Embed Size (px)
Citation preview
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 1/45
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 2/45
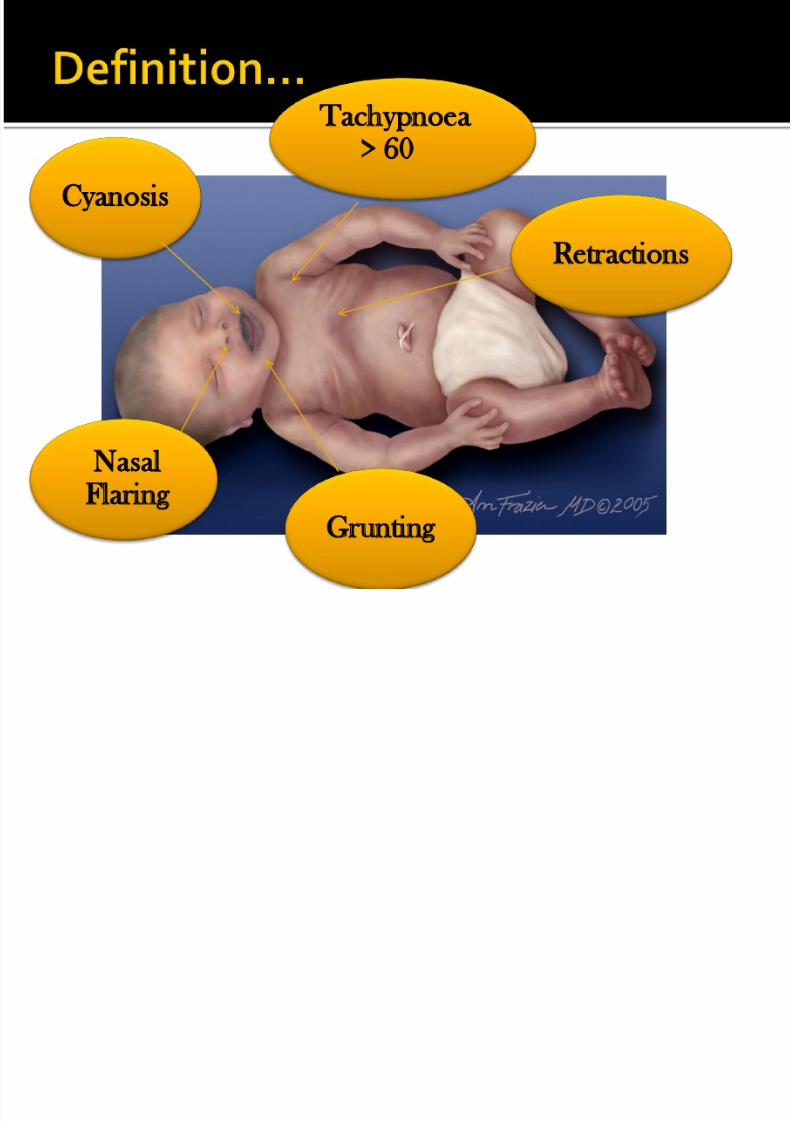
Tachypnoea> 60
Retractions
Grunting
NasalFlaring
Cyanosis
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 3/45
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 4/45
Most common diagnosis of respiratory distress
in the newborn
Also known as RDS type II/ Wet LungSyndrome
Usually follows uneventful normal preterm or
term vaginal delivery or cesarean delivery
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 5/45
Believed to be secondary to slow absorptionof fetal lung fluid resulting in
•decreased pulmonary compliance and tidal volume
•increased dead space
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 6/45
Early onset of tachypnea
Sometimes with retractions, or expiratory
grunting Occasionally cyanosis that is relieved by
minimal oxygen (<40%)
Lungs are generally clear
Usually recover rapidly within 3 days
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 7/45
Labs
