Embed Size (px)
Citation preview
Poster Design & Printing by Genigraphics® - 800.790.4001
Rare Congenital Sinonasal Teratoma with Rare Congenital Sinonasal Teratoma with Intracranial InvolvementIntracranial Involvement
Jesse Knight, MD, W. Edward Wood, MDDepartment of Otolaryngology, Geisinger Medical Center
Danville, Pennsylvania
INTRODUCTION DISCUSSION
Imaging
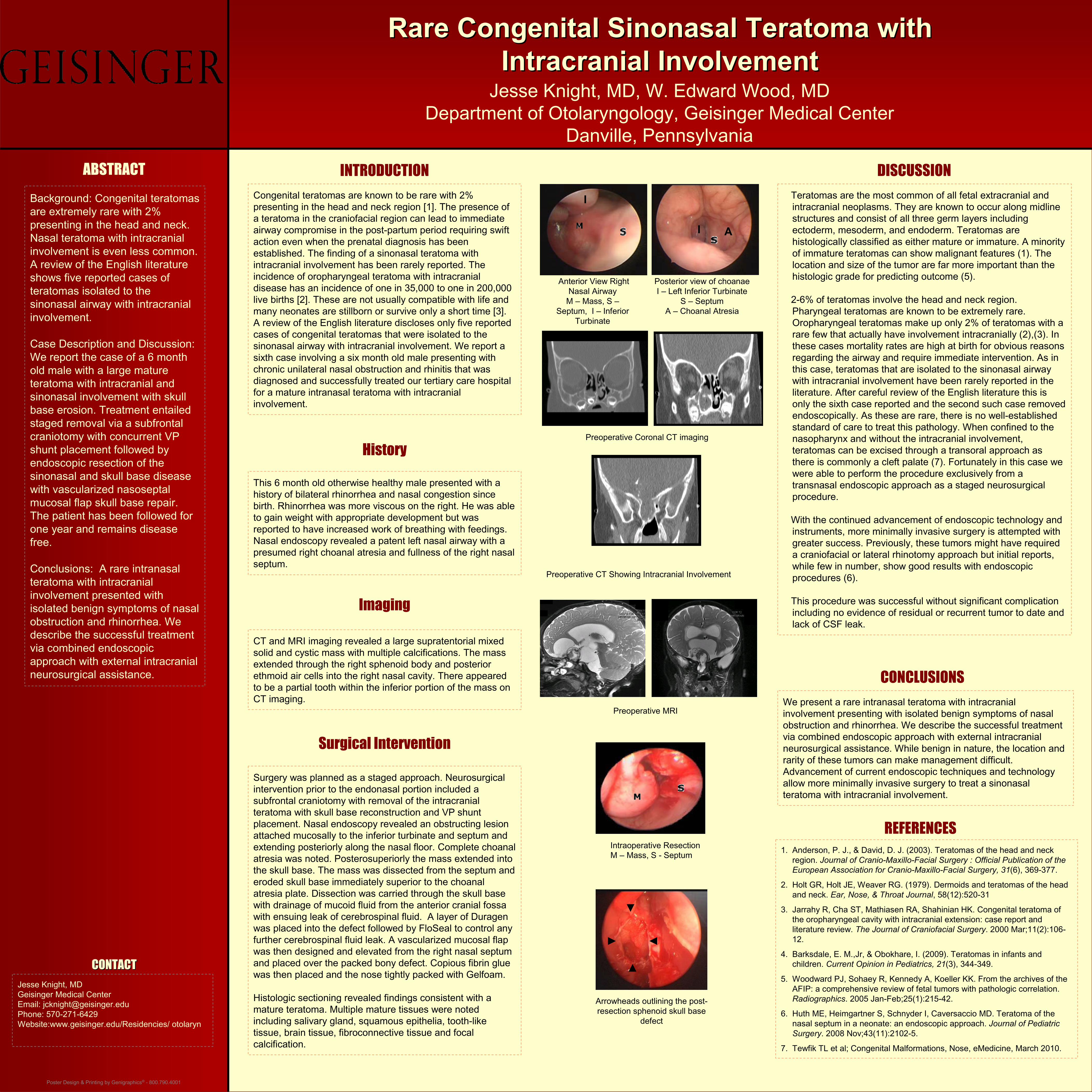
Preoperative Coronal CT imaging
Preoperative CT Showing Intracranial Involvement
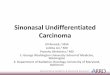
Anterior View Right Nasal Airway
M – Mass, S –Septum, I – Inferior
Turbinate
Posterior view of choanaeI – Left Inferior Turbinate
S – SeptumA – Choanal Atresia
ABSTRACT
Background: Congenital teratomas are extremely rare with 2% presenting in the head and neck. Nasal teratoma with intracranial involvement is even less common. A review of the English literature shows five reported cases of teratomas isolated to the sinonasal airway with intracranial involvement.
