Embed Size (px)
Citation preview
54 515355 52
68 696766
7275 74 73
35 32
4948
34 33
46 47
71
31
70
50
Reaching Out:An Action Plan on Social Exclusion
1
Contents
SummaryPrime Minister’s preface 3Foreword by Hilary Armstrong, Minister for the Cabinet Office 5
Section I: Introduction
Chapter 1: Executive summary 7
Section II: A renewed approach
Chapter 2: The issue and context 13
Chapter 3: Guiding principles 21
Section III: A lifetime approach
Chapter 4: Early Years 45
Chapter 5: Childhood and Teenage Years 57
Chapter 6: Adult Years 71
Section IV: The future
Chapter 7: Next steps 83
Annex A:
Grid of policy actions 87
Annex B:
Social Exclusion Task Force 95

3
Prime Minister’s preface
Tackling social exclusion is at the heart of this government’smission. It is our fundamental belief that everyone should havethe opportunity to achieve their potential in life.
Since 1997 we have made great progress. Over 2 million morepeople are in work. 800,000 children and 1 million pensionershave been lifted out of poverty. A minimum wage is in place.We have eradicated long-term youth unemployment. As aconsequence of the policies the Government has put in place,many more people in the UK enjoy more opportunities nowthan was the case a decade ago.
This Action Plan examines the reasons why, despite the huge progress we have made,there are still individuals and families who are cut off. About 2.5 per cent of everygeneration seem to be stuck in a lifetime of disadvantage. Their problems are multiple,entrenched and often passed down through generations.
But the message in this Plan is an overwhelmingly positive one. We believe it is possibleto extend opportunity to the least advantaged so that they enjoy more of the choices,chances and power that the rest of society takes for granted.
To achieve this, we need a radical revision of our methods for tackling social exclusion.This Plan is guided by five principles: early intervention; systematically identifying whatworks; better co-ordination of the many separate agencies; personal rights andresponsibilities; and intolerance of poor performance. It proposes a range of systemicreforms aimed at fundamentally changing the way we deliver help and support to thesocially excluded.
This Plan also concentrates on some key groups. We propose more support for veryyoung children born into vulnerable circumstances because we know the crucialimportance of the first months and years of a child’s life in framing their opportunities.
We propose action to reduce teenage pregnancy because we know that despite thegood job many young mothers do, teenage motherhood often leads to reducedopportunities for mother and child alike. We will publish a Green Paper on Children inCare aimed at increasing educational attainment and ensuring greater stability andcontinuity in care, including through an expansion of budget-holding lead professionals.We propose a more personalised service for adults with multiple problems, because we
know that tailored help is needed to address their needs, and that passing vulnerablepeople from service to service is neither good for them nor for the wider community.
This document is marked by ambition. The issues it deals with are not easy to solve, butthe belief that social exclusion is not inevitable, that it can be tackled, and that we canwork together to spread opportunity runs through every page.
September 2006
4
Reaching Out: An Action Plan on Social Exclusion
5
Foreword by Hilary Armstrong
When I worked as a community worker 30 years ago, I saw at first hand the difficulties and challenges that face the mostdeprived and excluded members of our society. It was clearjust how hard it was for people to develop and achieve theaspirations that the rest of us took for granted.
I also learnt that in all deprived communities people whowanted to improve their lives, with the right help and support,could achieve their aspirations. People who want to turn theirlives around can.
I have always believed that it is wrong for a society or agovernment to write people off.The cost is too great for them, their children and oursociety as a whole.We need to ensure everyone gets the opportunity to fulfil theirpotential, and to contribute to, and benefit from, our wider society.
This government has already created the opportunities which have enabled many morepeople from disadvantaged backgrounds to realise the aspirations they hold forthemselves and their families.
A stable economy with investment and reform of public services has provided theopportunities which, together with people’s hard work, has meant that incomes haverisen and educational attainment and employment increased, and programmes like SureStart ensure that many get a decent chance in life.
The less well-off have generally benefited most from our measures, extending theopportunities of living in the UK to a wider section of our society than ever before.
Now we want to build on this progress to go further.We want to work with everyoneto help them reach their potential. A society where most can improve their lives is betterthan one where only a few do. And a society where everyone can improve their lives isbetter than any.
This Action Plan shows our determination to ensure that even the hardest to reach, whomay not have been able to benefit from our reforms, get the chance to turn their livesaround. For these few people, their many disadvantages work together to make evenhaving the aspiration to succeed very difficult.
In every generation, opportunity and aspiration increase the life chances for moresections of our society – but around 2.5 per cent of every generation seem caught in alifetime of disadvantage and harm.
We are not a government willing to accept this as inevitable.
That is why we have produced this Action Plan to renew our drive against socialexclusion throughout the life-cycle. I am grateful to the many stakeholders who havecontributed to the development of this Action Plan.
It starts with our principle of early identification and intervention. I have always feltfrustrated when services have failed to use their understanding to intervene effectivelyand prevent foreseeable problems down the line – a tragedy of wasted potential andwasted lives, and a reinforced cycle of deprivation.We must ensure people have accessto help and support before problems escalate.
And we know what works.There are some great people driving excellent programmes,often outside the state sector, that are really making a difference to people’s lives.We willhighlight these and strengthen support for them, ensure the best work is shared, andwhere intervention is failing, we will take action.
At the moment the most disadvantaged are offered the same public services as the restof us.That simply isn’t working – a one-size-fits-all approach lets down our most needyand hard to reach. We therefore need to personalise our services, be more persistentand coordinated, and fit them around the needs of individuals if we are ever going totackle the hardest complexities of people’s lives.
Government can’t do it all. For too many people the problems have appearedinsurmountable and the system too inaccessible, preventing them from takingresponsibility for their lives. We are an enabling government – supporting the groups andorganisations helping people get themselves out of their difficulties and to gain control oftheir lives.To do this, people need support, encouragement and often a tough challenge.
No one should be written off – no one is too hard to reach. I don’t believe anyonedoesn’t want a better future for themselves and their children.This Action Plan will helpindividuals and the services that support them unlock their aspiration and help lift themout of poverty and exclusion.
Hilary ArmstrongMinister for the Cabinet Officeand Social Exclusion
6
Reaching Out: An Action Plan on Social Exclusion
Section I: IntroductionChapter1: Executive summary
7
Where are we now?1.1 The UK is a country of growing prosperity.The last decade has seen many more peoplein jobs, thanks to record levels of employment;crime has fallen by 44 per cent; the vastmajority of people – 19 out of 20 – have seentheir incomes rise by 2 to 3 per cent eachyear ; 800,000 children and 1 million pensionershave been lifted out of poverty; and we haveexperienced year-on-year increases ineducational attainment and life expectancy.These improvements have benefited less-well-off people the most, extending theopportunities of living in the UK to a widersection of our society than ever before.
1.2 But we can do more.We live in a societythat aspires to be fair and just.To achieve thisaspiration we must recognise that socialexclusion and the subsequent waste of humanpotential is bad for the whole country, as wellas for those individuals suffering from it.
1.3 Because of this achievement in reducingpoverty and increasing affluence, the persistentand deep-seated exclusion of a small minoritystands out ever more starkly.The disadvantagesthese individuals face are usually apparent earlyin life and can persist long into adulthood andold age.
1.4 Equally troubling is the ‘cycle ofdisadvantage’, which shows that deprivation inone generation is likely to pass down to thenext. For example, the daughter of a teenagemother is twice as likely as the daughter of anolder mother to become pregnant in her teenyears. It is, of course, not a certainty, but itdoes illustrate the fact that early experiencesin life have major effects on a person’s futurelife chances.
1.5 These patterns of early and persistentproblems are troubling, but predictions don’thave to come true.This Action Plan offers a
series of opportunities that, if taken, willmitigate the lifelong effects of social exclusionand prevent them being passed down tofuture generations.
1.6 This Action Plan shows that through earlyidentification, support and preventative actionpositive change is possible.We can tackleproblems before they become fully entrenchedand blight the lives of both individuals andwider society.
1.7 Some might ask why this agenda is stillimportant, particularly against a background ofgeneral success.The Government’s view is thatit is precisely because of those successes that itis vital to do more. No civilised country shouldignore the plight of the most excluded insociety and no one should be shut off fromthe opportunities, choices and options in lifewhich most of us take for granted.We knowthat once people are given the opportunity toexcel, they often do.The year-on-year increasesin educational attainment in our schools, forexample, have happened because of the hardwork of students and families that have takenadvantage of the conditions the Governmentcreated in the classroom. It is this commitmentto opportunity which is the driving forcebehind the policies set out in this Action Plan.
1.8 Tackling social exclusion also mattersbecause failing to do so creates a cost forsociety.The UK has enjoyed a strong economyand growing prosperity in recent years, but wewould be even more prosperous if the talentsof each and every member of the communitycould flourish.The need today to act to ensurethat opportunity is enjoyed by the wholecommunity is ever more urgent and demandsa response from government.
1.9 It is also the case that the behaviour ofsome people – particularly some of the mostchallenging families – causes real disruption
8
Reaching Out: An Action Plan on Social Exclusion
and distress to the community around them.The Respect Task Force is coordinating theGovernment’s response to this issue.ThisAction Plan applies a similar practical approach,but with a focus on interventions to reduce awide range of adverse outcomes, of whichanti-social behaviour is only one.
1.10 So both to enhance the opportunities forindividuals and families and for the good of thecountry as a whole, we set out here arenewed government commitment to tacklingthe social exclusion that remains even after theprogress of recent years.
Where are we going?1.11 It has become clearer that there aresmall groups of people whose needs areunique and complex and who are particularlydifficult to reach. Highly localised and tailoredresponses will be needed to extend theopportunities enjoyed by most people tothose suffering the effects of social exclusion.
1.12 This Action Plan opens the next chapterin our attack on entrenched exclusion, settingout:
• the principles that drive our approach, andhow these will inform our actions; and
• a series of immediate changes and pilotsbuilt around a lifetime approach to tacklingexclusion.
A renewed approach: guidingprinciples1.13 A lot of money is spent through publicservices on the most socially excluded people.But much of this spending is directed atmanaging the symptoms of exclusion onceproblems have become entrenched.The Government will build on its reforms ofrecent years, as set out in Support for Parents:
The Best Start for Children, to shift efforts from‘treatment’ to ‘prevention’ and break the cycleof disadvantage.
1.14 Five key guiding principles will inform theGovernment’s approach and actions:
•• Better identification and earlierintervention. We will develop and promotebetter prediction tools for use by front-linepractitioners, for example health visitors andcommunity midwives, and will seek toensure that those identified as at risk arefollowed up.
•• Systematically identifying ‘what works’. Wewill introduce a common approach acrossgovernment to rate programmes by thequality of the evidence behind them.Approved and rated programmes will begiven the opportunity to highlight blockagesto delivery.We will strengthen the capabilityof commissioners of public services and willexplore the best ways of disseminating whatworks, particularly around excellence inchildren’s and family services.
•• Promoting multi-agency working.The Government will strengthen the role ofLocal Area Agreements, publish informationabout the cross-agency costs of socialexclusion, and will explore how to extenddata sharing in relation to the mostexcluded or at-risk groups, including anyadditional powers that may be necessary.
• Personalisation, rights and responsibilities.We will pilot and explore service deliverybased on budget-holding lead professionalsand on brokering as ways of providingtailored programmes of support built aroundstrong and persistent relationships withthose at risk. In this context, we will also trialextending tariffs for delivery of particularoutcomes, and we will encouragepractitioners and brokers to agree explicit‘compacts’ with at risk families andindividuals.
9
Chapter 1: Executive summary
• Supporting achievement and managingunderperformance. We will work acrossGovernment to ensure that the nextgeneration of Public Service Agreementsadequately address the needs of the mostdisadvantaged. And we challenge local areasto come forward with appropriate andimaginative proposals to address the needsof the most excluded.The forthcoming LocalGovernment White Paper will set out a clearintervention strategy for underperforminglocal authorities, while at the same timegiving effective service providers more roomto innovate.
1.15 The challenges identified in thisdocument are profound and may take years toaddress. But these guiding principles offer aclear direction of travel that the Governmentwill pursue vigorously, notably in the context ofthe Comprehensive Spending Review, andother forthcoming policy developments.
A lifetime approach1.16 In this Action Plan we have focused onsome of the most excluded groups, such aschildren in care or adults leading chaotic lives –groups that have generally failed to fulfil theirpotential and accept the opportunities thatmost of us take for granted.
1.17 System reform can take years to deliver,and results can take decades to show.We willsupplement our drive for deeper reform withmore focused and immediate action that weare confident will make a difference.ThisAction Plan establishes a range of specificproposals that we believe to be of pivotalimportance throughout an individual’s lifetime,both in terms of their impact on the lifechances of the most excluded and in order to strengthen the case for wider reforms.
1.18 In the early years of life, long before achild enters school, behaviours are establishedthat profoundly change that child’s life chancesfor better or worse.We have introduced awide range of measures to improve thewell-being of all children by working to tacklechild poverty, establishing Sure Start Children’sCentres, and creating the National Academyfor Parenting Professionals. But now we wantto go further. International evidence suggeststhat intensive health-led home visiting duringpregnancy and the first two years of life canradically improve outcomes for both motherand child, particularly in the most at-riskfamilies. So we will:
•• establish 10 health-led parenting supportdemonstration projects from pre-birth toage 2, building in a rigorous evaluation ofdifferent levels of targeted support.Thesewill be based mainly around Sure StartChildren’s Centres; and
•• work with midwives and health visitors toimprove their skills to promote support andintervention during the early years; anddevelop commissioning guidance toencourage the spread of best practicenationally.
1.19 For children and teenagers, thoseparticularly at risk include children in care,teenage parents and those with the lowesteducational achievement, and these groupssignificantly overlap. Every Child Matters istransforming children’s services and bringingmany important innovations.
1.20 However, progress is patchy, and onsome issues, rigorous evidence about whatworks does not always inform how servicesoperate.There is a lack of appropriate data onoutcomes for some groups, hindering servicesfrom identifying those at risk and from
10
Reaching Out: An Action Plan on Social Exclusion
intervening early.There remain shortfalls in theavailability of high-quality services for children,which results in variable and ineffectivepractice, and there are significant barriers tomulti-agency working. Our objective is todeliver more personalised, holistic andevidence-based support to those who need it.Building on the Every Child Matters agenda, theGovernment will:
•• publish a Green Paper in October 2006 onchildren in care, setting out theGovernment’s proposals to transformoutcomes for this high-risk group, includingindividual budget-holding arrangements toensure that every child in care has someonewho understands their needs and has theleverage to secure the right support forthem;
•• publish a revised and updated TeenagePregnancy Strategy with a particular focuson areas where rates have either not fallenappreciably or have risen, including improvedsocial and relationships education; anexpanded media campaign; and betteraccess to contraceptives;
•• launch a series of pilots to test differentapproaches to tackling mental health andconduct disorders in childhood, includingintensive home-based interventions (such asmulti-systemic therapy) which willcomplement the Treatment Foster Carepilots that are already under way; and
•• continue to improve provision and capabilityaround parenting support and training; pilotbudget-holding practitioner models forchildren with additional needs; ensure theseactions are delivering a coherent whole-familyapproach for families at risk.
1.21 Adults living chaotic lives are often incontact with multiple agencies, with eachperson costing statutory services tens ofthousands of pounds every year. Individualagencies sometimes miss those who have
multiple needs, and may fail to look holisticallyat the individual.The Government willtherefore:
•• launch pilots to test the effectiveness ofalternative approaches to improvingoutcomes for people with chaotic lives andmultiple needs, the results of which will feeddirectly into further policy development;
•• accelerate measures to encourageemployment for those suffering from moresevere mental health problems, including theencouragement of individual placement andsupport approaches and anti-stigmaemployer-based campaigns; and
•• publish the Leitch Review later this yearsetting out progress and further measuresto address the poor lifetime prospects ofthose with few qualifications and skills.
Next steps1.22 In the coming months, the Governmentwill complement this Action Plan byimplementing further policies to improveoutcomes and opportunities for sociallyexcluded people.
1.23 The Government will continue aprogramme of active stakeholder engagementand discussion to inform these actions.Stakeholder discussions will also feed into awider 10-year strategic review of thelong-term drivers of social exclusion andgovernment responses.This Action Plan willhelp to frame the Government’s approach totackling disadvantage through theComprehensive Spending Review, which willreport in 2007.
1.24 A progress report on this Action Planwill be published in summer 2007, setting out:progress and early results; the conclusions ofstakeholder discussions; and policy changes andinvestments resulting from the various
11
Chapter 1: Executive summary
government papers and reviews relatingto exclusion that will be published over thecoming year.
1.25 Social exclusion cannot be addressed bygovernment alone. Individuals and the widercommunity, in addition to the private and thirdsectors, all have a role to play. But most of all,people who are suffering social exclusion mustwant progress for themselves and thosearound them. By working together we canensure that even the most excluded have astake in the society and economy oftomorrow by seizing the opportunities that lifein the UK offers today.
12
Reaching Out: An Action Plan on Social Exclusion
Section II: A renewed approachChapter 2:The issue and context
SummaryWe have much to be proud of in the progress that this country has madeover the last decade. Record levels of employment, sustained growth andlow inflation, year-on-year increases in educational attainment andincreases in welfare for vulnerable people have all contributed towards thesignificant falls in poverty we have experienced.
But against this background of success, the persistent and deep-seatedexclusion of a small minority has come to stand out ever moredramatically. The signs of their disadvantage appear early in life, and persistlong into adulthood. This minority may be trapped in a lifetime of povertyand social harm, with the end result that they are unable to help createand share the opportunities that most of us take for granted.
However, within the tragedy and waste of lifetime and inter-generationalexclusion, there is also a message of hope. It is possible, in principle, toidentify those most at risk, and to intervene early, holistically andpersistently, in order to expand opportunity and tackle the most deep-seated forms of exclusion. It is our sustained aspiration that everyoneshould have the opportunity to create and share in the successes of oursociety and economy.
13
Box 2.1: Progress to date: independent assessments“[This Government] has taken poverty and social exclusion very seriously and made genuineprogress in reducing disadvantage, especially among families with children.”
Joseph Rowntree Foundation, 2005
“The package of support for low-income working families with children is now one of themost generous in the world.”
Centre for Analysis of Social Exclusion, 2004
“With the relative poverty line set at 60 per cent of median income, there are now11.4 million individuals in poverty measured after housing costs and 9.2 million measuredbefore housing costs. . . down 2.4 million and 1 million respectively since 1996/97.”
Institute for Fiscal Studies, 2006
14
Reaching Out: An Action Plan on Social Exclusion
1 Office for National Statistics, Monthly Labour Market Statistics2 Department for Education and Skills (DfES) (2004) Five-year Strategy for Children and Learners3 Institute for Fiscal Studies (2006) Poverty and Inequality: 2006. Note that this data also contains a number of students who may under-reporttheir true income.
Progress in extendingprosperity and opportunityto all2.1 This Government has made great progressin tackling poverty and social exclusion andpromoting social justice. The Government hasworked with millions of households to lift themabove the poverty line, and concerted actionon child poverty has dramatically improved thelife chances of many of our children.
2.2 The benefits and opportunities generatedby our successful economy have been sharedby the many and not just by the few. Forexample, there are now 2.5 million morepeople in work than there were in 19971 and
access to higher education has been improvedto the extent that we now have 44 per centof 18–30-year-olds taking this opportunity,compared to 12 per cent of 18–21-year-oldsin 1980.2
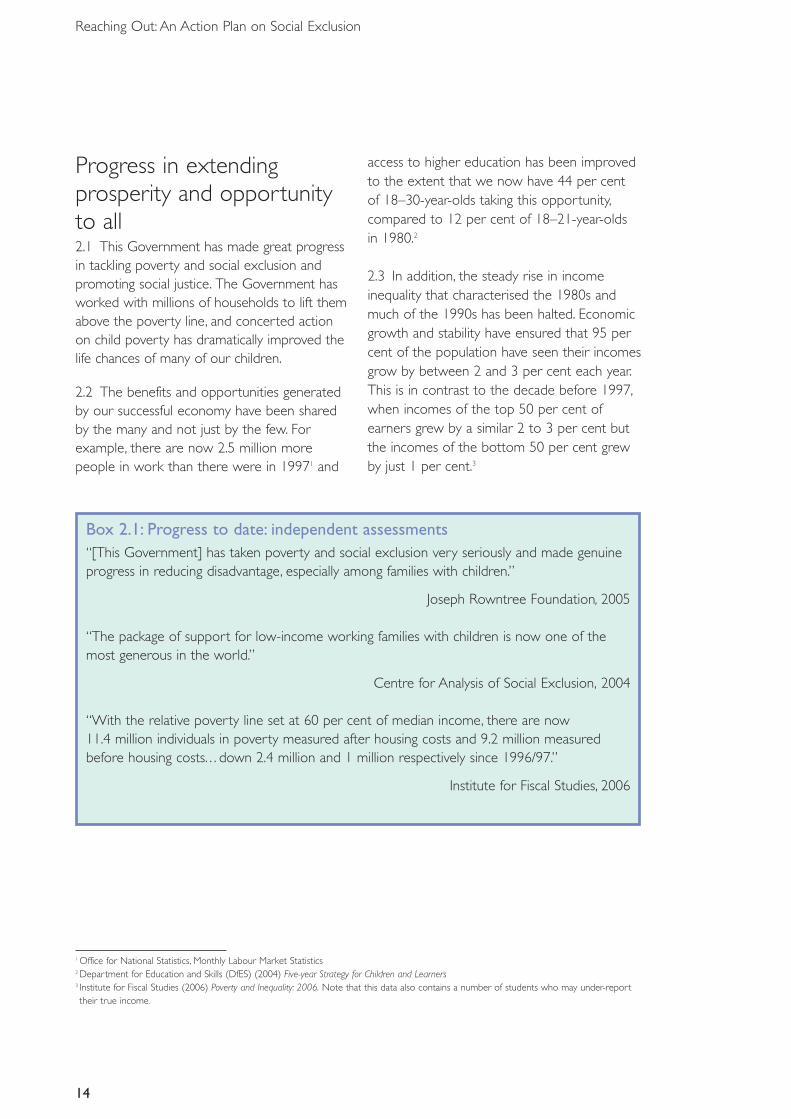
2.3 In addition, the steady rise in incomeinequality that characterised the 1980s andmuch of the 1990s has been halted. Economicgrowth and stability have ensured that 95 percent of the population have seen their incomesgrow by between 2 and 3 per cent each year.This is in contrast to the decade before 1997,when incomes of the top 50 per cent ofearners grew by a similar 2 to 3 per cent butthe incomes of the bottom 50 per cent grewby just 1 per cent.3
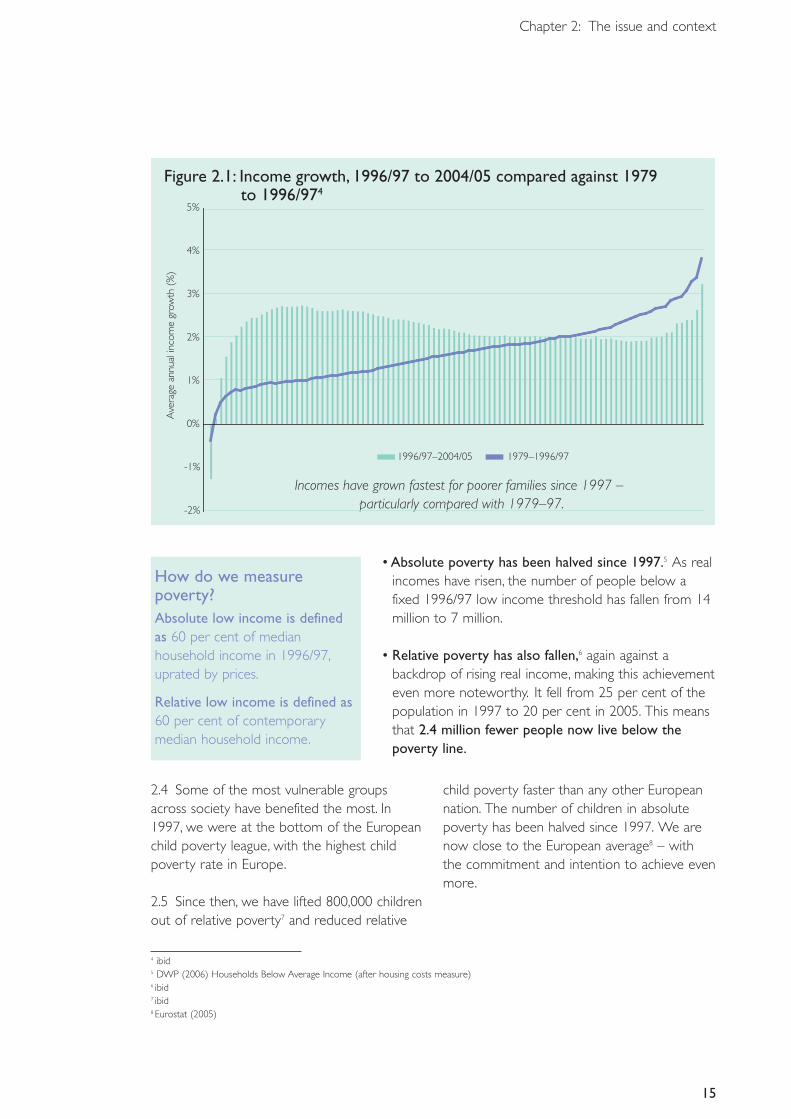
Figure 2.1: Income growth, 1996/97 to 2004/05 compared against 1979 to 1996/974
Incomes have grown fastest for poorer families since 1997 – particularly compared with 1979–97.-2%
-1%
0%
1%
2%
3%
4%
5%
Ave
rage
annu
alin
com
egr
owth
(%)
1996/97–2004/05 1979–1996/97
15
Chapter 2: The issue and context
2.4 Some of the most vulnerable groupsacross society have benefited the most. In1997, we were at the bottom of the Europeanchild poverty league, with the highest childpoverty rate in Europe.
2.5 Since then, we have lifted 800,000 childrenout of relative poverty7 and reduced relative
child poverty faster than any other Europeannation. The number of children in absolutepoverty has been halved since 1997. We arenow close to the European average8 – withthe commitment and intention to achieve evenmore.
4 ibid5 DWP (2006) Households Below Average Income (after housing costs measure)6 ibid7 ibid8 Eurostat (2005)
How do we measurepoverty?Absolute low income is definedas 60 per cent of medianhousehold income in 1996/97,uprated by prices.
Relative low income is defined as60 per cent of contemporarymedian household income.
• Absolute poverty has been halved since 1997.5 As realincomes have risen, the number of people below afixed 1996/97 low income threshold has fallen from 14million to 7 million.
• Relative poverty has also fallen,6 again against abackdrop of rising real income, making this achievementeven more noteworthy. It fell from 25 per cent of thepopulation in 1997 to 20 per cent in 2005. This meansthat 2.4 million fewer people now live below thepoverty line.
16
Reaching Out: An Action Plan on Social Exclusion
The drivers of change2.6 Increased prosperity and falling povertylevels are the result of three key factors:improved economic performance and higheremployment rates; better educationalattainment across all key stages; and increasedwelfare provision for the most vulnerablegroups and families.
• Since 1997, nearly 2.5 million more peoplehave found work,9 boosting the employmentrate to around 70 per cent. And there arenow around 1 million fewer people receivingbenefits.10
• There have been steady improvements ineducational attainment at every key stagesince 1997, with improvements for mostethnic groups and fastest progress in schoolsin the most disadvantaged areas. This hasbeen underpinned by a doubling ofinvestment in our schools and educationsystem since 1997.
• Reforms to the tax and benefits system since1997 mean that families with children will, byOctober 2006, be on average £1,500 a yearbetter off in real terms than they were in1997, with the poorest fifth being on average£3,400 a year better off.11
The results 2.7 Reducing overall levels of poverty has hadreal and concrete impacts on the quality of lifeand well-being of many of the mostdisadvantaged and vulnerable people in society.
• Real-terms increases in the value of the basicstate pension, along with the introduction ofthe Pension Credit, have helped lift over2 million pensioners out of absolute poverty
and 1 million out of relative poverty since1997.12 The end result is that pensionerpoverty has fallen to its lowest level in20 years.
• Between 1996 and 2004, the number ofpeople living in households suffering fromfuel poverty (defined as having to spendover 10 per cent of household income onfuel) fell from 6.5 million to 2 million.13
• Rising incomes among the poorest familieshave meant more spending on essentialgoods for their children – food, clothing,footwear, games and toys. Among thesefamilies, spending on non-essentials such ascigarettes and alcohol has not increased.Instead, disadvantaged parents are usingrising incomes to improve outcomes andprovide greater opportunities for theirchildren.14
2.8 And improvements are apparent in themost deprived areas. There are encouragingsigns that – through a combination of nationalfloor targets, coordinated local action throughlocal strategic partnerships and targetedneighbourhood interventions (such asneighbourhood management) – we arebeginning to turn the tide on the gap betweenthe most disadvantaged areas and the rest.
• The gap between the percentage of pupilsin the 88 most deprived areas and theEngland average achieving five or moreGCSEs at A* to C narrowed from 10.2 to8.1 percentage points between 1997/98 and2002/03.15
• The gap between the overall burglary rate inthe 88 most deprived areas and the Englandaverage reduced from 10.3 to 8.1
9 Office for National Statistics, Monthly Labour Market Statistics10 DWP benefits data11 Budget (2006) HMT12 DWP (2006) Household Below Average Income (after housing costs measure)13 Department of Trade and Industry (DTI) (2006) UK Fuel Poverty Strategy Fourth Annual Progress Report14 Gregg et al (2005) Family Expenditures Post-welfare Reform in the UK: Are Low-income Families Starting to Catch Up? CASE Working Paper 9915 DCLG (2006) Making it Happen in Neighbourhoods.The National Strategy for Neighbourhood Renewal – Four Years On. p.27
17
Chapter 2: The issue and context
percentage points between 1999/00 and2003/04.16
2.9 In addition there is evidence17 that thetargeting of neighbourhood renewal fund(NRF) through Local Strategic Partnerships isleading to improved service delivery, includingmulti-agency working in the mostdisadvantaged communities.
