Embed Size (px)
Citation preview

This article was downloaded by: [DUT Library]On: 04 October 2014, At: 15:18Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Child Neuropsychology: A Journal onNormal and Abnormal Development inChildhood and AdolescencePublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/ncny20
RD, ADHD, and their comorbidity froma dual route perspectiveChristien G. W. de Jong a , Robert Licht a , Joseph A. Sergeant a &Jaap Oosterlaan aa Department of Clinical Neuropsychology , VU UniversityAmsterdam , Amsterdam , The NetherlandsPublished online: 17 Oct 2011.
To cite this article: Christien G. W. de Jong , Robert Licht , Joseph A. Sergeant & Jaap Oosterlaan(2012) RD, ADHD, and their comorbidity from a dual route perspective, Child Neuropsychology: AJournal on Normal and Abnormal Development in Childhood and Adolescence, 18:5, 467-486, DOI:10.1080/09297049.2011.625354
To link to this article: http://dx.doi.org/10.1080/09297049.2011.625354
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &

Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

Child Neuropsychology, 2012, 18 (5), 467–486http://www.psypress.com/childneuropsychISSN: 0929-7049 print / 1744-4136 onlinehttp://dx.doi.org/10.1080/09297049.2011.625354
RD, ADHD, and their comorbidity from a dual route
perspective
Christien G. W. de Jong, Robert Licht, Joseph A. Sergeant, andJaap Oosterlaan
Department of Clinical Neuropsychology, VU University Amsterdam, Amsterdam, TheNetherlands
In order to achieve further insight into the comorbidity of reading disorder (RD) and attentiondeficit/hyperactivity disorder (ADHD), lexical processing and rapid naming were studied in RD andADHD. The Dual Route Cascaded model postulates that lexical processing contains two parallel pro-cesses: lexical route processing and sublexical route processing. An orthographic decision task and aphonological decision task were used to measure lexical and sublexical route processing, respectively.In addition, a rapid naming task was used to compare 27 children with RD, 18 children with ADHD,20 children with ADHD+RD, and 29 controls. RD and ADHD shared impairments in accuracy oforthographic and phonological decision making as well as in rapid naming, which suggest that RDand ADHD may be overlapping disorders that share deficits in both lexical route and sublexical routeprocessing. RD was dissociated from ADHD by being slower in both orthographical and phonologicaldecision making that indicates unique deficits in RD on lexical and sublexical speed.
Keywords: RD; ADHD; Lexical processing; Rapid naming; Comorbidity.
Reading disorder (RD) and attention deficit/hyperactivity disorder (ADHD) are twocommon childhood disorders that frequently co-occur with estimates varying between20%–40% (Del’Homme, Kim, Loo, Yang, & Smalley, 2007; Semrud-Clikeman et al.,1992). Previous studies targeting the origins of the comorbidity of RD and ADHD focusedon phonological processing and executive functioning with mixed results (Pennington,Groisser, & Welsh, 1993; Rucklidge & Tannock, 2002; Willcutt, Pennington, Olson,Chhabildas, & Hulslander, 2005). The current study explored other mechanisms postu-lated to underlie RD: lexical processing and rapid naming. These processes are considereduniquely impaired in RD; although there is evidence to suggest that lexical processing andrapid naming may also be deficient in ADHD (Semrud-Clikeman, Guy, Griffin, & Hynd,2000; Willcutt et al., 2005). By studying overlapping deficits, it may be possible to gaininsight into the factors contributing to the co-occurrence of both disorders (Willcutt et al.,2005), and by investigating the nonoverlapping deficits, it may be possible to determinewhy some children develop one but not the other disorder (Pennington et al., 1993).
Address correspondence to Christien de Jong, Department of Clinical Neuropsychology, VU UniversityAmsterdam, Van der Boechorststraat 1, 1081 BT Amsterdam, The Netherlands. E-mail: [email protected]
© 2012 Psychology Press, an imprint of the Taylor & Francis Group, an Informa business
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

468 C. G. W. DE JONG ET AL.
Lexical processing is the first focus of this study in order to clarify the origins ofthe comorbidity of RD and ADHD. The Dual Route Cascaded model has been a usefulframework to understand lexical processing in RD (Coltheart, Rastle, Perry, Langdon, &Ziegler, 2001). Briefly, the Dual Route Cascaded model postulates two parallel routes:the lexical route and the sublexical route. In the lexical route, a word that is read ismatched to whole word representations in the mental orthographic lexicon that contributesto efficient and fast reading. The sublexical route uses rules of grapheme-to-phoneme con-version, thus words will be read letter by letter. Both routes give access to the phonologicallexicon.
In languages with a regular orthography, such as Dutch, German, Greek, and Italian,grapheme-to-phoneme relations are highly consistent, thus beginning readers masterphonological processing skills after a few months of reading education (Caravolas, 2006).Learning to read in these languages relies therefore more on speed than on phonologicalprocessing skills (Georgiou, Parrila, & Papadopoulos, 2008). Indeed, in regular orthogra-phies children with RD have extremely slow but accurate reading (e.g., Italian: Brizzolaraet al., 2006; Dutch: De Jong & Van der Leij, 2003; German: Wimmer, 1993). Furthermore,in German, RD has been closely associated with speed impairments as assessed with rapidnaming (Wimmer, Mayringer, & Landerl, 1998). Thus, when phonological demands arereduced due to orthographical consistency, the influence of phonological skills on readingis limited but naming speed as an underlying cognitive deficit seems to play a decisive rolefor reading development. Bergmann and Wimmer (2008) argued that the slow but accu-rate reading of reading-disordered children in consistent orthographies is due to impaireddual route processing. They hypothesize that children with RD rely predominantly on thesublexical route and are impaired in progressing from laborious serial grapheme-phonemecoding to efficient parallel coding in the lexical route. They demonstrated inaccurate lex-ical route processing on an orthographical decision task in German children with RD(Bergmann & Wimmer, 2008). Compared to controls, children with RD had difficulty dis-tinguishing words (stored in the mental orthographic lexicon) from pseudohomophones(words that sound as valid words but are incorrectly spelled and therefore not stored in themental orthographic lexicon). In contrast, the children with RD showed accurate sublexicalroute processing, since they had few errors but slow speed in the phonological distinctionof pseudohomophones and nonwords that have to be decoded letter by letter (Bergmann& Wimmer, 2008). Thus, findings of Bergmann and Wimmer indicated inaccurate lexicalroute processing but intact sublexical route processing in children with RD in consistentorthographies.
Slow speed and impaired lexical route processing in children with RD in consistentorthographies may suggest that lexical route processing and rapid naming tap the same pro-cesses (Hawelka, Gagl, & Wimmer, 2010). Hawelka et al. hypothesized that orthographicalwhole word recognition of letter strings in the lexical route share similar cognitive pro-cesses as used during rapid naming of letters, numbers, colors, or objects. During bothorthographical whole word recognition and rapid naming, a stored representation mustbe recognized (e.g., a word during orthographical recognition or a letter, color, etc. dur-ing rapid naming) and coupled to phonological word representations to pronounce thewhole word or stimulus of the rapid naming task, respectively. Some studies confirmedthis idea, since rapid naming correlated more strongly with orthographical knowledge andless with phonological processing skills (Georgiou, Parrila, Kirby, & Stephenson; 2008)whereas others did not find a relation between orthographical skills and rapid naming
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

