Embed Size (px)
Citation preview
OXFAM GB Lucia Rost
March 2015
apcarea
Rapid Care Analysis Copperbelt, Zambia
1
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
CONTENT CONTENT ........................................................................................................................................... 1 ACRONYMS AND ABBREVIATIONS .......................................................................................................... 2 ACKNOWLEDGEMENT .......................................................................................................................... 3 MAP OF COPPERBELT REGION .............................................................................................................. 4 EXECUTIVE SUMMARY .......................................................................................................................... 5 OUTLINE OF THE REPORT...................................................................................................................... 8 PART 1 – INTRODUCTION AND BACKGROUND .............................................................................. 9
1.1 THE GEM PROJECT IN THE COPPERBELT REGION ................................................................. 10 1.2 WOMEN’S UNPAID CARE WORK ......................................................................................... 10 1.3 OXFAM’S WE CARE PROJECT ............................................................................................. 12 1.4 CARE WORK IN ZAMBIA, COPPERBELT REGION..................................................................... 13 1.5 THE RAPID CARE ANALYSIS IN THE COPPERBELT REGION ....................................................... 13
PART 2 - METHODOLOGY .............................................................................................................. 14 2.1 WHAT IS THE RCA? ........................................................................................................... 15 2.2 LOCATIONS AND PARTICIPANTS ........................................................................................... 15 2.3 RCA TOOLS ...................................................................................................................... 15 2.4 FACILITATION .................................................................................................................... 17 2.5 TRAINING ......................................................................................................................... 17 2.5 BRIEFING AND FEEDBACK................................................................................................... 18 2.6 LIMITATIONS ..................................................................................................................... 18 2.7 ETHICAL CONSIDERATIONS ................................................................................................. 18
PART 3 - FINDINGS ........................................................................................................................ 20 3.1 WHAT IS CARE WORK?.......................................................................................................21 3.2 WHY IS CARE IMPORTANT? ................................................................................................. 22 3.3 WHO DOES WHAT? ............................................................................................................ 23 3.4 WHO DOES WHAT CARE WORK? .......................................................................................... 23 3.5 NORMS, CULTURE AND CARE WORK .................................................................................... 28 3.6 AGE AND CARE WORK ........................................................................................................ 30 3.7 SEASONAL CHANGES IN CARE WORK .................................................................................... 33 3.8 NEGATIVE CONSEQUENCES OF ‘UNEQUAL’ AND ‘HEAVY’ CARE WORK........................................ 36 3.9 AVAILABLE INFRASTRUCTURE AND SERVICES FOR CARE WORK ................................................ 39 3.10 MOST PROBLEMATIC CARE ACTIVITIES .................................................................................. 42 3.11 SOLUTIONS....................................................................................................................... 43
PART 4 CONCLUSIONS & RECOMMENDATIONS ...................................................................... 51 4.2 RECOMMENDATIONS FOR THE GEM PROJECT ...................................................................... 52 4.2 RECOMMENDATIONS FOR INCLUDING CARE WORK IN OTHER PROJECTS ................................... 53 4.2 RECOMMENDATIONS FOR CONDUCTING THE RCA ................................................................. 55
APPENDICES ................................................................................................................................. 58
2
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Acronyms and Abbreviations
CINDI Children in Distress
CSO Civil Society Organisation
DFID Department for International Development
FGD Focus Group Discussion
GEM Gendered Enterprise and Markets
HCS Household Care Survey
RCA Rapid Care Analysis
SAP Sustainable Agriculture Program
SHF Smallholder farmers
UN United Nations
WE Care Women’s Economic Empowerment and Care-Evidence for Influencing Change

3
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Acknowledgement The project would not have been possible without the kind support and help of many people. I would like to thank everyone who was involved in the Rapid Care Analysis in the Copperbelt region. I want to thank Mr Thomas Tichar, Ms Thalia Kidder, Ms Jane Remme, Ms Yvonne Chibiya and Ms Lomthnuzi Jere who provided excellent guidance and support from Oxfam. I also extend my sincere thanks to Mrs Mpenza Mwanza, Mr Jones Chitondo, Mrs Joyce Phiri and Ms Emelda Nanyangwe who did a wonderful job at organising and managing the RCAs and to Mr Alfred Zimba, Ms Kunda Jesinta, Mr Nicholas Chama, Mr Isaac Mwakilima, Ms Deophister Kakungu, Ms Mwape Anita, Ms Doris Siankwilimba, Mr Nkonge Sydney, Mr Felix Sikana and Mr Kakoma Mathews for their great work on facilitating and coordinating the RCAs. My thanks and appreciations also go to the communities in Kitwe, Ndola, Mufulira and Kalulushi district who welcomed us warmly and enriched us with their lively participation.
4
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
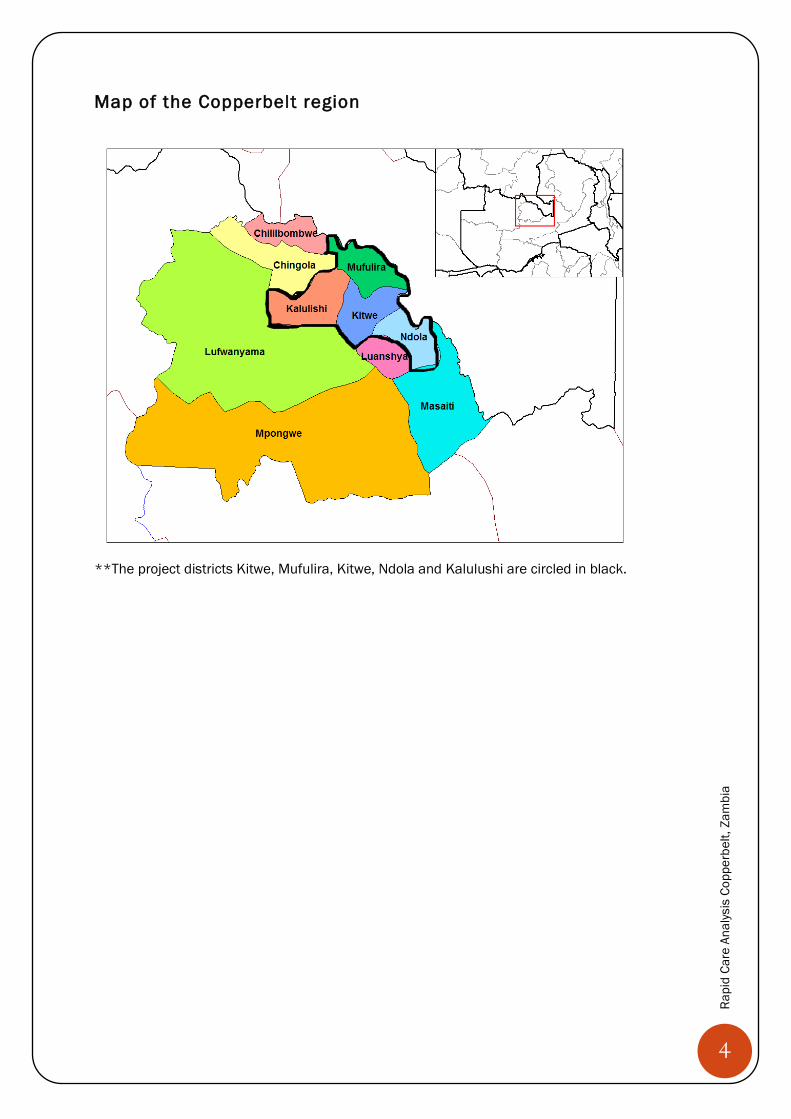
Map of the Copperbelt region
**The project districts Kitwe, Mufulira, Kitwe, Ndola and Kalulushi are circled in black.
5
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
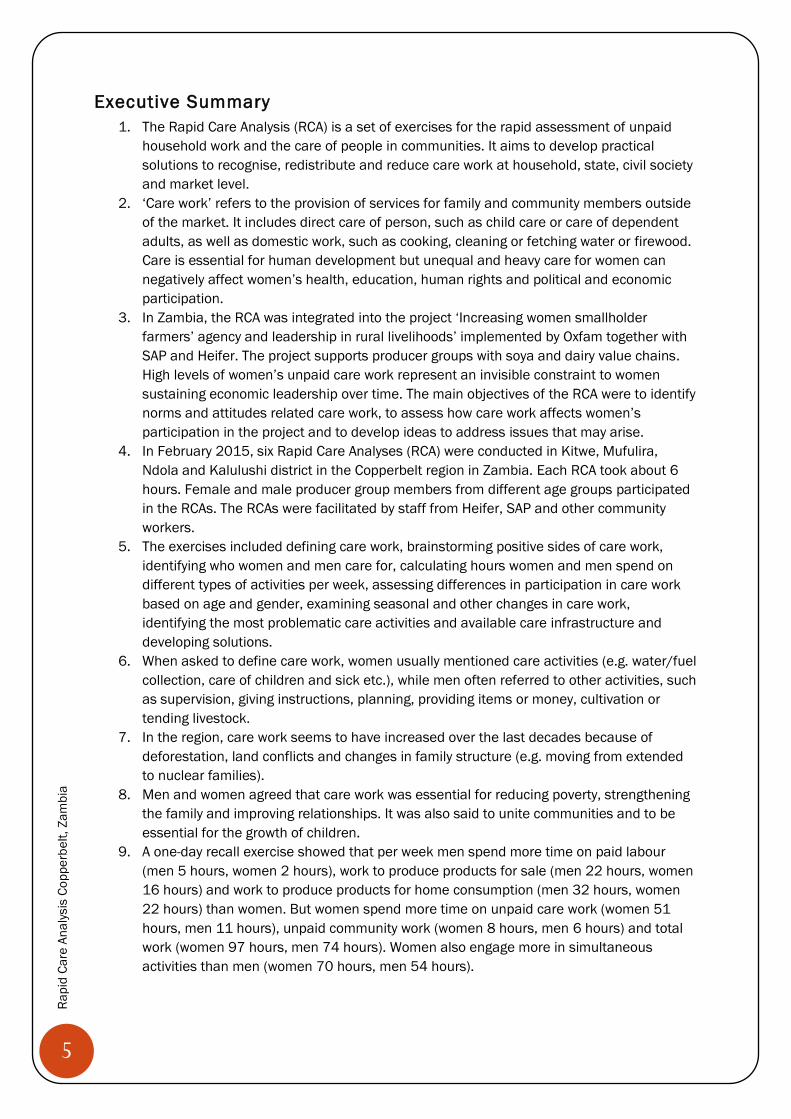
Executive Summary 1. The Rapid Care Analysis (RCA) is a set of exercises for the rapid assessment of unpaid
household work and the care of people in communities. It aims to develop practical solutions to recognise, redistribute and reduce care work at household, state, civil society and market level.
2. ‘Care work’ refers to the provision of services for family and community members outside of the market. It includes direct care of person, such as child care or care of dependent adults, as well as domestic work, such as cooking, cleaning or fetching water or firewood. Care is essential for human development but unequal and heavy care for women can negatively affect women’s health, education, human rights and political and economic participation.
3. In Zambia, the RCA was integrated into the project ‘Increasing women smallholder farmers’ agency and leadership in rural livelihoods’ implemented by Oxfam together with SAP and Heifer. The project supports producer groups with soya and dairy value chains. High levels of women’s unpaid care work represent an invisible constraint to women sustaining economic leadership over time. The main objectives of the RCA were to identify norms and attitudes related care work, to assess how care work affects women’s participation in the project and to develop ideas to address issues that may arise.
4. In February 2015, six Rapid Care Analyses (RCA) were conducted in Kitwe, Mufulira, Ndola and Kalulushi district in the Copperbelt region in Zambia. Each RCA took about 6 hours. Female and male producer group members from different age groups participated in the RCAs. The RCAs were facilitated by staff from Heifer, SAP and other community workers.
5. The exercises included defining care work, brainstorming positive sides of care work, identifying who women and men care for, calculating hours women and men spend on different types of activities per week, assessing differences in participation in care work based on age and gender, examining seasonal and other changes in care work, identifying the most problematic care activities and available care infrastructure and developing solutions.
6. When asked to define care work, women usually mentioned care activities (e.g. water/fuel collection, care of children and sick etc.), while men often referred to other activities, such as supervision, giving instructions, planning, providing items or money, cultivation or tending livestock.
7. In the region, care work seems to have increased over the last decades because of deforestation, land conflicts and changes in family structure (e.g. moving from extended to nuclear families).
8. Men and women agreed that care work was essential for reducing poverty, strengthening the family and improving relationships. It was also said to unite communities and to be essential for the growth of children.
9. A one-day recall exercise showed that per week men spend more time on paid labour (men 5 hours, women 2 hours), work to produce products for sale (men 22 hours, women 16 hours) and work to produce products for home consumption (men 32 hours, women 22 hours) than women. But women spend more time on unpaid care work (women 51 hours, men 11 hours), unpaid community work (women 8 hours, men 6 hours) and total work (women 97 hours, men 74 hours). Women also engage more in simultaneous activities than men (women 70 hours, men 54 hours).
6
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
10. Women and men agreed that women did more care work and only few participants reported that men engaged in care activities. Men usually said that women would not want their help with care work but women often disagreed.
11. It seemed like men were least likely to engage in childcare and cooking and more likely to provide support with collecting water or firewood, washing or caring for community members.
12. Participants mentioned the following reasons for gendered care responsibilities: tradition/culture, ‘natural’ maternal love, God creating women to do care work, perceptions of community members, male alcohol consumption and women having less decision-making power or being intimidated by men.
13. The age and care exercise showed that females of all age groups perform more care work than males. The difference between male and female involvement in care work is highest for middle-aged adults and lowest for children. Participants concluded that gender roles become internalised through socialisation in childhood and youth and that school performance of girls and female teenagers is affected by care work.
14. The dairy and soya value chains are at their peak approximately at the same time when care work is also at its peak. Participants concluded that they should distribute activities throughout the year, hire someone to help out in the most work intense months and share responsibilities,
15. Care work was said to affect participants’ involvement in the soya and dairy value chains and in other economic activities, as well as their participation in trainings, producer group activities, leadership and community work. It was also said to have negative effects on health and well-being.
16. Caring for the sick was most often selected as one of the most problematic activities (6 times, 63 dots), followed by child care (5 times, 37 dots), fetching water and cooking (3 times, 19 dots) and fetching firewood (2 times, 14 dots) and washing (1 time, 8 dots).
17. Participants mentioned the following household level solutions to reduce care work: working together as a family, developing a duty roster, teaching children to perform care work together, encouraging discussions between husbands and wives and changing culture and traditions.
18. State level solutions included providing clinics, schools, road networks, electricity, markets and other types of support, such as a hammer mills, police posts, elderly homes and orphanages.
19. Civil society level solutions included trainings on care work with husbands and wives and as part of the school curriculum, supporting home based care systems, advocacy for state services and direct support, such as providing stoves, loans, treadle pumps or services for children.
20. The main market level solutions were fuel efficient stoves, hammer mills, water pumps/ tanks and shellers for soya beans.
21. Overall, participants ranked the household and civil society level solutions higher than the solutions at state and market level.
22. Women and men participated actively in the discussions and women usually spoke up openly in front of their husbands. Participants often laughed when conservative views on gender roles were expressed and applauded when couples said that they were sharing tasks. Men usually engaged more in discussions on infrastructure and cultivation and women more in those about types of care work. Several participants suggested to conduct the RCA with couples.

7
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
23. Based on the RCA findings and discussions with several people, I propose the following recommendations for the project: 1) Include some RCA exercises in the pre-trainings for new producer groups, 2) Improve access to fuel efficient stoves, water sources, shellers and hammer mills, 3) Advocacy for state services and 4) Introduce group-based health care support system
24. Recommendations for including care work in other Oxfam projects include1) Integrate care work and RCA in “I Care About Her Campaign”, 2) Integrate care work and RCA in new education project, 3) Consider the care calendar in project design and execution
25. The main recommendations for conducting the RCA are structuring the training as an RCA, including a discussion on the value of care work, guiding participants through each hour of the day when filling in the one-day recall, adding project related work to the seasonal calendar, using the same key for all ranking exercises and producing ‘exercises cards’ and materials for participants.
8
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Outline of the report This report presents the findings from six RCAs in the Copperbelt region conducted in February 2015. The first chapter outlines the background of the RCAs in the Copperbelt region, providing basic information about the GEM project, unpaid care work and the WE care project. The second chapter summarises the methodology, in particular the exercises, the training, facilitation and potential limitations. The third chapter elaborates on the findings. As the findings from all six RCAs are very similar, the answers are combined in one chapter. But numbers in brackets link findings to the specific RCAs (1,2,3 for SAP RCAs and 5,6,7 for Heifer RCAs). Beige text boxes present quotes of participants to illustrate the findings. The last chapter outlines recommendations for the GEM project, for integrating care into other projects and for conducting the RCA.
RCA 2
RCA 4
9
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
PART 1 INTRODUCTION AND BACKGROUND
Women in RCA 3 d isc uss ing the one -day reca l l ho urs
10
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
The GEM Project in the Copperbelt region The Oxfam project ‘Increasing women smallholder farmers’ agency and leadership in rural livelihoods ‘ is a Department for International Development (DFID) funded project which runs from 2014-2017 and is being implemented in Bangladesh, Tajikistan and Zambia. The project uses Oxfam’s Gendered Enterprise and Markets (GEM) approach that builds the resilience and sustainability of smallholder farmers’ (SHF) livelihoods by improving their power in agricultural markets, promoting women’s economic leadership, and incorporating climate change adaptation and risk reduction. The GEM approach has so far been used in 14 countries across the world. The rationale is that an increase in family income and food security depends on 1) women’s empowerment and agency, 2) community capacity to manage risk and adapt to climate changes; and 3) SHF power and linkages in market systems and governmental policy-making. The project includes:
1) Capacity building of SHFs who work as producer groups e.g. training in leadership, crop and water management or participatory risk assessment 2) Empowerment through supporting especially women-focused producer groups and ensuring that women have representation 3) Advocacy at local, national and global level to improve decision-making of producer groups, influence private sector investment strategies and public sector spending and engage in cross-country learning and influencing.
In Zambia the GEM project areas are Mufulira, Kitwe, Kalulushi and Ndola districts in the Copperbelt region and the project is implemented with the help of two partner organisations. Heifer international are responsible for developing the dairy and the soya beans values chains in three districts and have been working with rural communities in 5 provinces since 1998. Sustainable Agriculture Program (SAP) manage the soya value chain in Kitwe and Ndola districts and have been working with smallholder farmers (SHF) since 2004. Through previous work with smallholder farmers in the region Oxfam has established solid relationships with Parmalat (dairy) and Astral Holdings (soya) in the Copperbelt. The Ministries of Agriculture and Livestock (MAL), Community Development and the Department of Water Affairs will support in the delivery of extension services and training in crop and livestock production. One of the main objectives of the GEM project is women’s empowerment and agency. This means promoting women’s ability to proactively influence decisions that affect their lives and wellbeing, supporting women-led producer groups and promoting new market roles for women. It also includes addressing high levels of women’s unpaid care work, which represents an invisible constraint to women sustaining economic leadership over time. In Zambia, the prevalence of HIV and child malnutrition puts a significant burden on women’s care work, given the continued lack of basic social services to rural communities.
Women’s Unpaid Care Work The term ‘unpaid care work’ has increasingly been used to describe direct care of persons and domestic work for family members and other households (Budlender, 2007). Housework is included in the term because it serves the well-being of people as a form of ‘indirect care’ (Folbre 2006). The term also includes care of dependents, as well as mutual care of ‘healthy adults’
11
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
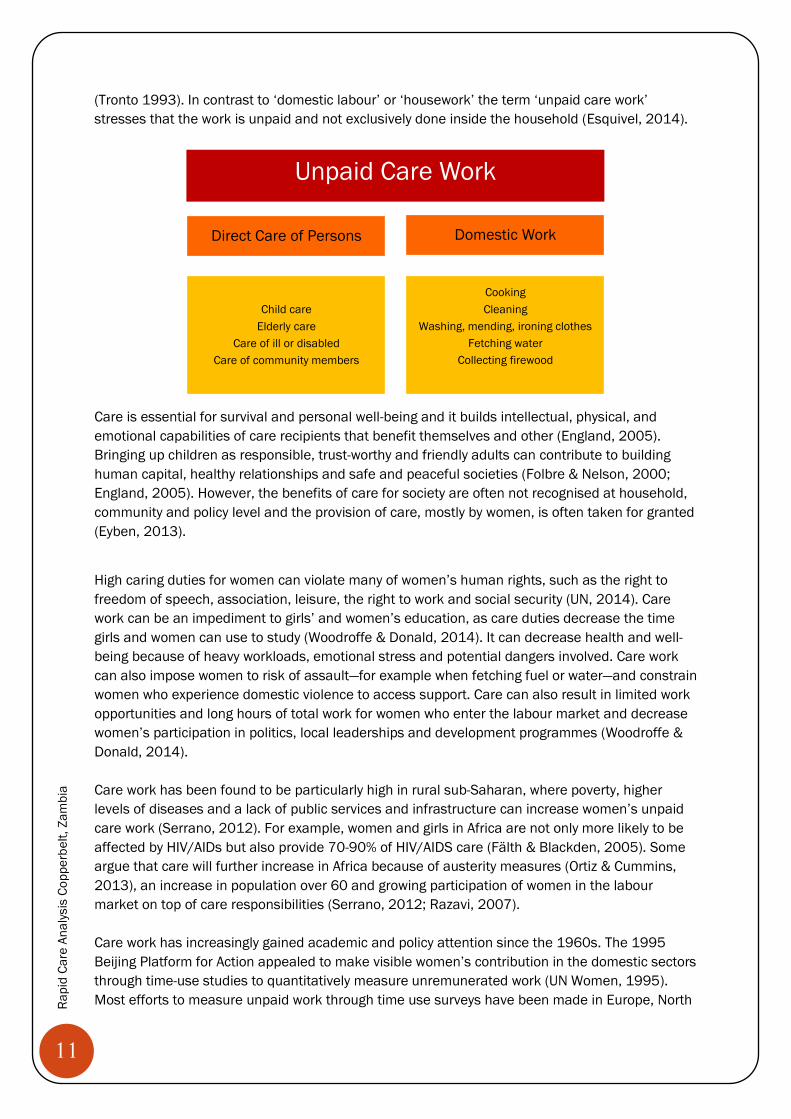
(Tronto 1993). In contrast to ‘domestic labour’ or ‘housework’ the term ‘unpaid care work’ stresses that the work is unpaid and not exclusively done inside the household (Esquivel, 2014).
