Embed Size (px)
Citation preview
Anju Malhotra
Laura Nyblade
Sulabha Parasuraman
Kerry MacQuarrie
Namita Kashyap
Sunayana Walia
Realizing ReproductiveChoice and Rights
Abortion andContraception in India
Copyright© 2003 International Center for Research on Women
Design: Manu Badlani
Anju Malhotra
Laura Nyblade
Sulabha Parasuraman
Kerry MacQuarrie
Namita Kashyap
Sunayana Walia
Realizing ReproductiveChoice and RightsAbortion andContraception in India
DedicationWe dedicate this report to all the women in Madhya Pradesh who so willingly shared their lives with us.
Research Team MembersInternational Center for Research on WomenDr. Anju MalhotraDr. Laura NybladeMs. Sunayana WaliaMs. Kerry MacQuarrie
International Institute for Population SciencesDr. Sulabha ParasuramanDr. Rajiv PrasadMs. Namita Kashyap
Government Medical College, NagpurDr. Chhaya SarodeyDr. Shuchita MundleMr. Suresh Ughade
Dr. Ravi Verma (formerly at IIPS; currently at Population Council)
AcknowledgementsThis study and report were made possible by the hard work, dedication, and input from numerousindividuals over the past three years.
We would like to thank the Clinical Epidemiology Unit at Government Medical College, Nagpur, forundertaking the dual challenge of bridging medical and social science research and conducting fieldwork forthe difficult initial phase of this study. In particular, support from Dr. Deepti Jain was critical in setting upand sustaining the study. Ms. Jyoti Nagarkar from YUVA provided training assistance for the first phase. Forthe main study, we are grateful to the International Institute for Population Studies (IIPS) and its director,Dr. Roy, for institutional and technical partnership. The team at IIPS was the backbone of the study and hasensured that these important data were collected and entered, often under difficult circumstances.
Most of all, we would like to thank the field team members who spent many months in the heat and thecold and often uncomfortable living conditions to collect and collate data from both near and remotesites in Madhya Pradesh: Ranjana Lal, Archana Ukude, Vijaya Gadkari, Shilpa Washimkar, ShilaSontake, Pranita Wagh, Firdoaus Jahan, Ashwini Yelkar, Veena Dalvi, Rashmi Soni, Rekha Deshmukh,Bharti Kashyap, Rekha Nigam, Reena L Pal, Nidhi Namdeo, Nutan Patil, Vaishali Bhoyae, ChetanaKhare, Rajitram Verma, R. C. Verma, Rajendra Verma, Rakesh Tripathy, S. V. Chindarkar, ShubhangiMore, Parasnath Verma, S. B. Nalavade, B. S. Badve, Kamlesh Mayekar, Ghanshyam Verma, andSandeep Mungekar.
We thank our professional colleagues who offered critical comments and feedback throughout the study, inparticular Bela Ganatra and Heidi Johnston. We would also like to thank the following ICRW staffmembers for their support and input: Anuradha Rajan, Nandita Bhatla, T. Venugopal, Amanda Bartelme,Monica Agarwal, Kathleen Barnett, Margo Young, Carole Mahoney, and Cheryl Morden.
Finally, we would like to thank the David and Lucile Packard Foundation for providing the financial supportfor this study.
Executive Summary .................................................................................. 5
I. Introduction .............................................................................................. 7Addressing Rights and Choice Internationally ........................................................................ 7The Indian Context ................................................................................................................... 8
II. Innovating a New Methodology .............................................................. 11The Need for a Better Methodology ...................................................................................... 11A New Approach .................................................................................................................... 12
1. Modifying the basic nature and structure of the survey instrument ........................... 122. Building flexibility into the interviewing process ....................................................... 133. Blending input from social science and medicine ...................................................... 13
The Initial Qualitative Phase .................................................................................................. 13The Pilot Survey Phase .......................................................................................................... 14The Full Scale Survey Phase .................................................................................................. 14
Sampling ......................................................................................................................... 15Survey instrument ........................................................................................................... 15Data structure ................................................................................................................. 16
III. Abortion Prevalence, Demand, and Perceptions .....................................17Abortion Prevalence ............................................................................................................... 17Demand for Abortion ............................................................................................................. 18Perceptions Regarding Abortion ............................................................................................ 19
Knowledge of legality ..................................................................................................... 19Social and cultural perceptions ...................................................................................... 19
IV. Contraceptive Use, Unwanted Pregnancies, and Abortion .....................21
V. The Abortion Experience from Women’s Perspectives ...........................24Reasons for Attempted Abortions .......................................................................................... 24Methods, Providers, Access, and Costs .................................................................................. 24Role of the Family .................................................................................................................. 26Health and Family Planning ................................................................................................... 27Sex Selective Abortions ......................................................................................................... 28
VI. Conclusions and Recommendations ........................................................30
References................................................................................................34
Table of Contents

4
Realizing Reproductive Choice and Rights
Figure 3.1 Percent of women who ever had, attempted, or wanted an abortion ........................... 17
Figure 3.2 Abortion ratio in Madhya Pradesh (ICRW and NFHS-2 data comparison) ................. 18
Figure 3.3 Met and unmet demand for abortion ............................................................................ 18
Figure 3.4 Percent of women who ever had an abortion (by rural/urban, education,and socioeconomic status) ............................................................................................................. 19
Figure 3.5 Women’s perceptions of ease of accessing abortion services ...................................... 19
Figure 3.6 Knowledge of abortion legality.................................................................................... 19
Figure 3.7 Approval of abortion (by reason) ................................................................................. 20
Figure 4.1 Women’s desires on childbearing preceding any given pregnancy.............................. 21
Figure 4.2 Contraceptive use in intervals where women wanted to preventor delay pregnancy......................................................................................................................... 22
Figure 4.3 Contraceptive use in intervals preceding attempted abortions .................................... 22
Figure 5.1 Reasons for attempting abortion .................................................................................. 24
Figure 5.2 Methods used for abortion (self-reported by women) ................................................. 25
Figure 5.3 Convenience of access to abortion provider ................................................................ 25
Figure 5.4 Provider fees for abortion (in rupees) .......................................................................... 26
Figure 5.5 Success rate of attempted abortion by whether or not someoneaccompanied the respondent .......................................................................................................... 26
Figure 5.6 Self-reported morbidity from successful and unsuccessful abortion attempts ............ 27
Figure 5.7 Post-abortion family planning advice .......................................................................... 27
Table 5.1 Pregnancy outcomes by status on sex determination test (urban and rural) .................. 28
Figures and Tables
5
International Center for Research on Women
Women’s control over their own child-bearing is a key component of repro-
ductive rights as defined by the Cairo agenda.To the extent that the de facto interpretation ofreproductive rights and choice has come to beidentified with the legal right to abortion,policy and advocacy efforts have failed toaddress the full range of factors that arecritical in defining women’s options regardingchildbearing in poor countries. For women indeveloping countries, abortion is often achoice that is derived from a lack of alterna-tives: the extent to which they resort to unsafeor safe abortions is fundamentally determinedby the realistic options they have for prevent-ing unwanted pregnancies in the first place. Ifreproductive rights are to be realized forwomen in developing countries, therefore, it isimportant to ensure that women’s basic needfor access to appropriate contraceptive optionsis addressed along with the need for safeabortion.
The International Center for Research onWomen designed and implemented an innova-tive, large-scale, household-based study inIndia in order to better understand the inter-relationships of contraceptive options andabortion prevalence for women in developingcountries. This study explores the domestic,societal, service-related, and policy-relatedcontext of the occurrence and resolution ofunwanted pregnancies among a sample ofapproximately 2400 women. It was conductedfrom 1999-2002 in the state of MadhyaPradesh, in partnership with the InternationalInstitute for Population Studies, Mumbai and
the Government Medical College, Nagpur.The central questions motivating the researchwere:
! How are women’s reproductive rights andchoice manifested in the decision-makingprocesses that determine contraceptiveuse, the occurrence of unwanted pregnan-cies, and the resolution of unwantedpregnancies?
! Under what circumstances are the actionsthat women take—or fail to take—indica-tive of their ability to formulate and actupon reproductive choices?
The study shows that the vast majority ofIndian women have limited reproductive rightsand choices despite the fact that abortion hasbeen legal in India through the MedicalTermination of Pregnancy (MTP) Act, passedin 1972. In India, the lack of safe, effective,accessible temporary methods of contracep-tion is as much a barrier to the realization ofreproductive rights and choice for women asthe ineffective and poor implementation of theabortion law.
Findings from the study show that abortionrates in Madhya Pradesh, India are consider-able, with almost one-fourth of currentlymarried women 15-39 experiencing at leastone abortion by their late thirties. Demand forabortion is even higher and failure rates atattempted abortions are substantial. Women’sknowledge of their legal right to abortion, atless than 10%, is abysmal. Despite the provi-sions of the MTP Act, women incur significant
Executive Summary
6
Realizing Reproductive Choice and Rights
financial costs and exert much effort to get anabortion. Rural, poor, and marginalizedwomen are especially disadvantaged in accessto adequate and safe abortion services. Themajority of abortions in rural areas werethrough dubious and potentially dangerousmeans, and self-reported morbidity fromabortion attempts is high.
Women’s limited mobility and decision-making power also means that influentialfamily members play a significant role inwomen’s ability to get abortions.
The data from the study also point to theunequivocal link between contraceptive accessand abortion. Despite the fact that demand forspacing methods is very high, contraceptiveuse among women in Madhya Pradesh is verylow, and mostly accounted for by sterilization.Women used temporary methods of contracep-tion in only 8% of the intervals where theyhad wanted to space their childbearing. Themost important reasons for non-use are lack ofinformation and access and opposition fromthe family.
The rate of contraceptive use was nearly thesame for women who attempted abortions andthose who did not. Yet, many women whoattempt abortions are pioneers in that they aremaking a concerted effort to use temporarymethods of contraception in an environmentwhere sterilization is the norm. Amongwomen who did try temporary methods andthen resorted to abortion, 75% had eitherdiscontinued due to health concerns or experi-enced method failure. The current system isfailing women at more than one level. Overthree-quarters of the women who had anabortion did not get follow-up advice oncontraception from a medical provider.
The most significant policy message emergingfrom the findings of this study is clear:Temporary methods of contraception must bemade a viable option for Indian women. Therhetoric for informed choice must be trans-lated into a serious, committed, and energizedeffort to provide women safe and effectiveforms of temporary contraception. This effort
requires addressing not only the supply sidefactors of service provision, but also thedemand side factors of women’s perceptions,knowledge, health concerns, and familyconstraints. This approach is also necessaryfor restructuring abortion services. Misinfor-mation, poor knowledge, limited decision-making ability, and poor health consequencesare currently a significant part of women’sexperience with abortion.
Government providers of abortion servicesneed to be more plentiful, better trained, andbetter equipped, especially in rural areas.Since the vast majority of abortions arecurrently provided through the private sector,the role of the private sector must be acknowl-edged and adequately addressed. A campaignto inform and educate women, their families,and service providers regarding the legal rightto abortion must be a first step in ensuring theenactment of this right. Additionally, the MTPAct itself requires revision to make it moretransparent and easily implemented.
Perhaps the most significant contribution ofour work is in highlighting the extent to whichcontraceptive use (or non-use) and abortionare interconnected. In women’s lives, thesetwo issues do not exist independently of eachother, and their separation in the healthinfrastructure does not serve women well. Ourfindings demonstrate that in order to realizereproductive rights and choice for women inthe developing world, it is essential to con-sider issues beyond the legalization of abor-tion. While most (although not all) women inthe Western world may consider basic accessto effective contraception a given, this is yet tobe the case in many countries of the develop-ing world, India being an important case inpoint. Similarly, the passage of a law legaliz-ing abortion is a necessary, but not a sufficientcondition for ensuring access to safe andeffective abortion services. It is equallyimportant to ensure that women are apprisedof their legal rights, service provision reachesa significant majority of women, and social,gender-based, and health-related barriers toaccessing services are addressed adequately.
7
International Center for Research on Women
IntroductionIrealistic options they have for preventingunwanted pregnancies in the first place. Ifreproductive rights are to be realized forwomen in developing countries, therefore, it isimportant to ensure that women’s basic needfor access to appropriate contraceptive optionsis addressed along with the need for safeabortion.
An important reason why the connectionbetween abortion and contraception forwomen in developing countries has not beenaddressed adequately is because it is poorlyunderstood. Although large scale surveys suchas the Demographic and Health Surveys(DHS) have provided valuable data on ratesand trends in contraceptive use across anumber of countries, they provide only limitedinformation on factors underlying women’sreproductive behavior, such as motivations forchildbearing, decision-making processesregarding contraception or abortion, orbarriers to accessing services. They also donot provide reliable data on abortion preva-lence. Thus far, depth of knowledge regardingreproductive choices and behavior fromwomen’s own perspective has come mostlyfrom small scale, community-based, qualita-tive studies; yet, these are difficult to general-ize. Higher quality, large-scale survey data onthese issues are essential, not only for betterestimating the number of women who arepracticing abortion, but also for adequatelyunderstanding the context in which womenmake contraceptive choices, experienceunwanted pregnancies, and resort to abortion.
Addressing Rights and ChoiceInternationallyIn the last decade, national and internationalstakeholders have struggled to operationalizewomen’s empowerment, rights, and choice, asarticulated in the Cairo agenda. This has notbeen an easy task, given the difficulties inreshaping health and family planning systems,social and economic conditions, and policyaction to more adequately reflect women’sneeds. For women in developing countries,moreover, the progress on rights has beenconstrained by the de facto identification ofreproductive rights with the legal right toabortion. This has meant that programmatic,policy, and advocacy efforts have not alwaysaddressed the full range of factors that arecritical in defining women’s options onreproductive matters in poor countries.