RD AND ADHD FROM A DUAL ROUTE PERSPECTIVE 469
(Moll, Fussenegger, Willburger, & Landerl, 2009). Although results are contradicting, itis suggested that lexical route processing and rapid naming share cognitive processes.
Previous findings may suggest that deficits in rapid naming and lexical route pro-cessing may be unique to RD. Although far less studied in ADHD, studies show that rapidnaming deficits and lexical route deficits are also observed in ADHD and thus are not lim-ited to RD (Kibby, Kroese, Krebbs, Hill, & Hynd, 2009; Li, Shu, McBride-Chang, Liu, &Xue, 2009; Raberger & Wimmer, 2003; Shanahan et al., 2006; Van de Voorde, Roeyers,Verté, & Wiersema, 2010; Willcutt et al., 2010). Deficits in rapid naming and lexical routeprocessing seem, therefore, important potential mechanisms to explain the overlap of RDand ADHD.
Although lexical processing in ADHD has not often been the object of research, thereis evidence of lexical route deficits in ADHD (Willcutt et al., 2005). Willcutt et al. com-pared an ADHD group with an ADHD+RD group, RD group, and a control group on anorthographical decision task. Children with ADHD were reported to be impaired in ortho-graphic processing compared to controls; although they were less impaired than childrenwith RD (Willcutt et al., 2005). Children with ADHD have not been found to differ fromcontrols on sublexical route processing, since no deficits in phonological processing wereobserved in ADHD (Pennington et al., 1993; Willcutt et al., 2005). These findings suggestthat both RD and ADHD may have impairments in lexical route processing, whereas sub-lexical route processing is slow but accurate in RD, at least in languages with a regularorthography.
The current study aimed to study the overlap and specificity of impairments in lexicaland sublexical route processing and rapid naming in Dutch children with RD and childrenwith ADHD compared to controls. Since rapid naming deficits may share the same pro-cesses as lexical route processing (Hawelka et al., 2010), we studied whether ADHD andRD in a consistent orthography are characterized by overlapping impairments in both lex-ical route processing and rapid naming. Slow but accurate sublexical route processing wasexpected to be limited to RD. Lexical and sublexical route processing have not been stud-ied previously in both ADHD and RD as potential mechanisms for explaining the originsof the comorbidity of ADHD and RD.
The children included were between 10–13 years of age, since at these ages readingis considered as fairly advantaged and both lexical and sublexical route processing, as wellas rapid naming are considered developed. We hypothesized that children with ADHD andchildren with RD have overlapping deficits in accuracy of lexical route processing andrapid naming, whereas only children with RD were predicted to be slower on sublexicalroute processing compared to controls. Children with RD and children with ADHD werenot expected to differ from controls on speed of lexical route processing or accuracy ofsublexical route processing.
A comorbid ADHD+RD group was included to test whether ADHD+RD is adistinct clinical condition from the single diagnosis of RD and ADHD. The comorbidADHD+RD group has been associated with a distinct profile on rapid naming but noton lexical processing, compared to both children with ADHD only and RD only (Bental& Tirosh, 2007; Rucklidge & Tannock, 2002; Shanahan et al., 2006). Two studies showedmore severe deficits in rapid naming in the comorbid condition (Bental & Tirosh, 2007;Rucklidge & Tannock, 2002), whereas one study observed less impaired rapid naming inchildren with comorbid ADHD+RD than in the single diagnosis groups (Shanahan et al.,2006). We expected a distinct profile on rapid naming for the comorbid ADHD+RD group.Since rapid naming and lexical route processing may share the same cognitive processes
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

470 C. G. W. DE JONG ET AL.
(Hawelka et al., 2010), we expected also a distinct profile on lexical route processing forthe comorbid ADHD+RD group compared to the single diagnosis groups.
METHOD
Recruitment of Participants
Children with RD and controls were recruited from regular primary schools. Childrenwith ADHD and children with ADHD+RD were recruited from child outpatient clinics,special education services, and an institute for remediation of RD.
RD Assessment
All children were screened for the presence of RD with the Three Minutes Test(TMT; Verhoeven, 1995). The TMT consists of three cards of increasing difficulty witheach card containing 150 words printed in five columns. The first two cards are used forchildren in the lower four classes of elementary education. In this study, only the thirdcard was used because the first two cards were deemed to be too easy for children between10–13 years who are in the last two years of elementary education. Children were asked toread as many words as possible in one minute. The total number of words correctly readwas converted into a reading grade equivalent (RGE; Struiksma, Van der Leij, & Vieijra,2004) that reflects the child’s actual reading level expressed in the number of months ofreading instruction (one year of instruction being equivalent to 10 months) (Van der Schoot,Licht, Horsley, & Sergeant, 2000). The extent of reading retardation was computed bysubtracting the RGE from the expected grade equivalent (EGE) expressed as the numberof months that the child had received formal reading instruction. For the TMT, adequatepsychometric properties have been reported (Verhoeven, 1995).
ADHD Assessment
In order to screen for ADHD symptomatology both at school and at home, teachersand parents of participating children were required to complete the Disruptive BehaviourDisorder rating scale (DBD; Oosterlaan, Scheres, Antrop, Roeyers, & Sergeant, 2001).The DBD contains 42 items and comprises four subscales composed of the Diagnostic andStatistical Manual of Mental Disorders, fourth edition (DSM-IV; American PsychiatricAssociation, 2000) items for inattention, hyperactivity/impulsivity, oppositional defiantdisorder (ODD), and conduct disorder (CD). The items were scored on a 4-point scale (notat all, just a little, pretty much, and very much). Higher scores indicate greater symptomseverity. Adequate psychometric properties have been reported (Oosterlaan et al., 2001).
Children meeting criteria for inclusion in the ADHD or ADHD+RD groups onthe basis of the parent and teacher DBD (see “Selection of Groups”) were adminis-tered the Diagnostic Interview for Children (PDISC-IV; National Institute of MentalHealth [NIMH], Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000; Dutch trans-lation; Ferdinand, Van der Ende, & Mesman, 1998) to confirm a diagnosis of ADHDand to establish associated disruptive disorders. The PDISC-IV is a structured diagnos-tic interview based on the DSM-IV and on the International Classification of Diseases,tenth edition (ICD-10). Adequate reliability and validity have been reported for precursorsof the PDISC-IV (Schwab-Stone et al., 1996).
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

RD AND ADHD FROM A DUAL ROUTE PERSPECTIVE 471
IQ Assessment
To estimate intelligence, four subtests of the Wechsler Intelligence Scale forChildren, third version (WISC-III, Wechsler, 1991; Kort et al., 2002) were used: PictureArrangement, Arithmetic, Block Design, and Vocabulary. These four subtests correlatebetween r = .93 to r = .95 with Full Scale IQ (Groth-Marnat, 1997).
Selection of Groups
Children in the RD and ADHD+RD were considered reading disordered when theyexperienced a delay of more than 15 months of reading instruction on the TMT (see Van derSchoot et al., 2000). Controls and children with ADHD were required to have a maximumreading delay of 15 months on the TMT.
To meet the criteria for an ADHD diagnosis, both parent and teacher rat-ings on the DBD fell at or above the 90th percentile on either the Inattention orHyperactivity/Impulsivity subscales or both. In addition, children were required to meetan ADHD diagnosis of either subtype based on the DSM-IV on the PDISC-IV. Controlsand children in the RD group were required to obtain scores below the 90th percentile onall subscales of the DBD. Children were entered in the ADHD+RD group when they metcriteria for both RD and ADHD.
The final sample consisted of 94 participants including 27 children with RD(14 boys), 18 children with ADHD (15 boys), 20 children with comorbid ADHD+RD(16 boys), and 29 controls (11 boys).
The 18 children in the ADHD group were all diagnosed with ADHD combined sub-type. In the ADHD+RD group, 9 children met criteria for ADHD combined subtype, 9 forADHD inattentive subtype, and 2 for ADHD-hyperactive/impulsive subtype. A comorbiddiagnosis of ODD or CD, according to the PDISC-IV or already clinically established,was not an exclusion criterion. In the ADHD group, 8 children had a comorbid diagnosisof ODD and in the ADHD+RD group 8 children also had a comorbid diagnosis of ODD.One child in the ADHD+RD group met the criteria for CD.
Twenty-three children in the ADHD groups were treated with stimulant medicationand discontinued use at least 24 hours prior to testing. Children with neurological disorders,such as epilepsy, were excluded from the study. All children were required to have an IQof at least 75.
Final participant characteristics are shown in Table 1. All included children agedbetween 10 and 13 years (Mage = 11.1 years, SD = 0.83). Groups did not differ in age.Children with ADHD+RD had a lower IQ than children with ADHD and control children.Findings on the DBD and the PDISC-IV confirmed the expected clinical group character-istics for ADHD of the ADHD and ADHD+RD groups and indicated that the two ADHDgroups did not differ in the severity of ADHD symptoms.
Since the children with RD were recruited at primary schools and the children inthe ADHD+RD group were recruited at a center for reading remediation, the RD groupmight have been less impaired in reading than the ADHD+RD group. However, the tworeading groups did not differ in severity of reading impairments as indicated by the TMT(see Table 1). The RD group showed an average delay of 26 months of reading instruction,whereas the ADHD+RD group had a mean delay of 33 months of reading instruction.These figures underline the severe reading impairment in the two reading disorderedgroups.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

