Embed Size (px)
Citation preview
Rapporteur Reports

Rapporteur Team
• Track 1• Dr Razia Hassan-Moosa
• Dr Bernadett Gosnell
• Track 2 • Sizulu Moyo
• Keobogile Tiro
• Track 3• Mike Strauss
• Dr Rochelle Nicola Adams
• Track 4• Nosipho Makhakhe
• Dr Zaynab Essack
• Patrick Nyamruze
• Sean Beckett
• Track 5• Dr Dhee Naidoo

PART 1
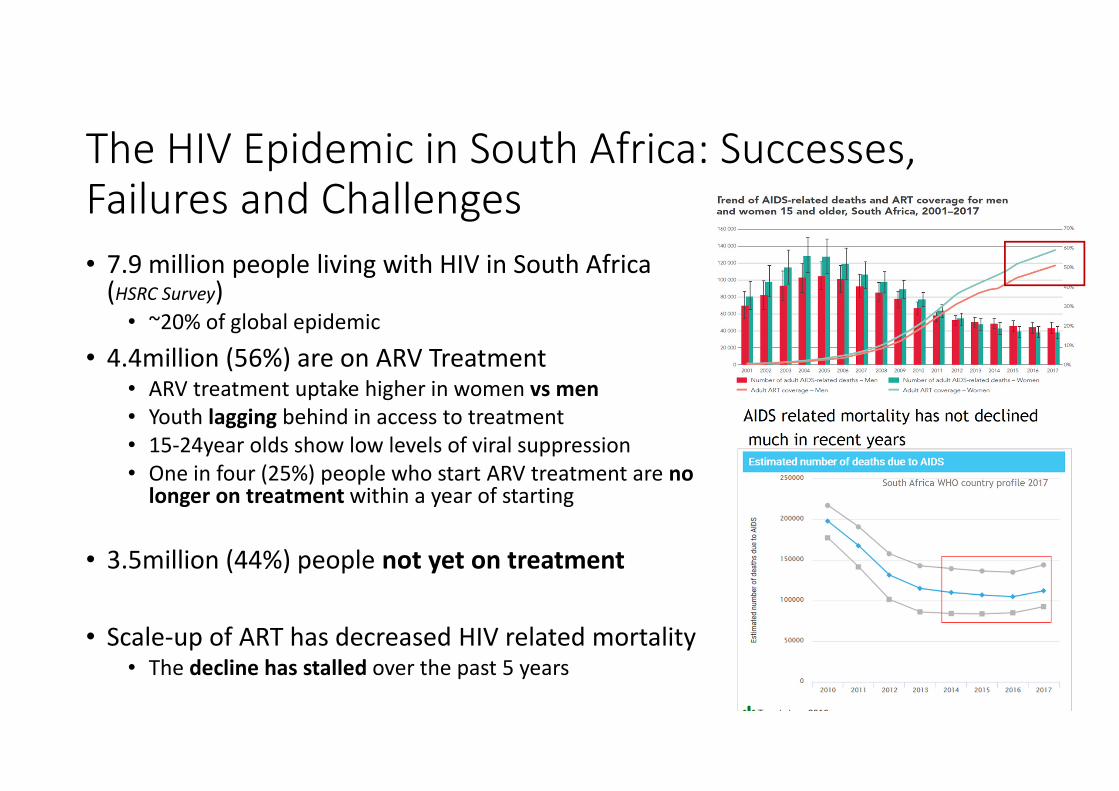
The HIV Epidemic in South Africa: Successes, Failures and Challenges
• 7.9 million people living with HIV in South Africa (HSRC Survey)
• ~20% of global epidemic
• 4.4million (56%) are on ARV Treatment• ARV treatment uptake higher in women vs men
• Youth lagging behind in access to treatment
• 15-24year olds show low levels of viral suppression
• One in four (25%) people who start ARV treatment are no longer on treatment within a year of starting
• 3.5million (44%) people not yet on treatment