FBC within normal limits
ABG showing mild to moderate hypercapnia,hypoxemia with a respiratory acidosis
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 8/45
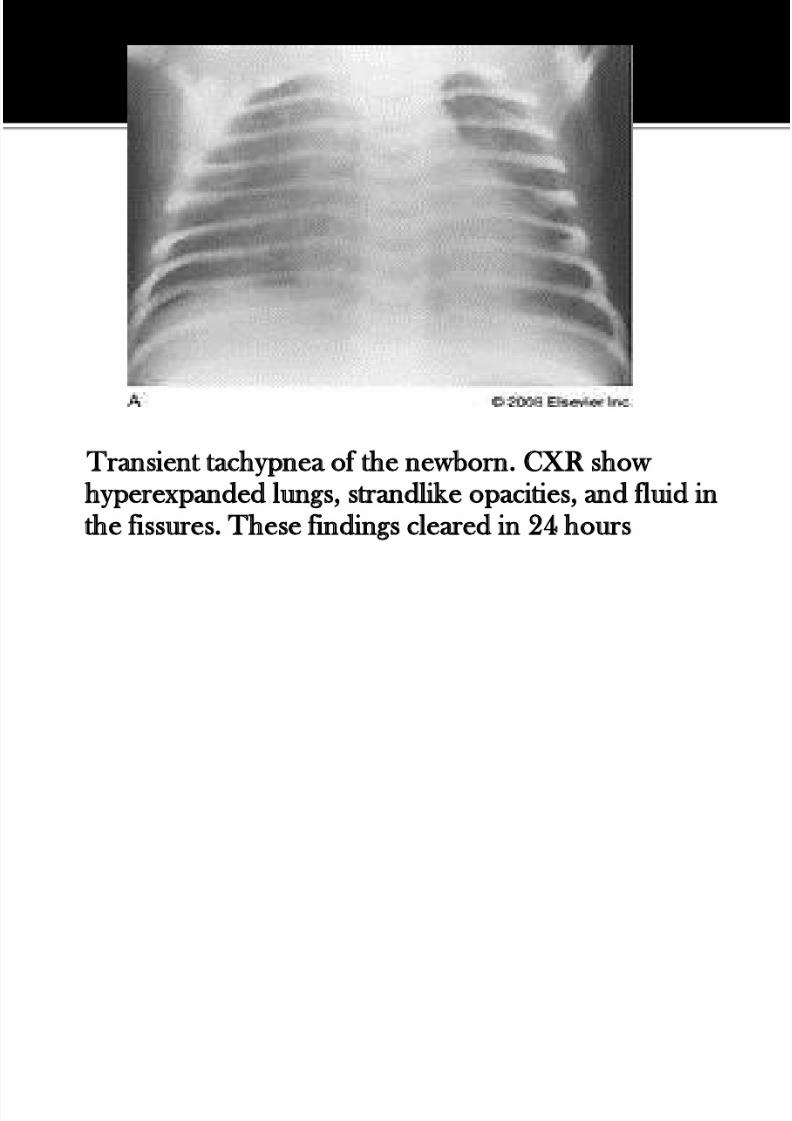
Findings..
prominent pulmonary vascular markings
fluid lines in the fissures
hyperaeration
flat diaphragms
occasionally, pleural fluid
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 9/45
Transient tachypnea of the newborn. CXR showhyperexpanded lungs, strandlike opacities, and fluid inthe fissures. These findings cleared in 24 hours
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 10/45
Supportive treatment :
Oxygen box
CPAP
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 11/45
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 12/45
Meconium-stained amniotic fluid is found in
10–15% of births and usually occurs in term or
post-term infants Meconium aspiration pneumonia develops in
5% of such infants
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 13/45
Infant passes meconium due to varying degreesof asphyxia in utero