In this work, we argue that women’s controlover their own childbearing is a key compo-nent of reproductive rights as defined by theCairo agenda, and that all effective and safemeans for ensuring this control must be on thepolicy and programmatic agenda. The legalright to abortion is certainly one importantcomponent to ensuring that women are able tocontrol their childbearing destinies. However,large proportions of women in the world lacknot only access to safe abortion, but alsoaccess to safe and effective contraception. Forthese women, abortion is often a choice that isderived from a lack of alternatives: the extentto which they resort to unsafe or safe abor-tions is fundamentally determined by the
8
Realizing Reproductive Choice and Rights
In order to better understand the interrelation-ships of contraceptive options and abortionprevalence for women in developing coun-tries, the International Center for Research onWomen designed and implemented an innova-tive, large-scale, household-based study inIndia. This study explores the domestic,societal, service-related, and policy-relatedcontext of the occurrence and resolution ofunwanted pregnancies among a sample ofapproximately 2400 women. It was conductedfrom 1999-2002 in the state of MadhyaPradesh, in partnership with IIPS, Mumbaiand the Government Medical College, Nagpur.
The central questions motivating theresearch were the following:
! How are women’s reproductive rights andchoice manifested in the decision-makingprocesses that determine a) contraceptiveuse; b) the occurrence of unwanted preg-nancies; and c) the resolution of unwantedpregnancies as either abortion or unwantedbirths?
! Under what circumstances do the actionsthat women take—or fail to take—indicatetheir ability to formulate and act uponreproductive choices?
The primary goal of this study is to provide thedocumentation needed for policy action topromote women’s reproductive health andrights more effectively. In particular, it aims toprovide data to facilitate policy action thatincreases women’s ability to formulate deci-sions regarding the number of children theywant to have; prevent unwanted pregnancies;and attain greater control over the timing andcircumstances of childbearing. The study isalso motivated by the need to implement highquality survey methodologies that are repli-cable in other settings and can effectivelyaddress the sensitive and complex issuesrelated to abortion and the processes of repro-ductive choice more broadly. Without suchinformation, there is sparse documentation toconvince policymakers of the importance ofthese issues or to devise concrete recommenda-tions for policy and programmatic action.
The Indian ContextIn India, the issue of reproductive rights andchoice must be seen in the context of a num-ber of factors. These include the officialpolicies regarding family planning and abor-tion and their implementation; the downwardtrend in family size desires and decliningfertility levels, and their effect on the demandfor contraception and abortion; and the socialand gender-related pressures, constraints, andoptions for women’s reproductive behavior.
In India, the Medical Termination of Preg-nancy (MTP) Act made abortion legal in 1972,and the legality of abortion has not been incontention. Paradoxically, however, the vastmajority of Indian women get abortionsoutside this legal framework. In part, this isdue to the inherent restrictions regardingregistered facilities and doctor consent builtinto the MTP Act, but it is also due to lack ofservices, poor implementation of the Act byproviders, and an even poorer understandingamong women regarding their legal rights(Gupte, Bandewar et al. 1997; Khan, Barge etal. 1999; Bandewar 2001; Johnston 2002).Unlike the U.S. where the exclusive focuswith regard to “choice” has been on thecontinued legalization of abortion, the relevantpolicy debate with regard to abortion in Indiacenters around women’s knowledge of theirlegal rights and the adequate implementationof the MTP Act.
The stated policy and actual implementationof the government family planning programpresent a set of contradictions with regard towomen’s rights and choice in India. SinceICPD 1994, the Indian government hasattempted to move from a longstanding policyof achieving specified targets on contraceptiveuse to greater emphasis on individual need andquality of care, but with uneven and limitedsuccess (Khan and Cernada 1996; Visaria,Jejeebhoy et al. 1999; Donaldson 2002). Forexample, a 1998 analysis of seven statesshows that implementation of the target-freeapproach varies considerably across states,with some states unwilling or unable to
9
International Center for Research on Women
abandon targets (Khan and Townsend 1999;Visaria and Visaria 1999). Similarly, despitethe policy’s stated commitment to principlesof informed choice, service providers often donot practice these principles (Baveja,Buckshee et al. 2000; Ninger 2001; Johnston2002). Data indicate that only in a smallnumber of highly urbanized centers are arange of contraceptive options available toIndian women. In poor, rural areas, contracep-tive supplies at Primary Health Centers andsub-centers are frequently inadequate orlacking altogether (Khan, Patel et al. 1999).Data from the second round of the NationalFamily Health Survey (NFHS-2) indicate thatonly 40% of women remember ever discussingfamily planning with a health worker; only10% had ever discussed the pill and evenfewer had ever discussed other temporarymethods; and only 15% of users of moderncontraceptives were informed about analternative method (IIPS and Macro 2000).
Existing demographic data for India suggestthat unwanted pregnancies may be at highlevels due to declining fertility preferencesand substantial unmet need for contraception.India has experienced declining fertility levelsand desired family sizes throughout the lastdecade. The total fertility rate fell from 3.4 to2.9 between 1992 and 1998, while the meanideal number of children fell from 2.9 to 2.7(IIPS 1995; IIPS and Macro 2000). This trendis accompanied by a rising demand for contra-ception, including spacing methods. However,permanent methods, specifically femalesterilization, continue to predominate, ac-counting for 71% of contraceptive use. In1998, 34% of currently married women weresterilized, but only 7% were using a spacingmethod, levels virtually unchanged since 1992(IIPS 1995; IIPS and Macro 2000).1
The extent to which the unmet need forcontraception results in unwanted pregnanciesand whether these are then resolved throughabortion or become unwanted fertility is aquestion that needs to be answered empiri-cally. In his analysis of the fertility transition
in 20 developing countries, Bongaarts (1997)has argued that during the early and middlephases of the demographic transition fromhigh to low fertility, levels of unwantedfertility are likely to be high as family sizepreferences decline but the means to ensurethem are not fully accessible. He suggests,moreover, that to the extent that contraceptiveuse is not maximized, induced abortion islikely to be the solution for implementingfertility preferences (Bongaarts 1997).
Family and gender-based constraints forwomen in India are also likely to be majordeterminants of unmet need for contraceptionand the practice of abortion. Research onfertility behavior in India indicates thatwomen face a number of social and domesticconstraints that limit their ability to act uponreproductive decisions. These include earlymarriage and the social pressure for earlychildbearing, poor access to knowledgeregarding contraception, lack of decision-making power in the household, limitedphysical mobility and access to services andproviders, and physical violence and coercionin sexual and family relations (Yinger 1998;Jejeebhoy 2000).
The continued strength of son preference inIndia is also well-documented (Arnold 1997;Arnold, Choe et al. 1998; Pande and Astone2001; Arnold, Kishor et al. 2002). Abortionfor sex selection in India receives a lot ofpublic attention, but it is not well-known whatpercentage of abortions are motivated by adesire for sons (Khanna 1997). Such data arenecessary because policy action required toaddress sex selection as a key motivator ofabortion is fundamentally different from thepolicy action necessary to address othermotivating factors for abortion.
The need to differentiate the motivatingfactors for abortion and to more preciselyidentify family and service-related constraintsregarding contraceptive use is especially acutein under-served “BIMARU” (sickly) statessuch as Madhya Pradesh. BIMARU states are
10
Realizing Reproductive Choice and Rights
large, Hindi speaking states within the heart-land of India. They are characterized by hugepopulations, limited infrastructure, and ahistory of underdevelopment. In MadhyaPradesh (MP), a state with 60 million people,fertility levels are relatively high (TFR=3.3per NFHS-2) and contraceptive use continuesto be limited largely to sterilization (37.9%),
with only 4.7% of married women usingtemporary methods (IIPS and Macro 2001).Lack of programmatic investment in the pasthas meant longstanding neglect of women’sreproductive health needs and rights. Address-ing these needs is one of the most criticalissues confronting policy makers and programpersonnel in India.
11
International Center for Research on Women
and review of abortion rates worldwide,Henshaw, Singh, and Haas (1999) state thatIndia is one of four prime areas in the world(along with China, Japan, and the formerSoviet Union) contributing most heavily to theunderreporting of abortion prevalence. Offi-cial records indicate approximately 550,000-600,000 induced abortions per year, yielding arate of about 2.7 per thousand women ofreproductive age, a gross underestimate bymost accounts (Chhabra and Nuna 1996;Henshaw, Singh et al. 1999). This is becausethe vast majority of abortions are performedby private providers who are not registered atMTP centers. Many women go to qualifiedprivate physicians, who are preferred overofficial government centers or clinics but areoutside the official system. Others, however,go to a range of unsafe providers out ofignorance of the law, lack of access, or lack ofmoney (Chhabra and Nuna 1996; Koster-Oyekan 1998; Ganatra, Hirve et al. 2000).
Indirect estimation techniques are often usedto correct the underestimation of poor officialdata on abortion. Estimation techniquestypically rely on records from hospitals andother healthcare facilities on women admittedfor abortion-related complications or deaths.Assumptions are then made on the number ofabortions that are not captured because theyoccur without complications requiring medicalattention, or because women with complica-tions go to non-official facilities for treatment,never access care, or die. For India, estimatesindicate anywhere from 1 million to 7 million
Innovating a New MethodologyIIThe Need for Better MethodologyAlthough the issue of abortion is highlyrelevant in India, it is poorly documented. Inher review of the existing literature on abor-tion in India, Johnston (2002) notes that “novalid data exist on the incidence of abortion inIndia.” Most existing research on abortion inIndia—and elsewhere in the developingworld—is sketchy in terms of confirmingprevalence, while research on motivation andprocesses is even more limited (Jejeebhoy1999; Johnston 2002). This is because for themost part, documentation on abortion islimited to extrapolations from official orprovider-based records. Efforts at collectingprimary data have been largely confined tointerviews with women at clinics servingabortion needs. Household or community-based research on abortion is rare, especiallyusing quantitative methodologies. Thismethodological limitation with the study ofabortion is not confined to India, but isprevalent in the literature on this issue formost developing countries. In a compilationof 22 studies funded by WHO on abortion inthe developing world, 20 were provider-basedand only two were household/community-based (Mundingo and Indriso 1999).
Official records provide estimates of theincidence of abortion based on reporting fromlegal abortion providers, and in most develop-ing countries, they underestimate the trueprevalence of abortion because this informa-tion routinely excludes abortions that occuroutside official settings. In their compilation
12
Realizing Reproductive Choice and Rights
induced abortions per year; the higher numberyields somewhere between 55-60 per thousandwomen of reproductive age, a rate that is 20times higher than the official rate (Chhabraand Nuna 1996; Khan, Barge et al. 1999).Clearly, numbers on the incidence of abortionbased on estimation techniques are roughestimates at best, based on extrapolation andnumerous assumptions (Figa-Talamanca 1989;Alan Guttmacher Institute (AGI) 1999).Moreover, both official and estimated preva-lence data capture little more than the numberof abortions that occur in a given time period.They cannot offer information on process,motivations, or access.
Provider or clinic-based studies attempt tocapture a wider range of factors throughinterviews with or recorded information onwomen who have come in for an abortion,undergone one, or have complications from afailed abortion. Such studies can providesignificant information on the service condi-tions and processes within the clinic setting.However, several researchers have found itdifficult to overcome the sensitivity surround-ing the discussion of abortion when respon-dents were interviewed in healthcare settings.Additionally, provider-based studies sufferfrom a major limitation due to the lack of acontrol or comparison group. By definition,clinic-based studies cannot compare womenwho are not getting an abortion with thosewho are, and therefore, cannot adequatelyexamine the determinants and dynamics ofhow and why women get abortions.
Household-based studies focusing on the issueof abortion are rare, and existing survey datathat include questions on abortion suggest thatmethodologically, the subject matter posessignificant challenges. As abortion is often asensitive and taboo topic, women are reluctantto discuss their experiences in a formalinterview setting. Surveys such as the Demo-graphic and Health Surveys end up providingunrealistically low prevalence rates throughquestions such as “Did you ever have aninduced abortion?” For example, less than
one percent of the women in Madhya Pradeshanswered “yes,” to this question for the IndianNational Family Health Survey in 1993 (IIPS1995).2 Qualitative approaches that allowinterviewers to build rapport with the respon-dents have been utilized to overcome thesensitivity associated with questions onabortion as well as for capturing detail onrelated contextual, process, and motivationalfactors. However, this approach allows foronly small case studies within geographicallylimited areas. Qualitative studies cannotmeasure prevalence, nor can they be general-ized to larger populations.
A New Approach: Methodology forthe StudyGiven existing challenges and gaps, the ICRWteam developed a methodological approachthat blends the best of quantitative and qualita-tive techniques to build a household-levelinstrument that offers the scale, consistency,and widespread applicability of a quantitativesurvey, but also the complexity, depth, andflexibility of the qualitative technique. Thishas meant the alteration of the traditionalsurvey approach in fundamental ways:
1. Modifying the basic nature and structureof the survey instrumentThe major strength of the survey instru-ment we have developed comes from theincorporation of a “narrative” techniquecommonly used in qualitative approachesinto the quantitative survey design. Whilethe questionnaire and the response matrixare structured, information is actuallyelicited through a more fluid and naturalconversational flow rather than close-endedquestions. This technique, which allowswomen to tell the interviewer “the story oftheir life,” overcomes the taboos associatedwith asking abortion-related questionsdirectly since the incidence of abortion, orany attempts at abortion, emerge naturallyin the storytelling process. The narrativealso allows us to cover a wide range ofdetails and decision-making processes in a
13
International Center for Research on Women
woman’s reproductive history, thus provid-ing a wealth of information for a moresophisticated analysis covering not just oneabortion incident, but the entire reproduc-tive life course.