• Scale-up of ART has decreased HIV related mortality• The decline has stalled over the past 5 years
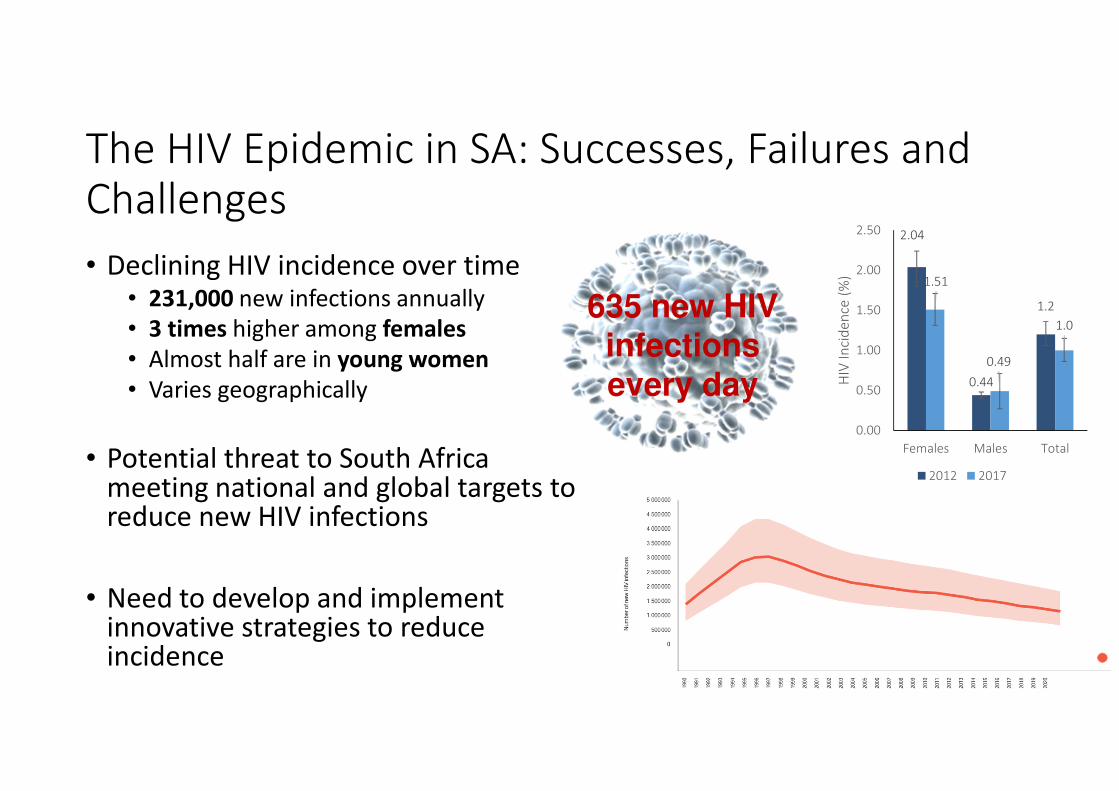
The HIV Epidemic in SA: Successes, Failures and Challenges
• Declining HIV incidence over time• 231,000 new infections annually
• 3 times higher among females
• Almost half are in young women
• Varies geographically
• Potential threat to South Africa meeting national and global targets to reduce new HIV infections
• Need to develop and implement innovative strategies to reduce incidence
2.04
0.44
1.2
1.51
0.49
1.0
0.00
0.50
1.00
1.50
2.00
2.50
Females Males Total
HIV
In
cid
en
ce (
%)
2012 2017
635 new HIV infections every day

Maturing HIV Epidemic
• People living with HIV are living longer into adulthood - Higher risk of comorbidity, accelerated aging
• Existing guidelines will require revision to cater for some of these
• E.g. current HIV testing guidelines do not emphasize testing of >50years