Obstruction of large and small airways withaspirated meconium
Aspiration may occur:
in utero
intrapartum postpartum period
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 14/45
Meconium consists of
secretion of the intestinal glands
bile pigmentsfatty acids
aminiotic fluid
intrauterine debris
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 15/45
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 16/45
Respiratory distress within the first hours, with
tachypnea, retractions, grunting, and cyanosis
Partial obstruction of some airways may lead topneumothorax or pneumomediastinum, or
both
Overdistention of the chest may be prominent
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 17/45
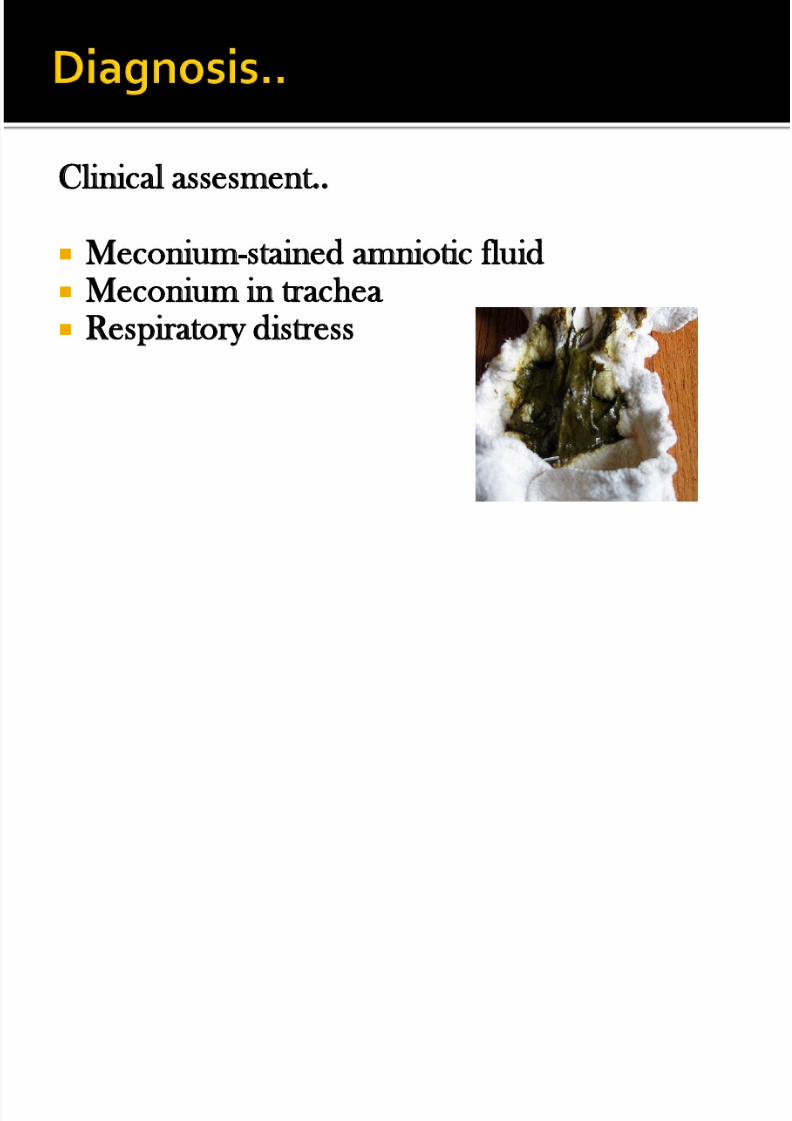
Clinical assesment..
Meconium-stained amniotic fluid Meconium in trachea Respiratory distress
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 18/45
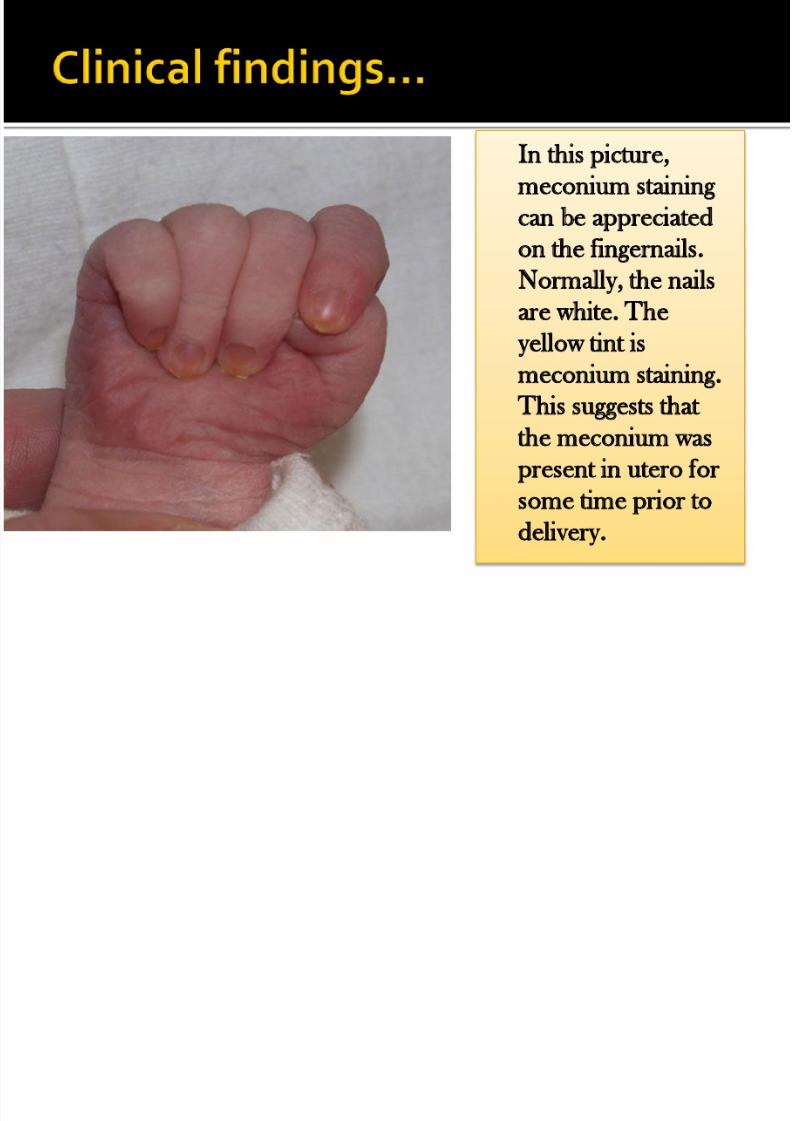
In this picture,
meconium staining
can be appreciated
on the fingernails.
Normally, the nailsare white. The
yellow tint is
meconium staining.
This suggests thatthe meconium was