Additionally, the survey instrument wasimplemented over two visits to the respon-dent rather than one, allowing the inter-viewer to build rapport before approachingsensitive topics and to cover a largernumber of questions without tiring therespondent. This structure also allowed usto include multiple related questions on thepractice of abortion, with internal checksfor consistency.
2. Building flexibility into the interviewingprocessIt was also clear that the instrument de-scribed above could not be implemented inthe field through traditional interviewingtechniques. Thus, an equally importantcomponent of the study design was toprovide extensive training to field inter-viewers, allowing them to understand thesubject matter and conceptual issuesintimately and to master the structure of thesurvey instrument. The interviewers hadto develop the confidence in their ability tostrike the right balance between beingflexible in the interview process andmaintaining consistency and rigor inrecording responses. Additionally, inorder to overcome the sensitivity issue, weconsidered it crucial that the interviewingprocess begin with rapport-buildingactivities, not only with the female respon-dents, but also with key community andfamily members, ensuring that the respon-dents would be candid and that important“gatekeepers” to women would be support-ive of the interview process.
3. Blending input from social science andmedicineThe study was designed with scientificinput and review from the social scienceand the medical professions. While the
main goal of the study was to documentwomen’s perceptions and experiencesrather than to document medical practice,we felt that both fields had importantperspectives and knowledge to contributetoward the design of a truly unique andinnovative approach. Thus in addition tothe social science and demographic exper-tise resident at ICRW, our principal part-ners included Ob-Gyns from the Govern-ment Medical College, Nagpur, as well asdemographers and statisticians from theInternational Institute of PopulationScience, Mumbai.3 Additionally, theresearch team vetted the research designwith a number of scientists with specialexpertise on reproductive health in Indiaand professional backgrounds in medicine,public health, sociology, anthropology, anddemography.
Given both the innovation and the riskassociated with our efforts, it was neces-sary to undertake some preliminary explo-ration and testing before launching the fullscale survey. Therefore, data collection inthe study was structured in three phases: 1)an initial qualitative phase; 2) a pilotsurvey phase; and 3) the full scale surveyphase.
The Initial Qualitative PhaseThe initial phase served two functions. First,it allowed us to explore the relevance of arange of important social, family, and indi-vidual determinants of unwanted pregnanciesand their resolution within the context ofMadhya Pradesh, India. We employed focusgroups, key informant interviews, and in-depthinterviews to discover the experiences andattitudes of not only women, but familymembers, community members and serviceproviders as well. Secondly, the in-depthinterviews with women during the qualitativephase utilized the narrative approach with fullflexibility. This confirmed for us that whenthe narrative approach is used, women arecomfortable sharing personal details about
14
Realizing Reproductive Choice and Rights
their reproductive, pregnancy, and abortionhistories. We used data from this phase tospecify the dimensions of abortion, choice,and rights that were most critical to be incor-porated into the pilot survey, which was toinclude a quantitative phase.
The qualitative phase was completed betweenSeptember 2000 and February 2001 in oneurban and two rural sites in the Chhindwaradistrict of Madhya Pradesh. The qualitativedata collection produced transcripts from 10focus groups, 17 key informant interviews,and 41 in-depth interviews covering youngermarried women, more mature married women,married men, unmarried women, mothers-in-law, and key community members and provid-ers such as panchayat leaders, anganwadiworkers, traditional birth attendants, ancilliarynurse midwives, physicians, and pharmacists.
An important finding from the qualitativephase was that in the Indian setting, althoughthe issue of abortion is less taboo than thoughtamong married women, it is highly tabooamong unmarried women. Other research onabortion and adolescent reproductive health inSouth Asia has also documented that premari-tal sexual activity for girls is so heavilystigmatized that any efforts at capturing itthrough surveys yield extremely unreliableresults (Ganatra, Hirve et al. 2000; Mathur,Malhotra et al. 2001). Thus, although we hadoriginally intended to study both married andunmarried women, this phase resulted in ourrestricting further research to only marriedwomen.
The Pilot Survey PhaseFollowing the data and methodologicalanalysis from the qualitative phase, we piloteda survey among 100 (50 rural and 50 urban)randomly selected married women within theChhindwara district of Madhya Pradesh.The purpose of the pilot was to test thetransferrability of the narrative approach to asurvey structure, the substantive adequacy andsensitivity of the questionnaire, and thelogistical feasibility of administering a
two-day questionnaire design. The researchteam designed an extensive two-day question-naire covering the most relevant issues emerg-ing from the qualitative phase, and focusingon women’s pregnancy history. This surveywas successfully administered in the field overa two month period. The daily logs kept bythe field staff and a review of the interviewschedules confirmed for us that the transfer-ence of the narrative technique from a qualita-tive to a quantitative medium was entirelyfeasible, and successfully implemented. Thisphase also brought to our attention severalimplementation details and options thatrequired fine-tuning, including the number ofinterviewers required, the use of closed asopposed to open codes for responses elicited,and the overall complexity of the codingstructure.
The Full Scale Survey PhaseThese concerns were addressed in developingthe full scale survey. Based on the pattern ofresponses in the pilot, we made the codingstructure less cumbersome by developingclosed-end response categories for mostquestions. Additionally, the entire surveyquestionnaire was trimmed and streamlined toeliminate redundancies and nonproductivequestions, reducing the interviewing time from2.5 hours (1 hour day one, and 1.5 hours daytwo) in the pilot phase to 1.75 hours (.5 hoursday one, and 1.25 hours day two). Theinstrument was finalized after input from thefield staff during the training process, andfieldwork was conducted between January andJune 2002.
The principal investigators conducted anintensive two week training for 18 fieldinterviewers, three of whom were from thefield staff from the first two phases. Theinterviewers, mostly natives of MadhyaPradesh, were young women in their 20s whowere selected based on their previous experi-ence in field research and high recommenda-tions from previous supervisors. The trainingprocess was structured around participatoryprinciples, allowing the interviewers to not
15
International Center for Research on Women
only absorb the structure and content of thequestionnaire, but also to provide considerableinput in modifying it. The interviewersdemonstrated great skill in understanding andcommunicating the complex and difficultnature of the questionnaire and gave helpfuland important input for revisions. For ex-ample, based on their feedback it became clearthat only the rough outlines of each questioncould be framed in English, whereas thespecific wording must be constructed in thenative language (Hindi in this case). Exten-sive quality control in the field was main-tained through constant supervision by anexperienced research officer as well asthrough frequent field visits by senior staff.The interviewers also relied on a trainingmanual developed by the research team as areference for addressing complex as well assimple issues.
SamplingFor the sample, six districts in MadhyaPradesh were purposively selected to ensuregeographic and cultural representation.Within each district, the sample is stratifiedfirst by 10 Primary Sampling Units (PSUs),and then 40 eligible women per PSU, yieldinga total sample of 2400 eligible women.Within this design, we oversampled urbanareas to ensure enough cases for analysis byrural-urban residence since abortion andcontraceptive experiences are likely to beradically different in the two areas. Eligibilitywas defined as currently married women, ages15-39, having at least one child.4 A majorpurpose of the cluster sampling design is tocollect not only household-level data, but alsocommunity-level information. A separate,small community-level questionnaire wasimplemented in each PSU to gather informa-tion on family planning and abortion provid-ers, available services, and general health,infrastructure and development conditions.
Survey instrumentThe unique structure of the survey instrumentdeveloped by the research team provides amajor breakthrough in abortion research.
As noted previously, the questionnaire spanstwo days of interviewing per eligible woman.The session on the first day is administered instandard survey format where questions withprecoded responses are asked of the womanregarding her:! household composition! socioeconomic status! demographic characteristics! husband’s characteristics! economic and decision-making status
within the family! family planning knowledge, opinions, and
practice! abortion knowledge, opinions, and practice! childbearing desires and experience
As the formal session of the first day ends, theinterviewer records a preliminary pregnancyhistory for the woman, using the birth of twosuccessive children as an anchor for probingon any pregnancies that may have occurredbetween these two births. The complexity ofthe preliminary pregnancy history then guidesthe time allocated for conducting the secondday interview, which can last from 1-1.5hours, and also helps predict the level ofdifficulty likely to be encountered. Thesecond day questionnaire requires a more in-depth recording of each pregnancy experiencea woman has had, using structured questionswith precoded responses, but also the flexibil-ity of the narrative method of interviewing.Here, for each pregnancy, the circumstancesbehind its occurrence are elicited, including:! household conditions! decision-making power! access, availability, desire, and decision-
making ability to use contraception
Once the occurrence of a given pregnancy isrecorded, the interviewer then conducts aseries of probes to see if there was any desire,and/or attempt to terminate the pregnancy.The follow-up questions then record the fullexperience of either delivering a live/stillbirth, experiencing a miscarriage, or attempt-ing a successful or unsuccessful abortion forthat specific pregnancy. If for a given
16
Realizing Reproductive Choice and Rights
pregnancy a woman attempted an abortion—successfully or unsuccessfully—then she isasked a set of questions regarding the stepstaken, multiple attempts, type of provider,treatment by provider, method for inducingabortion, complications, costs, transportation,support from husband or other familymembers, etc. This series of questions isrepeated for each pregnancy that a womanhas experienced.
Data structureThe structure of the questionnaire permitsanalysis of the data and an understanding of
the issues at several key levels: by individualwomen, by all pregnancies, and by the interval5
of time between the end of one pregnancy andthe beginning of the next. For example, we canexamine what percent of women have everexperienced an abortion, what percent of allpregnancies ended in abortion, or whethercontraception was used in the interval of timebetween the previous pregnancy and thecurrent one. In the following sections wepresent the results by examining the issues atthese multiple levels and therefore alternatelyrefer to women, pregnancies, or intervalsbetween pregnancies.
17
International Center for Research on Women
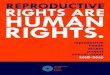
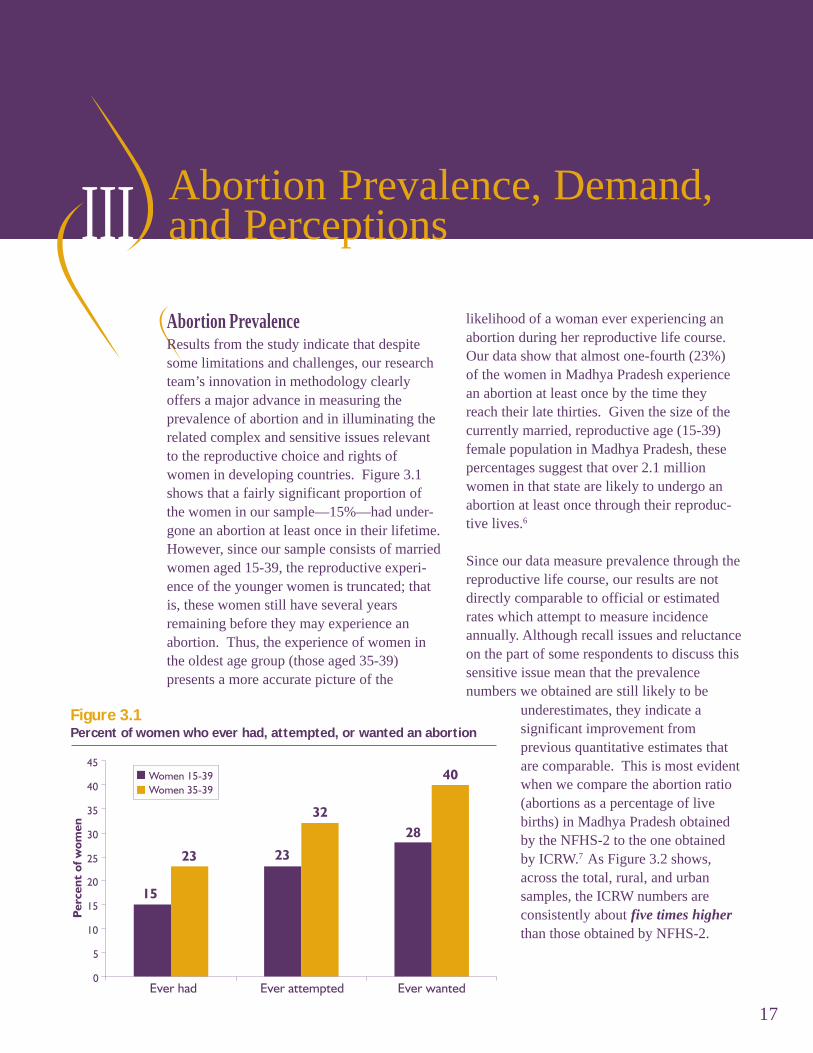
Abortion PrevalenceResults from the study indicate that despitesome limitations and challenges, our researchteam’s innovation in methodology clearlyoffers a major advance in measuring theprevalence of abortion and in illuminating therelated complex and sensitive issues relevantto the reproductive choice and rights ofwomen in developing countries. Figure 3.1shows that a fairly significant proportion ofthe women in our sample—15%—had under-gone an abortion at least once in their lifetime.However, since our sample consists of marriedwomen aged 15-39, the reproductive experi-ence of the younger women is truncated; thatis, these women still have several yearsremaining before they may experience anabortion. Thus, the experience of women inthe oldest age group (those aged 35-39)presents a more accurate picture of the
Abortion Prevalence, Demand,and Perceptions
likelihood of a woman ever experiencing anabortion during her reproductive life course.Our data show that almost one-fourth (23%)of the women in Madhya Pradesh experiencean abortion at least once by the time theyreach their late thirties. Given the size of thecurrently married, reproductive age (15-39)female population in Madhya Pradesh, thesepercentages suggest that over 2.1 millionwomen in that state are likely to undergo anabortion at least once through their reproduc-tive lives.6
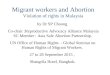
Since our data measure prevalence through thereproductive life course, our results are notdirectly comparable to official or estimatedrates which attempt to measure incidenceannually. Although recall issues and reluctanceon the part of some respondents to discuss thissensitive issue mean that the prevalencenumbers we obtained are still likely to be
Figure 3.1Percent of women who ever had, attempted, or wanted an abortion
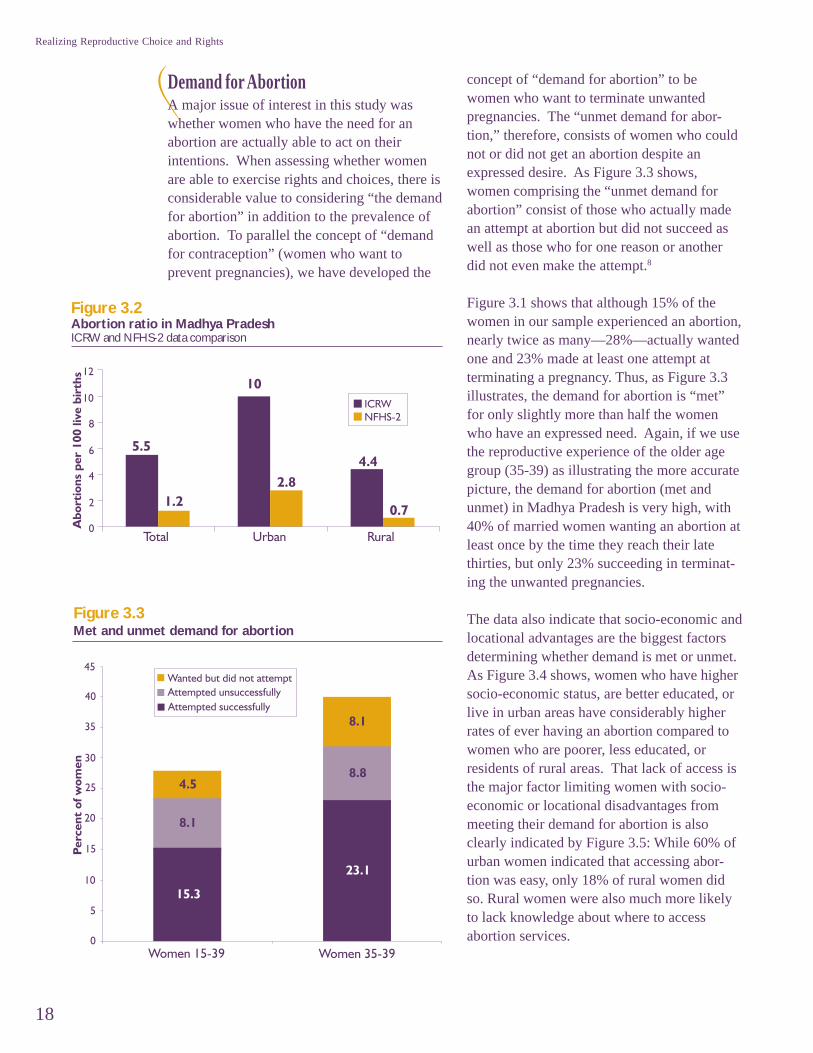
underestimates, they indicate asignificant improvement fromprevious quantitative estimates thatare comparable. This is most evidentwhen we compare the abortion ratio(abortions as a percentage of livebirths) in Madhya Pradesh obtainedby the NFHS-2 to the one obtainedby ICRW.7 As Figure 3.2 shows,across the total, rural, and urbansamples, the ICRW numbers areconsistently about five times higherthan those obtained by NFHS-2.
