Embed Size (px)
Citation preview

4/21/2009
1
RAPID EVALUATION RAPID EVALUATION & TREATMENT OF & TREATMENT OF
ACUTE RENAL FAILUREACUTE RENAL FAILURE
Shieva KhayamShieva Khayam--Bashi, M.D.Bashi, M.D.
Assoc Clin Prof , Dept. of Family & Community MedicineAssoc Clin Prof , Dept. of Family & Community Medicine
UCSF/ SFGH FCM Residency ProgramUCSF/ SFGH FCM Residency ProgramMedical Director, Skilled Nursing Facility/4A SFGHMedical Director, Skilled Nursing Facility/4A SFGH
Email: Email: [email protected]@fcm.ucsf.edu or or [email protected]@att.net415415--206206--35183518 Well, Mr.Osborne, Well, Mr.Osborne,
it may not be kidney stones, after all.it may not be kidney stones, after all.

4/21/2009
2
OVERVIEWOVERVIEW
ACUTE RENAL FAILURE:ACUTE RENAL FAILURE:
�� HistoryHistory�� Physical ExamPhysical Exam�� Evaluation: Lab/StudiesEvaluation: Lab/Studies�� TreatmentTreatment

4/21/2009
3
IN A NUTSHELL:IN A NUTSHELL:3 QUESTIONS TO EVALUATE:3 QUESTIONS TO EVALUATE:
�� PrePre--renalrenal ? are they ? are they DRYDRY??
�� PostPost--renal renal ?? are they are they OBSTRUCTEDOBSTRUCTED??
�� Renal Renal ? is it the ? is it the KIDNEYSKIDNEYS??
PREPRE--RENALRENAL
POSTPOST--RENALRENAL
Intrinsic renalIntrinsic renal
XX
XX
PREPRE--RENAL RENAL 6060--70%70%
POSTPOST--RENALRENAL55--10%10%
Intrinsic Intrinsic renalrenal30%30%
XX
XX

4/21/2009
4
ACUTE RENAL FAILUREACUTE RENAL FAILURE
casecase-- Mr. M.Mr. M.
�� 55 55 yoyo man, man, hxhx DM, HTN, DJD:DM, HTN, DJD:
�� 3 day h/o 3 day h/o N/V/poor N/V/poor popo intake/Diarrhea intake/Diarrhea
�� 1 day 1 day hxhx oliguriaoliguria ��anuriaanuria, confusion, , confusion, pruritispruritis
4/21/2009
5
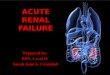
�� MedsMeds : Benazepril, Hctz, Glipizide, Ibuprofen: Benazepril, Hctz, Glipizide, Ibuprofen
�� PHYSICAL EXAMINATION: PHYSICAL EXAMINATION:
�� Vital Signs: Vital Signs: BP 95/50BP 95/50, , HR 125HR 125, , RR 28RR 28, O2: , O2: 91% RA91% RA�� Gen: Gen: confusedconfused , tired, tired�� HEENT: HEENT: mucus membranes DRYmucus membranes DRY�� Heart : Heart : tachycardictachycardic�� Lungs: Lungs: tachypneictachypneic , , diffuse ralesdiffuse rales�� Abdomen: no mass, NTAbdomen: no mass, NT�� Skin: excoriations, no rash/petechiae/purpuraSkin: excoriations, no rash/petechiae/purpura�� Prostate: normal sizeProstate: normal size
LabsLabs ::
Na= Na= 129129K=K= 6.06.0CO2=CO2= 2020BUN=BUN= 6464CreatCreat== 3.63.6 (baseline =1.2 one month ago)(baseline =1.2 one month ago)
Glucose=Glucose= 425425
4/21/2009
6
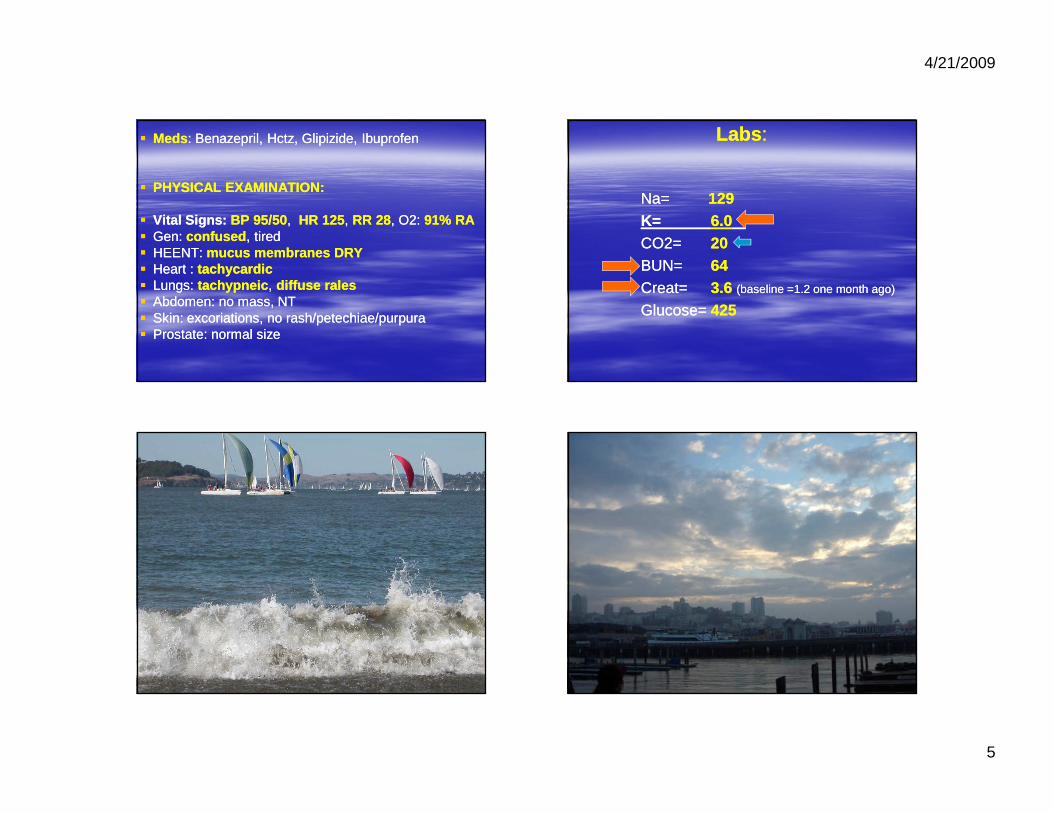
INITIAL TREATMENTINITIAL TREATMENT
�� IV STARTEDIV STARTED–– GIVEN GIVEN NS BOLUSESNS BOLUSESFOR HYPOTENSION FOR HYPOTENSION
�� FOLEY CATHETERFOLEY CATHETER INSERTED: NO INSERTED: NO URINE, not obstructedURINE, not obstructed
�� HYPERKALEMIAHYPERKALEMIA : EKG= WITHOUT : EKG= WITHOUT ACUTE CHANGES, TREATED WITH ACUTE CHANGES, TREATED WITH INSULIN/GLUCOSE,CALCIUM, INSULIN/GLUCOSE,CALCIUM, KAYEXALATEKAYEXALATE
�� HCTZ, ACEI, AND NSAIDS HELDHCTZ, ACEI, AND NSAIDS HELD
�� UA SENT FOR MICROSCOPY AND CX: UA SENT FOR MICROSCOPY AND CX: S.G.1.025S.G.1.025, , NO RBC, NO WBCNO RBC, NO WBC, , NO CELLULAR CASTSNO CELLULAR CASTS (HYALINE ONLY)(HYALINE ONLY)
�� RENAL U/SRENAL U/S NEGATIVE FOR NEGATIVE FOR HYDRONEPHROSIS (obstruction)HYDRONEPHROSIS (obstruction)
�� KUBKUB NEGATIVE FOR CALCULINEGATIVE FOR CALCULI
HOSPITAL COURSEHOSPITAL COURSE
�� OVER NEXT HOURS: BP INCREASED, OVER NEXT HOURS: BP INCREASED, UOP IMPROVED, MENTAL STATUS UOP IMPROVED, MENTAL STATUS CLEAREDCLEARED
�� BUN, CREAT DECREASEDBUN, CREAT DECREASED OVER NEXT OVER NEXT DAYS IN HOSPITAL, DAYS IN HOSPITAL, WITH IV FLUIDSWITH IV FLUIDS
�� Dx: Dx: AKIAKI ::PREPRE--RENAL AZOTEMIARENAL AZOTEMIA , , SECONDARY TO ACUTE VIRAL SECONDARY TO ACUTE VIRAL GASTROENTERITIS GASTROENTERITIS