Some left behind2.10 Against this background of millions liftedout of poverty, the highest employment rateson record and year-on-year improvements ineducational attainment, the more modestprogress of a few specific groups in our societystands out dramatically.
2.11 Those on the very lowest incomes haveseen the lowest rates of income growth.Thevery bottom 5 per cent of incomes haveincreased by around 1 per cent per year in realterms between 1996/97 and 2004/05, comparedwith annual increases of between 2 and 3 percent for the rest of the population.18
2.12 Despite improvements in averageeducational attainment, some groups continueto underachieve. For example, 33.3 per cent ofblack Caribbean boys achieved five GCSEs atA* to C compared with a national average of55 per cent.19 In addition, at any one time asmany as 11 per cent of 16–18-year-olds arenot in education, employment or training(NEET).20 This figure has remained broadlystatic for over 10 years.
2.13 With more than 2 million people havingentered the labour market, the employmentrates in almost all sections of society haverisen, including those of physically disabledpeople and lone parents. But there are a fewexceptions to this general trend. For thosewith no qualifications, for example,employment rates have actually decreasedfrom 51.7 per cent in 1997 to 49.6 per cent in2005.21 This partly reflects the characteristics ofthis shrinking group, but it also reflects thechanging nature of our economy and thereduced chances for those with no skills.
2.14 Similarly, while employment rates havebeen rising for those with most forms ofdisability, they have fallen among those withmoderate to severe mental illness from 14 percent in 2000 to 10 per cent in 2005.22
2.15 So while the vast majority have benefitedfrom the increased prosperity and opportunityof the last decade, there are a small minoritywho appear to have benefited less and whostill experience profound exclusion anddiminished life chances, when compared withthe average.The evidence suggests that theseare often the groups and individuals with themost complex and challenging problems.
2.16 Longitudinal surveys – which follow thelife histories of people over time – haverevealed a small proportion of people whoexperience particularly deep and persistentproblems throughout their lifetimes. Forexample, international evidence shows thataround 2.7 per cent of 15-year-olds – or 27 in1,000 – can be described as having multiple
16 ibid p. 2817 DCLG (forthcoming) NRF Impact and Outcome Study: Draft Report18 Institute for Fiscal Studies (2006) Poverty and Inequality: 2006 (note that this data also contains a number of students who may under-report
their true income)19DfES Statistical Release: Achievements at GCSE and equivalents for pupils at the end of key Stage 4 in 2005, for local authorities, by ethnicity20 DfES Statistical Release: Participation in Education,Training and Employment by 16–18-year-olds in England: 2003/200421 Labour Force Survey22 Labour Force Survey
18
Reaching Out: An Action Plan on Social Exclusion
problems, including alcohol and drug misuse,educational failure, contact with the police,early sexual activity and/or mental healthproblems.23 Experiencing a number ofproblems – or multiple disadvantages – canreinforce the barriers to getting ahead andincreases the likelihood of other relatedproblems later in life, contributing to lifetimesof unemployment, offending orinstitutionalisation.
2.17 However, our understanding of the riskand protective factors for later negativeoutcomes is becoming more sophisticated andhas the potential to help us identify warningsigns early.
2.18 We know that children born intodisadvantaged households have a higher
chance of experiencing similar problems totheir parents24 – this is known as the inter-generational cycle of disadvantage. It is apattern seen across many of the most at-riskgroups in our society, including teenageparents, children in care, those with pooreducational attainment and those engaging inanti-social behaviour and offending.
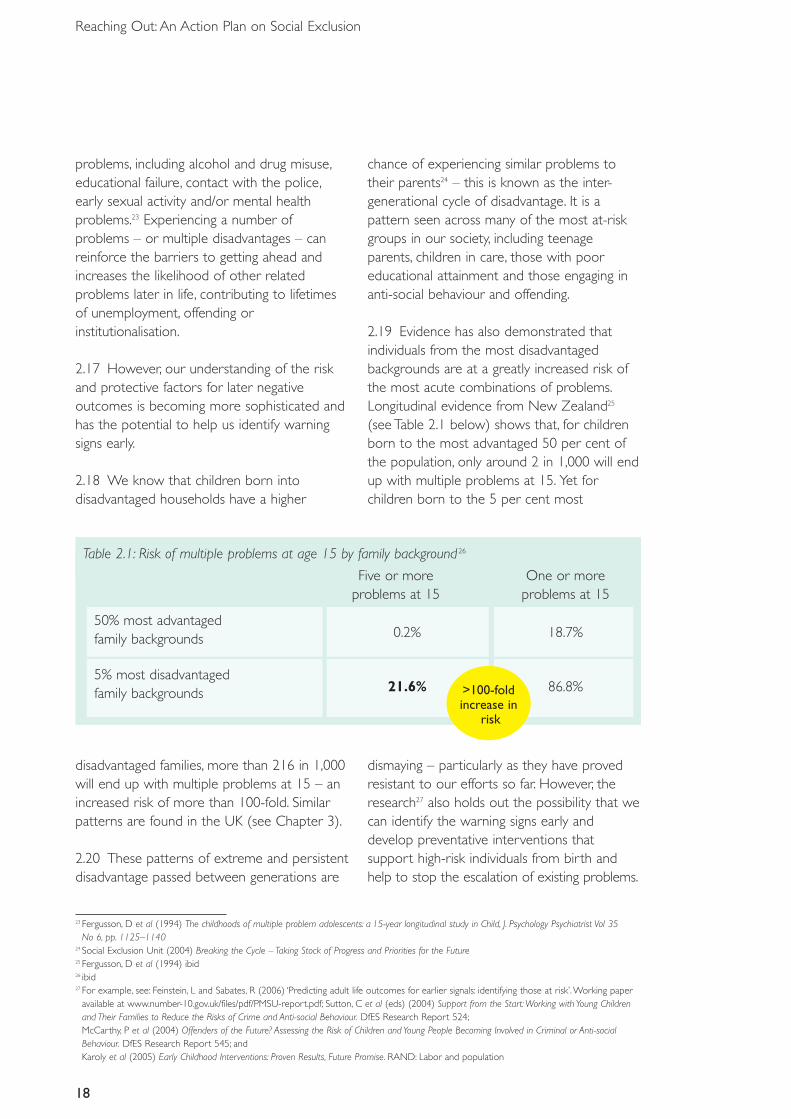
2.19 Evidence has also demonstrated thatindividuals from the most disadvantagedbackgrounds are at a greatly increased risk ofthe most acute combinations of problems.Longitudinal evidence from New Zealand25
(see Table 2.1 below) shows that, for childrenborn to the most advantaged 50 per cent ofthe population, only around 2 in 1,000 will endup with multiple problems at 15. Yet forchildren born to the 5 per cent most
>100-foldincrease in
risk
23 Fergusson, D et al (1994) The childhoods of multiple problem adolescents: a 15-year longitudinal study in Child, J. Psychology Psychiatrist Vol 35No 6, pp. 1125–1140
24 Social Exclusion Unit (2004) Breaking the Cycle – Taking Stock of Progress and Priorities for the Future25 Fergusson, D et al (1994) ibid26 ibid27 For example, see: Feinstein, L and Sabates, R (2006) ‘Predicting adult life outcomes for earlier signals: identifying those at risk’.Working paper
available at www.number-10.gov.uk/files/pdf/PMSU-report.pdf; Sutton, C et al (eds) (2004) Support from the Start:Working with Young Childrenand Their Families to Reduce the Risks of Crime and Anti-social Behaviour. DfES Research Report 524;McCarthy, P et al (2004) Offenders of the Future? Assessing the Risk of Children and Young People Becoming Involved in Criminal or Anti-socialBehaviour. DfES Research Report 545; and Karoly et al (2005) Early Childhood Interventions: Proven Results, Future Promise. RAND: Labor and population
disadvantaged families, more than 216 in 1,000will end up with multiple problems at 15 – anincreased risk of more than 100-fold. Similarpatterns are found in the UK (see Chapter 3).
2.20 These patterns of extreme and persistentdisadvantage passed between generations are
dismaying – particularly as they have provedresistant to our efforts so far. However, theresearch27 also holds out the possibility that wecan identify the warning signs early anddevelop preventative interventions thatsupport high-risk individuals from birth andhelp to stop the escalation of existing problems.
Table 2.1: Risk of multiple problems at age 15 by family background 26
Five or more One or moreproblems at 15 problems at 15
50% most advantaged family backgrounds 0.2% 18.7%
5% most disadvantaged family backgrounds 21.6% 86.8%
19
Chapter 2: The issue and context
Reaching the most excluded2.21 The focus of government efforts over thelast nine years has been about addressing thewidespread poverty and disadvantage that hadcome to mark out the UK over the 1970s and1980s. The increased opportunities that haveresulted from these policies have combinedwith the aspirations and hard work of deprivedfamilies to bring dividends, both in terms oftransformed lives for the previously poor andsocially excluded, and in terms of benefits towider society.
2.22 For example, it is estimated that the2.5 million extra people in work have released
around £5 billion per annum of publicspending for use on other public prioritiessuch as health and education, as well aspersonally benefiting from being included inthe day-to-day life of society.29
2.23 But against this background of success,the relative lack of progress of a small minoritystands out. In 1997, 4.8 million adults sufferedfrom five or more disadvantages. By 2003, thisnumber had dropped by 1.1 million to3.7 million.30 The individuals and families whohave failed to benefit from the improvementsand opportunities available are also those who tend to be caught in the deepest cyclesof deprivation and disadvantage. For this small
Box 2.2: Our approach to preventionPrevention means reducing the risk that individuals or families will experience problems laterin life, and it can also mean preventing existing problems from escalating, or early intervention.
Early intervention to prevent problems can be seen as having two meanings: early in terms ofage or early in terms of the onset of a problem – whatever the age of the individual.
Intervention at an early age – Evidence demonstrates that supporting families and childrenthrough their earliest years can pay dividends in terms of improved outcomes deliveredthrough cost-effective interventions. Research has identified specific factors in the early yearsand through childhood that have marked positive impacts upon a wide range of individualoutcomes that last through adolescence and into adulthood (see Chapter 3). An example isthe Nurse–Family Partnership.28
Interventions at an early age typically focus on promoting protective factors such as betterparenting styles, more access to quality childcare or tackling child poverty.
Intervention at the early stages of onset – We also know that better outcomes result fromintervening at the earliest stage of a particular problem becoming apparent – at the onset.For example, successful approaches to preventing street homelessness rely upon identifyingthe key signs that the individual is at risk of losing a tenancy – such as loss of employment ormental health problems – anticipating the risk of homelessness and then intervening tomaintain the tenancy and address the associated problems.
28 Olds, D (2006) The Nurse-Family Partnership: An evidence based preventive intervention, Infant Mental Health Journal 27, pp. 5–2529 DWP estimate (2006)30 Social Exclusion: the next steps forward. Speech by Rt Hon David Miliband MP, Minister for Communities and Local Government (2005)
20
Reaching Out: An Action Plan on Social Exclusion
minority, the barriers are not only economicbut also social and cultural.These subtlebarriers help to explain why even some of ourmost ambitious programmes aimed at breakingthe cycle of deprivation have had only amodest impact to date on the most excluded.
2.24 Cracking these issues means a stepchange in the way in which central and localgovernment – as well as the community andvoluntary sector – address social exclusion. Inother words, it means focusing on deepexclusion as well as wide exclusion.
2.25 The first step is to dispel the myth that itis not possible to identify and reach thosemost at risk of lifetimes of exclusion.The nextstep is to establish that there are interventionsthat work, and to ensure that these are widelytaken up.
2.26 Thirdly, we must do more to promotemulti-agency working to address multipleproblems. We must ensure that services areincentivised to work around the individual, asopposed to individuals working around theservice. And it must be clear that individualshave a right to take up the opportunities thatare available, but also that alongside rightscome responsibilities. Finally, we must makesure that we do not fail our most vulnerablemembers of society.
2.27 We want everyone to be able to sharein the progress that we have made as a nationover the last decade.This report aims to bethe next step in promoting the ability of allpeople to do so.The following chapter explainsthe guiding principles that will inform ourrenewed focus on social exclusion.
Box 2.3: “Social justice is not simply a moral ideal but an economic necessity… [This] is aplain fact obvious to anyone who has recognised the discouragement, the cynicism and angerwhich seep through the structure of our society, and which make people uneasy even if theyare themselves more successful than others.They are uneasy because they fear for their ownand their children’s future in such a society, and because, whatever their personal prospects,they do not really want to run their lives or their enterprises in a brightly lit and heavilyguarded tent, surrounded by a wasteland of bitterness and disappointment.”
Commission for Social Justice (1994) Social Justice: Strategies for National Renewal
Chapter 3: Guiding principles
SummaryThere are five guiding principles that will mark our approach to peopleexperiencing, or at risk of, severe social exclusion:1. Better identification and early intervention. We will develop and
promote better prediction tools for use on the front line, and will seekto ensure that those identified as being ‘at risk’ are followed up.
2. Identifying what works. A code of practice for high-qualityevaluation, to approve and rate intervention programmes, will bedeveloped. Highly rated programmes, will be given channels to highlightblockages to delivery.We will also strengthen the capability ofcommissioners of services and we will explore the role of a Centre forExcellence in Children’s and Family Services, which would identify,evaluate and disseminate what works.
3. Multi-agency working.We will strengthen the role of Local AreaAgreements, publish information about the cross-agency costs of socialexclusion, and explore how to extend information sharing betweenagencies in relation to the most excluded groups.
4. Personalisation, rights and responsibilities.We will build onexisting pilots and explore budget-holding lead practitioners andbrokers, extending tariffs for delivery of particular outcomes, and willencourage practitioners to agree explicit ‘compacts’ with at-risk familiesand individuals.
5. Supporting achievement and managing underperformance.We will work across government to ensure that the next generationof Public Service Agreements adequately address the needs of the mostexcluded and invite radical proposals from innovative local areas.Wewill explore in the Local Government White Paper how to strengthenperformance management, with a clear ladder of intervention aroundunderachieving provision, while giving effective service providers moreroom to innovate.
21
22
Reaching Out: An Action Plan on Social Exclusion
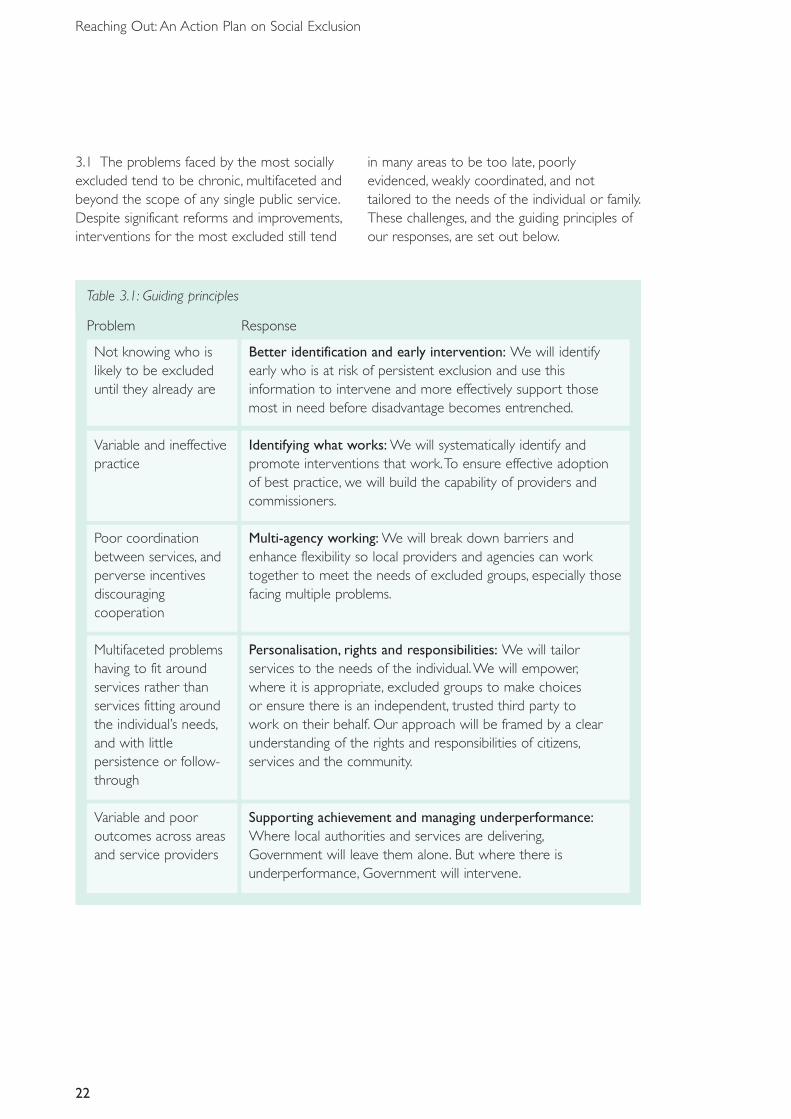
3.1 The problems faced by the most sociallyexcluded tend to be chronic, multifaceted andbeyond the scope of any single public service.Despite significant reforms and improvements,interventions for the most excluded still tend
in many areas to be too late, poorlyevidenced, weakly coordinated, and nottailored to the needs of the individual or family.These challenges, and the guiding principles ofour responses, are set out below.
Table 3.1: Guiding principles
Problem Response
Not knowing who is Better identification and early intervention: We will identify likely to be excluded early who is at risk of persistent exclusion and use this until they already are information to intervene and more effectively support those
most in need before disadvantage becomes entrenched.
Variable and ineffective Identifying what works: We will systematically identify and practice promote interventions that work.To ensure effective adoption
of best practice, we will build the capability of providers andcommissioners.
Poor coordination Multi-agency working: We will break down barriers and between services, and enhance flexibility so local providers and agencies can work perverse incentives together to meet the needs of excluded groups, especially those discouraging facing multiple problems.cooperation
Multifaceted problems Personalisation, rights and responsibilities: We will tailor having to fit around services to the needs of the individual.We will empower,services rather than where it is appropriate, excluded groups to make choices services fitting around or ensure there is an independent, trusted third party to the individual’s needs, work on their behalf. Our approach will be framed by a clear and with little understanding of the rights and responsibilities of citizens,persistence or follow- services and the community.through
Variable and poor Supporting achievement and managing underperformance:outcomes across areas Where local authorities and services are delivering,and service providers Government will leave them alone. But where there is
underperformance, Government will intervene.
23
Chapter 3: Guiding principles
3.2 We spend substantial sums of public moneyon the most excluded, across a range of publicservices.These costs include spending onbenefits, education, the criminal justice system,health and social services and housing.The vastmajority of this spending is directed at sortingout or offsetting problems after they arise, andrelatively little is spent on prevention.TheGovernment will reverse this focus.
3.3 Public services also have considerableinformation about the needs of the mostexcluded, but this is often held by separateorganisations with limited communicationbetween them.The challenge is to ensure thatthe impact of interventions for the mostexcluded is greater than the sum of the parts –the concern is that, for many, it is less.
Box 3.1: James: the financial benefits of early supportive interventionThe story of 15-year-old James, serving his second custodial sentence, is a catalogue of errorsand missed opportunities. His story is not untypical of those of young people at the ‘heavyend’ of the youth justice system.
First, no one listened to James’s mother when she struggled to control his behaviour at home.James was not asked for his views until he was 13 and had already been in a special schoolfor some years.The agencies involved did not communicate well with each other, key peopledid not attend his review meetings and despite the evidence of multiple problems, no onewas allocated to the family as a key worker or took overall charge.
Had things been different, James might have benefited from family support, pre-schooleducation, anger management, learning support and mentoring. If these had been providedfrom the start, and continued throughout James’s teenage years, much of his offending couldhave been avoided.The costs of these support services would have been £42,000 up to theage of 16, compared with the actual costs of £154,000 for the services he did receive,including court appearances and custody. In retrospect, preventative support services wouldhave saved over £112,000, vastly improving the experiences and life chances of James and hisfamily and mitigated the negative effects his offences had on others.
Of course, we do normally have the benefit of hindsight.The scale of any real savings dependscritically on our ability to predict. Nonetheless, the expenditure on James would have paid forthe cost of more than four of the support packages; so as long as our predictions were rightin at least one in four cases, there would have been a net saving.
Audit Commission, Youth Justice 2004
3.4 Although the Government has done a greatdeal to address specific problems such asJames’s – for example through giving additionalfunding to extend programmes such as YouthInclusion and Support Panels (see Box 3.7) theGovernment still does not work in this manner
as well as we could or as routinely as we could.We need to develop an approach where allagencies effectively intervene earlier to preventthe onset of more acute problems, including –but not restricted to – the risk of offending.
24
Reaching Out: An Action Plan on Social Exclusion
3.5 Identifying problems and intervening toprevent their occurrence or escalation is at theheart of the Government’s vision set out inEvery Child Matters.The development ofChildren’s Trusts has enabled good progress tobe made in ensuring that services are bettercoordinated around the needs of the individualand that there are clear lines of accountabilityfor the outcomes of the child.
3.6 Analysis shows that early intervention canbe highly cost-effective31 and that it is moreeffective to spend money during the early yearsrather than the later stages of childhood andteenage years. And the positive impacts ofsuccessful programmes have been shown tolast, thereby reducing the need for later formsof intervention.32
3.7 This is not to say that we should notprovide support at the onset of problems whenever they arise: targeted youth support, forexample, is helping to embed a coordinatedresponse to the onset of problems in theteenage years. But if we are to break theintergenerational cycle of disadvantage, then we
need to provide support as early as possible. Inshort, we are aiming for a more balancedapproach between preventative and remedialsupport.
3.8 In terms of the early identification of risk,there is a substantial and growing body ofevidence on the different factors known toaffect children’s chances of a happy and healthychildhood and of a life free from the prospectof social exclusion.
Risk, protection and resilience3.9 Longitudinal research is helping us tounderstand how risk and protective factorsinfluence the chances of individuals experiencingdamaging and costly problems in the future.33
3.10 In the early years, many of the mostimportant factors relate to the individual child,his or her family background and parenting.When children go to school, other factors suchas experience of education, peer group factorsand the presence of other significant adultfigures become more important.
31 Heckman, J and Masterov, D (2005) Skill Policies for Scotland. NBER Working Paper 1103232 Olds, D ibid33 See Farrington, D P (2003) Key results from the first 40 years of the Cambridge Study in Delinquent Development in T P Thornberry and
M D Krohn (eds), Taking Stock of Delinquency: An Overview of Findings from Contemporary Longitudinal Studies. New York: KluwerAcademic/Plenum
Better identification and early intervention
“We need a greater focus on ensuring children at risk are identified earlier.We need to beable to share information to identify children who require additional support.”
Every Child Matters, 2003
25
Chapter 3: Guiding principles
34 McCarthy, P et al (2004) Offenders of the Future? Assessing the Risk of Children and Young People Becoming Involved in Criminal or AntisocialBehaviour. DfES Research Report 545
35 Howard, S, Dryden, J and Johnson, B (1999) Childhood resilience: review and critique of the literature, Oxford Review of Education, vol. 25,no. 3, p. 308
36 Sutton, C et al (eds) (2004) Support from the Start. DfES Research Report 524
Box 3.2: Risk, protection and resilience34
RiskRisk factors can be described as factors that either singly or in combination have been shownto render children’s failure to thrive more likely.35 Children vary in terms of how they respondto risk and the presence of a risk factor does not automatically mean that someone will goon to experience a negative outcome. Risk and protective factors are context-dependent andvary over time and with different circumstances. Susceptibility to the impact of different riskschanges across the life course, hence key risk factors at age 3 are likely to be very differentfrom risk factors at age 13.36 Multiple risk factors increase the likelihood of poor outcomes,sometimes ‘interacting’ to multiply their overall effect.
ProtectionProtective factors can help children reduce risk.They consist of internal assets and externalstrengths.The more protective factors there are, the greater the likelihood that a child will beresilient to risk. There are four broad types of protective processes, those which: 1) reducethe impact of, or exposure to, risk; 2) reduce chain reactions to negative experiences; 3)promote self-esteem and achievement; and 4) provide positive relationships and newopportunities.
When risk factors in a child’s life are not amenable to change, interventions can help providecompensatory experiences or enhance protective factors. Many of the protective factorsidentified by research relate to the consistency and quality of care and support duringchildhood.
ResilienceThe majority of children with identifiable risk factors do not go on to a life of crime orentrenched exclusion. Despite challenging circumstances, children can develop resilience ofthree main types:
• by achieving positive outcomes even though they are at high risk;• by adapting successfully to stressful situations; and• by recovering quickly from a crisis.
Research studies have delineated the characteristics of resilient and non-resilient children.Children with a stronger sense of attachment to other people, a more positive outlook onlife, more plans for the future and more control over their lives are more likely todemonstrate resilience.
26
Reaching Out: An Action Plan on Social Exclusion
3.11 We have commissioned groundbreakingnew research from the Institute of Education atLondon University.37 The research examines thepotential for different types of indicators topredict later adolescent and adult adverseoutcomes.
3.12 The research is assessing how well we can identify those at risk of adverse outcomeslater in life from information gathered fromdifferent sources (for example, teachers, parentsand the children themselves through differentmethods) at different ages, and in relation torisks from different contexts (family, school,neighbourhoods and so on).
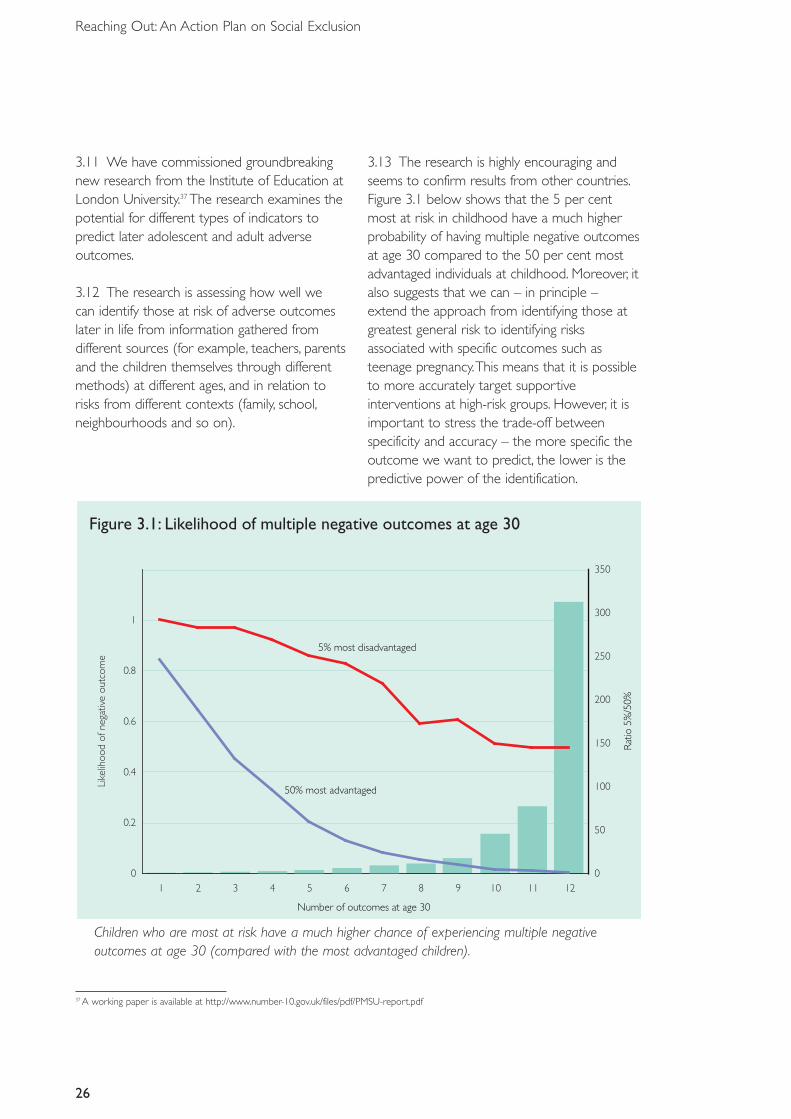
3.13 The research is highly encouraging andseems to confirm results from other countries.Figure 3.1 below shows that the 5 per centmost at risk in childhood have a much higherprobability of having multiple negative outcomesat age 30 compared to the 50 per cent mostadvantaged individuals at childhood. Moreover, italso suggests that we can – in principle –extend the approach from identifying those atgreatest general risk to identifying risksassociated with specific outcomes such asteenage pregnancy.This means that it is possibleto more accurately target supportiveinterventions at high-risk groups. However, it isimportant to stress the trade-off betweenspecificity and accuracy – the more specific theoutcome we want to predict, the lower is thepredictive power of the identification.
37 A working paper is available at http://www.number-10.gov.uk/files/pdf/PMSU-report.pdf
Figure 3.1: Likelihood of multiple negative outcomes at age 30
0
0.2
0.4
0.6
0.8
1
1 2 3 4 5 6 7 8 9 10 11 12
Number of outcomes at age 30
Like
lihoo
dof
nega
tive
outc
ome
0
50
100
150
200
250
300
350
5% most disadvantaged
50% most advantaged
Rat
io5%
/50%
Children who are most at risk have a much higher chance of experiencing multiple negativeoutcomes at age 30 (compared with the most advantaged children).
27
Chapter 3: Guiding principles
3.14 Information and data are crucial formaking predictions about later life outcomes.The research suggests that identification can bemade on the basis of a relatively small number of simple pieces of information, many of whichcan be easily captured or collated by those on the front line and in contact with vulnerable individuals.
