Embed Size (px)
Citation preview

Ser. SC;. Med. Vol. 35. No. 7. pp. 877.-890, 1992 Printed in Great Brirain. All rights reserved
0277-9536/92 $5.00 + 0.00 Copyright c 1992 Pergamon Press Ltd
RE-ASSESSING DISABILITY: THE IMPACT OF SCHISTOSOMAL INFECTION ON DAILY ACTIVITIES AMONG
WOMEN IN GEZIRA PROVINCE, SUDAN*
MELISSA PARKER?
Institute of Biological Anthropology, University of Oxford, 58 Banbury Road, Oxford OX2 6QS, U.K.
Abstract-Schistosoma mansoni is often perceived by governments and international aid agencies to present a major public health problem in the tropical and sub-tropical world. This perception persists in spite of the fact that biomedical practitioners and research workers disagree about the nature and extent of disease and disability caused by schistosomes. This paper raises the question of whether S. mans& should continue to be given priority as a public health problem in Gezira Province, Sudan. Biomedical and continuous observational data are blended with ethnographic information in order to develop a more integrated picture of the impact of S. mansoni on daily activity patterns among women.
Research took place in one village in the Gezira/Managil irrigation scheme. The study is characterized by a small sample and a paired design. That is, 11 infected women were paired with 11 uninfected women. These women were engaged in agricultural activities in the cotton picking season and they were matched for a wide range of social and economic factors that might otherwise have affected their working activities. Observations were conducted on a minute by minute basis in the cotton fields. These data, in combination with ethnographic information and data indicating female productive output, showed that infection with S. mansoni significantly altered activity patterns in the cotton fields. That is, infected women (with an arithmetic mean egg output of 1958 eggs/g) attempted to pick as much cotton as possible in the shortest time period feasible in the morning. This pattern was partially repeated by infected women who returned to the fields in the afternoon. However, a significant number of infected women felt too weak to sustain this work regime and the economic implications of this finding are discussed. Finally, Fisher’s exact probability test showed that infected women were significantly less likely to undertake persona1 care activities between cotton picking sessions and this result suggests they may have been too tired and/or had a diminished perception of their own well-being. The implications of these results for public health policy in Gezira Province are discussed.
Key words-S. mansoni, disability, women, Sudan
*Paper presented at the XIIth World Congress of Sociology in Madrid. 9-13 July 1990. Attendance at this Congress received financial support from the UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases.
tAddress for correspondence: Maternal and Child Epi- demiology Unit, London School of Hygiene and Tropical Medicine, Keppel Street, London WCIE 7HT, U.K.
fSchistosomiasis (or bilharziasis) is the broad descriptive term given to a group of chronic parasitic infections caused by schistosomes. The majority of human infec- tions are caused by four species of schistosome: S. hoematobium, S. intercalatum, S. japonicum and S. man- soni. These schistosomes have similar life-cycles involv- ing an aquatic snail intermediate host, the human definitive host and their mutual presence in a common environment where transmission occurs: typically irri- gated fields, irrigation and drainage channels, rivers, ponds and ditches.
INTRODUCTION
An estimated 200 million people worldwide are
infected with schistosomes and a further SOO-
600 million people are exposed to the risk of infection [l]. Each year substantial resources are allocated by governments and international aid agencies to impede the rate of transmission and hinder the development of schistosomal disease (more popularly known as bilharziasis)._j Yet there is considerable controversy concerning the extent of ill-health caused by schistosomes. Physiol- ogists, hospital-based clinicians and clinical epidemiologists disagree about the relationship between infective status, intensity of infection and the development of schistosomal disease [2, 31 as well as the relationship between infective
877

878 MELISSA PARKER
status, intensity of infection and the nature and extent of disability.*
In spite of this controversy investigators have rarely refrained from estimating the overall impact of schistosomal infection in communities where it is endemic. Lapage, for example, described schistosomi- asis as: “a lingering and often fatal disease which causes incalculable suffering and economic loss, and has crippled large human populations” [24]. Essophor refered to the fact that: “[bilharzia] results in the persistent sapping of the vitality of the greater part of the populace, apart from the small crop of late serious complications.. .” [25]. And a group of experts working for the World Health Organization recently wrote: “of all the parasitic infections that affect man, schistosomiasis is one of the most wide- spread. In terms of socioeconomic and public health importance in tropical and subtropical areas, it is second only to malaria” [26].
Such claims may be true. It is a contention of this paper, however, that existing knowledge is insuffi- cient to support these claims. Indeed, it is possible that some of these views reflect the authors’ own perception of schistosomal infection as something that is ‘exotic’, ‘dangerous’ and to be avoided ‘like the plague’. It is certainly interesting that el Tom [27] should report different perceptions of schistosomal infection among school children in central Sudan. Describing an epidemiological study on the preva- lence of S. haematobium (a species of schistosome which betrays its presence by the passing of blood in urine) he writes: “In Hager el Mak school in Kadugli town one of the very few non-infected boys was so ashamed of himself because his urine was unlike that of other boys that he cut his linger in order to add blood to his urine before submitting it for examin- ation.” It is, of course, unlikely that school children in Kadugli town are completely aware of the symp- toms of S. haematobium and the consequences of infection, and that one child’s behaviour there necess- arily reflects the thoughts and perceptions of other children in the region. Nevertheless, it is possible (if not probable) that biomedical practitioners and research workers have failed to appreciate the differ- ent ways in which their biomedical understanding of schistosomiasis is located within a complex nexus of social, cultural, economic and historic processes. Consequently, they have ignored data which suggests that the relationship between infection, disease and
*Disability may be thought about in many different ways. Physiologists generally assess disability (in relation to parasitic infection) according to indices of work capacity and physical fitness [447]. Hospital-based clinicians and clinical epidemiologists assess disability in terms of a patient’s reported symptoms such as abdominal pain, backpain and fatigue (g-121. Other attempts to assess disability include the investigation of schistosomal infec- tion on running performance [13, 141, educational achievement [14, 171 and productivity [17-221. See Parker [23] for a full critique of these approaches and the above-mentioned studies.
illness (however defined) is complex and poorly understood, and have allowed health care priorities to be formulated by epidemiological information alone.
The data presented in this paper attempts to address the issue of whether or not infection with S. mansoni is sufficiently debilitating to alter daily activity patterns among women engaged in agricul- tural work in the cotton picking season. Unlike research attempted by clinicians, physiologists and epidemiologists, this work is concerned with the daily experience of infection. In view of the chronic nature of infection, this aspect of an individual’s experience of infection is particularly important to comprehend. By focusing on the behavioural aspects of infection it is hoped that additional light will be shed on whether or not infection with S. mansoni is sufficiently debil- itating to be given priority as a major public problem in those communities in the developing world where it is endemic.
SELECTION OF VILLAGE
Fieldwork took place between April 1985 and May 1986 in Omdurman aj Jadida-a small, (officially-reg- istered) village in the Gezira/Managil irrigation scheme, Sudan [28]. The village was selected for a number of reasons; but primarily because it was expected to have a high prevalence and intensity of infection. That is, the village is located by a minor canal (which is generally considered to be the main source of transmission of schistosomiasis). Mollusci- tides had never been used in the canal to eliminate the snail vector; and the village had had no history of selective or mass chemotherapy. All water for dom- estic and agricultural use came directly from the canal as the village had no water pump or standpipes and pit latrines were not available to the village population.
FIELDWORK
The field-based research presented in this paper built upon knowledge and experience that I acquired in the course of two other studies undertaken in the Gezira/Managil irrigation scheme in 1981 and 1983. It involved living in the village with an extended family of 16 over a period of 14 months. I learnt to speak the local language and combined the collection of biomedical and continuous observational data with participant observation. Generally speaking, I stayed in the village for periods of 4-6 weeks and each period of fieldwork was followed by a break of 5-10 days.