III
18
Realizing Reproductive Choice and Rights
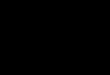
Demand for AbortionA major issue of interest in this study waswhether women who have the need for anabortion are actually able to act on theirintentions. When assessing whether womenare able to exercise rights and choices, there isconsiderable value to considering “the demandfor abortion” in addition to the prevalence ofabortion. To parallel the concept of “demandfor contraception” (women who want toprevent pregnancies), we have developed the
Figure 3.2Abortion ratio in Madhya PradeshICRW and NFHS-2 data comparison
Figure 3.3Met and unmet demand for abortion
concept of “demand for abortion” to bewomen who want to terminate unwantedpregnancies. The “unmet demand for abor-tion,” therefore, consists of women who couldnot or did not get an abortion despite anexpressed desire. As Figure 3.3 shows,women comprising the “unmet demand forabortion” consist of those who actually madean attempt at abortion but did not succeed aswell as those who for one reason or anotherdid not even make the attempt.8
Figure 3.1 shows that although 15% of thewomen in our sample experienced an abortion,nearly twice as many—28%—actually wantedone and 23% made at least one attempt atterminating a pregnancy. Thus, as Figure 3.3illustrates, the demand for abortion is “met”for only slightly more than half the womenwho have an expressed need. Again, if we usethe reproductive experience of the older agegroup (35-39) as illustrating the more accuratepicture, the demand for abortion (met andunmet) in Madhya Pradesh is very high, with40% of married women wanting an abortion atleast once by the time they reach their latethirties, but only 23% succeeding in terminat-ing the unwanted pregnancies.
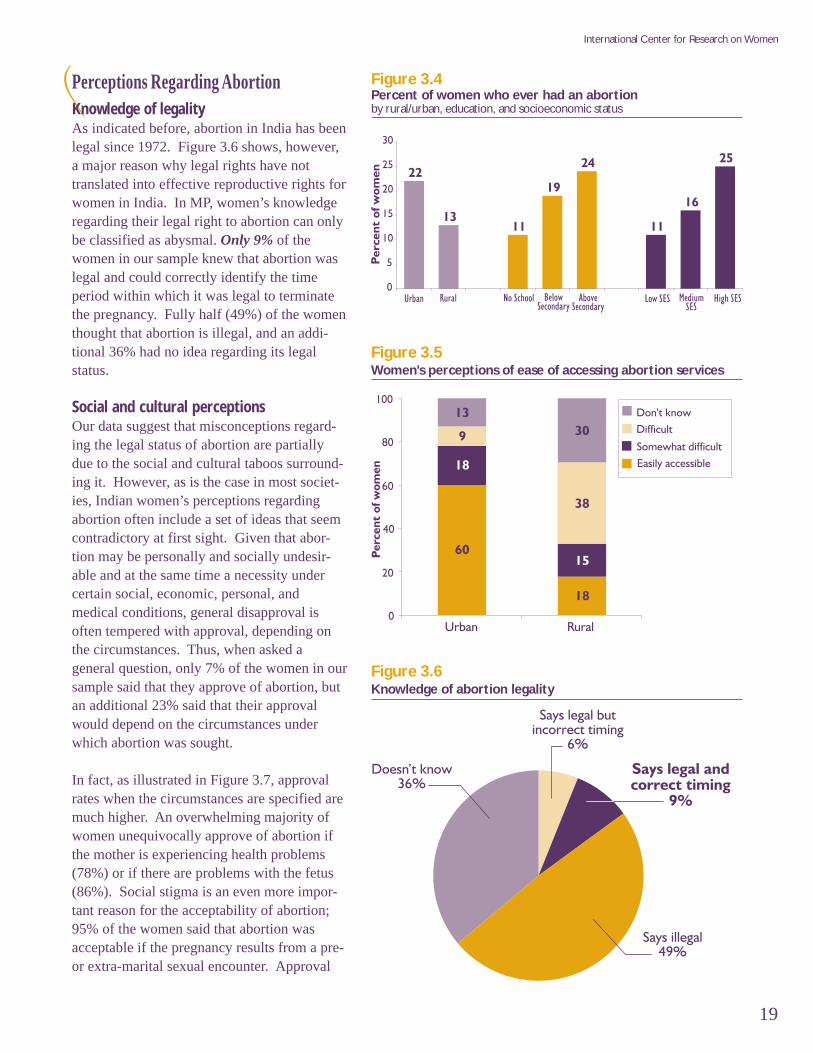
The data also indicate that socio-economic andlocational advantages are the biggest factorsdetermining whether demand is met or unmet.As Figure 3.4 shows, women who have highersocio-economic status, are better educated, orlive in urban areas have considerably higherrates of ever having an abortion compared towomen who are poorer, less educated, orresidents of rural areas. That lack of access isthe major factor limiting women with socio-economic or locational disadvantages frommeeting their demand for abortion is alsoclearly indicated by Figure 3.5: While 60% ofurban women indicated that accessing abor-tion was easy, only 18% of rural women didso. Rural women were also much more likelyto lack knowledge about where to accessabortion services.
19
International Center for Research on Women
Perceptions Regarding AbortionKnowledge of legalityAs indicated before, abortion in India has beenlegal since 1972. Figure 3.6 shows, however,a major reason why legal rights have nottranslated into effective reproductive rights forwomen in India. In MP, women’s knowledgeregarding their legal right to abortion can onlybe classified as abysmal. Only 9% of thewomen in our sample knew that abortion waslegal and could correctly identify the timeperiod within which it was legal to terminatethe pregnancy. Fully half (49%) of the womenthought that abortion is illegal, and an addi-tional 36% had no idea regarding its legalstatus.
Social and cultural perceptionsOur data suggest that misconceptions regard-ing the legal status of abortion are partiallydue to the social and cultural taboos surround-ing it. However, as is the case in most societ-ies, Indian women’s perceptions regardingabortion often include a set of ideas that seemcontradictory at first sight. Given that abor-tion may be personally and socially undesir-able and at the same time a necessity undercertain social, economic, personal, andmedical conditions, general disapproval isoften tempered with approval, depending onthe circumstances. Thus, when asked ageneral question, only 7% of the women in oursample said that they approve of abortion, butan additional 23% said that their approvalwould depend on the circumstances underwhich abortion was sought.
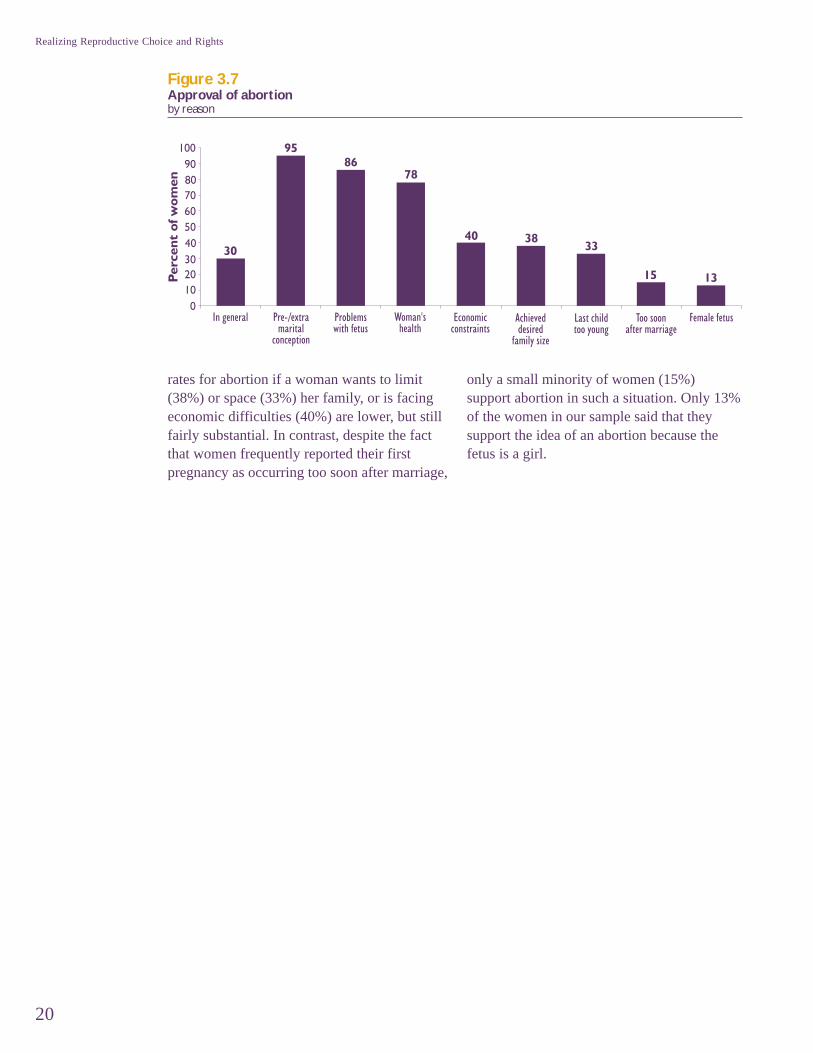
In fact, as illustrated in Figure 3.7, approvalrates when the circumstances are specified aremuch higher. An overwhelming majority ofwomen unequivocally approve of abortion ifthe mother is experiencing health problems(78%) or if there are problems with the fetus(86%). Social stigma is an even more impor-tant reason for the acceptability of abortion;95% of the women said that abortion wasacceptable if the pregnancy results from a pre-or extra-marital sexual encounter. Approval
Figure 3.4Percent of women who ever had an abortionby rural/urban, education, and socioeconomic status
Figure 3.5Women's perceptions of ease of accessing abortion services
Figure 3.6Knowledge of abortion legality
20
Realizing Reproductive Choice and Rights
rates for abortion if a woman wants to limit(38%) or space (33%) her family, or is facingeconomic difficulties (40%) are lower, but stillfairly substantial. In contrast, despite the factthat women frequently reported their firstpregnancy as occurring too soon after marriage,
only a small minority of women (15%)support abortion in such a situation. Only 13%of the women in our sample said that theysupport the idea of an abortion because thefetus is a girl.