3.15 The research also shows that comparinginformation from different areas, such aseducation, family background and health, canprovide more accurate assessments of risk thanhaving more detailed information from just one domain.
3.16 It is important to note that generally thisinformation is already known to serviceproviders.The key is to piece the informationtogether to understand the wider risks andneeds of the individual or family.
3.17 Some of the most powerful predictors arethemselves professional judgements. For
example, one of the best single predictors ofeducational attainment at age 16 – which isitself a key predictor of adult outcomes – isteacher ratings of parental interest at age 10.
3.18 Our objective must therefore be tosystematically build up the knowledge base ofthe key early warning signs of long-termexclusion; ensure that practitioners have accessto this knowledge and the systems in place touse it; and that interventions are targeted onthose most at risk.
3.19 While the report does not identify whichinterventions work best, it can be used to testwhether existing interventions are cost-effectiveand who should be targeted.
3.20 However, we must acknowledge thatpredictions will never be perfect. Some people,despite even the most adverse circumstances,will strive and succeed, while others will faildespite advantage.
Box 3.3: Healthier lives through better predictionAn innovative example of how data can be used to improve the lives of those most at risk ofadverse outcomes and also help save taxpayers’ money is predicting and preventing hospitaladmissions. Hospital admissions are very expensive and can in many cases be prevented ifat-risk individuals are identified early and treated in the community instead. In order to testsuch an approach, Croydon Primary Care Trust (PCT) has commissioned two predictive toolsfrom a consortium led by the King’s Fund.
The basic statistical model is known as PARR and is designed to identify people at risk of multiple unplanned hospital admissions in the forthcoming year. It requires routinecollection of primary care data.The model ranks the population by risk, and those most atrisk are being referred to community care for early, pre-emptive intervention.The model iscurrently being trialled to establish its effectiveness in saving lives, and preventing moreexpensive later care.
www.kingsfund.org.uk/health_topics/patients_at_risk/index.html
28
Reaching Out: An Action Plan on Social Exclusion
3.21 Even if the net is drawn widely, somewho are at risk and who would benefit fromearly intervention will be missed. At the sametime, we must also be cautious about labellingand stigmatisation. In general, where theinterventions are supportive and thedownstream costs of failing to intervene arelarge – such as extra support for the parentsof young children – we should err on the sideof providing better opportunities and support.On the other hand, where interventions aremore punitive, and where the benefits of theintervention are more uncertain, we must bemuch more cautious.
3.22 Finally, a powerful message from the frontline, as well as from the evidence presented inChapter 2, is that persistence is very important.Those experiencing entrenched and deep-seated exclusion are often harder to reach andharder to engage. Indeed, they may not knowhelp is available or may actively decline it. In theface of an unanswered door, letter or call, someof our mainstream services back off or give up.This cannot be an acceptable response to theplight of the most excluded. Where there arereasons for concern, this disengagement mustbe met with a redoubling of efforts to engage –personalisation with persistence.
ACTION 1:The Government will explore the potential of the new research by the Instituteof Education to build an identification tool for practitioners.
ACTION 2: By April 2007, the Government will begin trials of a new evidence-basedassessment tool for use by community midwives and health visitors to improve targeting and support.These will be evaluated as part of the health-led parenting supportdemonstration projects.
ACTION 3:The Government will explore how to ensure that those identified as being at riskare followed up, including at later critical life stages.
Identifying what works3.23 A great deal is known about what worksfor socially excluded people. Indeed, theproposals set out in this document are basedon what we know works.The UK NationalAction Plan on Social Inclusion38 containsinformation on good practice across the UK,linked to the views of a wide range ofstakeholders and to evidence of what worksacross Europe.
3.24 But, currently, there is very little systematicevaluation, collection or dissemination of whatworks in the UK, especially in children’s andsocial services which follow one standard.Thismeans that there can be variable and ineffectivepractice, and we are reliant on frequently over-stretched front-line practitioners taking theinitiative to identify and adopt best practice.
38 This Plan (NAPSI) is submitted to the EU Commission every three years and sets out how each member state is making a decisive impacton the eradication of poverty.The NAPSI will be published in September 2006
29
Chapter 3: Guiding principles
Evaluating what works3.25 There are a number of institutes andorganisations that evaluate and disseminate bestpractice through a number of mechanisms.TheNational Institute for Health and ClinicalExcellence (NICE) is perhaps the best known ofsuch mechanisms. But there are many others,including the DCLG Beacon scheme, run by theImprovement and Development Agency (IDeA),the Social Care Institute of Excellence (SCIE),Research in Practice (RIP), Government SocialResearch (GSR), and also governmentdepartments.
3.26 Currently, these and other organisationsuse a multitude of approaches to identify anddisseminate what works in service provision.Yet,there is no commonly agreed guideline as to
what constitutes a good evaluation – andtherefore a well evidenced programme.Thismakes it difficult for commissioners of servicesin local government, PCTs and elsewhere todetermine the effectiveness of programmes.Developing a common approach to conductingand interpreting evaluations would assistcommissioners in their decision-making andsend a clear signal to programme providers asto what good evaluation should look like.
3.27 Hence, the Social Exclusion Task Force andthe Government Social Research Unit (GSRU)will work with key stakeholders acrossWhitehall and beyond to develop and promotea code of practice and rating for high qualityevaluations.This will be supported by access toexpertise on evaluation and how to rate and
Box 3.4: Early intervention Beacon schemeThe Beacon scheme was set up to disseminate best practice in service delivery across localgovernment. Government ministers award Beacons on specific themes; the decision is basedon recommendations made by an independent advisory panel. Those chosen as Beacons holdthe status for a year, during which they share their experiences through a series of learningexchanges, open days, peer support and other learning activities.
Early intervention featured as one of the themes for the 2006/07 Beacon awards. The earlyintervention theme provides valuable practical examples of how to develop effective andinnovative children’s services that engage all providers and commissioners of services. Theearly intervention award sought to recognise:• the development of common information systems and information-sharing protocols;• the use of cross-partner databases to inform needs analysis and ongoing performance
measurement;• the implementation of common assessment protocols;• the allocation of the lead professional role;• governance in multi-agency teams; and• front-line training in new approaches and the engagement of children, young people, their
families and local communities in all the relevant processes.
The Beacon authorities reflect a range of contexts, including City of York Council, the LondonBorough of Tower Hamlets, Shropshire County Council, the Borough of Telford and Wrekinand Merseyside Fire and Rescue Authority.
30
Reaching Out: An Action Plan on Social Exclusion
approve the effectiveness of programmes. It isenvisaged that such a code might adhere to thefollowing benchmark criteria:
• positive effects that have been shown in atleast one empirical study using a robustexperimental design (such as a randomisedcontrol trial or a quasi-experimentalapproach), and preferably by the results of asystematic review or meta-analysis that hasestablished the balance of evidence;
• replication of the effects in more than onesite and context;
• provision of detail about the variation inoutcomes across different social groups andsocio-economic environments;
• a thorough analysis of the costs and benefitsof the programme; and
• documentation of the approach so that it canbe reliably reproduced.
3.28 In establishing a code of practice forevaluations and consequently a rating ofprogrammes, it will be important to ensure that small providers are not discriminatedagainst and that innovation in service provisionis not stifled.
Disseminating what works3.29 Determining the effectiveness ofintervention programmes through evaluations isa key first step in promoting what works.Disseminating, implementing and managing whatworks according to evidence-based guidelines
are also crucial.This should be done foremostby simplifying the current infrastructure andworking with and strengthening existing bodiessuch as the SCIE, RIP and IDeA. However, theGovernment will also consider the potentialrole of a Centre of Excellence for Children’sand Family Services (CECFS) to identify,evaluate and disseminate best practice forworking with socially excluded groups.TheCECFS should be building on existing bodiessuch as SCIE and a key early priority will be tostrengthen the evidence base on what worksfor children.
3.30 We will also strengthen channels forapproved and rated programmes to be able tohighlight blockages in the system – areas wherethey believe that best practice is not beingprovided, but where it could be done at thesame or lower cost than existing provision.
3.31 Two such channels could be LocalGovernment Overview and ScrutinyCommittees, and the Audit Commission.TheAudit Commission could use feedback fromapproved and rated providers as part of itsassessments of local government performance,helping to serve as an early sign of concern.Further details of how the performanceframework will operate will be explored in theforthcoming Local Government White Paper,and in the Office of the Third Sector plan onpublic service delivery.
ACTION 4:The Social Exclusion Task Force and the Government Social Research Unit willwork with key stakeholders across Whitehall and beyond to develop and promote a code ofpractice and common rating of high quality evaluations of programmes.
In addition, the Government will explore how to simplify the existing infrastructure in relationto spreading best practice. In particular we will consider the case for a Centre of Excellence for Children’s and Family Services, building on or situated within existing organisations.
3.32 Importantly, final discretion over localauthority service design and delivery mustalways remain with democratically electedgovernment at the local or national level.However, a key intent of these proposals will beto incentivise and highlight the use of evidence-based programmes in service delivery, and toincrease the range of evidence-based optionsavailable to commissioners.
Franchising3.33 Finally, as well as more informal forms ofpeer support and exchange, the spread of bestpractice can also be driven by ‘franchising’between local public service providers.Franchising, for example, allows high -performing local authorities (the provider) topartner authorities doing less well (the client) toimprove performance through managementsupport and skills transfer.The high-performinglocal authority’s support and skills are providedin return for an agreed fee, which includesperformance-related payments.The clientauthority, however, retains responsibility fordelivering services.
3.34 This approach has been used to partnerSwindon Borough Council (the client) with KentCounty Council (the provider) to improveSwindon’s social services.This arrangement hashelped Swindon to progress from a zero starrating in its adults’ and children’s social careservices in October 2004, to a two-star rating
by the end of 2006.We are exploring how tobest create a market for franchising and to drawup appropriate guidelines.
Multi-agency working3.35 The cross-cutting nature of socialexclusion means that the problems experiencedby vulnerable groups often reach beyond thescope of any one agency or service provider.
3.36 Joined-up working is vital to ensuring acoherent response to the complex needs ofsocially excluded groups. For example, theCrime and Disorder Act 1998 introduced multi-agency Youth Offending Teams, whose successhas been endorsed by the Audit Commission.Working together to share information at astrategic level (as is happening in Children’sTrusts through the development of children’sand young people’s plans) helps establish ashared understanding of the most pressingissues and the priority groups at a populationlevel.
3.37 This shared understanding is vital inensuring that scarce resources are focused mosteffectively on the people who need them most.Working together at the front line (for example,through multi-agency teams) allowsprofessionals to provide a coordinated andpersonalised response that is based on a fullunderstanding of an individual’s problems.
31
Chapter 3: Guiding principles
ACTION 5:The Government will ensure that approved and rated programmes, be they bythird sector or innovative public or private sector providers offering services to other areas,have clear channels to highlight blockages to best-practice delivery. For example, failures couldbe drawn to the attention of Local Authority Overview and Scrutiny Committees and theAudit Commission.
ACTION 6:The Government will continue to strengthen and support the capability ofcommissioners of services.We are examining how commissioning can be strengthened in central and local government and will publish proposals in due course.
3.38 Increased coordination between services,together with a programme of workforcereform, are helping to create the conditions inwhich practitioners are willing and motivated toshare information with other professionals inthe interests of providing coherent andconsistent support.
3.39 For example, the National OffenderManagement Service has recognised thatreducing re-offending can only be delivered inpartnership. A cross-government delivery boardis overseeing the implementation of theGovernment’s Reducing Re-offending DeliveryPlan and multi-agency partnership boards havebeen established to oversee the delivery ofregional reducing re-offending delivery plans.
Information and communicationtechnologies3.40 A vital tool of successful multi-agencyworking is the use of information andcommunication technologies (ICT).These havehelped to increase efficiency and productivity inthe private sector for some years. While moreand more public sector services are using ICTto improve service delivery, the potential existsto go further.
Overcoming barriers 3.41 However, there are a number of statutoryand cultural barriers that can inhibit agenciesworking together.These include:
• cultural barriers, and occasionally statutorybarriers, to the sharing of information;
• non-aligned geographical boundaries betweenservice providers or commissioners;
• different objectives and values; and• separate budget problems, where one service
provider incurs the cost of the possibleintervention, while another benefits fromthe saving.
3.42 LAAs are a key mechanism forencouraging joined-up agency working at a locallevel.Through these agreements, centralgovernment departments and local serviceproviders agree a number of key outcomes andtargets set in the local context.They help toclarify priorities and reduce the overall burdenof reporting.They are of growing importance asa mechanism for an increasing number of policyareas, but are of particular importance in thedelivery of cross-cutting issues, such as the social exclusion agenda.
32
Reaching Out: An Action Plan on Social Exclusion
Box 3.5:The Common Assessment Framework (CAF)39
The purpose of the CAF is to help practitioners assess children’s additional needs for servicesearlier and more effectively, develop a common understanding of those needs, and agree aprocess for working together to meet them.The aim is to provide better services earlier, andwithout the need for the family to repeat their story for a number of different, overlappingassessments. As such, early common assessment is part of the Government’s strategy to shiftthe focus from dealing with the consequences of difficulties in children’s lives to preventingthings from going wrong in the first place. Some common assessments might result in theidentification of a lead professional who will co-ordinate the actions set out in the assessment.
39 Brandon, M et al (2006) Evaluating the Common Assessment Framework and Lead Professional Guidance and Implementation. DfES ResearchReport 740
33
Chapter 3: Guiding principles
Box 3.6: Better delivery through digital technologyThe potential for digital information and communication technologies (ICT) to help make adifference to the lives and life chances of socially excluded people has so far been largelyunexplored and therefore unexploited.
Significant benefits arise from a variety of opportunities, and an awareness of the potential ofICT opens up a wider range of policy interventions to tackle emerging problems. Existingservices can be enhanced by adding a digital element, through facilitating better informationsharing, increasing accessibility and enlarging capacity and geographical reach – for substancemisusers, web-based support may provide anonymity, access in the middle of the night, andencourage the seeking of help earlier in the addiction cycle than the prospect of a personalvisit to a possibly distant centre (also, the age group likely to develop problems is very familiarwith ICT).40
Major initiatives launched by the Government will start to make a difference.
• The Digital Challenge will fund a world-leading example of a digital community, focusing onbenefiting those at risk of social exclusion.
• A Cabinet committee is addressing the barriers to data sharing.• Programmes such as PCs for Pupils will provide laptops and broadband access to pupils
who would not have the means to get them otherwise.
In addition, from October 2006, £2 million of grant funding will be available to fund ‘socialimpact demonstrators’ in UK online centres.These projects will explore the power ofsupported internet access to develop confidence and skills among people from sociallyexcluded groups, such as adults with mental health problems and families at risk, as well asolder people.The projects will involve excluded people in targeted activities based on whatthey say they need. UK online centres will support participants to become self-sufficient usersof online government services and will explore how the internet can motivate individuals tochange their lives.
But more needs to be done to explore how ICT can address the basic needs of thedisadvantaged.To develop this unexploited potential, the Government has set up the DigitalInclusion Team, overseen by DCLG, which will also take forward the findings of the SocialExclusion Unit report, Inclusion through Innovation, published in 2005.
40 Stonebridge A (2006) Closing the distance RSA Journal
3.43 Local service providers are represented inthe negotiation of LAAs by the upper-tier localauthority and other members of Local StrategicPartnerships (LSPs). LSPs bring together all thekey commissioners and providers of servicesand other partners in a local area.
3.44 The Government has already consultedon new proposals to strengthen cross-agencyworking, through strengthening LSPs.Theconsultation proposed underpinning thepartnerships with a duty to cooperate placedon key local service providers to produce andimplement the Community Strategy and LAA.These measures have significant potential tohelp cross-agency working for the mostexcluded, and have gained broad support.
3.45 Downstream costs may be picked up by acompletely different service to the one withresponsibility for providing the intervention inthe first place. For example, responsibility forimproving the educational attainment of a child
diagnosed with a conduct disorder lies with thelocal education authority, but the costs of failuretend to be picked up by the criminal justicesystem, Jobcentre Plus and the health service.
3.46 Making these downstream costs moretransparent and available to local and centralcommissioners of services, possibly coordinatedthrough Local Strategic Partnerships, couldprove a powerful tool in promoting improvedcross-agency working and provision.
3.47 Such information can help focus minds onearlier interventions, and could help LocalStrategic Partnerships strike innovative dealsacross providers and with central governmentto improve outcomes and reduce total costs tosociety. For example, information aboutdownstream costs borne by the criminal justicesystem within an area could help provide thebasis for an agreement between a centralgovernment body and a local partner, wherethe local partner provides enhanced education,
34
Reaching Out: An Action Plan on Social Exclusion
Box 3.7: Multi-agency working to stop youth offendingA good example of joined-up working is the Youth Inclusion and Support Panels (YISPs)which are multi-agency identification and planning groups that seek to prevent offending andanti-social behaviour by offering voluntary support to high-risk 8–13-year-olds and theirfamilies.The YISPs provide young people with key worker support, mentors, access todiversionary activities and parenting programmes.The multi-agency approach secures acommitment from each of the panel members to provide suitable resources.
There are currently 220 YISPs across England and Wales. In Sheffield, for example, the YISPincludes representatives from the education department, social services, the youth offendingteam, the police, housing services, Child and Adolescent Mental Health Services (CAMHS),Supporting Others through Volunteer Action (SOVA) and Connexions.The project also haslinks with agencies including the Sheffield Homes Anti-Social Behaviour Team, the HousingHigh Support Service, the SOVA Mentoring Scheme and the Local Education Authority (LEA)Inclusion Centres.
As SOVA is the YISP’s voluntary sector partner, each young person has access to a volunteermentor as part of his or her integrated support plan.The project also has a close relationshipwith Positive Activities for Young People (PAYP), ensuring guaranteed entry into their activitiesfor YISP young people and a role in the planning of PAYP schemes.
training and support to at-risk young men inreturn for financial incentives from the centre.
Personalisation, rights andresponsibilities3.48 Personalisation has been a key theme ofpublic service reform and improvement overrecent years in universal services, with personalhealth plans being one such example. Individuals– rightly – increasingly expect and demandservice provision that is tailored to theirparticular needs, rather than a generic servicethat they must fit into.
3.49 Because the most excluded people tendto experience multifaceted problems, there is aparticularly powerful case for personalisation,with tailored solutions and support.
3.50 The delivery of such support is mademuch easier by strong patterns of cross-agencyworking on the ground, in turn supported bycross-agency working at the strategic level (seeabove). For example, in a number of areascross-agency assessment or practitioner boardsmeet regularly – either formally or informally –to discuss their most complex cases and to
compare notes and coordinate actions. In manycases, a lead practitioner is agreed who canthen work with and coordinate other agenciesto provide timely and appropriate interventions.A good example is anti-social behaviourcoordinators.
3.51 Personalisation of services can beexpressed in other ways. For example, servicecommissioners can commission innovativeprovision designed specifically to provide awrap-around service for a particular clientgroup. Specialist facilities for children in care thatprovide education, counselling and other formsof nurturing and support are a familiar example.Intensive family support programmes, such asthose being promoted by the Respect ActionPlan, are another (see Box 3.10).
Individual budgets3.52 Another powerful approach topersonalisation is put the citizen in the role ofday-to-day commissioner of his or her ownservice provision, notably through the use ofindividual budgets, which enable a transparentallocation of resources (in cash or a notionalsum) based on an assessment need.
35
Chapter 3: Guiding principles
ACTION 7:The Government will strengthen the role of Local Area Agreements in theforthcoming Local Government White Paper, with the Social Exclusion Task Force workingclosely with DCLG and other departments to ensure that these changes will help driveforward improved multi-agency working around the most socially excluded.
ACTION 8:The Government will promote increased transparency of the downstream costsassociated with social exclusion.Wherever possible, this will be done by publishing simple,area-based information about per capita spending on key costs.This information can then beused by local service providers to strike innovative deals for better, and more cost-effective,service provision.
ACTION 9:The Government will explore how to extend data sharing in relation to the mostexcluded or at-risk groups, including any additional powers that may be necessary.
3.53 Recent pilots in social care illustrate thepotential of individual budgets to empowerusers and to personalise service provision.Individuals with care needs, or their leadprofessionals, can use the budgets to buy abespoke care package that meets their needsand preferences much better than existingprovision.
3.54 Individuals have used the budgets to buymore informal forms of care, and to ensure thatthe care is provided at a time that is moreconvenient for them. In short, the key advantagethat a budget-holding commissioner has over,say, a lead professional, is that with the budgetcomes the power to choose and shape theservice provision directly and thus driveimproved performance by service providers.
3.55 Individual budgets are currently beingpiloted in 13 local authorities and bring togetherresources from six different streams.The resultsof the pilots are expected in 2008, and willdetermine whether individual budgets are rolledout on a national level.
The lead professional3.56 As part of the move towards integratedchildren’s services, DfES piloted the ‘leadprofessional’ role in 2005/06. Following thepilots, DfES issued guidance in 2006 setting outthe key responsibilities of the lead professionaland outlining the skills and knowledge requiredfor that role.
3.57 DfES is now piloting a furtherdevelopment of the lead professional concept –the budget-holding lead professional. In this pilotthe lead professional holds all or some of thebudgets required to deliver publicly fundedservices for children with additional needs.
3.58 A key problem in relation to someexcluded groups is that they may be unable orunsuited to take responsibility for their ownbudget. In such instances, it may be moreappropriate to consider a brokering modelwhere a lead professional holds the budget onbehalf of the client. However, it should still beexpected that the broker – like a trustee – willact in the best interests of the client and take
36
Reaching Out: An Action Plan on Social Exclusion
Box 3.8: Individual budgets, the potential – Anna’s storyAnna receives support from a number of different agencies for her mobility-limiting disabilityin the form of an individual budget. Her ‘budget’ includes the cash equivalent of council-provided social care services, and cash transfers from the Independent Living Fund, theDisabled Facilities Grant and Access to Work. If Anna felt she needed it, she could havesupport from an advocate, or family and friends.
Having these resources together in one budget allows Anna to spend the money on theservices she needs the most, in a way that best meets her needs. Before Anna had anindividual budget she was reliant on social services to help her get ready for the day, but theearliest they could get to Anna was at 9.30am because of their shift patterns.This preventedAnna from returning to work as she was unable to get there before 11am. Now that Annacan employ her own care assistant she can purchase support from whoever she wants andarrange this support around her working hours, allowing her to return to work. Anna’s self-esteem and quality of life have improved since she has been able to organise her own careand return to work, and she has felt greatly empowered by this process.
their wishes fully into account. For example, fora child in care, the broker should seek to takeinto account the desires and needs of the childor young person, be that to remain in the area,go into a residential facility or into fostering.
3.59 Although the basic idea is simple,formidable barriers exist to moving to modelsof budget-holding lead practitioners or brokers.A key step in making it work is that individualservices have to make an assessment of thelikely spend on a given individual, linked to anestimate of what outcome this should deliver.Careful consideration also needs to be given toany additional bureaucracy that may be createdby a budget-holding lead professional, asopposed to the simpler lead practitioner model.
Payment for outcomes3.60 A complementary route to personalisationis where service commissioners or providersoffer a specific benefit or tariff, paid to theservice provider, that can be combined withother kinds of benefit or tariffs by the user orbroker. For example, in relation to employmentsupport we are moving to a model of providers being paid by results for taking thosecoming on to Incapacity Benefits back into thelabour market.
3.61 This shift towards paying providers basedon the outcomes they achieve for their clients,rather than the number of clients they areproviding services for, is a significant change andcould be expanded in the future to furtherpersonalise services around the individual. Forexample, the amount paid could reflect thedifficulty in achieving an outcome for theindividual concerned, recognising factors such asthe length of time they have been claimingbenefits, or the severity of a disability.
3.62 As the sophistication of the approachgrows, tariffs could increasingly reflect thepotential savings to society of the work-placement. If this approach is more widelyadopted by other services, it will provide anexciting opportunity to piece together budgetsto deliver bespoke services for the mostexcluded individuals.
Engagement3.63 While advocacy is an important hurdle,engagement of the most excluded is even morecrucial. Practitioners have repeatedly made thecase that there are particular windows ofopportunity – ‘fateful moments’ – when peopleare more likely to engage with services. Forexample, the birth of a child or the death of apartner are key moments when individuals aremore open to seek support and advice. Hence,personalisation of services for the mostexcluded may also mean seeking the bestmoment for support.
3.64 Who offers the support is also important.A particular strength of third sectororganisations is the high level of trust theyattract in relation to the most excluded.Thestrong focus of these providers on improvingsocial outcomes sends an important signal toservice users, allowing providers to engage withhard-to-reach groups that may distrust statutory services.
37
Chapter 3: Guiding principles
Rights and responsibilities3.65 An underlying theme of thepersonalisation agenda is that there should be a clear division of rights and responsibilitiesbetween the citizen, service provider and community.
3.66 The Government sees it as a key priorityto provide support to create opportunities forthe most excluded. If these opportunities areto be realised then they need to work withthe aspirations of disadvantaged individuals.However, the flip-side to this support is that, asfar as possible, individuals need to share andtake responsibility themselves, and particularlywhere their actions have an impact on thosearound them. For example, the parent of anat-risk child should be given support, but it is
also incumbent on them to take this support.This approach is illustrated by intensive familysupport projects – a highly personalisedapproach, but one that requires a clear senseof personal responsibility on the part of theadults involved, with clear consequences ifthose responsibilities are not met.
3.67 The Government’s New Dealprogrammes also illustrate this approach.Theseprogrammes provide an active service withtailored support to help people back intowork, matched by an obligation for people todo everything possible to help themselves.
3.68 And it appears to be working. Recentevaluative research shows that a pilotprogramme extending obligations to older
38
Reaching Out: An Action Plan on Social Exclusion
Box 3.9: Building expertise in ‘day-to-day’ commissioning – a gap?Ongoing reforms have moved public service providers in the direction of being strategiccommissioners of services, rather than necessarily being direct providers of services. Forexample, many local authorities now purchase a mixture of in-house, third sector and privatesector provision for children in care.
It is arguable that there is a neglected ‘middle’ in the service delivery chain around day-to-daybrokering of services, and that this particularly affects the most socially excluded. For example,there is typically a large gap between a director of children’s services and the providers whoare offering education, fostering and residential care for the several hundred children in theircare – let alone the many other children who could be considered at risk.While the directorof children’s services commissioning team may have a number of choices in terms of directprovision, there are currently very few providers who are able to take on the day-to-daybrokering or purchasing of service provision.
One innovative local authority has sought to address this issue by asking senior staff to eachtake a personal interest in a small number of children in care – to take on the role normallyadopted by a parent.This was felt to be an extremely effective way of developing a personalrelationship and improving outcomes. However, they also found that there were limits to thecapacity of staff to take on this role.
In Oregon, public service commissioners employ brokers to purchase tailored provision forpeople with disabilities. It may be that this is a gap in service provision that could be usefullyfilled with an active partnership between third sector providers and local and nationalgovernment.
workers – a particularly disadvantaged group –was effective in improving employmentoutcomes.Those mandated to undertake theIntensive Activity Period of New Deal 25 plus(which at present is voluntary for olderworkers and provides a variety of assistancelasting 13 to 52 weeks) were much more likelyto be in unsubsidised employment within ayear of entering the programme (29.8 percent), than those in a control group who werenot mandated (23.4 per cent).41
3.69 A focus on the rights and responsibilitiesof government and citizens also underpins theGovernment’s Respect Action Plan, and inongoing developments since. For example, on5 June 2006 the Government announced apilot scheme to ensure that people who areevicted as a result of their anti-social behaviour
undertake rehabilitation, or risk sanctions ontheir housing benefit.This measure is includedin the Welfare Reform Bill.
3.70 In addition, the DCA and CommunityLegal Service (CLS) play a key role in ensuringpeople understand their legal rights andresponsibilities, and how to exercise them.Evidence42 suggests that the provision of goodearly advice services prevents relatively simplecivil legal issues spiralling into more serious(and numerous) problems and can preventpeople tipping into social exclusion and helpthem move out of it.
3.71 Increasingly, service providers are seekingto make the compact between serviceprovision and citizen more explicit. Forexample, many schools are introducing
39
Chapter 3: Guiding principles
41 Dorsett, R and Speckesser, S (2006) Mandating IAP for Older New Dealers: An Interim Report of the Quantitative Evaluation. DWP ResearchReport 362
42 Pleasance, P (2006) Courses of Action: Civil Law and Social Justice, 2nd edn
Box 3.10: Family Intervention ProjectsFamily Intervention Projects provide holistic support designed to target some of the mostdisadvantaged and problematic families and improve their behaviour and deliver otheroutcomes. Family involvement in the projects is typically triggered by major problems thatmay otherwise lead to children being brought into care, or the family being evicted fordisruptive or anti-social behaviour. In around 40 per cent of families, one of the parents isfound to have significant and untreated mental health problems.
Interventions vary in intensity, partly reflecting the severity of the problems involved. Theserange from home visits and coordination of different service interventions, to full residentialinterventions where the family lives in adapted accommodation with 24-hour supervision andsupport, such as that pioneered in the ‘Dundee project’, commissioned by a local authoritybut delivered by NCH, a children’s charity, a third sector provider. Despite the relativeexpense of Family Intervention Projects, they have been found to be highly cost-effective aswell as improving outcomes for the families and communities involved.
The Government is on track to deliver the commitments it made in the Respect Action Planto roll out 50 Family Intervention Projects by the end of the year, which will deliver tailoredaccess to parenting provision, health and employment services for an estimated 1,000 familiesa year by mid-2007.
pupil–parent ‘contracts’ and these are also usedin relation to Educational MaintenanceAllowances. Even where these contracts arenot legally binding, they can have a powerfuleffect by simply making explicit what isexpected of each party involved.
3.72 Generally, the most effective contractsare personal to the individual or family, albeitwithin a common framework of expectancies.The Social Exclusion Task Force will seek toencourage and extend this approach.