Case Description and Discussion: We report the case of a 6 month old male with a large mature teratoma with intracranial and sinonasal involvement with skull base erosion. Treatment entailed staged removal via a subfrontal craniotomy with concurrent VP shunt placement followed by endoscopic resection of the sinonasal and skull base disease with vascularized nasoseptal mucosal flap skull base repair. The patient has been followed for one year and remains disease free.
Conclusions: A rare intranasal teratoma with intracranial involvement presented with isolated benign symptoms of nasal obstruction and rhinorrhea. We describe the successful treatment via combined endoscopic approach with external intracranial neurosurgical assistance.
Teratomas are the most common of all fetal extracranial and intracranial neoplasms. They are known to occur along midline structures and consist of all three germ layers including ectoderm, mesoderm, and endoderm. Teratomas are histologically classified as either mature or immature. A minority of immature teratomas can show malignant features (1). The location and size of the tumor are far more important than the histologic grade for predicting outcome (5).
2-6% of teratomas involve the head and neck region. Pharyngeal teratomas are known to be extremely rare. Oropharyngeal teratomas make up only 2% of teratomas with a rare few that actually have involvement intracranially (2),(3). In these cases mortality rates are high at birth for obvious reasons regarding the airway and require immediate intervention. As in this case, teratomas that are isolated to the sinonasal airway with intracranial involvement have been rarely reported in the literature. After careful review of the English literature this is only the sixth case reported and the second such case removed endoscopically. As these are rare, there is no well-established standard of care to treat this pathology. When confined to the nasopharynx and without the intracranial involvement, teratomas can be excised through a transoral approach as there is commonly a cleft palate (7). Fortunately in this case we were able to perform the procedure exclusively from a transnasal endoscopic approach as a staged neurosurgical procedure.
With the continued advancement of endoscopic technology and instruments, more minimally invasive surgery is attempted with greater success. Previously, these tumors might have required a craniofacial or lateral rhinotomy approach but initial reports, while few in number, show good results with endoscopic procedures (6).
This procedure was successful without significant complication including no evidence of residual or recurrent tumor to date andlack of CSF leak.
This 6 month old otherwise healthy male presented with a history of bilateral rhinorrhea and nasal congestion since birth. Rhinorrhea was more viscous on the right. He was able to gain weight with appropriate development but was reported to have increased work of breathing with feedings. Nasal endoscopy revealed a patent left nasal airway with a presumed right choanal atresia and fullness of the right nasal septum.
We present a rare intranasal teratoma with intracranial involvement presenting with isolated benign symptoms of nasal obstruction and rhinorrhea. We describe the successful treatmentvia combined endoscopic approach with external intracranial neurosurgical assistance. While benign in nature, the location and rarity of these tumors can make management difficult. Advancement of current endoscopic techniques and technology allow more minimally invasive surgery to treat a sinonasal teratoma with intracranial involvement.