4/21/2009
7
ACUTE RENAL FAILURE(ARF)ACUTE RENAL FAILURE(ARF)or or
ACUTE KIDNEY INJURY (AKI)ACUTE KIDNEY INJURY (AKI)�� Definition: Definition: nono universal definitionuniversal definition –– generally generally
noted by a noted by a rapid rise in Creat, BUN, rapid rise in Creat, BUN, +/+/-- decreased UOP :decreased UOP :
---- if the baseline Creat is < 2.5 mg/dl : ARF if the baseline Creat is < 2.5 mg/dl : ARF can be defined by an increase in serum can be defined by an increase in serum Creatinine of at least Creatinine of at least 0.5 mg/dl0.5 mg/dl , for 2 weeks , for 2 weeks or less or less ----Or, if the baseline Creat is > 2.5 mg/dl:Or, if the baseline Creat is > 2.5 mg/dl:ARF can be defined by an increase in serum ARF can be defined by an increase in serum Creatinine Creatinine by more than 20%.by more than 20%.
ARF / AKIARF / AKI
�� can be can be nonoliguricnonoliguric or can be or can be oliguricoliguric(oliguria=less than (oliguria=less than 400 ml urine400 ml urine output/day output/day in adults or less than ½ cc/kg/hr) in adults or less than ½ cc/kg/hr)
�� AnuriaAnuria usually has worse prognosis (except usually has worse prognosis (except in dehydration) and is defined as less than in dehydration) and is defined as less than 100 ml/day100 ml/day of urine output in adults. of urine output in adults.
�� ARF occurs in ~ 5% of hospitalized patients.ARF occurs in ~ 5% of hospitalized patients.
�� mortality rate estimates vary from 25mortality rate estimates vary from 25--90%.90%.
�� inin--hospital mortality rate is 40hospital mortality rate is 40--50% 50%
�� in intensive care settings, the mortality rate is in intensive care settings, the mortality rate is 7070--80%. 80%.

4/21/2009
8
Mortality is due to Complications:Mortality is due to Complications:
�� pulmonary edema 30pulmonary edema 30--50%50%�� cardiac (MI, arrhythmias) 30cardiac (MI, arrhythmias) 30--40%40%�� GI (GI bleed, pancreatitis) 30%GI (GI bleed, pancreatitis) 30%�� Infections 50Infections 50--70%70%�� Neurologic abnormalities 30Neurologic abnormalities 30--50%50%�� Electrolyte disorders (hyperkalemia, Electrolyte disorders (hyperkalemia,
metabolic acidosis, hyperuricemia, metabolic acidosis, hyperuricemia, hyperphosphatemia) 50hyperphosphatemia) 50--75%75%
Evaluating for Causes of AKI/ARF:Evaluating for Causes of AKI/ARF:
�� HistoryHistory
�� Physical ExamPhysical Exam
�� Lab/StudiesLab/Studies

4/21/2009
9
IN A NUTSHELL: IN A NUTSHELL:
Hx, PE, Labs are to determine :Hx, PE, Labs are to determine :
�� PrePre--renalrenal ? are they ? are they DRYDRY??
�� PostPost--renal renal ?? are they are they OBSTRUCTEDOBSTRUCTED??
�� Renal Renal ? is it the ? is it the KIDNEYSKIDNEYS??
HISTORYHISTORY