40
Reaching Out: An Action Plan on Social Exclusion
ACTION 10: Using the lessons from the pilots on budget-holding lead professionals, we willexplore whether, and how, to extend the funds held by lead professionals. In particular we willconsider how portions of budgets used for mainstream services could be applied to leadprofessionals’ budgets.
ACTION 11:The Government will explore extending tariffs, paid to service providers andreflecting social costs, for delivering particular outcomes in relation to those with multipleproblems and at risk of a lifetime of exclusion.
ACTION 12:The Government will continue to actively encourage a rights and responsibilitiesapproach to service delivery, encouraging service providers, individual brokers and leadpractitioners to agree clear and explicit divisions of responsibility with clients.
Supporting achievement andmanaging underperformance3.73 The Government’s approach to drivingimprovement in public service delivery hasgradually evolved from targets twinned withinvestment, to one that is supplemented by arange of more bottom-up and peer-drivenpressures to improve. Essentially, the approachcan be boiled down to the following: if you aredelivering, the Government will highlight yourachievements for others to follow, butotherwise leave you alone; but if you are failing,the Government will implement a ladder ofintervention to foster improvement andempower service users to deliver betterperformance.
3.74 Indeed, the Government invites andencourages local areas to come forward with
innovative and radical proposals such aspooled budgets and payment by results forprovision around those most at risk. In turn, wewill work to remove barriers to match thisambition – challenge us!
Clarity about targets3.75 Clarity about national and local prioritiesis a prerequisite for focusing efforts and alsomaking it possible to identify where there isfailure in delivery relative to our aspirations.The Comprehensive Spending Review to beannounced in summer 2007 will determine arevised set of national priority outcomesarticulated through the next generation ofnational Public Service Agreements. And theLocal Government White Paper, due to bepublished in autumn 2006, will consider howto further improve the delivery of national andlocal service priorities.
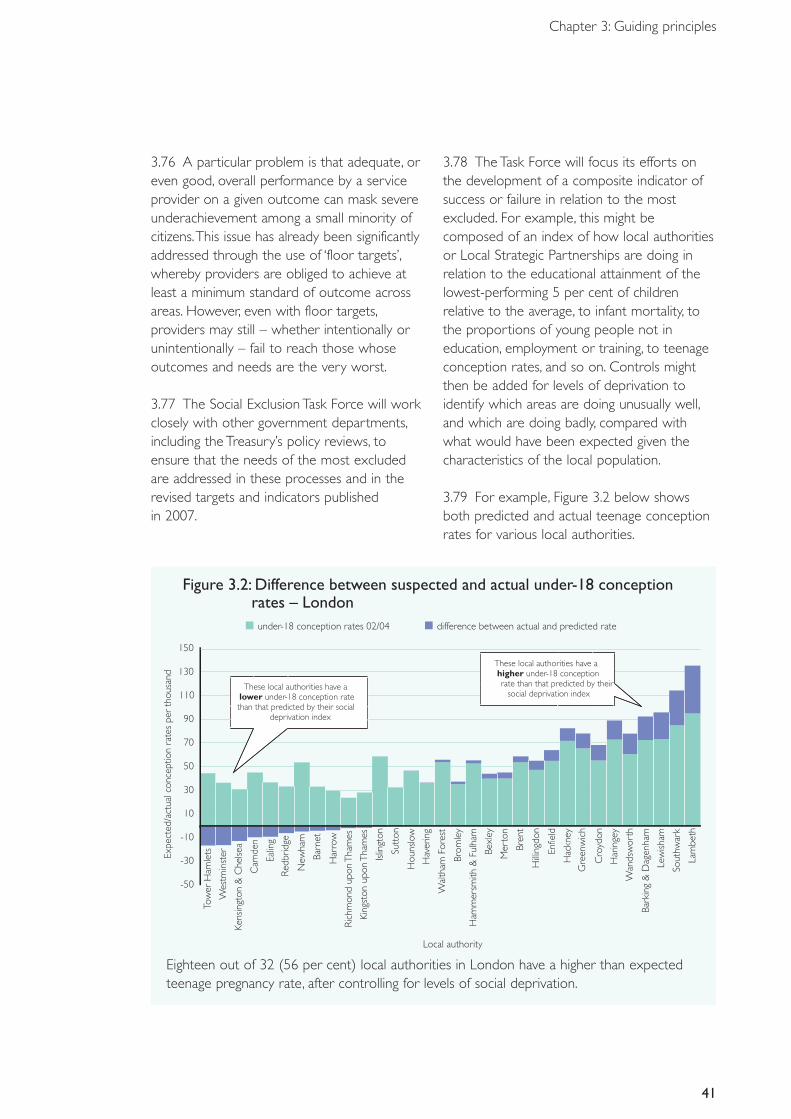
3.76 A particular problem is that adequate, oreven good, overall performance by a serviceprovider on a given outcome can mask severeunderachievement among a small minority ofcitizens.This issue has already been significantlyaddressed through the use of ‘floor targets’,whereby providers are obliged to achieve atleast a minimum standard of outcome acrossareas. However, even with floor targets,providers may still – whether intentionally orunintentionally – fail to reach those whoseoutcomes and needs are the very worst.
3.77 The Social Exclusion Task Force will workclosely with other government departments,including the Treasury’s policy reviews, toensure that the needs of the most excludedare addressed in these processes and in therevised targets and indicators published in 2007.
3.78 The Task Force will focus its efforts onthe development of a composite indicator ofsuccess or failure in relation to the mostexcluded. For example, this might becomposed of an index of how local authoritiesor Local Strategic Partnerships are doing inrelation to the educational attainment of thelowest-performing 5 per cent of childrenrelative to the average, to infant mortality, tothe proportions of young people not ineducation, employment or training, to teenageconception rates, and so on. Controls mightthen be added for levels of deprivation toidentify which areas are doing unusually well,and which are doing badly, compared withwhat would have been expected given thecharacteristics of the local population.
3.79 For example, Figure 3.2 below showsboth predicted and actual teenage conceptionrates for various local authorities.
41
Chapter 3: Guiding principles
Figure 3.2: Difference between suspected and actual under-18 conception rates – London
-50
-30
-10
10
Local authority
Expe
cted
/act
ualc
once
ptio
nra
tes
per
thou
sand
Tow
erH
amle
ts
Wes
tmin
ster
Kens
ingt
on&
Che
lsea
Cam
den
Ealin
g
Red
brid
ge
New
ham
Barn
et
Har
row
Ric
hmon
dup
onT
ham
es
King
ston
upon
Tha
mes
Islin
gton
Sutt
on
Hou
nslo
w
Hav
erin
g
Wal
tham
Fore
st
Brom
ley
Ham
mer
smith
&Fu
lham
Bexl
ey
Mer
ton
Bren
t
Hill
ingd
on
Enfie
ld
Hac
kney
Gre
enw
ich
Cro
ydon
Har
inge
y
Wan
dsw
orth
Bark
ing
&D
agen
ham
Lew
isham
Sout
hwar
k
Lam
beth
30
50
70
90
110
130
150
under-18 conception rates 02/04 difference between actual and predicted rate
These local authorities have alower under-18 conception rate than that predicted by their social
deprivation index
These local authorities have a higher under-18 conception rate than that predicted by their
social deprivation index
Eighteen out of 32 (56 per cent) local authorities in London have a higher than expectedteenage pregnancy rate, after controlling for levels of social deprivation.
Intervention in cases of failure3.80 The Government’s aim is to create thecircumstances for local authorities and otherlocal service providers to deliver excellentservices – including services relating to social exclusion. It is nevertheless essential to have measures in place to ensure thatunderperformance is detected early, thatserious failure is prevented and that significantproblems are dealt with swiftly and effectivelywhere they do arise.
3.81 The Local Government White Paper willexplore the performance framework for localauthorities working alone and in partnership.This work will include looking at measures todeal with problems or failure to deliver inrelation to social exclusion, or indeed anyother priority outcome. A similar approach willbe detailed in the forthcoming Green Paperon children in care.
3.82 Where local service providers areunderperforming in relation to children at riskor the most excluded adults, an interventionregime will kick in. This will be tailored to thenature of the service failure and will take toughaction where services are failing. The length ofthe intervention will vary with the degree ofunderperformance and necessary support,but ultimately the intention will be to buildcapability at the local level and then to step back.
3.83 Interventions for the socially excludedwill be consistent with the guiding principlesreferred to earlier in this chapter, such as moreeffective commissioning, contracting out, andthe use of individual budgets whereappropriate.
42
Reaching Out: An Action Plan on Social Exclusion
ACTION 13:The Task Force will work closely with the Treasury and other governmentdepartments to ensure that the next generation of Public Service Agreements address theunique challenges of the most socially excluded.
ACTION 14:The Government will explore how to strengthen our performance managementregime, with a clear ladder of intervention for the most excluded around underperformingprovision, while leaving good local statutory services alone.The forthcoming LocalGovernment White Paper will consider how the local government performance frameworkmight evolve to continue to drive genuine service improvements, and how to deal with casesof underperformance.
ACTION 15:The Task Force will explore alternative composite measures of social exclusionthat can be used by the Government to monitor progress and to focus targeted interventionand support.
Conclusion 3.84 The multiple and entrenched problemsfaced by the most excluded present aformidable challenge to public services.Yet thepotential prize is great – better and socially justoutcomes for the most excluded, alongsidefewer long-term harm and costs for the rest ofthe community.
3.85 The ongoing programme of publicservice reform offers improved interventionsaround the most excluded, as well as for thegeneral population. But the addedcomplications of the number of agenciesinvolved in the lives of the most excluded, thesmall absolute numbers of individualsconcerned and the separation betweeninvestment and return (both in time andacross agencies) all mean that special attentionand action are needed.
3.86 An effective response to the plight of themost excluded requires innovation inidentification and support, the structure of theworkforce, the application of best practice andthe incentives and system design itself.
3.87 These challenges and implied reforms areprofound, and will not be resolved by thisdocument alone. But the thinking presentedhere offers a clear direction of travel that theGovernment will be pursuing in the context of the coming Comprehensive SpendingReview and forthcoming publications such asthe Local Government White Paper, revisedcommissioning guidance and incapacity benefitsreforms.
3.88 This chapter has set out theGovernment’s renewed approach to tacklingsocial exclusion, based on a strongunderstanding of the current problems andwhat can be done about them. Section IIIoutlines how these principles will be applied orpiloted for excluded groups throughout anindividual’s lifetime – during the Early Years, theChildhood Years and the Adult Years.Implementing more focused and immediateinterventions will supplement and informdeeper systemic reform.
43
Chapter 3: Guiding principles

Section III: A lifetime approachChapter 4: Early Years
SummaryPregnancy and the first few years of life are crucial. Intensive health-ledhome-visiting during pregnancy and the first two years of life can radicallyimprove outcomes for both mother and child, particularly in the most at-risk families.The Government will therefore:
• establish 10 health-led parenting support demonstration projects frompre-birth to age 2, building in a rigorous evaluation of targeted support.These health service demonstration projects will mainly be based aroundSure Start Children’s Centres; and
• support the upskilling of midwives and health visitors to supportearly-years interventions, and develop commissioning guidance toencourage the spread of best practice nationally.
45
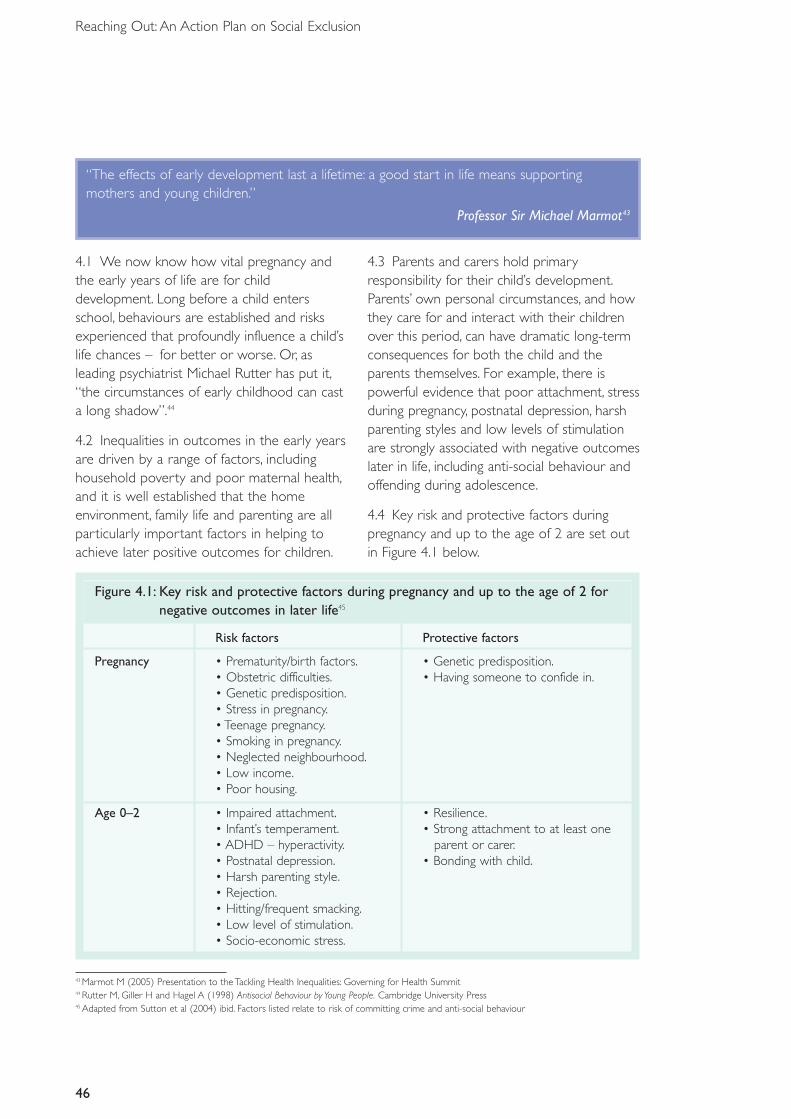
Figure 4.1: Key risk and protective factors during pregnancy and up to the age of 2 fornegative outcomes in later life45
Risk factors Protective factors
Pregnancy • Prematurity/birth factors. • Genetic predisposition.• Obstetric difficulties. • Having someone to confide in.• Genetic predisposition.• Stress in pregnancy.• Teenage pregnancy.• Smoking in pregnancy.• Neglected neighbourhood.• Low income.• Poor housing.
Age 0–2 • Impaired attachment. • Resilience.• Infant’s temperament. • Strong attachment to at least one • ADHD – hyperactivity. parent or carer.• Postnatal depression. • Bonding with child.• Harsh parenting style.• Rejection.• Hitting/frequent smacking.• Low level of stimulation.• Socio-economic stress.
46
Reaching Out: An Action Plan on Social Exclusion
43 Marmot M (2005) Presentation to the Tackling Health Inequalities: Governing for Health Summit44 Rutter M, Giller H and Hagel A (1998) Antisocial Behaviour by Young People. Cambridge University Press45 Adapted from Sutton et al (2004) ibid. Factors listed relate to risk of committing crime and anti-social behaviour
4.1 We now know how vital pregnancy andthe early years of life are for childdevelopment. Long before a child entersschool, behaviours are established and risksexperienced that profoundly influence a child’slife chances – for better or worse. Or, asleading psychiatrist Michael Rutter has put it,“the circumstances of early childhood can casta long shadow”.44
4.2 Inequalities in outcomes in the early yearsare driven by a range of factors, includinghousehold poverty and poor maternal health,and it is well established that the homeenvironment, family life and parenting are allparticularly important factors in helping toachieve later positive outcomes for children.
4.3 Parents and carers hold primaryresponsibility for their child’s development.Parents’ own personal circumstances, and howthey care for and interact with their childrenover this period, can have dramatic long-termconsequences for both the child and theparents themselves. For example, there ispowerful evidence that poor attachment, stressduring pregnancy, postnatal depression, harshparenting styles and low levels of stimulationare strongly associated with negative outcomeslater in life, including anti-social behaviour andoffending during adolescence.
4.4 Key risk and protective factors duringpregnancy and up to the age of 2 are set outin Figure 4.1 below.
“The effects of early development last a lifetime: a good start in life means supportingmothers and young children.”
Professor Sir Michael Marmot43
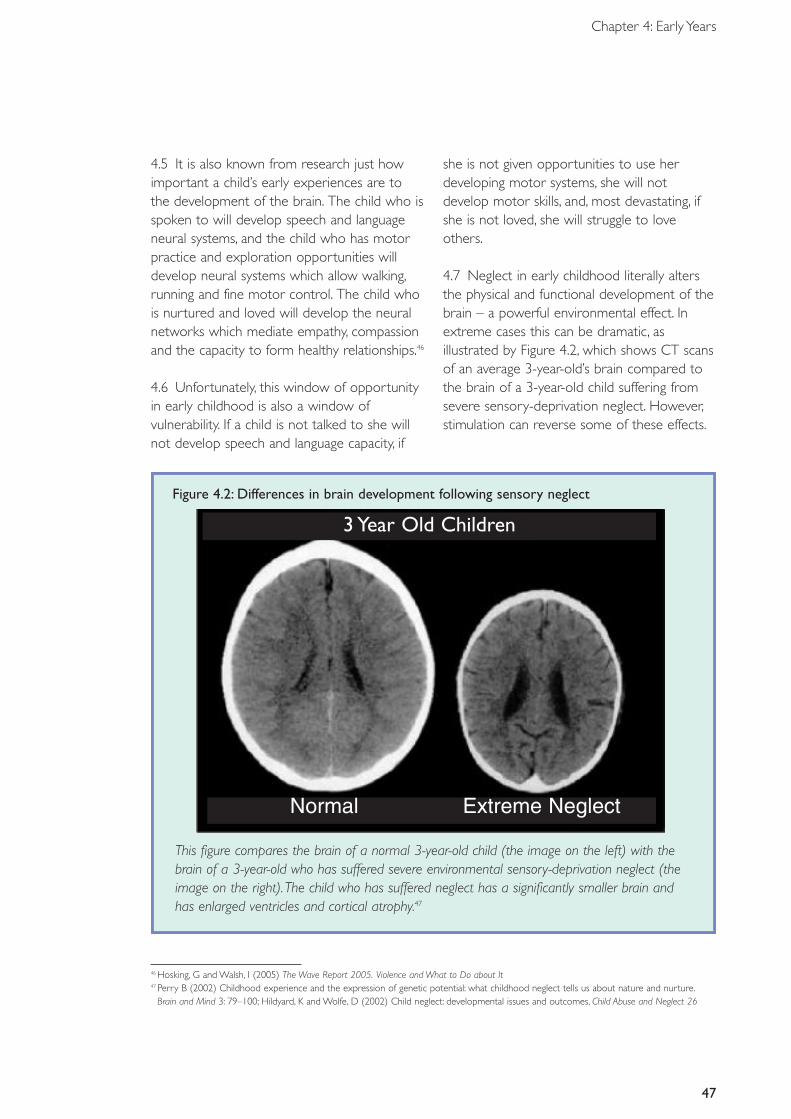
47
Chapter 4: Early Years
4.5 It is also known from research just howimportant a child’s early experiences are tothe development of the brain. The child who isspoken to will develop speech and languageneural systems, and the child who has motorpractice and exploration opportunities willdevelop neural systems which allow walking,running and fine motor control. The child whois nurtured and loved will develop the neuralnetworks which mediate empathy, compassionand the capacity to form healthy relationships.46
4.6 Unfortunately, this window of opportunityin early childhood is also a window ofvulnerability. If a child is not talked to she willnot develop speech and language capacity, if
she is not given opportunities to use herdeveloping motor systems, she will notdevelop motor skills, and, most devastating, ifshe is not loved, she will struggle to loveothers.
4.7 Neglect in early childhood literally altersthe physical and functional development of thebrain – a powerful environmental effect. Inextreme cases this can be dramatic, asillustrated by Figure 4.2, which shows CT scansof an average 3-year-old’s brain compared tothe brain of a 3-year-old child suffering fromsevere sensory-deprivation neglect. However,stimulation can reverse some of these effects.
46 Hosking, G and Walsh, I (2005) The Wave Report 2005. Violence and What to Do about It47 Perry B (2002) Childhood experience and the expression of genetic potential: what childhood neglect tells us about nature and nurture.
Brain and Mind 3: 79–100; Hildyard, K and Wolfe, D (2002) Child neglect: developmental issues and outcomes, Child Abuse and Neglect 26
Figure 4.2: Differences in brain development following sensory neglect
This figure compares the brain of a normal 3-year-old child (the image on the left) with thebrain of a 3-year-old who has suffered severe environmental sensory-deprivation neglect (theimage on the right).The child who has suffered neglect has a significantly smaller brain andhas enlarged ventricles and cortical atrophy.47
3 Year Old Children
Normal Extreme Neglect
48
Reaching Out: An Action Plan on Social Exclusion
4.8 The most effective forms of parenting canprotect against risks in early childhood and canhave dramatic effects on social and cognitivedevelopment.48 Poor parenting can exposechildren to greater risks and can contribute tothe development of potentially harmful patternsof behaviour. Intensive support can improveparenting and attachment, and can have dramaticimpacts upon parent and child outcomes. It hasbeen shown that these effects can continuethroughout adolescence and into adulthood.49
4.9 Pregnancy and birth is a critical time, whenit is possible to develop the resilience andprotective factors in children, therebydramatically improving their chances of going
on to lead healthy and fulfilling lives. It isimportant to seize this opportunity and toensure that maximum support is providedwhere it is most needed and where it canhave most effect.What is more, there is goodevidence of public demand for moreinformation and support with respect toparenting.50 The Fragile Families study in the USfound that parents are easier to engage andmore positive about changing their behaviourand lifestyle at the time of pregnancy andbirth. Midwives’ and health visitors’ abilities toaddress mothers’ concerns about pregnancy,labour and the physical health of the infantprovide them with credibility and persuasivepowers in the eyes of family members.
48 Sure Start Children’s Centres: Practice Guidance. (2005) DfES49 Olds, D (2006) The Nurse-Family Partnership: An evidence-based preventive intervention. Infant Mental Health Journal 27(1) 5–2550 Ghate, D and Hazel, N (2002) Parenting in Poor Environments. London and Philadelphia: Jessica Kingsley
“Like it or not, the most important mental and behavioural patterns, once established, aredifficult to change once children enter school.”
Nobel Laureate James Heckman
What the Government hasalready done4.10 Since 1997 this Government hasintroduced a wide range of measures toimprove the well-being and prospects of themost disadvantaged families and individuals,pushing the frontiers of the welfare state intothe early years. Key achievements include thefollowing.
• Tackling child poverty through welfarereforms, increasing employment andincreased financial and parenting support forfamilies with children.The Government’s goalis to eradicate child poverty by 2020, halvingit by 2010. Since 1997, 800,000 fewer
children now live in relative poverty. Thisdrive will continue, with increased focus onidentifying and supporting the remaining at-risk groups of families and children, providingmore personalised services and support forthe most vulnerable, and reforming the ChildSupport Agency.
• Ensuring that every child has the best startin life with the establishment of Sure Start,including 1,000 Children’s Centres open bythe end of September 2006 and theexpansion of early-years education, withmore than £17 billion invested in these areassince 1997. By 2010 there will be 3,500 SureStart Children’s Centres across the country,offering integrated early learning, health andparental services for the first time – arguably
49
Chapter 4: Early Years
one of the Government’s most ambitiousand innovative programmes of recent years.The Government is also investing in EarlyLearning Partnership demonstration projectsto help parents of 1–3-year-olds to supporttheir children's early learning. These serviceswill be delivered by voluntary andcommunity sector organisations to engagethe children in the hardest-to-reach familiesmost at risk of learning delay.
• New duties in the Childcare Act 2006requiring local authorities and their NHS andJobcentre Plus partners to work together toimprove the outcomes for all children up to5 and reduce inequalities between them, byensuring that early childhood services areintegrated to maximise access and benefitsto families.
• Free early learning and childcare for 3- and4-year-olds – shown by research evidenceto improve educational and social outcomesfor all children, but particularly for childrenfrom disadvantaged families. The entitlementwill be extended from 12.5 hours to15 hours per week (for 38 weeks a year) by 2010. A pilot to extend the provision to12,000 disadvantaged 2-year-olds is currentlytaking place.
• The creation of a National Academy forParenting Professionals, already announcedin the Respect Action Plan, as a centre ofexcellence in training, development andsupport for the parenting workforce. TheAcademy will act as a national centre andsource of advice on high-quality researchevidence on parenting and parentingsupport, combined with practical knowledgeof what works in different situations andwith different client groups. Organisationswill be invited to bid to deliver the NationalAcademy for Parenting Professionalsprogramme later in 2006.
• An end to the long-term use of bed andbreakfast accommodation for families withchildren. In March 2002 there were 6,960homeless families living in B&Bs. However,
through an increased focus on homelessnessprevention, on finding better forms ofaccommodation and on the sharing of goodpractice, and £50 million of funding, the vastmajority of local authorities have sustainedsuccess in ending the long-term use of B&Baccommodation for families with children.
Continuing challenges4.11 Clearly, enormous strides have beenmade in terms of the support available tofamilies with children. Public services andsupport in the early years are available forevery family. However, the intended universalnature of these services is incomplete. In someareas, the families with the greatest need donot always benefit as much as they shouldfrom the support available.The ‘inverse carelaw’ suggests that those with the greatest needor at greatest risk are sometimes the leastlikely to receive the services they need. Indeed,there are some children’s and family serviceswhere redressing the inverse care law hasproven difficult.
4.12 Public services struggle to support veryhigh-need families because such families aretypically harder to reach and harder toengage. More advantaged families are oftenthe most likely to ask for help, while thosewith more complex problems may not knowthat help is available or may even activelydecline it. If their needs are not met then theservices cannot be regarded as genuinelyuniversal.
4.13 In the early years, health visitors andmidwives are essential for early identification ofrisk factors, engagement with parents anddelivery of support.They can also shareinformation and support families to use otherservices such as Sure Start Children’s Centres,acting as the link between health services (inparticular general practice) and integratedsupport services.
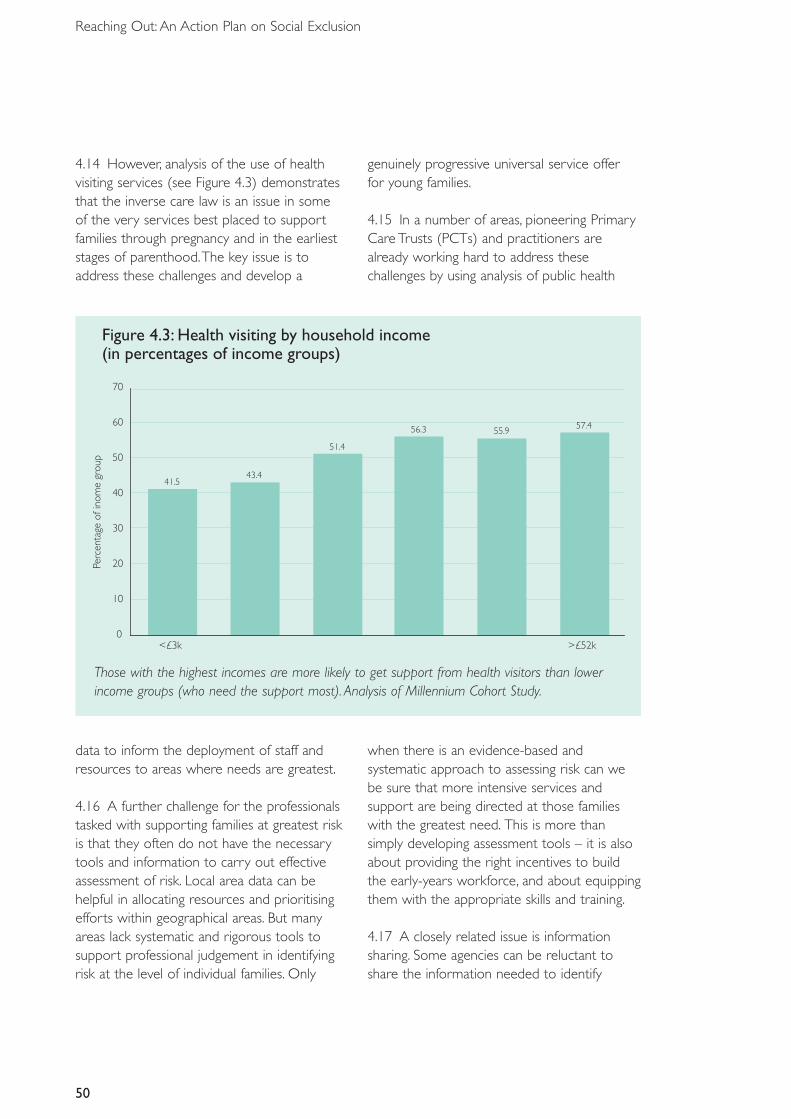
Figure 4.3: Health visiting by household income(in percentages of income groups)
41.543.4
51.4
56.3 55.957.4
0
10
20
30
40
50
60
70
<£3k
Perc
enta
geof
inom
egr
oup
>£52k
50
Reaching Out: An Action Plan on Social Exclusion
4.14 However, analysis of the use of healthvisiting services (see Figure 4.3) demonstratesthat the inverse care law is an issue in some of the very services best placed to supportfamilies through pregnancy and in the earlieststages of parenthood.The key issue is toaddress these challenges and develop a
genuinely progressive universal service offer for young families.
4.15 In a number of areas, pioneering PrimaryCare Trusts (PCTs) and practitioners arealready working hard to address thesechallenges by using analysis of public health
Those with the highest incomes are more likely to get support from health visitors than lowerincome groups (who need the support most). Analysis of Millennium Cohort Study.
data to inform the deployment of staff andresources to areas where needs are greatest.