In the course of this fieldwork I received a great deal of advice and help from a 16 year old female assistant as well as numerous men and women in positions of authority in the village. These included two local healers, the sheikh of the Mohamadeer and the she&h of the Hasaneeya.

Re-assessing disability 879
The Mohamadeer and the Hasaneeya are the two
most numerous and dominant ethnic groups in the village and they have a great deal in common. They are Muslims, speak Colloquial Sudanese Arabic and their domestic and work arrangements are characterized by a marked degree of segregration between the sexes.
positive for S. mansoni. Five (7.5%) women refused to participate.
The research topic and design was influenced by this segregation in the following two ways: first, the cotton picking season is the only time in the year when large numbers of women are engaged in agricul- tural work activities for a protracted period of time. It would not have been possible for a single investi- gator to have assessed the impact of S. mansoni on female activity patterns in the agricultural sector at any other time of year nor, therefore, to have inves- tigated the relationship between a woman’s infective status, her daily activity patterns and productive output.
Additional stool samples were, however, examined before pairing heavily infected women with women negative for S. mansoni. Egg output varies over time and the analysis of single stool samples can fail to detect light injections. I, therefore, collected a mini- mum of 5 different samples to ensure that negative results reflected an absence of infection with S. mansoni. In addition, a minimum of two samples were collected from selected women infected with S. mansoni in order to provide a more accurate assess- ment of their worm burden.*
The analysis of stool samples for S. mansoni pro- vided an opportunity to screen women for ascaris, hookworm, Taenia saginata and T. solium. Mid-day urine samples were also collected and a centrifugal technique [37] was used to screen women for S. haematobium.
Second, as a female research worker in an Arab, Muslim village, it was imperative that I worked with women. It would have been unaccept- able to have observed male work regimes and, simi- larly, it would have been unacceptable for a male fieldworker to have observed female work regimes. In view of the fact that women, rather than men, pick cotton and that the income generated from the production of cotton is so important to the national and local economy-I was particularly fortunate to be able to investigate the nature and extent of disability from S. mansoni among women at this time of year. The following two sections describe the biomedical and continuous observational data col- lected during this piece of fieldwork. Some of the ethnographic information which I used to interpret these quantitative data and thereby elucidate the relationship between infection, intensity of infection and daily behaviour is presented in the final section of this paper.
Pairing female cotton pickers
Infection with S. mansoni aside, women were matched as closely as possible for a wide range of variables that might otherwise have affected their daily activities. These included 5 parasitic infections (see above) as well as estimated age, ethnicity, socio- economic status, household composition (with par- ticular reference to available domestic labour) and access to the cotton fields. A woman’s access to the cotton fields varied according to whether she picked cotton on a hawasha (tenancy) that she rented, a hawasha that another family member rented or a hawasha where she was employed by someone with whom she had no strong familial link. It was, of course, impossible to control for some variables- principally, the motivation of a particular woman to pick cotton, her skill in picking and the extent to which activity patterns were affected by the presence of an observer.
SELECTION OF SAMPLE MINUTE BY MINUTE OBSERVATIONAL WORK
Parasitological screening of female cotton pickers
Women engaged in cotton picking activities were screened for S. mansoni immediately before the cotton season began. The cellophane faecal thick smear technique (Kato) was used to detect and quantify schistosome ova in stool samples [29] and the results breakdown as follows: 67 women worked in the cotton fields. Thirty (44.7%) women were negative for S. mansoni and 32 (47.8%) women were
In order to assess the nature and extent of agricul- tural activities undertaken by infected and uninfected women in the cotton fields, observations were under- taken on a continuous basis. Each infected woman was observed for one day and her pair-where poss- ible-on the following day. In the course of each day’s observation I collected the following infor- mation: first, the total time engaged in cotton picking and other agricultural activities during the morning and afternoon. _
*Research examining the distribution of eggs within a sample [30-331 and between samples for an individual over time 19, 11, 12,34-361 is not extensive. As a result it is not clear how many samples should be analysed to be sure that an individual is free from infection or whether their worm burden has been accurately recorded. The collection of 5 samnles from ‘uninfected’ women and 2 samples from infected women seemed sufficient from available evidence.
Second, observations were carried out on a minute by minute basis. Each period of observation lasted for 16 consecutive minutes and every period of observation was followed by a 14 minute interval. In the morning observations took place between 0730-0745, 0800-0815, 0830-0845, 0900-0915, 0930-0945 and 1000-1015 hr. In the afternoon, observational work was undertaken between

880 MELISA PARKER
1500-1515, 1530-1545, 1600-1615, 1630-1645 and 1700-l 715 hr respectively.
Every single activity undertaken by a woman during these periods of observation was recorded and these activities fall into the following five activity groups: posture, while picking cotton; types of rest in the cotton fields (e.g., sitting, lying down); work activities associated with cotton picking (e.g., putting cotton in sacks); other agricultural activities (e.g., collecting weeds for goats); all other activities not directly affecting a woman’s daily productive output.
Third, the total amount of cotton that each woman picked was weighed at the end of her morning and/or afternoon’s work in the fields. This was an easy task to undertake. Every woman ties a sack around her waist and she places every piece of cotton into her own sack. Friends and relatives working in the same field have their own sacks and they too put the cotton they pick into their own sacks.
ADDITIONAL INFORMATION RECORDED
Activities undertaken between cotton picking sessions
Minute by minute observations were not carried out between cotton picking sessions. However, at the end of each day’s observation, the participant was asked to recall the number and type of activities she had undertaken between morning and afternoon sessions.
Anthropometric and haematological measurements
The following anthropometric measurements were taken from all women participating in the observational work: height (cm), weight (kg), upper arm circumference (cm) and skinfold thicknesses at the sites biceps (mm), triceps (mm), sub- scapular (mm) and suprailiac (mm). These measurements were taken in accordance with the IBP methodology [38]. Blood samples were not analysed for malarial parasites but haemoglobin levels were assessed, using a compur Ml000 minipho- tometer.
All the anthropometric and haematological measurements were taken from women within five days of their day of observation. These data were not used to pair women infected with S. mansoni with women free from infection. But the subsequent analy- ses of these data helped to assess whether infected and uninfected women differed in their nutritional status.
Other signs of infection
A large number of diseases are endemic in the Gezira/Managil irrigation scheme. These include
*These figures have been calculated by taking the highest egg load recorded for each infected woman. The egg loads, therefore, refer to samples that were analysed either before, on, or immediately after each woman’s day of observation.
diarrhoeal diseases, infectious hepatitis, typhoid and meningitis. At the end of each day of observation I recorded whether a woman reported and/or exhibited signs of one or more of these infections.
RESULTS
Parasitological results
Twenty-two women (11 pairs) took part in this research. The 11 most heavily infected women (engaged in cotton picking activities) were paired with 11 women free from infection but also engaged in cotton picking activities. By international stan- dards the intensity of infection among these 11 infected women was high. That is, egg output ranged from 726 to 3768 eggs/g and the arithmetic mean egg load was 1958 eggs/g.*
The analysis of stool and urine samples for other parasitic infections revealed the following results: there were no recorded cases of hookworm, ascaris, T. solium and S. haematobium. Four women were positive for T. saginata and three of these women were negative for S. mansoni.
The sample
Infective status aside, each pair of women were closely matched for a wide range of social and economic variables. Some of this information is presented in Tables l(A) and (B).