4/21/2009
10
HistoryHistory ::
�� Ask for clues to help determine CAUSE: Ask for clues to help determine CAUSE: (dry vs. obstructed vs. kidneys?)(dry vs. obstructed vs. kidneys?)
1.1. “Are You Dry“Are You Dry?”:?”:�� Decreased PO intake? Decreased PO intake? �� Increased fluid Losses? (N/V/D/diuretic Increased fluid Losses? (N/V/D/diuretic
use)use)�� Other reasons for volume Other reasons for volume depletion?depletion?
�� anaphylaxis,sepsis,MIanaphylaxis,sepsis,MI//CHF,cirrhosisCHF,cirrhosis
History: History:
2.2. “Is There An Obstruction?”:“Is There An Obstruction?”:
�� Abdominal pain / signs of bladder obstruction?Abdominal pain / signs of bladder obstruction?�� SuddenSudden anuria?anuria?
�� Hematuria? Flank pain? Renal/bladder stones?Hematuria? Flank pain? Renal/bladder stones?
�� Weight loss / cancer symptoms? Weight loss / cancer symptoms?
History:History:
3.3. “Is it the Kidneys?”:“Is it the Kidneys?”:�� MEDSMEDS: : NephrotoxicNephrotoxic medicines? IV medicines? IV
contrast? contrast? aminoglycosidesaminoglycosides, , amphotericinamphotericin, , cisplatincisplatin, PCNs, , PCNs, cephalosporinscephalosporins, sulfas, , sulfas, NSAIDs, NSAIDs, rifampinrifampin??
�� Family HistoryFamily History Kidney Disease?Kidney Disease?
�� Previous urologic / Previous urologic / renal historyrenal history??�� AutoimmuneAutoimmune/ / vasculitisvasculitis history? history? �� ViralViral diseases which can affect kidneys?diseases which can affect kidneys?

4/21/2009
11
Also, ASK for SYMPTOMS which Also, ASK for SYMPTOMS which can be the can be the consequenceconsequence of ARF:of ARF:
�� EncephalopathyEncephalopathy ? (confusion/somnolence)? (confusion/somnolence)
�� Chest pain?Chest pain? ((pericarditispericarditis ))
�� CHF/Fluid CHF/Fluid overloadoverload symptoms?symptoms?
��Pulmonary or Peripheral Pulmonary or Peripheral EdemaEdema? ? ��Significant Significant HypertensionHypertension? ?
�� BleedingBleeding? (platelet dysfunction)? (platelet dysfunction)