4.16 A further challenge for the professionalstasked with supporting families at greatest riskis that they often do not have the necessarytools and information to carry out effectiveassessment of risk. Local area data can behelpful in allocating resources and prioritisingefforts within geographical areas. But manyareas lack systematic and rigorous tools tosupport professional judgement in identifyingrisk at the level of individual families. Only
when there is an evidence-based andsystematic approach to assessing risk can webe sure that more intensive services andsupport are being directed at those familieswith the greatest need. This is more thansimply developing assessment tools – it is alsoabout providing the right incentives to buildthe early-years workforce, and about equippingthem with the appropriate skills and training.
4.17 A closely related issue is informationsharing. Some agencies can be reluctant toshare the information needed to identify

51
Chapter 4: Early Years
at-risk households with other agencies whomay also be able to help them.
4.18 Innovative PCTs and Sure StartChildren’s Centres are already making greatstrides towards addressing these challenges.The Government is determined to supportthese efforts by helping to build the evidencebase for the most effective early interventionsfor socially excluded families.
Intensive early health-led support forfamilies most at risk4.19 What works in the early years ishigh-quality social support alongside antenatalclinical care.51 Health visitors and midwives canplay a pivotal role, as they provide a universallyavailable service at a time when parents aretypically highly receptive to external advice andsupport.We also know from some of themost innovative PCTs that health-led teamscan be particularly effective in engaging someof the most at-risk parents and families.
4.20 Internationally, we have identified anumber of practical approaches that are trulyoutstanding in terms of outcomes and long-term cost-effectiveness.52 From pre-birth to
age 2, the Nurse–Family Partnership model(see Box 4.1) shows sustained impacts53 andhas been found to be highly cost-effective.Rigorous independent evaluation in the USfound that for the highest-risk families theamount of downstream savings is over fourtimes the cost of the programme.54
4.21 Additionally, empirically tested group-based parenting programmes such as CarolynWebster-Stratton’s ‘Incredible Years’demonstrate impressive sustained impacts onmaternal health, child development andreduction of conduct problems.55
4.22 Importantly, both the Nurse–FamilyPartnership programme and Incredible Yearshave been found to be effective with familiessuffering high levels of deprivation. Someareas in the UK, particularly those linked toSure Start programmes, have begun to usethese approaches with dramatic success(see Box 4.2).
4.23 The Government will build on theseearly successes to target our earlyinterventions using best-known practice.
51 Sutton et al (2004) ibid52 Lynch, R D (2004) Exceptional Returns: Economic, Fiscal and Social Benefits of Investment in Childhood Development53 Olds, D (2006) The Nurse-Family Partnership: An evidence-based preventive intervention. Infant Mental Health Journal: 27(1) 5–2554 Karoly et al. (1998) Investing in our children.What we know and what we don’t know about costs and benefits of early childhood intervention. Santa
Monica, CA: RAND55 Hutchings, J (February 2006) What works in parenting programmes and why: practice and research using the Incredible Years parent
programme in Wales. Presentation to Communities that Care Conference
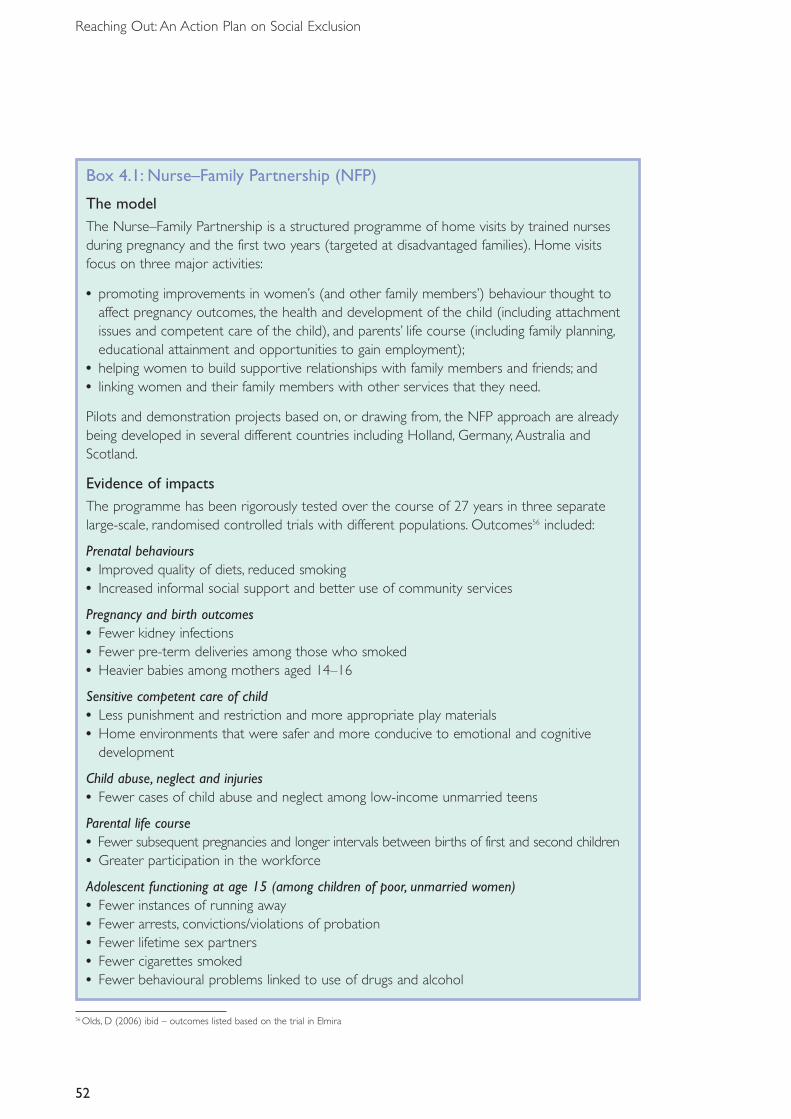
52
Reaching Out: An Action Plan on Social Exclusion
Box 4.1: Nurse–Family Partnership (NFP)
The modelThe Nurse–Family Partnership is a structured programme of home visits by trained nursesduring pregnancy and the first two years (targeted at disadvantaged families). Home visitsfocus on three major activities:
• promoting improvements in women’s (and other family members’) behaviour thought toaffect pregnancy outcomes, the health and development of the child (including attachmentissues and competent care of the child), and parents’ life course (including family planning,educational attainment and opportunities to gain employment);
• helping women to build supportive relationships with family members and friends; and• linking women and their family members with other services that they need.
Pilots and demonstration projects based on, or drawing from, the NFP approach are alreadybeing developed in several different countries including Holland, Germany, Australia andScotland.
Evidence of impactsThe programme has been rigorously tested over the course of 27 years in three separatelarge-scale, randomised controlled trials with different populations. Outcomes56 included:
Prenatal behaviours• Improved quality of diets, reduced smoking• Increased informal social support and better use of community services
Pregnancy and birth outcomes• Fewer kidney infections• Fewer pre-term deliveries among those who smoked• Heavier babies among mothers aged 14–16
Sensitive competent care of child• Less punishment and restriction and more appropriate play materials• Home environments that were safer and more conducive to emotional and cognitive
development
Child abuse, neglect and injuries• Fewer cases of child abuse and neglect among low-income unmarried teens
Parental life course• Fewer subsequent pregnancies and longer intervals between births of first and second children• Greater participation in the workforce
Adolescent functioning at age 15 (among children of poor, unmarried women)• Fewer instances of running away• Fewer arrests, convictions/violations of probation• Fewer lifetime sex partners• Fewer cigarettes smoked• Fewer behavioural problems linked to use of drugs and alcohol
56 Olds, D (2006) ibid – outcomes listed based on the trial in Elmira
53
Chapter 4: Early Years
4.24 The Government will demonstrate newapproaches to health visiting and midwifery,drawing on evidence-based programmes fromoverseas.The demonstration sites will help tobuild the English evidence base on health-ledparenting support in the early years, trailblazingpractical approaches to achieving the vision forhealth visiting and community midwifery that isset out in the National Service Framework forChildren,Young People and Maternity Services.57
4.25 The demonstration projects at a cost of £7 million will complement the raft ofparenting provision for school-aged childrenannounced earlier this year and will be mainlydelivered through the integrated children’s,families and community services provided bySure Start Children’s Centres.This will embeda strongly progressive universal model from
pregnancy until the age of 2, with intensivesupport for those at risk and a lighter touchfor others. It will build on the strengths ofexisting services provided by health visitorsand midwives. It will also test out new systemsand tools for a more systematic assessment ofneed drawing on research into risk andprotective factors during pregnancy and theearly years.
4.26 This programme of demonstrationprojects will work with local practitioners totest different levels of support, and evaluatethe impact on initial outcomes. It will developways of engaging parents, building skills andcapacities to cope with the challenges ofparenthood.These findings will provide bestpractice, which can be used by practitioners,PCTs and local authorities.
Box 4.2: Incredible YearsSignificant results have been achieved in 11 Sure Start centres in Wales and the Borders usingCarolyn Webster-Stratton’s ‘Incredible Years’ parenting programme. Families with a child aged3 or 4 with significant behavioural problems were targeted within the Sure Start area andattended 12 group sessions.These children and a control group were then tracked for 18months.The Sure Start intervention families showed significantly increased positive parentingand marked decreases in the quantity and intensity of child problem behaviours. Interventionchildren fell below the clinical cut-off on both the Eyberg Child Behaviour Inventory problemand intensity scales.
How the challenges will be met
ACTION 16: The Government will establish 10 health-led parenting support demonstrationprojects from pre-birth to age 2, building in a rigorous evaluation of targeted support.
57 DH/DfES (2004) National Service Framework for Children,Young People and Maternity Services: Maternity Services
ACTION 17: The Government will support the upskilling of midwives, health visitors andcommissioners to support early-years interventions; and will develop commissioning guidanceto encourage the spread of best practice nationally.
54
Reaching Out: An Action Plan on Social Exclusion
58 HMT (2005) Support for Parents: The Best Start for Children
4.27 The Government wants to see a step-change in outcomes for high-risk familieseverywhere. In parallel to the demonstrationsites, there will be a series of ‘Let’s talk abouthealth visiting’ events for health visitors andcommissioners in every Strategic HealthAuthority. The Government will also work withstakeholders to review the career pathwaysand educational preparation needed by nursesworking in the community, including healthvisitors.This work forms part of theModernising Nursing Careers agenda launchedin September 2006.
4.28 Midwives and health visitors alreadyreceive training in child development and thesocial and psychological needs of women andtheir families. A high level of skill is needed forworking in partnership with families on issuesof attachment, behaviour and risk. One of theoutcomes of the demonstration projects willbe the development of additional training andguidance for midwives and health visitors inhow to identify and engage at-risk families anddeliver effective interventions to supportparenting that can be rolled out more widely.
4.29 In the Respect Action Plan theGovernment has already announced thecreation of a National Academy for ParentingProfessionals as a Centre of Excellence intraining, development and support for theparenting workforce.The Academy will also actas a national centre and source of advice onhigh-quality research evidence on parentingand parenting support, combined with practicalknowledge of what works in differentsituations and with different client groups.Organisations will be invited to bid to deliverthe National Academy for ParentingProfessionals programme later in 2006.
4.30 As part of ongoing reviews, we willexamine existing indicators of early-yearsoutcomes, and will explore how planning,pooled budgets, commissioning, inspection andaccountability frameworks can best encourageeffective joint working between PCTs and localauthorities in relation to the very early years.
4.31 Finally, building on Support for Parents:TheBest Start for Children,58 the Government willtake steps to develop a system that is morepreventative and, where problems do arise,intervention comes earlier before problemsescalate.
4.32 The policy review of children and youngpeople, to inform the 2007 ComprehensiveSpending Review, will examine how we cansecure continued improvements towards astronger focus on prevention, including howpublic services can provide better support tofamilies and parents in the early years andbeyond.
Conclusion4.33 Pregnancy and the first three years of lifeare vital to child development, life chances andfuture achievement. Overseas programmessuch as the Nurse–Family Partnershipdemonstrate that home-visiting programmesled by nurses can have dramatic effects inenhancing the life chances of children andparents who are experiencing or at risk ofsocial exclusion.
4.34 Midwives and health visitors are ideallyplaced to identify children and families at riskand to provide intensive and structuredhome-visiting programmes to those who mightbenefit from additional support.TheGovernment will build on the successes of

55
Chapter 4: Early Years
pioneering PCTs and practitioners alreadyworking hard to support socially excludedfamilies and to embed the principle ofprogressive universalism into their work.Through the development of 10demonstration projects we will build the
English evidence base on health-led parentingsupport, pioneering genuinely preventativeservices which respond effectively to early-warning signs before problems have a chanceto escalate.

Chapter 5: Childhood and Teenage Years
SummaryFor children and teenagers, the Government will continue to build on theEvery Child Matters agenda, and:
• publish a Green Paper in October 2006 on children in care, setting outthe Government’s proposals to transform their outcomes.This willinclude proposals on individual budget-holding arrangements to ensurethat every child in care has someone who understands their personalneeds and has the leverage to secure the right support;
• publish a revised and updated Teenage Pregnancy Strategy with aparticular focus on local areas where there has been little or noimprovement on tackling the wider causes of teenage pregnancy;
• launch a series of pilots to test different approaches to tackling mentalhealth and conduct disorders in childhood, including intensive home-based interventions and Treatment Foster Care; and
• continue to improve provision and capability around parenting supportand training; pilot budget-holding practitioner models for children withadditional needs; ensure these actions are delivering a coherent whole-family approach for families at risk.
57
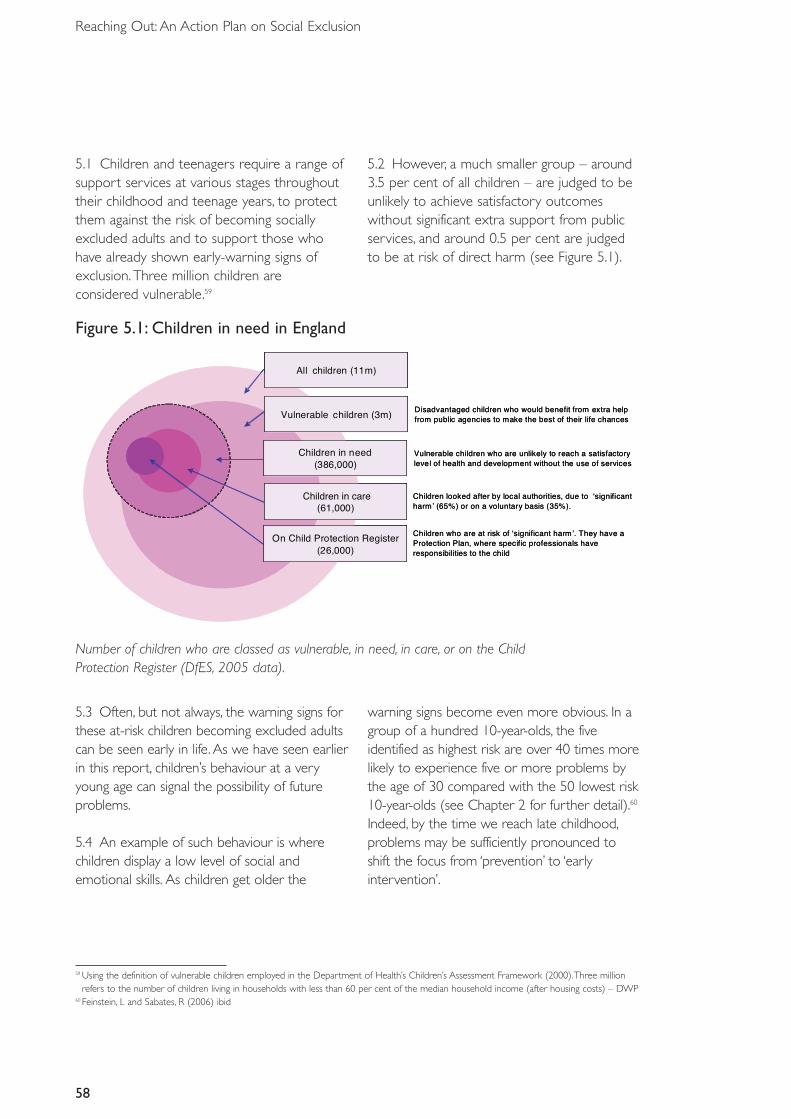
58
Reaching Out: An Action Plan on Social Exclusion
5.1 Children and teenagers require a range ofsupport services at various stages throughouttheir childhood and teenage years, to protectthem against the risk of becoming sociallyexcluded adults and to support those whohave already shown early-warning signs ofexclusion. Three million children areconsidered vulnerable.59
5.2 However, a much smaller group – around3.5 per cent of all children – are judged to beunlikely to achieve satisfactory outcomeswithout significant extra support from publicservices, and around 0.5 per cent are judgedto be at risk of direct harm (see Figure 5.1).
(61,000)
Children in Need(386,000)
On Child Protection Register(26,000)
All Children (11m)
Vulnerable Children (3m) Disadvantaged children who would benefit from extra helpfrom public agencies to make the best of their life chances
Vulnerable children who are unlikely to reach a satisfactorylevel of health and development without the use of services
Children looked after by local authorities, due to ʻsignificantharmʼ (65%) or on a voluntary basis (35%).
Children who are at risk of ʻsignificant harmʼ. They have a Protection Plan, where specific professionals haveresponsibilities to the child
Children in care(61,000)
Children in need(386,000)
On Child Protection Register(26,000)
All children (11m)
Vulnerable children (3m) Disadvantaged children who would benefit from extra helpfrom public agencies to make the best of their life chances
Vulnerable children who are unlikely to reach a satisfactorylevel of health and development without the use of services
Children looked after by local authorities, due to ʻsignificantharmʼ (65%) or on a voluntary basis (35%).
Children who are at risk of ʻsignificant harmʼ. They have a Protection Plan, where specific professionals haveresponsibilities to the child
Figure 5.1: Children in need in England
Number of children who are classed as vulnerable, in need, in care, or on the Child Protection Register (DfES, 2005 data).
5.3 Often, but not always, the warning signs forthese at-risk children becoming excluded adultscan be seen early in life. As we have seen earlierin this report, children’s behaviour at a veryyoung age can signal the possibility of futureproblems.
5.4 An example of such behaviour is wherechildren display a low level of social andemotional skills. As children get older the
warning signs become even more obvious. In agroup of a hundred 10-year-olds, the fiveidentified as highest risk are over 40 times morelikely to experience five or more problems bythe age of 30 compared with the 50 lowest risk10-year-olds (see Chapter 2 for further detail).60
Indeed, by the time we reach late childhood,problems may be sufficiently pronounced toshift the focus from ‘prevention’ to ‘earlyintervention’.
59 Using the definition of vulnerable children employed in the Department of Health’s Children’s Assessment Framework (2000).Three millionrefers to the number of children living in households with less than 60 per cent of the median household income (after housing costs) – DWP
60 Feinstein, L and Sabates, R (2006) ibid
59
Chapter 5: Childhood and Teenage Years
5.5 Children and young people who areespecially likely to suffer a lifetime of socialexclusion and limited life chances include:children in care, teenage mothers, and childrenwith the poorest educational attainment.Thesegroups are more likely to suffer from
unemployment, ill health, and many other pooroutcomes.They also significantly overlap. Forexample, children in care are much more likelyto be teenage mothers than their peers, andlow educational attainment is associated withboth teenage pregnancy and being in care.61
Box 5.1: Social and emotional learningRecent studies show that the impact of non-cognitive skills in influencing certain outcomescan be significant, including criminal activity and unemployment.62 When children lack socialand emotional skills they often disengage from schooling, leading to poor attainment andbehaviour problems.63 Social and emotional competence programmes have shown dramaticdecreases in classroom aggression and increases in pro-social behaviour.64
We know that society as a whole places a high value on such skills. For example, employersare especially keen to take on young people who demonstrate good relationship andleadership skills, often developed through their engagement in positive activities either in oroutside of school.
Empirically tested school-based social and emotional competence programmes, includingWebster-Stratton’s teacher training course, have shown dramatic decreases in classroomaggression and increases in pro-social behaviour.65 Drawing on evidence-based programmes,the Government has developed a whole-school programme, the Social and EmotionalAspects of Learning (SEAL), supplemented by small-group work for certain pupils. One-thirdof primary schools have already started to implement the SEAL programme, and anotherthird are expected to have done so by mid-2007. By creating positive social and emotionallearning environments and expanding empirically validated teacher training approaches, weexpect to see improved behaviour, attendance and attainment, as well as improved long-termoutcomes for the most at risk.
61 Teenage Pregnancy Next Steps – Guidance for LAs and PCTs on Effective Delivery of Local Strategies (July 2006)http://www.everychildmatters.gov.uk/_files/F7CB3099CE80C6B2AA12604BB52BE74A.pdf
62 See for example Heckman et al (2006) The Effect of Cognitive and Non-cognitive Abilities in Labour Market Outcomes and Social BehaviourWP 12006, National Bureau of Economic Research
63 Carneiro, P et al (2006) Which Skills Matter? Institute for Fiscal Studies64 Webster-Stratton, C and Reid, J (1999) Treating Children with Early-onset Conduct Problems:The Importance of Teacher Training. Paper presented
at the American Association of Behavior Therapy,Toronto 65 ibid
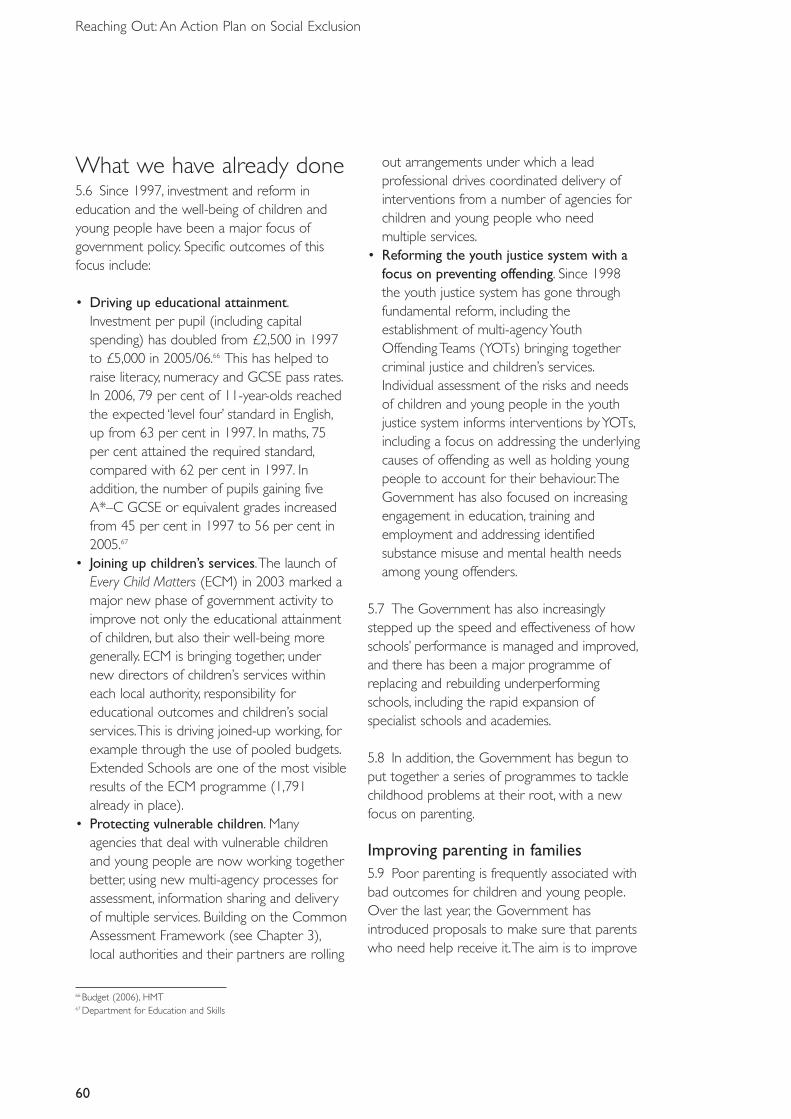
60
Reaching Out: An Action Plan on Social Exclusion
What we have already done5.6 Since 1997, investment and reform ineducation and the well-being of children andyoung people have been a major focus ofgovernment policy. Specific outcomes of thisfocus include:
• Driving up educational attainment.Investment per pupil (including capitalspending) has doubled from £2,500 in 1997to £5,000 in 2005/06.66 This has helped toraise literacy, numeracy and GCSE pass rates.In 2006, 79 per cent of 11-year-olds reachedthe expected ‘level four’ standard in English,up from 63 per cent in 1997. In maths, 75per cent attained the required standard,compared with 62 per cent in 1997. Inaddition, the number of pupils gaining fiveA*–C GCSE or equivalent grades increasedfrom 45 per cent in 1997 to 56 per cent in2005.67
• Joining up children’s services.The launch ofEvery Child Matters (ECM) in 2003 marked amajor new phase of government activity toimprove not only the educational attainmentof children, but also their well-being moregenerally. ECM is bringing together, undernew directors of children’s services withineach local authority, responsibility foreducational outcomes and children’s socialservices.This is driving joined-up working, forexample through the use of pooled budgets.Extended Schools are one of the most visibleresults of the ECM programme (1,791already in place).
• Protecting vulnerable children. Manyagencies that deal with vulnerable childrenand young people are now working togetherbetter, using new multi-agency processes forassessment, information sharing and deliveryof multiple services. Building on the CommonAssessment Framework (see Chapter 3),local authorities and their partners are rolling
out arrangements under which a leadprofessional drives coordinated delivery ofinterventions from a number of agencies forchildren and young people who needmultiple services.
• Reforming the youth justice system with afocus on preventing offending. Since 1998the youth justice system has gone throughfundamental reform, including theestablishment of multi-agency YouthOffending Teams (YOTs) bringing togethercriminal justice and children’s services.Individual assessment of the risks and needsof children and young people in the youthjustice system informs interventions by YOTs,including a focus on addressing the underlyingcauses of offending as well as holding youngpeople to account for their behaviour.TheGovernment has also focused on increasingengagement in education, training andemployment and addressing identifiedsubstance misuse and mental health needsamong young offenders.
5.7 The Government has also increasinglystepped up the speed and effectiveness of howschools’ performance is managed and improved,and there has been a major programme ofreplacing and rebuilding underperformingschools, including the rapid expansion ofspecialist schools and academies.
5.8 In addition, the Government has begun toput together a series of programmes to tacklechildhood problems at their root, with a newfocus on parenting.
Improving parenting in families5.9 Poor parenting is frequently associated withbad outcomes for children and young people.Over the last year, the Government hasintroduced proposals to make sure that parentswho need help receive it.The aim is to improve
66 Budget (2006), HMT67 Department for Education and Skills
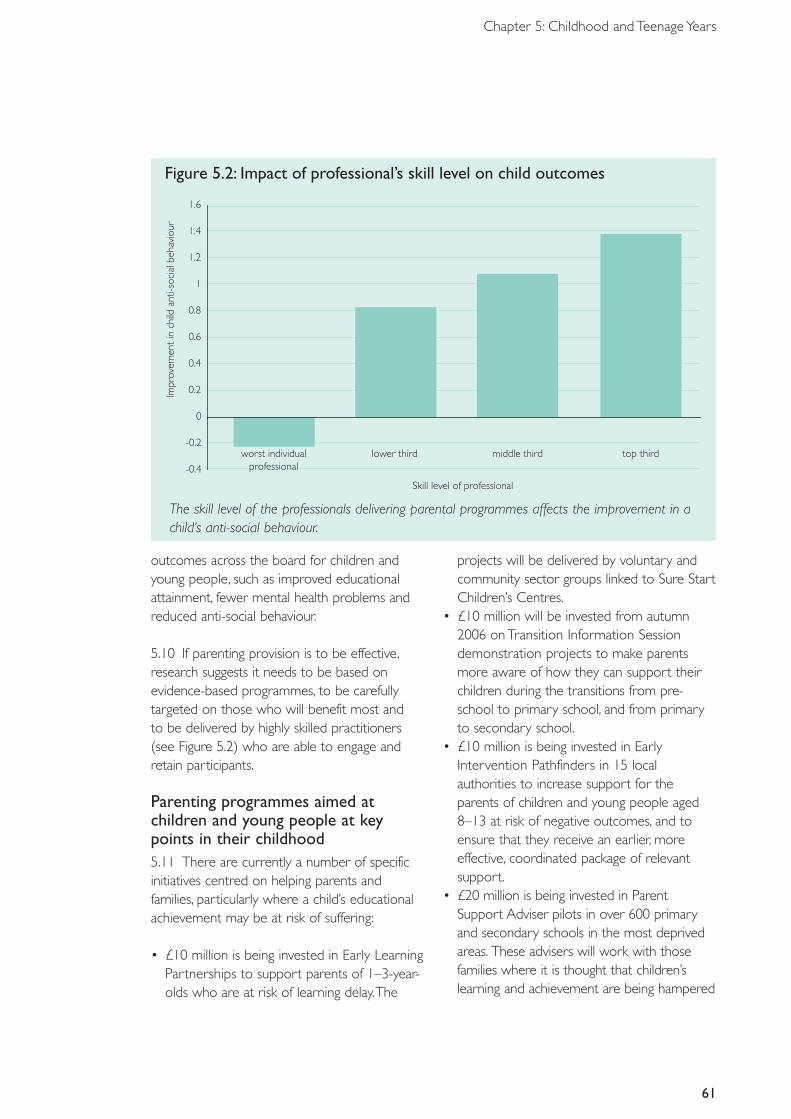
Figure 5.2: Impact of professional’s skill level on child outcomes
-0.4
-0.2
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
worst individualprofessional
lower third middle third top third
Skill level of professional
Impr
ovem
ent
inch
ildan
ti-so
cial
beha
viou
r
61
Chapter 5: Childhood and Teenage Years
outcomes across the board for children andyoung people, such as improved educationalattainment, fewer mental health problems andreduced anti-social behaviour.