Table I. (A) Female cotton workers listed by pair: table shows dates
of observation, time of year cotton picked (pick no.) and work
responsibilities (work)
Pair no. S.IlO. Date of observation Pick no. Work
01 02s February 03 01 02
01 01s March II 03 03
02 013 January 31 01 01
02 091 March I7 03 01
03 108 March 07 02 02
03 005 March 01 02 02
04 029 March 06 02 01
04 05s March 04 02 01
OS OS1 March 03 02 02
05 008 March OS 02 02
06 OS6 January 29 01 02
06 099 January 27 01 02
07 209 February 09 02 02
07 210 February I4 02 02
08 179 February I3 02 02
08 010 February I? 02 02
09 I61 February 07 01 02
09 II3 March I6 03 02
IO IS7 February IS 02 03
IO 021 February I I 02 03
II 065 March 23 03 02
II 109 March 24 03 02
Cotton is picked at three distinct intervals during the season (pick
no.): the amount of cotton available to pick at the beginning of
the season (pick 01) and the middle of the season (pick 02). does
not vary greatly. By comparison, there is less cotton to pick at
the end of the season (pick 03)
There are three types of women engaged in cotton picking activities
(work): those who rent a tenancy (01). those who work in the
fields on their relative’s tenancy (02) and those who work in the
fields for women or men with whom they have no direct familial
connectmn (03).

Re-assessing disability 881
Table I. (B) Female cotton workers listed by pairs: some biographical information
S. no
025 015
Estimated age
(years)
39 40
Ethnic status
01 01
Marital status
01 04
Total no. females Estimated age (years)/sex all > 14 yr in HH on kids born to women, and living observation day in HH on day of observation
02 07(2) 09(l) N(2) 14(l) 01 15(2) 20(l) 22(l)
013 41 01 04 02 091 38 01 02 02
108 25 01 01 01 005 24 01 01 01
029 35 01 03 01
055 35 01 02 01
09(2) 12(2) 17(l) lO(2) 12(l) 18(2) 23(2)
02(l) 06(2) 07(2) 09(I) 02(2) 05( 1) 06(I) 08(l)
Ol(2) 04(2) 06(l) 07(2) 08(2) 09(2) 12(l) 13(l)
15(2) 02(2) 04(2) 08(2) 1 l(2) 140) 18(l)
051 26 01 01 01 04(2) 06(l) 08(l) 008 30 01 01 01 06(l) 08(2) 12(l)
056 27 01 01 01 099 29 01 01 01
209 21 02 04 01 210 I8 01 01 01
179 33 02 01 01
010 34 01 01 01
161 24 02 01 00 113 29 01 01 00
I57 43 02 04 00
03(2) 06(2) 08(2) 09(l) 02( 1) 04(2) 06(2) 08(l)
09(2)
il(2) 12(l) 13(l) 15(l)
16(2) 06(l) 07(l) 09(l) 14(2)
03(I) 06(l) 08(2) 09(2)
lO(2) 12(i) 16(l) 20(l)
25(l) 13(2) 20(l)
065 26 01 01 00 07(l) 109 29 01 01 01 04(2) 08(2) 09(2) 13( 1)
Ethnic status: 01 = Hasaneeya 02 = Mohamadeer. Marital status: 01 = Married 02 = Married (Husband has 2 wives).
04 = Widowed 03 = Married (Husband has 3 wives). Sex of children: (I) = Male (2) = Female.
Continuous observational data
Each woman in each pair was observed for one day during the cotton picking season. Events which might have affected a woman’s work regime (such as attend- ing a funeral or wedding) did not take place for any of these women on their respective days of obser- vation. Moreover, with the exception of one woman, they did not take place either the day before or the day after the observational work.* The most import- ant results may be summarized as follows: first, all 22 women participating in this study went to the fields in the morning to pick cotton, and 18 women (81.82%) returned to the fields in the afternoon. Four women (18.18%) did not return to the fields, and these women were all infected with S. mansoni. In fact, the Fisher exact probability test (one-tail) showed that infected women were less likely to return to the fields than uninfected women, with the differ- ence significant at the 0.045 level. It is also striking that women who did not return to the fields in the afternoon gave fatigue as their reason.
*One woman who was infected with S. mansoni attended a bika (wake) the night before her day of observation. On the premis that her work activities might have been affected by a lack of sleep the preceding night I discarded the information collected from her first day of observation and undertook a second set of observations several days later.
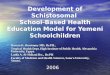
Second, infected women spent less total time in the fields in the morning and the afternoon and results from a paired t-test showed this difference to be highly significant in the morning (P = 0.008). This result is presented in Table 2. Third, statistical analy- ses of observational data collected on a minute by minute basis in the cotton fields revealed the follow- ing results: infected women spent less observed time picking cotton, compared to women free from infec- tion. They also spent less observed time engaged in other activities associated with cotton picking as well as work activities not associated with the production of cotton.
These findings refer to both morning and afternoon sessions, and contrast strongly with the fact that infected women spent a greater amount of observed time at rest. In the afternoon they also spent a greater amount of observed time engaged in activities not directly affecting productive out- put. In fact paired t-tests found some of these differences to be highly significant. That is, infected women spent significantly less observed time picking cotton in the morning (P = 0.009). In the afternoon, they spent significantly less observed time picking cotton (P = 0.034) and less observed time engaged in other agricultural work in the afternoon (P = 0.054). These results are presented in Table 3.
882 MELISSA PARKER
Table 2. Paired ~-test showing whether or not there is a difference in the amount of time (min) women spend in the cotton fields (uninfect&infected)
Standard error n n missing Mea” of “lean T P
Time difference, a.m. 7 4 + 28.3 07.3 + 3.96 0.008
Table 3. Paired I-tests showing whether or not there are differences by infective status in the time engaged in 6 main activities-as a proportion of total observed time (mi”) spent in the cotton fields
(uninfected-infected)
Main activities
a.m.
Picks cotton Other cotton work Other agricultural work Organisational work Rest Non productive work
p.“I.
Picks cotton Other cotton work Other agricultural work Organizational work
Rest Non productive work
n
II II II II II II
7 7 7 7
7 7
Mea”
+ 14.2 +01.4 +01.5
00.0 -02.7 fO0.I
+ 17.9 $ 02.7 f03.3
00.0
-04.9 -01.6
Standard error of mean
4.4 1.8 I.5 0.0 2.0 0.1
6.6 1.8 1.4 0.0
2.9 I.6
T P
+ 3.24 0.009 +0.77 0.461 +I.06 0.315
- -1.31 0.219 +l.Oil 0.341
+2.73 0.034 + I.51 0.181 + 2.39 0.054
- -
- I .67 0.146 -0.99 0.364
Posture
Posture provides a crude indication of the effort expended whilst picking cotton and, for the purposes of this study, five postures were identified: posture one entails standing upright and picking cotton. Posture two and posture three entail leaning forward to pick cotton at the approxi- mate angles of 80”-55” and M-30” respectively, and posture four entails bending over and picking cotton just a few centimetres from the ground. Posture five is hardly a posture at all-here, a woman sits on the ground and picks easily obtainable cotton at eye level.*
Paired t-tests were used to assess whether or not there were significant differences (by infective status) in the amount of time spent in these 5 postures. The results are presented in Table 4 and they show that uninfected women spent a signifi- cantly greater amount of observed time in posture 4 in the morning than infected women (P = 0.005). They also spent a greater amount of observed time in posture 1 and the difference is significant at the 0.029 level. In the afternoon, uninfected women spent more observed time in posture 4 and posture 1 but the difference is only significant for posture 1 (P = 0.029).