472 C. G. W. DE JONG ET AL.
Table 1 Clinical Characteristics of the RD, ADHD, ADHD + RD, and Control Groups.
RDn = 27
(14 boys)
ADHDn = 18
(15 boys)
ADHD + RDn = 20
(14 boys)
Cn = 29
(11 boys)
PairwiseGroup Comparisons
using Tukey∗
Measure M SD M SD M SD M SD
IQ 101.26 13.90 104.22 12.67 91.88 10.09 106.34 10.78 ADHD + RD< ADJD, C
Age 11.04 0.80 10.89 1.07 11.30 0.78 10.97 0.73 nsDBD Parents
Inattention 3.64 2.54 16.67 3.83 16.70 3.94 2.38 3.11 ADHD + RD,ADHD > RD, C
H/I 1.80 2.12 16.83 4.73 13.85 8.06 1.41 1.59 ADHD + RD,ADHD > RD, C
DBD TeacherInattention
1.93 2.31 15.94 5.33 14.30 5.55 1.54 2.31 ADHD + RD,ADHD > RD, C
H/I 0.63 1.36 16.22 1.36 12.10 6.92 0.46 1.03 ADHD + RD,ADHD > RD, C
PDISC-IVInattention
− − 15.50 1.04 15.22 2.90 − − ns
H/I − − 14.66 2.94 10.22 5.71 − − nsReading1
TMT card26.89 9.14 5.11 6.43 33.10 11.25 1.52 7.45 ADHD + RD,
RD > ADHD, C
Note. ADHD = attention deficit/hyperactivity disorder, DBD = Disruptive Behavior Disorder rating scale,IQ = Intelligence Quotient, H/I = hyperactivity/impulsivity, C = controls, PDISC-IV = Parent DiagnosticInterview Scale for Children, RD = reading disorder, TMT = Three Minute Test.
1Delay in months of education.∗p < .05.
Measures
Lexical Route Processing. Lexical route processing was assessed using an ortho-graphic decision task (Bergmann & Wimmer, 2008). In the orthographic decision task,participants decided whether letter strings, presented singly on a computer screen, werecorrectly spelled words (valid words, for example “kans” that means chance) or not (pseu-dohomophones, which were valid words in which one or two letters were changed andsounded like valid words when pronounced, for example “jeugt” of the valid word “jeugd”that means youth). Children were required to press the “z” key on a computer keyboardfor valid words and the “m” key for pseudohomophones. The stimuli were monosyllabicfour- or five-letter words with a CCVC, CVCC, CCVVC, or CVVCC structure (C =Consonant, V = Vowel; see Appendix A for the items). The mean frequency of the validwords was 368.9 out of 10 million words (SD = 581.8). The mean frequency of the validword derivations of the pseudohomophones was 377.7 (SD = 451.6) (Corpus GesprokenNederlands [CGN], 2004). The frequencies of the valid words and pseudohomophones didnot differ.
The orthographic decision task commenced with a practice block of 25 letter strings(both valid words and pseudohomophones, see Appendix A), which were repeated if thechild responded to 40% or more of the letter strings incorrectly. The practice block wasfollowed by two blocks of 50-letter strings. Each block contained 25 valid words and25 pseudohomophones shown in fixed random order. Each trial started with a fixationcross illuminated for 1000 ms. In order to counteract the tendency to react in an automatic
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

RD AND ADHD FROM A DUAL ROUTE PERSPECTIVE 473
fashion, responding was possible 300 ms after stimulus onset. The maximum trial durationwas 5000 ms.
Accuracy of orthographic decision making was assessed by d’ that is a measure ofthe ability to distinguish signal from noise (i.e., valid words versus pseudohomophones).The d’ of orthographic decision making was calculated as follows: probit (hit rate correctlyidentified valid words) – probit (false positive rate correctly identified pseudohomophones)(MacMillan & Creelman, 1991). In this formula, hit rate referred to the number of cor-rectly identified valid words divided by the total number of valid words; the false positiverate referred to the number of correctly identified pseudohomophones divided by the totalnumber of pseudohomophones. The hit rate and the false positive rate for each child werenormalized by a probit function because responses were binomial. Speed of orthographicdecision was measured by mean reaction time (MRT) of the correctly identified valid wordsand pseudohomophones.
Sublexical Route Processing. Sublexical route processing was assessed with aphonological decision task (Bergmann & Wimmer, 2008; Milne, Nicholson, & Corballis,2003). The phonological decision task had the same design as the orthographic decisiontask, only the type of letter strings differed between the tasks. In the phonological decisiontask, the child had to decide whether letter strings sounded like valid words if pronounced(pseudohomophones, for example “weetun” of the valid word “weten” that means to know)or not (nonwords, for example “poonun” that is pronounceable in Dutch but is meaning-less). The letter strings had six letters usually with a CVCVC structure. Children wererequired to press the “z” key on the keyboard for pseudohomophones and the “m” key fornonwords (see Appendix A for the items). The mean frequency of the valid words, deriva-tions of the pseudohomophones and nonwords, was 490.0 (SD = 653.7) out of one millionwords (CGN, 2004). The mean frequency of the pseudohomophones and nonwords of thephonological decision task did not differ.
Similarly, to the orthographic decision task, there was a practice block of 25 let-ter strings (both pseudohomophones and nonwords), which could be extended once by25 words if the child responded to 40% or more incorrectly. Thereafter, two blocksof 50-letter strings were presented. Each block contained 25 pseudohomophones and25 nonwords in fixed random order.
The accuracy measure, d’, was calculated as follows: probit (hit rate correctly iden-tified pseudohomophones) – probit (false positive rate correctly identified nonwords)(MacMillan & Creelman, 1991). Speed of phonological decision was measured with MRTof the correctly identified pseudohomophones and nonwords.
Rapid Naming. The rapid naming task consisted of four cards (Denckla, 1973).The first card containing 50 colored squares (yellow, blue, red, black, green), the secondcard containing 50 numbers (2, 6, 9, 4, 7), the third card containing 50 letters (O, A, S,T, P), and on the fourth card containing 50 objects (ball, fish, house, pencil, car) werepresented. On all cards, stimuli were printed in random order in five rows of 10 stim-uli each. Participants were required to name the items as quickly and as accurately aspossible. The dependent variable was the time required to name the items on each cardin seconds. Since there were few errors, errors were not analyzed (see Table 2 for errorpercentages).
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