5.10 If parenting provision is to be effective,research suggests it needs to be based onevidence-based programmes, to be carefullytargeted on those who will benefit most and to be delivered by highly skilled practitioners (see Figure 5.2) who are able to engage andretain participants.
Parenting programmes aimed atchildren and young people at keypoints in their childhood5.11 There are currently a number of specificinitiatives centred on helping parents andfamilies, particularly where a child’s educationalachievement may be at risk of suffering:
• £10 million is being invested in Early LearningPartnerships to support parents of 1–3-year-olds who are at risk of learning delay.The
projects will be delivered by voluntary andcommunity sector groups linked to Sure StartChildren’s Centres.
• £10 million will be invested from autumn2006 on Transition Information Sessiondemonstration projects to make parentsmore aware of how they can support theirchildren during the transitions from pre-school to primary school, and from primaryto secondary school.
• £10 million is being invested in EarlyIntervention Pathfinders in 15 localauthorities to increase support for theparents of children and young people aged8–13 at risk of negative outcomes, and toensure that they receive an earlier, moreeffective, coordinated package of relevantsupport.
• £20 million is being invested in ParentSupport Adviser pilots in over 600 primaryand secondary schools in the most deprivedareas. These advisers will work with thosefamilies where it is thought that children’slearning and achievement are being hampered
The skill level of the professionals delivering parental programmes affects the improvement in achild’s anti-social behaviour.
62
Reaching Out: An Action Plan on Social Exclusion
by parental problems or a lack of support athome, and will aim to identify ways in whichschools can work better with parents.
• The Government will also establish 10 health-led parenting support demonstration projectsfrom pre-birth to age 2 (see Chapter 4).
Projects to address anti-socialbehaviour and offending5.12 The Government is investing in a range of initiatives to tackle the growing problem ofanti-social behaviour:
• Fifty Family Intervention Projects (see alsoChapter 3) will be delivered by the end of2006, offering a range of rehabilitationmeasures to families that are causinganti-social behaviour, including parentingprogrammes and health and employmentservices.
• The Youth Justice Board has worked withYouth Offending Teams (YOTs) toapproximately double the number ofparenting support interventions to 11,000per year over the last two years. Some of theadditional funding of £45 million recentlymade available to YOTs, to fund youth crimeprevention programmes, will go towardsincreasing this figure even further.
Measures to ensure engagement5.13 While most parents welcome support andadvice, in a small minority of cases it can bedifficult to engage with parents.This is why theGovernment has already extended measuresaddressing the small minority of parents whorefuse offers of support:
• The Education and Inspection Bill, publishedin February 2006, introduces measures toenable schools and local authorities to makeearlier use of parenting contracts andempowers schools to apply for parentingorders.
• As part of the Respect Action Plan, the Policeand Justice Bill, published in January 2006,
contains proposals to enable a wider range of agencies to seek parenting contracts andorders where there is anti-social behaviour by young people in the community.
Continuing challenges5.14 Every Child Matters provides a powerfulframework to drive further improvements inoutcomes for all children, including the mostdisadvantaged. A series of initiatives continueto follow this Green Paper, such as the recentYouth Matters: Next Steps (2006) thatproposed measures to help teenagers andyoung people engage in a range of positiveactivities.These include volunteering, andimproving teenagers’ access to advice andinformation on education, health, social andpersonal matters and career choices. Foryoung people at risk of social exclusion, theGovernment is committed to reforming andsimplifying targeted support.This will enable abetter service to be provided, built aroundyoung people’s personal needs andcircumstances. Key to this will be drawing on,and learning from, best practice from anumber of programmes, such as the YoungPeople’s Development Programme. Building onthis, the Government will report on ways toimprove outcomes for young people in theyouth services strand of its policy review onchildren and young people in theComprehensive Spending Review 2007.
5.15 The Every Child Matters agenda is still in itsearly days, and there is (as expected) substantialvariability in progress across geographical areas.While some local authorities have been able toimplement structural changes in the way thatchildren’s services are delivered, others are stillrolling out these changes.
5.16 As well as structural variations in howservices are delivered, there are significantvariations in performance, both between localauthorities and between different groups of
Figure 5.3: Percentage in year 11 who achieved at least five A*–C GCSEs or GNVQs
10.0
20.0
30.0
40.0
50.0
60.0
2000 2001 2002 2003 2004 2005
Children in care All children
41.7%
45.5%
Perc
enta
ge
Year
63
Chapter 5: Childhood and Teenage Years
children. For example, teenage conceptions aredown 11 per cent since 1998, and now standat a 20-year low. But while some areas haveachieved reductions in teenage conceptions of40 per cent or more, others have seenincreases against the overall downward trend.68
5.17 In terms of variations between groups,traditionally disadvantaged children continue tomake up the overwhelming majority of loweducational achievers. For example, of the25 per cent of children getting the lowest scorein key stage 2 English results, 82 per cent hadspecial educational needs, were from a blackand minority ethnic background, or werereceiving free school meals.
5.18 Although we continue to spend a greatdeal of money, the outcomes for the mostdisadvantaged young people remainunacceptably poor. For example, we typicallyspend £110,000 each year on a child inresidential care, and spending on all children incare has increased by almost 50 per cent in fouryears.Yet only around 11 per cent of children incare get grades A*–C at GCSE compared with56 per cent of all children (Figure 5.3). Suchpoor outcomes may be a reflection of thetrauma and backgrounds experienced by thesechildren, rather than the care itself, but theseoutcomes contribute to a life of exclusion andneed to be improved.
5.19 Similarly, while teenage conception rateshave fallen, they remain up to six times higher inthe UK than in some other northern Europeannations, despite the fact that 30 years ago ourrates were similar.These figures pose aprofound challenge.
5.20 The key challenges and underlying barriersto delivering services for vulnerable anddisadvantaged children align closely with theproblems and guiding principles identified inChapter 3:
68 See forthcoming Teenage Pregnancy Strategy (Department for Education and Skills)
Educational outcomes for children in care have improved, but a large gap still remains.Source: Department for Education and Skills.
64
Reaching Out: An Action Plan on Social Exclusion
• Intervening too late.We are so focused – interms of time and resources – on picking upthe pieces for children who have sufferedfrom absent or neglectful parenting and/orinadequate support from social services, thatwe may not have enough of a focus onidentifying and supporting at-risk childrenearlier. Social services departments are oftenstretched and struggle to focus on preventiongiven their stock of families and individuals inneed.
• Variable and ineffective practice. Despitesignificant investments in – and upskilling of –the education and social services workforce,there remain shortfalls in the availability ofhigh-quality services for children. A particulararea of concern for the workforce is inresidential care homes for children where,although 80 per cent of staff are required tohave NVQ 3 or above, this standard is rarelymet. Frequent moves of accommodation andschool also adversely affect outcomes. Newand innovative practices and programmes –often available from third sector providers –are not widely disseminated, and we lack acentre of knowledge and accreditation forsuch schemes.
• Multi-agency working and personalisation ofprovision.The ability of local authorities tocommission the best services (in terms ofquality and value) for children relies on therebeing appropriate joint targets, joint workingand detailed information on outcomes forthese at-risk children.This is often not thecase. For example, there are often tensions indelivering services for children where specifichealth inputs are required, since Primary CareTrusts do not always prioritise children’sservices. For some groups (such as disabled
children or children in need) we still have littledata on outcomes. For children in care,although data is better, it is difficult to linkoutcomes to specific local authorities, and todisentangle the huge range of factorsresponsible for the different outcomes fordifferent children. Better data should help localauthorities to become better commissionersof services, and to use a wider variety ofperformance contracting measures such asperformance-related tariffs.69
• Performance management: Much of thecurrent method of ensuring that localauthorities and their partners are adequatelydelivering services to their children and youngpeople relies on inspection.70 But theinspection process reflects several dutiesplaced on local authorities and their partners.This creates a danger that there is insufficientfocus and leverage to ensure that the mostvulnerable children are being provided for.This danger is compounded by the fact thatvulnerable children often constitute arelatively small number of the totalpopulation of children, and have relativelylittle impact on average attainment andoutcome measures.
How the challenges will bemetChildren in care5.21 Although educational and other outcomeshave improved for children in care in recentyears, the gap has widened as the outcomes forall children have risen. Not only do childrenenter the care system with a range ofchallenges, but that system sometimes fails to
69 The Department for Education and Skills is currently developing a comprehensive outcomes framework to measure the extent to whichlocal authorities are achieving the five Every Child Matters outcome measures. But we must ensure that the most vulnerable groups’ outcomesare given sufficient focus in these measures
70 Currently, an Annual Performance Assessment (APA) is undertaken for children and young people’s services.This, alongside other evidence,informs the Joint Area Review (JAR). Either the APA or the JAR feeds into the annual Comprehensive Performance Assessment (CPA)categorisation
65
Chapter 5: Childhood and Teenage Years
meet those challenges through a lack ofsufficient care and support.
5.22 The Green Paper will offer a robustanalysis as to why the outcomes for children incare remain poor and propose actions toimprove these outcomes, covering:
• early intervention;• placement quality;• getting the best from school;• positive activities and other services outside
school; and• support while making the transition to
adulthood.
5.23 There will also be a range of clear leversand incentives to ensure that the systemdelivers and underperformance is swiftlyidentified and addressed.
5.24 For most children, parents actively navigatethe system of services and support that isavailable, organise appointments, and insist thatservices deliver for their children, as well asdirectly mentoring and fostering their child’sdevelopment. But for children in care, there is aneed for a lead professional to take on thatrole, drawing together a ‘team around the child’to ensure that they have access to the supportthey need, whichever agency provides it. Leadprofessionals could be allocated a budget foreach child in care, and could use it to buy intailored services (for example, sporting, leisureand cultural activities or additional tuitionservices). Rather than waiting their turn on localwaiting lists, children in care would thereby haveaccess to immediate provision.
5.25 The proposals in the Green Paper will bewide ranging, and will address causes ofunderperformance and opportunities forsuccess at every level: the individual socialworker, lead professional and teacher; theorganisation of the school, local authority andchildren’s trust; and the wider accountability and performance framework overseen byinspectorates and central governmentdepartments.
Teenage pregnancy5.26 In spite of reducing teenage pregnancyrates in many local areas, progress must beaccelerated in order to meet the PublicService Agreement target of cutting rates by50 per cent by 2010. We have publishedguidance for local authorities and Primary CareTrusts on effective delivery of local strategies.Given the substantial regional variability inprogress, we will concentrate first andforemost on those areas that have high andincreasing rates.
5.27 Analysis has identified a range ofunderlying factors that increase the risk ofteenage pregnancy (even when taking accountof deprivation), which are not necessarilyaddressed through local teenage pregnancystrategies.These include: poor educationalattainment; limited aspirations anddisengagement from education, employment ortraining; poor social and emotional skills; andparents not talking frankly to their childrenabout sex and relationships.To achieve under-18conception rates that are similar to those of ourEuropean neighbours, action is needed to
ACTION 18:The Government will publish a Green Paper on children in care in October2006, which will set out proposals to narrow the gap between the outcomes of children in care and other children, and will include proposals on individual budget holding for childrenin care.
66
Reaching Out: An Action Plan on Social Exclusion
Box 5.2:Teens & ToddlersA good example of a successful teenage pregnancy intervention programme is the ‘Teens &Toddlers’ scheme.Teens & Toddlers is an innovative, preventive intervention for 14–17-year-olds who are at risk of early pregnancy and parenthood.The programme also has a range ofeducational, social and developmental objectives that contribute to the main pregnancyprevention agenda.Teenagers at risk spend two hours a week with the toddler in the nurseryto understand the reality of caring for children and the responsibilities involved. In addition,participants receive life-coaching.The programme has been shown to lead to:
• improvements in participating teenagers’ understanding of sexual health, safer sex practices,and broader health risks;
• improved emotional health and development of social and relationship skills;• better understanding of the needs and development of young children and improved
parenting skills;• increased involvement in school and community, and preparation for work;• improved outcomes for the toddlers attended to; and• dramatic reductions in teenage conceptions.
Evaluation has shown that Teens & Toddlers is highly cost effective in reducing teenagepregnancy (at a cost of around £1,000 per teenager compared with £60,000 health andbenefit costs in the first five years of a teenage pregnancy). It is also well perceived by bothpractitioners and participating teenagers. It is currently run in several London boroughs. Formore information see http://www.teensandtoddlers.org/.
ACTION 19:The Government will publish an updated Teenage Pregnancy Strategy71 with a particular focus on failing local authorities and on the underlying causes of teenagepregnancy.
address these wider underlying causes. Inparticular the forthcoming Teenage PregnancyStrategy will address the following drivers ofteenage conception:
• disengagement from/dislike of school amongthose most at risk;
• low attendance/attainment at school;• lack of aspiration among young people in the
most disadvantaged communities;
• poor knowledge and skills among youngpeople in relation to sex, relationships andsexual health risks, in particular on developingthe confidence to resist pressure to engage inearly sexual activity;
• poor and inconsistent contraceptive useamong sexually active young people; and
• lack of support for parents and professionalson how best to discuss relationships, sex, andsexual health issues with young people.
71 Department for Education and Skills (September 2006)
67
Chapter 5: Childhood and Teenage Years
ACTION 20:The Government will launch pilots to test different interventions for tacklingmental health problems in childhood, such as ‘Multi-systemic Therapy’ and ‘Treatment FosterCare’, to prevent the onset of problems later in life.
ACTION 21: By summer 2007 the Government will review and consult on how well servicesaimed at at-risk children and adults are working together on the ground.We will identify anyfurther actions or powers that are needed to deliver a coherent whole-family approach forthose most in need of help, challenge and support.
Children and young people withmental health problems5.28 Children with conduct disorder aredisproportionately likely to require specialeducational provision, foster and residential careand state benefits, and to come into contactwith the criminal justice system. Costs foradolescents diagnosed with conduct disorderare 10 times higher by age 28 than for thosewith no problems, and 3.5 times higher than forthose with conduct problems.72
5.29 There are a number of promisinginterventions for tackling anti-social behaviour inchildren and young people.These include multi-systemic therapy (an intensive, home-basedintervention for families of children and youngpeople with social, emotional, and behaviouralproblems) and Treatment Foster Care (ahome-based alternative to group homes forchildren in care).73 However, much of theevidence is either international or based onvery local trials in the UK.
72 Scott et al (2001) Financial Cost of Social Exclusion: Follow Up Study of Anti-social Children and Adulthood British Medical Journal73 Harrington, R and Bailey, S (2003) The Scope for Preventing Antisocial Personality Disorder by Intervening in Adolescence NHS National
Programme on Forensic Mental Health R&D74 Henggler, S W et al (1993) Family preservation using multi-systemic treatment: long-term follow-up to a clinical trial with serious juvenile
offenders Journal of Children and Family Studies.Borduin, C M et al (1995) Multi-systemic treatment of serious juvenile offenders: long-term prevention of criminality and violence Journal ofConsulting and Clinical Psychology
Box 5.3: Multi-systemic TherapyMulti-systemic Therapy (MST) is a short-term, family-based treatment based on the belief thatthe best way to improve a young person’s behaviour is to provide practical advice and supportto the parent or carer to address the range of problems that the young person faces.
MST is most frequently used to reduce offending among high-risk groups. Evidence suggeststhat MST works: evaluations in the USA have found re-arrest rates are between 25 and70 per cent lower among young people undergoing MST, compared with those who are not.MST is currently being evaluated in the UK in a randomised controlled trial at the BrandonCentre in London.74
Families 5.30 As already discussed, the Government issharpening its focus on parenting through anumber of initiatives to help support parents inthose families where children and young peopleare at the highest risk of falling behind, anti-socialbehaviour, and other problems.The Government
will build on these programmes to ensure thatparenting support is available for families withadditional needs, to tackle problems earlier on.Additionally, although good parenting resolvesmany problems, it is critical that we ensure publicservices are fit to address wider family problemsto get the best for children.
68
Reaching Out: An Action Plan on Social Exclusion
5.31 The review’s focus will be to establish howto help the most challenging families with themost complex needs.This means making surethat children’s and adults’ services are working in tandem. For example, adults’ services shouldrecognise where adults are also parents andpart of a wider family within which children mayrequire additional support. Likewise, it will look at children’s services as part of a widerpicture where adult needs must be met to help the child.
5.32 This work will build on the systemreforms introduced through Every Child Mattersand the National Service Framework forChildren, as well as taking forward the RespectAction Plan commitment to develop a strategyto address the needs of the most challengingfamilies.
5.33 We recognise that there are severalprogrammes and new initiatives that seek toaddress the problems of children, young peopleand their families, including the parenting
programmes already described, work in adultservices (as discussed in the next section in thischapter) and ongoing work across governmentto ensure that families’ services are increasinglyjoined up.
5.34 The challenge is to bring these strands ofwork into a coherent whole-family approach forfamilies with the greatest needs. Of paramountimportance are: identifying problems acrossfamily members and sharing information;analysing how services engage with and workwith families with additional and complex needs;addressing issues that affect the thresholds forintervening with support for families; andaddressing the workforce so that practitionersare better aware of the multiple problemsaffecting families and their members. A key partof improving the delivery of services for familiesis to better tailor services to their individualneeds, for example through lead professionalswho hold their own budgets (see Box 5.4below).
Box 5.4: Budget-holding lead professionals An important element in promoting the delivery of more responsive and integrated servicesaround the needs of children and young people, and their families, has been the introductionof lead professionals for those who need additional support in a number of areas.The leadprofessional acts as a single point of contact, and ensures that children and families accessappropriate help where needed.This help will often come from many practitioners, so thelead professional helps ensure that support from different agencies can be delivered in amuch more organised way.
The 2006 Budget announced an expansion in the Single Account Holder Pilot to between12 and 15 local authorities, for children and families in need, noting that this role ‘can beenhanced by making the lead professional a single account holder, with a budget tocommission services directly from providers’.75
These pilots, running from summer 2006 for 18 months, will test whether budget-holdingenables lead professionals to more easily access services for children and families, and whetherthis allows children and their families to access services faster and with greater choice.Thesepilots will provide an important evidence base for policies to move budgets closer to thefamilies that need them, and could be part of a future system of delivery with much more userchoice and tailoring of services to individual needs. As already described, budget-holding leadprofessionals also form a key proposal of the Green Paper on children in care.
75 Budget (2006), HMT
69
Chapter 5: Childhood and Teenage Years
Conclusion5.35 Children and teenagers require a range ofsupport services at various stages throughouttheir childhood to protect them against the riskof becoming socially excluded adults. Since1997, investment and reform in education andthe well-being of children and young peoplehave been a major focus of government policy.But we need to do more to ensure that weintervene sufficiently early, that effective practiceis widely spread, that we personalise servicesthrough multi-agency working, and that weperformance manage service delivery to ensurethe most vulnerable are properly supported.We will begin to address these challengesthrough new strategies on children in care andteenage pregnancy, through pilots to establishthe effectiveness of interventions to tacklemental health problems in childhood, andthrough ensuring we deliver a coherent whole-family approach for families at risk.
Chapter 6: Adult Years
SummaryFor adults at risk of, or experiencing, chronic exclusion, the Government will:
• launch pilots to test the effectiveness of alternative approaches toimproving outcomes for people with chaotic lives and multiple needs;
• publish the Leitch Review later this year, setting out progress so far andfurther measures to address the poor lifetime prospects of those withfew qualifications and skills; and
• accelerate the implementation of measures to encourage employmentfor those with more severe mental health problems, including theencouragement of individual placement and support approaches andanti-stigma employer-based campaigns.
71
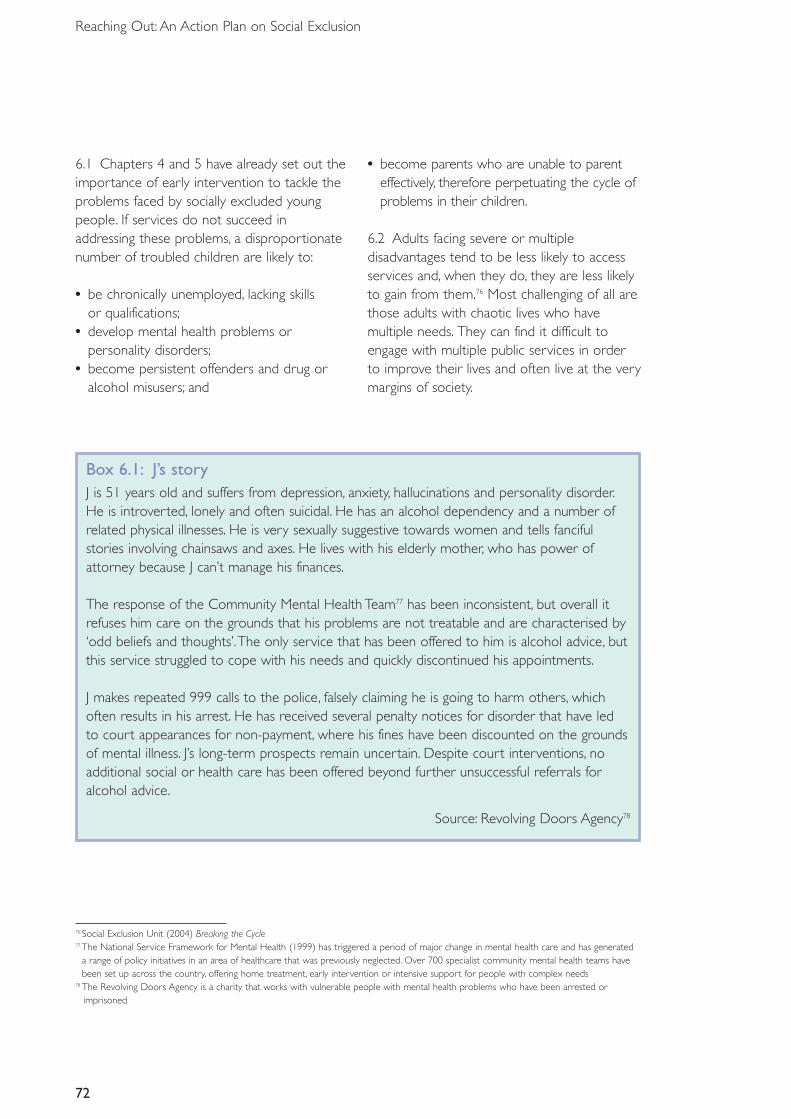
72
Reaching Out: An Action Plan on Social Exclusion
76 Social Exclusion Unit (2004) Breaking the Cycle77 The National Service Framework for Mental Health (1999) has triggered a period of major change in mental health care and has generated
a range of policy initiatives in an area of healthcare that was previously neglected. Over 700 specialist community mental health teams havebeen set up across the country, offering home treatment, early intervention or intensive support for people with complex needs
78 The Revolving Doors Agency is a charity that works with vulnerable people with mental health problems who have been arrested orimprisoned
6.1 Chapters 4 and 5 have already set out theimportance of early intervention to tackle theproblems faced by socially excluded youngpeople. If services do not succeed inaddressing these problems, a disproportionatenumber of troubled children are likely to:
• be chronically unemployed, lacking skills or qualifications;
• develop mental health problems orpersonality disorders;
• become persistent offenders and drug oralcohol misusers; and
• become parents who are unable to parenteffectively, therefore perpetuating the cycle ofproblems in their children.
6.2 Adults facing severe or multipledisadvantages tend to be less likely to accessservices and, when they do, they are less likelyto gain from them.76 Most challenging of all arethose adults with chaotic lives who havemultiple needs. They can find it difficult toengage with multiple public services in orderto improve their lives and often live at the verymargins of society.
Box 6.1: J’s storyJ is 51 years old and suffers from depression, anxiety, hallucinations and personality disorder.He is introverted, lonely and often suicidal. He has an alcohol dependency and a number ofrelated physical illnesses. He is very sexually suggestive towards women and tells fancifulstories involving chainsaws and axes. He lives with his elderly mother, who has power ofattorney because J can’t manage his finances.
The response of the Community Mental Health Team77 has been inconsistent, but overall itrefuses him care on the grounds that his problems are not treatable and are characterised by‘odd beliefs and thoughts’.The only service that has been offered to him is alcohol advice, butthis service struggled to cope with his needs and quickly discontinued his appointments.
J makes repeated 999 calls to the police, falsely claiming he is going to harm others, whichoften results in his arrest. He has received several penalty notices for disorder that have ledto court appearances for non-payment, where his fines have been discounted on the groundsof mental illness. J’s long-term prospects remain uncertain. Despite court interventions, noadditional social or health care has been offered beyond further unsuccessful referrals foralcohol advice.
Source: Revolving Doors Agency78
73
Chapter 6: Adult Years
What has already beenachieved?6.3 Since 1997, the Government hasintroduced a range of policies and programmesdesigned to tackle the problems faced by adultswith severe and multiple disadvantages.Theseprogrammes have offered tailored support inrelation to housing and homelessness, mentalhealth, substance misuse, the criminal justicesystem, skills development and employment.Key achievements and innovations include the following.
• Supporting people with complex needsthrough a wide range of programmes,including Supporting People, which enablesover 1 million vulnerable people to liveindependently. Since 1999, the Governmenthas rolled out 252 assertive outreach teams,which support 18,700 ‘hard-to-reach’ peoplewith mental illness to live in the community.There has also been a 73 per cent reductionin the number of rough sleepers since 1998,achieved by setting up multi-disciplinarycontact and assessment teams (CATs) inknown rough sleeping areas around thecountry, providing hostel bed spaces andensuring that specific needs such as drugabuse are addressed.
• Getting people with complex needs backinto the mainstream through innovations
such as Pathways to Work and the NewDeal for Skills.These have helped theemployment rate for disabled people to risefrom 38.1 per cent in spring 1998 to 46.6per cent in spring 2005.
• Reducing harms caused by those withcomplex needs through initiatives such as theReducing Re-offending Delivery Plan andimplementation of the National OffenderManagement Service, which seek to improvethe services available for adult offenders.Similarly, the Drug Interventions Programmeintegrates interventions to help drug-misusingoffenders to move out of crime and intotreatment.
• Working together to coordinate care forthe most vulnerable. For example, MultiAgency Public Protection Arrangements(MAPPAs) require the prison service, policeand probation services – supported byadditional agencies, including housing, healthand social services – to work together tomanage the risks posed by dangerousoffenders in the community (see Chapter 3).Within mental health services, the CareProgramme Approach has been designed toprovide systematic arrangements forassessing the health and social care needs ofpeople admitted into secondary mentalhealth services.
Box 6.2: Hostels Capital Improvement ProgrammeThe Government has introduced a £90 million Hostels Capital Improvement Programme to help address the needs of former rough sleepers.This is not just about providing betterbuildings – it is about changing the way services are delivered to people who are or havebeen street homeless, particularly those who have slept rough.The key outcome of theProgramme has been to reduce repeat homelessness.
74
Reaching Out: An Action Plan on Social Exclusion
Continuing challenges6.4 Despite this progress, there is still a groupof people with complex needs who are notbenefiting from services because their lives andengagement with services are too chaotic.These adults continue to face poor outcomesin the form of offending, long-term mental andphysical health problems, poor familyrelationships, continuing substance misuse,worklessness and deprivation.
6.5 These high-need individuals may lack basic skills, have mental health problems, bemisusing substances and be at risk of debt andhomelessness. Yet they are often also unableor unwilling to navigate their way throughpublic services to get the support they need.Their contact with services is insteadfrequently driven by problematic behaviourresulting from their chaotic lives – such asanti-social behaviour, criminality and poorparenting – and management revolves aroundsanctions such as prison, loss of tenancy andpossible removal of children.
6.6 Services are focused on delivering to themajority and are not well set up to addressthe needs of those with more complexproblems.Table 6.1 illustrates the wide rangeof services used by individuals with chaoticlives and multiple needs. It indicates thecomplexity of the system and the consequentdifficulties for individuals trying to get support.Each agency separately tries to manage theaspects of the individual’s needs that fall withintheir remit, and funding is similarly fragmentedalong service lines.
6.7 Individual agencies do generally focus onimproving outcomes for the neediest withintheir services (for example the most mentallyill or the most prolific offenders) but oftenmiss those who have multiple needs but needless help from any one service.Thus, peoplemay not meet the threshold of any givenagency to trigger a fuller intervention –despite the scale of their problems or theharms caused to the communities in whichthey live.
Box 6.3: The Prolific and other Priority Offenders programmeThe Prolific and other Priority Offenders (PPO) programme was launched in September2004. It tackles the relatively small, hard-core of offenders who commit a disproportionateamount of crime and cause disproportionate damage to their communities. Evaluationsuggests that offending reduced significantly in PPO cohorts in the first six months of theprogramme, and there has been a 10 per cent reduction in recorded convictions.
Box 6.4: Pathways to WorkIn November 2002, DWP launched Pathways to Work. The initiative supports people onincapacity benefit who would like to work but who face barriers in doing so. Pathways toWork provides work-focused interviews with specialist incapacity benefit personal advisers inJobcentre Plus, financial incentives to return to work and health-focused support. The pilotshave already helped to get 25,000 people back into work, and this programme will be rolledout nationally to be available to all new incapacity benefit claimants by April 2008.