These results suggest that uninfected women spend a greater amount of observed time doing
~_.__ I__ _-. ~_~
*I had no personal experience of picking cotton prior to this study. I, thus, spent a few days in the fields learning how to pick cotton before attempting to record female pos- ture on a minute by minute basis. The conversations and advice I received from women during this time helped to identify and grade the above-mentioned postures ac- cording to their perceptions of the degree of difficulty and the amount of energy expended whilst picking cotton.
the more difficult work in the morning as they spend more time picking the cotton that demanded maximal effort. Posture 4 entails, after all, bending over and picking cotton just a few centimetres from the ground. It is the hardest and most strenuous task that a woman can undertake in the fields and it is no surprise to find that posture 1 is also more common among these women. Posture 1 entails picking cotton in an upright position. Indeed, it would be impossible to sustain posture 4 without posture 1. It is however, interesting that uninfected women did not spend significantly more time picking cotton in posture 4 in the afternoon than infected women. This result is discussed in the final part of this paper.
Paired t-tests were used to assess whether or not there were significant differences in the amount of cotton picked by infective status. The results are presented in Table 5 and they show that uninfected women did not pick significantly more cotton in the morning than their infected pairs. These results are replicated in the afternoon, if those women who did not return to the fields (and their pairs) are excluded from the analysis. That is, uninfected women did not pick significantly more cotton than their infected pairs.
There is, however, a strong case for incorporating in the analysis those women who did not return to the fields in the afternoon (and their pairs). After all, these women felt too tired to work and this is an important factor to consider when assessing the impact of S. mansoni on productive output. In fact, very different results are generated when these women are included. The results are also presented in Table 5. They show that uninfected women picked more cotton than infected women and the result is close to significance (P = 0.061).

Re-assessing disability
Table 4. Paired t-tests showing whether or not female posture varies by infective status--calculated as a proportion of the total observed time (min) spent picking
cotton (uninfected-infected)
Posture Standard error (observed minutes) n Mean of mean T P
a.m. Posture I II +7.8 3.1 +2.6 0.029 Posture 2 II +1.4 4.7 +0.3 0.779 Posture 3 11 0.0 3.2 0.0 I.000 Posture 4 11 +5.0 1.4 +3.6 0.005 Posture 5 I1 0.0 0.0 - -
p.m. Posture I 7 + 10.7 3.8 +2.90 0.029 Posture 2 7 f03.1 4.5 +0.71 0.506 Posture 3 7 -01.6 2.1 -0.76 0.474 Posture 4 7 +03.1 2.8 +1.12 0.306 Posture 5 7 +00.1 0.1 + 1.00 0.356
Table 5. Paired f-tests showing whether or not there are differences by infective status in the total amount of cotton picked in the cotton fields (uninfected-uninfected)
Standard error Cotton picked n n miss Mean of mean T P
Total picked, a.m. 11 00 +0.4 0.7 +0.51 0.620 Total picked, p.m. 07 04 +0.2 0.7 f0.26 0.803 Total picked, p.m. II 00 +I.6 0.8 f2.12 0.061
883
Seasonality and productivity
Statistical tests were also employed to determine whether or not other factors significantly affected productive output. These included the effects of sea- sonality, renting a tenancy, age, haemoglobin levels, other intestinal parasites, ethnicity, marital status, household composition and available domestic labour.* Analyses of covariance were favoured, with the total amount of cotton picked in the morning and afternoon the dependent variables. With the excep- tion of seasonality, there were no significant results.
Seasonality appeared, however, to affect the total amount of cotton picked in the morning and the afternoon. That is, productive output fell with time, and the results are presented in Table 6. Accounting for seasonality, however, this table clearly shows that infected women continued to pick as much cotton as their uninfected pairs in the morning and the after- noon, so long as women who did not return to the fields were excluded from the afternoon analysis (n = 18). If they were included with a value of zero, however, infected women picked significantly less cotton (P = 0.034), in spite of a marked seasonal effect (P = 0.064).
In view of these findings, analyses of covariance were further employed to control for time; and to assess whether or not the differences detected between infected and uninfected women by paired t-test analyses could be maintained for the total time in the fields; the proportion of observed time spent picking cotton; the proportion of observed time engaged in postures one and four; and the proportion of
*Temperature and relative humidity may also affect pro- ductive output. Unfortunately these measurements were not recorded and their possible impact on work regimes cannot be assessed.
observed time engaged in other agricultural work. These results are not presented in a table but they suggested, overall, that seasonality did not affect female activity patterns in the morning or the after- noon. In other words it was deemed appropriate to stand by the initial paired t-test findings previously mentioned.
Activities undertaken between cotton picking sessions
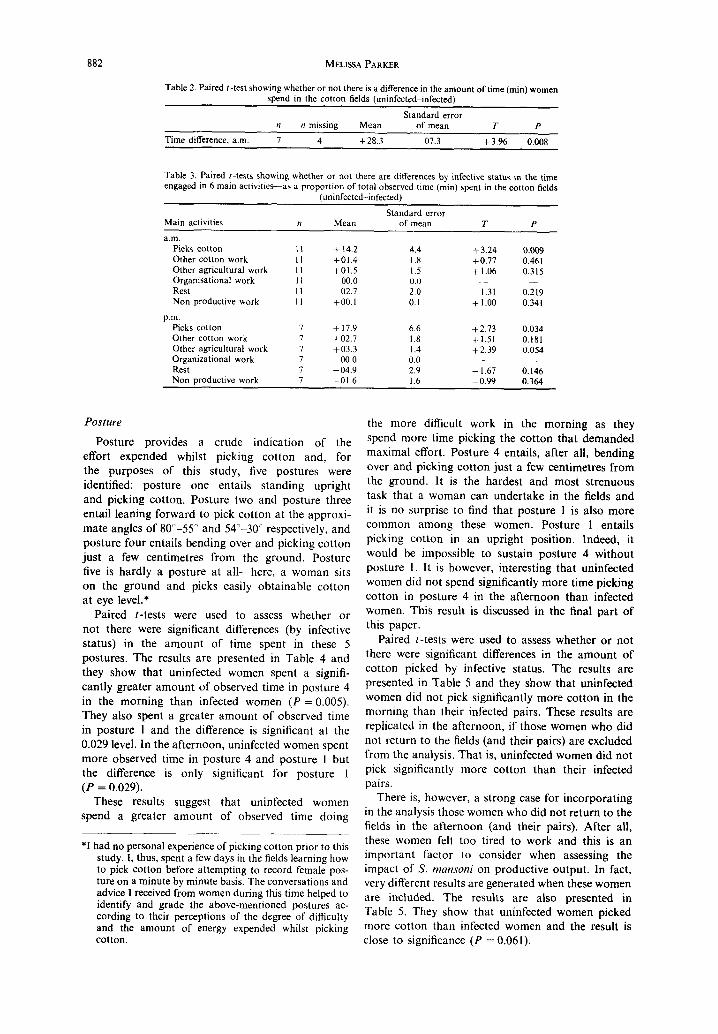
The activities undertaken between cotton picking sessions are recorded in Tables 7 and 8. By analysing the occurrence and total number of activities undertaken by women the following two conclusions can be drawn: first, infected women participated in recuperative and domestic work activities as fre- quently as women who were negative for S. mansoni.
Indeed, Fisher’s exact probability test (one-tail) did not find the occurrence of these activities to differ significantly by infective status. Second, infected women were less likely to participate in those activi- ties which did not directly affect or contribute to their domestic and agricultural productive output. In fact, Fisher’s exact probability test (one-tail) showed in- fected women to be significantly less likely to partici- pate in those activities defined as personal care (P = 0.010).
Anthropometric and haematological data
To assess whether or not selected anthropometric measurements varied by infective status, paired t- tests were carried out. With the exception of the biceps skinfold and upper arm circumference, there were no significant differences (see Table 9). In addition, haemoglobin levels did not vary signifi- cantly by infective status and the paired t-test result is also presented in Table 9. This result, in combi- nation with the anthropometric results, suggests that

884 MELISSA PARKER
Table 6. Analyses of covariance of total cotton picked in the morning and afternoon on time (from the beginning of the study) and infective status
Variable b I P n I1
Total cotton picked (kg), am:
Intercept 8.33 12.11 <O.OOl 22 0.38 Date (days) -0.02 ~3.32 0.004 Infected -0.95 - 1.58 0.131
Total cotton picked (kg), p.m.