Congenital teratomas are known to be rare with 2% presenting in the head and neck region [1]. The presence of a teratoma in the craniofacial region can lead to immediate airway compromise in the post-partum period requiring swift action even when the prenatal diagnosis has been established. The finding of a sinonasal teratoma with intracranial involvement has been rarely reported. The incidence of oropharyngeal teratoma with intracranial disease has an incidence of one in 35,000 to one in 200,000 live births [2]. These are not usually compatible with life and many neonates are stillborn or survive only a short time [3]. A review of the English literature discloses only five reported cases of congenital teratomas that were isolated to the sinonasal airway with intracranial involvement. We report a sixth case involving a six month old male presenting with chronic unilateral nasal obstruction and rhinitis that was diagnosed and successfully treated our tertiary care hospital for a mature intranasal teratoma with intracranial involvement.
History
1. Anderson, P. J., & David, D. J. (2003). Teratomas of the head and neck region. Journal of Cranio-Maxillo-Facial Surgery : Official Publication of the European Association for Cranio-Maxillo-Facial Surgery, 31(6), 369-377.
2. Holt GR, Holt JE, Weaver RG. (1979). Dermoids and teratomas of the head and neck. Ear, Nose, & Throat Journal, 58(12):520-31
3. Jarrahy R, Cha ST, Mathiasen RA, Shahinian HK. Congenital teratoma of the oropharyngeal cavity with intracranial extension: case report and literature review. The Journal of Craniofacial Surgery. 2000 Mar;11(2):106-12.
4. Barksdale, E. M.,Jr, & Obokhare, I. (2009). Teratomas in infants and children. Current Opinion in Pediatrics, 21(3), 344-349.
5. Woodward PJ, Sohaey R, Kennedy A, Koeller KK. From the archives of the AFIP: a comprehensive review of fetal tumors with pathologic correlation.Radiographics. 2005 Jan-Feb;25(1):215-42.
6. Huth ME, Heimgartner S, Schnyder I, Caversaccio MD. Teratoma of the nasal septum in a neonate: an endoscopic approach. Journal of Pediatric Surgery. 2008 Nov;43(11):2102-5.
7. Tewfik TL et al; Congenital Malformations, Nose, eMedicine, March 2010.
CONCLUSIONS
REFERENCES
Jesse Knight, MDGeisinger Medical CenterEmail: [email protected]: 570-271-6429Website:www.geisinger.edu/Residencies/ otolaryn
CONTACTCONTACT
CT and MRI imaging revealed a large supratentorial mixed solid and cystic mass with multiple calcifications. The mass extended through the right sphenoid body and posterior ethmoid air cells into the right nasal cavity. There appeared to be a partial tooth within the inferior portion of the mass onCT imaging.
Intraoperative ResectionM – Mass, S - Septum
Arrowheads outlining the post-resection sphenoid skull base
defect
Surgical Intervention
Surgery was planned as a staged approach. Neurosurgical intervention prior to the endonasal portion included a subfrontal craniotomy with removal of the intracranial teratoma with skull base reconstruction and VP shunt placement. Nasal endoscopy revealed an obstructing lesion attached mucosally to the inferior turbinate and septum and extending posteriorly along the nasal floor. Complete choanal atresia was noted. Posterosuperiorly the mass extended into the skull base. The mass was dissected from the septum and eroded skull base immediately superior to the choanal atresia plate. Dissection was carried through the skull base with drainage of mucoid fluid from the anterior cranial fossa with ensuing leak of cerebrospinal fluid. A layer of Duragen was placed into the defect followed by FloSeal to control any further cerebrospinal fluid leak. A vascularized mucosal flap was then designed and elevated from the right nasal septum and placed over the packed bony defect. Copious fibrin glue was then placed and the nose tightly packed with Gelfoam.
Histologic sectioning revealed findings consistent with a mature teratoma. Multiple mature tissues were noted including salivary gland, squamous epithelia, tooth-like tissue, brain tissue, fibroconnective tissue and focal calcification.
Preoperative MRI
I
I A