present in utero for
some time prior to
delivery.
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 19/45
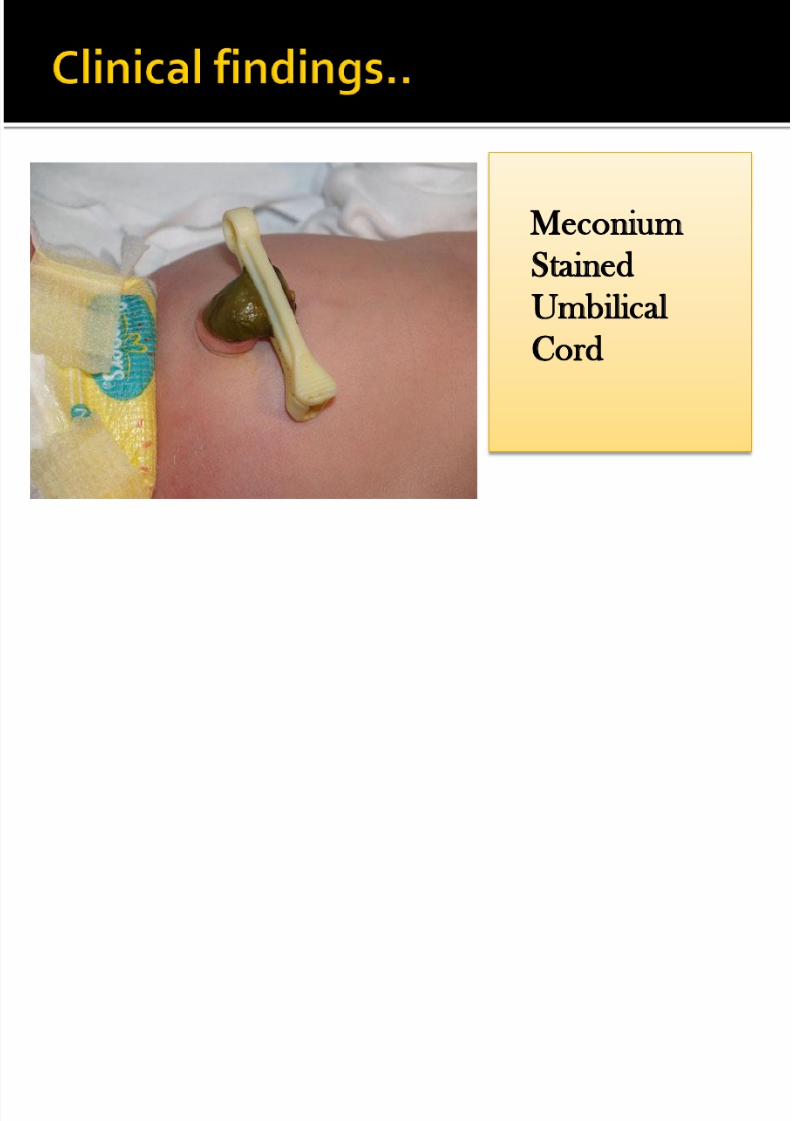
Meconium
StainedUmbilical
Cord
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 20/45
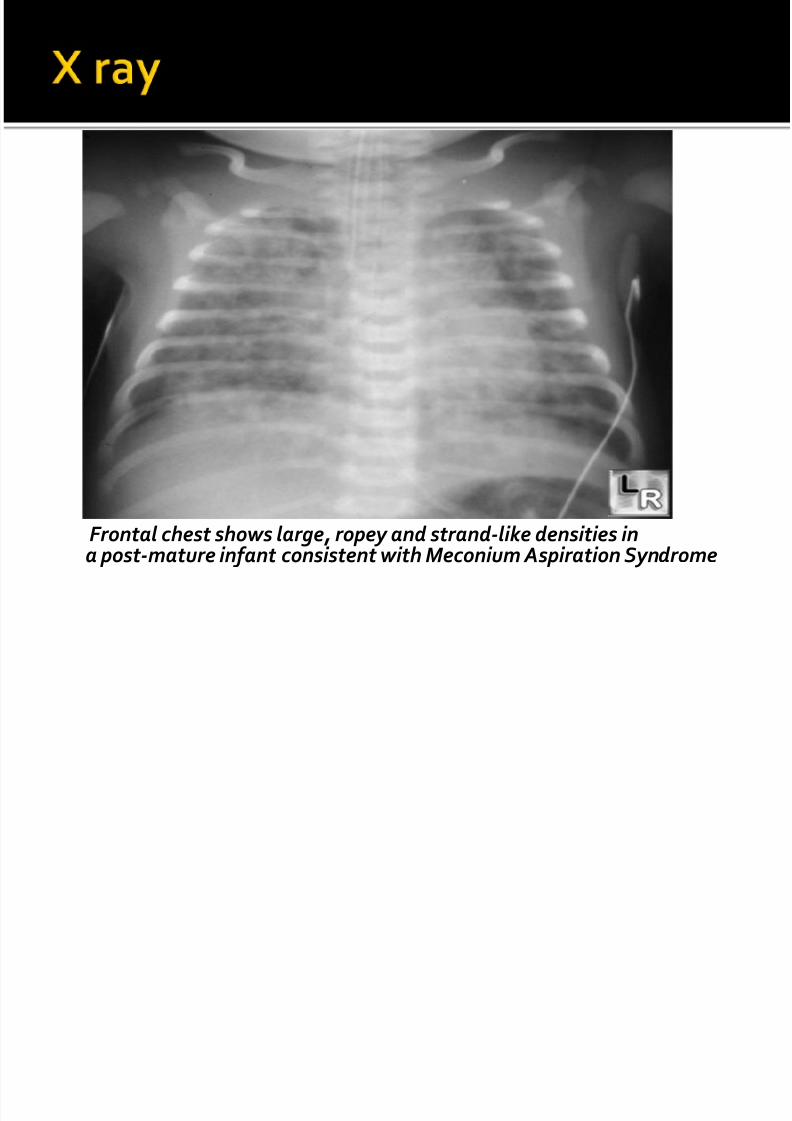
inhomogenous patchy infiltrates
coarse streaking of both lung fields
air traping air leak
pleural effusion
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 21/45
Frontal chest shows large, ropey and strand-like densities in
a post-mature infant consistent with Meconium Aspiration Syndrome
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 22/45
Non-vigorous infant endotracheal intubation
and suction
The oxygenation : PEEP Antibiotics
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 23/45
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 24/45
Aspiration of amniotic fluid
Pathogenic bacteria may accompany theaspirated material, and pneumonia may ensue
Most common organisms :
GBS
E.coli
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 25/45
PROM > 18 hr
Chorioamnionitis
