Embed Size (px)
Citation preview

Veroniek Saegeman, Laboratoriumgeneeskunde - Ziekenhuishygiëne, UZLeuven
Rapid diagnostic tests, (MDROs) and infection prevention

Background: impact of RDT on MDRO
Derde L et al, Lancet Infect Dis 2014
CDC, Management of MDRO in Healthcare settings, 2006

Background: impact of RDT on MDRO
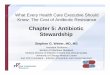
No statistical difference in acquisition of MDRO in conventional
screening vs rapid screening group
• 13 European ICUs, period 2008-2011
• Three phases: baseline – hygiene improvement – randomised controlled
phase: conventional vs rapid screening
• Primary outcome: acquisition of resistant bacteria per 100 patient-days
Derde L et al, Lancet Infect Dis 2014

Facts about RDT
M Bonten, ESCMID SHEA 2012
Beneficial effects
RDT may reduce the number of unnecessary isolation days
RDT may more rapidly detect spread among contact patients
and health care workers, allowing faster isolation of these
patients, thereby reducing transmission potential
Adverse effects
<100% sensitivity: may ↑ N° MDRO-transmission, carriers will
not be isolated
<100% specificity: may ↑ N° of isolation days, non-colonized
patients treated in isolation unnecessarily
Possible solution: use conventional microbiological cultures
as back-up

Microorganisms to discuss
Vancomycin resistant enterococci
Methicillin Resistant Staphylococcus aureus
Streptococcus group B
Clostridium difficile
Norovirus

Vancomycin resistant enterococci

Vancomycin resistant enterococci
• Usefulness of RDT
– Patients ‘at risk’ for VRE: fast result adapt Infection Control Measures
• Hospitalisation > 3 weeks with upgrading of care
• transplant patient
• room mate of VRE positive patient
• known VRE positive patient > 1 year ago
• hospitalisation on ward with VRE in previous year
Pre-emptive isolation at admission on ICU:
VRE PCR + culture for confirmation
• Pitfalls of RDT
– Xpert VanA/VanB: Possibility of false positive result for vanB
• Anaerobic gut bacteria eg. Clostridium spp.

Vancomycin resistant enterococci
• Pitfalls of RDT: false positive vanB
– Solution: enrichment broth overnight + new cutoff Ct for positivity
Zhou et al, JCM 2014

Vancomycin resistant enterococci
• Conclusion
– Report Van A/Van B negative RDT results only
– Withhold positive RDT results until confirmatory culture result

MRSA

MRSA
NVMM guideline, HRMO, 2012

MRSA
NVMM guideline, HRMO,
2012; Lucet et al, 2012
Infection control precautions
are based on first RDT
results (low MRSA prevalence)

MRSA
Luteijn et al, CMI, 2011
Meta-analysis of diagnostic accuracy of MRSA PCR and culture

MRSA
UZLeuven data
GeneXpert MRSA
culture neg pos inhibition NPV PPV
2012 neg 710 6 12 99,2 76
pos 6 19 0
2013 neg 1075 8 11 98,5 83,3
pos 16 40 0
2014 (1st sem)
neg 1076 16 5 98,4 66,7
pos 18 32 0
Sensitivity Xpert MRSA: <95%
MRSA prevalence > 3%
“Low” NPV risk of false negative PCR less effective IC policies
RDT most useful in low MRSA prevalence region
MRSA PCR useful on ICU with confirmation culture

MRSA
• Cost-effectiveness of RDT for MRSA on ICU
– Pre-emptive isolation = quarantine of patients at admission with increased risk for MRSA
• Increased length of stay in hospital, farmers, previously MRSA positive, hospital/LTCF transfer
• Multicenter study The Netherlands, 12 ICU units, conventional culture vs RDT, MRSA prevalence 3.1% (Wassenberg et al, 2012)
• Effect of RDT on median duration of isolation on ICU
– 44.3% reduction in isolation days compared to culture strategy (831 463 days)
Wassenberg et al, Crit Care, 2012

MRSA
• Cost-effectiveness of RDT for MRSA on ICU
– Pre-emptive isolation = quarantine of patients at admission with increased risk for MRSA
• Multicenter study The Netherlands, 12 ICU units, conventional culture vs RDT, MRSA prevalence 3,1% (Wassenberg et al, 2012)
• Effect of RDT on isolation costs in ICU
Wassenberg et al, Crit Care, 2012

MRSA
NVMM guideline, HRMO, 2012, Roisin et al, 2012
Advantages of RDT for MRSA
• Low prevalence setting: Reduction in the N° pre-emptive isolation days
– RDT seems a safe approach even with non-100%-optimal for screening of high-risk patients
• High prevalence setting: More rapid reduction in prevalence (CDC 2006, Management
of MDRO in healthcare settings)
– Initially, RDT requires higher numbers of isolation beds, which will be compensated in the long term
Pitfalls of RDT for MRSA
• Accurate distinguishing between MRSA and MSSA + MR CNS amplification of SCCmec-OrfX junction of S aureus
• False positives
• Partial deletions of SCCmec (mecA gene negative, SCCmec remnants)
• CC1 MSSA: additional annealing sequence at SCC integration site (3-5% prevalence)
• False negatives
• Variability in this SCCmec region, eg. PFGE type A20 (SCCmec type IV variants)

MRSA
Conclusion: RDT for MRSA
RDT based isolation measures on ICU, ‘low’ prevalence setting
=
• SAFE
• LESS ISOLATION DAYS
• COST REDUCTION to be determined (false-negatives)