• Newer technologies to improve monitoring of patients and associated complications
• Increase focus on the aging HIV population needed at the primary healthcare level to address co-morbidities related to chronic HIV and long term ART
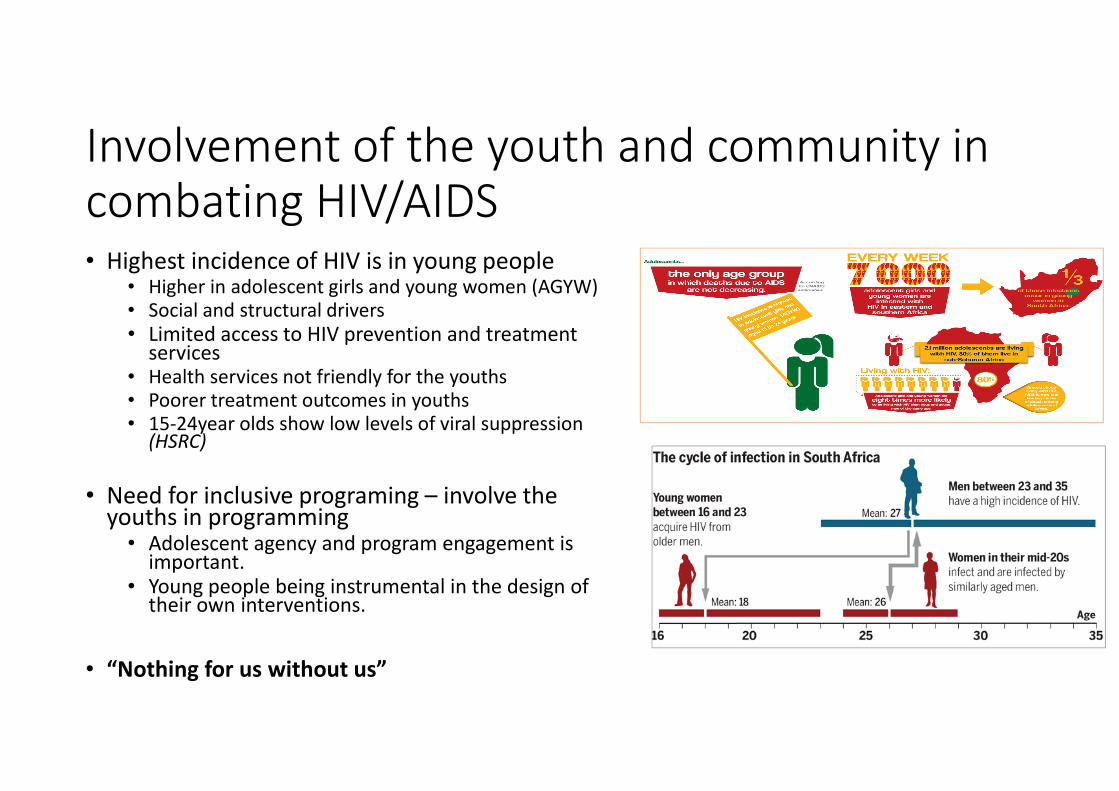
Involvement of the youth and community in combating HIV/AIDS• Highest incidence of HIV is in young people
• Higher in adolescent girls and young women (AGYW)
• Social and structural drivers
• Limited access to HIV prevention and treatment services
• Health services not friendly for the youths
• Poorer treatment outcomes in youths
• 15-24year olds show low levels of viral suppression (HSRC)
• Need for inclusive programing – involve the youths in programming
• Adolescent agency and program engagement is important.
• Young people being instrumental in the design of their own interventions.