4/21/2009
12
PHYSICAL EXAMINATIONPHYSICAL EXAMINATION
Physical Exam:Physical Exam:
�� Volume statusVolume status (orthostatic vital signs, (orthostatic vital signs, tachycardia, dry mucous membranes)tachycardia, dry mucous membranes)
�� NeuroNeuro: mental status, : mental status, asterixisasterixis((encephalopathyencephalopathy ) )
�� Heart: tachycardia, Heart: tachycardia, pericardial rubpericardial rub�� Lungs: signs of pulmonary edema Lungs: signs of pulmonary edema
((increased RR, decreased O2 sat, increased RR, decreased O2 sat, ralesrales ))�� Abdomen: bladder Abdomen: bladder distentiondistention , mass?, mass?�� Skin : Skin : petechiaepetechiae (HUS,TTP), palpable (HUS,TTP), palpable
purpurapurpura ((vasculitisvasculitis) , edema) , edema�� Pelvic/ Prostate exam (Pelvic/ Prostate exam (R/O obstructionR/O obstruction ))
4/21/2009
13
LABS / STUDIES
LABS/STUDIES:LABS/STUDIES:
�� CBC, CHEM 7CBC, CHEM 7: Na, : Na, KK , Cl, , Cl, CO2CO2, , BUNBUN, , CrCr , Glucose (STAT , Glucose (STAT EKGEKG if Hyperkalemic)if Hyperkalemic)
�� UA with microscopyUA with microscopy ((castscasts , RBC, , RBC, WBC, protein)WBC, protein)
�� Urine CultureUrine Culture
�� Renal ultrasoundRenal ultrasound (R/O Obstruction)(R/O Obstruction)�� Serum Na& Creat, Urine Na & Creat (to Serum Na& Creat, Urine Na & Creat (to
calculate calculate FENaFENa))�� OptionalOptional: KUB (for stones), CT Abdomen : KUB (for stones), CT Abdomen
(for masses)(for masses)
4/21/2009
14
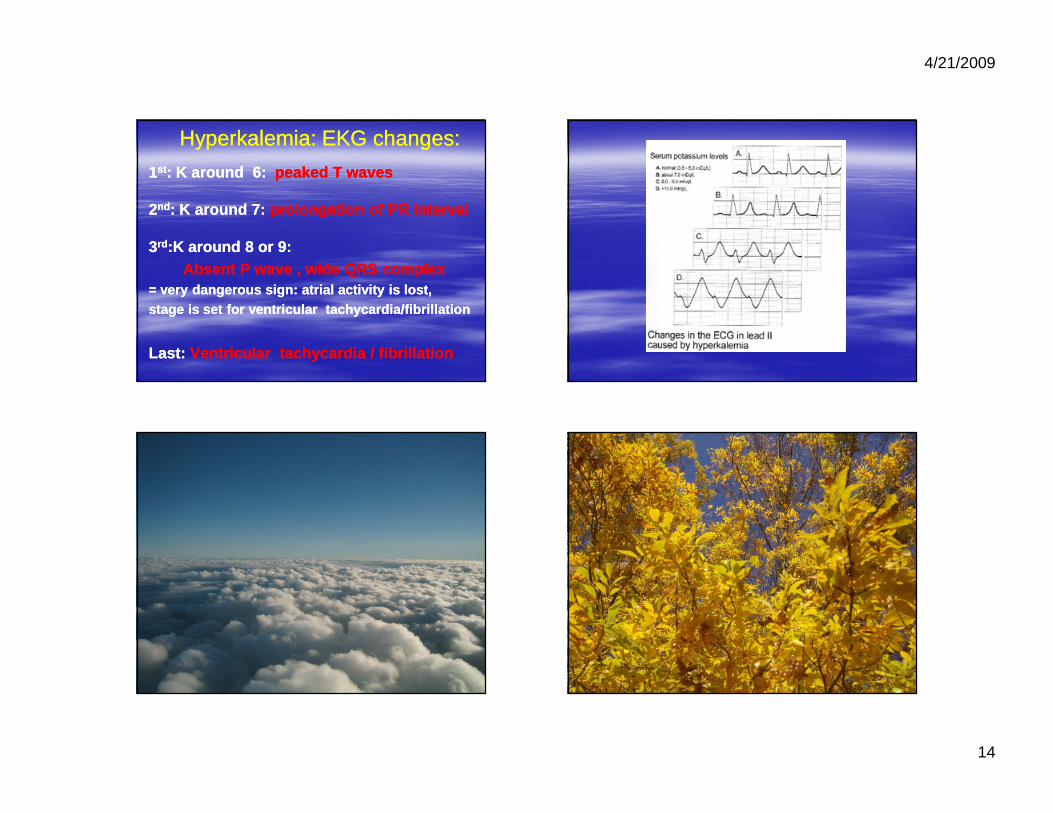
HyperkalemiaHyperkalemia: EKG changes:: EKG changes:
11stst : K around 6: : K around 6: peaked T waves peaked T waves
22ndnd : K around 7: : K around 7: prolongation of PR intervalprolongation of PR interval
33rdrd :K around 8 or 9: :K around 8 or 9: Absent P wave , wide QRS complexAbsent P wave , wide QRS complex
= very dangerous sign: = very dangerous sign: atrialatrial activity is lost, activity is lost, stage is set for ventricular tachycardia/fibrillat ionstage is set for ventricular tachycardia/fibrillat ion
Last: Last: Ventricular tachycardia / fibrillationVentricular tachycardia / fibrillation
4/21/2009
15
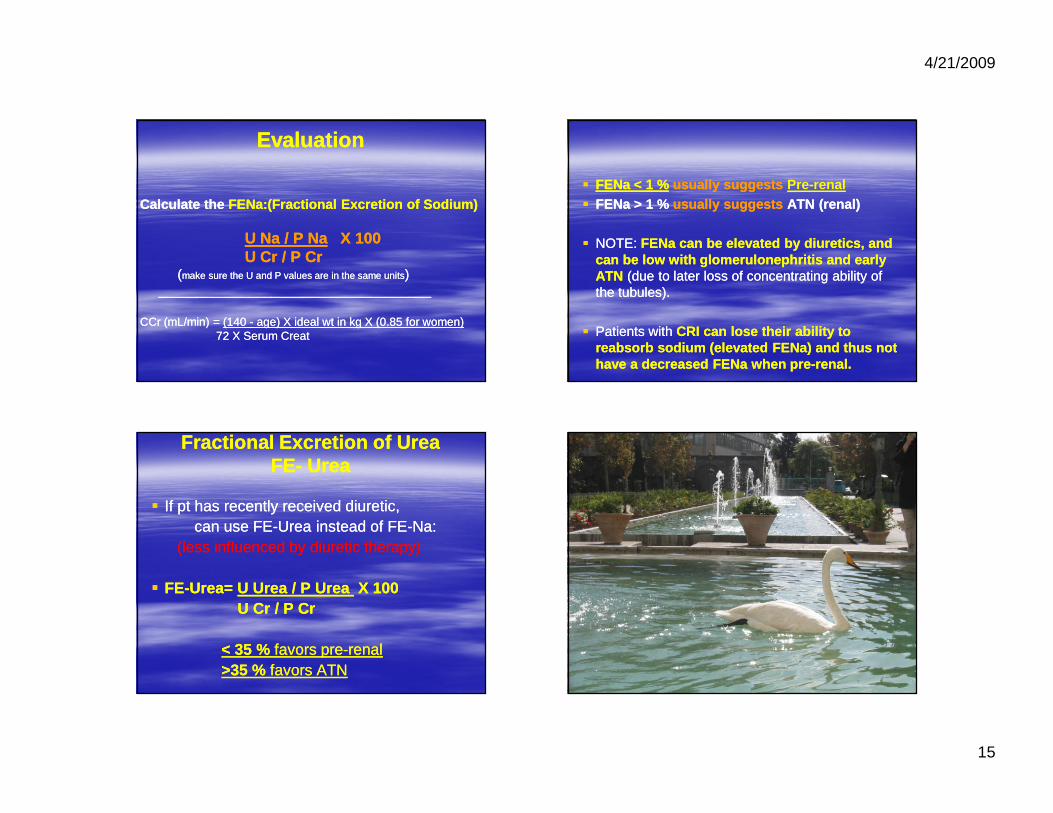
EvaluationEvaluation
Calculate the Calculate the FENa:(FENa:(Fractional Excretion of Sodium)Fractional Excretion of Sodium)
U Na / P NaU Na / P Na X 100X 100U Cr / P CrU Cr / P Cr
((make sure the U and P values are in the same unitsmake sure the U and P values are in the same units))________________________________________________________________________
CCr (mL/min) = CCr (mL/min) = (140 (140 -- age) X age) X ideal wt in kg ideal wt in kg X (X (0.85 for women)0.85 for women)72 X Serum Creat72 X Serum Creat
�� FENaFENa < 1 %< 1 % usually suggests usually suggests Pre-renal�� FENaFENa > 1 %> 1 % usually suggests usually suggests ATN (renal)ATN (renal)
�� NOTE: NOTE: FENaFENa can can be elevated by be elevated by diuretics, and diuretics, and can can be be low with low with glomerulonephritisglomerulonephritis and early and early ATNATN (due to (due to laterlater loss loss of concentrating ability of of concentrating ability of the tubules).the tubules).
�� Patients with Patients with CRI can lose their ability to CRI can lose their ability to reabsorb reabsorb sodium (elevated sodium (elevated FENaFENa) ) and thus not and thus not have a decreased have a decreased FENaFENa when prewhen pre--renal.renal.
Fractional Excretion of UreaFractional Excretion of UreaFEFE-- UreaUrea
�� If pt has recently received diuretic, If pt has recently received diuretic, can use FEcan use FE--Urea instead of FEUrea instead of FE--NaNa::
(less influenced by diuretic therapy)(less influenced by diuretic therapy)
�� FEFE--Urea= Urea= U Urea / P Urea U Urea / P Urea X 100X 100U Cr / P CrU Cr / P Cr
< 35 %< 35 % favors prefavors pre--renalrenal>35 %>35 % favors ATNfavors ATN