474 C. G. W. DE JONG ET AL.
Tabl
e2
Perf
orm
ance
ofth
eR
D,A
DH
D+
RD
and
Con
trol
Gro
ups
onL
exic
alPr
oces
sing
and
Rap
idN
amin
g.
RD
n=
27(1
4bo
ys)
AD
HD
n=
18(1
5bo
ys)
AD
HD
+R
Dn
=20
(16
boys
)C
n=
29(1
1bo
ys)
Mea
sure
MSD
MSD
MSD
MSD
Lex
ical
Rou
tePr
oces
sing
Acc
urac
yd’
Ort
hogr
aphi
cD
ecis
ion
Mak
ing
1.91
0.77
2.71
0.75
1.64
0.87
3.20
0.86
Spee
dM
RT
Val
idW
ords
(ms)
1666
.41
380.
8912
90.8
633
7.28
1733
.05
552.
1512
89.7
832
2.64
MR
TPs
eudo
hom
opho
nes
(ms)
2134
.65
526.
0715
40.6
348
5.41
2176
.63
568.
0915
55.5
232
0.44
Subl
exic
alR
oute
Proc
essi
ngA
ccur
acy
d’Ph
onol
ogic
alD
ecis
ion
Mak
ing
1.88
0.58
2.12
0.55
1.67
0.59
2.66
0.59
Spee
dM
RT
Pseu
doho
mop
hone
s(m
s)18
00.3
130
0.32
1501
.09
305.
3719
18.3
655
1.41
1436
.84
227.
09M
RT
Non
wor
ds(m
s)25
26.7
339
0.04
1861
.41
410.
9125
60.4
958
1.14
2095
.52
444.
03R
apid
Nam
ing
Col
ors
(s)/
Mea
nPe
rcen
tage
ofE
rror
s44
.00/
0.11
11.4
4/0.
4743
.89/
0.77
9.84
/1.
2145
.15/
0.33
7.91
/0.
7637
.66/
0.55
7.04
/0.
55L
ette
rs(s
)/M
ean
Perc
enta
geof
Err
ors
27.4
8/0.
907.
55/1.
6524
.94/
0.50
5.05
/1.
1031
.65/
1.30
6.44
/2.
2723
.03/
0.90
3.78
/0.
90N
umbe
rs(s
)/M
ean
Perc
enta
geof
Err
ors
29.8
5/0.
448.
80/1.
0126
.67/
0.37
5.87
/0.
9631
.90/
0.22
7.17
/0.
8423
.69/
0.59
5.27
/0.
59O
bjec
ts(s
)/M
ean
Perc
enta
geof
Err
ors
44.8
1/0.
208.
43/0.
8144
.94/
0.20
11.5
2/0.
8147
.45/
0.68
6.82
/2.
0140
.14/
0.20
7.47
/0.
20
Not
e.A
DH
D=
atte
ntio
nde
ficit/
hype
ract
ivity
diso
rder
,C=
cont
rols
,RD
=re
adin
gdi
sord
er,M
RT
=M
ean
Rea
ctio
nT
ime.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

RD AND ADHD FROM A DUAL ROUTE PERSPECTIVE 475
Procedure
For each child, first the DBD was obtained, when applicable the PDISC-IV wasadministered to the parents at their homes. When eligible, the children were individuallytested during the morning in a quiet room in their school, outpatient clinic, or remediationcenter, depending on where the children were recruited. The tests were administered ina single session in a fixed order. The orthographical decision task was administered first,followed by the four WISC-III subtests, the phonological decision test, the TMT, and therapid naming test. This study was approved by the local medical ethics committee andinformed consent was obtained from the parents of all participating children.
Statistical Analysis
The percentage of missing data was less than 5% for all variables. Missing datawere replaced by regression analysis (Tabachnick & Fidell, 2007). Extreme outliers werereplaced by the next most extreme value in the distribution plus one unit to reduce theirinfluence in the analyses (Tabachnick & Fidell, 2007).
In all analyses, group differences were studied using an analysis of variance(ANOVA) with two between-subjects factors: RD (two levels: present or absent) andADHD (two levels: present or absent). Group differences in accuracy of lexical routeand sublexical route processing were tested using two separate ANOVAs with d’ ortho-graphic decision making and d’ phonological decision making as dependent variables,respectively. To test whether speed in lexical route processing differed between groups, weperformed an ANOVA with word type (two levels: valid words and pseudohomophones ofthe orthographical decision task) as the within-subject factor. Group differences on speedof sublexical route processing were tested with an ANOVA with word type (two levels:pseudohomophones of the phonological decision task and nonwords) as the within-subjectfactor. In order to test group differences for speed of rapid naming, we used an ANOVAwith stimulus type as the within-subject factor (four levels: colors, objects, letters, num-bers). Since group differences were the focus of this study, main effects of within-subjectfactors are not reported in the interest of space limitations and are available on requestto the first author. Post hoc testing was performed using Tukey t-tests. All analyses wererepeated using IQ as a covariate since groups differed in IQ. In addition, we studied theeffect of sex on the results since sex ratios were unbalanced across the four groups.
RESULTS
Table 2 displays the results on the orthographic and phonological decision tasks andon the rapid naming task for the four groups.
Lexical Route Processing
Main effects for both RD and ADHD were found for d’ orthographic decisionthat measures accuracy of orthographic decision making, RD: F(1, 90) = 46.07, p <
.001, ηp2 = .33, and ADHD: F(1, 90) = 4.71, p < .03, ηp
2 = .05. These findingsindicate that both RD and ADHD are associated with poorer accuracy in lexical routeprocessing. The RD by ADHD interaction was not significant for d’ orthographic deci-sion, F(1, 90) = 0.41, p < .52, ηp
2 = .005, demonstrating that the performance of
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

476 C. G. W. DE JONG ET AL.
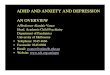
Differential Effects of Word Type on Orthographical DecisionMaking in RD
1200
1400
1600
1800
2000
2200
2400
2600
2800
Valid Words Pseudohomophones
Word Type
ms RD Absent
RD Present
Figure 1 Significant interaction between RD (present versus absent) and word type (valid words versuspseudohomophones) during orthographic decision making. Children with RD appeared relatively slower onpseudohomophones compared to valid words than children without RD.
the comorbid group reflects additive effects rather than interactive effects of ADHDand RD.
Children with RD had slower MRTs on the orthographic decision task than chil-dren without RD, indicating slower orthographic decision making speed in RD, F(1, 90)= 33.79, p < .001, ηp
2 = .27. However, the main effect of RD was modified by wordtype since the RD by word type interaction for MRT on the orthographic decision taskwas significant, F(1, 90) = 11.36, p < .001, ηp
2 = .11. Figure 1 shows that children withRD were relatively slower on pseudohomophones than valid words compared to childrenwithout RD. Post hoc testing showed that children with RD were slower than childrenwithout RD on both valid words, t(82) = 4.80, p < .001, and pseudohomophones,t(82) = 6.01, p < .001. Further, the ANOVA with word type as the within-subject fac-tor was reran for children with RD and children without RD separately. Both children withRD and children without RD were slower on pseudohomophones than on valid words, RDpresent: F(1, 46) = 119.1, p < .001, ηp
2 = .72, and RD absent: F(1, 46) = 45.09, p <
.001, ηp2 = .49.
In contrast, ADHD was not associated with slower orthographic decision makingspeed, F(1, 90) = 0.02, p < .87, ηp
2 < .001, nor was the ADHD by word type interactionsignificant, F(1, 90) = 0.11, p < .73, ηp
2 = .001. The RD by ADHD interaction was notsignificant for orthographic decision making speed, F(1, 90) = 0.12, p < .72, ηp
2 = .001,nor was the RD by ADHD by word type interaction significant, F(1, 90) = 0.005, p < .94,ηp
2 = .001.Taken together the findings for orthographic decision making speed indicate that
RD but not ADHD is associated with slow orthographic decision making speed suggestingslow lexical route processing in RD. The effects of RD on speed of lexical route processingwere not influenced by the presence or absence of comorbid ADHD.
Sublexical Route Processing
Main effects for both RD and ADHD were found for d’ phonological decision mak-ing that measures accuracy of phonological decision making, RD: F(1, 90) = 24.80, p <
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