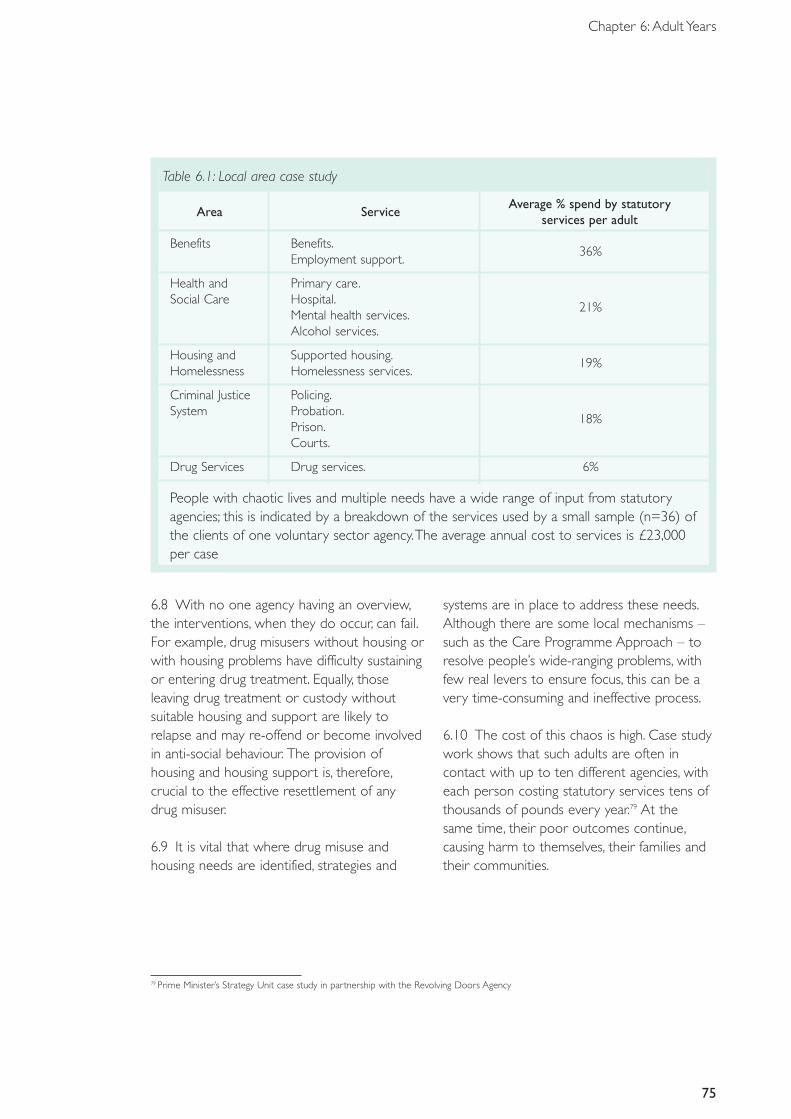
Table 6.1: Local area case study
Area ServiceAverage % spend by statutory
services per adult
Benefits Benefits.36%
Employment support.
Health and Primary care.Social Care Hospital.
21%Mental health services.Alcohol services.
Housing and Supported housing.19%
Homelessness Homelessness services.
Criminal Justice Policing.System Probation.
18%Prison.Courts.
Drug Services Drug services. 6%
75
Chapter 6: Adult Years
People with chaotic lives and multiple needs have a wide range of input from statutoryagencies; this is indicated by a breakdown of the services used by a small sample (n=36) ofthe clients of one voluntary sector agency.The average annual cost to services is £23,000per case
6.8 With no one agency having an overview,the interventions, when they do occur, can fail.For example, drug misusers without housing orwith housing problems have difficulty sustainingor entering drug treatment. Equally, thoseleaving drug treatment or custody withoutsuitable housing and support are likely torelapse and may re-offend or become involvedin anti-social behaviour. The provision ofhousing and housing support is, therefore,crucial to the effective resettlement of anydrug misuser.
6.9 It is vital that where drug misuse andhousing needs are identified, strategies and
systems are in place to address these needs.Although there are some local mechanisms –such as the Care Programme Approach – toresolve people’s wide-ranging problems, withfew real levers to ensure focus, this can be avery time-consuming and ineffective process.
6.10 The cost of this chaos is high. Case studywork shows that such adults are often incontact with up to ten different agencies, witheach person costing statutory services tens ofthousands of pounds every year.79 At the same time, their poor outcomes continue,causing harm to themselves, their families andtheir communities.
79 Prime Minister’s Strategy Unit case study in partnership with the Revolving Doors Agency
76
Reaching Out: An Action Plan on Social Exclusion
Meeting the challenges6.11 The Government’s vision is of publicservices that identify and persistently supportpeople with chaotic lives and multiple needs totake more control over and responsibility fortheir own lives. Some local areas already workwith those hard-to-reach adults with the mostsevere or multiple disadvantages, and there area range of schemes that work within thecurrent system to coordinate services.
6.12 As set out in Chapter 3, this meansensuring that best practice is identified andshared, multi-agency working is promoted,personalised support and challenges areoffered, and that there is a clear sense of accountability, responsibility andperformance management.
Identifying high-need, chaotic adults 6.13 Individual agencies understand who isusing their services, but there is often littleknowledge of the other services their clientsare using or knowledge of needs across
services.The Government will consider how itcan develop data-sharing mechanisms to allowdifferent services to flag concerns over a singleindividual, exploring experience gained fromapproaches such as MAPPA and establishedinformation-sharing protocols.
Identifying what works6.14 There are some international and localexamples of interventions that improveoutcomes for people with chaotic lives andmultiple needs. Yet there are considerable gapsin our knowledge about what works, and thesegaps need to be closed.
Multi-agency working, personalisationand performance management 6.15 Perhaps the single most importantconclusion is that there need to be clearresponsibilities and tailored responses forthose with chaotic lives and multiple needs.This applies both at the strategic level, forplanning service provision and priorities – thelocal strategic partnership – and at the level ofindividual case management.
Box 6.5: Achievements of the National Social Inclusion ProgrammeThe National Social Inclusion Programme coordinates implementation of the action points setout in the Social Exclusion Unit report on Mental Health and Social Exclusion. This work hasresulted in changes being made to benefit rules, greater access to further education throughcollaboration with the Learning and Skills Council, and the development of mental health-specific documents on housing management.The programme has also developed guidance for commissioners on vocational services, day services and direct payments.
ACTION 22: The Government will examine the effectiveness of alternative approaches toimproving outcomes for people with chaotic lives and multiple needs, pilot the mostpromising approaches and use the findings to inform further policy development.
77
Chapter 6: Adult Years
6.16 The Social Exclusion Task Force will workwith relevant departments to develop andevaluate alternative approaches to improvingoutcomes for people with chaotic lives andmultiple needs. Scoping work will involve anumber of innovative local areas and will resultin a better understanding of:
• the lifetime costs and current service useof people who are frequent users ofmultiple services;
• how local areas currently identify andmanage these people;
• what is already being done by local areas toimprove outcomes for people with chaoticlives and multiple needs; and
• how current incentives hinder local agenciesin working together.
6.17 Where quick wins can be identified, wewill implement change through existingdelivery mechanisms and programmes.
6.18 The scoping phase, led by the SocialExclusion Task Force in consultation withrelevant departments and agencies, will becompleted by the end of December 2006 and
will feed directly into a specification for pilots.These will build on structures and innovativeprovision that are already in place, but will testmore radical options for system reform.Theexact nature of the pilots will depend on thefindings from the scoping stage, but it isexpected that they will test:
• active identification and engagement ofhigh-need adults, including informationsharing for high-need adults;
• multi-agency working, such as caseconferencing or panels, enhanced duties tocooperate and joint targets or charge-backs;
• personalisation – through lead practitioners,budget-holding case managers and explicitcompacts with users; and
• performance management at provider orbroker level with an element ofoutcome-based reward.
6.19 The pilots, for which £6 million has beenidentified across government departmentsover three years, will be launched in 2007,with early results feeding back through existingdelivery mechanisms and programmes later inthe year.
78
Reaching Out: An Action Plan on Social Exclusion
Box 6.6: Innovative approaches to adults with multiple needsThe Revolving Doors Agency offers support to people with chaotic lives and multiple needswho have been arrested or imprisoned. Link Workers combine emotional and practicalsupport to help clients gain access to support from a range of services.The schemes workflexibly and persistently across the system, often engaging clients who have fallen through thenet of every other service.This approach has been shown to reduce offending whileimproving access to services.
The Multiple and Complex Needs Initiative is a scheme in Victoria, Australia, which wasestablished to stabilise lives, improve outcomes and use funds more efficiently for clients withcomplex needs. Funds are assigned from existing arrangements following the development ofa care plan.This care plan is case managed by a plan coordinator from within the existingservice system or from a third-sector intensive case management service. Individuals arereferred to the scheme through a regional coordinator and assessed by a panel ofindependent experts. Early indications are of improved coordination between services andmore stability in the lives of clients.
Turning Point Support Link in West Hertfordshire offers intensive community support andassertive outreach support to adults with severe and enduring mental health problems andcomplex needs. The service provides individually tailored community support/service-user-centred care through close inter-agency working and with a whole variety of other servicesand professionals. A qualitative evaluation found that the positive aspects of the service relateto the personalised, flexible, supportive way in which it operates.
The Personality Disorder Development Programme has piloted several innovative serviceapproaches for people with personality disorder and complex needs; as well as support andtraining for mainstream health and social care staff. Early indications show: that services cansuccessfully target people with personality disorders and complex needs; improved outcomesfor individuals; reduced use of other high-cost services such as in-patient psychiatric care;improved partnership working; and improved capabilities within mainstream services tomanage personality disorders.
80 DWP Longitudinal Study
Employment for people with severe mental health problems6.20 Employment is a key factor in bringingsocially excluded people into the mainstream.The onset of mental health problems isassociated with more than double the risk ofleaving employment compared with otherhealth conditions or impairments.There are
currently 70,000 people with severe mentalhealth problems on Incapacity Benefit, costingaround £280 million per year. Around 2,500people join the list each year, most of whomwill spend a lifetime on benefits.80 In 2005/06,the NHS spent £30.7 million on employmentservices for people with more severe mentalhealth problems. However, levels of
79
Chapter 6: Adult Years
Box 6.7: Individual Placement and Support approachThe Individual Placement and Support (IPS) approach is an evidence-based practice built onsix operational principles:
1. Finding employment in integrated/mainstream settings.2. Immediate job search, with minimal pre-vocational training.3. Support from vocational workers based in clinical teams, with employment an integral part
of the overall care plan.4. Job search driven by client choice and preferences.5. Continual assessment of people’s needs with support adjusted as necessary and assistance
in career progression.6. Access to ongoing support on an unlimited time basis once in work.
An example of the successful application of this approach is found in the South West Londonand St George’s Mental Health NHS Trust, which developed a vocational services strategy in2001.This strategy provided support to service users to gain and retain employment,mainstream education and voluntary work, and was based on the best available evidence onvocational rehabilitation for people with severe mental health problems.Throughimplementing this approach and working in partnership with other statutory and voluntarysector providers, the programme enabled 748 service users to gain and retain paidemployment in 2005/06, 387 to enter mainstream education or training, and 221 to take onvoluntary work. Of those supported, 59 per cent had a diagnosis of a psychosis.84
81 Labour Force Survey (Spring 2005). Office for National Statistics82 Healthcare Commission (2005) Survey of Users 2005 – Mental Health Services. London: Healthcare Commission83 Crowther, R, Marshall, M, Bond, G R and Huxley, P (2001) Vocational Rehabilitation for People with Severe Mental Illness (Cochrane Review). The
Cochrane Library84 South West London and St George’s Mental Health NHS Trust, Vocational Services Annual Report 2005/06
worklessness are 89 per cent for people withsevere mental health problems.81
6.21 Evidence shows that people with severemental health problems can and do want towork but over half who are in contact withmental health services do not receive any helpto find work, although they tell us they wouldlike to receive it.82 These people usually end upon long-term Incapacity Benefit and suffer socialexclusion in the form of deprivation, socialisolation and physical ill health.
6.22 There is strong evidence about ‘whatworks’ to enable people with severe mentalhealth problems to gain and retainemployment,83 in particular the IndividualPlacement and Support approach tovocational rehabilitation.Yet despite thisevidence, and that those with severe mentalillness are generally known to local CommunityMental Health Teams and local jobcentres,there are few incentives in the system tosupport implementation of this best practice.
80
Reaching Out: An Action Plan on Social Exclusion
6.23 In February 2006, the Department ofHealth (in conjunction with DWP) issuedguidance to commissioners in health and socialcare on commissioning vocational services forpeople with severe mental health problems.85
This guidance aimed at encouragingcommissioners to implement evidence-basedpractice within vocational services.
6.24 The Government will further supportthe implementation of this guidance bydeveloping dedicated teams within each ofthe eight Care Service ImprovementPartnership (CSIP) regions – led by theNational Social Inclusion Programme andworking closely with regional partners.Theseteams will be drawn from existing public,private and voluntary employmentorganisations and, working in conjunction withregional Government Offices anddevelopment agencies, will provide a practicalprogramme of focused regionalised activity.This work will be led by the Department ofHealth through CSIP’s regional developmentcentres.
6.25 The Government will refocus the Shiftanti-stigma and discrimination programme towork with employers to improveemployment opportunities for people withmental health problems and develop an anti-discriminatory code of practice for employersto help overcome reluctance to take onpeople with more severe mental healthproblems.
6.26 The Government will ensure that theneeds of people with mental health issues,including those with more severe mentalhealth problems, are addressed during thePathways to Work procurement process. DWPwill continue to assess the programme’s impacton people with different conditions (includingthose with mental illness) through the ongoingmonitoring and evaluation of the programme,building on any lessons learnt.
6.27 The Department of Health and DWPwill build on the work already under waythrough Pathways to Work and exploreoptions to develop further incentives to begiven to agencies that successfully enablepeople with severe mental health problems togain and retain work.
6.28 The Government is implementing arange of initiatives aimed at improving adultskills for the most disadvantaged. Skills for Lifeis the national strategy for improving adultliteracy, language and numeracy in order tomeet the PSA target of improving the basicskills levels of 2.25 million adults by 2010.Priority is given to adults without theequivalent of five good GCSEs.The LeitchReview to identify the UK’s optimal skills mixin 2020 to maximise economic growth,productivity and social justice, is consideringthe challenge involved in raising workforceskills at all levels. The Review’s final report willbe published later this year and will containrecommendations to address this issue.
ACTION 23: Building on current guidance and legislation, the Government will developdedicated regional teams to provide further support for the implementation of good practicearound the employment of those with severe mental health problems.
85 National Social Inclusion Programme et al (2006) Vocational Services for People with Severe Mental Health Problems: Commissioning Guidance.DH
81
Chapter 6: Adult Years
Conclusion6.29 The multiple and entrenched problemsfaced by at-risk adults present a formidablechallenge to public services.Yet the potentialprize is great – better outcomes for the mostexcluded alongside fewer long-term harms andlower costs for the rest of the community.
However, while there is general agreementthat having clearer case management andpersistence will benefit such adults, ourapproach is necessarily more tentative and willdeliberately explore a number of differentapproaches to improving outcomes for peoplewith chaotic lives and multiple needs.
Box 6.8: Welfare Reform BillIn July 2006, DWP published the Welfare Reform Bill.The measures in the Bill, together withthe other welfare reform measures, are intended to enable the Government to realise itsaspiration of an 80 per cent employment rate for people of working age and an inclusivesociety where there is opportunity for all. Key elements of the reform proposals include:
• a new Employment and Support Allowance that will simplify the existing benefits system forthose whose health affects their capacity for work;
• a focus on early intervention, with increased support to employers and employees inmanaging health in the workplace, improved absence and return to work management;
• more customer contact and more employment advice and support for individuals withhealth conditions to enable them to realise their ambition to return to work;
• housing benefit reform, which includes the national roll-out of the Local Housing Allowanceand a housing benefit sanction for those people facing eviction for anti-social behaviourwho will not accept the support they need to change their behaviour; and
• the ongoing development of disability rights to provide a level playing field for those withdisabilities.

Section IV: The futureChapter 7: Next steps
83
84
Reaching Out: An Action Plan on Social Exclusion
7.1 This report is the next chapter in theGovernment’s attack on the root causes ofdeep social exclusion, extending opportunityto more people in society than ever before.Tremendous progress has been made since1997 in tackling wider poverty anddisadvantage and many millions of peoplehave benefited. It is precisely because of thissuccess that the most disadvantaged andpersistently excluded groups have becomemore visible. It has also become apparent that what works for the vast majority ofdisadvantaged groups might not work for the most hard-to-reach individuals.
7.2 This Government, and many keystakeholders, are convinced that earlyintervention is often more cost-effective; thathard-to-reach groups can be identified; andthat effective interventions for these groups doexist.The challenge we therefore face andaddress in this Action Plan is how to shift the
balance away from reaction and more towardsearly identification and intervention.
7.3 As set out in this Action Plan, Governmentaction to tackle deep social exclusion will beguided by five guiding principles:
• better identification and early intervention;• systematic identification of what works;• better multi-agency working;• personalisation, and rights and responsibilities
where appropriate; and• supporting achievement and managing
underperformance.
7.4 As the table below sets out, there are manyother important chapters that will follow theAction Plan over the coming year.The SocialExclusion Task Force will work closely with alldepartments to ensure that the needs and theunique challenges of the most socially excludedare addressed.
Table 7.1: Next steps
Publication Lead dept Timing
Teenage Pregnancy Strategy.This will have a DfES Sept 06particular focus on areas with high rates and on tackling the underlying causes of teenage pregnancy.
National Action Plan for Social Inclusion.This DWP Sept 06Plan is submitted to the EU Commission every three years and sets out how each EU member state is making a decisive impact on the eradication of poverty.
Opportunity for All.This is the Government’s annual DWP Oct 06report measuring success in tackling poverty and social exclusion.
Children in Care Green Paper.This will DfES Oct 06explore how we can further improve outcomes for this high-risk group, including proposals on individual budget-holding arrangements.
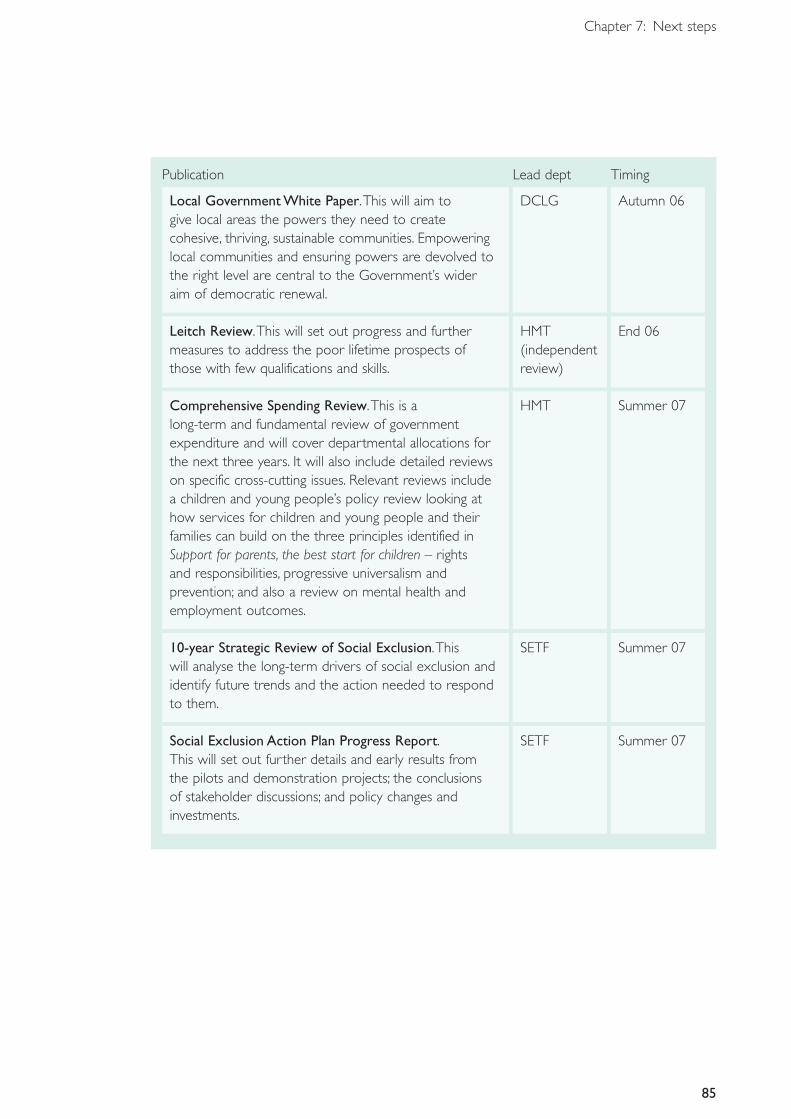
85
Chapter 7: Next steps
Publication Lead dept Timing
Local Government White Paper.This will aim to DCLG Autumn 06give local areas the powers they need to create cohesive, thriving, sustainable communities. Empowering local communities and ensuring powers are devolved to the right level are central to the Government’s wider aim of democratic renewal.
Leitch Review.This will set out progress and further HMT End 06measures to address the poor lifetime prospects of (independent those with few qualifications and skills. review)
Comprehensive Spending Review.This is a HMT Summer 07long-term and fundamental review of government expenditure and will cover departmental allocations for the next three years. It will also include detailed reviews on specific cross-cutting issues. Relevant reviews include a children and young people’s policy review looking at how services for children and young people and their families can build on the three principles identified in Support for parents, the best start for children – rights and responsibilities, progressive universalism and prevention; and also a review on mental health and employment outcomes.
10-year Strategic Review of Social Exclusion.This SETF Summer 07will analyse the long-term drivers of social exclusion and identify future trends and the action needed to respond to them.
Social Exclusion Action Plan Progress Report. SETF Summer 07This will set out further details and early results from the pilots and demonstration projects; the conclusions of stakeholder discussions; and policy changes and investments.
86
Reaching Out: An Action Plan on Social Exclusion
7.5 This Government will leave no onebehind. In this period of unprecedentedeconomic growth and social progress, our taskis to further extend the opportunities enjoyedby the vast majority of people in the UK today to those whose lives have been characterisedby deprivation and exclusion.With our shared vision and approach, coupled withmeaningful partnership between deliveryagencies and people in need, we can, and must,tackle the root causes of persistent deprivationin this country.
7.6 But social exclusion cannot be addressed bygovernment alone.The wider community has akey role to play too.The care system is a goodexample of ordinary citizens taking up a socialchallenge by fostering, and sometimes adopting,while progressive employers sometimes providevaluable employment opportunities to peoplewith long-term mental health challenges. Butmost of all, of course, people suffering socialexclusion, and those immediately around them,must want to progress too by seizing theopportunities that are available to them.
How to comment on the SocialExclusion Action Plan7.7 This Action Plan signals our direction of travel.We want to hear from you about its contents.
7.8 In particular we would welcome yourcomments on the principles and actions withinthe Plan.We would particularly welcomecomments from people working on theground delivering services, and want to hearabout innovative examples we can use intaking forward this important work.We alsoreiterate our invitation in Chapter 3 for localareas to come forward with innovative andradical proposals for provision around thosemost at risk.
7.9 Please contact us at:
• by email: [email protected]
• by post: Social Exclusion Action PlanPrime Minister’s Strategy UnitRoom 4.17 Admiralty Arch The Mall London SW1A 2WH
Annex A: Grid of policy actions
87
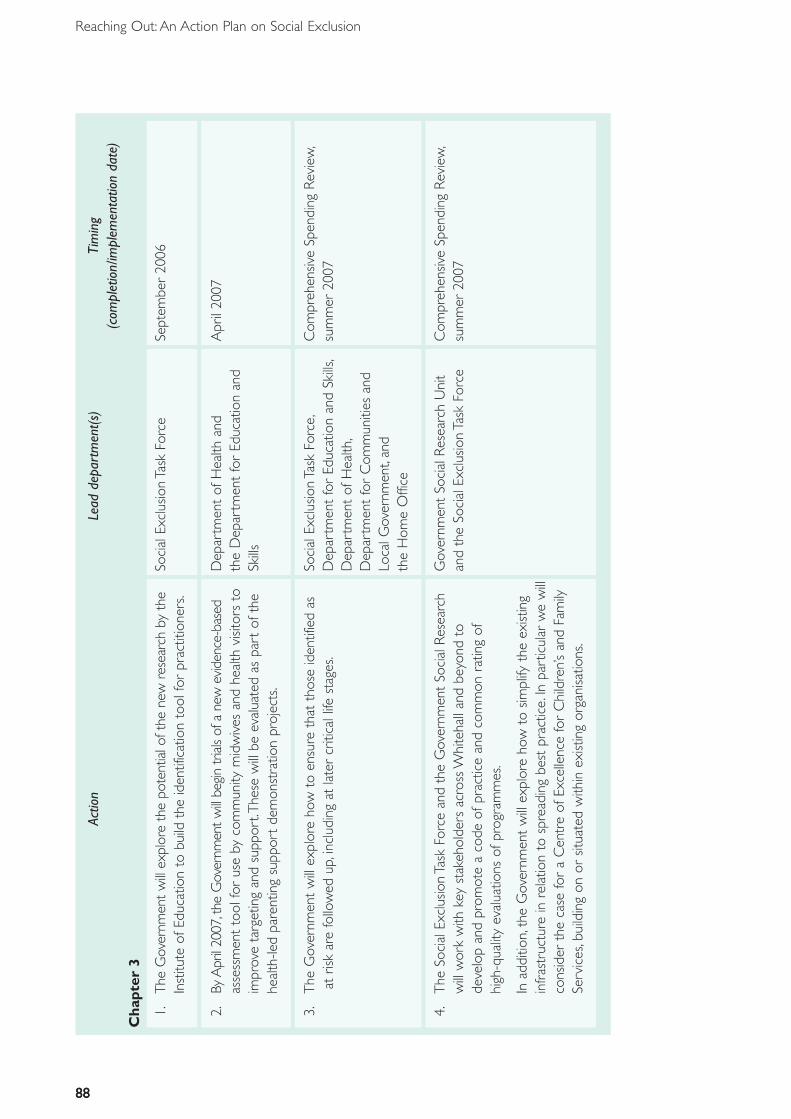
88
Reaching Out: An Action Plan on Social Exclusion
88
Actio
nLe
adde
part
men
t(s)
Tim
ing
(com
plet
ion/
impl
emen
tatio
nda
te)
Ch
apte
r3
1.Th
eG
over
nmen
tw
illex
plor
eth
epo
tent
ialo
fthe
new
rese
arch
byth
eSo
cial
Excl
usio
nTa
skFo
rce
Sept
embe
r20
06In
stitu
teof
Educ
atio
nto
build
the
iden
tific
atio
nto
olfo
rpr
actit
ione
rs.
2.By
Apr
il20
07,t
heG
over
nmen
twill
begi
ntr
ials
ofa
new
evid
ence
-bas
edD
epar
tmen
tof
Hea
lthan
dA
pril
2007
asse
ssm
ent
tool
for
use
byco
mm
unity
mid
wiv
esan
dhe
alth
visit
ors
toth
eD
epar
tmen
tfo
rEd
ucat
ion
and
impr
ove
targ
etin
gan
dsu
ppor
t.T
hese
will
beev
alua
ted
aspa
rtof
the
Skill
she
alth
-led
pare
ntin
gsu
ppor
tde
mon
stra
tion
proj
ects
.
3.T
heG
over
nmen
tw
illex
plor
eho
wto
ensu
reth
atth
ose
iden
tifie
das
Soci
alEx
clus
ion
Task
Forc
e,C
ompr
ehen
sive
Spen
ding
Rev
iew
,at
risk
are
follo
wed
up,i
nclu
ding
atla
ter
criti
call
ifest
ages
.D
epar
tmen
tfo
rEd
ucat
ion
and
Skill
s,su
mm
er20
07D
epar
tmen
tof
Hea
lth,
Dep
artm
ent
for
Com
mun
ities
and
Loca
lGov
ernm
ent,
and
the
Hom
eO
ffice
4.T
heSo
cial
Excl
usio
nTa
skFo
rce
and
the
Gov
ernm
ent
Soci
alR
esea
rch
Gov
ernm
ent
Soci
alR
esea
rch
Uni
tC
ompr
ehen
sive
Spen
ding
Rev
iew
,w
illw
ork
with
key
stak
ehol
ders
acro
ssW
hite
hall
and
beyo
ndto
and
the
Soci
alEx
clus
ion
Task
Forc
esu
mm
er20
07de
velo
pan
dpr
omot
ea
code
ofpr
actic
ean
dco
mm
onra
ting
ofhi
gh-q
ualit
yev
alua
tions
ofpr
ogra
mm
es.
Inad
ditio
n,th
eG
over
nmen
tw
illex
plor
eho
wto
simpl
ifyth
eex
istin
gin
fras
truc
ture
inre
latio
nto
spre
adin
gbe
stpr
actic
e.In
part
icul
arw
ew
illco
nsid
erth
eca
sefo
ra
Cen
tre
ofEx
celle
nce
for
Chi
ldre
n’s
and
Fam
ilySe
rvic
es,b
uild
ing
onor
situa
ted
with
inex
istin
gor
gani
satio
ns.
