Embed Size (px)
Citation preview
Raul Zini
Hip arthroscopyPresentation by
Thomas Byrd
Argalìa Editore Urbino
Raul Zini
Hip arthroscopyPresentation by
J. W. Thomas Byrd
Argalìa Editore Urbino
ISBN 978-88-89731-29-1
Copyright © 2010 Edizioni Argalìa Editore, Urbino.
Printed by Arti Grafiche Editoriali Srl, Urbino.
All rights reserved.

FOREWORD pag. 7R. Zini
PRESENTATION 9T. Byrd
GENERAL PRINCIPLES AND ARTHROSCOPIC TECNIQUEANATOMY OF THE FEMORAL HEAD AND NECK AND RELATED STRUCTURES, AND ANATOMICAL RISKS IN HIP ARTHROSCOPY 13
I. Saenz – O. FarinasDIFFERENTIAL DIAGNOSIS OF A PAINFUL HIP 23
F. Randelli – L. BanciARTHROSCOPIC ANATOMY OF THE HIP JOINT 43
V. Ilizaliturri – A. Tomic LoftkjaerTHE SUPINE POSITION 55
T. ByrdPERSONAL TECHNIQUE: MODIFIED SUPINE POSITION 71
R. Zini – G. PonzettoLATERAL POSITION ARTHROSCOPIC TECHNIQUE 77
A. FontanaINDICATIONS 83
R. Zini – A. Carraro – M. De BenedettoCOMPLICATIONS AND CONTRAINDICATIONS OF HIP ARTHROSCOPY 117
M. Bigoni – S. GuerrasioREHABILITATION AFTER HIP ARTHROSCOPY 131
S. Della Villa – K. Tsapralis – A. Salsi
SURGICAL TECHNIQUESSYNOVIAL AND CHONDRAL DISEASE: THE ROLE OF HIP ARTHROSCOPY 147
R. Buly – L. MoyaACETABULAR LABRUM TEARS 163
N. SantoriTRAUMATOLOGY 177
R. Zini – P. Pirani – M. Occhialini
FEMORO-ACETABULAR IMPINGEMENT- FEMORO-ACETABULAR IMPINGEMENT:
A CLINICAL AND DIAGNOSTIC CLASSIFICATION 185E. Sabetta – C. Ferraù
- ARTHROSCOPIC MANAGEMENT OF FEMORO-ACETABULAR IMPINGEMENT (FAI) 197T. Byrd – K. Jones
3
Index
4
Index
- ARTHROSCOPIC TREATMENT OF FEMORO-ACETABULAR IMPINGEMENT 211M. Philippon – C. Hay – K. Briggs – M. Schenker
- HIP ARTHROSCOPY FOR FEMORO-ACETABULAR IMPINGEMENT: PERSONAL TECHNIQUE AND INDICATIONS 223M. Leunig – N. Mondanelli – M. Kain
THE PERITROCHANTERIC COMPARTMENT 249B. T. Kelly – T. Maak – M. Cross – P. Fabricant
EDITOR
Raul Zini M.D.Orthopaedic SurgeonScientific Director Orthopaedic Department Maria Ceciclia HospitalGVM Care&Research Cotignola (RA), Italy
CONTRIBUTORS
Marco Bigoni, M.D.Attending Orthopaedic Surgeon,Academic Researcher,Clinica Ortopedica Università degli Studi di Milano-BicoccaAzienda Ospedaliera San Gerardo, Monza (Mb) Italy
Robert L. Buly, M.DAssistant Professor of Orthopaedic SurgeryTotal Joint Replacement and Adult Orthopaedic Sur-geryHospital for Special SurgeryNew York, USA
J. W. Thomas Byrd, M.D.Orthopaedic SurgeonNashville Sports Medicine FoundationNashville, Tennessee, USA
Stefano Della Villa, M.D.PhysiatristEducation and Research Department, Isokinetic Medical Group, Bologna, Italy
Andrea Fontana, M.D.Consultant Orthopaedic SurgeonIstituto Clinico San Siro Hip and Knee UnitMilan - ItalyConsultan Orthopaedic Surgeon Istituti Clinici Riz-zoli - Bologna Consultan Orthopaetic Surgeon University of Turin– Turin
Victor M. Ilizaliturri Jr., M.D.Professor of Hip and Knee Surgery, Universidad Na-cional Autónoma de México.Chief of Hip and Knee Surgery, National Rehabilita-tion Institute of Mexico.Mexico City Mexico.
Bryan T. Kelly, M.D.Assistant Attending, Orthopaedic Surgery, Hospitalfor Special SurgeryAssistant Professor, Orthopaedic Surgery, New YorkPresbyterian Hospital, Weill Medical College ofCornell UniversityCo-Director, Center for Hip Pain and Preservation,Hospital for Special Surgery New York, USA
Michael Leunig, M.D.Head of OrthopaedicsOrthopaedicsSchulthes ClinicZürichLower extremitiesZürich, Switzerland
Marc J. Philippon, M.D.Orthopaedic SurgeonSteadman Hawkins ClinicVail Co USA
Filippo Randelli, M.D.Orthopaedic SurgeonHip DepartmentIRCCS Policlinico San Donato San Donato Milanese (MI) – Italy
Ettore Sabetta, M.D.Director of Orthopaedic DepartmentAzienda Ospedaliera Reggio EmiliaArcispedale Santa Maria Nuova - Reggio Emilia -Italy
Ivan Saenz, M.D.Assistant professorHuman Anatomy and Embriology DepartmentFaculty of MedicineUniversity of BarcelonaOrthopedic SurgeonEmergency UnitHospital Espiritu Santo, Santa Coloma de GramanetBarcelona Spain
Nicola Santori, M.D.Orthopedic SurgeonRome American Hospital – Rome – Italy
CO-AUTHORS
Lorenzo BanciBiomedical Engineer Hip Department IRCCS Policlinico San Donato San Donato Milanese (MI), Italy
Karen K. Briggs, MPHSteadman Hawkins Research FoundationVail, CO USA
Andrea Carraro M.D.Orthopaedic SurgeonMaria Ceciclia HospitalGVM Care&Research Cotignola (RA), Italy
Michael B. Cross, M.D. Orthopaedic SurgeonCenter for Hip Pain and Preservation, Hospital for Spe-cial Surgery, New York, USA
Massimo De Benedetto M.D.Orthopaedic SurgeonMaria Ceciclia HospitalGVM Care&Research Cotignola (RA), Italy
Peter D. Fabrikant, M.D.Orthopaedic SurgeonCenter for Hip Pain and Preservation, Hospital for Spe-cial Surgery, New York, USA
Oscar Farinas, MDAssistant professorHuman Anatomy and Embriology DepartmentFaculty of MedicineUniversity of BarcelonaBarcelona Spain
Claudio Ferraù M.D.Orthopaedic SurgeonAzienda Ospedaliera Reggio EmiliaArcispedale Santa Maria NuovaReggio Emilia Italy
Stefano Guerrasio M.D.Orthopaedic SurgeonClinica Ortopedica Università degli Studi di Milano-Bic-occaAzienda Ospedaliera San Gerardo, Monza (MB) Italy
Kay S. Jones, M.S.N., R.NNashville Sports Medicine FoundationNashville, TN, USA
Connor J. Hay, BASteadman Hawkins Research FoundationVail, CO USA
Michael SH Kain M.D.MEMNA European Travelling Fellow Schulthess Klinik Zurich Switzerland
Alexander Tomic Loftkjaer MDFellow of Hip surgery at the National Rehabilitation Institute of Mexico.Mexico City Mexico
Travis G. Maak, M.D. Orthopaedic SurgeonCenter for Hip Pain and Preservation, Hospital for Spe-cial Surgery, New York, USA
Nicola Mondanelli, M.D.Consultant Orthopaedic SurgeonDepartment of Orthopaedics and TraumatologyAzienda Ospedaliero-Universitaria di CareggiFLORENCE Italy
Luis E. Moya, MDHospital for Special SurgeryNew York, USA
Marcello Occhialini M.D.Orthopaedic SurgeonMaria Ceciclia HospitalGVM Care&Research Cotignola (RA), Italy
Piergiorgio Pirani M.D.Orthopaedic SurgeonMaria Ceciclia HospitalGVM Care&Research Cotignola (RA), Italy
Giorgio Ponzetto M.D.Orthopaedic SurgeonMaria Ceciclia HospitalGVM Care&Research Cotignola (RA), Italy
Alessandro Salsi, PTPhysiotherapistEducation and Research Department, Isokinetic MedicalGroup, Bologna, Italy
Mara L. Schenker, MDSteadman Hawkins Research FoundationVail, CO, USA
Kyryakos Tsapralis, M.D.Sports PhysicianEducation and Research Department, Isokinetic MedicalGroup, Bologna, Italy

At present, hip arthroscopy arouses a very considerable interest and it is one of the great orthopaedic surgery’sinnovations of recent years. Hip has been the last joint in which traditional surgery has been called into question in favour of arthroscopicsurgery. It has not been a fast development and, until a few years ago, hip arthroscopy was considered a nichesurgery performed by just a few arthroscopists interested in discovering new opportunities and experimentingnew surgical techniques.The delay in the developing of hip arthroscopy, compared to other joints, is probably due to the fact that thisjoint is “anatomically” hard to deal with in arthroscopy and therefore requires a long learning curve even forskilful arthroscopists.As happened in the past with other joints, hip arthroscopy has been fundamental to know the hip in a differentway, to evaluate it from within, to better understand its complexity and to revaluate some important anatomicalstructures such as the acetabular labrum.I started my approach to hip arthroscopy at the beginning of the nineties after a visit in Cambridge toRichard Villar, who at the moment was the greatest expert in Europe. My interest was based on an innate cu-riosity for arthroscopic methodologies and the intuition that also hip arthroscopy could have a great not yetexplored potential; a good experience achieved in the arthroscopic surgery of other joints allowed me to havea not too complex approach to hip arthroscopy and therefore contributed to increase my interest and mypersonal casistic.My experience grew out of my business trips that turned to be fundamental since they gave me the chance tovisit and get to know some of the best hip arthroscopists of the world, like James Glick, Robert Buly, MichaelDienst, Thomas Byrd, Marc Philippon and Michael LeunigHip arthroscopy is now a reality also in Italy; it is routinely performed in several hospitals and many or-thopaedic surgeons have approached it enthusiastically.My wish to contribute to a further diffusion of this arthroscopic technique arises from all these considerations.I therefore decided to issue the first hip arthroscopy Italian book with the aim to gather in one volume all thelatest notions of general techniques and the more specific surgical methodologies.I think that the scientific cooperation both with great international and Italian experts, whom I sincerely thankfor having given their very important contribution, allows to well-define the present state of the art and the fu-ture fields of action of hip arthroscopy.I do hope that this volume will be interesting for those who already perform hip arthroscopy, but most of all forthose young orthopaedics who are interested in and want to investigate it thoroughly.A special thanks go to Thomas Byrd, who did me the honour of writing the introduction to this volume and topersonally present it during one of his masterly done lesson at the recent congress of the Italian Society ofArthroscopy.A due sincere thanks go to Smith&Nephew for the important contribution given to the publication of the vol-ume.My friend Gianluca Ruffi, who supported me in a fundamental way with his great expertise in dealing with for-eign authors, deserves my special gratitude.A last thanks go to my friends and team members, Giorgio Ponzetto, MD, Piergiorgio Pirani, MD, MarcelloOcchialini, MD, Andrea Carraro, MD and Massimo De Benedetto, who assisted me in selecting and filing theiconographic material and in the publication of this volume.
RAUL ZINI
Foreword


Hip arthroscopy has been an established technique for 20 years. However, the clinical applications of thisprocedure have grown exponentially within this decade. The technology has evolved from diagnostic to op-erative arthroscopy, beginning with simple resection techniques and now progressing to more sophisticatedrestorative procedures.The arthroscope has precipitated a better understanding of hip pathology and related disorders. We havemuch greater knowledge of the nature of labral tears, its healing capacity and methods of preservation. Vaststrides have been made in sorting out the etiology of hip disorders, such as the expanding understanding offemoroacetabular impingement, especially with its negative implications in young active adults. We also un-derstand how hip joint problems can lead to other secondary disorders such as athletic pubalgia and prob-lems of the lumbar spine.Professor Zini and his colleagues have put together a very timely text that reflects in detail on our currentknowledge of hip problems and indepth methods of treatment. The contributors offer valuable insight intothe developments in diagnostic methods and operative techniques. Pay close attention as this work will helpto guide you through the complexities of hip pathology that have been increasingly unveiled.
J.W. THOMAS BYRD
Presentation

General Principles and Arthroscopic Tecnique

The enarthrotic (ball-and-socket) hip or coxofemoral joint,which joins the leg to the pelvic girdle (thigh = coxa), is the mostperfect joint in the body.
It consists of the articular surfaces of the femoral head (spher-ical and convex) and the acetabulum or cotyloid cavity (sphericaland concave).
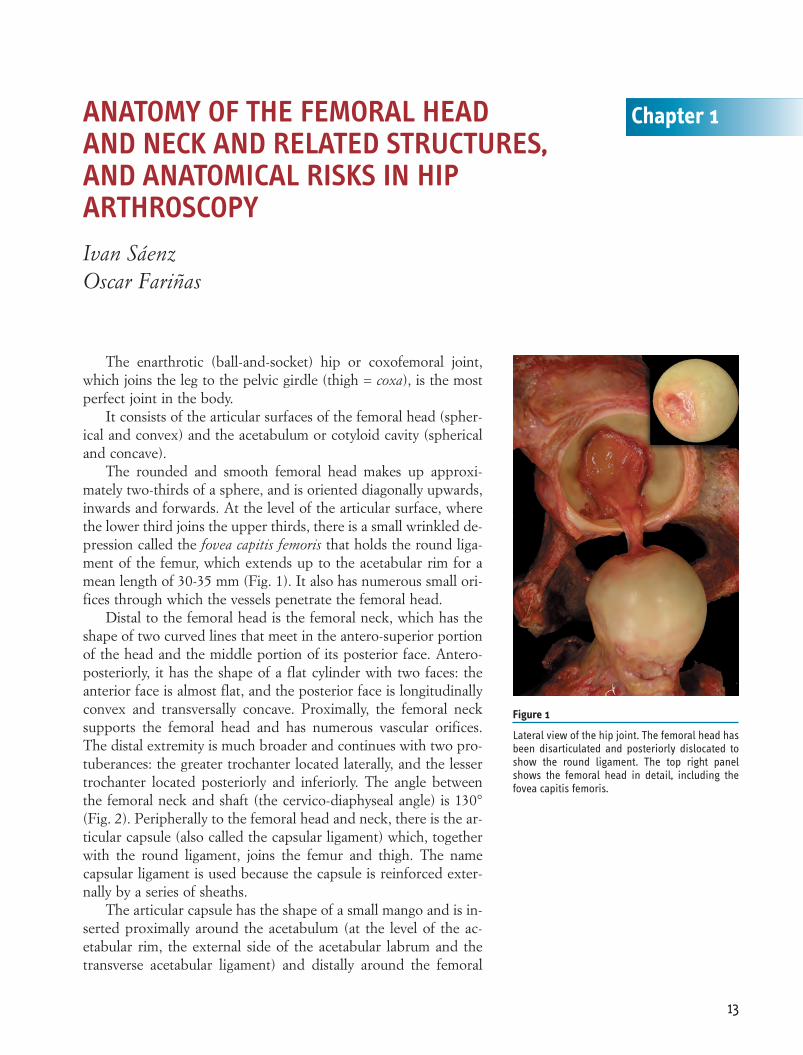
The rounded and smooth femoral head makes up approxi-mately two-thirds of a sphere, and is oriented diagonally upwards,inwards and forwards. At the level of the articular surface, wherethe lower third joins the upper thirds, there is a small wrinkled de-pression called the fovea capitis femoris that holds the round liga-ment of the femur, which extends up to the acetabular rim for amean length of 30-35 mm (Fig. 1). It also has numerous small ori-fices through which the vessels penetrate the femoral head.
Distal to the femoral head is the femoral neck, which has theshape of two curved lines that meet in the antero-superior portionof the head and the middle portion of its posterior face. Antero-posteriorly, it has the shape of a flat cylinder with two faces: theanterior face is almost flat, and the posterior face is longitudinallyconvex and transversally concave. Proximally, the femoral necksupports the femoral head and has numerous vascular orifices.The distal extremity is much broader and continues with two pro-tuberances: the greater trochanter located laterally, and the lessertrochanter located posteriorly and inferiorly. The angle betweenthe femoral neck and shaft (the cervico-diaphyseal angle) is 130°(Fig. 2). Peripherally to the femoral head and neck, there is the ar-ticular capsule (also called the capsular ligament) which, togetherwith the round ligament, joins the femur and thigh. The namecapsular ligament is used because the capsule is reinforced exter-nally by a series of sheaths.
The articular capsule has the shape of a small mango and is in-serted proximally around the acetabulum (at the level of the ac-etabular rim, the external side of the acetabular labrum and thetransverse acetabular ligament) and distally around the femoral
13
Chapter 1ANATOMY OF THE FEMORAL HEAD AND NECK AND RELATED STRUCTURES, AND ANATOMICAL RISKS IN HIP ARTHROSCOPY Ivan SáenzOscar Fariñas
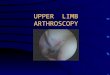
Figure 1
Lateral view of the hip joint. The femoral head hasbeen disarticulated and posteriorly dislocated toshow the round ligament. The top right panelshows the femoral head in detail, including thefovea capitis femoris.
neck (Fig. 3). The distal insertion of this articular capsule meritsattention because of its numerous surgical implications:
– Anteriorly, the capsule has a strong insertion at the level of theoblique line of the femur (a rough line that laterally joins theanterior edge of the greater trochanter with the lessertrochanter).
– Posteriorly, it is inserted at the level of the femoral neck intothe point of union between its external third and its two inter-nal thirds. It is therefore asymmetrical in relation to the ante-rior capsule in terms of the points of insertion and because theinsertion is very loose.
– Superiorly, it is inserted into an oblique line which joins thelines of anterior and posterior insertion.
– Inferiorly, it is inserted into the oblique line going to the lineof the back insertion passing through the top of the lessertrochanter.
The capsule has two classes of fibres: longitudinal and circular.The longidtudinal fibres are located superficially in a superior-in-ferior direction, cross the circular fibres, and merge with the cap-sular reinforcement ligaments. The circular fibres occupy the deepplane of the capsule and lie perpendicularly to the axis of the
14
Chapter 1
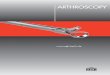
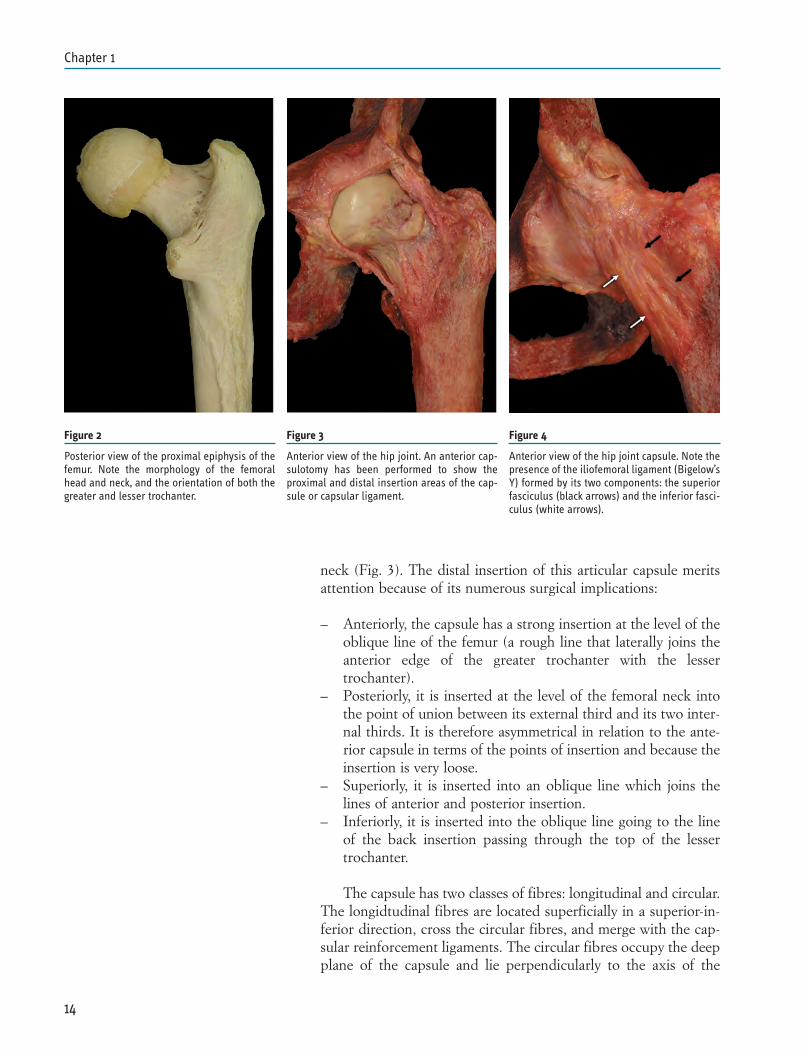
Figure 2
Posterior view of the proximal epiphysis of thefemur. Note the morphology of the femoralhead and neck, and the orientation of both thegreater and lesser trochanter.
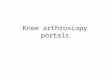
Figure 3
Anterior view of the hip joint. An anterior cap-sulotomy has been performed to show theproximal and distal insertion areas of the cap-sule or capsular ligament.
Figure 4
Anterior view of the hip joint capsule. Note thepresence of the iliofemoral ligament (Bigelow’sY) formed by its two components: the superiorfasciculus (black arrows) and the inferior fasci-culus (white arrows).
femoral neck; they are particularly visible in the posterior and in-ferior parts of the joint.
The capsular reinforcement ligaments are the iliofemoral, is-chiofemoral and arcuate ligaments.
1.- The iliofemoral ligament, also called the Y-ligament or lig-ament of Bigelow, originates between the antero-inferior iliacspine (below the tendon of the anterior rectus muscle of the thigh)and the acetabular rim (Fig. 4). During its descending course, itsfibres, which unfold like a fan, divide into two bands or fasciculi(superior and inferior): the superior fasciculus (iliopretro -chanteric) is inserted into the proximal part of the anterior in-tertrochanteric line (just below the tendon of the gluteus mimimusmuscle) and limits abduction and external rotation; the inferiorfasciculus (iliopretrochanteric) is inserted into the same area but isdistally thinner than the superior fasciculus, although its strengthis similar.
The function of the iliofemoral ligament is to limit the exten-sion of the hip, thus making it possible to remain standing withoutthe need for muscular action. It is the strongest of the ligamentsreinforcing the joint capsule of the hip.
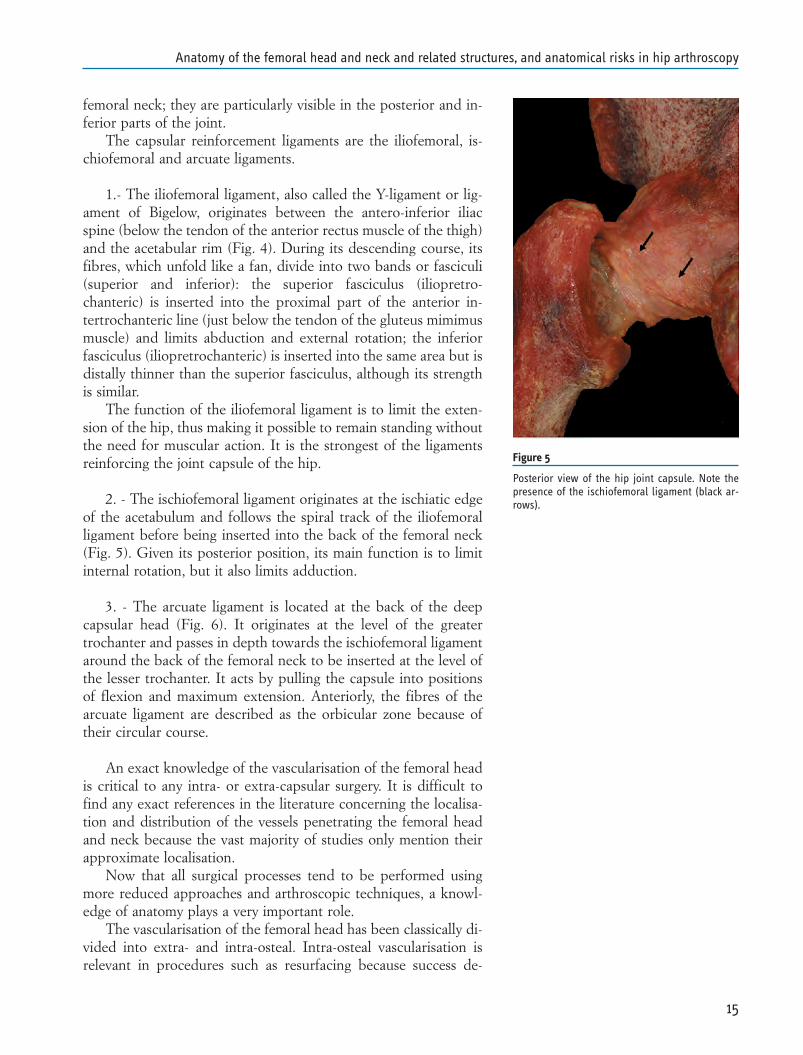
2. - The ischiofemoral ligament originates at the ischiatic edgeof the acetabulum and follows the spiral track of the iliofemoralligament before being inserted into the back of the femoral neck(Fig. 5). Given its posterior position, its main function is to limitinternal rotation, but it also limits adduction.
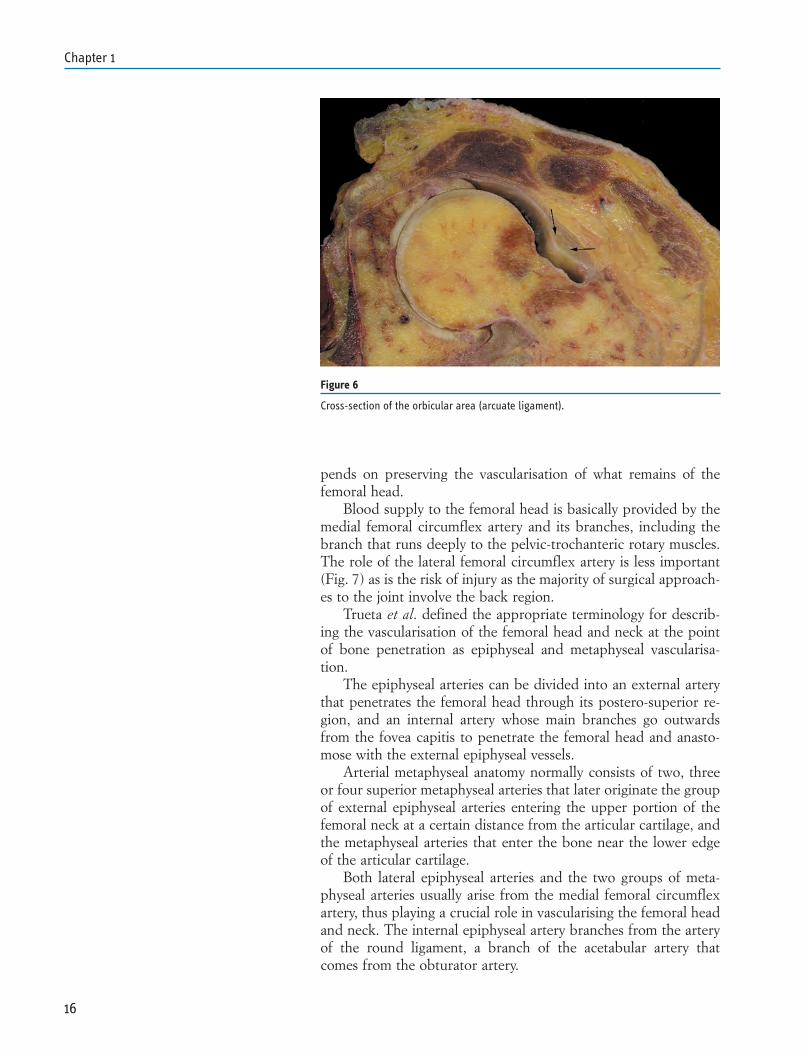
3. - The arcuate ligament is located at the back of the deepcapsular head (Fig. 6). It originates at the level of the greatertrochanter and passes in depth towards the ischiofemoral ligamentaround the back of the femoral neck to be inserted at the level ofthe lesser trochanter. It acts by pulling the capsule into positionsof flexion and maximum extension. Anteriorly, the fibres of thearcuate ligament are described as the orbicular zone because oftheir circular course.
An exact knowledge of the vascularisation of the femoral headis critical to any intra- or extra-capsular surgery. It is difficult tofind any exact references in the literature concerning the localisa-tion and distribution of the vessels penetrating the femoral headand neck because the vast majority of studies only mention theirapproximate localisation.
Now that all surgical processes tend to be performed usingmore reduced approaches and arthroscopic techniques, a knowl-edge of anatomy plays a very important role.
The vascularisation of the femoral head has been classically di-vided into extra- and intra-osteal. Intra-osteal vascularisation isrelevant in procedures such as resurfacing because success de-
15
Anatomy of the femoral head and neck and related structures, and anatomical risks in hip arthroscopy
Figure 5
Posterior view of the hip joint capsule. Note thepresence of the ischiofemoral ligament (black ar-rows).
pends on preserving the vascularisation of what remains of thefemoral head.
Blood supply to the femoral head is basically provided by themedial femoral circumflex artery and its branches, including thebranch that runs deeply to the pelvic-trochanteric rotary muscles.The role of the lateral femoral circumflex artery is less important(Fig. 7) as is the risk of injury as the majority of surgical approach-es to the joint involve the back region.
Trueta et al. defined the appropriate terminology for describ-ing the vascularisation of the femoral head and neck at the pointof bone penetration as epiphyseal and metaphyseal vascularisa-tion.
The epiphyseal arteries can be divided into an external arterythat penetrates the femoral head through its postero-superior re-gion, and an internal artery whose main branches go outwardsfrom the fovea capitis to penetrate the femoral head and anasto-mose with the external epiphyseal vessels.
Arterial metaphyseal anatomy normally consists of two, threeor four superior metaphyseal arteries that later originate the groupof external epiphyseal arteries entering the upper portion of thefemoral neck at a certain distance from the articular cartilage, andthe metaphyseal arteries that enter the bone near the lower edgeof the articular cartilage.
Both lateral epiphyseal arteries and the two groups of meta-physeal arteries usually arise from the medial femoral circumflexartery, thus playing a crucial role in vascularising the femoral headand neck. The internal epiphyseal artery branches from the arteryof the round ligament, a branch of the acetabular artery thatcomes from the obturator artery.
16
Chapter 1
Figure 6
Cross-section of the orbicular area (arcuate ligament).
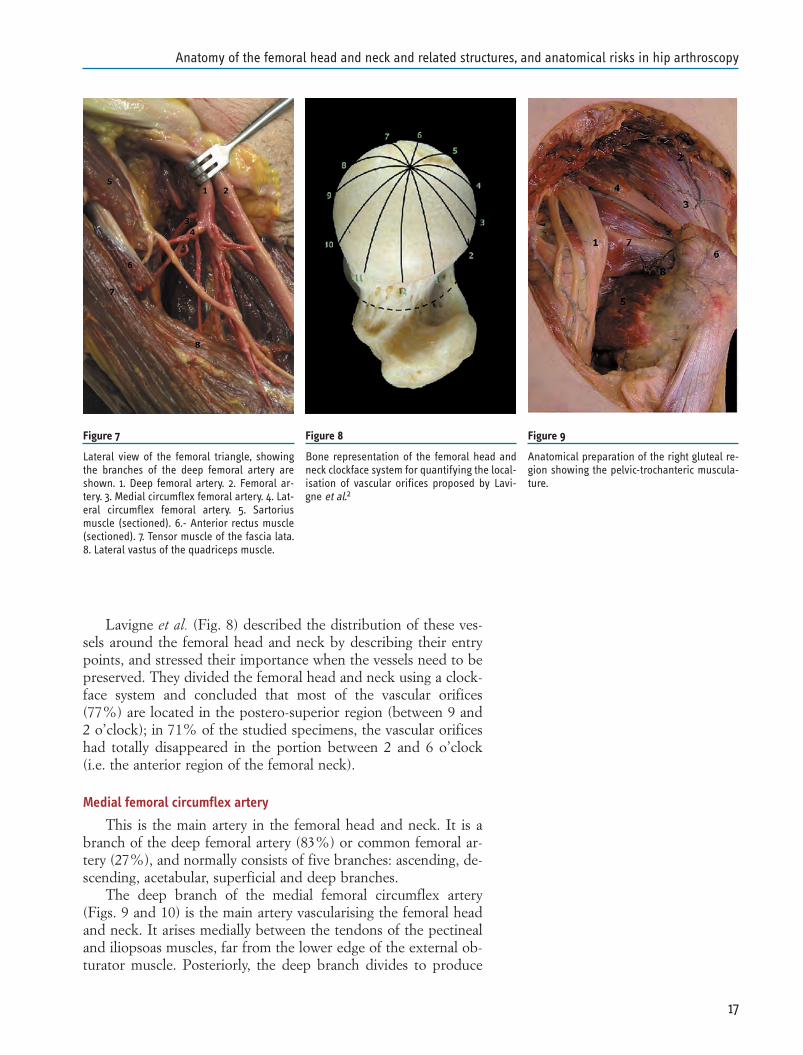
Lavigne et al. (Fig. 8) described the distribution of these ves-sels around the femoral head and neck by describing their entrypoints, and stressed their importance when the vessels need to bepreserved. They divided the femoral head and neck using a clock-face system and concluded that most of the vascular orifices(77%) are located in the postero-superior region (between 9 and2 o’clock); in 71% of the studied specimens, the vascular orificeshad totally disappeared in the portion between 2 and 6 o’clock(i.e. the anterior region of the femoral neck).
Medial femoral circumflex artery
This is the main artery in the femoral head and neck. It is abranch of the deep femoral artery (83%) or common femoral ar-tery (27%), and normally consists of five branches: ascending, de-scending, acetabular, superficial and deep branches.
The deep branch of the medial femoral circumflex artery(Figs. 9 and 10) is the main artery vascularising the femoral headand neck. It arises medially between the tendons of the pectinealand iliopsoas muscles, far from the lower edge of the external ob-turator muscle. Posteriorly, the deep branch divides to produce
17
Anatomy of the femoral head and neck and related structures, and anatomical risks in hip arthroscopy
Figure 7
Lateral view of the femoral triangle, showingthe branches of the deep femoral artery areshown. 1. Deep femoral artery. 2. Femoral ar-tery. 3. Medial circumflex femoral artery. 4. Lat-eral circumflex femoral artery. 5. Sartoriusmuscle (sectioned). 6.- Anterior rectus muscle(sectioned). 7. Tensor muscle of the fascia lata.8. Lateral vastus of the quadriceps muscle.
Figure 8
Bone representation of the femoral head andneck clockface system for quantifying the local-isation of vascular orifices proposed by Lavi-gne et al.2
Figure 9
Anatomical preparation of the right gluteal re-gion showing the pelvic-trochanteric muscula-ture.
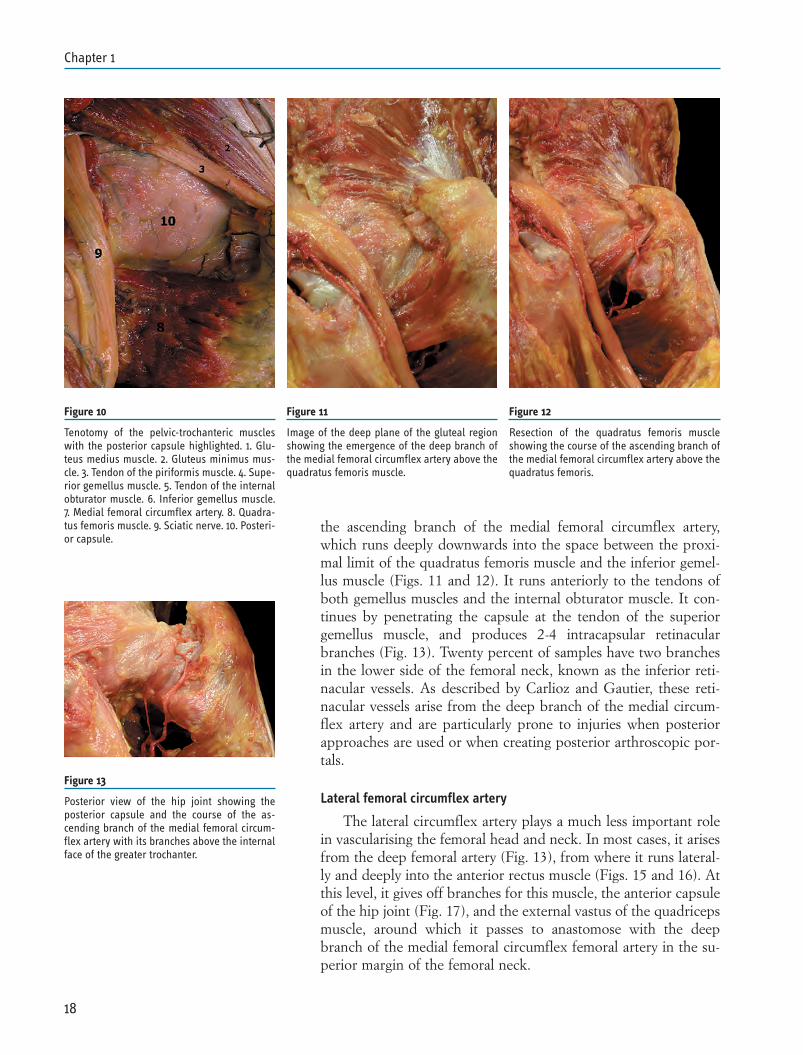
the ascending branch of the medial femoral circumflex artery,which runs deeply downwards into the space between the proxi-mal limit of the quadratus femoris muscle and the inferior gemel-lus muscle (Figs. 11 and 12). It runs anteriorly to the tendons ofboth gemellus muscles and the internal obturator muscle. It con-tinues by penetrating the capsule at the tendon of the superiorgemellus muscle, and produces 2-4 intracapsular retinacularbranches (Fig. 13). Twenty percent of samples have two branchesin the lower side of the femoral neck, known as the inferior reti-nacular vessels. As described by Carlioz and Gautier, these reti-nacular vessels arise from the deep branch of the medial circum-flex artery and are particularly prone to injuries when posteriorapproaches are used or when creating posterior arthroscopic por-tals.
Lateral femoral circumflex artery
The lateral circumflex artery plays a much less important rolein vascularising the femoral head and neck. In most cases, it arisesfrom the deep femoral artery (Fig. 13), from where it runs lateral-ly and deeply into the anterior rectus muscle (Figs. 15 and 16). Atthis level, it gives off branches for this muscle, the anterior capsuleof the hip joint (Fig. 17), and the external vastus of the quadricepsmuscle, around which it passes to anastomose with the deepbranch of the medial femoral circumflex femoral artery in the su-perior margin of the femoral neck.
18
Chapter 1
Figure 10
Tenotomy of the pelvic-trochanteric muscleswith the posterior capsule highlighted. 1. Glu-teus medius muscle. 2. Gluteus minimus mus-cle. 3. Tendon of the piriformis muscle. 4. Supe-rior gemellus muscle. 5. Tendon of the internalobturator muscle. 6. Inferior gemellus muscle.7. Medial femoral circumflex artery. 8. Quadra-tus femoris muscle. 9. Sciatic nerve. 10. Posteri-or capsule.
Figure 11
Image of the deep plane of the gluteal regionshowing the emergence of the deep branch ofthe medial femoral circumflex artery above thequadratus femoris muscle.
Figure 12
Resection of the quadratus femoris muscleshowing the course of the ascending branch ofthe medial femoral circumflex artery above thequadratus femoris.
Figure 13
Posterior view of the hip joint showing theposterior capsule and the course of the as-cending branch of the medial femoral circum-flex artery with its branches above the internalface of the greater trochanter.
NEUROVASCULAR RISKS OF HIP ARTHROSCOPY
The neurovascular risks depend on the location of the portalscreated during hip arthroscopy. As previously described, the por-tals used depend on which give best access to the working area:the middle and/or peripheral compartment. If we decide to workin the middle compartment, three portals are commonly used: theanterior, lateral and postero-lateral portals. If we decide to accessthe peripheral compartment, the most frequently used portals areanterior, proximal antero-lateral and distal antero-lateral.
Anterior portal
The risks of injuries associated with the anterior portal are dueto the femoral nerve, the lateral femoro-cutaneous nerve, and thedescending branch of the lateral femoral artery.
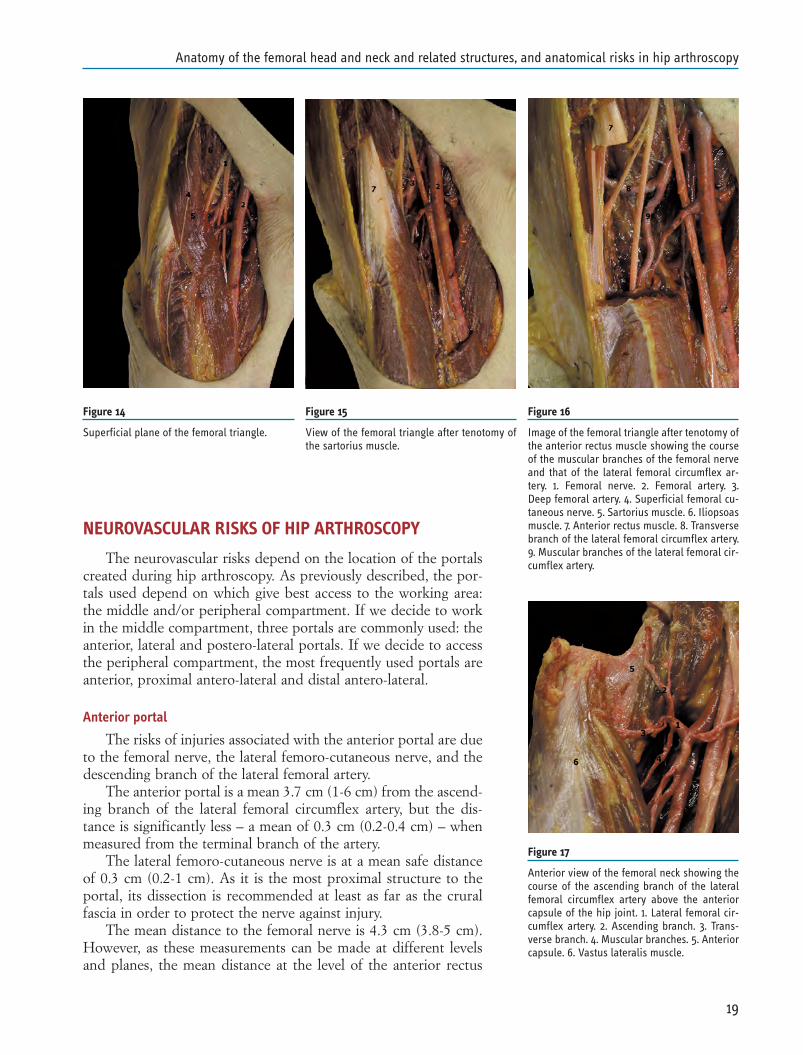
The anterior portal is a mean 3.7 cm (1-6 cm) from the ascend-ing branch of the lateral femoral circumflex artery, but the dis-tance is significantly less – a mean of 0.3 cm (0.2-0.4 cm) – whenmeasured from the terminal branch of the artery.
The lateral femoro-cutaneous nerve is at a mean safe distanceof 0.3 cm (0.2-1 cm). As it is the most proximal structure to theportal, its dissection is recommended at least as far as the cruralfascia in order to protect the nerve against injury.
The mean distance to the femoral nerve is 4.3 cm (3.8-5 cm).However, as these measurements can be made at different levelsand planes, the mean distance at the level of the anterior rectus
19
Anatomy of the femoral head and neck and related structures, and anatomical risks in hip arthroscopy
Figure 14
Superficial plane of the femoral triangle.
Figure 15
View of the femoral triangle after tenotomy ofthe sartorius muscle.
Figure 16
Image of the femoral triangle after tenotomy ofthe anterior rectus muscle showing the courseof the muscular branches of the femoral nerveand that of the lateral femoral circumflex ar-tery. 1. Femoral nerve. 2. Femoral artery. 3.Deep femoral artery. 4. Superficial femoral cu-taneous nerve. 5. Sartorius muscle. 6. Iliopsoasmuscle. 7. Anterior rectus muscle. 8. Transversebranch of the lateral femoral circumflex artery.9. Muscular branches of the lateral femoral cir-cumflex artery.
Figure 17
Anterior view of the femoral neck showing thecourse of the ascending branch of the lateralfemoral circumflex artery above the anteriorcapsule of the hip joint. 1. Lateral femoral cir-cumflex artery. 2. Ascending branch. 3. Trans-verse branch. 4. Muscular branches. 5. Anteriorcapsule. 6. Vastus lateralis muscle.

muscle is 4.3 cm, whereas it is 3.7 cm at the level of the cap-sule (10).
Antero-lateral portal
The antero-lateral portal is different when we consider thetrue antero-lateral portal and the lateral portal.
The only structure that may be injured is represented by thesuperior gluteal complex. Byrd concluded that the mean safe dis-tance in relation to the superior gluteal nerve is 4.4 cm (3.2-5.5cm). In brief, it is a sufficiently safe portal and the first that allowssurgery to be performed under radiological control.
Postero-lateral portal
The postero-lateral portal has traditionally always been consid-ered safe, with the sciatic nerve being the only nervous structureat risk However, it needs to be remembered that this portal is veryclose to the medial femoral circumflex artery when it becomesposterior.
Many authors have focused on the risk of injury to the lateralfemoral circumflex artery because of the positioning of the anteri-or portal. However, injuring this artery and its branches does notlead to vascular necrosis of the femoral head because it is not themain source of blood supply.
However, Sussmann has underlined the relationship betweenthis artery and the postero-lateral portal although, at the time theresults were analysed, only seven samples had been collected. Thisstudy estimated the distance of the portal from the course of themedial femoral circumflex artery and its branches as being 3-10mm.
Portals of the peripheral compartment
When creating these portals, the possible injuries will not leadto necrosis of the femoral head.
The three portals usually used to gain access to the peripheralcompartment are the anterior, proximal and distal antero-lateralportals, all of which are located at the level of the anterior area ofthe joint.
The studies carried out so far do not sufficiently describe theneurovascular relationships between the proximal and distal an-tero-lateral portals but, anatomically, they have the same risks asthe anterior portal: i.e. the danger of injuring the lateral femoralcircumflex artery and its capsular branches, the femoral nerveand, superficially, the lateral femoro-cutaneous nerve. However,safe distances may vary depending on the direction of the portalsboth proximally and distally.
20
Chapter 1
Figure 18
View of the gluteal area (the gluteus maximusand medius have been resected) showing therelationship between the superior gluteal neu-rovascular fascia and the greater trochanter. 1.Sciatic nerve. 2. Neurovascular fascia of thegluteus maximus muscle. 3. Gluteus minimusmuscle. 4. Piriformis muscle. 5. Quadratusfemoris muscle. 6. Insertion of the gluteusmedius muscle at the level of the greatertrochanter.
REFERENCES
1. Rouviere H, Delmas A. Anatomia humana descriptiva,topográfica y funcional. Tomo 3. Miembros. Sistema nerviosocentral. Masson 9ª ed.
2. Lavigne M, et al. Distribution of vascular foramina around thefemoral head and neck junction: relevance for conservative in-tracapsular procedures of the hip. Orthop Clin North Am.2005; 36:171-6, viii.
3. Gautier E, Ganz K, Krugel N, et al: Anatomy of the medialfemoral circumflex artery and its surgical implications. J. BoneJoint Surg Br 82:679-683, 2000
4. Beaulé P, et al: Vascularity of the arthritic femoral head alndhip resurfacing. J. Bone Joint Surg Br 88-A . Supplement 4 85-96.2006
5. Carliouz H, Pous JG, Rey JC. Les epiphysiolyses femorales su-perrieures. Rev Chir Orthop Reparatice Appar Mot.1968;54:388-481
6. Anil S. Ranawat, MD et al. Anatomy of the hip: Open andarthroscopic structure and function. Operative Techniques inOrthopaedics. 15:160-174.2005
7. Dorfmann H, Boyer T: Hip Arthroscopy utilizing the supineposition. Arthroscopy 12:264-267, 1996
8. Dorfmann H, Boyer T: Arthroscopy of the hip: 12 years of ex-perience. Arthroscopy 15:67-72, 1999
9. Wettstein M, et al: Arthroscopy of the Peripheral Compart-ment of the Hip. Oper Tech Orthop 15:225-230, 2005
10. Byrd Th:Hip arthroscopy:envolving frontiers. Elsevier 2004.11. Byrd JW, Pappas JN, Pedley MJ. Hip arthroscopy: An
anatomic study of portal placement and relationship to the ex-traarticular structures. Arthroscopy 1995;11:418-423.
12. McCarthy JC, Busconi B. The role of hip arthroscopy in thediagnosis and treatment of hip disease. Orthopedics 1995; 18:753-756
13. Sevitt S, Thompson RG. The distribution and anastomoses ofarteries supplying the head and neck of the femur. J Bone JointSurg Br 1965;47:560-573.
14. Toogood PA, Skalak A. Proximal femoral anatomy in the nor-mal population. Clin Orthop Relat Res 2009; 467(4): 876-885
15. Hewitt JD, Glisson RR, Guilak F, Vail TP. The mechanicalproperties of the human hip capsule ligaments. J Arthroplasty2002; 17(1): 82-89.
16. Martin HD, Savage A, Braly BA, Palmer IJ, Beall DP, Kelly B.The function of the hip capsular ligaments: a quantitative re-port. Arthroscopy 2008; 24(2): 188-195.
21
Anatomy of the femoral head and neck and related structures, and anatomical risks in hip arthroscopy
PROLOGUE
Effective treatment and prognosis require specificity and accu-racy in diagnosis. Differential diagnosis is used to differentiate be-tween one or more conditions, diseases or injuries that may sharesimilar signs or symptoms.
The process of a differential diagnosis involve a combinationof clinical history, physical examination with provocative tests anddiagnostic procedures. To perform a correct differential diagnosisthe clinician must have a wide working knowledge of a large rangeof pathologies. This short chapter will help the reader to performa good differential diagnosis and reach a definitive statement, be-fore treatment is engaged, in a painful hip of a young adult. Theintent is to draw a systematic review of common and uncommonpathologies which may affect the hip and of other pathologies thatmay mimic them (hip mimickers).
The diagnostic process has been divided into three section:history, physical examination and diagnostic procedures. Patho-logic conditions affecting the hip are classified as intra-articular,extra-articular and hip mimickers, according to the regionsaround and into the hip joint in which they may occur.
During this last decade the discover of new etiopathogeneticprocesses, improvements in hip arthroscopy and in magnetic reso-nance imaging (MRI) have led to a better understanding ofpathologies around the hip and consequently have broadened thedifferential diagnosis.
HIP PATHOLOGY CLASSIFICATION
Hip pathologies are classified in two main groups: intra-artic-ular and extra-articular (Table 1). For a comprehensive differentialdiagnosis a physician should always keep in mind to include in theextra-articular and hip mimicker groups also bone and soft tissueintrinsic pathologies (avascular necrosis, Bone Marrow EdemaSyndrome (BMES), osteoid osteoma and other bone and soft tis-sue neoplasm) or extrinsic pathologies (infections) (1).
23
DIFFERENTIAL DIAGNOSIS OF A PAINFUL HIPFilippo RandelliLorenzo Banci
Chapter 2

A PAINFUL HIP IN A YOUNG ADULT
Young adults may suffer of an extreme variety of hip diseases.Differential diagnosis may be challenging. In young adults, hippain often is related to physical activity. Classical “Hip pain”,coming from the joint (intra-articular pathologies), is referred as agroin pain that may o may not irradiate to the thigh. Sometime tillthe knee. But it is not rare to have a patient with a wider painaround different regions including groin, lateral, proximal anddistal part of the thigh and buttock. The anatomy of these regionsis complex and involves several musculoskeletal and neurologicalstructures which may be the cause of pain. Furthermore a com-plete diagnosis of a hip pain in young adults may be difficult be-cause two or more pathologies may coexist (Fig. 1). Only aschematic and comprehensive approach can help the orthopedicsurgeon in this difficult decision making process (Table 2).
HISTORY
An accurate diagnosis depend on a careful history of the pa-tient. The physician should collect more data as possible about thepatient and his/her pain. Then all data should be matched to havea first suspicious about the disease. In reality it is not so rare to geta nearly definitive diagnosis by simply listening to the patient.
The clinician should inquire about duration, location, frequen-cy, pattern, and radiation of pain. Intra-articular hip pain usuallypresents as groin discomfort and may radiate to the medial-anteri-or thigh.
Pain onset and duration often do not discriminate preciselybetween hip pathologies unless a traumatic event has occurred. Inpatients suffering from symptomatic femoroacetabular impinge-
24
Chapter 2
Table 1 Differential diagnosis in the painful hip
Intra-articular Extra-articular Hip mimickersLabral tears Internal snapping hip Adductor-rectus abdominis tears
Loose bodies External snapping hip Osteitis pubis
Femoro acetabular impingement Greater trochanteric pain syndrome Sports hernia
Chondral damage Bursitis Obturator neuropathy
Ligamentum teres tears Osteoid osteoma Piriformis syndrome
Development Dysplasia of the Hip Bone Marrow Edema Syndrome – Meralgia paresthetica (Roth)(DDH) BMES
Slipped capital femoral epiphysis Avascular Necrosis (AVN) of Spine derived Cruralgiathe femoral head
Post M. Perthes disease Bone and soft tissues neoplasms SI joint disease
Stress fractures Infections
Septic arthritis
Inflammatory arthritis and sinovitis
Figure 1
(A-B) Axial and sagittal CT scan views of a 33 yearold man initially diagnosed with CAM type FAIwith a high α-angle. (C) A bone scan confirmedthe suspicious of an osteoid osteoma then treatedwith a (D) CT guided radio frequency ablation
25
Differential diagnosis of a painful hip
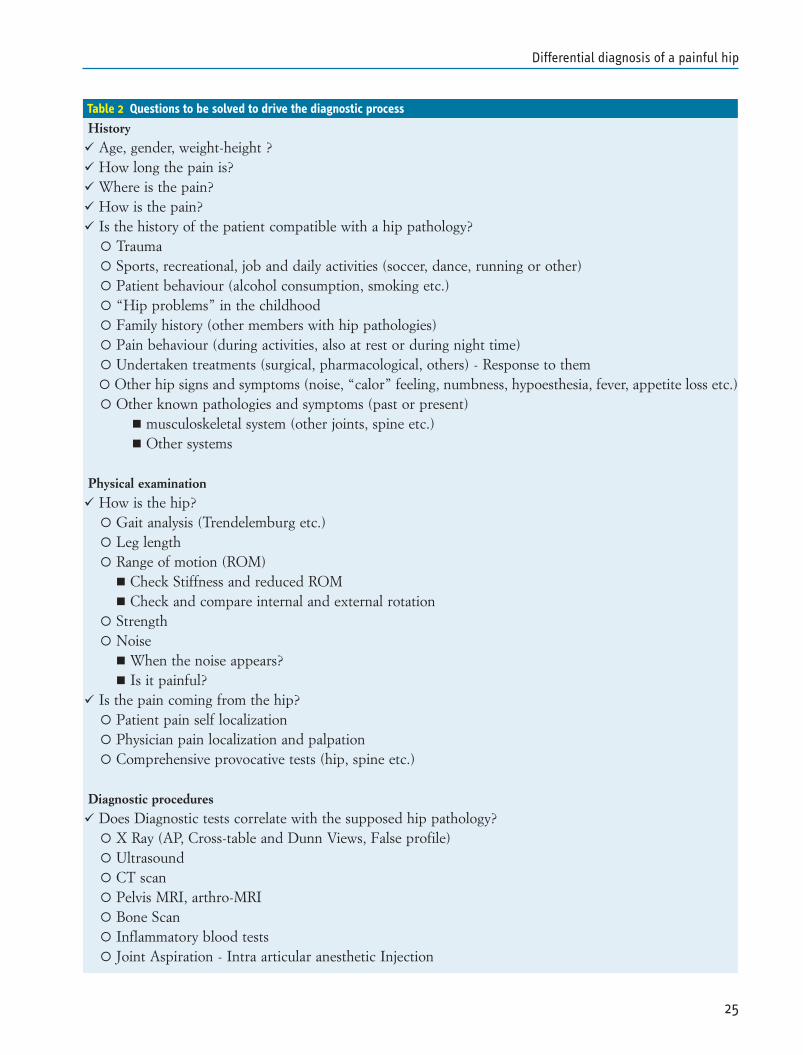
Table 2 Questions to be solved to drive the diagnostic process
History Age, gender, weight-height ? How long the pain is? Where is the pain? How is the pain? Is the history of the patient compatible with a hip pathology?
Trauma Sports, recreational, job and daily activities (soccer, dance, running or other) Patient behaviour (alcohol consumption, smoking etc.) “Hip problems” in the childhood Family history (other members with hip pathologies) Pain behaviour (during activities, also at rest or during night time) Undertaken treatments (surgical, pharmacological, others) - Response to them Other hip signs and symptoms (noise, “calor” feeling, numbness, hypoesthesia, fever, appetite loss etc.) Other known pathologies and symptoms (past or present)
musculoskeletal system (other joints, spine etc.) Other systems
Physical examination How is the hip?
Gait analysis (Trendelemburg etc.) Leg length Range of motion (ROM)
Check Stiffness and reduced ROM Check and compare internal and external rotation
Strength Noise
When the noise appears? Is it painful?
Is the pain coming from the hip? Patient pain self localization Physician pain localization and palpation Comprehensive provocative tests (hip, spine etc.)
Diagnostic procedures Does Diagnostic tests correlate with the supposed hip pathology?
X Ray (AP, Cross-table and Dunn Views, False profile) Ultrasound CT scan Pelvis MRI, arthro-MRI Bone Scan Inflammatory blood tests Joint Aspiration - Intra articular anesthetic Injection
ment (FAI), symptoms onset is commonly insidious and activity-related (2,3). Only one third of FAI patients refer to a specific ini-tial episode for the beginning of pain (3). FAI Pain occurs predom-inantly in the anterior groin and in the lateral hip and, for this rea-son, an accurate examination should be carried out for a possibleconcomitant greater trochanteric pain syndrome (GTPS). Otherless common pain location in FAI are knee, buttock and low back.Patients may complain both groin and buttock pain (3). Pain is de-scribed as dull, aching and sharp. Initially most FAI patients expe-rience moderate to marked pain that force them to limit theirsporting activities and progressively reduce their daily physical ac-tivities (4,5). Pain duration is important to asses the hypotheticaldamage. More time usually means more damage.
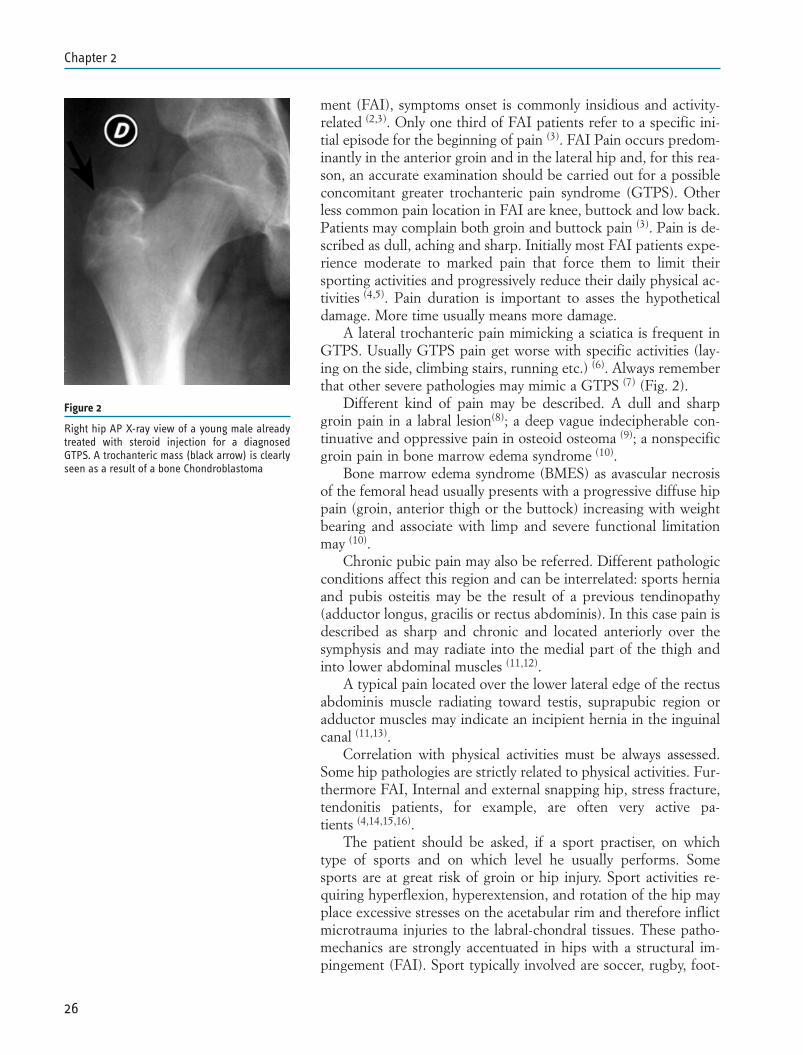
A lateral trochanteric pain mimicking a sciatica is frequent inGTPS. Usually GTPS pain get worse with specific activities (lay-ing on the side, climbing stairs, running etc.) (6). Always rememberthat other severe pathologies may mimic a GTPS (7) (Fig. 2).
Different kind of pain may be described. A dull and sharpgroin pain in a labral lesion(8); a deep vague indecipherable con-tinuative and oppressive pain in osteoid osteoma (9); a nonspecificgroin pain in bone marrow edema syndrome (10).
Bone marrow edema syndrome (BMES) as avascular necrosisof the femoral head usually presents with a progressive diffuse hippain (groin, anterior thigh or the buttock) increasing with weightbearing and associate with limp and severe functional limitationmay (10).
Chronic pubic pain may also be referred. Different pathologicconditions affect this region and can be interrelated: sports herniaand pubis osteitis may be the result of a previous tendinopathy(adductor longus, gracilis or rectus abdominis). In this case pain isdescribed as sharp and chronic and located anteriorly over thesymphysis and may radiate into the medial part of the thigh andinto lower abdominal muscles (11,12).
A typical pain located over the lower lateral edge of the rectusabdominis muscle radiating toward testis, suprapubic region oradductor muscles may indicate an incipient hernia in the inguinalcanal (11,13).
Correlation with physical activities must be always assessed.Some hip pathologies are strictly related to physical activities. Fur-thermore FAI, Internal and external snapping hip, stress fracture,tendonitis patients, for example, are often very active pa-tients (4,14,15,16).
The patient should be asked, if a sport practiser, on whichtype of sports and on which level he usually performs. Somesports are at great risk of groin or hip injury. Sport activities re-quiring hyperflexion, hyperextension, and rotation of the hip mayplace excessive stresses on the acetabular rim and therefore inflictmicrotrauma injuries to the labral-chondral tissues. These patho-mechanics are strongly accentuated in hips with a structural im-pingement (FAI). Sport typically involved are soccer, rugby, foot-
26
Chapter 2
Figure 2
Right hip AP X-ray view of a young male alreadytreated with steroid injection for a diagnosedGTPS. A trochanteric mass (black arrow) is clearlyseen as a result of a bone Chondroblastoma

ball, ice hockey, long-distance running, played at professional orsemi-professional level (4,17,18,19). Actually any hip high-demand-ing activity, either recreational or not, may be a risk factor for de-velopment of a symptomatic hip in presence of FAI. Pain general-ly worsened with activities. In same case, in the early phase of thepathology, pain is present only at the beginning of the training andthen disappear, leaving the patient with a false feeling of the un-derlying problem. Later, pain alleviation is possible only with rest.
Some important clinical signs about daily activities, as difficul-ties to tie their own shoes or sitting cross-legged, are often under-estimated by patients. Some totally degenerated hip may be bare-ly symptomatic. Those hips are usually stiff.
Patient behaviour as alcohol abuse is strictly related to avascu-lar necrosis of the femoral head.
Any hip problem in the childhood or a positive family historyshould be investigated. There are many hip pathologies in thechildhood that may become definitively symptomatic in the youngadult age (Dysplasia, M. Perthes, Epiphysiolysis). Dysplasia famil-iarity is well known and FAI familiarity is a growing issue formany hip surgeons.
Pain behaviour and response to pharmacological treatmentcan be helpful to differentiate between pathologies and sometimeto asses their severities. Night and rest pain is often present in os-teoid osteoma as sudden relief by NSAID (9,20) (Fig. 1).
Undertaken treatments should be investigated as well as pa-tient response to them. Some hip problem (mainly muscle strains.tendonitis and some peritrochanteric disordes) may be treatedmainly by conservative measures if those are well indicated andperformed.
Any other hip signs or symptoms, rather than pain, should becollected, if present. Hypoesthesia and paresthesia, for example,are never present in hip intra-articular pathologies. They are therule in Roth meralgia (21) and may be present in spine derivedpain.
Lower spine disorders are the more common mimickers of hippathologies and some time hip and spine disorders coexists. Thephysician should help the patient to carefully discriminate be-tween them either through the history either through a meticulousphysical examination. A mild elevation of body temperature andappetite loss may accompany hip oncologic diseases, rare but pos-sible in young adult, or inflammatory arthritis.
Patients complaining groin pain may have pathologies in otherorgans that may cause symptoms comparable to those of an hipdisorder. A history of abdominal and genitourinary pathologiesmay indicate that the pathology could be located there instead ofthe hip. Sports hernia is a growing pathology for general surgeons.It is strictly sport related and may have a correlation with FAI. Onthe other hand FAI and other hip pathologies can be confusedwith other system pathologies, especially gynaecological or urolog-ical. In my experience, for example, with endometriosis in female.
27
Differential diagnosis of a painful hip
Finally there are new extra-hip entities nowadays recognized as apart of what we could call the FAI syndrome. Pubis osteitis, forexample, could be due to a reduce range of motion of a FAI af-fected hip.
Any previous surgeries and any previous traumatic event relat-ed to the affected hip should be registered.
PHYSICAL EXAMINATION
Clinical examination should confirm the initial suspicious, ass-es the relevance of the pathology and drive next diagnostic proce-dures. Furthermore clinical evaluation should check other signs orreproducible symptoms sometime underestimated by the patient.For example young adults tend to underestimate important clini-cal signs as reduced range of motion (especially rotations) if theyare pain free.
Observation is the first step of the physical examination and itbegins when the patient enters the office. The examiner shouldsuddenly note patient’s gait and posture. Then the hip is checkedin normal condition before provocative tests. Lastly pain is re-searched and provocative test performed.
Gait Analysis
Painful hips are often associated with a slight/mild limp. Tren-delenburg’s sign is rare and present in severe dysplastic cases ormedius gluteus lesion (6). Young patients, even with disabling hippain, generally do not use cane, crutches or other assistive devicesduring walking.
Leg length
Checking length leg discrepancy (LLD) is an important step ofthe physical examination. There many pathologies that may resultin a shortened limb (Dysplasia, M. Perthes, Epiphysiolysis) andthere are some pathologies that are related with LLD (GTPS). Weare checking LLD in FAI patients and first results are showing aLLD or a patient feeling of LLD in many of our patients. Interest-ingly this feeling is normally accentuated after surgery.
Range of motion (ROM)
Intra-articular pathologies reduces range of motion (22). ManyFAI patients have decreased internal rotation, adduction and flex-ion. In this patient internal rotation decreases with increasing flex-ion and adduction. Affected hips typically have an internal rota-tion in flexion between 9° to 11 and a flexion averaging between90° to 100° (3,23).
Some patients present with instability characterized by an ab-normal ROM and laxity.
The physician should always check and compare internal andexternal rotation of both hips. Retroversion of the femoral neck
28
Chapter 2

and reduce femoral antitorsion angle will result in limited internalrotation and abnormal external rotation. This can be an aggravat-ing issue in a FAI syndrome.
Noise
Some hip pathologies produce noise (internal and externalsnapping hip). Noises can be painful or not. Usually noises are re-producible from the patients. Sometime a noise can be only felt bypatients and not reproducible by the examiner, especially if notcarefully researched. First the examiner should differentiate be-tween external from internal noise (14). An external noise comingfrom the fascia lata are easier to diagnose just laying one handover the greater trochanter and asking the patient to reproducethe noise (14,24,25). Internal noise often require specific hip move-ments as in snapping psoas syndrome where the examiner bringsthe hip from a flexed, abducted, externally rotated position downinto extension with internal rotation. It is mandatory to ask thepatient if the noise produces or not pain and/or discomfort (14,26).
Strength
Different muscles group should be checked: Abductors, Flex-ors, External and Internal Rotators, Adductors and Extensors. Incase of a muscle-tendon disorder pain is elicited by these manoeu-vres, especially if resisted.
Dealing with muscles weakness one should always keep inmind spine related pathologies.
Abductors are usually involved in GTPS (6).
Pain Research
Differently from intra-articular pathologies, extra-articularones and groin injuries are conditions which can be well recog-nized by palpation. The physician ask the patient where he feelspain and then upon physical examination, direct compression onspecific area try to recreate patient’s typical pain and symptoms.Always, during palpation, search for local mass, especially if re-ferred by the patient. Skin temperature variations should be re-searched too.
Tendinopathy of the gluteus minimus or medius, often presentin case of greater trochanter pain syndrome (GTPS), generallymay produce tenderness to palpation over the superior-lateral as-pects of the greater trochanter (6,27,28). Distension, swelling and in-flammation of the trochanteric bursae, which can be secondarycaused by tendinosis or tears of the gluteal muscles or snapping ofthe iliotibial band over the greater trochanter, may be the cause oftenderness too (24,29).
Tenderness over the iliopsoas tendon may be indicative of bur-sitis of the iliopsoas bursa caused by snapping or retraction of theiliopsoas tendon (30,31).
29
Differential diagnosis of a painful hip

Iliopubic stress fracture patients typically report pain uponpalpation or percussion of the affected area (15).
Dysaesthesia or paraesthesia over the lateral, anterior or medi-al aspects of the proximal thigh may be the sign of a spine rootcompression, a neuropathy or a nerve entrapment at the pelvis.Altered skin sensation and superficial pain over the groin and themedial part of the thigh may be caused by the ilioinguinal nerve,genitofemoral nerve or obturator nerve entrapment (32,33,34); if thealtered skin sensation to palpation is localized over the lateral andanterior aspects of the proximal thigh neuropathy may involve thelateral femoral cutaneous nerve (21). Pain on palpation on the sci-atic notch with the hip flexed, adducted and internally rotatedmay be indicative of a piriformis syndrome. Patients typicallycomplain of a dull ache in the buttock that may radiate down theposterior thigh. This pain is difficult to distinguish from radicularpain caused by sciatic nerve root compression (35).
Tenderness with palpation over the symphysis pubis and pubicrami may be the clinical finding of osteitis pubis. Pain may radiateinto the adductor muscles origin, the lower abdomen and testis.Lack of such tenderness over the symphysis pubis usually ex-cludes the diagnosis (36,37).
A localised tenderness at or just above the pubic crest mayrepresent an incipient hernia. These patients generally complainunilateral inguinal pain that often radiate to the pubic tubercleand inner thigh. Occasionally a subtle bulge in the skin surfacecan be appreciated on the affected inguinal region when the pa-tient is observed from above while standing (11,12).
Comprehensive provocative tests
The majority of patients suffering from chondro-labral pathol-ogy associated with FAI demonstrates a positive anterior impinge-ment test (FADIR test, Flexion ADduction and Internal Rotation- Fig. 3) which is considered as the most reliable and consistentphysical exam finding. In anterior impingement test the patient isin a supine position and the affected hip is passively flexed be-yond 90°. Then the hip is internally rotated while an adductionforce is applied. The test is considered positive if reproducing pa-tient typical hip or groin pain (8,5,3).
The Patrick’s or FABER test (Flexion, ABduction and Exter-nal Rotation - Fig. 4) has been originally describe to differentiatebetween sacroiliac from hip pathologies. The FABER test is oftenpositive in FAI patients and reproduce the anterior hip pain. Incase of SI joint pathology a posterior pain is referred.
Other helpful, but less specific and sensitive tests are theFABER test, the resisted straight leg raise test, the log roll test andthe posterior impingement test (5).
In the resisted straight leg raise test the hip joint is activelyflexed to approximately 30˚, with the knee extended. The examin-er apply pressure just above the knee, toward the examinationtable. The test is positive if reproduce groin pain (11).
30
Chapter 2
Figure 3
Anterior impingement test or FADIR, Flexion AD-duction and Internal Rotation test
Figure 4
The Patrick’s or FABER test (Flexion, ABductionand External Rotation)

In the log roll test the patient laying supine with hip e knee re-laxed. The examiner rotate internally end externally the affectedhip.
The posterior impingement test (EABER test, ExtensionABuction and External Rotation) the posterior labrum is checkedand the patient laying at the edge of the table to allow extension.
An external snapping hip can be elicited with the modifiedOber test (Fig. 5): an internally adducted and internally rotatedhip is passively extended, abducted and externally rotated repro-ducing patient noise. The examiner leaves his hand laying on thegreater trochanter (38).
The iliopsoas snapping test (Fig. 6), in case of internal hipsnapping, give a palpable and audible snap moving the affectedhip from a flexed, abducted and external rotated position into ex-tension, adduction and internal rotation (14).
The modified Thomas test may be helpful in diagnosis iliop-soas retraction or tendonitis-bursitis: patient is placed in a supineposition with the knees bent over the edge of the examinationtable, flexed to 90°. Patient is instructed to flex the nonaffectedhip and knee and hold the knee to the chest while the affected hipin extended passively. The test is positive if produce pain anterior-ly over the iliopsoas or the thigh can’t be extended at the level ofthe table (38).
The resisted abduction test is useful to evaluate medius glu-teus lesion (6).
Resisted adduction or abduction of a internally rotated andflexed hip can reproduce the symptoms of a piriformis syndrome,as the sciatic nerve is in tension (39,40,41).
Straight-leg raise test (Lasegue) and femoral nerve tension test(Wasserman) are generally negative in case of hip pathologies incontrast to patients with radicular causes of sciatica (41).
DIAGNOSTIC PROCEDURESRadiography
X-rays should always be the first diagnostic procedure in de-tecting hip pathologies. Radiographic evaluation remains one ofthe most important diagnostic tests for a large number of patholo-gies. A real standard Antro-Posterior (AP) view (Fig. 7), a frog-legview (Fig. 8) and a cross-table lateral view (Fig. 9) or a 45° and90° Dunn view (Fig. 10) of the affected hip are the best images tohave. To get those views right a precise patient positioning and x-ray tube is mandatory.
FAI diagnosis is made by good X-ray views. Further exams arethen needed only to asses the severity of the disease and its surgi-cal indication. Cam deformity is usually evaluated by frog-leg,cross-table and Dunn views where an osseous prominence (bump)at the head-neck junction or an aspherical femoral head are bestseen . Sometime a pistol-grip deformity is well seen also on a APview. An herniation pit (a little superficial bone cyst) may be seen
31
Differential diagnosis of a painful hip
Figure 5
Modified Ober test (Fig.5): an internally adductedand internally rotated hip is passively extended,abducted and externally rotated reproducing pa-tient noise. The examiner leaves his hand layingon the greater trochanter
Figure 6
Iliopsoas snapping test. Moving the affected hipfrom a flexed, abducted and external rotated posi-tion into extension, adduction and internal rota-tion a noise is produced and, sometime, painelicited
on the anterosuperior femoral neck, close to the physis as a sign ofpossible local reaction.
Pincer deformities can be only determined on a well per-formed standardized AP view. Pincer signs on x-ray are different:the crossover sign, the posterior wall sign, ischial sign and coxaprofunda (8,4,42,43).
Another useful view for detecting acetabular version and an-tero-posterior joint line space is the Lequesne false profile view(Fig. 11).
Pelvis AP view is also used to asses joint degeneration usingthe Tönnis classification (44):0° No signs of OA1° Increased sclerosis, slight joint narrowing, no or slight loss ofhead sphericity2° Small cysts, moderate joint space narrowing, moderate loss ofhead sphericity3° Large cysts, severe joint space narrowing, severe deformity ofthe head
Further radiographic findings may include osteochondralloose bodies (45,46), foreign bodies, labrum ossification, os acetab-uli, tendon calcification, heterotopic ossification, cortical defectand stress fracture of the pelvis, bone cysts, osteolityc lesions etc.
When osteitis pubis and pelvic instability are suspected, imag-ing tests should comprise standing AP plain radiograph of thepelvis and one-legged stance AP plain radiographs (flamingostress views) of the symphysis pubis. Flamingo stress views arepositive if a displacement of 2 mm or more is demonstrated acrossthe symphysis pubis between the upper margins of the superiorpubic rami. Symphyseal joint laxity or disruption can be radiogra-phycally assessed by widening of the joint space of more than 7mm (18).
Typical radiographic findings of osteitis pubis are degenerativeperiosteal changes in articular cortical surfaces at the symphysis
32
Chapter 2
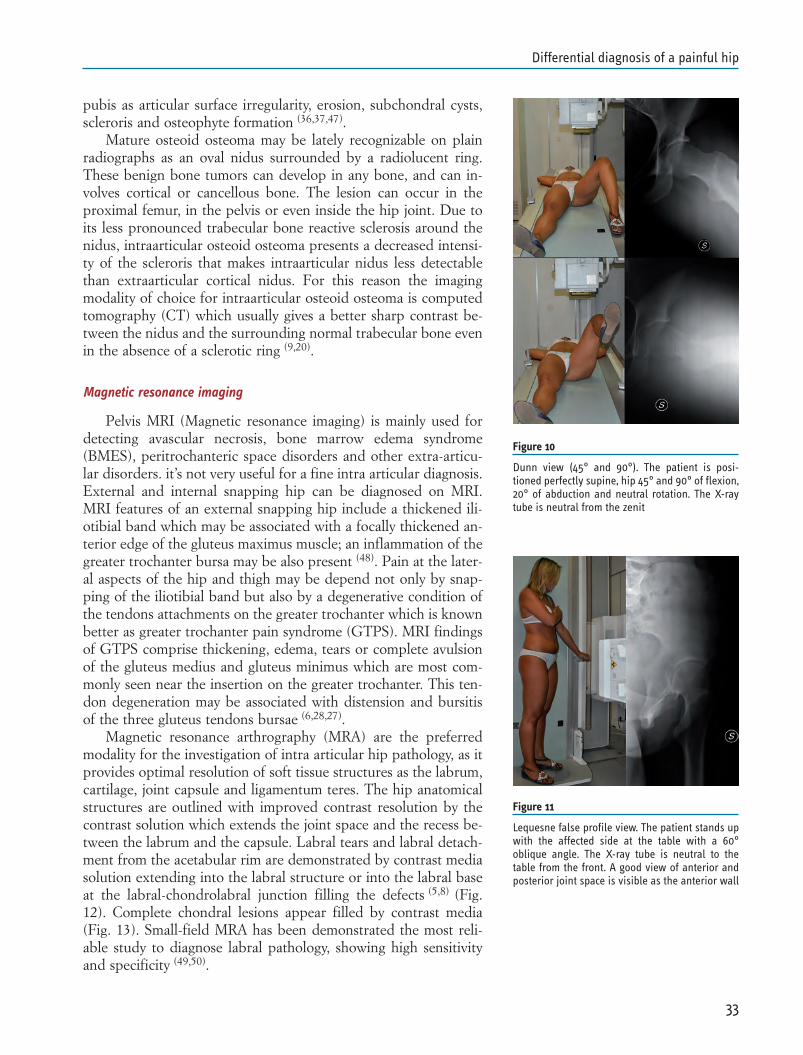
Figure 9
Cross-table lateral view. The patient is positionedperfectly supine, affected hip laying on the table.Non affected hip flexed 90°. X-ray receiving pan-el aside the affected hip at 45° from the longitudi-nal patient axis. The X-ray tube is coming frommedial at 45° from the same axis. Hip rotation isdecided depending on which anterior part of theneck should be visualized. In this case the hip isslightly externally rotated to better visualize an-tero medial femoral neck
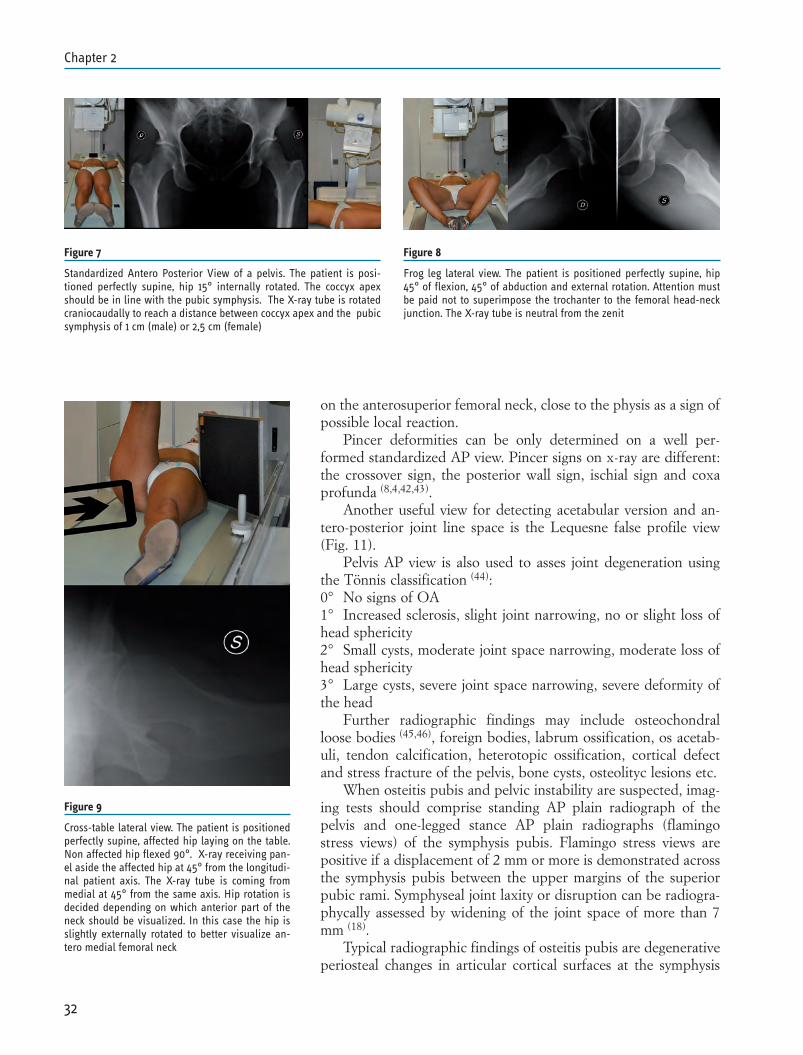
Figure 7
Standardized Antero Posterior View of a pelvis. The patient is posi-tioned perfectly supine, hip 15° internally rotated. The coccyx apexshould be in line with the pubic symphysis. The X-ray tube is rotatedcraniocaudally to reach a distance between coccyx apex and the pubicsymphysis of 1 cm (male) or 2,5 cm (female)
Figure 8
Frog leg lateral view. The patient is positioned perfectly supine, hip45° of flexion, 45° of abduction and external rotation. Attention mustbe paid not to superimpose the trochanter to the femoral head-neckjunction. The X-ray tube is neutral from the zenit
pubis as articular surface irregularity, erosion, subchondral cysts,scleroris and osteophyte formation (36,37,47).
Mature osteoid osteoma may be lately recognizable on plainradiographs as an oval nidus surrounded by a radiolucent ring.These benign bone tumors can develop in any bone, and can in-volves cortical or cancellous bone. The lesion can occur in theproximal femur, in the pelvis or even inside the hip joint. Due toits less pronounced trabecular bone reactive sclerosis around thenidus, intraarticular osteoid osteoma presents a decreased intensi-ty of the scleroris that makes intraarticular nidus less detectablethan extraarticular cortical nidus. For this reason the imagingmodality of choice for intraarticular osteoid osteoma is computedtomography (CT) which usually gives a better sharp contrast be-tween the nidus and the surrounding normal trabecular bone evenin the absence of a sclerotic ring (9,20).
Magnetic resonance imaging
Pelvis MRI (Magnetic resonance imaging) is mainly used fordetecting avascular necrosis, bone marrow edema syndrome(BMES), peritrochanteric space disorders and other extra-articu-lar disorders. it’s not very useful for a fine intra articular diagnosis.External and internal snapping hip can be diagnosed on MRI.MRI features of an external snapping hip include a thickened ili-otibial band which may be associated with a focally thickened an-terior edge of the gluteus maximus muscle; an inflammation of thegreater trochanter bursa may be also present (48). Pain at the later-al aspects of the hip and thigh may be depend not only by snap-ping of the iliotibial band but also by a degenerative condition ofthe tendons attachments on the greater trochanter which is knownbetter as greater trochanter pain syndrome (GTPS). MRI findingsof GTPS comprise thickening, edema, tears or complete avulsionof the gluteus medius and gluteus minimus which are most com-monly seen near the insertion on the greater trochanter. This ten-don degeneration may be associated with distension and bursitisof the three gluteus tendons bursae (6,28,27).
Magnetic resonance arthrography (MRA) are the preferredmodality for the investigation of intra articular hip pathology, as itprovides optimal resolution of soft tissue structures as the labrum,cartilage, joint capsule and ligamentum teres. The hip anatomicalstructures are outlined with improved contrast resolution by thecontrast solution which extends the joint space and the recess be-tween the labrum and the capsule. Labral tears and labral detach-ment from the acetabular rim are demonstrated by contrast mediasolution extending into the labral structure or into the labral baseat the labral-chondrolabral junction filling the defects (5,8) (Fig.12). Complete chondral lesions appear filled by contrast media(Fig. 13). Small-field MRA has been demonstrated the most reli-able study to diagnose labral pathology, showing high sensitivityand specificity (49,50).
33
Differential diagnosis of a painful hip
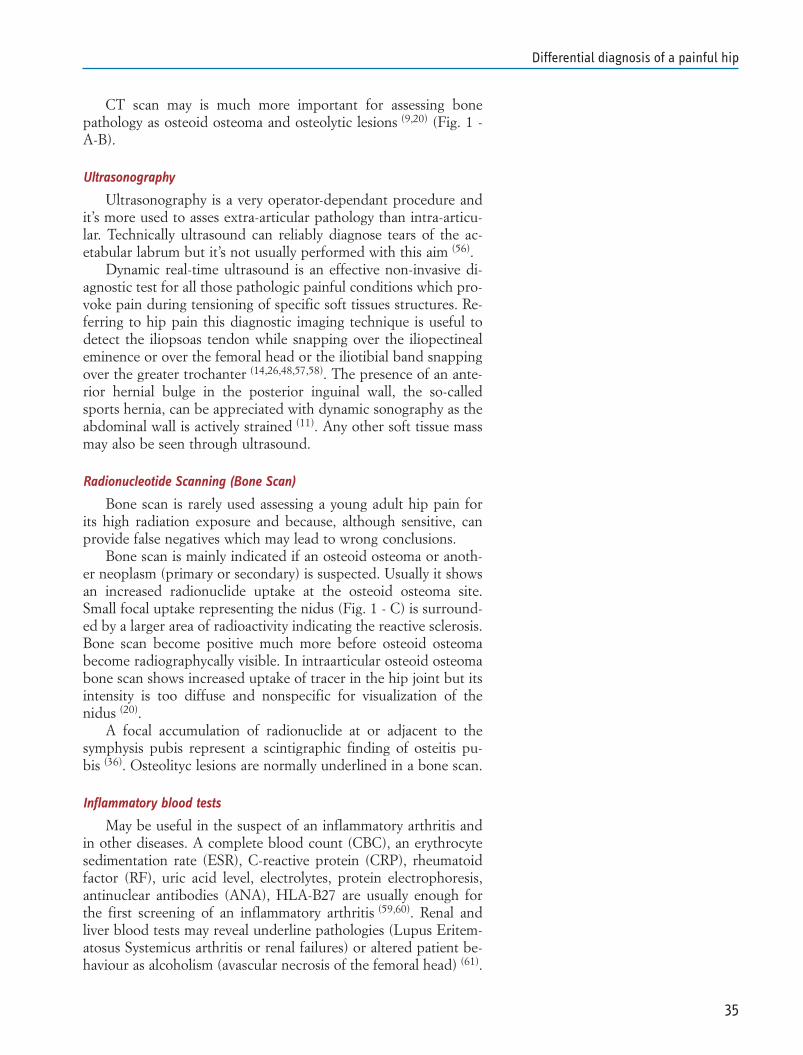
Figure 10
Dunn view (45° and 90°). The patient is posi-tioned perfectly supine, hip 45° and 90° of flexion,20° of abduction and neutral rotation. The X-raytube is neutral from the zenit
Figure 11
Lequesne false profile view. The patient stands upwith the affected side at the table with a 60°oblique angle. The X-ray tube is neutral to thetable from the front. A good view of anterior andposterior joint space is visible as the anterior wall

Moreover MRA can provide multiplanar images of the hip, al-lowing the best visualization and mapping of the joint space. MRAis also used for evaluation of the femoral head asphericity by thealpha-angle measurement in cam femoroacetabular impingementand less for assessment of acetabular retroversion (42).
MRI and MRA may also be used to asses femoral anteversionand anti torsion angle, important in a comprehensive treatment ofa FAI or dysplastic hip.
Ossified or cartilaginous loose bodies inside the joint space areeasily identified by MRI and, better by MRA (22,45,46).
Other degenerative conditions of the hip joint which can bevisible on MRA are ligamentum teres tears (51,52), chondral dam-ages (53), capsular laxity, synovitis (1). Nevertheless, these soft tis-sue damages may be often underestimated only with only a MRAstudy. Arthroscopy, with a direct inspection of the real severity ofthe lesions, remains the gold standard for the definitive diagnosisof chondral damage and cartilage pathology (53).
Image findings of tears or avulsions at the attachment sites ofthe adductor longus, gracilis and rectus abdominis muscles can beseen on MRI if suspected.
Differential diagnosis between BMES and other diseases asso-ciated with bone marrow edema is possible, as demarcation of os-teonecrotic bone areas as well as osteoarthritic changes, bone tu-mors, osteomyelitis or fractures can clearly be detected withMRI (54).
Visualization on MRI of an articular surface irregularity of thesymphysis pubis with an alteration of the width of the joint spaceand paraarticular pubic bone marrow edema on coronal and axialimages are the criteria for the diagnosis of osteitis pubis (19). Injuryto the symphysis pubis is often associated to enthesopathies of ad-ductor muscles and anterior abdominal wall muscles.
Because rectus abdominis and adductor dysfunction is usuallya initial condition that leads to osteitis pubis, the two conditionsmay often coexist. Also herniation of the posterior wall of the in-guinal canal may be a secondary event to a primary muscular in-jury that cause pelvis instability and symphyseal laxity (11,13,17,18).
CT scan
CT scan can be useful in some instance during the differentialdiagnosis of a painful hip. It has been used with 3D, surface ren-dering and oblique radial reformation in order to assess the con-tour of the anterior lateral impingement surface in patients withsuspected FAI with good results. Its radiological exposure andlow sensitivity for chondral and labrum degeneration makes CTseldom used for this purpose. Furthermore CT scan has a low res-olution on soft tissues. CT scan may be useful in particular FAIcases with abnormal deformities as abnormal femoral anteversionand anti torsion angle. 3D CT scan may also be usefull in preop-erative planning during the management of complex deformi-ties (55).
34
Chapter 2
Figure 12
Frontal MRA (magnetic resonance arthrography)view of a 33 year old woman with a labral tearsand partial detachment from the acetabular rim,demonstrated by contrast media solution extend-ing into the chondrolabral junction (white arrow)filling the defects
Figure 13
Sagittal MRA (magnetic resonance arthrography)view of a 38 year old woman with a painful hip. Agrade 4 antero superior chondral lesion appearsfilled by contrast media (white arrow)
CT scan may is much more important for assessing bonepathology as osteoid osteoma and osteolytic lesions (9,20) (Fig. 1 -A-B).
Ultrasonography
Ultrasonography is a very operator-dependant procedure andit’s more used to asses extra-articular pathology than intra-articu-lar. Technically ultrasound can reliably diagnose tears of the ac-etabular labrum but it’s not usually performed with this aim (56).
Dynamic real-time ultrasound is an effective non-invasive di-agnostic test for all those pathologic painful conditions which pro-voke pain during tensioning of specific soft tissues structures. Re-ferring to hip pain this diagnostic imaging technique is useful todetect the iliopsoas tendon while snapping over the iliopectinealeminence or over the femoral head or the iliotibial band snappingover the greater trochanter (14,26,48,57,58). The presence of an ante-rior hernial bulge in the posterior inguinal wall, the so-calledsports hernia, can be appreciated with dynamic sonography as theabdominal wall is actively strained (11). Any other soft tissue massmay also be seen through ultrasound.
Radionucleotide Scanning (Bone Scan)
Bone scan is rarely used assessing a young adult hip pain forits high radiation exposure and because, although sensitive, canprovide false negatives which may lead to wrong conclusions.
Bone scan is mainly indicated if an osteoid osteoma or anoth-er neoplasm (primary or secondary) is suspected. Usually it showsan increased radionuclide uptake at the osteoid osteoma site.Small focal uptake representing the nidus (Fig. 1 - C) is surround-ed by a larger area of radioactivity indicating the reactive sclerosis.Bone scan become positive much more before osteoid osteomabecome radiographycally visible. In intraarticular osteoid osteomabone scan shows increased uptake of tracer in the hip joint but itsintensity is too diffuse and nonspecific for visualization of thenidus (20).
A focal accumulation of radionuclide at or adjacent to thesymphysis pubis represent a scintigraphic finding of osteitis pu-bis (36). Osteolityc lesions are normally underlined in a bone scan.
Inflammatory blood tests
May be useful in the suspect of an inflammatory arthritis andin other diseases. A complete blood count (CBC), an erythrocytesedimentation rate (ESR), C-reactive protein (CRP), rheumatoidfactor (RF), uric acid level, electrolytes, protein electrophoresis,antinuclear antibodies (ANA), HLA-B27 are usually enough forthe first screening of an inflammatory arthritis (59,60). Renal andliver blood tests may reveal underline pathologies (Lupus Eritem-atosus Systemicus arthritis or renal failures) or altered patient be-haviour as alcoholism (avascular necrosis of the femoral head) (61).
35
Differential diagnosis of a painful hip

Joint Aspiration - Intra or extra articular anesthetic Injection
Addressing a hip joint with a needle may have different pur-poses in a differential diagnosis process. First synovial fluid maybe analysed and cultured. Second a local anesthetic can be deliv-ered in those cases where the real source of patient main complainis unclear, usually between spine or hip (62).
Third there is a known good correlation between pain reliefafter hip local anesthetic and pain relief after hip arthroplasty (63).Less is known about correlation between local anesthetic andarthroscopy.
Anyway local anesthetic are unable to differentiate betweendifferent intra capsular pathologies and injection result should al-ways be well pounded.
Diagnosis of extra-articular disorders, as bursitis, tendonitisand neuropathies around the hip can be confirmed, and sometime treated, by local anesthetic and corticosteroid injection.
36
Chapter 2
REFERENCES
1. Tibor LM, Sekiya JK. Differential diagnosis of pain around thehip joint. Arthroscopy. 2008 Dec;24(12):1407-21.
2. Philippon MJ, Stubbs AJ, Schenker ML, Maxwell RB, GanzR, Leunig M. Arthroscopic management of femoroacetabularimpingement: osteoplasty technique and literature review. AmJ Sports Med. 2007 Sep;35(9):1571-80.
3. Clohisy JC, Knaus ER, Hunt DM, Lesher JM, Harris-HayesM, Prather H. Clinical presentation of patients with sympto-matic anterior hip impingement. Clin Orthop Relat Res. 2009Mar;467(3):638-44.
4. Philippon MJ, Schenker ML. Arthroscopy for the treatment offemoroacetabular impingement in the athlete. Clin SportsMed. 2006 Apr;25(2):299-308.
5. Groh MM, Herrera J. A comprehensive review of hip labraltears. Curr Rev Musculoskelet Med. 2009 Jun;2(2):105-17.
6. Lequesne M, Mathieu P, Vuillemin-Bodaghi V, Bard H, DjianP. Gluteal tendinopathy in refractory greater trochanter painsyndrome: Diagnostic value of two clinical tests. Arthritis andRheumatism. 2008;59:241-46.
7. Cheng-Li Lin, Ming-Tung Huang and Chii-Jeng Lin. Snappinghip caused by a venous hemangioma of the gluteus maximusmuscle: a case report. Journal of Medical Case Reports 2008,2:386.
8. Beaulé PE, O’Neill M, Rakhra K. Acetabular labral tears. JBone Joint Surg Am. 2009 Mar 1;91(3):701-10.
9. Efstathopoulos N, Sapkas G, Xypnitos FN, Lazarettos I, Kor-res D, Nikolaou VS. Recurrent intra-articular osteoid osteomaof the hip after radiofrequency ablation: a case report and re-view of the literature. Cases J. 2009 Jul 17;2:6439.
10. Korompilias AV, Karantanas AH, Lykissas MG, Beris AE.Bone marrow edema syndrome. Skeletal Radiol. 2009May;38(5):425-36.
11. Garvey JFW, Read JW, Turner A. Sportsman hernia: what canwe do? Hernia. 2010;14:17-25.
12. Campanelli G. Pubic inguinal pain syndrome: the so-calledsports hernia. Hernia. 2010;14:1-4.
13. Zoga AC, Kavanagh EC, Omar IM, Morrison WB, KoulourisG, Lopez H, Chaabra A, Domesek J, Meyers WC. Athleticpubalgia and the “sports hernia”: MR imaging findings. Radi-ology. 2008;247:797-07.
14. Winston P, Awan R, Cassidy JD, Bleakney RK. Clinical exam-ination and ultrasound of self-reported snapping hip syn-drome in elite ballet dancers. Am J Sports Med. 2007Jan;35(1):118-26.
15. Monteleone GP Jr. Stress fractures in the athlete. Orthop ClinNorth Am. 1995 Jul;26(3):423-32.
16. Johnson AW, Weiss CB Jr, Wheeler DL. Stress fractures of thefemoral shaft in athletes—more common than expected. A
37
Differential diagnosis of a painful hip
new clinical test. Am J Sports Med. 1994 Mar-Apr;22(2):248-56.
17. Cunningham PM, Brennan D, O’Connell M, MacMahon P,O’Neill P, Eustace S. Patterns of bone and soft-tissue injury atthe symphysis pubis in soccer players: observations at MRI.AJR Am J Roentgenol. 2007 Mar;188(3):W291-6.
18. Koulouris G. Imaging review of groin pain in elite athletes: ananatomic approach to imaging findings. AJR Am JRoentgenol. 2008 Oct;191(4):962-72.
19. Verrall GM, Slavotinek JP, Fon GT. Incidence of pubic bonemarrow oedema in Australian rules football players: relation togroin pain. Br J Sports Med. 2001 Feb;35(1):28-33.
20. Papathanassiou ZG, Megas P, Petsas T, Papachristou DJ, Ni-las J, Siablis D. Osteoid osteoma: diagnosis and treatment. Or-thopedics. 2008 Nov;31(11):1118.
21. Ivins GK. Meralgia paresthetica, the elusive diagnosis: clinicalexperience with 14 adult patients. Ann Surg. 2000Aug;232(2):281-6.
22. Boyer T, Dorfmann H. Arthroscopy in primary synovial chon-dromatosis of the hip: description and outcome of treatment.J Bone Joint Surg Br. 2008 Mar;90(3):314-8.
23. Kubiak-Langer M, Tannast M, Murphy SB, Siebenrock KA,Langlotz F. Range of motion in anterior femoroacetabular im-pingement. Clin Orthop Relat Res. 2007 May;458:117-24.
24. Farr D, Selesnick H, Janecki C, Cordas D. Arthroscopic bur-sectomy with concomitant iliotibial band release for the treat-ment of recalcitrant trochanteric bursitis. Arthroscopy. 2007Aug;23(8):905.e1-5.
25. Provencher MT, Hofmeister EP, Muldoon MP. The surgicaltreatment of external coxa saltans (the snapping hip) by Z-plasty of the iliotibial band. Am J Sports Med. 2004Mar;32(2):470-6.
26. Deslandes M, Guillin R, Cardinal E, Hobden R, Bureau NJ.The snapping iliopsoas tendon: new mechanisms using dy-namic sonography. AJR Am J Roentgenol. 2008Mar;190(3):576-81.
27. Bird PA, Oakley SP, Shnier R, Kirkham BW. Prospective eval-uation of magnetic resonance imaging and physical examina-tion findings in patients with greater trochanteric pain syn-drome. Arthritis Rheum. 2001 Sep;44(9):2138-45.
28. Kingzett-Taylor A, Tirman PF, Feller J, McGann W, Prieto V,Wischer T, Cameron JA, Cvitanic O, Genant HK. Tendinosisand tears of gluteus medius and minimus muscles as a cause ofhip pain: MR imaging findings. AJR Am J Roentgenol. 1999Oct;173(4):1123-6.
29. Baker CL, Massie V, Hurt WG, Savory CG. Arthroscopic bur-sectomy for recalcitrant trochanteric bursitis. Arthroscopy.2007;23:827-832.
30. Blankenbaker DG, De Smet AA, Keene JS. Sonography of theiliopsoas tendon and injection of the iliopsoas bursa for diag-
38
Chapter 2
nosis and management of the painful snapping hip. SkeletalRadiol. 2006 Aug;35(8):565-71.
31. Johnston CAM, Wiley JP, Lindsay DM, Wiseman DA. Iliop-soas bursitis and tendonitis. Sport Med. 1998;25(4):271-283.
32. Tipton JS. Obturator neuropathy. Curr Rev MusculoskeletMed. 2008 Dec;1(3-4):234-7.
33. Bradshaw C, McCrory P, Bell S, Brukner P. Obturator nerveentrapment. A cause of groin pain in athletes. Am J SportsMed. 1997 May-Jun;25(3):402-8.
34. Harms BA, DeHaas DR Jr, Starling JR. Diagnosis and manage-ment of genitofemoral neuralgia. Arch Surg. 1984;119:339-41.
35. Jawish RM, Assoum HA, Khamis CF. Anatomical, clinical andelectrical observations in piriformis syndrome. J Orthop SurgRes. 2010 Jan 21;5(1):3.
36. O’Connell MJ, Powell T, McCaffrey NM, O’Connell D, Eu-stace SJ. Symphyseal cleft injection in the diagnosis and treat-ment of osteitis pubis in athletes. AJR Am J Roentgenol. 2002Oct;179(4):955-9.
37. Williams PR, Thomas DP, Downes EM. Osteitis pubis and in-stability of the pubic symphysis. When nonoperative measuresfail. Am J Sports Med. 2000 May-Jun;28(3):350-5.
38. Malanga GA, Nadler SF. Physical examination of the hip. In:Musculoskeletal physical examination, an evidence-based ap-proach. Philadelphia, PA: Elsevier Mosby. 2006:251-79.
39. Windisch G, Braun EM, Anderhuber F. Piriformis muscle:Clinical anatomy and consideration of the piriformis syn-drome. Surg Radiol Anat. 2007;29:37-45.
40. Reus M, de Dios Bernà J, Vàzquez V, Redondo MV, Alonso J.Piriformis syndrome: A simple technique for US-guided infil-tration of the perisciatic nerve. Preliminary results. Eur Radi-ol. 2008;18:616-20.
41. Filler AG, Haynes J, Jordan SE, et al. Sciatica of nondisc ori-gin and piriformis syndrome: Diagnosis by magnetic reso-nance neurography and interventional magnetic resonance im-aging with outcome study of resulting treatment. J NeurosurgSpine. 2005;2:99-15.
42. Siebenrock KA, Schoeniger R, Ganz R. Anterior femoro-ac-etabular impingement due to acetabular retroversion. Treat-ment with periacetabular osteotomy. J Bone Joint Surg Am.2003;85-A:278-86.
43. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influ-ences the pattern of damage to the acetabular cartilage. J BoneJoint Surg Br. 2005;87-B:1012-18.
44. Tönnis D. Normal values of the hip joint for the evaluation ofx-rays in children and adults. Clin Orthop 1976;119:39-47
45. Lim SJ, Chung HW, Choi YL, et al. Operative treatment ofprimary synovial osteochondromatosis of the hip. J Bone JointSurg Am. 2006;88-A:2456-64.
46. Knoeller SM. Synovial osteochondromatosis of the hip joint:
39
Differential diagnosis of a painful hip
etiology, diagnostic investigation and therapy. Acta OrthopBelg 2001;67:201-10.
47. Brennan D, O’Connell MJ, Ryan M, Cunningham P, Taylor D,Cronin C, O’Neill P, Eustace S. Secondary cleft sign as amarker of injury in athletes with groin pain: MR image appear-ance and interpretation. Radiology. 2005 Apr;235(1):162-7.
48. Krishnamurthy G, Connolly BL, Narayanan U, Babyn PS. Im-aging findings in external snapping hip syndrome. Pediatr Ra-diol. 2007 Dec;37(12):1272-4.
49. Chan YS, Lien LC, Hsu HL, Wan YL, Lee MS, Hsu KY, ShihCH. Evaluating hip labral tears using magnetic resonancearthrography: a prospective study comparing hip arthroscopyand magnetic resonance arthrography diagnosis. Arthroscopy.2005;21:1250.
50. Toomayan GA, Holman WR, Major NM, Kozlowicz SM, VailTP. Sensitivity of MR arthrography in the evaluation of acetab-ular labral tears. AJR Am J Roentgenol. 2006;186:449-53.
51. Bardakos NV, Villar RN. The ligamentum teres of the adulthip. J Bone Joint Surg Br. 2009;91-B:8-15.
52. Rao J, Zhou YX, Villar RN. Injury to the ligamentum teres.Mechanism, findings, and results of treatment. Clin SportsMed. 2001 Oct;20(4):791-9.
53. Crawford K, Philippon MJ, Sekiya JK, Rodkey WG, SteadmanJR. Microfracture of the hip in athletes. Clin Sports Med. 2006Apr;25(2):327-35.
54. Hayes CW, Conway WF, Daniel WW. MR imaging of bonemarrow edema pattern: transient osteoporosis, transient bonemarrow edema syndrome, or osteonecrosis. Radiographics.1993 Sep;13(5):1001-11.
55. Beaulé PE, Zaragoza E, Motamedi K, Copelan N, Dorey FJ.Three-dimensional computed tomography of the hip in the as-sessment of femoroacetabular impingement. J Orthop Res2005;23:1286-92.
56. Troelsen A., Mechlenburg I., Gelineck J., Bolvig L., JacobsenS. and Søballe K.. What is the role of clinical tests and ultra-sound in acetabular labral tear diagnostics? Acta Orthopaedi-ca 2009; 80 (3): 314–318.
57. Pelsser V, Cardinal E, Hobden R, Aubin B, Lafortune M. Ex-traarticular snapping hip: sonographic findings. AJR Am JRoentgenol. 2001 Jan;176(1):67-73.
58. Allen GM, Wilson DJ. Ultrasound in sports medicine – a crit-ical evaluation. Eur J Radiol. 2007;62:79-85.
59. Sonkar GK, Usha, Singh S. Is HLA-B27 a useful test in the di-agnosis of juvenile spondyloarthropathies? Singapore Med J.2008 Oct;49(10):795-9.
60. Cauli A, Dessole G, Fiorillo MT, Vacca A, Mameli A, Bitti P,Passiu G, Sorrentino R, Mathieu A. Increased level of HLA-B27 expression in ankylosing spondylitis patients comparedwith healthy HLA-B27-positive subjects: a possible further
40
Chapter 2

susceptibility factor for the development of disease. Rheuma-tology (Oxford). 2002 Dec;41(12):1375-9.
61. Troum O. M., Crues J. V., The Young Adult With Hip Pain:Diagnosis and Medical
Treatment, Circa 2004. Clin Orthop 2004;418:9-17.62. Deshmukh AJ, Thakur RR, Goyal A, Klein DA, Ranawat AS,
Rodriguez JA. Accuracy of diagnostic injection in differentiat-ing source of atypical hip pain. J Arthroplasty. 2010 Sep;25(6Suppl):129-33. Epub 2010 May 31.
63. Illgen RL 2nd, Honkamp NJ, Weisman MH, Hagenauer ME,Heiner JP, Anderson PA. The Diagnostic and Predictive Valueof Hip Anesthetic Arthrograms in Selected Patients Before To-tal Hip Arthroplasty. J Arthroplasty. 2006 Aug;21(5):724-30.
41
Differential diagnosis of a painful hip