RD AND ADHD FROM A DUAL ROUTE PERSPECTIVE 477
Differential Effects of Word Type on Phonological DecisionMaking in RD
1200
1400
1600
1800
2000
2200
2400
2600
2800
Pseudohomophones NonwordsWord Type
ms RD Absent
RD Present
Figure 2 Significant interaction between RD (present versus absent) and word type (pseudohomophones versusnonwords) during phonological decision making. Children with RD appeared relatively slower on nonwords thanon pseudohomophones compared to children without RD.
.001, ηp2 = .21, and ADHD: F(1, 90) = 9.32, p < .003, ηp
2 = .09. These results showthat, contrary to predictions, both RD and ADHD were associated with poorer accuracyof sublexical route processing. The RD by ADHD interaction was not significant for d’phonological decision making, F(1, 90) = 1.77, p < .18, ηp
2 = .01, indicating that theperformance of the comorbid group reflects additive effects rather than interactive effectsof ADHD and RD.
Children with RD had slower MRTs on the phonological decision task than childrenwithout RD, indicating slower phonological decision making speed in RD, F(1, 90) =36.95, p < .001, ηp
2 = .29. The RD by word type interaction for MRT for the phonolog-ical decision task was significant, F(1, 90) = 11.36, p < .001, ηp
2 = .11. Figure 2 showsthat children with RD were relatively slower in processing nonwords than pseudohomo-phones than children without RD. Post hoc comparisons indicated that children with RDwere slower than children without RD on pseudohomophones, t(82) = 5.20, p < .001,and nonwords, t(82) = 5.81, p < .001. Further, the ANOVA with word type as the within-subject factor was reran for children with RD and children without RD separately. It wasfound that both children with RD and children without RD were slower on nonwords thanon pseudohomophones, RD present: F(1, 46) = 223.38, p < .001, ηp
2 = .83, and RDabsent: F(1, 46) = 84.09, p < .001, ηp
2 = .69.ADHD, in contrast, was not associated with phonological decision making speed,
F(1, 90) = 0.02, p < .95, ηp2 < .001. Unexpectedly, ADHD interacted significantly with
word type for MRT for the phonological decision task, F(1, 90) = 7.75, p < .007, ηp2 =
.07. Follow-up tests, however, could not identify significant differences between childrenwith ADHD compared to children without ADHD on pseudohomophones and nonwords,pseudohomophones: t(92) = 1.23, p > .10, and nonwords, t(92) = 1.04, p > .10. Thesefindings suggest that the ADHD by word type interaction does not pinpoint meaningfuldifferences in phonological decision making speed for nonwords and pseudohomophonesin ADHD. The RD by ADHD interaction and the RD by ADHD by word type interactionwere not significant for MRT for the phonological decision task, F(1, 90) = 1.04, p < .30,ηp
2 = .01, and F(1, 90) = 2.42, p < .12, ηp2 = .02, respectively.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

478 C. G. W. DE JONG ET AL.
These results indicate that RD, but not ADHD, is associated with slower sublexi-cal route processing. The effects of RD on speed of sublexical route processing were notinfluenced by the presence or absence of comorbid ADHD.
Rapid Naming
Main effects for rapid naming were noted for both RD and ADHD, RD: F(1, 90)= 11.35, p < .001, ηp
2 = .11, and ADHD: F(1, 90) = 5.47, p < .02, ηp2 = .05. These
results suggest that slower rapid naming is implicated in both RD and ADHD. The RD byADHD interaction was not significant, F(1, 90) = 0.28, p < .59, ηp
2 = .003, indicatingthat the performance of the comorbid group reflects additive rather than interactive effectsof ADHD and RD.
RD and ADHD did not significantly interact with stimulus type, RD: F(3, 235) =0.29, p < .29, ηp
2 = .01, ADHD: F(3, 235) = 0.32, p < .77, ηp2 = .004. The RD by
ADHD by stimulus type interaction was not significant, F(3, 235) = 2.27, p < .09, ηp2 =
.02. These results indicate that stimulus type of rapid naming did not have a differentialeffect on the groups.
Effects of IQ and Sex
Covarying for IQ left findings unchanged with one exception: Main effects of ADHDdisappeared on accuracy of orthographic decision making after covarying for IQ.
Since sex ratios were unbalanced, we tested whether sex impacted our results. Fornone of the dependent variables was a significant ADHD by sex, RD by sex, ADHD byRD by sex interaction effect obtained (ηp
2 range: .002 to .02). Since sex did not interactwith ADHD or RD, we concluded that our results were not influenced by sex.
DISCUSSION
This study focused on the overlap and specificity of impairments in lexical andsublexical route processing, as well as rapid naming in RD and ADHD. As expected,impairments in lexical route processing were found in both RD and ADHD since bothdisorders were associated with poor accuracy of orthographic decision making. However,lexical route impairments were more severe in RD: Children with RD were not onlyless accurate compared to children without RD but also slower on orthographic decisionmaking and on pseudohomophones (which are orthographically more complex than validwords) in particular.
Contrary to predictions, both RD and ADHD were associated with deficient sub-lexical route processing since both RD and ADHD were associated with less accuracy inphonological decision making. Sublexical route processing impairments were more severein RD, since RD was also associated with slower sublexical route processing. Childrenwith RD showed the expected speed impairments on phonological decision making ingeneral and on nonwords (which place higher demands on sublexical processing thanpseudohomophones) in particular.
As predicted, both RD and ADHD exhibited slower rapid naming. For all rapid nam-ing measures, findings for RD were unaffected by the presence or absence of comorbidADHD. Likewise, the results for ADHD were unaffected by the presence or absence ofcomorbid RD.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

RD AND ADHD FROM A DUAL ROUTE PERSPECTIVE 479
We did not expect inaccurate sublexical route processing in ADHD or RD. Thereare at least two possible explanations for our finding in RD. First, our unexpected findingmight have been due to length of the nonwords and pseudohomophones used in the phono-logical decision task. The so-called “word-length effect” refers to the common finding thatlonger words take more time to recognize than shorter words since more letters have tobe decoded (De Luca, Barca, Burani, & Zoccolotti, 2008; Juphard, Carbonnel, & Valdois,2004; Martens & De Jong, 2006). Since children with RD are slower in decoding letters,these children are more disadvantaged by the word-length effect compared to typicallydeveloping readers (Martens & De Jong, 2006; Zoccolotti et al., 2005). Because words inthe phonological decision task always consisted of six letters, we were not able to studythe impact of word length in this task. However, we were able to test the word-length effectin the orthographical decision task, since this task consisted of four- and five-letter words.We found that word length did not affect speed of orthographical decision in ADHD, RD,or both ADHD and RD. However, word length affected accuracy of orthographical deci-sion in both ADHD and RD because both ADHD and RD were more associated withlower accuracy on five-letter words than on four-letter words (data available on requestto the first author). On the basis of this finding, it could be argued that our findings onaccuracy of orthographical decision in ADHD and RD might have been confounded bythe word-length effect, whereas speed on orthographical decision in ADHD and RD is notlikely to be influenced by the word-length effect. Future studies should focus on whetherinaccurate phonological decision in ADHD and RD might have been (partly) due to theword-length effect.
Second, the unexpected finding of poorer accuracy in phonological decision in RDmight be explained in terms of the slow sublexical route processing. Because of the fixedpacing of the phonological decision task, responses that exceed the response window resultin omission errors. Indeed, we found that RD, but not ADHD, interacted with word type(two levels: pseudohomophones and nonwords) for omission errors on the phonologicaldecision task, RD by word type; F(1, 90) = 6.11, p < .01, ηp
2 = .06; ADHD by wordtype; F(1, 90) = 0.08, p < .77, ηp
2 = .001; ADHD by RD by word type; F(1, 90) =0.32, p < .57, ηp
2 = .004. This interaction was explained by a higher number of omissionerrors on nonwords than on pseudohomophones in children with RD compared to childrenwithout RD. These findings may indicate that inaccurate phonological decision in RD wasa reflection of the expected longer sublexical route decoding time in RD that was furtherunderlined by the longer decoding time of the nonwords in particular.
The unexpected inaccurate sublexical processing in ADHD may be due to deficitsin working memory reported in ADHD (Martinussen et al., 2005). Since letter strings inthe phonological decision task could not be processed in an automatic fashion like thevalid words in the orthographic decision task and since letter strings in the phonologicaldecision task were longer than in the orthographical decision task (on which no speedimpairments were observed in ADHD), letter strings of the phonological decision taskmay have required more working memory resources than the orthographical decision task.Future studies should elaborate on this issue and investigate the possibility that sublexicalroute deficits in ADHD are due to or associated with working memory demands.
We found that a slow speed of lexical and sublexical route processing was related tohaving RD but not ADHD. Slow speed of lexical and sublexical route processing togetherwith slow speed on all stimulus types of rapid naming in RD support the double-deficithypothesis model of RD (Wolf & Bowers, 1999). This model postulates that a deficit inphonological processing is the core deficit of RD. In addition, this model proposes slowrapid naming as a second independent underlying cognitive impairment in RD. Especially
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