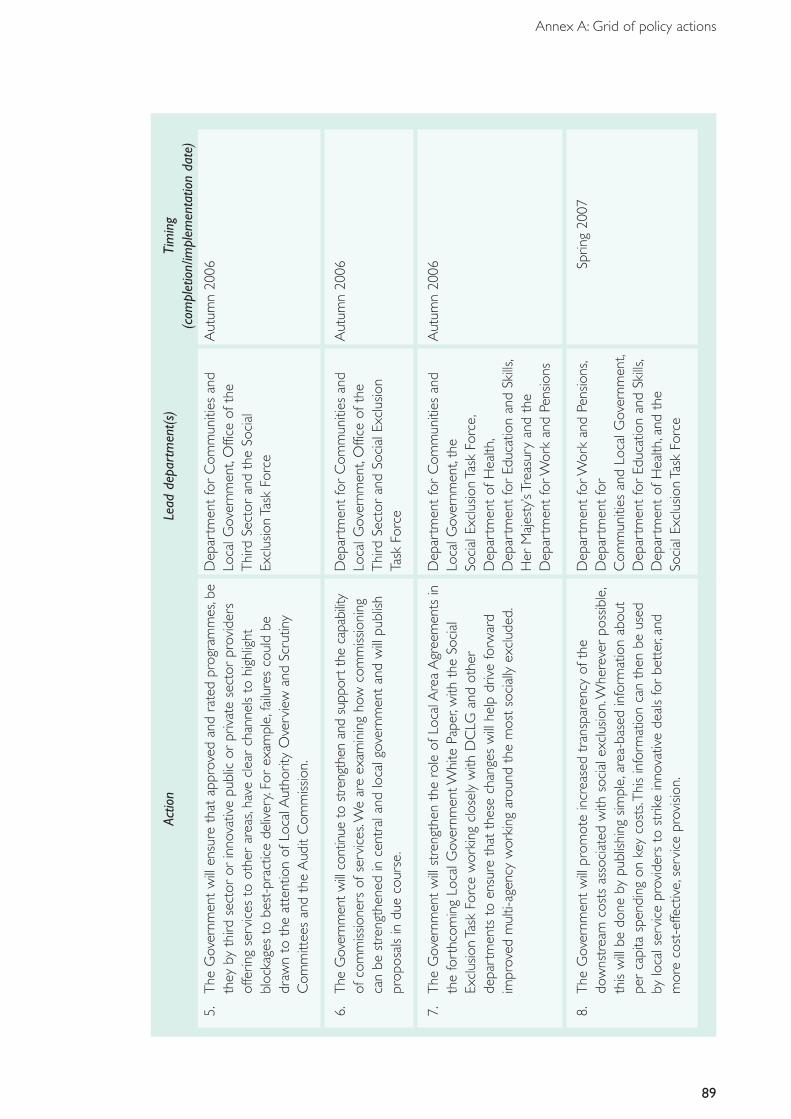
Annex A: Grid of policy actions
89
Actio
nLe
adde
part
men
t(s)
Tim
ing
(com
plet
ion/
impl
emen
tatio
nda
te)
5.T
heG
over
nmen
tw
illen
sure
that
appr
oved
and
rate
dpr
ogra
mm
es,b
eD
epar
tmen
tfo
rC
omm
uniti
esan
dA
utum
n20
06th
eyby
third
sect
oror
inno
vativ
epu
blic
orpr
ivat
ese
ctor
prov
ider
sLo
calG
over
nmen
t,O
ffice
ofth
eof
ferin
gse
rvic
esto
othe
rar
eas,
have
clea
rch
anne
lsto
high
light
Thi
rdSe
ctor
and
the
Soci
albl
ocka
ges
tobe
st-p
ract
ice
deliv
ery.
For
exam
ple,
failu
res
coul
dbe
Excl
usio
nTa
skFo
rce
draw
nto
the
atte
ntio
nof
Loca
lAut
horit
yO
verv
iew
and
Scru
tiny
Com
mitt
ees
and
the
Aud
itC
omm
issio
n.
6.Th
eG
over
nmen
tw
illco
ntin
ueto
stre
ngth
enan
dsu
ppor
tth
eca
pabi
lity
Dep
artm
ent
for
Com
mun
ities
and
Aut
umn
2006
ofco
mm
issio
ners
ofse
rvic
es.W
ear
eex
amin
ing
how
com
miss
ioni
ngLo
calG
over
nmen
t,O
ffice
ofth
eca
nbe
stre
ngth
ened
ince
ntra
land
loca
lgov
ernm
ent
and
will
publ
ishT
hird
Sect
oran
dSo
cial
Excl
usio
npr
opos
als
indu
eco
urse
.Ta
skFo
rce
7.T
heG
over
nmen
tw
illst
reng
then
the
role
ofLo
calA
rea
Agr
eem
ents
inD
epar
tmen
tfo
rC
omm
uniti
esan
dA
utum
n20
06th
efo
rthc
omin
gLo
calG
over
nmen
tWhi
tePa
per,
with
the
Soci
alLo
calG
over
nmen
t,th
eEx
clus
ion
Task
Forc
ew
orki
ngcl
osel
yw
ithD
CLG
and
othe
rSo
cial
Excl
usio
nTa
skFo
rce,
depa
rtm
ents
toen
sure
that
thes
ech
ange
sw
illhe
lpdr
ive
forw
ard
Dep
artm
ent
ofH
ealth
,im
prov
edm
ulti-
agen
cyw
orki
ngar
ound
the
mos
tso
cial
lyex
clud
ed.
Dep
artm
ent
for
Educ
atio
nan
dSk
ills,
Her
Maj
esty
’sTr
easu
ryan
dth
eD
epar
tmen
tfo
rWor
kan
dPe
nsio
ns
8.T
heG
over
nmen
tw
illpr
omot
ein
crea
sed
tran
spar
ency
ofth
eD
epar
tmen
tfo
rWor
kan
dPe
nsio
ns,
Sprin
g20
07do
wns
trea
mco
sts
asso
ciat
edw
ithso
cial
excl
usio
n.W
here
ver
poss
ible
,D
epar
tmen
tfo
rth
isw
illbe
done
bypu
blish
ing
simpl
e,ar
ea-b
ased
info
rmat
ion
abou
tC
omm
uniti
esan
dLo
calG
over
nmen
t,pe
rca
pita
spen
ding
onke
yco
sts.
Thi
sin
form
atio
nca
nth
enbe
used
Dep
artm
ent
for
Educ
atio
nan
dSk
ills,
bylo
cals
ervi
cepr
ovid
ers
tost
rike
inno
vativ
ede
als
for
bett
er,a
ndD
epar
tmen
tof
Hea
lth,a
ndth
em
ore
cost
-effe
ctiv
e,se
rvic
epr
ovisi
on.
Soci
alEx
clus
ion
Task
Forc
e
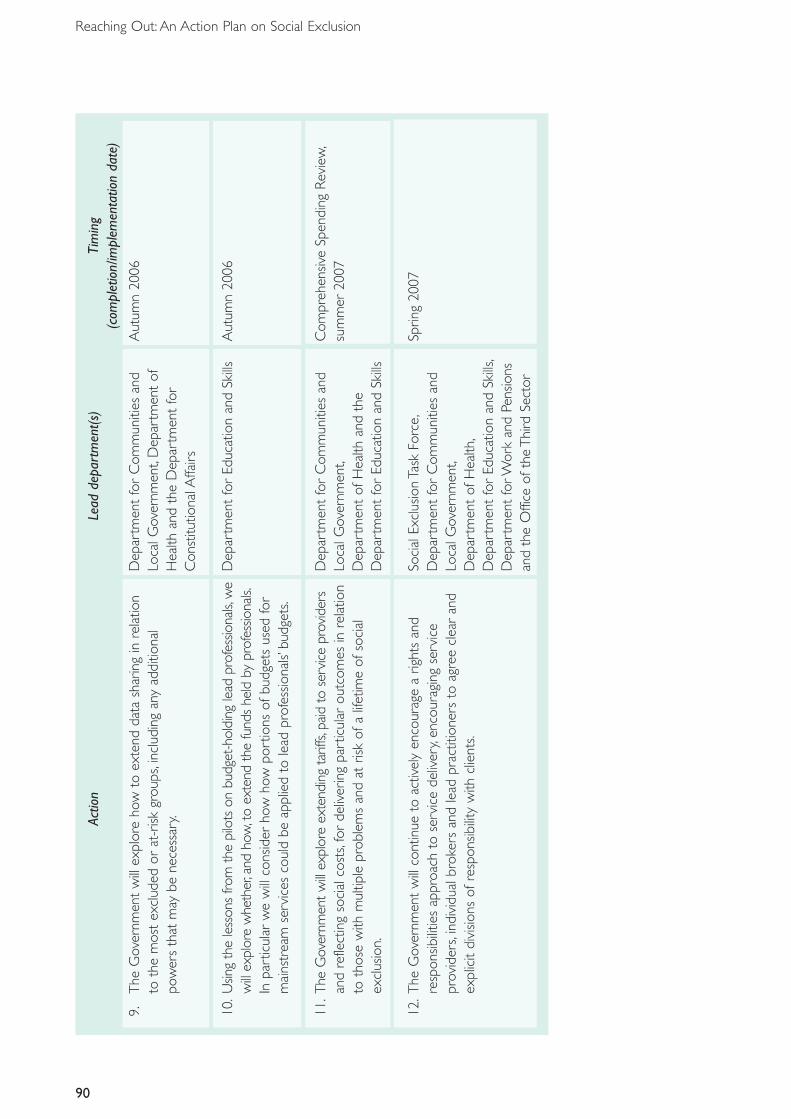
90
Reaching Out: An Action Plan on Social Exclusion
Actio
nLe
adde
part
men
t(s)
Tim
ing
(com
plet
ion/
impl
emen
tatio
nda
te)
9.T
heG
over
nmen
tw
illex
plor
eho
wto
exte
ndda
tash
arin
gin
rela
tion
Dep
artm
ent
for
Com
mun
ities
and
Aut
umn
2006
toth
em
ost
excl
uded
orat
-risk
grou
ps,i
nclu
ding
any
addi
tiona
lLo
calG
over
nmen
t,D
epar
tmen
tof
pow
ers
that
may
bene
cess
ary.
Hea
lthan
dth
eD
epar
tmen
tfo
rC
onst
itutio
nalA
ffairs
10.U
sing
the
less
ons
from
the
pilo
tson
budg
et-h
oldi
ngle
adpr
ofes
siona
ls,w
eD
epar
tmen
tfo
rEd
ucat
ion
and
Skill
sA
utum
n20
06w
illex
plor
ew
heth
er,a
ndho
w,t
oex
tend
the
fund
she
ldby
prof
essio
nals.
Inpa
rtic
ular
we
will
cons
ider
how
how
port
ions
ofbu
dget
sus
edfo
rm
ains
trea
mse
rvic
esco
uld
beap
plie
dto
lead
prof
essio
nals’
budg
ets.
11.T
heG
over
nmen
tw
illex
plor
eex
tend
ing
tarif
fs,p
aid
tose
rvic
epr
ovid
ers
Dep
artm
ent
for
Com
mun
ities
and
Com
preh
ensiv
eSp
endi
ngR
evie
w,
and
refle
ctin
gso
cial
cost
s,fo
rde
liver
ing
part
icul
arou
tcom
esin
rela
tion
Loca
lGov
ernm
ent,
sum
mer
2007
toth
ose
with
mul
tiple
prob
lem
san
dat
risk
ofa
lifet
ime
ofso
cial
Dep
artm
ent
ofH
ealth
and
the
excl
usio
n.D
epar
tmen
tfo
rEd
ucat
ion
and
Skill
s
12.T
heG
over
nmen
tw
illco
ntin
ueto
activ
ely
enco
urag
ea
right
san
dSo
cial
Excl
usio
nTa
skFo
rce,
Sprin
g20
07re
spon
sibili
ties
appr
oach
tose
rvic
ede
liver
y,en
cour
agin
gse
rvic
eD
epar
tmen
tfo
rC
omm
uniti
esan
dpr
ovid
ers,
indi
vidu
albr
oker
san
dle
adpr
actit
ione
rsto
agre
ecl
ear
and
Loca
lGov
ernm
ent,
expl
icit
divi
sions
ofre
spon
sibili
tyw
ithcl
ient
s.D
epar
tmen
tof
Hea
lth,
Dep
artm
ent
for
Educ
atio
nan
dSk
ills,
Dep
artm
ent
forW
ork
and
Pens
ions
and
the
Offi
ceof
the
Thi
rdSe
ctor
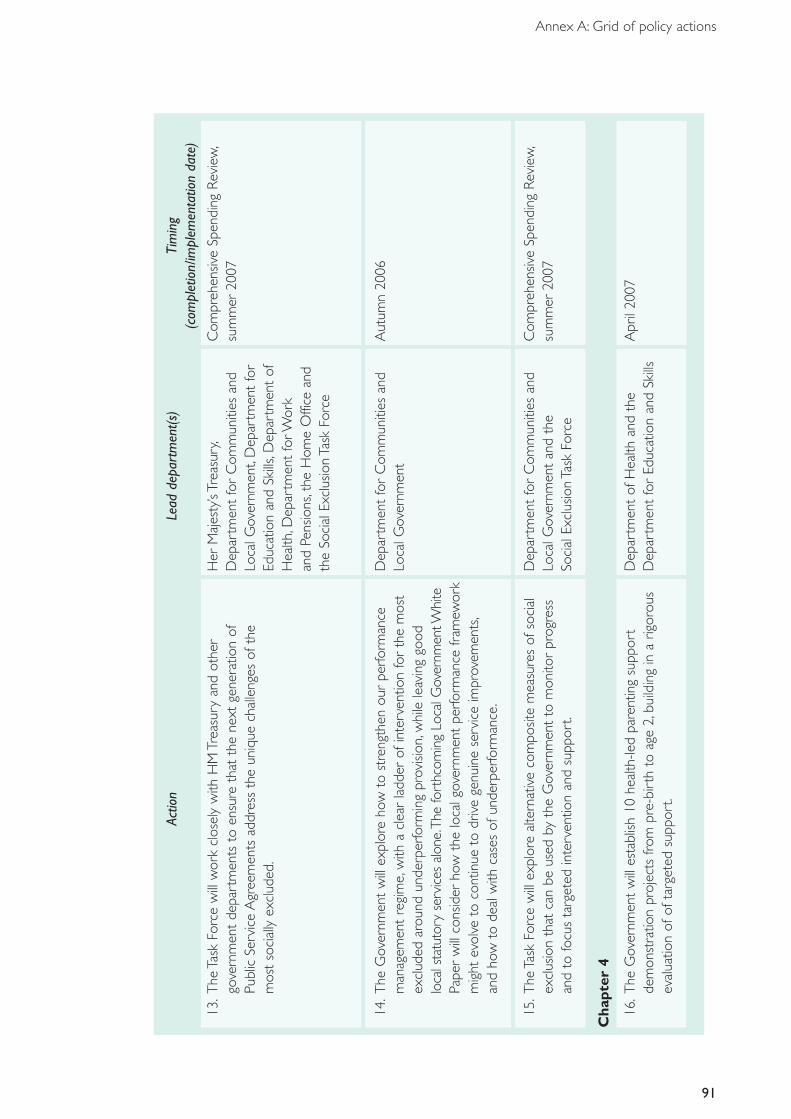
91
Annex A: Grid of policy actions
Actio
nLe
adde
part
men
t(s)
Tim
ing
(com
plet
ion/
impl
emen
tatio
nda
te)
13.T
heTa
skFo
rce
will
wor
kcl
osel
yw
ithH
MTr
easu
ryan
dot
her
Her
Maj
esty
’sTr
easu
ry,
Com
preh
ensiv
eSp
endi
ngR
evie
w,
gove
rnm
ent
depa
rtm
ents
toen
sure
that
the
next
gene
ratio
nof
Dep
artm
ent
for
Com
mun
ities
and
sum
mer
2007
Publ
icSe
rvic
eA
gree
men
tsad
dres
sth
eun
ique
chal
leng
esof
the
Loca
lGov
ernm
ent,
Dep
artm
ent
for
mos
tso
cial
lyex
clud
ed.
Educ
atio
nan
dSk
ills,
Dep
artm
ent
ofH
ealth
,Dep
artm
ent
forW
ork
and
Pens
ions
,the
Hom
eO
ffice
and
the
Soci
alEx
clus
ion
Task
Forc
e
14.T
heG
over
nmen
tw
illex
plor
eho
wto
stre
ngth
enou
rpe
rform
ance
Dep
artm
ent
for
Com
mun
ities
and
Aut
umn
2006
man
agem
ent
regi
me,
with
acl
ear
ladd
erof
inte
rven
tion
for
the
mos
tLo
calG
over
nmen
tex
clud
edar
ound
unde
rper
form
ing
prov
ision
,whi
lele
avin
ggo
odlo
cals
tatu
tory
serv
ices
alon
e.Th
efo
rthc
omin
gLo
calG
over
nmen
tWhi
tePa
per
will
cons
ider
how
the
loca
lgov
ernm
ent
perfo
rman
cefr
amew
ork
mig
htev
olve
toco
ntin
ueto
driv
ege
nuin
ese
rvic
eim
prov
emen
ts,
and
how
tode
alw
ithca
ses
ofun
derp
erfo
rman
ce.
15.T
heTa
skFo
rce
will
expl
ore
alte
rnat
ive
com
posit
em
easu
res
ofso
cial
Dep
artm
ent
for
Com
mun
ities
and
Com
preh
ensiv
eSp
endi
ngR
evie
w,
excl
usio
nth
atca
nbe
used
byth
eG
over
nmen
tto
mon
itor
prog
ress
Loca
lGov
ernm
ent
and
the
sum
mer
2007
and
tofo
cus
targ
eted
inte
rven
tion
and
supp
ort.
Soci
alEx
clus
ion
Task
Forc
e
Ch
apte
r4
16.T
heG
over
nmen
tw
illes
tabl
ish10
heal
th-le
dpa
rent
ing
supp
ort
Dep
artm
ent
ofH
ealth
and
the
Apr
il20
07de
mon
stra
tion
proj
ects
from
pre-
birt
hto
age
2,bu
ildin
gin
arig
orou
sD
epar
tmen
tfo
rEd
ucat
ion
and
Skill
sev
alua
tion
ofof
targ
eted
supp
ort.
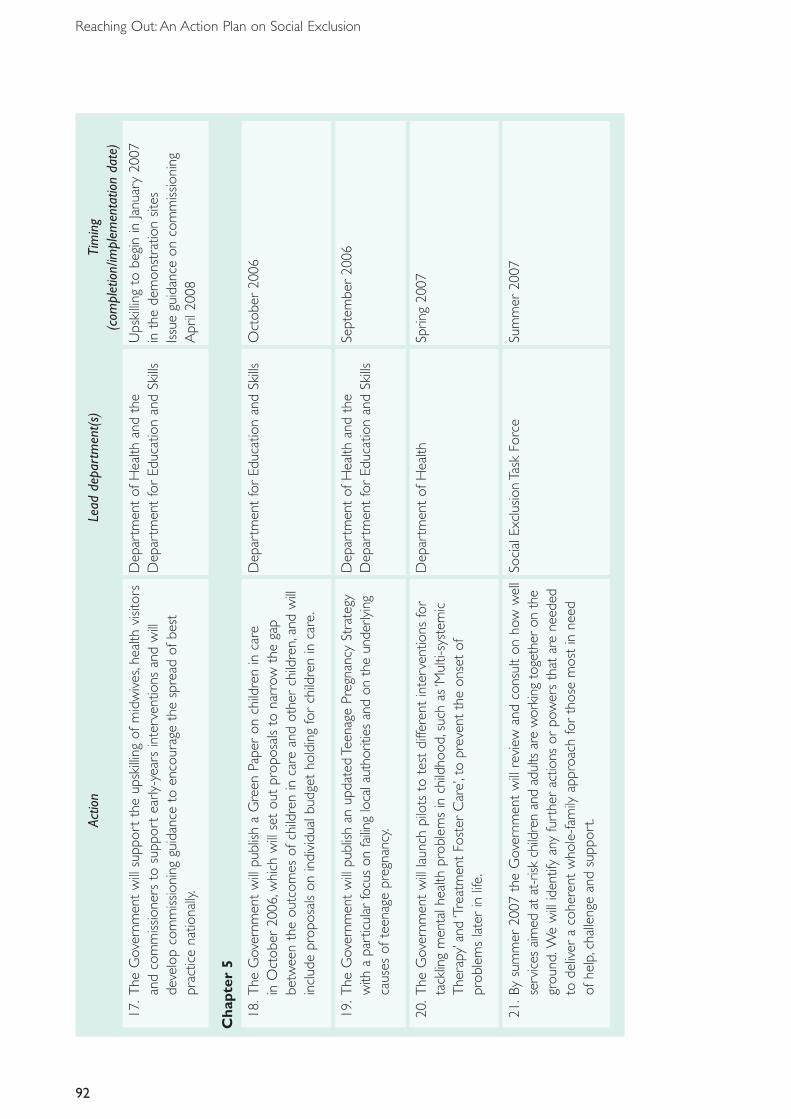
92
Reaching Out: An Action Plan on Social Exclusion
Actio
nLe
adde
part
men
t(s)
Tim
ing
(com
plet
ion/
impl
emen
tatio
nda
te)
17.T
heG
over
nmen
tw
illsu
ppor
tth
eup
skill
ing
ofm
idw
ives
,hea
lthvi
sitor
sD
epar
tmen
tof
Hea
lthan
dth
eU
pski
lling
tobe
gin
inJa
nuar
y20
07an
dco
mm
issio
ners
tosu
ppor
tea
rly-y
ears
inte
rven
tions
and
will
Dep
artm
ent
for
Educ
atio
nan
dSk
ills
inth
ede
mon
stra
tion
sites
deve
lop
com
miss
ioni
nggu
idan
ceto
enco
urag
eth
esp
read
ofbe
stIss
uegu
idan
ceon
com
miss
ioni
ngpr
actic
ena
tiona
lly.
Apr
il20
08
Ch
apte
r5
18.T
heG
over
nmen
tw
illpu
blish
aG
reen
Pape
ron
child
ren
inca
reD
epar
tmen
tfo
rEd
ucat
ion
and
Skill
sO
ctob
er20
06in
Oct
ober
2006
,whi
chw
illse
tou
tpr
opos
als
tona
rrow
the
gap
betw
een
the
outc
omes
ofch
ildre
nin
care
and
othe
rch
ildre
n,an
dw
illin
clud
epr
opos
als
onin
divi
dual
budg
etho
ldin
gfo
rch
ildre
nin
care
.
19.T
heG
over
nmen
tw
illpu
blish
anup
date
dTe
enag
ePr
egna
ncy
Stra
tegy
Dep
artm
ent
ofH
ealth
and
the
Sept
embe
r20
06w
itha
part
icul
arfo
cus
onfa
iling
loca
laut
horit
ies
and
onth
eun
derly
ing
Dep
artm
ent
for
Educ
atio
nan
dSk
ills
caus
esof
teen
age
preg
nanc
y.
20.T
heG
over
nmen
tw
illla
unch
pilo
tsto
test
diffe
rent
inte
rven
tions
for
Dep
artm
ent
ofH
ealth
Sprin
g20
07ta
cklin
gm
enta
lhea
lthpr
oble
ms
inch
ildho
od,s
uch
as‘M
ulti-
syst
emic
The
rapy
’and
‘Tre
atm
ent
Fost
erC
are’
,to
prev
ent
the
onse
tof
prob
lem
sla
ter
inlif
e.
21.B
ysu
mm
er20
07th
eG
over
nmen
tw
illre
view
and
cons
ult
onho
ww
ell
Soci
alEx
clus
ion
Task
Forc
eSu
mm
er20
07se
rvic
esai
med
atat
-risk
child
ren
and
adul
tsar
ew
orki
ngto
geth
eron
the
grou
nd.W
ew
illid
entif
yan
yfu
rthe
rac
tions
orpo
wer
sth
atar
ene
eded
tode
liver
aco
here
ntw
hole
-fam
ilyap
proa
chfo
rth
ose
mos
tin
need
ofhe
lp,c
halle
nge
and
supp
ort.
93
Annex A: Grid of policy actions
Actio
nLe
adde
part
men
t(s)
Tim
ing
(com
plet
ion/
impl
emen
tatio
nda
te)
Ch
apte
r6
22.T
heG
over
nmen
tw
illex
amin
eth
eef
fect
iven
ess
ofal
tern
ativ
eD
epar
tmen
tfo
rC
omm
uniti
esan
dSc
opin
gph
ase:
win
ter
2006
appr
oach
esto
impr
ovin
gou
tcom
esfo
rpe
ople
with
chao
ticliv
esan
dan
dLo
calG
over
nmen
t,th
eH
ome
Pilo
tsbe
gin:
sprin
g20
07m
ultip
lene
eds,
pilo
tth
em
ost
prom
ising
appr
oach
esan
dus
eth
eO
ffice
,Dep
artm
ent
ofH
ealth
,fin
ding
sto
info
rmfu
rthe
rpo
licy
deve
lopm
ent.
Dep
artm
ent
forW
ork
and
Pens
ions
and
the
Soci
alEx
clus
ion
Task
Forc
e
23.B
uild
ing
oncu
rren
tgu
idan
cean
dle
gisla
tion,
the
Gov
ernm
ent
will
Dep
artm
ent
forW
ork
and
Pens
ions
Apr
il20
07de
velo
pde
dica
ted
regi
onal
team
sto
prov
ide
furt
her
supp
ort
for
the
and
the
Dep
artm
ent
ofH
ealth
impl
emen
tatio
nof
good
prac
tice
arou
ndem
ploy
men
tof
thos
ew
ithse
vere
men
talh
ealth
prob
lem
s.

Annex B: Social Exclusion Task Force
The Social Exclusion Task Force (SETF) was set up in June 2006. Its missionis to further extend the opportunities enjoyed by the vast majority ofpeople in the UK today to those whose lives have been characterised bydeprivation and exclusion.
Initially the Task Force has concentrated on identifying those most at riskand focused on specific hard-to-reach groups, including children in care,people with mental health problems and teenagers at risk of pregnancy.Wewill work closely with all departments to ensure that the needs of themost socially excluded are addressed.
The Task Force draws together the expertise of some staff from theformer Social Exclusion Unit (SEU) in the Department for Communitiesand Local Government (DCLG) and policy specialists from the PrimeMinister’s Strategy Unit. It is based in the Cabinet Office and reports toHilary Armstrong, Minister for the Cabinet Office and Social Exclusion, andParliamentary Secretary Pat McFadden.
The Social Exclusion Task Force is committed to:
• evidence-based policy-making;• working together with stakeholders; and• giving a voice to disadvantaged groups within government.
95
96
Reaching Out: An Action Plan on Social Exclusion
The Social Exclusion Task Force consists of thefollowing people:
Matt Barnes is seconded from the NationalCentre for Social Research.
Alistair Bogaars worked at the Home Officein the Community Safety and LocalGovernment Unit on Local Area Agreements.
Rachael Clapson from the SEU worked on avariety of short projects on strategy,empowerment, asset inequality and frequentmovers. Previously she worked forHM Treasury and on housing policy.
Tim Crosier previously was a policy analystwith the Australian Government Departmentof Family and Community Services.
Chris Cuthbert was head of Research at theSEU, worked for a number of years in theprivate sector and DfES where he specialisedin policies relating to children and families –particularly relating to prevention andintegrated children’s services.
Claire Etches led the SEU’s work on mentalhealth and carried out research on the impactof moving frequently. Prior to this, Claireworked in the Foreign Office.
Ajay Gambhir worked at DWP as a labourmarket economist. He is a policy analyst at thePMSU, and previously also spent several yearsworking as a consultant in the ICT industry.
David Halpern is Acting Director of the SocialExclusion Task Force. He is Chief Analyst andSenior Policy Adviser at the Prime Minister’sStrategy Unit, and previously he held posts atCambridge, Oxford and Harvard.
Axel Heitmueller joined the PMSU fromDWP where he was an economic adviser. Healso works as a research associate at theLondon Business School on Eastern Europeanlabour markets and immigration.
Matt Hudson is seconded from the Centre forEconomic and Social Inclusion.
Alun Hughes has worked for DWP, theScotland Office and the Cabinet Office andhas produced various social exclusion reportsin relation to neighbourhood renewal,transport, jobs and enterprise and youngadults with complex needs.
Andy Jackson worked previously in the SEU.He trained as a teacher and has an activeinterest in music education and specialeducational needs.
David Jackson has worked for an independentthink tank and the Home Office.
Hinna Jawaid has previously worked in theSEU and DWP.
Simon Kearney-Mitchell leads on externalrelations and publications, and was previouslyat the SEU.
Kate O’Neill has worked in the Office forDisability Issues and in the voluntary sector onregeneration and financial exclusion issues.
Paul Oroyemi previously worked as an analystin the SEU and HM Treasury.
Luke O’Shea led the SEU report Sure Start toLater Life, and previously worked for DfES onthe Sure Start programme.
97
Annex B: Social Exclusion Task Force
John Pavel is a member of the PMSU, has heldnumerous posts within the Civil Serviceincluding work on public service reform,terrorism, indirect taxation and EU financialservices legislation and and was previously thePrincipal Private Secretary to the PermanentSecretary at the Treasury.
Miles Rinaldi also works for St Georges NHSMental Health Trust and the Department ofHealth.
Allison Smith has a research background inolder people and social exclusion in Englandand Canada and recently completed her PhDin Social Gerontology.
Julie Stephenson was seconded from DCLGand previously worked in the Department forConstitutional Affairs where she workedextensively on family and children’s legislation.
Liz Tatlow is seconded from Matrix Researchand Consultancy Ltd where she led the localhealth team, working with communities on arange of projects.
Arvind Thandi works on external relations andpublications and was previously at the SEU.
Cabinet Office70 WhitehallLondon SW1A 2AS
Telephone: 020 7276 1234
E-mail: [email protected] address: www.cabinetoffice.gov.uk
Publication date: September 2006
© Crown copyright 2006
The text in this document may be reproduced free of charge in any format or media without requiringspecific permission.This is subject to the material not being used in a derogatory manner or in amisleading context.The source of the material must be acknowledged as Crown copyright and the titleof the document must be included when reproduced as part of another publication or service.
The material used in this publication is constituted from 75% post-consumer waste and 25% virgin fibre
Ref: 276684/0906/D16
Prepared for the Cabinet Office by COI
All of the photography has been posed by models and published with the permission of the followingphotographic agencies and suppliers:Brand X Pictures, front cover, square 50; page 56. iD8 Photography, front cover, square 34.Image Source. JobCentre Plus/DWP, back cover, square 56. John Birdsall Social Images Photo Library,back cover, square 56. Photofusion Picture Library, front cover, square 52; back cover, square 36.Science Photo Library, back cover, square 41. Third Avenue, front cover, square 48
60 59 58 57 56
6361 62 64 65
767780 79 78
40
42
39 37
45444341
38 36