LANDMARKS AND TOPOGRAPHIC ANATOMY OF THE HIP JOINT
Surface landmarks around the hip joint and their relationshipto anatomic structures around the hip joint are the corner stone ofhip arthroscopy. Understanding portal placement in relation tothese landmarks and the anatomic structures around the portalpath in every anatomic layer is paramount in the performance ofsafe and successful hip arthroscopy.
The most important and apparent skin landmarks around thehip joint are the greater trochanter and the anterior superior iliacspine. When hip arthroscopy is performed the greater trochanterand the anterior superior iliac spine should be marked before thecase is started (Fig. 1).
In hip arthroscopy, the hip joint is divided in two main com-partments: the central and peripheral compartment. The centralcompartment can be only accessed with traction to produce sepa-ration between the acetabulum and the femoral head (1, 2). Thecentral compartment contains the acetabular articular cartilage,the acetabular labrum, the acetabular fossa and its contents andmost of the femoral head. The peripheral compartment, which isusually accessed without traction, is extraarticular but intracapsu-lar, and contains part of the femoral head, the femoral neck, thehip capsule, its synovial folds and the zona orbicularis (3). A thirdcompartment around the hip joint has been recently described asthe peritrochanteric space (4), which is located lateral to thegreater trochanter under the iliotibial band.
Byrd performed a cadaveric antomic study and described therelation of the classic central compartment portals, skin landmarksand the anatomic structures around the hip joint (5). According toByrd, the anterolateral portal is situated at the superior anteriorcorner of the greater trochanter, the posterolateral portal is situat-ed at the posterior superior corner of the greater trochanter andthe direct anterior portal is at the intersection of a horizontal linecoming anteriorly fro the tip of the greater trochanter and a verti-
43
Chapter 3ARTHROSCOPIC ANATOMY OF THE HIP JOINTVictor M. Ilizaliturri Alexander Tomic Loftkjaer

cal line coming down from the anterior superior iliac spine. Thesciatic nerve lies about 1.5cm posterior to the posterior aspect ofthe greater trochanter. The femoral neurovascular bundle lies me-dial to the vertical line coming down from the anterior superior il-iac spine. Two or three branches of the lateral femorocutaneousnerve lie at the site of the direct anterior portal (the lateralfemorocutaneous nerve is the structure which is at most risk of in-jury by puncture when portals are established). Because the an-terolateral portal lays most centrally in the safe zone (between theposterior aspect of the greater trochanter and a vertical line com-ing down from the anterior superior iliac spine) it is always thefirst established. The anterolateral portal penetrates the gluteusmedius before entering the lateral aspect of the hip capsule at its
44
Chapter 3
Figure 1
Clinical photograph that demonstrates the position of surface landmarks and portals in aright hip. The patient is positioned lateral. The greater trochanter (GT) and anterior supe-rior iliac spine (ASIS) have been outlined. The anterolateral (AL) and posterolateral (PL)portals are located at the anterior superior and posterior superior corners of the tip ofthe greater trochanter (GT). One centimeter lateral to the crossing of a vertical line com-ing down from the anterior superior iliac spine (ASIS) and a horizontal line directed an-teriorly from the tip of the greater trochanter (GT) is the direct anterior portal (DA). Ac-cessory portals are presented using white dots. The proximal anterolateral accessory por-tal (PALA), mid-anterior portal (MAP), proximal mid-anterior portal (PMAP), the per-itrochanteric space portal (PSP) and the distal anterolateral accessory portal (DALA) aredemonstrated.
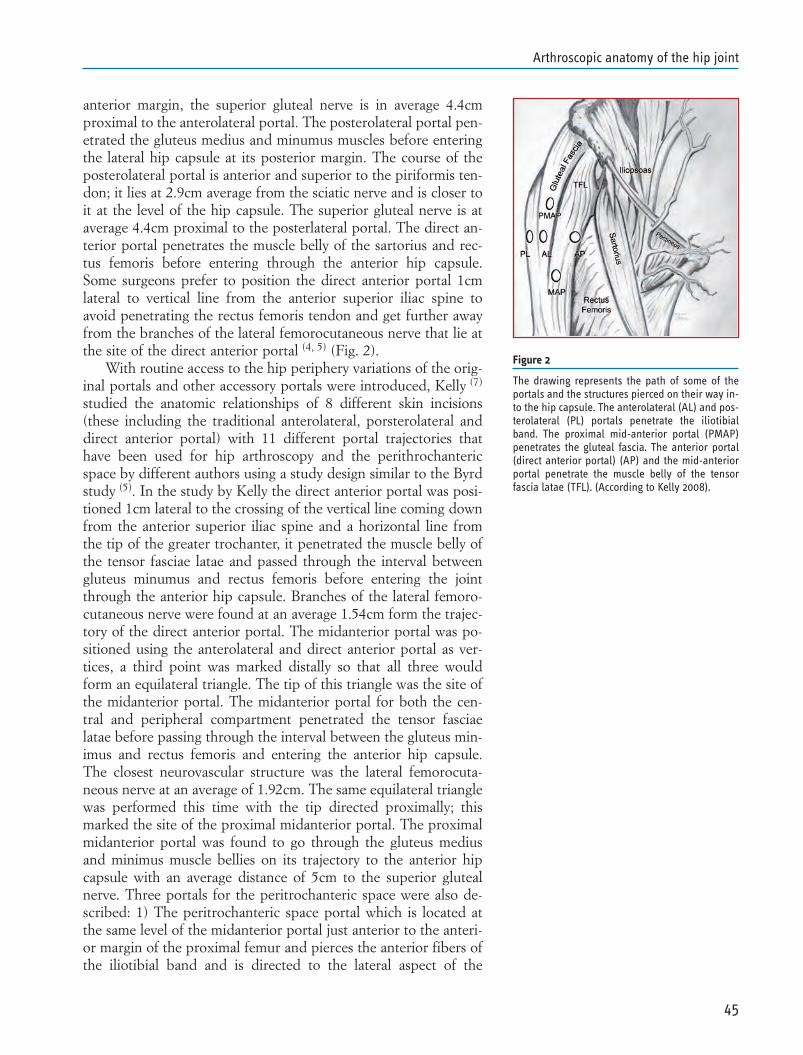
anterior margin, the superior gluteal nerve is in average 4.4cmproximal to the anterolateral portal. The posterolateral portal pen-etrated the gluteus medius and minumus muscles before enteringthe lateral hip capsule at its posterior margin. The course of theposterolateral portal is anterior and superior to the piriformis ten-don; it lies at 2.9cm average from the sciatic nerve and is closer toit at the level of the hip capsule. The superior gluteal nerve is ataverage 4.4cm proximal to the posterlateral portal. The direct an-terior portal penetrates the muscle belly of the sartorius and rec-tus femoris before entering through the anterior hip capsule.Some surgeons prefer to position the direct anterior portal 1cmlateral to vertical line from the anterior superior iliac spine toavoid penetrating the rectus femoris tendon and get further awayfrom the branches of the lateral femorocutaneous nerve that lie atthe site of the direct anterior portal (4, 5) (Fig. 2).
With routine access to the hip periphery variations of the orig-inal portals and other accessory portals were introduced, Kelly (7)
studied the anatomic relationships of 8 different skin incisions(these including the traditional anterolateral, porsterolateral anddirect anterior portal) with 11 different portal trajectories thathave been used for hip arthroscopy and the perithrochantericspace by different authors using a study design similar to the Byrdstudy (5). In the study by Kelly the direct anterior portal was posi-tioned 1cm lateral to the crossing of the vertical line coming downfrom the anterior superior iliac spine and a horizontal line fromthe tip of the greater trochanter, it penetrated the muscle belly ofthe tensor fasciae latae and passed through the interval betweengluteus minumus and rectus femoris before entering the jointthrough the anterior hip capsule. Branches of the lateral femoro-cutaneous nerve were found at an average 1.54cm form the trajec-tory of the direct anterior portal. The midanterior portal was po-sitioned using the anterolateral and direct anterior portal as ver-tices, a third point was marked distally so that all three wouldform an equilateral triangle. The tip of this triangle was the site ofthe midanterior portal. The midanterior portal for both the cen-tral and peripheral compartment penetrated the tensor fasciaelatae before passing through the interval between the gluteus min-imus and rectus femoris and entering the anterior hip capsule.The closest neurovascular structure was the lateral femorocuta-neous nerve at an average of 1.92cm. The same equilateral trianglewas performed this time with the tip directed proximally; thismarked the site of the proximal midanterior portal. The proximalmidanterior portal was found to go through the gluteus mediusand minimus muscle bellies on its trajectory to the anterior hipcapsule with an average distance of 5cm to the superior glutealnerve. Three portals for the peritrochanteric space were also de-scribed: 1) The peritrochanteric space portal which is located atthe same level of the midanterior portal just anterior to the anteri-or margin of the proximal femur and pierces the anterior fibers ofthe iliotibial band and is directed to the lateral aspect of the
45
Arthroscopic anatomy of the hip joint
Figure 2
The drawing represents the path of some of theportals and the structures pierced on their way in-to the hip capsule. The anterolateral (AL) and pos-terolateral (PL) portals penetrate the iliotibialband. The proximal mid-anterior portal (PMAP)penetrates the gluteal fascia. The anterior portal(direct anterior portal) (AP) and the mid-anteriorportal penetrate the muscle belly of the tensorfascia latae (TFL). (According to Kelly 2008).
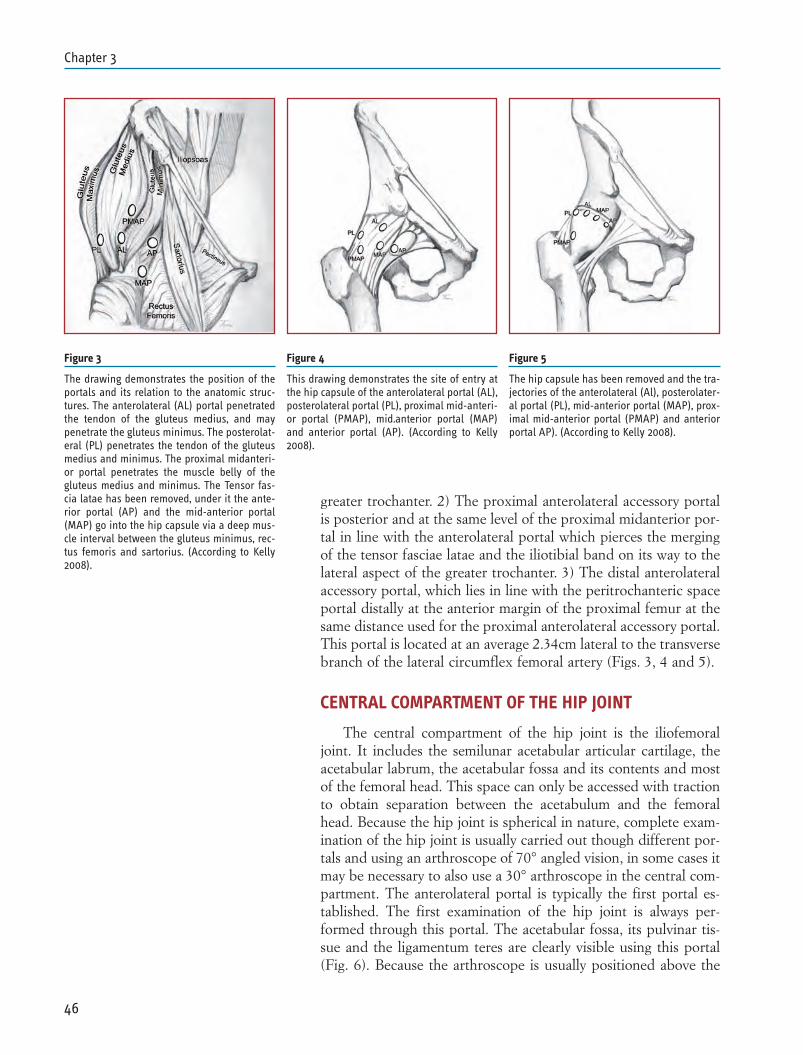
greater trochanter. 2) The proximal anterolateral accessory portalis posterior and at the same level of the proximal midanterior por-tal in line with the anterolateral portal which pierces the mergingof the tensor fasciae latae and the iliotibial band on its way to thelateral aspect of the greater trochanter. 3) The distal anterolateralaccessory portal, which lies in line with the peritrochanteric spaceportal distally at the anterior margin of the proximal femur at thesame distance used for the proximal anterolateral accessory portal.This portal is located at an average 2.34cm lateral to the transversebranch of the lateral circumflex femoral artery (Figs. 3, 4 and 5).
CENTRAL COMPARTMENT OF THE HIP JOINT
The central compartment of the hip joint is the iliofemoraljoint. It includes the semilunar acetabular articular cartilage, theacetabular labrum, the acetabular fossa and its contents and mostof the femoral head. This space can only be accessed with tractionto obtain separation between the acetabulum and the femoralhead. Because the hip joint is spherical in nature, complete exam-ination of the hip joint is usually carried out though different por-tals and using an arthroscope of 70° angled vision, in some cases itmay be necessary to also use a 30° arthroscope in the central com-partment. The anterolateral portal is typically the first portal es-tablished. The first examination of the hip joint is always per-formed through this portal. The acetabular fossa, its pulvinar tis-sue and the ligamentum teres are clearly visible using this portal(Fig. 6). Because the arthroscope is usually positioned above the
46
Chapter 3
Figure 3
The drawing demonstrates the position of theportals and its relation to the anatomic struc-tures. The anterolateral (AL) portal penetratedthe tendon of the gluteus medius, and maypenetrate the gluteus minimus. The posterolat-eral (PL) penetrates the tendon of the gluteusmedius and minimus. The proximal midanteri-or portal penetrates the muscle belly of thegluteus medius and minimus. The Tensor fas-cia latae has been removed, under it the ante-rior portal (AP) and the mid-anterior portal(MAP) go into the hip capsule via a deep mus-cle interval between the gluteus minimus, rec-tus femoris and sartorius. (According to Kelly2008).
Figure 4
This drawing demonstrates the site of entry atthe hip capsule of the anterolateral portal (AL),posterolateral portal (PL), proximal mid-anteri-or portal (PMAP), mid.anterior portal (MAP)and anterior portal (AP). (According to Kelly2008).
Figure 5
The hip capsule has been removed and the tra-jectories of the anterolateral (Al), posterolater-al portal (PL), mid-anterior portal (MAP), prox-imal mid-anterior portal (PMAP) and anteriorportal AP). (According to Kelly 2008).

acetabular fossa when initially inserted, the acetabular fossa andits contents are frequently the first image obtained from the insideof the hip joint. The medial and superior aspects of the femoralhead are also visible. By turning the vision of the arthroscope pos-teriorly and anteriorly the posterior acetabulum and posteriorlabrum and the anterior acetabulum and anterior labrum are visu-alized (Fig. 7). The next portals are typically established using di-rect arthroscopic vision. For direct anterior portal the so calledanterior femoral triangle must be identified; the triangle is formedby the free margin of the anterior labrum, the femoral head andthe lateral limit of the field of vision. The area in the center of thetriangle is the anterior hip capsule and the site of entry of thespinal needle for portal establishment. Once the anterior portal isestablished a capsulotomy, which is performed parallel to thelabral margin is usually performed to increase mobility of instru-ments in the joint and provide easy access to the capsular side ofthe labrum (Fig. 8). If a posterolateral portal is used it can be es-tablished by turning the vision of the arthroscope lateral to locatethe free margin of the lateral labrum, this requires pulling thescope lateral and the surgeon should be careful not to pull-out thearthroscope from inside the hip capsule. Once the free margin ofthe lateral labrum is visible, the needle can be advanced throughthe posterolateral portal into the hip joint between the free marginof the labrum and the femoral head (Fig. 9). By changing theviewing portal to the direct anterior portal the best image of thelateral labrum, lateral hip capsule and the lateral surface of thefemoral head is obtained. From this view it is also easier to assist
47
Arthroscopic anatomy of the hip joint
Figure 6
Arthroscopic photograph in a right hip.The anterolateral portal is the viewingportal with a 70° arthroscope in this pho-tograph. The femoral head (FH) is at thebottom. The ligamentum teres (LT) and itsattachments to the femoral head and infe-rior acetabular fossa are observed. Pulv-inar tissue (P) is observed proximal to theligamentum teres (LT) inside the acetabu-lar fossa. A radiofrequency probe is beinginserted from the direct anterior portal.
Figure 7
Arthroscopic photograph, the anterolater-al portal is the viewing portal with a 70°arthroscope. The vision is directed anteri-orly to view the anterior acetabulum (AA)and the anterior labrum (L). A cartilagedelamination lesion (CD) without a tear isobserved on the anterior acetabulum(AA). To the bottom the femoral head (FH)is observed. The acetabular fossa (AF) isto the left.

placement of the posterolateral portal if difficulties are encoun-tered (Fig. 10). One should remember that the spherical nature ofthe hip joint may complicate instrument passage and access to theareas of pathology, in other words, because of the 70° angulationof the arthroscopic vision, most of the central compartment canbe explored from any of the central compartment portals, but get-ting an instrument to the area of pathology may require to try ac-cess from different portals to obtain different trajectories and theuse of angle, curved of bendable instruments.
48
Chapter 3
Figure 8
Sequence of arthroscopic photographs demonstrating establishment of the direct anteri-or portal in a right hip. A 70° arthroscope is in position at the anterolateral portal withthe vision directed anteriorly. A) The so called anterior triangle is observed. B) The supe-rior limit of the anterior triangle is the free margin of the anterior labrum (L), the inferi-or limit is the femoral head (FH) and the lateral limit is the limit of the field of vision. Thesurface area of the triangle (in white) is the hip capsule. C) A needle is introduced at thedirect anterior portal. Inside the hip it enters through the anterior triangle piercing theanterior hip capsule (AC) between the free margin of the anterior labrum (L) and thefemoral head. D) A capsulotomy is performed on the anterior hip capsule (HC) to increaseinstrument mobility and facilitate instrument interchange. The anterior labrum (L) andthe femoral head (FH) are to the left.
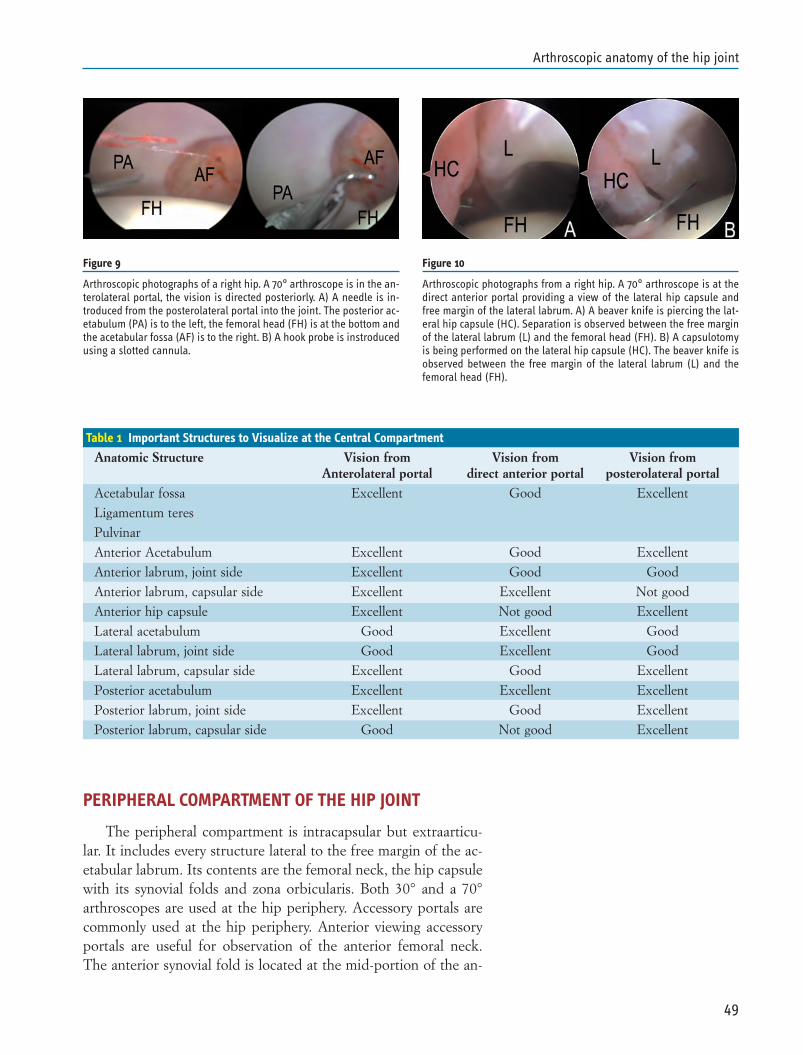
PERIPHERAL COMPARTMENT OF THE HIP JOINT
The peripheral compartment is intracapsular but extraarticu-lar. It includes every structure lateral to the free margin of the ac-etabular labrum. Its contents are the femoral neck, the hip capsulewith its synovial folds and zona orbicularis. Both 30° and a 70°arthroscopes are used at the hip periphery. Accessory portals arecommonly used at the hip periphery. Anterior viewing accessoryportals are useful for observation of the anterior femoral neck.The anterior synovial fold is located at the mid-portion of the an-
49
Arthroscopic anatomy of the hip joint
Figure 9
Arthroscopic photographs of a right hip. A 70° arthroscope is in the an-terolateral portal, the vision is directed posteriorly. A) A needle is in-troduced from the posterolateral portal into the joint. The posterior ac-etabulum (PA) is to the left, the femoral head (FH) is at the bottom andthe acetabular fossa (AF) is to the right. B) A hook probe is instroducedusing a slotted cannula.
Figure 10
Arthroscopic photographs from a right hip. A 70° arthroscope is at thedirect anterior portal providing a view of the lateral hip capsule andfree margin of the lateral labrum. A) A beaver knife is piercing the lat-eral hip capsule (HC). Separation is observed between the free marginof the lateral labrum (L) and the femoral head (FH). B) A capsulotomyis being performed on the lateral hip capsule (HC). The beaver knife isobserved between the free margin of the lateral labrum (L) and thefemoral head (FH).
Table 1 Important Structures to Visualize at the Central Compartment
Anatomic Structure Vision from Vision from Vision fromAnterolateral portal direct anterior portal posterolateral portal
Acetabular fossa Excellent Good Excellent
Ligamentum teres
Pulvinar
Anterior Acetabulum Excellent Good Excellent
Anterior labrum, joint side Excellent Good Good
Anterior labrum, capsular side Excellent Excellent Not good
Anterior hip capsule Excellent Not good Excellent
Lateral acetabulum Good Excellent Good
Lateral labrum, joint side Good Excellent Good
Lateral labrum, capsular side Excellent Good Excellent
Posterior acetabulum Excellent Excellent Excellent
Posterior labrum, joint side Excellent Good Excellent
Posterior labrum, capsular side Good Not good Excellent
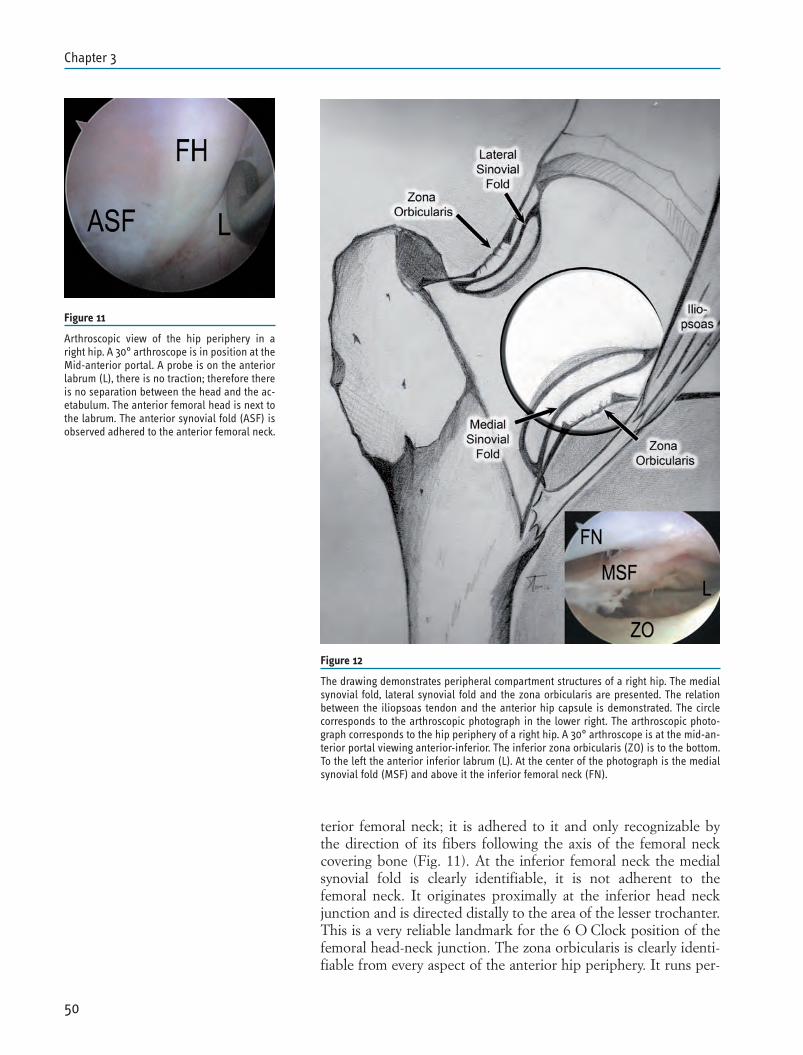
terior femoral neck; it is adhered to it and only recognizable bythe direction of its fibers following the axis of the femoral neckcovering bone (Fig. 11). At the inferior femoral neck the medialsynovial fold is clearly identifiable, it is not adherent to thefemoral neck. It originates proximally at the inferior head neckjunction and is directed distally to the area of the lesser trochanter.This is a very reliable landmark for the 6 O Clock position of thefemoral head-neck junction. The zona orbicularis is clearly identi-fiable from every aspect of the anterior hip periphery. It runs per-
50
Chapter 3
Figure 11
Arthroscopic view of the hip periphery in aright hip. A 30° arthroscope is in position at theMid-anterior portal. A probe is on the anteriorlabrum (L), there is no traction; therefore thereis no separation between the head and the ac-etabulum. The anterior femoral head is next tothe labrum. The anterior synovial fold (ASF) isobserved adhered to the anterior femoral neck.
Figure 12
The drawing demonstrates peripheral compartment structures of a right hip. The medialsynovial fold, lateral synovial fold and the zona orbicularis are presented. The relationbetween the iliopsoas tendon and the anterior hip capsule is demonstrated. The circlecorresponds to the arthroscopic photograph in the lower right. The arthroscopic photo-graph corresponds to the hip periphery of a right hip. A 30° arthroscope is at the mid-an-terior portal viewing anterior-inferior. The inferior zona orbicularis (ZO) is to the bottom.To the left the anterior inferior labrum (L). At the center of the photograph is the medialsynovial fold (MSF) and above it the inferior femoral neck (FN).

pendicular to the direction of the femoral neck and forms an hourglass shape narrowing of the hip capsule around the mid portionof the length of the femoral neck. Arthroscopically it looks like acircumferential narrowing of the space around the femoral neck.The medial sinovial fold is in close relation with the zona orbicu-laris at the inferior femoral neck (Fig. 12). Behind the anterior hipcapsule between the zona orbucularis and the anterior-inferiorlabrum is the iliopsoas bursa containing the iliopsoas tendon. Insome patients there is a normal communication between the bur-sa and the hip capsule (Fig. 13). Proximal to the lateral femoralneck is the lateral synovial fold; this fold runs from the greatertrochanter upward along the lateral margin of the neck to the lat-eral femoral head neck junction (Fig. 14). The lateral synovial foldis a reliabable landmark of the lateral femoral epiphyseal vesselsthat provide the most important blood supply to the femoralhead.
PERITROCHANTERIC SPACE
The peritrochanteric space of the hip corresponds to the virtu-al space beneath the fascia and over the muscle layer (4). Thisspace does not naturally connect to the intrarticular space of thehip, and thus, the technique corresponds to an endoscopy ratherthan an arthroscopy. The virtual space is dilated by the entrance offluid during the intervention allowing the visualization of existingstructures. Anatomical structures that may be assessed by this pro-cedure include muscles (Short external rotators, Gluteus max-imus, gluteus medius, gluteus minimus, vastus lateralis, tensor fas-cia lata), bursas (greater trochanteric bursa), fascia (iliotibialband), and bony structures (greater trochanter, linea aspera, lesser
51
Arthroscopic anatomy of the hip joint
Figure 13
Arthroscopic photograph of a right hip. A30° arthroscope is at the midanterior por-tal. The probe is between the medial syn-ovial fold (MSF) and the femoral neck(FN). The zona orbicularis is not visiblebecause it is behind the scope. The iliop-soas tendon (PT) can be observed throughthe very thin anterior hip capsule.
Figure 14
Arthroscopic photograph of a right hip. A30° arthroscope is in the proximal mid-anterior portal. TheFemoral neck (FN) isat the bottom of the photograph.

trochanter). Access to these different structures is gained throughspecifically placed portals.
Two different techniques have been described to access thiscompartment: 1) Access is obtained by a window created on theiliotibial band (8, 9). For this procedure endoscopy begins lateral tothe iliotibial band and the peritrochanteric space is only accessedafter a defect is created lateral to the greater trochanter. Greatertrochanteric bursa is identified through the defect on the fascia.When a decompression of the iliotibial band is indicated the re-lease is part of the treatment and it can be used for access. Thevastus lateralis tendon and the gluteus medius can only be visual-ized after the bursa is removed (Fig. 15). 2) Access is obtained byestablishing portals that pierce the iliotibial band (4). This elimi-nates the need to create a defect on the iliotibial band. Whenthere is no need to release the iliotibial band this technique avoidscrating a defect on it.
52
Chapter 3
Figure 15
Endoscopic series of photographs from the peritrocchanteric space in a right hip. A 30° arthroscope is in a distal trochanteric portal. A) A small el-liptical window has been created on the iliotibial band lateral (ITB) to the greater trocanter. The greater trochanteric bursa is visualized throughthe defect. B) After resection of the bursa, the vastus lateralis (VL) is at the bottom, the greater trochanter is at the center under the conjoint ten-don and the insertion of the gluteus medius (GM) is at the top. A shaver is in use to complete bursal resection. C) A probe is used top inspect themuscle fibers of the gluteus medius (GM) proximal to the greater trochanter.
REFERENCES
1. Dienst M, Seil R, Gödde S, Brang M, Becker K, Georg T,Kohn D. Effects of traction, distension and joint position ondistraction of the hip joint: an experimental study in cadavers.Arthroscopy 2002; 18: 865-871.
2. Byrd JW, Chern KY. Traction versus distension for distractionof the hip joint during hip arthroscopy. Arthroscopy 1997; 13:346-349.
3. Dienst M, Godde S, Seil R, el al. Hip arthroscopy withouttraction in vivo anatomy of the peripheral joint cavity.Arthroscopy 2001; 17: 924-931.
4. Voos JE, Rudzki JR, Shindle MK, Martin H, Kelly BT. Arthro-scopic anatomy and surgical techniques for peritrochantericspace disorders in the hip. Arthroscopy 2007; 23: 1246e1-e5.
5. Byrd JWT, Pappas JN, Pedley MJ: Hip arthroscopy: ananatomic study of portal placement and relationship to the ex-traarticular structures. Arthroscopy 11:418-423, 1995.
6. Ilizaliturri VM Jr, Mangino G, Valero FS, Camacho-Galindo J.Hip arthroscopy of the central and peripheral compartmentby the lateral approach. Tech Orthop 2005; 20: 32-36.
7. Robertson WJ, Kelly BT. The safe zone for hip arthroscopy: acadevirc assessment of central, peripheral and lateral compart-ment portal placement. Arthroscopy 2008; 24: 1019-1026.
8. Ilizaliturri VM Jr, Martinez-Escalante FA, Chaidez PA, Cama-cho-Galindo J. Endoscopic iliotibial band release for externalsnapping hip syndrome. Arthroscopy 2006; 22: 505-510.
9. Baker CL, Massie V, Hurt G, Savory CG. Arthroscopic bur-sectomy for recalcitrant trochanteric bursistis. Arthroscopy(2007). 23: 827-832.
53
Arthroscopic anatomy of the hip joint


INTRODUCTION
Arthroscopy of the hip can be effectively performed with thepatient in either the supine or lateral position. The choice is large-ly dictated by the surgeon’s personal preference. The merits of thesupine position are outlined as follows. Positioning of the patientis simple and can be accomplished in just a few minutes. The pro-cedure can be performed on virtually any standard fracture tablewith an orientation to the joint that is familiar to orthopaedic sur-geons accustomed to managing hip fractures. With this position,the layout of the operating room is user-friendly for the surgeon,assistants, and operating room staff. There is reliable access for allstandard portal placements and it easily accommodates reposition-ing for arthroscopy of the peripheral compartment as well as iliop-soas bursoscopy to access the iliopsoas tendon. A final importantadvantage of the supine position regards intraabdominal fluid ex-travasation. This is a potentially serious complication of hiparthroscopy and has been reported only in the lateral position (1,
2). With the patient on their side, the abdominal and pelvic cavitylie in a dependent position, creating a reservoir into which gravityflow will allow fluid to collect.
The hip joint has both an intraarticular and a peripheral com-partment. Most hip pathology is found within the intraarticularregion; therefore, distraction is necessary to achieve arthroscopicaccess. Performing hip arthroscopy without traction has not beenpopular because it does not allow access to the intraarticular re-gion. However, it is now recognized that this method can be a use-ful adjunct to the traction technique (3, 4). Hip flexion relaxes thecapsule and allows access to the peripheral compartment, which isintracapsular, but extraarticular. Numerous lesions are encoun-tered in this area that may be overlooked with traction alone, suchas synovial disease and free-floating loose bodies. Femoral sidedimpingement lesions (cam impingement) are best addressed fromthe peripheral compartment. Hip flexion also allows generous ac-cess to the capsule for plication or thermal modulation.
55
Chapter 4THE SUPINE POSITIONJ. W. Thomas Byrd

DICTUMS ON HIP ARTHROSCOPY
Regardless of the position or technique that is chosen for per-forming this procedure, there are several dictums that should bethoroughly understood. First, a successful outcome is most clearlydependent on proper patient selection. A technically well execut-ed procedure will fail when performed for the wrong reason. Thismay include failure of the procedure to meet the patient’s expec-tations. Secondly, the patient must be properly positioned in orderfor the case to go well. Poor positioning will assure a difficult pro-cedure. Thirdly, simply gaining access to the hip joint is not anoutstanding technical accomplishment. The paramount issue is ac-cessing the joint in as atraumatic a fashion as possible. Due to itsconstrained architecture and dense soft tissue envelope, the po-tential for inadvertent iatrogenic scope trauma is significant and,perhaps to some extent, unavoidable. Thus, every reasonable stepshould be taken to keep this concern to a minimum. Perform theprocedure as carefully as possible and be certain that it is beingperformed for the right reason.
OR SET-UPAnesthesia
The procedure is performed as an out-patient under generalanesthesia. Epidural is an appropriate alternative, but requires anadequate motor block to ensure muscle relaxation.
Patient Positioning
A fracture table can be used, or a versatile distractor has beendeveloped that can be adapted to a standard OR table. The pa-tient is positioned supine. An oversized (12cm outer diameter)formed urethane perineal post is used. This is positioned laterallyagainst the medial thigh of the operative leg (Fig. 1). Lateralizingthe perineal post adds a slight transverse component to the direc-tion of the traction vector (Fig. 2). It also distances the post fromthe area of the pudendal nerve, lessening the risk of compressionneuropraxia.
The operative hip is positioned in extension and approximate-ly 25° of abduction. Slight flexion might relax the capsule and fa-cilitate distraction, but excessive flexion should be avoided be-cause it places tension on the sciatic nerve and may increase therisk of traction neuropraxia. Neutral rotation of the extremity dur-ing portal placement is important for proper orientation but free-dom of rotation of the foot plate during the procedure facilitatesvisualization of the femoral head.
The contralateral extremity is abducted as necessary to ac-commodate positioning of the image intensifier between the legs.Prior to distracting the operative hip, slight traction is applied tothe non-operative leg. This stabilizes the torso on the table and
56
Chapter 4
Figure 1
The patient is positioned on the fracture table sothat the perineal post is placed as far laterally aspossible towards the operative hip resting againstthe medial thigh. (Reprinted with permission J.W.Thomas Byrd, M.D.)
Figure 2
The optimal vector for distraction is oblique rela-tive to the axis of the body and more closely coin-cides with the axis of the femoral neck than thefemoral shaft. This oblique vector is partially cre-ated by abduction of the hip and partially accentu-ated by a small transverse component to the vec-tor. (Reprinted with permission J.W. Thomas Byrd,M.D.)
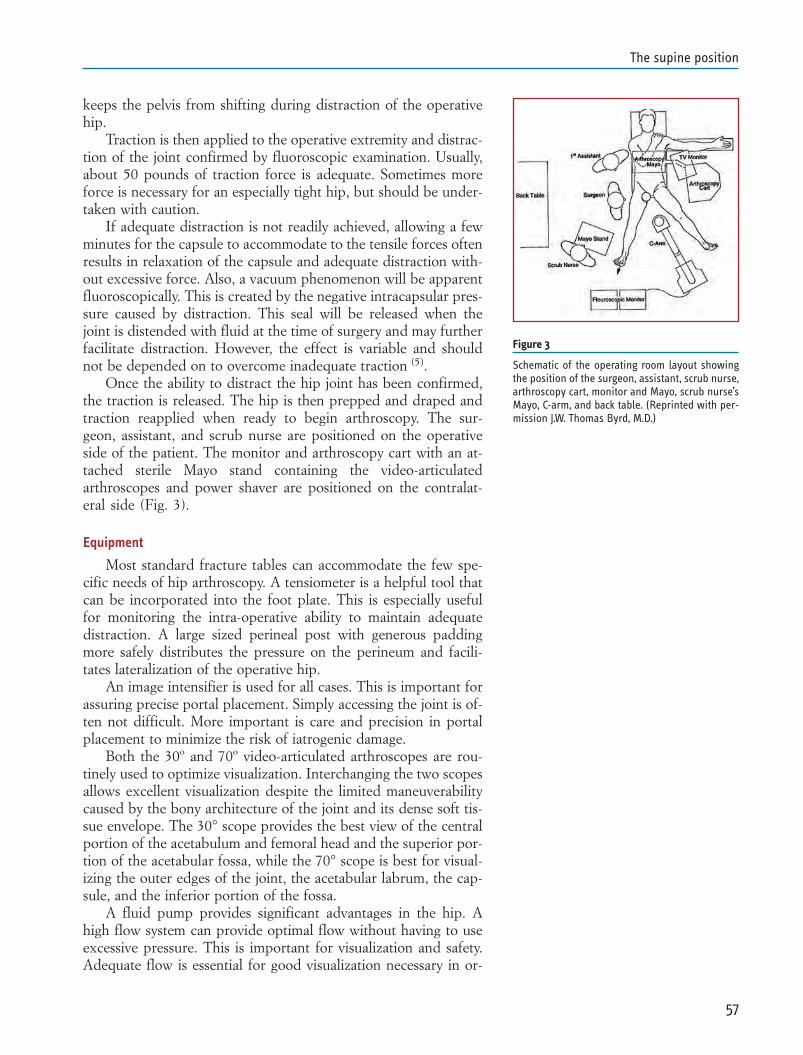
keeps the pelvis from shifting during distraction of the operativehip.
Traction is then applied to the operative extremity and distrac-tion of the joint confirmed by fluoroscopic examination. Usually,about 50 pounds of traction force is adequate. Sometimes moreforce is necessary for an especially tight hip, but should be under-taken with caution.
If adequate distraction is not readily achieved, allowing a fewminutes for the capsule to accommodate to the tensile forces oftenresults in relaxation of the capsule and adequate distraction with-out excessive force. Also, a vacuum phenomenon will be apparentfluoroscopically. This is created by the negative intracapsular pres-sure caused by distraction. This seal will be released when thejoint is distended with fluid at the time of surgery and may furtherfacilitate distraction. However, the effect is variable and shouldnot be depended on to overcome inadequate traction (5).
Once the ability to distract the hip joint has been confirmed,the traction is released. The hip is then prepped and draped andtraction reapplied when ready to begin arthroscopy. The sur-geon, assistant, and scrub nurse are positioned on the operativeside of the patient. The monitor and arthroscopy cart with an at-tached sterile Mayo stand containing the video-articulatedarthroscopes and power shaver are positioned on the contralat-eral side (Fig. 3).
Equipment
Most standard fracture tables can accommodate the few spe-cific needs of hip arthroscopy. A tensiometer is a helpful tool thatcan be incorporated into the foot plate. This is especially usefulfor monitoring the intra-operative ability to maintain adequatedistraction. A large sized perineal post with generous paddingmore safely distributes the pressure on the perineum and facili-tates lateralization of the operative hip.
An image intensifier is used for all cases. This is important forassuring precise portal placement. Simply accessing the joint is of-ten not difficult. More important is care and precision in portalplacement to minimize the risk of iatrogenic damage.
Both the 30º and 70º video-articulated arthroscopes are rou-tinely used to optimize visualization. Interchanging the two scopesallows excellent visualization despite the limited maneuverabilitycaused by the bony architecture of the joint and its dense soft tis-sue envelope. The 30° scope provides the best view of the centralportion of the acetabulum and femoral head and the superior por-tion of the acetabular fossa, while the 70° scope is best for visual-izing the outer edges of the joint, the acetabular labrum, the cap-sule, and the inferior portion of the fossa.
A fluid pump provides significant advantages in the hip. Ahigh flow system can provide optimal flow without having to useexcessive pressure. This is important for visualization and safety.Adequate flow is essential for good visualization necessary in or-
57
The supine position
Figure 3
Schematic of the operating room layout showingthe position of the surgeon, assistant, scrub nurse,arthroscopy cart, monitor and Mayo, scrub nurse’sMayo, C-arm, and back table. (Reprinted with per-mission J.W. Thomas Byrd, M.D.)
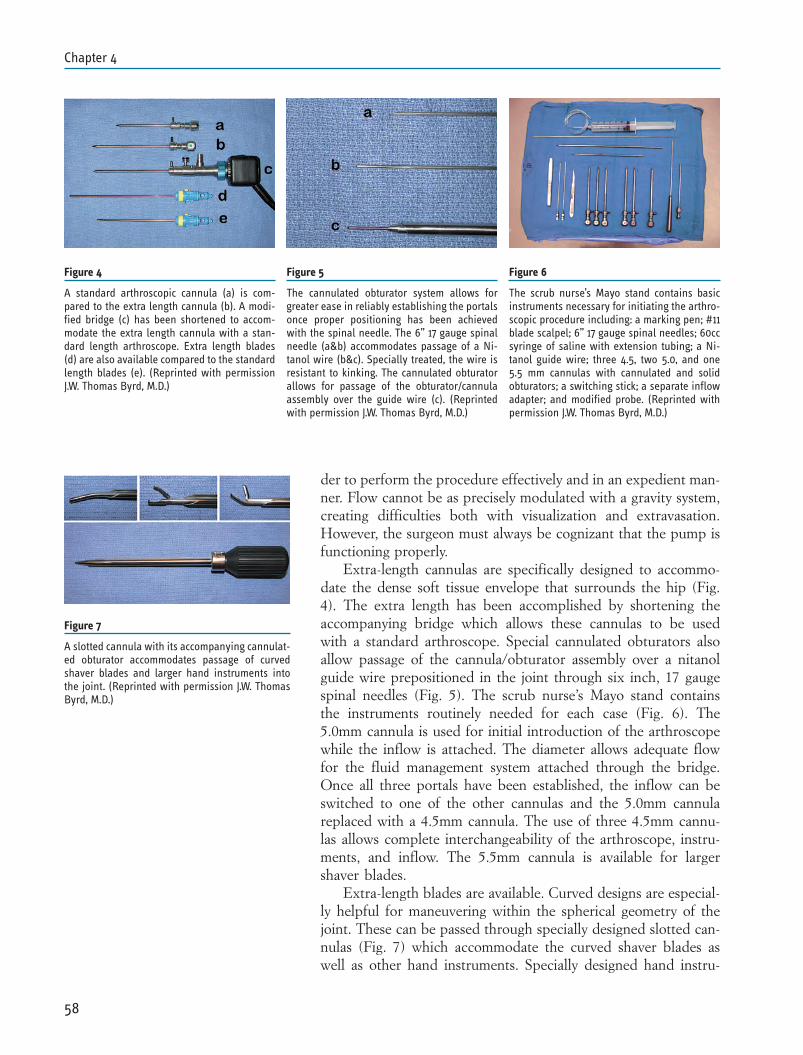
der to perform the procedure effectively and in an expedient man-ner. Flow cannot be as precisely modulated with a gravity system,creating difficulties both with visualization and extravasation.However, the surgeon must always be cognizant that the pump isfunctioning properly.
Extra-length cannulas are specifically designed to accommo-date the dense soft tissue envelope that surrounds the hip (Fig.4). The extra length has been accomplished by shortening theaccompanying bridge which allows these cannulas to be usedwith a standard arthroscope. Special cannulated obturators alsoallow passage of the cannula/obturator assembly over a nitanolguide wire prepositioned in the joint through six inch, 17 gaugespinal needles (Fig. 5). The scrub nurse’s Mayo stand containsthe instruments routinely needed for each case (Fig. 6). The5.0mm cannula is used for initial introduction of the arthroscopewhile the inflow is attached. The diameter allows adequate flowfor the fluid management system attached through the bridge.Once all three portals have been established, the inflow can beswitched to one of the other cannulas and the 5.0mm cannulareplaced with a 4.5mm cannula. The use of three 4.5mm cannu-las allows complete interchangeability of the arthroscope, instru-ments, and inflow. The 5.5mm cannula is available for largershaver blades.
Extra-length blades are available. Curved designs are especial-ly helpful for maneuvering within the spherical geometry of thejoint. These can be passed through specially designed slotted can-nulas (Fig. 7) which accommodate the curved shaver blades aswell as other hand instruments. Specially designed hand instru-
58
Chapter 4
Figure 4
A standard arthroscopic cannula (a) is com-pared to the extra length cannula (b). A modi-fied bridge (c) has been shortened to accom-modate the extra length cannula with a stan-dard length arthroscope. Extra length blades(d) are also available compared to the standardlength blades (e). (Reprinted with permissionJ.W. Thomas Byrd, M.D.)
Figure 5
The cannulated obturator system allows forgreater ease in reliably establishing the portalsonce proper positioning has been achievedwith the spinal needle. The 6” 17 gauge spinalneedle (a&b) accommodates passage of a Ni-tanol wire (b&c). Specially treated, the wire isresistant to kinking. The cannulated obturatorallows for passage of the obturator/cannulaassembly over the guide wire (c). (Reprintedwith permission J.W. Thomas Byrd, M.D.)
Figure 6
The scrub nurse’s Mayo stand contains basicinstruments necessary for initiating the arthro-scopic procedure including: a marking pen; #11blade scalpel; 6” 17 gauge spinal needles; 60ccsyringe of saline with extension tubing; a Ni-tanol guide wire; three 4.5, two 5.0, and one5.5 mm cannulas with cannulated and solidobturators; a switching stick; a separate inflowadapter; and modified probe. (Reprinted withpermission J.W. Thomas Byrd, M.D.)
Figure 7
A slotted cannula with its accompanying cannulat-ed obturator accommodates passage of curvedshaver blades and larger hand instruments intothe joint. (Reprinted with permission J.W. ThomasByrd, M.D.)
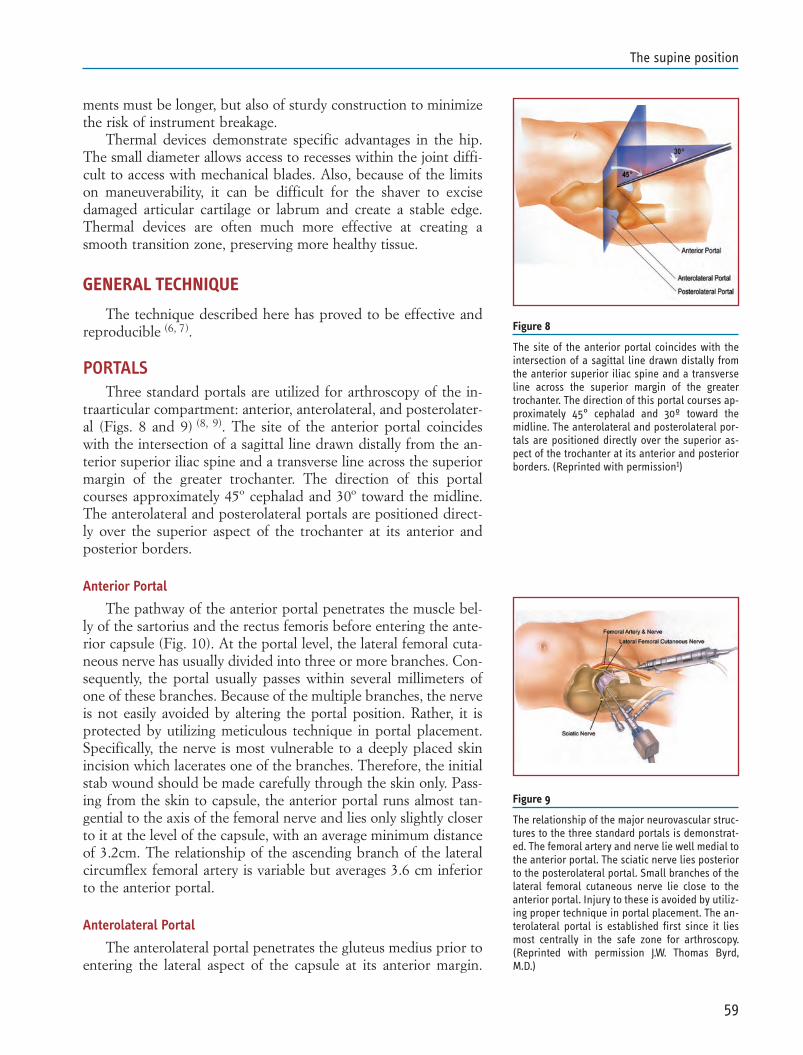
ments must be longer, but also of sturdy construction to minimizethe risk of instrument breakage.
Thermal devices demonstrate specific advantages in the hip.The small diameter allows access to recesses within the joint diffi-cult to access with mechanical blades. Also, because of the limitson maneuverability, it can be difficult for the shaver to excisedamaged articular cartilage or labrum and create a stable edge.Thermal devices are often much more effective at creating asmooth transition zone, preserving more healthy tissue.
GENERAL TECHNIQUE
The technique described here has proved to be effective andreproducible (6, 7).
PORTALSThree standard portals are utilized for arthroscopy of the in-
traarticular compartment: anterior, anterolateral, and posterolater-al (Figs. 8 and 9) (8, 9). The site of the anterior portal coincideswith the intersection of a sagittal line drawn distally from the an-terior superior iliac spine and a transverse line across the superiormargin of the greater trochanter. The direction of this portalcourses approximately 45º cephalad and 30º toward the midline.The anterolateral and posterolateral portals are positioned direct-ly over the superior aspect of the trochanter at its anterior andposterior borders.
Anterior Portal
The pathway of the anterior portal penetrates the muscle bel-ly of the sartorius and the rectus femoris before entering the ante-rior capsule (Fig. 10). At the portal level, the lateral femoral cuta-neous nerve has usually divided into three or more branches. Con-sequently, the portal usually passes within several millimeters ofone of these branches. Because of the multiple branches, the nerveis not easily avoided by altering the portal position. Rather, it isprotected by utilizing meticulous technique in portal placement.Specifically, the nerve is most vulnerable to a deeply placed skinincision which lacerates one of the branches. Therefore, the initialstab wound should be made carefully through the skin only. Pass-ing from the skin to capsule, the anterior portal runs almost tan-gential to the axis of the femoral nerve and lies only slightly closerto it at the level of the capsule, with an average minimum distanceof 3.2cm. The relationship of the ascending branch of the lateralcircumflex femoral artery is variable but averages 3.6 cm inferiorto the anterior portal.
Anterolateral Portal
The anterolateral portal penetrates the gluteus medius prior toentering the lateral aspect of the capsule at its anterior margin.
59
The supine position
Figure 8
The site of the anterior portal coincides with theintersection of a sagittal line drawn distally fromthe anterior superior iliac spine and a transverseline across the superior margin of the greatertrochanter. The direction of this portal courses ap-proximately 45° cephalad and 30º toward themidline. The anterolateral and posterolateral por-tals are positioned directly over the superior as-pect of the trochanter at its anterior and posteriorborders. (Reprinted with permission1)
Figure 9
The relationship of the major neurovascular struc-tures to the three standard portals is demonstrat-ed. The femoral artery and nerve lie well medial tothe anterior portal. The sciatic nerve lies posteriorto the posterolateral portal. Small branches of thelateral femoral cutaneous nerve lie close to theanterior portal. Injury to these is avoided by utiliz-ing proper technique in portal placement. The an-terolateral portal is established first since it liesmost centrally in the safe zone for arthroscopy.(Reprinted with permission J.W. Thomas Byrd,M.D.)
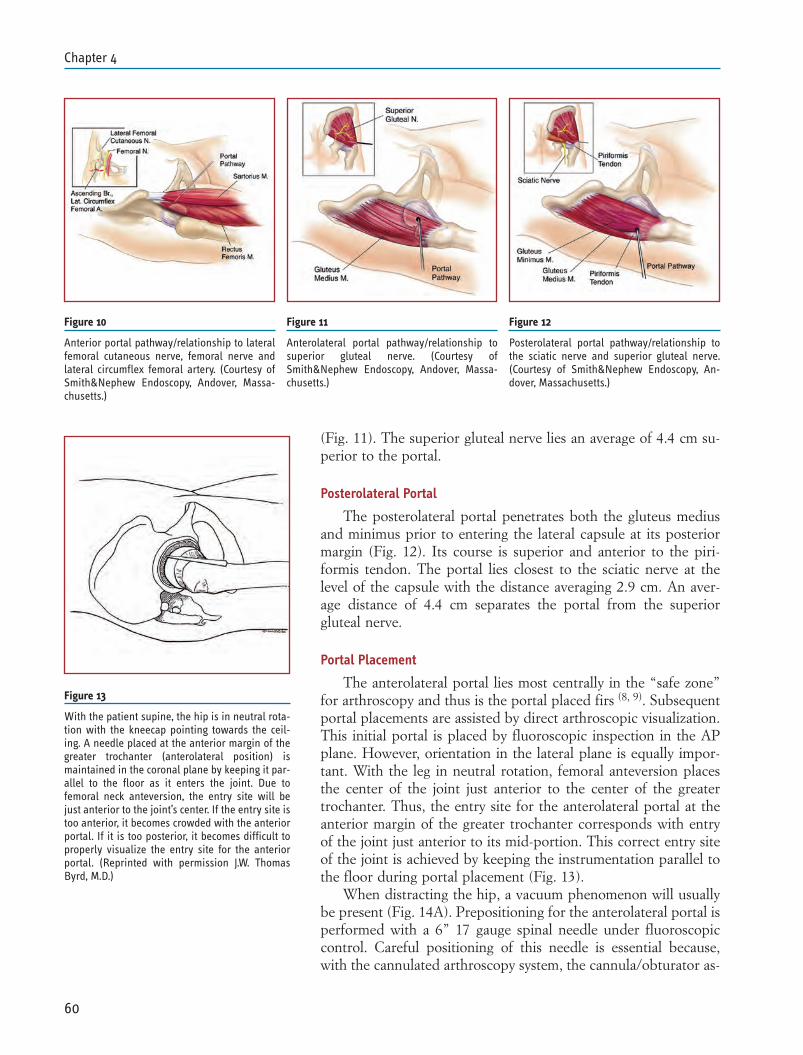
(Fig. 11). The superior gluteal nerve lies an average of 4.4 cm su-perior to the portal.
Posterolateral Portal
The posterolateral portal penetrates both the gluteus mediusand minimus prior to entering the lateral capsule at its posteriormargin (Fig. 12). Its course is superior and anterior to the piri-formis tendon. The portal lies closest to the sciatic nerve at thelevel of the capsule with the distance averaging 2.9 cm. An aver-age distance of 4.4 cm separates the portal from the superiorgluteal nerve.
Portal Placement
The anterolateral portal lies most centrally in the “safe zone”for arthroscopy and thus is the portal placed firs (8, 9). Subsequentportal placements are assisted by direct arthroscopic visualization.This initial portal is placed by fluoroscopic inspection in the APplane. However, orientation in the lateral plane is equally impor-tant. With the leg in neutral rotation, femoral anteversion placesthe center of the joint just anterior to the center of the greatertrochanter. Thus, the entry site for the anterolateral portal at theanterior margin of the greater trochanter corresponds with entryof the joint just anterior to its mid-portion. This correct entry siteof the joint is achieved by keeping the instrumentation parallel tothe floor during portal placement (Fig. 13).
When distracting the hip, a vacuum phenomenon will usuallybe present (Fig. 14A). Prepositioning for the anterolateral portal isperformed with a 6” 17 gauge spinal needle under fluoroscopiccontrol. Careful positioning of this needle is essential because,with the cannulated arthroscopy system, the cannula/obturator as-
60
Chapter 4
Figure 13
With the patient supine, the hip is in neutral rota-tion with the kneecap pointing towards the ceil-ing. A needle placed at the anterior margin of thegreater trochanter (anterolateral position) ismaintained in the coronal plane by keeping it par-allel to the floor as it enters the joint. Due tofemoral neck anteversion, the entry site will bejust anterior to the joint’s center. If the entry site istoo anterior, it becomes crowded with the anteriorportal. If it is too posterior, it becomes difficult toproperly visualize the entry site for the anteriorportal. (Reprinted with permission J.W. ThomasByrd, M.D.)
Figure 11
Anterolateral portal pathway/relationship tosuperior gluteal nerve. (Courtesy ofSmith&Nephew Endoscopy, Andover, Massa-chusetts.)
Figure 10
Anterior portal pathway/relationship to lateralfemoral cutaneous nerve, femoral nerve andlateral circumflex femoral artery. (Courtesy ofSmith&Nephew Endoscopy, Andover, Massa-chusetts.)
Figure 12
Posterolateral portal pathway/relationship tothe sciatic nerve and superior gluteal nerve.(Courtesy of Smith&Nephew Endoscopy, An-dover, Massachusetts.)
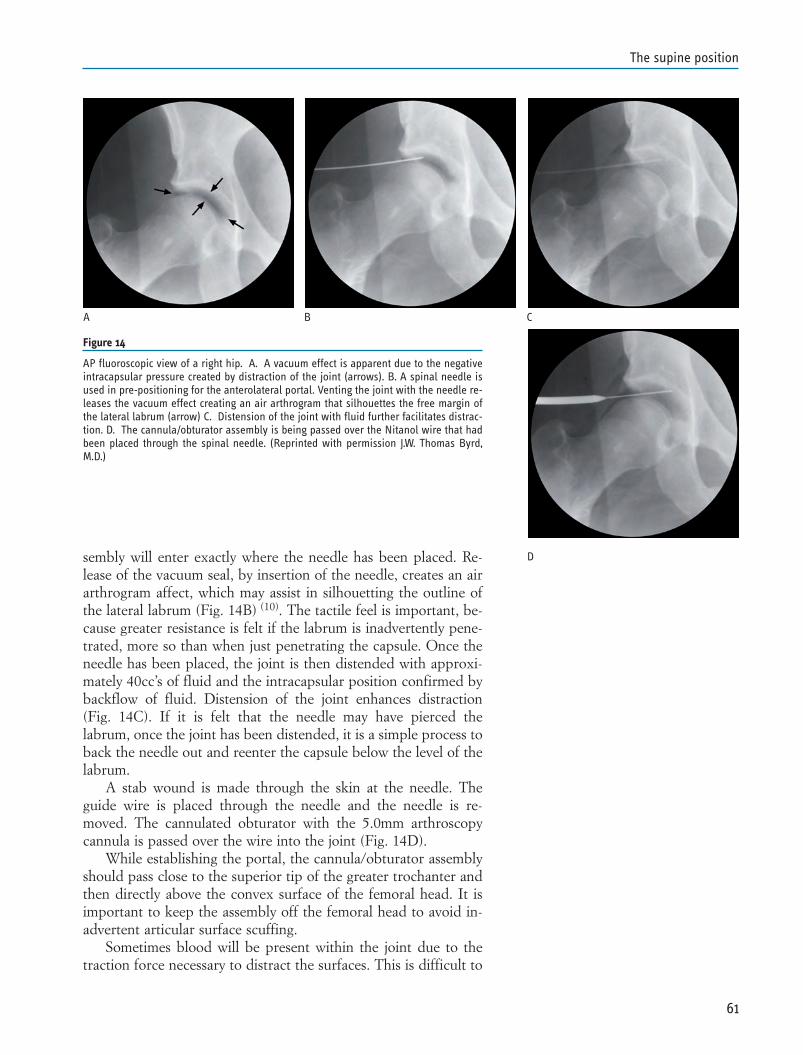
sembly will enter exactly where the needle has been placed. Re-lease of the vacuum seal, by insertion of the needle, creates an airarthrogram affect, which may assist in silhouetting the outline ofthe lateral labrum (Fig. 14B) (10). The tactile feel is important, be-cause greater resistance is felt if the labrum is inadvertently pene-trated, more so than when just penetrating the capsule. Once theneedle has been placed, the joint is then distended with approxi-mately 40cc’s of fluid and the intracapsular position confirmed bybackflow of fluid. Distension of the joint enhances distraction(Fig. 14C). If it is felt that the needle may have pierced thelabrum, once the joint has been distended, it is a simple process toback the needle out and reenter the capsule below the level of thelabrum.
A stab wound is made through the skin at the needle. Theguide wire is placed through the needle and the needle is re-moved. The cannulated obturator with the 5.0mm arthroscopycannula is passed over the wire into the joint (Fig. 14D).
While establishing the portal, the cannula/obturator assemblyshould pass close to the superior tip of the greater trochanter andthen directly above the convex surface of the femoral head. It isimportant to keep the assembly off the femoral head to avoid in-advertent articular surface scuffing.
Sometimes blood will be present within the joint due to thetraction force necessary to distract the surfaces. This is difficult to
61
The supine position
Figure 14
AP fluoroscopic view of a right hip. A. A vacuum effect is apparent due to the negativeintracapsular pressure created by distraction of the joint (arrows). B. A spinal needle isused in pre-positioning for the anterolateral portal. Venting the joint with the needle re-leases the vacuum effect creating an air arthrogram that silhouettes the free margin ofthe lateral labrum (arrow) C. Distension of the joint with fluid further facilitates distrac-tion. D. The cannula/obturator assembly is being passed over the Nitanol wire that hadbeen placed through the spinal needle. (Reprinted with permission J.W. Thomas Byrd,M.D.)
A B C
D

clear until a separate egress has been established. However, vent-ing fluid with the spinal needle from anterior will clear the field ofview.
Once the arthroscope has been introduced, the anterior portalis placed next. Positioning is now facilitated by visualization fromthe arthroscope as well as fluoroscopy. The 70° scope works bestfor directly viewing where the instrumentation penetrates the cap-sule. Pre-positioning is again performed with the 17 gauge spinalneedle, entering the joint directly underneath the free edge of theanterior labrum. As the cannula/obturator assembly is introduced,it is lifted up to stay off the articular surface of the femoral headwhile passing underneath the acetabular labrum.
If proper attention is given to the topographical anatomy inpositioning the anterior portal, the femoral nerve lies well medialto the approach (8, 9). However, the lateral femoral cutaneousnerve lies quite close to this portal. It is best avoided by utilizingproper technique in portal placement. The nerve is most vulnera-ble to laceration by a skin incision placed too deeply.
Lastly, the posterolateral portal is introduced. The fluoroscop-ic guidelines are similar to the anterolateral portal. Rotating thelens of the arthroscope posteriorly brings the entry site under-neath the posterior labrum into view. Placement under arthro-scopic control ensures that the instrumentation does not stray pos-teriorly, potentially placing the sciatic nerve at risk. The hip re-mains in neutral rotation during placement of the posterolateralportal. External rotation of the hip would move the greatertrochanter more posteriorly and, since this is the main topograph-ical landmark, the sciatic nerve might be more at risk for injury(Fig. 15).
Portal Placement for Peripheral Joint(7, 11, 12)
After completing arthroscopy of the interior of the hip, the in-struments can be removed and traction released for access to theperipheral compartment. The hip is flexed approximately 45°which relaxes the anterior capsule (Fig. 16). From the anterolater-al entry site, the spinal needle penetrates the capsule on the ante-rior neck of the femur under fluoroscopic control (Figs. 17A andB). Using the guide wire, the cannula obturator assembly is thenplaced (Fig. 17C). The 5mm cannula is preferable with the inflowattached to the scope.
For instrumentation, an ancillary portal is placed 5cm distalto the anterolateral portal. Once again prepositioning is per-formed with the 17 gauge spinal needle, directly observingthrough the arthroscope where the needle enters the peripheralcompartment (Fig. 17D). Many loose bodies reside in this areaand can be retrieved. Recontouring of the femoral head associat-ed with cam impingement is best addressed from the peripheralcompartment. This also provides superior access to the synoviallining and capsule, which is important for performing a thorough
62
Chapter 4
Figure 15
Neutral rotation of the operative hip is essentialfor protection of the sciatic nerve during place-ment of the posterolateral portal. (Courtesy ofSmith&Nephew Endoscopy, Andover, Massachu-setts.)
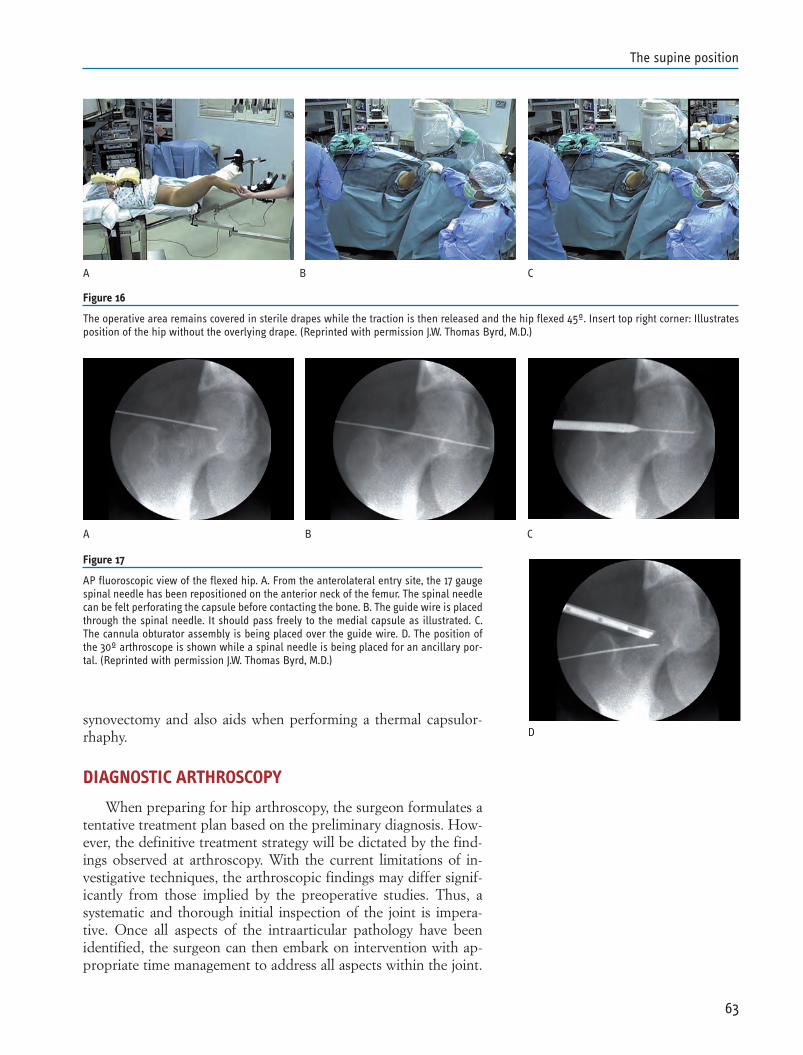
synovectomy and also aids when performing a thermal capsulor-rhaphy.
DIAGNOSTIC ARTHROSCOPY
When preparing for hip arthroscopy, the surgeon formulates atentative treatment plan based on the preliminary diagnosis. How-ever, the definitive treatment strategy will be dictated by the find-ings observed at arthroscopy. With the current limitations of in-vestigative techniques, the arthroscopic findings may differ signif-icantly from those implied by the preoperative studies. Thus, asystematic and thorough initial inspection of the joint is impera-tive. Once all aspects of the intraarticular pathology have beenidentified, the surgeon can then embark on intervention with ap-propriate time management to address all aspects within the joint.
63
The supine position
Figure 17
AP fluoroscopic view of the flexed hip. A. From the anterolateral entry site, the 17 gaugespinal needle has been repositioned on the anterior neck of the femur. The spinal needlecan be felt perforating the capsule before contacting the bone. B. The guide wire is placedthrough the spinal needle. It should pass freely to the medial capsule as illustrated. C.The cannula obturator assembly is being placed over the guide wire. D. The position ofthe 30º arthroscope is shown while a spinal needle is being placed for an ancillary por-tal. (Reprinted with permission J.W. Thomas Byrd, M.D.)
BA C
A B C
D
Figure 16
The operative area remains covered in sterile drapes while the traction is then released and the hip flexed 45º. Insert top right corner: Illustratesposition of the hip without the overlying drape. (Reprinted with permission J.W. Thomas Byrd, M.D.)
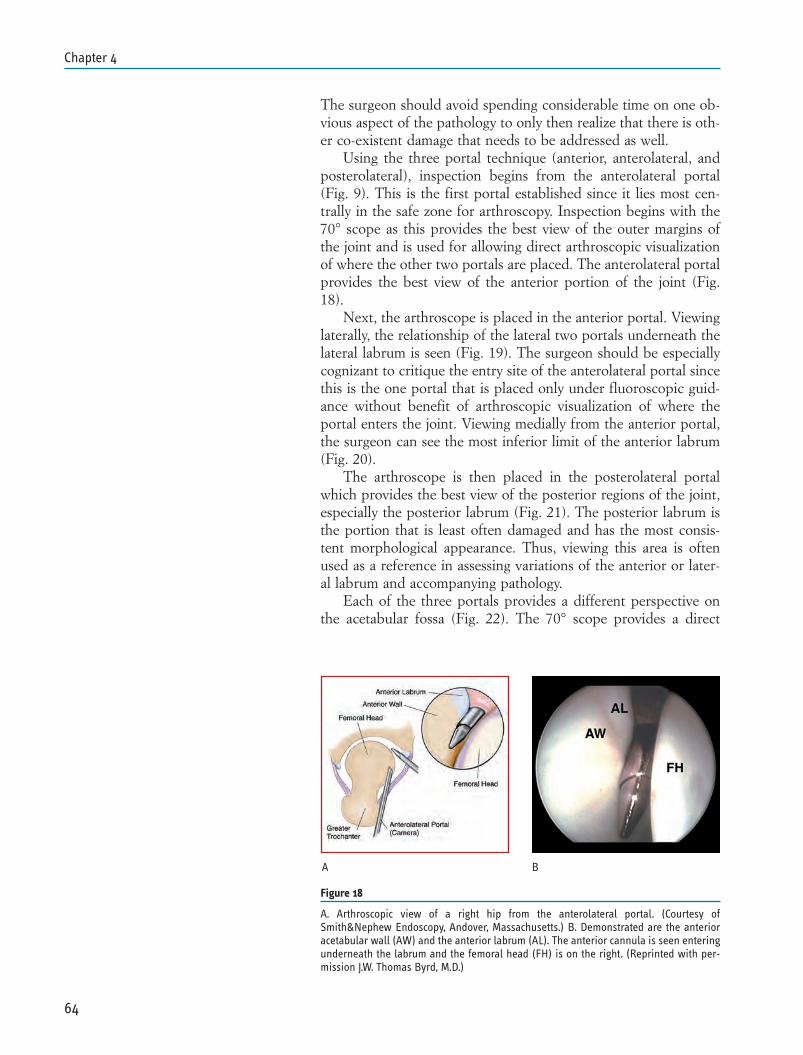
The surgeon should avoid spending considerable time on one ob-vious aspect of the pathology to only then realize that there is oth-er co-existent damage that needs to be addressed as well.
Using the three portal technique (anterior, anterolateral, andposterolateral), inspection begins from the anterolateral portal(Fig. 9). This is the first portal established since it lies most cen-trally in the safe zone for arthroscopy. Inspection begins with the70° scope as this provides the best view of the outer margins ofthe joint and is used for allowing direct arthroscopic visualizationof where the other two portals are placed. The anterolateral portalprovides the best view of the anterior portion of the joint (Fig.18).
Next, the arthroscope is placed in the anterior portal. Viewinglaterally, the relationship of the lateral two portals underneath thelateral labrum is seen (Fig. 19). The surgeon should be especiallycognizant to critique the entry site of the anterolateral portal sincethis is the one portal that is placed only under fluoroscopic guid-ance without benefit of arthroscopic visualization of where theportal enters the joint. Viewing medially from the anterior portal,the surgeon can see the most inferior limit of the anterior labrum(Fig. 20).
The arthroscope is then placed in the posterolateral portalwhich provides the best view of the posterior regions of the joint,especially the posterior labrum (Fig. 21). The posterior labrum isthe portion that is least often damaged and has the most consis-tent morphological appearance. Thus, viewing this area is oftenused as a reference in assessing variations of the anterior or later-al labrum and accompanying pathology.
Each of the three portals provides a different perspective onthe acetabular fossa (Fig. 22). The 70° scope provides a direct
64
Chapter 4
Figure 18
A. Arthroscopic view of a right hip from the anterolateral portal. (Courtesy ofSmith&Nephew Endoscopy, Andover, Massachusetts.) B. Demonstrated are the anterioracetabular wall (AW) and the anterior labrum (AL). The anterior cannula is seen enteringunderneath the labrum and the femoral head (FH) is on the right. (Reprinted with per-mission J.W. Thomas Byrd, M.D.)
A B
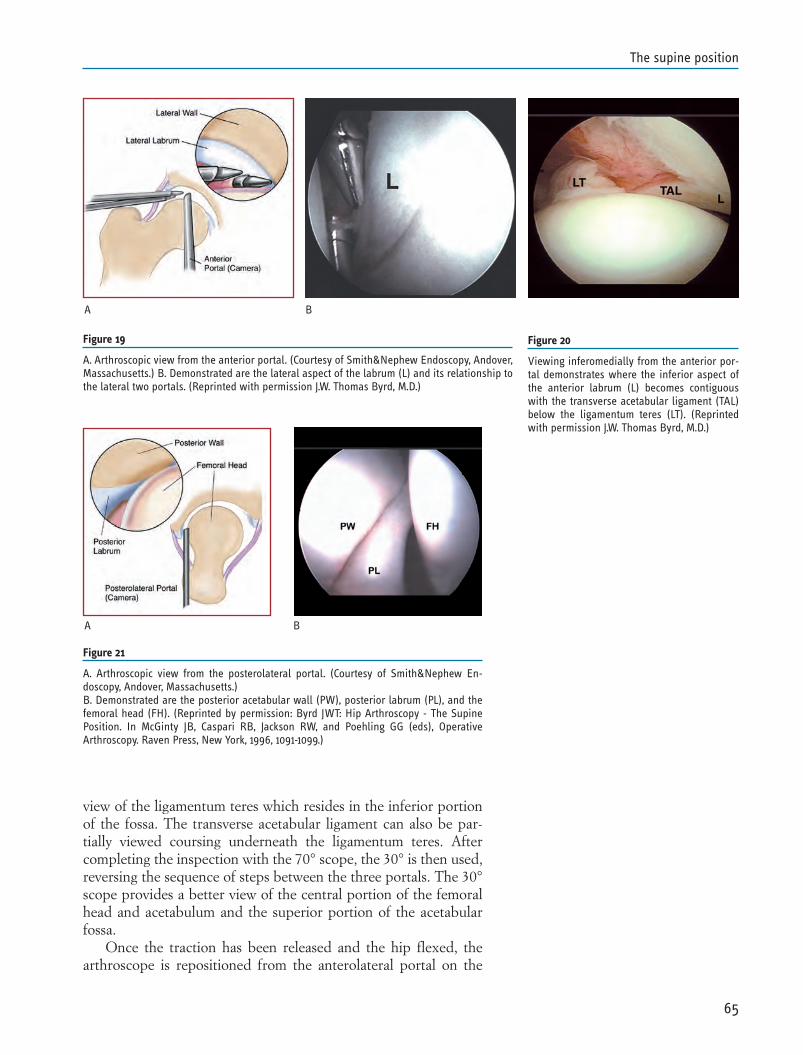
view of the ligamentum teres which resides in the inferior portionof the fossa. The transverse acetabular ligament can also be par-tially viewed coursing underneath the ligamentum teres. Aftercompleting the inspection with the 70° scope, the 30° is then used,reversing the sequence of steps between the three portals. The 30°scope provides a better view of the central portion of the femoralhead and acetabulum and the superior portion of the acetabularfossa.
Once the traction has been released and the hip flexed, thearthroscope is repositioned from the anterolateral portal on the
65
The supine position
Figure 20
Viewing inferomedially from the anterior por-tal demonstrates where the inferior aspect ofthe anterior labrum (L) becomes contiguouswith the transverse acetabular ligament (TAL)below the ligamentum teres (LT). (Reprintedwith permission J.W. Thomas Byrd, M.D.)
Figure 21
A. Arthroscopic view from the posterolateral portal. (Courtesy of Smith&Nephew En-doscopy, Andover, Massachusetts.)B. Demonstrated are the posterior acetabular wall (PW), posterior labrum (PL), and thefemoral head (FH). (Reprinted by permission: Byrd JWT: Hip Arthroscopy - The SupinePosition. In McGinty JB, Caspari RB, Jackson RW, and Poehling GG (eds), OperativeArthroscopy. Raven Press, New York, 1996, 1091-1099.)
A B
Figure 19
A. Arthroscopic view from the anterior portal. (Courtesy of Smith&Nephew Endoscopy, Andover,Massachusetts.) B. Demonstrated are the lateral aspect of the labrum (L) and its relationship tothe lateral two portals. (Reprinted with permission J.W. Thomas Byrd, M.D.)
A B
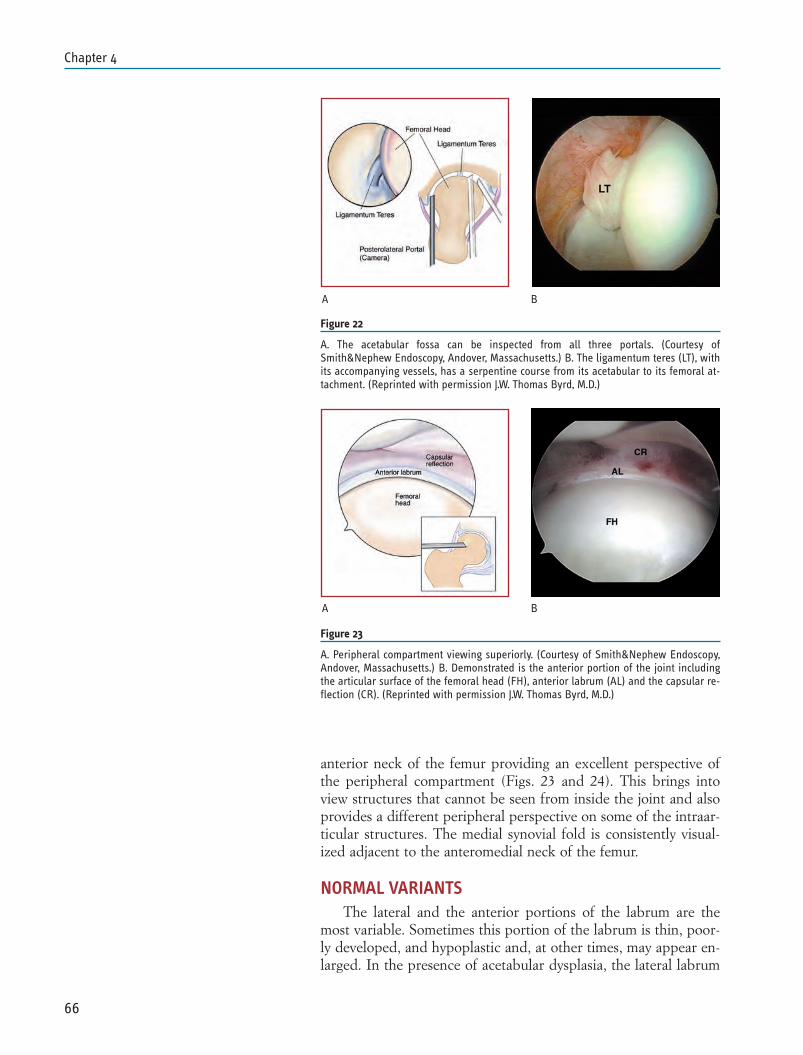
anterior neck of the femur providing an excellent perspective ofthe peripheral compartment (Figs. 23 and 24). This brings intoview structures that cannot be seen from inside the joint and alsoprovides a different peripheral perspective on some of the intraar-ticular structures. The medial synovial fold is consistently visual-ized adjacent to the anteromedial neck of the femur.
NORMAL VARIANTSThe lateral and the anterior portions of the labrum are the
most variable. Sometimes this portion of the labrum is thin, poor-ly developed, and hypoplastic and, at other times, may appear en-larged. In the presence of acetabular dysplasia, the lateral labrum
66
Chapter 4
A B
Figure 23
A. Peripheral compartment viewing superiorly. (Courtesy of Smith&Nephew Endoscopy,Andover, Massachusetts.) B. Demonstrated is the anterior portion of the joint includingthe articular surface of the femoral head (FH), anterior labrum (AL) and the capsular re-flection (CR). (Reprinted with permission J.W. Thomas Byrd, M.D.)
A B
Figure 22
A. The acetabular fossa can be inspected from all three portals. (Courtesy ofSmith&Nephew Endoscopy, Andover, Massachusetts.) B. The ligamentum teres (LT), withits accompanying vessels, has a serpentine course from its acetabular to its femoral at-tachment. (Reprinted with permission J.W. Thomas Byrd, M.D.)
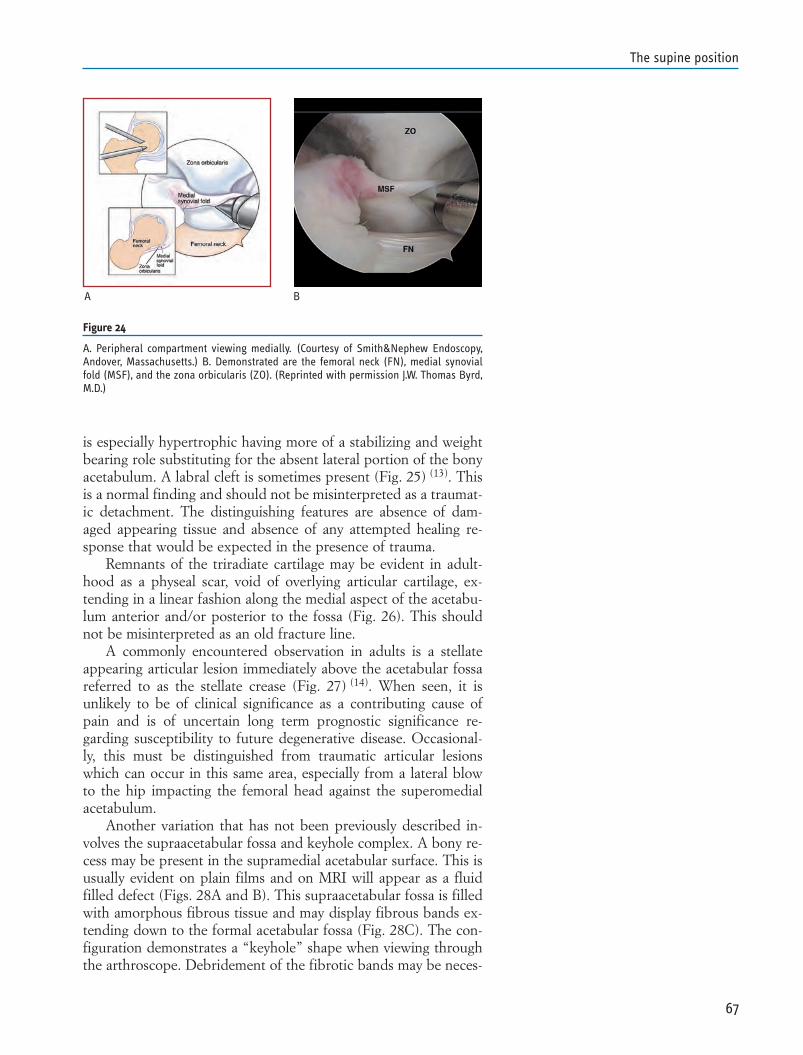
is especially hypertrophic having more of a stabilizing and weightbearing role substituting for the absent lateral portion of the bonyacetabulum. A labral cleft is sometimes present (Fig. 25) (13). Thisis a normal finding and should not be misinterpreted as a traumat-ic detachment. The distinguishing features are absence of dam-aged appearing tissue and absence of any attempted healing re-sponse that would be expected in the presence of trauma.
Remnants of the triradiate cartilage may be evident in adult-hood as a physeal scar, void of overlying articular cartilage, ex-tending in a linear fashion along the medial aspect of the acetabu-lum anterior and/or posterior to the fossa (Fig. 26). This shouldnot be misinterpreted as an old fracture line.
A commonly encountered observation in adults is a stellateappearing articular lesion immediately above the acetabular fossareferred to as the stellate crease (Fig. 27) (14). When seen, it isunlikely to be of clinical significance as a contributing cause ofpain and is of uncertain long term prognostic significance re-garding susceptibility to future degenerative disease. Occasional-ly, this must be distinguished from traumatic articular lesionswhich can occur in this same area, especially from a lateral blowto the hip impacting the femoral head against the superomedialacetabulum.
Another variation that has not been previously described in-volves the supraacetabular fossa and keyhole complex. A bony re-cess may be present in the supramedial acetabular surface. This isusually evident on plain films and on MRI will appear as a fluidfilled defect (Figs. 28A and B). This supraacetabular fossa is filledwith amorphous fibrous tissue and may display fibrous bands ex-tending down to the formal acetabular fossa (Fig. 28C). The con-figuration demonstrates a “keyhole” shape when viewing throughthe arthroscope. Debridement of the fibrotic bands may be neces-
67
The supine position
A B
Figure 24
A. Peripheral compartment viewing medially. (Courtesy of Smith&Nephew Endoscopy,Andover, Massachusetts.) B. Demonstrated are the femoral neck (FN), medial synovialfold (MSF), and the zona orbicularis (ZO). (Reprinted with permission J.W. Thomas Byrd,M.D.)
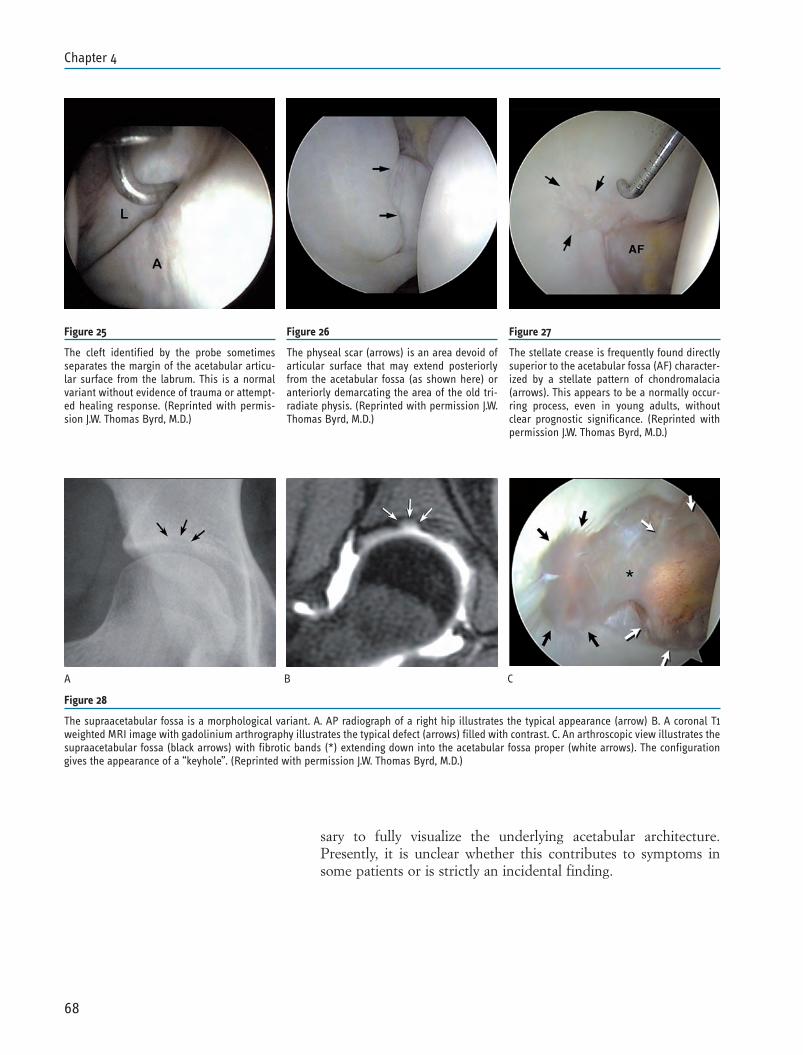
sary to fully visualize the underlying acetabular architecture.Presently, it is unclear whether this contributes to symptoms insome patients or is strictly an incidental finding.
68
Chapter 4
Figure 26
The physeal scar (arrows) is an area devoid ofarticular surface that may extend posteriorlyfrom the acetabular fossa (as shown here) oranteriorly demarcating the area of the old tri-radiate physis. (Reprinted with permission J.W.Thomas Byrd, M.D.)
A B C
Figure 27
The stellate crease is frequently found directlysuperior to the acetabular fossa (AF) character-ized by a stellate pattern of chondromalacia(arrows). This appears to be a normally occur-ring process, even in young adults, withoutclear prognostic significance. (Reprinted withpermission J.W. Thomas Byrd, M.D.)
Figure 28
The supraacetabular fossa is a morphological variant. A. AP radiograph of a right hip illustrates the typical appearance (arrow) B. A coronal T1weighted MRI image with gadolinium arthrography illustrates the typical defect (arrows) filled with contrast. C. An arthroscopic view illustrates thesupraacetabular fossa (black arrows) with fibrotic bands (*) extending down into the acetabular fossa proper (white arrows). The configurationgives the appearance of a “keyhole”. (Reprinted with permission J.W. Thomas Byrd, M.D.)
Figure 25
The cleft identified by the probe sometimesseparates the margin of the acetabular articu-lar surface from the labrum. This is a normalvariant without evidence of trauma or attempt-ed healing response. (Reprinted with permis-sion J.W. Thomas Byrd, M.D.)
REFERENCES
1. Sampson TG: Complications of hip arthroscopy. Clin SportsMed 2001;20(4):831-836.
2. Bartlett CS, DiFelice GS, Buly RL, et al: Cardiac arrest as a re-sult of intraabdominal extravasation of fluid during arthro-scopic removal of a loose body from the hip joint of a patientwith an acetabular fracture. J Ortho Trauma, 1998;12(4):294-299.
3. Dienst M, Godde S, Seil R, Hammer D, Kohn D: Hiparthroscopy without traction: in vivo anatomy of the peripher-al hip joint cavity. Arthroscopy, 2001:17(9);924-931.
4. Dienst M: Hip arthroscopy without traction. In Byrd JWT(ed) Operative Hip Arthroscopy Second Edition, Springer,2005, 170-188.
5. Byrd JWT, Chern KY: Traction vs distension for distraction ofthe hip joint during arthroscopy. Arthroscopy, 1997;13(3):346-349.
6. Byrd JWT: The supine approach. In Byrd JWT (ed) OperativeHip Arthroscopy Second Edition, New York, Springer, 2005,145-169.
7. Byrd JWT: Hip arthroscopy. J Am Acad Ortho Surgeons, pub-lication pending, 2005.
8. Byrd JWT, Pappas JN, Pedley MJ: Hip arthroscopy: ananatomic study of portal placement and relationship to the ex-tra-articular structures, Arthroscopy, 1995;11(4):418-423.
9. Byrd JWT: Portal anatomy. In Byrd JWT (ed) Operative HipArthroscopy Second Edition, New York, Springer, 2005, 110-116.
10. Byrd JWT: Avoiding the labrum in hip arthroscopy.Arthroscopy. 2000;16(7):770-773.
11. Dienst M, Godde S, Seil R, Hammer D, Kohn D: Hiparthroscopy without traction: in vivo anatomy of the peripher-al hip joint cavity. Arthroscopy 2001:17(9);924-931.
12. Dienst M: Hip arthroscopy without traction. In Byrd JWT(ed) Operative Hip Arthroscopy Second Edition, New York,Springer, 2005,170-188.
13. Byrd, JWT: Labral Lesions, an Elusive Source of Hip Pain:Case Reports and Review of the Literature. Arthroscopy.12(5):603-612;1996.
14. Villar R, Santori N: Arthroscopic Anatomy of the Hip. In ByrdJWT (ed) Operative Hip Arthroscopy Second Edition, NewYork, Springer, 2005,117-128.
69
The supine position