Figure 3.7Approval of abortionby reason
21
International Center for Research on Women
In India, it is critical to understand the rolethat contraceptive availability and use plays
in allowing women to translate their desiresabout childbearing into reality. Our data allowus to map a comprehensive picture thatcaptures the connection between a woman’sviews about the timing and desirability of anygiven pregnancy, her use of contraceptionpreceding that pregnancy, and her follow-upactions on resolving an unwanted pregnancy.
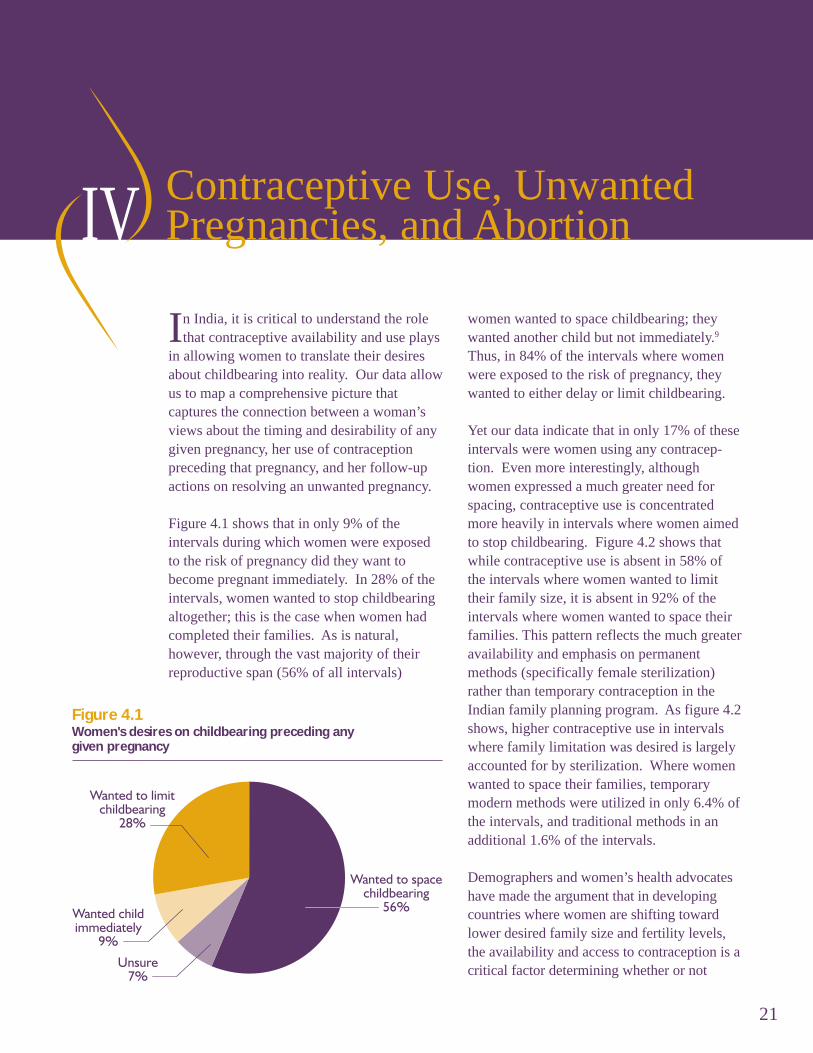
Figure 4.1 shows that in only 9% of theintervals during which women were exposedto the risk of pregnancy did they want tobecome pregnant immediately. In 28% of theintervals, women wanted to stop childbearingaltogether; this is the case when women hadcompleted their families. As is natural,however, through the vast majority of theirreproductive span (56% of all intervals)
Contraceptive Use, UnwantedPregnancies, and Abortion
women wanted to space childbearing; theywanted another child but not immediately.9
Thus, in 84% of the intervals where womenwere exposed to the risk of pregnancy, theywanted to either delay or limit childbearing.
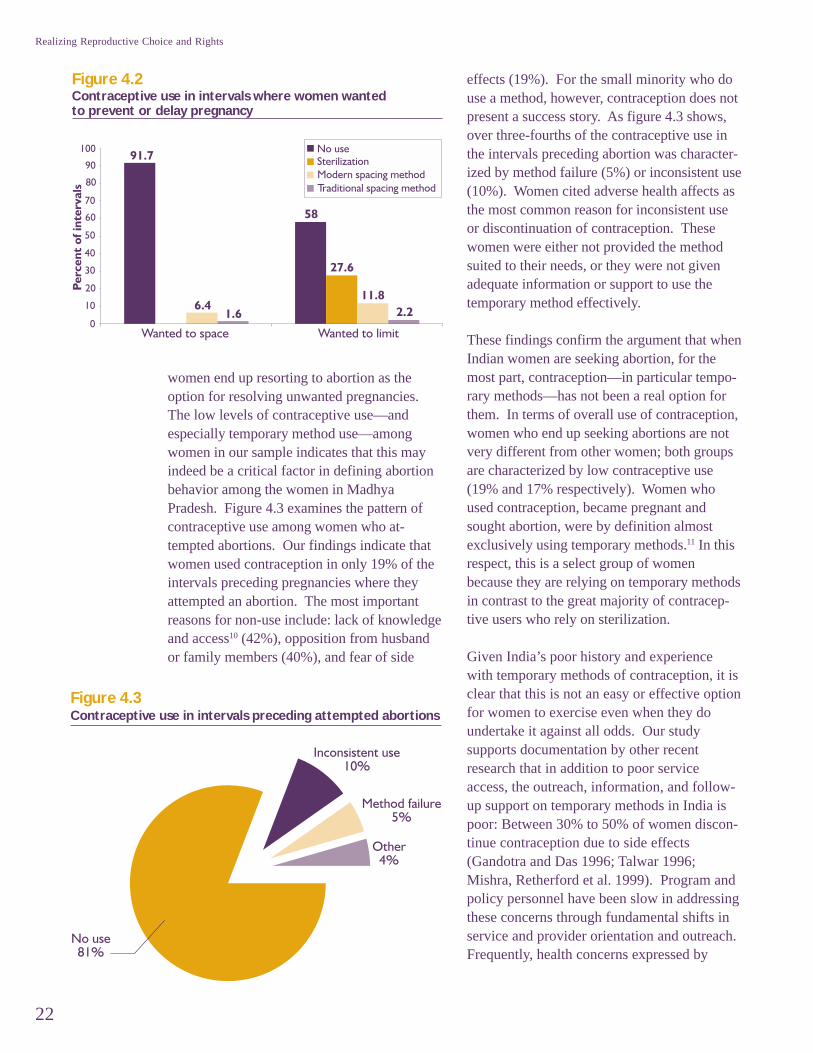
Yet our data indicate that in only 17% of theseintervals were women using any contracep-tion. Even more interestingly, althoughwomen expressed a much greater need forspacing, contraceptive use is concentratedmore heavily in intervals where women aimedto stop childbearing. Figure 4.2 shows thatwhile contraceptive use is absent in 58% ofthe intervals where women wanted to limittheir family size, it is absent in 92% of theintervals where women wanted to space theirfamilies. This pattern reflects the much greateravailability and emphasis on permanentmethods (specifically female sterilization)rather than temporary contraception in theIndian family planning program. As figure 4.2shows, higher contraceptive use in intervalswhere family limitation was desired is largelyaccounted for by sterilization. Where womenwanted to space their families, temporarymodern methods were utilized in only 6.4% ofthe intervals, and traditional methods in anadditional 1.6% of the intervals.
Demographers and women’s health advocateshave made the argument that in developingcountries where women are shifting towardlower desired family size and fertility levels,the availability and access to contraception is acritical factor determining whether or not
Figure 4.1Women's desires on childbearing preceding anygiven pregnancy
IV
22
Realizing Reproductive Choice and Rights
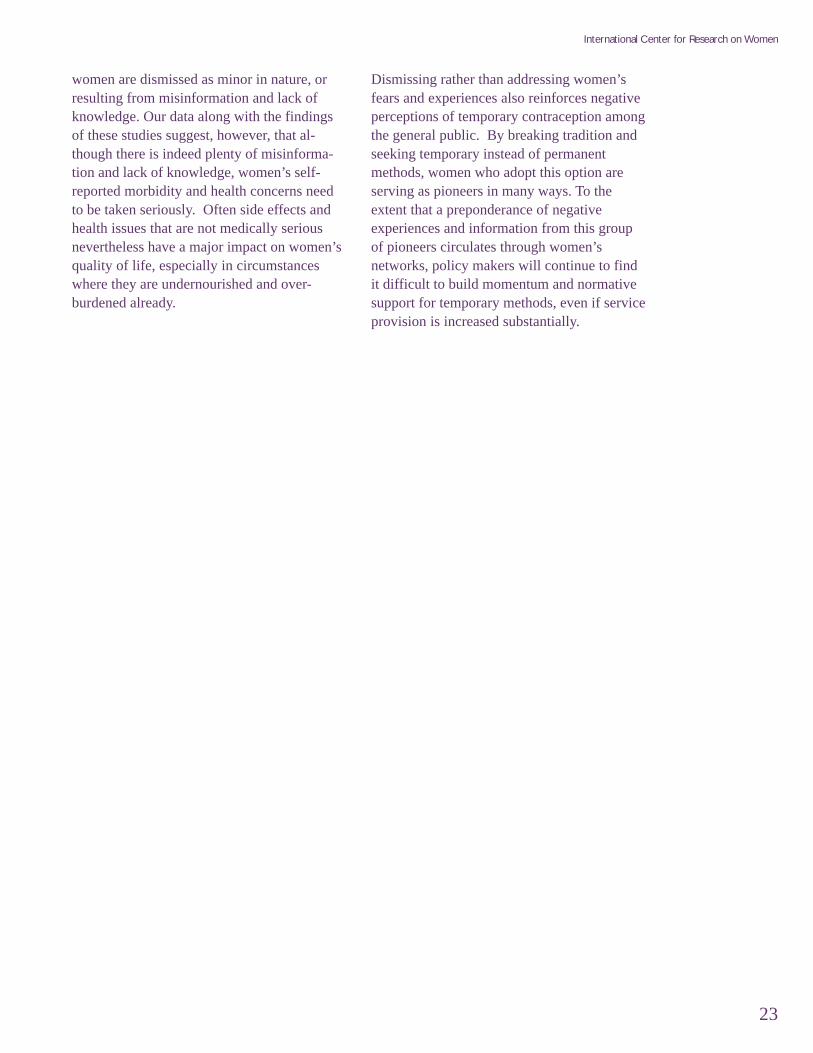
women end up resorting to abortion as theoption for resolving unwanted pregnancies.The low levels of contraceptive use—andespecially temporary method use—amongwomen in our sample indicates that this mayindeed be a critical factor in defining abortionbehavior among the women in MadhyaPradesh. Figure 4.3 examines the pattern ofcontraceptive use among women who at-tempted abortions. Our findings indicate thatwomen used contraception in only 19% of theintervals preceding pregnancies where theyattempted an abortion. The most importantreasons for non-use include: lack of knowledgeand access10 (42%), opposition from husbandor family members (40%), and fear of side
effects (19%). For the small minority who douse a method, however, contraception does notpresent a success story. As figure 4.3 shows,over three-fourths of the contraceptive use inthe intervals preceding abortion was character-ized by method failure (5%) or inconsistent use(10%). Women cited adverse health affects asthe most common reason for inconsistent useor discontinuation of contraception. Thesewomen were either not provided the methodsuited to their needs, or they were not givenadequate information or support to use thetemporary method effectively.
These findings confirm the argument that whenIndian women are seeking abortion, for themost part, contraception—in particular tempo-rary methods—has not been a real option forthem. In terms of overall use of contraception,women who end up seeking abortions are notvery different from other women; both groupsare characterized by low contraceptive use(19% and 17% respectively). Women whoused contraception, became pregnant andsought abortion, were by definition almostexclusively using temporary methods.11 In thisrespect, this is a select group of womenbecause they are relying on temporary methodsin contrast to the great majority of contracep-tive users who rely on sterilization.
Given India’s poor history and experiencewith temporary methods of contraception, it isclear that this is not an easy or effective optionfor women to exercise even when they doundertake it against all odds. Our studysupports documentation by other recentresearch that in addition to poor serviceaccess, the outreach, information, and follow-up support on temporary methods in India ispoor: Between 30% to 50% of women discon-tinue contraception due to side effects(Gandotra and Das 1996; Talwar 1996;Mishra, Retherford et al. 1999). Program andpolicy personnel have been slow in addressingthese concerns through fundamental shifts inservice and provider orientation and outreach.Frequently, health concerns expressed by
Figure 4.2Contraceptive use in intervals where women wantedto prevent or delay pregnancy
Figure 4.3Contraceptive use in intervals preceding attempted abortions
23
International Center for Research on Women
women are dismissed as minor in nature, orresulting from misinformation and lack ofknowledge. Our data along with the findingsof these studies suggest, however, that al-though there is indeed plenty of misinforma-tion and lack of knowledge, women’s self-reported morbidity and health concerns needto be taken seriously. Often side effects andhealth issues that are not medically seriousnevertheless have a major impact on women’squality of life, especially in circumstanceswhere they are undernourished and over-burdened already.
Dismissing rather than addressing women’sfears and experiences also reinforces negativeperceptions of temporary contraception amongthe general public. By breaking tradition andseeking temporary instead of permanentmethods, women who adopt this option areserving as pioneers in many ways. To theextent that a preponderance of negativeexperiences and information from this groupof pioneers circulates through women’snetworks, policy makers will continue to findit difficult to build momentum and normativesupport for temporary methods, even if serviceprovision is increased substantially.