4/21/2009
16
Can make Laboratory Can make Laboratory DIAGNOSIS of ARF/AKI by :DIAGNOSIS of ARF/AKI by :
1. UA with 1. UA with MICROSCOPYMICROSCOPY(looking at urine sediment : cells / casts) (looking at urine sediment : cells / casts)
2. URINE Na 2. URINE Na
3. FE3. FE--NaNa
DIAGNOSIS URINE SEDIMENT Urine Na DIAGNOSIS URINE SEDIMENT Urine Na FENaFENa
PrerenalPrerenal Normal, or Normal, or hyaline castshyaline casts <20 <20 mEqmEq/L/L <1%<1%
IntrarenalIntrarenalTubularTubular necrosis Granularnecrosis Granular, , tubulartubular epithelialepithelial >20 >20 mEqmEq/L /L >>1% 1%
(ATN) (ATN) cell castscell casts, muddy brown casts, muddy brown casts
Interstitial nephritis Interstitial nephritis WBC,RBC, mild WBC,RBC, mild proteinuriaproteinuria, >20 , >20 mEqmEq/L /L >>1% 1% (AIN)(AIN) granular and epithelial cell casts, granular and epithelial cell casts,
WBC casts, WBC casts, eosinophilseosinophils ! ! ****
GlomerulonephritisGlomerulonephritis HematuriaHematuria(RBC), (RBC), proteinuriaproteinuria, >20 , >20 mEqmEq/L /L <1%<1%(GN)(GN) RBC castsRBC casts, granular casts, granular casts
Vascular disorders Normal or RBC, >20 Vascular disorders Normal or RBC, >20 mEqmEq/L /L <1%<1%mild mild proteinuriaproteinuria_______________________________ _______________________________
PostrenalPostrenal Normal or RBCs, Normal or RBCs, granular casts, WBC >20 granular casts, WBC >20 mEqmEq/L >1%/L >1%
** ** NOTE: WBCs in urine, but negative leukocyte esteras e reaction NOTE: WBCs in urine, but negative leukocyte esteras e reaction can be clue for can be clue for eosinophiluriaeosinophiluria

4/21/2009
17
�� Hylaine casts: Hylaine casts: prepre--renalrenal
�� Granular cast + tubular epithelial cell Granular cast + tubular epithelial cell casts: casts: ATN,AIN :ATN,AIN :
�� WBC cast: WBC cast: AIN , chronic GNAIN , chronic GN ::
�� RBC casts : RBC casts : GN:GN:
�� Oval fat bodies: Oval fat bodies: nephrotic syndromenephrotic syndrome ::

4/21/2009
18
Urinalysis Urinalysis microscopy/sedimentmicroscopy/sediment ::
�� Hyaline and fine granular casts often seen in Hyaline and fine granular casts often seen in prepre--renal failurerenal failure
�� Tubular epithelial cells or Tubular epithelial cells or casts,coarsecasts,coarse granular casts: granular casts: ATN,AINATN,AIN
�� RBC, RBC CASTS RBC, RBC CASTS proteinuriaproteinuria��suggestssuggests GlomerulonephritisGlomerulonephritis
�� + protein +/+ protein +/-- Oval fat bodiesOval fat bodies �� nephroticnephrotic syndromesyndrome (check (check albumin and 24 hr urine protein) albumin and 24 hr urine protein)
�� + blood on Dipstick but + blood on Dipstick but no RBCsno RBCs on microscopic on microscopic �� consider consider RhabdomyolysisRhabdomyolysis , check serum CK level, check serum CK level
�� WBC/casts, WBC/casts, eosinophilseosinophils ��acute interstitial nephritisacute interstitial nephritis