Care is essential for survival and personal well-being and it builds intellectual, physical, and emotional capabilities of care recipients that benefit themselves and other (England, 2005). Bringing up children as responsible, trust-worthy and friendly adults can contribute to building human capital, healthy relationships and safe and peaceful societies (Folbre & Nelson, 2000; England, 2005). However, the benefits of care for society are often not recognised at household, community and policy level and the provision of care, mostly by women, is often taken for granted (Eyben, 2013).
High caring duties for women can violate many of women’s human rights, such as the right to freedom of speech, association, leisure, the right to work and social security (UN, 2014). Care work can be an impediment to girls’ and women’s education, as care duties decrease the time girls and women can use to study (Woodroffe & Donald, 2014). It can decrease health and well-being because of heavy workloads, emotional stress and potential dangers involved. Care work can also impose women to risk of assault—for example when fetching fuel or water—and constrain women who experience domestic violence to access support. Care can also result in limited work opportunities and long hours of total work for women who enter the labour market and decrease women’s participation in politics, local leaderships and development programmes (Woodroffe & Donald, 2014). Care work has been found to be particularly high in rural sub-Saharan, where poverty, higher levels of diseases and a lack of public services and infrastructure can increase women’s unpaid care work (Serrano, 2012). For example, women and girls in Africa are not only more likely to be affected by HIV/AIDs but also provide 70-90% of HIV/AIDS care (Fälth & Blackden, 2005). Some argue that care will further increase in Africa because of austerity measures (Ortiz & Cummins, 2013), an increase in population over 60 and growing participation of women in the labour market on top of care responsibilities (Serrano, 2012; Razavi, 2007). Care work has increasingly gained academic and policy attention since the 1960s. The 1995 Beijing Platform for Action appealed to make visible women’s contribution in the domestic sectors through time-use studies to quantitatively measure unremunerated work (UN Women, 1995). Most efforts to measure unpaid work through time use surveys have been made in Europe, North
Direct Care of Persons Domestic Work
Child care Elderly care
Care of ill or disabled Care of community members
Cooking Cleaning
Washing, mending, ironing clothes Fetching water
Collecting firewood
Unpaid Care Work
12
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
America and Australia (Budlender, 2008). Several studies have pointed to a lack of visibility of care work in development policy (e.g. Chopra, 2013; Bibler & Zuckerman, 2013), arguing that such omission occurs because rethinking the implications of care would require a reassessment of the whole gendered capitalist political system that is based on women’s unpaid care as a safety-net (Eyben, 2013). However, recently care work has been more widely discussed in development and the Open Working Group (OWG) on the post 2015 Sustainable Development Goals reflects these debates and includes a target on unpaid care work under Goal 5—‘Achieve gender equality and empower all women and girls’1.
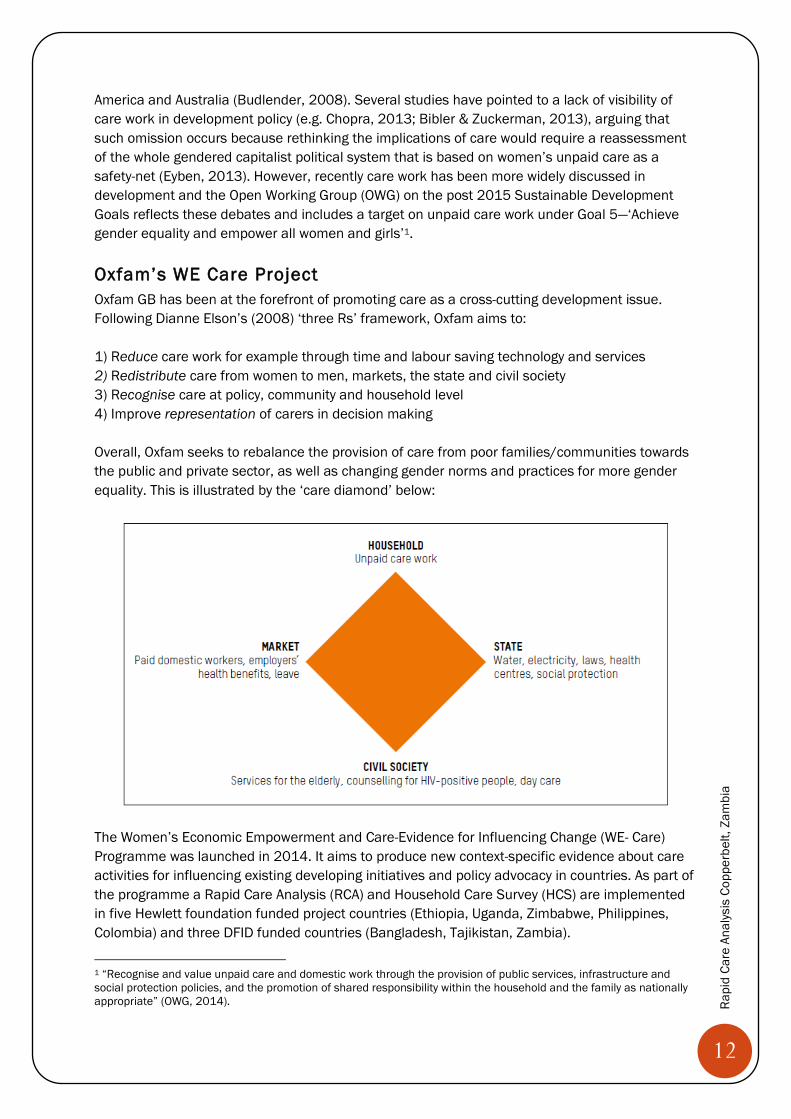
Oxfam’s WE Care Project Oxfam GB has been at the forefront of promoting care as a cross-cutting development issue. Following Dianne Elson’s (2008) ‘three Rs’ framework, Oxfam aims to: 1) Reduce care work for example through time and labour saving technology and services 2) Redistribute care from women to men, markets, the state and civil society 3) Recognise care at policy, community and household level 4) Improve representation of carers in decision making Overall, Oxfam seeks to rebalance the provision of care from poor families/communities towards the public and private sector, as well as changing gender norms and practices for more gender equality. This is illustrated by the ‘care diamond’ below:
The Women’s Economic Empowerment and Care-Evidence for Influencing Change (WE- Care) Programme was launched in 2014. It aims to produce new context-specific evidence about care activities for influencing existing developing initiatives and policy advocacy in countries. As part of the programme a Rapid Care Analysis (RCA) and Household Care Survey (HCS) are implemented in five Hewlett foundation funded project countries (Ethiopia, Uganda, Zimbabwe, Philippines, Colombia) and three DFID funded countries (Bangladesh, Tajikistan, Zambia).
1 “Recognise and value unpaid care and domestic work through the provision of public services, infrastructure and social protection policies, and the promotion of shared responsibility within the household and the family as nationally appropriate” (OWG, 2014).
13
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Household Care Survey The Household Care Survey aims to build understanding about pathways of positive change for more equitable care provision in households and communities. It asks about time use and enabling/disenabling factors and is implemented before and after the implementation of ‘care strategies’. Rapid Care Analysis The Rapid Care Analysis is a set of exercises for the rapid assessment of unpaid household work and the care of people in communities. It aims to provide women and men with a space to explore the issue of care together and to collaboratively develop practical solutions. Care work in Zambia, Copperbelt region There seems to be little literature about care work in Zambia, especially specific to the Copperbelt region. The Women’s Empowerment in Agriculture Index was tested in the Eastern province in Zambia and out of the five categories (production decision-making, access to productive resources, control over use of income, community leadership and time allocation/workloads), workloads was the factor contributing mostly to women’s disempowerment (31.3%) (Malapit et al., 2014). GEMSA and VSO-RAISA produced a ‘Make Care Work Count: Policy Handbook’ to help country facilitators in Southern Africa with advocacy for the recognition of care providers’ unpaid labour in policy making. The handbook focuses mainly on direct care of persons and shows that across Southern Africa, unpaid, voluntary, informal networks of care providers have emerged to care for sick people, especially those affected by HIV, malaria and TB to fill the health care gap left by governments. It ranks Zambian care work policies as mediocre, as there are limited trainings for carers and no care policies on remuneration, logistic and material support, psychosocial support and gender equality.
Oxfam’s 2011 Effectiveness Review of Women’s Empowerment and Livelihood Support in the Copperbelt did not address care work. This might have contributed to the mixed findings that the project positively affected women’s ability to influence community governance and ownership of strategic assets but did not affect involvement in household decision making and self-efficacy (Oxfam, 2011).
Objectives of the Rapid Care Analysis in Zambia In Zambia, six RCAs were implemented in the four project intervention districts. The overall objective was to develop good practice to reduce, redistribute and recognise care work so that women can increase their income, agency and ability to influence decisions individually and collectively. This includes the following questions: 1) What are norms, perceptions and attitudes around care work and gender roles at the start of the project? 2) How does women’s care work affect their economic empowerment and income? 3) What would be good principles to influence other stakeholders to be aware of women’s unpaid care work and to encourage them to address the issue, especially states and markets?
14
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
PART 2
METHODOLOGY
Man in RCA 4 filling in the one-day recall
15
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
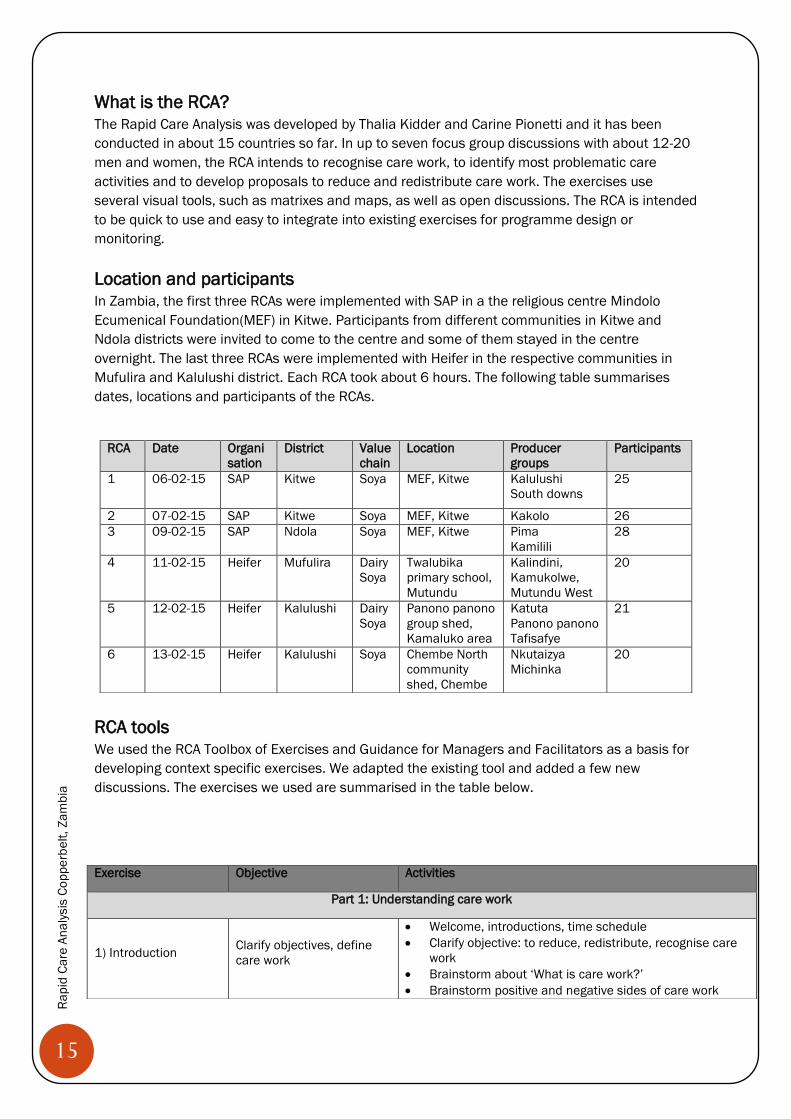
What is the RCA? The Rapid Care Analysis was developed by Thalia Kidder and Carine Pionetti and it has been conducted in about 15 countries so far. In up to seven focus group discussions with about 12-20 men and women, the RCA intends to recognise care work, to identify most problematic care activities and to develop proposals to reduce and redistribute care work. The exercises use several visual tools, such as matrixes and maps, as well as open discussions. The RCA is intended to be quick to use and easy to integrate into existing exercises for programme design or monitoring. Location and participants In Zambia, the first three RCAs were implemented with SAP in a the religious centre Mindolo Ecumenical Foundation(MEF) in Kitwe. Participants from different communities in Kitwe and Ndola districts were invited to come to the centre and some of them stayed in the centre overnight. The last three RCAs were implemented with Heifer in the respective communities in Mufulira and Kalulushi district. Each RCA took about 6 hours. The following table summarises dates, locations and participants of the RCAs.
RCA tools We used the RCA Toolbox of Exercises and Guidance for Managers and Facilitators as a basis for developing context specific exercises. We adapted the existing tool and added a few new discussions. The exercises we used are summarised in the table below.
RCA Date Organisation
District Value chain
Location Producer groups
Participants
1 06-02-15 SAP Kitwe Soya MEF, Kitwe Kalulushi South downs
25
2 07-02-15 SAP Kitwe Soya MEF, Kitwe Kakolo 26 3 09-02-15 SAP Ndola Soya MEF, Kitwe Pima
Kamilili 28
4 11-02-15 Heifer Mufulira Dairy Soya
Twalubika primary school, Mutundu
Kalindini, Kamukolwe, Mutundu West
20
5 12-02-15 Heifer Kalulushi Dairy Soya
Panono panono group shed, Kamaluko area
Katuta Panono panono Tafisafye
21
6 13-02-15 Heifer Kalulushi Soya Chembe North community shed, Chembe
Nkutaizya Michinka
20
Exercise Objective Activities
Part 1: Understanding care work
1) Introduction Clarify objectives, define care work
x Welcome, introductions, time schedule x Clarify objective: to reduce, redistribute, recognise care
work x Brainstorm about ‘What is care work?’ x Brainstorm positive and negative sides of care work
16
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
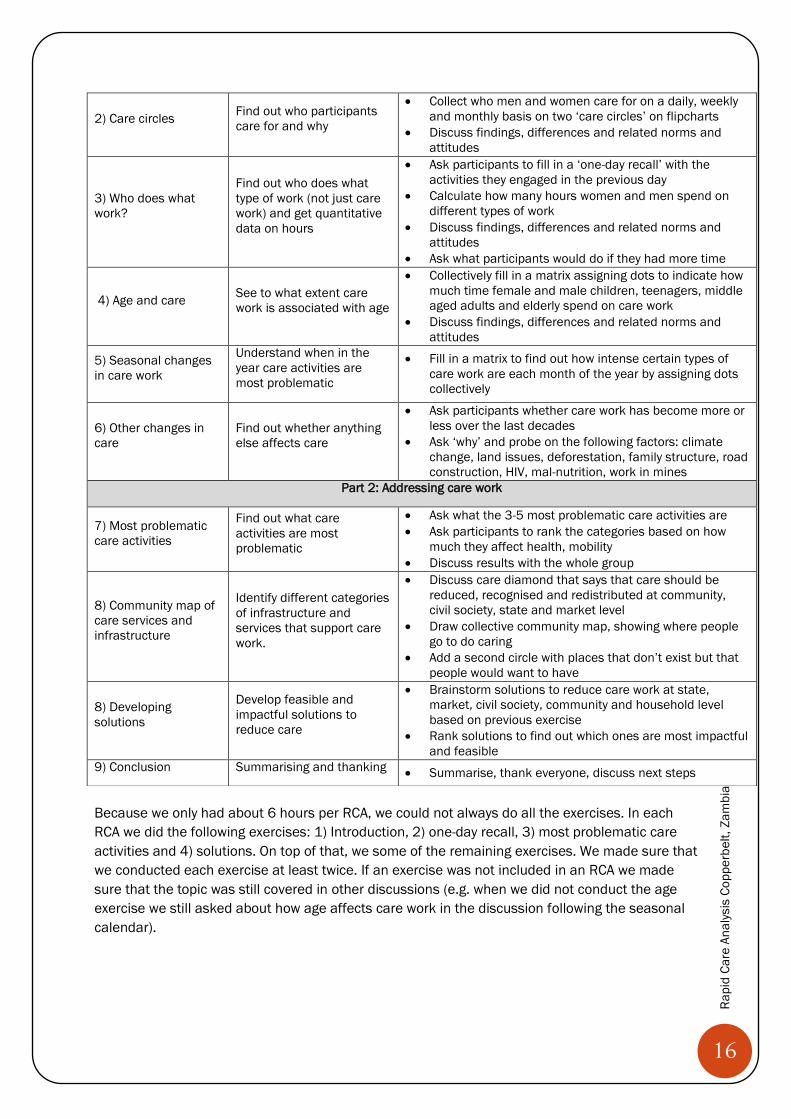
Because we only had about 6 hours per RCA, we could not always do all the exercises. In each RCA we did the following exercises: 1) Introduction, 2) one-day recall, 3) most problematic care activities and 4) solutions. On top of that, we some of the remaining exercises. We made sure that we conducted each exercise at least twice. If an exercise was not included in an RCA we made sure that the topic was still covered in other discussions (e.g. when we did not conduct the age exercise we still asked about how age affects care work in the discussion following the seasonal calendar).
2) Care circles Find out who participants care for and why
x Collect who men and women care for on a daily, weekly and monthly basis on two ‘care circles’ on flipcharts
x Discuss findings, differences and related norms and attitudes
3) Who does what work?