24
Realizing Reproductive Choice and Rights
As stated before, one of the unique fea-tures of the data we have collected is that
we can present information on key aspects ofthe abortion experience as articulated by thewomen themselves. In this section, we discussthe why and how of the abortion experience interms of reasons for seeking abortion, themethods and providers used by women, thefinancial fees paid, and the effort and mobilityrequired to access services. We also discussthe importance of other family members inaccessing effective services, the self-reportedmorbidity from abortion, and the extent towhich follow-up family planning advice orcounseling is given to women who haveabortions. Finally, we discuss the extent towhich our data indicate the practice of sex-selective abortions in Madhya Pradesh.
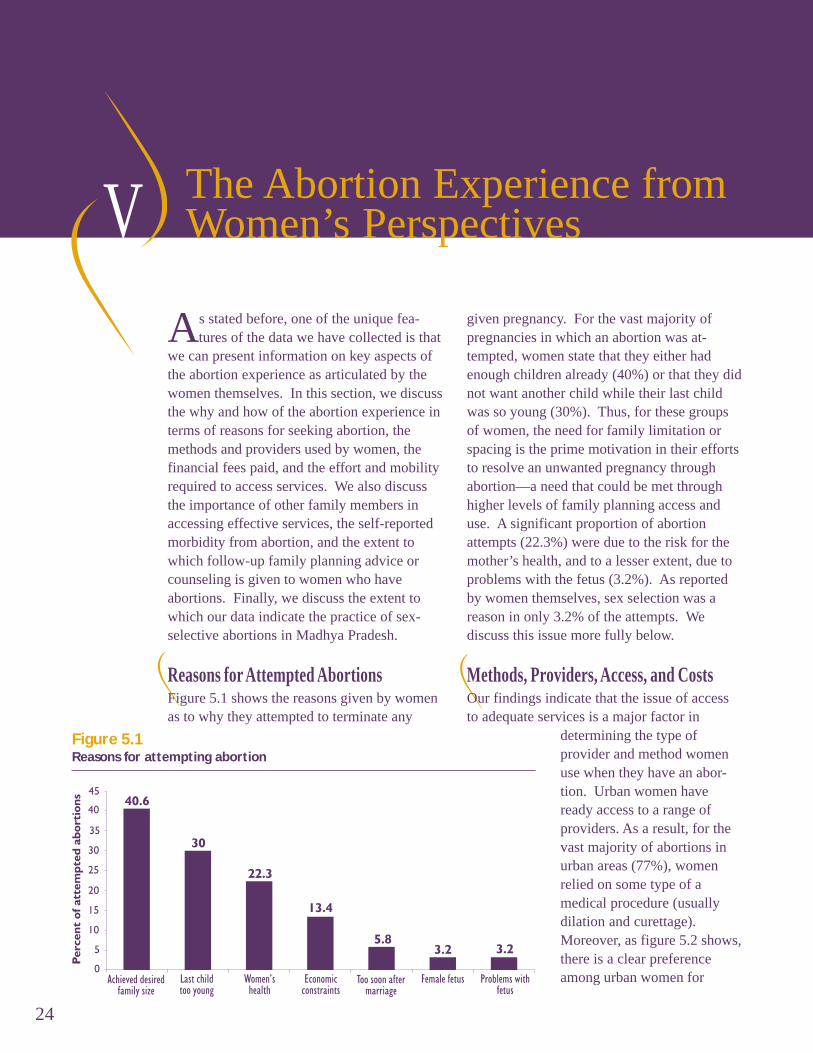
Reasons for Attempted AbortionsFigure 5.1 shows the reasons given by womenas to why they attempted to terminate any
The Abortion Experience fromWomen’s Perspectives
given pregnancy. For the vast majority ofpregnancies in which an abortion was at-tempted, women state that they either hadenough children already (40%) or that they didnot want another child while their last childwas so young (30%). Thus, for these groupsof women, the need for family limitation orspacing is the prime motivation in their effortsto resolve an unwanted pregnancy throughabortion—a need that could be met throughhigher levels of family planning access anduse. A significant proportion of abortionattempts (22.3%) were due to the risk for themother’s health, and to a lesser extent, due toproblems with the fetus (3.2%). As reportedby women themselves, sex selection was areason in only 3.2% of the attempts. Wediscuss this issue more fully below.
Methods, Providers, Access, and CostsOur findings indicate that the issue of accessto adequate services is a major factor in
Figure 5.1Reasons for attempting abortion
determining the type ofprovider and method womenuse when they have an abor-tion. Urban women haveready access to a range ofproviders. As a result, for thevast majority of abortions inurban areas (77%), womenrelied on some type of amedical procedure (usuallydilation and curettage).Moreover, as figure 5.2 shows,there is a clear preferenceamong urban women for
V
25
International Center for Research on Women
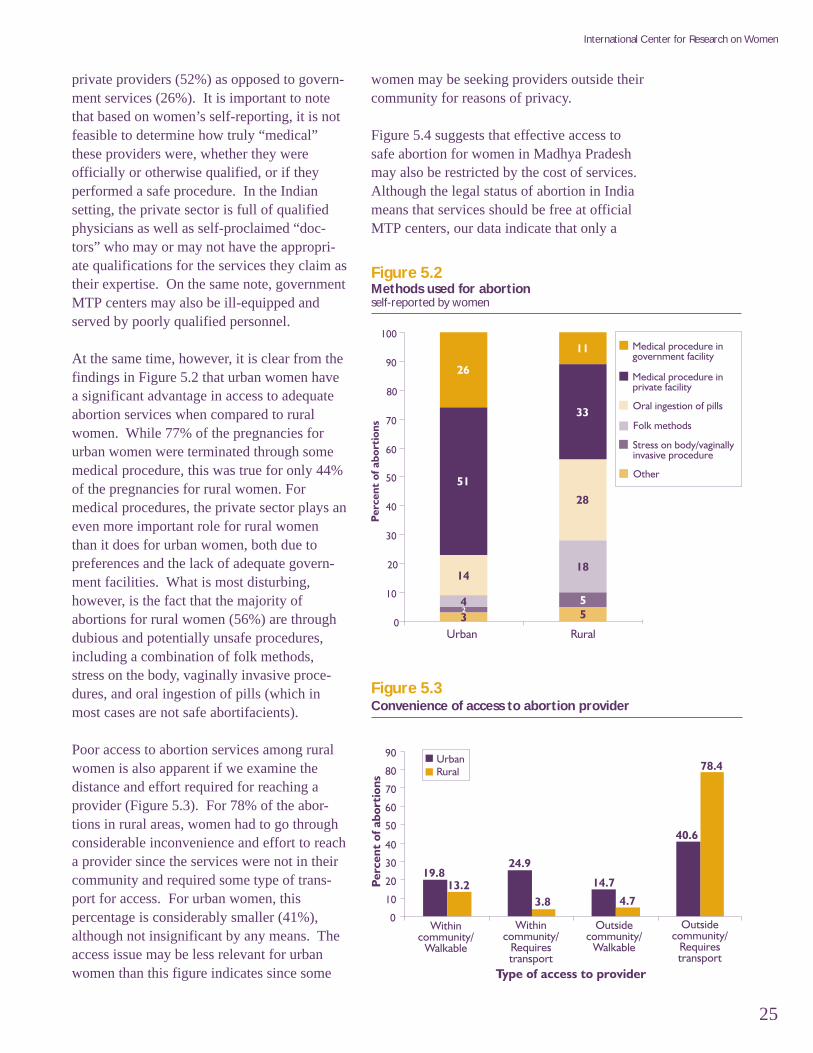
private providers (52%) as opposed to govern-ment services (26%). It is important to notethat based on women’s self-reporting, it is notfeasible to determine how truly “medical”these providers were, whether they wereofficially or otherwise qualified, or if theyperformed a safe procedure. In the Indiansetting, the private sector is full of qualifiedphysicians as well as self-proclaimed “doc-tors” who may or may not have the appropri-ate qualifications for the services they claim astheir expertise. On the same note, governmentMTP centers may also be ill-equipped andserved by poorly qualified personnel.
At the same time, however, it is clear from thefindings in Figure 5.2 that urban women havea significant advantage in access to adequateabortion services when compared to ruralwomen. While 77% of the pregnancies forurban women were terminated through somemedical procedure, this was true for only 44%of the pregnancies for rural women. Formedical procedures, the private sector plays aneven more important role for rural womenthan it does for urban women, both due topreferences and the lack of adequate govern-ment facilities. What is most disturbing,however, is the fact that the majority ofabortions for rural women (56%) are throughdubious and potentially unsafe procedures,including a combination of folk methods,stress on the body, vaginally invasive proce-dures, and oral ingestion of pills (which inmost cases are not safe abortifacients).
Poor access to abortion services among ruralwomen is also apparent if we examine thedistance and effort required for reaching aprovider (Figure 5.3). For 78% of the abor-tions in rural areas, women had to go throughconsiderable inconvenience and effort to reacha provider since the services were not in theircommunity and required some type of trans-port for access. For urban women, thispercentage is considerably smaller (41%),although not insignificant by any means. Theaccess issue may be less relevant for urbanwomen than this figure indicates since some
Figure 5.2Methods used for abortionself-reported by women
Figure 5.3Convenience of access to abortion provider
women may be seeking providers outside theircommunity for reasons of privacy.
Figure 5.4 suggests that effective access tosafe abortion for women in Madhya Pradeshmay also be restricted by the cost of services.Although the legal status of abortion in Indiameans that services should be free at officialMTP centers, our data indicate that only a

26
Realizing Reproductive Choice and Rights
small proportion of abortions are cost free(9.5%). Moreover, if we look at the distribu-tion of provider fees paid, it becomes apparentthat approximately one-third of the abortionscost between Rs.100-500, a fairly significantamount given the very limited resources ofmost families in MP, and the even morelimited resources of most women.12 Equallynoteworthy is the fact that an additional one-third of the abortions actually cost in excess ofRs. 500, an amount that would be difficult to
Figure 5.4Provider fees for abortion (in rupees)
Figure 5.5Success rate of attempted abortion by whether or notsomeone accompanied the respondent
pay for all except the most privileged groupof women.
Role of the FamilyA wealth of evidence indicates that Indianwomen have limited power and control ondecision-making regarding reproductive andchildbearing issues (Yinger, Viswanathan et al.1998; Jejeebhoy 2000). With regard toabortion, there is little existing documentationregarding the decision-making processes andhow they affect the outcome of a givenpregnancy (Jejeebhoy 1999). Among womenseeking abortion, our data portray two simulta-neously different profiles on the family’sinvolvement. For a significant proportion ofattempted abortions, women say that thedecision was their own (44%), but for anequally significant proportion, they report it asa decision by both husband and wife (50%).Unilaterally or jointly, husbands had the majordecision-making role in 20% of attemptedabortions while the in-laws played a muchsmaller role, with decision-making input inapproximately 5% of the abortion attempts.Similarly, data on consultation and discussionregarding the process of getting an abortionalso show bifurcated results, with a little overhalf the attempts (53%) being undertaken bywomen without consultation with anyone, andthe rest primarily with consultation with thehusband (42%) and sometimes the mother-in-law (9%). Our data confirm the findings ofother studies on the importance of otherhousehold decisionmakers in determiningwhether or not a woman has an abortion(Johnston 2002).
These data and our qualitative work indicatethat many women are afraid to approach theirfamilies with the issue of abortion—especiallyif the family has been opposed to contracep-tive use and family planning—while othersrealize that familial support is their bestchance at getting the abortion. And indeed, ourdata show that women are much more likely tobe successful in their attempts at abortionwhen the more powerful actors in the family,especially husbands and elder women, are
27
International Center for Research on Women
actively involved. As Figure 5.5 shows, this isespecially true in urban areas: While only 24%of attempted abortions were successful whenwomen were unaccompanied by anyone, over70% were successful when they were accom-panied by the husband, mother, or mother-in-law. Thus, an urban woman increases thelikelihood of actually getting an abortion byalmost threefold if she is fortunate or wiseenough to have one of these family memberspresent.
Husbands and elderly women in the family arekey to success not only because they have thepower of assertion in the family, but alsobecause they are likely to have the knowledge,financial resources, and mobility to ensure thatan adequate provider is sought. On their own,women are much more likely to be limited tonearby and ineffective providers or options.Furthermore, providers in MP frequentlyrequire women to have a husband or elderlyfamily member present before undertaking theprocedure. Although still substantial, in ruralareas the difference in success rates based onwhether or not a woman was accompanied isless dramatic. This is probably simply be-cause everyone in rural areas—women, men,and elders—lacks access to abortion-relatedinformation and services.