4/21/2009
19
TreatmentTreatment
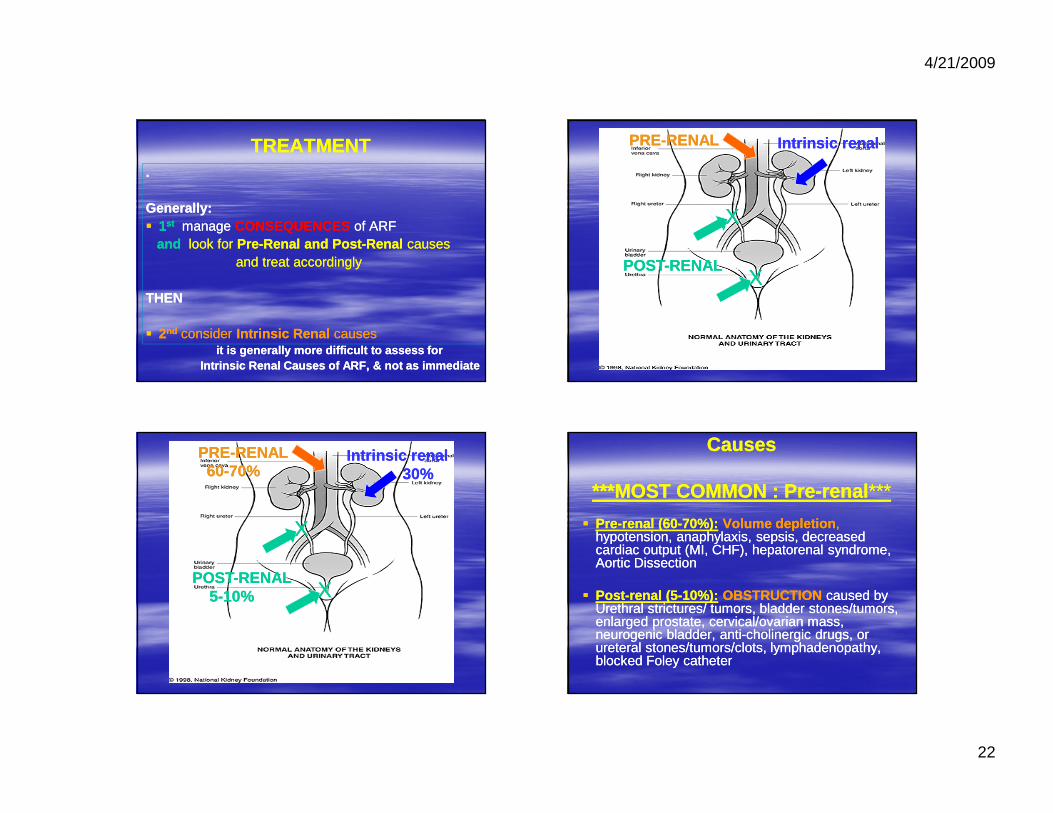
TREATMENTTREATMENT..
GenerallyGenerally::�� 11stst managemanage CONSEQUENCESCONSEQUENCES of of ARFARF
andand look for look for PrePre--Renal and PostRenal and Post--RenalRenal causes causes and treat accordingly and treat accordingly
THEN THEN
�� 22ndnd consider consider Intrinsic RenalIntrinsic Renal causes causes it is generally more difficult to assess for it is generally more difficult to assess for
Intrinsic Renal Causes of ARF, & not as immediateIntrinsic Renal Causes of ARF, & not as immediate
INTERVENTIONS/TREATMENTINTERVENTIONS/TREATMENT
�� Give IV Fluids as trial, since preGive IV Fluids as trial, since pre--renal is renal is most common most common cause (60cause (60--70%)70%)… … (unless (unless volume overloaded)volume overloaded)
�� Foley catheterFoley catheter –– to relieve obstruction/ urine to relieve obstruction/ urine retention. retention. (5(5--10%)10%)
�� If If Foley is already in Foley is already in placeplace��flushflush with NSwith NS(to clear any sediment/clot obstructing)(to clear any sediment/clot obstructing)
MOST LIFEMOST LIFE--THREATENING THREATENING CONSEQUENCESCONSEQUENCES::
�� hyperkalemia hyperkalemia
�� acidosisacidosis
�� fluid overload (CHF)fluid overload (CHF)
4/21/2009
20
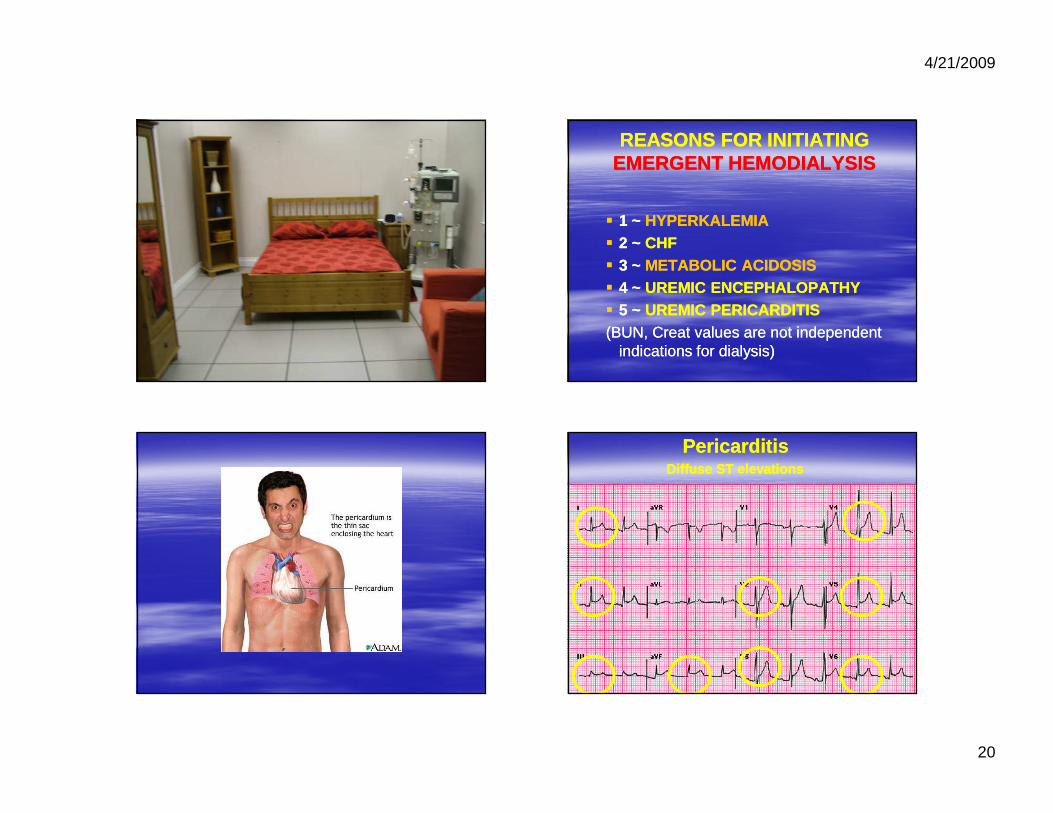
REASONS FOR INITIATING REASONS FOR INITIATING EMERGENT HEMODIALYSISEMERGENT HEMODIALYSIS
�� 1 ~ 1 ~ HYPERKALEMIAHYPERKALEMIA�� 2 ~ 2 ~ CHFCHF�� 3 ~ 3 ~ METABOLIC ACIDOSISMETABOLIC ACIDOSIS�� 4 ~ 4 ~ UREMIC ENCEPHALOPATHYUREMIC ENCEPHALOPATHY�� 5 ~ 5 ~ UREMIC PERICARDITISUREMIC PERICARDITIS(BUN, (BUN, CreatCreat values are not independent values are not independent
indications for dialysis)indications for dialysis)
PericarditisPericarditisDiffuse ST elevationsDiffuse ST elevations