Hip arthroscopy can be performed positioning the patient ei-ther in lateral decubitus or supine position.
The choice is dictated by the surgeon’s personal habits and ex-periences even if over time we find in literature a progressive in-crease of satisfaction rating and use of supine position rather thanlateral.
In supine decubitus technique a traumatology bed is used andpatient is positioned supine.
The operative limb is positioned with hip in slight abduction,intrarotation and flexion; extended knee; foot is placed in a limbtraction support device.
Controlateral limb is positioned in extension, slight abduction,neutral rotation, with foot in a support applying a counterbalanc-ing traction to the one applied to the operative limb. Counter-trac-tion, lateralized toward operative hip, is placed in the perineal re-gion.
In lateral decubitus technique, patient is positioned on thecounterlateral side to the operative limb, on a fracture table pro-viding a podalic support to apply traction to the operative limb,while countertraction is placed in perineal area and no furthertraction is needed on the non-operative limb side; traction mustbe perfomed with abducted, flexed, intrarotated hip and extend-ed knee.
In literature both systems are emphasized by their users and ineffect both positions together with surgeon’s good experience canprovide a correct performance of hip arthroscopy surgery.
Who claims lateral decubitus to be better, underlines how thisposition is more intuitive and comfortable for surgeons used toperform hip surgery in lateral position; it is also considered by farthe best position in case of obese patients.
Who instead uses decubitus supine, claims that this is a moreintuitive, simple and comfortable position because operative hip isless high than in lateral and therefore there is no need for the sur-geon to use platforms as often happens in lateral position; it is al-so claimed that a better use of brilliance amplifier and passing
71
Chapter 5PERSONAL TECHNIQUE: MODIFIED SUPINE POSITIONRaul ZiniGiorgio Ponzetto
more easily from central compartment arthroscopy to peripheral,is possible.
PERSONAL EXPERIENCE
Our hip arthroscopy experience began in 1995 with lateral po-sition that has been replaced in 1999 by supine position; thischange is due to the belief that this position allows a simplificationof some pre-operating phases too complex and long for the med-ical staff; transition to supine position provided us with a progres-sive reduction of patient preparation time; we have also noted thatover time the new position proved to be simpler and more effec-tive.
The use of fluoroscopy in decubitus supine position is easierand gives more guarantees to maintain sterility in the operativefield; unlike the lateral decubitus position providing the antero-posterior projection alone, the supine gives also the possibility tohave either axial or lateral vision, that in rare cases might be nec-essary to provide.
According to us, supine decubitus position provides a bettersurgeon position, meaning operating surgeon comfort, since thereis a minor contact and collision with the brilliance amplifier, thatcan be removed and reinserted anytime in the operative field.
Besides, in decubitus supine position, hip arthroscopic anato-my seems much more intuitive, provides better spatial orientationand easier anatomic reference points visualization and portals po-sitioning.
Final confirmation of our choice was given to us when westarted to complete the central compartment arthroscopy with theperipheral compartment one without traction; in fact technicaltime to pass from traction arthroscopy of central compartment toperipheral one without traction, that represents a difficult mo-ment mainly for scrub nurses, seems much easier.
PERSONAL MODIFIED TECHNIQUE
Along with a supine position experience increase, we notedsome critic points and difficulties that according to us could beimproved with technical devices we progressively started to use.
Above all, we wanted to improve maneuverability of bril-liance amplifier and allow a better traction on the operativelimb, acting mainly on the controlateral limb countertraction,without contemporaneously increasing the risks of a raised pubiscompression.
Besides, we wanted to provide the patient with a better intra-operatory condition since he undergoes peripheral anesthesia andtherefore can complain of the onset of lombalgy due to lumbar hy-perlordosis; position has been therefore modified in order to levellumbar lordosis and discharge rachis from stresses that, consider-
72
Chapter 5

ing surgery duration, can cause painful symptoms or at least intra-operatory discomforts.
Patient is supine positioned on trauma table; hip is extended,rotation is neutral and knee is extended with patella at the zenith;foot is placed in a foot holder linked to traction (Fig. 1); once op-erative limb is put in traction in order to obtain a sufficient artic-ular distraction, it is intrarotated over 45° to make the femoralneck parallel to the ground plane.
Controlateral limb is placed on a gynecological stirrup withabducted flexion of hip, flexed knee, loose foot (Fig. 2); non op-erative limb is not put in traction.
A countertraction, called post, is exerted at the pelvis. Thispost has to be well padded to avoid an excessive compression ofobturator and pudendal nerves. Today on the market we find re-markable diameter special posts dedicated to hip arthroscopy.They are very soft and therefore minimize the possibility of com-pressive risks (Fig. 3). Gel pads used to pad in layers the operat-ing table metal post are also available.
A well padded restraint support to avoid decubitus bedsores isplaced at the chest in order to counterbalance tilting of trunk dur-ing traction (Fig. 4).
In case a peripheral compartment arthroscopy is expected tobe performed, before starting surgery, a further gynaecologicalstirrup or padded thigh holder, later due to be used forarthroscopy without traction, is fixed to the table traction arm.
To perform peripheral compartment arthroscopy, traction isinitially removed, hip is flexed and gynaecological stirrup is placedunder knee, thus remaining outside sterile field and keeping theselected limb flexion. (Fig. 5)
73
Personal technique: modified supine position
Figure 1
Positioning with personal technique
Figure 2
Detail of controlateral limb positioning
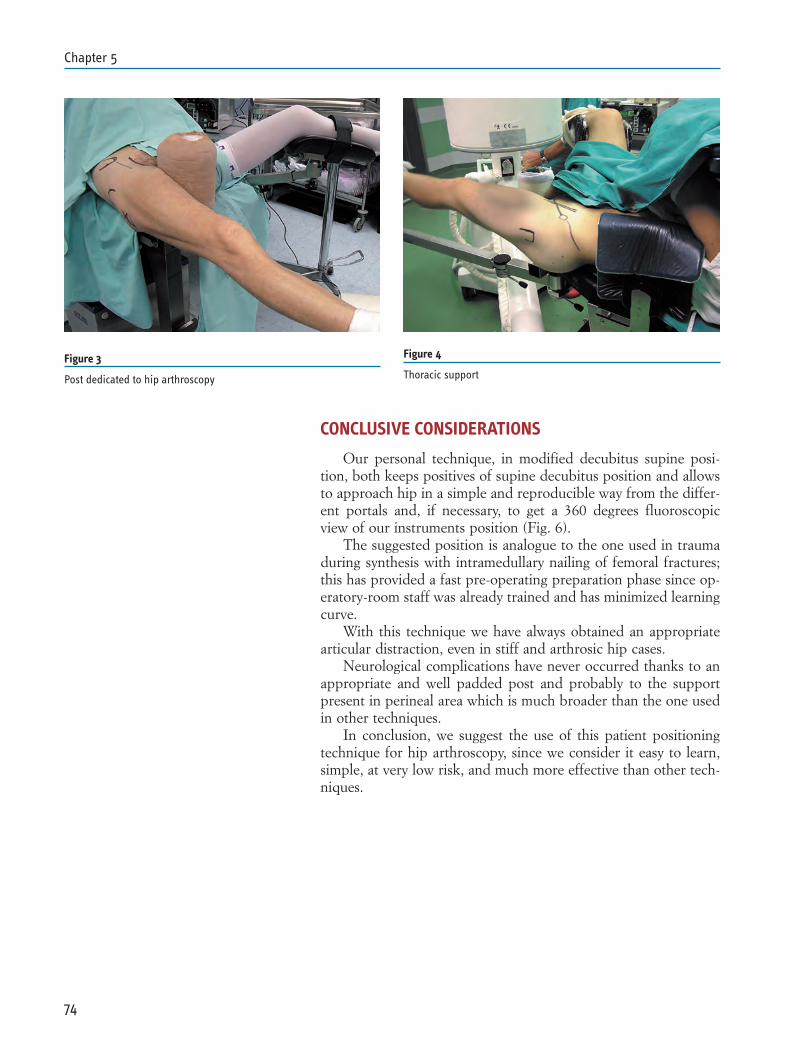
CONCLUSIVE CONSIDERATIONS
Our personal technique, in modified decubitus supine posi-tion, both keeps positives of supine decubitus position and allowsto approach hip in a simple and reproducible way from the differ-ent portals and, if necessary, to get a 360 degrees fluoroscopicview of our instruments position (Fig. 6).
The suggested position is analogue to the one used in traumaduring synthesis with intramedullary nailing of femoral fractures;this has provided a fast pre-operating preparation phase since op-eratory-room staff was already trained and has minimized learningcurve.
With this technique we have always obtained an appropriatearticular distraction, even in stiff and arthrosic hip cases.
Neurological complications have never occurred thanks to anappropriate and well padded post and probably to the supportpresent in perineal area which is much broader than the one usedin other techniques.
In conclusion, we suggest the use of this patient positioningtechnique for hip arthroscopy, since we consider it easy to learn,simple, at very low risk, and much more effective than other tech-niques.
74
Chapter 5
Figure 4
Thoracic supportFigure 3
Post dedicated to hip arthroscopy

REFERENCES
1. Byrd JWT: The supine approach. In Byrd JWT (ed) OperativeHip Arthroscopy Second Edition, New York, Springer, 2005,145-169.
2. Dienst M, Godde S, Seil R, Hammer D, Kohn D: Hiparthroscopy without traction: in vivo anatomy of the peripher-al hip joint cavity. Arthroscopy, 2001:17(9);924-931
3. Glick JM, Sampson TG, Gordon RB, Behr JT, Schmidt E:Hip arthroscopy by the lateral approach. Arthroscopy 1987;3:4-12.
75
Personal technique: modified supine position
Figure 5
Flexed hip positioning without traction for peripheral compartmentarthroscopy
Figure 6
Fluoroscopy usage in axillary projection

INTRODUCTION
In the last years, thanks to the growing surgical techniques de-velopment and the extension of hip arthroscopy indications, a sig-nificant debate is open on patient positioning (1, 2, 3) and on ad-vantages and disadvantages resulting from having a patient in asupine or lateral position during surgery.
There is no doubt that patient positioning choice depends onseveral aspects.
The surgeon first, in order to save money, has to consider us-ing the traction systems available in the hospital where he works,adapting to them, despite the numerous specific hip arthroscopytraction devices available on the market.
The habit to perform hip surgery is another extremely impor-tant and not secondary aspect. Many surgeons showing interest inand understanding the utility of this surgery have in fact a signifi-cant experience in hip prosthetic surgery. It is certain, therefore,that choosing to perform surgery with patient either in supine orlateral decubitus position can also be influenced by a personalhabit to perform prosthetic surgery, since this last can influencethe personal perception of anatomy and surgical findings.
That said, it is necessary to determine scientifically strengthsand weaknesses of the two positions in order to help with thechoice and give the most objective possible guideline.
PATIENT AND OPERATING ROOM SETUP
Patient preparation before surgery follows a standard pathwith no special attention to lateral decubitus position. There is al-so no restriction concerning the choice of anesthesia: bothepi/peridural and general anesthesia can be used. In the last casethe choice to perform patient intubation rather than to use a la-ryngeal mask is completely at the surgeon’s discretion. Sometimes,mainly treating femoral acetabular impingement, the use of aperidural catheter is also indicated to control pain symptomatol-ogy, in the immediate post-surgical period.
77
Chapter 6LATERAL POSITION ARTHROSCOPIC TECHNIQUEAndrea Fontana

OPERATING-ROOM SETUP AND PATIENT POSITIONINGON TRACTION BED
Hip surgery starts when patient is placed on the operatingtable and traction is applied. It is therefore essential that the sur-geon follows carefully this initial preparation and traction apply-ing phase as well as the presence in the operating –room of skillednurse staff adequately trained to perform the correct maneuvers.
Normal traction systems, commonly used in traumatology totreat femoral fractures, can be applied to perform hip arthroscopyin lateral decubitus position. Usually this systems provide compo-nents to place the patient in lateral decubitus position. The usageof a special horizontal well padded counter traction “roll” is ad-vised, as represented in Figs. 1 and 2.
Traction with patient in lateral decubitus position provides anoptimal joint diastasis.
Two forces are applied: one is longitudinal to inferior limb ax-is, the other is vertical, applied upwards by the roll placed in thegroin.
The force resulting from the two applied, follows the femoralneck direction according to the cervical diaphyseal angle (Fig. 1).The traction provides therefore an optimal joint diastasis andeveryone knows how important this is to insert arthroscopic in-strumentary avoiding to tear labrum, acetabulum and femoralhead cartilage surface (5).
Once the patient is placed and the traction is applied, operat-ing-room is organized and prepared in a very simple and schemat-ic way (Fig. 3). The operating surgeon stands in front of the pelvisbehind the patient and next to the scrub nurse and the table withsurgical instruments. A second table, when available, can belinked to the operating bed proximally and placed over the pa-tient to support the arthroscopic instruments making the sur-geon’s task easier (Fig. 4). The arthroscopic tower, brilliance am-
78
Chapter 6
Figure 1 Figure 2
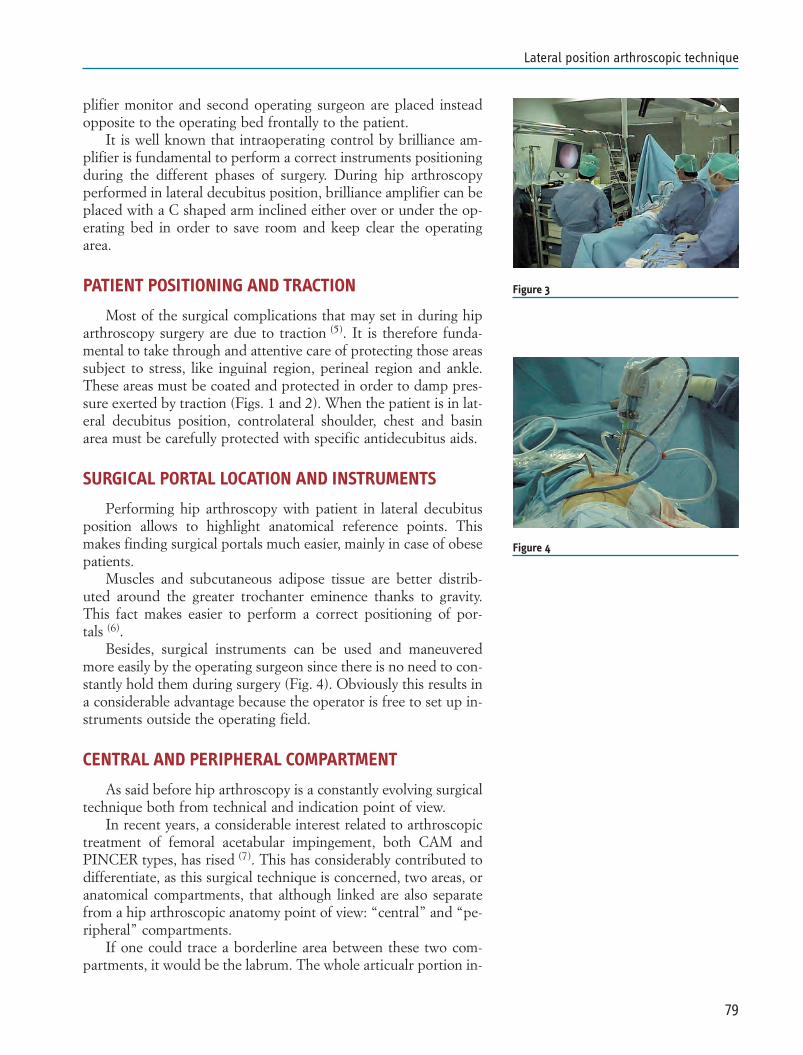
plifier monitor and second operating surgeon are placed insteadopposite to the operating bed frontally to the patient.
It is well known that intraoperating control by brilliance am-plifier is fundamental to perform a correct instruments positioningduring the different phases of surgery. During hip arthroscopyperformed in lateral decubitus position, brilliance amplifier can beplaced with a C shaped arm inclined either over or under the op-erating bed in order to save room and keep clear the operatingarea.
PATIENT POSITIONING AND TRACTION
Most of the surgical complications that may set in during hiparthroscopy surgery are due to traction (5). It is therefore funda-mental to take through and attentive care of protecting those areassubject to stress, like inguinal region, perineal region and ankle.These areas must be coated and protected in order to damp pres-sure exerted by traction (Figs. 1 and 2). When the patient is in lat-eral decubitus position, controlateral shoulder, chest and basinarea must be carefully protected with specific antidecubitus aids.
SURGICAL PORTAL LOCATION AND INSTRUMENTS
Performing hip arthroscopy with patient in lateral decubitusposition allows to highlight anatomical reference points. Thismakes finding surgical portals much easier, mainly in case of obesepatients.
Muscles and subcutaneous adipose tissue are better distrib-uted around the greater trochanter eminence thanks to gravity.This fact makes easier to perform a correct positioning of por-tals (6).
Besides, surgical instruments can be used and maneuveredmore easily by the operating surgeon since there is no need to con-stantly hold them during surgery (Fig. 4). Obviously this results ina considerable advantage because the operator is free to set up in-struments outside the operating field.
CENTRAL AND PERIPHERAL COMPARTMENT
As said before hip arthroscopy is a constantly evolving surgicaltechnique both from technical and indication point of view.
In recent years, a considerable interest related to arthroscopictreatment of femoral acetabular impingement, both CAM andPINCER types, has rised (7). This has considerably contributed todifferentiate, as this surgical technique is concerned, two areas, oranatomical compartments, that although linked are also separatefrom a hip arthroscopic anatomy point of view: “central” and “pe-ripheral” compartments.
If one could trace a borderline area between these two com-partments, it would be the labrum. The whole articualr portion in-
79
Lateral position arthroscopic technique
Figure 3
Figure 4

side the labrum area, represents the central compartment. Vicev-ersa the whole area outside the labrum, represents the peripheralarea.
Distinction between these two compartments implies not onlyan anatomic differentiation but also a different arthroscopic surgi-cal approach. Not only portals to central compartment are differ-ent from the peripheral one, but also limb positioning and tractionapplication change (5). In fact, while to approach the central com-partment it is necessary to achieve articular heads diastasis andtherefore apply traction, no traction is necessary to approach theperipheral one, but limb is placed in light flexion and extrarota-tion to provide an adequate detensioning of the articular capsule.
We therefore guess how patient positioning influences thepossibility to explore and approach easily both hip arthroscopiccompartments.
Lateral decubitus position, as described before, allows optimaltraction forces distibution and articular diastasis that provides anexcellent portal to central hip compartment.
Lateral decubitus position provides also an easy access to pe-ripheral compartment. In this case traction must be released andlimb kept in light flexion and extrarotation.
Common knee “sling” devices to support inferior limb posi-tion can be used together with traditional traction supports, thosecommonly used in traumatology.
However, specific traction devices providing an easy change ofinferior limb position and a fast passage between the two com-partments exist on the market.
CONCLUSION
As already said at the beginning, different elements can influ-ence the choice to perform hip arthroscopy with patient in lateraldecubitus position. There is no doubt that lateral decubitus posi-tion gives remarkable advantages and according to me is prefer-able.
This position provides in fact an optimal exposition of hiptrochanteric region, facilitating a correct localization of arthro-scopic portals, even in obese patients. This allows to obtain a com-plete hip arthroscopic vision and to approach easily both centraland peripheral compartments and therefore arthroscopically treateven the most complex and difficult to investigate hip pathologies.
Since lateral decubitus position provides an optimal articulardiastasis, it consequently allows to insert arthroscopic instrumentsmore easily and reduce complications occurrence.
Finally, this position provides the surgeon with a better han-dling in performing surgery. Brilliance amplifier can be placed lesscumbersomely and operator can better manage instruments evenoutside the operating field.
80
Chapter 6

REFERENCES
1 Byrd J W. Hip arthroscopy utilizing the supine position.Arthroscopy. 1994 June; 10(3):275-80.
2 Glick J M, Sampson T G, Gordon R B, Behr J T, Schmidt E.Hip arthroscopy by the lateral approach. Arthroscopy. 1987;3(1): 4-12.
3 Dominic Carreira, Hip Arthroscopy; Charles A. Bush-Joseph,orthopedics 2006; 29:517
4 K. Kong, P. Chien, J. Wong, D. Yip, Peroneal padding: an al-ternative to a peroneal post in hip arthroscopy Arthroscopy;Vol. 19, 9, 1027-1029.
5 Clarke M T, Arora A, Villar R N. Hip arthroscopy: Complica-tions in 1054 cases. Clinical Orthopaedics and Related Re-search .2003 Jan; 406: 84-88.
6 McCarthy J C (2003) Early Hip Disorders Springer Verlag ed.7 Operative Hip Arthroscopy J.W. Thomas Byrd (Editor) 8 E. Rath; V. Benkovich; D. Lebel; N. Elkrinawi; S. Bloom; M.
Kremer; and D. Atar, Hip Arthroscopy – the Peripheral Com-partment, Journal of Bone and Joint Surgery - British Volume,Vol 90-B, Issue SUPP_III, 507. 2008
81
Lateral position arthroscopic technique

82

Indication to hip arthroscopy may compass a huge variety ofpathologies related to this joint in its complex, affecting either thecentral compartment, properly called coxofemoral joint, or the pe-ripheral compartment, or the periarticular structures, for whichendoscopic surgery term, is more appropriate.
When a classification of hip arthroscopy indications is ap-proached, the still actual difficulty of achieving an accurate clini-cal and instrumental diagnosis must not be under evaluated.
This difficulty is linked to a not always easy evaluation of theobjective and symptomatologic picture and to the frequent lack ofa complete and accurate image diagnostic support.
It is for this reason that, one of the more frequent indicationto hip arthroscopy, is still “coxalgia with unknown reasons”, chap-ter in which are filed all the coxofemoral pain cases to whom clin-ic and radiology cannot give an answer. Arthroscopy is initially adiagnostic procedure that allows, in most cases, to have a diagno-sis that will afterward be completed with the surgical time.
Knowledge and arthroscopic experience evolution led in theselast years to a progressive indications evolution that may regardmultiples pathologies involving synovial, cartilage, ligament andbony hip structures.
In this chapter will be examined all of actual indications to hiparthroscopy; most important topics will be treated in followingproper chapters that can be referred to for a closer examination.Less frequent indications will be mainly examined as they refer toless widespread and known pathologies.
Indications to hip arthroscopy will be classified , both morefrequent and more rare or less widespread ones, and gathered in-to main chapters.
CENTRAL COMPARTMENT PATHOLOGY
– ACETABULAR LABRUM PATHOLOGY– OSTEOCHONDRAL PATHOLOGY
83
Chapter 7INDICATIONSRaul Zini Andrea Carraro Massimo De Benedetto
– DEGENERATIVE PATHOLOGY– SYNOVIAL PATHOLOGY– TRAUMATIC PATHOLOGY– INFECTIVE PATHOLOGY– PAINFUL HIP ARTHROPROSTESIS– PERTHES DISEASE
PERIPHERAL COMPARTMENT PATHOLOGY
– FEMORO-ACETABULAR IMPINGEMENT– “OS ACETABULARIS” IMPINGEMENT– EPIPHYSIOLYSIS– POST-TRAUMATIC OSTEOPHYTOSIS– CALCIFICATIONS AND OSSIFICATIONS
EXTRA-ARTICULAR PATHOLOGY
– INTERNAL AND EXTERNAL SNAPPING HIP– TROCHANTERIC BURSITIS– GLUTEUS MEDIUS AND MINIMUS TENDINOPATHIES
CENTRAL COMPARTMENT PATHOLOGY
Hip central compartment coincides with coxo-femoral joint. Itis a very narrow articular space due to its peculiar congruence,typical of femoral head and acetabular joint. For this reason, artic-ular distraction is mandatory to be able to access it with arthro-scopic surgical instruments and perform whatever surgical proce-dure.
It is possible to visualize, diagnose and treat pathologies offemoral head, acetabulum, acetabular labrum that contour acetab-ulum itself, round ligament (or teres ligament), fovea capitis, partof the articular capsule.
Coxo femoral joint pathologies that find indication to an oper-ative hip arthroscopy are many and may be distinguished and clas-sified in different groups that will be examined later on.
Most important pathologies will be treated synthetically, as wego into them thoroughly in specific chapters in this book’s secondpart.
ACETABULAR LABRUM PATHOLOGY
Acetabular labrum lesions are the most frequent indications tohip arthroscopy. Acetabular labrum lesion genesis may be trau-
84
Chapter 7
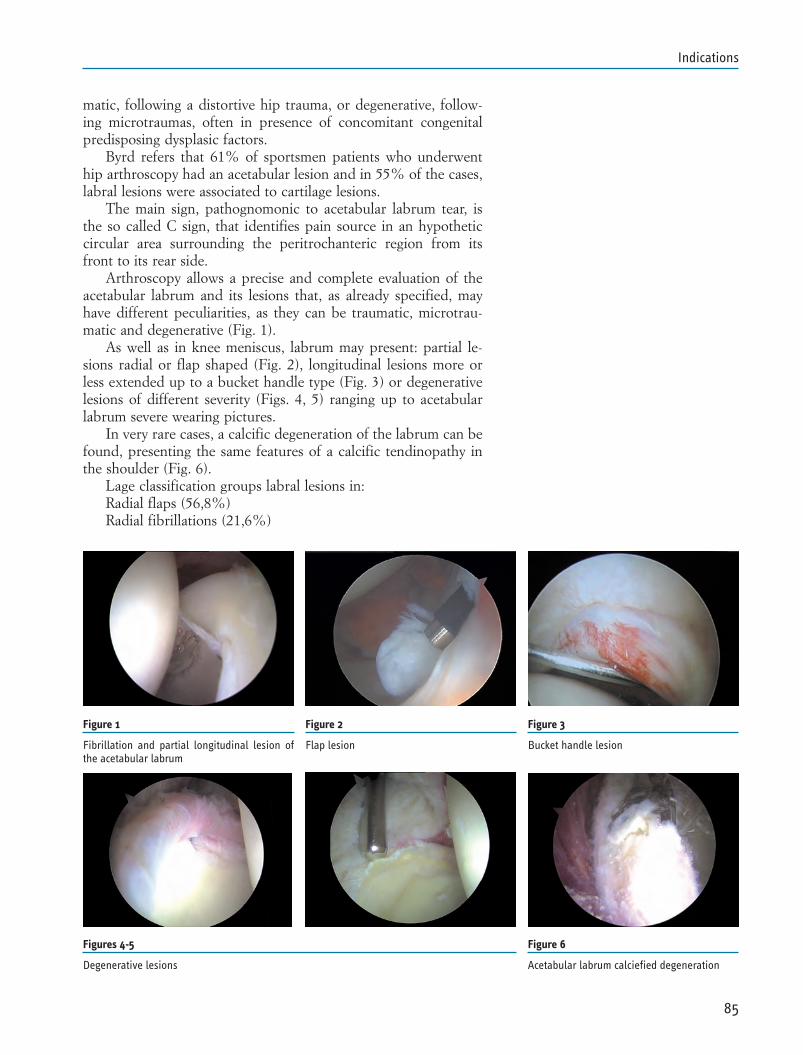
matic, following a distortive hip trauma, or degenerative, follow-ing microtraumas, often in presence of concomitant congenitalpredisposing dysplasic factors.
Byrd refers that 61% of sportsmen patients who underwenthip arthroscopy had an acetabular lesion and in 55% of the cases,labral lesions were associated to cartilage lesions.
The main sign, pathognomonic to acetabular labrum tear, isthe so called C sign, that identifies pain source in an hypotheticcircular area surrounding the peritrochanteric region from itsfront to its rear side.
Arthroscopy allows a precise and complete evaluation of theacetabular labrum and its lesions that, as already specified, mayhave different peculiarities, as they can be traumatic, microtrau-matic and degenerative (Fig. 1).
As well as in knee meniscus, labrum may present: partial le-sions radial or flap shaped (Fig. 2), longitudinal lesions more orless extended up to a bucket handle type (Fig. 3) or degenerativelesions of different severity (Figs. 4, 5) ranging up to acetabularlabrum severe wearing pictures.
In very rare cases, a calcific degeneration of the labrum can befound, presenting the same features of a calcific tendinopathy inthe shoulder (Fig. 6).
Lage classification groups labral lesions in:Radial flaps (56,8%)Radial fibrillations (21,6%)
85
Indications
Figure 1
Fibrillation and partial longitudinal lesion ofthe acetabular labrum
Figure 2
Flap lesion
Figure 3
Bucket handle lesion
Figures 4-5
Degenerative lesions
Figure 6
Acetabular labrum calciefied degeneration
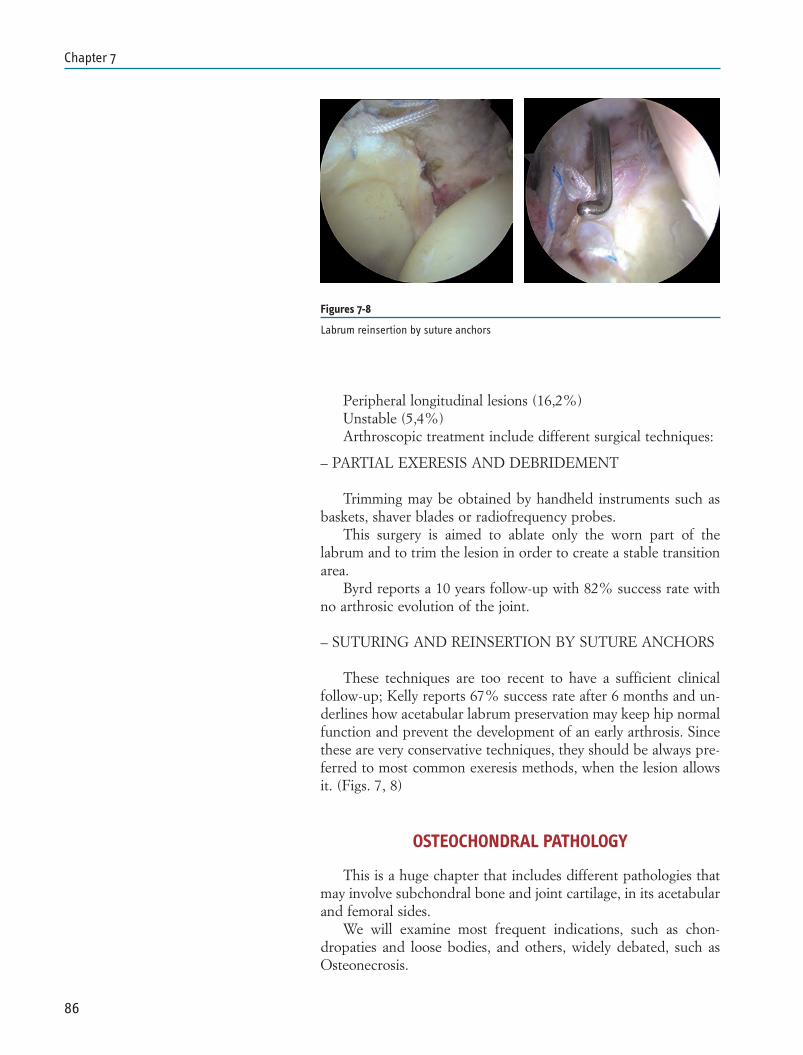
Peripheral longitudinal lesions (16,2%)Unstable (5,4%)Arthroscopic treatment include different surgical techniques:
– PARTIAL EXERESIS AND DEBRIDEMENT
Trimming may be obtained by handheld instruments such asbaskets, shaver blades or radiofrequency probes.
This surgery is aimed to ablate only the worn part of thelabrum and to trim the lesion in order to create a stable transitionarea.
Byrd reports a 10 years follow-up with 82% success rate withno arthrosic evolution of the joint.
– SUTURING AND REINSERTION BY SUTURE ANCHORS
These techniques are too recent to have a sufficient clinicalfollow-up; Kelly reports 67% success rate after 6 months and un-derlines how acetabular labrum preservation may keep hip normalfunction and prevent the development of an early arthrosis. Sincethese are very conservative techniques, they should be always pre-ferred to most common exeresis methods, when the lesion allowsit. (Figs. 7, 8)
OSTEOCHONDRAL PATHOLOGY
This is a huge chapter that includes different pathologies thatmay involve subchondral bone and joint cartilage, in its acetabularand femoral sides.
We will examine most frequent indications, such as chon-dropaties and loose bodies, and others, widely debated, such asOsteonecrosis.
86
Chapter 7
Figures 7-8
Labrum reinsertion by suture anchors
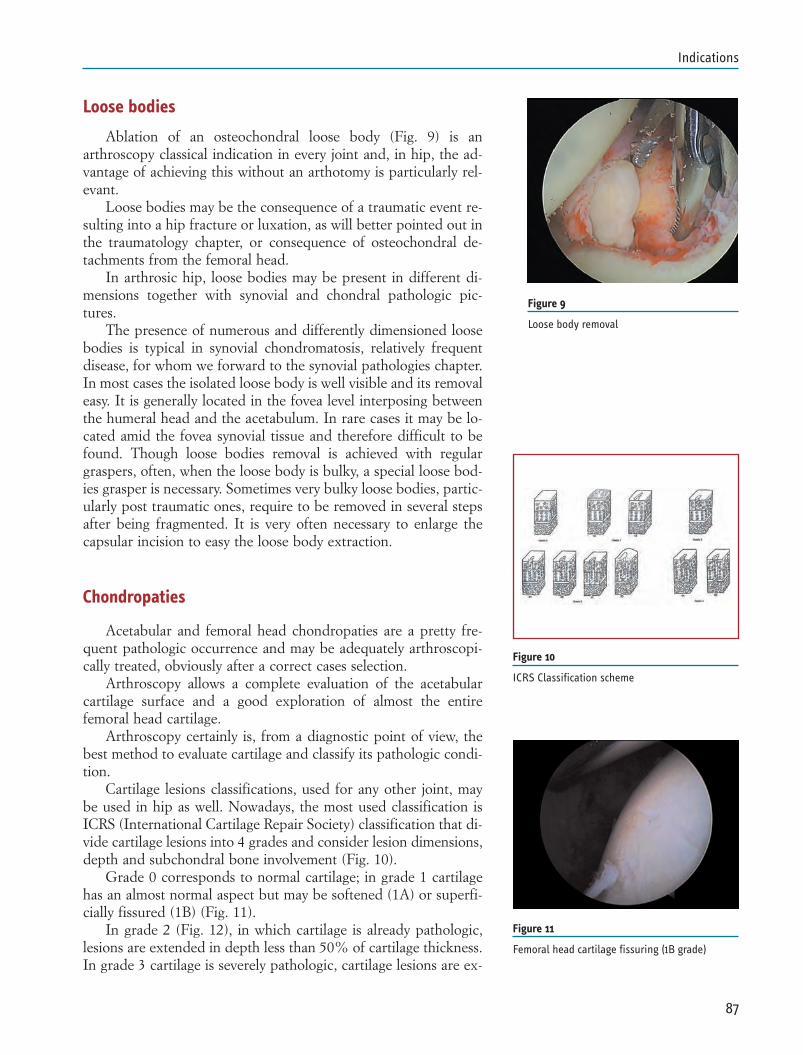
Loose bodies
Ablation of an osteochondral loose body (Fig. 9) is anarthroscopy classical indication in every joint and, in hip, the ad-vantage of achieving this without an arthotomy is particularly rel-evant.
Loose bodies may be the consequence of a traumatic event re-sulting into a hip fracture or luxation, as will better pointed out inthe traumatology chapter, or consequence of osteochondral de-tachments from the femoral head.
In arthrosic hip, loose bodies may be present in different di-mensions together with synovial and chondral pathologic pic-tures.
The presence of numerous and differently dimensioned loosebodies is typical in synovial chondromatosis, relatively frequentdisease, for whom we forward to the synovial pathologies chapter.In most cases the isolated loose body is well visible and its removaleasy. It is generally located in the fovea level interposing betweenthe humeral head and the acetabulum. In rare cases it may be lo-cated amid the fovea synovial tissue and therefore difficult to befound. Though loose bodies removal is achieved with regulargraspers, often, when the loose body is bulky, a special loose bod-ies grasper is necessary. Sometimes very bulky loose bodies, partic-ularly post traumatic ones, require to be removed in several stepsafter being fragmented. It is very often necessary to enlarge thecapsular incision to easy the loose body extraction.
Chondropaties
Acetabular and femoral head chondropaties are a pretty fre-quent pathologic occurrence and may be adequately arthroscopi-cally treated, obviously after a correct cases selection.
Arthroscopy allows a complete evaluation of the acetabularcartilage surface and a good exploration of almost the entirefemoral head cartilage.
Arthroscopy certainly is, from a diagnostic point of view, thebest method to evaluate cartilage and classify its pathologic condi-tion.
Cartilage lesions classifications, used for any other joint, maybe used in hip as well. Nowadays, the most used classification isICRS (International Cartilage Repair Society) classification that di-vide cartilage lesions into 4 grades and consider lesion dimensions,depth and subchondral bone involvement (Fig. 10).
Grade 0 corresponds to normal cartilage; in grade 1 cartilagehas an almost normal aspect but may be softened (1A) or superfi-cially fissured (1B) (Fig. 11).
In grade 2 (Fig. 12), in which cartilage is already pathologic,lesions are extended in depth less than 50% of cartilage thickness.In grade 3 cartilage is severely pathologic, cartilage lesions are ex-
87
Indications
Figure 9
Loose body removal
Figure 10
ICRS Classification scheme
Figure 11
Femoral head cartilage fissuring (1B grade)
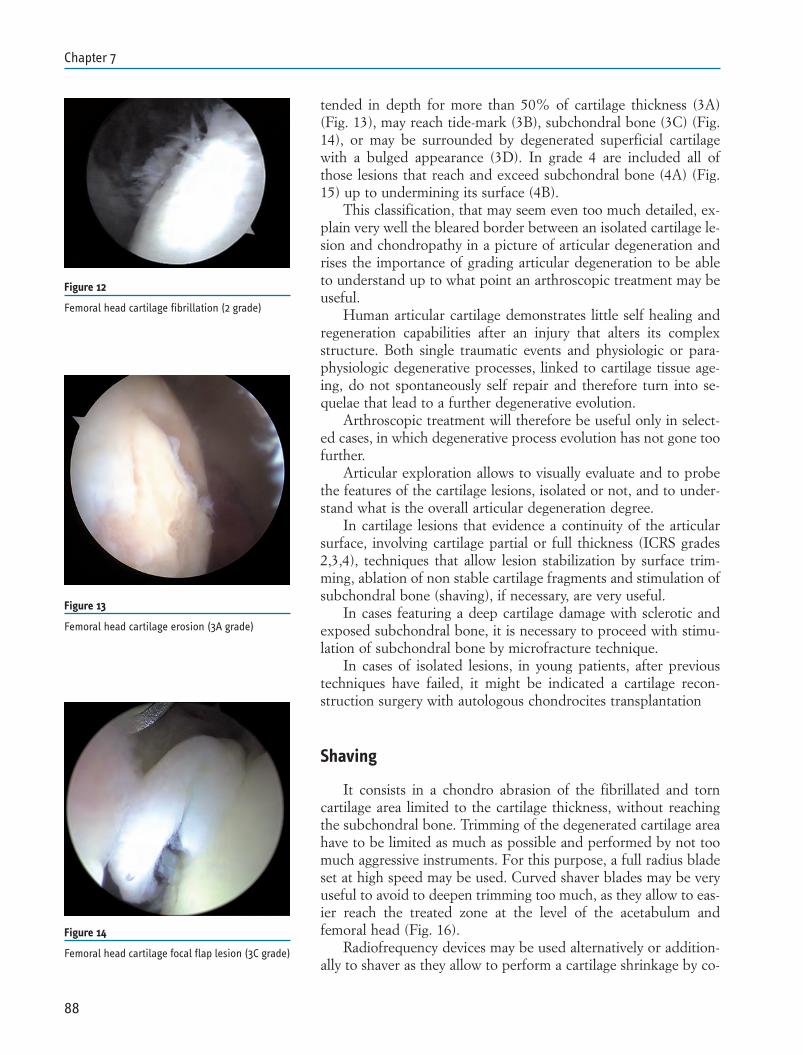
tended in depth for more than 50% of cartilage thickness (3A)(Fig. 13), may reach tide-mark (3B), subchondral bone (3C) (Fig.14), or may be surrounded by degenerated superficial cartilagewith a bulged appearance (3D). In grade 4 are included all ofthose lesions that reach and exceed subchondral bone (4A) (Fig.15) up to undermining its surface (4B).
This classification, that may seem even too much detailed, ex-plain very well the bleared border between an isolated cartilage le-sion and chondropathy in a picture of articular degeneration andrises the importance of grading articular degeneration to be ableto understand up to what point an arthroscopic treatment may beuseful.
Human articular cartilage demonstrates little self healing andregeneration capabilities after an injury that alters its complexstructure. Both single traumatic events and physiologic or para-physiologic degenerative processes, linked to cartilage tissue age-ing, do not spontaneously self repair and therefore turn into se-quelae that lead to a further degenerative evolution.
Arthroscopic treatment will therefore be useful only in select-ed cases, in which degenerative process evolution has not gone toofurther.
Articular exploration allows to visually evaluate and to probethe features of the cartilage lesions, isolated or not, and to under-stand what is the overall articular degeneration degree.
In cartilage lesions that evidence a continuity of the articularsurface, involving cartilage partial or full thickness (ICRS grades2,3,4), techniques that allow lesion stabilization by surface trim-ming, ablation of non stable cartilage fragments and stimulation ofsubchondral bone (shaving), if necessary, are very useful.
In cases featuring a deep cartilage damage with sclerotic andexposed subchondral bone, it is necessary to proceed with stimu-lation of subchondral bone by microfracture technique.
In cases of isolated lesions, in young patients, after previoustechniques have failed, it might be indicated a cartilage recon-struction surgery with autologous chondrocites transplantation
Shaving
It consists in a chondro abrasion of the fibrillated and torncartilage area limited to the cartilage thickness, without reachingthe subchondral bone. Trimming of the degenerated cartilage areahave to be limited as much as possible and performed by not toomuch aggressive instruments. For this purpose, a full radius bladeset at high speed may be used. Curved shaver blades may be veryuseful to avoid to deepen trimming too much, as they allow to eas-ier reach the treated zone at the level of the acetabulum andfemoral head (Fig. 16).
Radiofrequency devices may be used alternatively or addition-ally to shaver as they allow to perform a cartilage shrinkage by co-
88
Chapter 7
Figure 12
Femoral head cartilage fibrillation (2 grade)
Figure 13
Femoral head cartilage erosion (3A grade)
Figure 14
Femoral head cartilage focal flap lesion (3C grade)
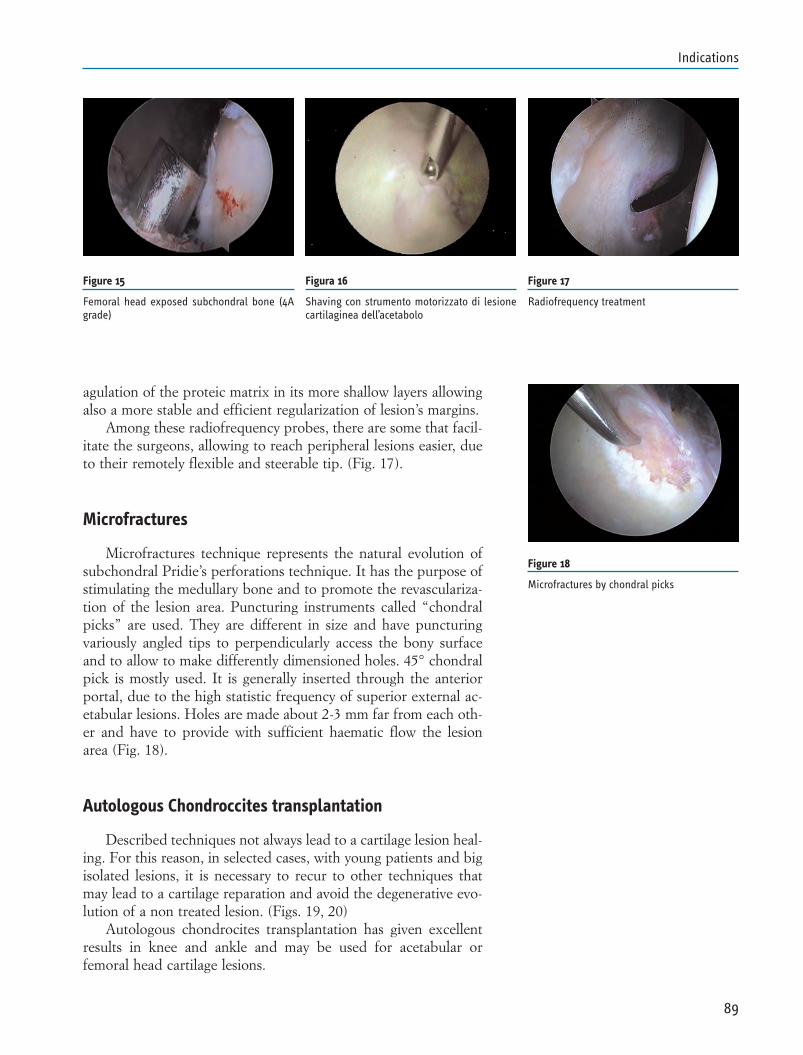
agulation of the proteic matrix in its more shallow layers allowingalso a more stable and efficient regularization of lesion’s margins.
Among these radiofrequency probes, there are some that facil-itate the surgeons, allowing to reach peripheral lesions easier, dueto their remotely flexible and steerable tip. (Fig. 17).
Microfractures
Microfractures technique represents the natural evolution ofsubchondral Pridie’s perforations technique. It has the purpose ofstimulating the medullary bone and to promote the revasculariza-tion of the lesion area. Puncturing instruments called “chondralpicks” are used. They are different in size and have puncturingvariously angled tips to perpendicularly access the bony surfaceand to allow to make differently dimensioned holes. 45° chondralpick is mostly used. It is generally inserted through the anteriorportal, due to the high statistic frequency of superior external ac-etabular lesions. Holes are made about 2-3 mm far from each oth-er and have to provide with sufficient haematic flow the lesionarea (Fig. 18).
Autologous Chondroccites transplantation
Described techniques not always lead to a cartilage lesion heal-ing. For this reason, in selected cases, with young patients and bigisolated lesions, it is necessary to recur to other techniques thatmay lead to a cartilage reparation and avoid the degenerative evo-lution of a non treated lesion. (Figs. 19, 20)
Autologous chondrocites transplantation has given excellentresults in knee and ankle and may be used for acetabular orfemoral head cartilage lesions.
89
Indications
Figure 15
Femoral head exposed subchondral bone (4Agrade)
Figura 16
Shaving con strumento motorizzato di lesionecartilaginea dell’acetabolo
Figure 17
Radiofrequency treatment
Figure 18
Microfractures by chondral picks
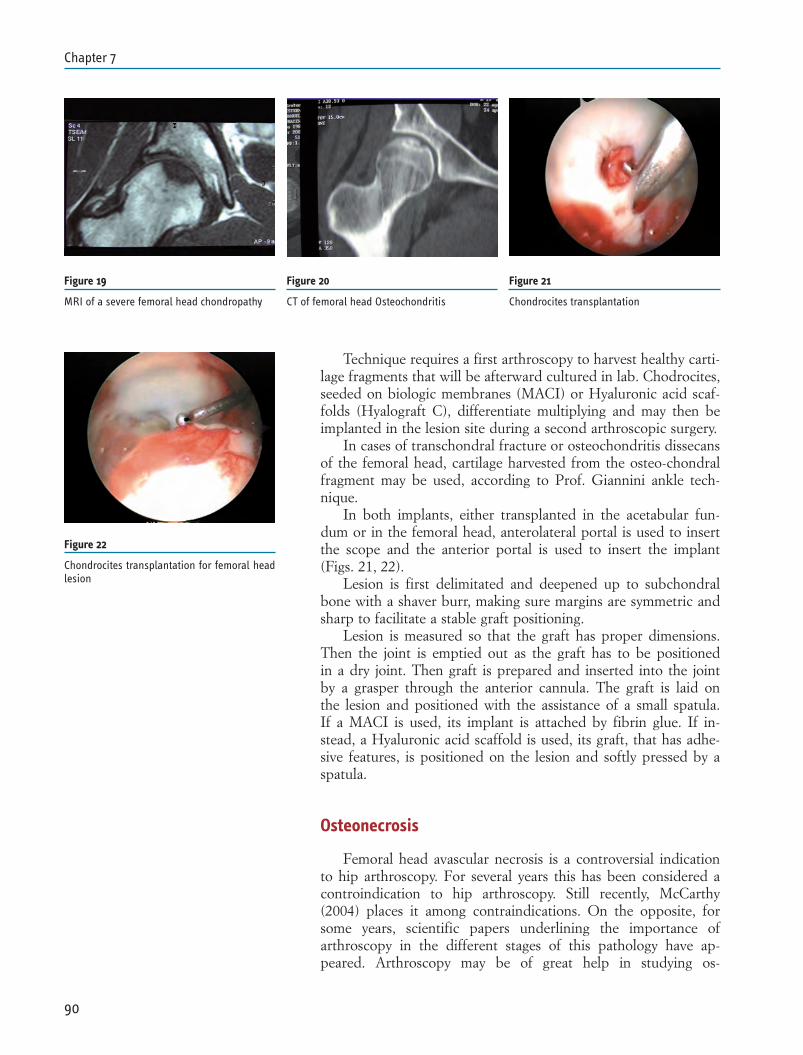
Technique requires a first arthroscopy to harvest healthy carti-lage fragments that will be afterward cultured in lab. Chodrocites,seeded on biologic membranes (MACI) or Hyaluronic acid scaf-folds (Hyalograft C), differentiate multiplying and may then beimplanted in the lesion site during a second arthroscopic surgery.
In cases of transchondral fracture or osteochondritis dissecansof the femoral head, cartilage harvested from the osteo-chondralfragment may be used, according to Prof. Giannini ankle tech-nique.
In both implants, either transplanted in the acetabular fun-dum or in the femoral head, anterolateral portal is used to insertthe scope and the anterior portal is used to insert the implant(Figs. 21, 22).
Lesion is first delimitated and deepened up to subchondralbone with a shaver burr, making sure margins are symmetric andsharp to facilitate a stable graft positioning.
Lesion is measured so that the graft has proper dimensions.Then the joint is emptied out as the graft has to be positionedin a dry joint. Then graft is prepared and inserted into the jointby a grasper through the anterior cannula. The graft is laid onthe lesion and positioned with the assistance of a small spatula.If a MACI is used, its implant is attached by fibrin glue. If in-stead, a Hyaluronic acid scaffold is used, its graft, that has adhe-sive features, is positioned on the lesion and softly pressed by aspatula.
Osteonecrosis
Femoral head avascular necrosis is a controversial indicationto hip arthroscopy. For several years this has been considered acontroindication to hip arthroscopy. Still recently, McCarthy(2004) places it among contraindications. On the opposite, forsome years, scientific papers underlining the importance ofarthroscopy in the different stages of this pathology have ap-peared. Arthroscopy may be of great help in studying os-
90
Chapter 7
Figure 19
MRI of a severe femoral head chondropathy
Figure 20
CT of femoral head Osteochondritis
Figure 21
Chondrocites transplantation
Figure 22
Chondrocites transplantation for femoral headlesion
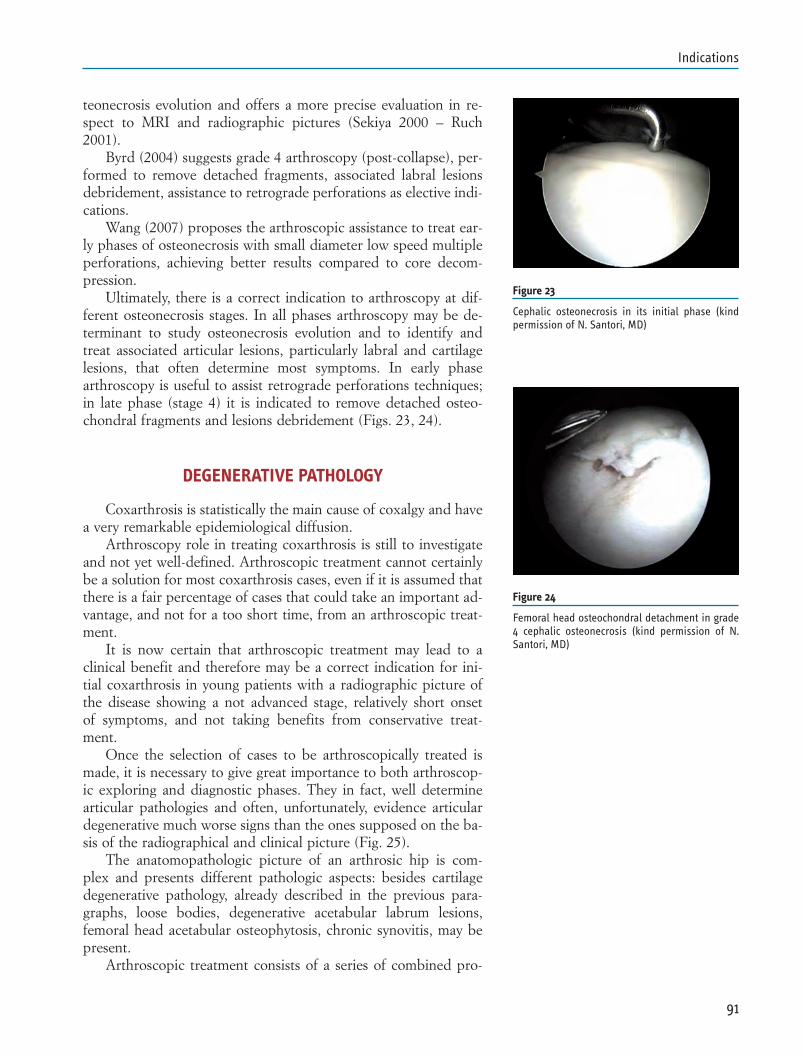
teonecrosis evolution and offers a more precise evaluation in re-spect to MRI and radiographic pictures (Sekiya 2000 – Ruch2001).
Byrd (2004) suggests grade 4 arthroscopy (post-collapse), per-formed to remove detached fragments, associated labral lesionsdebridement, assistance to retrograde perforations as elective indi-cations.
Wang (2007) proposes the arthroscopic assistance to treat ear-ly phases of osteonecrosis with small diameter low speed multipleperforations, achieving better results compared to core decom-pression.
Ultimately, there is a correct indication to arthroscopy at dif-ferent osteonecrosis stages. In all phases arthroscopy may be de-terminant to study osteonecrosis evolution and to identify andtreat associated articular lesions, particularly labral and cartilagelesions, that often determine most symptoms. In early phasearthroscopy is useful to assist retrograde perforations techniques;in late phase (stage 4) it is indicated to remove detached osteo-chondral fragments and lesions debridement (Figs. 23, 24).
DEGENERATIVE PATHOLOGY
Coxarthrosis is statistically the main cause of coxalgy and havea very remarkable epidemiological diffusion.
Arthroscopy role in treating coxarthrosis is still to investigateand not yet well-defined. Arthroscopic treatment cannot certainlybe a solution for most coxarthrosis cases, even if it is assumed thatthere is a fair percentage of cases that could take an important ad-vantage, and not for a too short time, from an arthroscopic treat-ment.
It is now certain that arthroscopic treatment may lead to aclinical benefit and therefore may be a correct indication for ini-tial coxarthrosis in young patients with a radiographic picture ofthe disease showing a not advanced stage, relatively short onsetof symptoms, and not taking benefits from conservative treat-ment.
Once the selection of cases to be arthroscopically treated ismade, it is necessary to give great importance to both arthroscop-ic exploring and diagnostic phases. They in fact, well determinearticular pathologies and often, unfortunately, evidence articulardegenerative much worse signs than the ones supposed on the ba-sis of the radiographical and clinical picture (Fig. 25).
The anatomopathologic picture of an arthrosic hip is com-plex and presents different pathologic aspects: besides cartilagedegenerative pathology, already described in the previous para-graphs, loose bodies, degenerative acetabular labrum lesions,femoral head acetabular osteophytosis, chronic synovitis, may bepresent.
Arthroscopic treatment consists of a series of combined pro-
91
Indications
Figure 23
Cephalic osteonecrosis in its initial phase (kindpermission of N. Santori, MD)
Figure 24
Femoral head osteochondral detachment in grade4 cephalic osteonecrosis (kind permission of N.Santori, MD)
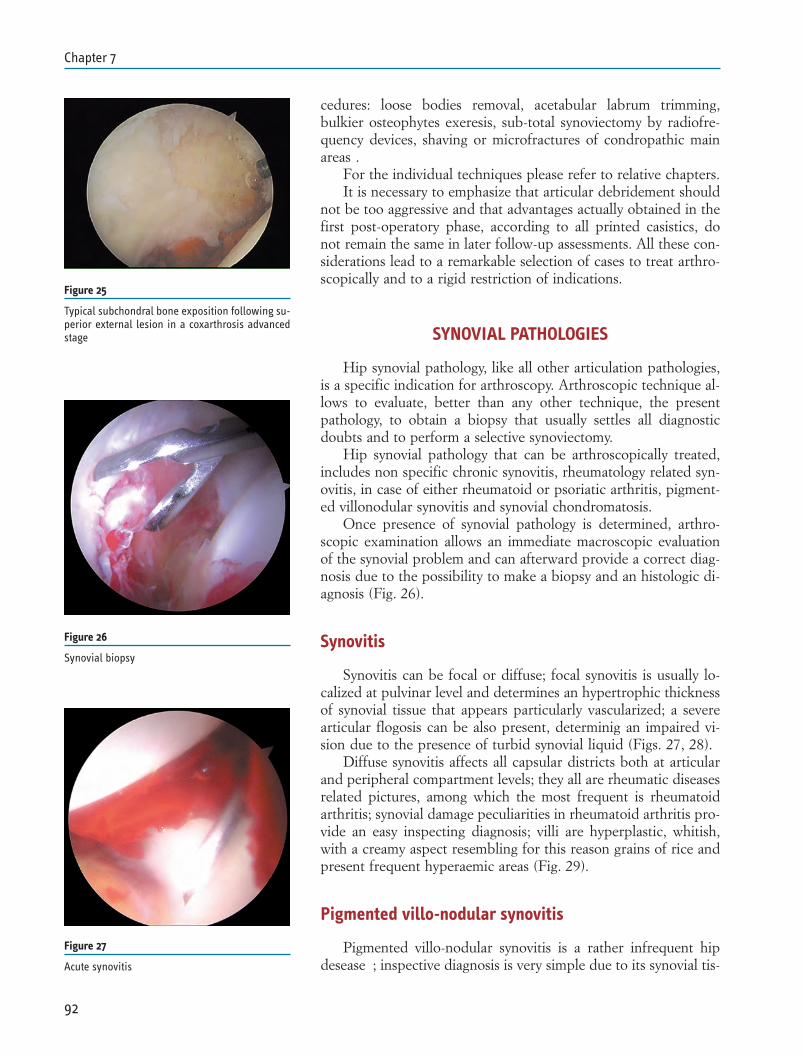
cedures: loose bodies removal, acetabular labrum trimming,bulkier osteophytes exeresis, sub-total synoviectomy by radiofre-quency devices, shaving or microfractures of condropathic mainareas .
For the individual techniques please refer to relative chapters.It is necessary to emphasize that articular debridement should
not be too aggressive and that advantages actually obtained in thefirst post-operatory phase, according to all printed casistics, donot remain the same in later follow-up assessments. All these con-siderations lead to a remarkable selection of cases to treat arthro-scopically and to a rigid restriction of indications.
SYNOVIAL PATHOLOGIES
Hip synovial pathology, like all other articulation pathologies,is a specific indication for arthroscopy. Arthroscopic technique al-lows to evaluate, better than any other technique, the presentpathology, to obtain a biopsy that usually settles all diagnosticdoubts and to perform a selective synoviectomy.
Hip synovial pathology that can be arthroscopically treated,includes non specific chronic synovitis, rheumatology related syn-ovitis, in case of either rheumatoid or psoriatic arthritis, pigment-ed villonodular synovitis and synovial chondromatosis.
Once presence of synovial pathology is determined, arthro-scopic examination allows an immediate macroscopic evaluationof the synovial problem and can afterward provide a correct diag-nosis due to the possibility to make a biopsy and an histologic di-agnosis (Fig. 26).
Synovitis
Synovitis can be focal or diffuse; focal synovitis is usually lo-calized at pulvinar level and determines an hypertrophic thicknessof synovial tissue that appears particularly vascularized; a severearticular flogosis can be also present, determinig an impaired vi-sion due to the presence of turbid synovial liquid (Figs. 27, 28).
Diffuse synovitis affects all capsular districts both at articularand peripheral compartment levels; they all are rheumatic diseasesrelated pictures, among which the most frequent is rheumatoidarthritis; synovial damage peculiarities in rheumatoid arthritis pro-vide an easy inspecting diagnosis; villi are hyperplastic, whitish,with a creamy aspect resembling for this reason grains of rice andpresent frequent hyperaemic areas (Fig. 29).
Pigmented villo-nodular synovitis
Pigmented villo-nodular synovitis is a rather infrequent hipdesease ; inspective diagnosis is very simple due to its synovial tis-
92
Chapter 7
Figure 25
Typical subchondral bone exposition following su-perior external lesion in a coxarthrosis advancedstage
Figure 26
Synovial biopsy
Figure 27
Acute synovitis
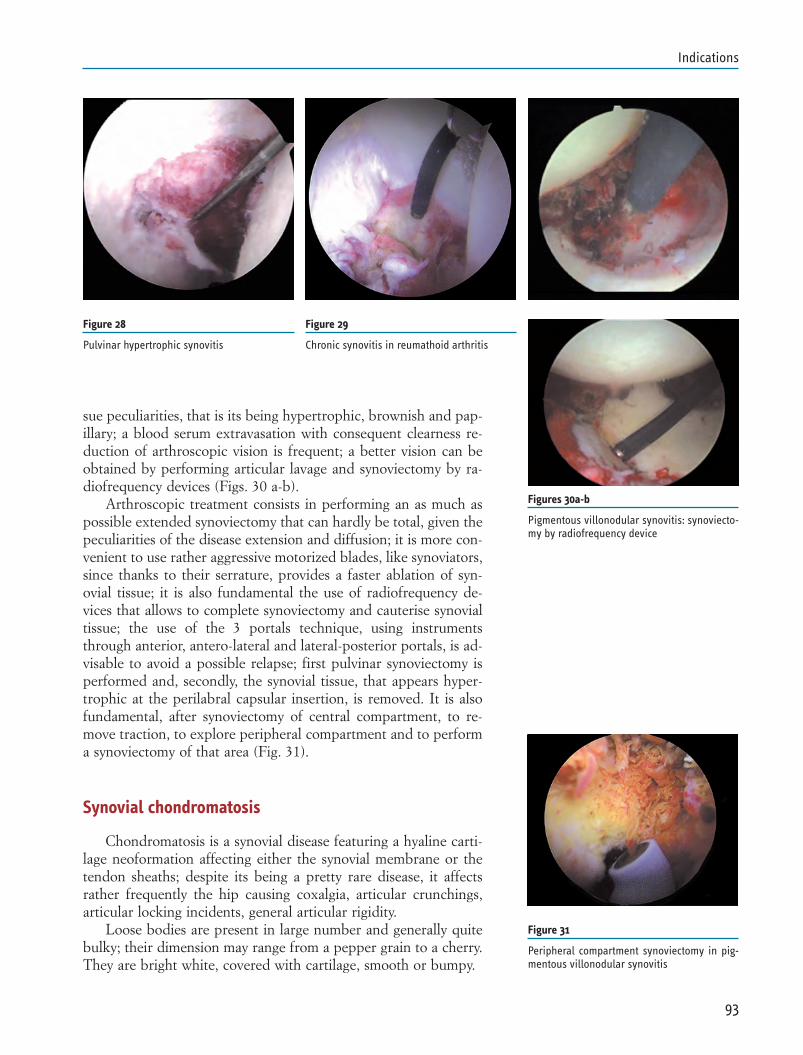
sue peculiarities, that is its being hypertrophic, brownish and pap-illary; a blood serum extravasation with consequent clearness re-duction of arthroscopic vision is frequent; a better vision can beobtained by performing articular lavage and synoviectomy by ra-diofrequency devices (Figs. 30 a-b).
Arthroscopic treatment consists in performing an as much aspossible extended synoviectomy that can hardly be total, given thepeculiarities of the disease extension and diffusion; it is more con-venient to use rather aggressive motorized blades, like synoviators,since thanks to their serrature, provides a faster ablation of syn-ovial tissue; it is also fundamental the use of radiofrequency de-vices that allows to complete synoviectomy and cauterise synovialtissue; the use of the 3 portals technique, using instrumentsthrough anterior, antero-lateral and lateral-posterior portals, is ad-visable to avoid a possible relapse; first pulvinar synoviectomy isperformed and, secondly, the synovial tissue, that appears hyper-trophic at the perilabral capsular insertion, is removed. It is alsofundamental, after synoviectomy of central compartment, to re-move traction, to explore peripheral compartment and to performa synoviectomy of that area (Fig. 31).
Synovial chondromatosis
Chondromatosis is a synovial disease featuring a hyaline carti-lage neoformation affecting either the synovial membrane or thetendon sheaths; despite its being a pretty rare disease, it affectsrather frequently the hip causing coxalgia, articular crunchings,articular locking incidents, general articular rigidity.
Loose bodies are present in large number and generally quitebulky; their dimension may range from a pepper grain to a cherry.They are bright white, covered with cartilage, smooth or bumpy.
93
Indications
Figure 28
Pulvinar hypertrophic synovitis
Figure 29
Chronic synovitis in reumathoid arthritis
Figures 30a-b
Pigmentous villonodular synovitis: synoviecto-my by radiofrequency device
Figure 31
Peripheral compartment synoviectomy in pig-mentous villonodular synovitis
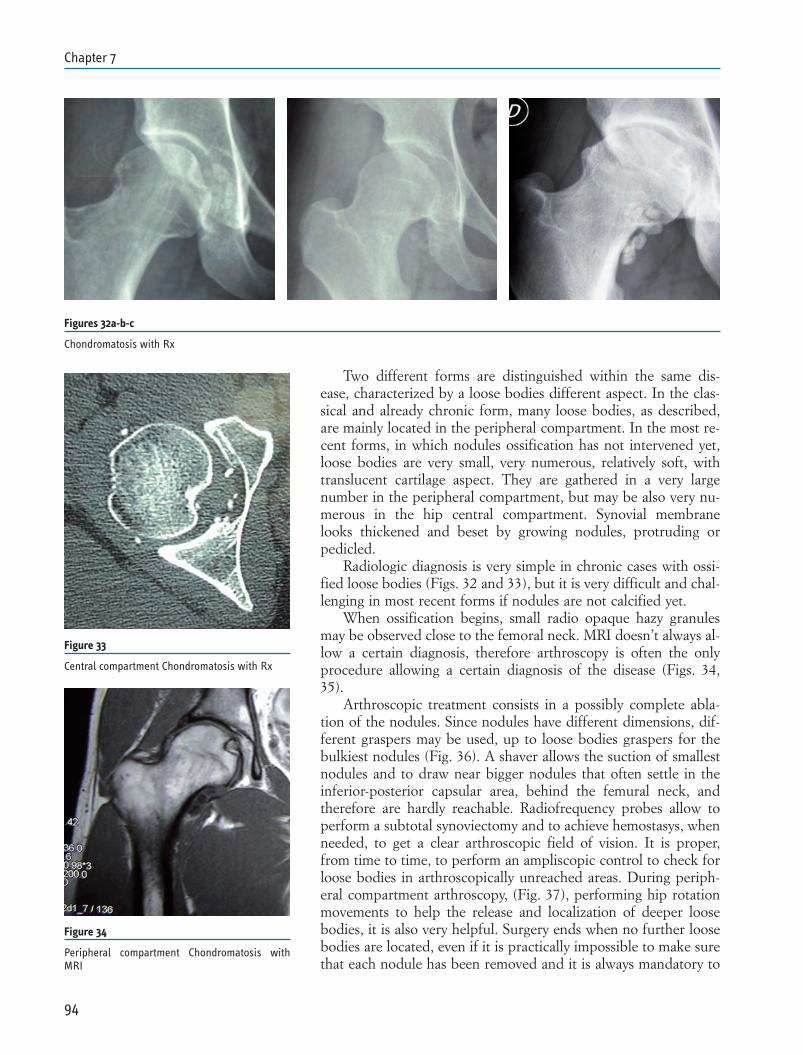
Two different forms are distinguished within the same dis-ease, characterized by a loose bodies different aspect. In the clas-sical and already chronic form, many loose bodies, as described,are mainly located in the peripheral compartment. In the most re-cent forms, in which nodules ossification has not intervened yet,loose bodies are very small, very numerous, relatively soft, withtranslucent cartilage aspect. They are gathered in a very largenumber in the peripheral compartment, but may be also very nu-merous in the hip central compartment. Synovial membranelooks thickened and beset by growing nodules, protruding orpedicled.
Radiologic diagnosis is very simple in chronic cases with ossi-fied loose bodies (Figs. 32 and 33), but it is very difficult and chal-lenging in most recent forms if nodules are not calcified yet.
When ossification begins, small radio opaque hazy granulesmay be observed close to the femoral neck. MRI doesn’t always al-low a certain diagnosis, therefore arthroscopy is often the onlyprocedure allowing a certain diagnosis of the disease (Figs. 34,35).
Arthroscopic treatment consists in a possibly complete abla-tion of the nodules. Since nodules have different dimensions, dif-ferent graspers may be used, up to loose bodies graspers for thebulkiest nodules (Fig. 36). A shaver allows the suction of smallestnodules and to draw near bigger nodules that often settle in theinferior-posterior capsular area, behind the femural neck, andtherefore are hardly reachable. Radiofrequency probes allow toperform a subtotal synoviectomy and to achieve hemostasys, whenneeded, to get a clear arthroscopic field of vision. It is proper,from time to time, to perform an ampliscopic control to check forloose bodies in arthroscopically unreached areas. During periph-eral compartment arthroscopy, (Fig. 37), performing hip rotationmovements to help the release and localization of deeper loosebodies, it is also very helpful. Surgery ends when no further loosebodies are located, even if it is practically impossible to make surethat each nodule has been removed and it is always mandatory to
94
Chapter 7
Figures 32a-b-c
Chondromatosis with Rx
Figure 33
Central compartment Chondromatosis with Rx
Figure 34
Peripheral compartment Chondromatosis withMRI
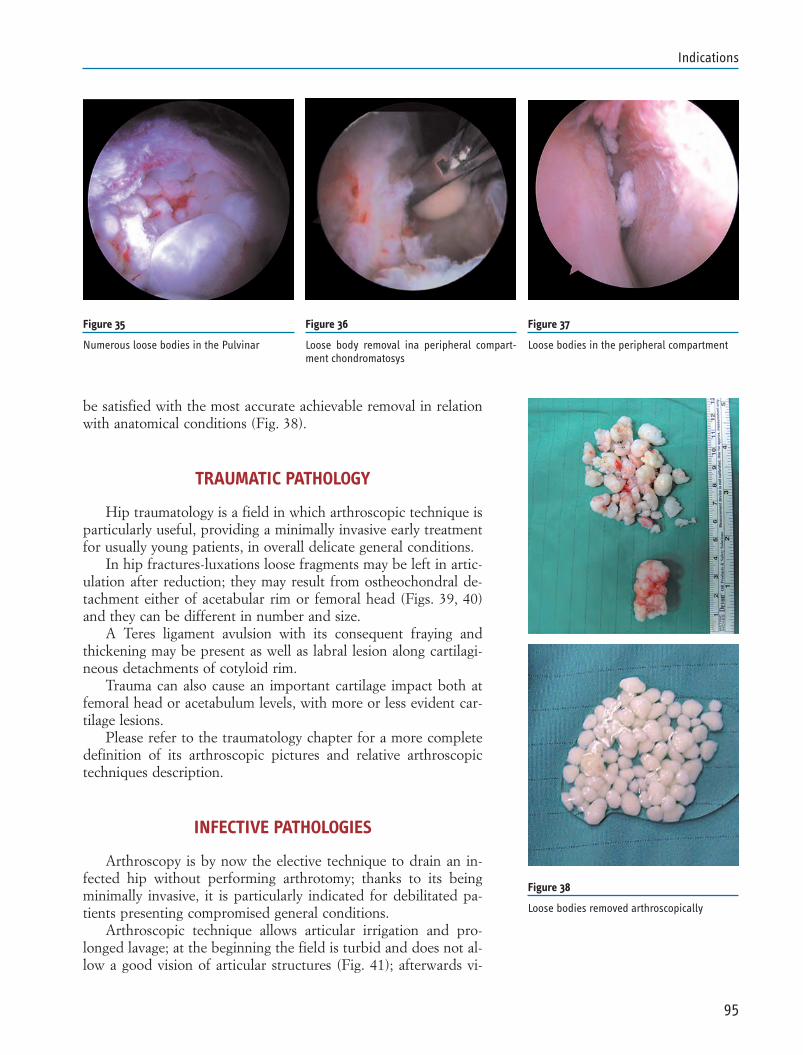
be satisfied with the most accurate achievable removal in relationwith anatomical conditions (Fig. 38).
TRAUMATIC PATHOLOGY
Hip traumatology is a field in which arthroscopic technique isparticularly useful, providing a minimally invasive early treatmentfor usually young patients, in overall delicate general conditions.
In hip fractures-luxations loose fragments may be left in artic-ulation after reduction; they may result from ostheochondral de-tachment either of acetabular rim or femoral head (Figs. 39, 40)and they can be different in number and size.
A Teres ligament avulsion with its consequent fraying andthickening may be present as well as labral lesion along cartilagi-neous detachments of cotyloid rim.
Trauma can also cause an important cartilage impact both atfemoral head or acetabulum levels, with more or less evident car-tilage lesions.
Please refer to the traumatology chapter for a more completedefinition of its arthroscopic pictures and relative arthroscopictechniques description.
INFECTIVE PATHOLOGIES
Arthroscopy is by now the elective technique to drain an in-fected hip without performing arthrotomy; thanks to its beingminimally invasive, it is particularly indicated for debilitated pa-tients presenting compromised general conditions.
Arthroscopic technique allows articular irrigation and pro-longed lavage; at the beginning the field is turbid and does not al-low a good vision of articular structures (Fig. 41); afterwards vi-
95
Indications
Figure 35
Numerous loose bodies in the Pulvinar
Figure 37
Loose bodies in the peripheral compartment
Figure 36
Loose body removal ina peripheral compart-ment chondromatosys
Figure 38
Loose bodies removed arthroscopically
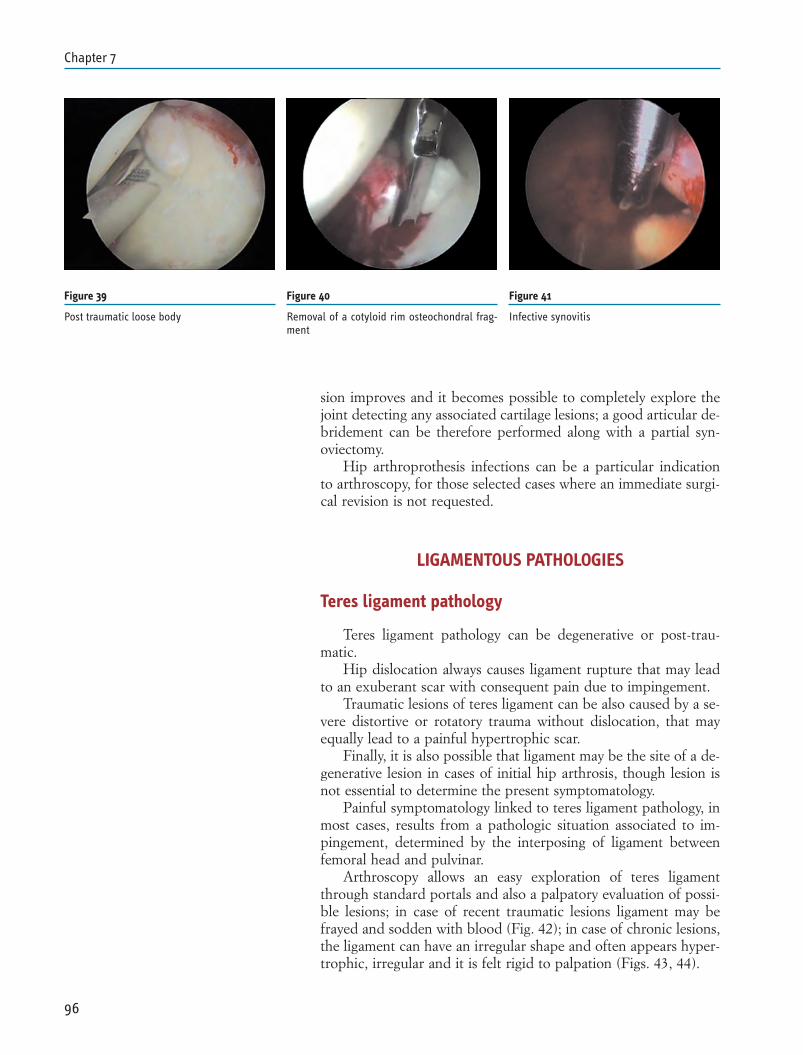
sion improves and it becomes possible to completely explore thejoint detecting any associated cartilage lesions; a good articular de-bridement can be therefore performed along with a partial syn-oviectomy.
Hip arthroprothesis infections can be a particular indicationto arthroscopy, for those selected cases where an immediate surgi-cal revision is not requested.
LIGAMENTOUS PATHOLOGIES
Teres ligament pathology
Teres ligament pathology can be degenerative or post-trau-matic.
Hip dislocation always causes ligament rupture that may leadto an exuberant scar with consequent pain due to impingement.
Traumatic lesions of teres ligament can be also caused by a se-vere distortive or rotatory trauma without dislocation, that mayequally lead to a painful hypertrophic scar.
Finally, it is also possible that ligament may be the site of a de-generative lesion in cases of initial hip arthrosis, though lesion isnot essential to determine the present symptomatology.
Painful symptomatology linked to teres ligament pathology, inmost cases, results from a pathologic situation associated to im-pingement, determined by the interposing of ligament betweenfemoral head and pulvinar.
Arthroscopy allows an easy exploration of teres ligamentthrough standard portals and also a palpatory evaluation of possi-ble lesions; in case of recent traumatic lesions ligament may befrayed and sodden with blood (Fig. 42); in case of chronic lesions,the ligament can have an irregular shape and often appears hyper-trophic, irregular and it is felt rigid to palpation (Figs. 43, 44).
96
Chapter 7
Figure 39
Post traumatic loose body
Figure 40
Removal of a cotyloid rim osteochondral frag-ment
Figure 41
Infective synovitis
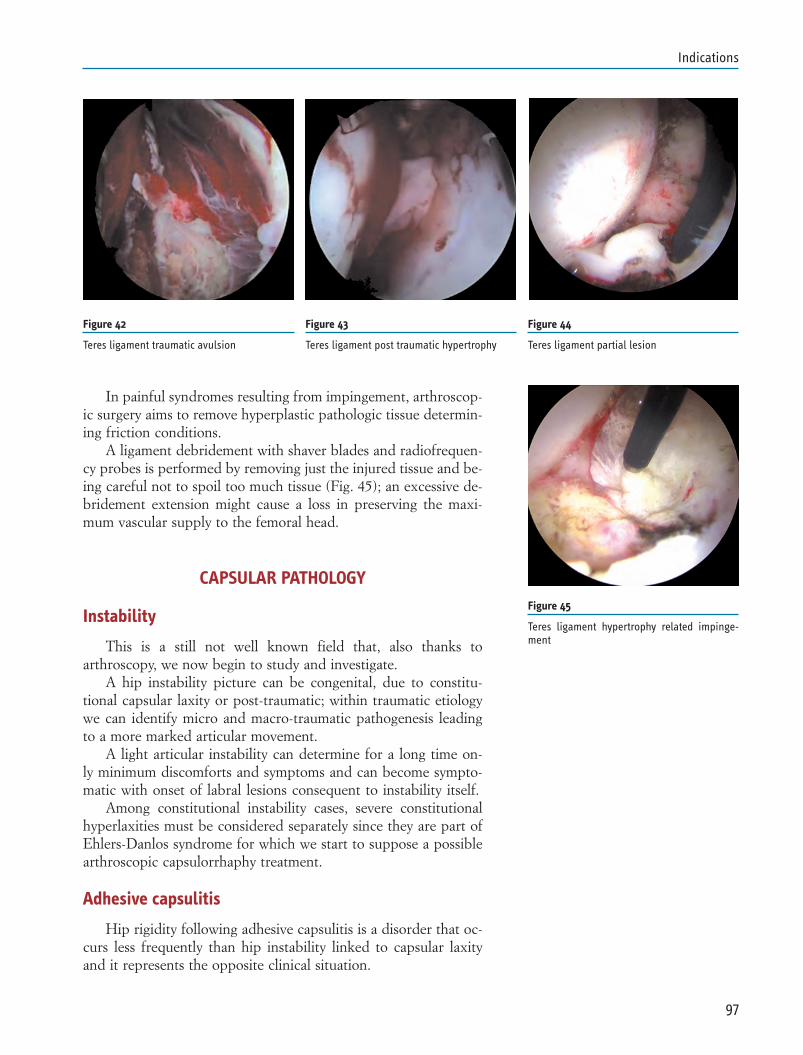
In painful syndromes resulting from impingement, arthroscop-ic surgery aims to remove hyperplastic pathologic tissue determin-ing friction conditions.
A ligament debridement with shaver blades and radiofrequen-cy probes is performed by removing just the injured tissue and be-ing careful not to spoil too much tissue (Fig. 45); an excessive de-bridement extension might cause a loss in preserving the maxi-mum vascular supply to the femoral head.
CAPSULAR PATHOLOGY
Instability
This is a still not well known field that, also thanks toarthroscopy, we now begin to study and investigate.
A hip instability picture can be congenital, due to constitu-tional capsular laxity or post-traumatic; within traumatic etiologywe can identify micro and macro-traumatic pathogenesis leadingto a more marked articular movement.
A light articular instability can determine for a long time on-ly minimum discomforts and symptoms and can become sympto-matic with onset of labral lesions consequent to instability itself.
Among constitutional instability cases, severe constitutionalhyperlaxities must be considered separately since they are part ofEhlers-Danlos syndrome for which we start to suppose a possiblearthroscopic capsulorrhaphy treatment.
Adhesive capsulitis
Hip rigidity following adhesive capsulitis is a disorder that oc-curs less frequently than hip instability linked to capsular laxityand it represents the opposite clinical situation.
97
Indications
Figure 42
Teres ligament traumatic avulsion
Figure 43
Teres ligament post traumatic hypertrophy
Figure 44
Teres ligament partial lesion
Figure 45
Teres ligament hypertrophy related impinge-ment
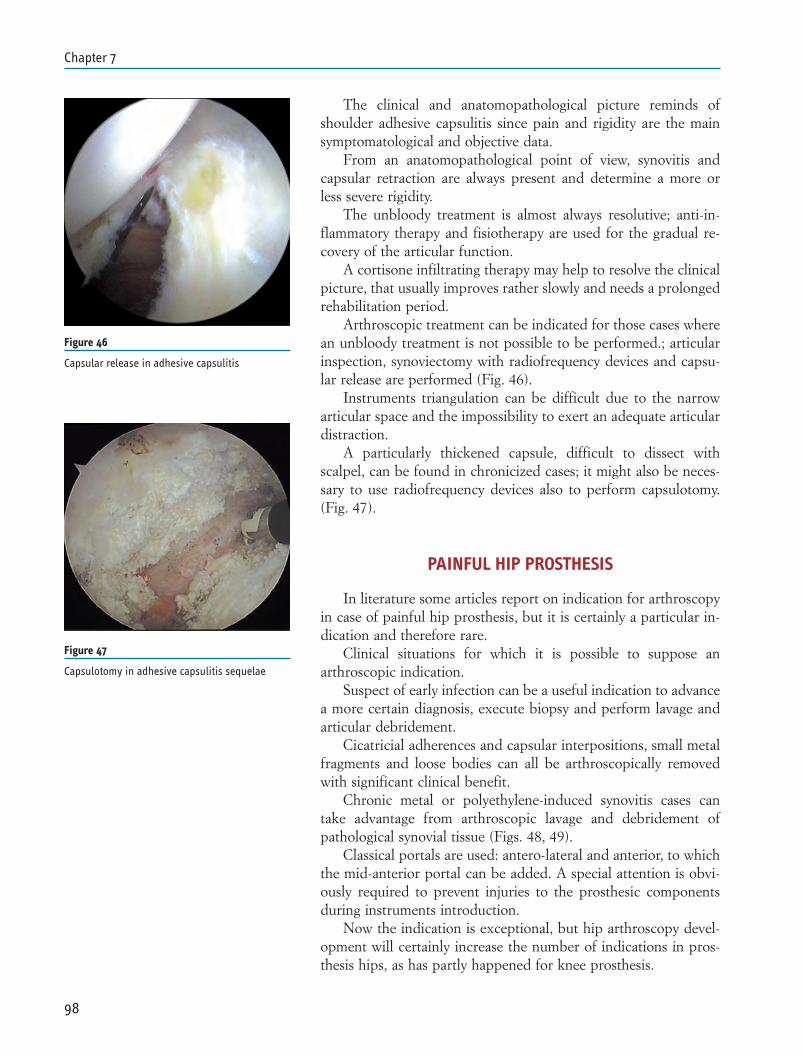
The clinical and anatomopathological picture reminds ofshoulder adhesive capsulitis since pain and rigidity are the mainsymptomatological and objective data.
From an anatomopathological point of view, synovitis andcapsular retraction are always present and determine a more orless severe rigidity.
The unbloody treatment is almost always resolutive; anti-in-flammatory therapy and fisiotherapy are used for the gradual re-covery of the articular function.
A cortisone infiltrating therapy may help to resolve the clinicalpicture, that usually improves rather slowly and needs a prolongedrehabilitation period.
Arthroscopic treatment can be indicated for those cases wherean unbloody treatment is not possible to be performed.; articularinspection, synoviectomy with radiofrequency devices and capsu-lar release are performed (Fig. 46).
Instruments triangulation can be difficult due to the narrowarticular space and the impossibility to exert an adequate articulardistraction.
A particularly thickened capsule, difficult to dissect withscalpel, can be found in chronicized cases; it might also be neces-sary to use radiofrequency devices also to perform capsulotomy.(Fig. 47).
PAINFUL HIP PROSTHESIS
In literature some articles report on indication for arthroscopyin case of painful hip prosthesis, but it is certainly a particular in-dication and therefore rare.
Clinical situations for which it is possible to suppose anarthroscopic indication.
Suspect of early infection can be a useful indication to advancea more certain diagnosis, execute biopsy and perform lavage andarticular debridement.
Cicatricial adherences and capsular interpositions, small metalfragments and loose bodies can all be arthroscopically removedwith significant clinical benefit.
Chronic metal or polyethylene-induced synovitis cases cantake advantage from arthroscopic lavage and debridement ofpathological synovial tissue (Figs. 48, 49).
Classical portals are used: antero-lateral and anterior, to whichthe mid-anterior portal can be added. A special attention is obvi-ously required to prevent injuries to the prosthesic componentsduring instruments introduction.
Now the indication is exceptional, but hip arthroscopy devel-opment will certainly increase the number of indications in pros-thesis hips, as has partly happened for knee prosthesis.
98
Chapter 7
Figure 46
Capsular release in adhesive capsulitis
Figure 47
Capsulotomy in adhesive capsulitis sequelae
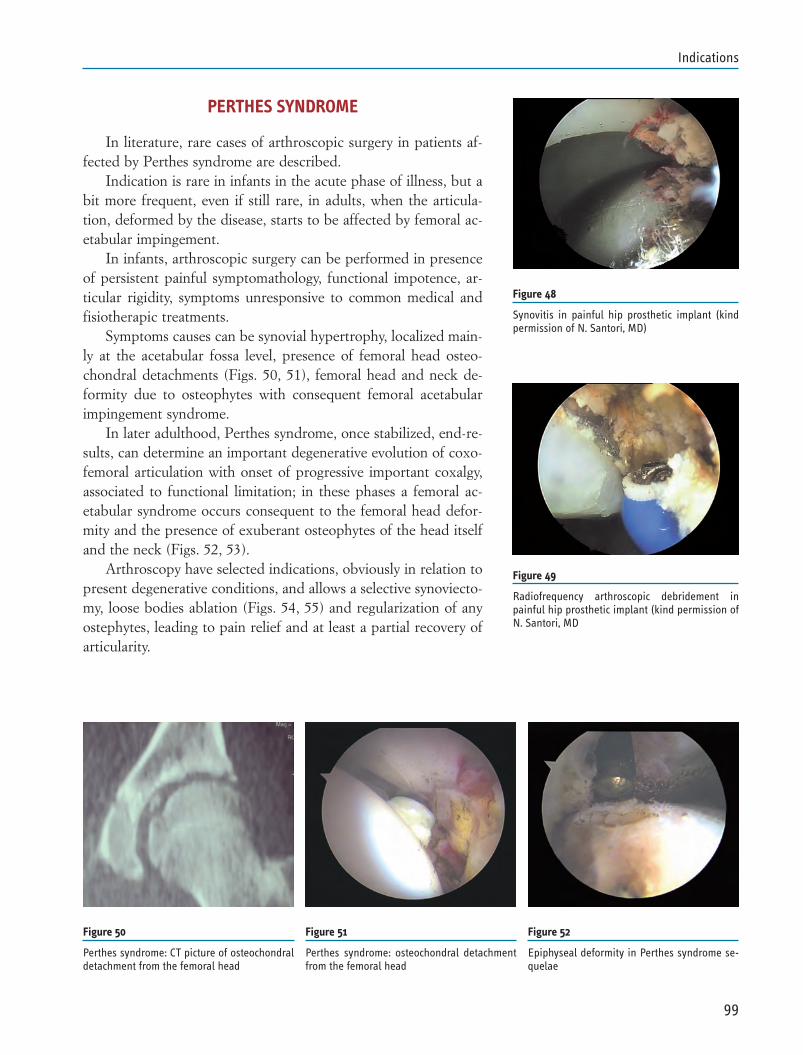
PERTHES SYNDROME
In literature, rare cases of arthroscopic surgery in patients af-fected by Perthes syndrome are described.
Indication is rare in infants in the acute phase of illness, but abit more frequent, even if still rare, in adults, when the articula-tion, deformed by the disease, starts to be affected by femoral ac-etabular impingement.
In infants, arthroscopic surgery can be performed in presenceof persistent painful symptomathology, functional impotence, ar-ticular rigidity, symptoms unresponsive to common medical andfisiotherapic treatments.
Symptoms causes can be synovial hypertrophy, localized main-ly at the acetabular fossa level, presence of femoral head osteo-chondral detachments (Figs. 50, 51), femoral head and neck de-formity due to osteophytes with consequent femoral acetabularimpingement syndrome.
In later adulthood, Perthes syndrome, once stabilized, end-re-sults, can determine an important degenerative evolution of coxo-femoral articulation with onset of progressive important coxalgy,associated to functional limitation; in these phases a femoral ac-etabular syndrome occurs consequent to the femoral head defor-mity and the presence of exuberant osteophytes of the head itselfand the neck (Figs. 52, 53).
Arthroscopy have selected indications, obviously in relation topresent degenerative conditions, and allows a selective synoviecto-my, loose bodies ablation (Figs. 54, 55) and regularization of anyostephytes, leading to pain relief and at least a partial recovery ofarticularity.
99
Indications
Figure 48
Synovitis in painful hip prosthetic implant (kindpermission of N. Santori, MD)
Figure 49
Radiofrequency arthroscopic debridement inpainful hip prosthetic implant (kind permission ofN. Santori, MD
Figure 50
Perthes syndrome: CT picture of osteochondraldetachment from the femoral head
Figure 51
Perthes syndrome: osteochondral detachmentfrom the femoral head
Figure 52
Epiphyseal deformity in Perthes syndrome se-quelae
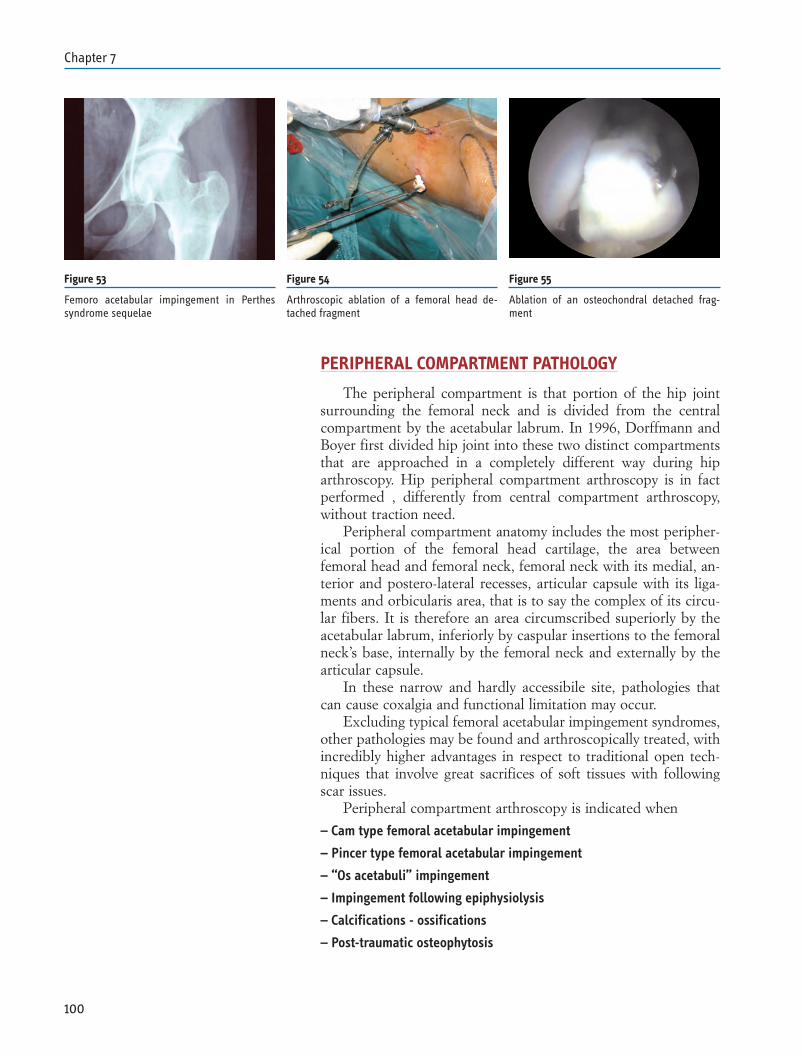
PERIPHERAL COMPARTMENT PATHOLOGY
The peripheral compartment is that portion of the hip jointsurrounding the femoral neck and is divided from the centralcompartment by the acetabular labrum. In 1996, Dorffmann andBoyer first divided hip joint into these two distinct compartmentsthat are approached in a completely different way during hiparthroscopy. Hip peripheral compartment arthroscopy is in factperformed , differently from central compartment arthroscopy,without traction need.
Peripheral compartment anatomy includes the most peripher-ical portion of the femoral head cartilage, the area betweenfemoral head and femoral neck, femoral neck with its medial, an-terior and postero-lateral recesses, articular capsule with its liga-ments and orbicularis area, that is to say the complex of its circu-lar fibers. It is therefore an area circumscribed superiorly by theacetabular labrum, inferiorly by caspular insertions to the femoralneck’s base, internally by the femoral neck and externally by thearticular capsule.
In these narrow and hardly accessibile site, pathologies thatcan cause coxalgia and functional limitation may occur.
Excluding typical femoral acetabular impingement syndromes,other pathologies may be found and arthroscopically treated, withincredibly higher advantages in respect to traditional open tech-niques that involve great sacrifices of soft tissues with followingscar issues.
Peripheral compartment arthroscopy is indicated when
– Cam type femoral acetabular impingement
– Pincer type femoral acetabular impingement
– “Os acetabuli” impingement
– Impingement following epiphysiolysis
– Calcifications - ossifications
– Post-traumatic osteophytosis
100
Chapter 7
Figure 53
Femoro acetabular impingement in Perthessyndrome sequelae
Figure 54
Arthroscopic ablation of a femoral head de-tached fragment
Figure 55
Ablation of an osteochondral detached frag-ment