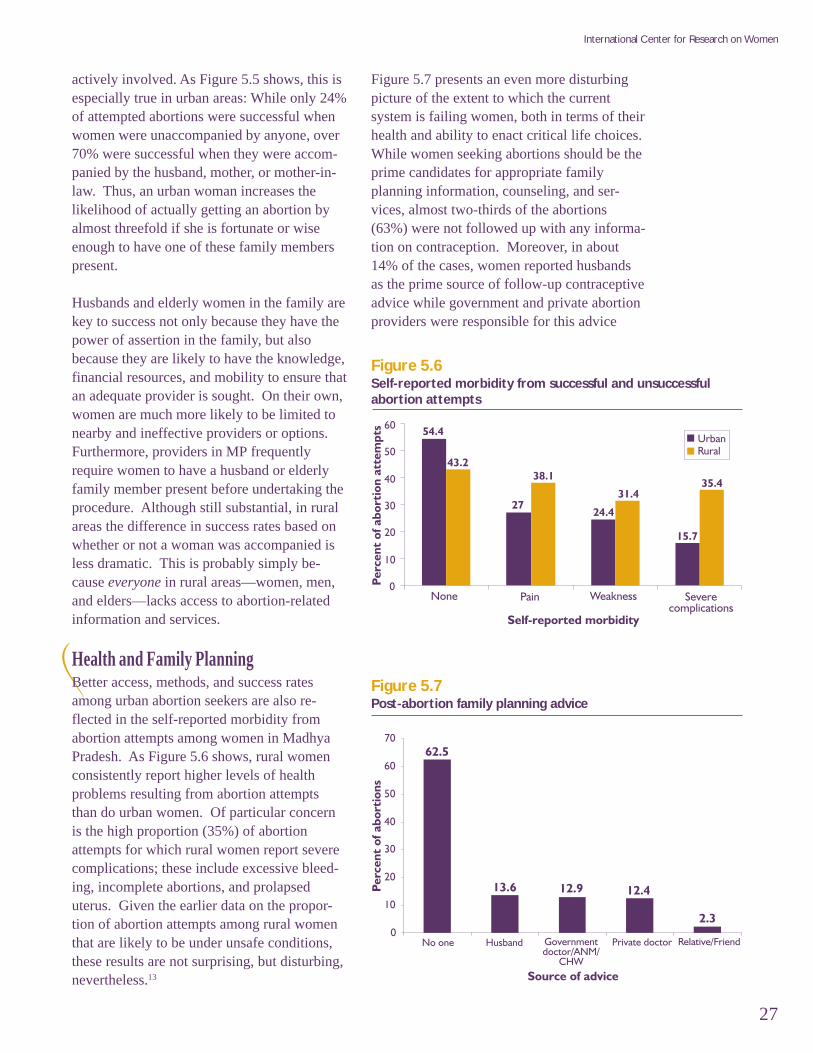
Health and Family PlanningBetter access, methods, and success ratesamong urban abortion seekers are also re-flected in the self-reported morbidity fromabortion attempts among women in MadhyaPradesh. As Figure 5.6 shows, rural womenconsistently report higher levels of healthproblems resulting from abortion attemptsthan do urban women. Of particular concernis the high proportion (35%) of abortionattempts for which rural women report severecomplications; these include excessive bleed-ing, incomplete abortions, and prolapseduterus. Given the earlier data on the propor-tion of abortion attempts among rural womenthat are likely to be under unsafe conditions,these results are not surprising, but disturbing,nevertheless.13
Figure 5.6Self-reported morbidity from successful and unsuccessfulabortion attempts
Figure 5.7 presents an even more disturbingpicture of the extent to which the currentsystem is failing women, both in terms of theirhealth and ability to enact critical life choices.While women seeking abortions should be theprime candidates for appropriate familyplanning information, counseling, and ser-vices, almost two-thirds of the abortions(63%) were not followed up with any informa-tion on contraception. Moreover, in about14% of the cases, women reported husbandsas the prime source of follow-up contraceptiveadvice while government and private abortionproviders were responsible for this advice
Figure 5.7Post-abortion family planning advice
28
Realizing Reproductive Choice and Rights
following only 25% of the abortions. Thus,the same system that sets women up forabortions does little to prevent their comingback for more.
Sex Selective AbortionsSex selective abortions in India have attracteda lot of attention in recent years. As fertilitypreferences decline and ultrasound andamniocentesis technologies become readilyavailable, parents are realizing their strongpreference for sons by aborting female fetuses.The data from the 2001 Census have beenparticularly alarming in showing an increasein the overall and juvenile (0-6) sex ratios(proportion of males to females) in a numberof Indian states. What is the picture withregard to sex selective abortions in MadhyaPradesh based on our data?
Since the campaigns against sex selectiveabortions have made it a sensitive issue onwhich women in a survey setting may notrespond truthfully, data based on women’sdirect responses may not be the ideal tool fordetermining the level of sex selective abor-tions in a population. In our survey, we triedto minimize this response bias by addressingthe issue through a series of indirect questions,
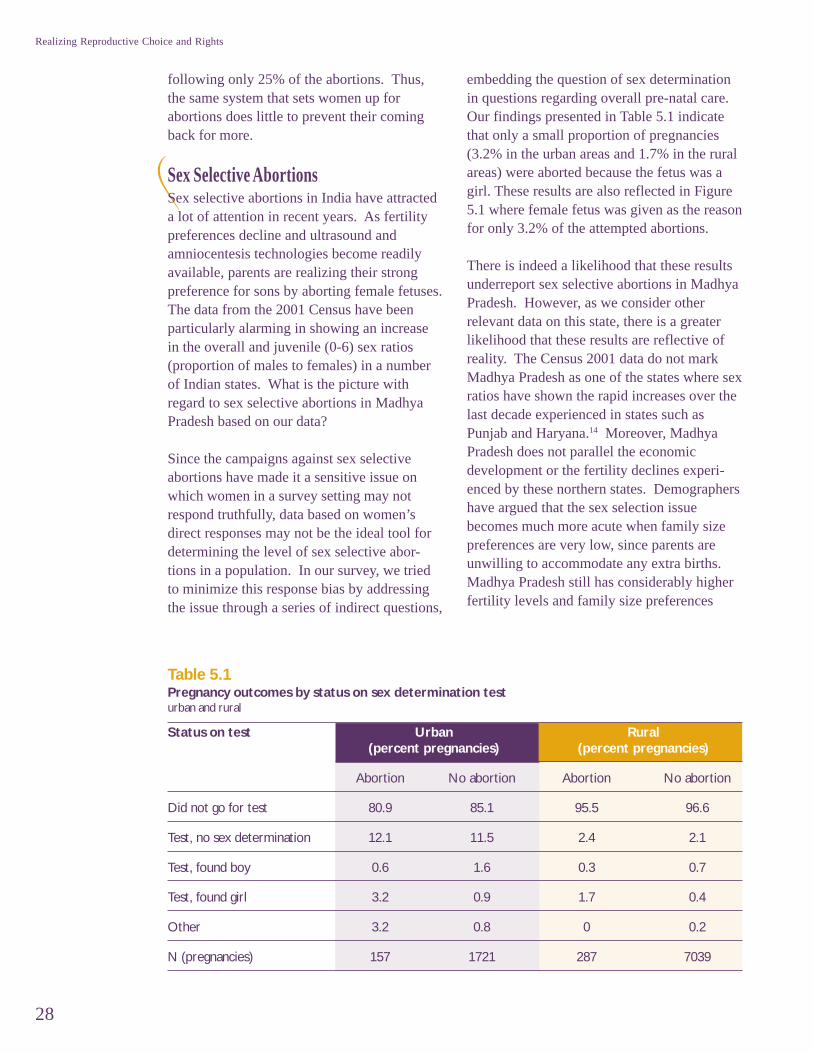
embedding the question of sex determinationin questions regarding overall pre-natal care.Our findings presented in Table 5.1 indicatethat only a small proportion of pregnancies(3.2% in the urban areas and 1.7% in the ruralareas) were aborted because the fetus was agirl. These results are also reflected in Figure5.1 where female fetus was given as the reasonfor only 3.2% of the attempted abortions.
There is indeed a likelihood that these resultsunderreport sex selective abortions in MadhyaPradesh. However, as we consider otherrelevant data on this state, there is a greaterlikelihood that these results are reflective ofreality. The Census 2001 data do not markMadhya Pradesh as one of the states where sexratios have shown the rapid increases over thelast decade experienced in states such asPunjab and Haryana.14 Moreover, MadhyaPradesh does not parallel the economicdevelopment or the fertility declines experi-enced by these northern states. Demographershave argued that the sex selection issuebecomes much more acute when family sizepreferences are very low, since parents areunwilling to accommodate any extra births.Madhya Pradesh still has considerably higherfertility levels and family size preferences
Table 5.1Pregnancy outcomes by status on sex determination testurban and rural
Status on test Urban Rural(percent pregnancies) (percent pregnancies)
Abortion No abortion Abortion No abortion
Did not go for test 80.9 85.1 95.5 96.6
Test, no sex determination 12.1 11.5 2.4 2.1
Test, found boy 0.6 1.6 0.3 0.7
Test, found girl 3.2 0.9 1.7 0.4
Other 3.2 0.8 0 0.2
N (pregnancies) 157 1721 287 7039
29
International Center for Research on Women
when compared to states more noted for sexselective abortions. Also, given that 77% ofthe MP population is rural with poor access toeven basic health services, the availability ofsex determination technology is much morelimited in this state.
Finally, it is important to note that althoughsex-selective abortions are worthy of policyattention because they reinforce discrimina-tion against the girl child in such a dramaticmanner, the vast majority of abortions are not
due to sex selection, even in the states wherethe practice is most prevalent. For example,using data from NFHS-2, Arnold, Kishor, andRoy (2002) estimate approximately 100,000sex-selective abortions, following ultrasoundor amniocentesis tests, out of approximately1.3 million total induced abortions to ever-married women in India each year. Althoughthe overall numbers are underestimates, theiranalysis indicates that sex selective abortionscomprise only about 7.7% of all inducedabortions.
30
Realizing Reproductive Choice and Rights
This study shows most vividly that the vast majority of Indian women do not have reproduc-tive rights and choice despite the fact that abortion has been legal in India since 1972. Our
findings demonstrate that in order to realize reproductive rights and choice for women in devel-oping countries, it is essential to consider issues beyond the legalization of abortion. Resultspresented in this work show that in India, the lack of safe, effective, accessible temporary meth-ods of contraception is as much a barrier to the realization of reproductive rights and choice forwomen as the ineffective and poor implementation of the abortion law. While most (although notall) women in the Western world may consider basic access to effective contraception a given,
Conclusions andRecommendations
Abortion1. Abortion rates in MP, India are considerable, with
almost one-fourth of currently married women 15-39 experiencing an abortion at least once by thetime they reach their late thirties.
2. Demand for abortion is even higher, with four inten currently married women 15-39 wanting anabortion at least once by the time they reach theirlate thirties. Failure rates for women attempting anabortion are substantial (35%).
3. Women’s knowledge of their legal right to abortionis abysmal. Only 9% of women knew that abortionwas legal and within what time period.
4. The vast majority of abortions were attemptedbecause women wanted to limit their family size orspace their childbearing (76%). Financial reasonsand the mother’s health were also importantreasons. In MP, sex selection accounts for only 3%of abortion attempts.
5. Rural, poor, and marginalized women are especiallydisadvantaged with regard to access to adequateand safe abortion services. The majority of abor-tions in rural areas (56%) were through dubious
and potentially dangerous means, and only aminority were through a medical procedure from aprivate or government provider. Rural women alsoreport fairly high levels of severe complications(33%) following abortion attempts. Given that thatvast majority of women in MP live in rural areas(77%) and are poor, these are numbers for seriousconcern.
6. Despite the provisions of the MTP Act, for mostwomen, abortion is not cost free or readily acces-sible from government providers. A significantmajority of abortions were sought from privaterather than government providers, frequently atsubstantial cost and effort on the woman’s part.
7. Family members play a significant role in women’sdecisions regarding abortion, and even more so indetermining success if an abortion is attempted.Women accompanied by influential family mem-bers—husbands, mothers-in-law, mothers—weremuch more likely to access adequate services andget an abortion than women who made the efforton their own.
Key Findings
30
Realizing Reproductive Choice and Rights
VI
31
International Center for Research on Women
this is yet to be the case in many countries ofthe developing world, India being a case inpoint. Similarly, the passage of a law legaliz-ing abortion is a necessary, but not a sufficientcondition for ensuring access to safe andeffective abortion services. It is equallyimportant to ensure that women are apprisedof their legal rights, service provision reachesa significant majority of women, and social,gender-based, and health related barriers toaccessing services are addressed adequately.
RecommendationsThe most significant policy message emergingfrom the findings of this study is clear:temporary methods of contraception must bemade a viable option for Indian women.Given that women in India are expressingspacing as an overwhelming concern in theirchildbearing preferences, sterilization cannotcontinue to be the primary focus and emphasis
of the Indian family planning program.Instead, the rhetoric for informed choice mustbe translated into a serious, committed, andenergized effort at providing women safe andeffective forms of temporary contraception.
To make temporary methods a viable optionfor Indian women, it is important to addressnot only the supply side factors of serviceprovision, but also the demand side factors ofwomen’s perceptions, knowledge, healthconcerns, and family constraints. Our datashow that women are not using temporarymethods despite tremendous need in partbecause they don’t know about them, or whereto get them; in part because influential familymembers such as husbands, mothers-in-law, ormothers oppose their use; and in part becausethey themselves mistrust these methods. Themistrust arises from misinformation, but alsofrom women’s poor experiences with these
Contraception1. The demand for contraception, even in a relatively
poor, underdeveloped state of India such as MadhyaPradesh, is very high. Women wanted to delay orprevent pregnancy in 84% of the intervals wherethey had any possibility of becoming pregnant.
2. In contrast, actual contraceptive use in MadhyaPradesh is extremely low. Women were usingcontraception in only 17% of the intervals wherethey had wanted to delay or prevent pregnancy.
3. Despite the fact that women’s overwhelmingcontraceptive need is for spacing births, sterilizationaccounts for most of contraceptive use in MadhyaPradesh. Women used temporary methods in only8% of the intervals where they had wanted tospace their childbearing.
4. The rate of contraceptive use was nearly the samefor women who attempted abortions and thosewho did not.
5. Women who attempt abortions are pioneers in thatthey are making a concerted effort to use tempo-rary methods of contraception in an environmentwhere sterilization is the norm. However, of thewomen who tried temporary methods and thenhad an abortion, 75% discontinued either due tohealth concerns or experienced method failure.