Find out who does what type of work (not just care work) and get quantitative data on hours
x Ask participants to fill in a ‘one-day recall’ with the activities they engaged in the previous day
x Calculate how many hours women and men spend on different types of work
x Discuss findings, differences and related norms and attitudes
x Ask what participants would do if they had more time
4) Age and care See to what extent care work is associated with age
x Collectively fill in a matrix assigning dots to indicate how much time female and male children, teenagers, middle aged adults and elderly spend on care work
x Discuss findings, differences and related norms and attitudes
5) Seasonal changes in care work
Understand when in the year care activities are most problematic
x Fill in a matrix to find out how intense certain types of care work are each month of the year by assigning dots collectively
6) Other changes in care
Find out whether anything else affects care
x Ask participants whether care work has become more or less over the last decades
x Ask ‘why’ and probe on the following factors: climate change, land issues, deforestation, family structure, road construction, HIV, mal-nutrition, work in mines
Part 2: Addressing care work
7) Most problematic care activities
Find out what care activities are most problematic
x Ask what the 3-5 most problematic care activities are x Ask participants to rank the categories based on how
much they affect health, mobility x Discuss results with the whole group
8) Community map of care services and infrastructure
Identify different categories of infrastructure and services that support care work.
x Discuss care diamond that says that care should be reduced, recognised and redistributed at community, civil society, state and market level
x Draw collective community map, showing where people go to do caring
x Add a second circle with places that don’t exist but that people would want to have
8) Developing solutions
Develop feasible and impactful solutions to reduce care
x Brainstorm solutions to reduce care work at state, market, civil society, community and household level based on previous exercise
x Rank solutions to find out which ones are most impactful and feasible
9) Conclusion Summarising and thanking x Summarise, thank everyone, discuss next steps
17
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
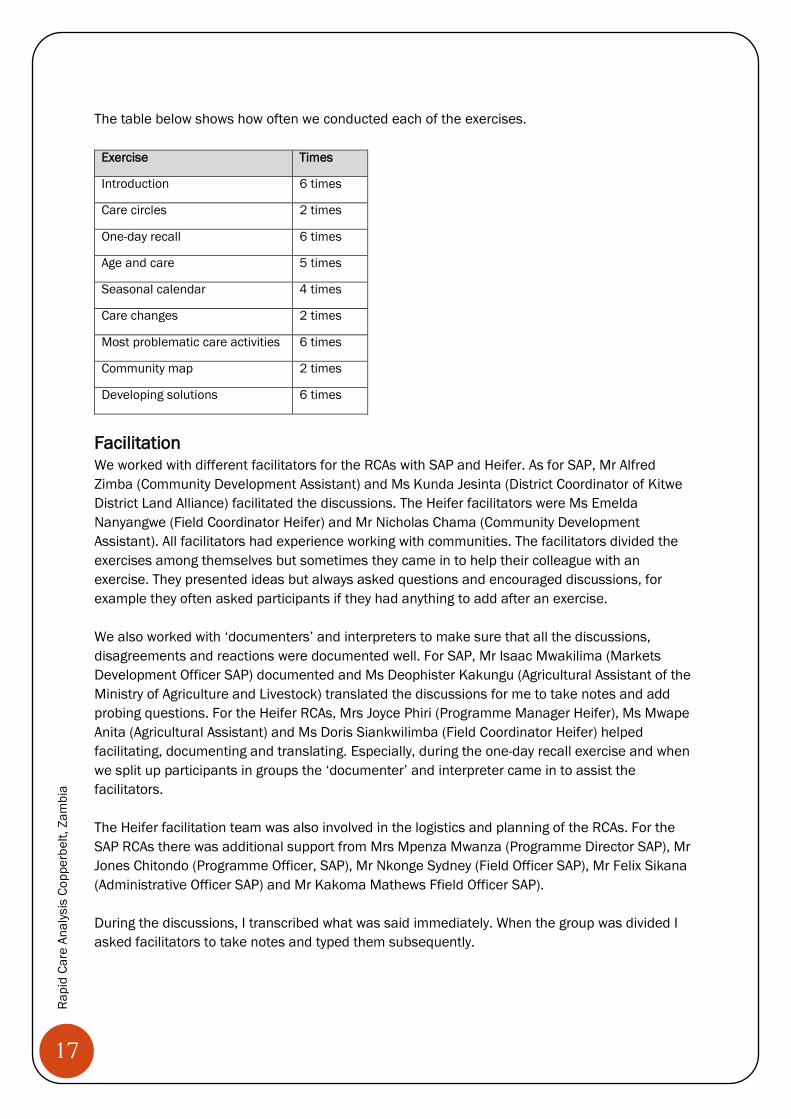
The table below shows how often we conducted each of the exercises.
Exercise Times
Introduction 6 times
Care circles 2 times
One-day recall 6 times
Age and care 5 times
Seasonal calendar 4 times
Care changes 2 times
Most problematic care activities 6 times
Community map 2 times
Developing solutions 6 times
Facilitation We worked with different facilitators for the RCAs with SAP and Heifer. As for SAP, Mr Alfred Zimba (Community Development Assistant) and Ms Kunda Jesinta (District Coordinator of Kitwe District Land Alliance) facilitated the discussions. The Heifer facilitators were Ms Emelda Nanyangwe (Field Coordinator Heifer) and Mr Nicholas Chama (Community Development Assistant). All facilitators had experience working with communities. The facilitators divided the exercises among themselves but sometimes they came in to help their colleague with an exercise. They presented ideas but always asked questions and encouraged discussions, for example they often asked participants if they had anything to add after an exercise. We also worked with ‘documenters’ and interpreters to make sure that all the discussions, disagreements and reactions were documented well. For SAP, Mr Isaac Mwakilima (Markets Development Officer SAP) documented and Ms Deophister Kakungu (Agricultural Assistant of the Ministry of Agriculture and Livestock) translated the discussions for me to take notes and add probing questions. For the Heifer RCAs, Mrs Joyce Phiri (Programme Manager Heifer), Ms Mwape Anita (Agricultural Assistant) and Ms Doris Siankwilimba (Field Coordinator Heifer) helped facilitating, documenting and translating. Especially, during the one-day recall exercise and when we split up participants in groups the ‘documenter’ and interpreter came in to assist the facilitators. The Heifer facilitation team was also involved in the logistics and planning of the RCAs. For the SAP RCAs there was additional support from Mrs Mpenza Mwanza (Programme Director SAP), Mr Jones Chitondo (Programme Officer, SAP), Mr Nkonge Sydney (Field Officer SAP), Mr Felix Sikana (Administrative Officer SAP) and Mr Kakoma Mathews Ffield Officer SAP). During the discussions, I transcribed what was said immediately. When the group was divided I asked facilitators to take notes and typed them subsequently.
18
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Training We had a two-days combined training on the RCA tools with staff from Oxfam (Ms Lomthunzi Jere), SAP (Mr Jones Chitondo, Mr Isaac Mwakilima, Mr Nkonge Sydney, Heifer (Mrs Joyce Phiri, Ms Emelda Nanyangwe, Ms Doris Siankwilimba) and the facilitators working for the Ministry of Community Development (Ms Evelyn Chanda, Mr Nicholas Chama, Mr Alfred Zimba), the Ministry of Agriculture (Ms Deophister Kakungu, Ms Mwape Anita) and the Kitwe District Land Alliance (Ms Kunda Jesinta). The logistics for the training were kindly organised by SAP staff and the training was held in Kitwe in the hired board room of the local NGO Children in Distress (CINDI). After introductions, we brainstormed what care work was in groups of two. Afterwards, I gave a presentation on debates and concepts related to care work, explaining types of care work, reasons for addressing care work, the WE Care project, the RCA exercises and experiences from other countries. Subsequently, participants entered the ‘RCA competition’. In teams of two (with someone they did not know) they prepared one exercise on the first and another one on the second day, using the general RCA guidelines and toolbox and Zambia specific guidelines. After preparations, each group facilitated their exercises with the rest of the group as participants. Participants adapted the tools while practicing them and the discussions were very interesting and insightful. In the end we ranked each group’s performance and shared the ‘RCA prize’. After the first three RCAs with SAP, we held a recap training with Heifer staff. After a short introductory presentation, participants each picked two ‘exercises cards’ that summarised the main steps for an exercise. Participants had some time to prepare and then presented each exercise in 10-15 min. After clarifying questions and making further adjustments to the exercises, we had an RCA quiz. The quiz included six multiple choice questions about the RCA and care work more generally. Briefings and feedback After the training days and after each RCA we had a brief feedback session discussing what went well and what did not. This was useful to decide on the tools for the next day and to adapt exercises. For example, we decided to go through each hour of the one-day recall as a group rather than leaving the participants to fill in the table on their own. Ethical considerations Throughout the research the priority was always to protect the physical, social and psychological well-being of the participants and to respect their rights, interests, sensitivities and privacy. We asked participants for consent to take photos and to write a report about the findings. Participant anonymity was strictly maintained and we secured the physical notes and photos. Limitations We made an effort not to impose definitions and assumptions, for example asking participants what they thought was care work rather than showing the ‘global care categories’. However, the presence of several NGO workers might have pushed participants to express positive views of the project, for examples participants repeatedly said how Heifer/SAP have brought them ‘knowledge’
19
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
and improved their lives and they were reluctant to say that they did not have time for project activities. Previous trainings might also have shaped participants’ answers. Most participants had received a ‘gender training’ before and it sometimes seemed like they were repeating messages from previous training exercises, for example saying ‘change starts with us’ or ‘we have to share tasks’. Group dynamics between men and women, husbands and wives and community members who knew each other might also have shaped participants’ answers. We are aware that not only the research questions and concepts but also the approaches and methodologies we used are products of interactions between personal attributes and current discourses. Although we made an effort to adapt the tools to the local context, using tools developed at a ‘global level’ and working with a consultant from Germany/England with little knowledge of the Zambian context might have made the tools and findings less locally relevant. Emelda Nanyangwe leading the introduction in RCA 4
Jesinta explaining the care diamond in RCA 3
20
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
PART 3
FINDINGS
Women and men in RCA 6 discussing state level solutions
21
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
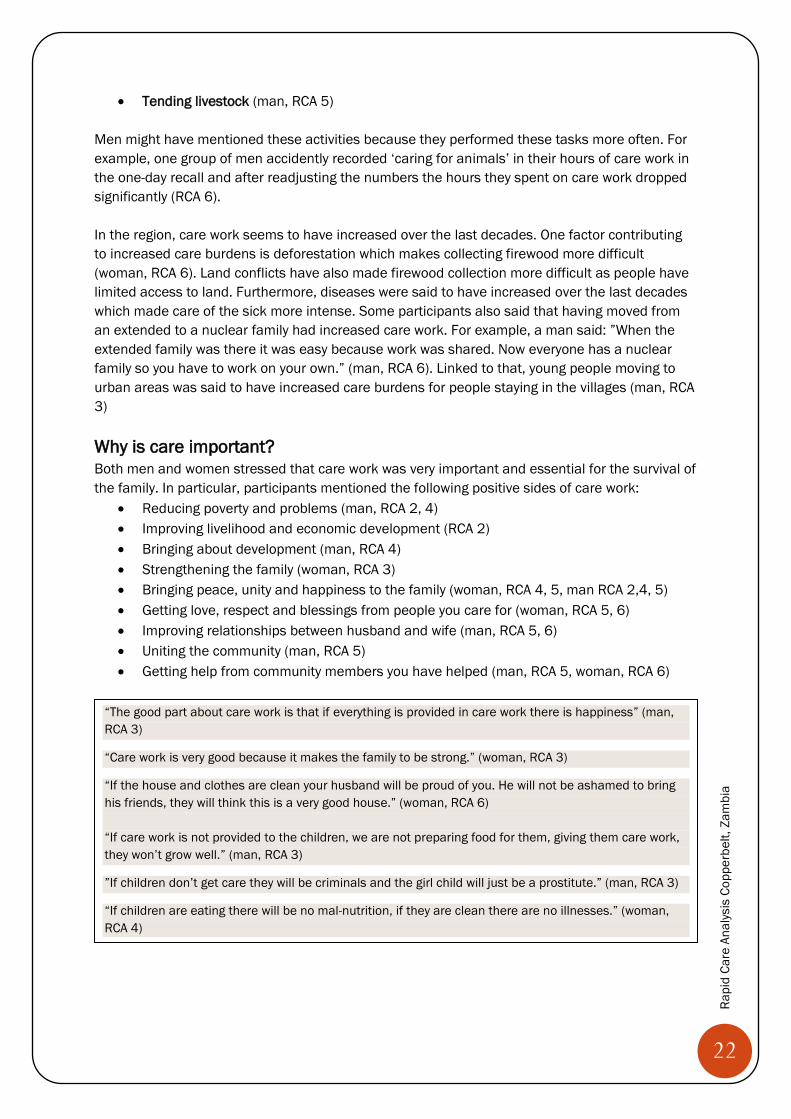
What is care work? There were several translations for ‘care work’ in the local language Bemba (e.g. ‘ukkusunga’, ‘ukusakamana’, ‘ukutangata’, ‘ukubaka’). Participants agreed that the best translation was ‘ukusakamana’ which means caring for or being concerned about something. Some people understood care as something physical (man, RCA 2), relational (man, RCA 2), as “keeping something nicely” (man, RCA 3) or “keeping something in mind” (woman, RCA 3). Two women and one man said that care work was only “small” compared to men’s “heavy work” (RCA 2, 5) but usually people seemed to agree that care work was tiring and time-consuming. When we asked for examples of care work, it was usually women speaking up. They mentioned activities from all the ‘global care categories’:
x Fetching water (women RCA 1, 3, 4, 5) x Fetching firewood (man, RCA 4) x Meal preparation (woman, RCA 1, 2, 4, 5), including “looking for relish (woman, RCA 1)
and “preparing food and keeping food security “ (woman, RCA 1). x Cleaning the house (woman, RCA 1, 3, 5), including “making sure that you have a toilet to
maintain a clean surrounding” (woman, RCA 4) x Washing clothes (woman, RCA 1, 2) x Child care, including “making sure they look nice” (woman, RCA 2), “planning or making
sure children go to school” (woman, RCA 2,4), “being concerned about your children’s health” (woman, RCA 4), “bathing children” (woman, RCA 4,5), “taking children to school” (woman, RCA 4), teaching children “how to cultivate” (woman, RCA 5) and “washing for the children” (man, RCA 1, woman, RCA 2).
x Care of community members and sick/elderly, including “caring for the sick” (woman, RCA 2) or “visiting the sick“ (woman, RCA 5), “caring for neighbours” (woman, RCA 1), “weeding or cultivating for sick neighbours” (woman, RCA 5), “washing for a sick neighbour” and “massage her back” (woman, RCA 4), “bathing the elderly” (woman, RCA 1), “caring for the community or doing volunteering work” (woman, RCA 2), “giving a hand to repair a neighbour’s house” (man, RCA 3)
On top of that, women said that the following activities were also care work:
x “Going to the bed room”, “taking care of the husband at night” (woman, RCA 1) or “looking after the husband” (woman, RCA 4)
x “Checking if everyone (in the family) is okay” (woman, RCA 3) x “Being concerned about your soya production” (woman, RCA 4) x “Washing one’s face” (woman, RCA 5)
Interestingly men often said that activities were care work that were not part of the ‘global care categories’:
x Supervision, including “supervising that children go to school” (man, RCA 1) x Giving instructions, including giving “instructions so that things work” (man, RCA 1) and
telling “the children to look after the things we are keeping” (man, RCA 3) x Planning, including planning on “how to keep myself, my children” (man, RCA 1) x Providing items or money, including food, clothes, solar lamps and charcoal (man RCA 2,
3, 4), x Security and “ensuring peace” (man, RCA 4) x Cultivation (man, RCA 1,3) or taking “produce to sell to the market” (man, RCA 1)
22
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
x Tending livestock (man, RCA 5) Men might have mentioned these activities because they performed these tasks more often. For example, one group of men accidently recorded ‘caring for animals’ in their hours of care work in the one-day recall and after readjusting the numbers the hours they spent on care work dropped significantly (RCA 6). In the region, care work seems to have increased over the last decades. One factor contributing to increased care burdens is deforestation which makes collecting firewood more difficult (woman, RCA 6). Land conflicts have also made firewood collection more difficult as people have limited access to land. Furthermore, diseases were said to have increased over the last decades which made care of the sick more intense. Some participants also said that having moved from an extended to a nuclear family had increased care work. For example, a man said: ”When the extended family was there it was easy because work was shared. Now everyone has a nuclear family so you have to work on your own.” (man, RCA 6). Linked to that, young people moving to urban areas was said to have increased care burdens for people staying in the villages (man, RCA 3) Why is care important? Both men and women stressed that care work was very important and essential for the survival of the family. In particular, participants mentioned the following positive sides of care work:
x Reducing poverty and problems (man, RCA 2, 4) x Improving livelihood and economic development (RCA 2) x Bringing about development (man, RCA 4) x Strengthening the family (woman, RCA 3) x Bringing peace, unity and happiness to the family (woman, RCA 4, 5, man RCA 2,4, 5) x Getting love, respect and blessings from people you care for (woman, RCA 5, 6) x Improving relationships between husband and wife (man, RCA 5, 6) x Uniting the community (man, RCA 5) x Getting help from community members you have helped (man, RCA 5, woman, RCA 6)
Who does what?
“The good part about care work is that if everything is provided in care work there is happiness” (man, RCA 3)
“Care work is very good because it makes the family to be strong.” (woman, RCA 3)
“If the house and clothes are clean your husband will be proud of you. He will not be ashamed to bring his friends, they will think this is a very good house.” (woman, RCA 6) “If care work is not provided to the children, we are not preparing food for them, giving them care work, they won’t grow well.” (man, RCA 3)
”If children don’t get care they will be criminals and the girl child will just be a prostitute.” (man, RCA 3)
“If children are eating there will be no mal-nutrition, if they are clean there are no illnesses.” (woman, RCA 4)
23
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
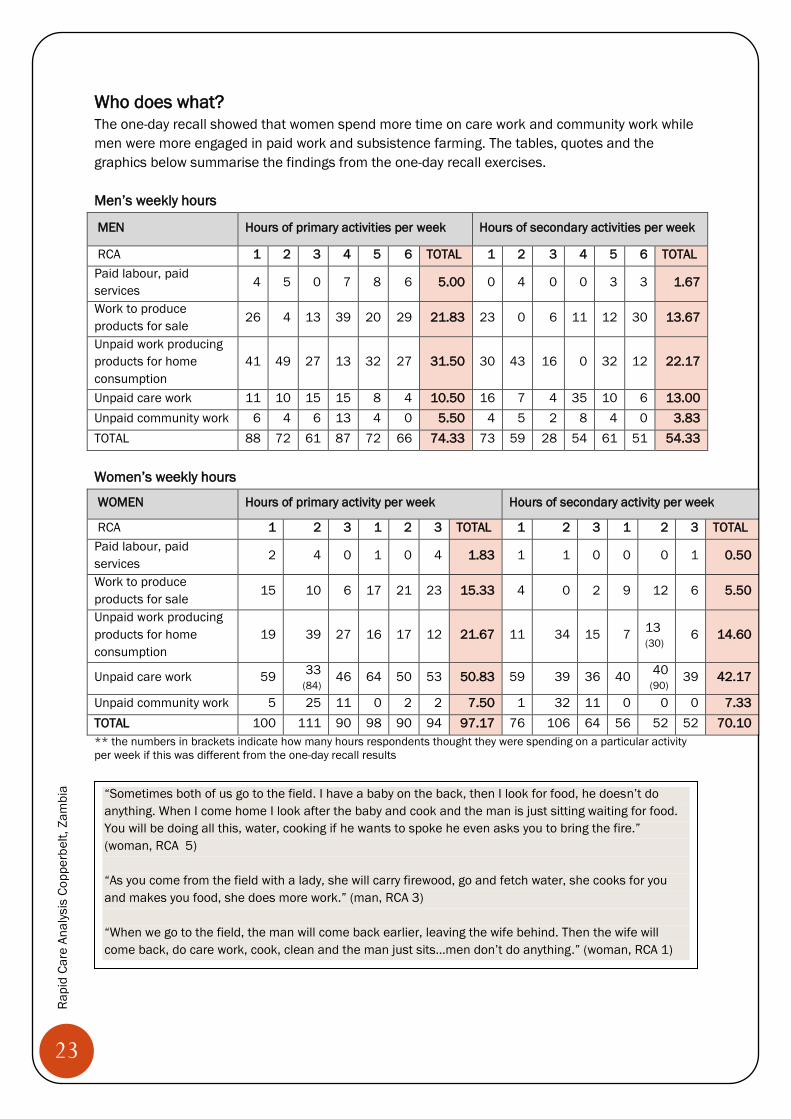
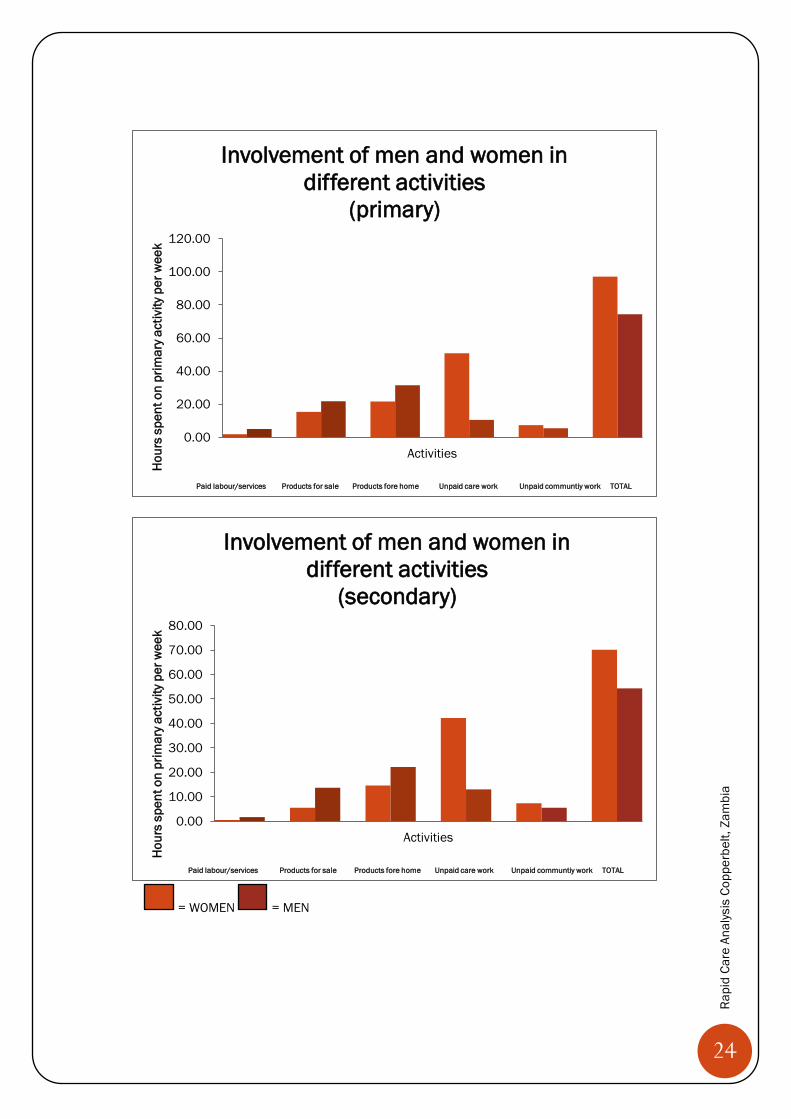
Who does what? The one-day recall showed that women spend more time on care work and community work while men were more engaged in paid work and subsistence farming. The tables, quotes and the graphics below summarise the findings from the one-day recall exercises. Men’s weekly hours
MEN Hours of primary activities per week Hours of secondary activities per week
RCA 1 2 3 4 5 6 TOTAL 1 2 3 4 5 6 TOTAL Paid labour, paid services
4 5 0 7 8 6 5.00 0 4 0 0 3 3 1.67
Work to produce products for sale
26 4 13 39 20 29 21.83 23 0 6 11 12 30 13.67
Unpaid work producing products for home consumption
41 49 27 13 32 27 31.50 30 43 16 0 32 12 22.17
Unpaid care work 11 10 15 15 8 4 10.50 16 7 4 35 10 6 13.00 Unpaid community work 6 4 6 13 4 0 5.50 4 5 2 8 4 0 3.83 TOTAL 88 72 61 87 72 66 74.33 73 59 28 54 61 51 54.33 Women’s weekly hours
WOMEN Hours of primary activity per week Hours of secondary activity per week
RCA 1 2 3 1 2 3 TOTAL 1 2 3 1 2 3 TOTAL Paid labour, paid services
2 4 0 1 0 4 1.83 1 1 0 0 0 1 0.50
Work to produce products for sale
15 10 6 17 21 23 15.33 4 0 2 9 12 6 5.50
Unpaid work producing products for home consumption
19 39 27 16 17 12 21.67 11 34 15 7 13 (30) 6 14.60
Unpaid care work 59 33 (84) 46 64 50 53 50.83 59 39 36 40 40
(90) 39 42.17
Unpaid community work 5 25 11 0 2 2 7.50 1 32 11 0 0 0 7.33 TOTAL 100 111 90 98 90 94 97.17 76 106 64 56 52 52 70.10 ** the numbers in brackets indicate how many hours respondents thought they were spending on a particular activity per week if this was different from the one-day recall results
“Sometimes both of us go to the field. I have a baby on the back, then I look for food, he doesn’t do anything. When I come home I look after the baby and cook and the man is just sitting waiting for food. You will be doing all this, water, cooking if he wants to spoke he even asks you to bring the fire.” (woman, RCA 5) “As you come from the field with a lady, she will carry firewood, go and fetch water, she cooks for you and makes you food, she does more work.” (man, RCA 3) “When we go to the field, the man will come back earlier, leaving the wife behind. Then the wife will come back, do care work, cook, clean and the man just sits…men don’t do anything.” (woman, RCA 1)
24
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
= WOMEN = MEN
0.00
20.00
40.00
60.00
80.00
100.00
120.00
Activities
Hou
rs s
pent
on
prim
ary a
ctiv
ity p
er w
eek
Involvement of men and women in different activities
(primary)
Paid labour/services Products for sale Products fore home Unpaid care work Unpaid communtiy work TOTAL
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
Activities
Hou
rs s
pent
on
prim
ary a
ctiv
ity p
er w
eek
Involvement of men and women in different activities
(secondary)
Paid labour/services Products for sale Products fore home Unpaid care work Unpaid communtiy work TOTAL
25
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Discussions among women We discussed the results of the one-day recall first separately among women and men and then as a group. When discussing the weekly averages for each activity women talked passionately, loudly and often at the same time. They often said that they spent even more time on care work than captured by the one-day recall. One woman said she spent 200 hours a week on care work (RCA 1) but usually women agreed that they spent about 12 hours a day (84 hours a week ) on care work (RCA 1, 2, 3). Women also agreed that they engaged in more total work than men. They often concluded that care work prevented them from engaging in work “that brings money” (woman, RCA 5) and that they had to start spending more time on productive work (RCA 6). When the one-day recall was about a Sunday, women said that they usually spent more time on selling products (RCA 3).