Intercept 6.56 9.32 t0.00l IX 0.30 Date (days) -0.02 -2.49 0.025 Infected -0.32 -0.49 0.630
Total cotton picked (kg), p.m. Intercept 6.80 6.21 t0.00l 22 0.27 Date (days) -0.02 ~ I .97 0.064 Infected -2.19 - 2.29 0.034
women did not differ a great deal in their nutritional status.
Blood samples were not analysed for malarial parasites. The fact that a paired t-test did not reveal any significant differences in haemoglobin levels suggests, however, that infected women did not experience the debilitating consequences of malaria with any greater or lesser frequency than women free from infection with S. mansoni.
Other signs of infection
Women did not report or exhibit symptoms associ- ated with diarrhoeal diseases, infectious hepatitis, typhoid or meningitis. In combination with the para- sitological and haematological data previously men- tioned it seems reasonable to suppose that other important infections endemic in the Gezira/Managil scheme did not mask or crowd out the effects of S. mansoni during this study.
DISCUSSION
Apprasial of methodology
The data presented in this paper concern a small number of women, a paired design and a limited number of observations. I had initially intended to work with 12 pairs of women (rather than 1 l), and to observe each woman in each pair for two days
(rather than one day), but I had never intended to work with a large sample. It is, of course, true that small samples and a paired design sometimes prohibit the conclusive establishment of relationships and associations between variables. They also place a great deal of pressure on a single investigator as it only takes one woman to withdraw to lose two; and were several women to withdraw, a whole study would collapse. For the purposes of this research, however, the advantages of working with a small sample and a paired design outweighed these difficulties.
Some of these advantages include the following: first, it was possible to select finely matched pairs of women. With constraints of time (imposed by fund- ing), it would not have been possible, as a single investigator, to have acquired an adequate knowledge and understanding of the various social and econ- omic factors that affect a woman’s work regime from a large group of women. A pilot study undertaken in the region in 1983 had already shown that this type of information could not be elicited from question- naires without first establishing a close rapport with participants and their families, and/or participants acquiring a full understanding of the work in hand [39].
Second, small samples can free a single investigator to spend a considerable amount of time with each
Table 7. The number of women who undertook the following 9 actwities between cotton “ickine sessions bv infective status
Infected (n = II)
Uninfected (n = II)
Main activities Present Absent Present
Work activities: Cookmg IO 01 07 Childcare 01 IO 01 Other household activities 07 04 09
Recuperative activities: Eating II 00 00 Rest 09 02 07
Activities not directly contributing to daily productive output: Personal care 01 IO 07 Religious activites 00 II 08 Social visits 03 ox 06
Other: Records name on
Absent
04 IO 02
II 04
04 03 05
electoral register 01 10 00 II
Re-assessing disability 885
Table 8. Total number of activities undertaken by infected and uninfected women between cotton picking sessions
Main activities Infected Uninfected
Work activities: Cooking 22 13 Child care 01 01 Other household activities II 15
Recuperative activities: Eating 27 25 Rest 12 09
Activities not directly contributing to daily productive output: Personal care 01 07 Religious activities 00 03 Social visits 03 06
Other: Records name on
electoral register 01 00
participant. In so doing, it is possible to acquire an understanding of each person’s thoughts about the work and allay any fears they may have about contributing to the research. In this particular study it was crucial that all the participants felt comfortable with the idea of an English female investigator recording the minutae of their daily activities. Fear, anxiety and a desire by women to be seen to be doing the ‘right’ thing at the ‘right’ time could have affected their activities and rendered these observational data worse than useless. Instead, frequent contact and discussion with this small group of women enabled many problems associated with these continuous observational data to be overcome [40].
Third, single investigators working with a small sample can collect a wide range of information associated with the topic or question presented for investigation. In this study, for instance, it was possible to collect very detailed observational, haematological, anthropometric and parasitological data. More importantly, it was possible to use ethno- graphic information acquired over a period of 14 months fieldwork to interpret these quantitative data. In other words, the combination and integration of different types of information has enabled a more holistic picture of the impact of S. mansoni on female behaviour and daily life to be developed.
Interpretation of results
The information generated by the above-men- tioned design and described in the preceding sections,
raise several important questions. These focus on the following key findings: in the morning, infected women spent significantly less time in the fields and significantly less observed time picking cotton. Although they did not pick significantly less cotton, their infective status altered their activity patterns considerably. That is, they picked as much cotton as possible in the shortest time period feasible. In the afternoon, this pattern was partially repeated by those women who returned to the fields. That is, infected women continued to spend significantly less observed time picking cotton and they did not pick significantly less cotton than their uninfected pairs. They did, however, forsake participating in other important agricultural activities to achieve this. It is interesting, too, that 18.18% of women participating in this study did not return to the fields in the afternoon, and these women were all infected with S. mansoni. Without exception, they said they were too tired to pick cotton; and the activities undertaken in the village during these working hours confirm this finding.
Although infection by S. mansoni undoubtedly exerts an effect in the afternoon, the results from continuous observational and time-use data raise several important questions: why do infected women, having made the decision to work in the fields, work apparently more efficiently than their uninfected pairs? Is it possible to gauge the economic conse- quences of infection by analysing these observational and productive data?
With regard to the first question, several hypoth- eses were considered. First, is it possible that unin- fected women spent more time in the fields and more observed time picking cotton with the same pro- ductive output as their infected pairs, simply because they undertook the hardest work? Are they behaving in an altruistic way towards their infected female compatriots by attempting the most difficult work and picking the most inaccessible cotton?
This is an unlikely scenario. Uninfected women, it is true, spent significantly more observed time in posture 4 and posture I in the morning. In the afternoon, they also spent more observed time in posture 4 and posture 1, but posture 4 dropped from significance in the paired t-test analysis and posture 1 dropped from significance once seasonality has been accounted for in the analysis of covariance. It is,
Table 9. Paired f-tests showing whether or not there are differences by infective status for 7 anthropometric measurements and haemoglobin (uninfected-infected)
Standard error Variable n n missine Mean of mean T P
Height IO I -1.1 2.7 -0.42 0.684 Weight IO I t4.0 3.4 +I.18 0.268 Biceps (log IO) 10 I f0.1 0.1 + 2.43 0.038 Triceps (log IO) IO I -0.0 0.0 +0.61 0.559 Subscap (log IO) IO I t2.0 1.2 + 1.64 0. I36 Supiliac (log IO) IO I to.1 0.1 + 1.26 0.240 Uarmcirc 09 2 -2.9 1.2 +2.38 0.045 Haemoglobin 08 3 t8.1 8.8 +0.92 0.387

886 MELISSA PARKER
therefore, unlikely that uninfected women behaved in an altruistic way in the morning and then changed their feelings and behaviour in the afternoon! There are, after all, more tangible and direct ways to compensate those debilitated by infection (such as the provision of resources and income). Furthermore, infected and uninfected women did not know their infective status on their respective days of obser- vation.
A second explanation for why infected women may have spent less time in the fields and less observed time picking cotton, with the same productive output, concerns the seasonal availability of cotton. In spite of making every effort to observe infected women and their uninfected pairs on consecutive days, this did not, in fact, happen for every pair. Infected women tended to be observed at the beginning of the season (when cotton was more plentiful); and uninfected women towards the end of the season (when there was less cotton to pick).