• “Nothing for us without us”
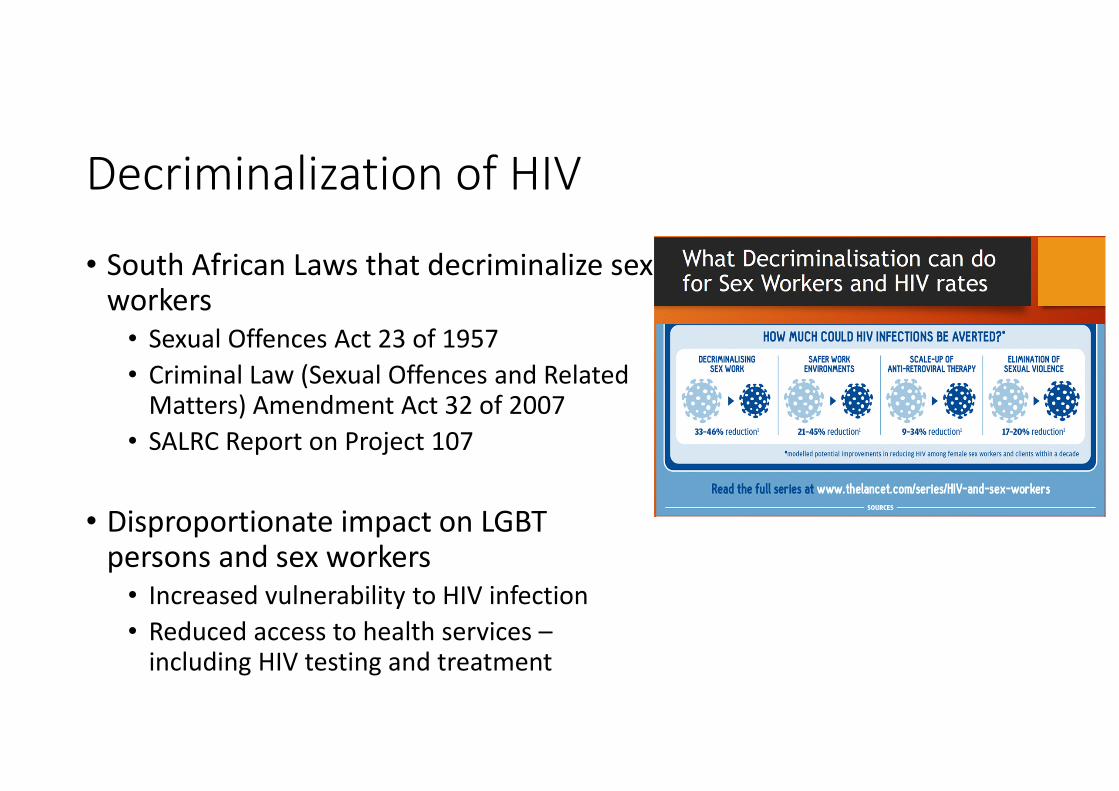
Decriminalization of HIV
• South African Laws that decriminalize sex workers
• Sexual Offences Act 23 of 1957
• Criminal Law (Sexual Offences and Related Matters) Amendment Act 32 of 2007
• SALRC Report on Project 107
• Disproportionate impact on LGBT persons and sex workers
• Increased vulnerability to HIV infection
• Reduced access to health services –including HIV testing and treatment
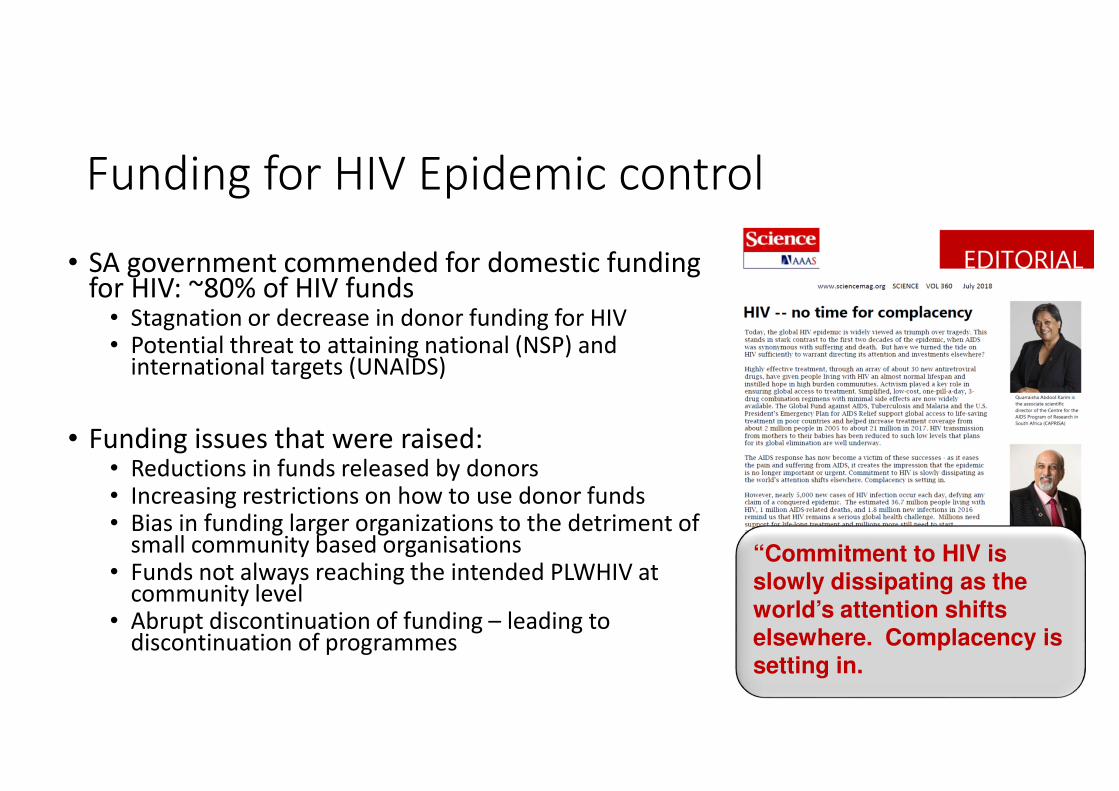
Funding for HIV Epidemic control
• SA government commended for domestic funding for HIV: ~80% of HIV funds
• Stagnation or decrease in donor funding for HIV• Potential threat to attaining national (NSP) and
international targets (UNAIDS)
• Funding issues that were raised:• Reductions in funds released by donors• Increasing restrictions on how to use donor funds• Bias in funding larger organizations to the detriment of
small community based organisations• Funds not always reaching the intended PLWHIV at
community level• Abrupt discontinuation of funding – leading to
discontinuation of programmes
“Commitment to HIV is slowly dissipating as the
world’s attention shifts elsewhere. Complacency is setting in.

Reinvigorating the HIV/AIDS response: No complacency
• Need for a way forward for South Africa from the government
• Need for engagement of youth and community