6. Despite tremendous need, temporary methods ofcontraception have not been an option that womenin Madhya Pradesh have been able to access or useeffectively. The most important reasons for non-use are lack of information and access (42%), alongwith opposition from the family (40%).
7. The current system is failing women at more thanone level. Over 75% of women’s experiences withabortion were not followed up with advice oncontraception from a medical provider.
31
International Center for Research on Women

32
Realizing Reproductive Choice and Rights
methods. Except for limited NGO efforts,little has been done in the health system toaddress these fundamental problems. Respectfor women’s bodies and attention to theirneeds are the principles that are at the core ofthe concept of reproductive rights. It iscritical that instead of dismissing women’shealth concerns, lack of proper information,and familial constraints to service access,the Indian family planning program beginaddressing these issues systematically.
It is equally important to address demand sidefactors in structuring abortion services. Ourdata show that self-reported morbidity fromabortion attempts is high, and that women’saccess to effective abortion services is highlydependent on the involvement of influentialfamily members. Misinformation and lack ofknowledge also pose serious barriers to access-ing safe abortions. Most importantly, however,our data point to the need for the better integra-tion of abortion and family planning services.This need is strikingly apparent in the very highproportion of abortions that are not followed upwith family planning advice. Perhaps the mostsignificant contribution of our work is inhighlighting the extent to which contraceptiveuse (or non-use) and abortion are intercon-nected. In women’s lives, these two issues donot exist independently of each other, and theirseparation in the health infrastructure does notserve women well.
Policy action is required to reshape theprogrammatic structure and implementation ofabortion services in India. Not only mustgovernment providers be more plentiful, bettertrained, and better equipped (especially inrural areas), but the significant role of theprivate sector must also be acknowledged.Policy makers need to create a true partnershipwith private sector providers, finding the
balance between the two extremes of over-regulation and absolute laissez-faire (both ofwhich currently exist simultaneously).
On the legal front, several actions are requiredas well. Clearly, the legality of abortion for thelast 30 years has had little relevance for manyIndian women. A campaign to inform andeducate women and their families regardingthe legal right to abortion must be a first step inensuring the enactment of this right. Aneducation campaign informing providers of theprecise provisions of the law is as necessary asan education campaign for the public. Addi-tionally, the MTP Act itself requires revision.An amendment to the Act passed in the lastfew months, to simplify registration proceduresfor providers, suggests that pressure fromcommitted stakeholders and constituencies canmake a difference. However, future amend-ments to the Act must focus on making it moretransparent and easily implemented.
Next StepsThe data from this study have been importantin shedding light on the meaning of rights andchoice in one—albeit fairly large—corner ofthe world. ICRW researchers have demon-strated that innovation in survey methodologycan enable one study to capture an accuratemeasurement of abortion prevalence, itsconnection with contraception use, and a morecomprehensive picture of women’s reproduc-tive lives. It is important that this approachand methodology be replicated in otherdeveloping countries (as well as in other partsof India), so that the reality of women’s livesfrom their own perspectives can be docu-mented in a number of other social andpolitical contexts. Such documentation isessential for bringing meaning to the conceptsof rights and choice internationally.
33
International Center for Research on Women
1 The unmet need for family planning is substantially greater than is obvious at first glance. The NFHS-2 calculates unmet need at 15.8% inIndia, using a limited definition of currently married, fecund women who do not want any additional children or who do not want anotherchild for at least two years. In poorer, disadvantaged, high fertility settings such as the BIMARU (sickly) states, unmet need is higher. AnICRW study in Sitapur, Uttar Pradesh calculated unmet need at 31.7% when using this same definition, but at 54.8% when using anexpanded definition where method dissatisfaction, non-protection by post-partum amenorhea, and incorrect traditional method use werealso accounted for (Yinger 1998).
2 The NFHS-2 uses a more sophisticated approach. A question about abortion is asked during the collection of birth histories by asking if anabortion occurred between any given two births. Our methodology uses a similar approach as part of the Day 1 questionnaire, although wedo not directly focus on an abortion between two births, but rather on first determining if there are missing pregnancies between births thatmay have been resolved through abortion. NHFS-2’s numbers from these data have yet to be published.
3 The study design was approved by the Institutional Review Boards of each partner institution.
4 Women without children are less likely to have pregnancy histories to record while women older than 39 may present considerable recallbias.
5 More specifically, an interval is the period between marriage and the first pregnancy, between any two pregnancies, or the period follow-ing the last pregnancy. The latter is classified as an open interval while the former two are classified as closed intervals. The intervalfollowing a last pregnancy may also be considered closed if the woman or her husband is sterilized and the woman is not at risk ofbecoming pregnant.
6 The 2001 census gives total female population in MP as 28,928,245. Based on the NFHS-2, the ratio of currently married women ages15-39 to all women is 0.3193. Therefore, we calculate that there are approximately 9,235,697 married women aged 15-39 in MadhyaPradesh currently. We estimate that 2,124,210 of these women will have at least one abortion by the time they reach 39 based on ourfinding that 23% of our sample aged 35-39 have ever had an abortion.
7 Abortion ratios from the NFHS-2 were calculated for the equivalent sample—married women 15-39 with at least one child—in MP as thatused by ICRW.
8 In this study, we define an attempted abortion from the woman’s perspective rather than a technically medical perspective. A woman wasconsidered to have attempted an abortion if she said she wanted to terminate a pregnancy and took some action with the intention ofterminating it, whether or not that action is medically proven to result in an abortion.
9 Our definition of not wanting a child immediately is not wanting another child for at least two years. This definition is most frequentlyused when describing unmet need for contraception.
10 The responses classified as “lack of knowledge and access” include: did not know about contraceptives; did not know where to get them;contraceptives not available; and felt shy obtaining contraceptives.
11 Of the 19% of intervals where contraception was used prior to an abortion attempt, 18% were characterized by (mostly modern) tempo-rary method use, and 1% by failed sterilization.
12 At the current exchange rate, one dollar is equivalent to approximately Rs. 48. The relative value of Rs 100-500 or over Rs. 500,however, has to be determined in the context of the local setting. The data on household circumstances show that the monthly householdexpenses of 77% of the families that we surveyed are less than Rs. 3000, and that over half the families have a difficult time meeting theirmonthly expenses.
13 It is important to note that at least in one aspect our study underreports morbidity: The very nature of sample survey excludes women whohave died from attempted abortions.
14 For example, while the juvenile sex ratio in Punjab climbed from 114.3 in 1991 to 126.1 in 2001, and in Haryana from 113.8 to 122.0,the juvenile sex ratio in Madhya Pradesh experienced a much less steep increase from 104.4 to 108.1 during the decade.
End Notes
34
Realizing Reproductive Choice and Rights
Alan Guttmacher Institute (AGI). 1999.Sharing Responsibility: Women, Society, andAbortion Worldwide. New York, AGI.
Arnold, F. 1997.Gender Preferences for Children. Calverton,MD, Macro International.
Arnold, F, MK Choe, et al. 1998.“Son Preference, the Family-buildingProcess and Child Mortality in India.”Population Studies 52(3): 301-315.
Arnold, F., S. Kishor, et al. 2002.“Sex Selective Abortions in India.”Population and Development Review28(4):759-785.
Bandewar, Sunita. 2001.Abortion Legislation and Access to SafeAbortion Care Services: The IndianExperience. Advocating for Abortion Access:Eleven Country Studies. B. Klugman and D.Budlender. Johannesburg, Women’s HealthProject: 135-155.
Baveja, R, K Buckshee, et al. 2000.“Evaluating Contraceptive Choice throughthe Method-mix Approach: An IndianCouncil of Medical Research (ICMR) TaskForce Study.” Contraception 61(2): 113-119.
Bongaarts, J. 1997.“Trends in Unwanted Childbearing in theDeveloping World.” Studies in FamilyPlanning 28(4): 267-277.
Chhabra, R and SC Nuna. 1996.Abortion in India: An Overview. New Delhi,Veerendra Press.
Donaldson, PJ. 2002.“The Elimination of Contraceptive AcceptorTargets and the Evolution of PopulationPolicy in India.” Population Studies 56(1):97-110.
Figa-Talamanca, I. 1989.An Overview of Research Methodologies forthe Study of Public Health Aspects ofInduced Abortion. Population Council’sRobert H. Ebert program on Critical Issuesin Reproductive Health, in collaborationwith International Projects AssistanceServices, World Health Organization. F.Coeytaux, A. Leonard and E. Royston. NewYork, Population Council, InternationalProjects Assistance Services, World HealthOrganization.
Ganatra, BR, SS Hirve, et al. 2000.Induced Abortions in Rural WesternMaharashtra: Prevalence and Patterns.Reproductive Health in India: New Evidenceand Issues. Pune, India.
References
Gandotra, MM and NP Das. 1996.Factors Influencing Choice of a Contracep-tive and the Reasons for its Discontinuation.Spacing as an Alternative Strategy. India’sFamily Welfare Programme. M Khan and GCernada. Delhi, BR Publishing Corporation:95-114.
Gupte, M, S Bandewar, et al. 1997.“Abortion Needs of Women in India: A CaseStudy of Rural Maharashtra.” ReproductiveHealth Matters 5(9): 77-86.
Henshaw, SK, S Singh, et al. 1999.“The Incidence of Abortion Worldwide.”International Family Planning Perspectives25(Supplement): S30-S38.
International Institute for PopulationSciences (IIPS). 1995.
National Family Health Survey: India 1992-93. Mumbai, IIPS.
IIPS and ORC Macro. 2000.National Family Health Survey (NFHS-2):India 1998-99: India. Mumbai, IIPS.
IIPS and ORC Macro. 2001.National Family Health Survey (NFHS-2):India 1998-99: Madhya Pradesh. Mumbai,IIPS.
Jejeebhoy, SJ. 1999.“Reproductive Health Information in India:What are the Gaps?” Economic and PoliticalWeekly 34(42-43): 3075-3080.
Jejeebhoy, SJ. 2000.Women’s Autonomy in Rural India: ItsDimensions, Determinants, and the Influenceof Context. Women’s Empowerment andDemographic Processes: Moving BeyondCairo. H Presser and G Sen. New York,Oxford University Press.
Johnston, Heidi Bart. 2002.Abortion Practice in India: A Review ofLiterature. Mumbai, Centre for Enquiry intoHealth and Allied Themes (CEHAT)/Healthwatch.
Khan, ME, S Barge, et al. 1999.Abortion in India: Current Situation andFuture Challenges. Implementing aReproductive Health Agenda in India: TheBeginning. S Pachuri and S Subramanian.New Delhi, Population Council.
Khan, ME and George Cernada. 1996.Spacing as an Alternative Strategy: India’sFamily Welfare Programme. Delhi, BRPublishing Corporation.
Khan, ME, BC Patel, et al. 1999.The Quality of Family Planning Services inUttar Pradesh from the Perspective of ServiceProviders. Improving Quality of Care inIndia’s Family Welfare Programme. M.Koening and M. Khan. New Delhi,Population Council.
Khan, ME and J Townsend. 1999.Target-free Approach: Emerging Evidence.Implementing a Reproductive Health Agendain India: The Beginning. S. Pachauri and S.Subramanian. New Delhi, PopulationCouncil.
Khanna, SK. 1997.“Traditions and Reproductive Technology inan Urbanizing North Indian Village.” SocialScience and Medicine 44(2): 171-180.
Koster-Oyekan, W. 1998.“Why Resort to Illegal Abortion in Zambia?Findings of a Community-based Study inWestern Province.” Social Science andMedicine 46(10): 1303-1312.
Mathur, S, A Malhotra, et al. 2001.“Adolescent Girls’ Life Aspirations andReproductive Health in Nepal.” ReproductiveHealth Matters 9(17): 91-100.
Mishra, VK, RD Retherford, et al. 1999.Reasons for Discontinuing and NotIntending to Use Contraception in India.Mumbai, India, International Institute forPopulation Sciences: 36.
Mundingo, AI and C Indriso, Eds. 1999.Abortion in the Developing World. NewDelhi, Vistaar Publications.
Ninger, LJ. 2001.“Indian Women Often Select Methods otherthan those their Providers Recommend.”International Family Planning Perspectives27(1): 50-51.
Pande, R and NM Astone. 2001.Explaining Son Preference in Rural India:The Role of Women’s Social and EconomicPosition. 2001 Annual Meeting of thePopulation Association of America,Washington, DC.
Talwar, PP. 1996.Choice, Acceptance and Continuation ofSpacing Methods in India. Spacing as anAlternative Strategy. India’s Family WelfareProgramme. M Khan and G Cernada. Delhi,BR Publishing Corporation: 115-142.
Visaria, L, S Jejeebhoy, et al. 1999.“From Family Planning to ReproductiveHealth: Challenges Facing India.” Interna-tional Family Planning Perspectives25 (Supplement): S44-S49.
35
International Center for Research on Women
Visaria, L and P Visaria. 1999.Field-Level Reflections of Policy Change.Implementing a Reproductive Health Agendain India: The Beginning. S. Pachauri and S.Subramanian. New Delhi, PopulationCouncil.
Yinger, NV. 1998.Unmet Need for Family Planning: ReflectingWomen’s Perspectives. Washington, DC,International Center for Research on Women.
Yinger, NV, H Viswanathan, et al. 1998.Reaching Women: Unmet Need for FamilyPlanning in Uttar Pradesh, India.Washington, DC, International Center forResearch on Women.

International Center for Research on Women1717 Massachusetts Avenue, NWSuite 302Washington, DC 20036, U.S.A.
Tel: (202) 797-0007Fax: (202) 797-0020e-mail: [email protected]
www.icrw.org