Analyses of covariance were thus employed to control for seasonality and to explore the possibility that uninfected women picked less cotton because there was less cotton to pick. But the findings reached by these techniques, in common with those arising from paired t-test analyses, showed that uninfected women continued to pick as much cotton as women infected by S. mansoni.
Neither of these explanations shed explanatory light on the findings generated by paired t-test analy- ses. They also sidestep the difficult question of whether or not women infected with S. mansoni knew or felt themselves to be ill, and the extent to which this may have been acknowledged and accounted for, by friends and relatives working in the fields and/or undertaking domestic work activities.
Although there were substantial difficulties in obtaining information relevant to this question, sev- eral important points can be made at this juncture. First, none of the women participating in this study knew their infective status on their day of obser- vation. They had not sought clinical advice from Managil or other towns in the vicinity, and very few enquired about the results of stools submitted for examination in the village. Second, this finding does not suggest that women infected with S. mansoni in this study felt fit and healthy. There are a number of therapeutic pathways that a woman can take, either individually or simultaneously, to alleviate symptoms and signs of illness. There is insufficient space in this paper to discuss the extent to which a woman’s age, social status, access to economic resources and her perceptions of the etiology, nosology and symptoma- tology of the illncs:; affects her behaviour. It is, however, worth mentioning that consultation with a biomedical pratitioner is rarely the first or even the preferred type of consultation, whatever the illness.
Women are rather cautious about seeking biomed- ical advice for a variety of reasons. These include the following: biomedical diagnosis in Managil hospital
and other hospitals in Gezira Province is free but the service is erratic, unpleasant and time-consuming. The private clinics in the towns provide a quicker and more reliable service but consultations are expensive. Moreover, the drugs prescribed by biomedical prac- titioners in the hospitals and the clinics have to be brought from local pharmacies. These drugs are frequently unavailable and/or too expensive for many women. The unsatisfactory nature of biomedical care helps to explain why some women did not seek clinical advice and why so few women expressed an interest in discovering whether the stools they had submitted for examination in the village were positive or negative.
There are other reasons too. Schistosomiasis (or bilharziasis) was known as harzie by many people in Omdurman aj Jadida. A number of men and school children had clearly learnt about the link between contaminated water, infection with schistosomes and the consequences of infection for an individual’s health. However, none of the women in this study had been to primary school and while they may have overheard or participated in conversations about hank they did not equate infection with a feeling of malaise, tiredness and a general sense of ill-health.
This is not surprising. Unlike malaria and infec- tious hepatitis, schistosomal infection does not have an easily identifiable and visible set of symptoms. It is a chronic infection which does not necessarily exert a constant effect over time. It is, thus, unlikely that women infected with S. mansoni consciously modified their behaviour in the knowledge that they were infected with this intestinal parasite (inspite of the fact that more than 80% of infected women said they felt tired and weak on their day of observation). It is also improbable that household members compen- sated for the disability these women experienced in the knowledge that they were infected by S. mansoni.
The hypotheses and background information described so far provide a useful backdrop for the final and most compelling explanation for the behavioural differences detected between women. It is this: infected women, over short periods of time, are more efficient at picking cotton. Although they did not know their infective status on their day of observation, and although they did not, therefore, have any biomedical understanding of the debility they experienced, they did know that they had limited staying power. Consequently, they attempted to pick-in as short a time period as possible-a suffi- cient quantity of cotton to generate the income required to purchase essential goods.
Supporting evidence for this view includes the fact that infected women spent less observed time engaged in other agricultural work activities-notably the collection of weeds for goats, with this variable significantly different in the afternoon. This finding is interesting. Collecting weeds for goats is an import- ant activity as weeds are a staple food and affect the volume of milk produced by goats. Milk, in turn,

Re-assessing disability 887
affects the nutritional well-being of household mem- bers. And it is significant, if not surprising, that infected women did not feel able to participate in these activities as frequently or extensively as their uninfected pairs.
The provision of adequate food supplies is a male responsibility. Even though male heads of house do not, or cannot, always fulfil these responsibilities, the onus of responsibility lies with them to provide sufficient food for household members. It is under- standable, therefore, that women with limited energy and debilitated by infection should utilise their time in the fields by picking as much cotton as possible in the shortest time feasible. In so doing, they attempt to earn sufficient income to meet other pressing needs. These include the purchase of essential household items and clothes for their children. Furthermore, several women put money aside for the purchase of food, if they knew or felt that their husband, brother or father might not fulfil their responsibilities in the coming year.
The discussion, so far, has paid little attention to the social context of work and the pressures placed upon women to fulfil certain duties in the agricultural sector. Briefly, women are either tenant farmers with responsibilities to harvest and sell a reasonable quan- tity of cotton to the government (through the Sudan Gezira Board) or they are employed by male or female tenant farmers to pick cotton on a daily basis, and paid according to their productive output. Either way, the income generated by the production of cotton has a critical input into the household economy.
At the risk of simplification, responsibilities are generally shared between all household members according to age, gender, household size and com- position, access to economic resources etc. Each member has a clear idea of the duties they are expected to perform. In fact, the collective nature of households in Omdurman aj Jadida ensures that members who do not regularly fulfil these expec- tations are reprimanded by other family members. In other words, all women participating in this study faced considerable pressures to go to the fields; and a feeling of malaise and tiredness would not have been deemed a legitimate reason to stay in the village day after day. These pressures add further explana- tory power to the view that infected women found it necessary to pick in as short a time period as possible a sufficient quantity of cotton to generate income to purchase essential items.
That said, a number of infected women felt too weak to sustain this work regime. But the economic implications of this finding are difficult to gauge. It is possible that infected women and their families experienced a decline in their economic well-being, if household members did not or could not compensate for any loss of income. Alternatively, household members may have stood in for absent women or generated income from other sources. In so doing,
they may have forestalled a drop in their economic well-being. Without additional information concern- ing an infected woman’s overall loss in productive output over time, and the extent of intra and inter household compensation, it is difficult to determine the impact of an infected woman’s loss in earning power.
Data indicating productive output and potential economic loss should not, however, be emphasized at the expense of ethnographic information concerning perceptions of health and well-being. In the “lust for absolute proof’ [41] and the increasing use of cost- benefit analysis by health planners to accord priority to the control of one disease rather than another, it is easy to lose sight of those aspects of infection that cannot be given a numeric or economic value. In this respect, the finding that infected women were signifi- cantly less likely to undertake personal care activities [such as using haluwa (an ointment which removes body hairs) to clean their bodies; combing and plat- ting hair etc.] is interesting and suggests that women were too tired and/or had a diminished perception of their own well-being.
Ismail [42] has drawn attention to the time and importance given to ‘beauty care’ and other personal care activities among urban women in northern Sudan. In Omdurman aj Jadida, and many other parts of rural Gezira, women attribute similar im- portance to these activities but the exacting nature of their work often prevents them from spending as much time on these activities as they would wish. The differences detected between infected and unin- fected women may, therefore, be important but there was insufficient time to address the following ques- tions: do women infected with S. mansoni feel miser- able? Do they have less self-esteem? Are they perceived as less attractive by other villagers? What- ever the answers to questions such as these, it is necessary for further investigators to study the social consequences of the behavioural differences detected between women, if we are to understand at least some of the effects of S. mansoni on non-economic activities.
In sum, minute by minute observational data are by far the most accurate way to record the impact of infection with S. mansoni on daily activity patterns. In fact, these observational data-in combination with anthropometric, haematological, parasitological and ethnographic information-have shown, for the first time, that infection with S. mansoni (at recorded egg loads) is debilitating and interferes with daily activities.