FEMORO-ACETABULAR IMPINGEMENT
Femoral acetabular impingement is that syndrome determinedby different conditions leading to a conflict between femoral headand cotyloid rim.
The produced friction leads to a progressive wearing of the ac-etabular labrum and a cartilage damage, evolving into an arthrosicpicture over time.
Impingement favoring conditions are congenital malforma-tions altering either acetabular or femoral neck morphology.These determine different pathological pictures called pincer-typeand cam-type respectively.
In pincer impingement morphologic alteration occurs againstthe acetabulum and consists of an acetabular rim prominence withovercoverage and consequent early contact between femoral headand acetabulum (Fig. 56).
This leads to a labral lesion while cartilage remains intact for along time. Cartilage wear appears lately in the postero-inferiorside of the head and leads to an either postero-superior or centralosteoarthrosis.
In cam impingement, morphologic alteration occurs insteadagainst the head-neck junction that appears aspherical; the bonyprominence bumps against the rim leading to an acetabularlabrum flap lesion and a progressive damage to the acetabular car-tilage (Fig. 57); picture evolves into an antero-superior os-theoarthrosis; this is a typical pathology occurring in young males,usually related to sporting activity.
Femoral-acetabular impingement gathers a high percentage ofhip arthroscopic indications achieving better results in proportionto the earliness of diagnosis and treatment.
Arthroscopy is performed starting from central compartment,making an evaluation of acetabular labrum and its pathology, ac-etabular cartilage and femoral head.
Then we pass to the peripheral compartment evaluating thecervical-cephalic passage morphology, which is often site of dis-plasic alteration and osteophytes (Figs. 58, 59).
Arthroscopic treatment varies in relation to the impingementtype to treat; in pincer impingement surgical times are performedin succession. They consist of central compartment debridement,acetabular labral lesion treatment, resection of cotyloid ostheo-phyte and any paracotyloid ossicles. Labral pathology treatmentmay vary in relation to the anatomo-pathological damage; in casea severe labral wearing occurs, a debridement with shaver and ra-diofrequency devices is performed; if instead, the labrum appearsstill intact it is detached and moved to a stable implant area andsuccessively, once bony protrusion has been treated, it is reinsert-ed by suture anchors (Fig. 60).
In cam impingement a first surgical time with debridement ofcartilage and labral lesions in central compartment is also per-formed; acetabular labrum is always preserved and stably reinsert-
101
Indications
Figure 56
Pincer type impingement
Figure 57
Cam type impingement
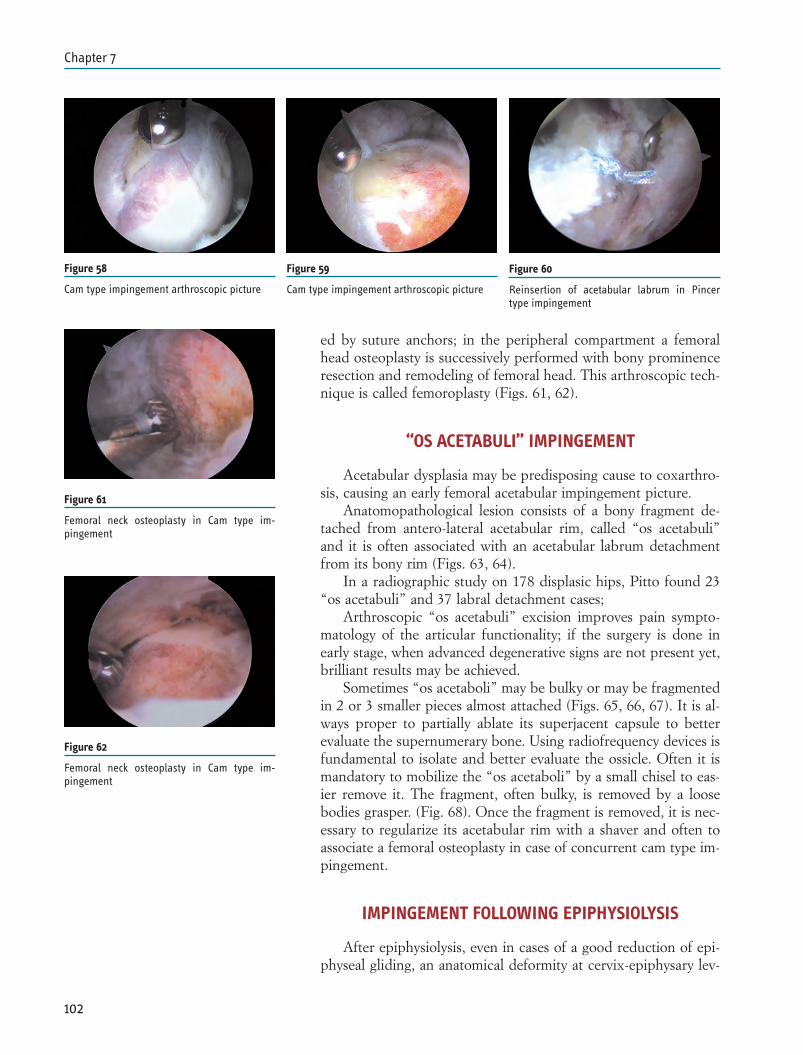
ed by suture anchors; in the peripheral compartment a femoralhead osteoplasty is successively performed with bony prominenceresection and remodeling of femoral head. This arthroscopic tech-nique is called femoroplasty (Figs. 61, 62).
“OS ACETABULI” IMPINGEMENT
Acetabular dysplasia may be predisposing cause to coxarthro-sis, causing an early femoral acetabular impingement picture.
Anatomopathological lesion consists of a bony fragment de-tached from antero-lateral acetabular rim, called “os acetabuli”and it is often associated with an acetabular labrum detachmentfrom its bony rim (Figs. 63, 64).
In a radiographic study on 178 displasic hips, Pitto found 23“os acetabuli” and 37 labral detachment cases;
Arthroscopic “os acetabuli” excision improves pain sympto-matology of the articular functionality; if the surgery is done inearly stage, when advanced degenerative signs are not present yet,brilliant results may be achieved.
Sometimes “os acetaboli” may be bulky or may be fragmentedin 2 or 3 smaller pieces almost attached (Figs. 65, 66, 67). It is al-ways proper to partially ablate its superjacent capsule to betterevaluate the supernumerary bone. Using radiofrequency devices isfundamental to isolate and better evaluate the ossicle. Often it ismandatory to mobilize the “os acetaboli” by a small chisel to eas-ier remove it. The fragment, often bulky, is removed by a loosebodies grasper. (Fig. 68). Once the fragment is removed, it is nec-essary to regularize its acetabular rim with a shaver and often toassociate a femoral osteoplasty in case of concurrent cam type im-pingement.
IMPINGEMENT FOLLOWING EPIPHYSIOLYSIS
After epiphysiolysis, even in cases of a good reduction of epi-physeal gliding, an anatomical deformity at cervix-epiphysary lev-
102
Chapter 7
Figure 60
Reinsertion of acetabular labrum in Pincertype impingement
Figure 61
Femoral neck osteoplasty in Cam type im-pingement
Figure 62
Femoral neck osteoplasty in Cam type im-pingement
Figure 59
Cam type impingement arthroscopic picture
Figure 58
Cam type impingement arthroscopic picture
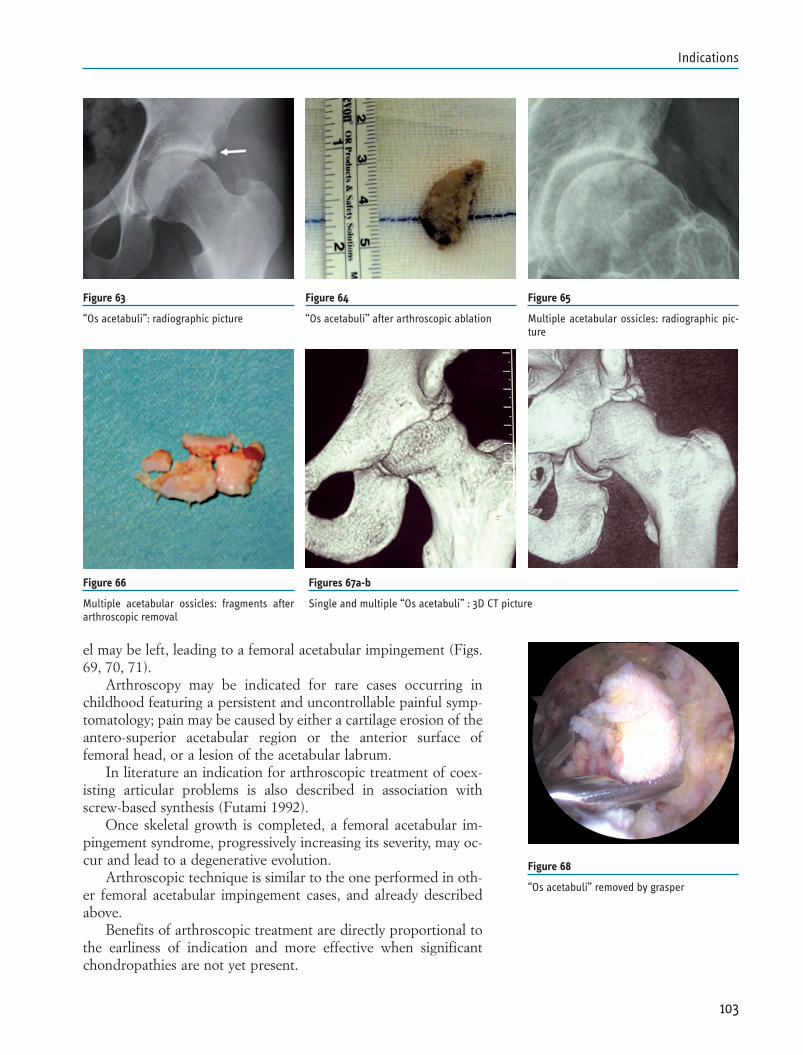
el may be left, leading to a femoral acetabular impingement (Figs.69, 70, 71).
Arthroscopy may be indicated for rare cases occurring inchildhood featuring a persistent and uncontrollable painful symp-tomatology; pain may be caused by either a cartilage erosion of theantero-superior acetabular region or the anterior surface offemoral head, or a lesion of the acetabular labrum.
In literature an indication for arthroscopic treatment of coex-isting articular problems is also described in association withscrew-based synthesis (Futami 1992).
Once skeletal growth is completed, a femoral acetabular im-pingement syndrome, progressively increasing its severity, may oc-cur and lead to a degenerative evolution.
Arthroscopic technique is similar to the one performed in oth-er femoral acetabular impingement cases, and already describedabove.
Benefits of arthroscopic treatment are directly proportional tothe earliness of indication and more effective when significantchondropathies are not yet present.
103
Indications
Figure 68
“Os acetabuli” removed by grasper
Figure 63
“Os acetabuli”: radiographic picture
Figure 65
Multiple acetabular ossicles: radiographic pic-ture
Figure 64
“Os acetabuli” after arthroscopic ablation
Figure 66
Multiple acetabular ossicles: fragments afterarthroscopic removal
Figures 67a-b
Single and multiple “Os acetabuli” : 3D CT picture
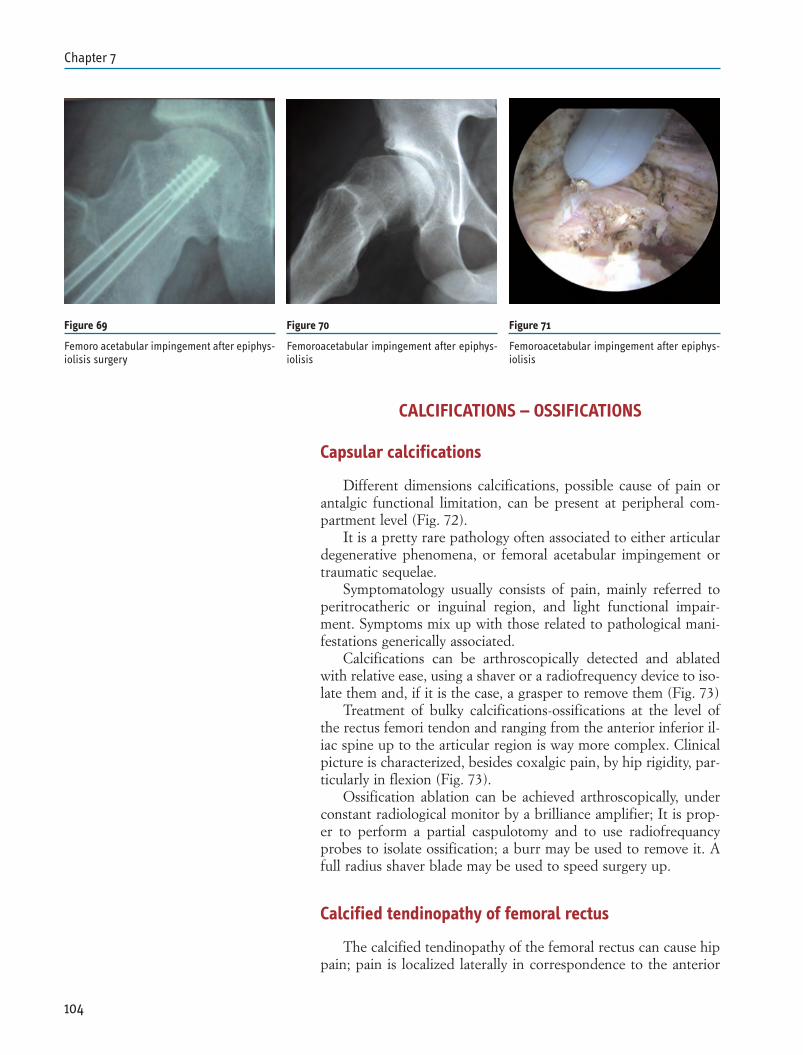
CALCIFICATIONS – OSSIFICATIONS
Capsular calcifications
Different dimensions calcifications, possible cause of pain orantalgic functional limitation, can be present at peripheral com-partment level (Fig. 72).
It is a pretty rare pathology often associated to either articulardegenerative phenomena, or femoral acetabular impingement ortraumatic sequelae.
Symptomatology usually consists of pain, mainly referred toperitrocatheric or inguinal region, and light functional impair-ment. Symptoms mix up with those related to pathological mani-festations generically associated.
Calcifications can be arthroscopically detected and ablatedwith relative ease, using a shaver or a radiofrequency device to iso-late them and, if it is the case, a grasper to remove them (Fig. 73)
Treatment of bulky calcifications-ossifications at the level ofthe rectus femori tendon and ranging from the anterior inferior il-iac spine up to the articular region is way more complex. Clinicalpicture is characterized, besides coxalgic pain, by hip rigidity, par-ticularly in flexion (Fig. 73).
Ossification ablation can be achieved arthroscopically, underconstant radiological monitor by a brilliance amplifier; It is prop-er to perform a partial caspulotomy and to use radiofrequancyprobes to isolate ossification; a burr may be used to remove it. Afull radius shaver blade may be used to speed surgery up.
Calcified tendinopathy of femoral rectus
The calcified tendinopathy of the femoral rectus can cause hippain; pain is localized laterally in correspondence to the anterior
104
Chapter 7
Figure 69
Femoro acetabular impingement after epiphys-iolisis surgery
Figure 70
Femoroacetabular impingement after epiphys-iolisis
Figure 71
Femoroacetabular impingement after epiphys-iolisis
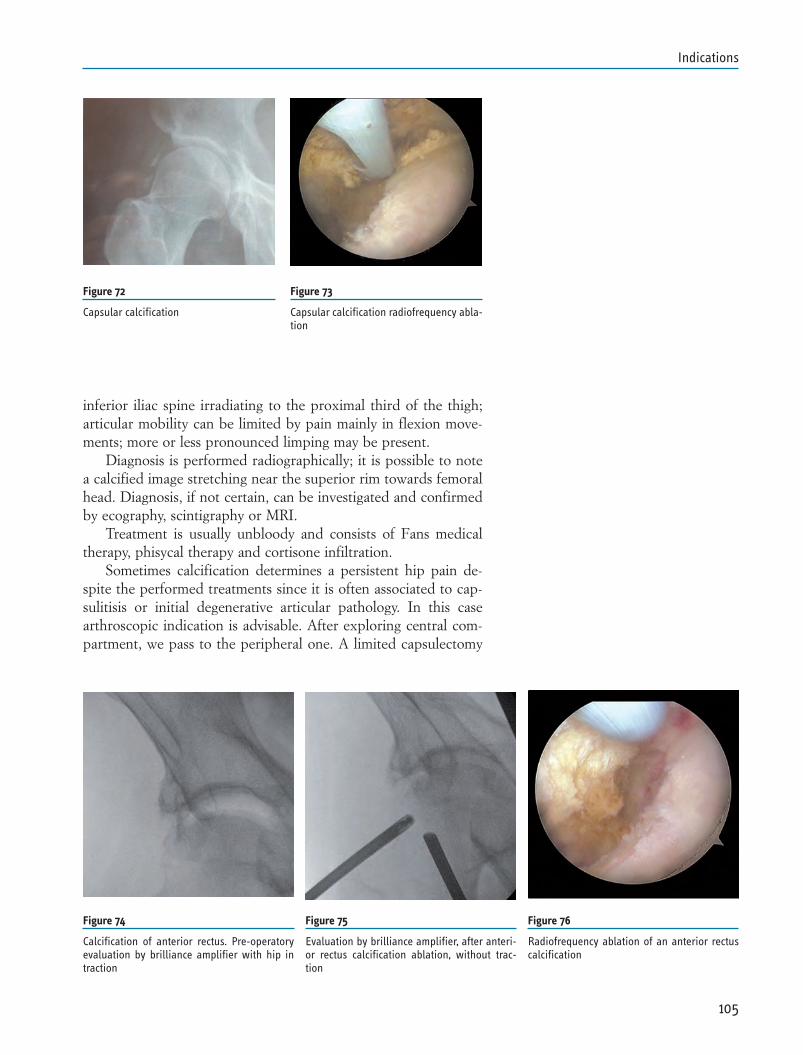
inferior iliac spine irradiating to the proximal third of the thigh;articular mobility can be limited by pain mainly in flexion move-ments; more or less pronounced limping may be present.
Diagnosis is performed radiographically; it is possible to notea calcified image stretching near the superior rim towards femoralhead. Diagnosis, if not certain, can be investigated and confirmedby ecography, scintigraphy or MRI.
Treatment is usually unbloody and consists of Fans medicaltherapy, phisycal therapy and cortisone infiltration.
Sometimes calcification determines a persistent hip pain de-spite the performed treatments since it is often associated to cap-sulitisis or initial degenerative articular pathology. In this casearthroscopic indication is advisable. After exploring central com-partment, we pass to the peripheral one. A limited capsulectomy
105
Indications
Figure 72
Capsular calcification
Figure 73
Capsular calcification radiofrequency abla-tion
Figure 74
Calcification of anterior rectus. Pre-operatoryevaluation by brilliance amplifier with hip intraction
Figure 75
Evaluation by brilliance amplifier, after anteri-or rectus calcification ablation, without trac-tion
Figure 76
Radiofrequency ablation of an anterior rectuscalcification
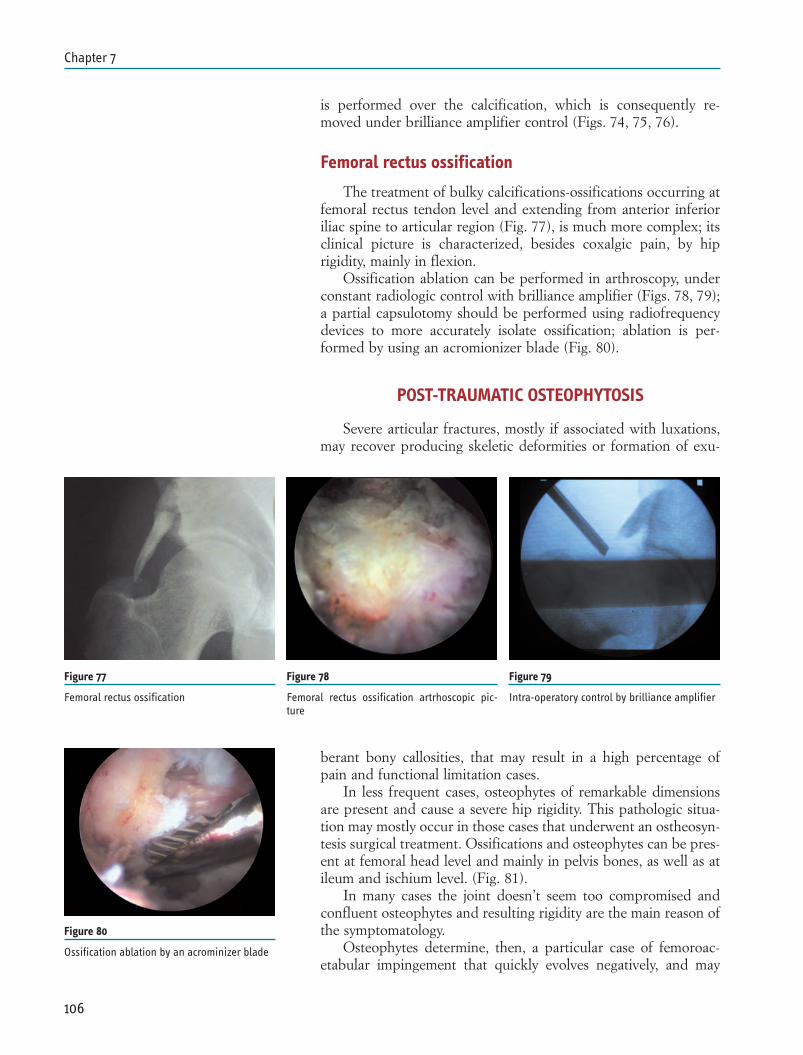
is performed over the calcification, which is consequently re-moved under brilliance amplifier control (Figs. 74, 75, 76).
Femoral rectus ossification
The treatment of bulky calcifications-ossifications occurring atfemoral rectus tendon level and extending from anterior inferioriliac spine to articular region (Fig. 77), is much more complex; itsclinical picture is characterized, besides coxalgic pain, by hiprigidity, mainly in flexion.
Ossification ablation can be performed in arthroscopy, underconstant radiologic control with brilliance amplifier (Figs. 78, 79);a partial capsulotomy should be performed using radiofrequencydevices to more accurately isolate ossification; ablation is per-formed by using an acromionizer blade (Fig. 80).
POST-TRAUMATIC OSTEOPHYTOSIS
Severe articular fractures, mostly if associated with luxations,may recover producing skeletic deformities or formation of exu-
berant bony callosities, that may result in a high percentage ofpain and functional limitation cases.
In less frequent cases, osteophytes of remarkable dimensionsare present and cause a severe hip rigidity. This pathologic situa-tion may mostly occur in those cases that underwent an ostheosyn-tesis surgical treatment. Ossifications and osteophytes can be pres-ent at femoral head level and mainly in pelvis bones, as well as atileum and ischium level. (Fig. 81).
In many cases the joint doesn’t seem too compromised andconfluent osteophytes and resulting rigidity are the main reason ofthe symptomatology.
Osteophytes determine, then, a particular case of femoroac-etabular impingement that quickly evolves negatively, and may
106
Chapter 7
Figure 77
Femoral rectus ossification
Figure 78
Femoral rectus ossification artrhoscopic pic-ture
Figure 79
Intra-operatory control by brilliance amplifier
Figure 80
Ossification ablation by an acrominizer blade
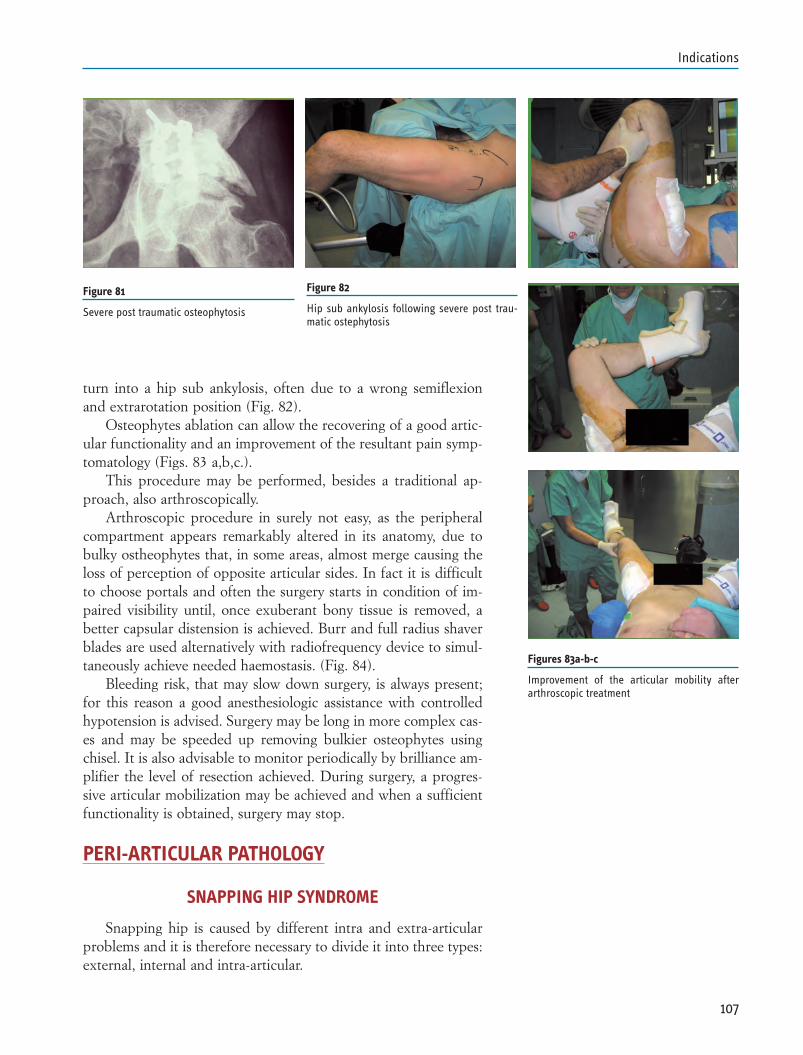
turn into a hip sub ankylosis, often due to a wrong semiflexionand extrarotation position (Fig. 82).
Osteophytes ablation can allow the recovering of a good artic-ular functionality and an improvement of the resultant pain symp-tomatology (Figs. 83 a,b,c.).
This procedure may be performed, besides a traditional ap-proach, also arthroscopically.
Arthroscopic procedure in surely not easy, as the peripheralcompartment appears remarkably altered in its anatomy, due tobulky ostheophytes that, in some areas, almost merge causing theloss of perception of opposite articular sides. In fact it is difficultto choose portals and often the surgery starts in condition of im-paired visibility until, once exuberant bony tissue is removed, abetter capsular distension is achieved. Burr and full radius shaverblades are used alternatively with radiofrequency device to simul-taneously achieve needed haemostasis. (Fig. 84).
Bleeding risk, that may slow down surgery, is always present;for this reason a good anesthesiologic assistance with controlledhypotension is advised. Surgery may be long in more complex cas-es and may be speeded up removing bulkier osteophytes usingchisel. It is also advisable to monitor periodically by brilliance am-plifier the level of resection achieved. During surgery, a progres-sive articular mobilization may be achieved and when a sufficientfunctionality is obtained, surgery may stop.
PERI-ARTICULAR PATHOLOGY
SNAPPING HIP SYNDROME
Snapping hip is caused by different intra and extra-articularproblems and it is therefore necessary to divide it into three types:external, internal and intra-articular.
107
Indications
Figure 82
Hip sub ankylosis following severe post trau-matic ostephytosis
Figures 83a-b-c
Improvement of the articular mobility afterarthroscopic treatment
Figure 81
Severe post traumatic osteophytosis
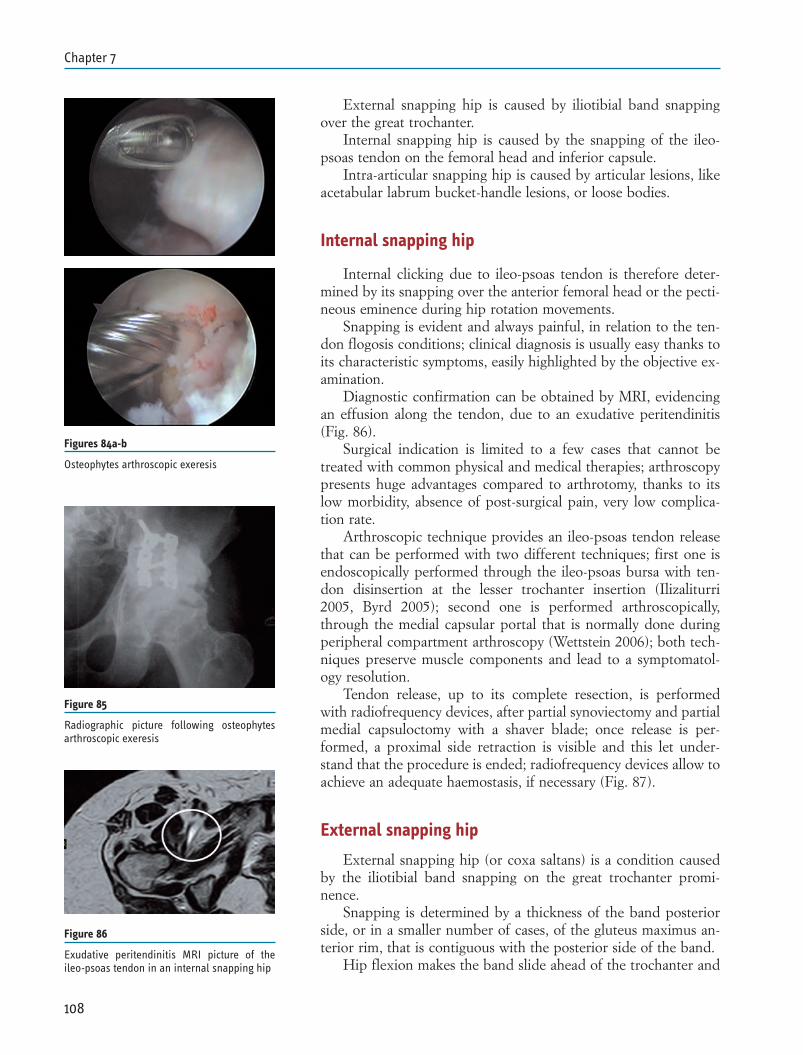
External snapping hip is caused by iliotibial band snappingover the great trochanter.
Internal snapping hip is caused by the snapping of the ileo-psoas tendon on the femoral head and inferior capsule.
Intra-articular snapping hip is caused by articular lesions, likeacetabular labrum bucket-handle lesions, or loose bodies.
Internal snapping hip
Internal clicking due to ileo-psoas tendon is therefore deter-mined by its snapping over the anterior femoral head or the pecti-neous eminence during hip rotation movements.
Snapping is evident and always painful, in relation to the ten-don flogosis conditions; clinical diagnosis is usually easy thanks toits characteristic symptoms, easily highlighted by the objective ex-amination.
Diagnostic confirmation can be obtained by MRI, evidencingan effusion along the tendon, due to an exudative peritendinitis(Fig. 86).
Surgical indication is limited to a few cases that cannot betreated with common physical and medical therapies; arthroscopypresents huge advantages compared to arthrotomy, thanks to itslow morbidity, absence of post-surgical pain, very low complica-tion rate.
Arthroscopic technique provides an ileo-psoas tendon releasethat can be performed with two different techniques; first one isendoscopically performed through the ileo-psoas bursa with ten-don disinsertion at the lesser trochanter insertion (Ilizaliturri2005, Byrd 2005); second one is performed arthroscopically,through the medial capsular portal that is normally done duringperipheral compartment arthroscopy (Wettstein 2006); both tech-niques preserve muscle components and lead to a symptomatol-ogy resolution.
Tendon release, up to its complete resection, is performedwith radiofrequency devices, after partial synoviectomy and partialmedial capsuloctomy with a shaver blade; once release is per-formed, a proximal side retraction is visible and this let under-stand that the procedure is ended; radiofrequency devices allow toachieve an adequate haemostasis, if necessary (Fig. 87).
External snapping hip
External snapping hip (or coxa saltans) is a condition causedby the iliotibial band snapping on the great trochanter promi-nence.
Snapping is determined by a thickness of the band posteriorside, or in a smaller number of cases, of the gluteus maximus an-terior rim, that is contiguous with the posterior side of the band.
Hip flexion makes the band slide ahead of the trochanter and
108
Chapter 7
Figure 86
Exudative peritendinitis MRI picture of theileo-psoas tendon in an internal snapping hip
Figures 84a-b
Osteophytes arthroscopic exeresis
Figure 85
Radiographic picture following osteophytesarthroscopic exeresis
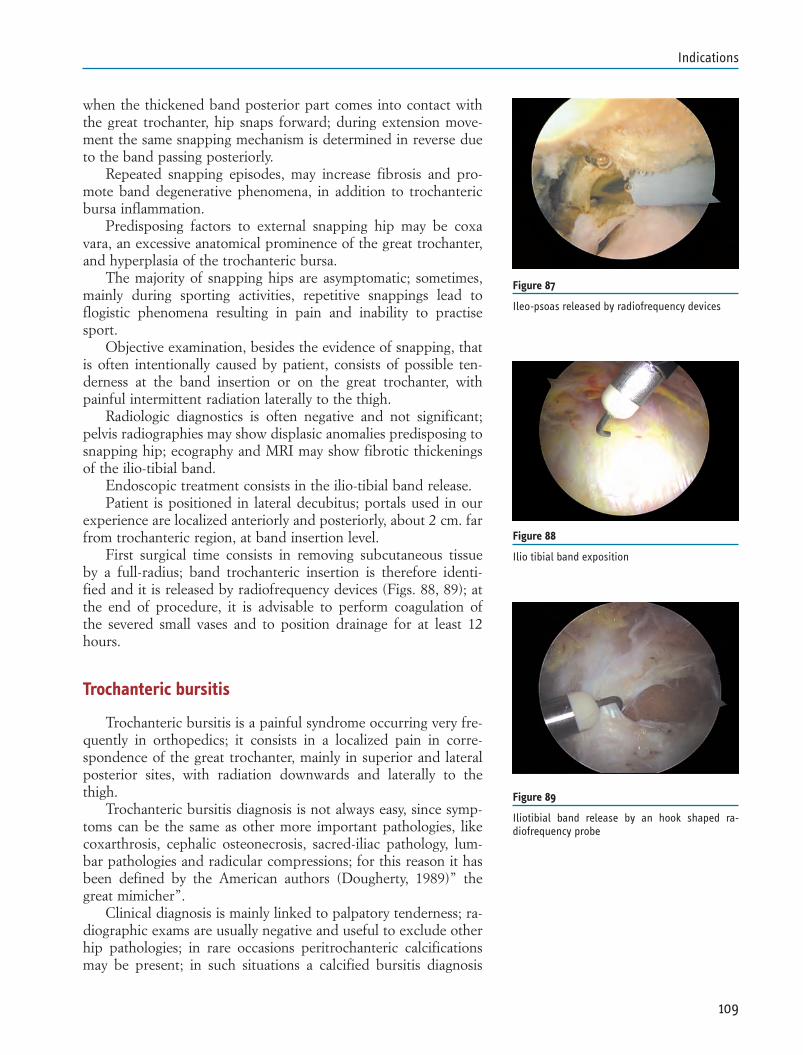
when the thickened band posterior part comes into contact withthe great trochanter, hip snaps forward; during extension move-ment the same snapping mechanism is determined in reverse dueto the band passing posteriorly.
Repeated snapping episodes, may increase fibrosis and pro-mote band degenerative phenomena, in addition to trochantericbursa inflammation.
Predisposing factors to external snapping hip may be coxavara, an excessive anatomical prominence of the great trochanter,and hyperplasia of the trochanteric bursa.
The majority of snapping hips are asymptomatic; sometimes,mainly during sporting activities, repetitive snappings lead toflogistic phenomena resulting in pain and inability to practisesport.
Objective examination, besides the evidence of snapping, thatis often intentionally caused by patient, consists of possible ten-derness at the band insertion or on the great trochanter, withpainful intermittent radiation laterally to the thigh.
Radiologic diagnostics is often negative and not significant;pelvis radiographies may show displasic anomalies predisposing tosnapping hip; ecography and MRI may show fibrotic thickeningsof the ilio-tibial band.
Endoscopic treatment consists in the ilio-tibial band release.Patient is positioned in lateral decubitus; portals used in our
experience are localized anteriorly and posteriorly, about 2 cm. farfrom trochanteric region, at band insertion level.
First surgical time consists in removing subcutaneous tissueby a full-radius; band trochanteric insertion is therefore identi-fied and it is released by radiofrequency devices (Figs. 88, 89); atthe end of procedure, it is advisable to perform coagulation ofthe severed small vases and to position drainage for at least 12hours.
Trochanteric bursitis
Trochanteric bursitis is a painful syndrome occurring very fre-quently in orthopedics; it consists in a localized pain in corre-spondence of the great trochanter, mainly in superior and lateralposterior sites, with radiation downwards and laterally to thethigh.
Trochanteric bursitis diagnosis is not always easy, since symp-toms can be the same as other more important pathologies, likecoxarthrosis, cephalic osteonecrosis, sacred-iliac pathology, lum-bar pathologies and radicular compressions; for this reason it hasbeen defined by the American authors (Dougherty, 1989)” thegreat mimicher”.
Clinical diagnosis is mainly linked to palpatory tenderness; ra-diographic exams are usually negative and useful to exclude otherhip pathologies; in rare occasions peritrochanteric calcificationsmay be present; in such situations a calcified bursitis diagnosis
109
Indications
Figure 87
Ileo-psoas released by radiofrequency devices
Figure 88
Ilio tibial band exposition
Figure 89
Iliotibial band release by an hook shaped ra-diofrequency probe
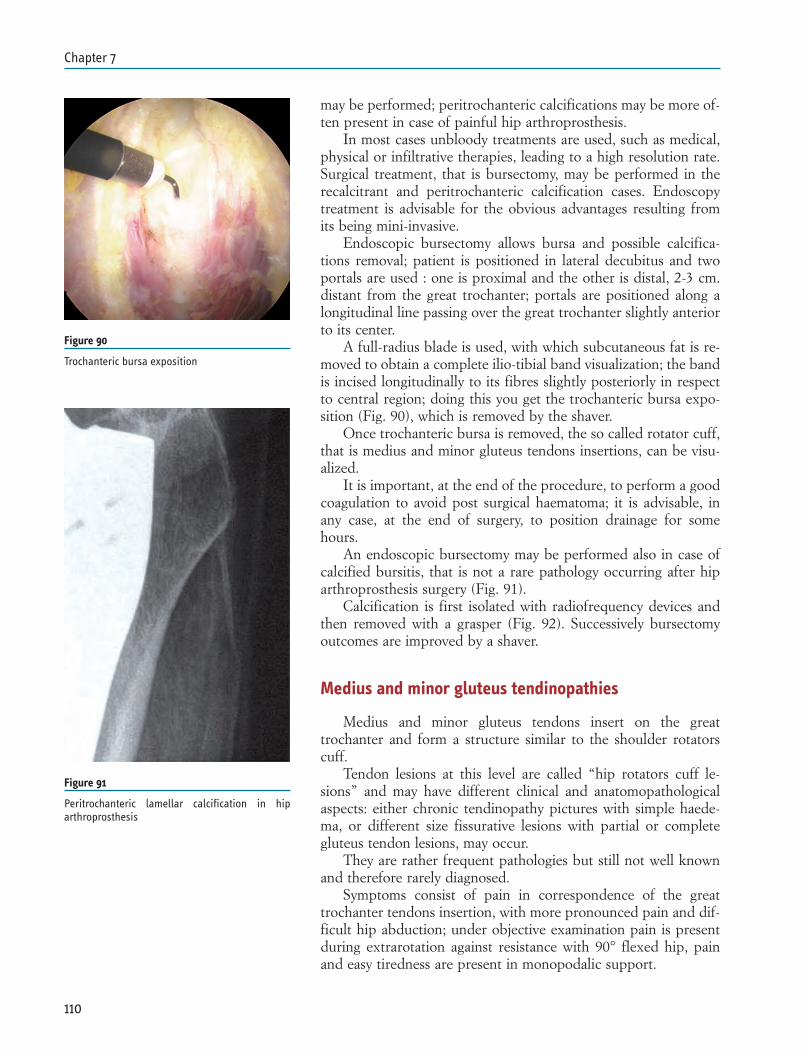
may be performed; peritrochanteric calcifications may be more of-ten present in case of painful hip arthroprosthesis.
In most cases unbloody treatments are used, such as medical,physical or infiltrative therapies, leading to a high resolution rate.Surgical treatment, that is bursectomy, may be performed in therecalcitrant and peritrochanteric calcification cases. Endoscopytreatment is advisable for the obvious advantages resulting fromits being mini-invasive.
Endoscopic bursectomy allows bursa and possible calcifica-tions removal; patient is positioned in lateral decubitus and twoportals are used : one is proximal and the other is distal, 2-3 cm.distant from the great trochanter; portals are positioned along alongitudinal line passing over the great trochanter slightly anteriorto its center.
A full-radius blade is used, with which subcutaneous fat is re-moved to obtain a complete ilio-tibial band visualization; the bandis incised longitudinally to its fibres slightly posteriorly in respectto central region; doing this you get the trochanteric bursa expo-sition (Fig. 90), which is removed by the shaver.
Once trochanteric bursa is removed, the so called rotator cuff,that is medius and minor gluteus tendons insertions, can be visu-alized.
It is important, at the end of the procedure, to perform a goodcoagulation to avoid post surgical haematoma; it is advisable, inany case, at the end of surgery, to position drainage for somehours.
An endoscopic bursectomy may be performed also in case ofcalcified bursitis, that is not a rare pathology occurring after hiparthroprosthesis surgery (Fig. 91).
Calcification is first isolated with radiofrequency devices andthen removed with a grasper (Fig. 92). Successively bursectomyoutcomes are improved by a shaver.
Medius and minor gluteus tendinopathies
Medius and minor gluteus tendons insert on the greattrochanter and form a structure similar to the shoulder rotatorscuff.
Tendon lesions at this level are called “hip rotators cuff le-sions” and may have different clinical and anatomopathologicalaspects: either chronic tendinopathy pictures with simple haede-ma, or different size fissurative lesions with partial or completegluteus tendon lesions, may occur.
They are rather frequent pathologies but still not well knownand therefore rarely diagnosed.
Symptoms consist of pain in correspondence of the greattrochanter tendons insertion, with more pronounced pain and dif-ficult hip abduction; under objective examination pain is presentduring extrarotation against resistance with 90° flexed hip, painand easy tiredness are present in monopodalic support.
110
Chapter 7
Figure 90
Trochanteric bursa exposition
Figure 91
Peritrochanteric lamellar calcification in hiparthroprosthesis
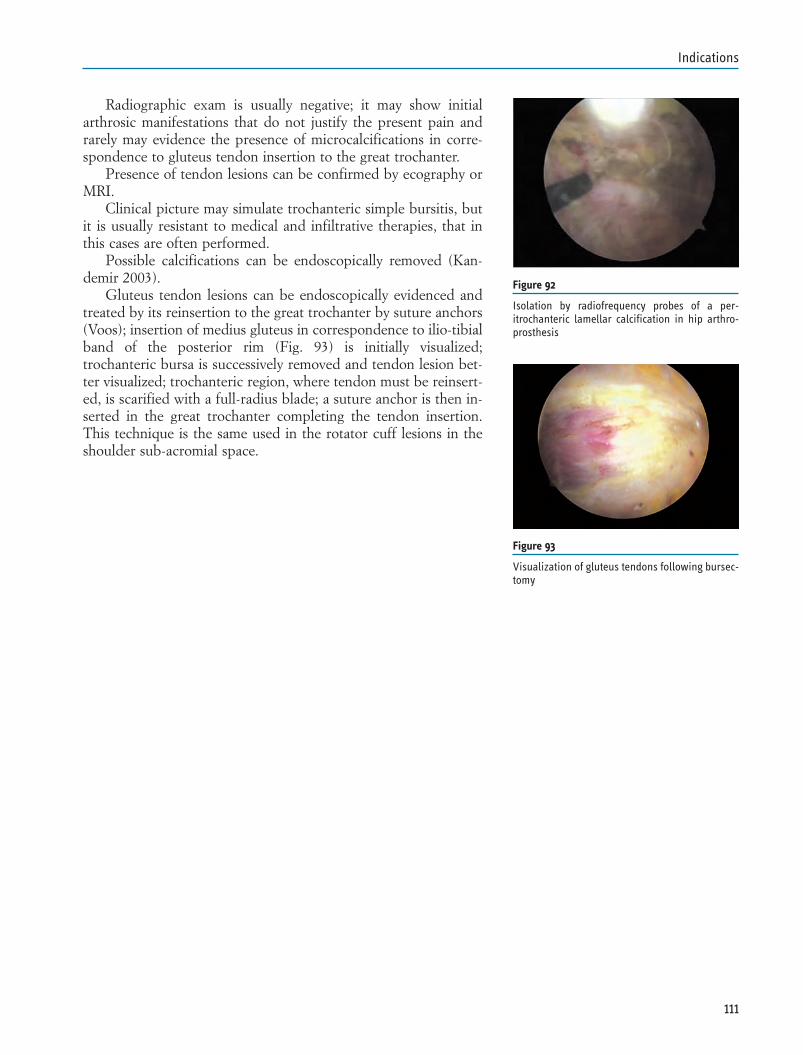
Radiographic exam is usually negative; it may show initialarthrosic manifestations that do not justify the present pain andrarely may evidence the presence of microcalcifications in corre-spondence to gluteus tendon insertion to the great trochanter.
Presence of tendon lesions can be confirmed by ecography orMRI.
Clinical picture may simulate trochanteric simple bursitis, butit is usually resistant to medical and infiltrative therapies, that inthis cases are often performed.
Possible calcifications can be endoscopically removed (Kan-demir 2003).
Gluteus tendon lesions can be endoscopically evidenced andtreated by its reinsertion to the great trochanter by suture anchors(Voos); insertion of medius gluteus in correspondence to ilio-tibialband of the posterior rim (Fig. 93) is initially visualized;trochanteric bursa is successively removed and tendon lesion bet-ter visualized; trochanteric region, where tendon must be reinsert-ed, is scarified with a full-radius blade; a suture anchor is then in-serted in the great trochanter completing the tendon insertion.This technique is the same used in the rotator cuff lesions in theshoulder sub-acromial space.
111
Indications
Figure 92
Isolation by radiofrequency probes of a per-itrochanteric lamellar calcification in hip arthro-prosthesis
Figure 93
Visualization of gluteus tendons following bursec-tomy
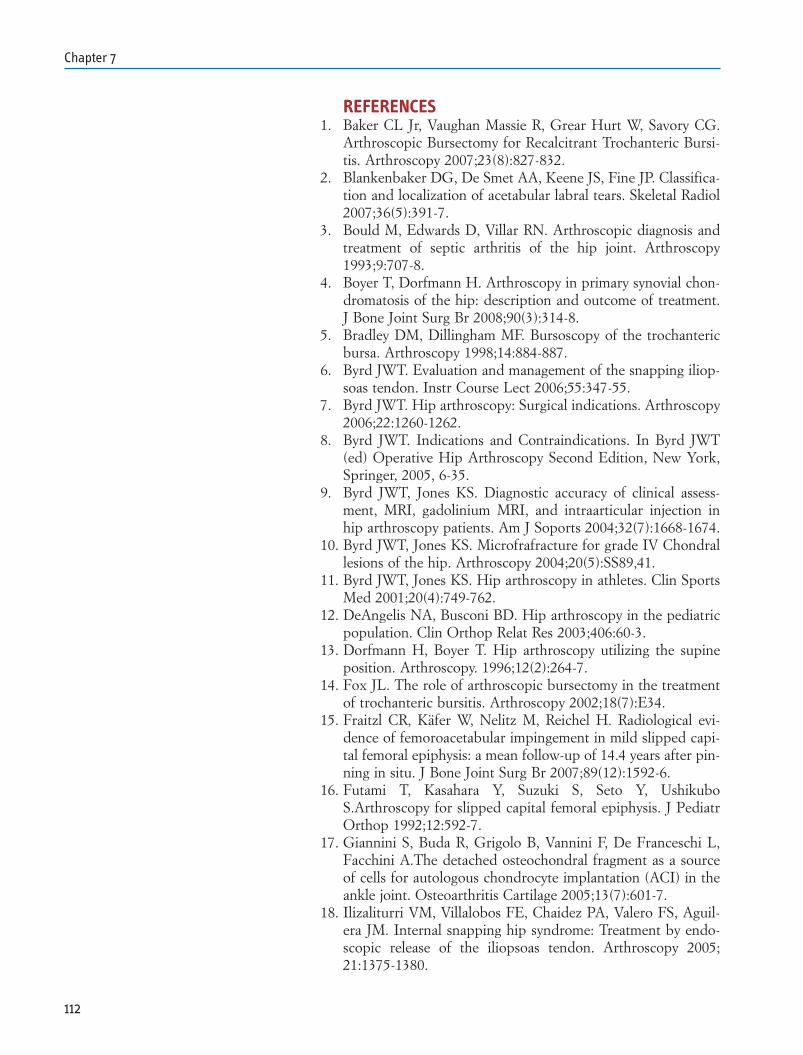
REFERENCES1. Baker CL Jr, Vaughan Massie R, Grear Hurt W, Savory CG.
Arthroscopic Bursectomy for Recalcitrant Trochanteric Bursi-tis. Arthroscopy 2007;23(8):827-832.
2. Blankenbaker DG, De Smet AA, Keene JS, Fine JP. Classifica-tion and localization of acetabular labral tears. Skeletal Radiol2007;36(5):391-7.
3. Bould M, Edwards D, Villar RN. Arthroscopic diagnosis andtreatment of septic arthritis of the hip joint. Arthroscopy1993;9:707-8.
4. Boyer T, Dorfmann H. Arthroscopy in primary synovial chon-dromatosis of the hip: description and outcome of treatment.J Bone Joint Surg Br 2008;90(3):314-8.
5. Bradley DM, Dillingham MF. Bursoscopy of the trochantericbursa. Arthroscopy 1998;14:884-887.
6. Byrd JWT. Evaluation and management of the snapping iliop-soas tendon. Instr Course Lect 2006;55:347-55.
7. Byrd JWT. Hip arthroscopy: Surgical indications. Arthroscopy2006;22:1260-1262.
8. Byrd JWT. Indications and Contraindications. In Byrd JWT(ed) Operative Hip Arthroscopy Second Edition, New York,Springer, 2005, 6-35.
9. Byrd JWT, Jones KS. Diagnostic accuracy of clinical assess-ment, MRI, gadolinium MRI, and intraarticular injection inhip arthroscopy patients. Am J Soports 2004;32(7):1668-1674.
10. Byrd JWT, Jones KS. Microfrafracture for grade IV Chondrallesions of the hip. Arthroscopy 2004;20(5):SS89,41.
11. Byrd JWT, Jones KS. Hip arthroscopy in athletes. Clin SportsMed 2001;20(4):749-762.
12. DeAngelis NA, Busconi BD. Hip arthroscopy in the pediatricpopulation. Clin Orthop Relat Res 2003;406:60-3.
13. Dorfmann H, Boyer T. Hip arthroscopy utilizing the supineposition. Arthroscopy. 1996;12(2):264-7.
14. Fox JL. The role of arthroscopic bursectomy in the treatmentof trochanteric bursitis. Arthroscopy 2002;18(7):E34.
15. Fraitzl CR, Käfer W, Nelitz M, Reichel H. Radiological evi-dence of femoroacetabular impingement in mild slipped capi-tal femoral epiphysis: a mean follow-up of 14.4 years after pin-ning in situ. J Bone Joint Surg Br 2007;89(12):1592-6.
16. Futami T, Kasahara Y, Suzuki S, Seto Y, UshikuboS.Arthroscopy for slipped capital femoral epiphysis. J PediatrOrthop 1992;12:592-7.
17. Giannini S, Buda R, Grigolo B, Vannini F, De Franceschi L,Facchini A.The detached osteochondral fragment as a sourceof cells for autologous chondrocyte implantation (ACI) in theankle joint. Osteoarthritis Cartilage 2005;13(7):601-7.
18. Ilizaliturri VM, Villalobos FE, Chaidez PA, Valero FS, Aguil-era JM. Internal snapping hip syndrome: Treatment by endo-scopic release of the iliopsoas tendon. Arthroscopy 2005;21:1375-1380.
112
Chapter 7
19. Ilizaliturri VM Jr, Martinez-Escalante FA, Chaidez PA, Cama-cho-Galindo J. Endoscopic iliotibial band release for externalsnapping hip syndrome. Arthroscopy 2006;22:505-10.
20. Kandemir U, Bharam S, Phillippon MJ, Fu FH. Endoscopictreatment of calcific tendinitis of gluteus medius and minimus.Arthroscopy 2003;19:E4.
21. Kelly BT, Buly RL. Hip Arthroscopy Update. HSSJ 2005;1:40-48.
22. Kelly BT, Weiland DE, Schenker ML, Philippon MJ. Arthro-scopic labral repair in the hip: surgical technique and reviewof the literature. Arthroscopy 2005;21:1496-504.
23. Khanduja V, Villar RN. Arthroscopic surgery of the hip. Cur-rent concepts and recent advances. J Bone Joint Surg Br2006;88:1557-66.
24. Klaue K, Durnin CW, Ganz R. The acetabular rim syndrome.A clinical presentation of dysplasia of the hip. J Bone JointSurg Br 1991;73(3):423-9.
25. Kocher MS, Kim YJ, Millis MB, Mandiga R, Siparsky P,Micheli LJ, Kasser JR. Hip arthroscopy in children and adoles-cents. J Pediatr Orthop 2005;25(5):680-6.
26. Krebs VE. The role of hip arthroscopy in the treatment of syn-ovial disorders and loose bodies. Clin Orthop Relat Res2003;406:48-59.
27. Kuklo TR, Mackenzie WG, Keeler KA. Hip arthroscopy inLegg-Calve-Perthes disease. Arthroscopy 1999;15(1):88-92.
28. Kusma M, Jung J, Dienst M, Goedde S, Kohn D, Seil R.Arthroscopic treatment of an avulsion fracture of the ligamen-tum teres of the hip in an 18-year-old horse rider. Arthroscopy2004;20 Suppl 2:64-6.
29. Lage LA, Patel JV, Villar RN.The acetabular labral tear: anarthroscopic classification. Arthroscopy 1996;12:269-72.
30. Lubowitz JH, Poehling GG. Hip arthroscopy: An emerginggold standard. Arthroscopy 2006;22:1257-1259.
31. Mah ET, Bradley CM. Aust N Z. Arthroscopic removal ofacrylic cement from unreduced hip prosthesis. J Surg1992;62:508-10.
32. Martin RL, Irrgang JJ, Sekiya JK. The diagnostic accuracy of aclinical examination in determining intra-articular hip pain forpotential hip arthroscopy candidates. Arthroscopy 2008[doi:10.1016/j.arthro.2008.04.75].
33. McCarthy JC, Jibodh SR, Lee JA. The role of arthroscopy inevaluation of painful hip arthroplasty. Clin Orthop Relat Res2009;467(1):174-80.
34. McCarthy JC. Hip arthroscopy: when it is and when it is notindicated. Instr Course Lect 2004;53:615-21.
35. McCarthy J, Lee J. Surgical indications, In McCarthy (Ed)Early Hip Disorders, Springer-Verlag, New York 2003,57-67.
36. Nusem I, Jabur MK, Playford EG. Arthroscopic treatment ofseptic arthritis of the hip. Arthroscopy 2006;22(8):902.e1-3.
37. O’Leary JA, Berend K, Vail TP. The relationship between di-
113
Indications
agnosis and outcome in arthroscopy of the hip. Arthroscopy2001;17:181-188.
38. Pitto RP, Klaue K, Ganz R, Ceppatelli S. Acetabular rimpathology secondary to congenital hip dysplasia in the adult. Aradiographic study. Chir Organi Mov 1995;80(4):361-8.
39. Rao J, Zhou YX, Villar RN. Injury to the ligamentum teres.Mechanism, findings, and results of treatment. Clin SportsMed 2001;20(4):791-9.
40. Ruch DS, Sekiya J, Dickson Schaefer W, Koman LA, Pope TL,Poehling GG. The role of hip arthroscopy in the evaluation ofavascular necrosis. Orthopedics 2001;24(4):339-43.
41. Sarkar JS, Haddad FS, Crean SV, Brooks P. Acute calcific ten-dinitis of the rectus femoris. J Bone Joint Surg Br1996;78(5):814-6.
42. Sekiya JK, Ruch DS, Hunter DM, Pope TL Jr, Koman LA,Poehling GG, Russell GB. Hip arthroscopy in staging avascu-lar necrosis of the femoral head. J South Orthop Assoc 2000Winter;9(4):254-61.
43. Shindle MK, Voos JE, Heyworth BE, Mintz DN, Moya LE,Buly RL, Kelly BT. Hip Arthroscopy in the Athletic Patient:Current Techniques and Spectrum of Disease. J Bone JointSurg Am 2007;89:29-43.
44. Sim FH. Synovial proliferative disorders: role of synoviectomy.Arthroscopy 1985;1(3):198-204.
45. Smart LR,Oetgen M, Noonan B, Medvecky M. Beginning HipArthroscopy: Indications, Positioning, Portals, Basic Tech-niques, and Complications. Arthroscopy 2007;23:1348-1353.
46. Suzuki S, Kasahara Y, Seto Y, Futami T, Furukawa K, NishinoY. Arthroscopy in 19 children with Perthes’ disease. Patholog-ic changes of the synovium and the joint surface. Acta OrthopScand 1994;65(6):581-4.
47. Tibor LM, Sekiya JK. Differential Diagnosis of Pain Aroundthe Hip Joint. Arthroscopy 2008;24(12):1407-1421.
48. Voos JE, Ranawat AS, Kelly BT. The peritrochanteric space ofthe hip. Instr Course Lect 2009;58:193-201.
49. Voos JE, Shindle MK, Pruett A, Asnis PD, Kelly BT. Endo-scopic repair of gluteus medius tendon tears of the hip. Am JSports Med 2009 ;37(4):743-7.
50. Voos JE, Rudzki JR, Shindle MK, Martin H, Kelly BT. Arthro-scopic anatomy and surgical techniques for peritrochantericspace disorders in the hip. Arthroscopy 2007;23:1246.e1-5.
51. Walton NP, Jahromi I, Lewis PL. Chondral degeneration andtherapeutic hip arthroscopy. Int Orthop 2004;28:354-356.
52. Wang ZG, Wang Y, Liu YJ, Li ZL, Cai X, Wei M. Clinicalevaluation of small diameter decompression and arthroscopyin the treatment of early avascular necrosis of femoral head.Zhonghua Yi Xue Za Zhi. 2007 Aug ;87(29):2041-4. Chinese.
53. Wettstein M, Jung J, Dienst M. Arthroscopic psoas tenotomy.Arthroscopy 2006;22(8):907.e1-4.
54. Yamamoto Y, Usui I. Arthroscopic surgery for degenerative
114
Chapter 7

rupture of the ligamentum teres femoris. Arthroscopy2006;22:689.e1-3.
55. Yamamoto Y, Hamada Y, Ide T, Usui I. Arthroscopic surgeryto treat intra-articular type snapping hip. Arthroscopy2005;21(9):1120-5.
115
Indications

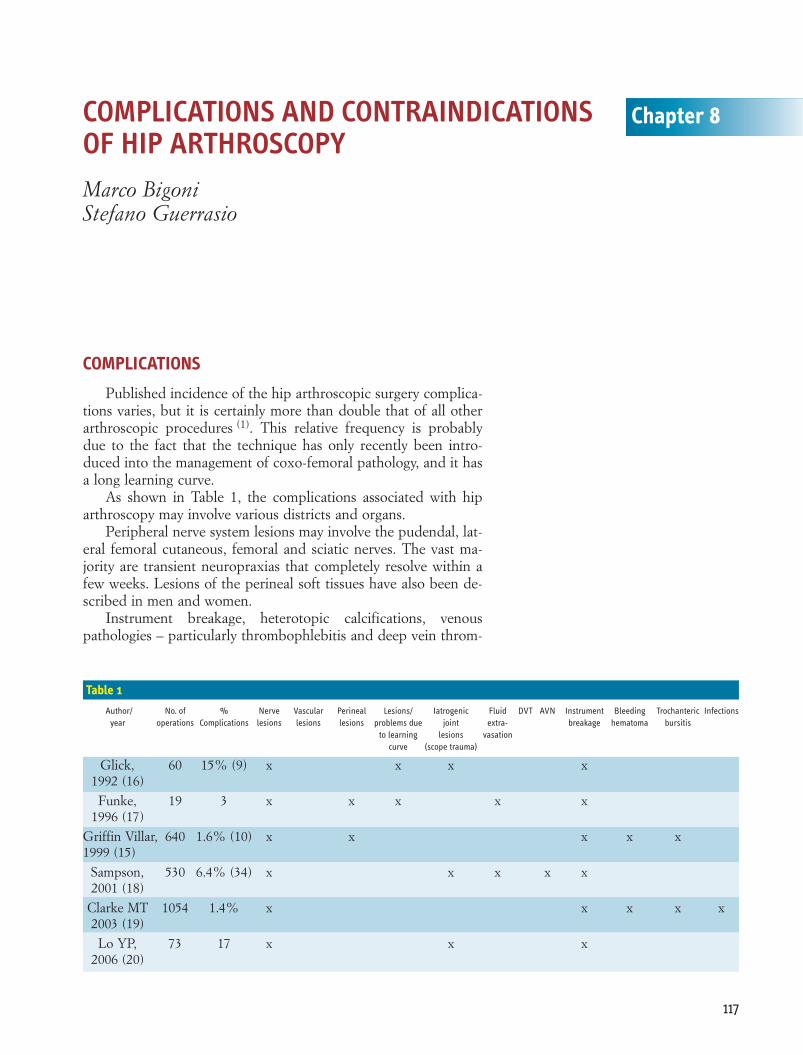
COMPLICATIONS
Published incidence of the hip arthroscopic surgery complica-tions varies, but it is certainly more than double that of all otherarthroscopic procedures (1). This relative frequency is probablydue to the fact that the technique has only recently been intro-duced into the management of coxo-femoral pathology, and it hasa long learning curve.
As shown in Table 1, the complications associated with hiparthroscopy may involve various districts and organs.
Peripheral nerve system lesions may involve the pudendal, lat-eral femoral cutaneous, femoral and sciatic nerves. The vast ma-jority are transient neuropraxias that completely resolve within afew weeks. Lesions of the perineal soft tissues have also been de-scribed in men and women.
Instrument breakage, heterotopic calcifications, venouspathologies – particularly thrombophlebitis and deep vein throm-
117
Chapter 8COMPLICATIONS AND CONTRAINDICATIONS OF HIP ARTHROSCOPYMarco BigoniStefano Guerrasio
Table 1
Author/ No. of % Nerve Vascular Perineal Lesions/ Iatrogenic Fluid DVT AVN Instrument Bleeding Trochanteric Infectionsyear operations Complications lesions lesions lesions problems due joint extra- breakage hematoma bursitis
to learning lesions vasationcurve (scope trauma)
Glick, 60 15% (9) x x x x1992 (16)
Funke, 19 3 x x x x x1996 (17)
Griffin Villar, 640 1.6% (10) x x x x x1999 (15)
Sampson, 530 6.4% (34) x x x x x2001 (18)
Clarke MT 1054 1.4% x x x x x2003 (19)
Lo YP, 73 17 x x x2006 (20)
bosis (DVT), problems due to the extravasation of abdominal flu-ids, and soft tissue infections are further complications that maybe encountered in this type of surgery (2-7).
Many authors attribute most of their own errors to the learn-ing phase, especially the inadequacy of traction systems. Accord-ing to Griffin and Villar, there is no correlation between complica-tions and the level of experience of senior surgeons (2).
Complications may occur during the course of surgery, in theimmediate postoperative period, or in the medium/long term, de-pending on the structures involved and the type of lesion. Howev-er, the same complication may have different characteristics of on-set depending on the entity of the lesion itself. For purposes ofsimplicity, we will divide the complications into preoperative, in-tra- and perioperative, and postoperative complications.
PREOPERATIVE COMPLICATIONSAnesthesiological complications
Appropriate patient selection and a correct evaluation of co-morbidities make the risk of complications due to local and gener-al anesthesia similar to that associated with other forms of hip sur-gery.
Complications in patient positioning and traction
The choice of supine or lateral decubitus is surgeon-depend-ent. Various authors (but it is sufficient to perform only one hiparthroscopy with inadequate traction systems to understand thedifficulties and insidiousness of this type of surgery) have empha-sised the need for adequate traction systems in order to be able toensure appropriate but not aggressive joint diastasis, thus allowinggood articular access without causing traumas due to the distrac-tion of the vascular nerve fasciae (3, 4, 8). There have been descrip-tions of transient neuropraxias involving the peroneal and saphe-nous nerves, and transient foot and ankle pain (5).
INTRA- AND PERIOPERATIVE COMPLICATIONSNeurovascular lesions due to direct trauma: the creation of portals
These lesions are directly due to the creation of the arthro-scopic portals, the importance of which has prompted us to dedi-cate an entire section to the subject (see below).
The lateral femoral cutaneous nerve is the most at risk, andcan be easily lesioned when creating the anterior portal (9). Avoid-ing cutting the skin too deeply at the time of incision can reducethe risk of direct nerve damage (10). However, lesions of smallnerve branches can occur even in the case of an appropriate surgi-cal technique.
118
Chapter 8
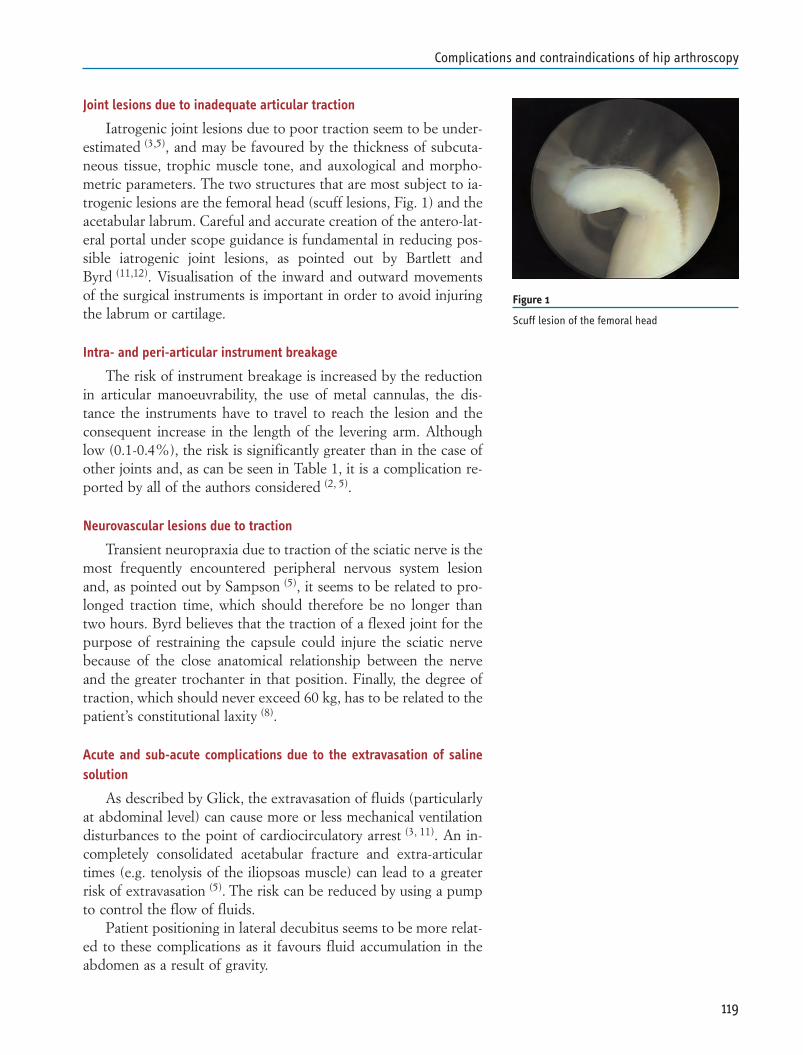
Joint lesions due to inadequate articular traction
Iatrogenic joint lesions due to poor traction seem to be under-estimated (3,5), and may be favoured by the thickness of subcuta-neous tissue, trophic muscle tone, and auxological and morpho-metric parameters. The two structures that are most subject to ia-trogenic lesions are the femoral head (scuff lesions, Fig. 1) and theacetabular labrum. Careful and accurate creation of the antero-lat-eral portal under scope guidance is fundamental in reducing pos-sible iatrogenic joint lesions, as pointed out by Bartlett andByrd (11,12). Visualisation of the inward and outward movementsof the surgical instruments is important in order to avoid injuringthe labrum or cartilage.
Intra- and peri-articular instrument breakage
The risk of instrument breakage is increased by the reductionin articular manoeuvrability, the use of metal cannulas, the dis-tance the instruments have to travel to reach the lesion and theconsequent increase in the length of the levering arm. Althoughlow (0.1-0.4%), the risk is significantly greater than in the case ofother joints and, as can be seen in Table 1, it is a complication re-ported by all of the authors considered (2, 5).
Neurovascular lesions due to traction
Transient neuropraxia due to traction of the sciatic nerve is themost frequently encountered peripheral nervous system lesionand, as pointed out by Sampson (5), it seems to be related to pro-longed traction time, which should therefore be no longer thantwo hours. Byrd believes that the traction of a flexed joint for thepurpose of restraining the capsule could injure the sciatic nervebecause of the close anatomical relationship between the nerveand the greater trochanter in that position. Finally, the degree oftraction, which should never exceed 60 kg, has to be related to thepatient’s constitutional laxity (8).
Acute and sub-acute complications due to the extravasation of salinesolution
As described by Glick, the extravasation of fluids (particularlyat abdominal level) can cause more or less mechanical ventilationdisturbances to the point of cardiocirculatory arrest (3, 11). An in-completely consolidated acetabular fracture and extra-articulartimes (e.g. tenolysis of the iliopsoas muscle) can lead to a greaterrisk of extravasation (5). The risk can be reduced by using a pumpto control the flow of fluids.
Patient positioning in lateral decubitus seems to be more relat-ed to these complications as it favours fluid accumulation in theabdomen as a result of gravity.
119
Complications and contraindications of hip arthroscopy
Figure 1
Scuff lesion of the femoral head
Need for arthrotomy
Inadequate selection of the patient and pathology to be treat-ed may make it impossible to complete the surgical procedure andthus prevent the resolution of the symptoms. Rare but always pos-sible intraoperative adverse events may make it necessary to per-form an arthrotomy or synthesis. Arthroscopists need to have theinstruments and materials for synthesis available in case of intra-operative fractures and must be capable of performing an arthro-tomic phase.
POSTOPERATIVE COMPLICATIONSLesions due to perineal compression (inappropriate lower limb traction)
The positioning of a post at perineal on a Maquet operatingtable in order to counterbalance traction exposes the perineal re-gion to high levels of compression and the related risks, includingpudendal and obturator neuropraxias, and cutaneous lesions ofthe region and perineal organs (2-4, 10, Tab 1). These complicationscan be avoided by using special traction systems or well-paddedposts, although it is worth pointing out that the neuropraxias tendto disappear completely within a few weeks.
Finally, in order to avoid excessive perineal compression, it isadvisable to use the minimum traction force necessary to ensuresufficient joint diastasis to perform the articular (central) phasewhich, as mentioned above, should not last longer than two hours.
Deep vein thrombosis (DVT)
No certain cases of post-arthroscopic DVT have been de-scribed in the literature.
Failure to resolve symptoms
The persistence of symptoms after surgery may depend onmany factors, including some that are potentially avoidable: • an incorrect surgical indication• a failure to recognise the pathology intraoperatively• inadequate instruments• incorrect/incomplete surgical manoeuvres/procedures
Avascular necrosis of the femoral head: AVN (see Neurovascular compli-cations below)
Villar and Byrd have described a post-arthroscopic progres-sion of femoral head AVN of uncertain significance (13), andSampson has described AVN after arthroscopy performed to treata lesion of the labrum (5).
Medico-legal implications: incomplete informed consent
We believe that an appropriate and dedicated informed con-sent document should be prepared that takes into account the
120
Chapter 8
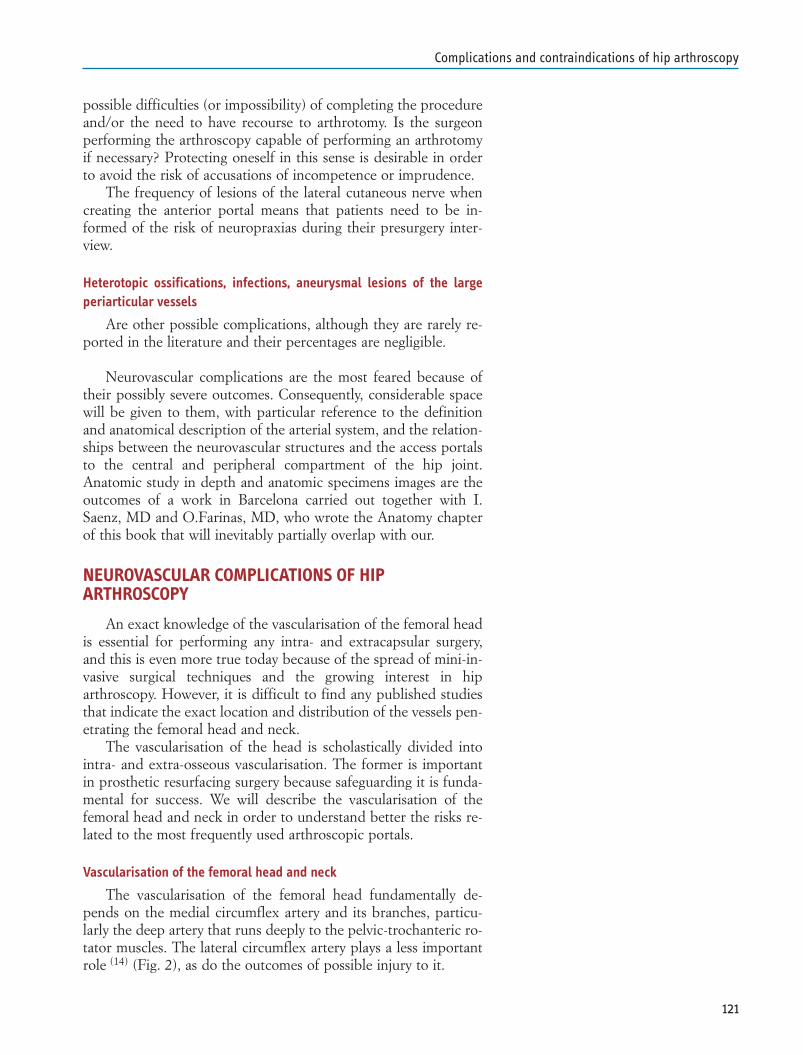
possible difficulties (or impossibility) of completing the procedureand/or the need to have recourse to arthrotomy. Is the surgeonperforming the arthroscopy capable of performing an arthrotomyif necessary? Protecting oneself in this sense is desirable in orderto avoid the risk of accusations of incompetence or imprudence.
The frequency of lesions of the lateral cutaneous nerve whencreating the anterior portal means that patients need to be in-formed of the risk of neuropraxias during their presurgery inter-view.
Heterotopic ossifications, infections, aneurysmal lesions of the largeperiarticular vessels
Are other possible complications, although they are rarely re-ported in the literature and their percentages are negligible.
Neurovascular complications are the most feared because oftheir possibly severe outcomes. Consequently, considerable spacewill be given to them, with particular reference to the definitionand anatomical description of the arterial system, and the relation-ships between the neurovascular structures and the access portalsto the central and peripheral compartment of the hip joint.Anatomic study in depth and anatomic specimens images are theoutcomes of a work in Barcelona carried out together with I.Saenz, MD and O.Farinas, MD, who wrote the Anatomy chapterof this book that will inevitably partially overlap with our.
NEUROVASCULAR COMPLICATIONS OF HIPARTHROSCOPY
An exact knowledge of the vascularisation of the femoral headis essential for performing any intra- and extracapsular surgery,and this is even more true today because of the spread of mini-in-vasive surgical techniques and the growing interest in hiparthroscopy. However, it is difficult to find any published studiesthat indicate the exact location and distribution of the vessels pen-etrating the femoral head and neck.
The vascularisation of the head is scholastically divided intointra- and extra-osseous vascularisation. The former is importantin prosthetic resurfacing surgery because safeguarding it is funda-mental for success. We will describe the vascularisation of thefemoral head and neck in order to understand better the risks re-lated to the most frequently used arthroscopic portals.
Vascularisation of the femoral head and neck
The vascularisation of the femoral head fundamentally de-pends on the medial circumflex artery and its branches, particu-larly the deep artery that runs deeply to the pelvic-trochanteric ro-tator muscles. The lateral circumflex artery plays a less importantrole (14) (Fig. 2), as do the outcomes of possible injury to it.
121
Complications and contraindications of hip arthroscopy
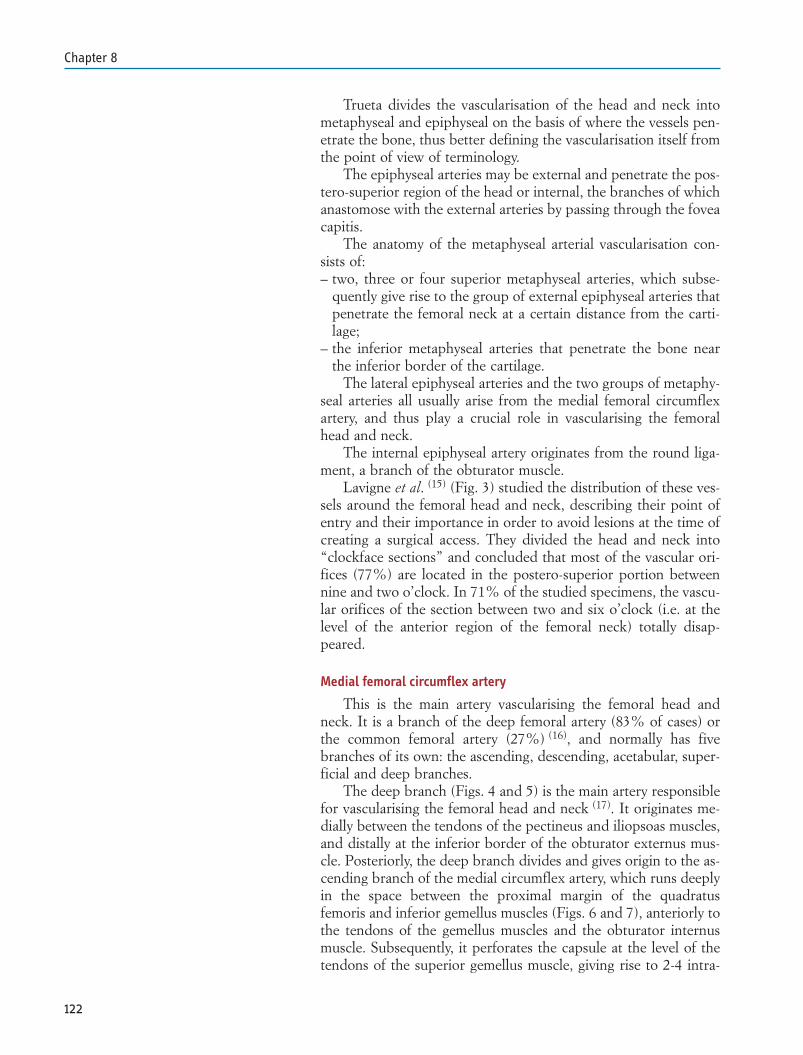
Trueta divides the vascularisation of the head and neck intometaphyseal and epiphyseal on the basis of where the vessels pen-etrate the bone, thus better defining the vascularisation itself fromthe point of view of terminology.
The epiphyseal arteries may be external and penetrate the pos-tero-superior region of the head or internal, the branches of whichanastomose with the external arteries by passing through the foveacapitis.
The anatomy of the metaphyseal arterial vascularisation con-sists of: – two, three or four superior metaphyseal arteries, which subse-
quently give rise to the group of external epiphyseal arteries thatpenetrate the femoral neck at a certain distance from the carti-lage;
– the inferior metaphyseal arteries that penetrate the bone nearthe inferior border of the cartilage.
The lateral epiphyseal arteries and the two groups of metaphy-seal arteries all usually arise from the medial femoral circumflexartery, and thus play a crucial role in vascularising the femoralhead and neck.
The internal epiphyseal artery originates from the round liga-ment, a branch of the obturator muscle.
Lavigne et al. (15) (Fig. 3) studied the distribution of these ves-sels around the femoral head and neck, describing their point ofentry and their importance in order to avoid lesions at the time ofcreating a surgical access. They divided the head and neck into“clockface sections” and concluded that most of the vascular ori-fices (77%) are located in the postero-superior portion betweennine and two o’clock. In 71% of the studied specimens, the vascu-lar orifices of the section between two and six o’clock (i.e. at thelevel of the anterior region of the femoral neck) totally disap-peared.
Medial femoral circumflex artery
This is the main artery vascularising the femoral head andneck. It is a branch of the deep femoral artery (83% of cases) orthe common femoral artery (27%) (16), and normally has fivebranches of its own: the ascending, descending, acetabular, super-ficial and deep branches.
The deep branch (Figs. 4 and 5) is the main artery responsiblefor vascularising the femoral head and neck (17). It originates me-dially between the tendons of the pectineus and iliopsoas muscles,and distally at the inferior border of the obturator externus mus-cle. Posteriorly, the deep branch divides and gives origin to the as-cending branch of the medial circumflex artery, which runs deeplyin the space between the proximal margin of the quadratusfemoris and inferior gemellus muscles (Figs. 6 and 7), anteriorly tothe tendons of the gemellus muscles and the obturator internusmuscle. Subsequently, it perforates the capsule at the level of thetendons of the superior gemellus muscle, giving rise to 2-4 intra-
122
Chapter 8

capsular retinacular branches (17) (Fig. 8). In 20% of the speci-mens, we found two branches in the inferior portion of thefemoral neck, known as the inferior retinacular vessels: as de-scribed by Carlioz (18) and Gautier (17), these vessels come fromthe deep branch of the medial circumflex artery, and are thereforepotentially at risk of injury when creating the posterior portals orgaining posterior access to the hip joint.
Lateral femoral circumflex artery
The lateral femoral circumflex artery plays a much less impor-tant role in vascularising the femoral head and neck (19). In mostcases, it arises from the deep femoral artery (Fig. 8), and then runslaterally and deeply beneath the anterior rectus muscle (Figs. 10and 11) before giving rise to branches for the rectus muscle itself,the anterior capsule of the coxo-femoral joint (9), and the vastuslateralis muscle, which it surrounds, and then anastomoses itselfwith the deep branch of the medial circumflex artery at the levelof the superior part of the femoral neck.
POTENTIAL RISKS WHEN CREATING ARTHROSCOPICPORTALS
The type and entity of the risk of neurovascular lesions associ-ated with hip arthroscopy are related to the creation of the arthro-scopic portals. As described in the literature, the choice (andtherefore the creation) of the portals is strictly related to theanatomical region of interest, which may be located in the centralor peripheral compartment (20, 21). Three portals are usually usedwhen working on the central compartment (the anterior, antero-lateral and postero-lateral portals), whereas those used to gain ac-cess to the peripheral compartment are the anterior, proximal an-tero-lateral and distal antero-lateral portals (22) (Fig. 2).
Anterior portal
The anatomical structures at risk when creating the anteriorportal are: 1. the lateral femoral cutaneous nerve2. the ascending branch of the lateral femoral artery (9, 23).
The anterior portal is located an average of 3.7 cm (range 1-6cm) from the ascending branch of the lateral circumflex artery(Fig. 3), but this distance is considerably less if calculated in rela-tion to the terminal branch of the artery, which is located at an av-erage distance of 0.3 cm (range 02-0.4 cm).
The risk of lesioning the lateral femoral cutaneous nerve isgreater because it is located an average of 0.3 cm from the portal(range 0.2-1 cm): it is therefore recommended to make a subcuta-neous dissection until reaching the fascia lata in order to be able
123
Complications and contraindications of hip arthroscopy
Figure 2
Relationship between portals and pelvi-trochanteric structures1. Gluteus minor muscle; 2. Piriformis muscle; 3. Pelvi-trochanteric muscles; 4. Sciatic nerve; 5. Greater trochanter; 6. Gluteus medius tendon; 7.Ischial tuberosity
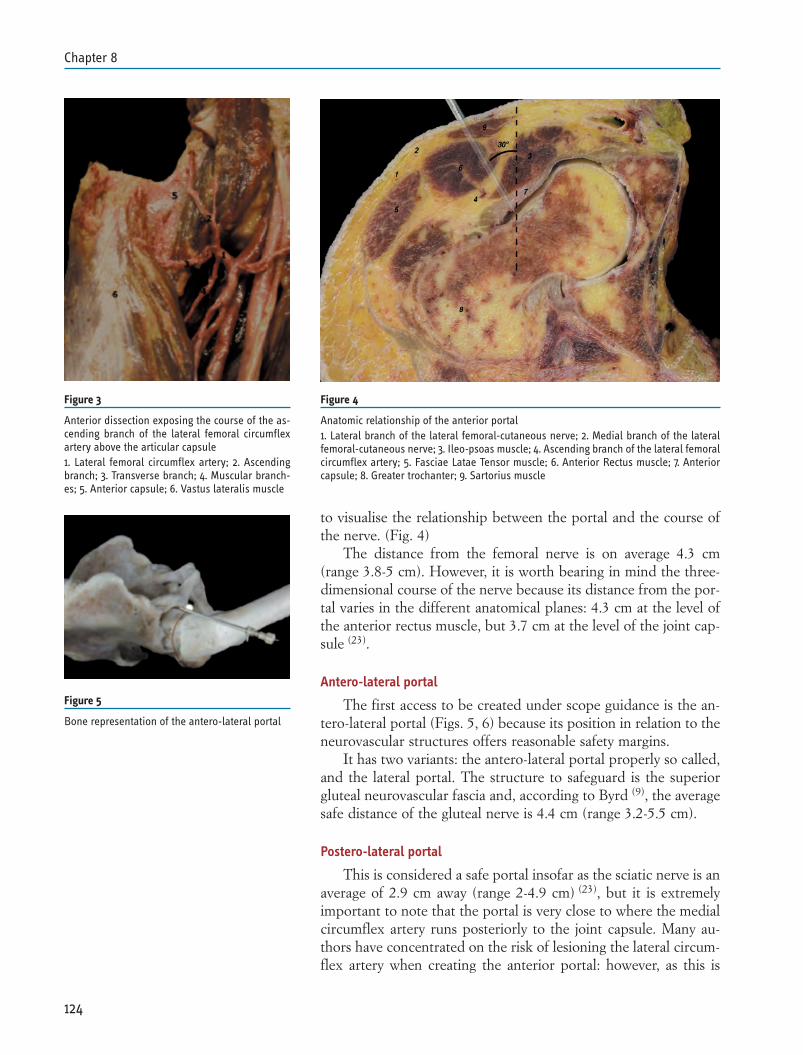
to visualise the relationship between the portal and the course ofthe nerve. (Fig. 4)
The distance from the femoral nerve is on average 4.3 cm(range 3.8-5 cm). However, it is worth bearing in mind the three-dimensional course of the nerve because its distance from the por-tal varies in the different anatomical planes: 4.3 cm at the level ofthe anterior rectus muscle, but 3.7 cm at the level of the joint cap-sule (23).
Antero-lateral portal
The first access to be created under scope guidance is the an-tero-lateral portal (Figs. 5, 6) because its position in relation to theneurovascular structures offers reasonable safety margins.
It has two variants: the antero-lateral portal properly so called,and the lateral portal. The structure to safeguard is the superiorgluteal neurovascular fascia and, according to Byrd (9), the averagesafe distance of the gluteal nerve is 4.4 cm (range 3.2-5.5 cm).
Postero-lateral portal
This is considered a safe portal insofar as the sciatic nerve is anaverage of 2.9 cm away (range 2-4.9 cm) (23), but it is extremelyimportant to note that the portal is very close to where the medialcircumflex artery runs posteriorly to the joint capsule. Many au-thors have concentrated on the risk of lesioning the lateral circum-flex artery when creating the anterior portal: however, as this is
124
Chapter 8
Figure 3
Anterior dissection exposing the course of the as-cending branch of the lateral femoral circumflexartery above the articular capsule1. Lateral femoral circumflex artery; 2. Ascendingbranch; 3. Transverse branch; 4. Muscular branch-es; 5. Anterior capsule; 6. Vastus lateralis muscle
Figure 4
Anatomic relationship of the anterior portal1. Lateral branch of the lateral femoral-cutaneous nerve; 2. Medial branch of the lateralfemoral-cutaneous nerve; 3. Ileo-psoas muscle; 4. Ascending branch of the lateral femoralcircumflex artery; 5. Fasciae Latae Tensor muscle; 6. Anterior Rectus muscle; 7. Anteriorcapsule; 8. Greater trochanter; 9. Sartorius muscle
Figure 5
Bone representation of the antero-lateral portal
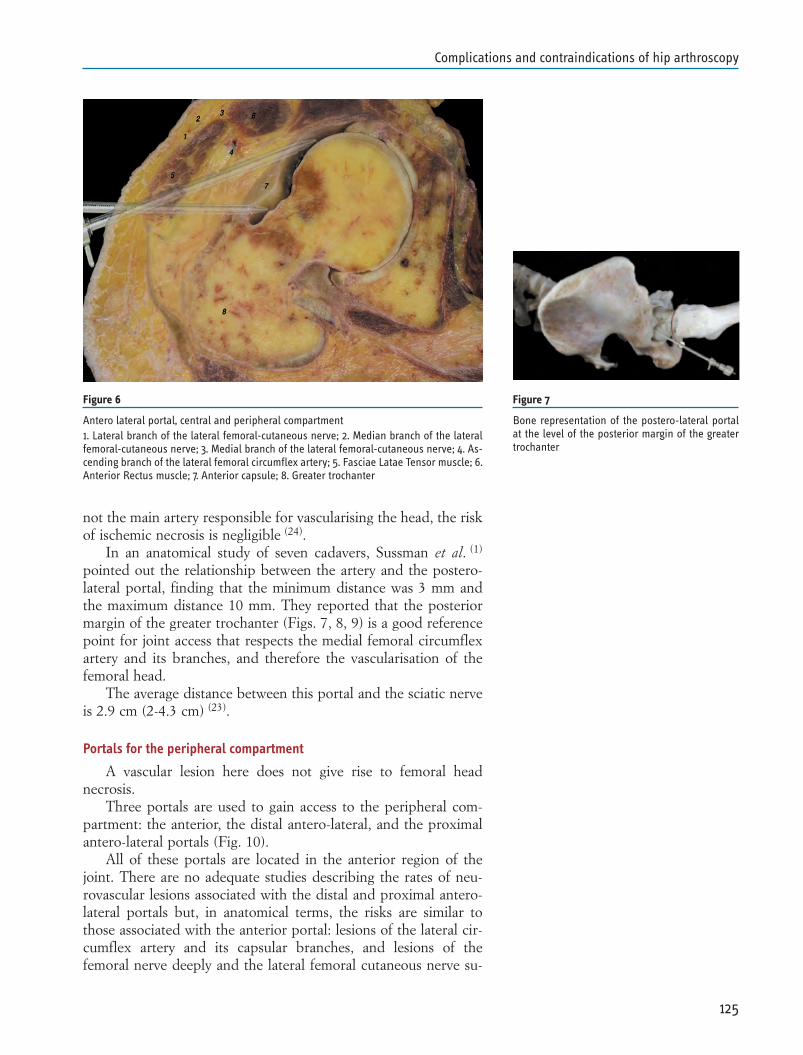
not the main artery responsible for vascularising the head, the riskof ischemic necrosis is negligible (24).
In an anatomical study of seven cadavers, Sussman et al. (1)
pointed out the relationship between the artery and the postero-lateral portal, finding that the minimum distance was 3 mm andthe maximum distance 10 mm. They reported that the posteriormargin of the greater trochanter (Figs. 7, 8, 9) is a good referencepoint for joint access that respects the medial femoral circumflexartery and its branches, and therefore the vascularisation of thefemoral head.
The average distance between this portal and the sciatic nerveis 2.9 cm (2-4.3 cm) (23).
Portals for the peripheral compartment
A vascular lesion here does not give rise to femoral headnecrosis.
Three portals are used to gain access to the peripheral com-partment: the anterior, the distal antero-lateral, and the proximalantero-lateral portals (Fig. 10).
All of these portals are located in the anterior region of thejoint. There are no adequate studies describing the rates of neu-rovascular lesions associated with the distal and proximal antero-lateral portals but, in anatomical terms, the risks are similar tothose associated with the anterior portal: lesions of the lateral cir-cumflex artery and its capsular branches, and lesions of thefemoral nerve deeply and the lateral femoral cutaneous nerve su-
125
Complications and contraindications of hip arthroscopy
Figure 6
Antero lateral portal, central and peripheral compartment1. Lateral branch of the lateral femoral-cutaneous nerve; 2. Median branch of the lateralfemoral-cutaneous nerve; 3. Medial branch of the lateral femoral-cutaneous nerve; 4. As-cending branch of the lateral femoral circumflex artery; 5. Fasciae Latae Tensor muscle; 6.Anterior Rectus muscle; 7. Anterior capsule; 8. Greater trochanter
Figure 7
Bone representation of the postero-lateral portalat the level of the posterior margin of the greatertrochanter
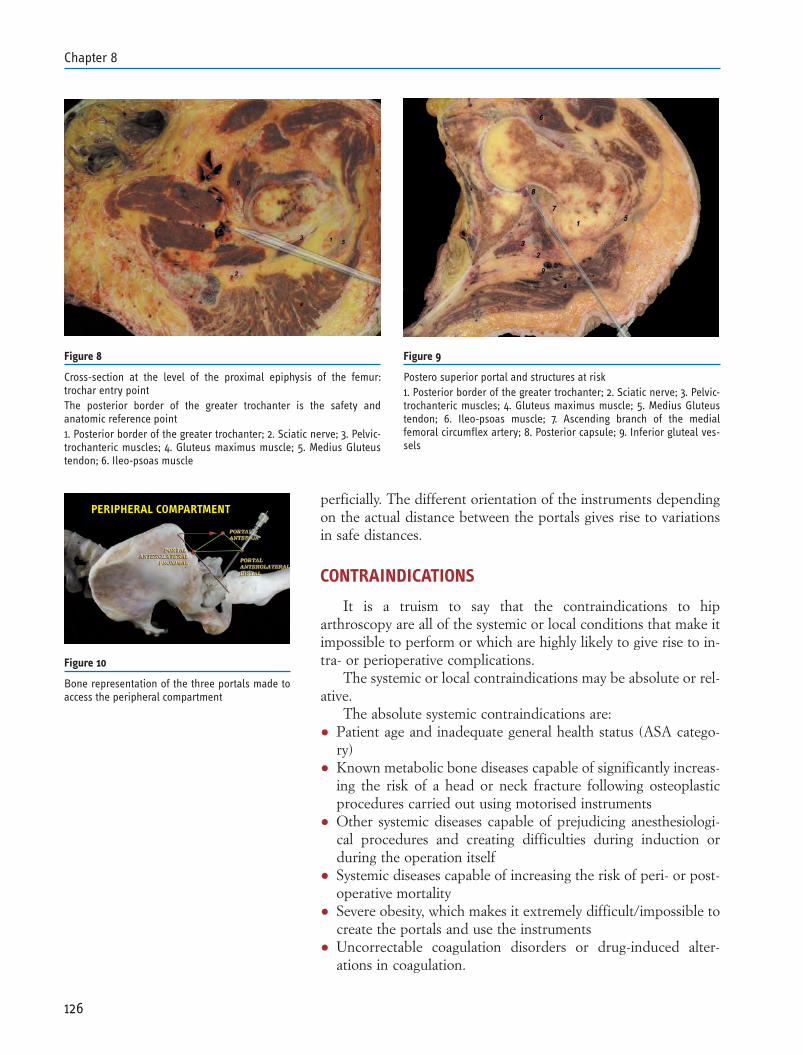
perficially. The different orientation of the instruments dependingon the actual distance between the portals gives rise to variationsin safe distances.
CONTRAINDICATIONS
It is a truism to say that the contraindications to hiparthroscopy are all of the systemic or local conditions that make itimpossible to perform or which are highly likely to give rise to in-tra- or perioperative complications.
The systemic or local contraindications may be absolute or rel-ative.
The absolute systemic contraindications are:• Patient age and inadequate general health status (ASA catego-
ry)• Known metabolic bone diseases capable of significantly increas-
ing the risk of a head or neck fracture following osteoplasticprocedures carried out using motorised instruments
• Other systemic diseases capable of prejudicing anesthesiologi-cal procedures and creating difficulties during induction orduring the operation itself
• Systemic diseases capable of increasing the risk of peri- or post-operative mortality
• Severe obesity, which makes it extremely difficult/impossible tocreate the portals and use the instruments
• Uncorrectable coagulation disorders or drug-induced alter-ations in coagulation.
126
Chapter 8
Figure 8
Cross-section at the level of the proximal epiphysis of the femur:trochar entry pointThe posterior border of the greater trochanter is the safety andanatomic reference point1. Posterior border of the greater trochanter; 2. Sciatic nerve; 3. Pelvic-trochanteric muscles; 4. Gluteus maximus muscle; 5. Medius Gluteustendon; 6. Ileo-psoas muscle
Figure 9
Postero superior portal and structures at risk1. Posterior border of the greater trochanter; 2. Sciatic nerve; 3. Pelvic-trochanteric muscles; 4. Gluteus maximus muscle; 5. Medius Gluteustendon; 6. Ileo-psoas muscle; 7. Ascending branch of the medialfemoral circumflex artery; 8. Posterior capsule; 9. Inferior gluteal ves-sels
Figure 10
Bone representation of the three portals made toaccess the peripheral compartment
PERIPHERAL COMPARTMENT

The relative systemic contraindications are:• Moderate obesity• Correctable coagulation disorders or drug-induced alterations
in coagulation• Systemic diseases that may be pharmacologically corrected pre-
or perioperatively in such a way as to reduce significantly therisks related to the anesthesiological and surgical procedures.
When considering local contraindications, it is useful to makea topographical analysis of the potential sites of a contraindicationfrom the depth of the joint to the skin surface.
Once again, the contraindications may be absolute or relative.The following have been described in the literature (25,26):
• Previous traumas (fractures/dislocations) of the hip joint, withsequelae that make it extremely difficult or impossible to createthe surgical portals or distract the joint
• Coxa profunda/acetabular protrusion• Advanced stage arthrosis/ankylosis• Severe dysplasia• Cartilage and subchondral bone lesions at high risk of worsen-
ing after surgery• Femoral head osteonecrosis and collapse.• Grade III-IV heterotopic ossifications/periarticular calcifica-
tions• Skin wounds, cellulitis.
127
Complications and contraindications of hip arthroscopy
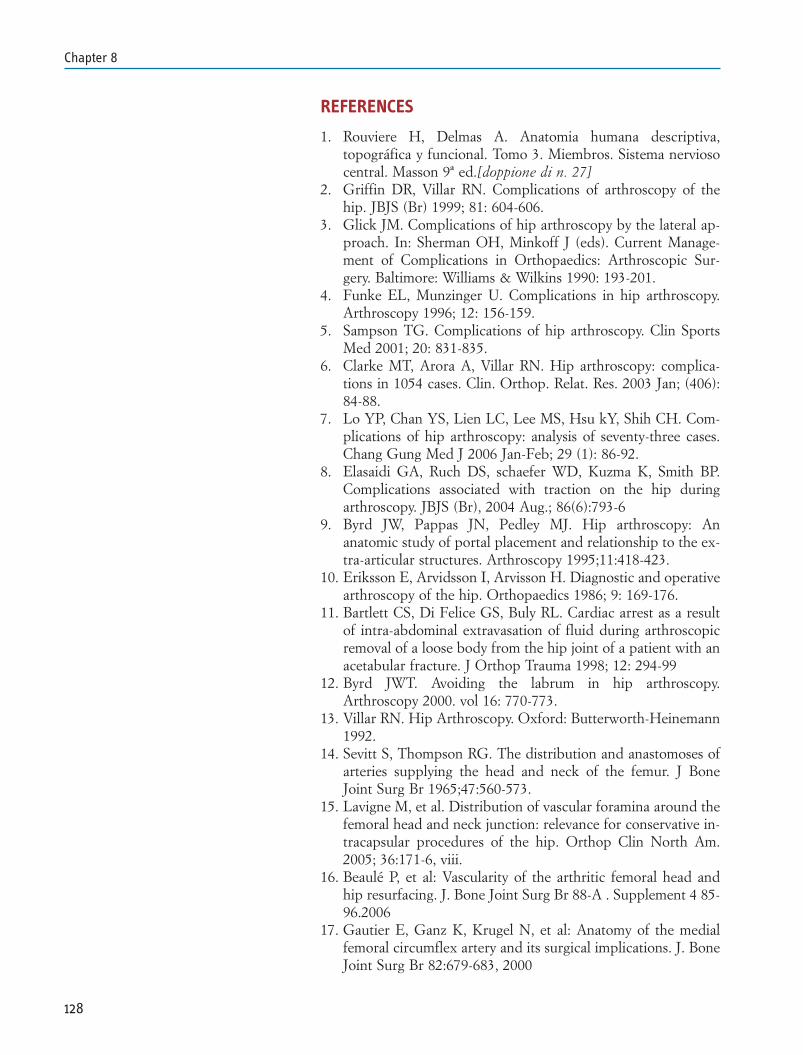
REFERENCES
1. Rouviere H, Delmas A. Anatomia humana descriptiva,topográfica y funcional. Tomo 3. Miembros. Sistema nerviosocentral. Masson 9ª ed.[doppione di n. 27]
2. Griffin DR, Villar RN. Complications of arthroscopy of thehip. JBJS (Br) 1999; 81: 604-606.
3. Glick JM. Complications of hip arthroscopy by the lateral ap-proach. In: Sherman OH, Minkoff J (eds). Current Manage-ment of Complications in Orthopaedics: Arthroscopic Sur-gery. Baltimore: Williams & Wilkins 1990: 193-201.
4. Funke EL, Munzinger U. Complications in hip arthroscopy.Arthroscopy 1996; 12: 156-159.
5. Sampson TG. Complications of hip arthroscopy. Clin SportsMed 2001; 20: 831-835.
6. Clarke MT, Arora A, Villar RN. Hip arthroscopy: complica-tions in 1054 cases. Clin. Orthop. Relat. Res. 2003 Jan; (406):84-88.
7. Lo YP, Chan YS, Lien LC, Lee MS, Hsu kY, Shih CH. Com-plications of hip arthroscopy: analysis of seventy-three cases.Chang Gung Med J 2006 Jan-Feb; 29 (1): 86-92.
8. Elasaidi GA, Ruch DS, schaefer WD, Kuzma K, Smith BP.Complications associated with traction on the hip duringarthroscopy. JBJS (Br), 2004 Aug.; 86(6):793-6
9. Byrd JW, Pappas JN, Pedley MJ. Hip arthroscopy: Ananatomic study of portal placement and relationship to the ex-tra-articular structures. Arthroscopy 1995;11:418-423.
10. Eriksson E, Arvidsson I, Arvisson H. Diagnostic and operativearthroscopy of the hip. Orthopaedics 1986; 9: 169-176.
11. Bartlett CS, Di Felice GS, Buly RL. Cardiac arrest as a resultof intra-abdominal extravasation of fluid during arthroscopicremoval of a loose body from the hip joint of a patient with anacetabular fracture. J Orthop Trauma 1998; 12: 294-99
12. Byrd JWT. Avoiding the labrum in hip arthroscopy.Arthroscopy 2000. vol 16: 770-773.
13. Villar RN. Hip Arthroscopy. Oxford: Butterworth-Heinemann1992.
14. Sevitt S, Thompson RG. The distribution and anastomoses ofarteries supplying the head and neck of the femur. J BoneJoint Surg Br 1965;47:560-573.
15. Lavigne M, et al. Distribution of vascular foramina around thefemoral head and neck junction: relevance for conservative in-tracapsular procedures of the hip. Orthop Clin North Am.2005; 36:171-6, viii.
16. Beaulé P, et al: Vascularity of the arthritic femoral head andhip resurfacing. J. Bone Joint Surg Br 88-A . Supplement 4 85-96.2006
17. Gautier E, Ganz K, Krugel N, et al: Anatomy of the medialfemoral circumflex artery and its surgical implications. J. BoneJoint Surg Br 82:679-683, 2000
128
Chapter 8
18. Carliouz H, Pous JG, Rey JC. Les epiphysiolyses femorales su-perrieures. Rev Chir Orthop Reparatice Appar Mot.1968;54:388-481
19. Anil S. Ranawat, MD et al. Anatomy of the hip: Open andarthroscopic structure and function. Operative Techniques inOrthopaedics. 15:160-174.2005
20. Dorfmann H, Boyer T. Hip arthroscopy utilizing the supineposition. Arthroscopy 12:264-267, 1996
21. Dorfmann H, Boyer T: Arthroscopy of the hip: 12 years of ex-perience. Arthroscopy 15:67-72, 1999
22. Wettstein M, et al: Arthroscopy of the Peripheral Compart-ment of the Hip. Oper Tech Orthop 15:225-230, 2005
23. Byrd Th: Hip arthroscopy: evolving frontiers. Elsevier 2004.24. McCarthy JC, Busconi B. The role of hip arthroscopy in the
diagnosis and treatment of hip disease. Orthopedics 1995;18:753-756
25. Kelly BT, Buly RL. Hip Arthroscopy Update. HSSJ (2005) 1;40-48.
26. McCarthy JC. Hip arthroscopy: when it is and it is not indicat-ed. Instr Course Lect 2004
27. Rouviere H, Delmas A. Anatomia humana descriptiva,topográfica y funcional. Tomo 3. Miembros. Sistema nerviosocentral. Masson 9ª ed[doppione di n. 1]
28. Byrd JWT, Pappas JN, Pedley MJ. Hip arthroscopy: ananatomic study. [mancano nome della rivista, pagg., ecc.
129
Complications and contraindications of hip arthroscopy

Chapter 9
INTRODUCTION
Two elements must be taken into consideration when speakingof rehabilitation after hip arthroscopy.
First there is a number of clinical conditions which can bene-fit from hip arthroscopy (1, 2) ranging from femoroacetabular im-pingement in an athlete (3) to the removal of a loose body in amiddle aged patient, to the controversial chapter of initial hiparthritis (4, 5). Thus it is not possible to generalize. Common reha-bilitative guidelines can be given but the individual protocol mustbe personalized according to the type of pathology, the age of thepatient, and the functional goals set.
Coherence between the “philosophical” decision to operateusing arthroscopy and a relative rehabilitation program is the sec-ond element to be considered.
If arthroscopy is selected so as to minimize the aggressivenessof the surgical procedure and to allow faster functional recovery,then the rehabilitation program chosen must fully meet these ob-jectives. This is why rehabilitation should start early. It shouldproceed progressively in order to avoid under or overstress the tis-sues around the joint and should aim toward the maximum func-tional recovery possible for each patient in treatment (6).
The majority of patients who opt for arthroscopy do not do sojust to solve pain issues. They choose it in order to achieve thehigh quality of life they had before surgery, doing more than justbasic activities of daily living. In most cases, patients desire to re-turn to a fully active lifestyle, moving around without any particu-lar restraints, and possibly going back to practice their favouritesport (7, 8, 9, 10).
Arthroscopy and rehabilitation must therefore both representstages of the same path to recovery; a path built on the balance be-tween the anatomic and clinical conditions of the patient and hisor her functional and sport expectations.
131
REHABILITATION AFTER HIP ARTHROSCOPYStefano Della VillaKyriakos TsapralisAlessandro Salsi