• Integration to maximize on efficiency: Get the different sectors to work together and achieve synergy, and avoid working in silos.
• Need to discuss how to increase funding for HIV interventions to ensure that we sustain the gains that have been made
• Health system strengthening to cater for the expanding HIV programme
• Need to adopt innovative approaches to HIV programming and monitoring
Part 2
Track 1: Clinical sciences and biomedical innovations, technologies and responsesTrack 1: Clinical sciences and biomedical innovations, technologies and responsesTrack 1: Clinical sciences and biomedical innovations, technologies and responsesTrack 1: Clinical sciences and biomedical innovations, technologies and responses
SummarySummarySummarySummary
• Care at the coal face-treatment
This session comprised of presentations that focused on HIV treatment and outcomes.
Topics included virological outcomes of a tenofivir based first line regimen
Virological suppression rates of patients on third line ART
Tenofivir associated renal dysfunction
• Double Trouble-co-morbidities
This session highlighted HIV associated co-morbidities
Topics included cardio-metabolic factors
Drug resistant and drug susceptible TB, HPV in MSM and the aging HIV patient
• Detective technologies-viral and human genetics
This session highlighted viral and human genetics related to HIV
Topics included association of HLA alleles with HIV
Nanopore next generation sequencing and HIV drug resistance mutations.
