 2014 Accreditation Council for Graduate Medical Education
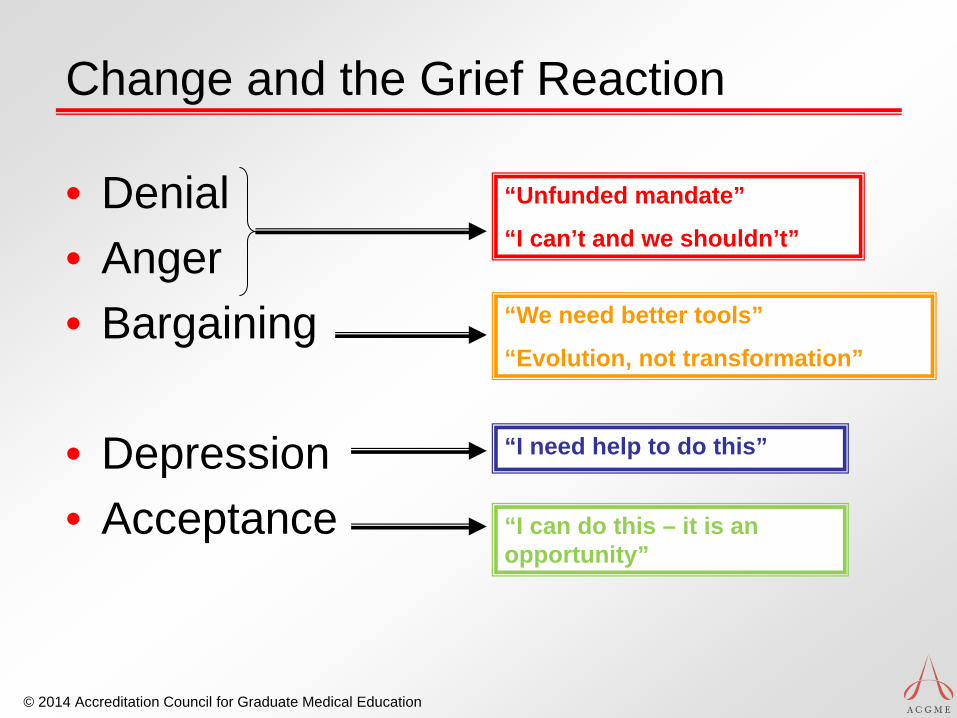
Change and the Grief Reaction
• Denial • Anger • Bargaining
• Depression • Acceptance
“Unfunded mandate”
“I can’t and we shouldn’t”
“We need better tools”
“Evolution, not transformation”
“I need help to do this”
“I can do this – it is an opportunity”