WHEN TO BEGIN REHABILITATION
Postoperative rehabilitation protocols commonly used afterminimally invasive total hip arthroplasty show that starting a reha-bilitation protocol early is safe and fulfils its potential benefits. (11,
12)
Despite this experience, in a similar situation, we agree withEnseki et al (13) that arthroscopic techniques often carry particularconcerns regarding range of motion, weight bearing precautionsand initiation of strength activities. It is essential to have a differ-ent approach depending on the specific procedure used such asloose body removal, labral tear resection, labral repair, osteochon-droplasty, shaving, microfractures.
Continuous passive motion (CPM) is useful right after surgery,as well as active exercises both for knee and ankle (Fig. 1). In ouropinion, regular common rehabilitation, including three visits aweek with the rehabilitation specialist, should start a week aftersurgery and the progression of the exercises should balance, ineach specific case, the advantages of a rapid recovery and the prin-ciples of tissue healing.
Rehabilitation in the swimming pool is also very useful (14, 15),but it should start only after two weeks, when the stitches are re-moved and the wound is healed (Fig. 2). Two weeks before start-ing rehabilitation in a pool may seem as a long time. It is howevernecessary to wait as pool water may irritate and infect the wound.Furthermore, our experience has shown that water-resistant band-ages do not guarantee complete protection.
PRECAUTIONS OF THE SURGEON
Before analyzing the rehabilitative guidelines after hiparthroscopy, we would like to point out how important it is for theorthopaedic surgeon to decide on precautions regarding weightbearing and range of motion for each patient. Informing the pa-tient about these parameters increases his/her compliance and ad-herence to the rehabilitation program (Fig. 3).
Only the surgeon who has performed the arthroscopy is awareof the specific situation of the tissues involved and can therefore,foresee the level of attention needed for their recovery.
Santori et al (16), recommend the use of crutches for three daysfollowed by full weight bearing, limiting flexion within 100° fortwo weeks, and limiting external rotation for four weeks afterlabral tear resection. In the case of labral repair, however, they rec-ommend no weight bearing for three weeks and early mobilizationto avoid joint stiffness.
In the case of femoroacetabular impingement treated with ac-etabuloplasty, Byrd et al (17) recommend weight bearing as tolerat-ed by the patient, while no weight bearing for three weeks is rec-ommended after femoroplasty. In both cases they agree to startearly joint mobilization.
132
Chapter 9
Figure 1
Continuous passive motion (CPM) right after sur-gery for hip, knee and ankle prevents muscle stiff-ness and reduces inflammation
Figure 2
Rehabilitation in the pool is a safe way to increaseROM and to progressively recover more complexpatterns
Figure 3
Education of the patient allows a better under-standing of the injury and rehabilitation plan andincreases his/her compliance
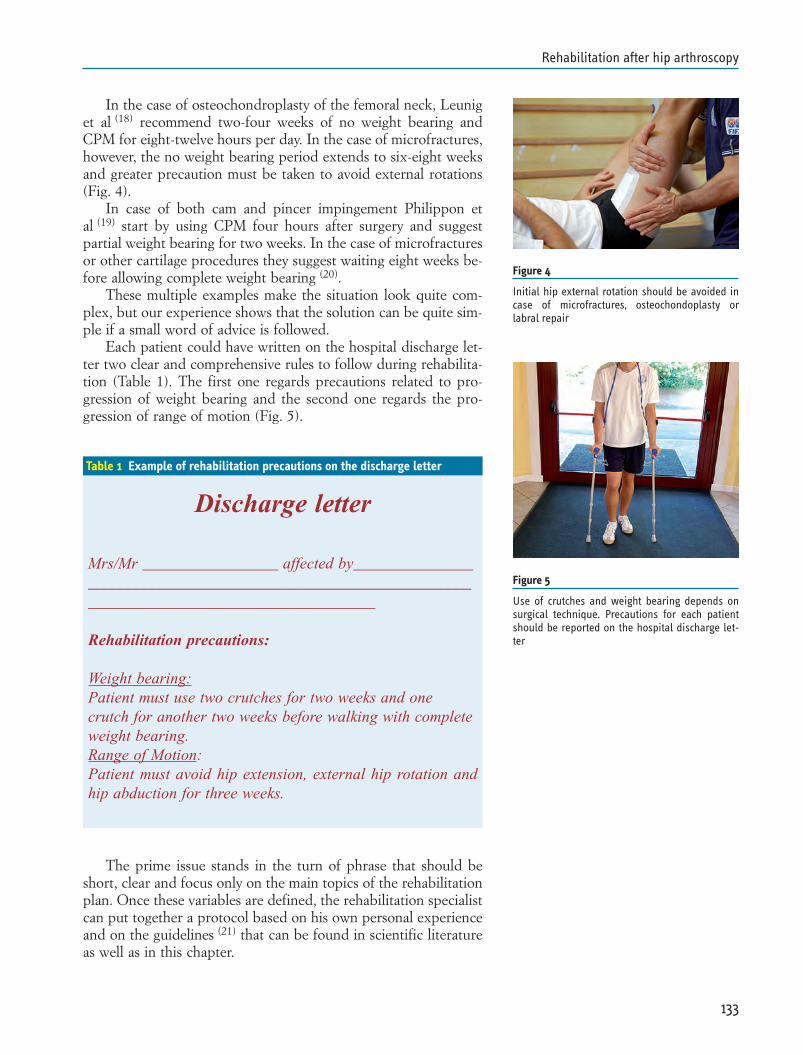
In the case of osteochondroplasty of the femoral neck, Leuniget al (18) recommend two-four weeks of no weight bearing andCPM for eight-twelve hours per day. In the case of microfractures,however, the no weight bearing period extends to six-eight weeksand greater precaution must be taken to avoid external rotations(Fig. 4).
In case of both cam and pincer impingement Philippon etal (19) start by using CPM four hours after surgery and suggestpartial weight bearing for two weeks. In the case of microfracturesor other cartilage procedures they suggest waiting eight weeks be-fore allowing complete weight bearing (20).
These multiple examples make the situation look quite com-plex, but our experience shows that the solution can be quite sim-ple if a small word of advice is followed.
Each patient could have written on the hospital discharge let-ter two clear and comprehensive rules to follow during rehabilita-tion (Table 1). The first one regards precautions related to pro-gression of weight bearing and the second one regards the pro-gression of range of motion (Fig. 5).
The prime issue stands in the turn of phrase that should beshort, clear and focus only on the main topics of the rehabilitationplan. Once these variables are defined, the rehabilitation specialistcan put together a protocol based on his own personal experienceand on the guidelines (21) that can be found in scientific literatureas well as in this chapter.
133
Rehabilitation after hip arthroscopy
Figure 4
Initial hip external rotation should be avoided incase of microfractures, osteochondoplasty orlabral repair
Figure 5
Use of crutches and weight bearing depends onsurgical technique. Precautions for each patientshould be reported on the hospital discharge let-ter
Table 1 Example of rehabilitation precautions on the discharge letter
Discharge letter
Mrs/Mr _________________ affected by___________________________________________________________________________________________________
Rehabilitation precautions:
Weight bearing:Patient must use two crutches for two weeks and onecrutch for another two weeks before walking with completeweight bearing. Range of Motion: Patient must avoid hip extension, external hip rotation andhip abduction for three weeks.
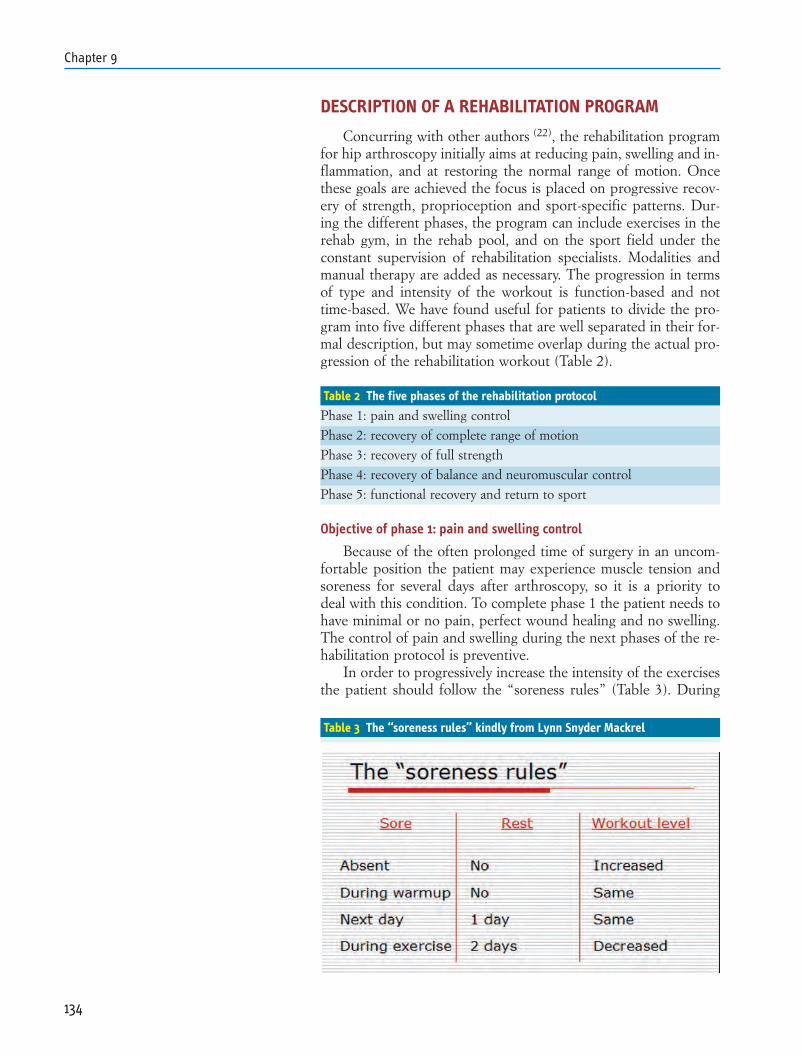
DESCRIPTION OF A REHABILITATION PROGRAM
Concurring with other authors (22), the rehabilitation programfor hip arthroscopy initially aims at reducing pain, swelling and in-flammation, and at restoring the normal range of motion. Oncethese goals are achieved the focus is placed on progressive recov-ery of strength, proprioception and sport-specific patterns. Dur-ing the different phases, the program can include exercises in therehab gym, in the rehab pool, and on the sport field under theconstant supervision of rehabilitation specialists. Modalities andmanual therapy are added as necessary. The progression in termsof type and intensity of the workout is function-based and nottime-based. We have found useful for patients to divide the pro-gram into five different phases that are well separated in their for-mal description, but may sometime overlap during the actual pro-gression of the rehabilitation workout (Table 2).
Objective of phase 1: pain and swelling control
Because of the often prolonged time of surgery in an uncom-fortable position the patient may experience muscle tension andsoreness for several days after arthroscopy, so it is a priority todeal with this condition. To complete phase 1 the patient needs tohave minimal or no pain, perfect wound healing and no swelling.The control of pain and swelling during the next phases of the re-habilitation protocol is preventive.
In order to progressively increase the intensity of the exercisesthe patient should follow the “soreness rules” (Table 3). During
134
Chapter 9
Table 2 The five phases of the rehabilitation protocol
Phase 1: pain and swelling control
Phase 2: recovery of complete range of motion
Phase 3: recovery of full strength
Phase 4: recovery of balance and neuromuscular control
Phase 5: functional recovery and return to sport
Table 3 The “soreness rules” kindly from Lynn Snyder Mackrel

phase 1 the progression of the walking pattern should be careful-ly followed by the rehabilitation specialist in accordance with sur-geon’s precautions.
Objective of phase 2: recovery of full range of motion
Early mobilization of the ankle, knee and hip with passive andthen active exercises are very useful from the onset of rehabilita-tion. In the first few weeks precautions are usually followed forexternal rotation and abduction.
To progressively increase the intensity of the range of motionexercises the patient should follow the precautions of the surgeon.
Each range of motion exercise session should start with awarm up activity on a stationary bike (Fig. 6) and should finishwith a cool down with ice pack (Fig. 7). Active, assisted and pas-sive movement with the help of the physical therapist could beadded when the progression of the range of motion is too slow(Fig. 8).
Passive stretching could be useful to increase flexibility of thetissues around the joint (Figs. 9, 10, 11, 12).
To complete phase 2 the patient has to reach the same range ofmotion on both limbs.
135
Rehabilitation after hip arthroscopy
Figure 8
The therapist produces an external rota-tion while hip is abducted and flexed at90°
Figure 9
Soft hip pompage reduces tension on cap-sular structures
Figure 10
Stretching for lateral capsular structuresand iliotibial band
Figure 11
Assisted stretching with rope for ham-string muscles. Low back is placed in hori-zontal position
Figure 7
Cryotherapy at the end of the session is ef-fective in decreasing pain and swelling
Figure 6
Stationary bike with adjustable seat used both forwarm-up and increasing ROM. Initially resistanceis minimal in order to avoid excessive hip involve-ment

Objective of phase 3: recovery of strength
While in orthopaedics the study of muscle groups is often con-ducted to identify the best surgical access, in rehabilitation it isnecessary for understanding their role as motors and stabilizers ofa joint’s movement (23, 24).
From this point of view, the hip is particularly complex asmany muscles from the trunk and the lower limb act upon it bothdirectly and indirectly.
Recovering the strength of the muscles directly related to thehip is not enough to restore proper biomechanical function of thejoint itself. Adequate core stability and good control of the kneeand ankle joints are also necessary. The recovery of strength formuscles such as iliopsoas, gluteus maximus, piriform, gluteusmedius, is particularly important for recovering a normal gait pat-tern (Figs. 13, 14, 15, 16).
Objective of phase 4: recovery of balance and neuromuscular control
Phase 4 pays special attention to complete recovery of propri-oception. Balance exercises on unstable boards and mini trampo-lines are introduced progressively with increasing difficulty: atfirst with no weight bearing, followed by weight bearing on both
136
Chapter 9
Figure 12
Assisted stretching for iliopsoas muscle withoutarching lower back
Figure 13
Strengthening exercise for iliop-soas muscle using weight (in hipflexion)
Figure 14
Progression of strength activitiesfor gluteus maximus begin twoweeks after surgery (in hip exten-sion)
Figure 15
Strengthening exercise for piri-formis muscle using elastic resist-ance (in external hip rotation)
Figure 16
Strengthening activity using man-ual resistance for lateral musclechain including gluteus medius,quadratus lumborum, iliotibialband (in hip abduction)

feet, then on one foot, and finally with extreme disturbance (Figs.17, 18). A workout of this type, with simple exercises, can be per-formed carefully as of phases 2 and 3. More complex exercises(Fig. 19) involving high instability can only be inserted in phase 4when muscle strength is sufficient.
Neuromuscular control of complex movements involves pre-cise muscle synchronicity and synergy requiring various steps: theability to conceive movement at cortical level, the ability to coor-dinate movement at subcortical level, the ability to modulatemovement at spinal level, and the strength to carry out that partic-ular movement thanks to sufficient tone of muscles involved.
Proper neuromotor control protects tissues from mechanicalstress that is developed when patient is progressively gaining fullfunction.
Objective of phase 5: complete functional recovery and return to sport
This phase ends with occupational therapy. Patients who donot practice sport can complete this phase either in the gym or inthe pool, simulating daily routine activities. Professional athletes,however, must carry out sport-specific exercises on the field orcourt under the supervision of athletic trainers.
The literature confirms cases of complete recovery at the pre-injury level after hip arthroscopy (25, 26, 27). According to our expe-rience, in order to ensure a high probability of achieving the afore-
137
Rehabilitation after hip arthroscopy
Figure 17
Low instability proprioceptive exer-cise. Single leg balance on a foamwith opened or closed eyes
Figure 18
High instability exercise in order to improve neu-romotor control using unstable surfaces such asfoam and tilt-board
Figure 19
Skipping on trampoline with lateral destabiliza-tion allows better activation of gluteus mediusand improves lumbopelvic stability

mentioned, on-field or on-court rehabilitation must receive thesame consideration as rehab in the gym or in the pool.
Details of rehabilitation program performed in each one ofthese facilities are explained in the following chapters.
REHABILITATION FACILITIES
Just as a surgeon needs a surgery room to do his job, the phys-ical therapist needs an adequate, well supplied facility. Appropri-ate facilities such as a pool, a gym, and a field/court are necessaryfor proper rehabilitation. The use of these three settings at precisetime can protect against potential overload during the initial phas-es and can allow the patient to reach maximum functional recov-ery at the end of rehabilitation.
The gym is still considered the most common rehabilitationarea where an average of 60% of the total sessions are held andwhere modalities, manual therapy, massage therapy and other spe-cific exercises of the first four phases are carried out.
Right after removing stitches (around day 14), if the wound isin good condition, the patient should start rehabilitation in thepool which will cover about 20% of the total sessions. Water of-fers many advantages: allowing work in the absence of gravity,controlling weight bearing progression, promoting joint mobiliza-tion, and simulating complex specific patterns (Fig. 20).
Rehabilitation on field/court is usually handled by the team’scoach and is not directly controlled by the physician and physicaltherapists that have worked with the athlete until then. The intro-duction of specifically educated athletic trainers in the rehabilita-tion team ensures constant supervision of the patient, exactly asthe physical therapists do in the gym. The progression of each ex-ercise on the field follows basic science rules respecting the mus-culoskeletal and neurological components involved in the recoveryprocess.
Rehabilitation in the gym
In the rehab gym pain and swelling are managed throughmodalities and specific drainage massage. Particular attention isthen focused on the recovery of full range of motion in order toprevent a persistent limp and to avoid joint stiffness. A stretchingprotocol involving posterior, anterior and lateral muscle chain iscarried out respecting patients’ sensations. Correct walking reedu-cation includes exercises in front of a mirror so that the patientcan observe and correct his own gait. Introduction of open kinet-ic chain exercises (Fig. 21) initially begins with low impact exercis-es. Isotonic devices are used with progressive resistance. Closedkinetic chain exercises (Fig. 22) are soon introduced on a horizon-tal elastic leg press, which allows the patient to perform very lighteccentric and plyometric exercises. The restoration of propriocep-tive abilities occurs by way of increasingly difficult exercises. Atfirst unstable boards are inserted. Then we move on to the use of
138
Chapter 9
Figure 20
Walking and running are basic patterns for differ-ent sport activities. Water allows fast and safe re-covery of movement
Figure 21
Open kinetic chain exercise for gluteus maximuswithout weight

proprioceptive paths which become increasingly more complexwith the addition of core stability elements. Exercises with a ballin unstable situations are performed in order to gain confidencewith it. We also begin working on sport-specific endurancethrough incremental workout on treadmill and elliptical device(Fig. 23). Finally, the program in the gym includes skipping on thetrampoline and other specific skills before passing to the on-fieldrehabilitation.
Rehabilitation in the pool
The potential of aquatic rehabilitation in orthopaedic diseaseshas greatly advanced in the last decade and has offered a new per-spective (28). It is considered not only an ideal way to protect re-paired tissues and to recover the normal range of motion but alsoan opportunity to start at once the progressive recovery of morecomplex movements. The protocol includes an initial phase ofself-stretching repetitions with the use of a lifejacket (Fig. 24).Particular attention is paid to the physiological motor pattern ofstep taking. The exercises for strengthening different musclegroups may be progressively started. The eccentric workout isheightened by decreasing the depth of immersion and that de-pends on the type of surgical technique used. Progressively com-plex proprioceptive exercises, including sport-specific patterns areadded simultaneously. This greatly motivates the patient and alsomaintains motor patterns which have been lost due to surgerywithout overloading the injured tissues. For example, having thepatient walk in water with the intention of bunting a ball rightwhere the therapist tosses it, will achieve completely different re-sults than having him or her simply walk in water. This approachdoes not only stimulate the musculoskeletal system, it also stimu-lates neuroplasticity.
Rehabilitation on sport field
Consensus statement of the American College of Sports Med-icine (29) states that providing sport-specific assessment and train-ing, to serve as a basis for reconditioning, is essential for the ath-lete’s rehabilitation. Various authors agree that the ultimate mile-stone of an athlete’s rehabilitation is the complete recovery ofsport-specific movements he or she was capable of before injury.Other authors (30) state functional sport-specific rehabilitation as afundamental part of the process. According to the general agree-ments and to our philosophy, when the patient is an athlete, we al-so suggest the introduction of a part of rehabilitation on the fieldafter hip arthroscopy (Fig. 25). In the first few sessions patientsare submitted to global coordination and running exercises on astraight line including bipedal jumps and land-offs. Then, focus isplaced on eccentric loads, running with stops and single/doublefoot leaps. Exercises with the ball are introduced. Progressivechanges in direction and speed while running along with more in-
139
Rehabilitation after hip arthroscopy
Figure 22
Closed kinetic chain exercise on a horizontal elas-tic press using unstable surface such as a swissexercise ball
Figure 23
Running on an elliptical device in the rehab gymbefore performing normal running activity on thefield reduces ground reaction forces and allows aprogressive loading on the knee joint
Figure 24
Self-stretching exercises using lifejacket of differ-ent size improve flexibility and increase range ofmotion

tense aerobic workout are then performed. During the last ses-sions, the focus is on improving each sport-specific pattern whilesimulating normal match conditions. During rehabilitation ses-sions lactate threshold tests are performed in order to optimizeaerobic and anaerobic workout and also to obtain athletic condi-tion as close as possible to the pre-injury level (Fig. 26).
HOW TO PUT TOGETHER A SPECIFIC PROTOCOL
Based on the preceding paragraphs, we suggest putting to-gether a specific rehabilitation protocol for each patient dividedinto five phases. Its progression should depend on precautionssuggested by the surgeon and the patient’s functional response(criteria-based progression).
On the other hand, time-based progression offers the advan-tage of giving precise rules and avoiding early overload risks butdoes not take into consideration the patient’s compliance, thusslowing down recovery times especially in the final phases of reha-bilitation. There is no clear scientific evidence regarding rehabili-tation protocols. In fact, there is still much controversy in the in-ternational scientific debate, not only on recent surgical proce-dures such as hip arthroscopy, but also on other joints which havebeen well studied over the last twenty years, such as the knee (31).
This is why, in our plan for hip arthroscopy for femoroacetab-ular impingement, we have underlined not only the goals to bemet in each phase, but also the approximate time necessary beforecontinuing onto the next one (Table 4). The protocol plan at-tached should be considered only an example as a surgeon, whenconducting hip arthroscopy, may have to perform one or moresurgical procedures at the same time. Femoroacetabular impinge-ment may be treated by femoroplasty, labral repair or microfrac-tures, thus making it impossible to standardize a protocol.
Generally speaking, the surgeon’s precautions must be takeninto great consideration and must be respected during the firsttwo phases. In the second two phases, overload must be avoidedto prevent hip flexor tendonitis, trochanteric bursitis and synovi-tis. In the last phase, attention must be given to the perfect recov-ery of sport-specific patterns before allowing safe return to profes-sional sport.
140
Chapter 9
Figure 25
Restoring sport-specific patterns is the goal of arehabilitation plan after hip arthroscopy. Complexexercises with a ball are progressively introducedon the field
Table 4 Example of rehabilitation plan after arthroscopy for femoroacetabular impingement (30 visits in 8 weeks)
1° 2° 3° 4° 5° 6° 7° 8° Totalweek week week week week week week week
Number of rehab sessions in the gym 3 3 2 2 2 2 2 2 18
Number of rehab sessions in the pool 2 2 2 6
Number of rehab sessions on the sport field 2 2 2 6
Figure 26
Reconditioning before return to sport protectsfrom re-injuries. Lactate threshold tests are usefulto determine specific aerobic and anaerobic work-out

CONCLUSIONS
Hip arthroscopy has led to important advantages both on di-agnostic fronts, by clarifying different types of injuries, and onfunctional recovery fronts, by allowing good recovery of active lifein a short period of time. Despite this positive outlook, we shouldremember that results are not always those desired. There is still alarge margin for improvement both on surgical indications andtechniques and on rehabilitation protocols. According to the pres-ent scientific evidence, there are three solid points after hiparthroscopy. The first one is the importance of having brief but ef-ficient communication between the orthopaedic surgeon and therehabilitation specialist regarding precautions necessary in eachcase depending on the different surgical procedures used. Thiswould avoid having very detailed, but often quite standard, proto-cols. The second one is knowing and respecting the tissue healingproperties according to the characteristics of each patient. Thethird one is following a progression of the rehabilitation protocolwhich goes beyond the simple pain relief and points to the maxi-mum functional recovery through subsequent regaining of rangeof motion, strength, neuromuscular control, and sport-specificpatterns.
141
Rehabilitation after hip arthroscopy
REFERENCES
1. Diulus CA, Krebs VE, Hanna G, Barsoum WK. Hiparthroscopy technique and indications. J Arthroplasty. 2006;21: 68-73.
2. Rühmann O. Arthroscopy of the hip joint: indication, tech-nique, results. Dtsch Arztebl Int. 2008; 105: 559-66.
3. Philippon MJ, Yen YM, Briggs KK, Kuppersmith DA,Maxwell RB. Early outcomes after hip arthroscopy forfemoroacetabular impingement in the athletic adolescent pa-tient: a preliminary report. J Pediatr Orthop. 2008; 28: 705-10.
4. Byrd JW, Jones KS. Hip arthroscopy for labral pathology:prospective analysis with 10-year follow-up. Arthroscopy. 2009;25: 365-8.
5. Byrd JW, Jones KS. Prospective analysis of hip arthroscopywith 10-year follow up. Clin Orthop Relat Res. 2010; 468: 741-6.
6. Brunner A, Horisberger M, Herzog RF. Sports and recreationactivity of patients with femoroacetabular impingement beforeand after arthroscopic osteoplasty. Am J Sports Med. 2009; 37:917-22.
7. Philippon MJ, Schenker ML. Arthroscopy for the treatment offemoroacetabular impingement in the athlete. Clin Sports Med.2006; 25: 299-308, ix.
8. Byrd JW, Jones KS. Hip arthroscopy in athletes: 10-year fol-low-up. Am J Sports Med. 2009; 37: 2140-3.
9. Philippon M, Schenker M, Briggs K, Kuppersmith D.Femoroacetabular impingement in 45 professional athletes: as-sociated pathologies and return to sport following arthroscop-ic decompression. Knee Surg Sports Traumatol Arthrosc. 2007;15: 908-14.
10. Philippon MJ, Briggs KK, Yen YM, Kuppersmith DA. Out-comes following hip arthroscopy for femoroacetabular im-pingement with associated chondrolabral dysfunction: mini-mum two-year follow-up. J Bone Joint Surg Br. 2009; 91: 16-23.
11. Berger RA, Jacobs JJ, Meneghini RM, Della Valle C, PaproskyW, Rosenberg AG. Rapid rehabilitation and recovery withminimally invasive total hip arthroplasty. Clin Orthop RelatRes. 2004; (429): 239-47.
12. Vavken P, Kotz R, Dorotka R. Minimally invasive hip replace-ment: a meta-analysis. Z Orthop Unfall. 2007; 145: 152-6.
13. Enseki KR, Martin RL, Draovitch P, Kelly BT, Philippon MJ,Schenker ML. The hip joint: arthroscopic procedures andpostoperative rehabilitation. J Otrhop Sports Phys Ther. 2006;36: 516-25.
14. Kim E, Kim T, Kang H, Lee J, Childers MK. Aquatic versusland-based exercises as early functional rehabilitation for eliteathletes with acute lower extremity ligament injury: a pilotstudy. PM R. 2010; 1.
15. Harmer AR, Naylor JM, Crosbie J, Russell T. Land-based ver-
142
Chapter 9
sus water-based rehabilitation following total knee replace-ment: a randomized, single-blind trial. Arthritis Rheum. 2009;61: 184-91.
16. Santori N, Villar RN. Acetabular labral tears: result of arthro-scopic partial limbectomy. Arthroscopy. 2000; 16: 11-5.
17. Byrd JW, Jones KS. Arthroscopic femoroplasty in the manage-ment of cam-type femoroacetabular impingement. Clin OrthopRelat Res. 2009; 467: 739-46.
18. Leunig M, Huff TW, Ganz R. Femoroacetabular impinge-ment: treatment of the acetabular side. Instr Course Lect. 2009;58: 223-9.
19. Philippon MJ, Stubbs AJ, Schenker ML, Maxwell RB, GanzR, Leunig M. Arthroscopic management of femoroacetabularimpingement: osteoplasty technique and literature review. AmJ Sports Med. 2007; 35:1571-80.
20. Crawford K, Philippon MJ, Sekiya JK, Rodkey WG, SteadmanJR. Microfracture of the hip in athletes. Clin Sports Med. 2006;25: 327-35, x.
21. Enseki KR, Martin R, Kelly BT. Rehabilitation after arthro-scopic decompression for femoroacetabular impingement.Clin Sports Med. 2010; 29: 247-55, viii.
22. Stalzer S, Wahoff M, Scanlan M. Rehabilitation following hiparthroscopy. Clin Sports Med. 2006; 25: 337-57, x.
23. Byrd JW. Hip arthroscopy: patient assessment and indications.Instr Course Lect. 2003; 52: 711-9.
24. Byrd JW. Hip arthroscopy: surgical indications. Arthroscopy.2006; 22: 1260-2.
25. Griffin KM. Rehabilitation of the hip. Clin Sports Med. 2001;20: 837-50, viii.
26. Bharam S. Labral tears, extra-articular injuries, and hiparthroscopy in the athlete. Clin Sports Med. 2006; 25: 279-92,ix.
27. Singh PJ, O’Donnell JM. The outcome of hip arthroscopy inAustralian football league players: a review of 27 hips.Arthroscopy. 2010; 26: 743-9.
28. Becker BE. Aquatic therapy: scientific foundations and clinicalrehabilitation applications. PM R. 2009; 1: 859-72.
29. Herring SA, Bergfeld JA, Boyd J, Duffey T, Fields KB, GranaWA, Indelicato P, Kibler WB, Pallay R, Putukian M, Sallis RE.The team physician and return to play issues: a consensusstatement. Med Sci Sports Exerc. 2002; 34: 1212-14.
30. Kvist J. Rehabilitation following anterior cruciate ligament in-jury: current recommendations for sports participation. SportsMed. 2004; 34: 269-80.
31. Pezzullo DJ, Fadale P. Current controversies in rehabilitationafter anterior cruciate ligament reconstruction. Sports MedArtrosc. 2010; 18: 43-7.
143
Rehabilitation after hip arthroscopy

Surgical Techniques

INTRODUCTION
Hip arthroscopy has become a useful tool in the treatment ofa wide variety of hip disorders. Not only is it possible to confirmthe diagnosis using hip arthroscopy, it is may also be possible todefinitively treat or at least temporize until a more invasive opera-tion is undertaken. Making the correct diagnosis before surgery isimportant. It should be possible to do this with a thorough histo-ry and physical along with plain radiographs. Ancillary tests suchas MRI and CT scans can be used to improve the accuracy of thediagnosis. In rheumatologic disorders, laboratory tests are alsohelpful. It is extremely important to know the natural history ofunderlying disorders in order to predict whether or not hiparthroscopy alone will suffice.
There are conditions which are primarily “intrinsic” to the hipjoint, such as synovial chondromatosis or pigmented villonodularsynovitis, where the problem seems to arise solely from within thejoint itself. “Extrinsic” disorders are those that cause damage byacting upon the hip joint from the outside. These conditions caninclude rheumatoid or osteoarthritis, hip dysplasia, femoroacetab-ular impingement, septic arthritis or trauma. The final commonpathway is progressive joint destruction unless intervention is un-dertaken. This chapter will discuss the options in the treatment ofsynovial and cartilage disorders in the hip.
SYNOVIAL DISORDERS
Synovial Chondromatosis
In this unusual disorder of unknown etiology, the synoviumproduces cartilaginous bodies which bud off from the synoviumand then cause damage within the joint by their mechanical pres-ence. In the past, the diagnosis was often difficult to make becausethe loose bodies may not be calcified. The advancement of highresolution MRI scanning has made it extremely easy to make thediagnosis.
147
Chapter 10SYNOVIAL AND CHONDRAL DISEASE: THE ROLE OF HIP ARTHROSCOPYRobert L. BulyLuis E. Moya

It can be difficult or even impossible to cure this disorder un-less a complete synovectomy is performed. This can be difficult todo because it may jeopardize the blood supply to the femoral headif the debridement is performed at the postero-superior head-neckjunction. Surgical decision making usually comes down to makinga choice between an open or arthroscopic procedure. The groupfrom Bern, Switzerland has reported on a series of eight casestreated successfully by surgical dislocation and a “modified” totalsynovectomy. The word “modified” is used because of the con-cern about the blood supply to the femoral head (52).
At a mean followup of 6.5 years, two patients required totalhip replacement for osteoarthritis but did not have recurrentchondromatosis. The remaining six patients had no evidence ofrecurrent disease.
Lim (41) reported on a series of 21 patients with synovial chon-dromatosis treated with either a surgical dislocation or an arthro-tomy without dislocation at a mean of 4.4 years followup.. Therewere 2 recurrences in the 13 cases treated without dislocation andnone in the 8 cases with dislocation; this finding was not statisti-cally significant. While the recurrence rate was lower with disloca-tion, the complication rate was higher.
Boyer (3) treated 120 patients arthroscopically for this disorder,111 of which were available for followup. Excellent or good out-comes were reported in 56.7% while 20% had undergone totalhip replacement. Open surgery was required in 38% while 21%required more than one arthroscopy. They conclude that hiparthroscopy is certainly a beneficial procedure in the treatment ofthis disorder.
In treating this condition arthroscopically, it is important togain maximum access. Before undertaking this procedure, pre-op-erative planning is important. If the joint is absolutely packed withhundreds of loose bodies, many of which are larger than the diam-eter of the cannulae, it may be more prudent to proceed directlyto an open procedure. At times, numerous loose bodies may becongealed into a large mass, often several centimeters in diameter,which can completely fill the acetabular fossa.
Surgery may be performed in either the lateral or supine posi-tion (5,6,20,21). The surgeon should use whichever standard portalswill permit full access to the joint. These can be lateral, postero-lateral, antero-lateral or anterior. Traction is required to fully visu-alize the central compartment. In addition, accessory portals es-tablished more distally can permit access to the peripheral com-partment and the inferior recess of the joint (13). When accessingthe peripheral compartment, there is no need for traction; there-fore the capsule is more distended and movement within the jointis easier. In addition to removing the bodies, as much synovium aspossible should be removed with a shaver or radiofrequencyprobe in an effort to slow down recurrence. For very large loosebodies, it may be necessary to enlarge the portal size in the capsulewith a knife or radiofrequency probe before attempting to extract
148
Chapter 10
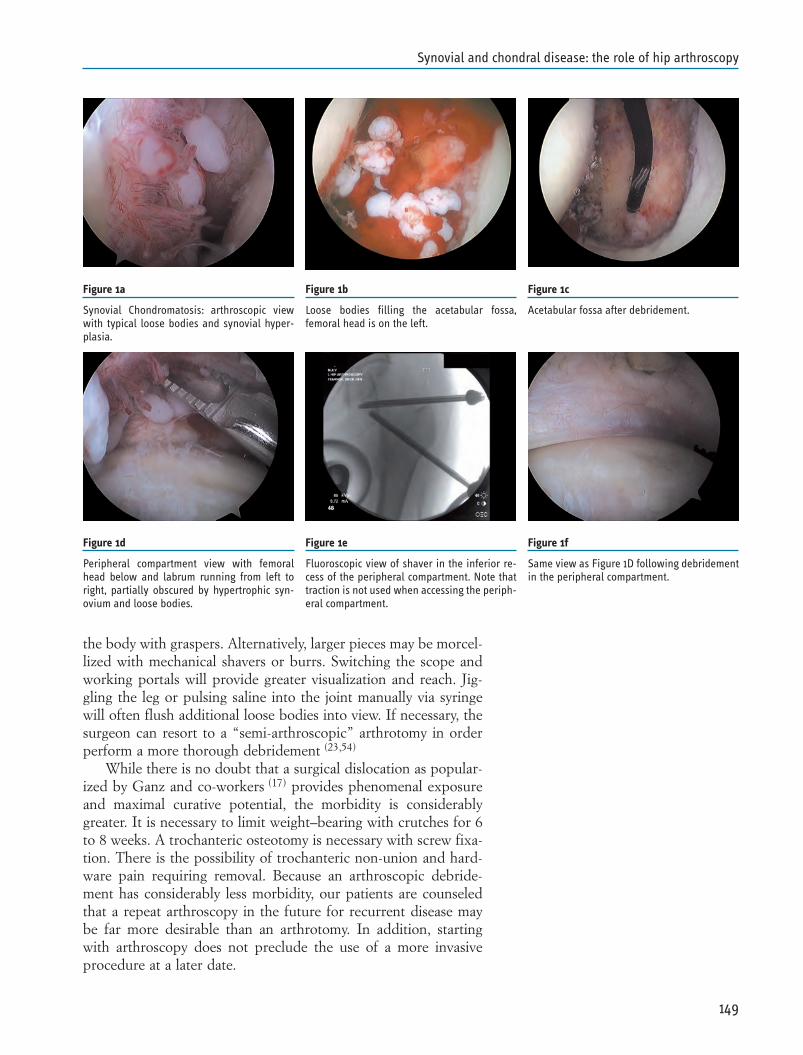
the body with graspers. Alternatively, larger pieces may be morcel-lized with mechanical shavers or burrs. Switching the scope andworking portals will provide greater visualization and reach. Jig-gling the leg or pulsing saline into the joint manually via syringewill often flush additional loose bodies into view. If necessary, thesurgeon can resort to a “semi-arthroscopic” arthrotomy in orderperform a more thorough debridement (23,54)
While there is no doubt that a surgical dislocation as popular-ized by Ganz and co-workers (17) provides phenomenal exposureand maximal curative potential, the morbidity is considerablygreater. It is necessary to limit weight–bearing with crutches for 6to 8 weeks. A trochanteric osteotomy is necessary with screw fixa-tion. There is the possibility of trochanteric non-union and hard-ware pain requiring removal. Because an arthroscopic debride-ment has considerably less morbidity, our patients are counseledthat a repeat arthroscopy in the future for recurrent disease maybe far more desirable than an arthrotomy. In addition, startingwith arthroscopy does not preclude the use of a more invasiveprocedure at a later date.
149
Synovial and chondral disease: the role of hip arthroscopy
Figure 1a
Synovial Chondromatosis: arthroscopic viewwith typical loose bodies and synovial hyper-plasia.
Figure 1b
Loose bodies filling the acetabular fossa,femoral head is on the left.
Figure 1c
Acetabular fossa after debridement.
Figure 1d
Peripheral compartment view with femoralhead below and labrum running from left toright, partially obscured by hypertrophic syn-ovium and loose bodies.
Figure 1e
Fluoroscopic view of shaver in the inferior re-cess of the peripheral compartment. Note thattraction is not used when accessing the periph-eral compartment.
Figure 1f
Same view as Figure 1D following debridementin the peripheral compartment.
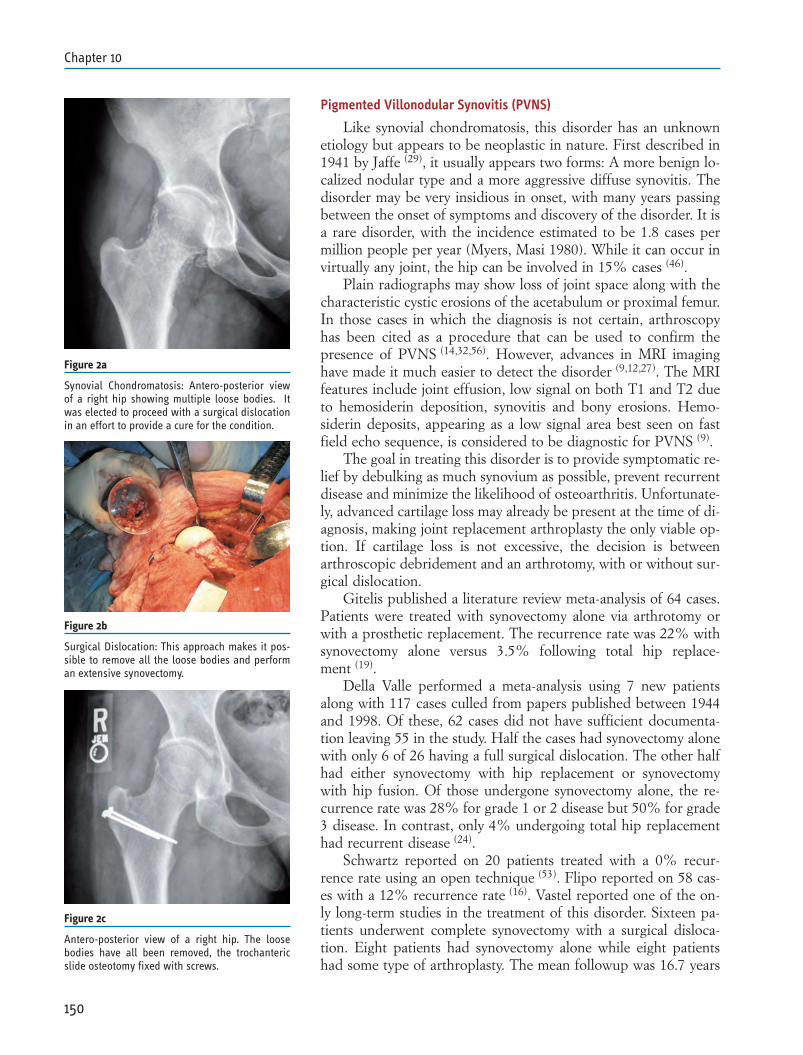
Pigmented Villonodular Synovitis (PVNS)
Like synovial chondromatosis, this disorder has an unknownetiology but appears to be neoplastic in nature. First described in1941 by Jaffe (29), it usually appears two forms: A more benign lo-calized nodular type and a more aggressive diffuse synovitis. Thedisorder may be very insidious in onset, with many years passingbetween the onset of symptoms and discovery of the disorder. It isa rare disorder, with the incidence estimated to be 1.8 cases permillion people per year (Myers, Masi 1980). While it can occur invirtually any joint, the hip can be involved in 15% cases (46).
Plain radiographs may show loss of joint space along with thecharacteristic cystic erosions of the acetabulum or proximal femur.In those cases in which the diagnosis is not certain, arthroscopyhas been cited as a procedure that can be used to confirm thepresence of PVNS (14,32,56). However, advances in MRI imaginghave made it much easier to detect the disorder (9,12,27). The MRIfeatures include joint effusion, low signal on both T1 and T2 dueto hemosiderin deposition, synovitis and bony erosions. Hemo-siderin deposits, appearing as a low signal area best seen on fastfield echo sequence, is considered to be diagnostic for PVNS (9).
The goal in treating this disorder is to provide symptomatic re-lief by debulking as much synovium as possible, prevent recurrentdisease and minimize the likelihood of osteoarthritis. Unfortunate-ly, advanced cartilage loss may already be present at the time of di-agnosis, making joint replacement arthroplasty the only viable op-tion. If cartilage loss is not excessive, the decision is betweenarthroscopic debridement and an arthrotomy, with or without sur-gical dislocation.
Gitelis published a literature review meta-analysis of 64 cases.Patients were treated with synovectomy alone via arthrotomy orwith a prosthetic replacement. The recurrence rate was 22% withsynovectomy alone versus 3.5% following total hip replace-ment (19).
Della Valle performed a meta-analysis using 7 new patientsalong with 117 cases culled from papers published between 1944and 1998. Of these, 62 cases did not have sufficient documenta-tion leaving 55 in the study. Half the cases had synovectomy alonewith only 6 of 26 having a full surgical dislocation. The other halfhad either synovectomy with hip replacement or synovectomywith hip fusion. Of those undergone synovectomy alone, the re-currence rate was 28% for grade 1 or 2 disease but 50% for grade3 disease. In contrast, only 4% undergoing total hip replacementhad recurrent disease (24).
Schwartz reported on 20 patients treated with a 0% recur-rence rate using an open technique (53). Flipo reported on 58 cas-es with a 12% recurrence rate (16). Vastel reported one of the on-ly long-term studies in the treatment of this disorder. Sixteen pa-tients underwent complete synovectomy with a surgical disloca-tion. Eight patients had synovectomy alone while eight patientshad some type of arthroplasty. The mean followup was 16.7 years
150
Chapter 10
Figure 2a
Synovial Chondromatosis: Antero-posterior viewof a right hip showing multiple loose bodies. Itwas elected to proceed with a surgical dislocationin an effort to provide a cure for the condition.
Figure 2b
Surgical Dislocation: This approach makes it pos-sible to remove all the loose bodies and performan extensive synovectomy.
Figure 2c
Antero-posterior view of a right hip. The loosebodies have all been removed, the trochantericslide osteotomy fixed with screws.

with only one patient followed for less than eight years. Only onepatient had recurrent disease, detected 14 years after cup arthro-plasty. All eight patients treated with synovectomy alone went onto develop secondary osteoarthritis with four of them requiring to-tal hip replacement (62).
Virtually all series of reported cases have involved open treat-ment. There are very few cases reported with arthroscopic tech-nique and no large series. Sim (56), Dorfman (14), Krebs (37),Janssens (32) and Godde (22) have all reported that arthroscopy canbe helpful in treating PVNS of the hip. Arthroscopic treatment ofthis disorder is similar to that of synovial chondromatosis. Thegoal of surgery is to confirm the diagnosis, assess the degree ofdamage and debride as much synovium as possible to providesymptomatic relief and to minimize the chance of recurrence. Thesurgical technique is similar to that outlined above for synovialchondromatosis, keeping in mind that the diffuse form is muchmore difficult to treat because of the extensive distribution withinthe joint. Also, a complete synovectomy is virtually impossiblewhen done arthroscopically. While arthroscopy is less invasive, ifthe cartilage is still viable it may be worth considering an arthro-tomy to enhance the chance of a cure. If it is known in advancethat the nodular form exists, then an arthroscopic debridementshould certainly be attempted first. The authors have been able toeradicate one nodular tumor arthroscopically while another pa-tient required arthrotomy for residual PVNS after an attemptedarthroscopic debridement (Figs. 3a-3e).
Rheumatologic Disorders
These disorders differ from synovial chondromatosis andPVNS in that the initiation of synovial proliferation seems to bedue to an external systemic trigger. They are similar in that thesynovitis releases enzymes and creates inflammation leading topain, swelling and ultimately destruction of the articular cartilage.These conditions include, but are not limited to: rheumatoidarthritis, juvenile rheumatoid arthritis, ankylosing spondylitis, pso-riatic arthritis and lupus. Agents that block tumor necrosis factorsuch as etanercept, adalimumab and infliximab have extended thearmamentarium of DMARDS’s (disease modifying antirheumaticdrugs), reducing the severity of joint involvement.
For years, open synovectomy has been advocated for rheuma-toid arthritis and JRA in a variety of joints when medical treat-ment alone is not sufficient and joint destruction has not pro-gressed to the point where arthroplasty or fusion is the only re-maining option. Very few reports are available on the efficacy ofhip arthroscopy in treating rheumatologic synovitis. Holgerssonreported on the use of hip arthroscopy in 13 patients with juvenilerheumatoid arthritis. While the study reported that it provided amore effective way to assess cartilage and to obtain histologic ma-terial, it was not effective in providing relief (26). As with diffusePVNS or synovial chondromatosis, it may be preferable to per-
151
Synovial and chondral disease: the role of hip arthroscopy
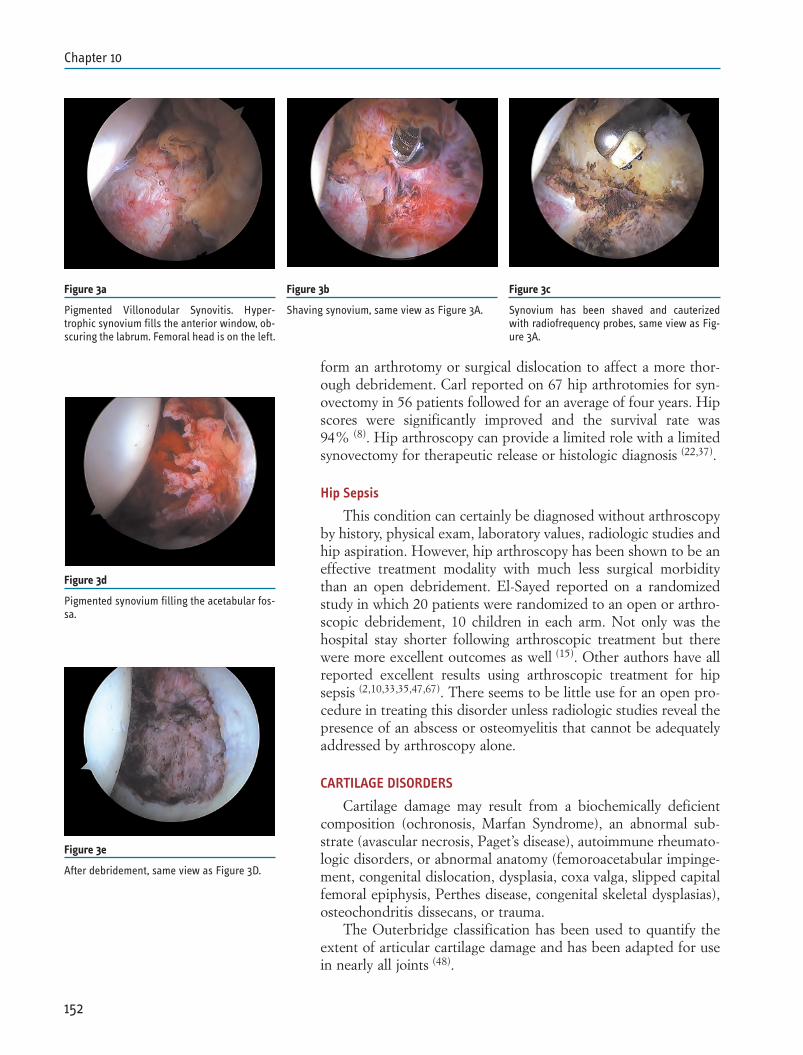
form an arthrotomy or surgical dislocation to affect a more thor-ough debridement. Carl reported on 67 hip arthrotomies for syn-ovectomy in 56 patients followed for an average of four years. Hipscores were significantly improved and the survival rate was94% (8). Hip arthroscopy can provide a limited role with a limitedsynovectomy for therapeutic release or histologic diagnosis (22,37).
Hip Sepsis
This condition can certainly be diagnosed without arthroscopyby history, physical exam, laboratory values, radiologic studies andhip aspiration. However, hip arthroscopy has been shown to be aneffective treatment modality with much less surgical morbiditythan an open debridement. El-Sayed reported on a randomizedstudy in which 20 patients were randomized to an open or arthro-scopic debridement, 10 children in each arm. Not only was thehospital stay shorter following arthroscopic treatment but therewere more excellent outcomes as well (15). Other authors have allreported excellent results using arthroscopic treatment for hipsepsis (2,10,33,35,47,67). There seems to be little use for an open pro-cedure in treating this disorder unless radiologic studies reveal thepresence of an abscess or osteomyelitis that cannot be adequatelyaddressed by arthroscopy alone.
CARTILAGE DISORDERS
Cartilage damage may result from a biochemically deficientcomposition (ochronosis, Marfan Syndrome), an abnormal sub-strate (avascular necrosis, Paget’s disease), autoimmune rheumato-logic disorders, or abnormal anatomy (femoroacetabular impinge-ment, congenital dislocation, dysplasia, coxa valga, slipped capitalfemoral epiphysis, Perthes disease, congenital skeletal dysplasias),osteochondritis dissecans, or trauma.
The Outerbridge classification has been used to quantify theextent of articular cartilage damage and has been adapted for usein nearly all joints (48).
152
Chapter 10
Figure 3a
Pigmented Villonodular Synovitis. Hyper-trophic synovium fills the anterior window, ob-scuring the labrum. Femoral head is on the left.
Figure 3b
Shaving synovium, same view as Figure 3A.
Figure 3c
Synovium has been shaved and cauterizedwith radiofrequency probes, same view as Fig-ure 3A.
Figure 3d
Pigmented synovium filling the acetabular fos-sa.
Figure 3e
After debridement, same view as Figure 3D.
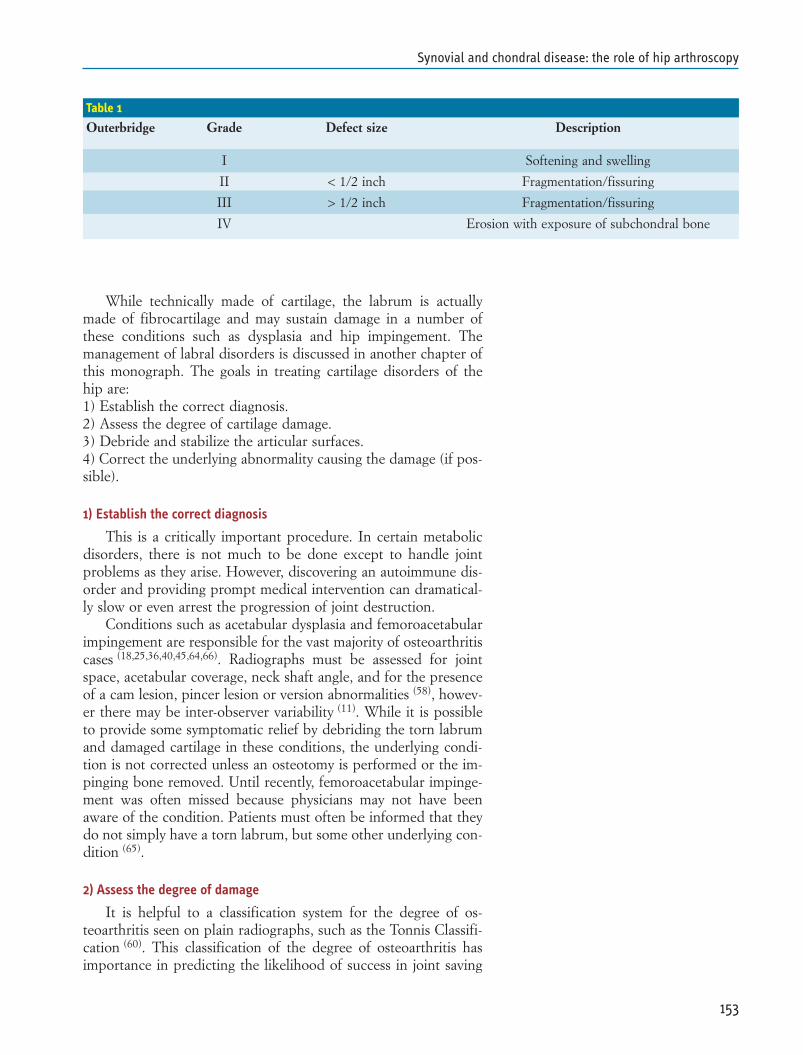
While technically made of cartilage, the labrum is actuallymade of fibrocartilage and may sustain damage in a number ofthese conditions such as dysplasia and hip impingement. Themanagement of labral disorders is discussed in another chapter ofthis monograph. The goals in treating cartilage disorders of thehip are:1) Establish the correct diagnosis.2) Assess the degree of cartilage damage.3) Debride and stabilize the articular surfaces.4) Correct the underlying abnormality causing the damage (if pos-sible).
1) Establish the correct diagnosis
This is a critically important procedure. In certain metabolicdisorders, there is not much to be done except to handle jointproblems as they arise. However, discovering an autoimmune dis-order and providing prompt medical intervention can dramatical-ly slow or even arrest the progression of joint destruction.
Conditions such as acetabular dysplasia and femoroacetabularimpingement are responsible for the vast majority of osteoarthritiscases (18,25,36,40,45,64,66). Radiographs must be assessed for jointspace, acetabular coverage, neck shaft angle, and for the presenceof a cam lesion, pincer lesion or version abnormalities (58), howev-er there may be inter-observer variability (11). While it is possibleto provide some symptomatic relief by debriding the torn labrumand damaged cartilage in these conditions, the underlying condi-tion is not corrected unless an osteotomy is performed or the im-pinging bone removed. Until recently, femoroacetabular impinge-ment was often missed because physicians may not have beenaware of the condition. Patients must often be informed that theydo not simply have a torn labrum, but some other underlying con-dition (65).
2) Assess the degree of damage
It is helpful to a classification system for the degree of os-teoarthritis seen on plain radiographs, such as the Tonnis Classifi-cation (60). This classification of the degree of osteoarthritis hasimportance in predicting the likelihood of success in joint saving
153
Synovial and chondral disease: the role of hip arthroscopy
Table 1
Outerbridge Grade Defect size Description
I Softening and swelling
II < 1/2 inch Fragmentation/fissuring
III > 1/2 inch Fragmentation/fissuring
IV Erosion with exposure of subchondral bone

operations (61,63). Improvements in MRI scan resolution has vastlyimproved the ability to predict the degree of articular cartilagedamage present, even before performing arthroscopy (30,31,44,48).
At surgery, it is important to document the location of articu-lar cartilage damage on the head and socket, the degree of degen-eration and the size of the defect. The location of the damage hasusually been expressed in terms of a clock face (50). A six zonemapping system has been proposed in an effort to standardize thelocation of cartilage defects (28). Even with high-resolution scan-ning, there may even more damage than suspected. The authorshave encountered numerous cases where the cartilage damage wasthought to be grade 2 or grade 3 based on the MRI scan, but in-stead there was full thickness delamination. This is most oftenseen in cam impingement. Pincer impingement usually lead tomore direct damage to the labrum (55).
3) Debride and stabilize the articular surfaces
As in any joint, the goal of surgical treatment is to preserve asmuch articular cartilage as possible. This is done by debriding anyunstable cartilage flaps back to a stable edge. Loose bodies,whether they are generated from neoplasia, trauma or a degenera-tive process must be removed. If deemed appropriate, a microfrac-ture can be performed in an effort to regenerate fibrocartilage inthe defect, as has been done in other joints, such as the knee (57).(Figure) In a study by Philippon, nine patients underwent revisionarthroscopy following a previous microfracture at an average of 20months followup. Eight of the nine patients had a successful out-come; with grade 1 or 2 fibrocartilage seen at surgery with a fill per-centage averaging 91% (25-100%) while one patient underwent to-tal hip replacement (49). The authors have performed a microfrac-ture in 94% of cases treated arthroscopically for cam impingementthat had grade 4 cartilage lesions. Grade 4 lesions had the strongestpredictive effect upon outcome, but even when present, good orexcellent results were possible in over 50% of cases (4). Anecdotal-ly, investigators at various hip arthroscopy meetings have presentedinstances where repairs with fibrin glue, autogenous cartilage graft-ing and osteochondral plug grafting have been presented, but thereis as yet no scientific papers on the subject. If there has been an os-teochondral fracture, open reduction and internal fixation shouldbe performed because there is a better opportunity restore the ar-ticular cartilage than there is with an injury that shears off articularcartilage alone. (Figure) It may be acceptable to simply remove anosteochondral fragment if it is very small or does not involve the su-perior weightbearing portion of the femoral head, such as a Pipkintype I fracture.
Hip arthroscopy has been shown to be beneficial in debridingthe cartilage defects found in Perthe’s disease (51). Byrd found themost improvement at ten-year followup in the treatment of loosebodies and traumatic cartilage defects. In contrast, the resultswere often less than favorable when treating osteoarthritis, 79%
154
Chapter 10
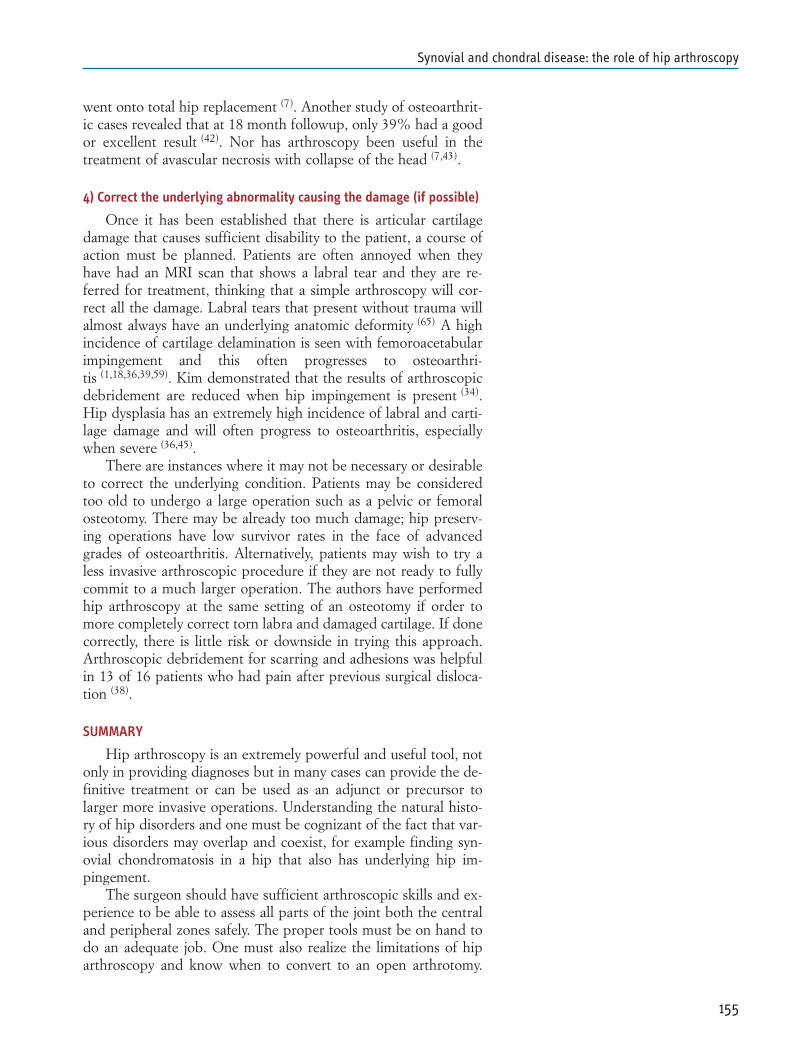
went onto total hip replacement (7). Another study of osteoarthrit-ic cases revealed that at 18 month followup, only 39% had a goodor excellent result (42). Nor has arthroscopy been useful in thetreatment of avascular necrosis with collapse of the head (7,43).
4) Correct the underlying abnormality causing the damage (if possible)
Once it has been established that there is articular cartilagedamage that causes sufficient disability to the patient, a course ofaction must be planned. Patients are often annoyed when theyhave had an MRI scan that shows a labral tear and they are re-ferred for treatment, thinking that a simple arthroscopy will cor-rect all the damage. Labral tears that present without trauma willalmost always have an underlying anatomic deformity (65) A highincidence of cartilage delamination is seen with femoroacetabularimpingement and this often progresses to osteoarthri-tis (1,18,36,39,59). Kim demonstrated that the results of arthroscopicdebridement are reduced when hip impingement is present (34).Hip dysplasia has an extremely high incidence of labral and carti-lage damage and will often progress to osteoarthritis, especiallywhen severe (36,45).
There are instances where it may not be necessary or desirableto correct the underlying condition. Patients may be consideredtoo old to undergo a large operation such as a pelvic or femoralosteotomy. There may be already too much damage; hip preserv-ing operations have low survivor rates in the face of advancedgrades of osteoarthritis. Alternatively, patients may wish to try aless invasive arthroscopic procedure if they are not ready to fullycommit to a much larger operation. The authors have performedhip arthroscopy at the same setting of an osteotomy if order tomore completely correct torn labra and damaged cartilage. If donecorrectly, there is little risk or downside in trying this approach.Arthroscopic debridement for scarring and adhesions was helpfulin 13 of 16 patients who had pain after previous surgical disloca-tion (38).
SUMMARY
Hip arthroscopy is an extremely powerful and useful tool, notonly in providing diagnoses but in many cases can provide the de-finitive treatment or can be used as an adjunct or precursor tolarger more invasive operations. Understanding the natural histo-ry of hip disorders and one must be cognizant of the fact that var-ious disorders may overlap and coexist, for example finding syn-ovial chondromatosis in a hip that also has underlying hip im-pingement.
The surgeon should have sufficient arthroscopic skills and ex-perience to be able to assess all parts of the joint both the centraland peripheral zones safely. The proper tools must be on hand todo an adequate job. One must also realize the limitations of hiparthroscopy and know when to convert to an open arthrotomy.
155
Synovial and chondral disease: the role of hip arthroscopy

For example, it may be foolish to attempt an arthroscopic de-bridement in a hip pressure packed with large loose bodies. Oneshould not miss the opportunity to perform an open reductionand internal fixation of osteochondral fractures when appropriate.Do take the opportunity to definitively correct all underlying ab-normalities, especially in younger patients. Doing so may preventosteoarthritis that would otherwise be inevitable. Do not overlookthe possibility of inflammatory arthritis, which may have a subtle,insidious onset and be mistaken for other conditions. The tech-niques used in hip arthroscopy are evolving rapidly and the proce-dure has become firmly entrenched in the surgical treatment repi-toire of hip disorders.
156
Chapter 10
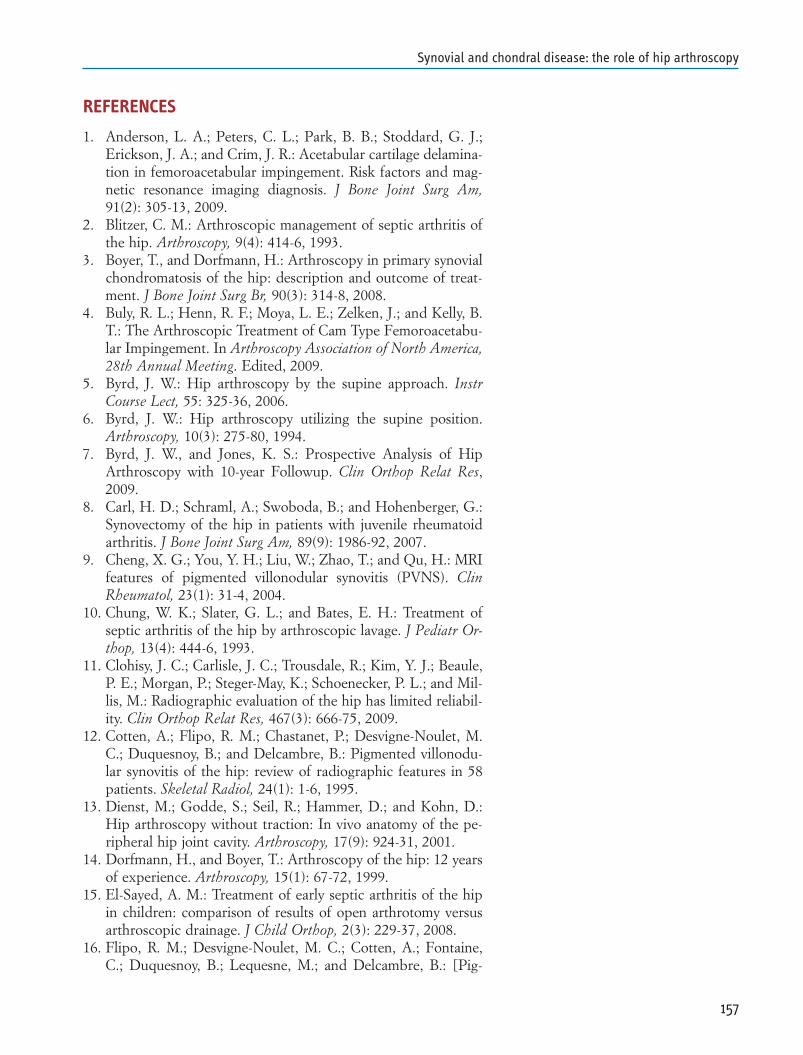
REFERENCES
1. Anderson, L. A.; Peters, C. L.; Park, B. B.; Stoddard, G. J.;Erickson, J. A.; and Crim, J. R.: Acetabular cartilage delamina-tion in femoroacetabular impingement. Risk factors and mag-netic resonance imaging diagnosis. J Bone Joint Surg Am,91(2): 305-13, 2009.
2. Blitzer, C. M.: Arthroscopic management of septic arthritis ofthe hip. Arthroscopy, 9(4): 414-6, 1993.
3. Boyer, T., and Dorfmann, H.: Arthroscopy in primary synovialchondromatosis of the hip: description and outcome of treat-ment. J Bone Joint Surg Br, 90(3): 314-8, 2008.
4. Buly, R. L.; Henn, R. F.; Moya, L. E.; Zelken, J.; and Kelly, B.T.: The Arthroscopic Treatment of Cam Type Femoroacetabu-lar Impingement. In Arthroscopy Association of North America,28th Annual Meeting. Edited, 2009.
5. Byrd, J. W.: Hip arthroscopy by the supine approach. InstrCourse Lect, 55: 325-36, 2006.
6. Byrd, J. W.: Hip arthroscopy utilizing the supine position.Arthroscopy, 10(3): 275-80, 1994.
7. Byrd, J. W., and Jones, K. S.: Prospective Analysis of HipArthroscopy with 10-year Followup. Clin Orthop Relat Res,2009.
8. Carl, H. D.; Schraml, A.; Swoboda, B.; and Hohenberger, G.:Synovectomy of the hip in patients with juvenile rheumatoidarthritis. J Bone Joint Surg Am, 89(9): 1986-92, 2007.
9. Cheng, X. G.; You, Y. H.; Liu, W.; Zhao, T.; and Qu, H.: MRIfeatures of pigmented villonodular synovitis (PVNS). ClinRheumatol, 23(1): 31-4, 2004.
10. Chung, W. K.; Slater, G. L.; and Bates, E. H.: Treatment ofseptic arthritis of the hip by arthroscopic lavage. J Pediatr Or-thop, 13(4): 444-6, 1993.
11. Clohisy, J. C.; Carlisle, J. C.; Trousdale, R.; Kim, Y. J.; Beaule,P. E.; Morgan, P.; Steger-May, K.; Schoenecker, P. L.; and Mil-lis, M.: Radiographic evaluation of the hip has limited reliabil-ity. Clin Orthop Relat Res, 467(3): 666-75, 2009.
12. Cotten, A.; Flipo, R. M.; Chastanet, P.; Desvigne-Noulet, M.C.; Duquesnoy, B.; and Delcambre, B.: Pigmented villonodu-lar synovitis of the hip: review of radiographic features in 58patients. Skeletal Radiol, 24(1): 1-6, 1995.
13. Dienst, M.; Godde, S.; Seil, R.; Hammer, D.; and Kohn, D.:Hip arthroscopy without traction: In vivo anatomy of the pe-ripheral hip joint cavity. Arthroscopy, 17(9): 924-31, 2001.
14. Dorfmann, H., and Boyer, T.: Arthroscopy of the hip: 12 yearsof experience. Arthroscopy, 15(1): 67-72, 1999.
15. El-Sayed, A. M.: Treatment of early septic arthritis of the hipin children: comparison of results of open arthrotomy versusarthroscopic drainage. J Child Orthop, 2(3): 229-37, 2008.
16. Flipo, R. M.; Desvigne-Noulet, M. C.; Cotten, A.; Fontaine,C.; Duquesnoy, B.; Lequesne, M.; and Delcambre, B.: [Pig-
157
Synovial and chondral disease: the role of hip arthroscopy
mented villonodular synovitis of the hip. Results of a nationalsurvey apropos of 58 cases]. Rev Rhum Ed Fr, 61(2): 85-95,1994.
17. Ganz, R.; Gill, T. J.; Gautier, E.; Ganz, K.; Krugel, N.; andBerlemann, U.: Surgical dislocation of the adult hip a tech-nique with full access to the femoral head and acetabulumwithout the risk of avascular necrosis. J Bone Joint Surg Br,83(8): 1119-24, 2001.
18. Ganz, R.; Parvizi, J.; Beck, M.; Leunig, M.; Notzli, H.; andSiebenrock, K. A.: Femoroacetabular impingement: a causefor osteoarthritis of the hip. Clin Orthop, (417): 112-20, 2003.
19. Gitelis, S.; Heligman, D.; and Morton, T.: The treatment ofpigmented villonodular synovitis of the hip. A case report andliterature review. Clin Orthop Relat Res, (239): 154-60, 1989.
20. Glick, J. M.: Hip arthroscopy by the lateral approach. InstrCourse Lect, 55: 317-23, 2006.
21. Glick, J. M.; Sampson, T. G.; Gordon, R. B.; Behr, J. T.; andSchmidt, E.: Hip arthroscopy by the lateral approach.Arthroscopy, 3(1): 4-12, 1987.
22. Godde, S.; Kusma, M.; and Dienst, M.: [Synovial disordersand loose bodies in the hip joint. Arthroscopic diagnostics andtreatment]. Orthopade, 35(1): 67-76, 2006.
23. Gondolph-Zink, B.; Puhl, W.; and Noack, W.: Semiarthro-scopic synovectomy of the hip. Int Orthop, 12(1): 31-5, 1988.
24. Gonzalez Della Valle, A.; Piccaluga, F.; Potter, H. G.; Salvati,E. A.; and Pusso, R.: Pigmented villonodular synovitis of thehip: 2- to 23-year followup study. Clin Orthop Relat Res, (388):187-99, 2001.
25. Goodman, D. A.; Feighan, J. E.; Smith, A. D.; Latimer, B.; Bu-ly, R. L.; and Cooperman, D. R.: Subclinical slipped capitalfemoral epiphysis. Relationship to osteoarthrosis of the hip. JBone Joint Surg Am, 79(10): 1489-97, 1997.
26. Holgersson, S.; Brattstrom, H.; Mogensen, B.; and Lidgren,L.: Arthroscopy of the hip in juvenile chronic arthritis. J Pedi-atr Orthop, 1(3): 273-8, 1981.
27. Hughes, T. H.; Sartoris, D. J.; Schweitzer, M. E.; and Resnick,D. L.: Pigmented villonodular synovitis: MRI characteristics.Skeletal Radiol, 24(1): 7-12, 1995.
28. Ilizaliturri, V. M., Jr. et al.: A geographic zone method to de-scribe intra-articular pathology in hip arthroscopy: cadavericstudy and preliminary report. Arthroscopy, 24(5): 534-9, 2008.
29. Jaffe, H. L.; Lichtenstein, L.; and Sutro, C. J.: Pigmented vil-lonodular synovitis, bursitis and tenosynovitis. A discussion ofthe synovial and bursal equivalents of the tenosynovial lesioncommonly denoted as xanthoma, xanthogranulosoma, giantcell tumor or myeloplaxoma of the tendon sheath, with someconsideration of this tendon sheath lesion itself. Arch Pathol.,31: 731-765, 1941.
30. James, S.; Miocevic, M.; Malara, F.; Pike, J.; Young, D.; and
158
Chapter 10
Connell, D.: MR imaging findings of acetabular dysplasia inadults. Skeletal Radiol, 35(6): 378-84, 2006.
31. James, S. L.; Ali, K.; Malara, F.; Young, D.; O’Donnell, J.; andConnell, D. A.: MRI findings of femoroacetabular impinge-ment. AJR Am J Roentgenol, 187(6): 1412-9, 2006.
32. Janssens, X.; Van Meirhaeghe, J.; Verdonk, R.; Verjans, P.; Cu-velier, C.; and Veys, E. M.: Diagnostic arthroscopy of the hipjoint in pigmented villonodular synovitis. Arthroscopy, 3(4):283-7, 1987.
33. Kaminski, A.; Muhr, G.; and Kutscha-Lissberg, F.: Modifiedopen arthroscopy in the treatment of septic arthritis of the hip.Ortop Traumatol Rehabil, 9(6): 599-603, 2007.
34. Kim, K. C.; Hwang, D. S.; Lee, C. H.; and Kwon, S. T.: Influ-ence of femoroacetabular impingement on results of hiparthroscopy in patients with early osteoarthritis. Clin OrthopRelat Res, 456: 128-32, 2007.
35. Kim, S. J.; Choi, N. H.; Ko, S. H.; Linton, J. A.; and Park, H.W.: Arthroscopic treatment of septic arthritis of the hip. ClinOrthop Relat Res, (407): 211-4, 2003.
36. Kim, Y. J.; Ganz, R.; Murphy, S. B.; Buly, R. L.; and Millis, M.B.: Hip joint-preserving surgery: beyond the classic osteotomy.Instr Course Lect, 55: 145-58, 2006.
37. Krebs, V. E.: The role of hip arthroscopy in the treatment ofsynovial disorders and loose bodies. Clin Orthop Relat Res,(406): 48-59, 2003.
38. Krueger, A.; Leunig, M.; Siebenrock, K. A.; and Beck, M.: Hiparthroscopy after previous surgical hip dislocation forfemoroacetabular impingement. Arthroscopy, 23(12): 1285-1289 e1, 2007.
39. Leunig, M.; Beaule, P. E.; and Ganz, R.: The concept offemoroacetabular impingement: current status and future per-spectives. Clin Orthop Relat Res, 467(3): 616-22, 2009.
40. Leunig, M.; Parvizi, J.; and Ganz, R.: Nonarthroplasty surgicaltreatment of hip osteoarthritis. Instr Course Lect, 55: 159-66,2006.
41. Lim, S. J.; Chung, H. W.; Choi, Y. L.; Moon, Y. W.; Seo, J. G.;and Park, Y. S.: Operative treatment of primary synovial os-teochondromatosis of the hip. J Bone Joint Surg Am, 88(11):2456-64, 2006.
42. Margheritini, F., and Villar, R. N.: The efficacy of arthroscopyin the treatment of hip osteoarthritis. Chir Organi Mov, 84(3):257-61, 1999.
43. McCarthy, J. C.: Hip arthroscopy: when it is and when it is notindicated. Instr Course Lect, 53: 615-21, 2004.
44. Mintz, D. N.; Hooper, T.; Connell, D.; Buly, R.; Padgett, D. E.;and Potter, H. G.: Magnetic resonance imaging of the hip: de-tection of labral and chondral abnormalities using noncontrastimaging. Arthroscopy, 21(4): 385-93, 2005.
45. Murphy, S. B.; Ganz, R.; and Muller, M. E.: The prognosis inuntreated dysplasia of the hip. A study of radiographic factors
159
Synovial and chondral disease: the role of hip arthroscopy
that predict the outcome. J Bone Joint Surg Am, 77(7): 985-9,1995.
46. Myers, B. W., and Masi, A. T.: Pigmented villonodular synovi-tis and tenosynovitis: a clinical epidemiologic study of 166 cas-es and literature review. Medicine (Baltimore), 59: 223-238,1980.
47. Nusem, I.; Jabur, M. K.; and Playford, E. G.: Arthroscopictreatment of septic arthritis of the hip. Arthroscopy, 22(8): 902e1-3, 2006.
48. Outerbridge, R. E.: The etiology of chondromalacia patellae. JBone Joint Surg Br, 43-B: 752-7, 1961.
49. Philippon, M. J.; Schenker, M. L.; Briggs, K. K.; and Maxwell,R. B.: Can microfracture produce repair tissue in acetabularchondral defects? Arthroscopy, 24(1): 46-50, 2008.
50. Philippon, M. J.; Stubbs, A. J.; Schenker, M. L.; Maxwell, R.B.; Ganz, R.; and Leunig, M.: Arthroscopic management offemoroacetabular impingement: osteoplasty technique and lit-erature review. Am J Sports Med, 35(9): 1571-80, 2007.
51. Roy, D. R.: Arthroscopic findings of the hip in new onset hippain in adolescents with previous Legg-Calve-Perthes disease.J Pediatr Orthop B, 14(3): 151-5, 2005.
52. Schoeniger, R.; Naudie, D. D.; Siebenrock, K. A.; Trousdale,R. T.; and Ganz, R.: Modified complete synovectomy preventsrecurrence in synovial chondromatosis of the hip. Clin OrthopRelat Res, 451: 195-200, 2006.
53. Schwartz, H. S.; Unni, K. K.; and Pritchard, D. J.: Pigmentedvillonodular synovitis. A retrospective review of affected largejoints. Clin Orthop Relat Res, (247): 243-55, 1989.
54. Sekiya, J. K.; Wojtys, E. M.; Loder, R. T.; and Hensinger, R.N.: Hip arthroscopy using a limited anterior exposure: an al-ternative approach for arthroscopic access. Arthroscopy, 16(1):16-20, 2000.
55. Siebenrock, K. A.; Schoeniger, R.; and Ganz, R.: Anteriorfemoro-acetabular impingement due to acetabular retrover-sion. Treatment with periacetabular osteotomy. J Bone JointSurg Am, 85-A(2): 278-86, 2003.
56. Sim, F. H.: Synovial proliferative disorders: role of synovecto-my. Arthroscopy, 1(3): 198-204, 1985.
57. Steadman, J. R.; Briggs, K. K.; Rodrigo, J. J.; Kocher, M. S.;Gill, T. J.; and Rodkey, W. G.: Outcomes of microfracture fortraumatic chondral defects of the knee: average 11-year fol-low-up. Arthroscopy, 19(5): 477-84, 2003.
58. Tannast, M.; Kubiak-Langer, M.; Langlotz, F.; Puls, M.; Mur-phy, S. B.; and Siebenrock, K. A.: Noninvasive three-dimen-sional assessment of femoroacetabular impingement. J OrthopRes, 25(1): 122-31, 2007.
59. Tanzer, M., and Noiseux, N.: Osseous abnormalities and earlyosteoarthritis: the role of hip impingement. Clin Orthop RelatRes, (429): 170-7, 2004.
60. Tonnis, D.: Congenital Dysplasia and Dislocation of the Hip
160
Chapter 10
in Children and Adults. Edited, 121-3, Berlin, Springer-Verlag,1987.
61. Trousdale, R. T.; Ekkernkamp, A.; Ganz, R.; and Wallrichs, S.L.: Periacetabular and intertrochanteric osteotomy for thetreatment of osteoarthrosis in dysplastic hips. J Bone Joint SurgAm, 77(1): 73-85, 1995.
62. Vastel, L.; Lambert, P.; De Pinieux, G.; Charrois, O.; Ker-boull, M.; and Courpied, J. P.: Surgical treatment of pigment-ed villonodular synovitis of the hip. J Bone Joint Surg Am,87(5): 1019-24, 2005.
63. Voos, J. E.; Ranawat, A. S.; Pellicci, P. M.; Buly, R. L.; and Sal-vati, E. A.: Varus rotational osteotomies for adults with hipdysplasia: a 20-year followup. Clin Orthop Relat Res, 457: 138-43, 2007.
64. Wagner, S.; Hofstetter, W.; Chiquet, M.; Mainil-Varlet, P.;Stauffer, E.; Ganz, R.; and Siebenrock, K. A.: Early os-teoarthritic changes of human femoral head cartilage subse-quent to femoro-acetabular impingement. Osteoarthritis Carti-lage, 11(7): 508-18, 2003.
65. Wenger, D. E.; Kendell, K. R.; Miner, M. R.; and Trousdale, R.T.: Acetabular labral tears rarely occur in the absence of bonyabnormalities. Clin Orthop, (426): 145-50, 2004.
66. Wenger, D. R., and Bomar, J. D.: Human hip dysplasia: evolu-tion of current treatment concepts. J Orthop Sci, 8(2): 264-71,2003.
67. Yamamoto, Y.; Ide, T.; Hachisuka, N.; Maekawa, S.; and Aka-matsu, N.: Arthroscopic surgery for septic arthritis of the hipjoint in 4 adults. Arthroscopy, 17(3): 290-297, 2001.
161
Synovial and chondral disease: the role of hip arthroscopy


ANATOMY
The acetabular labrum is a triangular shaped fibrocartilagesimilar to those found in other joints of our body (1). It surroundsthe bony part of the acetabulum getting a C shape and it extends,to complete the ring that surrounds the acetabulum, with thetransverse ligament (Fig. 1). This is a ligamentous structure thatbridges over the lower rim of the cotyloid fossa (Fig. 2). It rarelyhappens that the acetabular labrum does not extend to the trans-verse ligament but it ends on the acetabular rim just like withmenisci on the tibial plateau.
This is a rare case but it is neither pathological nor combinedwith any symptomatology. With its presence it contributes to thearticular stability, increasing the joint surface by 22% and by 33%in volume of the cotyloid fossa (2).
Labrum has an average width of 5,3 mm (range 3-12 mm). Itis tendentially thicker anteriorly and superiorly and less thick at itsposterior portion (1).Thickness and dimensions are increasedwhen dysplasia occurs, particularly in those cases with initial prox-imal subluxation of the femural head.
In such cases, the labrum role changes, getting a support andretention function to limit the lateral and proximal migration ofthe femoral head (3).
The different function and morphology of the labrum in thehip dysplasia must be carefully evaluated in case of a labrum tear.
In these patients, an extensive labral ablation may unstabilizea poorly balanced complex, increasing chances of proximal migra-tion of the femural head (3,4).
Under histologic analysis, the normal acetabular labrum isclosely adherent to the acetabular bone, with a 1-2 mm transitionzone rich of collagen and calcified cartilage (2).
The acetabular labrum is mainly lacking in vascularization andfed only by synovial liquid. However, likewise the meniscus, theglenoid labrum and the triangular fibrocartilage, the peripheralportion is microvascularized by the adjacent capsule.
163
Chapter 11ACETABULAR LABRUM TEARSNicola Santori
Figure 1a-b
A) Right hip MRI frontal scan. Labrum profile withits function of increasing acetabular concavity isevident. B) 70° scope arthroscopic vision of the ac-etabular labrum antero lateral portion
a)
b)
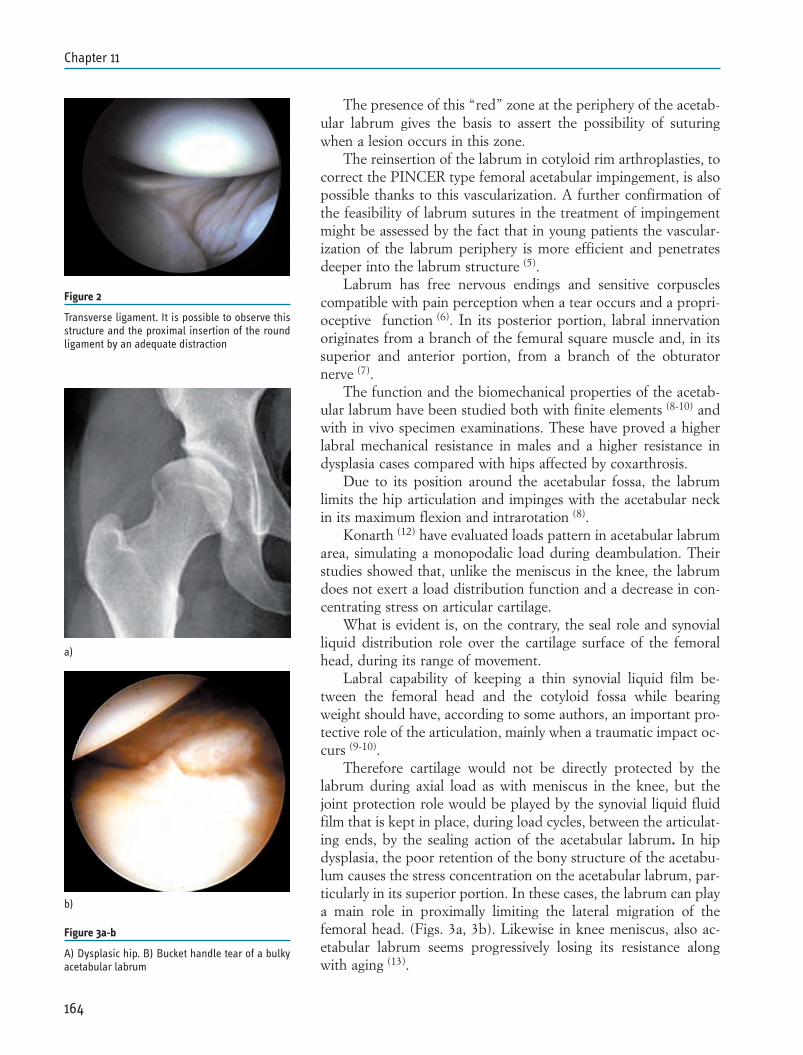
The presence of this “red” zone at the periphery of the acetab-ular labrum gives the basis to assert the possibility of suturingwhen a lesion occurs in this zone.
The reinsertion of the labrum in cotyloid rim arthroplasties, tocorrect the PINCER type femoral acetabular impingement, is alsopossible thanks to this vascularization. A further confirmation ofthe feasibility of labrum sutures in the treatment of impingementmight be assessed by the fact that in young patients the vascular-ization of the labrum periphery is more efficient and penetratesdeeper into the labrum structure (5).
Labrum has free nervous endings and sensitive corpusclescompatible with pain perception when a tear occurs and a propri-oceptive function (6). In its posterior portion, labral innervationoriginates from a branch of the femural square muscle and, in itssuperior and anterior portion, from a branch of the obturatornerve (7).
The function and the biomechanical properties of the acetab-ular labrum have been studied both with finite elements (8-10) andwith in vivo specimen examinations. These have proved a higherlabral mechanical resistance in males and a higher resistance indysplasia cases compared with hips affected by coxarthrosis.
Due to its position around the acetabular fossa, the labrumlimits the hip articulation and impinges with the acetabular neckin its maximum flexion and intrarotation (8).
Konarth (12) have evaluated loads pattern in acetabular labrumarea, simulating a monopodalic load during deambulation. Theirstudies showed that, unlike the meniscus in the knee, the labrumdoes not exert a load distribution function and a decrease in con-centrating stress on articular cartilage.
What is evident is, on the contrary, the seal role and synovialliquid distribution role over the cartilage surface of the femoralhead, during its range of movement.
Labral capability of keeping a thin synovial liquid film be-tween the femoral head and the cotyloid fossa while bearingweight should have, according to some authors, an important pro-tective role of the articulation, mainly when a traumatic impact oc-curs (9-10).
Therefore cartilage would not be directly protected by thelabrum during axial load as with meniscus in the knee, but thejoint protection role would be played by the synovial liquid fluidfilm that is kept in place, during load cycles, between the articulat-ing ends, by the sealing action of the acetabular labrum. In hipdysplasia, the poor retention of the bony structure of the acetabu-lum causes the stress concentration on the acetabular labrum, par-ticularly in its superior portion. In these cases, the labrum can playa main role in proximally limiting the lateral migration of thefemoral head. (Figs. 3a, 3b). Likewise in knee meniscus, also ac-etabular labrum seems progressively losing its resistance alongwith aging (13).
164
Chapter 11
Figure 2
Transverse ligament. It is possible to observe thisstructure and the proximal insertion of the roundligament by an adequate distraction
Figure 3a-b
A) Dysplasic hip. B) Bucket handle tear of a bulkyacetabular labrum
a)
b)
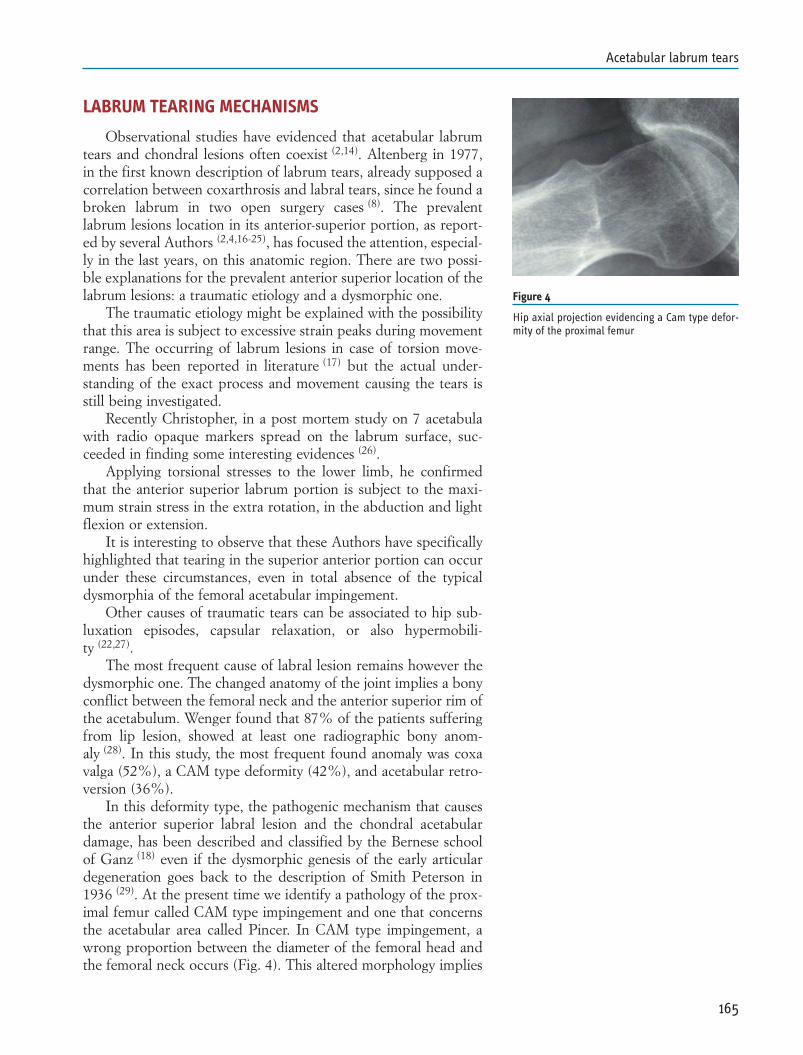
LABRUM TEARING MECHANISMS
Observational studies have evidenced that acetabular labrumtears and chondral lesions often coexist (2,14). Altenberg in 1977,in the first known description of labrum tears, already supposed acorrelation between coxarthrosis and labral tears, since he found abroken labrum in two open surgery cases (8). The prevalentlabrum lesions location in its anterior-superior portion, as report-ed by several Authors (2,4,16-25), has focused the attention, especial-ly in the last years, on this anatomic region. There are two possi-ble explanations for the prevalent anterior superior location of thelabrum lesions: a traumatic etiology and a dysmorphic one.
The traumatic etiology might be explained with the possibilitythat this area is subject to excessive strain peaks during movementrange. The occurring of labrum lesions in case of torsion move-ments has been reported in literature (17) but the actual under-standing of the exact process and movement causing the tears isstill being investigated.
Recently Christopher, in a post mortem study on 7 acetabulawith radio opaque markers spread on the labrum surface, suc-ceeded in finding some interesting evidences (26).
Applying torsional stresses to the lower limb, he confirmedthat the anterior superior labrum portion is subject to the maxi-mum strain stress in the extra rotation, in the abduction and lightflexion or extension.
It is interesting to observe that these Authors have specificallyhighlighted that tearing in the superior anterior portion can occurunder these circumstances, even in total absence of the typicaldysmorphia of the femoral acetabular impingement.
Other causes of traumatic tears can be associated to hip sub-luxation episodes, capsular relaxation, or also hypermobili-ty (22,27).
The most frequent cause of labral lesion remains however thedysmorphic one. The changed anatomy of the joint implies a bonyconflict between the femoral neck and the anterior superior rim ofthe acetabulum. Wenger found that 87% of the patients sufferingfrom lip lesion, showed at least one radiographic bony anom-aly (28). In this study, the most frequent found anomaly was coxavalga (52%), a CAM type deformity (42%), and acetabular retro-version (36%).
In this deformity type, the pathogenic mechanism that causesthe anterior superior labral lesion and the chondral acetabulardamage, has been described and classified by the Bernese schoolof Ganz (18) even if the dysmorphic genesis of the early articulardegeneration goes back to the description of Smith Peterson in1936 (29). At the present time we identify a pathology of the prox-imal femur called CAM type impingement and one that concernsthe acetabular area called Pincer. In CAM type impingement, awrong proportion between the diameter of the femoral head andthe femoral neck occurs (Fig. 4). This altered morphology implies
165
Acetabular labrum tears
Figure 4
Hip axial projection evidencing a Cam type defor-mity of the proximal femur
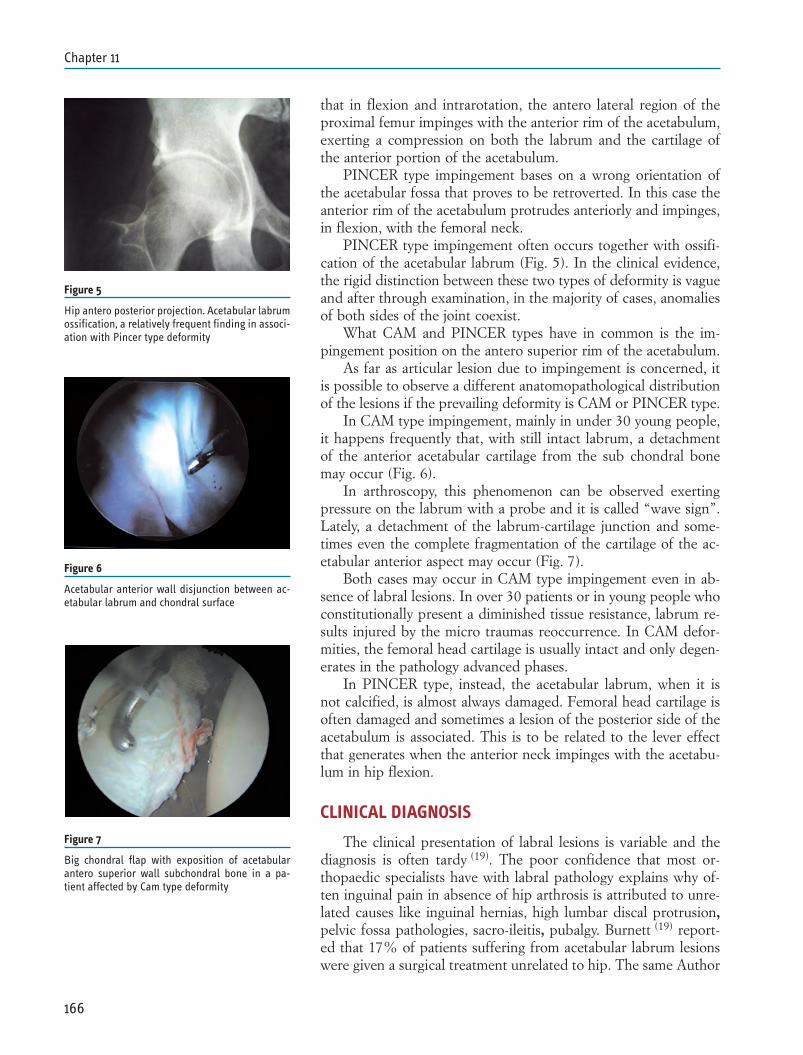
that in flexion and intrarotation, the antero lateral region of theproximal femur impinges with the anterior rim of the acetabulum,exerting a compression on both the labrum and the cartilage ofthe anterior portion of the acetabulum.
PINCER type impingement bases on a wrong orientation ofthe acetabular fossa that proves to be retroverted. In this case theanterior rim of the acetabulum protrudes anteriorly and impinges,in flexion, with the femoral neck.
PINCER type impingement often occurs together with ossifi-cation of the acetabular labrum (Fig. 5). In the clinical evidence,the rigid distinction between these two types of deformity is vagueand after through examination, in the majority of cases, anomaliesof both sides of the joint coexist.
What CAM and PINCER types have in common is the im-pingement position on the antero superior rim of the acetabulum.
As far as articular lesion due to impingement is concerned, itis possible to observe a different anatomopathological distributionof the lesions if the prevailing deformity is CAM or PINCER type.
In CAM type impingement, mainly in under 30 young people,it happens frequently that, with still intact labrum, a detachmentof the anterior acetabular cartilage from the sub chondral bonemay occur (Fig. 6).
In arthroscopy, this phenomenon can be observed exertingpressure on the labrum with a probe and it is called “wave sign”.Lately, a detachment of the labrum-cartilage junction and some-times even the complete fragmentation of the cartilage of the ac-etabular anterior aspect may occur (Fig. 7).
Both cases may occur in CAM type impingement even in ab-sence of labral lesions. In over 30 patients or in young people whoconstitutionally present a diminished tissue resistance, labrum re-sults injured by the micro traumas reoccurrence. In CAM defor-mities, the femoral head cartilage is usually intact and only degen-erates in the pathology advanced phases.
In PINCER type, instead, the acetabular labrum, when it isnot calcified, is almost always damaged. Femoral head cartilage isoften damaged and sometimes a lesion of the posterior side of theacetabulum is associated. This is to be related to the lever effectthat generates when the anterior neck impinges with the acetabu-lum in hip flexion.
CLINICAL DIAGNOSIS
The clinical presentation of labral lesions is variable and thediagnosis is often tardy (19). The poor confidence that most or-thopaedic specialists have with labral pathology explains why of-ten inguinal pain in absence of hip arthrosis is attributed to unre-lated causes like inguinal hernias, high lumbar discal protrusion,pelvic fossa pathologies, sacro-ileitis, pubalgy. Burnett (19) report-ed that 17% of patients suffering from acetabular labrum lesionswere given a surgical treatment unrelated to hip. The same Author
166
Chapter 11
Figure 5
Hip antero posterior projection. Acetabular labrumossification, a relatively frequent finding in associ-ation with Pincer type deformity
Figure 6
Acetabular anterior wall disjunction between ac-etabular labrum and chondral surface
Figure 7
Big chondral flap with exposition of acetabularantero superior wall subchondral bone in a pa-tient affected by Cam type deformity