Discussions among men Men were even more sceptical of the results of the one-day recall. Some criticised that the exercise was only done for one day (RCA 4) and that the distinction between products for sale and home consumption was not clear (RCA 4, 6). Others said that they actually spent more time on community work (RCA 6) or less time on care work (RCA 1). Some men concluded that they produced too many products for home consumption rather than for sale: “This is why we don’t progress in our business because we are not producing products for sale” (man, RCA 6). Men sometimes laughed about the fact that they only spent a few hours on care work (RCA 1). Participants often agreed that men rested more than women. Who does what care work? Everyone agreed that women spent more time on care work. In the ‘care circle exercise’, women mentioned many more people they cared for. Women said they cared on a daily basis for their husbands (RCA 1,4), other family members (RCA 1, 4), children (RCA 4), grandchildren (RCA 4), aunties, neighbours, visitors, in-laws (RCA 4). They said that they cared monthly for elderly, orphans, widows and the community, especially through helping at funerals (RCA 1) and yearly for church members, producer group members and Heifer staff (RCA 4). Men had difficulties finding people they cared for which made women laugh and ‘attack’ men jokingly. For example, some men said that they cared for their wives and children on a daily basis
“It hurts that all the things that we have been doing is just care work.” (woman, RCA 5) “This is why we women in Zambia we don’t progress. Because we spend most of the time on care work, we cannot do the work that makes us progress and this is also causing us dying early” (woman, RCA 5) “We are vulnerable, we concentrate so much on care work and not on the work that brings us money.” (woman, RCA 6) “Because we are spending so much time on care work there will be no development in the home.” (woman, RCA 6)
26
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
by providing money or accommodation (man, RCA 4) and women loudly contradicted: ”This is not care work, you failed!! The men have failed miserably they don’t do any care work!” Some men said that they took children to school or the clinic (man, RCA 1), collected firewood (man, RCA 1), collected food (man, RCA 1), fetched water (man, RCA 1), swept (man, RCA 1) or helped children with homework (old man, RCA 1). However, women seemed to disagree with men saying they did care work, often shaking their heads, laughing, asking them “really?” or saying loudly: “men don’t do care work!” (woman, RCA 1) or “ah, you don’t!” (woman, RCA 1). Men sometimes contradicted, shouting loudly: “we do!” but some men also agreed that they did not do care work, for example: “men don’t give care work to the family they leave everything to women.” (man, RCA 1). In RCA 1 the discussions got so heated that one man said: “you are intimidating us!”. Only few women said that their husbands helped them with care work. Julia and Samuel2 told everyone that they were working together. When Julia said: “My husband has prepared some meals, firewood, collecting water” the group starts applauding and Samuel added: “My wife has given me respect this is why I have helped her with care work. She is a good woman.”. Julia is a leader in several groups and Samuel has received gender training and repeatedly said that he loved his wife (RCA 2). Men often said that women would not want them to help with care work and some also said that they would be worried that their wives would start taking advantage of them if they started helping with care work.
Women usually disagreed saying that they would want their husbands to help them with care work, for example a woman in RCA 2 said: “Men were saying women don’t want to be helped, but we want them to help us!”. It seemed like childcare was the care activity that men were least likely to get engaged in. Cooking was also considered more difficult for men to do than other activities, such as collecting water or firewood or washing (RCA 2, 6).
2 The names have been changed
“Women themselves refuse to be helped. They say ‘no my friends will be laughing at me’.” (man RCA 2) “Even when you do care work, she will l refuse: ‘no a man is not supposed to be in the kitchen’ and if you force her she will say ‘you want to get my responsibility as a woman’.”(man RCA 2) “ Women have a problem. If you try to help them they will take advantage of you.” (man, RCA 4) “If you help women they will start bragging to our neighbours how their husbands help them.” (man, RCA 6). “If we wash and cook, the woman lose the respect for you.” man, RCA 2)
27
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
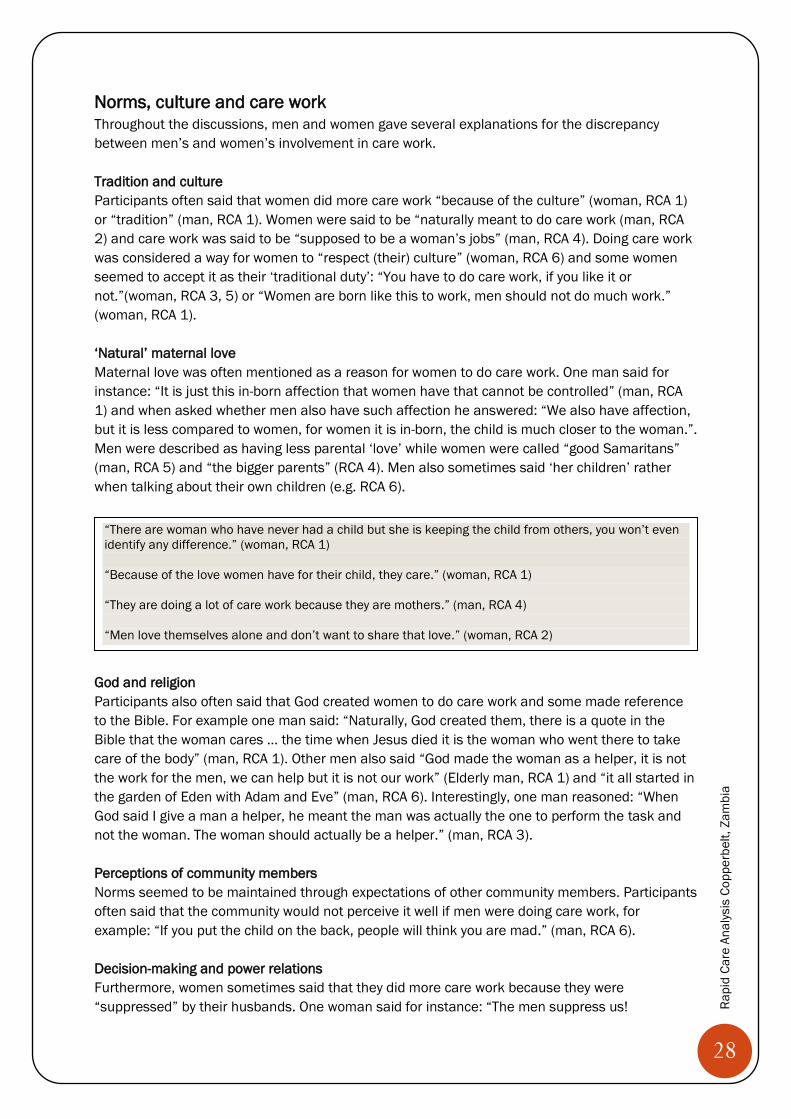
Results from the one-day recall for men, RCA Care circle for women, RCA 1
“Child care is very difficult and the kids enjoy with their mothers.” (man, RCA 6) “For the men usually when the babies are very young they say ‘I don’t want to carry the baby I don’t want to drop it’ and when the babies are older they say ‘I don’t want to be disturbed when I am listening to the news.’” (woman, RCA 5) “Imagine that this woman has a baby, there is no way she can tell me to wash the nappies.” (man, RCA 6) “When it comes to meal preparation, it is very difficult, but washing you can help her.” (man, RCA 2)
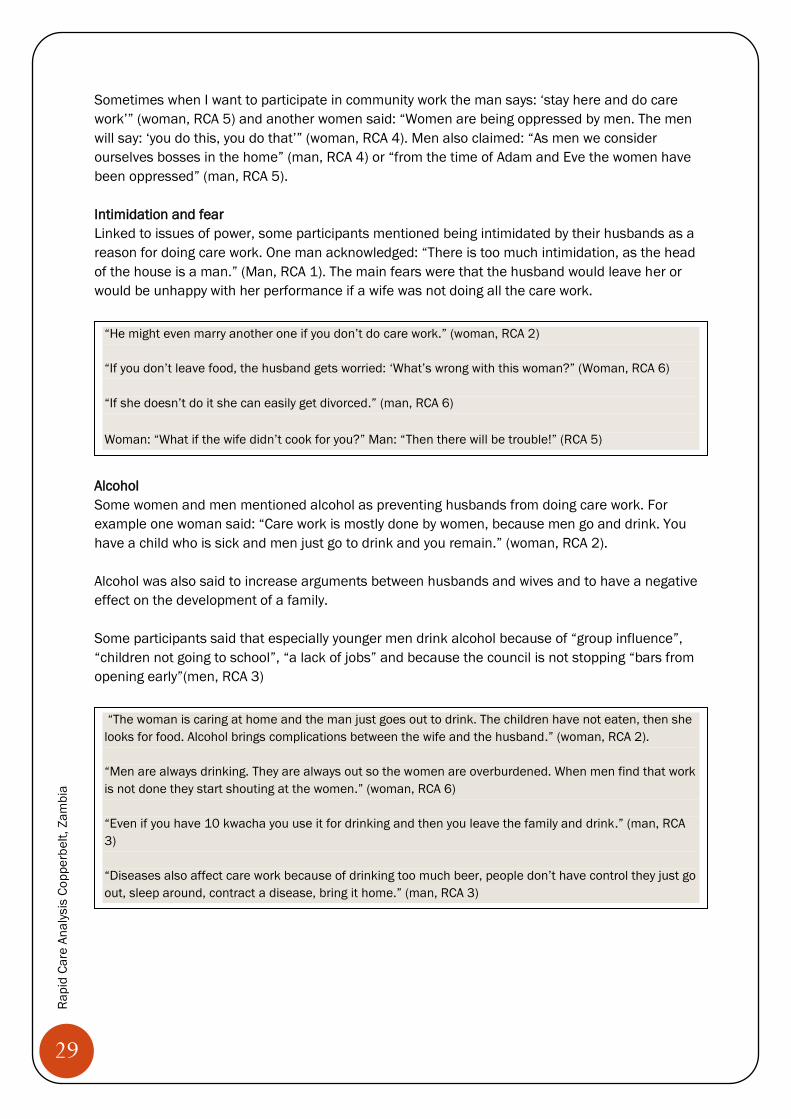
Men in RCA 3 discussing the one-day recall
28
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Norms, culture and care work Throughout the discussions, men and women gave several explanations for the discrepancy between men’s and women’s involvement in care work. Tradition and culture Participants often said that women did more care work “because of the culture” (woman, RCA 1) or “tradition” (man, RCA 1). Women were said to be “naturally meant to do care work (man, RCA 2) and care work was said to be “supposed to be a woman’s jobs” (man, RCA 4). Doing care work was considered a way for women to “respect (their) culture” (woman, RCA 6) and some women seemed to accept it as their ‘traditional duty’: “You have to do care work, if you like it or not.”(woman, RCA 3, 5) or “Women are born like this to work, men should not do much work.” (woman, RCA 1). ‘Natural’ maternal love Maternal love was often mentioned as a reason for women to do care work. One man said for instance: “It is just this in-born affection that women have that cannot be controlled” (man, RCA 1) and when asked whether men also have such affection he answered: “We also have affection, but it is less compared to women, for women it is in-born, the child is much closer to the woman.”. Men were described as having less parental ‘love’ while women were called “good Samaritans” (man, RCA 5) and “the bigger parents” (RCA 4). Men also sometimes said ‘her children’ rather when talking about their own children (e.g. RCA 6).
God and religion Participants also often said that God created women to do care work and some made reference to the Bible. For example one man said: “Naturally, God created them, there is a quote in the Bible that the woman cares … the time when Jesus died it is the woman who went there to take care of the body” (man, RCA 1). Other men also said “God made the woman as a helper, it is not the work for the men, we can help but it is not our work” (Elderly man, RCA 1) and “it all started in the garden of Eden with Adam and Eve” (man, RCA 6). Interestingly, one man reasoned: “When God said I give a man a helper, he meant the man was actually the one to perform the task and not the woman. The woman should actually be a helper.” (man, RCA 3). Perceptions of community members Norms seemed to be maintained through expectations of other community members. Participants often said that the community would not perceive it well if men were doing care work, for example: “If you put the child on the back, people will think you are mad.” (man, RCA 6). Decision-making and power relations Furthermore, women sometimes said that they did more care work because they were “suppressed” by their husbands. One woman said for instance: “The men suppress us!
“There are woman who have never had a child but she is keeping the child from others, you won’t even identify any difference.” (woman, RCA 1) “Because of the love women have for their child, they care.” (woman, RCA 1) “They are doing a lot of care work because they are mothers.” (man, RCA 4) “Men love themselves alone and don’t want to share that love.” (woman, RCA 2)
29
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Sometimes when I want to participate in community work the man says: ‘stay here and do care work’” (woman, RCA 5) and another women said: “Women are being oppressed by men. The men will say: ‘you do this, you do that’” (woman, RCA 4). Men also claimed: “As men we consider ourselves bosses in the home” (man, RCA 4) or “from the time of Adam and Eve the women have been oppressed” (man, RCA 5). Intimidation and fear Linked to issues of power, some participants mentioned being intimidated by their husbands as a reason for doing care work. One man acknowledged: “There is too much intimidation, as the head of the house is a man.” (Man, RCA 1). The main fears were that the husband would leave her or would be unhappy with her performance if a wife was not doing all the care work.