Foul smelling amniotic fluid
Maternal fever before delivery
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 26/45
Congenital Pneumonia
Intrapartum Pneumonia
Postnatal Pneumonia
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 27/45
Lab Ix ;
Septic work up : CBC, CRP, ESR
CXR
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 28/45
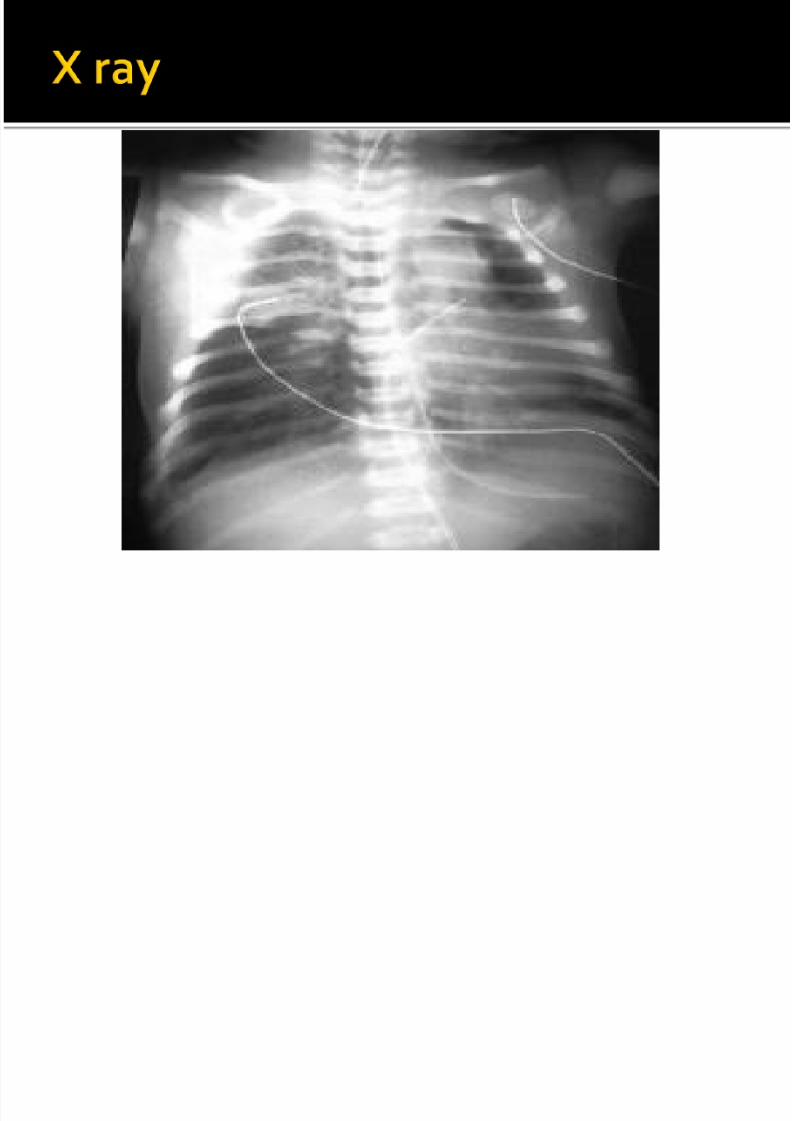
Patchy infiltration or bronchopneumonia
Hypoaeration
Ground glass appearanceAir bronchogram
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 29/45

8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 30/45
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 31/45
Antibiotics
IV C Penicillin 50000unit/kg 12hly
IV Gentamycin 4mg/kg daily
Oxygen therapy

8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 32/45
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 33/45
Occurs primarily in premature infants
60–80% : GA < 28 wk
15–30% : GA 32-36 wk5% : GA >37 wk
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 34/45
increased frequency is associated with
diabetic mothers
delivery before 37 wk gestation