proved that the average time for diagnosis, from the symptomatol-ogy occurrence is 21 months and that patients consult an averageof 3,3 specialists before obtaining a correct diagnosis.
Some of the diagnostic elements evidenced by the objectiveexamination and the clinic history are the following: inguinal painin the 92% of cases, hip lateral pain in the 59%, gluteal pain inthe 38%, weight bearing pain in the 91%, nocturnal pain in the71%, limp in 39%, positive Trendelemburg in 38% and positiveimpingement test in the 95%. Actually a large part of this sympto-matology is not specific at all for labral lesion but can be compat-ible with many intra-articular hip pathologies. Similar symptomsoccur especially in initial arthrosis and in those pathologies thatimply an articular effusion (loose body, chondromathosis, synovi-tis, round ligament tear etc). A symptom that, according to my ex-perience, is important to search for in the clinic history of labrumlesion, is acute pain in change of direction movements, in everydaylife or during sport activity. These patients do not have any symp-tomatology in everyday life but complain of this pain in sport ac-tivity.
An accurate objective examination enables to exclude withreasonable certainty extra articular causes for coxalgia. The im-pingement test, FADIR test, is performed with patient in a supineposition with a 90° hip flection and stressing in intra rotation andadduction. In “pure” labral lesions, there is no limit to intrarota-tion and adduction other than that driven by pain.
In labral pathology combined with impingement pain occurstogether with a “mechanical “ limitation of the intrarotation (Fig.8).
Impingement occurring between the anterior acetabulum rimand the head-neck junction jams the intrarotation and pushes thehip in extrarotation when flexion is over 90°. It is typical offemoral acetabular impingement to observe that suffering limb ex-trarotates while crouching (Fig. 9).
INSTRUMENTAL DIAGNOSIS
Instrumental diagnosis of labral lesions is not simple. Conven-tional MRI cannot be considered reliable because it is providedwith a good sensitivity but also with an unsatisfying specificity (20).
MRI with contrast media has been considered the golden stan-dard technique for instrumental diagnosis since Petersilge wrotehis article in 1996.
The outcomes obtained by this author have not been achievedby other studies and at the present time this methodology is con-sidered to have a sensitivity ranging between 63% and 94% and aspecificity ranging between 44% and 75% and with an accuracybetween 63% and 94% (31-34).
Labral lesions are classified in three types with arthro MRI,and are extended to 6 since each one can be divided into A and B,as proposed by Czerny in 1996 and still generally accepted (36).
167
Acetabular labrum tears
Figure 8
Femoral acetabular impingement test (FADIRtest). Intrarotation range lessening is associated topain. In traumatic labral lesions there is no in-trarotation range restriction
Figura 9
Impingment femoroacetabolare monolaterale Dx.Nell’eseguire lo squat l’anca di dx è forzata in ex-trarotazione.
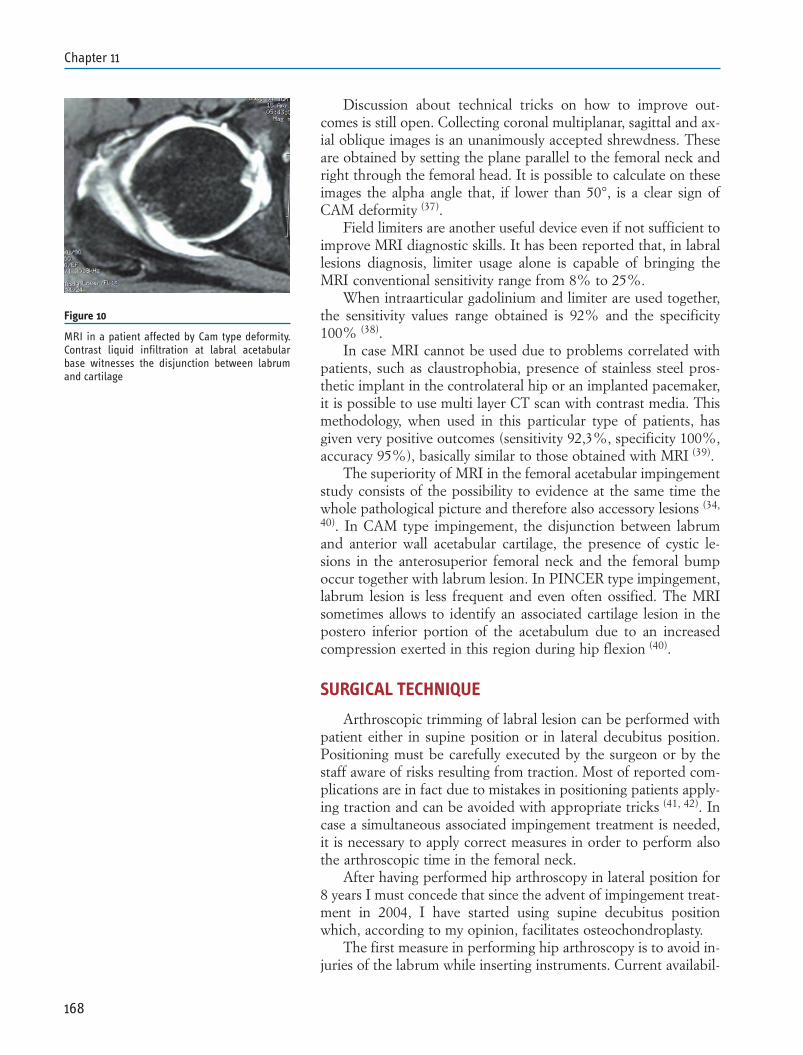
Discussion about technical tricks on how to improve out-comes is still open. Collecting coronal multiplanar, sagittal and ax-ial oblique images is an unanimously accepted shrewdness. Theseare obtained by setting the plane parallel to the femoral neck andright through the femoral head. It is possible to calculate on theseimages the alpha angle that, if lower than 50°, is a clear sign ofCAM deformity (37).
Field limiters are another useful device even if not sufficient toimprove MRI diagnostic skills. It has been reported that, in labrallesions diagnosis, limiter usage alone is capable of bringing theMRI conventional sensitivity range from 8% to 25%.
When intraarticular gadolinium and limiter are used together,the sensitivity values range obtained is 92% and the specificity100% (38).
In case MRI cannot be used due to problems correlated withpatients, such as claustrophobia, presence of stainless steel pros-thetic implant in the controlateral hip or an implanted pacemaker,it is possible to use multi layer CT scan with contrast media. Thismethodology, when used in this particular type of patients, hasgiven very positive outcomes (sensitivity 92,3%, specificity 100%,accuracy 95%), basically similar to those obtained with MRI (39).
The superiority of MRI in the femoral acetabular impingementstudy consists of the possibility to evidence at the same time thewhole pathological picture and therefore also accessory lesions (34,
40). In CAM type impingement, the disjunction between labrumand anterior wall acetabular cartilage, the presence of cystic le-sions in the anterosuperior femoral neck and the femoral bumpoccur together with labrum lesion. In PINCER type impingement,labrum lesion is less frequent and even often ossified. The MRIsometimes allows to identify an associated cartilage lesion in thepostero inferior portion of the acetabulum due to an increasedcompression exerted in this region during hip flexion (40).
SURGICAL TECHNIQUE
Arthroscopic trimming of labral lesion can be performed withpatient either in supine position or in lateral decubitus position.Positioning must be carefully executed by the surgeon or by thestaff aware of risks resulting from traction. Most of reported com-plications are in fact due to mistakes in positioning patients apply-ing traction and can be avoided with appropriate tricks (41, 42). Incase a simultaneous associated impingement treatment is needed,it is necessary to apply correct measures in order to perform alsothe arthroscopic time in the femoral neck.
After having performed hip arthroscopy in lateral position for8 years I must concede that since the advent of impingement treat-ment in 2004, I have started using supine decubitus positionwhich, according to my opinion, facilitates osteochondroplasty.
The first measure in performing hip arthroscopy is to avoid in-juries of the labrum while inserting instruments. Current availabil-
168
Chapter 11
Figure 10
MRI in a patient affected by Cam type deformity.Contrast liquid infiltration at labral acetabularbase witnesses the disjunction between labrumand cartilage
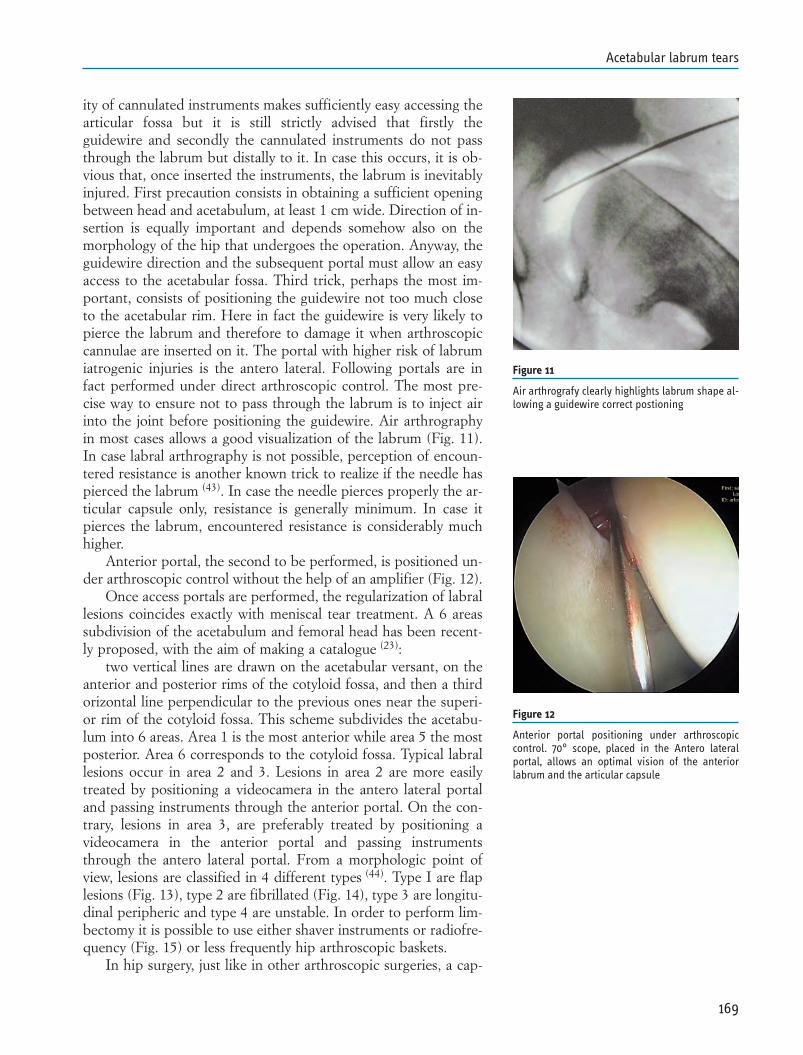
ity of cannulated instruments makes sufficiently easy accessing thearticular fossa but it is still strictly advised that firstly theguidewire and secondly the cannulated instruments do not passthrough the labrum but distally to it. In case this occurs, it is ob-vious that, once inserted the instruments, the labrum is inevitablyinjured. First precaution consists in obtaining a sufficient openingbetween head and acetabulum, at least 1 cm wide. Direction of in-sertion is equally important and depends somehow also on themorphology of the hip that undergoes the operation. Anyway, theguidewire direction and the subsequent portal must allow an easyaccess to the acetabular fossa. Third trick, perhaps the most im-portant, consists of positioning the guidewire not too much closeto the acetabular rim. Here in fact the guidewire is very likely topierce the labrum and therefore to damage it when arthroscopiccannulae are inserted on it. The portal with higher risk of labrumiatrogenic injuries is the antero lateral. Following portals are infact performed under direct arthroscopic control. The most pre-cise way to ensure not to pass through the labrum is to inject airinto the joint before positioning the guidewire. Air arthrographyin most cases allows a good visualization of the labrum (Fig. 11).In case labral arthrography is not possible, perception of encoun-tered resistance is another known trick to realize if the needle haspierced the labrum (43). In case the needle pierces properly the ar-ticular capsule only, resistance is generally minimum. In case itpierces the labrum, encountered resistance is considerably muchhigher.
Anterior portal, the second to be performed, is positioned un-der arthroscopic control without the help of an amplifier (Fig. 12).
Once access portals are performed, the regularization of labrallesions coincides exactly with meniscal tear treatment. A 6 areassubdivision of the acetabulum and femoral head has been recent-ly proposed, with the aim of making a catalogue (23):
two vertical lines are drawn on the acetabular versant, on theanterior and posterior rims of the cotyloid fossa, and then a thirdorizontal line perpendicular to the previous ones near the superi-or rim of the cotyloid fossa. This scheme subdivides the acetabu-lum into 6 areas. Area 1 is the most anterior while area 5 the mostposterior. Area 6 corresponds to the cotyloid fossa. Typical labrallesions occur in area 2 and 3. Lesions in area 2 are more easilytreated by positioning a videocamera in the antero lateral portaland passing instruments through the anterior portal. On the con-trary, lesions in area 3, are preferably treated by positioning avideocamera in the anterior portal and passing instrumentsthrough the antero lateral portal. From a morphologic point ofview, lesions are classified in 4 different types (44). Type I are flaplesions (Fig. 13), type 2 are fibrillated (Fig. 14), type 3 are longitu-dinal peripheric and type 4 are unstable. In order to perform lim-bectomy it is possible to use either shaver instruments or radiofre-quency (Fig. 15) or less frequently hip arthroscopic baskets.
In hip surgery, just like in other arthroscopic surgeries, a cap-
169
Acetabular labrum tears
Figure 11
Air arthrografy clearly highlights labrum shape al-lowing a guidewire correct postioning
Figure 12
Anterior portal positioning under arthroscopiccontrol. 70° scope, placed in the Antero lateralportal, allows an optimal vision of the anteriorlabrum and the articular capsule
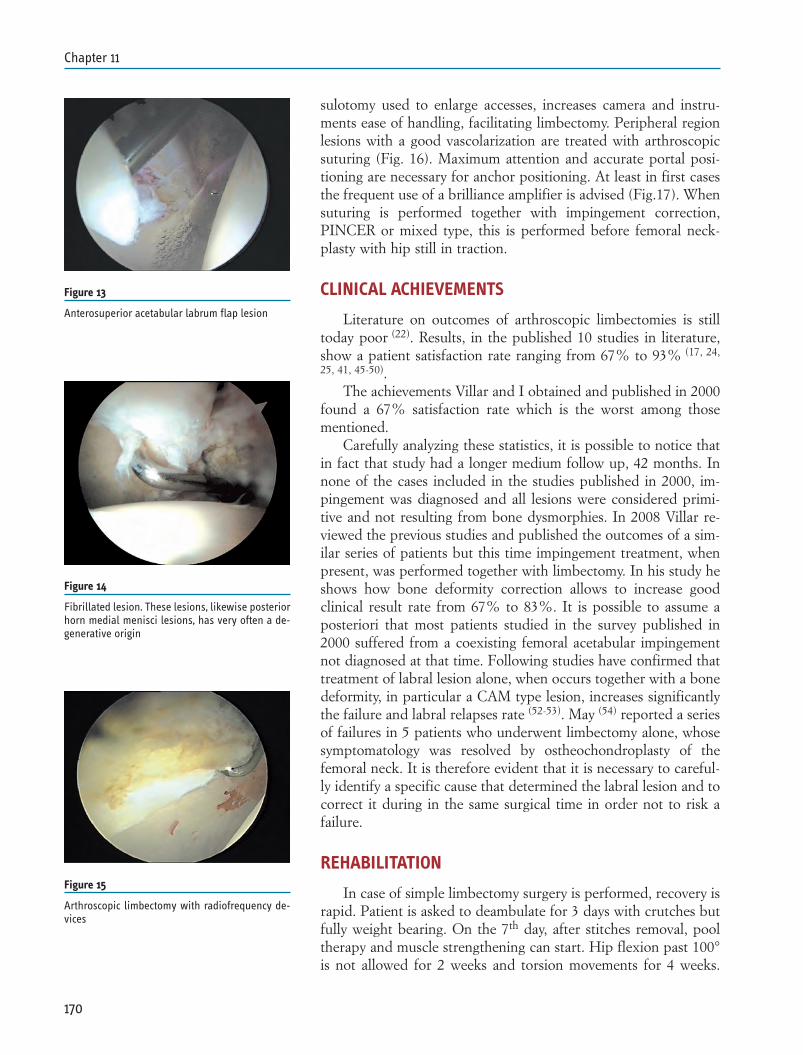
sulotomy used to enlarge accesses, increases camera and instru-ments ease of handling, facilitating limbectomy. Peripheral regionlesions with a good vascolarization are treated with arthroscopicsuturing (Fig. 16). Maximum attention and accurate portal posi-tioning are necessary for anchor positioning. At least in first casesthe frequent use of a brilliance amplifier is advised (Fig.17). Whensuturing is performed together with impingement correction,PINCER or mixed type, this is performed before femoral neck-plasty with hip still in traction.
CLINICAL ACHIEVEMENTS
Literature on outcomes of arthroscopic limbectomies is stilltoday poor (22). Results, in the published 10 studies in literature,show a patient satisfaction rate ranging from 67% to 93% (17, 24,
25, 41, 45-50).The achievements Villar and I obtained and published in 2000
found a 67% satisfaction rate which is the worst among thosementioned.
Carefully analyzing these statistics, it is possible to notice thatin fact that study had a longer medium follow up, 42 months. Innone of the cases included in the studies published in 2000, im-pingement was diagnosed and all lesions were considered primi-tive and not resulting from bone dysmorphies. In 2008 Villar re-viewed the previous studies and published the outcomes of a sim-ilar series of patients but this time impingement treatment, whenpresent, was performed together with limbectomy. In his study heshows how bone deformity correction allows to increase goodclinical result rate from 67% to 83%. It is possible to assume aposteriori that most patients studied in the survey published in2000 suffered from a coexisting femoral acetabular impingementnot diagnosed at that time. Following studies have confirmed thattreatment of labral lesion alone, when occurs together with a bonedeformity, in particular a CAM type lesion, increases significantlythe failure and labral relapses rate (52-53). May (54) reported a seriesof failures in 5 patients who underwent limbectomy alone, whosesymptomatology was resolved by ostheochondroplasty of thefemoral neck. It is therefore evident that it is necessary to careful-ly identify a specific cause that determined the labral lesion and tocorrect it during in the same surgical time in order not to risk afailure.
REHABILITATION
In case of simple limbectomy surgery is performed, recovery israpid. Patient is asked to deambulate for 3 days with crutches butfully weight bearing. On the 7th day, after stitches removal, pooltherapy and muscle strengthening can start. Hip flexion past 100°is not allowed for 2 weeks and torsion movements for 4 weeks.
170
Chapter 11
Figure 13
Anterosuperior acetabular labrum flap lesion
Figure 14
Fibrillated lesion. These lesions, likewise posteriorhorn medial menisci lesions, has very often a de-generative origin
Figure 15
Arthroscopic limbectomy with radiofrequency de-vices
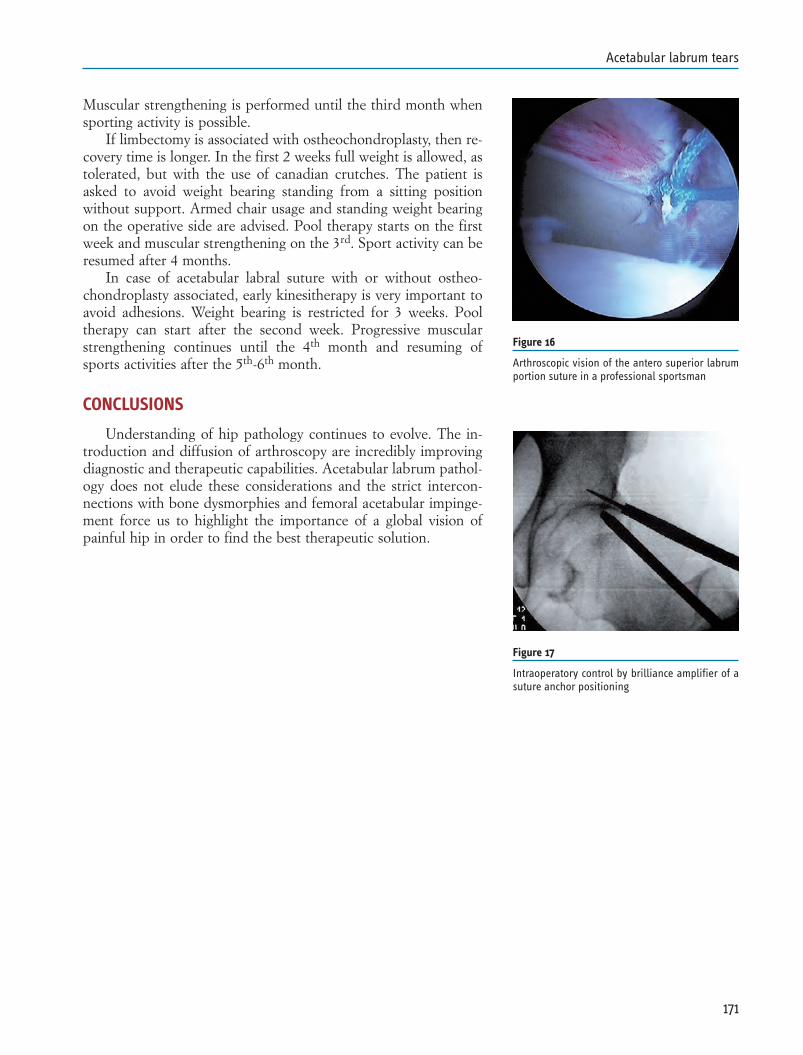
Muscular strengthening is performed until the third month whensporting activity is possible.
If limbectomy is associated with ostheochondroplasty, then re-covery time is longer. In the first 2 weeks full weight is allowed, astolerated, but with the use of canadian crutches. The patient isasked to avoid weight bearing standing from a sitting positionwithout support. Armed chair usage and standing weight bearingon the operative side are advised. Pool therapy starts on the firstweek and muscular strengthening on the 3rd. Sport activity can beresumed after 4 months.
In case of acetabular labral suture with or without ostheo-chondroplasty associated, early kinesitherapy is very important toavoid adhesions. Weight bearing is restricted for 3 weeks. Pooltherapy can start after the second week. Progressive muscularstrengthening continues until the 4th month and resuming ofsports activities after the 5th-6th month.
CONCLUSIONS
Understanding of hip pathology continues to evolve. The in-troduction and diffusion of arthroscopy are incredibly improvingdiagnostic and therapeutic capabilities. Acetabular labrum pathol-ogy does not elude these considerations and the strict intercon-nections with bone dysmorphies and femoral acetabular impinge-ment force us to highlight the importance of a global vision ofpainful hip in order to find the best therapeutic solution.
171
Acetabular labrum tears
Figure 16
Arthroscopic vision of the antero superior labrumportion suture in a professional sportsman
Figure 17
Intraoperatory control by brilliance amplifier of asuture anchor positioning
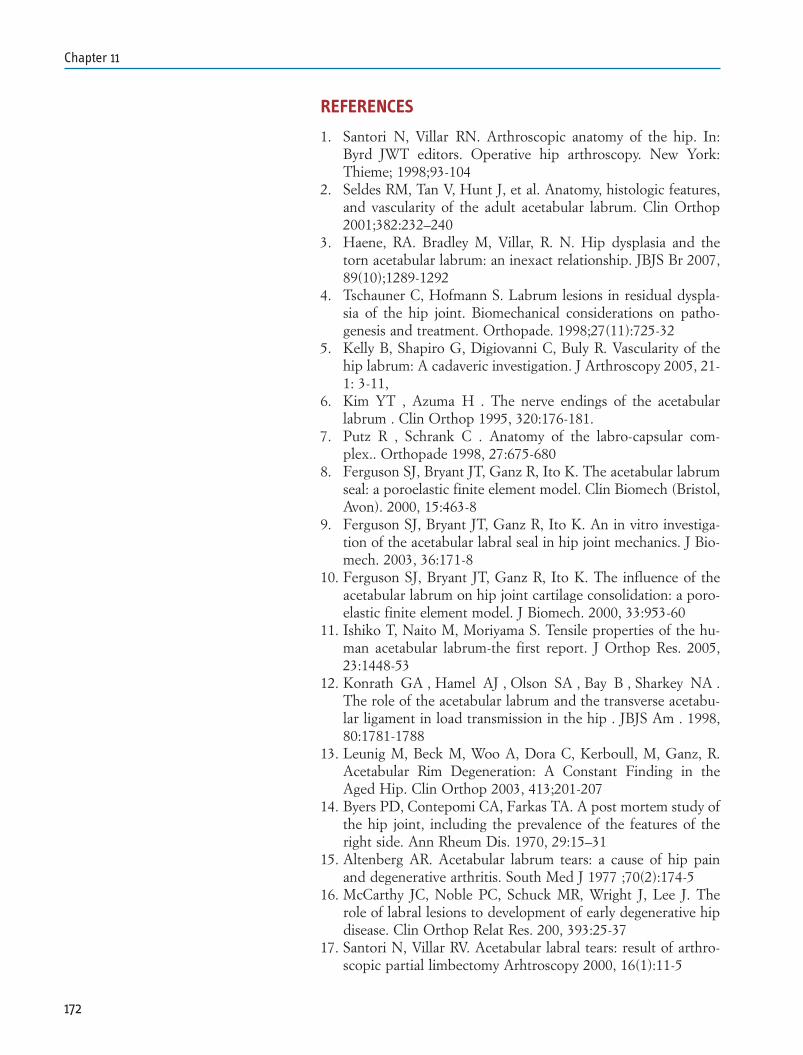
REFERENCES
1. Santori N, Villar RN. Arthroscopic anatomy of the hip. In:Byrd JWT editors. Operative hip arthroscopy. New York:Thieme; 1998;93-104
2. Seldes RM, Tan V, Hunt J, et al. Anatomy, histologic features,and vascularity of the adult acetabular labrum. Clin Orthop2001;382:232–240
3. Haene, RA. Bradley M, Villar, R. N. Hip dysplasia and thetorn acetabular labrum: an inexact relationship. JBJS Br 2007,89(10);1289-1292
4. Tschauner C, Hofmann S. Labrum lesions in residual dyspla-sia of the hip joint. Biomechanical considerations on patho-genesis and treatment. Orthopade. 1998;27(11):725-32
5. Kelly B, Shapiro G, Digiovanni C, Buly R. Vascularity of thehip labrum: A cadaveric investigation. J Arthroscopy 2005, 21-1: 3-11,
6. Kim YT , Azuma H . The nerve endings of the acetabularlabrum . Clin Orthop 1995, 320:176-181.
7. Putz R , Schrank C . Anatomy of the labro-capsular com-plex.. Orthopade 1998, 27:675-680
8. Ferguson SJ, Bryant JT, Ganz R, Ito K. The acetabular labrumseal: a poroelastic finite element model. Clin Biomech (Bristol,Avon). 2000, 15:463-8
9. Ferguson SJ, Bryant JT, Ganz R, Ito K. An in vitro investiga-tion of the acetabular labral seal in hip joint mechanics. J Bio-mech. 2003, 36:171-8
10. Ferguson SJ, Bryant JT, Ganz R, Ito K. The influence of theacetabular labrum on hip joint cartilage consolidation: a poro-elastic finite element model. J Biomech. 2000, 33:953-60
11. Ishiko T, Naito M, Moriyama S. Tensile properties of the hu-man acetabular labrum-the first report. J Orthop Res. 2005,23:1448-53
12. Konrath GA , Hamel AJ , Olson SA , Bay B , Sharkey NA .The role of the acetabular labrum and the transverse acetabu-lar ligament in load transmission in the hip . JBJS Am . 1998,80:1781-1788
13. Leunig M, Beck M, Woo A, Dora C, Kerboull, M, Ganz, R.Acetabular Rim Degeneration: A Constant Finding in theAged Hip. Clin Orthop 2003, 413;201-207
14. Byers PD, Contepomi CA, Farkas TA. A post mortem study ofthe hip joint, including the prevalence of the features of theright side. Ann Rheum Dis. 1970, 29:15–31
15. Altenberg AR. Acetabular labrum tears: a cause of hip painand degenerative arthritis. South Med J 1977 ;70(2):174-5
16. McCarthy JC, Noble PC, Schuck MR, Wright J, Lee J. Therole of labral lesions to development of early degenerative hipdisease. Clin Orthop Relat Res. 200, 393:25-37
17. Santori N, Villar RV. Acetabular labral tears: result of arthro-scopic partial limbectomy Arhtroscopy 2000, 16(1):11-5
172
Chapter 11
18. Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, SiebenrockKA. Femoroacetabular impingement: a cause for osteoarthritisof the hip. Clin Orthop Relat Res. 2003, 417:112–120
19. Burnett RS, Della Rocca G, Prather H. Clinical presentationsof patient with tears of the acetabular labrum. JBJS 2006,88A;1448-1457
20. Mintz DN, Hooper T, Connell D, Buly R, Padgett DE, Pot-ter HG. Magnetic resonance imaging of the hip: Detection oflabral and chondral abnormalities using noncontrast imaging.Arthroscopy. 2005, 21:385–393
21. Shindle MK, Voos JE, Heyworth BE, Mintz DN, Moya LE,Buly RL, Kelly BT. Hip arthroscopy in the athletic patient:current techniques and spectrum of disease. JBJS Am. 2007,89 Suppl 3
22. Clohisy JC, Beaule PE, O’’Malley A,. Safran MR, SchoeneckerP. Arthroscopic Management of Labral Tears in the Hip JBJSAm 2008, 1:90:2-19
23. Ilizaliturri VM Jr, Byrd JW, Sampson TG, Guanche CA,Philippon MJ, Kelly BT, Dienst M, Mardones R, Shonnard P,Larson CM. A geographic zone method to describe intra-artic-ular pathology in hip arthroscopy: cadaveric study and prelim-inary report. Arthroscopy. 2008, 24(5):534-9
24. Guanche CA, Sikka RS. Acetabular labral tears with underly-ing chondromalacia: a possible association with high-level run-ning. Arthroscopy.2005, 21:580 -5.
25. Farjo LA, Glick JM, Sampson TG. Hip arthroscopy for ac-etabular labral tears. Arthroscopy.1999, 15:132 -7
26. Christopher J, Thompson MT , Crawford, MJ, Alexander J,McCarthy J, Noble P. Tensile Strain in the Anterior Part of theAcetabular Labrum During Provocative Maneuvering of theNormal Hip. JBJS Am 90(7), 2008, 1464-1472
27. Kelly BT, Weiland DE, Schenker ML, Philippon MJ. Arthro-scopic labral repair in the hip: surgical technique and reviewof the literature. Arthroscopy 2005, 21:1496-504.
28. Wenger DE, Kendell KR, Miner MR, Trousdale RT. Acetabu-lar labral tears rarely occur in the absence of bony abnormali-ties. Clin Orthop 2004, 426:145-50.
29. Smith-Petersen MN. Treatment of malum coxae senilis, oldslipped upper femoral epiphysis, intrapelvic protrusion of theacetabulum, and coxa plana by means of acetabuloplasty. JBJS1936,18:869-80.
30. Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieber-man JM, Buly R. Acetabular labral tears: evaluation with MRarthrography. Radiology. 1996, ;200(1):231-5.
31. 2Leunig M, Werlen S, Ito K, Ganz R. Evaluation of the ac-etabular labrum by MR arthrography. JBJS Br. 1997,79:230–234
32. Keeney JA, Peelle MW, Jackson J, Rubin D, Maloney WJ,Clohisy JC. Magnetic resonance arthrography versus
173
Acetabular labrum tears
arthroscopy in the evaluation of articular hip pathology. ClinOrthop Relat Res. 2004, 163–169
33. Byrd JWT, Jones KS. Diagnostic accuracy of clinical assess-ment, magnetic resonance imaging, magnetic resonancearthrography, and intra-articular injection in hip arthroscopypatients. Am J Sports Med. 2004, 32:1668–1674
34. Chan YS, Lien LC, Hsu HL, et al. Evaluating hip labraltears using magnetic resonance arthrography: A prospectivestudy comparing hip arthroscopy and magnetic resonancearthrography diagnosis. Arthroscopy. 2005, 21:1250–1256
35. Kubo T, Horii M, Harada Y, et al. Radial-sequence magnet-ic resonance imaging in evaluation of acetabular labrum. J Or-thop Sci. 1999, 4:328–332
36. Czerny C, Hofmann S, Neuhold A, et al. “Lesions of the ac-etabular labrum: accuracy of MR imaging and MR arthrogra-phy in detection and staging.” Radiology 1996, 200: 225-230
37. Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K,Hodler J. The contour of the femoral head-neck junction as apredictor for the risk of anterior impingement. JBJS Br. 2002,84:556 -60
38. Toomayan GA, Holman WR, Major NM, Kozlowicz S, VailTP. Sensitivity of MR Arthrography in the Evaluation of Ac-etabular Labral Tears. AJR 2006, 186:449-453
39. YamamotoY, Tonotsuka H, Ueda T, HamadaY. Usefulness ofRadial Contrast-Enhanced Computed Tomography for the Di-agnosis of Acetabular Labrum Injury. Arthroscopy 2007,23,12: 1290-1294
40. Pfirrmann CW, Mengiardi B, Dora C. Cam and pincerfemoroacetabular impingement: characteristic MR arthro-graphic findings in 50 patients. Radiology 2006, 240(3):778-85.
41. Byrd JW, Jones KS. Prospective analysis of hip arthroscopywith 2-year follow-up. Arthroscopy.2000, 16:578 -87.
42. Smart LR, Oetgen M, Noonan B, Medvecky M. Beginning hiparthroscopy: indications, positioning, portals, basic tech-niques, and complications. Arthroscopy.2007, 23:1348 -53.
43. Byrd T. Avoiding the labrum in hip arthroscopy. Arthroscopy2000, 16,7:770-773.
44. Lage La, Patel RJ, Villar RN. The acetabular labral tear: anarthroscopic classification. Arthroscopy 1996, 12(3):269-72
45. McCarthy J, Barsoum W, Puri L, Lee JA, Murphy S, Cooke P.The role of hip arthroscopy in the elite athlete.Clin OrthopRelat Res .2003, 406:71 -4.
46. Philippon MJ, Schenker ML, Briggs KK, Kuppersmith DA,Maxwell RB, Stubbs AJ. Revision hip arthroscopy. Am JSports Med. 2007, 35:1918 -21
47. Saw T, Villar R. Footballer’s hip a report of six cases. JBJSBr.2004, 86:655 -8
48. Ilizaliturri VM Jr, Nossa-Barrera JM, Acosta-Rodriguez E, Ca-macho-Galindo J. Arthroscopic treatment of femoroacetabular
174
Chapter 11
impingement secondary to paediatric hip disorders. JBJS Br.2007, 89:1025 -30.
49. Potter BK, Freedman BA, Andersen RC, Bojescul JA, KukloTR, Murphy KP. Correlation of Short Form-36 and disabilitystatus with outcomes of arthroscopic acetabular labral de-bridement. Am J Sports Med. 2005, 33:864 -70
50. O’Leary JA, Berend K, Vail TP. The relationship between di-agnosis and outcome in arthroscopy of the hip.Arthroscopy .2001, 17:181 -8
51. Bardakos, N. V.; Vasconcelos, J. C.; Villar, R. N. Early out-come of hip arthroscopy for femoroacetabular impingement:the role of femoral osteoplasty in symptomatic improvement.JBJS Br 2008, 90(12);1570-1575
52. Philippon M, Schenker M, Briggs K, Kuppersmith D.Femoroacetabular impingement in 45 professional athletes: as-sociated pathologies and return to sport following arthroscop-ic decompression. Knee Surg Sports Traumatol Arthrosc.2007,15:908 -14.
53. Heyworth BE, Shindle MK, Voos JE, Rudzki JR, Kelly BT. Ra-diologic and intraoperative findings in revision hiparthroscopy. Arthroscopy.2007, 23:1295 -302
54. May O, Matar WY, Beaulé PE. Treatment of failed arthro-scopic acetabular labral debridement by femoral chondro-os-teoplasty: a case series of five patients. J Bone Joint Surg [Br]2007, 89-B:595-8.
175
Acetabular labrum tears


INTRODUCTION
Hip traumatology is one of the fields for which arthroscopictreatment is most indicated.
In severe hip trauma cases with fracture-dislocation, differentsized articular loose bodies, starting from cotyloid rim or femoralhead, may be left after luxation reduction; complete teres ligamentlesions are always present and acetabular labral lesions can alsooccur; varying extent blunt lesions can occur against articular car-tilage.
Arthroscopy allows a minimally invasive post-acute treatmentwith no need to expose articulation and redislocate femoral head,and minimizes risks of open treatment.
However, the best advantage of a targeted arthroscopic treat-ment, providing joint fragments removal and articular sanification,consists mainly in reducing risks of arthrosic evolution which mayoccur if left untreated. The choice not to operate was very fre-quent until not long ago, supported by the belief that refrainingfrom treatment was a lesser evil than a too aggressive and riskysurgical approach.
According to literature (Upadhyay-1983) (1), post-traumaticarthrosic risk is very high in luxation cases, with percentages vary-ing between 24% and 54%, and it is strictly correlated to thepresent lesions extent.
Predisposing factors of this constant arthrosic evolution aredue to an osteochondral fragments persistence within the joint,that produces an increase of lytic enzymes developing in articulararea thanks to the presence of loose cartilage particles.
The reason why a 24% of arthrosic evolution occur also insimple dislocations, could be that in such cases there is a highprobability that radiographically not visible articular microfrag-ments are present. Katayama has asserted that CT and MRI hipstudies after simple traumatic dislocation may not evidence carti-lage fragments inferior to 5 mm.; therefore also these authors sug-gest arthroscopy as a mean to obtain a complete joint assessment
177
Chapter 12TRAUMATOLOGYRaul ZiniPiergiorgio PiraniMarcello Occhialini

and cleaning, providing a reduction of the potential risk ofarthrosic evolution.
In literature, there are not many studies on the arthroscopictechnique use in hip traumatology, but all Authors agree on itsgreat avail.
Keene and Villar in 1994 (4) are the first to highlight the cer-tain avail of arthroscopic removal of loose bodies following trau-matic hip dislocation.
In 1996 Byrd (5) publishes three cases of young adults who un-derwent hip arthroscopy to remove post traumatic loose frag-ments.
In 2001 Kashiwagi (6) deals with a case of bone fragment re-moval associated with teres ligament avulsion.
Yamamoto in 2003 (7) highlights the importance ofarthroscopy in traumatology reporting the first numerically rele-vant casistic of 10 patients and 11 hips that underwent arthro-scopic surgery; in 7 cases debridement of not diagnosed ostheo-chondral small fragments was performed, in 2 cases larger frag-ments were removed; in 2 cases a fragment synthesis with bio-re-absorbable pins was associated.
Svoboda and Murphy in 2004 (8) suggest the importance ofarthroscopy to remove fragments after posterior hip dislocation.
Mullis in 2006 (9) shows a series of 36 patients with 39 operat-ed hips; in 92% of cases loose bodies were removed; they were al-so found in 78% of cases that under x-ray and CT examinationsseemed negative.
Owens in 2006 (10) reports on 11 cases of articular fragmentsremoval associated to statistically relevant labral lesions thatshowed no following problem or complication.
INDICATIONS
After posterior hip fracture-dislocation, articular ostheochon-dral fragments may be left, either cotyloid rim detached fragmentsor femoral head fragments.
Thompson-Epstein classification describes 5 types of patho-logical pictures of progressive importance; type 1 corresponds tosimple traumatic dislocation without significant apparent fracturesor with small detached fragments; type 2 describes a posteriorcotyloid rim large fragment detachment; in type 3 there is a frac-ture with comminuted posterior cotyloid rim fragment; type 4 isfracture of the acetabular floor; type 5 is fracture of femoral head.
Pipkin classification is a sub-classification of the Thompson-Epstein type 5 fracture dislocation. He describes 4 different typesof increasing severity lesions: type 1 describes a femoral head os-theochondral more or less bulky fragment; 2-3 and 4 types de-scribe more severe cases involving also femoral neck and acetabu-lum.
An arthroscopic treatment is provided for those patients
178
Chapter 12
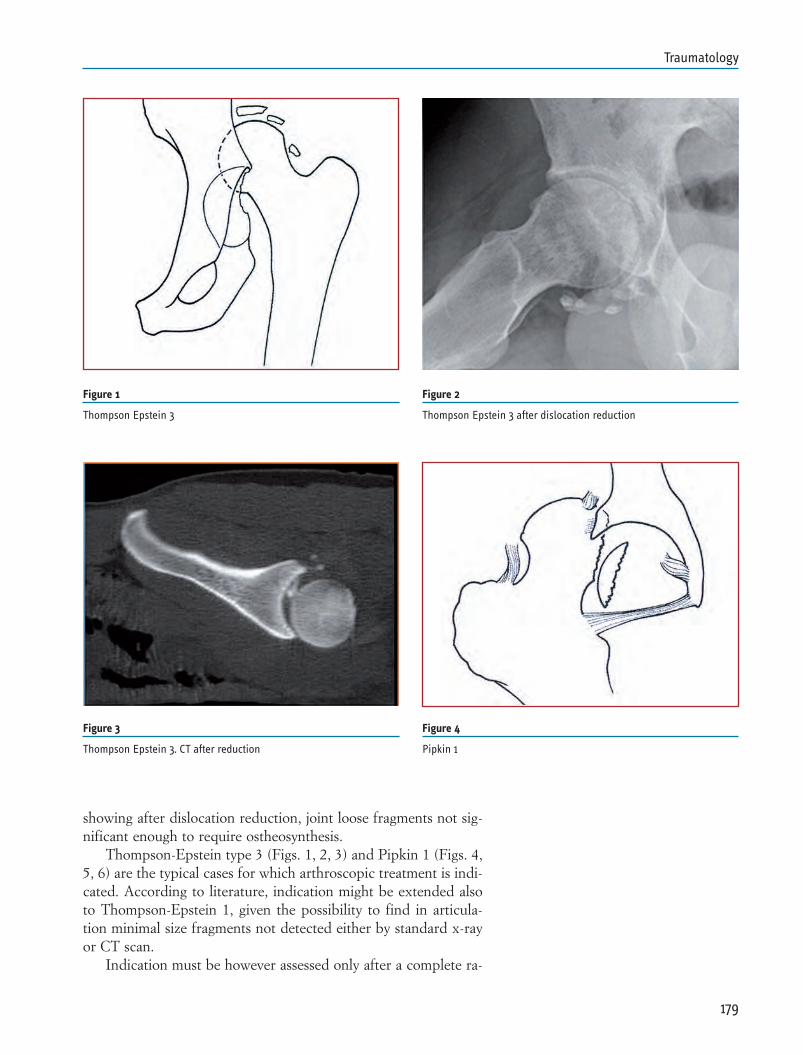
showing after dislocation reduction, joint loose fragments not sig-nificant enough to require ostheosynthesis.
Thompson-Epstein type 3 (Figs. 1, 2, 3) and Pipkin 1 (Figs. 4,5, 6) are the typical cases for which arthroscopic treatment is indi-cated. According to literature, indication might be extended alsoto Thompson-Epstein 1, given the possibility to find in articula-tion minimal size fragments not detected either by standard x-rayor CT scan.
Indication must be however assessed only after a complete ra-
179
Traumatology
Figure 1
Thompson Epstein 3
Figure 2
Thompson Epstein 3 after dislocation reduction
Figure 3
Thompson Epstein 3. CT after reduction
Figure 4
Pipkin 1
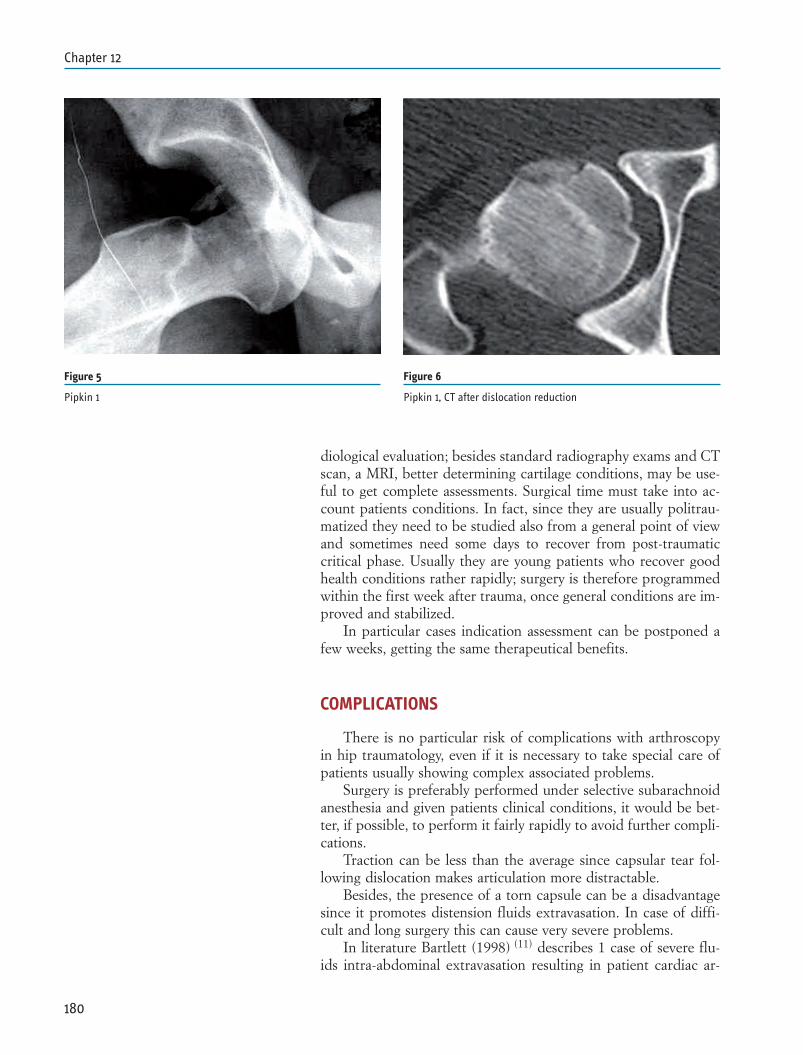
diological evaluation; besides standard radiography exams and CTscan, a MRI, better determining cartilage conditions, may be use-ful to get complete assessments. Surgical time must take into ac-count patients conditions. In fact, since they are usually politrau-matized they need to be studied also from a general point of viewand sometimes need some days to recover from post-traumaticcritical phase. Usually they are young patients who recover goodhealth conditions rather rapidly; surgery is therefore programmedwithin the first week after trauma, once general conditions are im-proved and stabilized.
In particular cases indication assessment can be postponed afew weeks, getting the same therapeutical benefits.
COMPLICATIONS
There is no particular risk of complications with arthroscopyin hip traumatology, even if it is necessary to take special care ofpatients usually showing complex associated problems.
Surgery is preferably performed under selective subarachnoidanesthesia and given patients clinical conditions, it would be bet-ter, if possible, to perform it fairly rapidly to avoid further compli-cations.
Traction can be less than the average since capsular tear fol-lowing dislocation makes articulation more distractable.
Besides, the presence of a torn capsule can be a disadvantagesince it promotes distension fluids extravasation. In case of diffi-cult and long surgery this can cause very severe problems.
In literature Bartlett (1998) (11) describes 1 case of severe flu-ids intra-abdominal extravasation resulting in patient cardiac ar-
180
Chapter 12
Figure 5
Pipkin 1
Figure 6
Pipkin 1, CT after dislocation reduction
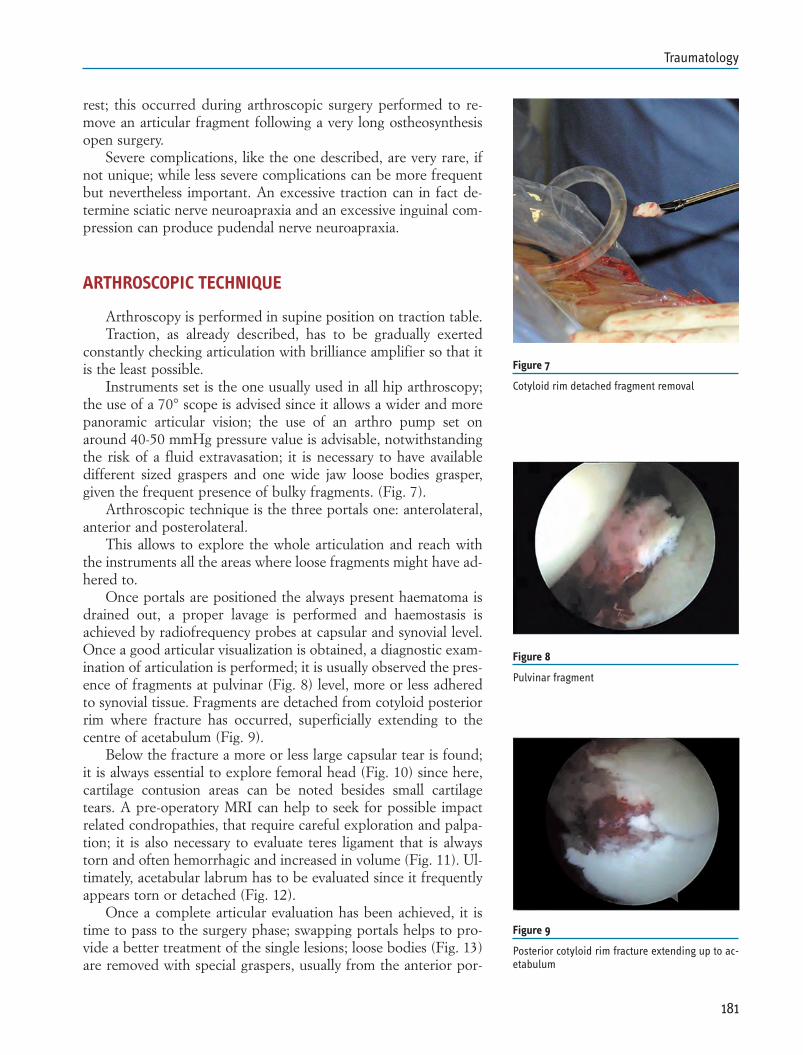
rest; this occurred during arthroscopic surgery performed to re-move an articular fragment following a very long ostheosynthesisopen surgery.
Severe complications, like the one described, are very rare, ifnot unique; while less severe complications can be more frequentbut nevertheless important. An excessive traction can in fact de-termine sciatic nerve neuroapraxia and an excessive inguinal com-pression can produce pudendal nerve neuroapraxia.
ARTHROSCOPIC TECHNIQUE
Arthroscopy is performed in supine position on traction table.Traction, as already described, has to be gradually exerted
constantly checking articulation with brilliance amplifier so that itis the least possible.
Instruments set is the one usually used in all hip arthroscopy;the use of a 70° scope is advised since it allows a wider and morepanoramic articular vision; the use of an arthro pump set onaround 40-50 mmHg pressure value is advisable, notwithstandingthe risk of a fluid extravasation; it is necessary to have availabledifferent sized graspers and one wide jaw loose bodies grasper,given the frequent presence of bulky fragments. (Fig. 7).
Arthroscopic technique is the three portals one: anterolateral,anterior and posterolateral.
This allows to explore the whole articulation and reach withthe instruments all the areas where loose fragments might have ad-hered to.
Once portals are positioned the always present haematoma isdrained out, a proper lavage is performed and haemostasis isachieved by radiofrequency probes at capsular and synovial level.Once a good articular visualization is obtained, a diagnostic exam-ination of articulation is performed; it is usually observed the pres-ence of fragments at pulvinar (Fig. 8) level, more or less adheredto synovial tissue. Fragments are detached from cotyloid posteriorrim where fracture has occurred, superficially extending to thecentre of acetabulum (Fig. 9).
Below the fracture a more or less large capsular tear is found;it is always essential to explore femoral head (Fig. 10) since here,cartilage contusion areas can be noted besides small cartilagetears. A pre-operatory MRI can help to seek for possible impactrelated condropathies, that require careful exploration and palpa-tion; it is also necessary to evaluate teres ligament that is alwaystorn and often hemorrhagic and increased in volume (Fig. 11). Ul-timately, acetabular labrum has to be evaluated since it frequentlyappears torn or detached (Fig. 12).
Once a complete articular evaluation has been achieved, it istime to pass to the surgery phase; swapping portals helps to pro-vide a better treatment of the single lesions; loose bodies (Fig. 13)are removed with special graspers, usually from the anterior por-
181
Traumatology
Figure 7
Cotyloid rim detached fragment removal
Figure 8
Pulvinar fragment
Figure 9
Posterior cotyloid rim fracture extending up to ac-etabulum
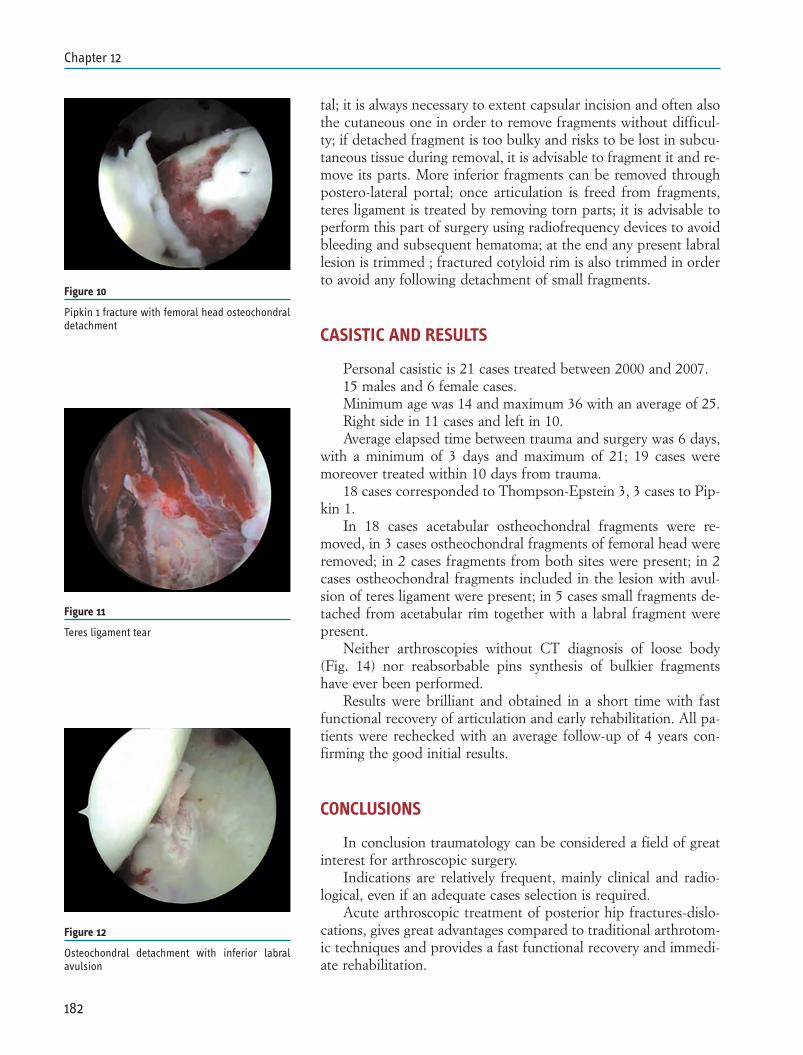
tal; it is always necessary to extent capsular incision and often alsothe cutaneous one in order to remove fragments without difficul-ty; if detached fragment is too bulky and risks to be lost in subcu-taneous tissue during removal, it is advisable to fragment it and re-move its parts. More inferior fragments can be removed throughpostero-lateral portal; once articulation is freed from fragments,teres ligament is treated by removing torn parts; it is advisable toperform this part of surgery using radiofrequency devices to avoidbleeding and subsequent hematoma; at the end any present labrallesion is trimmed ; fractured cotyloid rim is also trimmed in orderto avoid any following detachment of small fragments.
CASISTIC AND RESULTS
Personal casistic is 21 cases treated between 2000 and 2007.15 males and 6 female cases.Minimum age was 14 and maximum 36 with an average of 25.Right side in 11 cases and left in 10.Average elapsed time between trauma and surgery was 6 days,
with a minimum of 3 days and maximum of 21; 19 cases weremoreover treated within 10 days from trauma.
18 cases corresponded to Thompson-Epstein 3, 3 cases to Pip-kin 1.
In 18 cases acetabular ostheochondral fragments were re-moved, in 3 cases ostheochondral fragments of femoral head wereremoved; in 2 cases fragments from both sites were present; in 2cases ostheochondral fragments included in the lesion with avul-sion of teres ligament were present; in 5 cases small fragments de-tached from acetabular rim together with a labral fragment werepresent.
Neither arthroscopies without CT diagnosis of loose body(Fig. 14) nor reabsorbable pins synthesis of bulkier fragmentshave ever been performed.
Results were brilliant and obtained in a short time with fastfunctional recovery of articulation and early rehabilitation. All pa-tients were rechecked with an average follow-up of 4 years con-firming the good initial results.
CONCLUSIONS
In conclusion traumatology can be considered a field of greatinterest for arthroscopic surgery.
Indications are relatively frequent, mainly clinical and radio-logical, even if an adequate cases selection is required.
Acute arthroscopic treatment of posterior hip fractures-dislo-cations, gives great advantages compared to traditional arthrotom-ic techniques and provides a fast functional recovery and immedi-ate rehabilitation.
182
Chapter 12
Figure 10
Pipkin 1 fracture with femoral head osteochondraldetachment
Figure 11
Teres ligament tear
Figure 12
Osteochondral detachment with inferior labralavulsion
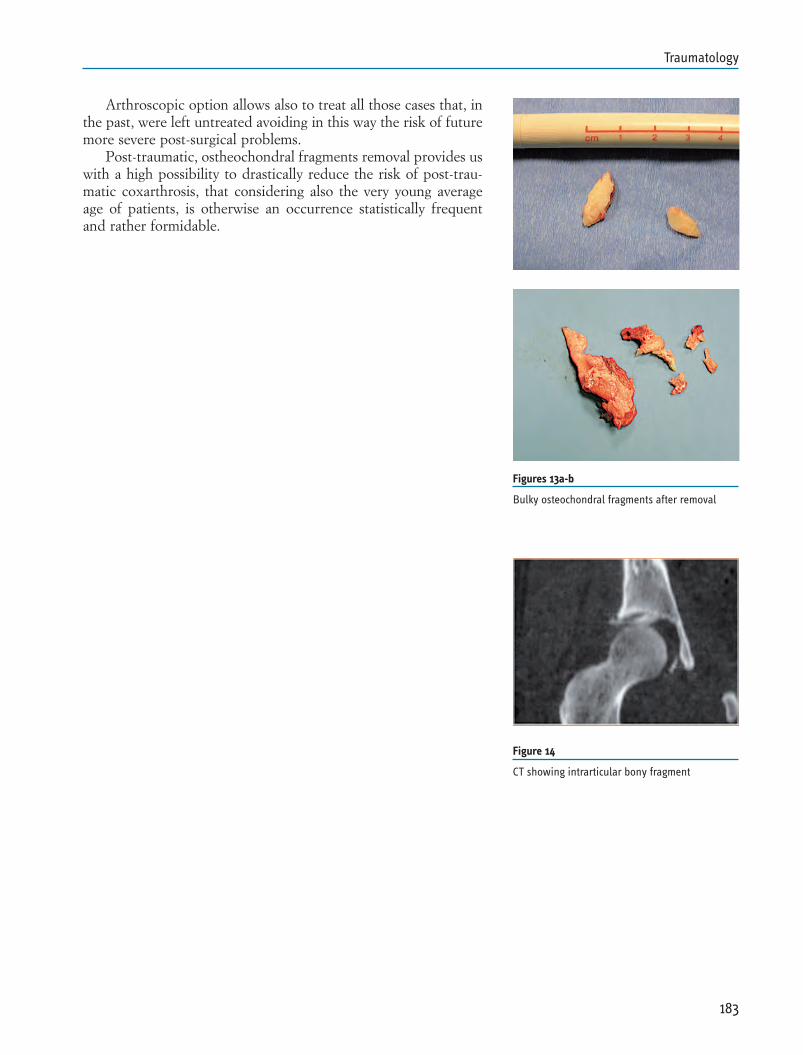
Arthroscopic option allows also to treat all those cases that, inthe past, were left untreated avoiding in this way the risk of futuremore severe post-surgical problems.
Post-traumatic, ostheochondral fragments removal provides uswith a high possibility to drastically reduce the risk of post-trau-matic coxarthrosis, that considering also the very young averageage of patients, is otherwise an occurrence statistically frequentand rather formidable.
183
Traumatology
Figures 13a-b
Bulky osteochondral fragments after removal
Figure 14
CT showing intrarticular bony fragment
REFERENCES
1. Upadhyay Ss, Moulton A, Srikrishnamurthi K. An analysis ofthe late effects of traumatic posterior dislocation of the hipwithout fractures. J Bone Joint Surg (BR) 1983; 65: 150-2
2. Evans Ch, Mazzocchi R, Nelson Dd. Experimental arthritis in-duced by intraarticular injection of allogenic cartilaginous par-ticles into rabbit knee. Arthritis Reum 1984; 27: 200-208
3. Katayama G, Sawaguchi T, Akagawa S. Treatment of traumat-ic fracture-dislocation of the hip with intraarticular fragments.Orthop Surg Traumatol 1987; 30: 1057-1065
4. Keene Gs, Villar Rn. Arthroscopic loose bodies retrieval fol-lowing traumatic hip dislocation. Injury, 1994 Oct; 25(8): 507-10.
5. Byrd Jw. Hip arthroscopy for posttraumatic loose fragments inthe young active adult: three case report. Clin J Sport Med.1996 Apr: 6(2): 129-33
6. Kashiwagi N, Suzuki S, Seto Y. Arthroscopic treatment fortraumatic hip dislocation with avulsion fracture of the liga-mentum teres. Arthroscopy 2001 Jan; 17(1): 67-9
7. Yamamoto Y, Ide T, Ono T, Hamada Y. Usefulness of arthro-scopic surgery in hip trauma cases. Arthroscopy. 2003 Mar;19(3): 269-73.
8. Svoboda Sj, Williams Dm, Murphy Kp. Hip arthroscopy forostechondral loose body remomal after a posterior hip disloca-tion. Arthroscoppy. 2003 Sep: 19(7); 777-81.
9. Mullis Bh, Dahners Le. Hip arthroscopy to remove loose bod-ies after traumatic dislocation. J Orthop Trauma 2006; 20:22-6
10. Owens Bd, Busconi Bd. Arthroscopy for hip dislocation andfracture-dislocation. Am J Orthop. 2006 Dec; 35(12): 584-7.
11. Bartlett Cs, Di Felice Gs, Buly Rl, Quinn Tj, Green Ds, HelfetDl. Cardiac arrest as a result of intraabdominal extravasationof fluid during arthroscopiuc removal of a loose body from thehip joint of a patient with an acetabular fracture. JOT May1998, 12: 4
184
Chapter 12
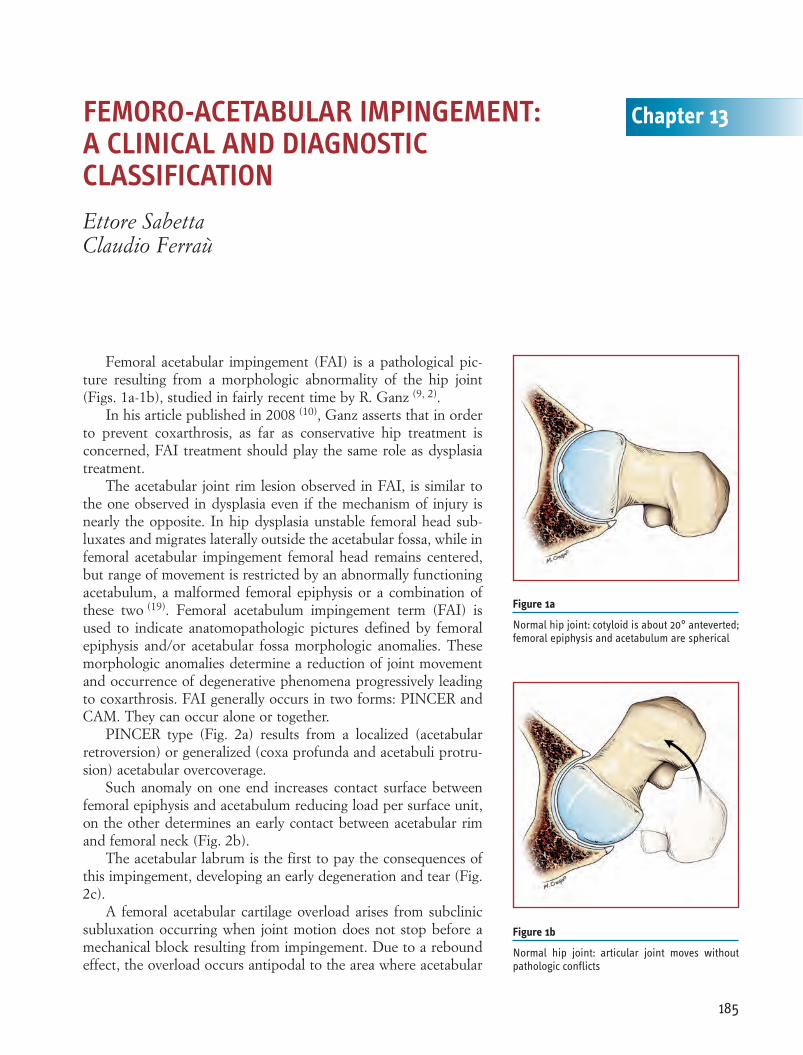
Femoral acetabular impingement (FAI) is a pathological pic-ture resulting from a morphologic abnormality of the hip joint(Figs. 1a-1b), studied in fairly recent time by R. Ganz (9, 2).
In his article published in 2008 (10), Ganz asserts that in orderto prevent coxarthrosis, as far as conservative hip treatment isconcerned, FAI treatment should play the same role as dysplasiatreatment.
The acetabular joint rim lesion observed in FAI, is similar tothe one observed in dysplasia even if the mechanism of injury isnearly the opposite. In hip dysplasia unstable femoral head sub-luxates and migrates laterally outside the acetabular fossa, while infemoral acetabular impingement femoral head remains centered,but range of movement is restricted by an abnormally functioningacetabulum, a malformed femoral epiphysis or a combination ofthese two (19). Femoral acetabulum impingement term (FAI) isused to indicate anatomopathologic pictures defined by femoralepiphysis and/or acetabular fossa morphologic anomalies. Thesemorphologic anomalies determine a reduction of joint movementand occurrence of degenerative phenomena progressively leadingto coxarthrosis. FAI generally occurs in two forms: PINCER andCAM. They can occur alone or together.
PINCER type (Fig. 2a) results from a localized (acetabularretroversion) or generalized (coxa profunda and acetabuli protru-sion) acetabular overcoverage.
Such anomaly on one end increases contact surface betweenfemoral epiphysis and acetabulum reducing load per surface unit,on the other determines an early contact between acetabular rimand femoral neck (Fig. 2b).
The acetabular labrum is the first to pay the consequences ofthis impingement, developing an early degeneration and tear (Fig.2c).
A femoral acetabular cartilage overload arises from subclinicsubluxation occurring when joint motion does not stop before amechanical block resulting from impingement. Due to a reboundeffect, the overload occurs antipodal to the area where acetabular
185
Chapter 13FEMORO-ACETABULAR IMPINGEMENT: A CLINICAL AND DIAGNOSTIC CLASSIFICATIONEttore SabettaClaudio Ferraù
Figure 1a
Normal hip joint: cotyloid is about 20° anteverted;femoral epiphysis and acetabulum are spherical
Figure 1b
Normal hip joint: articular joint moves withoutpathologic conflicts
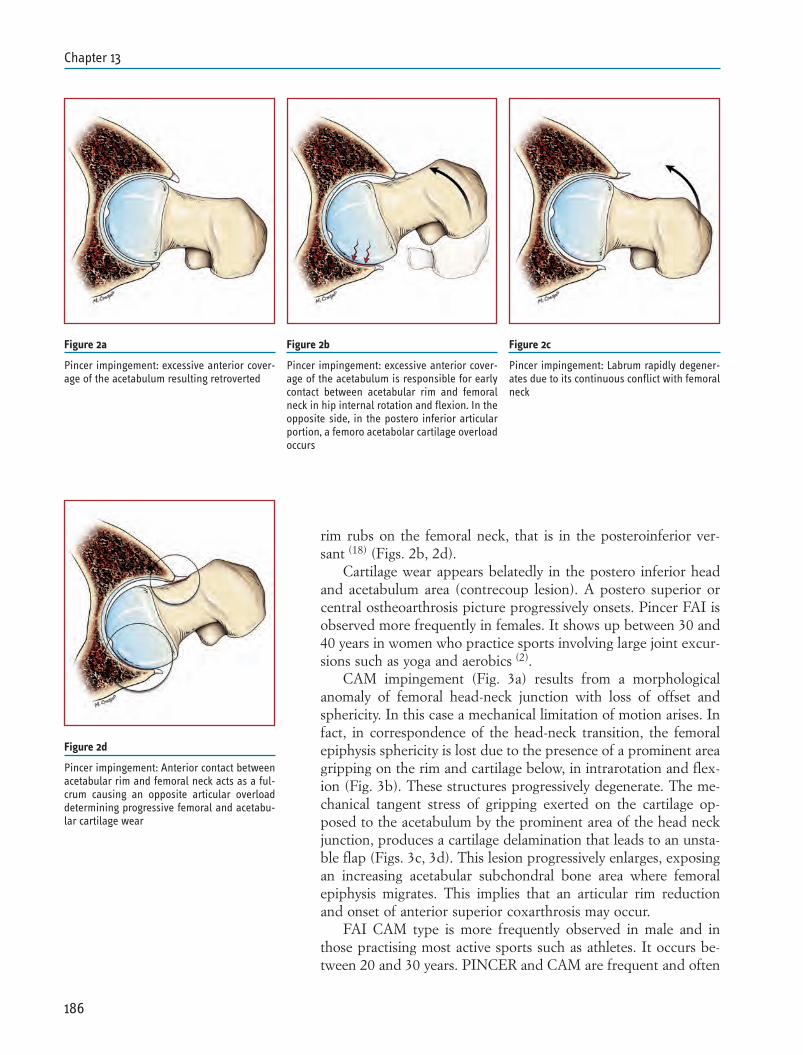
rim rubs on the femoral neck, that is in the posteroinferior ver-sant (18) (Figs. 2b, 2d).
Cartilage wear appears belatedly in the postero inferior headand acetabulum area (contrecoup lesion). A postero superior orcentral ostheoarthrosis picture progressively onsets. Pincer FAI isobserved more frequently in females. It shows up between 30 and40 years in women who practice sports involving large joint excur-sions such as yoga and aerobics (2).
CAM impingement (Fig. 3a) results from a morphologicalanomaly of femoral head-neck junction with loss of offset andsphericity. In this case a mechanical limitation of motion arises. Infact, in correspondence of the head-neck transition, the femoralepiphysis sphericity is lost due to the presence of a prominent areagripping on the rim and cartilage below, in intrarotation and flex-ion (Fig. 3b). These structures progressively degenerate. The me-chanical tangent stress of gripping exerted on the cartilage op-posed to the acetabulum by the prominent area of the head neckjunction, produces a cartilage delamination that leads to an unsta-ble flap (Figs. 3c, 3d). This lesion progressively enlarges, exposingan increasing acetabular subchondral bone area where femoralepiphysis migrates. This implies that an articular rim reductionand onset of anterior superior coxarthrosis may occur.
FAI CAM type is more frequently observed in male and inthose practising most active sports such as athletes. It occurs be-tween 20 and 30 years. PINCER and CAM are frequent and often
186
Chapter 13
Figure 2a
Pincer impingement: excessive anterior cover-age of the acetabulum resulting retroverted
Figure 2b
Pincer impingement: excessive anterior cover-age of the acetabulum is responsible for earlycontact between acetabular rim and femoralneck in hip internal rotation and flexion. In theopposite side, in the postero inferior articularportion, a femoro acetabolar cartilage overloadoccurs
Figure 2c
Pincer impingement: Labrum rapidly degener-ates due to its continuous conflict with femoralneck
Figure 2d
Pincer impingement: Anterior contact betweenacetabular rim and femoral neck acts as a ful-crum causing an opposite articular overloaddetermining progressive femoral and acetabu-lar cartilage wear
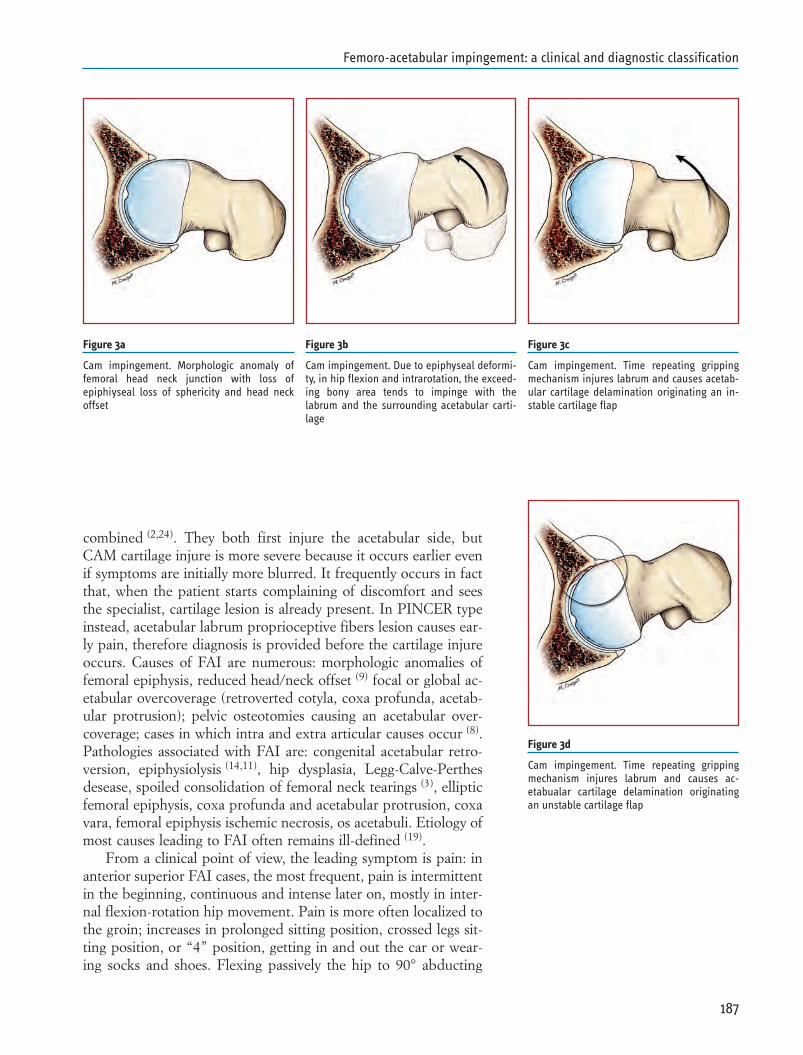
combined (2,24). They both first injure the acetabular side, butCAM cartilage injure is more severe because it occurs earlier evenif symptoms are initially more blurred. It frequently occurs in factthat, when the patient starts complaining of discomfort and seesthe specialist, cartilage lesion is already present. In PINCER typeinstead, acetabular labrum proprioceptive fibers lesion causes ear-ly pain, therefore diagnosis is provided before the cartilage injureoccurs. Causes of FAI are numerous: morphologic anomalies offemoral epiphysis, reduced head/neck offset (9) focal or global ac-etabular overcoverage (retroverted cotyla, coxa profunda, acetab-ular protrusion); pelvic osteotomies causing an acetabular over-coverage; cases in which intra and extra articular causes occur (8).Pathologies associated with FAI are: congenital acetabular retro-version, epiphysiolysis (14,11), hip dysplasia, Legg-Calve-Perthesdesease, spoiled consolidation of femoral neck tearings (3), ellipticfemoral epiphysis, coxa profunda and acetabular protrusion, coxavara, femoral epiphysis ischemic necrosis, os acetabuli. Etiology ofmost causes leading to FAI often remains ill-defined (19).
From a clinical point of view, the leading symptom is pain: inanterior superior FAI cases, the most frequent, pain is intermittentin the beginning, continuous and intense later on, mostly in inter-nal flexion-rotation hip movement. Pain is more often localized tothe groin; increases in prolonged sitting position, crossed legs sit-ting position, or “4” position, getting in and out the car or wear-ing socks and shoes. Flexing passively the hip to 90° abducting
187
Femoro-acetabular impingement: a clinical and diagnostic classification
Figure 3a
Cam impingement. Morphologic anomaly offemoral head neck junction with loss ofepiphiyseal loss of sphericity and head neckoffset
Figure 3b
Cam impingement. Due to epiphyseal deformi-ty, in hip flexion and intrarotation, the exceed-ing bony area tends to impinge with thelabrum and the surrounding acetabular carti-lage
Figure 3c
Cam impingement. Time repeating grippingmechanism injures labrum and causes acetab-ular cartilage delamination originating an in-stable cartilage flap
Figure 3d
Cam impingement. Time repeating grippingmechanism injures labrum and causes ac-etabualar cartilage delamination originatingan unstable cartilage flap
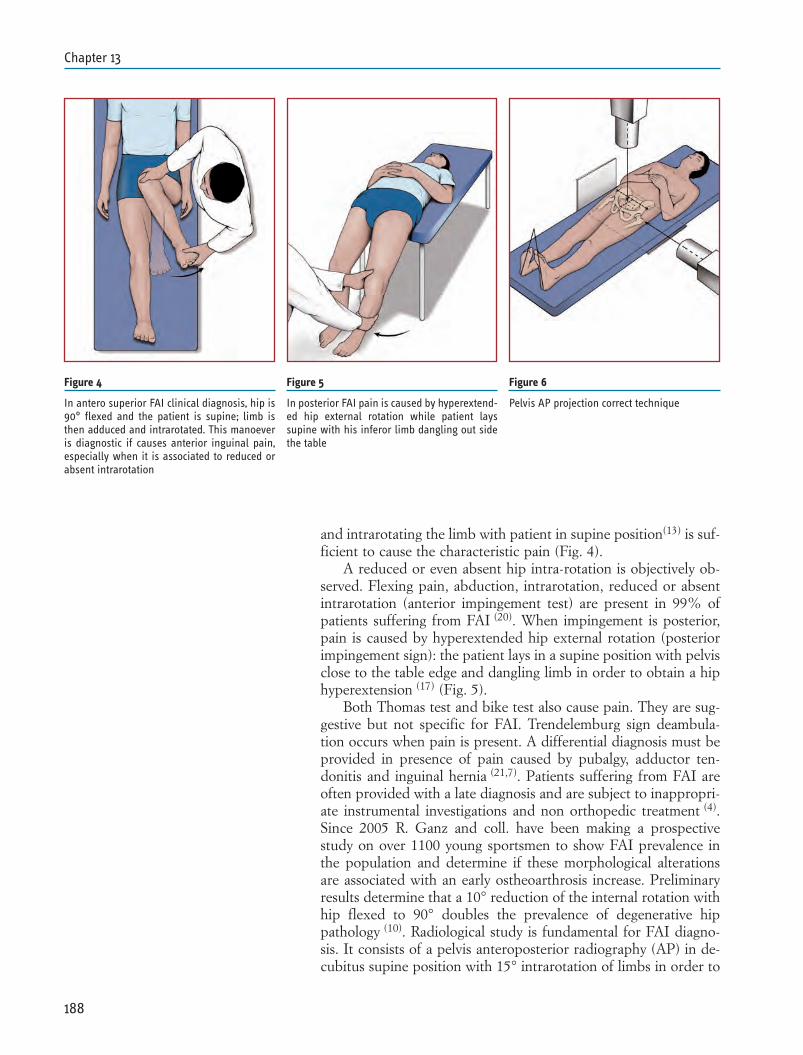
and intrarotating the limb with patient in supine position(13) is suf-ficient to cause the characteristic pain (Fig. 4).
A reduced or even absent hip intra-rotation is objectively ob-served. Flexing pain, abduction, intrarotation, reduced or absentintrarotation (anterior impingement test) are present in 99% ofpatients suffering from FAI (20). When impingement is posterior,pain is caused by hyperextended hip external rotation (posteriorimpingement sign): the patient lays in a supine position with pelvisclose to the table edge and dangling limb in order to obtain a hiphyperextension (17) (Fig. 5).
Both Thomas test and bike test also cause pain. They are sug-gestive but not specific for FAI. Trendelemburg sign deambula-tion occurs when pain is present. A differential diagnosis must beprovided in presence of pain caused by pubalgy, adductor ten-donitis and inguinal hernia (21,7). Patients suffering from FAI areoften provided with a late diagnosis and are subject to inappropri-ate instrumental investigations and non orthopedic treatment (4).Since 2005 R. Ganz and coll. have been making a prospectivestudy on over 1100 young sportsmen to show FAI prevalence inthe population and determine if these morphological alterationsare associated with an early ostheoarthrosis increase. Preliminaryresults determine that a 10° reduction of the internal rotation withhip flexed to 90° doubles the prevalence of degenerative hippathology (10). Radiological study is fundamental for FAI diagno-sis. It consists of a pelvis anteroposterior radiography (AP) in de-cubitus supine position with 15° intrarotation of limbs in order to
188
Chapter 13
Figure 4
In antero superior FAI clinical diagnosis, hip is90° flexed and the patient is supine; limb isthen adduced and intrarotated. This manoeveris diagnostic if causes anterior inguinal pain,especially when it is associated to reduced orabsent intrarotation
Figure 5
In posterior FAI pain is caused by hyperextend-ed hip external rotation while patient layssupine with his inferor limb dangling out sidethe table
Figure 6
Pelvis AP projection correct technique
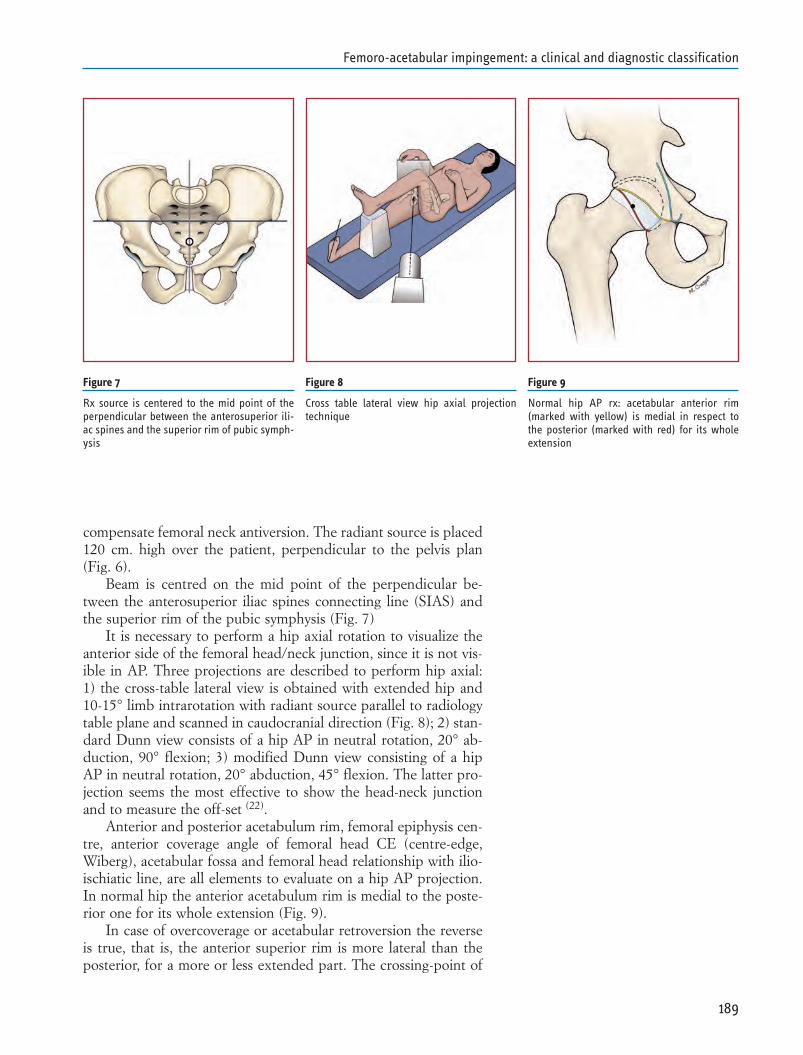
compensate femoral neck antiversion. The radiant source is placed120 cm. high over the patient, perpendicular to the pelvis plan(Fig. 6).
Beam is centred on the mid point of the perpendicular be-tween the anterosuperior iliac spines connecting line (SIAS) andthe superior rim of the pubic symphysis (Fig. 7)
It is necessary to perform a hip axial rotation to visualize theanterior side of the femoral head/neck junction, since it is not vis-ible in AP. Three projections are described to perform hip axial:1) the cross-table lateral view is obtained with extended hip and10-15° limb intrarotation with radiant source parallel to radiologytable plane and scanned in caudocranial direction (Fig. 8); 2) stan-dard Dunn view consists of a hip AP in neutral rotation, 20° ab-duction, 90° flexion; 3) modified Dunn view consisting of a hipAP in neutral rotation, 20° abduction, 45° flexion. The latter pro-jection seems the most effective to show the head-neck junctionand to measure the off-set (22).
Anterior and posterior acetabulum rim, femoral epiphysis cen-tre, anterior coverage angle of femoral head CE (centre-edge,Wiberg), acetabular fossa and femoral head relationship with ilio-ischiatic line, are all elements to evaluate on a hip AP projection.In normal hip the anterior acetabulum rim is medial to the poste-rior one for its whole extension (Fig. 9).
In case of overcoverage or acetabular retroversion the reverseis true, that is, the anterior superior rim is more lateral than theposterior, for a more or less extended part. The crossing-point of
189
Femoro-acetabular impingement: a clinical and diagnostic classification
Figure 8
Cross table lateral view hip axial projectiontechnique
Figure 7
Rx source is centered to the mid point of theperpendicular between the anterosuperior ili-ac spines and the superior rim of pubic symph-ysis
Figure 9
Normal hip AP rx: acetabular anterior rim(marked with yellow) is medial in respect tothe posterior (marked with red) for its wholeextension
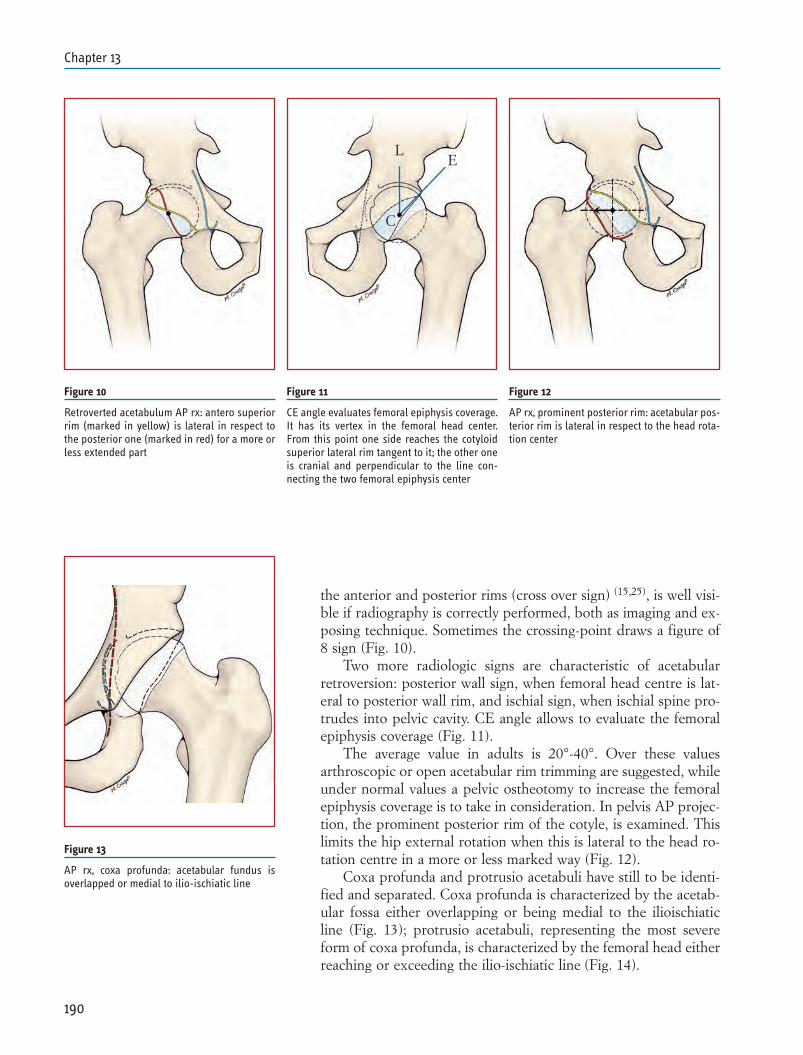
the anterior and posterior rims (cross over sign) (15,25), is well visi-ble if radiography is correctly performed, both as imaging and ex-posing technique. Sometimes the crossing-point draws a figure of8 sign (Fig. 10).
Two more radiologic signs are characteristic of acetabularretroversion: posterior wall sign, when femoral head centre is lat-eral to posterior wall rim, and ischial sign, when ischial spine pro-trudes into pelvic cavity. CE angle allows to evaluate the femoralepiphysis coverage (Fig. 11).
The average value in adults is 20°-40°. Over these valuesarthroscopic or open acetabular rim trimming are suggested, whileunder normal values a pelvic ostheotomy to increase the femoralepiphysis coverage is to take in consideration. In pelvis AP projec-tion, the prominent posterior rim of the cotyle, is examined. Thislimits the hip external rotation when this is lateral to the head ro-tation centre in a more or less marked way (Fig. 12).
Coxa profunda and protrusio acetabuli have still to be identi-fied and separated. Coxa profunda is characterized by the acetab-ular fossa either overlapping or being medial to the ilioischiaticline (Fig. 13); protrusio acetabuli, representing the most severeform of coxa profunda, is characterized by the femoral head eitherreaching or exceeding the ilio-ischiatic line (Fig. 14).
190
Chapter 13
Figure 11
CE angle evaluates femoral epiphysis coverage.It has its vertex in the femoral head center.From this point one side reaches the cotyloidsuperior lateral rim tangent to it; the other oneis cranial and perpendicular to the line con-necting the two femoral epiphysis center
Figure 12
AP rx, prominent posterior rim: acetabular pos-terior rim is lateral in respect to the head rota-tion center
Figure 10
Retroverted acetabulum AP rx: antero superiorrim (marked in yellow) is lateral in respect tothe posterior one (marked in red) for a more orless extended part
L
C
E
Figure 13
AP rx, coxa profunda: acetabular fundus isoverlapped or medial to ilio-ischiatic line
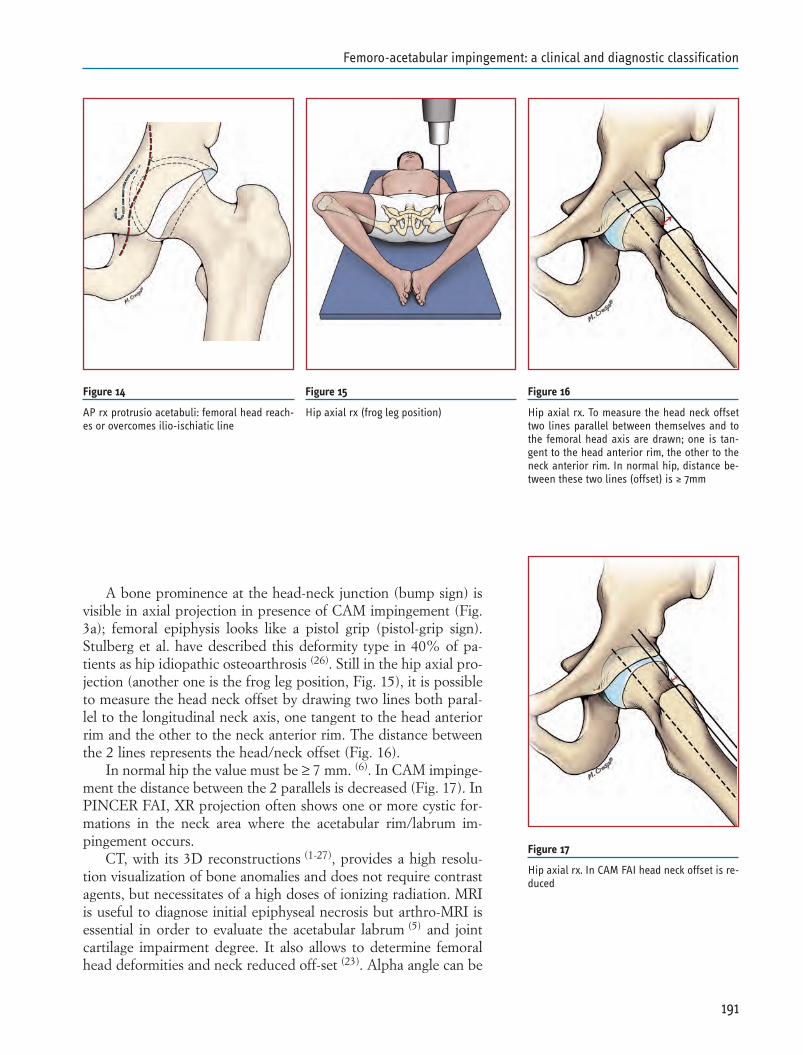
A bone prominence at the head-neck junction (bump sign) isvisible in axial projection in presence of CAM impingement (Fig.3a); femoral epiphysis looks like a pistol grip (pistol-grip sign).Stulberg et al. have described this deformity type in 40% of pa-tients as hip idiopathic osteoarthrosis (26). Still in the hip axial pro-jection (another one is the frog leg position, Fig. 15), it is possibleto measure the head neck offset by drawing two lines both paral-lel to the longitudinal neck axis, one tangent to the head anteriorrim and the other to the neck anterior rim. The distance betweenthe 2 lines represents the head/neck offset (Fig. 16).
In normal hip the value must be ≥ 7 mm. (6). In CAM impinge-ment the distance between the 2 parallels is decreased (Fig. 17). InPINCER FAI, XR projection often shows one or more cystic for-mations in the neck area where the acetabular rim/labrum im-pingement occurs.
CT, with its 3D reconstructions (1-27), provides a high resolu-tion visualization of bone anomalies and does not require contrastagents, but necessitates of a high doses of ionizing radiation. MRIis useful to diagnose initial epiphyseal necrosis but arthro-MRI isessential in order to evaluate the acetabular labrum (5) and jointcartilage impairment degree. It also allows to determine femoralhead deformities and neck reduced off-set (23). Alpha angle can be
191
Femoro-acetabular impingement: a clinical and diagnostic classification
Figure 14
AP rx protrusio acetabuli: femoral head reach-es or overcomes ilio-ischiatic line
Figure 15
Hip axial rx (frog leg position)
Figure 16
Hip axial rx. To measure the head neck offsettwo lines parallel between themselves and tothe femoral head axis are drawn; one is tan-gent to the head anterior rim, the other to theneck anterior rim. In normal hip, distance be-tween these two lines (offset) is ≥ 7mm
Figure 17
Hip axial rx. In CAM FAI head neck offset is re-duced
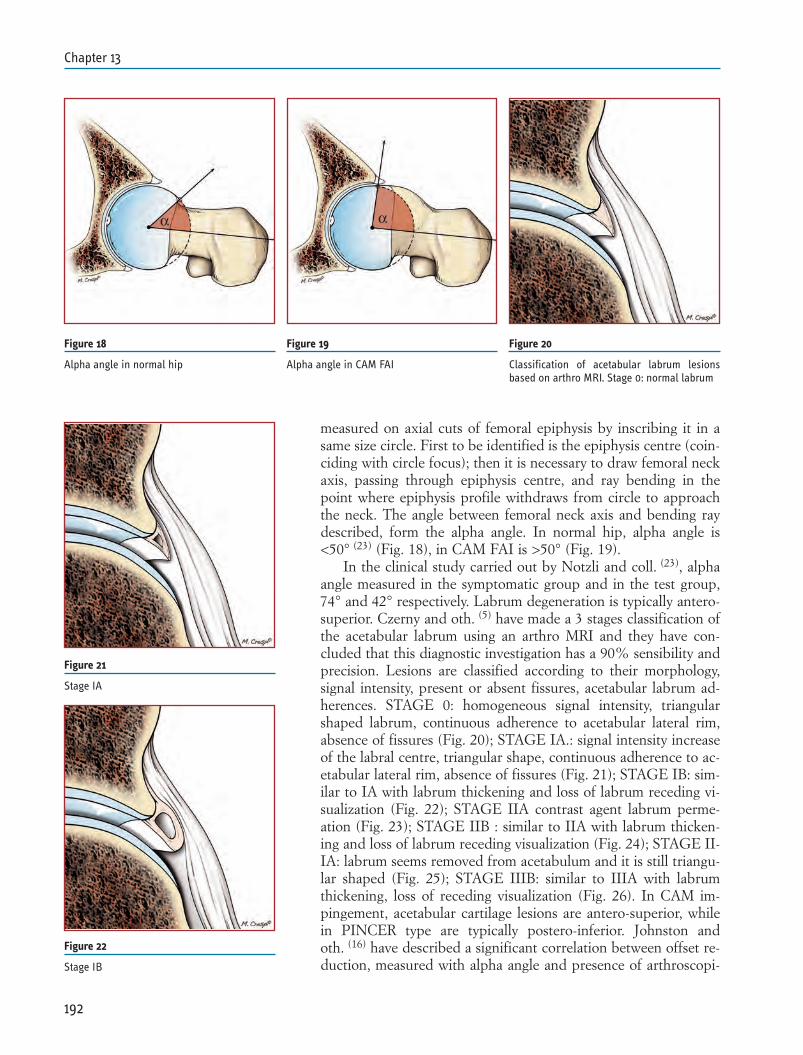
measured on axial cuts of femoral epiphysis by inscribing it in asame size circle. First to be identified is the epiphysis centre (coin-ciding with circle focus); then it is necessary to draw femoral neckaxis, passing through epiphysis centre, and ray bending in thepoint where epiphysis profile withdraws from circle to approachthe neck. The angle between femoral neck axis and bending raydescribed, form the alpha angle. In normal hip, alpha angle is<50° (23) (Fig. 18), in CAM FAI is >50° (Fig. 19).
In the clinical study carried out by Notzli and coll. (23), alphaangle measured in the symptomatic group and in the test group,74° and 42° respectively. Labrum degeneration is typically antero-superior. Czerny and oth. (5) have made a 3 stages classification ofthe acetabular labrum using an arthro MRI and they have con-cluded that this diagnostic investigation has a 90% sensibility andprecision. Lesions are classified according to their morphology,signal intensity, present or absent fissures, acetabular labrum ad-herences. STAGE 0: homogeneous signal intensity, triangularshaped labrum, continuous adherence to acetabular lateral rim,absence of fissures (Fig. 20); STAGE IA.: signal intensity increaseof the labral centre, triangular shape, continuous adherence to ac-etabular lateral rim, absence of fissures (Fig. 21); STAGE IB: sim-ilar to IA with labrum thickening and loss of labrum receding vi-sualization (Fig. 22); STAGE IIA contrast agent labrum perme-ation (Fig. 23); STAGE IIB : similar to IIA with labrum thicken-ing and loss of labrum receding visualization (Fig. 24); STAGE II-IA: labrum seems removed from acetabulum and it is still triangu-lar shaped (Fig. 25); STAGE IIIB: similar to IIIA with labrumthickening, loss of receding visualization (Fig. 26). In CAM im-pingement, acetabular cartilage lesions are antero-superior, whilein PINCER type are typically postero-inferior. Johnston andoth. (16) have described a significant correlation between offset re-duction, measured with alpha angle and presence of arthroscopi-
192
Chapter 13
Figure 18
Alpha angle in normal hip
Figure 19
Alpha angle in CAM FAI
Figure 20
Classification of acetabular labrum lesionsbased on arthro MRI. Stage 0: normal labrum
Figure 21
Stage IA
Figure 22
Stage IB
α α
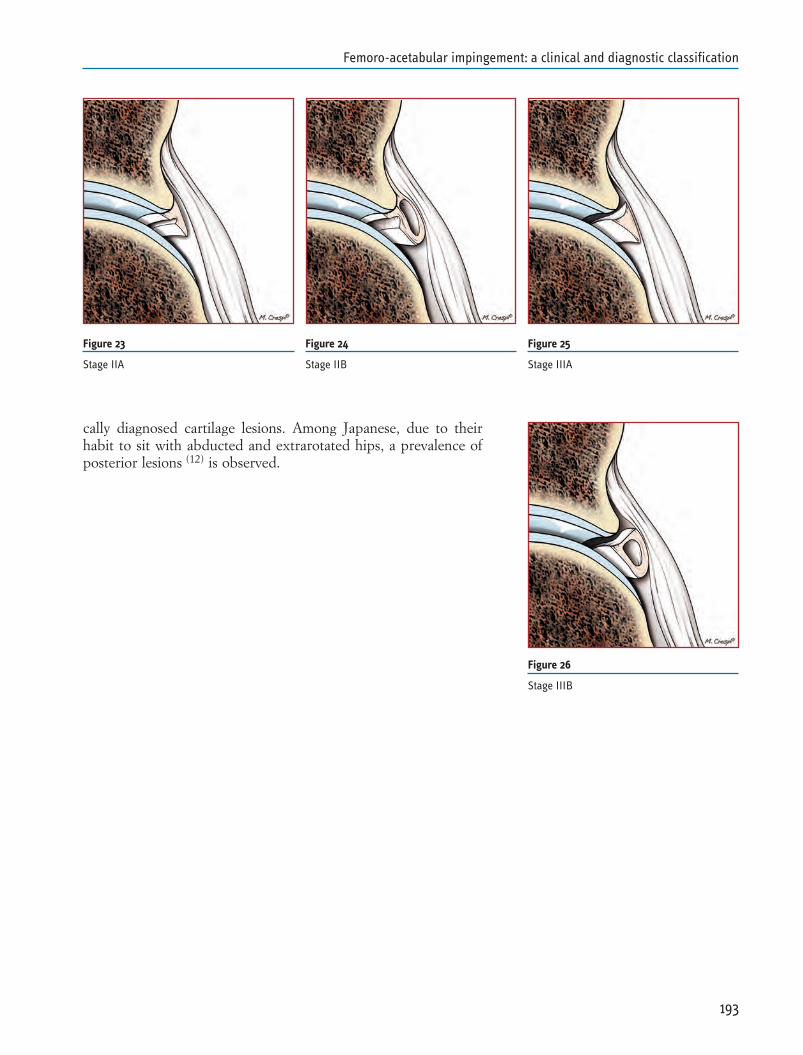
cally diagnosed cartilage lesions. Among Japanese, due to theirhabit to sit with abducted and extrarotated hips, a prevalence ofposterior lesions (12) is observed.
193
Femoro-acetabular impingement: a clinical and diagnostic classification
Figure 23
Stage IIA
Figure 24
Stage IIB
Figure 25
Stage IIIA
Figure 26
Stage IIIB
REFERENCES
1. Beaule PE, Zaragoza E, Motamedi K, Copelan M, Dorey FJ.Three-dimensional computer tomography of the hip in the as-sessment of femoroacetabular impingement. J Orthop Res2005;23:1286-92
2. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influ-ences the pattern of damage to the acetabular cartilage:femoroacetabular impingement as a cause of early osteoarthri-tis of the hip. J Bone Joint Surgery Br 2005;87:1012-1018
3. Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. An-terior femoroacetabular impingiement. Part II. Midterm Re-sults of Surgical Treatment. Clin Orthop Relat Res2004;418:67-73
4. Burnett RS, Della RoccaGJ, Prather H, et al. Clinical presen-tation of patients with tears of acetabular labrum. J Bone JointSurgery Am 2006;88:1448-1457
5. Czerny C, Hofmann S, Neuhold A, Tschauner C, Engel A,Recht MP,Kramer J. Lesion of the acetabular labrum: accuran-cy of MR arthrography in detection and staging. Radiology1996;200:225-30
6. Eijer H, Leunig M, Mahomed MN, Ganz R. Crosstable lateralradiograph for screening of anterior femoral head-neck offsetin patients with femoro-acetabular impingement. Hip Int2001;11:37-41
7. Ekberg O, Persson NH, Abrahamsson PA, et al. Long stand-ing groin pain in athletes: a multidisciplinary approach. SportsMed 1997;31:97
8. Espinosa N, Beck M, Rothenfluh DA, Ganz R, Leunig M.Treatment of femoroacetabular impingement: preliminary re-sults of labral refixation. Surgical technique. J Bone Joint Sur-gery Am 2007;89:36-53
9. Ganz R, Parvizi J, Beck M, Leuning M, Nötzli H, SiebenrockKA. Femoroacetabular impingement: a cause of osteoarthritisof the hip. Clin Orthop 2003;417:112-120
10. Ganz R, Leuning M, Leuning-Ganz K, Harris W. The etiologyof osteoarthritis of the hip: an integrated mechanical concept.Clin Orthop Relat Res 2008;466:264-272
11. Goodman DA, Feighan JE, Smith AD, Latimer B, Buly RL,Cooperman DR. Subclinical slipped capital femoral epiphysis.Relationship to osteoarthrosis of the hip. J Bone Joint SurgeryAm 1997;79:1489-97
12. Hase T, Ueo T. Acetabular labral tear: arthroscopic diagnosisand treatment. Arthroscopy 1999 Mar;15(2):138-41.
13. Hofmann S, Tschauner CH, Graf R. Mechanical causes of os-teoarthritis in young adults. Hip Int 2003;13(Suppl 2):3-9
14. Ito K, Minka MA 2nd, Leuning M, Werlen S, Ganz R.Femoroacetabular impingement and the cam-effect. A MRI-based quantitative anatomical study of the femoral head-neckoffset. J Bone Joint Surgery Br 2001;83:171-176
194
Chapter 13
15. Jamali AA, Miladenov K, Meyer DC, et al. Anteroposteriorpelvic radiographs to assess acetabular retroversion: high va-lidity of the ”cross-over sign”. J Orthop Res 2007;25:758-765
16. Johnston LJ, Schenker ML, Briggs KK, Philippon MJ. Rela-tionship between offset angle alpha and hip chondral injury infemoroacetabular impingement. Arthroscopy 2008 June;6:669-75
17. Kubiak-Langer M, Tanast M, Murphy SB, et al. Range of mo-tion in anterior femoroacetabular impingement. Clin OrthopRelat Res 2007;458:117
18. Lavigne M, Parvizi J, Beck M, Siebenrock KA, Ganz R, Leu-nig M. Anterior femoroacetabular impingement. Part I. Tech-niques of joint preserving surgery. Clin Orthop Relat Res.2004;418:61-6
19. Leuning M, Beaulé PE, Ganz R. The concept of femoroac-etabular impingement. Current status and future prospectives.Clin Orthop Relat Res. 2008 Symposium: femoroacetabular im-pingement: current status of diagnosis and treatment
20. Marc J. Clinical presentation of femoroacetabular impinge-ment. Knee Surg Sports Traumatol Arthrosc 2007;15:1041–1047
21. McCarthy JC, Lee J. Arthroscopic findings in acetabular dys-plasia: a paradigm to evaluate chondral injures. Clin Orthop2002;405:122
22. Meyer DC, Beck M, Ellis T, et al. Comparison of six radi-ographic projections to assess femoral head/neck asphericity.Clin Orthop Relat Res 2006;445:181-185
23. Nötzli HP, Wyss TS, Stoecklin CH, Schmid MR, Treiber K,Jodler J. The contour of the femoral head-neck junction as apredictor for the risk of anterior impingement. J Bone JointSurgery Br 2002;84:556-60
24. Sampson TG. Arthroscopic treatment of femoroacetabular im-pingement: a proposed technique with clinical experience. In-str Course Lect 2006;55:337
25. Siebenrock KA, Shoeniger R, Ganz R. Anterior femoroacetab-ular impingement due to acetabular retroversion. Treatmentwith periacetabular osteotomy. J Bone Joint Surgery Am2003;85:278-286
26. Stulberg SD, Cordell LD, Harris WH, Ramsey PL,MacHewen GD. Unrecognized childhood hip desease: a ma-jor cause of idiopathic osteoarthritis of the hip. In: The Hip.Proc 3rd meeting of The Hip Society. St Luis: CV Mosby Co,1975:212-28
27. Tannast M, Kubiak-Langer M, Langlotz F, et al. Noninvasivethree-dimensional assessment of femoroacetabular impinge-ment. J Orthop Res 2007;25:122
195
Femoro-acetabular impingement: a clinical and diagnostic classification