Alcohol Some women and men mentioned alcohol as preventing husbands from doing care work. For example one woman said: “Care work is mostly done by women, because men go and drink. You have a child who is sick and men just go to drink and you remain.” (woman, RCA 2). Alcohol was also said to increase arguments between husbands and wives and to have a negative effect on the development of a family. Some participants said that especially younger men drink alcohol because of “group influence”, “children not going to school”, “a lack of jobs” and because the council is not stopping “bars from opening early”(men, RCA 3)
“He might even marry another one if you don’t do care work.” (woman, RCA 2) “If you don’t leave food, the husband gets worried: ‘What’s wrong with this woman?” (Woman, RCA 6) “If she doesn’t do it she can easily get divorced.” (man, RCA 6) Woman: “What if the wife didn’t cook for you?” Man: “Then there will be trouble!” (RCA 5)
“The woman is caring at home and the man just goes out to drink. The children have not eaten, then she looks for food. Alcohol brings complications between the wife and the husband.” (woman, RCA 2). “Men are always drinking. They are always out so the women are overburdened. When men find that work is not done they start shouting at the women.” (woman, RCA 6) “Even if you have 10 kwacha you use it for drinking and then you leave the family and drink.” (man, RCA 3) “Diseases also affect care work because of drinking too much beer, people don’t have control they just go out, sleep around, contract a disease, bring it home.” (man, RCA 3)
30
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
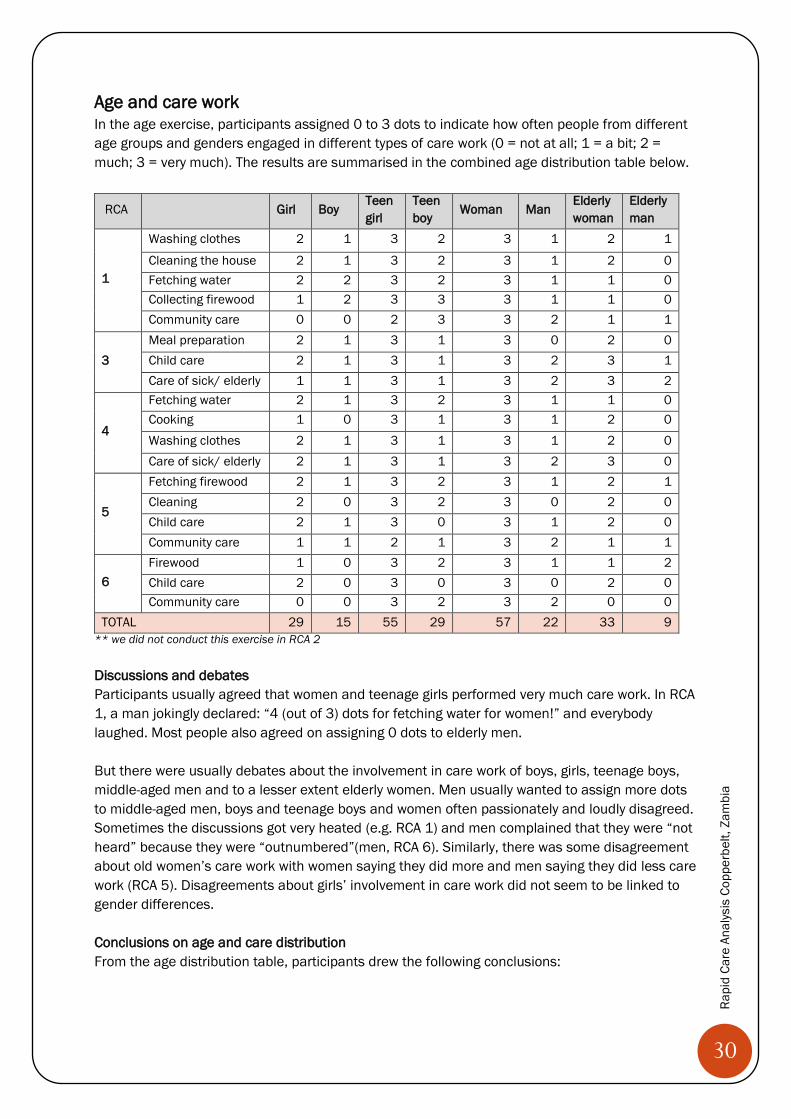
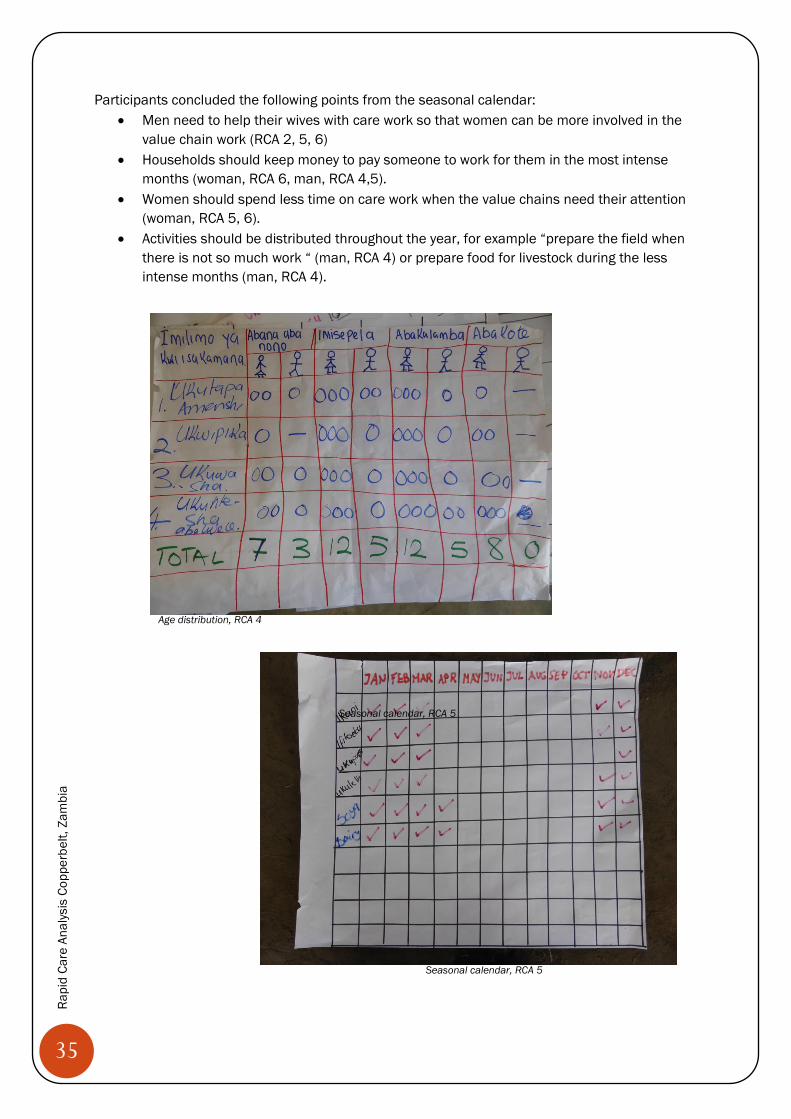
Age and care work In the age exercise, participants assigned 0 to 3 dots to indicate how often people from different age groups and genders engaged in different types of care work (0 = not at all; 1 = a bit; 2 = much; 3 = very much). The results are summarised in the combined age distribution table below.
RCA Girl Boy Teen girl
Teen boy
Woman Man Elderly woman
Elderly man
1
Washing clothes 2 1 3 2 3 1 2 1
Cleaning the house 2 1 3 2 3 1 2 0 Fetching water 2 2 3 2 3 1 1 0 Collecting firewood 1 2 3 3 3 1 1 0 Community care 0 0 2 3 3 2 1 1
3 Meal preparation 2 1 3 1 3 0 2 0 Child care 2 1 3 1 3 2 3 1 Care of sick/ elderly 1 1 3 1 3 2 3 2
4
Fetching water 2 1 3 2 3 1 1 0 Cooking 1 0 3 1 3 1 2 0 Washing clothes 2 1 3 1 3 1 2 0 Care of sick/ elderly 2 1 3 1 3 2 3 0
5
Fetching firewood 2 1 3 2 3 1 2 1 Cleaning 2 0 3 2 3 0 2 0 Child care 2 1 3 0 3 1 2 0 Community care 1 1 2 1 3 2 1 1
6 Firewood 1 0 3 2 3 1 1 2 Child care 2 0 3 0 3 0 2 0 Community care 0 0 3 2 3 2 0 0
TOTAL 29 15 55 29 57 22 33 9 ** we did not conduct this exercise in RCA 2 Discussions and debates Participants usually agreed that women and teenage girls performed very much care work. In RCA 1, a man jokingly declared: “4 (out of 3) dots for fetching water for women!” and everybody laughed. Most people also agreed on assigning 0 dots to elderly men. But there were usually debates about the involvement in care work of boys, girls, teenage boys, middle-aged men and to a lesser extent elderly women. Men usually wanted to assign more dots to middle-aged men, boys and teenage boys and women often passionately and loudly disagreed. Sometimes the discussions got very heated (e.g. RCA 1) and men complained that they were “not heard” because they were “outnumbered”(men, RCA 6). Similarly, there was some disagreement about old women’s care work with women saying they did more and men saying they did less care work (RCA 5). Disagreements about girls’ involvement in care work did not seem to be linked to gender differences. Conclusions on age and care distribution From the age distribution table, participants drew the following conclusions:
31
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
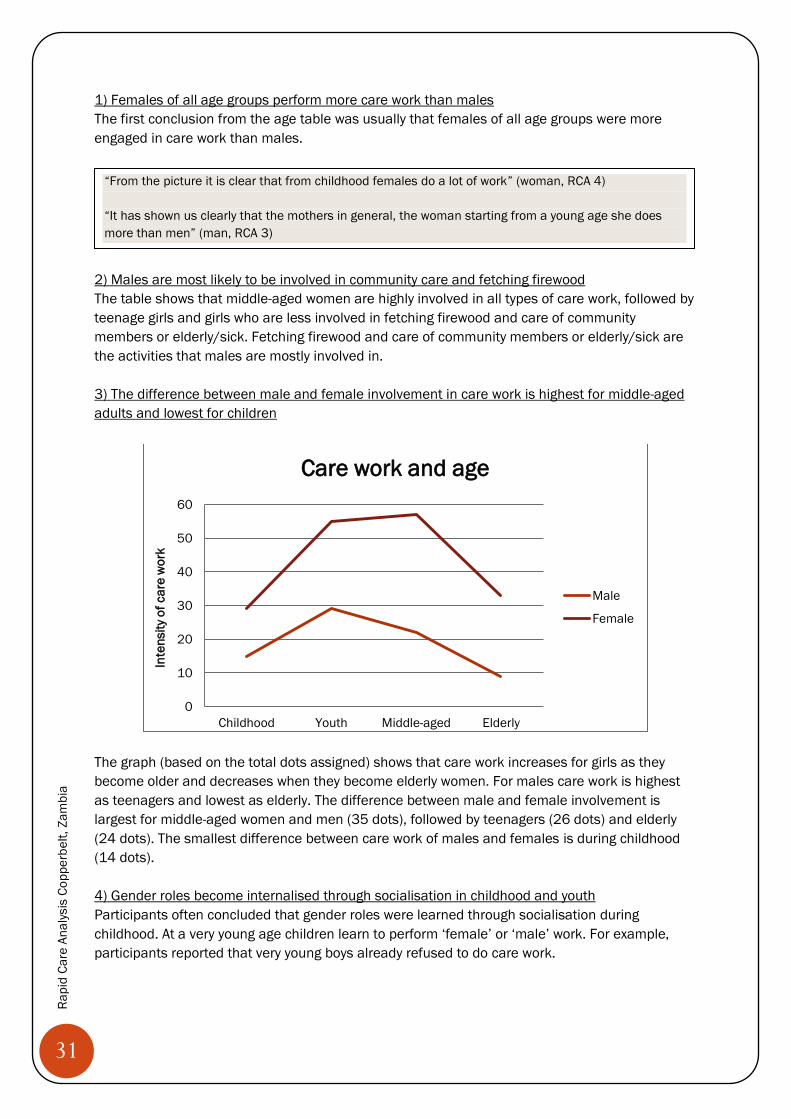
1) Females of all age groups perform more care work than males The first conclusion from the age table was usually that females of all age groups were more engaged in care work than males.
2) Males are most likely to be involved in community care and fetching firewood The table shows that middle-aged women are highly involved in all types of care work, followed by teenage girls and girls who are less involved in fetching firewood and care of community members or elderly/sick. Fetching firewood and care of community members or elderly/sick are the activities that males are mostly involved in. 3) The difference between male and female involvement in care work is highest for middle-aged adults and lowest for children
The graph (based on the total dots assigned) shows that care work increases for girls as they become older and decreases when they become elderly women. For males care work is highest as teenagers and lowest as elderly. The difference between male and female involvement is largest for middle-aged women and men (35 dots), followed by teenagers (26 dots) and elderly (24 dots). The smallest difference between care work of males and females is during childhood (14 dots). 4) Gender roles become internalised through socialisation in childhood and youth Participants often concluded that gender roles were learned through socialisation during childhood. At a very young age children learn to perform ‘female’ or ‘male’ work. For example, participants reported that very young boys already refused to do care work.
0
10
20
30
40
50
60
Childhood Youth Middle-aged Elderly
Inte
nsity
of c
are
wor
k
Care work and age
Male
Female
“From the picture it is clear that from childhood females do a lot of work” (woman, RCA 4) “It has shown us clearly that the mothers in general, the woman starting from a young age she does more than men” (man, RCA 3)
32
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
It became clear that both men and women played a role in socialising their children and in telling them to share care work.
5) The school performance of girls and female teenagers is affected by care work Participants always mentioned girls’ workloads as a critical point affecting their school performance. Especially men were very passionate about changing work patterns so that their daughters could do better at school.
“You find that a girl child will be making toys, which shows that she is prepared to give care work to the family, unlike a baby boy who is making other things.” (man, RCA 1) “When you are a young girl you are socialised to look after the home. When you are a young boy you are socialised to go out and look for things.” (man, RCA 4) “My son, if the mother tells him to wash plates he runs away because he know that his sister will do it.” (man, RCA 6) “We ask boys but they refuse to fetch water.” (woman, RCA 4)
“The women have a problem because even from an early age they just involve the girls and not the boys. Women should make sure that boys and girls are involved at the same time.” (man, RCA 6). “I collect vegetables, leave them, tell the girl child ‘do this, don’t go to school’.” (woman, RCA 1) “Parents stop boys to do care work, washing clothes.” (woman, RCA 1) “The burden of educating the children, telling them about care work is not just for women but for both husbands and wives.” (woman, RCA 6)
“Because of the girl child over-working she does not have time to study, so performance is going down.” (man, RCA 1) “It affects the girls, she fetches water, she goes to school. When she comes home, you tell her to go get tomatoes. She does everything. She will not remember what she learned at school.” (man, RCA 2) “Because the girls have so much to do the boys will perform better at school. Even if she is in class she will just think of everything she has to do.” (man, RCA 4) ”From my experience as a teacher between a boy child and a girl child there is a very big difference! The boys attend classes. In a week the girls don’t participate very much at school. If you ask them they say: ‘my mother left and told me to do care work’ … we told the parents to assign less care work to girls and the government also says the girl child should be educated but parents at home make them do all this care work.” (male teacher, RCA 2) “ When I went to Solewezi my cousin has a child, they overload her with work. She had a 50% performance at school. She is not performing well. We should give her a chance to do school work.” (man, RCA 3)
33
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
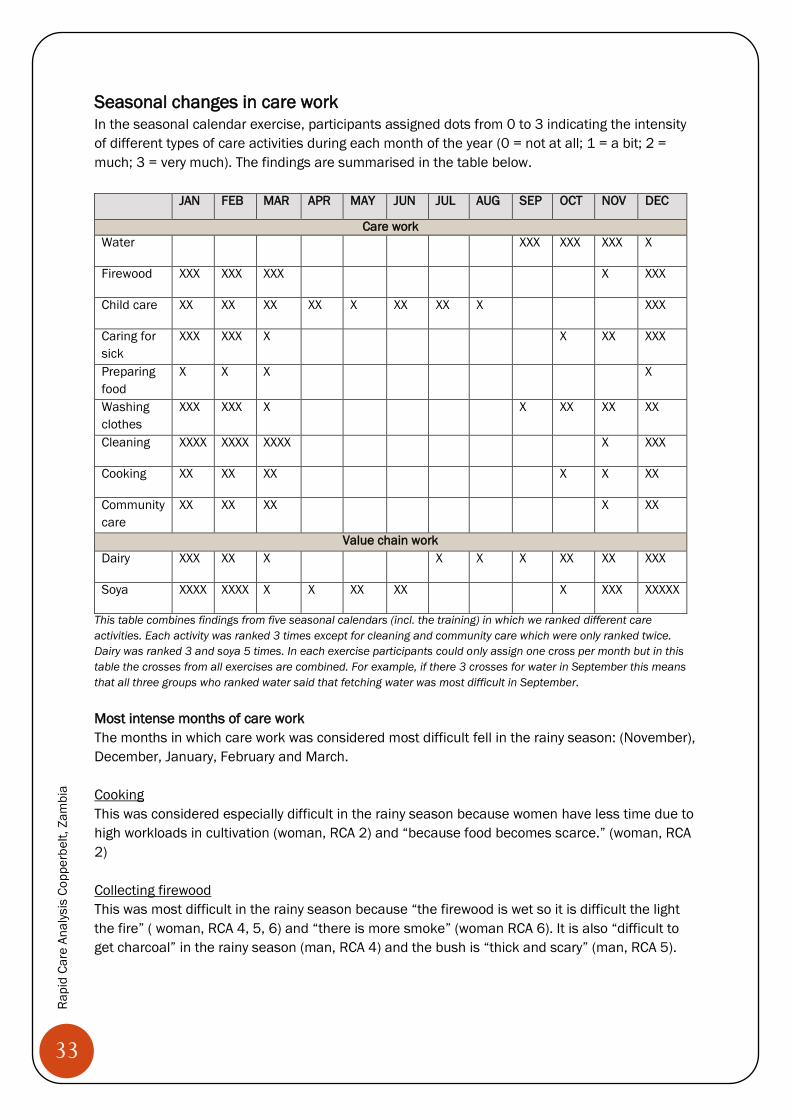
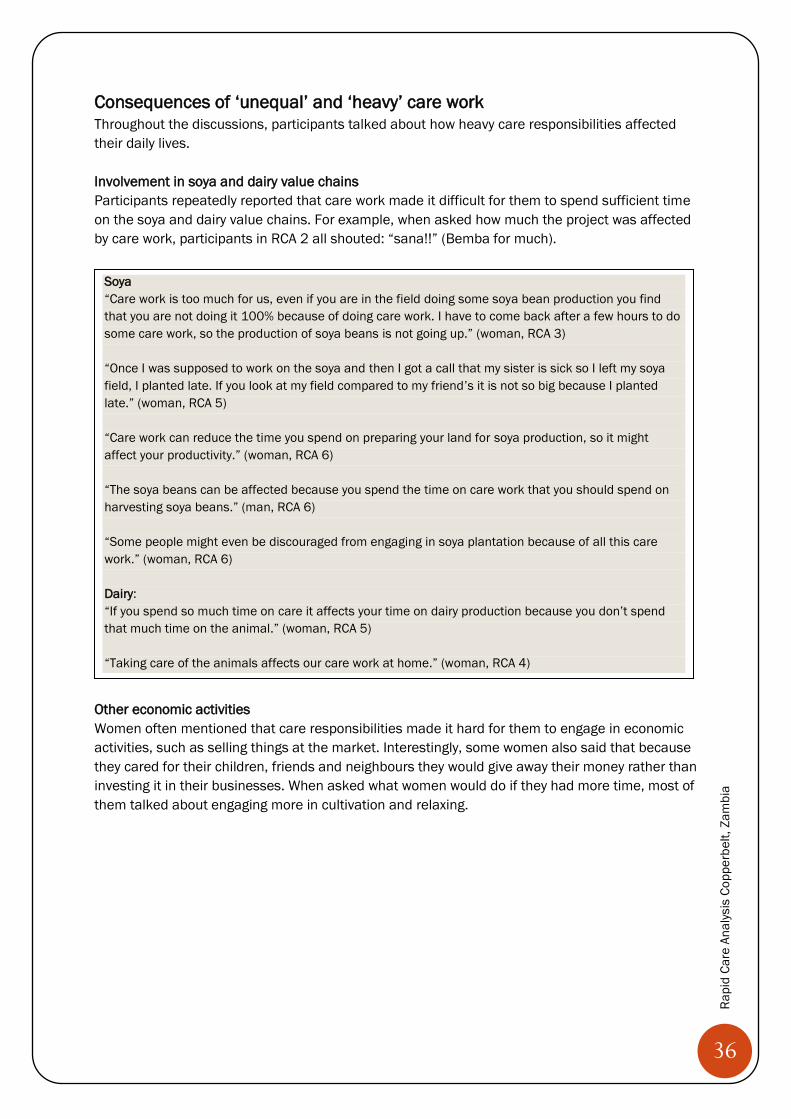
Seasonal changes in care work In the seasonal calendar exercise, participants assigned dots from 0 to 3 indicating the intensity of different types of care activities during each month of the year (0 = not at all; 1 = a bit; 2 = much; 3 = very much). The findings are summarised in the table below.
JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC
Care work Water XXX XXX XXX X
Firewood XXX XXX XXX X XXX
Child care XX XX XX XX X XX XX X XXX
Caring for sick
XXX XXX X X XX XXX
Preparing food
X X X X
Washing clothes
XXX XXX X X XX XX XX
Cleaning XXXX XXXX XXXX X XXX
Cooking XX XX XX X X XX
Community care
XX XX XX X XX
Value chain work Dairy XXX XX X X X X XX XX XXX
Soya XXXX XXXX X X XX XX X XXX XXXXX
This table combines findings from five seasonal calendars (incl. the training) in which we ranked different care activities. Each activity was ranked 3 times except for cleaning and community care which were only ranked twice. Dairy was ranked 3 and soya 5 times. In each exercise participants could only assign one cross per month but in this table the crosses from all exercises are combined. For example, if there 3 crosses for water in September this means that all three groups who ranked water said that fetching water was most difficult in September. Most intense months of care work The months in which care work was considered most difficult fell in the rainy season: (November), December, January, February and March. Cooking This was considered especially difficult in the rainy season because women have less time due to high workloads in cultivation (woman, RCA 2) and “because food becomes scarce.” (woman, RCA 2) Collecting firewood This was most difficult in the rainy season because “the firewood is wet so it is difficult the light the fire” ( woman, RCA 4, 5, 6) and “there is more smoke” (woman RCA 6). It is also “difficult to get charcoal” in the rainy season (man, RCA 4) and the bush is “thick and scary” (man, RCA 5).
34
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Washing clothes This was “most difficult in the rainy season because it is very difficult for clothes to dry” (woman, RCA 2, 4). Cleaning This was most problematic during rainy season because of the rains and mud (woman, RCA 2, 6) and because of having to cut the grass on the compound (man, RCA 4, 5). Cleaning was also said to be especially hard during mango season in September when “you have a lot of mangos and there are a lot of flies and you have to make sure that things are clean.” (woman, RCA 4). Caring for the sick This was said to be most intense in the rainy season because of higher incidents of malaria and water borne diseases (woman, RCA 2, 4). Community care This was also difficult in the rainy season because of too much other work, especially cultivation (man RCA 4, woman RCA 6). Child care This was said to be difficult during school holidays because children would be at home (man, RCA 4). It was also considered problematic during the winter season because children would be inside the kitchen which would increase work for women and the likelihood of children getting burned by the fire (man, RCA 2). Fetching water This was considered most problematic in the dry season because “water levels are very low and most of the wells would have dried up” (woman, RCA 4). This means that people “have to walk a long way to fetch water” (woman, RCA 4). Most intense months of value chain work The value chain work was also most intense during the rainy season. Dairy This was considered particularly difficult in the rainy season because of ticks and flies transmitting diseases (man, RCA 4, 5). In the dry season it was also considered problematic because of having to walk far to get grass for the animals (man, RCA 4). Soya Soya was said to be most intense during preparation of the field (December) planting (February) and harvest (May and June) (woman, RCA 6). Conclusions The seasonal calendar shows that the dairy and soya value chains are at their peak approximately at the same time when care work is also at its peak. This was perceived as an interesting finding for project design.
