Embed Size (px)
Citation preview
Rate of Obstructive Coronary Disease Rate of Obstructive Coronary Disease in Elective Diagnostic Cathin Elective Diagnostic Cath
Manesh R. Patel, MDManesh R. Patel, MD
Assistant Professor of MedicineAssistant Professor of Medicine
Director Cath Lab Research – Duke University Medical CenterDirector Cath Lab Research – Duke University Medical Center
DisclosuresDisclosures
Interventional cardiologistInterventional cardiologist Clinical Cardiovascular MRI and Vascular Clinical Cardiovascular MRI and Vascular
UltrasoundUltrasound
Division of CardiologyDivision of Cardiology Majority of Revenue from cardiovascular Majority of Revenue from cardiovascular
imagingimaging
GenzymeGenzyme Advisory BoardAdvisory Board
Chair of Writing Group for ACC/AHA Coronary Chair of Writing Group for ACC/AHA Coronary Revascularization Appropriateness CriteriaRevascularization Appropriateness Criteria
The Challenge in Cardiology PracticeThe Challenge in Cardiology Practice

Patient Case - Mrs. MPatient Case - Mrs. M
58 years old with DM58 years old with DM
Lives independentlyLives independently Shops, Cleans, works in bankShops, Cleans, works in bank
7/08 seen by PCP 7/08 seen by PCP Occasional Chest “ache” with walking at grocery Occasional Chest “ache” with walking at grocery
storestore Cramping in calves Cramping in calves
Referred to Duke Cardiology / Vascular Clinic for Referred to Duke Cardiology / Vascular Clinic for evaluationevaluation

What would you do?What would you do?
How do you determine risk and identify How do you determine risk and identify disease?disease?
What data do you need to determine if invasive What data do you need to determine if invasive angiography and subsequent coronary angiography and subsequent coronary revascularization will improve here symptoms revascularization will improve here symptoms and/or longevityand/or longevity

Step 1 - How do you decide pre-test probabilityStep 1 - How do you decide pre-test probability

Clinical Decision Making - Question 1Clinical Decision Making - Question 1
Which is the best model to calculate pretest Which is the best model to calculate pretest probability of CAD in this patient?probability of CAD in this patient?
A. Framingham Risk ScoreA. Framingham Risk Score
B. Diamond Forrester ScoreB. Diamond Forrester Score
C. TIMI UA/NSTEMI ScoreC. TIMI UA/NSTEMI Score
D. GRACE ScoreD. GRACE Score

Decision Question 2Decision Question 2
Based on the Diamond-Forrester Based on the Diamond-Forrester classification, the pretest probability of this classification, the pretest probability of this patient having CAD is:patient having CAD is:
A.A. Very LowVery Low
B.B. LowLow
C.C. IntermediateIntermediate
D.D. HighHigh

Stratifying patients with Chest painStratifying patients with Chest pain
Intermediate Probability = 10-90%Intermediate Probability = 10-90%
ACC/AHA Chronic Stable Angina GuidelinesACC/AHA Chronic Stable Angina Guidelines

Question # 1Question # 1
In patients with intermediate pre-test probability of In patients with intermediate pre-test probability of coronary artery disease - what cardiovascular test coronary artery disease - what cardiovascular test should be done to diagnose and risk stratify for should be done to diagnose and risk stratify for coronary artery disease?coronary artery disease?

Imaging Use Imaging Use
Non-invasive cardiac imaging has improved Non-invasive cardiac imaging has improved assessment of cardiac function, anatomy, and assessment of cardiac function, anatomy, and pathology.pathology.

Imaging UseImaging Use
Medicare spending on imaging services more than Medicare spending on imaging services more than doubled from 2000 through 2006doubled from 2000 through 2006
Source: GAO Analysis of Medicare Data, Report GAO-08-452.


How good are we at identifying obstructive CAD?
All ACC-NCDR patients who had cardiac catheterization
1,989,779 patients at 663 sites
Exclude: Prior MI, PCI, CABG, Cardiac Transplant, Valve surgery
629,325 patients at 663 sites
1,148,405 patients at 663 sites
Exclude: Emergent admission symptoms (AMI and ACS) and cardiogenic shock
397,954 patients at 663 sites
Exclude: other diagnostic cath indications
Rate of Obstructive CAD*
60.3%
36.2%
37.5%
51.7%
January 2004-April 2008January 2004-April 2008

Rate of Obstructive CADRate of Obstructive CAD
Obstructive CADObstructive CAD ≥ ≥ 50% LM or ≥ 70% Epicardial Vessel 50% LM or ≥ 70% Epicardial Vessel 38%38% ≥ ≥ 50% Any vessel 50% Any vessel 41%41%
Minimal CADMinimal CAD < 20% stenosis in any vessel< 20% stenosis in any vessel 39%39%entire cohortentire cohort