4/21/2009
21
PericarditisPericarditisDiffuse ST elevations, PRDiffuse ST elevations, PR depressionsdepressions
Until you can get the pt to Until you can get the pt to dialysis, treat accordingly:dialysis, treat accordingly:
�� 11 HYPERKALEMIAHYPERKALEMIA :: treat with glucose/ insulin,treat with glucose/ insulin,IV calcium, Kayexalate, Furosemide , check EKG IV calcium, Kayexalate, Furosemide , check EKG STAT and monitor …STAT and monitor …
�� 22 CHFCHF:: Oxygen, diuresis…Oxygen, diuresis…�� 33 METABOLIC ACIDOSISMETABOLIC ACIDOSIS :: bicarbonate if severe bicarbonate if severe
pH<7.2 ...pH<7.2 ...�� 44 UREMIC ENCEPHALOPATHY:UREMIC ENCEPHALOPATHY: treat seizures, treat seizures,
agitation ...agitation ...�� 55 UREMIC PERICARDITIS:UREMIC PERICARDITIS: treat pain (NO treat pain (NO
NSAIDS!!)NSAIDS!!)
AVOID: KCL, KAVOID: KCL, K--SPARING DIURETICS, ACE SPARING DIURETICS, ACE INHIBITORS, NSAIDS, NEPHROTOXIC DRUGS, INHIBITORS, NSAIDS, NEPHROTOXIC DRUGS, IV CONTRAST …..IV CONTRAST …..
4/21/2009
22
TREATMENTTREATMENT..
GenerallyGenerally::�� 11stst managemanage CONSEQUENCESCONSEQUENCES of of ARFARF
andand look for look for PrePre--Renal and PostRenal and Post--RenalRenal causes causes and treat accordingly and treat accordingly
THEN THEN
�� 22ndnd consider consider Intrinsic RenalIntrinsic Renal causes causes it is generally more difficult to assess for it is generally more difficult to assess for
Intrinsic Renal Causes of ARF, & not as immediateIntrinsic Renal Causes of ARF, & not as immediate
PREPRE--RENALRENAL
POSTPOST--RENALRENAL
Intrinsic renalIntrinsic renal
XX
XX
PREPRE--RENAL RENAL 6060--70%70%
POSTPOST--RENALRENAL55--10%10%
Intrinsic Intrinsic renalrenal30%30%
XX
XX
CausesCauses
***MOST COMMON : Pre***MOST COMMON : Pre--renalrenal ******
�� PrePre--renal (60renal (60--70%):70%): Volume depletionVolume depletion ,,hypotension, anaphylaxis, sepsis, decreased hypotension, anaphylaxis, sepsis, decreased cardiac output (MI, CHF), hepatorenal syndrome, cardiac output (MI, CHF), hepatorenal syndrome, Aortic DissectionAortic Dissection
�� PostPost--renal (5renal (5--10%):10%): OBSTRUCTIONOBSTRUCTION caused by caused by Urethral strictures/ tumors, bladder stones/tumors, Urethral strictures/ tumors, bladder stones/tumors, enlarged prostate, cervical/ovarian mass, enlarged prostate, cervical/ovarian mass, neurogenic bladder, antineurogenic bladder, anti--cholinergic drugs, or cholinergic drugs, or ureteral stones/tumors/clots, lymphadenopathy, ureteral stones/tumors/clots, lymphadenopathy, blocked Foley catheterblocked Foley catheter

4/21/2009
23
CAUSESCAUSES�� Intrinsic Renal (30Intrinsic Renal (30--40%):40%):
�� *** *** 90% 90% = Acute = Acute Tubular NecrosisTubular Necrosis (ATN)(ATN) induced by induced by hypotension, hypotension, nephrotoxinsnephrotoxins / drugs (/ drugs (aminoglycosidesaminoglycosides, , amphotericinamphotericin, IV contrast, chemotherapy, , IV contrast, chemotherapy, rhabdomyolysisrhabdomyolysis))
• • Acute Interstitial NephritisAcute Interstitial Nephritis (AIN):(AIN): (can be as late as 10(can be as late as 10--14 14 days after last dose of antibiotic, only 1/3 have days after last dose of antibiotic, only 1/3 have eosinophilseosinophils in in urine): urine): egeg, due to PCN, Sulfa, , due to PCN, Sulfa, QuinolonesQuinolones, , CephalosporinsCephalosporins, , NSAIDS, diuretics..NSAIDS, diuretics..
�� VascularVascular causes such as Emboli (from causes such as Emboli (from SBE,MI,Afib,leftSBE,MI,Afib,leftheart heart thrombi,aorticthrombi,aortic atheromas,postatheromas,post aortic surgery), aortic surgery), Renal Renal Artery Artery Thrombosis, or worsening of Renal Artery Thrombosis, or worsening of Renal Artery StenosisStenosis / / renal artery atherosclerosisrenal artery atherosclerosis
�� NephritisNephritis such as acute such as acute glomerulonephritisglomerulonephritis , SLE, , SLE, vasculitidesvasculitides
�� renal renal infectioninfection , renal , renal infiltrationinfiltration (lymphoma, (lymphoma, sarcoidsarcoid))
INTRINSIC RENAL:INTRINSIC RENAL:
1. 1. Interstitial nephritisInterstitial nephritis
�� Clinical clues:Clinical clues: Medications, fever, rash, Medications, fever, rash, eosinophiliaeosinophilia (hypersensitivity)(hypersensitivity)
�� Urine Sediment:Urine Sediment: WBCs, WBC casts, WBCs, WBC casts, eosinophilseosinophils ((eoseos only seen by Hansel’s staining of WBC)only seen by Hansel’s staining of WBC)
�� Protein:CreatinineProtein:Creatinine RatioRatio: 30 to 3,000 mg of : 30 to 3,000 mg of protein per g of protein per g of creatininecreatinine
�� Other TestsOther Tests: : less common= less common= CMV, HIV, HBVCMV, HIV, HBV, , ACE ACE level; SSlevel; SS--A, A, SSSS--BB ((AbAb to to ribonuclearribonuclear proteins :proteins :antiSSantiSS--A = A = antianti--Ro antibody; Ro antibody; antiSSantiSS--B B = anti= anti--La antibody) La antibody) ((SjogrensSjogrens , SLE), SLE)
((TxTx= withdraw offending agent; +/= withdraw offending agent; +/-- steroids possibly n eeded)steroids possibly needed)