480 C. G. W. DE JONG ET AL.
in languages with regular orthographies, speed deficits in reading are characteristic forindividuals with RD (Van den Bos, 1998), which is underlined by our findings. Wolf andBowers argued that impairments in speed of rapid naming might pinpoint a generalizedtemporal processing deficit. It is unclear, however, whether RD is characterized by generalspeed deficits since some studies found slower speed of processing in both RD and ADHD;although in these studies, RD was more impaired than ADHD (Shanahan et al., 2006;Willcutt et al., 2005). Future studies should determine whether general speed impairmentsare unique to RD, or whether only speed in the reading domain is implicated in RD.
Our findings indicate that both RD and ADHD are associated with deficits inrapid naming, which confirms earlier findings (Semrud-Clikeman et al., 2000; Tannock,Martinussen, & Frijters, 2000). Neuroscientific evidence may explain the overlap in rapidnaming between RD and ADHD. Following, Nicholson, Fawcett, and Dean (2001), RD isdue to a failure in automatization of processing because of impairments in the cerebellum,which becomes evident in deficient rapid naming, but also in deficient balance and skilledmotor behavior. Deficits in the cerebellum occur also in ADHD (e.g., Bledsoe, Semrud-Clikeman, & Pliszka, 2009; Vaidya & Stollstorff, 2008), which may explain rapid namingdeficits in children with ADHD. Further studies should investigate whether rapid namingdeficits in ADHD and RD may be due to common impairments in the cerebellum.
In contrast to the findings of Rucklidge and Tannock (2002) and Bental and Tirosh(2007), no evidence was found here for a distinct profile of rapid naming impairmentsin comorbid ADHD+RD group. No evidence was found for the etiological subtypehypothesis that proposes that comorbid ADHD+RD is a different disorder than the sin-gle diagnoses ADHD and RD (Purvis & Tannock, 2000). Our results, in contrast, indicatethat there were overlapping impairments in RD and ADHD on rapid naming and accuracyof lexical and sublexical processing, providing support for the common etiology hypothe-sis, which states that common underlying etiological factors may lead to different disorders(Willcutt et al., 2005).
The results of the current study should be interpreted in the light of some limitations.First, the ADHD+RD group had a lower IQ than the ADHD and control group. Althoughresults remained essentially unchanged after covarying for IQ, the main effect of ADHDon accuracy of orthographic decision disappeared, which suggest that impairments in lexi-cal route processing in ADHD were at least partly dependent on IQ. Future studies shouldmatch groups on IQ to isolate possible effects of IQ. Second, our groups were not balancedin the distribution of both sexes. However, sex did not interact with RD or ADHD for anyof the dependent variables. Third, children in the RD group and the comorbid ADHD+RDgroup were recruited at different settings that might have caused differences in severityof reading deficits; that however appeared not the case. Fourth, the orthographical deci-sion task consisted of four- or five-letter strings, whereas the phonological decision taskconsisted of six-letter strings. Future studies should use an orthographical and a phonolog-ical decision task containing letter strings equal in length to rule out possible confoundingeffects of the word-length effect. Fifth, the two ADHD groups had different ADHD subtyperates: The ADHD group consisted only of children with ADHD combined type, whereas allthree subtypes of ADHD were represented in the ADHD+RD group. However, since therewas no indication that the two ADHD groups performed differently, we assume that thedifferent ADHD subtype rates had no effects on the results. Lastly, in this study rapid nam-ing total time was used. However, it remains unclear how rapid naming total time is relatedto reading since it may be a multicomponent measure. Data on interitem pauses and onarticulation time of rapid naming suggest that these two components are independent and
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

RD AND ADHD FROM A DUAL ROUTE PERSPECTIVE 481
contribute uniquely to reading (Georgiou, Parrilla, & Kirby, 2009). Future studies shouldincorporate these two components of rapid naming to clarify this issue.
In summary, RD and ADHD may be overlapping disorders with shared deficitsin lexical route processing, sublexical route processing and rapid naming. RD can bedissociated from ADHD by lexical and sublexical speed. No support was obtained forADHD+RD as a separable clinical entity, since ADHD+RD could not be distinguishedfrom either ADHD or RD.
Original manuscript received December 2, 2010Revised manuscript accepted August 20, 2011
First published online October 18, 2011
REFERENCES
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders(text revision). Washington, DC: Author.
Bental, B., & Tirosh, E. (2007). The relationship between attention, executive functions and readingdomain abilities in attention deficit hyperactivity disorder and reading disorder: A comparativestudy. Journal of Child Psychology and Psychiatry, 48, 455–463.
Bergmann, J., & Wimmer, H. (2008). A dual-route perspective on poor reading in a regu-lar orthography: Evidence from phonological and orthographic lexical decisions. CognitiveNeuropsychology, 25, 653–676.
Bledsoe, J., Semrud-Clikeman, M., & Pliszka, S. R. (2009). A magnetic resonance imaging studyof the cerebellar vermis in chronically treated and treatment-naïve children with attention-deficit/hyperactivity disorder combined type. Biological Psychiatry, 65, 620–624.
Brizzolara, D., Chilosi, A., Cipriani, P., DiFilippo, G., Gasperini, F., Mazzotti, S., et al. (2006). Dophonologic and rapid automatized naming deficits differentially affect dyslexic children withand without a history of language delay: A study of Italian dyslexic children. Cognitive andBehavioral Neurology, 19, 141–149.
Caravolas, M. (2006). The foundations of literacy in Czech: Not so different from English afterall? Paper presented at the 11th annual conference of the Society for the Scientific Studiesof Reading, Vancouver, Canada.
Coltheart, M., Rastle, K., Perry, C., Langdon, R., & Ziegler, J. C. (2001). DRC: A dual route cascadedmodel of visual word recognition and reading aloud. Psychological Review, 108, 204–256.
Corpus Gesproken Nederlands [CGN; Corpus Spoken Dutch]. (2004). Versie 1.0 NederlandseTaalunie.
De Jong, P. F., & Van der Leij, A. (2003). Developmental changes in the manifestations of a phono-logical deficit in dyslexic children learning to read a regular orthography. Journal of EducationalPsychology, 95, 22–40.
De Luca, M., Barca, L., Burani, C., & Zoccolotti, P. (2008). The effect of word length and other sub-lexical, lexical, and semantic variables on developmental reading deficits. Cognitive BehavioralNeurology, 21, 227–235.
Del’Homme, M., Kim, T. S., Loo, S. K., Yang, M. H., & Smalley, S. L. (2007). Familial associationand frequency of learning disabilities in ADHD sibling pair families. Journal of Abnormal ChildPsychology, 35, 55–62.
Denckla, M. B. (1973). Colour-naming in dyslexic boys. Cortex, 8, 164–176.Ferdinand, R. F., Van der Ende, J., & Mesman, J. (1998). Diagnostic Interview Schedule for
Children, DISC-IV. Nederlandse Vertaling [Dutch Translation]. Unpublished manuscript.Sophia Kinderziekenhuis, Rotterdam, The Netherlands.
Georgiou, G. K., Parrila, R., & Kirby, J. R. (2009). RAN components and reading development fromGrade 3 to 5: What underlies their relationship? Scientific Studies of Reading, 13, 508–534.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