35
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Participants concluded the following points from the seasonal calendar: x Men need to help their wives with care work so that women can be more involved in the
value chain work (RCA 2, 5, 6) x Households should keep money to pay someone to work for them in the most intense
months (woman, RCA 6, man, RCA 4,5). x Women should spend less time on care work when the value chains need their attention
(woman, RCA 5, 6). x Activities should be distributed throughout the year, for example “prepare the field when
there is not so much work “ (man, RCA 4) or prepare food for livestock during the less intense months (man, RCA 4).
Age distribution, RCA 4
Seasonal calendar, RCA 5
Seasonal calendar, RCA 5
36
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Consequences of ‘unequal’ and ‘heavy’ care work
Throughout the discussions, participants talked about how heavy care responsibilities affected their daily lives. Involvement in soya and dairy value chains Participants repeatedly reported that care work made it difficult for them to spend sufficient time on the soya and dairy value chains. For example, when asked how much the project was affected by care work, participants in RCA 2 all shouted: “sana!!” (Bemba for much).
Other economic activities Women often mentioned that care responsibilities made it hard for them to engage in economic activities, such as selling things at the market. Interestingly, some women also said that because they cared for their children, friends and neighbours they would give away their money rather than investing it in their businesses. When asked what women would do if they had more time, most of them talked about engaging more in cultivation and relaxing.
Soya “Care work is too much for us, even if you are in the field doing some soya bean production you find that you are not doing it 100% because of doing care work. I have to come back after a few hours to do some care work, so the production of soya beans is not going up.” (woman, RCA 3) “Once I was supposed to work on the soya and then I got a call that my sister is sick so I left my soya field, I planted late. If you look at my field compared to my friend’s it is not so big because I planted late.” (woman, RCA 5) “Care work can reduce the time you spend on preparing your land for soya production, so it might affect your productivity.” (woman, RCA 6) “The soya beans can be affected because you spend the time on care work that you should spend on harvesting soya beans.” (man, RCA 6) “Some people might even be discouraged from engaging in soya plantation because of all this care work.” (woman, RCA 6) Dairy: “If you spend so much time on care it affects your time on dairy production because you don’t spend that much time on the animal.” (woman, RCA 5) “Taking care of the animals affects our care work at home.” (woman, RCA 4)
37
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Participation in trainings and producer groups A few participants said that care work affected their participation in trainings and producer group activities because it took up much of their time (woman, RCA 2, 5).
But women also often said that they can do care work and participate in trainings if they plan well (RCA 2, 3, 5). For example, one woman said: “We have to plan. If I know that I have a community programme at 8.00 am I have to get up early to do all the care work before.” (woman, RCA 5) Leadership and community work Participants also sometimes said that it was difficult to balance leadership and care responsibilities.
“In 2010, we had made charcoal and we had 60 bags and then my husband fell sick and the illness was sudden and the husband was sick for 2 months and it was during the rainy season so the charcoal was getting soaked because we didn’t sell the charcoal on time because I was looking after the husband. And when we sold it there was so much charcoal so we didn’t get much money!” (woman, RCA 5) “I had tomatoes in my garden and then my sister fell sick in Chingola and I went to care for her. My husband doesn’t know how to sell tomatoes. He called me to ask because he has never sold things at the market but he didn’t manage. I couldn’t sell the tomatoes and I couldn’t buy another treadle pump from Heifer.” (woman, RCA 5) “We spend most time on care work rather than other things which is holding us back from contributing to development and economic activities.” (woman, RCA 1) “When women go and sell at the market they will buy drinks and food to care for their friends instead of keeping the money and investing in other things.” (woman, RCA 5) “Maybe you have a budget for 200 kwacha to invest in your business but you rather invest in the future of the child by paying school fees or maybe a neighbour tells you that a family member has died, so you give money to the neighbour.” (woman, RCA 5)
“Sometimes there is a training and then there is a funeral in the neighbourhood you rather go to help at the funeral than to the training, also if the child is sick.” (man, RCA 5) “When this lady wanted to come for the meeting this is when the baby pooed so first she had to clean the baby this is why she is late”(man pointing at woman with baby,” RCA 5) “Sometimes this work affects participation in producer groups because women have so much to do and they think people in producer groups are just wasting time.” (man, RCA 5)
“If you are a leader, for instance in a producer group, your care work might be affected because of attending meetings.” (woman, RCA 5) “If for instance a woman wants to participate in community activities and then she also has responsibilities at home, this might be at the same time, so she will be late for the community work because of the care work.” (man, RCA 5) “We fail to do community work because we have a lot of household chores.” (woman, RCA 2)
38
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Health and well-being Women and men often said that care work can have negative effects on the care giver’s health, for example causing pain or physical exhaustion.
On top of these major points, participants said that high care responsibilities could have the following negative consequences:
x Decrease the quality of life (man, RCA 2) x Affect mobility (RCA 2) x Lead to arguments between husband and wife (woman, RCA 5) x Affect children, especially girls (e.g. early marriage, being “dirty”, not having time for
school because of care work) (RCA 2) x Make people who are cared for lazy (man, RCA 4, 5)3 x People might not appreciate your efforts with care work (woman, RCA 5)
Woman and man in RCA 4 during a discussion
3 “It brings about laziness. If you are caring so much for your community members they know that someone is caring for them they just sit back and don’t work, especially the neighbours” (man, RCA 4); “Some people become lazy, if you are looking after people and washing for them it makes them lazy because they know that there is someone washing and looking after them.” (man, RCA 5)
“If care work is only done by one person there is no help it will be very difficult for her to do care work. She can even get sick, it can even lead to death.” (man, RCA 3) “Care brings about illnesses. If you are working too much the body will get tired.” (man, RCA 4) “Because most of these things are done by women maybe her fingers are hurt from washing, she doesn’t even have time to rest.” (man, RCA 6) “The chest can also pain from care work, like fetching water, it is making our life spam short, washing, cleaning the house, now I developed a chest pain. I already got 7 injections!” (woman, RCA 5)
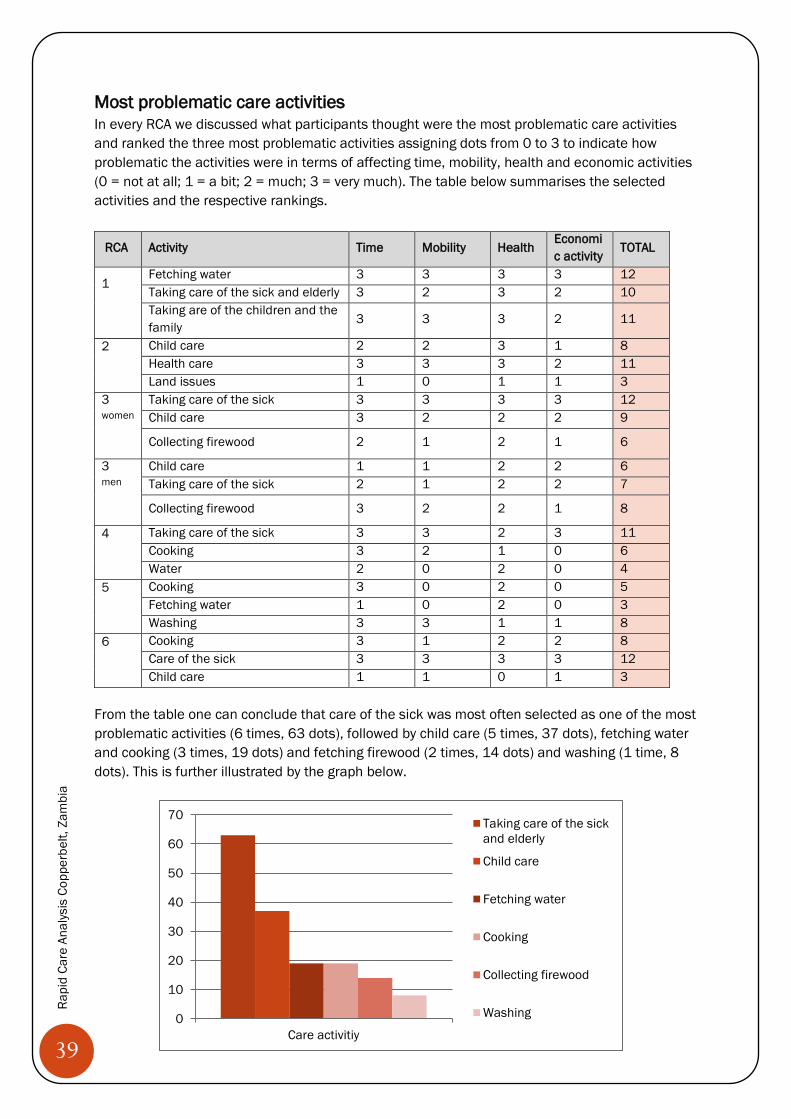
39
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Most problematic care activities
In every RCA we discussed what participants thought were the most problematic care activities and ranked the three most problematic activities assigning dots from 0 to 3 to indicate how problematic the activities were in terms of affecting time, mobility, health and economic activities (0 = not at all; 1 = a bit; 2 = much; 3 = very much). The table below summarises the selected activities and the respective rankings.
RCA Activity Time Mobility Health Economic activity
TOTAL
1
Fetching water 3 3 3 3 12 Taking care of the sick and elderly 3 2 3 2 10 Taking are of the children and the family
3 3 3 2 11
2
Child care 2 2 3 1 8 Health care 3 3 3 2 11 Land issues 1 0 1 1 3
3 women
Taking care of the sick 3 3 3 3 12 Child care 3 2 2 2 9
Collecting firewood 2 1 2 1 6
3 men
Child care 1 1 2 2 6 Taking care of the sick 2 1 2 2 7
Collecting firewood 3 2 2 1 8
4
Taking care of the sick 3 3 2 3 11 Cooking 3 2 1 0 6 Water 2 0 2 0 4
5
Cooking 3 0 2 0 5 Fetching water 1 0 2 0 3 Washing 3 3 1 1 8
6
Cooking 3 1 2 2 8 Care of the sick 3 3 3 3 12 Child care 1 1 0 1 3
From the table one can conclude that care of the sick was most often selected as one of the most problematic activities (6 times, 63 dots), followed by child care (5 times, 37 dots), fetching water and cooking (3 times, 19 dots) and fetching firewood (2 times, 14 dots) and washing (1 time, 8 dots). This is further illustrated by the graph below.
0
10
20
30
40
50
60
70
Care activitiy
Taking care of the sickand elderly
Child care
Fetching water
Cooking
Collecting firewood
Washing
40
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
1) Taking care of the sick Looking after the sick and elderly was chosen as the most problematic activity because of high number of illnesses and a lack of access to health facilities.
2) Child care Child care was considered the second most problematic care activity, especially when children are very young, sick (woman, RCA 4) or “when they are fighting” (woman, RCA 1).
The main issue making child care difficult was that schools were very far and expensive. Accompanying children to school was said to take up time and to affect health (woman, RCA 2). Letting children walk to school on their own was also said to affect one’s health because of the fear that something could happen. Similarly, planning for school fees was said to cause stress.
“At home there is a sick person. I don’t have much time. I want to go somewhere but I just stay at home, so other activities are affected.” (Woman, RCA 1)
“You cannot leave a sick or elderly person with a small child, so you cannot leave the house.” (woman, RCA 1)
“When you have a sick person you cannot go to the field and cultivate, to do something,. The mind will be just at home with the person you left.” (woman, RCA 1)
“It also affects us health wise because if a person is sick you cannot do anything, you are stressed too much.” (woman, RCA 3)
“When you have a patient and the clinic is far you are being affected with you economic activities.” (man, RCA 2)
“Even three dots doesn’t count how much we are affected.” (woman RCA 2)
“If the child is sick you are not doing anything else, you will just take care of the child.” (woman, RCA 4) “We are being affected because if a child is sick you as a mother also get sick, you can’t do anything,” (woman, RCA 3) “Child care is very difficult, it takes a lot of time, you cannot leave the baby alone.” (woman, RCA 3) “It is very difficult taking care of the child, you cannot sleep maybe the body temperature has risen, maybe the child is crying you don’t know what to do.” (woman, RCA 3)
“Because the school is far it prevents me from doing other activities because I have to take the children to school.” (woman, RCA 2) “It has affected the health because the school is very far you have to carry the child.” (woman, RCA 2) “The child is not with you and you don’t know what is happening to the child, so you cannot concentrate.” (woman, RCA 2) “When a child comes to another grade it becomes a challenge because you start wondering how you are going to sponsor that child. You won’t be sleeping, you keep thinking: ‘how am I going to care for them?’” (woman, RCA 1)
41
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Interestingly, men often said that child care affected mobility and economic activities, while women said that it did not. For example a man said: “You are delayed for an economic activity because you first have to look after the children” (RCA 6) and a woman said “mobility is not affected, you just put the baby on the back and then you go.” (RCA 3). 3) Cooking Cooking was considered a problem because it had to be done very often (woman, RCA 4) and was said to affect health (woman, RCA 4).
4) Fetching water Fetching water was selected as one of the most problematic activities because of the large distances to water sources, limited access to boreholes and a lack of water in the dry season (RCA 1, 2). Fetching water was also said to affect health by causing chest pains (woman, RCA 4). There was a debate about whether fetching water affected mobility or not.
People agreed that water was also a critical issue for the soya and dairy value chains. For example a woman said: “They gave us soya beans and water was very difficult.” (RCA 1) and another one said: “Because of water keeping livestock becomes a challenge.” (woman, RCA 1). 5) Fetching firewood Collecting firewood was considered a challenge because of large distances, poor transport and land being divided into farms. Participants also talked about potential snake bites when picking up the wood and cuts when splitting it. Furthermore, they mentioned potential dangers for women collecting firewood on their own in the bush.
“Because we have to cook in the morning, in the afternoon and in the evening. At what time can we be mobile?” (woman, RCA 4) “If you are always by the fire cooking you can be burned,” (man, RCA 4) “Your eyes are affected by the smoke.” (woman, RCA 6) “Cooking affects economic activities. You want to take vegetables from the garden to sell and then your husband says: ‘I want food’, Then when you go to the market your customers have already bought the vegetables from someone else.” (woman, RCA 6)
“Fetching water is very difficult. It might take two hours to fetch water because of the distance to and from the water source.” (Man, RCA 1).
“Where we go and fetch water it is very far, sometimes it is first comes first serves, it is very difficult.”(woman, RCA 2)
“Some communities don’t have boreholes, it is very far.” (Male youth, RCA 1)
“There is a small river, where I am staying but when it is raining like this, it is not safe.” (woman, RCA 2)
42
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Other non-care activities that participants considered problematic were:
x receiving inputs from the project late (man, RCA 2) x land related struggles and uncertainties (man, RCA 2) x “looking after dairy animals” (woman, RCA 1)
Available infrastructure and services for care work In the community map exercise, participants listed the following types of available infrastructure, equipment and services that helped them with care work:
x Basic school (RCA 2, 6) x Community school (RCA 2) x Nursery school (RCA 2) x Orphanage (RCA 2) x Camp extension officer /agricultural assistance (RCA 6) x Church (RCA 2, 6) x Neighbours (RCA 6) x Cooperative (RCA 2) x Health post (RCA 6) x Home based care and community health workers (RCA 6) x Crop fields (RCA 6) x Storage shed (RCA 2) x Hammer mill (RCA 2) x Well (RCA 6) x Roads (RCA 6) x Market (RCA 6)
“There is no good transport, so they carry things on their heads and the markets are very far.” (male youth, RCA 1) “ “Where we go to collect firewood it is very far and we usually go to collect firewood twice a week.” (woman, RCA 3) “Collecting firewood is very difficult for me because it is far and very dangerous going alone in the field.” (woman, RCA 3) “When we put the firewood on the head we have a problem. Maybe a snake has gone in the firewood, so we pick it up together and it can bite you.” (woman, RCA 3) “The axe we are using to cut the logs it sometimes hits us.” (woman, RCA 3) “The area has been divided into farms. If you stray into someone else’s farm you can be arrested.” (woman, RCA 6)
43
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Solutions and ideas Following the ‘care diamond’ that shows that care work should be recognised, redistributes and reduced at household, state, civil society and market level (see page 12), we brainstormed solutions at the four different levels. Household level Participants mentioned two main solutions at the household level. Working together as a family
x Sharing responsibilities between husbands and wives, including care work (RCA 4, 5, 6) x “Helping one another if one is not feeling ok” (RCA 1) x Planning and agreeing on who does what (woman, RCA 2, 4, 5) x Develop duty roster for care work at home (man, RCA 4) x Dialogue, educating one another, being open, asking others for help with work (RCA 3, 4) x Open discussions about care work encouraged by a man (RCA 3) x Men taking a leading role in redistributing care work (RCA 1, 3, 4) x Both parents teaching boys and girls to do care work (RCA 4, 5, 6)
Involving the community
x Changing culture/traditions so that men can also do care work (RCA 1) x Men taking a leading role in changing culture (RCA 1) x Teaching other men to help their wives (man, RCA 3) x Come together as a community to demand schools and hospitals (RCA 2)
”It is important to share responsibilities, for example when the women gets water I do cultivation so that our investment is not affected.” (man, RCA 5)
“We should leave time for women to do other work, productive work and she also needs to relax.” (man, RCA 1) “We have children, a man washing people should not say ‘she is abusing him’. He should also do it, against the culture.” (woman, RCA 1)
“A girl and a boy child should be raised as one, both of them should do the same, we should also tell the boy child to do the work, so that the girl child can concentrate.” (man, RCA 2)
“The parents should lead an example. They should be the first ones to share responsibilities. If I don’t fetch firewood, get water how can I tell my son to fetch firewood and water?”( man, RCA 5) “We should go out there and teach people, we should take the leading role in changing the culture.” (man, RCA 1)
“We must work against traditions that are not helpful, women having to do care work is a negative tradition,, we should share.” (man, RCA 4)
“Us men we should take a lead in changing things. We don’t realise that the care work is over burdening,” (man RCA 3) “All us men, especially us who are leaning this training we should go out there and disseminate the information to everyone that it is too much, we need to take a lead so that women can also relax.” (man, RCA 3)
44
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
State level Generally, participants agreed that the government should provide:
x Health care centres/ clinics/ hospitals and health care staff (RCA 1, 2, 3, 4, 5, 6) x Boreholes (RCA 1, 2, 3, 4, 5, 6,) x Government schools and teachers, especially secondary schools (RCA 1, 2, 3, 4, 5, 6) x Roads and bridges (RCA 1, 2, 4, 5, 6) x Electricity (RCA 4, 5, 6) x A police post (RCA 2, 4, 6) x Houses for service providers (RCA 4,5) x Ploughs (RCA 4) x A hammer mill (RCA 5) x Solar energy (RCA 5) x Elderly homes (RCA 3) x Orphanage (RCA 6) x Support such as food, groceries (RCA 3) x Markets (RCA 2)
Participants also mentioned that the government should:
x Introduce a policy so that bars open later (woman, RCA 2) x Pass policies for land security (RCA 2) x Train home based care givers (RCA 3) x Raise awareness on gender equality/ implement women’s empowerment programmes
(woman, RCA 4, man, RCA 5)
Schools “Children walk about 8 km to the school.” (woman, RCA 1) “There were teachers sent here but because the schools are not very good the teachers don’t come to teach. Teachers don’t want to move here because the houses are not very good and there is no electricity.” (man, RCA 5) “Currently there are no secondary school so pupils go on Monday and come back on Friday and they are unsupervised. There are no boarding schools.” (woman, RCA 6) Clinics “The health centre from South Down is very far. They have closed a clinic because no one wanted to work there because it is quite in the bush.” (man, RCA 1) “In Kakolo B, we don’t have a clinic, the nearest requires that you cycle for 15-20km.” (man, RCA 2) “If there could be a clinic and more health services. At the moment we have to walk to Kalulushi which is 20km, even if it is at night-“ (RCA 6) Electricity “The state should bring electricity here. Sometimes it is very dark. It would be easier to store perishable things in the fridge and there would be enough light during the night to cook.” (woman, RCA 4)
45
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Civil society level Solutions at civil society level included trainings, advocacy and direct support. Trainings
x Sensitising/ training/ awareness on care work for husbands and wives (RCA 1, 4, 5, 6) x Awareness on care work in schools/ lobbying to include care work in school curriculum
(RCA 4, 5)/ teaching children about care work (RCA 4)/ conducting the RCA at schools (RCA 3)
x Supporting home based care (RCA 1, 3) x Educating people not to drink beer (RCA 3)
Advocacy
x Lobbying and advocacy for state services (RCA 1) x Lobbying for quality health and education facilities (RCA 6) x Lobbying to get secure land (RCA 2) x Working together with the Government and churches (RCA 5)
Direct support x Promoting gas stoves so that people stop using charcoal and firewood (RCA 5) x Providing bicycles and treadle pumps (RCA 1) x Giving out farming loans (RCA 2)
Roads “Another thing we want the government to look at are the roads. The roads are very bad and vehicles can’t come through.” (woman, RCA 4) Markets “The government should bring in markets, bigger markets in the community so that we can start selling our products and then when we have a lot of money we can hire someone to do the work.” (woman, RCA 4) ”It is two hours walking to the market and you are carrying a luggage on your head so it is quite a challenge.” (woman, RCA 2) Water “Clean water, boreholes, this time we are drinking dirty water and this affects our health and the stomachs, we want to drink clean water.” (woman, RCA 5) Police post “We need a police post so that there is security in our community and that there will be less theft.” (man, RCA 6) Hammer mill “Bring a hammer mill nearby, we take the maize very far, 3-4 hours to go and come back and sometimes when we go there we find out that there is no electricity and we start waiting.” (woman, RCA 5)
46
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
x Looking after orphans and elderly (RCA 6) x Helping families with children (RCA 2) x Initiating and supporting early childhood education classes/ pre-schools (RCA 6) x Organising football clubs for youth (RCA 3) x Taking over some of the work (RCA 3, 4)
Market level The market level was mainly understood in terms of time and labour saving equipment. The solutions included: Cooking equipment
x Hammer mill for maize (RCA 4, 6) x Hand mill for maize (RCA 6) x Fuel efficient stove (RCA 4, 5, 6) x Paraffin stoves (RCA 1, 3) x Solar stoves (RCA 3) x Food warmers (RCA 4) x Tila lamo lamp (for cooking at night) (RCA 3)
Water equipment
x Hand pump for water (RCA 3, 4, 6) x A near-by well or borehole (RCA 5) x Wind mill (RCA 4) x Water tanks/drums (RCA 3,6) x Wheelbarrow (for fetching water) (RCA 3) x Basins to wash in and washing paste (RCA 3)
Shops/ markets
x A market to sell products (RCA 5) x Shop for mealie meal (maize flour) (RCA 6) x Pharmacy for selling drugs (RCA 6)
Child care related equipment
x Bicycles, mosquito nets, beddings, school uniforms, balls, dolls (RCA 3) Although facilitators emphasised that we were looking at equipment reducing time spent on care work, participants often talked about farm related equipment:
x Sheller for soya beans (RCA 1, 2) x Planter for soya beans (man, RCA 1) x Walking tractor (RCA 1) x Fertilisers, weed killers, chemicals (RCA 1, 3) x Milk coolers (RCA 4) x Shovel, hoes, axes, slathers (RCA 3)
Usually women mentioned more equipment related to care work and men talked more about farm related equipment. The types of equipment that were mentioned most often were: Fuel efficient
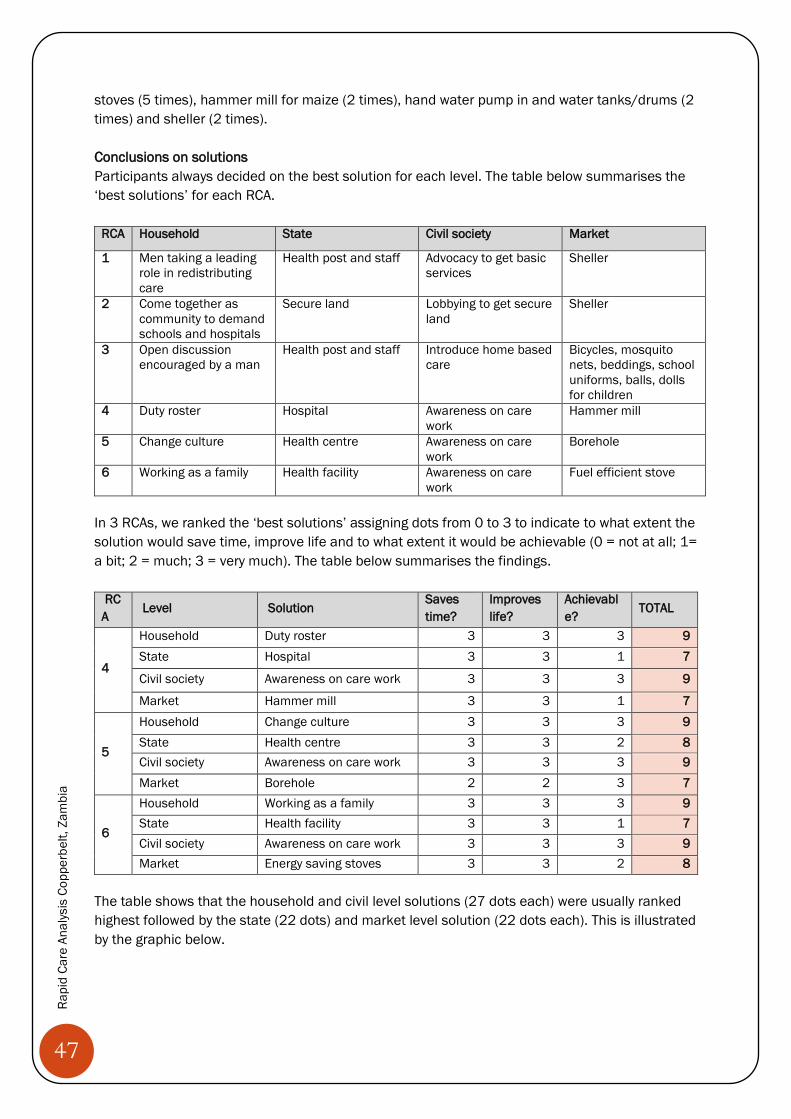
47
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
stoves (5 times), hammer mill for maize (2 times), hand water pump in and water tanks/drums (2 times) and sheller (2 times). Conclusions on solutions Participants always decided on the best solution for each level. The table below summarises the ‘best solutions’ for each RCA.