multifetal pregnancies
cesarean section delivery
precipitous delivery
asphyxia cold stress
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 35/45
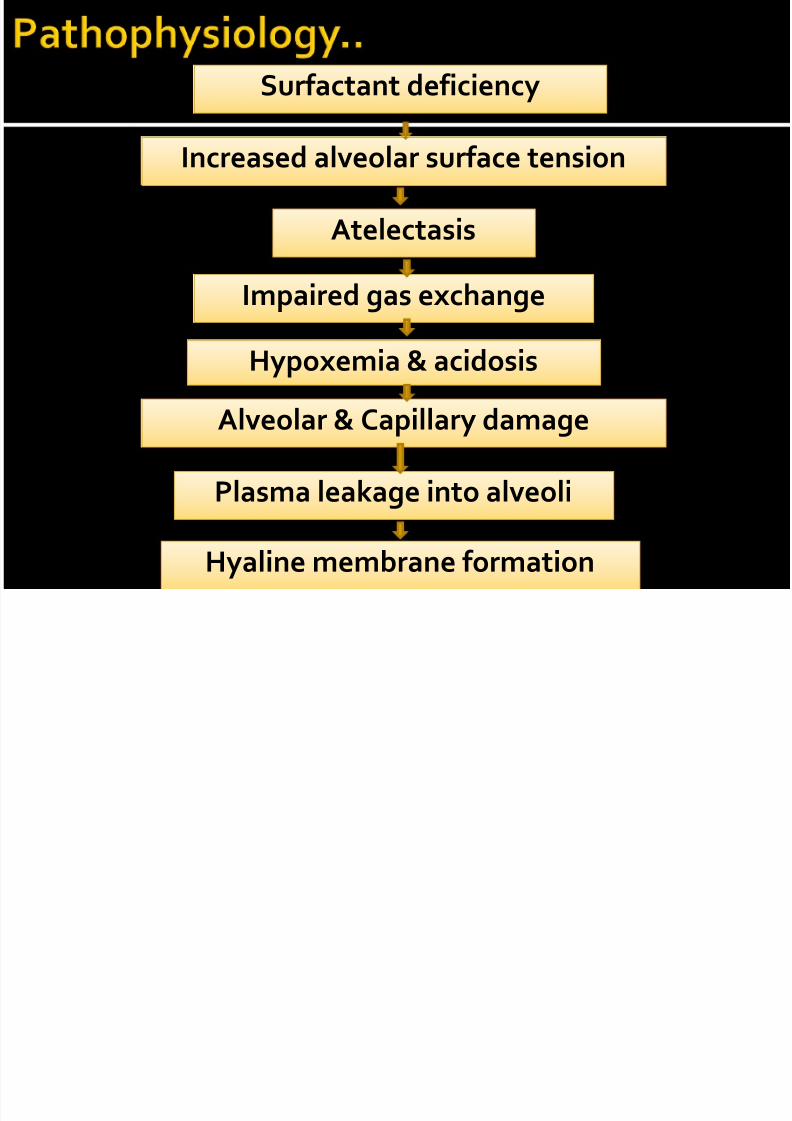
Plasma leakage into alveoli Hyaline membrane formation
Surfactant deficiency Increased alveolar surface tension
Atelectasis Impaired gas exchange Hypoxemia & acidosis
Alveolar & Capillary damage
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 36/45
Usually appear within minutes of birth
Characteristically
tachypnea, prominent (often audible) grunting,
intercostal and subcostal retractions, nasal flaring
cyanosis
Breath sounds : or ↓
Fine rales, especially over the lung bases posteriorly
Progressive worsening of cyanosis and dyspnea
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 37/45
Fine reticulogranular appearance (ground
glass appearance)
Air bronchogramHypoaeration
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 38/45
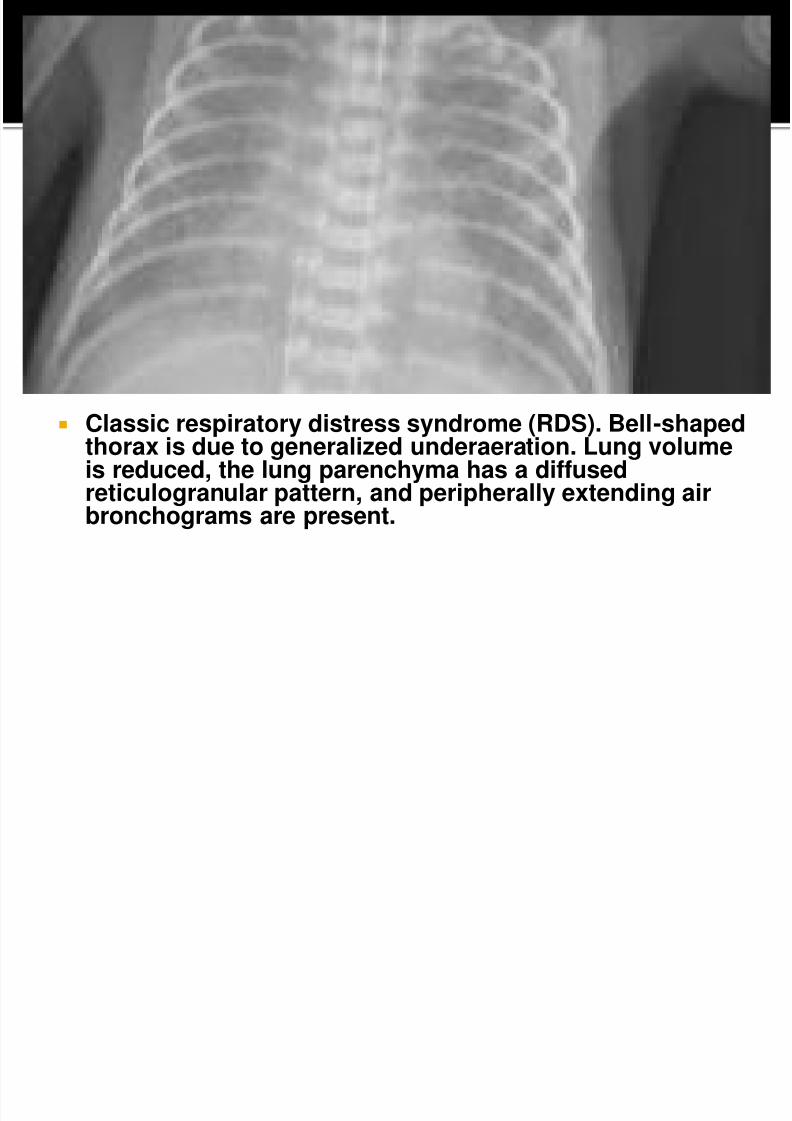