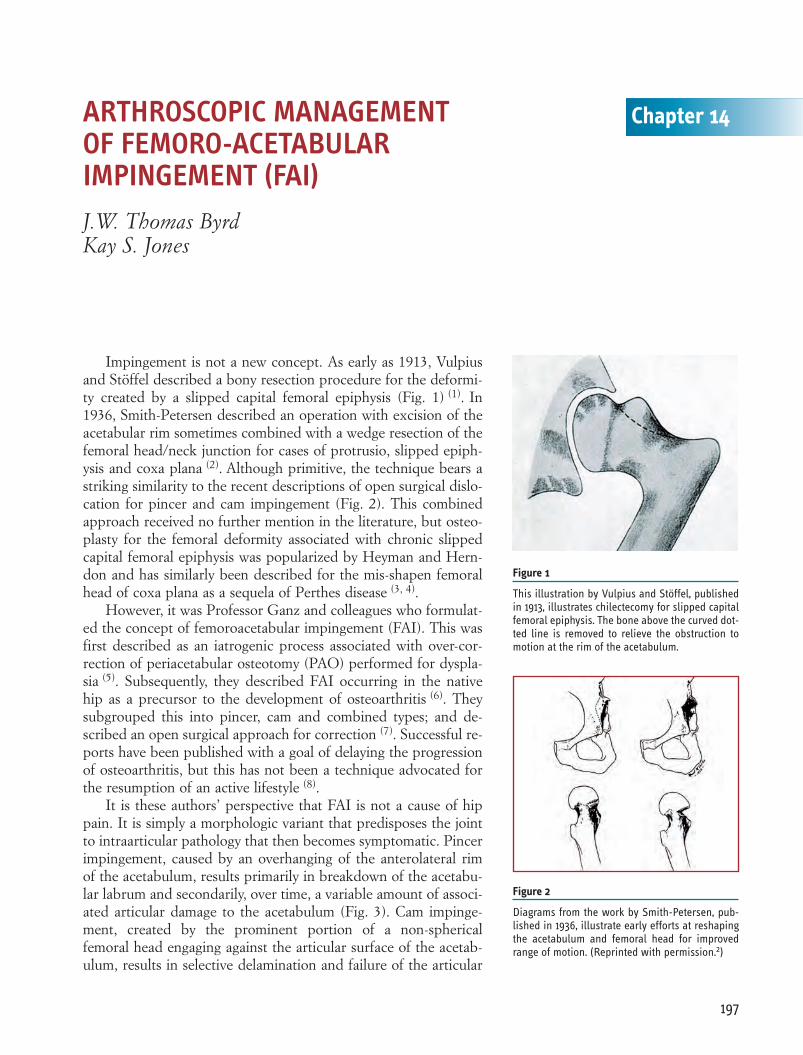
Impingement is not a new concept. As early as 1913, Vulpiusand Stöffel described a bony resection procedure for the deformi-ty created by a slipped capital femoral epiphysis (Fig. 1) (1). In1936, Smith-Petersen described an operation with excision of theacetabular rim sometimes combined with a wedge resection of thefemoral head/neck junction for cases of protrusio, slipped epiph-ysis and coxa plana (2). Although primitive, the technique bears astriking similarity to the recent descriptions of open surgical dislo-cation for pincer and cam impingement (Fig. 2). This combinedapproach received no further mention in the literature, but osteo-plasty for the femoral deformity associated with chronic slippedcapital femoral epiphysis was popularized by Heyman and Hern-don and has similarly been described for the mis-shapen femoralhead of coxa plana as a sequela of Perthes disease (3, 4).
However, it was Professor Ganz and colleagues who formulat-ed the concept of femoroacetabular impingement (FAI). This wasfirst described as an iatrogenic process associated with over-cor-rection of periacetabular osteotomy (PAO) performed for dyspla-sia (5). Subsequently, they described FAI occurring in the nativehip as a precursor to the development of osteoarthritis (6). Theysubgrouped this into pincer, cam and combined types; and de-scribed an open surgical approach for correction (7). Successful re-ports have been published with a goal of delaying the progressionof osteoarthritis, but this has not been a technique advocated forthe resumption of an active lifestyle (8).
It is these authors’ perspective that FAI is not a cause of hippain. It is simply a morphologic variant that predisposes the jointto intraarticular pathology that then becomes symptomatic. Pincerimpingement, caused by an overhanging of the anterolateral rimof the acetabulum, results primarily in breakdown of the acetabu-lar labrum and secondarily, over time, a variable amount of associ-ated articular damage to the acetabulum (Fig. 3). Cam impinge-ment, created by the prominent portion of a non-sphericalfemoral head engaging against the articular surface of the acetab-ulum, results in selective delamination and failure of the articular
197
Chapter 14ARTHROSCOPIC MANAGEMENT OF FEMORO-ACETABULAR IMPINGEMENT (FAI)J.W. Thomas ByrdKay S. Jones
Figure 1
This illustration by Vulpius and Stöffel, publishedin 1913, illustrates chilectecomy for slipped capitalfemoral epiphysis. The bone above the curved dot-ted line is removed to relieve the obstruction tomotion at the rim of the acetabulum.
Figure 2
Diagrams from the work by Smith-Petersen, pub-lished in 1936, illustrate early efforts at reshapingthe acetabulum and femoral head for improvedrange of motion. (Reprinted with permission.2)
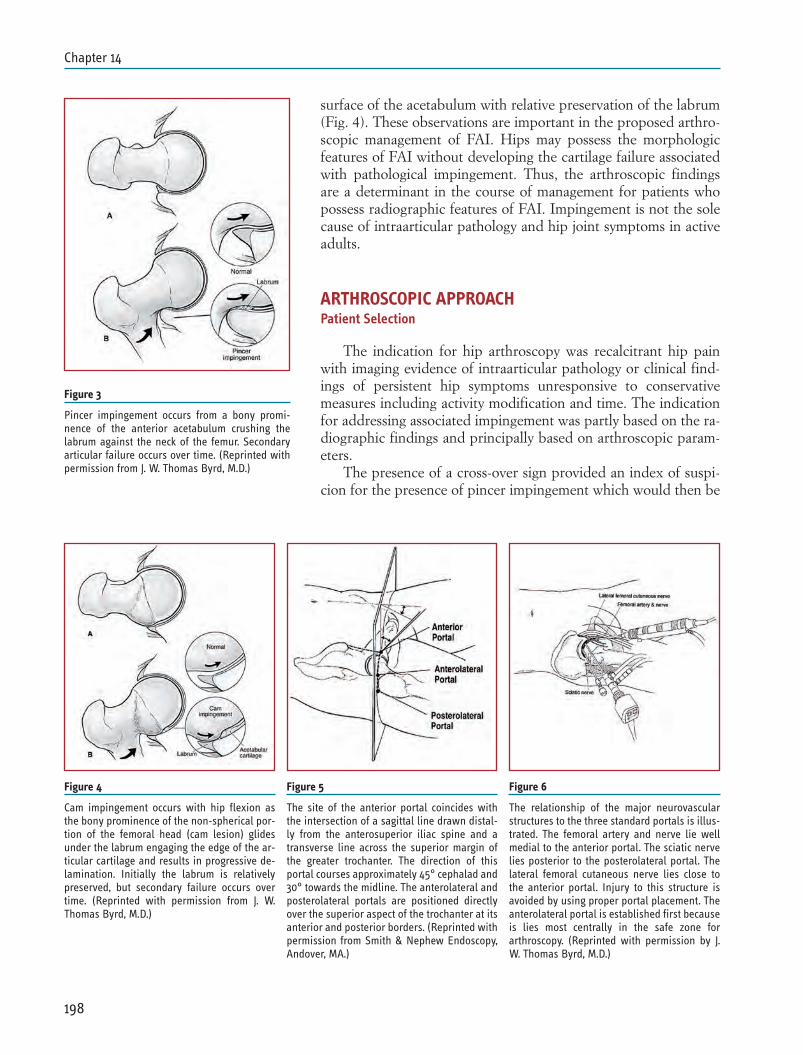
surface of the acetabulum with relative preservation of the labrum(Fig. 4). These observations are important in the proposed arthro-scopic management of FAI. Hips may possess the morphologicfeatures of FAI without developing the cartilage failure associatedwith pathological impingement. Thus, the arthroscopic findingsare a determinant in the course of management for patients whopossess radiographic features of FAI. Impingement is not the solecause of intraarticular pathology and hip joint symptoms in activeadults.
ARTHROSCOPIC APPROACHPatient Selection
The indication for hip arthroscopy was recalcitrant hip painwith imaging evidence of intraarticular pathology or clinical find-ings of persistent hip symptoms unresponsive to conservativemeasures including activity modification and time. The indicationfor addressing associated impingement was partly based on the ra-diographic findings and principally based on arthroscopic param-eters.
The presence of a cross-over sign provided an index of suspi-cion for the presence of pincer impingement which would then be
198
Chapter 14
Figure 4
Cam impingement occurs with hip flexion asthe bony prominence of the non-spherical por-tion of the femoral head (cam lesion) glidesunder the labrum engaging the edge of the ar-ticular cartilage and results in progressive de-lamination. Initially the labrum is relativelypreserved, but secondary failure occurs overtime. (Reprinted with permission from J. W.Thomas Byrd, M.D.)
Figure 5
The site of the anterior portal coincides withthe intersection of a sagittal line drawn distal-ly from the anterosuperior iliac spine and atransverse line across the superior margin ofthe greater trochanter. The direction of thisportal courses approximately 45° cephalad and30° towards the midline. The anterolateral andposterolateral portals are positioned directlyover the superior aspect of the trochanter at itsanterior and posterior borders. (Reprinted withpermission from Smith & Nephew Endoscopy,Andover, MA.)
Figure 6
The relationship of the major neurovascularstructures to the three standard portals is illus-trated. The femoral artery and nerve lie wellmedial to the anterior portal. The sciatic nervelies posterior to the posterolateral portal. Thelateral femoral cutaneous nerve lies close tothe anterior portal. Injury to this structure isavoided by using proper portal placement. Theanterolateral portal is established first becauseis lies most centrally in the safe zone forarthroscopy. (Reprinted with permission by J.W. Thomas Byrd, M.D.)
Figure 3
Pincer impingement occurs from a bony promi-nence of the anterior acetabulum crushing thelabrum against the neck of the femur. Secondaryarticular failure occurs over time. (Reprinted withpermission from J. W. Thomas Byrd, M.D.)
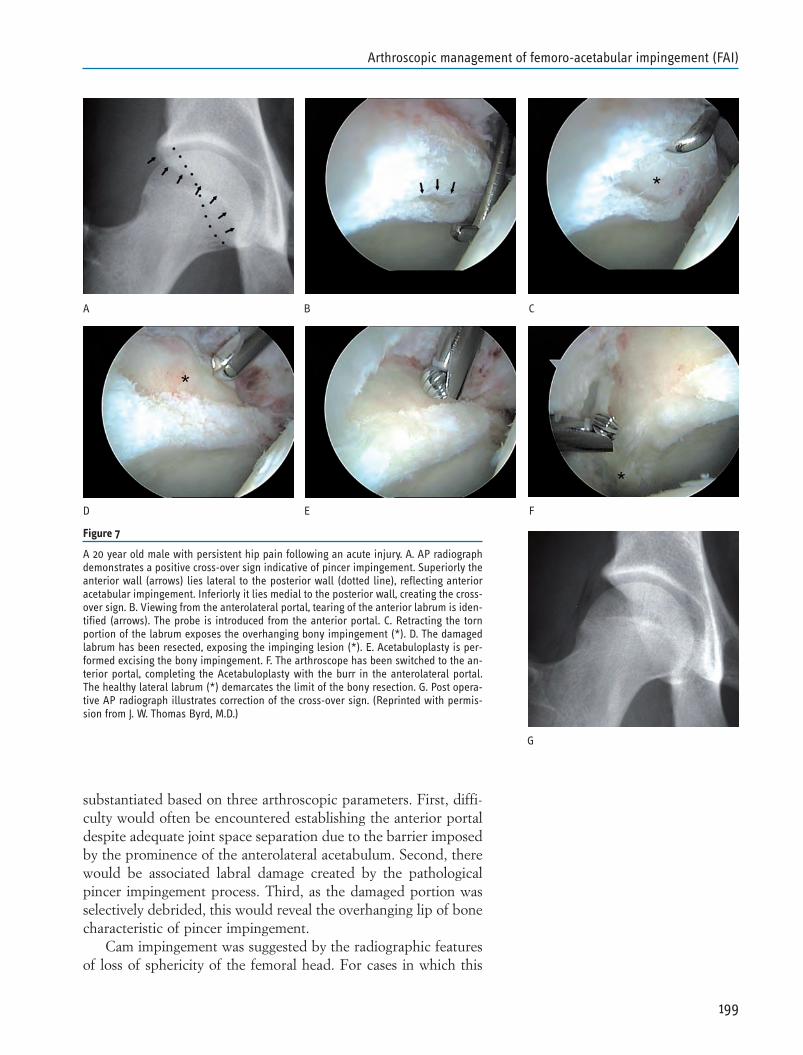
substantiated based on three arthroscopic parameters. First, diffi-culty would often be encountered establishing the anterior portaldespite adequate joint space separation due to the barrier imposedby the prominence of the anterolateral acetabulum. Second, therewould be associated labral damage created by the pathologicalpincer impingement process. Third, as the damaged portion wasselectively debrided, this would reveal the overhanging lip of bonecharacteristic of pincer impingement.
Cam impingement was suggested by the radiographic featuresof loss of sphericity of the femoral head. For cases in which this
199
Arthroscopic management of femoro-acetabular impingement (FAI)
Figure 7
A 20 year old male with persistent hip pain following an acute injury. A. AP radiographdemonstrates a positive cross-over sign indicative of pincer impingement. Superiorly theanterior wall (arrows) lies lateral to the posterior wall (dotted line), reflecting anterioracetabular impingement. Inferiorly it lies medial to the posterior wall, creating the cross-over sign. B. Viewing from the anterolateral portal, tearing of the anterior labrum is iden-tified (arrows). The probe is introduced from the anterior portal. C. Retracting the tornportion of the labrum exposes the overhanging bony impingement (*). D. The damagedlabrum has been resected, exposing the impinging lesion (*). E. Acetabuloplasty is per-formed excising the bony impingement. F. The arthroscope has been switched to the an-terior portal, completing the Acetabuloplasty with the burr in the anterolateral portal.The healthy lateral labrum (*) demarcates the limit of the bony resection. G. Post opera-tive AP radiograph illustrates correction of the cross-over sign. (Reprinted with permis-sion from J. W. Thomas Byrd, M.D.)
A B C
D E F
G
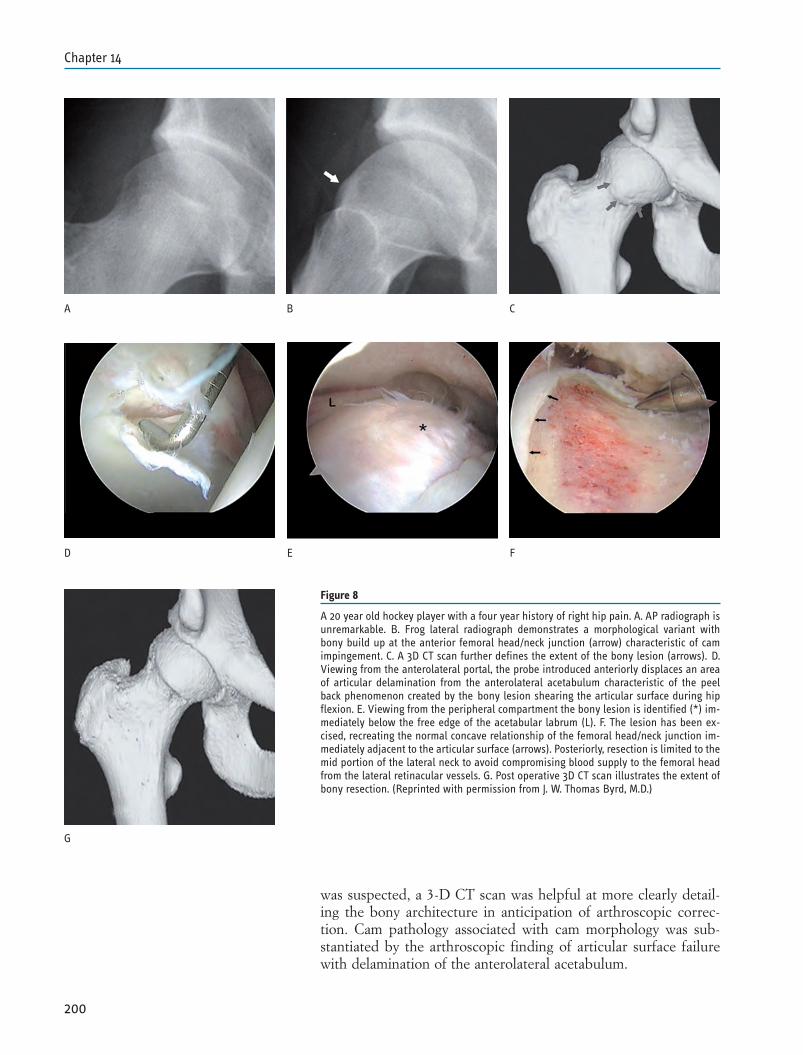
was suspected, a 3-D CT scan was helpful at more clearly detail-ing the bony architecture in anticipation of arthroscopic correc-tion. Cam pathology associated with cam morphology was sub-stantiated by the arthroscopic finding of articular surface failurewith delamination of the anterolateral acetabulum.
200
Chapter 14
Figure 8
A 20 year old hockey player with a four year history of right hip pain. A. AP radiograph isunremarkable. B. Frog lateral radiograph demonstrates a morphological variant withbony build up at the anterior femoral head/neck junction (arrow) characteristic of camimpingement. C. A 3D CT scan further defines the extent of the bony lesion (arrows). D.Viewing from the anterolateral portal, the probe introduced anteriorly displaces an areaof articular delamination from the anterolateral acetabulum characteristic of the peelback phenomenon created by the bony lesion shearing the articular surface during hipflexion. E. Viewing from the peripheral compartment the bony lesion is identified (*) im-mediately below the free edge of the acetabular labrum (L). F. The lesion has been ex-cised, recreating the normal concave relationship of the femoral head/neck junction im-mediately adjacent to the articular surface (arrows). Posteriorly, resection is limited to themid portion of the lateral neck to avoid compromising blood supply to the femoral headfrom the lateral retinacular vessels. G. Post operative 3D CT scan illustrates the extent ofbony resection. (Reprinted with permission from J. W. Thomas Byrd, M.D.)
A B C
D E F
G

Technique
The basic principles developed in the early 1990’s have servedas the foundation for the subsequent establishment of methods ofaddressing femoroacetabular impingement (9, 11). While correctivesurgery has been performed for impingement due to post-trau-matic osteophytes since early in the development of the technique,femoroacetabular impingement as a formal indication has been in-corporated only since 2003 (12, 15).
Pincer impingement is addressed from the central compart-ment using the standard supine 3-portal technique (anterior, an-terolateral and posterolateral) that has been previously described(Figs. 5-7)(11, 12). After completely inspecting the joint, attention isturned to the labral lesion. Selective debridement of the damagedportion will reveal the overhanging lip of bone instead of the nor-mal capsular reflection from the labrum. Once the damaged tissuehas been removed, exposing the pincer lesion, the bone is then re-contoured with a spherical burr. Generous capsulotomies aroundthe portals facilitate maneuverability and access. The pincer lesionis addressed switching the arthroscope and instrumentation be-tween the anterior and anterolateral portals. Proximally, the boneis resected flush with the anterior column of the acetabulum. Theanteromedial and lateral extent of the bony resection is dictatedby the margin of healthy labrum. The bone is recontoured to cre-ate a smooth transition with the healthy portion of the labrum,which is preserved. A variable amount of associated secondary ar-ticular damage may be present which is addressed with a chon-droplasty or microfracture for Grade IV lesions.
Addressing cam impingement begins with arthroscopy of thecentral compartment where the presence of cam pathology is doc-umented (Figs. 8 and 9). The characteristic feature is articular fail-ure of the anterolateral acetabulum. Depending on the location ofthe cam lesion, the articular damage may be more anterior or lat-eral. The classic example is articular delamination beginning at itsjunction with the base of the labrum. Often this is a full thicknessGrade IV lesion although sometimes it may be a deep Grade IIIlesion. In early disease, there may be a substantial area of closedGrade I articular blistering, but this must be distinguished fromsimple articular softening which can be a normal variation in theconsistency of the surface. There is often associated failure of thelabrum at its base, but there is a disproportionate amount of artic-ular abnormality relative to the labral pathology. The articulardamage is addressed with chondroplasty and microfracture as dic-tated by its severity. The associated labral pathology is conserva-tively debrided, creating a stable edge. Debridement can selective-ly be limited to the articular side of the labrum, allowing preserva-tion of its capsular surface, maintaining much of the labral sub-stance.
After completing arthroscopy of the central compartment, thecam lesion is addressed from the peripheral compartment. Thereare numerous variations on how this can be accessed for address-
201
Arthroscopic management of femoro-acetabular impingement (FAI)
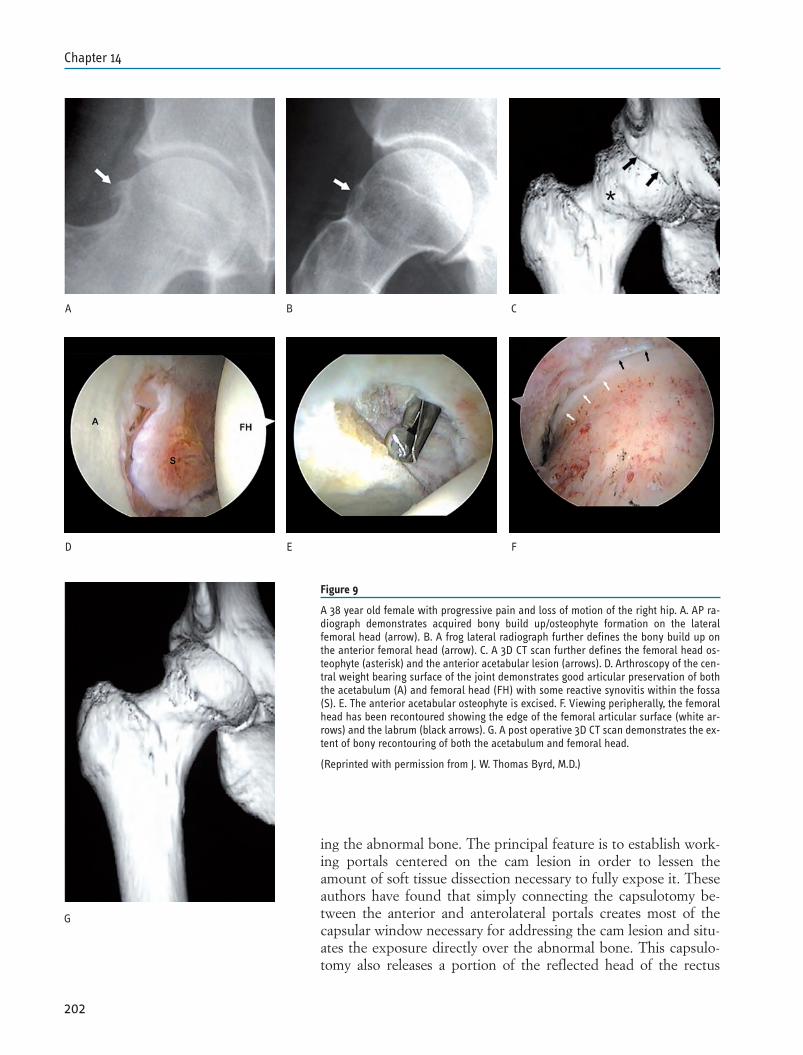
ing the abnormal bone. The principal feature is to establish work-ing portals centered on the cam lesion in order to lessen theamount of soft tissue dissection necessary to fully expose it. Theseauthors have found that simply connecting the capsulotomy be-tween the anterior and anterolateral portals creates most of thecapsular window necessary for addressing the cam lesion and situ-ates the exposure directly over the abnormal bone. This capsulo-tomy also releases a portion of the reflected head of the rectus
202
Chapter 14
Figure 9
A 38 year old female with progressive pain and loss of motion of the right hip. A. AP ra-diograph demonstrates acquired bony build up/osteophyte formation on the lateralfemoral head (arrow). B. A frog lateral radiograph further defines the bony build up onthe anterior femoral head (arrow). C. A 3D CT scan further defines the femoral head os-teophyte (asterisk) and the anterior acetabular lesion (arrows). D. Arthroscopy of the cen-tral weight bearing surface of the joint demonstrates good articular preservation of boththe acetabulum (A) and femoral head (FH) with some reactive synovitis within the fossa(S). E. The anterior acetabular osteophyte is excised. F. Viewing peripherally, the femoralhead has been recontoured showing the edge of the femoral articular surface (white ar-rows) and the labrum (black arrows). G. A post operative 3D CT scan demonstrates the ex-tent of bony recontouring of both the acetabulum and femoral head.
(Reprinted with permission from J. W. Thomas Byrd, M.D.)
A B C
D E F
G

femoris. The posterolateral portal can be removed and the anteri-or and anterolateral portals are simply backed out of the centralcompartment. The traction is released, and the hip flexed approx-imately 35°. Failure to adequately create the capsulotomy beforereleasing the traction can result in the instrumentation being teth-ered proximally and hinders maneuverability in the periphery. Asthe hip is flexed under arthroscopic visualization, the line of de-marcation between healthy cartilage and abnormal fibrocartilagethat covers the cam lesion can usually be identified. Flexing thehip so that this line of demarcation is just below the rim of the ac-etabulum allows the acetabulum to be partly used as a template indetermining the circumferential line of resection adjacent to thearticular surface. Excessive flexion will cause a portion of the camlesion to disappear underneath the acetabulum and result in inad-equate resection.
A cephalad anterolateral portal is established approximately5cm above the anterolateral portal, entering through the capsulo-tomy that has already been established. These proximal and distalanterolateral portals work well for accessing and addressing thecam lesion. The anterior portal can be removed or maintained if itis needed for better access to the medial side of the femoral neck.
Most of the work for performing the recontouring of the camlesion (femoroplasty) lies in the soft tissue preparation. This in-cludes capsular debridement as necessary to assure complete visu-alization of the lesion and then removal of the fibrocartilage andscar that covers the abnormal bone. With the hip flexed, the prox-imal portal provides better access for the lateral and posterior por-tion, while the distal portal is more anterior relative to the jointand provides best access for the anterior part of the lesion. Thelateral synovial fold is identified as the arthroscopic landmark forthe retinacular vessels and care is taken to preserve this structureduring the recontouring. Switching between the portals is impor-tant to fully appreciate the three-dimensional anatomy of the re-contouring. Trying to complete the work with the arthroscope in asingle portal without switching heightens the risk of creating a pla-nar resection and not recreating the spherical anatomy.
Once the bone has been fully exposed, recontouring is per-formed with a spherical burr. Initial bony resection is performedat the articular junction to fully demarcate the line of resection aswell as its depth. The resection is then tapered distally to make itflush with the natural neck of the femur. Particular attention isgiven to make sure that the bony resection is adequate, but doesnot notch the femoral neck or leave a potential stress riser. Theseauthors begin the resection at the lateral/posterior limit of the camlesion with the arthroscope in the more distal portal and instru-mentation in the more proximal portal. The posterior extent ofthe resection is usually the most difficulty; the resection is also themost critical to avoid notching the tensile surface of the femoralneck; and particular attention must be given to avoiding and pre-serving the lateral retinacular vessels. Then, switching the arthro-
203
Arthroscopic management of femoro-acetabular impingement (FAI)

scope to the proximal portal, the burr is introduced distally andthe reshaping is completed along the anterior head and neck junc-tion. Lastly attention is given to make sure that all bone debris isremoved as thoroughly as possible to lessen the likelihood of de-veloping heterotopic ossification.
Rehabilitation
Formal supervised physical therapy begins within one or twodays following surgery. The protocol is variable depending on thepathology encountered and procedure performed. In general, anemphasis is on optimizing range of motion with early implementa-tion of closed chain joint stabilization and core strengthening ex-ercises.
With acetabuloplasty, weightbearing is allowed as tolerated.Crutches are used for approximately one week until the gait pat-tern is normalized as dictated by the accompanying pain from theprocedure. With femoroplasty, the patient is allowed to weightbear as tolerated but crutches are used for four weeks as a precau-tionary measure against any awkward twisting episodes. Once nor-mal muscle tone and response patterns have been regained, thesewill adequately protect the joint for normal forces. Impact loadingis avoided for three months while the bone fully remodels.
The rehab protocol is modified for microfracture by keepingthe patient on a strict protected weightbearing status for twomonths. The patient is allowed place the weight of their leg on theground which provides optimal neutralization of forces across thejoint.
A formal structured rehab protocol is continued for threemonths. For athletes, functional progression is then advanced astolerated. While some athletes may resume unrestricted activitiesquickly, usually it is anticipated that another one to three monthsare necessary for full participation.
RESULTS
Since 1993, all patients undergoing hip arthroscopy at thiscenter have been prospectively assessed using a modified Harriship score preoperatively and then postoperatively at 3, 12, 24, 60and 120 month (16, 18). Arthroscopic management of femoroac-etabular impingement has been performed in 227 hips in 220 pa-tients (7 bilateral) with minimum 12 month follow up (average 17months). There has been 100% follow up of all patients. The av-erage age was 34 years (range 13-77). There were 148 males and72 females with 130 right and 97 left hips. The average improve-ment was 21 points (preop 66; postop 87) with 85% improved atmost recent follow up. The results over time are outlined in Fig.10 with continued improvement noted throughout the first yearand results maintained in those with two-year follow up. Overall,using the Harris classification, there were 88 excellent, 99 good,
204
Chapter 14
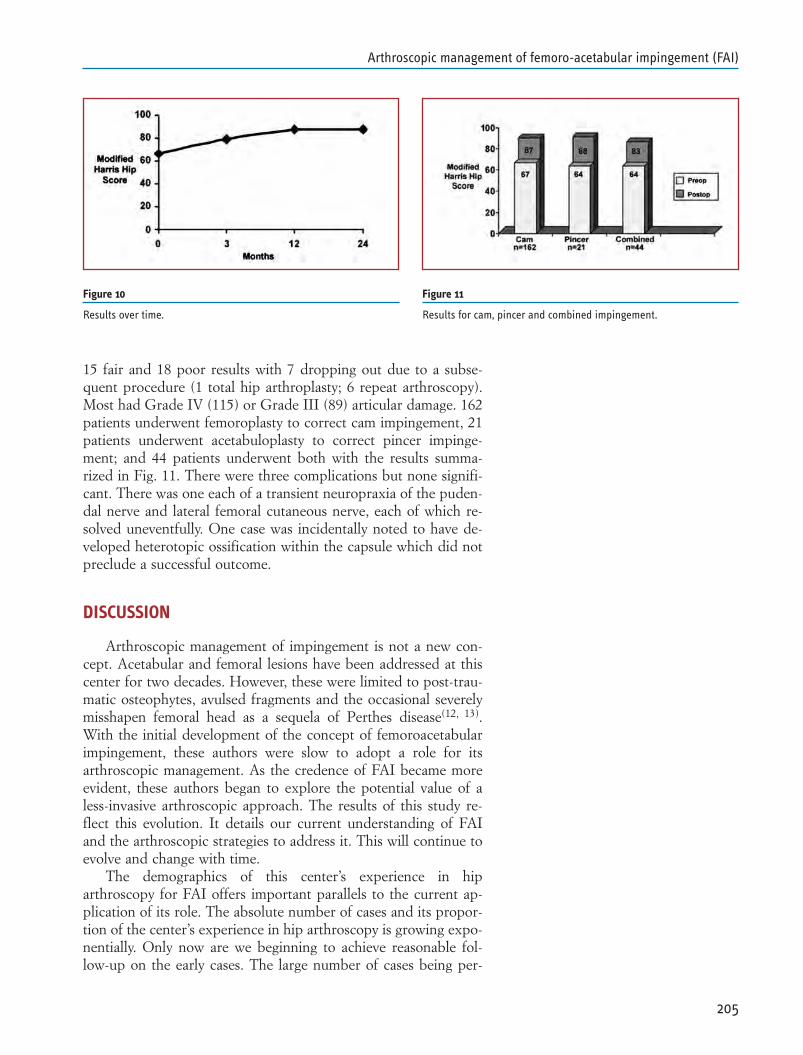
15 fair and 18 poor results with 7 dropping out due to a subse-quent procedure (1 total hip arthroplasty; 6 repeat arthroscopy).Most had Grade IV (115) or Grade III (89) articular damage. 162patients underwent femoroplasty to correct cam impingement, 21patients underwent acetabuloplasty to correct pincer impinge-ment; and 44 patients underwent both with the results summa-rized in Fig. 11. There were three complications but none signifi-cant. There was one each of a transient neuropraxia of the puden-dal nerve and lateral femoral cutaneous nerve, each of which re-solved uneventfully. One case was incidentally noted to have de-veloped heterotopic ossification within the capsule which did notpreclude a successful outcome.
DISCUSSION
Arthroscopic management of impingement is not a new con-cept. Acetabular and femoral lesions have been addressed at thiscenter for two decades. However, these were limited to post-trau-matic osteophytes, avulsed fragments and the occasional severelymisshapen femoral head as a sequela of Perthes disease(12, 13).With the initial development of the concept of femoroacetabularimpingement, these authors were slow to adopt a role for itsarthroscopic management. As the credence of FAI became moreevident, these authors began to explore the potential value of aless-invasive arthroscopic approach. The results of this study re-flect this evolution. It details our current understanding of FAIand the arthroscopic strategies to address it. This will continue toevolve and change with time.
The demographics of this center’s experience in hiparthroscopy for FAI offers important parallels to the current ap-plication of its role. The absolute number of cases and its propor-tion of the center’s experience in hip arthroscopy is growing expo-nentially. Only now are we beginning to achieve reasonable fol-low-up on the early cases. The large number of cases being per-
205
Arthroscopic management of femoro-acetabular impingement (FAI)
Figure 10
Results over time.
Figure 11
Results for cam, pincer and combined impingement.

formed based only on modest preliminary results emphasizes anelement of caution. The hope is that greater experience will onlylead to better outcomes, but time will tell.
In this series of impingement cases, these authors report a dis-proportionate prevalence of cam lesions. This is probably influ-enced by the criteria upon which surgical correction is based. Ifthe labrum is intact, then the patient does not have pincer pathol-ogy. For a patient with a positive cross-over sign and a healthylabrum, these authors have been hesitant to take down normal tis-sue in order to correct a radiographic variant based on the con-ceptual concern that this variant is bad, even in the absence ofjoint pathology. While the labrum can be refixed, its appearancewill never come close to that of the native uninjured tissue.
These authors question, although do not discount, the radi-ographic indices of pincer morphology. It is unclear what rele-vance the radiographic measures of a properly centered supinexray have in relation to the way that an individual orients thepelvis with functional weightbearing activities. Many factors mayinfluence an individual’s pelvic orientation. A singular example isvariability of lumbar kyphosis or lordosis that can accentuatepelvic flexion or extension and significantly alter functional over-or under-coverage from the acetabulum. As difficult as it is to ob-tain a properly centered, standardized supine AP radiographicview of the pelvis, attempting to accomplish this with a standingradiograph would be fraught with even greater inconsistenciesand thus is unlikely to be better suited to assessing functionallyrelevant radiographic indices.
In relation to this report there are four important questions.First, does surgical correction (open or arthroscopic) of femoroac-etabular impingement result in successful outcomes? There is am-ple data that, using various outcomes instruments, a significantportion of patients are improved by surgical intervention.
A second question is whether surgical correction of femoroac-etabular impingement alters the natural history of this disorder.While successful results have been reported, in absence of a truecontrol cohort in whom the disorder is untreated, this questioncannot be answered with scientific validity.
Third, how do the results of arthroscopic management com-pare to those of the open method? Clearly, arthroscopy offers amuch less invasive technique, lower risks of complications, and aneasier recovery without hospitalization. However, is it as effective?While there are no single institution studies that compare openversus arthroscopic methods, the literature increasingly supportsthat, in properly selected cases, successful results can be accom-plished with arthroscopic techniques. Visualization and assess-ment of the adequacy of recontouring is more complete with anopen approach. With proper patient selection and planning, it ap-pears that the arthroscopic methodology can come close to ac-complishing this recontouring with the precision that has beendocumented with open surgery. Aided by computed 3-D tomogra-
206
Chapter 14

phy which serves as a road map for the arthroscopic surgeon,planning and performance of the recontouring can be successfullyaccomplished.
The fourth and final question is: Does the arthroscopic correc-tion of underlying impingement lead to superior results versusarthroscopy simply addressing the soft tissue pathology alone?Clearly, correction of the underlying impingement represents amore extensive surgical undertaking with potentially greater prob-lems. There are no randomized studies comparing the results ofarthroscopy with and without correction of the impingement.However, in this center, there is ample historical data containedwithin a 15 year database from which to answer this question.There are many patients who underwent arthroscopy prior to rec-ognizing FAI as an entity, and in whom this was not corrected.This study will be a separate undertaking in which all of these re-tained records must be reviewed in order to obtain a matchedcontrol cohort of patients with impingement in whom this was notcorrected. Stay tuned.
With these questions posed, here is what this author’s data re-flects. Early experience in arthroscopic management of femoroac-etabular impingement has resulted in 83% good and excellent re-sults. This cohort represents more advanced pathology with 90%Grade IV (115) and Grade III (89) articular damage. Overall 85%were improved with only one (0.4%) requiring conversion to a to-tal hip arthroplasty. These results compare favorably to outcomesreported with open surgical dislocation including Beck, et al, whodescribed 68% successful outcomes with 26% conversion to totalhip arthroplasty and Murphy, et al, who described 65% successfuloutcomes with 30% conversion to arthroplasty(8, 19)
This data substantiates the role of arthroscopy in the manage-ment of femoroacetabular impingement. With ongoing data col-lection, better prognostic indicators can be identified to more pre-cisely select patients in whom a favorable outcome can be expect-ed. However, as the technique is further refined and can be per-formed with even less morbidity, this option may be offered tomore marginal candidates in whom the alternatives are limited.Thus, it is difficult to forecast how these results may change withgrowing experience but this current data justifies its role with cur-rent applications.
CONCLUSIONS
Many patients with femoroacetabular impingement may beappropriately suited for arthroscopic management. Successful out-comes can be expected in the majority of cases but requires metic-ulous attention to the details of the procedure. There are severalmerits to the arthroscopic method. As a less invasive procedure, itis performed on an outpatient basis with few complications andfacilitates the postoperative rehabilitation. The arthroscopic pro-cedure may be better suited for individuals returning to an active
207
Arthroscopic management of femoro-acetabular impingement (FAI)

lifestyle. Also, imaging studies may underestimate the severity ofarticular loss which may only become evident during arthroscopyand, again, may be better suited for this less invasive method inthe presence of occult advanced disease.
208
Chapter 14
REFERENCES
1. Vulpius O, Stöffel A: Orthopäadische Operationslehre.Stuttgart, F. Enke, 1913.
2. Smith-Petersen MN: Treatment of malum coxae senilis, oldslipped upper femoral epiphysis, intrapelvic protrusion of theacetabulum, and coxa plana by means of acetabuloplasty. JBone Joint Surg Am. 1936;18:869-880.
3. Heyman CH, Herndon CH: Slipped femoral epiphysis withsevere displacement: a conservative operative treatment. JBone Joint Surg Am. 1957;39:293-413.
4. Garceau GJ: Surgical treatment of coxa plana. J Bone JointSurg Br. 1964;46:779-780.
5. Myers SR, Eijer H, Ganz R: Anterior femoroacetabular im-pingement after periacetabular osteotomy. Clin Orthop 1999;363; 81-92.
6. Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, SiebenrockKA: Femoroacetabular impingement: a cause for osteoarthritisof the hip. Clin Orthop 2003: 417;112-120.
7. Lavigne M, Parvizi J, Beck M, Siebenrock KA, Ganz R, Leu-nig M: Anterior femoroacetabular impingement: part I. Tech-niques of joint preserving surgery. Clin Orthop 2004; 418; 61-66.
8. Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R: An-terior femoroacetabular impingement: part II. Midterm resultsof surgical treatment. Clin Orthop 2004:418;67-73.
9. Byrd JWT: Hip Arthroscopy Utilizing the Supine Position,Arthroscopy, 10(3):275-280;1994.
10. Byrd JWT: The Supine Approach. In Byrd JWT (ed) Opera-tive Hip Arthroscopy Second Edition, New York, Springer,2005, 145-169.
11. Byrd, JWT: Hip Arthroscopy: The Supine Position. In IrelandML (Ed): Instr Course Lect. Sports Medicine, 2005;5:235-244.
12. Byrd JWT: Indications and Contraindications. In Byrd JWT(ed) Operative Hip Arthroscopy, New York, Thieme, 1998, 7-24.
13. Byrd JWT: Arthroscopy of Select Hip Lesions. In Byrd JWT(ed) Operative Hip Arthroscopy, New York, Thieme, 1998,153-170.
14. Byrd JWT: Hip Arthroscopy: Evolving Frontiers: Op Tech inOrthop. Special issue: Novel Techniques in Hip Surgery,Beaule PE, Garbuz DS (eds), 14(2):58-67;2004.
15. Byrd JWT: Hip morphology and related pathology. In John-son, DH and Pedowitz, RA: Practical Orthopaedic SportsMedicine & Arthroscopy, Lippincott Williams & Wilkins,Pennsylvania, 2007, 491-503.
16. Byrd JWT, Jones KS: Prospective Analysis of Hip Arthroscopywith Two Year Follow Up. Arthroscopy, 16(6):578-587;2000.
17. Byrd JWT, Jones KS: Prospective analysis of hip arthroscopywith five year follow up. Arthroscopy 19(6):88;2003.
209
Arthroscopic management of femoro-acetabular impingement (FAI)

18. Byrd JWT, Jones KS: Prospective analysis of hip arthroscopywith ten year follow up. Presented at AAOS 74th AnnualMeeting, San Diego, CA February 16, 2007.
19. Murphy S, Tannast M, Kim YJ, Buly R, Millis MD: Debride-ment of the adult hip for femoroacetabular impingement. In-dications and preliminary clinical results. Clin Orthop.429;178-181;2004.
210
Chapter 14

ABSTRACT
Femoroacetabular impingement (FAI) has been recently rec-ognized as a cause of hip pain, labral pathology, chondral damage,and eventually osteoarthritis in the hip patient. Historically, treat-ment for FAI consisted of an open approach with surgical disloca-tion. The operative trauma sustained during the open procedurecombined with the lengthy long-term rehabilitation requirementsplace large limitations on this approach and encourages the devel-opment of a less invasive technique. As a result, an arthroscopicapproach to treat FAI has been developed and the purpose of thischapter is to report this approach for the treatment of both camand pincer-type impingement in the hip.
INTRODUCTION
Femoroacetabular impingement (FAI) has been recently re-vealed as a significant cause of hip pain and as a predictor of ear-ly onset hip osteoarthritis (1, 2, 3). This term describes the underly-ing structural abnormalities in bony morphology, which may alterthe force distribution in the joint and can potentially cause injuryto the capsulolabral structure and articular cartilage.
The concept of FAI has been defined by Ganz and col-leagues (4, 5, 6). In this condition, a structural or spatial abnormali-ty of the femur (cam) or acetabulum (pincer) damages the chon-drolabral structures during normal joint movement. Cam impinge-ment occurs when an abnormally shaped femoral head contacts anormal acetabulum. Pincer impingement involves a normalfemoral head contacting an abnormally shaped, deep, or retrovert-ed acetabulum. The patterns of labral and chondral injury result-ing from the impingement appear to be unique to the distinct typeof impingement (5). In cam impingement, the osseous prominence(“bump”) at the proximal femoral head-neck junction or de-creased head-neck offset produces a shearing force, displacing thelabrum towards the capsule and the adjacent articular cartilage in-
211
Chapter 15ARTHROSCOPIC TREATMENT OF FEMORO-ACETABULAR IMPINGEMENTMarc J. PhilipponConnor J. HayKaren K. BriggsMara L. Schenker
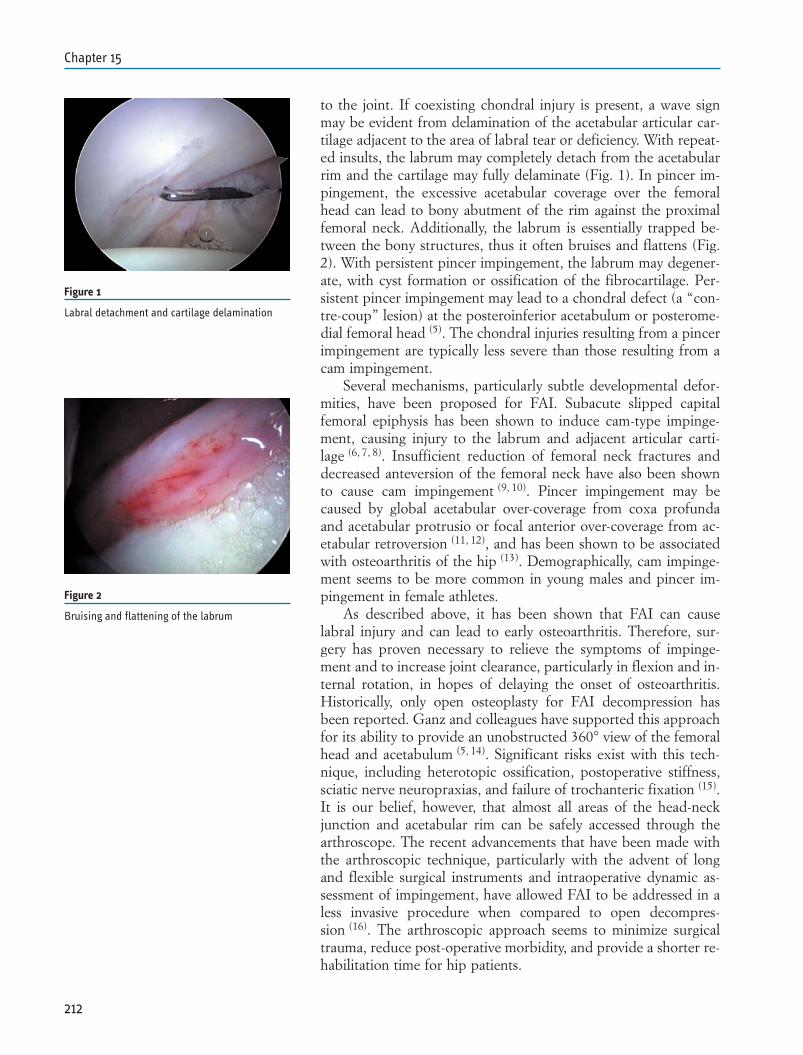
to the joint. If coexisting chondral injury is present, a wave signmay be evident from delamination of the acetabular articular car-tilage adjacent to the area of labral tear or deficiency. With repeat-ed insults, the labrum may completely detach from the acetabularrim and the cartilage may fully delaminate (Fig. 1). In pincer im-pingement, the excessive acetabular coverage over the femoralhead can lead to bony abutment of the rim against the proximalfemoral neck. Additionally, the labrum is essentially trapped be-tween the bony structures, thus it often bruises and flattens (Fig.2). With persistent pincer impingement, the labrum may degener-ate, with cyst formation or ossification of the fibrocartilage. Per-sistent pincer impingement may lead to a chondral defect (a “con-tre-coup” lesion) at the posteroinferior acetabulum or posterome-dial femoral head (5). The chondral injuries resulting from a pincerimpingement are typically less severe than those resulting from acam impingement.
Several mechanisms, particularly subtle developmental defor-mities, have been proposed for FAI. Subacute slipped capitalfemoral epiphysis has been shown to induce cam-type impinge-ment, causing injury to the labrum and adjacent articular carti-lage (6, 7, 8). Insufficient reduction of femoral neck fractures anddecreased anteversion of the femoral neck have also been shownto cause cam impingement (9, 10). Pincer impingement may becaused by global acetabular over-coverage from coxa profundaand acetabular protrusio or focal anterior over-coverage from ac-etabular retroversion (11, 12), and has been shown to be associatedwith osteoarthritis of the hip (13). Demographically, cam impinge-ment seems to be more common in young males and pincer im-pingement in female athletes.
As described above, it has been shown that FAI can causelabral injury and can lead to early osteoarthritis. Therefore, sur-gery has proven necessary to relieve the symptoms of impinge-ment and to increase joint clearance, particularly in flexion and in-ternal rotation, in hopes of delaying the onset of osteoarthritis.Historically, only open osteoplasty for FAI decompression hasbeen reported. Ganz and colleagues have supported this approachfor its ability to provide an unobstructed 360° view of the femoralhead and acetabulum (5, 14). Significant risks exist with this tech-nique, including heterotopic ossification, postoperative stiffness,sciatic nerve neuropraxias, and failure of trochanteric fixation (15).It is our belief, however, that almost all areas of the head-neckjunction and acetabular rim can be safely accessed through thearthroscope. The recent advancements that have been made withthe arthroscopic technique, particularly with the advent of longand flexible surgical instruments and intraoperative dynamic as-sessment of impingement, have allowed FAI to be addressed in aless invasive procedure when compared to open decompres-sion (16). The arthroscopic approach seems to minimize surgicaltrauma, reduce post-operative morbidity, and provide a shorter re-habilitation time for hip patients.
212
Chapter 15
Figure 1
Labral detachment and cartilage delamination
Figure 2
Bruising and flattening of the labrum
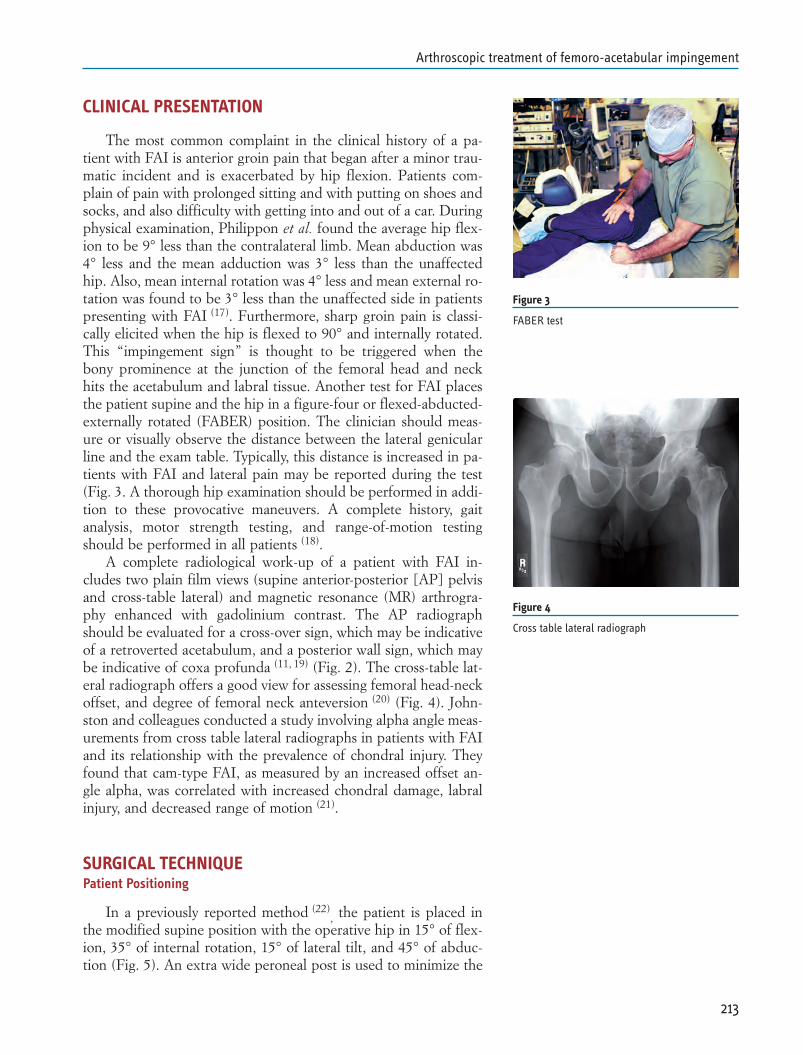
CLINICAL PRESENTATION
The most common complaint in the clinical history of a pa-tient with FAI is anterior groin pain that began after a minor trau-matic incident and is exacerbated by hip flexion. Patients com-plain of pain with prolonged sitting and with putting on shoes andsocks, and also difficulty with getting into and out of a car. Duringphysical examination, Philippon et al. found the average hip flex-ion to be 9° less than the contralateral limb. Mean abduction was4° less and the mean adduction was 3° less than the unaffectedhip. Also, mean internal rotation was 4° less and mean external ro-tation was found to be 3° less than the unaffected side in patientspresenting with FAI (17). Furthermore, sharp groin pain is classi-cally elicited when the hip is flexed to 90° and internally rotated.This “impingement sign” is thought to be triggered when thebony prominence at the junction of the femoral head and neckhits the acetabulum and labral tissue. Another test for FAI placesthe patient supine and the hip in a figure-four or flexed-abducted-externally rotated (FABER) position. The clinician should meas-ure or visually observe the distance between the lateral genicularline and the exam table. Typically, this distance is increased in pa-tients with FAI and lateral pain may be reported during the test(Fig. 3. A thorough hip examination should be performed in addi-tion to these provocative maneuvers. A complete history, gaitanalysis, motor strength testing, and range-of-motion testingshould be performed in all patients (18).
A complete radiological work-up of a patient with FAI in-cludes two plain film views (supine anterior-posterior [AP] pelvisand cross-table lateral) and magnetic resonance (MR) arthrogra-phy enhanced with gadolinium contrast. The AP radiographshould be evaluated for a cross-over sign, which may be indicativeof a retroverted acetabulum, and a posterior wall sign, which maybe indicative of coxa profunda (11, 19) (Fig. 2). The cross-table lat-eral radiograph offers a good view for assessing femoral head-neckoffset, and degree of femoral neck anteversion (20) (Fig. 4). John-ston and colleagues conducted a study involving alpha angle meas-urements from cross table lateral radiographs in patients with FAIand its relationship with the prevalence of chondral injury. Theyfound that cam-type FAI, as measured by an increased offset an-gle alpha, was correlated with increased chondral damage, labralinjury, and decreased range of motion (21).
SURGICAL TECHNIQUEPatient Positioning
In a previously reported method (22), the patient is placed in
the modified supine position with the operative hip in 15° of flex-ion, 35° of internal rotation, 15° of lateral tilt, and 45° of abduc-tion (Fig. 5). An extra wide peroneal post is used to minimize the
213
Arthroscopic treatment of femoro-acetabular impingement
Figure 3
FABER test
Figure 4
Cross table lateral radiograph

risk of pudendal nerve injury. Traction is first applied to break thejoint’s vacuum seal. The leg is then slightly adducted over thepost, thereby venting the capsule and laterally displacing thefemoral head. Additional traction, typically requiring 25 to 50pounds of force, is then required to create approximately 10 mmof joint distraction for safe surgical instrument clearance and fluo-roscopic imaging is utilized to confirm this distraction. Minimalcountertraction is also applied to the contralateral leg to reducethe amount of traction necessary on the operative leg.
Portal placement
Two portals (anterolateral and anterior) are recommended forsafe and adequate decompression of FAI and optimal visualizationfor the treatment of associated intraarticular pathologies (Fig. 6).Using the 70° arthroscope, the anterolateral portal provides a viewof the cental compartment (anterior capsule, labrum, and anteriorchondral surface of the femoral head), iliofemoral ligament, iliop-soas tendon, cotyloid fossa, ligamentum teres, transverse ligament,and most of the acetabulum. The posterosuperior labrum, posteri-or capsule, posterior recess, and ligamentum teres may be visual-ized through the anterior portal. Additionally, the anterior portalprovides a good view of the peripheral compartment, includingthe anterior femoral neck, head-neck junction, zona orbicularis,and distal insertion of the capsular ligaments. Under direct visual-ization, a spinal needle is introduced into the capsule using thezona orbicularis as an anatomic landmark. A guidewire is then in-serted through the spinal needle and a cannulated blunt trochar isused to safely establish the access into the joint.
Cam Procedure
The first step in treating cam impingement is to address the as-sociated intraarticular pathology. This may include labral repair ordebridement, and microfracture chondroplasty of femoral or ac-etabular chondral defects. The next step occurs after the imping-ing lesion has been visualized with the scope in the anterior por-tal. A long motorized shaver is introduced through the lateral por-tal to debride any capsular tissue that may be obstructing a com-plete view of the femoral head-neck junction. Osteoplasty of theimpinging lesion is then performed with a long motorized burrthrough the lateral portal. Throughout the procedure, the hip maybe flexed and extended, abducted and adducted, and internallyand externally rotated to dynamically assess the impinging lesion.In these hip positions, the motorized burr may be used to resectany impinging bone. Caution should be taken when approachingthe anterolateral and posterolateral aspects of the head-neck junc-tion since branches of the medial circumflex artery (lateral retinac-ular vessels) perforate the joint capsule and run along these re-
214
Chapter 15
Figure 5
Modified supine position
Figure 6
Portal placement

gions of the femoral neck (Fig. 7). Understanding the anatomy ofthe vasculature is critical to avoid avascular necrosis following os-teoplasty (23).
The goal of cam debridement is to eliminate the osteophytethat impinges the labrum and acetabular rim, and restore theanatomic sphericity of the femoral head. An obvious concern thathas been raised in FAI decompression is how much bone can beremoved without increasing the risk of femoral neck fracture. Arecent cadaveric study demonstrated that resection of up to 30%of the anterolateral head-neck junction of a morphologically nor-mal femur did not alter the load-bearing capacity (24). A resectionlarger than 30%, however, did result in a decreased load requiredfor fracture. Although this study should be used as a guideline formaximal resection, it is difficult to interpret the results with re-gards to morphologically abnormal head-neck junctions. In ourexperience, burring to a depth of approximately 5-8 mm has beenclinically observed to be a safe and effective procedure.
To assess joint clearance following osteoplasty, the operativehip should be flexed beyond 90° and internally rotated under di-rect visualization through the anterior portal. Furthermore, the legshould be brought into full abduction and again flexed to 90°, andinternally and externally rotated. If impingement is visualized inthis position, further resection of the lesion is needed. Successfuldecompression is concluded when no further impingement be-tween the femoral head-neck, the labrum, and the acetabular rimis observed during the dynamic testing.
Pincer Procedure
Pincer impingement in the hip occurs when the acetabulumprovides anterior over-coverage of the femoral head. The first stepto resecting a pincer lesion is defining the margins by probingwith a flexible instrument. As mentioned above, other clues torecognizing pincer impingement may include observing a bruised,flattened, degenerative, or cystic labrum (5). The amount of rimthat can be safely removed can be determined based on the centeredge angle measurement following radiological workup.
Once the acetabular rim is measured and the margins of a pin-cer lesion have been recognized, a motorized shaver is used toclear all soft tissue from the overhanging acetabulum and to definethe plane between the labrum and the acetabular rim. If the lesionis moderately sized, a motorized burr is inserted into the anteriorportal and the overhang is carefully resected in a “rim trimming”procedure. If the lesion is large, an arthroscopic osteotome may beused through the anterior portal to carefully separate the antero-superior labrum from its insertion on the pincer lesion. The os-teotome is then placed on the anterosuperior acetabulum andsmall portions of the rim are resected until a majority of the lesionhas been removed (Fig. 8). The motorized burr then completesthe resection by reshaping the acetabulum. It is critical to avoid
215
Arthroscopic treatment of femoro-acetabular impingement
Figure 7
Vessels along femoral head and neck

over-resection of the rim to prevent future instability in the pa-tient. If detached during the pincer procedure, the labrum shouldbe reattached to the superior acetabular rim with suture an-chors (21).
In a recent study, we showed that the amount of change incenter edge angle can be accurately predicted based on theamount of acetabulum removed following the treatment of pincer-type impingement (25). Using a regression model, the authorsfound the change in the CE angle could be determined by the fol-lowing formula: Change in CE angle = 2.1 + (0.2 X rim reductionin millimeters). Therefore, five millimeters of bony resectionequals 3.2 degrees change in center edge angle (25).
Following resection of the pincer impingement, it is importantto slide the arthroscope into the peripheral compartment throughthe anterior portal to visualize the head-neck junction. Mixedcam-pincer impingement disorders are a very common finding (1)
and for the best post-operative outcomes, it may be necessary tosurgically address both pathologies.
POST-OPERATIVE MANAGEMENT
After resection of the cam or pincer impingement, autologous-derived platelet gel is injected directly onto the femoral neck to re-duce bleeding and promote early tissue healing. Early range-of-motion exercises are performed within four post-operative hoursto reduce the risk of developing tissue adhesions. Twenty poundsof flat-foot weight-bearing is then recommended for two weeks inpatients undergoing a standard arthroscopy for cam or pincer im-pingement. If microfracture or other chondral work is performed,this may be extended to eight weeks. Special foot boots are wornat night for 14-21 days for abduction and rotation control. A mod-ified brace is used during ambulation for 14-21 post-operativedays for muscle control and slight abduction. A continuous pas-sive motion machine is utilized for two post-operative weeks forfour hours each day. Overall, rehabilitation is crucial to successfuloutcomes following hip arthroscopy (26).
OUTCOMES
We followed 124 patients who underwent arthroscopic treat-ment for femoroacetabular impingement by the senior author be-tween March 2005 and October 2005 (27). These patients were aminimum 2 years from surgery and completed subjective ques-tionnaires at the time of latest follow-up. Their modified Harriship scores improved from 58 pre-operatively to 84 post-operative-ly and their average patient satisfaction was 8.4 out of 10 (27). Fur-thermore, the senior author performed arthroscopic hip surgeryon 16 adolescent athletes between March 2005 and May 2006 (28).
216
Chapter 15
Figure 8
Osteotome used to remove pincer lesion from ac-etabulum
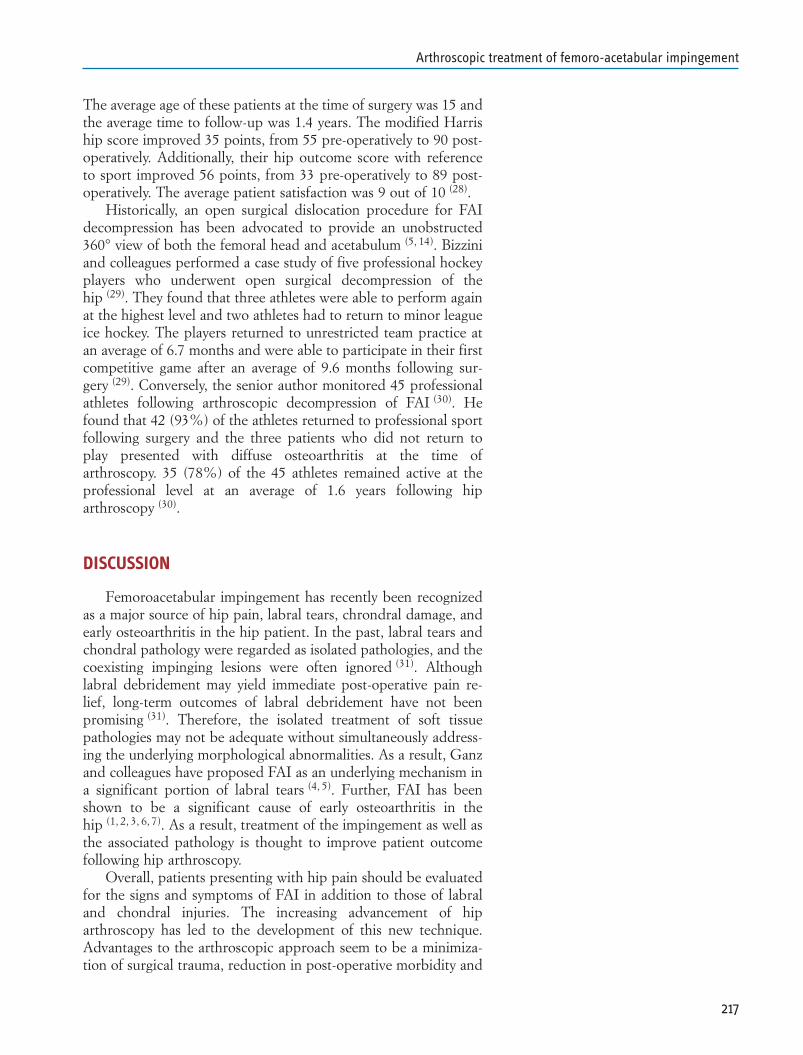
The average age of these patients at the time of surgery was 15 andthe average time to follow-up was 1.4 years. The modified Harriship score improved 35 points, from 55 pre-operatively to 90 post-operatively. Additionally, their hip outcome score with referenceto sport improved 56 points, from 33 pre-operatively to 89 post-operatively. The average patient satisfaction was 9 out of 10 (28).
Historically, an open surgical dislocation procedure for FAIdecompression has been advocated to provide an unobstructed360° view of both the femoral head and acetabulum (5, 14). Bizziniand colleagues performed a case study of five professional hockeyplayers who underwent open surgical decompression of thehip (29). They found that three athletes were able to perform againat the highest level and two athletes had to return to minor leagueice hockey. The players returned to unrestricted team practice atan average of 6.7 months and were able to participate in their firstcompetitive game after an average of 9.6 months following sur-gery (29). Conversely, the senior author monitored 45 professionalathletes following arthroscopic decompression of FAI (30). Hefound that 42 (93%) of the athletes returned to professional sportfollowing surgery and the three patients who did not return toplay presented with diffuse osteoarthritis at the time ofarthroscopy. 35 (78%) of the 45 athletes remained active at theprofessional level at an average of 1.6 years following hiparthroscopy (30).
DISCUSSION
Femoroacetabular impingement has recently been recognizedas a major source of hip pain, labral tears, chrondral damage, andearly osteoarthritis in the hip patient. In the past, labral tears andchondral pathology were regarded as isolated pathologies, and thecoexisting impinging lesions were often ignored (31). Althoughlabral debridement may yield immediate post-operative pain re-lief, long-term outcomes of labral debridement have not beenpromising (31). Therefore, the isolated treatment of soft tissuepathologies may not be adequate without simultaneously address-ing the underlying morphological abnormalities. As a result, Ganzand colleagues have proposed FAI as an underlying mechanism ina significant portion of labral tears (4, 5). Further, FAI has beenshown to be a significant cause of early osteoarthritis in thehip (1, 2, 3, 6, 7). As a result, treatment of the impingement as well asthe associated pathology is thought to improve patient outcomefollowing hip arthroscopy.
Overall, patients presenting with hip pain should be evaluatedfor the signs and symptoms of FAI in addition to those of labraland chondral injuries. The increasing advancement of hiparthroscopy has led to the development of this new technique.Advantages to the arthroscopic approach seem to be a minimiza-tion of surgical trauma, reduction in post-operative morbidity and
217
Arthroscopic treatment of femoro-acetabular impingement

an enhanced recovery. By treating FAI arthroscopically at an earlystage, it is hopeful that osteoarthritis progression will be delayedor completely prevented and long-term results will improve.
218
Chapter 15
REFERENCES
1. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influ-ences the pattern of damage to the acetabular cartilage. J BoneJoint Surg Br 2005; 87-B(7): 1012-1018.
2. Ganz R, Parvizi J, Beck M, et al. Femoroacetabular impinge-ment: a cause for osteoarthritis of the hip. Clin Orthop 2003;417: 112-120.
3. Wagner S, Hofstetter W, Chiquet, et al. Early osteoarthriticchanges of human femoral head cartilage subsequent tofemoro-acetabular impingement. Osteoarthritis Cartilage2003; 11(7): 508-518.
4. Ito K, Minka MA, Leunig M, et al. Femoroacetabular im-pingement and the cam-effect: a mri-based quantitativeanatomical study of the femoral head-neck offset. J Bone JointSurg (Br) 2001; 83-B(2): 171-176.
5. Lavigne M, Parvizi J, Beck M, et al. Anterior femoroacetabu-lar impingement: part 1: techniques of joint preserving sur-gery. Clin Orthop 2004; 418: 61-66.
6. Notzli HP, Wyss TF, Steocklin CH, et al. The contour of thefemoral head-neck junction as a predictor for the risk of ante-rior impingement. J Bone Joint Surg (Br) 2002; 84-B(4): 556-560.
7. Goodman DA, Feighan JE, Smith AD, et al. Subclinicalslipped capital femoral epiphysis: relationship to osteoarthro-sis of the hip. J Bone Joint Surg 1997; 79: 1489-1497.
8. Leunig M, Casillas MM, Hamlet M, et al. Slipped capitalfemoral epiphysis: early mechanical damage to the acetabularcartilage by a prominent femoral metaphysis. Acta OrthopScand 2000; 71(4): 370-375.
9. Siebenrock KA, Wahab KH, Werlen S, et al. Abnormal exten-sion of the femoral head epiphysis as a cause of cam impinge-ment. Clin Orthop 2004; 418: 54-60.
10. Eijer H, Myers SR, Ganz R. Anterior femoroacetabular im-pingement after femoral neck fractures. J Orthop Trauma2001; 15(7): 475-481.
11. Tonnis D, Dortmund, Heinecke A. Acetabular and femoralanteversion: relationship with osteoarthritis of the hip. J BoneJoint Surg 1999; 81-A(12): 1747-1770.
12. Reynolds D, Lucas J, Klaue K. Retroversion of the acetabu-lum: a cause of hip pain. J Bone Joint Surg 1999; 81-B(2): 281-288.
13. Siebenrock KA, Schoeniger R, Ganz R. Anterior femoroac-etabular impingement due to acetabular retroversion: treat-ment with periacetabular osteotomy. J Bone Joint Surg 2003;85-A(2): 278-286.
14. Ganz R, Gill TJ, Gautier E, et al. Surgical dislocation of theadult hip a technique with full access to the femoral head andacetabulum without the risk of avascular necrosis. J Bone JointSurg (Br) 2001; 83(8): 1119-24.
219
Arthroscopic treatment of femoro-acetabular impingement
15. Eijer H, Myers SR, Ganz R. Anterior femoroacetabular im-pingement after femoral neck fractures. J Orthop Trauma2001; 15: 475-481.
16. Philippon MJ, Stubbs AJ, Schenker ML, et al. Arthroscopicmanagement of femoroacetabular impingement: OsteoplastyTechnique and Literature Review. Am J Sports Med 2007;35(9): 1571-1580.
17. Philippon MJ, Maxwell RB, Johnston TL, et al. Clinical pres-entation of femoroacetabular impingement. Knee Surg SportsTraumatol Arthrosc 2007.
18. Kelly BT, Williams RJ, Philippon MJ. Hip arthroscopy: cur-rent indications, treatment options, and management issues.Am J Sports Med 2003; 31(6): 1020-37.
19. Eijer H, Leunig M, Mahomed N, Ganz R. Cross-table lateralradiographs for screening of anterior femoral head-neck offsetin patients with femoroacetabular impingement. Hip Int 2001;11: 37-41.
20. Siebenrock KA, Kalbermatten DF, Ganz R. Effect of pelvic tilton acetabular retroversion: a study of pelves from cadavers.Clin Orthop 2003; 407: 241-248.
21. Johnston TL, Schenker ML, Briggs KK, et al. Relationship be-tween offset angle alpha and hip chondral injury in femoroac-etabular impingement. Arthroscopy 2008; 24(6): 669-675.
22. Kelly BT, Weiland DE, Schenker ML, Philippon MJ. CurrentConcepts: Arthroscopic labral repair in the hip: surgical tech-nique and review of the literature. Arthroscopy 2005; 21(12):1496-504.
23. Gautier E, Ganz K, Krugel N, et al. Anatomy of the medialfemoral circumflex artery and its surgical implications. J BoneJoint Surg (Br) 2000; 82-B(5): 679-83.
24. Lavigne M, Kalhor M, Beck M, et al. Distribution of vascularforamina around the femoral head and neck junction: rele-vance for conservative intracapsular procedures of the hip.Orthop Clin N Am 2005; 36: 171-6.
25. Wolff AB, Philippon MJ, Briggs KK, et al. Acetabular rim re-duction for the treatment of femoroacetabular impingementcorrelates with pre- and post-operative center edge angle.American Academy of Orthopaedic Surgeons Annual Meet-ing, 2009.
26. Wahoff M, Briggs K, Philippon M. Hip arthroscopy rehabili-tation: evidence-based practice. OKU Sports Med Update2009; In Press.
27. Philippon MJ, Briggs KK, Yen YM, et al. Outcomes followinghip arthroscopy for femoroacetabular impingement with asso-ciated chondrolabral dysfunction: minimum two year follow-up. J Bone J Surg Br. 2009; In Press.
28. Philippon MJ, Yen YM, Briggs KK, et al. Early outcomes afterhip arthroscopy for femoroacetabular impingement in the ath-letic adolescent patient: a preliminary report. J Pediatr Orthop2008; 28(7): 705-10.
220
Chapter 15
29. Bizzini M, Notzli H, Maffiuletti N. Femoroacetabular im-pingement in professional ice hockey players: a case series offive athletes after open surgical decompression of the hip. AmJ Sports Med 2007; 35: 1955-1959.
30. Philippon M, Schenker M, Briggs K, et al. Femoroacetabularimpingement in 45 professional athletes: associated patholo-gies and return to sport following arthroscopic decompres-sion. Knee Surg Sports Traumatol Arthrosc 2007.
31. Farjo LA, Glick JM, Sampson TG. Hip arthroscopy for ac-etabular labral tears. Arthroscopy 1999; 15(2): 132-7.
221
Arthroscopic treatment of femoro-acetabular impingement

INTRODUCTION
The first described attempt to hip arthroscopy was made byBurman in 1931, and he stated that “It is manifestly impossible toinsert a needle between the head of the femur and the acetabu-lum”. (Burman 1931)[n1] Advances in hip arthroscopy have comea long way; but compared to the knee and the shoulder technicaladvances have been the much slower for hip arthroscopy. This isdue to the anatomy of the hip joint, which limits arthroscopic ac-cess and manoeuvrability of instruments.
At the same time, significant advances in understanding hippathology have been made in the last years, and actual hypothesisis that small alterations in hip morphology can cause mechanicaldamage with movement over time, leading to early onset of OA.(Ganz 2003, Wenger 2004, Beck 2005, Ganz 2008) The termfemoroacetabular impingement (FAI) is used to describe thesemorphologic alterations, and observations made during open sur-gical treatment for FAI have led to the understanding of thepathology and its mechanism and to the hypothesis that FAI maybe a cause of “primary” OA. (Ganz 2003, Beck 2004, Ito 2001)Surgical dislocation of the hip allowed also for the attribution ofthe various damage patterns within the joint to different FAI mor-phologies. (Beck 2005) Two different types of FAI have been iden-tified, pincer and cam type, although as high as 70% of casesshow a combined form.(Beck 2005, Ganz 2003).
The pincer type is characterized by a local (e.g., acetabularretroversion) or global (e.g., coxa profunda or protrusio) overcov-erage of the acetabulum, and it leads to linear impact of the ac-etabular rim against the head-neck junction. The first structure tofail is the labrum, which degenerates with intrasubstance fissuring,ganglion formation and ossifications. Then the acetabular cartilageadjacent to the involved labrum undergoes degeneration. Withtime, the impact area on the femoral neck shows saddlelike ero-sion. The femoral head cartilage remains uninvolved over a longperiod; only late in the process will there be cartilage abrasion inthe posteroinferior joint, on the head and/or on the acetabulum,
223
Chapter 16HIP ARTHROSCOPY FOR FEMORO-ACETABULAR IMPINGEMENT: PERSONAL TECHNIQUE AND INDICATIONSMichael LeunigNicola Mondanelli Michael SH Kain

called “countercoup lesion”. The cam type is defined by a non-spherical extension of the femoral head which impacts into the ac-etabular cavity. The labrum remains uninvolved over a rather longperiod, while the acetabular cartilage avulses from the labrum it-self and then off the subchondral bone, and often cysts develop atthe head-neck junction. The cartilage of the nonspherical portionof the head (nonweightbearing area) shows surface damage earlyin the disease process, while it is only when the defect on the ac-etabular cartilage is large enough and the femoral head will mi-grate into it, that the cartilage of the spherical portion of the head(weightbearing area) becomes involved (Figs. 1 and 2). AlthoughFAI can take place everywhere around the femoroacetabular joint,the most common site is anterolateral and is produced by internalrotation of the femur in flexion. Pincer impingement is seen morefrequently in middle-aged women with a desire for athletic activi-ties, while cam impingement is more common in young and athlet-ic males. Cam FAI is more destructive than pincer FAI, althoughthe symptoms are often less pronounced: the labrum is known tocontain nociceptive fibers, (Kim 1995) this is the most likely ex-planation for the increased pain reported by women sufferingfrom pincer FAI compared to men with cam FAI.
Being FAI is an intrarticular problem, and being the surgicaldislocation described to treat the problem quite demanding andinvasive, a large interest in arthroscopic treatment of FAI raised.(Sampson 2005, Bare 2005, Weiland 2005, McCarthy 2006,Philippon 2007, Ilizaliturri 2008) Surgical dislocation remains themost effective way to treat FAI and address all the morphologicalproblems. There are many theoretical advantages of hiparthroscopy over open hip surgery if arthroscopy can achieve thesame surgical goals as an open approach. Arthroscopy can bedone as an outpatient or one-night procedure; it eliminates theneed for a large incision, and avoids dislocation, allowing for anearlier recovery and removes the risk of a throcanteric non-union.By avoiding dislocation, hip arthroscopy eliminates the need tocut the ligamentum teres, and although vascular studies demon-strated that the femoral head viability is independent from it,(Beck 2004, Ganz 2001, Gautier 2000, Nötzli 2002) nerve endingsin the ligamentum can play a role in proprioception which is notyet understood. (Leunig 2000) Finally, capsuloligamentous struc-tures are less disrupted, diminishing the risk of post-operative in-stability. (Byrd 1994, Glick 2001, Mccarthy 1995).
Different techniques for hip arthroscopy have been described,as well as different techniques for the arthroscopic treatment ofFAI. Here we present our indications for arthroscopic treatmentof FAI and our actual technique, which consists in a 2-portals ap-proach, starting with central compartment arthroscopy while intraction, and then to focus attention to the peripheral compart-ment, both in traction and after release of it, with patient in thesupine position.
224
Chapter 16
Figure 1
Femoroacetabular impingement: A) normal hip, B)cam FAI, C) pincer FAI, D) combined FAI. (FromLavigne et al.ref)
A
B D
C
Figure 2
Mechanism of lesion of FAI. A, B) pincer type; C, D)cam type. (From Beck et al. ref)
A
C D
B
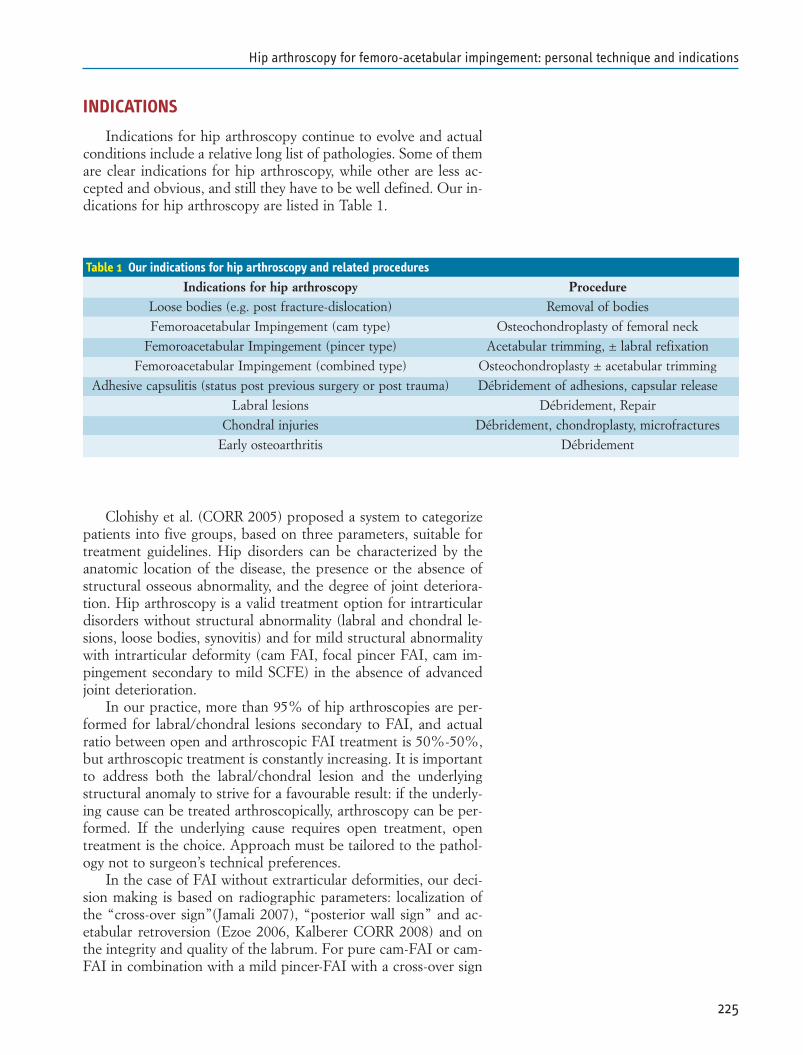
INDICATIONS
Indications for hip arthroscopy continue to evolve and actualconditions include a relative long list of pathologies. Some of themare clear indications for hip arthroscopy, while other are less ac-cepted and obvious, and still they have to be well defined. Our in-dications for hip arthroscopy are listed in Table 1.
Clohishy et al. (CORR 2005) proposed a system to categorizepatients into five groups, based on three parameters, suitable fortreatment guidelines. Hip disorders can be characterized by theanatomic location of the disease, the presence or the absence ofstructural osseous abnormality, and the degree of joint deteriora-tion. Hip arthroscopy is a valid treatment option for intrarticulardisorders without structural abnormality (labral and chondral le-sions, loose bodies, synovitis) and for mild structural abnormalitywith intrarticular deformity (cam FAI, focal pincer FAI, cam im-pingement secondary to mild SCFE) in the absence of advancedjoint deterioration.
In our practice, more than 95% of hip arthroscopies are per-formed for labral/chondral lesions secondary to FAI, and actualratio between open and arthroscopic FAI treatment is 50%-50%,but arthroscopic treatment is constantly increasing. It is importantto address both the labral/chondral lesion and the underlyingstructural anomaly to strive for a favourable result: if the underly-ing cause can be treated arthroscopically, arthroscopy can be per-formed. If the underlying cause requires open treatment, opentreatment is the choice. Approach must be tailored to the pathol-ogy not to surgeon’s technical preferences.
In the case of FAI without extrarticular deformities, our deci-sion making is based on radiographic parameters: localization ofthe “cross-over sign”(Jamali 2007), “posterior wall sign” and ac-etabular retroversion (Ezoe 2006, Kalberer CORR 2008) and onthe integrity and quality of the labrum. For pure cam-FAI or cam-FAI in combination with a mild pincer-FAI with a cross-over sign
225
Hip arthroscopy for femoro-acetabular impingement: personal technique and indications
Table 1 Our indications for hip arthroscopy and related procedures
Indications for hip arthroscopy ProcedureLoose bodies (e.g. post fracture-dislocation) Removal of bodies
Femoroacetabular Impingement (cam type) Osteochondroplasty of femoral neck
Femoroacetabular Impingement (pincer type) Acetabular trimming, ± labral refixation
Femoroacetabular Impingement (combined type) Osteochondroplasty ± acetabular trimming
Adhesive capsulitis (status post previous surgery or post trauma) Débridement of adhesions, capsular release
Labral lesions Débridement, Repair
Chondral injuries Débridement, chondroplasty, microfractures
Early osteoarthritis Débridement

within the superior quarter, we prefer an arthroscopic approachto perform the osteochondroplasty procedure on the femoralhead-neck. If the labrum is intact, the rim is not addressed. If thelabrum is degenerated or ruptured, it is arthroscopically resected.If pure pincer-FAI (both local or global) or prevalent pincer in acombined cam-and-pincer FAI is shown by X-rays and MRI, witha cross-over sign in the second quarter and an intact labrum, asurgical dislocation is preferred. The labrum is detached from thecircumference of the bony rim and reattached after rim trimmingwith anchors, being the arthroscopic approach to the more medi-al and posterior parts of the labrum usually not possible. If a ma-jor structural osseous anomaly is present, a different approachmust be chosen; e.g. if FAI is due to acetabular retroversion, withan inferior cross-over sign, a positive posterior wall sign and a is-chial spine projected into the pelvis, an inverse pelvic osteotomyhas to be considered. (Siebenrock CORR 2003) Finally, in thecase of a patient with FAI, which presents already secondary signsof OA, with degenerative labral and cartilage damage, subchon-dral bone sclerosis and joint space reduction, a hip resurfacingprocedure is considered, via the same surgical dislocation ap-proach.
SURGICAL TECHNIQUESetup of the O.R.
To perform a hip arthroscopy very well organized and in-structed team and dedicated instruments are necessary. Cameraswith 70° and 30° optic must be available, being the first the mostuseful and used during the procedure. The 70° scope is useful tovisualize the periphery of the joint, the acetabular labrum and theinferior portion of the cotyloid fossa, while the 30° scope providesview of the central portion of the acetabulum and of the femoralhead and the superior portion of the fossa, (Dvorak 1990, ByrdTech Orthop 2005) In our practice, for the treatment of FAI wejust need the 70° camera (Karl Storz Endoskope, Tuttlingen, D).
An arthroscopic pump provides significant advantages in thehip. A high flow system allows fluid distension of the joint withoutexcessive pressure being needed. This is important for adequatevisualization and safety, being the risk of fluid extravasation to pe-riarticular tissues and intrabdominal space with higher pressure,while a gravity system does not allow to precisely modulate theflow. We use the FMS duo(r)+ pump (Fluid Management System,DePuy Mitek, Inc., Raynham, MA, USA), which can control in-flow and outflow to maintain a constant pressure, has integratedshaver function or can interface with other current shaver. In ourpractice, we do not establish an outflow portal, as it is not essen-tial. Pump pressure is set at 50 mmHg, and Adrenaline 0.1 mg isadded to every 5L-saline sack to help obtain haemostasis and im-prove visualization.
226
Chapter 16

An image intensifier is useful to help in some steps of the pro-cedure, like distraction of the joint, portal placement, and to eval-uate the degree of bony resection performed. Preoperative APand frog-lateral views are obtained prior to draping the patient fortwo purposes. First, it ensures that good quality images can be ob-tained intra-operatively and secondarily it gives the surgeon a ref-erence for comparison of any bony resection.
Dedicated instruments for hip arthroscopy are helpful andneed to be available. Regular knee or shoulder instruments can beused but occasionally they are too short, both in larger patientsand when tissue swelling occurs during the procedure. Forarthroscopy for FAI, the surgeon should ensure the proper equip-ment is available consisting of cannulated obturators, slotted can-nulas, extended irrigators, arthroscopic scalpel, and an assortmentof basket punches and graspers designed for the hip. These mustbe longer and of sturdy construction, too, to minimize the risk ofbreakage. Special and large shaver blades and motorized burrshave been developed. Extra-length cannulas have been accom-plished shortening the accompanying bridge, which allows thesecannulas to be used with standard arthroscopes. We also use aspecial cannulated blunt obturator or switching stick that is adapt-ed to attach to a removable T-handle so it can be used over a Niti-nol guide wire. Nitinol is a Nickel-Titanium alloy with a shapememory property that is flexible and resistant to kinking. Cannu-las of different diameter (4.5, 5.0. and 5.5 mm) are available, andslotted cannulas have been designed to switch the scope and in-struments from a portal to the other or to let curved instrumentspass. Thermal ablation and radiofrequency devices demonstratespecific advantages in the hip. Their small diameter and flexibilityallow access to recesses within the joint difficult to access with me-chanical blades, and they are often much more effective at creat-ing smooth transition zones. (Byrd Tech Orthop 2005)
Patient positioning
The patient is supine on a standard fracture table and placedunder general anaesthesia, which allows for the use of paralytics,in order to obtain optimal hip distraction with the least amount oftraction. Regional (spinal) anaesthesia can also be used, but an ad-equate motor blockade to ensure complete muscle relaxation ismore difficult to be achieved.
Care must be taken to protect the genitalia, and the perinealbolster has to be very well padded. We use a 20 cm-diameter ure-thane post to distribute the pressure on a larger surface and tolower the risk of pudendal nerve injury (compression neurapraxia)or genitalia haematoma after prolonged traction. (Sampson 2001,McCarthy Instr Course Lect 2006, Clarke 2003, Funke 1996) Thepost is placed more on the operative side, against the medial thigh,to achieve some lateralization of the thigh itself, and facilitate theoptimal traction vector for distraction of the joint that is oblique
227
Hip arthroscopy for femoro-acetabular impingement: personal technique and indications