Obstructive CAD Disease At Cath (NCDR data)Obstructive CAD Disease At Cath (NCDR data)
397,954 patients 2004-2008 without known CAD/MI or 397,954 patients 2004-2008 without known CAD/MI or prior PCI/CABG undergoing diagnostic cath to R/O CADprior PCI/CABG undergoing diagnostic cath to R/O CAD
59% of patients with positive non-invasive tests have no 59% of patients with positive non-invasive tests have no obstructive CAD on invasive angiography (obstructive CAD on invasive angiography (False positiveFalse positive))
All Patients
No Stress Test
Positive Stress Result
Equivocal Stress Result
Negative Stress Result
All patients 376,430 16% 68% 4% 12%
No CAD 233,518 (62%)
65% 59% 73% 72%
CAD 142,912 (38%)
35% 41% 27% 28%
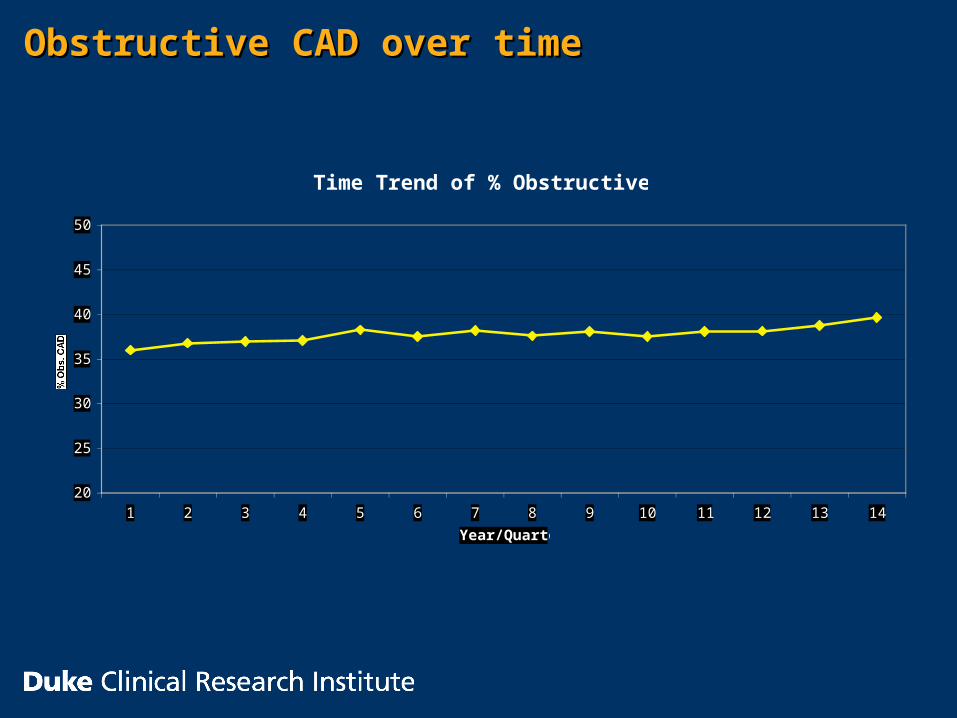
Obstructive CAD over timeObstructive CAD over time
Time Trend of % Obstructive CAD
20
25
30
35
40
45
50
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Year/Quarter
% Obs. CAD

ACC-NCDR StudyACC-NCDR Study
Current risk stratification including non-invasive Current risk stratification including non-invasive testing used to inform decisions to perform testing used to inform decisions to perform angiography to identify obstructive CAD need angiography to identify obstructive CAD need significant improvementsignificant improvement


![Manesh B. Kokare, Ph.D. (IIT Kharagpur)...[32] Prasanna Porwal, Samiksha Pachade, Ravi Kamble, Manesh Kokare, Girish Deshmukh, Vivek Sahasrabuddhe, and Fabrice Meriaudeau, “Indian](https://img.pdfslide.us/doc/110x75/5eda0d24b3745412b570ac9e/manesh-b-kokare-phd-iit-kharagpur-32-prasanna-porwal-samiksha-pachade.jpg)
![Manesh B. Kokare, Ph.D. (IIT Kharagpur) · [26]. Aarti Manjramkar and Manesh Kokare, “Automated Red Lesion Detection Algorithms: An Overview” Springer Journal of Medical and Biological](https://img.pdfslide.us/doc/110x75/5ec7ec11b0586619b6106c80/manesh-b-kokare-phd-iit-kharagpur-26-aarti-manjramkar-and-manesh-kokare.jpg)