Track 1: Clinical sciences and biomedical innovations, technologies and responsesTrack 1: Clinical sciences and biomedical innovations, technologies and responsesTrack 1: Clinical sciences and biomedical innovations, technologies and responsesTrack 1: Clinical sciences and biomedical innovations, technologies and responses
SummarySummarySummarySummary
• PrEP
This session highlighted new data on PrEP
Success and failures of PrEP
Retaining young women on oral PrEP
Adherence and HIV sero-conversion data from the Dapivirine vaginal ring study
Track 2: Possibilities and limits of big dataTrack 2: Possibilities and limits of big dataTrack 2: Possibilities and limits of big dataTrack 2: Possibilities and limits of big data----epidemiology, mathematical modelling and surveillance epidemiology, mathematical modelling and surveillance epidemiology, mathematical modelling and surveillance epidemiology, mathematical modelling and surveillance
SummarySummarySummarySummary
• Implementation Science: Towards 90-90-90 targets
The presentation were on data from a general population level in South Africa
from a sub-district in KZN
from pregnant women
There is progress toward 90-90-90 targets with pockets of success.
Testing is low in younger people and males.
Recommendation: increase testing by increasing access and knowledge of self-testing
• Comorbidities and co-infections.
High prevalence of congenital CMV in children exposed to HIV
The study could have included other babies in neonatal unit, as CMV is ubiquitous
Another study showed value of qPCR for more accurate diagnosis of PCP, as rule out test.
Track 2: Possibilities and limits of big dataTrack 2: Possibilities and limits of big dataTrack 2: Possibilities and limits of big dataTrack 2: Possibilities and limits of big data----epidemiology, mathematical modelling and surveillance epidemiology, mathematical modelling and surveillance epidemiology, mathematical modelling and surveillance epidemiology, mathematical modelling and surveillance
SummarySummarySummarySummary
• Adolescents and youth: age disparate and transgender relationships.
Three presentations were on age disparate relations. All showed higher prevalence of HIV in AGYW in these relationships.
Second study evaluated why cohort studies had shown no increased risk of HIV in age disparate relationships.
Recommendation: continue interventions addressing these relationships
A key issue was to balance “moral” issues vs real needs of AGYW that drive them to age disparate relationships.
Track 3: Implementation science: technologies, innovations and methods of scaling up effective Track 3: Implementation science: technologies, innovations and methods of scaling up effective Track 3: Implementation science: technologies, innovations and methods of scaling up effective Track 3: Implementation science: technologies, innovations and methods of scaling up effective
treatmenttreatmenttreatmenttreatment
SummarySummarySummarySummary
• mHealth innovations for combatting the HIV and AIDS epidemic
When implemented at large scale, mhealth interventions have the potential to improve efficiencies in the health system
improve the quality of care, reduce the cost of delivering health services and more effectively reach key and vulnerable populations
• Digital innovations for combatting the HIV and AIDS epidemics
This session explored innovative approaches utilised for improving health care systems:
1. electronic data collection tools
2. data analysis to monitor progress and adapt interventions
3. Interventions to improve existing electronic system data entry
4. electronic clinical decision support tools for nurses
5. real time visualization and analysis of electronic research surveillance data
Track 3: Implementation science: technologies, innovations and methods of scaling up effective Track 3: Implementation science: technologies, innovations and methods of scaling up effective Track 3: Implementation science: technologies, innovations and methods of scaling up effective Track 3: Implementation science: technologies, innovations and methods of scaling up effective
treatmenttreatmenttreatmenttreatment
SummarySummarySummarySummary
• Implementation Science: Innovations for scaling up effective interventions
presenters shared a variety of research and implementation projects that have taken an innovative approach to scaling up interventions
Scaling up interventions that have been shown to work on a small scale can be challenging.
Scaling-up interventions in an era of increasingly scarce funding is challenging and complicated work that requires continual commitment and responsiveness to people’s needs to ensure the most positive health outcomes and the sustainability of programmes that work.