4/21/2009
24
INTRINSIC RENAL: INTRINSIC RENAL:
2. 2. GlomerulonephritisGlomerulonephritis�� Clinical clues: Clinical clues: History and physical examination: History and physical examination:
infections; rash, arthritis; patient older than 40 yearsinfections; rash, arthritis; patient older than 40 years�� Urine Sediment:Urine Sediment: DysmorphicDysmorphic RBCs or RBCs or RBC castsRBC casts�� Protein:CreatinineProtein:Creatinine RatioRatio: > 30 to > 3,500 mg of : > 30 to > 3,500 mg of
protein per g of protein per g of creatininecreatinine�� Other TestsOther Tests : : C3 and C4 for all patientsC3 and C4 for all patients
----Tests for infections: Tests for infections: antianti--ASO, ASO, HIV, HIV, HBsAgHBsAg, , HCV, RPR, blood HCV, RPR, blood culturescultures----Tests if there is rash or arthritis: ANA, ANCA, Tests if there is rash or arthritis: ANA, ANCA, cryoglobulincryoglobulin, anti, anti--GBM GBM ----Tests if patient is > 40 Tests if patient is > 40 years:SPEPyears:SPEP, UPEP, UPEP
INTRINSIC RENAL: INTRINSIC RENAL:
3. 3. VasculitisVasculitis�� Clinical clues:Clinical clues: Constitutional symptoms, Constitutional symptoms,
peripheral neuropathy, rash, respiratory peripheral neuropathy, rash, respiratory symptomssymptoms
�� Urine Sediment:Urine Sediment: RBCs; granular casts RBCs; granular casts �� Protein:CreatinineProtein:Creatinine RatioRatio: > 30 to > 3,500 mg : > 30 to > 3,500 mg
of protein per g of of protein per g of creatininecreatinine�� Other TestsOther Tests: : C3, C4, ANA, ANCA; C3, C4, ANA, ANCA; HBsAgHBsAg, ,
HCV, HCV, cryoglobulinscryoglobulins, ESR, RF, SS, ESR, RF, SS--A, SSA, SS--B, B, HIV HIV
(SS(SS--A = antiA = anti--Ro antibody; SSRo antibody; SS--B = antiB = anti--La antibody)La antibody)�� Treatment = Treatment = txtx complications +/complications +/-- immunesuppressantsimmunesuppressants

4/21/2009
25
A Few Caveats:A Few Caveats:�� In In GN, acute postGN, acute post--renal obstructionrenal obstruction , and some , and some
vascularvascular diseasesdiseases, FENa may often be < 1%, FENa may often be < 1%
�� Protein deficientProtein deficient states can produce a states can produce a
lowerlower BUN/creatBUN/creat ratio in preratio in pre--renal states.renal states.
�� GI bleeding, high protein diet, corticosteroidsGI bleeding, high protein diet, corticosteroidscan cause a can cause a higher higher BUNBUN level.level.
�� CreatinineCreatinine can be can be increasedincreased with certain meds: with certain meds: trimethoprim, cimetidinetrimethoprim, cimetidine
A Few A Few Final NotesFinal Notes::
�� Remember to Remember to adjust doses of all drugsadjust doses of all drugs for for new GFR/Creat clearance new GFR/Creat clearance
�� For ATN from For ATN from rhabdomyolysisrhabdomyolysis , treat with , treat with IV bicarbonate: D5W w/ 3 amps NaHCO3/L IV bicarbonate: D5W w/ 3 amps NaHCO3/L at 100at 100--150ml/hr, titrate to high volume UOP, 150ml/hr, titrate to high volume UOP, and use furosemide to force diuresis.and use furosemide to force diuresis.
�� Historically, diuretics have often been used Historically, diuretics have often been used to convert oliguric to nonto convert oliguric to non--oliguric renal oliguric renal failure. This is of unclear benefit and may failure. This is of unclear benefit and may cause increased mortality.cause increased mortality.
�� Recent studies show no benefit for use of Recent studies show no benefit for use of renalrenal--dose dopamine.dose dopamine.
4/21/2009
26
PREVENTIONPREVENTION

4/21/2009
27
PreventionPrevention of contrast nephropathy of contrast nephropathy in patients with risk factors for ARF in patients with risk factors for ARF
(elderly, CKD, hepatic disease)(elderly, CKD, hepatic disease)
�� Hold MetforminHold Metformin x 48 hrs prior to IV contrastx 48 hrs prior to IV contrast�� Hold diuretics and NSAIDSHold diuretics and NSAIDS and any potentially and any potentially
nephrotoxic meds if possible nephrotoxic meds if possible �� Start IV fluidsStart IV fluids : normal saline x 24 hrs prior to contrast: normal saline x 24 hrs prior to contrast
�� Sodium BicarbonateSodium Bicarbonate : recent RCT showed 12% : recent RCT showed 12% absolute risk reduction w/ administration of NaHCO3 absolute risk reduction w/ administration of NaHCO3 prior to contrast load:prior to contrast load:
---- dosage: 154 mEq/L Sodium Bicarbonate as a bolus dosage: 154 mEq/L Sodium Bicarbonate as a bolus of 3cc/kg/hr for 1 hour prior to contrast, followed by of 3cc/kg/hr for 1 hour prior to contrast, followed by infusion of 1 cc/kg/hr for 6 hours after procedure.infusion of 1 cc/kg/hr for 6 hours after procedure.
PreventionPreventionof contrast nephropathyof contrast nephropathy
�� Use oral Use oral acetylcysteineacetylcysteine (Mucomyst)(Mucomyst) before before administering iodinated contrast loads in administering iodinated contrast loads in patients with risk factors patients with risk factors
�� Dose = 600 mg po bid the day before and Dose = 600 mg po bid the day before and the day of the study, along with adequate the day of the study, along with adequate hydration. (4 doses total)hydration. (4 doses total)

4/21/2009
28