Group B Streptococcus

Group B Streptococcus
Aim of screening antenatal
• Since universal screening of pregnant women 35-37 wks: reduction of the risk of early-onset GBS infection in neonates from 1,5 (1980s) 0,34 (2010) /1000 births
• >70% of Early-onset neonatal GBS infections mothers with negative/unknown colonisation status at 35-37 wks’ gestation (Poncelet et al, 2013)

Group B Streptococcus
Routine culture
• LIM broth for optimal sensitivity
• Up to 5% non-haemolytic not granadaene producing strains
• At 35-37 weeks of pregnancy
– PPV of antenatal screening for GBS colonisation at delivery: 59%
– NPV: 92%
RDT
• RT-PCR: eg. Xpert GBS: detects a conserved target sequence adjacent to cfb gene (encoding S. agalactiaeCAMP factor)
• Intrapartum testing possible

Group B Streptococcus
RDT: multicentre evaluation
Buchan et al, J Clin Microbiol 2015

Group B Streptococcus
Conclusions for using GBS RDT in routine
• 35-37 weeks culture screening vs RDT at time of delivery
– 13.6% vs 4.5% unnecessary antibiotic prophylaxis
– Possibility of increased antimicrobial resistance to penicillin, clindamycin, erythromycin
– Cost of an Early-Onset GBS infection > 19.000 euro
• Remaining questions
– RDT decentralized
– Cost-effectiveness studies ongoing
– European Consensus, Florence 2013: intrapartum screening recommended using rapid real-time testing
– BHC recommendations in preparation

Clostridium difficile

Clostridium difficile
Planche and Wilcox 2015
Bagdasarian et al, JAMA 2015

Clostridium difficile
Planche and Wilcox 2015
JAMA 2015

Clostridium difficile
• RDT (NAAT) tests for toxin gene detection
– Improved sensitivity over immunoassays
– Detect strains (with toxin genes) rather than presence of free toxins
– Fail to discriminate between CDI and asymptomatic colonization with C. difficile
– Clear drawbacks as stand-alone diagnostic tests (Wilcox, 2012, CMI;
Planche et al, Infect Dis Clin N Am 2015)
• PPVs for NAATs = 54% (in comparison with cell cytotoxin assay)
overdiagnosis of CDI, overtreatment and overuse of isolation
measures
– CDI diagnosed by NAAT: 30% lower complication rates than CDI diagnosed by EIA / cytotoxin assay (Longtin et al, CID, 2013)

Clostridium difficile
Berry et al, J Hosp Infect, 2014
Correlation RT-PCR with clinical diagnosis of CDI

Clostridium difficile
Berry et al, J,Hosp Infect, 2014
Sensitivity of PCR > cell
culture cytotoxicity and
GDH
(clinical diagnosis =
golden standard)
! 30-day mortality
higher in PCR+ /
CCNA+ group (27%)
than in PCR+ / CCNA –
group (19%)

Clostridium difficile
• Conclusions
– Multistep algorithm based on GDH / toxin EIA and NAAT most informative at this moment
– Further studies urgently needed comparing diagnostic strategies with clinical diagnosis of CDI

Norovirus

Norovirus
MacCannell T et al, HICPAC 2011
• Background of norovirus infection
• ssRNA virus of the family Caliciviridae
• Most human infections: genogroups GI and GII
• Norovirus: >50% of reported gastro-enteritis outbreaks in hospitals and LTC facilities
• Significant costs related to isolation precautions and PPE, ward closures, supplemental environmental cleaning, staff cohorting
• Clinical diagnosis:
• golden standard for laboratory diagnosis: RT-PCR

Norovirus
MacCannell T et al, HICPAC 2011
• Diagnosis of a norovirus infection
• Specimen: stool > rectal swab > vomitus
• Timing: within 2-3 days after onset of illness
• golden standard for laboratory diagnosis: RT-PCR
• Also available: ELISA, Electron microscopy: low sensitivity

Norovirus
• Diagnosis of a norovirus outbreak
• Specimen collection
• Min N° stool samples from symptomatic patients needed to confirm an outbreak
• N° of stools: whole stools of ≥ 5 ill persons diagnosis of outbreak
Method N° pos results
(Total N° stools of
symptomatic persons)
Sensitivity (%)
EIA ≥ 1 (6) 71-92
RT-PCR ≥ 1 (2-4) >84
≥ 2 (5-11) >92

Norovirus
• Diagnosis of a norovirus outbreak
• Specimen collection
• One stool specimen: diagnostic capacity for an outbreak of PCR > EM or ELISA
• Detection limit RT-PCR: 101-103 PCR detectable units/amplification reaction ↔ 107 PDU/mL in acute phase infection (Green et al, 2003)
PCR = gold standard

Norovirus
MacCannell T et al, HICPAC 2011
• Diagnosis of a norovirus outbreak
• Concluding recommendation for use of PCR technique (CDC-HICPAC 2011)
• Surveillance
No literature to determine whether active case-finding and tracking of new norovirus cases were directly associated with shorter outbreaks or more efficient outbreak containment
• Norovirus detectable for days-weeks after initial infection no requirement for PCR in patients who have formed stools

Norovirus
Norovirus Working Party, NHS UK

Norovirus
• a norovirus outbreak in real life: batch in-house RT-PCR

Norovirus
• a norovirus outbreak: RDT effect on isolation days

Norovirus
• Conclusions
– Depending on isolation policy for diarrhoea: Norovirus vs other enteropathogens
• RDT possibly helpful in reduction of isolation days

Conclusions
• RDT are powerful tools in infection prevention: reduction in isolation days
• Their high costs is an important drawback
• Further economical and clinical studies needed to determine their place in diagnostic algorithms