Track 4: Social drivers of the epidemic: society, race, class, culture, stigma, violence, diversity and Track 4: Social drivers of the epidemic: society, race, class, culture, stigma, violence, diversity and Track 4: Social drivers of the epidemic: society, race, class, culture, stigma, violence, diversity and Track 4: Social drivers of the epidemic: society, race, class, culture, stigma, violence, diversity and
challenges challenges challenges challenges
SummarySummarySummarySummary
• Innovative approach to social behavior change
Experiences of adolescent girls and young women (ADGYW) in the DREAMS program: lessons from Kenya
HIV knowledge and access to services helped adolescents to better navigate sexual relationships
The recommendation from this study was that programs targeting male partners of ADGYW need to be enhanced
Progress in implementing a sexual violence reduction program to ensure safer learning environments within schools: lessons from Khayelitsha, Western Cape:
The program challenged harmful gender norms and toxic masculinity and reinforced messaging around mutual respect, love and emotional intimacy.
The program also intersected GBV policy and programming as well as integrate boys and LGBTIQ learners to mitigate their vulnerability.
Track 4: Social drivers of the epidemic: society, race, class, culture, stigma, violence, diversity and Track 4: Social drivers of the epidemic: society, race, class, culture, stigma, violence, diversity and Track 4: Social drivers of the epidemic: society, race, class, culture, stigma, violence, diversity and Track 4: Social drivers of the epidemic: society, race, class, culture, stigma, violence, diversity and
challenges challenges challenges challenges
SummarySummarySummarySummary
• Innovative approach to social behavior change
1. HIV back on the funding agenda:
HIV funds not reaching community organisations that are instrumental in providing services for PLHIV. There is bias in funding being given to larger organisations to the detriment of small community organisations.
2. Involvement of the youth and community in combating HIV/AIDS
Adolescent agency and program engagement is important.
Young people being instrumental in the design of their own interventions.
Young people calling for interventions that help them to deal with motherhood. Most interventions are focused on prevention of pregnancy.
3. No complacency-reinvigorating the HIV/AIDS response: the way forward for South Africa from the government; youth; community and innovation perspectives.
We need to think of how do we bring all these components together in a multi layered prevention program
The Challenges is getting all the difference sectors to work together and achieve synergy and avoid working in silos.
Track 5: Social justice: relationships and power community, polices, laws, health systems, human rights, Track 5: Social justice: relationships and power community, polices, laws, health systems, human rights, Track 5: Social justice: relationships and power community, polices, laws, health systems, human rights, Track 5: Social justice: relationships and power community, polices, laws, health systems, human rights,
donor agencies and statedonor agencies and statedonor agencies and statedonor agencies and state
SummarySummarySummarySummary
• Community Participation in HIV/AIDS
This session focused on the role of traditional leaders and healers in fighting the HIV epidemic and the role they play in encouraging the community to seek HIV services.
• Human Rights, Ethics & Healthcare
HIV is a human rights issue that needs to be addressed
• Key populations and Access to Health Services
Stigma was the common trend that came across through the session
Stigma had been faced by transgender women, post-prison release inmates, adolescence girls, sex workers and intravenous drug users
• Research Ethics, Principles and Processes
Overall consensus from the speakers and the audiences that community engagement is a key component for the research process.
• Resources, Constrains, Policy & Governance
Structural processes need to be in place so as the proper structures are working in order for policies and governance can work effectively

Concluding general remarksConcluding general remarksConcluding general remarksConcluding general remarks
1. HIV back on the funding agenda:
HIV funds not reaching community organisations that are instrumental in providing services for PLHIV. There is bias in funding being given to larger organisations to the detriment of small community organisations.
2. Involvement of the youth and community in combating HIV/AIDS
Adolescent agency and program engagement is important.
Young people being instrumental in the design of their own interventions.
Young people calling for interventions that help them to deal with motherhood. Most interventions are focused on prevention of pregnancy.
3. No complacency-reinvigorating the HIV/AIDS response: the way forward for South Africa from the government; youth; community and innovation perspectives.
We need to think of how do we bring all these components together in a multi layered prevention program
The Challenges is getting all the difference sectors to work together and achieve synergy and avoid working in silos.





