relative to the axis of the body and parallel to the femoral neckrather than to the femoral shaft. (Byrd 1994, Byrd 2001) This alsodistances the post from the area of the pudendal nerve.
Both feet are in boots so minimal counter traction can beplaced on the non-operative limb, while the operative limb is at-tached to the traction table via a pneumatic system (SPIDER,Tenet Medical Engineering Inc., Calgary, AB, CAN; distributed bySmith & Nephew, Andover, MA, USA). Such a system allows sta-ble positioning and traction of the limb, but care must be taken tocorrectly position it at the beginning of the procedure because itconserve plenty ability to maintain traction as long as the distalball-joint is only positioned 20 cm above the proximal ball-joint(Fig. 3). For the second part of the procedure, when we releasetraction, the SPIDER offers the possibility of easily moving thelimb and then maintaining the new position. It can be used evenwith large and heavy patients. A tensiometer can be incorporatedin the footplate, if one is concerned about the amount of tractionbeing used. (Byrd Tech Orthop 2005)
Mild traction is applied to the contralateral limb, which isslightly abducted, this allows for adduction of the operative legand the C-arm of image intensifier to come in between the legs toobtain anteroposterior (AP) and frog-lateral views of the hip.
In order to obtain adequate hip distraction, the operative limbis initially positioned in slightly flexion (10°), maximal internal ro-tation and 30° of abduction to improve the vector of force. Underfluoroscopic control, traction is gently applied. Then the operativelimb is adducted to neutral; adequate distraction is confirmedwith of joint-space widening in the AP plane on image intensifier(Fig. 4). If distraction has been sufficient, a joint opening of 6 to10 mm and a radiolucent arc around the apex of the femoral headrepresenting a vacuum within the joint can be seen. On the imageintensifier, it is possible to see the different opacities of the bone,of the cartilage of the femoral head, and sometimes of the labrum,with respect to the vacuum/air arthrogram. (Byrd Arthroscopy2000 avoiding the labrum) If there is difficultly obtaining distrac-tion, one option can be to enter the peripheral compartment first,to perform a partial capsulotomy and then apply more traction.(Dienst 2005)
Distraction is maintained and the limb is prepped in the usualmanner as for proximal femur fractures, paying attention to leaveaccess to anterior and lateral hip and proximal thigh. The time oftraction application is noted, and continuous traction time is lim-ited to less than 2 hours.
Approach and portal placement
The surgeon takes position in front of the hip and the assistantdistal to the surgeon, to help manoeuvring the leg. Two Mayostands are prepped; one is positioned proximal to the surgeon,with the more frequently used instruments, and the other at the
228
Chapter 16
Figure 3
The pneumatic leg holder
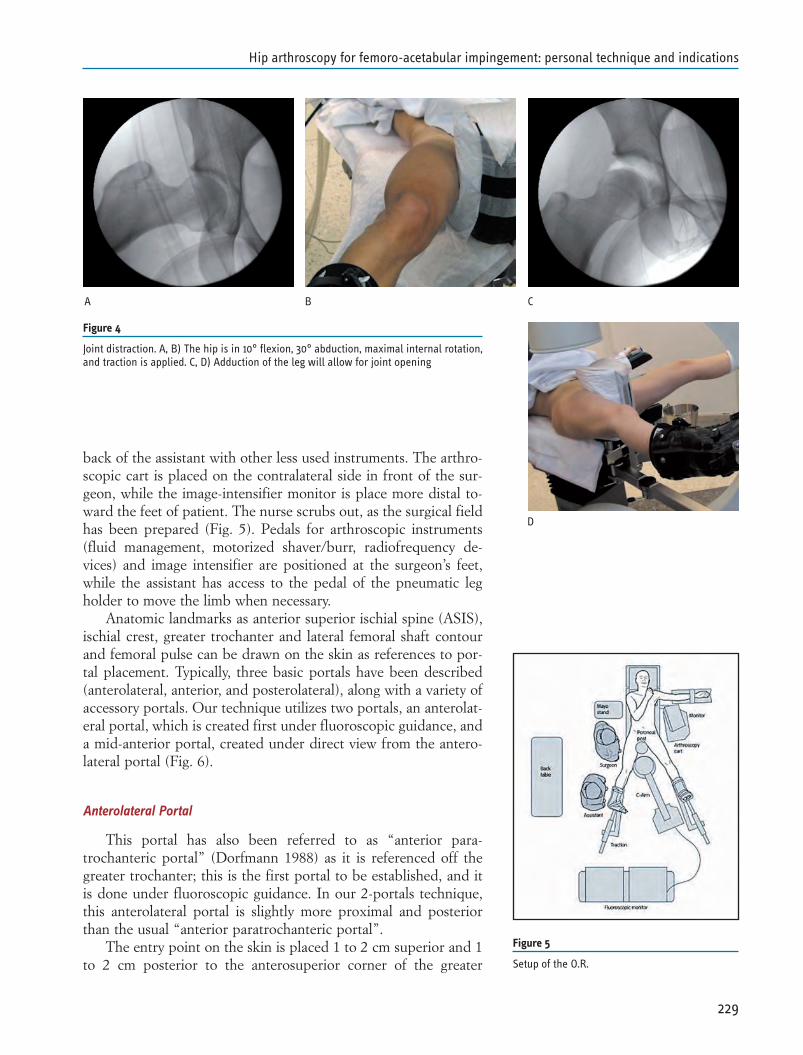
back of the assistant with other less used instruments. The arthro-scopic cart is placed on the contralateral side in front of the sur-geon, while the image-intensifier monitor is place more distal to-ward the feet of patient. The nurse scrubs out, as the surgical fieldhas been prepared (Fig. 5). Pedals for arthroscopic instruments(fluid management, motorized shaver/burr, radiofrequency de-vices) and image intensifier are positioned at the surgeon’s feet,while the assistant has access to the pedal of the pneumatic legholder to move the limb when necessary.
Anatomic landmarks as anterior superior ischial spine (ASIS),ischial crest, greater trochanter and lateral femoral shaft contourand femoral pulse can be drawn on the skin as references to por-tal placement. Typically, three basic portals have been described(anterolateral, anterior, and posterolateral), along with a variety ofaccessory portals. Our technique utilizes two portals, an anterolat-eral portal, which is created first under fluoroscopic guidance, anda mid-anterior portal, created under direct view from the antero-lateral portal (Fig. 6).
Anterolateral Portal
This portal has also been referred to as “anterior para-trochanteric portal” (Dorfmann 1988) as it is referenced off thegreater trochanter; this is the first portal to be established, and itis done under fluoroscopic guidance. In our 2-portals technique,this anterolateral portal is slightly more proximal and posteriorthan the usual “anterior paratrochanteric portal”.
The entry point on the skin is placed 1 to 2 cm superior and 1to 2 cm posterior to the anterosuperior corner of the greater
229
Hip arthroscopy for femoro-acetabular impingement: personal technique and indications
Figure 4
Joint distraction. A, B) The hip is in 10° flexion, 30° abduction, maximal internal rotation,and traction is applied. C, D) Adduction of the leg will allow for joint opening
A B C
D
Figure 5
Setup of the O.R.
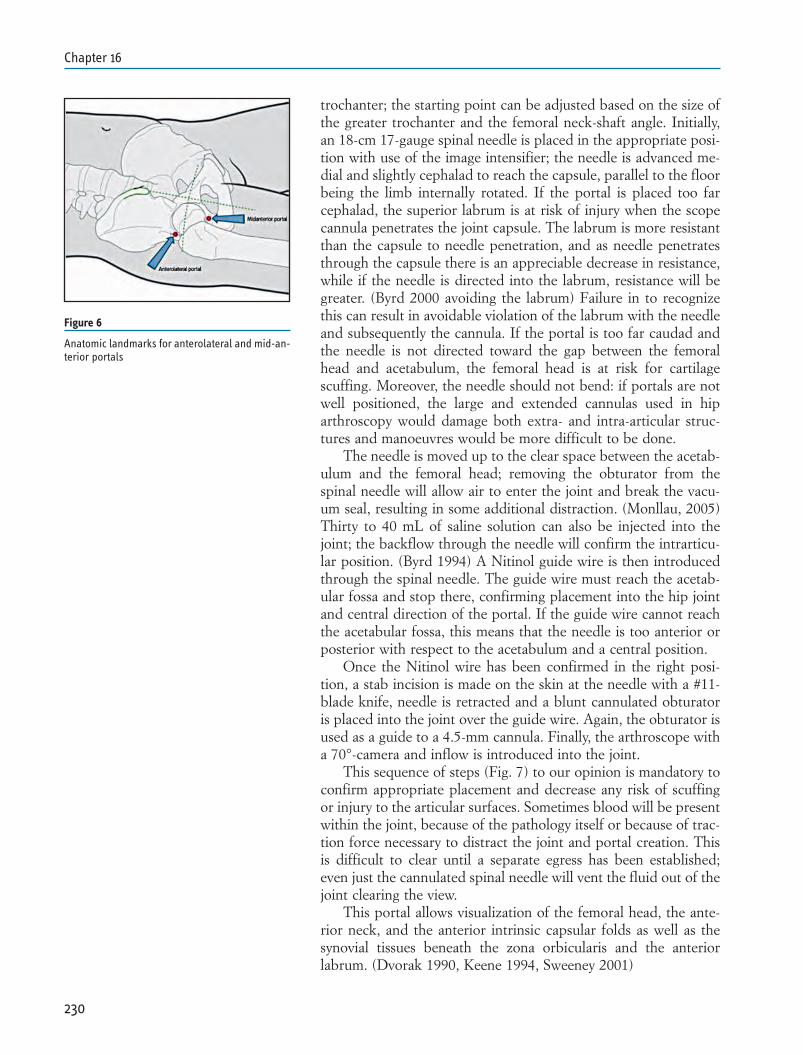
trochanter; the starting point can be adjusted based on the size ofthe greater trochanter and the femoral neck-shaft angle. Initially,an 18-cm 17-gauge spinal needle is placed in the appropriate posi-tion with use of the image intensifier; the needle is advanced me-dial and slightly cephalad to reach the capsule, parallel to the floorbeing the limb internally rotated. If the portal is placed too farcephalad, the superior labrum is at risk of injury when the scopecannula penetrates the joint capsule. The labrum is more resistantthan the capsule to needle penetration, and as needle penetratesthrough the capsule there is an appreciable decrease in resistance,while if the needle is directed into the labrum, resistance will begreater. (Byrd 2000 avoiding the labrum) Failure in to recognizethis can result in avoidable violation of the labrum with the needleand subsequently the cannula. If the portal is too far caudad andthe needle is not directed toward the gap between the femoralhead and acetabulum, the femoral head is at risk for cartilagescuffing. Moreover, the needle should not bend: if portals are notwell positioned, the large and extended cannulas used in hiparthroscopy would damage both extra- and intra-articular struc-tures and manoeuvres would be more difficult to be done.
The needle is moved up to the clear space between the acetab-ulum and the femoral head; removing the obturator from thespinal needle will allow air to enter the joint and break the vacu-um seal, resulting in some additional distraction. (Monllau, 2005)Thirty to 40 mL of saline solution can also be injected into thejoint; the backflow through the needle will confirm the intrarticu-lar position. (Byrd 1994) A Nitinol guide wire is then introducedthrough the spinal needle. The guide wire must reach the acetab-ular fossa and stop there, confirming placement into the hip jointand central direction of the portal. If the guide wire cannot reachthe acetabular fossa, this means that the needle is too anterior orposterior with respect to the acetabulum and a central position.
Once the Nitinol wire has been confirmed in the right posi-tion, a stab incision is made on the skin at the needle with a #11-blade knife, needle is retracted and a blunt cannulated obturatoris placed into the joint over the guide wire. Again, the obturator isused as a guide to a 4.5-mm cannula. Finally, the arthroscope witha 70°-camera and inflow is introduced into the joint.
This sequence of steps (Fig. 7) to our opinion is mandatory toconfirm appropriate placement and decrease any risk of scuffingor injury to the articular surfaces. Sometimes blood will be presentwithin the joint, because of the pathology itself or because of trac-tion force necessary to distract the joint and portal creation. Thisis difficult to clear until a separate egress has been established;even just the cannulated spinal needle will vent the fluid out of thejoint clearing the view.
This portal allows visualization of the femoral head, the ante-rior neck, and the anterior intrinsic capsular folds as well as thesynovial tissues beneath the zona orbicularis and the anteriorlabrum. (Dvorak 1990, Keene 1994, Sweeney 2001)
230
Chapter 16
Figure 6
Anatomic landmarks for anterolateral and mid-an-terior portals
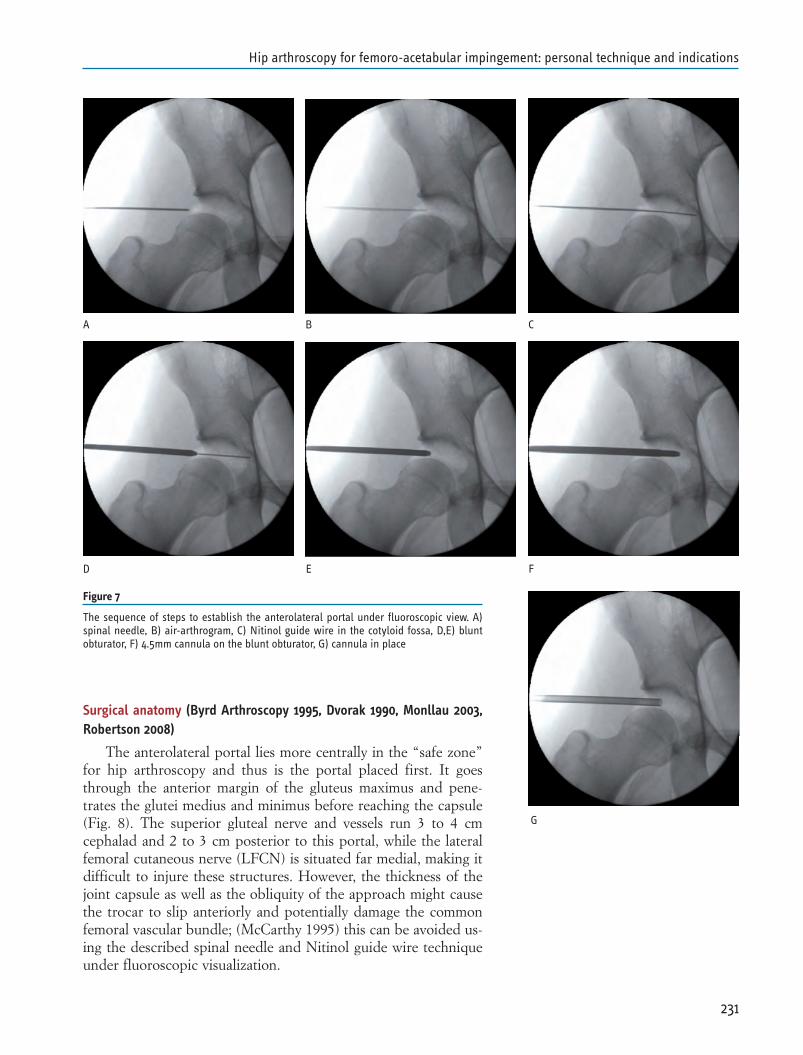
Surgical anatomy (Byrd Arthroscopy 1995, Dvorak 1990, Monllau 2003,Robertson 2008)
The anterolateral portal lies more centrally in the “safe zone”for hip arthroscopy and thus is the portal placed first. It goesthrough the anterior margin of the gluteus maximus and pene-trates the glutei medius and minimus before reaching the capsule(Fig. 8). The superior gluteal nerve and vessels run 3 to 4 cmcephalad and 2 to 3 cm posterior to this portal, while the lateralfemoral cutaneous nerve (LFCN) is situated far medial, making itdifficult to injure these structures. However, the thickness of thejoint capsule as well as the obliquity of the approach might causethe trocar to slip anteriorly and potentially damage the commonfemoral vascular bundle; (McCarthy 1995) this can be avoided us-ing the described spinal needle and Nitinol guide wire techniqueunder fluoroscopic visualization.
231
Hip arthroscopy for femoro-acetabular impingement: personal technique and indications
Figure 7
The sequence of steps to establish the anterolateral portal under fluoroscopic view. A)spinal needle, B) air-arthrogram, C) Nitinol guide wire in the cotyloid fossa, D,E) bluntobturator, F) 4.5mm cannula on the blunt obturator, G) cannula in place
A B C
D E F
G
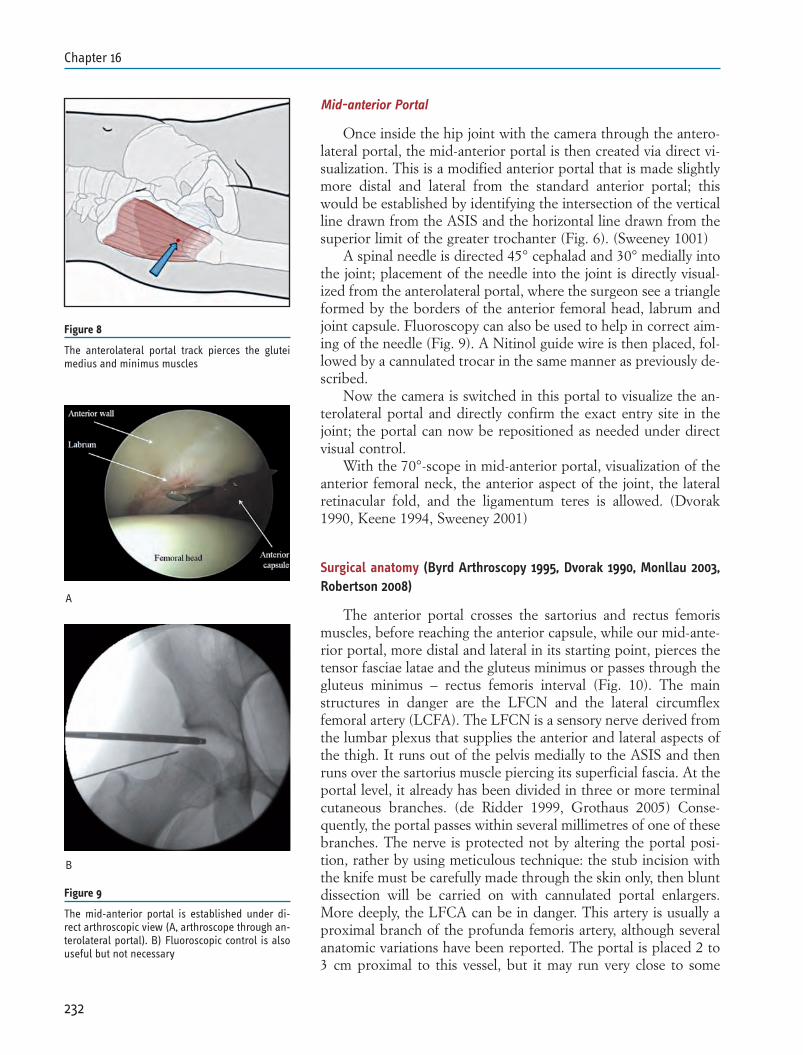
Mid-anterior Portal
Once inside the hip joint with the camera through the antero-lateral portal, the mid-anterior portal is then created via direct vi-sualization. This is a modified anterior portal that is made slightlymore distal and lateral from the standard anterior portal; thiswould be established by identifying the intersection of the verticalline drawn from the ASIS and the horizontal line drawn from thesuperior limit of the greater trochanter (Fig. 6). (Sweeney 1001)
A spinal needle is directed 45° cephalad and 30° medially intothe joint; placement of the needle into the joint is directly visual-ized from the anterolateral portal, where the surgeon see a triangleformed by the borders of the anterior femoral head, labrum andjoint capsule. Fluoroscopy can also be used to help in correct aim-ing of the needle (Fig. 9). A Nitinol guide wire is then placed, fol-lowed by a cannulated trocar in the same manner as previously de-scribed.
Now the camera is switched in this portal to visualize the an-terolateral portal and directly confirm the exact entry site in thejoint; the portal can now be repositioned as needed under directvisual control.
With the 70°-scope in mid-anterior portal, visualization of theanterior femoral neck, the anterior aspect of the joint, the lateralretinacular fold, and the ligamentum teres is allowed. (Dvorak1990, Keene 1994, Sweeney 2001)
Surgical anatomy (Byrd Arthroscopy 1995, Dvorak 1990, Monllau 2003,Robertson 2008)
The anterior portal crosses the sartorius and rectus femorismuscles, before reaching the anterior capsule, while our mid-ante-rior portal, more distal and lateral in its starting point, pierces thetensor fasciae latae and the gluteus minimus or passes through thegluteus minimus – rectus femoris interval (Fig. 10). The mainstructures in danger are the LFCN and the lateral circumflexfemoral artery (LCFA). The LFCN is a sensory nerve derived fromthe lumbar plexus that supplies the anterior and lateral aspects ofthe thigh. It runs out of the pelvis medially to the ASIS and thenruns over the sartorius muscle piercing its superficial fascia. At theportal level, it already has been divided in three or more terminalcutaneous branches. (de Ridder 1999, Grothaus 2005) Conse-quently, the portal passes within several millimetres of one of thesebranches. The nerve is protected not by altering the portal posi-tion, rather by using meticulous technique: the stub incision withthe knife must be carefully made through the skin only, then bluntdissection will be carried on with cannulated portal enlargers.More deeply, the LFCA can be in danger. This artery is usually aproximal branch of the profunda femoris artery, although severalanatomic variations have been reported. The portal is placed 2 to3 cm proximal to this vessel, but it may run very close to some
232
Chapter 16
Figure 8
The anterolateral portal track pierces the gluteimedius and minimus muscles
Figure 9
The mid-anterior portal is established under di-rect arthroscopic view (A, arthroscope through an-terolateral portal). B) Fluoroscopic control is alsouseful but not necessary
A
B
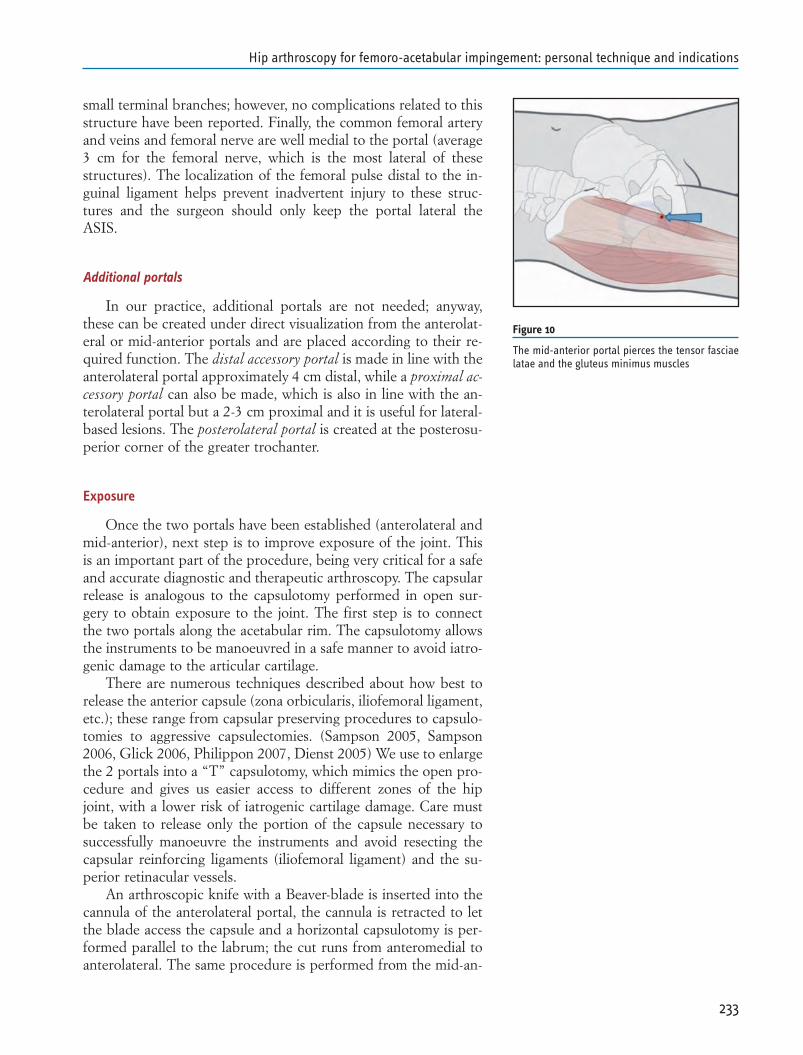
small terminal branches; however, no complications related to thisstructure have been reported. Finally, the common femoral arteryand veins and femoral nerve are well medial to the portal (average3 cm for the femoral nerve, which is the most lateral of thesestructures). The localization of the femoral pulse distal to the in-guinal ligament helps prevent inadvertent injury to these struc-tures and the surgeon should only keep the portal lateral theASIS.
Additional portals
In our practice, additional portals are not needed; anyway,these can be created under direct visualization from the anterolat-eral or mid-anterior portals and are placed according to their re-quired function. The distal accessory portal is made in line with theanterolateral portal approximately 4 cm distal, while a proximal ac-cessory portal can also be made, which is also in line with the an-terolateral portal but a 2-3 cm proximal and it is useful for lateral-based lesions. The posterolateral portal is created at the posterosu-perior corner of the greater trochanter.
Exposure
Once the two portals have been established (anterolateral andmid-anterior), next step is to improve exposure of the joint. Thisis an important part of the procedure, being very critical for a safeand accurate diagnostic and therapeutic arthroscopy. The capsularrelease is analogous to the capsulotomy performed in open sur-gery to obtain exposure to the joint. The first step is to connectthe two portals along the acetabular rim. The capsulotomy allowsthe instruments to be manoeuvred in a safe manner to avoid iatro-genic damage to the articular cartilage.
There are numerous techniques described about how best torelease the anterior capsule (zona orbicularis, iliofemoral ligament,etc.); these range from capsular preserving procedures to capsulo-tomies to aggressive capsulectomies. (Sampson 2005, Sampson2006, Glick 2006, Philippon 2007, Dienst 2005) We use to enlargethe 2 portals into a “T” capsulotomy, which mimics the open pro-cedure and gives us easier access to different zones of the hipjoint, with a lower risk of iatrogenic cartilage damage. Care mustbe taken to release only the portion of the capsule necessary tosuccessfully manoeuvre the instruments and avoid resecting thecapsular reinforcing ligaments (iliofemoral ligament) and the su-perior retinacular vessels.
An arthroscopic knife with a Beaver-blade is inserted into thecannula of the anterolateral portal, the cannula is retracted to letthe blade access the capsule and a horizontal capsulotomy is per-formed parallel to the labrum; the cut runs from anteromedial toanterolateral. The same procedure is performed from the mid-an-
233
Hip arthroscopy for femoro-acetabular impingement: personal technique and indications
Figure 10
The mid-anterior portal pierces the tensor fasciaelatae and the gluteus minimus muscles
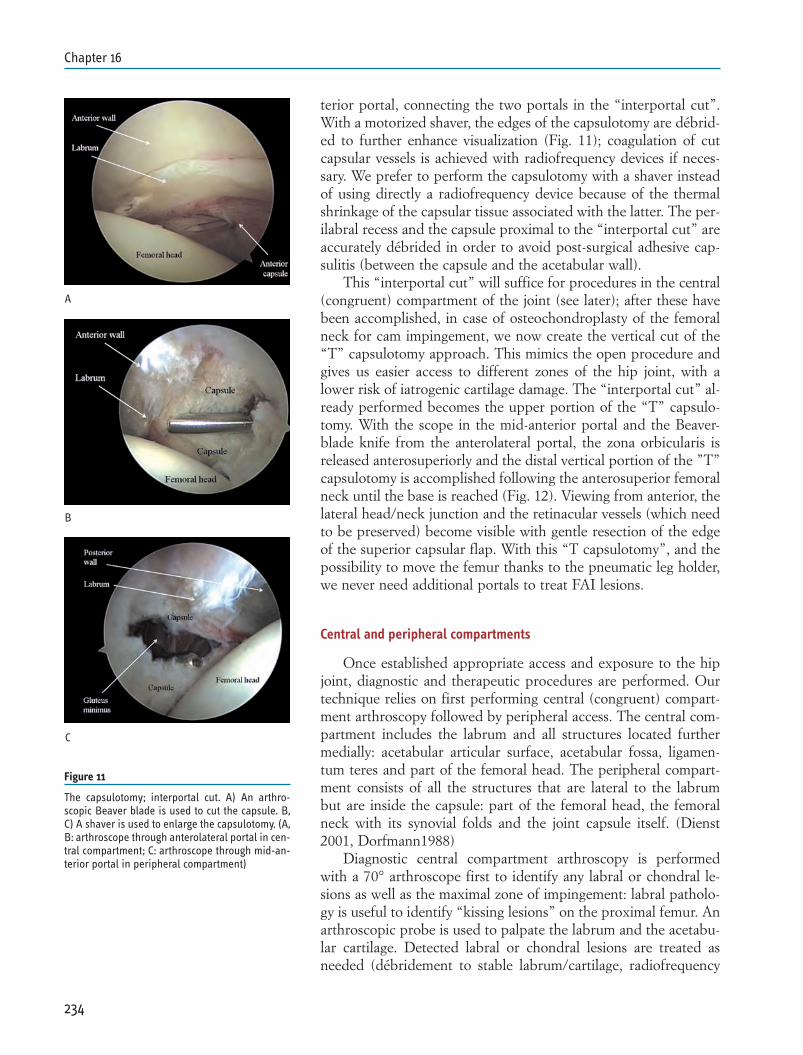
terior portal, connecting the two portals in the “interportal cut”.With a motorized shaver, the edges of the capsulotomy are débrid-ed to further enhance visualization (Fig. 11); coagulation of cutcapsular vessels is achieved with radiofrequency devices if neces-sary. We prefer to perform the capsulotomy with a shaver insteadof using directly a radiofrequency device because of the thermalshrinkage of the capsular tissue associated with the latter. The per-ilabral recess and the capsule proximal to the “interportal cut” areaccurately débrided in order to avoid post-surgical adhesive cap-sulitis (between the capsule and the acetabular wall).
This “interportal cut” will suffice for procedures in the central(congruent) compartment of the joint (see later); after these havebeen accomplished, in case of osteochondroplasty of the femoralneck for cam impingement, we now create the vertical cut of the“T” capsulotomy approach. This mimics the open procedure andgives us easier access to different zones of the hip joint, with alower risk of iatrogenic cartilage damage. The “interportal cut” al-ready performed becomes the upper portion of the “T” capsulo-tomy. With the scope in the mid-anterior portal and the Beaver-blade knife from the anterolateral portal, the zona orbicularis isreleased anterosuperiorly and the distal vertical portion of the ”T”capsulotomy is accomplished following the anterosuperior femoralneck until the base is reached (Fig. 12). Viewing from anterior, thelateral head/neck junction and the retinacular vessels (which needto be preserved) become visible with gentle resection of the edgeof the superior capsular flap. With this “T capsulotomy”, and thepossibility to move the femur thanks to the pneumatic leg holder,we never need additional portals to treat FAI lesions.
Central and peripheral compartments
Once established appropriate access and exposure to the hipjoint, diagnostic and therapeutic procedures are performed. Ourtechnique relies on first performing central (congruent) compart-ment arthroscopy followed by peripheral access. The central com-partment includes the labrum and all structures located furthermedially: acetabular articular surface, acetabular fossa, ligamen-tum teres and part of the femoral head. The peripheral compart-ment consists of all the structures that are lateral to the labrumbut are inside the capsule: part of the femoral head, the femoralneck with its synovial folds and the joint capsule itself. (Dienst2001, Dorfmann1988)
Diagnostic central compartment arthroscopy is performedwith a 70° arthroscope first to identify any labral or chondral le-sions as well as the maximal zone of impingement: labral patholo-gy is useful to identify “kissing lesions” on the proximal femur. Anarthroscopic probe is used to palpate the labrum and the acetabu-lar cartilage. Detected labral or chondral lesions are treated asneeded (débridement to stable labrum/cartilage, radiofrequency
234
Chapter 16
Figure 11
The capsulotomy; interportal cut. A) An arthro-scopic Beaver blade is used to cut the capsule. B,C) A shaver is used to enlarge the capsulotomy. (A,B: arthroscope through anterolateral portal in cen-tral compartment; C: arthroscope through mid-an-terior portal in peripheral compartment)
A
B
C
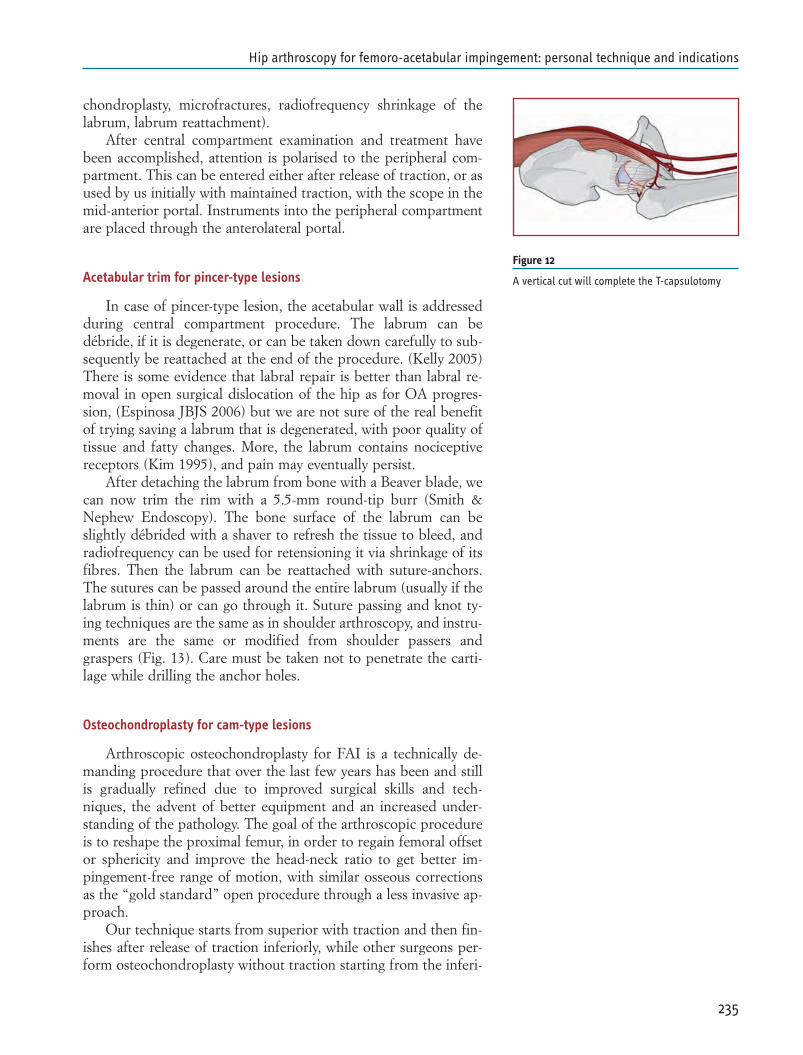
chondroplasty, microfractures, radiofrequency shrinkage of thelabrum, labrum reattachment).
After central compartment examination and treatment havebeen accomplished, attention is polarised to the peripheral com-partment. This can be entered either after release of traction, or asused by us initially with maintained traction, with the scope in themid-anterior portal. Instruments into the peripheral compartmentare placed through the anterolateral portal.
Acetabular trim for pincer-type lesions
In case of pincer-type lesion, the acetabular wall is addressedduring central compartment procedure. The labrum can bedébride, if it is degenerate, or can be taken down carefully to sub-sequently be reattached at the end of the procedure. (Kelly 2005)There is some evidence that labral repair is better than labral re-moval in open surgical dislocation of the hip as for OA progres-sion, (Espinosa JBJS 2006) but we are not sure of the real benefitof trying saving a labrum that is degenerated, with poor quality oftissue and fatty changes. More, the labrum contains nociceptivereceptors (Kim 1995), and pain may eventually persist.
After detaching the labrum from bone with a Beaver blade, wecan now trim the rim with a 5.5-mm round-tip burr (Smith &Nephew Endoscopy). The bone surface of the labrum can beslightly débrided with a shaver to refresh the tissue to bleed, andradiofrequency can be used for retensioning it via shrinkage of itsfibres. Then the labrum can be reattached with suture-anchors.The sutures can be passed around the entire labrum (usually if thelabrum is thin) or can go through it. Suture passing and knot ty-ing techniques are the same as in shoulder arthroscopy, and instru-ments are the same or modified from shoulder passers andgraspers (Fig. 13). Care must be taken not to penetrate the carti-lage while drilling the anchor holes.
Osteochondroplasty for cam-type lesions
Arthroscopic osteochondroplasty for FAI is a technically de-manding procedure that over the last few years has been and stillis gradually refined due to improved surgical skills and tech-niques, the advent of better equipment and an increased under-standing of the pathology. The goal of the arthroscopic procedureis to reshape the proximal femur, in order to regain femoral offsetor sphericity and improve the head-neck ratio to get better im-pingement-free range of motion, with similar osseous correctionsas the “gold standard” open procedure through a less invasive ap-proach.
Our technique starts from superior with traction and then fin-ishes after release of traction inferiorly, while other surgeons per-form osteochondroplasty without traction starting from the inferi-
235
Hip arthroscopy for femoro-acetabular impingement: personal technique and indications
Figure 12
A vertical cut will complete the T-capsulotomy
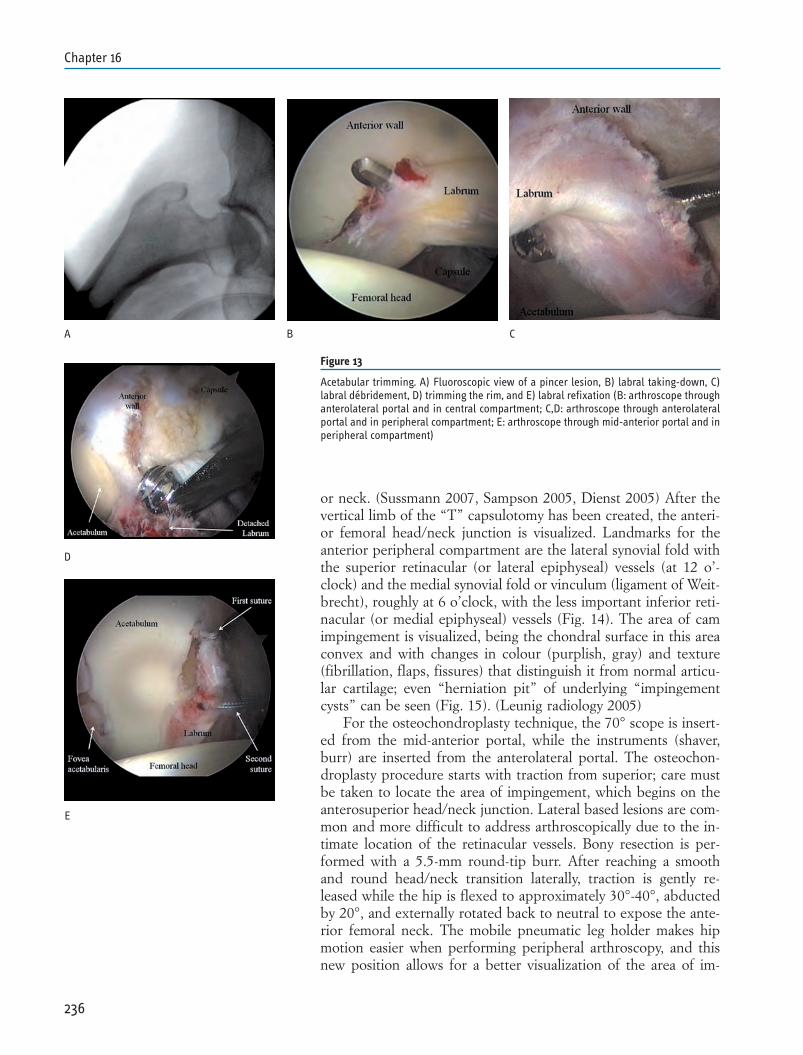
or neck. (Sussmann 2007, Sampson 2005, Dienst 2005) After thevertical limb of the “T” capsulotomy has been created, the anteri-or femoral head/neck junction is visualized. Landmarks for theanterior peripheral compartment are the lateral synovial fold withthe superior retinacular (or lateral epiphyseal) vessels (at 12 o’-clock) and the medial synovial fold or vinculum (ligament of Weit-brecht), roughly at 6 o’clock, with the less important inferior reti-nacular (or medial epiphyseal) vessels (Fig. 14). The area of camimpingement is visualized, being the chondral surface in this areaconvex and with changes in colour (purplish, gray) and texture(fibrillation, flaps, fissures) that distinguish it from normal articu-lar cartilage; even “herniation pit” of underlying “impingementcysts” can be seen (Fig. 15). (Leunig radiology 2005)
For the osteochondroplasty technique, the 70° scope is insert-ed from the mid-anterior portal, while the instruments (shaver,burr) are inserted from the anterolateral portal. The osteochon-droplasty procedure starts with traction from superior; care mustbe taken to locate the area of impingement, which begins on theanterosuperior head/neck junction. Lateral based lesions are com-mon and more difficult to address arthroscopically due to the in-timate location of the retinacular vessels. Bony resection is per-formed with a 5.5-mm round-tip burr. After reaching a smoothand round head/neck transition laterally, traction is gently re-leased while the hip is flexed to approximately 30°-40°, abductedby 20°, and externally rotated back to neutral to expose the ante-rior femoral neck. The mobile pneumatic leg holder makes hipmotion easier when performing peripheral arthroscopy, and thisnew position allows for a better visualization of the area of im-
236
Chapter 16
Figure 13
Acetabular trimming. A) Fluoroscopic view of a pincer lesion, B) labral taking-down, C)labral débridement, D) trimming the rim, and E) labral refixation (B: arthroscope throughanterolateral portal and in central compartment; C,D: arthroscope through anterolateralportal and in peripheral compartment; E: arthroscope through mid-anterior portal and inperipheral compartment)
A B C
D
E
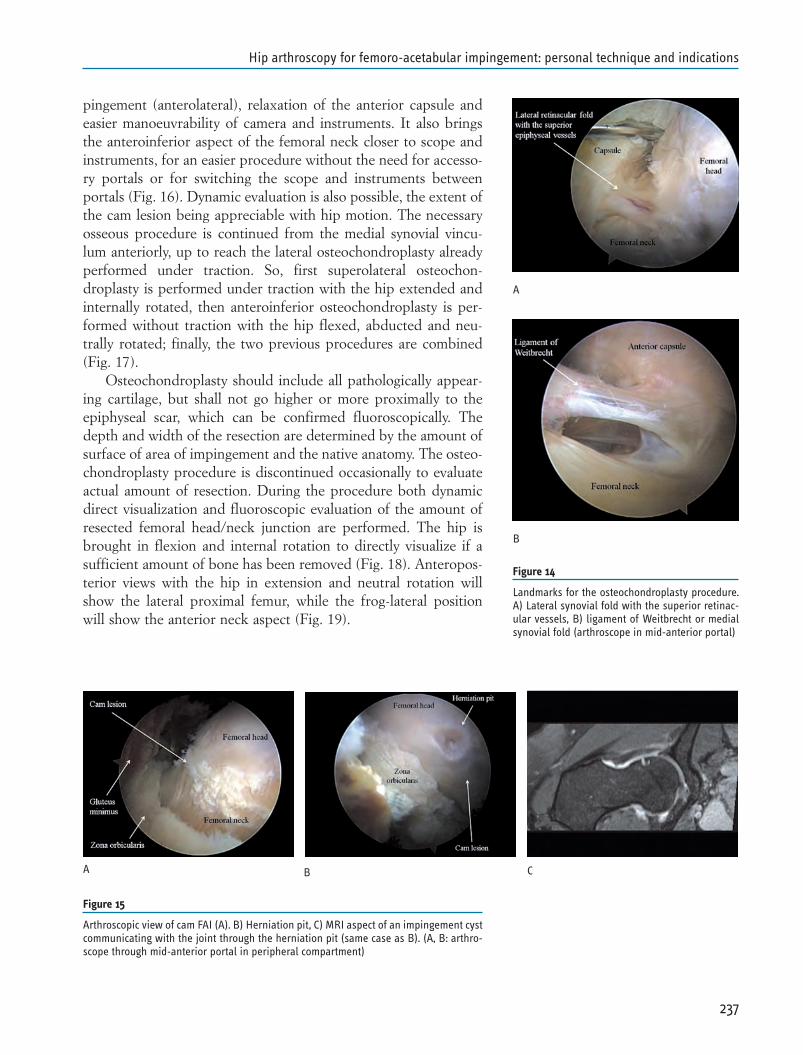
pingement (anterolateral), relaxation of the anterior capsule andeasier manoeuvrability of camera and instruments. It also bringsthe anteroinferior aspect of the femoral neck closer to scope andinstruments, for an easier procedure without the need for accesso-ry portals or for switching the scope and instruments betweenportals (Fig. 16). Dynamic evaluation is also possible, the extent ofthe cam lesion being appreciable with hip motion. The necessaryosseous procedure is continued from the medial synovial vincu-lum anteriorly, up to reach the lateral osteochondroplasty alreadyperformed under traction. So, first superolateral osteochon-droplasty is performed under traction with the hip extended andinternally rotated, then anteroinferior osteochondroplasty is per-formed without traction with the hip flexed, abducted and neu-trally rotated; finally, the two previous procedures are combined(Fig. 17).
Osteochondroplasty should include all pathologically appear-ing cartilage, but shall not go higher or more proximally to theepiphyseal scar, which can be confirmed fluoroscopically. Thedepth and width of the resection are determined by the amount ofsurface of area of impingement and the native anatomy. The osteo-chondroplasty procedure is discontinued occasionally to evaluateactual amount of resection. During the procedure both dynamicdirect visualization and fluoroscopic evaluation of the amount ofresected femoral head/neck junction are performed. The hip isbrought in flexion and internal rotation to directly visualize if asufficient amount of bone has been removed (Fig. 18). Anteropos-terior views with the hip in extension and neutral rotation willshow the lateral proximal femur, while the frog-lateral positionwill show the anterior neck aspect (Fig. 19).
237
Hip arthroscopy for femoro-acetabular impingement: personal technique and indications
A
B
A B C
Figure 15
Arthroscopic view of cam FAI (A). B) Herniation pit, C) MRI aspect of an impingement cystcommunicating with the joint through the herniation pit (same case as B). (A, B: arthro-scope through mid-anterior portal in peripheral compartment)
Figure 14
Landmarks for the osteochondroplasty procedure.A) Lateral synovial fold with the superior retinac-ular vessels, B) ligament of Weitbrecht or medialsynovial fold (arthroscope in mid-anterior portal)
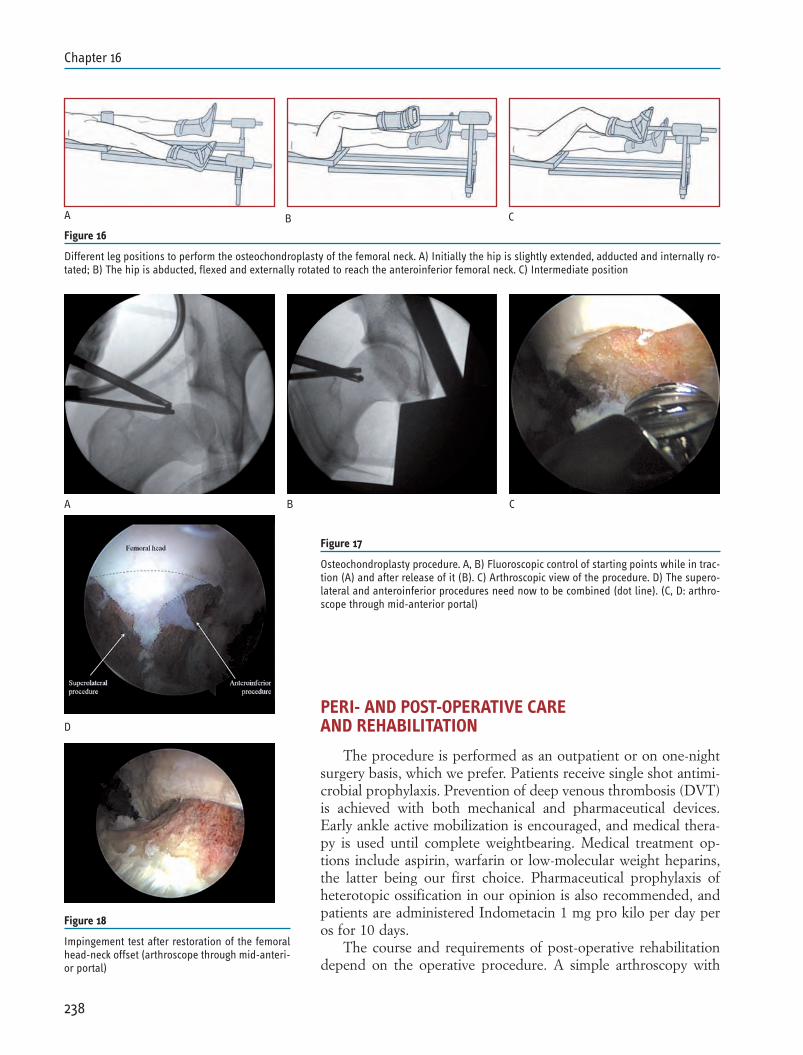
PERI- AND POST-OPERATIVE CARE AND REHABILITATION
The procedure is performed as an outpatient or on one-nightsurgery basis, which we prefer. Patients receive single shot antimi-crobial prophylaxis. Prevention of deep venous thrombosis (DVT)is achieved with both mechanical and pharmaceutical devices.Early ankle active mobilization is encouraged, and medical thera-py is used until complete weightbearing. Medical treatment op-tions include aspirin, warfarin or low-molecular weight heparins,the latter being our first choice. Pharmaceutical prophylaxis ofheterotopic ossification in our opinion is also recommended, andpatients are administered Indometacin 1 mg pro kilo per day peros for 10 days.
The course and requirements of post-operative rehabilitationdepend on the operative procedure. A simple arthroscopy with
238
Chapter 16
A B C
Figure 16
Different leg positions to perform the osteochondroplasty of the femoral neck. A) Initially the hip is slightly extended, adducted and internally ro-tated; B) The hip is abducted, flexed and externally rotated to reach the anteroinferior femoral neck. C) Intermediate position
A B C
D
Figure 17
Osteochondroplasty procedure. A, B) Fluoroscopic control of starting points while in trac-tion (A) and after release of it (B). C) Arthroscopic view of the procedure. D) The supero-lateral and anteroinferior procedures need now to be combined (dot line). (C, D: arthro-scope through mid-anterior portal)
Figure 18
Impingement test after restoration of the femoralhead-neck offset (arthroscope through mid-anteri-or portal)
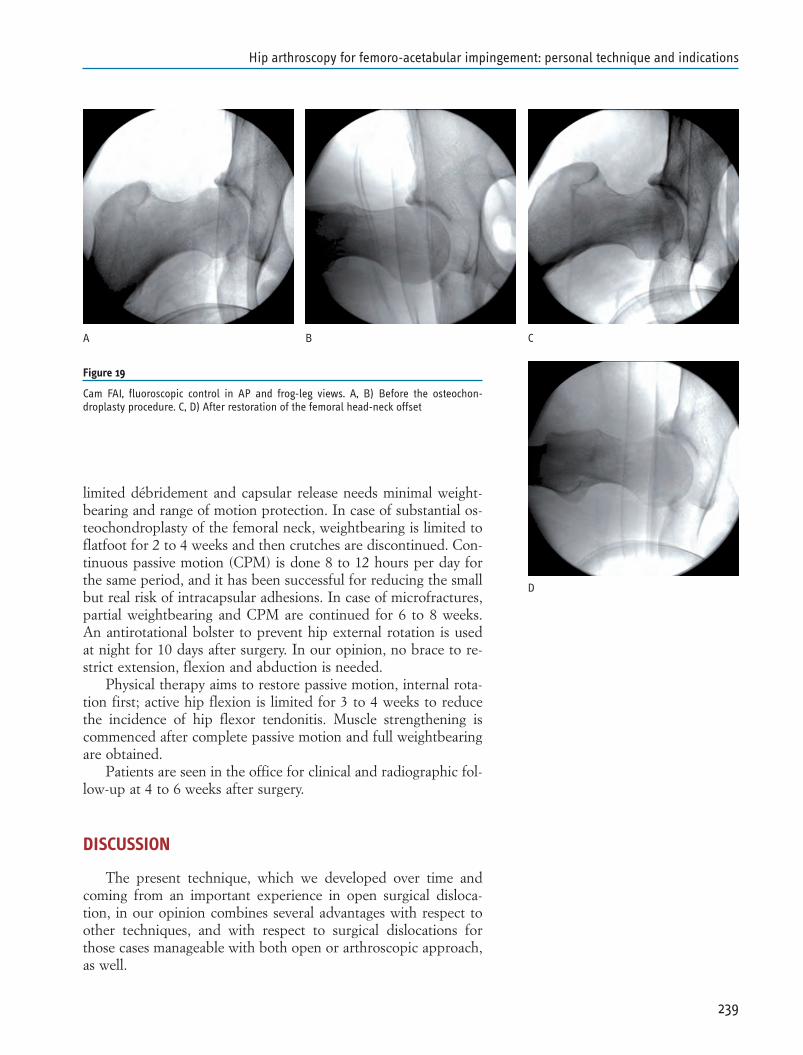
limited débridement and capsular release needs minimal weight-bearing and range of motion protection. In case of substantial os-teochondroplasty of the femoral neck, weightbearing is limited toflatfoot for 2 to 4 weeks and then crutches are discontinued. Con-tinuous passive motion (CPM) is done 8 to 12 hours per day forthe same period, and it has been successful for reducing the smallbut real risk of intracapsular adhesions. In case of microfractures,partial weightbearing and CPM are continued for 6 to 8 weeks.An antirotational bolster to prevent hip external rotation is usedat night for 10 days after surgery. In our opinion, no brace to re-strict extension, flexion and abduction is needed.
Physical therapy aims to restore passive motion, internal rota-tion first; active hip flexion is limited for 3 to 4 weeks to reducethe incidence of hip flexor tendonitis. Muscle strengthening iscommenced after complete passive motion and full weightbearingare obtained.
Patients are seen in the office for clinical and radiographic fol-low-up at 4 to 6 weeks after surgery.
DISCUSSION
The present technique, which we developed over time andcoming from an important experience in open surgical disloca-tion, in our opinion combines several advantages with respect toother techniques, and with respect to surgical dislocations forthose cases manageable with both open or arthroscopic approach,as well.
239
Hip arthroscopy for femoro-acetabular impingement: personal technique and indications
A B C
D
Figure 19
Cam FAI, fluoroscopic control in AP and frog-leg views. A, B) Before the osteochon-droplasty procedure. C, D) After restoration of the femoral head-neck offset

The supine position is simple and can be accomplished in fewminutes, it can be performed on any standard fracture table withan orientation of the joint that is familiar to orthopaedic surgeons.It also let easily obtain a frog-lateral view, which is useful to assessthe amount of bony resection needed/performed pre-operatively,during, and at the end of the procedure. There is reliable accessfor all portal placements. Finally, intraabdominal fluid extravasa-tion that is a potentially serious complication of hip arthroscopyhas been reported only in the lateral position. (Funke 1996;Bartlett 1998; Sampson 2001, Haupt 2008) Anyway, regardless ofthe position, poor positioning will assure a difficult procedure.
Carefully portal placement and entry into the joint is very im-portant when performing hip arthroscopy, both to avoid iatro-genic damage and to easily perform the necessary procedures. Di-rect trauma to neurovascular structures is little more than a theo-retical issue in hip arthroscopy; these structures are at a safe dis-tance when proper technique in patient positioning and portalplacement is observed. Byrd (chapter 2005) described one case offemoral nerve palsy and one case of laceration of the femoralnerve. The LFCN is always vulnerable to injury from the anteriorportal, (Byrd 1995) but, again, proper technique with sharp inci-sion of only the skin will avoid injuries to this nerve. Anatomy ofthe LFCN and meticulous portal placement has been describedpreviously. Only two cases of permanent damage to this nerve hasbeen reported. (Eriksson 1986, Byrd chapter 2005)
Damage to the labrum on entry into the joint is a possiblecomplication that can be avoided with technical shrewdness.(Byrd arthroscopy 2000) Scuffing of the femoral head can also oc-cur to various extent, even with good distraction of the joint, andtrue frequency is certainly underreported. (Sampson 2001)Whether such injuries actually produce symptoms or are clinicallyrelevant at all is not known; Sampson (2001) reported 2 cases outof 530 procedures (0.4%) and 3 out of 1001 (0.3%) in an updat-ed report (Sampson 2005) of relevant cartilage scuffing and relat-ed them to inadequate traction.
The use of a mobile pneumatic leg holder, while guaranteesthe same reliability and efficacy in joint distraction during the ini-tial part of the procedure, it also allows for easy moving of the legand maintaining of the new position. Regular traction table isprobably easier to position, already available in every hospital andof any expense, but it does not allow for complete range of motionespecially in combined flexion and rotations (both internal andexternal). New traction devices specifically designed for hiparthroscopy show to our opinion some disadvantages. They re-quire longer time and more personnel for positioning the patient;abduction of the contralateral leg is not adjustable and the handleof the boot is very bulky, both interfering with the C-arm; ma-noeuvring of the leg requires the help of unscrubbed personnel.With a mobile pneumatic leg holder the high degree of hip motionallows to visualize the entire area of impingement from the mid-
240
Chapter 16

anterior portal (where it is the scope), and it makes the anteroin-ferior femoral neck accessible to instruments (which are usedfrom the anterolateral portal). Therefore, we are able to performthe femoral osteochondroplasty procedure without the need foraccessory portals or for switching the scope and instruments be-tween portals. If the surgeon will not go to the femur, the femurmust come to the surgeon. Dynamic evaluation is also accurate,being possible to bring the femur in maximal flexion and internalrotation (impingement test) and maximal flexion-abduction-exter-nal rotation (FABER test).
To gain good exposure via a “T” capsulotomy is to our opin-ion another important point: this will improve visualization of thebony structures and retinacular folds and will make manoeuvringof the instruments easier, reducing the risk for iatrogenic damageto articular cartilage. In combination with the mobility of the legthanks to the pneumatic leg holder, the capsulotomy makes possi-ble to reach the entire anterior proximal femur without the needof additional portals. One can argue that such a capsulotomy willallow for excessive fluid extravasation into the proximal thigh.Some fluid extravasation in the soft tissue of proximal thigh iscommon and has no clinical relevance. It is important to performthe procedure in an expeditious way, and as traction should bediscontinued after 2 hours to avoid traction-related complications,excessive time in the peripheral compartment can cause soft tissueswelling, muscle damage and bleeding in the anterolateral thigh,as well. The use of low-pressure fluid management can help avoid-ing excessive fluid extravasation while maintaining good visibility.Anyway, fluid will drain from the portals or be reabsorbed withinthe first postoperative hours, and no related complications havebeen reported. Another issue about capsulotomy is eventual post-operative laxity or a symptomatic capsular herniation into themuscles, and we are aware that some surgeons like to close thecapsule with stitches. To our opinion capsular closure is not nec-essary, as the defect in the capsule is very small and the surround-ed muscles (gluteus minimus and rectus femoris) strictly adhere tothe capsular plan and will form a natural barrier and template forscar formation. In addition, we never saw fluid-soaked muscles orarticular herniations on follow-up MRI.
As for the timing of the procedure, we prefer to start with thecentral compartment. Our opinion is that first step of hiparthroscopy shall always be a diagnostic evaluation of the entirejoint, to fully understand the comprehensive joint pathology, andsubsequently treat what deserves to be treated. More, labrum andgross cartilage pathology can be well appreciated in pre-operativediagnostic work-out, (Leunig 1997, Leunig 2004, Chan 2005)while subtle cartilage and other soft tissues alterations are not al-ways visualized even at gadolinium-enhanced magnetic resonancearthrography (MRA). (Schmid 2003, Keeney 2004, Byrd 2004,Knuesel 2004) Arthroscopic findings may differ significantly fromthose pointed out from the pre-operative diagnostic studies,
241
Hip arthroscopy for femoro-acetabular impingement: personal technique and indications

(Baber 1999) and the surgeon risks to spend time in treating anobvious aspect of the pathology (e.g., cam lesion) and then to re-alize that there are other related damages that need to be address(e.g. large chondral flap).
When performing acetabular trimming for a pincer-type de-formity, surgeon must decide how to manage the labrum. If thelabrum is partially torn, or intact, it has to be detached from un-derlying bone to perform the osseous trimming, and then it has tobe reattached with the use of suture-anchors. Espinosa et al. (ref)showed that labral refixation is better than labral excision whenperforming open procedures for FAI; still it remains questionableif a degenerated labrum is better refixed rather than excised. Thelabrum contains nociceptive nerve-endings, (Kim 1995) and even-tually a refixed degenerated labrum may not heal to bone, and willbe painful, requiring subsequent procedure to débride it. Intra-operative evaluation of the osteochondroplasty of the femoralneck is quite simple to perform, while evaluation of the acetabularside is more demanding. We therefore consider pre-operativeplanning to be useful to evaluate the amount of acetabular rimthat need to be trimmed (both in arthroscopic and open proce-dures), without resulting in poor femoral head coverage and sub-sequent instability or excessive compressive and shear stresses; weaim to get a final lateral centre edge angle of 27° to 30°.
As for the osteochondroplasty procedure of a cam-type lesion,we believe that there are some advantages starting the procedurefrom superolateral while still in traction. First, we are already un-der traction as we pointed out before, and this will grant better vi-sualization and protection of the labrum while burring the femoralneck. The superior retinacular vessels are a reliable landmark, andosseous resection must spare them not to compromise blood sup-ply to the femoral head. (Ganz 2001, Gautier 2000, Sussmann2007 23-12) Last, but not least, lateral based lesions are commonand more difficult to address arthroscopically due to their inti-mate location to the retinacular vessels, and we prefer to addressthis location at the beginning of the procedure rather than at theend. After trimming the lateral part of the femoral neck, tractionis released and the leg moved to reach and treat the anteroinferiorpart of the neck. At this point is also possible to perform dynam-ic testing, and the procedure is continued as needed.
Over-resection of the cam impingement is as harmful as under-resection: in the second case, symptoms and pathology will notsolve, in the first case, risk of femoral neck fracture, avascularnecrosis (AVN) or loss of the suction seal of the labrum, whicheventually can bring to hip instability. It is also important to createa smooth transition zone, avoiding a “cookie bite” resection. Inaddition, one must critically evaluate the medial and lateral extentof the resection. Cam bone is usually sclerotic due to repetitiveimpingement, and fibrocystic alterations are also present; typicalare subchondral cysts (impingement cysts), which need to bedébrided. If soft cancellous bone is encountered, the surgeon may
242
Chapter 16

not be in the area of maximal deformity, being the incorrect loca-tion of osteoplasty most commonly too medial.
Infection is a potential and serious complication of every sur-gical procedure. To our knowledge, only one case of septic arthri-tis after hip arthroscopy has been reported; the patient was oper-ated on for a synovial chondromatosis and he did not receive anyprophylaxis. (Clarke 2003) Hip arthroscopy is a surgical proce-dure, and even if the risk of sepsis is very low, we recommendedthe use of antimicrobial prophylaxis. Antithromboembolic pro-phylaxis is also used, although thrombophlebitis and DVTs orpulmonary embolism are an infrequent complication of lowerlimb arthroscopic procedures, being the incidence of subclinicalentities greater when routinely investigated. No studies on inci-dence of DVT in hip arthroscopy have been conducted, nor havediagnostic surveys been routinely performed in published hiparthroscopy series. To our knowledge only Byrd reported of onepossible case of distal DVT in an athlete 2 month after hiparthroscopy, (Byrd, chapter 2005) and a review of 27 papers in-cluding 5554 cases has revealed a 0% rate of DVT and PE. (Bush-nell 2008) Finally, heterotopic ossification is a recognized compli-cation associated with surgical hip dislocation (Ganz 2001) andthe risk with arthroscopy is very small, but still may happen. (Byrd2000) We think that the capsulotomy approach could eventuallyincrease this risk and so medical prevention with NSAID’s is rec-ommended.
CONCLUSIONS
Femoroacetabular impingement is a very important factor inthe pathogenesis of hip OA, particularly in cases considered up tonow to be idiopathic in origin. Open treatment of FAI has beendeveloped, and results are encouraging. Nevertheless, surgical ap-proach is very demanding and concerns still exist about the risk ofAVN of the femoral head and of trochanteric nonunion.Arthroscopy is less invasive but it must aim to obtain same resultsas open procedures.
Some are the keys to success in arthroscopic treatment forFAI. First, a successful outcome depends on proper patient selec-tion. A technically well-executed procedure fails if performed forthe wrong indication; this includes the procedure to meet patient’sexpectations. Second, patient positioning is of paramount rele-vance. Poor positioning will return a difficult or impossible proce-dure. Third, access to the hip joint must be achieved as atraumat-ic as possible. Finally, of course, the procedure must be carried onas carefully as possible. Care must be taken to avoid resection inthe region of lateral epiphyseal vessels penetration. It is on the ex-act knowledge of blood supply (Gautier 2000) to the femoral headthat operative treatment for FAI has been developed, (Ganz 2001,
243
Hip arthroscopy for femoro-acetabular impingement: personal technique and indications

Lavigne 2004, Leunig 2005, Nötzli 2002) and arthroscopic ap-proach has to respect the blood supply as open surgery does.
The hip joint remains the least common of the major joints tobe treated with arthroscopy, because of technical limitations. Fur-ther development of dedicated arthroscopic hip instruments, anda better understanding of hip impingement by the orthopaediccommunity, will allow more arthroscopic techniques to be used asanother approach to treat the impinging hip.
244
Chapter 16
REFERENCES
1. Baber YF, Robinson AH, Villar RN. Is diagnostic arthroscopyof the hip worthwhile? A prospective review of 328 adults in-vestigated for hip pain. J Bone Joint Surg Br 1999;81-B:600-603.
2. Bare AA, Gaunche CA. Hip impingement: the role ofarthroscopy. Orthopedics 2005;28:266-273.
3. Bartlett CS, DiFelice GC, Buly RL et al. Cardiac arrest as a re-sult of intraabdominal extravasation of fluid during arthro-scopic removal of a loos body from the hip joint of a patientwith an acetabular fracture. J Orthop Trauma 1998;12:294-299.
4. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influ-ences the pattern of damage to the acetabular cartilage:Femoroacetabular impingement as a cause of early osteoarthri-tis of the hip. J Bone Joint Surg Br 2005;87-B:1012-1018.
5. Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. An-terior femoroacetabular impingement: Part II. Midterm resultsof surgical treatment. Clin Orthop Relat Res 2004:67-73.
6. Burman MS. Arthroscopy or the direct visualization of joints:an experimental cadaver study. J Bone Joint Surg 1931;29:669-695.
7. Bushnell BD, Anz AW, Bert JM. Venous thromboembolism inlower extremity arthroscopy. Arthroscopy 2008;24(5):604-611.
8. Byrd JWT, Jones KS. Diagnostic accuracy of clinical assess-ment, magnetic resonance imaging, magnetic resonancearthrography, and intra-articular injection in hip arthroscopypatients. Am J Sports Med 2004;32:1668-1674.
9. Byrd JWT, Jones KS. Hip arthroscopy in athletes. Clin SportsMed 2001;20(4):749-762.
10. Byrd JWT, Jones KS. Prospective analysis of hip arthroscopywith 2-year follow-up. Arthroscopy 2000;16:578-587.
11. Byrd JWT, Pappas JN, Pedley MJ. Hip arthroscopy: ananatomic study of portal placement and relationship to the ex-tra-articular structures. Arthroscopy 1995;11:418-423.
12. Byrd JWT. Hip Arthroscopy Utilizing the Supine Position.Arthroscopy 1994;10(3):275-280.
13. Byrd JWT. Avoiding the labrum in hip arthroscopy.Arthroscopy 2000;16:770-773.
14. Byrd JWT. Complications associated with hip arthroscopy. In:Byrd JWT (ed). Operative hip arthroscopy. 2nd Ed. New York,Springer, 2005:229-235.
15. Byrd JWT. Hip arthroscopy, the supine approach: techniqueand anatomy of the intrarticular and peripheral compart-ments. Tech Orthop 2005;20(1):17-31.
16. Chan YS, Lien LC, Hsu HL, Wan YL, Lee MS, Hsu KY, ShihCH. Evaluating hip labral tears using magnetic resonancearthrography: a prospective study comparing hip arthroscopyand magnetic resonance arthrography diagnosis. Arthroscopy2005;21(10):1250.e1-1250.e8.
245
Hip arthroscopy for femoro-acetabular impingement: personal technique and indications
17. Clarke MT, Arora A, Villar RN. Hip arthroscopy: complica-tions in 1054 cases. Clin Orthop Relat Res 2003;406:84-88.
18. Clohishy JC, Keeney JA, Schoenecker PL. Preliminary assess-ment and treatment guidelines for hip disorders in youngadults. Clin Orthop Relat Res 2005;441:168-179.
19. de Ridder VA, de Lange S, Popta Jv. Anatomical Variations ofthe Lateral Femoral Cutaneous Nerve and the Consequencesfor Surgery. J Orthop Trauma 1999;13(3):207-211.
20. Dienst M, Gödde S, Seil R, Hammer D, Kohn D. Hiparthroscopy without traction: In vivo anatomy of the peripher-al hip joint cavity. Arthroscopy 2001;17(9):924-931.
21. Dienst M. Hip arthroscopy: technique and anatomy. OperTech Sports Med 2005;13:13-23.
22. Dorfmann H, Boyer T, De Bie B. Arthoscopie de anche. RevRhum Mal Osteoartic 1988;55(1):33-36.
23. Dvorak M, Duncan CP, Day B. Arthroscopic anatomy of thehip. Arthroscopy 1990;6:264-273.
24. Eriksson E, Arvidsson I, Arvidsson H. Diagnostic and opera-tive arthroscopy of the hip. Orthopaedics 1986;9:169-176.
25. Espinosa N, Rothenfluh DA, Beck M, Ganz R, Leunig M.Treatment of femoro-acetabular impingement: preliminary re-sults of labral refixation. J Bone Joint Surg Am. 2006;88:925-935.
26. Ezoe M, Naito M, Inoue T. The prevalence of acetabularretroversion among various disorders of the hip. J Bone JointSurg Am 2006;88-A:372-379.
27. Funke EL, Munzinger U. Complications in hip arthroscopy.Arthroscopy 1996;12:156-159.
28. Ganz R, Gill TJ, Gautier E, Krugel N, Berlemann U. Surgicaldislocation of the adult hip: a technique with full access to thefemoral head and acetabulum without the risk of avascularnecrosis. J Bone Joint Surg Br 2001;83-B:1119-1124.
29. Ganz R, Leunig M, Leunig-Ganz K, Harris WH. The etiologyof osteoarthritis of the hip: an integrated mechanical concept.Clin Orthop Relat Res 2008;466(2):264-272.
30. Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, SiebenrockKA. Femoroacetabular impingement: A cause for osteoarthri-tis of the hip. Clin Orthop Relat Res 2003;417:112-120.
31. Gautier E, Ganz K, Krugel N, Gill TJ, Ganz R. Anatomy ofthe medial femoral circumflex artery and its surgical implica-tions. J Bone Joint Surg Br 2000;82-B:679-683.
32. Glick JM. Hip arthroscopy. The lateral approach. Clin SportsMed 2001;20:733-747.
33. Grothaus, MC, HoltM, Mekhail AO, Ebraheim NA, YeastingRA. Lateral Femoral Cutaneous Nerve: an anatomic study.Clin Orthop Relat Res 2005;437:164-168.
34. Haupt U, Völkle D, Waldherr C, Beck M. Intra- andretroperitoneal irrigation liquid after arthroscopy of the hipjoint. Arthroscopy 2008;24(8):966-968.
35. Ilizaliturri VM Jr, Orozco-Rodriguez L, Acosta-Rodríguez E,
246
Chapter 16
Camacho-Galindo J. Arthroscopic treatment of cam-typefemoroacetabular impingement: preliminary report at 2 yearsminimum follow-up. J Arthroplasty 2008;23(2):226-234.
36. Ito K, Minka MA II, Leunig M, Werlen S, Ganz R. Femoroac-etabular impingement and the cam-effect. A MRI-based quan-titative anatomical study of the femoral head-neck offset. JBone Joint Surg Br 2001;83-B:171-176.
37. Jamali AA, Mladenov K, Meyer DC, Martinez A, Beck M,Ganz R, Leunig M. Anteroposterior pelvic radiographs to as-sess acetabular retroversion: high validity of the “Cross-over-sign”. J Orthop Res 2007;25:758-765.
38. Kalberer F, Sierra RJ, Madan SS, Ganz R, Leunig M. Ischialspine projection into the pelvis: a new sign for acetabularretroversion. Clin Orthop Relat Res 2008;466(3):677-83.
39. Keene GS, Villar RN. Arthroscopic Anatomy of the Hip: AnIn Vivo Study. Arthroscopy 1994;10(4):392-399.
40. Keeney JA, Peelle MW, Jackson J, Rubin D, Maloney WJ, Clo-hisy JC. Magnetic resonance arthrography versus arthroscopyin the evaluation of articular hip pathology. Clin Orthop RelatRes 2004;429:163-169.
41. Kelly BT, Weiland DE, Schenker ML, Philippon MJ. Arthro-scopic labral repair in the hip: surgical technique and reviewof the literature. Arthroscopy. 2005;21:1496-1504.
42. Kim YT, Azuma H. The nerve endings of the acetabularlabrum. Clin Orthop Relat Res 1995;320:176–181.
43. Knuesel PR, Pfirrmann CW, Noetzli HP, Dora C, Zanetti M,Hodler J, Kuehn B. MR arthrography of the hip: diagnosticperformance of a dedicated water-excitation 3D double-echosteady-state sequence to detect cartilage lesions. Am JRoentgenol 2004;183(6):1729-1735.
44. Lavigne M, Parvizi J, Beck M, Siebenrock KA, Ganz R, Leu-nig M. Anterior femoroacetabular impingement: Part I. Tech-niques of joint preserving surgery. Clin Orthop Relat Res2004;418:61-66.
45. Leunig M, Beck M, Dora C, Ganz R. Femoroacetabular im-pingement: aetiology and surgical concepts. Op Tech Orthop2005;15:247-255.
46. Leunig M, Beck M, Stauffer E, Hertel R, Ganz R. Free nerveendings in the ligamentum capitis femoris. Acta Orthop Scand2000;71:452-454.
47. Leunig M, Beck M, Kalhor M, Kim YJ, Werlen S, Ganz R: Fi-brocystic changes at anterosuperior femoral neck: prevalencein hips with femoroacetabular impingement. Radiology2005;236:237-246.
48. Leunig M, Podeszwa D, Beck M, Werlen S, Ganz R. Magnet-ic resonance arthrography of labral disorders in hips with dys-plasia and impingement. Clin Orthop Relat Res 2004;418:74-80.
49. Leunig M, Werlen S, Ungersböck A, Ito K, Ganz R. Evalua-tion of the acetabular labrum by MR arthrography. J Bone
247
Hip arthroscopy for femoro-acetabular impingement: personal technique and indications
Joint Surg Br 1997;79-B(2):230-234. Erratum in: J Bone JointSurg Br 1997;79-B(4):693.
50. McCarthy JC, Day B, Busconi B. Hip arthroscopy: applica-tions and techniques. J Am Acad Orthop Surg 1995;3:115-122.
51. McCarthy JC, Lee J. Hip arthroscopy: indications, outcomes,and complications. Instr Course Lect 2006;55:301-308.
52. Monllau JC, Reina-de la Torre F, Puig L, Rodriguéz-Baeza A.Arthroscopic approaches to the hip joint. Tech Orthop2005;20(1):2-8.
53. Monllau JC, Solano A, Léon A, Hinarejos P, Ballester J. Tomo-graphic study of the arthroscopic approaches to the hip joint.Arthroscopy 2003;19(4):368-372.
54. Nötzli HP, Siebenrock KA, Hempfing A, Ramseier LE, GanzR. Perfusion of the femoral head during surgical dislocation ofthe hip: monitoring by laser doppler flowmetry. J Bone JointSurg Br 2002;84-B:300-304.
55. Philippon MJ, Stubbs AJ, Schenker ML, Maxwell RB, GanzR, Leunig M. Arthroscopic management of femoroacetabularimpingement: osteoplasty technique and literature review. AmJ Sports Med 2007;35:1571-1580.
56. Robertson WJ, Kelly BT. The safe zone for hip arthroscopy: acadaveric assessment of central, peripheral, and lateral com-partment portal placement. Arthroscopy 2008;24(9):1019-26.
57. Sampson TG, Arthroscopic treatment of femoroacetabular im-pingement: a proposed technique with clinical experience. In-str Course Lect 2006;55:337-346.
58. Sampson TG. Arthroscopic treatment of femoroacetabular im-pingement. Tech Orthop 2005;20(1):56-62.
59. Sampson TG. Complications of hip arthroscopy. Clin SportsMed 2001;20:831-835.
60. Schmid MR, Nötzli HP, Zanetti M, Wyss TF, Hodler J. Carti-lage lesions in the hip: diagnostic effectiveness of MR arthrog-raphy. Radiology. 2003;226:382-386.
61. Siebenrock KA, Schöniger R, Ganz R. Anterior femoro-ac-etabular impingement due to acetabular retroversion. Treat-ment with periacetabular osteotomy. J Bone Joint Surg Am2003;85-A(2):278-286.
62. Sussmann PS, Ranawat AS, Lipman J, Lorich DG, PadgettDE, Kelly BT. Arthroscopic versus open osteoplasty of thehead-neck junction: a cadaveric investigation. Arthroscopy2007;23(12):1257-64.
63. Sweeney HJ. Arthroscopy of the hip. Anatomy and portals.Clin Sports Med 2001;20:697-702.
64. Weiland DE, Philippon MJ. Arthroscopic technique offemoroacetabular impingement. Oper Tech Orthop2005;15(3):256-260.
65. Wenger DE, Kendell KR, Miner MR, Trousdale RT. Acetabu-lar labral tears rarely occur in the absence of bony abnormali-ties. Clin Orthop Relat Res 2004;426:145-150.
248
Chapter 16

INTRODUCTION
The wide differential diagnosis for hip-related pain, which in-cludes both extrarticular and intrarticular pathology as well as re-ferred symptoms from the lumbar spine and pelvis, leads to inher-ent complexity in patient evaluation and management (35, 42). For-tunately, the advances in hip arthroscopy and magnetic resonanceimaging (MRI) have increased the understanding of the associatedanatomy and pathology about the hip (35, 37). Moreover, these ad-vances have broadened arthroscopic applications to include treat-ment of intrarticular pathology such as femoroacetabular impinge-ment, labral tears, ligamentum teres tears, loose bodies, synovialchondromatosis, and chondral lesions (26).
Recently, hip arthroscopy has allowed visualization and subse-quent treatment of extrarticular pathology found in the per-itrochanteric compartment including: trochanteric bursitis, exter-nal coxa saltans or “snapping hip”, and gluteus medius and min-imus tears. These pathologies commonly manifest as tenderness topalpation in the region surrounding the greater trochanter andthus have been collectively referred to as greater trochanteric painsyndrome (GTPS) (35, 37). While historically this entity has beenunderappreciated, when recognized it has been treated either con-servatively (18) or with open surgery (20, 43). Conservative modali-ties have included anesthetic and steroid injections in combinationwith physical therapy, while refractory cases have been addressedwith open surgery (7, 20, 43). However, as we will describe, thesecases can now be treated in an arthroscopic fashion. For example,external coxa saltans can be effectively treated with arthroscopicrelease of the external snapping iliotibial band (ITB) (22). Gluteusmedius and minimus repairs, performed arthroscopically, have al-so been described and may address pain previously related to re-calcitrant trochanteric bursitis (37). In addition, refractorytrochanteric bursitis can be treated with arthroscopic trochantericbursectomy (18, 41). Arthroscopic treatment of these pathologieshas not only provided a minimally invasive surgical option for re-
249
THE PERITROCHANTERIC COMPARTMENTBryan T. KellyTravis G. Maak Michael B. Cross Peter D. Fabricant
Chapter 17

fractory patients, but has also advanced the knowledge of thesepathologic entities and the associated anatomy.
This chapter aims to review the current understanding of theperitrochanteric space including the patient evaluation, relevantanatomy, arthroscopic techniques and the associated pathologythat may be encountered and addressed.
PATIENT EVALUATION
Evaluation of hip pain requires conducting a comprehensivepatient history in order to differentiate between intrarticular andextrarticular pathology. Unlike intrarticular pathology, extrarticu-lar pathology often presents as lateral hip pain in the per-itrochanteric compartment. When this complaint is localized, fur-ther differentiation among various peritrochanteric pathologiescan then be achieved by focusing on characteristics specific toeach pathologic condition. These specific associations will be dis-cussed in the section specific to each disorder.
Following completion of the patient history, a thorough physi-cal examination of the hip joint and surrounding anatomy, specif-ically the lateral region of the hip, can then further narrow the dif-ferential to allow accurate diagnosis. In order to conduct an effec-tive physical examination, a complete knowledge of the aforemen-tioned origins and insertions of the hip musculature is required.Confounding intrarticular pathology that can refer to the per-itrochanteric region makes this understanding even more criticalas insertional pain may be the critical exam finding. Palpation ofthese regions may allow discrimination between intrarticular andextrarticular pathology as referred intrarticular pathology may oc-cur during active or passive hip motion, but should not create re-gions that are tender to direct palpation.
Muscle strength testing should also be conducted, specificallyfocused on comparing hip abductor function in painful and pain-less states. The hip should be placed in flexion to evaluate the ten-sor fascia latae, neutral for the gluteus medius, and extension forthe gluteus maximus. Moreover, the knee should be both flexedand extended to differentially tense and relax the ITB, respectively.
Finally, evaluation of abductor muscle contractures may beachieved using Ober’s test. This maneuver is commonly conduct-ed with the patient on his or her side while testing the hip in ex-tension to assess tensor fascia latae tension followed by knee flex-ion to relax the ITB. With the knee in flexion the gluteus mediuscontracture can be evaluated. Lastly, hip internal rotation shouldbe allowed such that the knee may contact the examination tablein a normal tension-free state.
ANATOMY
Advances in magnetic resonance imaging sequences as well asother radiographic techniques have increased the surgeon’s ability
250
Chapter 17
to identify intrarticular and extrarticular disorders around the hip.Improvements in instrumentation and arthroscopic techniqueshave provided increased visualization and subsequent treatmentof hip pathology. In addition, these advances both radiographical-ly and arthroscopically have furthered the understanding of intrar-ticular anatomy and the biomechanics of the hip. The current un-derstanding of extrarticular hip anatomy and pathology has alsobeen advanced by descriptions of arthroscopic approaches to andtreatment of disorders in the peritrochanteric compartment (37).
The greater trochanter (GT) is a reproducible, palpable land-mark to the peritrochanteric space. This osseous prominence aris-es at the junction of the femoral shaft and neck. Three greatertrochanteric bursae (the subgluteus maximus bursa, subgluteusmedius bursa, and gluteus minimus bursa)exist in most patientsand provide cushioning for the tensor fascia latae, ITB, and glu-teus tendons (2, 42). The subgluteus maximus bursa is the largestbursa and is located lateral to the greater trochanter between thegluteus maximus and medius tendons. This bursa has been furtherclassified into three subbursae: deep, secondary deep, and super-ficial subgluteus maximus bursa. The deep subgluteus maximusbursae is the largest of these subbursae and is also the most fre-quently implicated in GTPS (42).
Muscular attachments to the GT include the piriformis, obtu-rator externus and obturator internus, which attach medially andgluteus medius and minimus, which insert more laterally. The glu-teus medius tendon has insertional footprints on the lateral facetand superoposterior facet of the greater trochanter (33). The areaof the lateral facet footprint is larger and rectangular in shape,while the superoposterior facet is smaller, more robust and circu-lar. The gluteus minimus has long and capsular tendon footprints,which exist on the anterior facet of the greater trochanter (4). Fi-nally, the tensor fascia latae, ITB and gluteus maximus comprise afibromuscular sheath that lies superficial to the gluteus mediusand minimus tendons.
Arthroscopic evaluation of the potential space that forms theperitrochanteric compartment of the hip is easily allowed using re-producible anatomic landmarks. The borders of this potentialspace include the iliotibial band and tensor fascia latae laterally,vastus lateralis inferomedially, abductor tendons (i.e. gluteusmedius and minimus) superomedially, gluteus maximus muscle su-periorly and gluteus maximus tendon insertion on the linea asperaposteriorly. Efficient and complete evaluation of this space re-quires a routine, reproducible sequence to ensure that all patholo-gy is effectively evaluated and addressed.
ARTHROSCOPIC EVALUATION
The central, intrarticular compartment is first inspected withthe arthroscope to assess for concomitant hip pathology prior toexamining the lateral compartment of the hip, as degenerative
251
The peritrochanteric compartment

arthrosis may exist in the presence of degenerative abductor tears.With this done, complete attention is directed to the extrarticularspaces. The peritrochanteric compartment of the hip is then en-tered using the aforementioned anatomic landmarks. Thetrochanteric bursa is of variable thickness depending on thelength of symptoms and degree of inflammation and exists withinthis potential space.
Examination of the space is performed through the placementof three portals.
The first portal is the mid anterior portal. It provides the bestaccess into the peritrochanteric space. The portal is placed 2 cmlateral to the anterior superior iliac spine (ASIS) centered over thelateral prominence of the greater trochanter in the interval be-tween the tensor fascia latae and sartorius. The cannula is direct-ed into the peritrochanteric space with the leg in 0-20 degrees offlexion, 20 degrees of abduction, and 10-15 degrees of internal ro-tation. The cannula is aimed posterior and swept back and forthbetween the iliotibial band overlying the greater trochanteric bur-sa and the greater trochanter. This technique is analogous to ac-cessing the subacromial space in the shoulder where the iliotibialband is analogous to the undersurface of the acromion. When theportal is placed appropriately, a clear space lying between the ili-otibial band and the greater trochanter can be easily identified. Ifin doubt, cannula placement can be confirmed under fluoroscopy.The distal anterolateral accessory portal is placed midway betweenthe tip of the greater trochanter and the vastus tubercle along theposterior one-third of the greater trochanteric midline. This portalplacement facilitates access distally and proximally for both diag-nostic evaluation and operative intervention. The proximal an-terolateral accessory portal is placed proximal to the tip of thegreater trochanter in line with the distal anterolateral portal. Thisportal facilitates more proximal work, and can also be used formore distal visualization.
Proper portal placement is crucial to understanding the per-itrochanteric space and should be first oriented at the gluteusmaximus insertion into the linea aspera. Inspection should pro-ceed in a circular fashion starting distally and posterior at the glu-teus maximus insertion. This is done using the 70 degree scopeplaced into the anterior portal, and both the light source and cam-era are positioned proximally and oriented distally. The per-itrochanteric space is typically distended with approximately 50mmHg pressurization. Hemostasis can be obtained with either ra-diofrequency ablation or standard coagulation. Sometimes fibri-nous bands in this area will require excision.
TROCHANTERIC BURSITIS
Trochanteric bursitis is a common and often chronic inflam-matory condition in the elderly female with a history of repetitiveactivity such as long distance running, as well as iliotibial band
252
Chapter 17

(ITB) syndrome, coxa saltans, hip arthroplasty or osteotomy, andlow back pain (11-13, 16, 36, 41). Schapira et al (34) elaborated on thisbroad differential diagnosis in a 2-year follow-up observationalstudy of 72 patients with symptomatic trochanteric bursitis. Thisstudy documented 91.6% of these patients had concomitantpathology including osteoarthritis of the ipsilateral hip or lumbarspine. Despite these confounding factors and broad differential,however, careful physical and radiographic evaluations can effec-tively diagnosis trochanteric bursitis.
The patient history and physical examination provide the firstcritical step in narrowing the wide differential diagnosis.Trochanteric bursitis most commonly occurs in middle aged fe-males with a female to male predilection of 4:1, although an in-creasing incidence in the young, active population has been re-cently identified (3, 17, 39). The typical patient presentation includesa history of pain localized to the greater trochanter as well as radi-ation down the lateral thigh or into the buttock. The pain may bechronic and activity-related, as well as exacerbated with directpressure on the inflamed bursa such as that which occurs with ly-ing on the affected side. In addition, tenderness can be elicitedwith direct palpation of this region during the physical examina-tion. Further examination may reveal a positive Patrick-FABERE(flexion, abduction, external rotation and extension) test and painwith abduction against resistance. The previously described Obertest has also been used to assess the tension of the iliotibial band,with a positive result when high tension exists.
The history and physical examination can be supplementedwith radiographic and other diagnostic modalities including plainradiographs, dynamic ultrasound, MRI, and corticosteroid/anes-thetic injections. The utility of corticosteroid/anesthetic injectioninto the greater trochanteric bursa for both diagnosis and treat-ment has significantly reduced the utility of MRI for diagnosis oftrochanteric bursitis. Previous data have documented resolutionof symptoms in 66% of cases and reduction in 33% for patientstreated non-operatively with this modality (16). Nevertheless, de-spite its clear efficacy, repeated or incorrectly positioned injectionshave been associated with gluteus medius injury and thus thismodality should be used carefully (29). Failure to respond to thistreatment may prompt further radiographic investigation includ-ing: plain radiographs to evaluate for loose bodies or synovialchondromatosis, diagnostic ultrasound to evaluate for gluteusmedius tears, gluteus minimus tears and external coxa saltans, andMRI to exclude these tears, as well as assess the degree of inflam-mation in the greater trochanteric bursa (3, 25, 35). Previous retro-spective data in patients with greater trochanteric pain syndromehas documented an incidence of gluteus medius tendonitis in62.5%, gluteus medius tears in 45.8%, and trochanteric bursitis inonly 8.3%(5).
When trochanteric bursitis is suspected, either non-operativeor operative management may be required for effective treatment.
253
The peritrochanteric compartment
Non-operative management should be the mainstay of treatmentexcept in refractory cases. In addition to the aforementionedgreater trochanteric anesthetic/corticosteroid injections, non-op-erative treatment includes rest, anti-inflammatory medication, ice,and physical therapy including flexibility training, stretching andimprovement in gait kinematics (34, 35, 42). Refractory cases may re-quire operative intervention through either open or arthroscopictechniques (7, 18, 20, 41, 43). Both techniques describe excision of thegreater trochanteric bursa and have been associated with signifi-cant improvements in pain and Harris Hip Scores in previousstudies(3, 18).
Following portal placement and initial diagnostic arthroscopy,the initial arthroscopic view includes the insertion of the gluteusmaximus into the posterior border of the iliotibial band, which isthe starting point to begin a step wise inspection of the space. Thisinsertion can be probed and the bursa can be cleaned from thisarea with a motorized shaver. Looking proximally with the cam-era, the longitudinal lines of the vastus lateralis are identified andcan be traced up to the insertion at the vastus tubercle looking im-mediately anterior to the anterior facet. The gluteus minimus ten-don and muscle are visualized anteriorly with the scope sourceand camera placed laterally looking anterosuperior. As the scopeis rotated superiorly, the gluteus medius will come into view withits insertion into the greater trochanter. It should be thoroughlyprobed and visualized to identify the presence of full-thicknesstendon insertional tears. Further release of the fibrinous bands ofthe trochanteric bursa overlying this area may be required for bet-ter access and visualization through the posterior portal. In casesof trochanteric bursitis, these fibrous bands are inflamed and canbe thick. Use of electrocautery or an arthroscopic 5.5mm shaver isuseful to remove this tissue. Finally, the scope should be turnedtoward the iliotibial band. In particular, the posterior one third ofthe iliotibial band is implicated in coxa saltans externus and maycause direct abrasive wear to the greater trochanter.
EXTERNAL COXA SALTANS-SNAPPING HIP
External Coxa Saltans is commonly described as a palpable oraudible snapping of the hip during flexion and extension (1, 32, 40).These symptoms often occur during athletic activities that requireflexion, extension and abduction, but may also occur during activ-ities of daily living. The patient history often includes a traumaticevent prior to the onset of the snapping sensation. The physicalexamination should begin in a supine position and then thegreater trochanter should be palpated as the hip is flexed. A pal-pable snapping sensation overlying the greater trochanter may beelicited and can often be eliminated with direct pressure at theproximal aspect of the greater trochanter. In addition to historyand physical examination findings, radiographic evaluation is crit-ical and includes plain radiographs to identify loose bodies or syn-
254
Chapter 17

ovial chondromatosis as well as dynamic ultrasonography (10).MRI rarely aids in the diagnosis of a snapping hip.
The anatomic structures visualized by dynamic ultrasound forexternal coxa saltans typically include structures immediatelyoverlying the greater trochanter such as the iliotibial band (ITB)and the anterior border of the gluteus maximus. Although intraar-ticular structures have been suggested as contributing to snappinghip, most commonly a thick, tense ITB or gluteus maximus ten-don is the causative structure. Extension of the hip places the ITBposterior to the greater trochanter and flexion forces an anteriortranslation of the ITB over the greater trochanter which, whilephysiologic, may also create a snapping sensation and resultant in-flammation and pain.
In most cases, non-operative treatment of this painful, snap-ping sensation is effective. This methodology includes rest,stretching, activity modification, physical therapy, oral anti-inflam-matory medications and corticosteroid injections (1, 23). Whilerare, failure of non-operative management of external coxa saltansmay require operative intervention. Open surgical techniques forrecalcitrant external coxa saltans have been previously describedand include partial excision of the ITB overlying the greatertrochanter as well as greater trochanteric bursectomy (43). A moreminimally invasive approach may also be employed in which a z-plasty of the ITB is performed. White et al (40) also reported per-forming relaxing, transverse step cuts along a 10 cm longitudinalincision in the fascia overlying the greater trochanter.
Given the rarity of these cases, however, retrospective out-come studies on operative intervention have produced mixed re-sults although relief has been demonstrated in a majority of cas-es (6, 32). A review of 9 patients with symptomatic external coxasaltans with 22.9 month mean follow up demonstrated completeresolution of snapping and 7 out of 7 patients returned to full ac-tivity (32). White et al (40) reviewed 16 patients treated with thetransverse step cut technique and documented 87.5% resolutionof symptoms at a mean of 32.5 months post-operatively.
If the presence of coxa saltans externus is identified (or snap-ping of the iliotibial band over this area) and it has been refracto-ry to non-operative treatment, a release may be required with theuse of an electrocautery device or beaver blade. The releaseshould be performed along the posterolateral portion of thegreater trochanter beginning at the vastus tubercle insertion ex-tending to the tip of the greater trochanter in a z-type fashion, 1cm anterior, 3 cm distal, and 1 cm posterior, with slight variationsof this being required by digital and instrumented palpation inview of the particular fibers under the greatest amount of tension.
Notably, this procedure is uncommonly performed in isolationbut may be useful after abductor repair as this may aid in reduc-ing impingement of the iliotibial band on the repaired gluteusmedius.
255
The peritrochanteric compartment

GLUTEUS MEDIUS AND MINIMUS TEARS
Tears at the insertion of the gluteus medius and minimus atthe greater trochanter have been compared with similar insertion-al tears of the rotator cuff tendons at the greater tuberosity of thehumerus (8, 24, 27). These similarities have resulted in the coining ofthe term “Rotator Cuff Tears of the Hip” to describe insertionaltears of the gluteus medius and minimus. These tears are morecommonly identified in the gluteus medius and can occur as fullthickness, partial thickness and interstitial tears (28, 33). In a man-ner similar to the rotator cuff of the shoulder, calcific tendonitiscan present at the hip and can be related to gluteus medius andminimus tears (9, 19, 30). This pathologic condition can contributeto the process of injury and subsequent degeneration beginningwith tendinosis and progressing to eventual tearing in either thegluteus medius, minimus, or both.
The actual incidence and prevalence of these tears is currentlyunknown; however, recent data suggests that tears may occur inup to 10% and 25% of middle-aged men and women, respective-ly. It has been postulated that this increased female prevalencemay be due to the wider female pelvis (8, 21, 28, 31, 35). Femoral neckfractures have also been associated with these tears, with a 22%tear incidence documented in 50 patients with femoral neck frac-tures (8). In addition, Howell et al (21). documented a 20% preva-lence of degenerative tears in a prospective study of 176 patientswith osteoarthritis who were planned for total hip arthroplasty.
As previously mentioned, accurate treatment of gluteusmedius and minimus tears requires a focused history, physical ex-amination, radiographic evaluation and pre-operative planning.Symptoms related to gluteus medius and minimus tears common-ly present as tenderness to palpation at the greater trochanteric in-sertion, lateral hip pain, and hip abductor weakness (31, 35). Theonset of these symptoms is most often insidious and atraumatic,although traumatic events may be described. A prolonged single-leg stance may reproduce the described pain (31). Physical exami-nation may also elicit weakness and pain with resisted external ro-tation in ninety degrees of hip flexion or resisted abduction withhip extension.
In addition to history and physical examination, radiographicevaluation is crucial to accurate diagnosis and may include plainradiographs, ultrasound, and magnetic resonance imaging. Plainradiographs commonly do not demonstrate evidence of pathology;however, calcific tendonosis may be visible at the greatertrochanteric insertion. Ultrasonographic evidence of increased flu-id and thickened abductor tendons can be indicative of tendinosisor tendon tear (14, 28). However, confirmation of gluteus medius orminimus tendon tears often requires MRI, especially in the settingof concurrent acute or refractory trochanteric bursitis. Moreover,recent advances in MRI allow differentiation between partial andfull-thickness tears as well as intrasubstance fatty atrophy. Cvitan-
256
Chapter 17
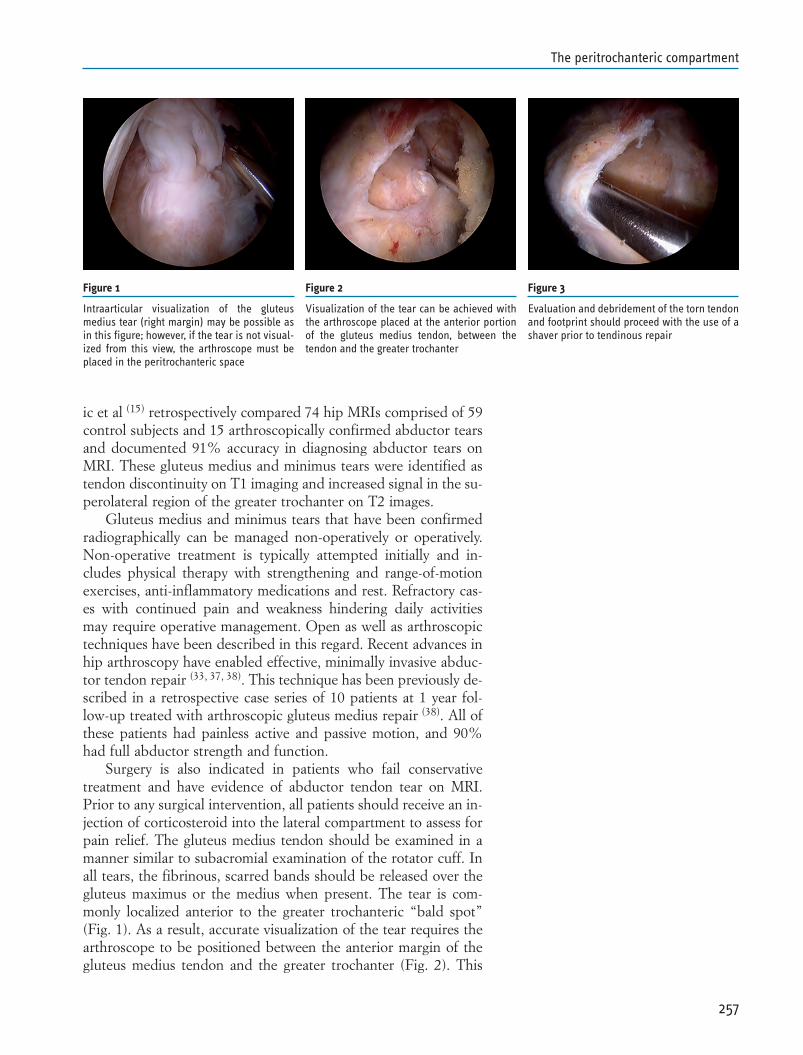
ic et al (15) retrospectively compared 74 hip MRIs comprised of 59control subjects and 15 arthroscopically confirmed abductor tearsand documented 91% accuracy in diagnosing abductor tears onMRI. These gluteus medius and minimus tears were identified astendon discontinuity on T1 imaging and increased signal in the su-perolateral region of the greater trochanter on T2 images.
Gluteus medius and minimus tears that have been confirmedradiographically can be managed non-operatively or operatively.Non-operative treatment is typically attempted initially and in-cludes physical therapy with strengthening and range-of-motionexercises, anti-inflammatory medications and rest. Refractory cas-es with continued pain and weakness hindering daily activitiesmay require operative management. Open as well as arthroscopictechniques have been described in this regard. Recent advances inhip arthroscopy have enabled effective, minimally invasive abduc-tor tendon repair (33, 37, 38). This technique has been previously de-scribed in a retrospective case series of 10 patients at 1 year fol-low-up treated with arthroscopic gluteus medius repair (38). All ofthese patients had painless active and passive motion, and 90%had full abductor strength and function.
Surgery is also indicated in patients who fail conservativetreatment and have evidence of abductor tendon tear on MRI.Prior to any surgical intervention, all patients should receive an in-jection of corticosteroid into the lateral compartment to assess forpain relief. The gluteus medius tendon should be examined in amanner similar to subacromial examination of the rotator cuff. Inall tears, the fibrinous, scarred bands should be released over thegluteus maximus or the medius when present. The tear is com-monly localized anterior to the greater trochanteric “bald spot”(Fig. 1). As a result, accurate visualization of the tear requires thearthroscope to be positioned between the anterior margin of thegluteus medius tendon and the greater trochanter (Fig. 2). This
257
The peritrochanteric compartment
Figure 1
Intraarticular visualization of the gluteusmedius tear (right margin) may be possible asin this figure; however, if the tear is not visual-ized from this view, the arthroscope must beplaced in the peritrochanteric space
Figure 2
Visualization of the tear can be achieved withthe arthroscope placed at the anterior portionof the gluteus medius tendon, between thetendon and the greater trochanter
Figure 3
Evaluation and debridement of the torn tendonand footprint should proceed with the use of ashaver prior to tendinous repair
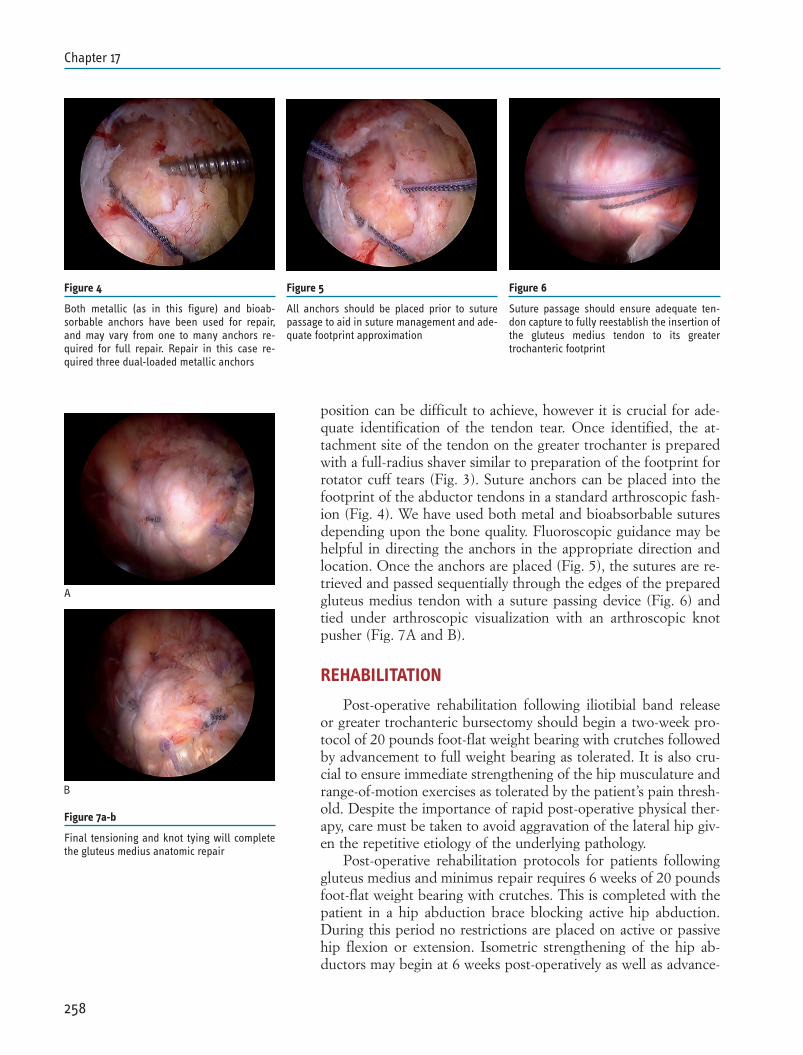
position can be difficult to achieve, however it is crucial for ade-quate identification of the tendon tear. Once identified, the at-tachment site of the tendon on the greater trochanter is preparedwith a full-radius shaver similar to preparation of the footprint forrotator cuff tears (Fig. 3). Suture anchors can be placed into thefootprint of the abductor tendons in a standard arthroscopic fash-ion (Fig. 4). We have used both metal and bioabsorbable suturesdepending upon the bone quality. Fluoroscopic guidance may behelpful in directing the anchors in the appropriate direction andlocation. Once the anchors are placed (Fig. 5), the sutures are re-trieved and passed sequentially through the edges of the preparedgluteus medius tendon with a suture passing device (Fig. 6) andtied under arthroscopic visualization with an arthroscopic knotpusher (Fig. 7A and B).
REHABILITATION
Post-operative rehabilitation following iliotibial band releaseor greater trochanteric bursectomy should begin a two-week pro-tocol of 20 pounds foot-flat weight bearing with crutches followedby advancement to full weight bearing as tolerated. It is also cru-cial to ensure immediate strengthening of the hip musculature andrange-of-motion exercises as tolerated by the patient’s pain thresh-old. Despite the importance of rapid post-operative physical ther-apy, care must be taken to avoid aggravation of the lateral hip giv-en the repetitive etiology of the underlying pathology.
Post-operative rehabilitation protocols for patients followinggluteus medius and minimus repair requires 6 weeks of 20 poundsfoot-flat weight bearing with crutches. This is completed with thepatient in a hip abduction brace blocking active hip abduction.During this period no restrictions are placed on active or passivehip flexion or extension. Isometric strengthening of the hip ab-ductors may begin at 6 weeks post-operatively as well as advance-
258
Chapter 17
Figure 4
Both metallic (as in this figure) and bioab-sorbable anchors have been used for repair,and may vary from one to many anchors re-quired for full repair. Repair in this case re-quired three dual-loaded metallic anchors
Figure 5
All anchors should be placed prior to suturepassage to aid in suture management and ade-quate footprint approximation
Figure 6
Suture passage should ensure adequate ten-don capture to fully reestablish the insertion ofthe gluteus medius tendon to its greatertrochanteric footprint
Figure 7a-b
Final tensioning and knot tying will completethe gluteus medius anatomic repair
A
B

ment to full weight bearing. Strengthening and activity is furtheradvanced at 12 weeks, although running is restricted until sym-metric, bilateral abductor strength is demonstrated on examina-tion. This restriction ensures adequate symmetric pelvic support.
SUMMARY
A thorough understanding of the peritrochanteric compart-ment and greater trochanteric pain syndrome is important to theorthopaedic surgeon given the high prevalence in the population.Effective identification and evaluation of the underlying disordersincluding gluteus medius and minimus tears, external coxa saltansand trochanteric bursitis is crucial to guiding appropriate treat-ment modalities. Efficiently utilizing the patient history and phys-ical examination in combination with the radiographic evaluationand a diagnostic injection will enable the treating physician to cor-rectly identify and manage a patient presenting with lateral hippain. Non-operative management remains the mainstay of treat-ment for these disorders; however, refractory cases may requireoperative intervention. Advances in arthroscopic techniques haveprovided a more effective and less invasive method to identify andtreat patients with recalcitrant greater trochanteric pain syndrome.
259
The peritrochanteric compartment
REFERENCES
1. Allen, W. C., and Cope, R.: Coxa Saltans: The Snapping HipRevisited. J Am Acad Orthop Surg, 3(5): 303-308, 1995.
2. Armfield, D. R.; Towers, J. D.; and Robertson, D. D.: Radi-ographic and MR imaging of the athletic hip. Clin Sports Med,25(2): 211-39, viii, 2006.
3. Baker, C. L., Jr.; Massie, R. V.; Hurt, W. G.; and Savory, C. G.:Arthroscopic bursectomy for recalcitrant trochanteric bursitis.Arthroscopy, 23(8): 827-32, 2007.
4. Beck, M.; Sledge, J. B.; Gautier, E.; Dora, C. F.; and Ganz, R.:The anatomy and function of the gluteus minimus muscle. JBone Joint Surg Br, 82(3): 358-63, 2000.
5. Bird, P. A.; Oakley, S. P.; Shnier, R.; and Kirkham, B. W.:Prospective evaluation of magnetic resonance imaging andphysical examination findings in patients with greatertrochanteric pain syndrome. Arthritis Rheum, 44(9): 2138-45,2001.
6. Brignall, C. G., and Stainsby, G. D.: The snapping hip. Treat-ment by Z-plasty. J Bone Joint Surg Br, 73(2): 253-4, 1991.
7. Brooker, A. F., Jr.: The surgical approach to refractorytrochanteric bursitis. Johns Hopkins Med J, 145(3): 98-100,1979.
8. Bunker, T. D.; Esler, C. N.; and Leach, W. J.: Rotator-cuff tearof the hip. J Bone Joint Surg Br, 79(4): 618-20, 1997.
9. Callaghan, B. D.: Unusual calcification in the region of thegluteus medius and minimus muscles. Australas Radiol, 21(4):362-6, 1977.
10. Choi, Y. S.; Lee, S. M.; Song, B. Y.; Paik, S. H.; and Yoon, Y.K.: Dynamic sonography of external snapping hip syndrome. JUltrasound Med, 21(7): 753-8, 2002.
11. Clancy, W. G.: Runners’ injuries. Part two. Evaluation andtreatment of specific injuries. Am J Sports Med, 8(4): 287-9,1980.
12. Collee, G.; Dijkmans, B. A.; Vandenbroucke, J. P.; and Cats,A.: Greater trochanteric pain syndrome (trochanteric bursitis)in low back pain. Scand J Rheumatol, 20(4): 262-6, 1991.
13. Collee, G.; Dijkmans, B. A.; Vandenbroucke, J. P.; Rozing, P.M.; and Cats, A.: A clinical epidemiological study in low backpain. Description of two clinical syndromes. Br J Rheumatol,29(5): 354-7, 1990.
14. Connell, D. A.; Bass, C.; Sykes, C. A.; Young, D.; and Ed-wards, E.: Sonographic evaluation of gluteus medius and min-imus tendinopathy. Eur Radiol, 13(6): 1339-47, 2003.
15. Cvitanic, O.; Henzie, G.; Skezas, N.; Lyons, J.; and Minter, J.:MRI diagnosis of tears of the hip abductor tendons (gluteusmedius and gluteus minimus). AJR Am J Roentgenol, 182(1):137-43, 2004.
16. Ege Rasmussen, K. J., and Fano, N.: Trochanteric bursitis.
260
Chapter 17
Treatment by corticosteroid injection. Scand J Rheumatol,14(4): 417-20, 1985.
17. Farr, D.; Selesnick, H.; Janecki, C.; and Cordas, D.: Arthro-scopic bursectomy with concomitant iliotibial band release forthe treatment of recalcitrant trochanteric bursitis. Arthroscopy,23(8): 905 e1-5, 2007.
18. Fox, J. L.: The role of arthroscopic bursectomy in the treat-ment of trochanteric bursitis. Arthroscopy, 18(7): E34, 2002.
19. Gordon, E. J.: Trochanteric bursitis and tendinitis. Clin Or-thop, 20: 193-202, 1961.
20. Govaert, L. H.; van der Vis, H. M.; Marti, R. K.; and Albers,G. H.: Trochanteric reduction osteotomy as a treatment for re-fractory trochanteric bursitis. J Bone Joint Surg Br, 85(2): 199-203, 2003.
21. Howell, G. E.; Biggs, R. E.; and Bourne, R. B.: Prevalence ofabductor mechanism tears of the hips in patients with os-teoarthritis. J Arthroplasty, 16(1): 121-3, 2001.
22. Ilizaliturri, V. M., Jr.; Villalobos, F. E., Jr.; Chaidez, P. A.;Valero, F. S.; and Aguilera, J. M.: Internal snapping hip syn-drome: treatment by endoscopic release of the iliopsoas ten-don. Arthroscopy, 21(11): 1375-80, 2005.
23. Jacobson, T., and Allen, W. C.: Surgical correction of the snap-ping iliopsoas tendon. Am J Sports Med, 18(5): 470-4, 1990.
24. Kagan, A., 2nd: Rotator cuff tears of the hip. Clin Orthop Re-lat Res, (368): 135-40, 1999.
25. Karpinski, M. R., and Piggott, H.: Greater trochanteric painsyndrome. A report of 15 cases. J Bone Joint Surg Br, 67(5):762-3, 1985.
26. Kelly, B. T.; Williams, R. J., 3rd; and Philippon, M. J.: Hiparthroscopy: current indications, treatment options, and man-agement issues. Am J Sports Med, 31(6): 1020-37, 2003.
27. Kingzett-Taylor, A.; Tirman, P. F.; Feller, J.; McGann, W.; Pri-eto, V.; Wischer, T.; Cameron, J. A.; Cvitanic, O.; and Genant,H. K.: Tendinosis and tears of gluteus medius and minimusmuscles as a cause of hip pain: MR imaging findings. AJR AmJ Roentgenol, 173(4): 1123-6, 1999.
28. Kong, A.; Van der Vliet, A.; and Zadow, S.: MRI and US ofgluteal tendinopathy in greater trochanteric pain syndrome.Eur Radiol, 17(7): 1772-83, 2007.
29. LaBan, M. M.; Weir, S. K.; and Taylor, R. S.: ‘Bald trochanter’spontaneous rupture of the conjoined tendons of the gluteusmedius and minimus presenting as a trochanteric bursitis. AmJ Phys Med Rehabil, 83(10): 806-9, 2004.
30. Leonard, M. H.: Trochanteric syndrome; calcareous and non-calcareous tendonitis and bursitis about the trochanter major.J Am Med Assoc, 168(2): 175-7, 1958.
31. Lequesne, M.; Mathieu, P.; Vuillemin-Bodaghi, V.; Bard, H.;and Djian, P.: Gluteal tendinopathy in refractory greatertrochanter pain syndrome: diagnostic value of two clinicaltests. Arthritis Rheum, 59(2): 241-6, 2008.
261
The peritrochanteric compartment
32. Provencher, M. T.; Hofmeister, E. P.; and Muldoon, M. P.: Thesurgical treatment of external coxa saltans (the snapping hip)by Z-plasty of the iliotibial band. Am J Sports Med, 32(2): 470-6, 2004.
33. Robertson, W. J.; Gardner, M. J.; Barker, J. U.; Boraiah, S.;Lorich, D. G.; and Kelly, B. T.: Anatomy and dimensions ofthe gluteus medius tendon insertion. Arthroscopy, 24(2): 130-6, 2008.
34. Schapira, D.; Nahir, M.; and Scharf, Y.: Trochanteric bursitis:a common clinical problem. Arch Phys Med Rehabil, 67(11):815-7, 1986.
35. Tibor, L. M., and Sekiya, J. K.: Differential diagnosis of painaround the hip joint. Arthroscopy, 24(12): 1407-21, 2008.
36. Tortolani, P. J.; Carbone, J. J.; and Quartararo, L. G.: Greatertrochanteric pain syndrome in patients referred to orthopedicspine specialists. Spine J, 2(4): 251-4, 2002.
37. Voos, J. E.; Rudzki, J. R.; Shindle, M. K.; Martin, H.; and Kel-ly, B. T.: Arthroscopic anatomy and surgical techniques forperitrochanteric space disorders in the hip. Arthroscopy,23(11): 1246 e1-5, 2007.
38. Voos, J. E.; Shindle, M. K.; Pruett, A.; Asnis, P. D.; and Kelly,B. T.: Endoscopic repair of gluteus medius tendon tears of thehip. Am J Sports Med, 37(4): 743-7, 2009.
39. Walker, P.; Kannangara, S.; Bruce, W. J.; Michael, D.; and Vander Wall, H.: Lateral hip pain: does imaging predict responseto localized injection? Clin Orthop Relat Res, 457: 144-9,2007.
40. White, R. A.; Hughes, M. S.; Burd, T.; Hamann, J.; and Allen,W. C.: A new operative approach in the correction of externalcoxa saltans: the snapping hip. Am J Sports Med, 32(6): 1504-8, 2004.
41. Wiese, M.; Rubenthaler, F.; Willburger, R. E.; Fennes, S.; andHaaker, R.: Early results of endoscopic trochanter bursectomy.Int Orthop, 28(4): 218-21, 2004.
42. Williams, B. S., and Cohen, S. P.: Greater trochanteric painsyndrome: a review of anatomy, diagnosis and treatment.Anesth Analg, 108(5): 1662-70, 2009.
43. Zoltan, D. J.; Clancy, W. G., Jr.; and Keene, J. S.: A new oper-ative approach to snapping hip and refractory trochantericbursitis in athletes. Am J Sports Med, 14(3): 201-4, 1986.
262
Chapter 17


in collaborazione con








![Food & Packaging Catalogue - globalfw.com.au · A 12211035 Bertagni Ravioli Buffalo Mozzarella 250g [6] Ctn 1 A 12211040 Zini Agnoloti Lobster & Ricotta 1kg Pkt 1 A 12211065 Zini](https://img.pdfslide.us/doc/110x75/5c66fd3509d3f252168d2b6a/food-packaging-catalogue-a-12211035-bertagni-ravioli-buffalo-mozzarella.jpg)