482 C. G. W. DE JONG ET AL.
Georgiou, G. K., Parrila, R., Kirby, J. P., & Stephenson, K. (2008). Rapid naming components andtheir relationship with phonological awareness, orthographic knowledge, speed of processing,and different reading outcomes. Scientific Studies of Reading, 12, 325–350.
Groth-Marnat, G. (1997). Handbook of Psychological Assessment (3rd ed.). New York, NY: JohnWiley and Sons.
Hawelka, S., Gagl, B., & Wimmer, H. (2010). A dual-route perspective on eye movements of dyslexicreaders. Cortex, 115, 367–379.
Juphard, A., Carbonnel, S., & Valdois, S. (2004). Length effect in reading and lexical decision:Evidence from skilled readers and a developmental dyslexic participant. Brain and Cognition,55, 332–340.
Kibby, M. Y., Kroese, J. M., Krebbs, H., Hill, C. E., & Hynd, G. W. (2009). The pars triangularis indyslexia and ADHD: A comprehensive approach. Brain and Language, 111, 46–54.
Kort, W., Compaan, E. L., Bleichrodt, N., Resing, W. C. M., Schittekatte, M., Bosman, M., et al.(2002). WISC-III (Dutch translation of the Wechsler Intelligence Scales for Children, 3rd ed.).Amsterdam, The Netherlands: NDC/NIP.
Li, H., Shu, H., McBride-Chang, C., Liu, H. Y., & Xue, J. (2009). Paired associate learning in Chinesechildren with dyslexia. Journal of Experimental Child Psychology, 103, 135–151.
MacMillan, N. A., & Creelman, C. D. (1991). Signal detection theory: A user’s guide. Cambridge:Cambridge University Press.
Martens, V. E. G., & De Jong, P. F. (2006). The effect of word length on lexical decision in dyslexicand normal reading children. Brain and Language, 98, 140–149.
Martinussen, R., Hayden, J., Hogg-Johnson, S., & Tannock, R. (2005). A meta-analysis of WM withattention-deficit/hyperactivity disorder. Journal of American Academy of Child and AdolescentPsychiatry, 44, 377–384.
Milne, R. D., Nicholson, T., & Corballis, M. C. (2003). Lexical access and phonological decoding inadult dyslexic subtypes. Neuropsychology, 17, 362–368.
Moll, K., Fussenegger, B., Willburger, E., & Landerl, K. (2009). RAN is not a measure of ortho-graphic processing: Evidence from the asymmetric German orthography. Scientific Studies ofReading, 13, 1–25.
Nicholson, R. I., Fawcett, A. J., & Dean, P. (2001). Developmental dyslexia: The cerebellar deficithypothesis. TRENDS in Neurosciences, 24, 508–511.
Oosterlaan, J., Scheres, A., Antrop, I., Roeyers, H., & Sergeant, J. A. (2001). Vragenlijst voorGedragsproblemen bij Kinderen (VvGK): Nederlandse Bewerking van de Disruptive BehaviourRating Scale [Disruptive Behaviour Disorders Rating Scale]. Lisse, The Netherlands: HarcourtTest.
Pennington, B. F., Groisser, D., & Welsh, M. C. (1993). Contrasting cognitive deficits in atten-tion deficit hyperactivity disorder versus reading disability. Developmental Psychology, 29,511–523.
Purvis, K. L., & Tannock, R. (2000). Phonological processing, not inhibitory control, differenti-ates ADHD and reading disability. Journal of the American Academy of Child and AdolescentPsychiatry, 39, 485–494.
Raberger, T., & Wimmer, H. (2003). On the automaticity/cerebellar deficit hypothesis of dyslexia:Balancing and continuous rapid naming in dyslexic and ADHD children. Neuropsychologia, 41,1493–1497.
Rucklidge, J. J., & Tannock, R. (2002). Neuropsychological profiles of adolescents with ADHD:Effects of reading difficulties and gender. Journal of Child Psychology and Psychiatry, 43,988–1003.
Schwab-Stone, M. E., Shaffer, D., Dulcan, M. K., Jensen, P. S., Fisher, P., Bird, H. R., et al. (1996).Criterion validity of the NIMH Diagnostic Interview Schedule for Children Version 2.3 (DISC-2.3). Journal of the American Academy of Child and Adolescent Psychiatry, 35, 878–888.
Semrud-Clikeman, M., Biederman, J., Sprich-Buckmeister, S., Lehman, B. A., Faraone, S. V., &Norman, D. (1992). Comorbidity between ADHD and LD: A review and report in clinically
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

RD AND ADHD FROM A DUAL ROUTE PERSPECTIVE 483
referred sample. Journal of American Academy of Child and Adolescent Psychiatry, 31,439–448.
Semrud-Clikeman, M., Guy, K., Griffin, J. D., & Hynd, G. W. (2000). Rapid naming deficits inchildren and adolescents with reading disabilities and attention deficit hyperactivity disorder.Brain and Language, 74, 70–83.
Shaffer, D., Fisher, P., Lucas, C. P., Dulcan, M. K., & Schwab-Stone, M. E. (2000). NIMH DiagnosticInterview Schedule for Children Version IV (NIMH DISC-IV): Description, differences fromprevious versions, and reliability of some common diagnoses. Journal of the American Academyof Child and Adolescent Psychiatry, 39, 28–38.
Shanahan, M. A., Pennington, B. F., Yerys, B. E., Scott, A., Boada, R., Willcutt, E. G., et al. (2006).Processing speed deficits in attention deficit/hyperactivity disorder and reading disability.Journal of Abnormal Child Psychology, 34, 585–602.
Struiksma, A. J. C., Van der Leij, A., & Vieijra, J. P. M. (2004). Diagnostiek van technisch lezenen aanvankelijk spellen [Diagnostics of technical reading and spelling]. Amsterdam, TheNetherlands: VU Boekhandel/ Uitgeverij B.V (VU University press).
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics (5th ed.). Boston, MA: Allynand Bacon.
Tannock, R., Martinussen, R., & Frijters, J. (2000). Naming speed performance and stimulanteffects indicate effortful, semantic processing deficits in attention-deficit hyperactivity disorder.Journal of Abnormal Child Psychology, 28, 237–252.
Vaidya, C. J., & Stollstorff, M. (2008). Cognitive neuroscience of attention deficit hyperactivity dis-order: Current status and working hypotheses. Developmental Disabilities Research Reviews,14, 261–267.
Van de Voorde, S., Roeyers, H., Verté, S., & Wiersema, J. R. (2010). Working memory, response inhi-bition, and within-subject variability in children with attention-deficit/hyperactivity disorder orreading disorder. Journal of Clinical and Experimental Neuropsychology, 14, 366–379.
Van den Bos, K. P. (1998). IQ, phonological awareness and continuous-naming speed related toDutch poor decoding children’s performance on two word identification tests. Dyslexia, 4,73–89.
Van der Schoot, M., Licht, R., Horsley, T. M., & Sergeant, J. A. (2000). Inhibitory deficits in readingdisability depend on subtype: Guessers but not spellers. Child Neuropsychology, 6, 297–312.
Verhoeven, L. (1995). Drie-minuten-toets [Three Minutes Test]. Arnhem, The Netherlands: CITO.Wechsler, D. (1991). Wechsler Intelligence Scale for Children (3rd ed.). San Antonio, TX: The
Psychological Corporation.Willcutt, E. G., Betjemann, R. S., McGrath, L. M., Chhabildas, N. A., Olson, R. K., DeFries, J. C.
et al. (2010). Etiology and neuropsychology of comorbidity between RD and ADHD: The casefor multiple-deficit models. Cortex, 46, 1345–1361.
Willcutt, E. G., Pennington, B. F., Olson, R. K., Chhabildas, N., & Hulslander, J.(2005). Neuropsychological analyses of comorbidity between reading disability andattention-deficit/hyperactivity disorder: In search of the common deficit. DevelopmentalNeuropsychology, 27, 35–78.
Wimmer, H. (1993). Characteristics of developmental dyslexia in a regular writing system. AppliedPsycholinguistics, 14, 1–33.
Wimmer, H., Mayringer, H., & Landerl, K. (1998). Poor reading: A deficit in skill automatization ora phonological deficit? Scientific Studies of Reading, 2, 321–340.
Wolf, M., & Bowers, G. P. (1999). The double deficit hypothesis for the developmental dyslexias.Journal of Educational Psychology, 91, 415–438.
Zoccolotti, P., de Luca, M., di Pace, E., Gasperini, F., Judica, A., & Spinelli, D. (2005). Word lengtheffect in early reading and in developmental dyslexia. Brain and Language, 93, 369–373.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