RCA Household State Civil society Market
1 Men taking a leading role in redistributing care
Health post and staff Advocacy to get basic services
Sheller
2 Come together as community to demand schools and hospitals
Secure land Lobbying to get secure land
Sheller
3 Open discussion encouraged by a man
Health post and staff Introduce home based care
Bicycles, mosquito nets, beddings, school uniforms, balls, dolls for children
4 Duty roster Hospital Awareness on care work
Hammer mill
5 Change culture Health centre Awareness on care work
Borehole
6 Working as a family Health facility Awareness on care work
Fuel efficient stove
In 3 RCAs, we ranked the ‘best solutions’ assigning dots from 0 to 3 to indicate to what extent the solution would save time, improve life and to what extent it would be achievable (0 = not at all; 1= a bit; 2 = much; 3 = very much). The table below summarises the findings.
RCA
Level Solution Saves time?
Improves life?
Achievable?
TOTAL
4
Household Duty roster 3 3 3 9 State Hospital 3 3 1 7
Civil society Awareness on care work 3 3 3 9
Market Hammer mill 3 3 1 7
5
Household Change culture 3 3 3 9 State Health centre 3 3 2 8 Civil society Awareness on care work 3 3 3 9 Market Borehole 2 2 3 7
6
Household Working as a family 3 3 3 9 State Health facility 3 3 1 7 Civil society Awareness on care work 3 3 3 9 Market Energy saving stoves 3 3 2 8
The table shows that the household and civil level solutions (27 dots each) were usually ranked highest followed by the state (22 dots) and market level solution (22 dots each). This is illustrated by the graphic below.
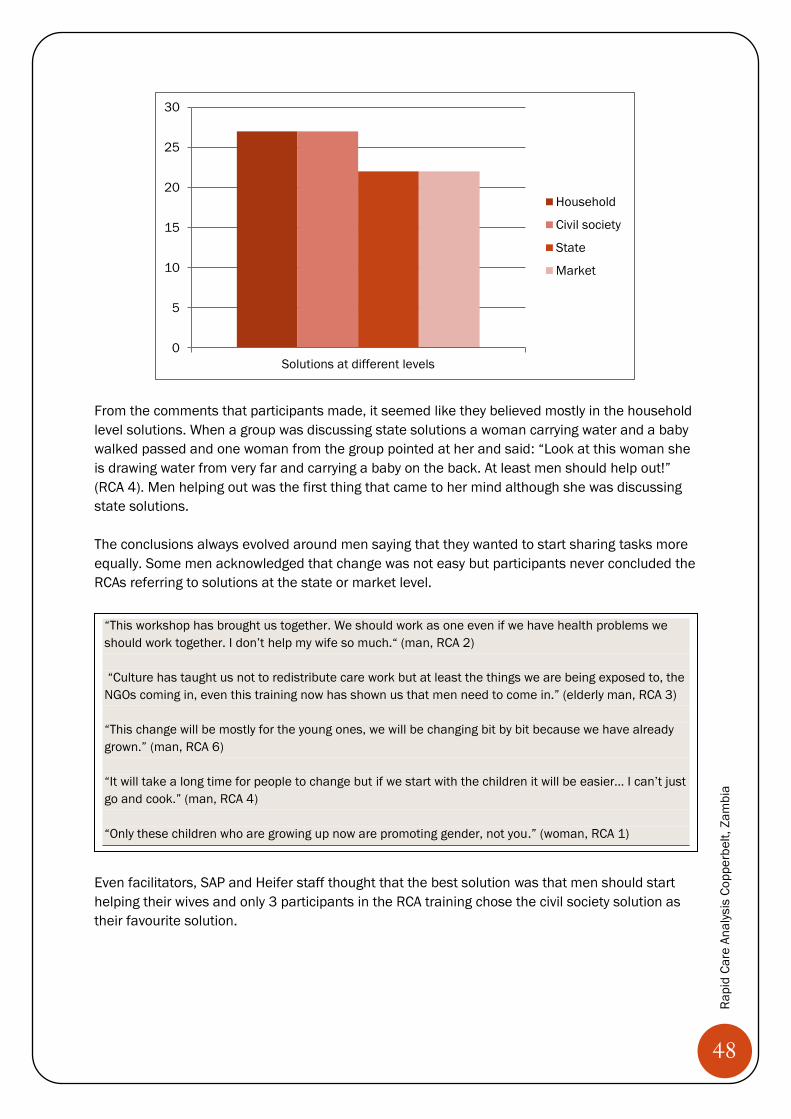
48
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
From the comments that participants made, it seemed like they believed mostly in the household level solutions. When a group was discussing state solutions a woman carrying water and a baby walked passed and one woman from the group pointed at her and said: “Look at this woman she is drawing water from very far and carrying a baby on the back. At least men should help out!” (RCA 4). Men helping out was the first thing that came to her mind although she was discussing state solutions. The conclusions always evolved around men saying that they wanted to start sharing tasks more equally. Some men acknowledged that change was not easy but participants never concluded the RCAs referring to solutions at the state or market level.
Even facilitators, SAP and Heifer staff thought that the best solution was that men should start helping their wives and only 3 participants in the RCA training chose the civil society solution as their favourite solution.
0
5
10
15
20
25
30
Solutions at different levels
Household
Civil society
State
Market
“This workshop has brought us together. We should work as one even if we have health problems we should work together. I don’t help my wife so much.“ (man, RCA 2) “Culture has taught us not to redistribute care work but at least the things we are being exposed to, the NGOs coming in, even this training now has shown us that men need to come in.” (elderly man, RCA 3) “This change will be mostly for the young ones, we will be changing bit by bit because we have already grown.” (man, RCA 6) “It will take a long time for people to change but if we start with the children it will be easier… I can’t just go and cook.” (man, RCA 4) “Only these children who are growing up now are promoting gender, not you.” (woman, RCA 1)
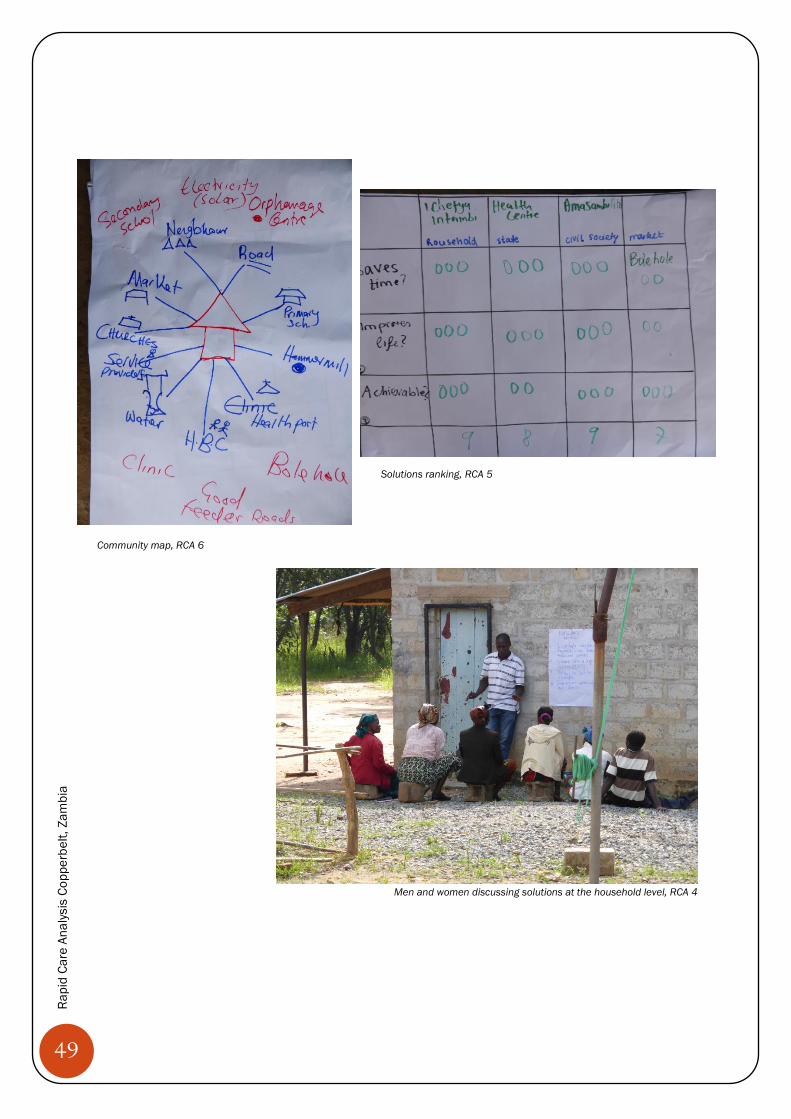
49
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Solutions ranking, RCA 5 Solutions ranking, RCA 5 Community map, RCA 6
Men and women discussing solutions at the household level, RCA 4
50
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Participation, interactions and feedback Many women and men were engaged in the discussions, although a few participants usually said more and a few said less. Elderly men were usually rather quiet but there were a few who participated vividly. Usually there were 1-2 men in their 30-40s in each RCA who dominated the discussions and often talked passionately about men having to change. There was only one group in which women did not speak up much, but in all other groups they expressed their views confidently, even when their husbands were in the same room. There was one situation in which a wife seemed intimidated by her husband. The husband, a very dominant man, said that his wife would not want him to help her. The wife, a very young woman, was asked whether this was true. Everyone laughed and seemed excited. The woman stood up and repeated exactly what her husband had said, even using the same words: “ I refuse to be helped” (woman, RCA 2). It seemed to be a common pattern that men participated more when we talked about infrastructure and state services and that women were more engaged in questions related to care work (e.g. equipment for care work, problems of care work). When men said that they did not do care work or that caring roles were given by ‘culture’, ‘tradition’ or ‘God’, participants often started laughing. When participants said that tasks should be shared more equally, the group often applauded loudly. Participants often said that they would have benefitted more from the RCA if their spouses had also participated.
Some participants proposed to conduct the RCA with all producer groups or to conduct trainings on the issue. One man said: “You should have taught us about this much earlier! Then we would have shared responsibilities much earlier and our daughters would be engineers by now!” (RCA 4)
“Why did you not call us as couples? Even if I went home and started explaining this it would not make any difference.” (woman, RCA 5) “It is even worse if I go home and tell him we have to share care work. This will even bring more problems.” (woman, RCA 5) “If it was husband and wife this training would helped but if it is just me alone my wife will be confused.” (man, RCA 4)
51
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
PART 4
CONCLUSIONS AND RECOMMENDATIONS
Women and men in RCA 6 discussing the most problematic care activities

52
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Recommendations for the GEM project The findings show that care work affects women’s participation in the project and hence emphasise the importance of addressing care work in the project. Based on the RCA findings and discussions with different Oxfam and partner organisation staff, we propose the following recommendations:
1. Include some RCA exercises in the pre-trainings for new producer groups Participants often proposed to conduct the RCA with all producer groups. If there is no capacity to add an extra day to the exiting trainings, some RCA exercises can easily be integrated in existing pre-trainings, such as in the gender training (e.g. one-day recall, age and care distribution) or the agricultural or business plan training (e.g. seasonal calendar and a shortened versions of the most problematic activities and solutions). Referring to care work in several trainings will help to promote it as a cross-cutting rather than ‘just as a gender issue’. Integrating RCA exercises in the baseline training can raise awareness about the issue, generate data on care in the community at the start of the project intervention and it can provide relevant information for improving the value chain work (e.g. about timing for training, special support required). Based on the suggestions of several participants, I propose to conduct the exercises with couples. It might also be useful to invite a few children of producer group members, especially because working with youth was a suggestion brought forward by several community members. Heifer already conduct some of the training units with couples and their oldest children and it might be an idea to include RCA exercises in these trainings.
2. Improve access to fuel efficient stoves and/or water, shellers and hammer mills Fuel efficient stoves were mentioned as a priority in five out of six RCAs (RCA 1, 3, 4, 5, 6) and two groups ranked it their best market level solution. Especially with deforestation and land conflicts, fetching firewood has become more problematic. Participants said that fuel efficient stoves would reduce the time women spend on collecting firewood and the negative effects of fumes on health (RCA 6). In RCA 6, I asked who owned a fuel-efficient stove and no one raised their hands. Participants agreed that the “technology is here but the people who know how to build the stoves are few.” (man, RCA 6). As the stoves do not require much material (mainly cement), training people on how to make the stoves would probably be sufficient. This could be done in collaboration with other NGOs or the private sector already involved in constructing fuel efficient stoves. Fetching water for washing, cooking and cleaning was said to take up much time and energy, especially in the dry season. More than that, water is essential for the dairy and soya value chains, for instance participants reported having difficulties getting enough water for their cows. Water borne diseases were also often mentioned when talking about care of the sick which was by far the most problematic and most time-consuming care activity. Constructing boreholes was one of the main priority for state intervention in all RCAs. Water related equipment was also considered important by community members. Three groups proposed to get hand water pumps (RCA 3, 4, 6) and two groups advocated for water tanks/drums (RCA 3,6). Advocacy for state support with water supply would not only reduce care work but would also directly benefit the value chains. Other interventions would be to improve access to shellers for soya beans (proposed in RCA 1, 2)
53
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
and/or hammer mills for maize (proposed in RCA 4, 6). The sheller was ranked the best solution in two groups (RCA 1, 2) because “the production (of soya beans) is so involving”” (woman, RCA 1). The hammer mill was also considered very important because” without food you don’t have energy and you can get all kinds of diseases. You cannot do care work or any other work in the home.” (man, RCA 4). Advocacy for state support with hammer mills or linking up with Astral holdings who is promoting the soya value chain for the shellers would be an idea.
3. Advocacy for state services A lack of infrastructure and basic services seemed to be the main issue causing long hours of care work for women. A lack of health clinics was especially problematic as it increased the time women spent on caring for sick people, which was the most problematic care activity in most groups. A lack of secondary schools, boreholes and road networks were similarly problematic. The findings from the RCA (e.g. numbers of hours spent on care work, most problematic care activity ranking, quotes on specific types of care work and infrastructure) could be used to emphasise the importance and urgency of state support with providing basic infrastructure and services.
4. Introduce group-based health care support system Caring for sick people was by far the most problematic care activity taking up much of women’s and men’s time and affecting their engagement in the value chains. Health clinics would improve the situation drastically but in the short-run it might be useful to introduce a peer support system. Several participants proposed to introduce home based care systems which have been established in some areas by several NGOs. However, in these systems the home based care workers are usually women which perpetuates women’s role as carers and increases their workloads. It might be useful to combine home-based care training with RCA exercises and it would be important to involve men in such initiatives. This was also confirmed by RCA participants shouting loudly: “everyone, male or female should be involved in home based care!”(RCA 3). It would also be essential to make sure that the initiative would not impose an extra burden on participants, for example through introducing compensation for home based carers in the form of payment or support with care or cultivation work by community members. It would be useful to work together with other NGOs implementing home based care systems. For instance, SAP has previously worked together with World Vision on training people to provide medical care from home. Instead of establishing a new system it might be more effective to work with other NGOs and raise awareness about care at the same time. Recommendations for including care work in other projects
1. Integrate care work and RCA in “I Care About Her Campaign” The ‘ I care about her campaign’ works with men to address violence against women. Oxfam and partners have identified about 50-100 male champions (also incl. police men) in different regions in Zambia who conduct exercises with male community members. The exercises are based on 17 cards addressing the topics: Violence statistics, forms of violence, how are men viewed by women?, human rights, parenting of boys, parenting of girls, myths about rape, beliefs about wife beating, property grabbing, the role of women in perpetuating violence and gender inequality, the effect of violence on men, what do you want your daughter to become?, steps of action.