Classic respiratory distress syndrome (RDS). Bell-shapedthorax is due to generalized underaeration. Lung volumeis reduced, the lung parenchyma has a diffusedreticulogranular pattern, and peripherally extending airbronchograms are present.
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 39/45
Specific treatment : Surfactant
surfactant therapy should be instituted only if
there are facilities for ventilation.
The efficacy of surfactant in reducing the
duration of ventilation is proven.
Prophylactic surfactant use is recommended
for any neonate< 28 weeks and < 1000 gms.
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 40/45
1. Survanta
– 100mg of phospholipids/kg/dose (4mL/kg)
– Repeat > 6H after the previous dose if the infant
remains intubated and requires at least 30% O2 tomaintain PaO2 <80mmHg
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 41/45
Supportive treatment
CPAP
Ventilator
Apnea
PaCO2 > 60 mmHg
Low PaO2 (on CPAP with high FiO2)
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 42/45
ROP
BPD
Pneumothorax Infection
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 43/45
Most important is prevention of prematurity Avoidance of unnecessary or poorly timed
cesarean section Prenatal administration of corticosteroids
between 24- 34 wks gestation reduces risk ofrespiratory distress when risk of preterm
delivery is high. Post natal steroids may decrease mortality but
may increase risk of cerebral palsy.
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 44/45
Antenatal steroids will prevent the occurrence andseverity of RDS in preterm babies between 24 and34 weeks of gestation.
Optimal effect of antenatal steroids is seen if
delivery occurs after 24 hours of the initiation of therapy. Effect lasts for 7 days If delivery is anticipated below 34 weeks of
gestation.Dose recommended is:Inj Betamethasone 12 mg 1M every 24 hrs x 2 doses; or
Inj Dexamethasone 6 mg 1M every 12 hrs x 4 doses.
Multiple courses of antenatal steroids are not beneficialand hence are not recommended
8/2/2019 rds theva
http://slidepdf.com/reader/full/rds-theva 45/45


















![RDS 323 Restorative Dental Sciences [ RDS]](https://img.pdfslide.us/doc/110x75/6235ee36aafa9c66c73cc0cf/rds-323-restorative-dental-sciences-rds.jpg)