484 C. G. W. DE JONG ET AL.
APPENDIX A
Words: Orthographical Decision Task
Pseudohomophones ValidWords∗
Frequency EnglishTranslation∗
ValidWord
Frequency EnglishTranslation∗
bant band 222 ribbon baard 33 beardbeelt beeld 319 picture bank 284 couchblat blad 85 leave bleek 286 palebloet bloed 170 blood blik 199 canbreet breed 161 broad broer 308 brotherdoot dood 539 death doos 74 boxdraat draad 43 thread draak 15 dragonfaak vaak 1577 often gast 115 guestfast vast 867 solid graag 1078 readilyfies vies 124 dirty grauw 12 greyflet flat 68 flat groen 184 greenfuil vuil 30 dirt hond 247 doggelt geld 1433 money huid 101 skingijt geit 10 goat kaars 10 candlegragt gracht 19 canal kast 194 cupboardgreis grijs 62 grey klaar 690 readyhant hand 926 hand kont 33 bottomhaut hout 275 wood kous 7 stockinghont hond 247 dog kwaad 184 angryhuit huid 101 skin lang 1861 longkaard kaart 318 card leeg 166 emptykand kant 1266 lace licht 443 lightkaud koud 205 cold macht 139 powerklijn klein 806 small mand 42 basketkord kort 494 short meel 7 flourkweit kwijt 448 lost meid 73 maidenlant land 855 land naald 24 needleleew leeuw 15 lion naast 752 nextlugt lucht 320 sky niets 1000 nothingmeew meeuw 8 seagull nooit 2462 nevermont mond 307 mouth post 82 mailniews nieuws 277 news riem 20 beltnoort moord 64 murder rond 821 roundpund punt 728 point schot 49 shotrant rand 109 edge snoep 18 candyreik rijk 129 rich spuit 11 syringeront rond 821 round taal 362 languagesaak zaak 540 case tent 289 tentschad schat 74 treasure traan 15 tearseep zeep 26 soap vaas 35 vasesneew sneeuw 122 snow vals 39 falsespeit spijt 108 regret vier 2375 fourtant tand 12 tooth vlot 42 quicktauw touw 56 robe vraag 1399 questiontrijn trein 419 train vroeg 982 earlyvagt vacht 11 fur vuil 30 dirtveif vijf 1895 five zaag 4 saw
(Continued)
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

RD AND ADHD FROM A DUAL ROUTE PERSPECTIVE 485
APPENDIX A (Continued)
Pseudohomophones ValidWords∗
Frequency EnglishTranslation∗
ValidWord
Frequency EnglishTranslation ∗
vrauw vrouw 1055 woman zaal 123 roomzaat zaad 9 seed zeer 648 veryzagt zacht 109 soft zucht 66 sighPractice Itemseent eend 9 duck blind 38 blindflees vlees 181 meat boot 170 boatfork vork 21 fork eens 2406 agreementjeugt jeugd 140 youth flink 245 sturdymoort moord 64 murder juist 931 correctregts rechts 158 right kans 441 chancesgelp schlep 2 shell koord 11 cordsorg zorg 259 sorrow nicht 16 niecesgool school 1171 school slaaf 14 slavetrem tram 34 tramway straf 80 punishmentvend vent 116 fellow vest 13 vestvilm film 442 film zwaar 289 heavyzant zand 72 sand
∗Words in italics are not in the task but are mentioned for clarification purposes.
Words: Phonological Decision Task
Nonwords Pseudohomophones Valid Word∗ Frequency EnglishTranslation
begun beerun beren 5 bearsbekkur bakkur bakker 53 bakerbissun binnun binnen 1631 indoorsbortun bogtun bochten 11 curvesbuidun buitun buiten 939 outdoorsdaapun daagun dagen 930 daysdeefun deelun delen 184 to sharedoldur dogtur dochter 226 daughterfaudun fautun fouten 80 mistakesgaalun gaatun gaten 222 holesgeetun geefun geven 1397 to givehaadun haafun haven 76 harborhaapun haalun halen 810 to getheutel heuful heuvel 39 hilljaalun jaagun jagen 34 to huntkaagur kaamur kamer 551 roomkoepun koejun koeien 111 cowskoogun koopun kopen 579 to buylaamun laakun laken 15 sheetmaafun maakun maken 3137 to makemiggun middun midden 345 midstmoelur moedur moeder 1417 mother
(Continued)
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4

486 C. G. W. DE JONG ET AL.
APPENDIX A (Continued)
Nonwords Pseudohomophones Valid Word∗ Frequency EnglishTranslation
moonun moogun mogen 649 to allowmorpun morgun morgen 1048 tomorrowneerul naagul nagel 3 nailnoepun noemun noemen 483 to namenuffer nummur nummer 366 numberpangur pantur panter 2 pantherpoetur poedur poeder 7 powderpoonun pootun poten 45 legsraatun raadun raden 46 to guessraagun raakun raken 135 to hitsaarun saamun samen 887 togethersoedul soepul soepel 19 leantaagul taaful tafel 454 tabletukkel tunnul tunnel 48 tunnelvaatur vaadur vader 1182 fathervaapun vaarun varen 45 sailveisur veifur vijfer 27 pondvoenen voelun voelen 184 to feelvorgun volgun volgen 222 to followwaamun waagun wagen 79 carwaffur wakkur wakker 225 awakeweedun weetun weten 1717 to knowwindur wintur winter 98 winterzaanun zaakun zaken 544 businesszijtun zijlun zeilen 68 to sailzildur zilfur zilver 37 silverPractice Itemsbegun bauwun bouwen 254 to buildbuuwun buurun buren 107 neighborsdeefun deelun delen 184 to sharegeegul geefun geven 1397 to givehaakur haalun halen 810 to gethaldur heldur helder 119 clearhoogun hollun hollen 15 to runjaamun jammur jammer 544 pitykaggun kaggul kachel 43 stovekoepun koejun koeien 111 cowsmoelur moedur moeder 1417 mothermiggun moogun mogen 649 to allowmorpun morgun morgen 1048 tomorrownandun nagtun nachten 46 nightspeikun peilun pijlen 7 arrowspoonun pootun poten 45 legsrokkul rommul rommel 24 messsoedul soepul soepel 19 flexibletukkel tunnul tunnel 48 tunnelvagtug vogtug vochtig 30 moistvoenen volgun volgen 222 to followvorgun voogul vogel 53 birdweekul weetun weten 1717 to knowwoopun woonun wonen 471 to livezaanun zaakun zaken 544 business
∗Words in italics are not in the task but are mentioned for clarification purposes.
Dow
nloa
ded
by [
DU
T L
ibra
ry]
at 1
5:18
04
Oct
ober
201
4