54
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Together with Ms Misozi Tembo and Mr Mutinta Twaambo who work on the ‘I care about her campaign’, we came up with the following ideas on how care work can be integrated into the ‘I care about her campaign’:
1. Training the champions on care work, potentially through conducting an RCA. It would be helpful to ask them to bring their wives and their oldest daughters or sons, so that we can collect the hours people from different age and gender groups spend on different types of activities. The champions can use the findings from the RCAs for their exercises with community members. It might be useful to create some materials (such as the age and care graphs for females and males) that can be shared with community members.
2. Adding a card on care work. This card can be based on the RCA exercises. It would be interesting to look at the effect of unequal and heavy care work on girls’ school performance (age and care exercise) and on women’s economic activities (seasonal calendar exercise). It would also be useful to frame care work as a development (positive sides of care work exercise) and to discuss what type of care work is most problematic (most problematic activities exercise). The card can then be used by the champions to discuss the issue with community members. As planned for the other cards, it would help to produce a brochure on the topic for participants to take home and share.
3. Integrating care work into other cards/ exercises. Several of the topics are linked to care work and it would be fruitful to make this link explicit in the discussions. This applies in particular to exercises on human rights, parenting of boys, parenting of girls, what do you want your daughter to become, the role of women in perpetuating violence/gender inequality and steps of actions.
4. Addressing care work in a TV discussion. Care work could also be a topic in one of the TV discussions as part of the campaign in which ‘exemplary men’ talk about a topic of one of the cards on TV. The show could raise awareness about the positive sides of care work as well as about the negative effects if care work is heavy and unequal. It would also be useful to introduce the care diamond, emphasising that care work should be addressed at household, civil society, market and state level. The TV show can also be used to advocate for state support with care work.
5. Record and share testimonial on care work. As part of the new ‘I care about her campaign’ strategy testimonials of ‘exemplary men’ will be recorded. The testimonials will be broadcast during the TV discussions and through local radio stations and they will also be shown during community discussions. These testimonials could also address care work and convey the message that doing care work is not in contradiction with meeting expectations of ‘masculinity’.
2. Integrate care work and RCA in new education project
The age and care exercise showed that gender roles become internalised at a young age and that they are reinforced by parents assigning ‘female’ tasks to girls and ‘male’ tasks to boys. Several participants in the RCA proposed to raise awareness about care work at schools and to include care work in the school curriculum. The GEM project is not targeting students but it would be possible to work together with the education project. The new EU funded education project works on improving community schools in the Eastern province and Copperbelt region (Mufulira district). It improves school infrastructure, trains
55
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
teachers and also includes a component on education of girls. This component involves community discussions, child club trainings and reintegrating young mothers into school. Together with Mr James Kayamba (Project Officer Education), we propose the following initiatives to integrate care work into the education project:
1. Conduct parts of the RCAs with students, especially the one-day recall and age and gender exercise to collect data on how many hours girls and boys spend on care work.
2. Use the findings from the RCA for community and child club discussions to emphasise the importance of distributing care work, especially to improve girls’ school performance.
3. Advocate for school policies that assign care work at school to both boys and girls (such as sweeping/cleaning the school).
4. Advocate for changes in the school curriculum and materials so that both men and women are represented as carers and care work is addressed in class.
3. Consider the care calendar in project design and execution
As the seasonal calendar has shown that care work and value chain work are at their peak at the same time, it would be useful to consider the seasonal care calendar in project planning and execution. The care calendar could be considered when selecting suitable value chains. Measures to assist people with care or cultivation work in the most intense months could be thought of from the start of the project and RCAs, trainings, research or other meetings should ideally be held in months when care work and value chain work are not particularly high. As part of raising awareness on care work in project design and implementation, Ms Lomthunzi Jere proposed to conduct an RCA with Oxfam staff and to include knowledge of care work in trainings and job descriptions. Recommendations for conducting the RCA The following recommendations for future RCAs can be concluded from the Zambian experience. Framing Several participants and facilitators said that they were positively surprised that the RCA was ‘not just another gender training’. They said that people would respond better if care was framed as a ‘development’ rather than a ‘gender’ issue. We tried to follow this advice during RCAs by stressing the care diamond, but discussions were still quite ‘household level’ focussed. It also seemed like some people understood the RCA as an ‘awareness raising tool’ rather than a ‘research tool’. How to best frame the RCA is an important question to consider. Training It was helpful to work with people from different organisations in the training and to ask participants to conduct the exercises with the rest of the group. Preparing country specific guidelines that explained the different steps seemed useful. Exercises 1) Introduction: Collecting types of care work before showing the ‘global care categories’ worked
well. We also asked people to brainstorm the positive and negative sides of care work. This triggered very interesting discussions and clarified why we were talking about care work.
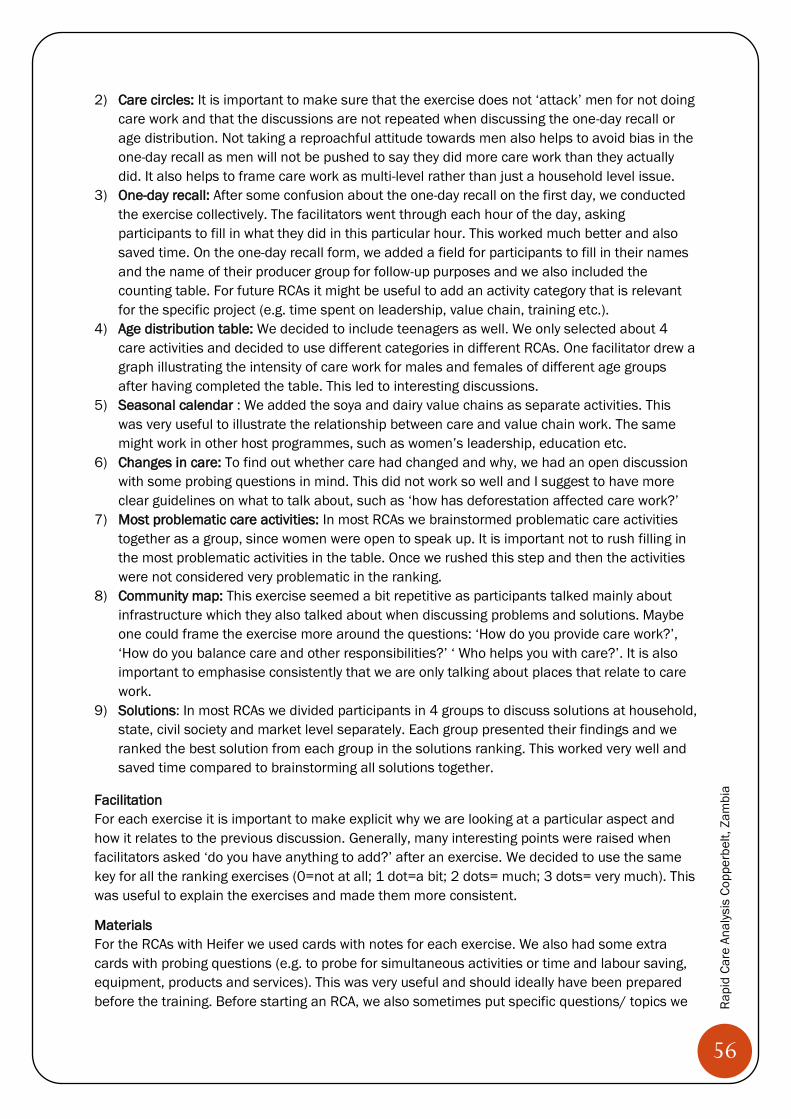
56
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
2) Care circles: It is important to make sure that the exercise does not ‘attack’ men for not doing care work and that the discussions are not repeated when discussing the one-day recall or age distribution. Not taking a reproachful attitude towards men also helps to avoid bias in the one-day recall as men will not be pushed to say they did more care work than they actually did. It also helps to frame care work as multi-level rather than just a household level issue.
3) One-day recall: After some confusion about the one-day recall on the first day, we conducted the exercise collectively. The facilitators went through each hour of the day, asking participants to fill in what they did in this particular hour. This worked much better and also saved time. On the one-day recall form, we added a field for participants to fill in their names and the name of their producer group for follow-up purposes and we also included the counting table. For future RCAs it might be useful to add an activity category that is relevant for the specific project (e.g. time spent on leadership, value chain, training etc.).
4) Age distribution table: We decided to include teenagers as well. We only selected about 4 care activities and decided to use different categories in different RCAs. One facilitator drew a graph illustrating the intensity of care work for males and females of different age groups after having completed the table. This led to interesting discussions.
5) Seasonal calendar : We added the soya and dairy value chains as separate activities. This was very useful to illustrate the relationship between care and value chain work. The same might work in other host programmes, such as women’s leadership, education etc.
6) Changes in care: To find out whether care had changed and why, we had an open discussion with some probing questions in mind. This did not work so well and I suggest to have more clear guidelines on what to talk about, such as ‘how has deforestation affected care work?’
7) Most problematic care activities: In most RCAs we brainstormed problematic care activities together as a group, since women were open to speak up. It is important not to rush filling in the most problematic activities in the table. Once we rushed this step and then the activities were not considered very problematic in the ranking.
8) Community map: This exercise seemed a bit repetitive as participants talked mainly about infrastructure which they also talked about when discussing problems and solutions. Maybe one could frame the exercise more around the questions: ‘How do you provide care work?’, ‘How do you balance care and other responsibilities?’ ‘ Who helps you with care?’. It is also important to emphasise consistently that we are only talking about places that relate to care work.
9) Solutions: In most RCAs we divided participants in 4 groups to discuss solutions at household, state, civil society and market level separately. Each group presented their findings and we ranked the best solution from each group in the solutions ranking. This worked very well and saved time compared to brainstorming all solutions together.
Facilitation For each exercise it is important to make explicit why we are looking at a particular aspect and how it relates to the previous discussion. Generally, many interesting points were raised when facilitators asked ‘do you have anything to add?’ after an exercise. We decided to use the same key for all the ranking exercises (0=not at all; 1 dot=a bit; 2 dots= much; 3 dots= very much). This was useful to explain the exercises and made them more consistent.
Materials For the RCAs with Heifer we used cards with notes for each exercise. We also had some extra cards with probing questions (e.g. to probe for simultaneous activities or time and labour saving, equipment, products and services). This was very useful and should ideally have been prepared before the training. Before starting an RCA, we also sometimes put specific questions/ topics we
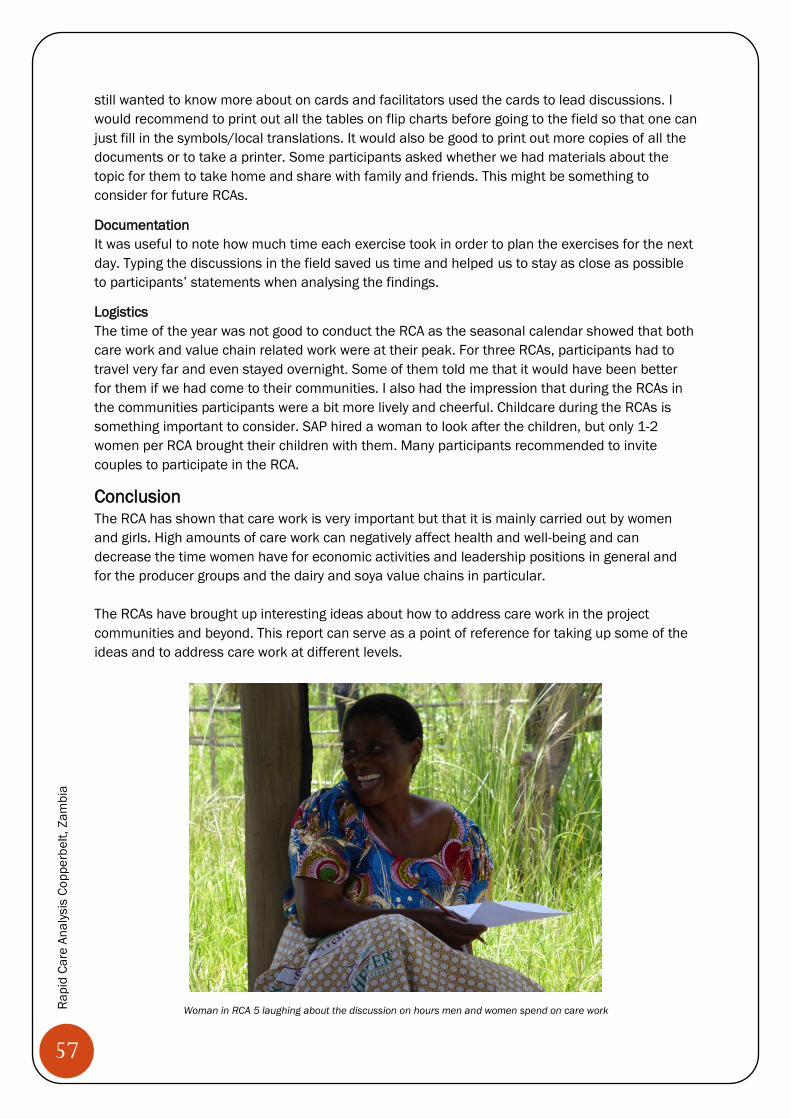
57
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
still wanted to know more about on cards and facilitators used the cards to lead discussions. I would recommend to print out all the tables on flip charts before going to the field so that one can just fill in the symbols/local translations. It would also be good to print out more copies of all the documents or to take a printer. Some participants asked whether we had materials about the topic for them to take home and share with family and friends. This might be something to consider for future RCAs.
Documentation It was useful to note how much time each exercise took in order to plan the exercises for the next day. Typing the discussions in the field saved us time and helped us to stay as close as possible to participants’ statements when analysing the findings.
Logistics The time of the year was not good to conduct the RCA as the seasonal calendar showed that both care work and value chain related work were at their peak. For three RCAs, participants had to travel very far and even stayed overnight. Some of them told me that it would have been better for them if we had come to their communities. I also had the impression that during the RCAs in the communities participants were a bit more lively and cheerful. Childcare during the RCAs is something important to consider. SAP hired a woman to look after the children, but only 1-2 women per RCA brought their children with them. Many participants recommended to invite couples to participate in the RCA.
Conclusion The RCA has shown that care work is very important but that it is mainly carried out by women and girls. High amounts of care work can negatively affect health and well-being and can decrease the time women have for economic activities and leadership positions in general and for the producer groups and the dairy and soya value chains in particular. The RCAs have brought up interesting ideas about how to address care work in the project communities and beyond. This report can serve as a point of reference for taking up some of the ideas and to address care work at different levels.
Woman in RCA 5 laughing about the discussion on hours men and women spend on care work
58
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
PART 4
APPENDICES
Man helping woman with one-day recall in RCA 4

59
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
References Budlender, D. (2007). A critical review of selected time use surveys. Gender and
Development Programme Paper 2. Budlender, D. (2008). The statistical evidence on care and non-care work across six countries.
Gender and Development Programme Paper Number 4. Chopra, D. (2013). A feminist political economy analysis of public policies related to care:
A thematic review. Institute of Development Studies: Evidence Report, 9, 1-26. Folbre, N. & Nelson, J. A. (2000). Love or money--or both?. The Journal of Economic
Perspectives, 14(4),123-140. Folbre, N. (2006). Measuring care: Gender empowerment, and the care economy. Journal of
Human Development, 7(2), 183-99. GEMSA (2010). Making Care Work Count: A Policy Handbook. Elson, D. (2008). The Three R's of Unpaid Work: Recognition, Reduction and
Redistribution. Paper presented at the Expert Group Meeting on Unpaid Work, Economic Development and Human Well-Being, UNDP, New York, November 2008.
England, P. (2005). Emerging theories of care work. Annual Review of Sociology, 3, 381- 399.
Esquivel, V. (2013). Care in households and communities: Background paper on conceptual issues. Oxfam research reports.
Eyben, R. (2013). Getting unpaid care onto development agendas. IDS in Focus Policy Briefing 31.
Fälth, A. & Blackden, M. (2009). Care work: Gender equality and poverty reduction. UN Policy Brief.
Malapit, H. J., Sproule, K., Kovarik, C., Meinzen-Dick, R., Quisumbing, A., Ramzan, F. Hogue, E. & Alkire, S. (2014). Measuring progress toward empowerment: women’s empowerment in agriculture index: Baseline report.
Open Working Group (OWG) (2014). Proposal for sustainable development goals. Retrieved from http://sustainabledevelopment.un.org/focussdgs.html
Ortiz, I & Cummins, M. (2013). The age of austerity: A review of public expenditures and adjustment measures in 181 countries. Initiative for policy Dialogue and the South Centre Working Paper.
Oxfam GB (2011). Copperbelt Livelihoods Project Effectiveness Review – Full Report Women’s Empowerment and Livelihood Support.
Razavi, S. (2007). The political and social economy of care in a development context: Conceptual issues, research questions and policy options. Geneva: UNRISD.
Serrano, M. D. (2012). Unpaid care work in Africa. Bilabao: Fundación BBVA. Tronto, J. C. (1987). Beyond gender difference to a theory of care. Signs, 12(4), 644-663. UN Women (1995). Fourth world conference on women: Beijing declaration. Retrieved from
http://www.un.org/womenwatch/daw/beijing/beijingdeclaration.html UN (2014). Unpaid work, poverty and women’s human rights. United Nations Human
Rights: office of the high commissioner for Human Rights. Woodroffe, J. & Donald, K. (2014) Unpaid care: A priority for the post-2015 development
goals and beyond. Gender and Development Network Briefings 6. Zuckerman, E. & Greenberg, M. (2004). The gender dimensions of post-conflict
reconstruction: An analytical framework for policymakers. Gender and Development, 12(3).
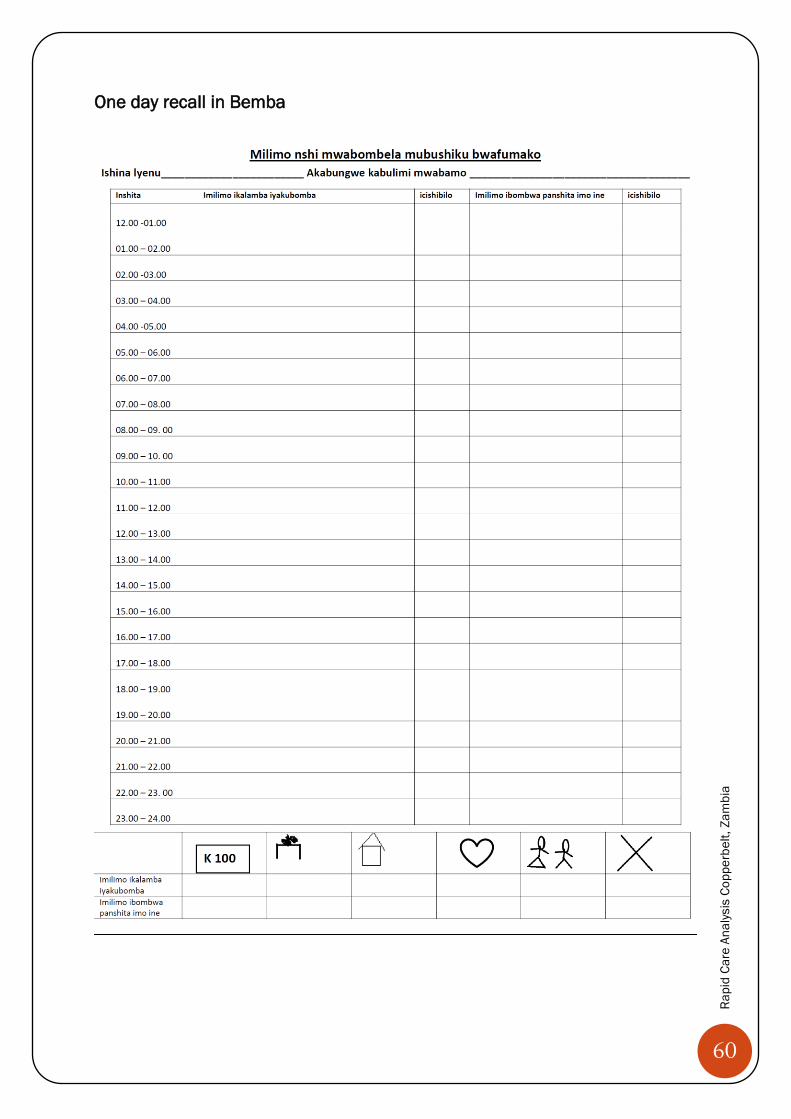
60
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
One day recall in Bemba
61
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
Attendance lists RCA 1
62
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
RCA 2
63
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
RCA 3
64
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
RCA 4
65
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
RCA 5
66
Rapi
d Ca
re A
nalys
is C
oppe
rbel
t, Za
mbi
a
RCA 6