Policy implications
The implications of these results for public health policy are not straightforward: first, the results pre- sented in this paper are not applicable to populations outside the Gezira/Managil irrigation scheme. The impact of schistosomal infection on daily activities is complex. This paper has shown that it is possible to
888 MELISSA PARKER
understand some of this complexity by locating biomedical information in its specific ecological, social, cultural and economic context. It is thus likely that the nature and extent of disability varies a great deal between populations. Second, it would be premature to draw firm conclusions about the impact of S. mansoni on daily activities in the Gezira/Managil irrrigation scheme from a single and exploratory piece of research. It would certainly be interesting and helpful to know if similar results could be generated in this region by employing the same design but working with a larger sample of women.
Nevertheless, the data presented in this paper suggest that it is far from clear whether S. mansoni
should continue to be accorded priority as a public health problem in Gezira Province. Too many important questions remain unanswered: does S. mansoni exert a constant effect on female activities over time? What are the social, economic and biological ramifications of the recorded differ- ences detected between infected and uninfected women working in the fields? Does S. mansoni
alter activity patterns among men, children and those women solely engaged in domestic work activi- ties? Of course, a number of biomedical, social and economic questions also remain unanswered [43] but this should not deflect attention from the above questions.
This inter-disciplinary study also highlights some of the problems associated with the inter- pretation of epidemiological information. The data clearly show that social, cultural and ecological factors affect the nature and extent of disability, and that the relationship between infection, intensity of infection and daily activities is, therefore, complex. The findings generated by another study that I under- took in the same village (over a period of 5 months) in 1985 draws further attention to the complex re- lationship between infection, intensity of infection and disability [44]. This study examined the effects of S. mansoni on daily activities among women nursing newborn infants and engaged in domestic work. These women were not involved in any agricultural work; and the methods and approaches employed in this study were similar to those employed in the preceding study. That is, 24 women (12 pairs) took part in inter-disciplinary research involving the col- lection of biomedical and continuous observational data. Each woman in each pair was observed for two consecutive days and continuous observations were undertaken over a period of 6 hours. Statistical analyses showed that infected women (with an arith- metic mean egg load of 860 eggs/g) did not spend significantly different amounts of time engaged in domestic work, infant and child care, social activities,
_
*See Parker [23] for a detailed breakdown of the time engaged in agricultural and domestic activities by in- fected and uninfected women.
rest or non-essential activities. In other words, S. mansoni did not appear to impair daily activities at all.
Together, these studies suggest that S. mansoni
exerts a differential impact on daily activities according to the nature and extent of work undertaken by women. This variability cannot be explained by the fact that infected women engaged in agricultural work had heavier egg loads than infected women engaged in domestic work. By inter- national standards all the women infected with S. mansoni had ‘heavy’ infestations of schistosomes. There is no parasitological research to support the idea that differences detected between these two groups of infected women could explain why S. mansoni altered activities in one sphere rather than another.
It is much more likely that variations in work load and heat load, rather than egg load, accounted for the differential impact of S. mansoni on female activities. Women engaged in agricultural activities worked for longer and more continuous periods of time than women engaged in domestic work. A great deal of energy and effort is required to undertake and com- plete domestic activities but these activities generally happen over relatively short periods of time. Washing clothes, for example, is unlikely to take more than an hour; and cooking ‘asidah (a kind of solid porridge made from fermented flour) or kisra (a wafer-like bread made from millet), though neither pleasant nor simple, rarely takes more than 10 and 25 min respect- ively. In addition, several important work activities afford an opportunity for recuperation during the day (for example, a women may lie down and breastfeed her infant).*
Women engaged in agricultural work, in addition to working for longer and more continuous periods of time, may spend as much as 30-40 min walking from the village to the fields before they even start their work. In the course of the day they are, there- fore, exposed to direct sunlight and the heat load placed upon them is much greater than that experi- enced by women engaged in domestic work. The activities of this latter group take place in the home and/or enclosed cooking areas and they are protected from such intense solar radiation.
In sum, the impact of S. mansoni on daily activities is complex and variable. It is inappropriate to rely on epidemiological information to determine whether or not S. mansoni presents a major public health problem. The limits of epidemiology, however, raise the following questions: how much weight should be given to the clinical, physiological, be- havioural, social and economic aspects of infection? What criteria, if any, can usefully be applied to the evaluation of these different aspects of infection? Research workers will find it helpful to continue to work on S. mansoni in an interdisciplinary way and, without doubt, they should do this with zest!
Re-assessing disability 889
Acknowledgemenrs-The data in this paper were collected, analysed and presented in partial fulfilment of the require- ments of a D.Phil thesis at the Institute of Biological Anthropology, University of Oxford, England. I am extremely grateful to Geoffrey Ainsworth Harrison for his help and advice throughout this project. I am also grateful to Tim Allen, the organisers of the Blue Nile Health Project (Ahmed Babiker, Alan Fenwick, Asim Daffalla, Ahmed el Gadal), Gerry Brush. David Evans, Nick Mascie-Taylor and Robert Sturrock for their help with this research. Above all, I would like to thank the people of Omdurman aj Jadida. The study was funded by a Medical Research Council Studentship (U.K.), the Rockefeller Foundation (U.S.A.) and the Royal Anthropological Institute (U.K.).
1.
2.
3.
4.
5.
6.
I.
8.
9.
10.
11.
12.
13.
14.
REFERENCES
Mott K. Schistosomiasis control. In The Biology of Schisfosmomes: from Genes to Latrines (Edited by Rollinson D. and Simnson A. J. F.). Academic Press, London, 1987. . Tanner M. Evaluation of public health impact of schistosomiasis. Trop. Med. Parasit. 40, 143-148, 1989. Jordan P. Schistokomiasis-the St Lucia Project. Cambridge Universitv Press, Cambridge. 1985. Collins K. C., Brotherhood J. R., Davies C. T. M., Dore C., Hackett A. J., Imms F. J., Musgrove J., Weiner J. S., Amin M. A., el Karim M., Ismail H. M., Omer A. H. S. and Sukkar M. Y. Physiological per- formance and work capacity of Sudanese cane cutters with Schistosoma mansoni infection. Am. J. Trap. Med. Hyg. 25, 410-421. 1976. Omer A. H. S. and El Din Ahmed N. Assessment of physical performance and lung function in Schistosoma mansoni infection. East Afi. Med J. 51, 217-222, 1974. Awad el Karim M. A. Collins K. J., Brotherhood J. R., Dore C., Weiner J. S., Sukkar M. Y., Omer A. H. S. and Amin M. A. Quantitative egg excretion and work capacity in a Gezira population infected with Schistosoma mansoni. Am. J. Trop. Med. Hyg. 29, 54-61, 1980. van Ee J. H. and Polderman A. M. Physiological performance and work capacity of tin mine labourers infested with schistosomiasis in Zaire. Trap. Geogr. Med. 36. 259-266, 1984. Omer A. H. S., Hamilton P. J. S., de C. Marshall T. F. and Draper C. C. Infection with Schistosoma mansoni in the Gezira area of the Sudan. J. Trap. Med. Hyg. 79, 151-157, 1976. Cook J. A., Baker S. T., Warren K. S. and Jordan P. A controlled study of morbidity of schistosomiasis in St Lucian children, based on quantitative egg excretion. Am. J. Trap. Med. Hyg. 23, 625-633. 1974. Cline B. L., Rymzo W. T., Hiatt R. A., Knight W. B. and Berrios-Duran L. A. Morbidity from Schistosoma mansoni in a Puerto Rican community: A population- based study. Am. J. Trap. Med. Hyg. 26, 109-117, 1977. Arap Siongok T. K., Mahmoud A. A. F., Ouma J., Warren K. S., Muller A. S., Handa A. K. and Hauser H. B. Morbidity in Schistosoma mansoni in relation to intensity of infection: study of a community in Machakos, Kenya. Am. J. Trap. Med. Hyg. 25, 273-284, 1976. Smith D. H., Warren K. S. and Mahmoud A. A. F. Morbidity in Schistosoma mansoni in relation to inten- sity of infection: study of a community in Kisumu, Kenva. Am. J. Troo. Med. Hvp. 28. 220-229. 1979. Okpala I. Studies on Schistoiima haematobizk infec- tion in school children in Epe, Western Nigeria. W. Afr. Med. J. 10, 4022412, 1961. Walker A. R. P., Walker B. F., Richardson D. and Smit P. J. Running performance in South Aftrican Bantu
15.
16.
17.
18.
19.
20.
21.
22.
23.
24. 25.
26.
27.
28.
29
children with shistosomiasis. Trap. Geogr. Med. 24, 347-352, 1971. Abdalla A., Badran A. and Gala1 S. The effect of bilharziasis on the mental power and scholastic achieve- ment of school children. J. Egypt. Pub1 Hith Ass. 39, 135-146, 1964. Walker A. R. P., Walker B. F. and Richardson B. D. Studies on schistosomiasis in a South African Bantu schoolchild population. Am. J. Trap. Med. Hyg. 19, 7922814, 1970. Weisbrod B. A., Andreano R. L., Baldwin R. E., Epstein E. H. and Kelley A. C. Diseases and economic development. Int. J. Sot. Econom. 1, 111-117, 1974. Foster R. Schistosomiasis on an irrigated estate in East Africa. III. Effects of asymptomatic infection on health and industrial efficiency. J. Trap. Med. Hyg. 70, 185-195, 1967. Fenwick A. and Figenschou B. H. The effect of Schisto- soma mansoni on the productivity of cane cutters on a sugar estate in Tanzania. Bull. Wld Hlth Org. 47, 567-572, 1972. Weisbrod B. A., Andreano R. L., Baldwin R. E., Epstein E. H. and Kelley A. C. Disease and Economic Development. The Impact of Parasitic Diseases in St Lucia. University of Wisconsin Press, Madison. 1973. Baldwin R. E. and Weisbrod B. A. Disease and.labour productivity. EC. Dev. Cult. Change 22, 414-435, 1974. Barbosa F. S. and Pereira Da Costa D. P. Incapacitat- ing effects of Schistosoma mansoni on the productivity of sugar-cane cutters in northeastern Brazil. Am. J. Epidemiol. 114, 102-l 11, 1981. Parker M. A. The effects of Schistosoma mansoni on female activity patterns and infant growth in Gezira Province, Sudan. D.Phil thesis, University of Oxford, 1989. Lapage G. Schistosomiasis. Nature 209, 29-30, 1966. Essophor C. U. Lets kill bilharzia with sociology. Cent. Afr. J. Med. 6, 216, 1960. World Health Organization. The control of schistoso- miasis. Report of a WHO expert committee. Techn. Rep. Series. No. 728, 1985. el Tom A. R. An epidemiological study on the preva- lence of urinary bilharziasis among the school child population in Northern and Southern Kordofan Provinces. MD thesis (Public health), University of Khartoum, 1976. The irrigation scheme was established in 1925 under Anglo-Egyptian colonial rule. The production of cotton was encouraged for a variety of reasons. These included an attempt to provide the declining Lancashire cotton industry with a cheap and reliable source of cotton. The scheme has expanded and changed since 1925 but it still produces a great deal of cotton. In 1984, for example, the Gezira/Managil irrigation scheme produced 75% of the country’s cotton and this generated some 45% of Sudan’s foreign exchange. Prior to the establishment of the irrigation scheme, the population was estimated to be 135,000, In 1983, however, there was an enumerated population of 2,025,125 million living in 1515 villages and 500 small ‘unregistered’ villages. The construction of a large network of irrigation canals and a substantial increase in population has facilitated the spread of water-borne diseases such as malaria and schistosomia- sis. In fact, the Blue Nile Health Project was initiated in 1979 by the Ministry of Health, Sudan; the World Health Organization and a number of international aid agencies to develop and implement a strategy for the control of water-borne diseases. The project was expected to run for 10 years at an estimated cost of $154 million. However, it is now expected to run until 1993 for a variety of economic and political reasons. World Health Organization. Cellophane faecal thick smear technique (Kato) for diagnosis of intestinal

890 MELISSA PARKER
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
schistosomiasis and gastrointestinal helminth infections. PDP/83.3, Geneva, 1983. Martin L. K. and Beaver P. C. Evaluation of Kato thick-smear technique for quantitative diagnosis of helminth infections. Am. J. Trap. Med. Hyg. 17, 382-391, 1968. Chaia G., Chaia A. B. Q., McAullife J., Katz N. and Gasper D. Coprological diagnosis of schistosomiasis. II. Comparative study of quantitative methods. Rev. Inst. Med. Trap. Sao Paulo, 10, 349-353, 1968. Woodstock L., Cook J. A. Peters P. A. and Warren K. S. Random distribution of Schistosome eggs in the feces of patients with Schistosomiasis mansoni. J. Infect. Dis. 124, 613-614, 1971. Blair D. M., Weber M. C. and Clarke V. de V. Macroscopic and microscopic methods in the diagnosis of intestinal bilharziasis. Cent. Afr. J. Med. 15, Suppl. 2-8, 1969. Warren K. S., Mahmoud A. A. F., Cummings P., Murphy D. J. and Houser H. B. Schistosoma mansoni in Yemeni in California: duration of infection, presence of disease and therapeutic management. Am. J. Trap. Med. Hyg. 23, 902-909. 1974. Barreto M. L., Silva J. T. F., Mott K. E. and Lehman J. S. Stability of faecal egg excretion in Schistosoma mansoni infection. Trans. R. Sot. Trap. Med. Hyg. 72, _- 181-187, 1978. Loureiro S. and Galvao A. Analysis of components of variation in Schistosoma mansoni egg counting. Rev. Inst. Med. Trop. Sao Paulo. 25, 22-24, 1983. Parker M. The effects of Schistosoma mansoni on female activity patterns and infant growth in Gezira Province, Sudan. D.Phil. Thesis, UniversityofOxford, p. 113 1989. Weiner J. S. and Lourie J. A. Human Biology: A Guide to Field Methods. Blackwell Scientific, Oxford, 1969. Unpublished results from research conducted by M. A. Parker in Gezira Province, Sudan.
40.
41.
42.
43.
44.
It is impossible to prove that female activity patterns were unaffected by my presence. However, the possi- bility of observer bias was minimized by the following actions: first, participants did not know whether or not they had been selected for the study until I turned up at their house on the morning that continuous observations were to be undertaken. The ‘surprise’ nature of the visit meant that it was fairly easy to determine whether or not selected women were planning to go to the fields. Second, I had lived in the village for IO months before this work was undertaken. A great deal was known about my personal background and the style of work was familiar to the women concerned (as I had already undertaken a similar study on female activities in the domestic sphere). Consequently, it was possible to fade into the background and to record events as they unfolded during the day. The fact that no-one refused to participate in the observational work in the cotton fields and that so much anthropometric, haematological and parasitological information could be collected reflects, to some extent, the co-operation of the women concerned; and the relative merits of working with a small sample. And the fact that women did not return to the fields in the afternoon suggests that women did not feel pressurized by me to go to the fields. Marmot M. G. Epidemiology and the art of the soluble. The Lancet 1, 897-900, 1986. Ismail E. T. Social Environment and Daily Routine of Sudanese Women: a Case Study of Urban Middle Class Housewives. Reimer, Berlin, 1982. Parker M. Does schistosomal infection impair the health of women? (Part of a projected collection of essays to be edited by TDR, WHO). Parker M. The effects of Schistosoma mansoni on female activity patterns and infant growth in Gezira Province, Sudan. D.Phil. Thesis, University of Oxford.